corneal topography
TRANSCRIPT
CORNEAL TOPOGRAPHY

INTRODUCTION Cornea is the most powerful refractive
element of the eye contributing 43D(70%) of refractive power of eye.
Since the shape of corneal surface determines its refractive power , even a minor modification of its surface can lead to significant alteration of image formed on retina.
NORMAL CORNEA Prolate shape Anterior surface of cornea: Elliptical Horizontal dia: 11.5mm Vertical dia:10.6mm Posterior surface of cornea is circular with
average diameter of 11.5mm Thickness of cornea: 0.52mm at centre 0.8mm at periphery 1mm at limbus Anterior radius of curvature:7.8mm Posterior radius of curvature:6.5mm

ZONES OF CORNEA CENTRAL ZONE: Approximately 4mm
diameter. Also called the apical zone PARACENTRAL ZONE: 4-8mm diameter.
Flatter than the central zone. Central + Paracentral zone= optical
zone. PERIPHERAL ZONE: 8-11 mm. It is the
zone where the normal cornea flattens the most and becomes ashperic.
LIMBAL ZONE

Corneal topography refers to study of the shape of corneal surface
SYSTEMS TO MEASURE CORNEAL TOPOGRAPHY Placido based Elevation based Interferometric Rasterstereography Schiempflug imaging

KERATOMETRY Devised by Helmholtz,who originally
used the term ophthalmometer Calculations are based on the geometry
of a spherical reflecting surface Based on fact that anterior surface of
cornea acts as convex mirror and size of image varies with curvature
Helps to measure the radius of curvature of anterior corneal surface from 4 reflected points within central 3mm of cornea
Helmholtz keratometer Bausch and lomb keratometer Javal schiotz keratometer

OPTICAL PRINCIPAL OF KERATOMETER
I/O=v/u Since image is formed near F so v=F=r/2 therefore r can be calculated as 2uI/O Thus for known object size ,
measurement of image size will help determine radius of curvature.
In all keratometers u is constant
being focal distance of viewing telescope
To overcome the natural movements of patients eye for accurate measurements, the principle of image doubling is used.
The readings are obtained by aligning the images with one another
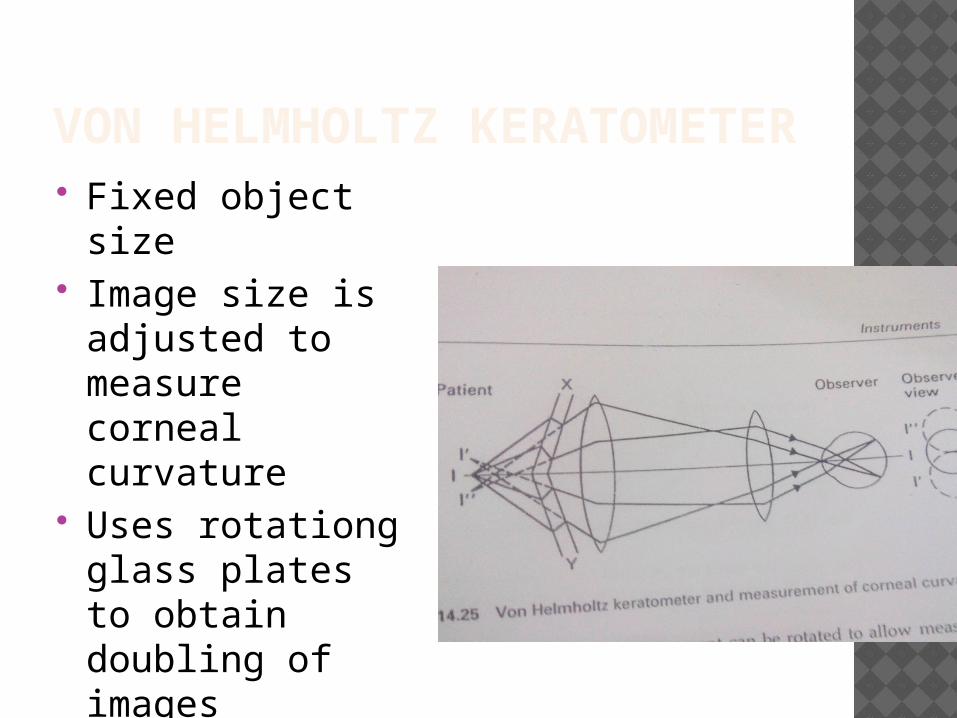
VON HELMHOLTZ KERATOMETER Fixed object size Image size is
adjusted to measure corneal curvature
Uses rotationg glass plates to obtain doubling of images

BAUSCH AND LOMB KERATOMETER Also based on
principle of constant object size and variable image size


JAVAL SCHIOTZ KERATOMETER Based on
principle of variable object and constant image size.
Doubling of image is achieved by wollaston prism

LIMITATIONS OF KERATOMERY Assumes cornea to be spherical Details of only central 3mm ignoring
peripheral corneal zones Loses accuracy when measuring very
steep or flat corneas Small corneal irregularities preclude the
use due to irregular astigmatism.

KERATOSCOPY

HAND HELD PLACIDO DISC KERATOSCOPE consists of
equally spaced alternating black and white rings with a hole in the centre to observe patients cornea.
Utilizes corneal reflections (purkinje image ) of bright rings
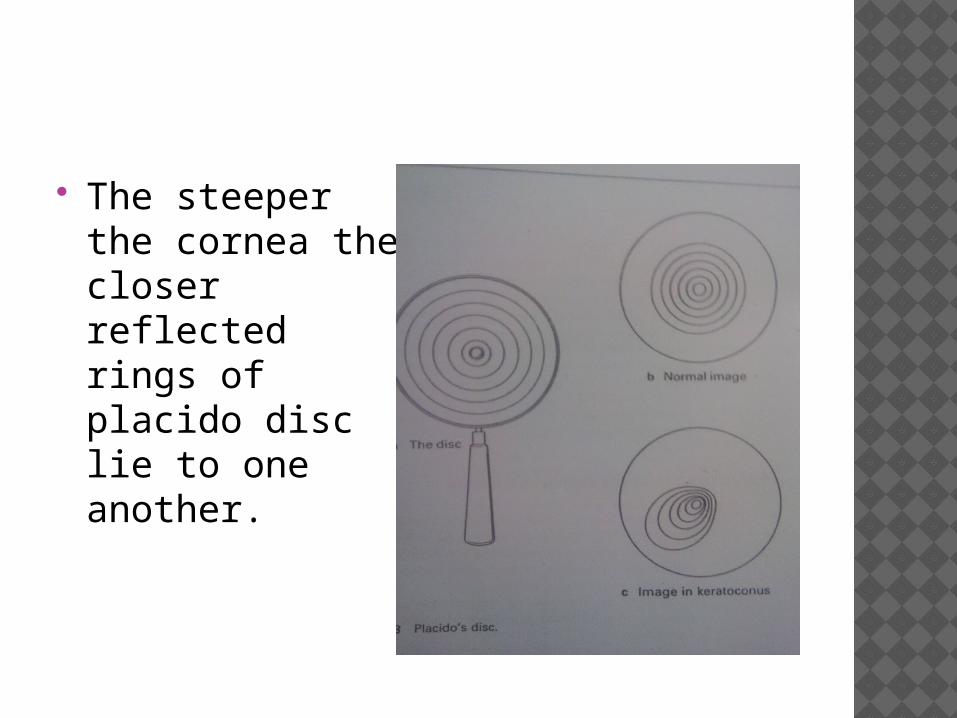
The steeper the cornea the closer reflected rings of placido disc lie to one another.

DISADVANTAGE:1. small degree of abnormality of corneal
shape are not easily identifiable.2. Cannot be used in corneas with
epithelial defects and stromal ulcers etc because of nonreflection of image by the cornea.
3. Anatomy of nose and orbit may limit field size and restrict the corneal area that can be examined

PHOTOKERATOSCOPY A photographic film camera attached to
a keratoscope. Current photokeratoscopes(eg Nidek
PKS 1000 or keracorneoscope) have 9-15 rings which cover 55-75% of corneal surface.
Closer the line steeper is the corneal surface and the farther apart the lines flatter is the corneal surface.
Corneal cylinders of upto 3D can escape detection by use of photokeratoscopy.

ORBSCAN Scanning slit
topography system. 40 scanning slit
beams(20 from left and 20 from right) to scan the cornea
Each of the 40 slit images triangulates one slice of ocular surface.
Total duration of examination 1.5sec
Orbscan II :the placido disc added in orbscan 1
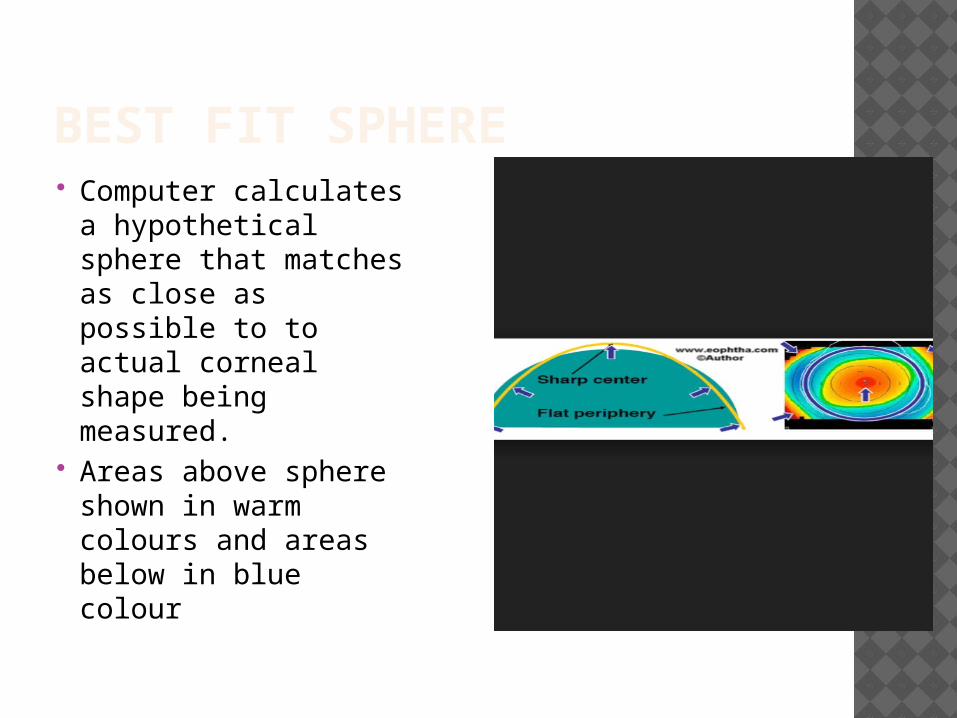
BEST FIT SPHERE Computer
calculates a hypothetical sphere that matches as close as possible to to actual corneal shape being measured.
Areas above sphere shown in warm colours and areas below in blue colour

SCHEIMPFLUG IMAGING The
Pentacam(Oculus Inc) obtains images of anterior segment by rotating Schiempflug camera which is a digital charged coupling device.
ADVANTAGES OF PENTACAM Takes 50 meridonial sections through
centre of cornea which allows the system to realign the central thinnest point of each section before it reconstructs the corneal image. Thus it eliminates any eye movement occurring during the examination.
Enables measurement of corneas with severe irregularities such as keratoconus that may not be amenable to placido imaging
Enables calculation of pachymetry from limbus to limbus

RASTERSTEREOGRAPHY It projects a calibrated grid onto
fluroscein stained tear film, takes photographs and uses computer assisted algorithms to analyse the pictures.
The accuracy of the system is 0.3D for diameter of 7mm.

INTERFEROMETRY Uses the technique of lightwave
interfernce. The interference fringes can cover the
entire anterior ocular surface not just cornea.
Not in widespread clinical use.

INTERPRETATION OF CORNEAL TOPOGRAPHY
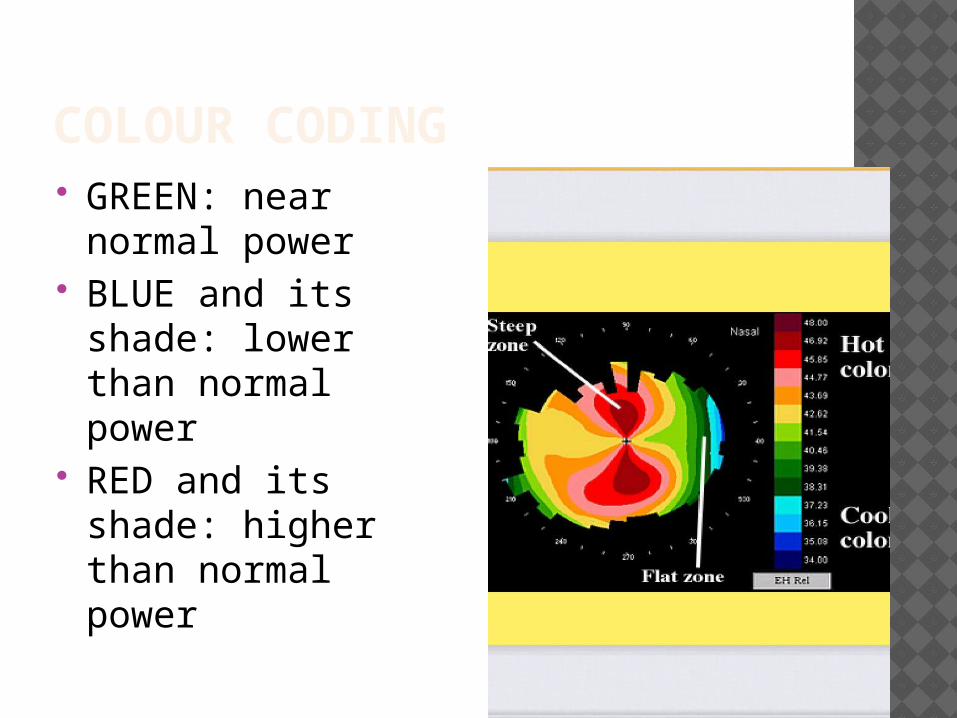
COLOUR CODING GREEN: near
normal power BLUE and its
shade: lower than normal power
RED and its shade: higher than normal power

SCALES USED NORMALISED SCALE(VARIABLE
SCALE): Different colour scales assigned to each
map Instrument identifies actual minimal and
maximal keratometric diopteric value of particular cornea
Gives more detailed description

ABSOLUTE SCALE(FIXED SCALE) Preset colour scale with same diopteric
steps Minimum and maximum assigned to
same colours Larger increment in steps(0.5D) so may
miss subtle changes

TOPOGRAPHIC DISPLAYS: CORNEAL MAP AXIAL
MAP(SAGGITAL MAP): original and most commonly used map.
Measures radius of curvature for a comparable sphere with centre of rotation on the axis of videokeratoscope.
Localised changes in curvature and peripheral changes are poorly represented.

LOCAL TANGENTIAL CURVATURE MAP(INSTANTANEOUS MAP): it displays tangential radius of curvature or tangential power which is calculated by referring to a neighbouring point and not to axis of videokeratoscope.
Reflects local changes and peripheral data better than axial map

REFRACTIVE MAP: displays refractive power of cornea.
ELEVATION MAP: displays corneal elevation relative to a reference plane.
DIFFERENCE MAP: displays changes in certain values between 2 maps.
RELATIVE MAP: displays some values by comparing them to an arbitrary standard..

BASIC TOPOGRAPHIC INDICES Simulated keratometry(Sim
K) :maximum power of surface along any axis and the power orthogonal to that axis(Sim K1 and Sim K2)
Surface Regularity Index(SRI): measure regularity in central 4.5mm
Zero for smooth surface, increases with increasing astigmatism
Surface Asymmetry Index(SAI):weighted summation of differences in corneal power between corresponding points 180 degrees apart

Asphericity: described quantitavely by the Q value
Q=0 for sphere Q<0 for prolate surface Q>0 for oblate surface Normal cornea has Q value of -0.26

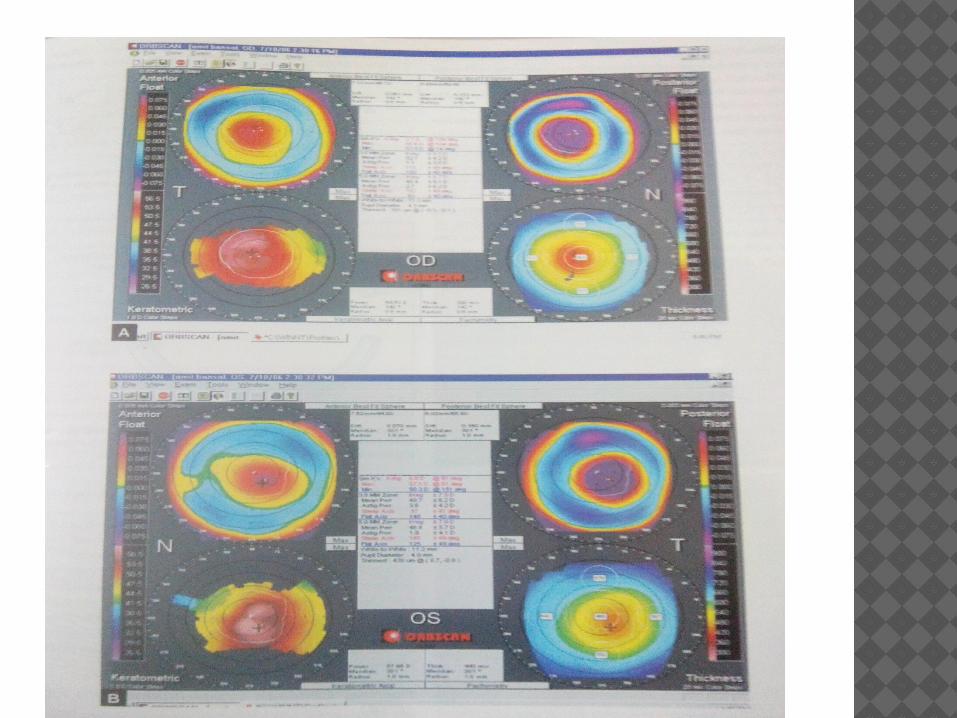
ANALYSIS OF ORBSCAN QUAD MAP

Anterior Float(Elevation Best Sphere):
Anterior best fit sphere is calculated to best match the anterior corneal surface.
Elevation BFS map subtracts the calculated BFS against the eye surface.
Posterior Float(Elevation Best Sphere Map): describes the back surface of the cornea in the same manner.
Keratometric(mean Power) Map:displays refractive power of anterior surface of cornea
Thickness (Pachymetry )map: displays corneal thickness
Warm colour indicates thinner cornea

MIDDLE BOX DATA Keratometric
reading White to white
distance in mm Thinnest point of
cornea Angle kappa
readings Irregularity within
central 3mm and 5mm

CORNEAL TOPOGRAPHY IN NORMAL CASES Normal cornea flattens progressively
from centre to periphery, nasal area flattening more than temporal area
Approximate distribution of keratographic pattern varies as
Round(23%) Oval(21%) Symmetric bow tie typical for regular
astigmatism(18%) Asymmetric bow tie(32%) Irregular(7%)
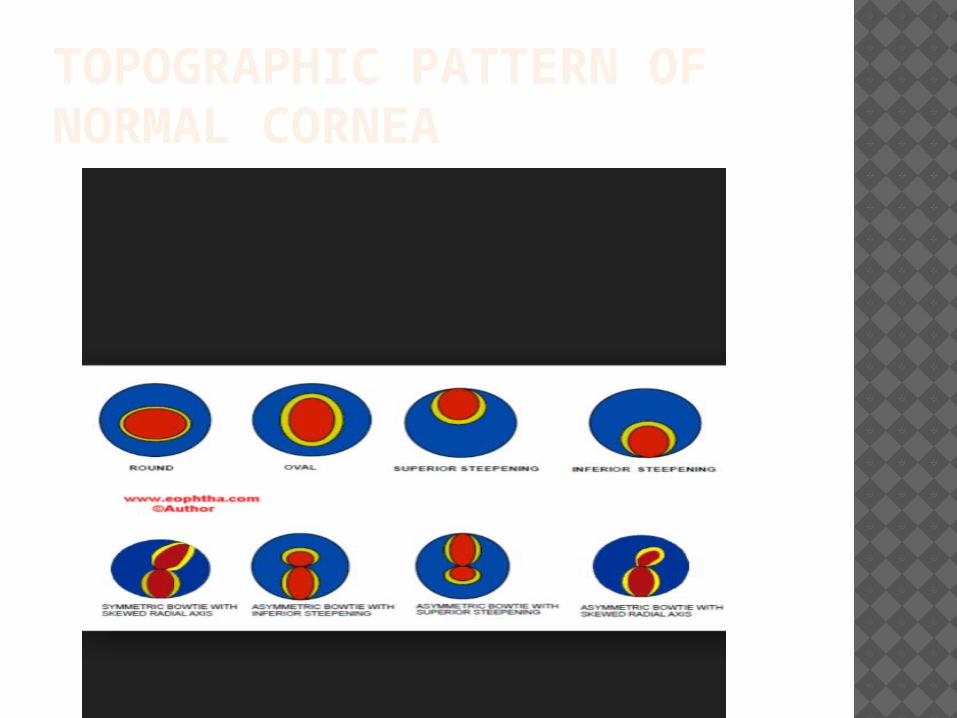
TOPOGRAPHIC PATTERN OF NORMAL CORNEA

KERATOCONUS Typically there is inferior area of
steepening. Area of increased power surrounded by
concentric areas of decreased power An inferior superior power asymmetry A skewing of the steepest radial axis
above and below the horizontal meridian

Keratoconus Predictability Index(KPI): derived from 8 topographic indices.
KPI of >0.23 is indicative of keratoconus
KISA % index: product of central K reading, I-S value,
astigmatism measured by Sim K value and Skewed radial axis index(SRAX).
60%-or more is suspect100% diagnostic

KERATOCONUS RABINOWITZ DIAGNOSTIC CRITERIA : Consists of 3 topography derived indices1.Keratometry value of 47.2 D or greater
in the central cornea2. Inferior –Superior asymmetry value – 1.4D-1.9D is suggestive and >1.9D is
diagnostic3. Posterior float elevation >40 micro m
suggestive of posterior ectasia

PELLUCID MARGINAL DEGENERATION Classical butterfly
appearance Against the rule
astigmatism in early stage
Thinning is concentric to the limbus generally between 4 to 8 O clock position
TERRIENS MARGINAL DEGENRATION Flattening over areas of peripheral
thinning(mostly superior and inferior cornea)
High against the rule or oblique astigmatism is a common feature
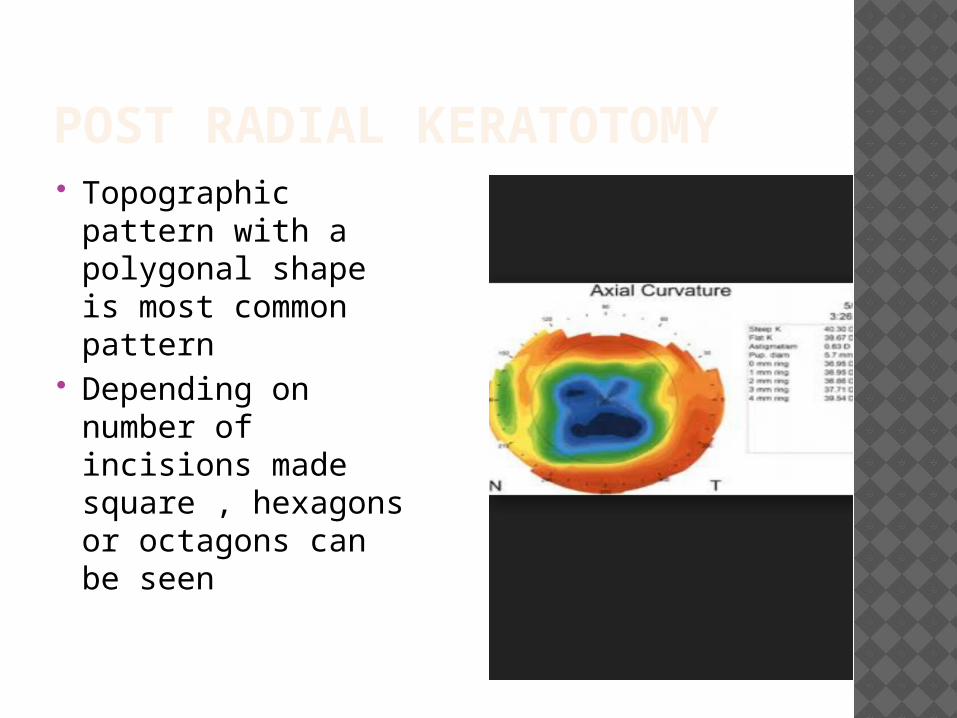
POST RADIAL KERATOTOMY Topographic
pattern with a polygonal shape is most common pattern
Depending on number of incisions made square , hexagons or octagons can be seen
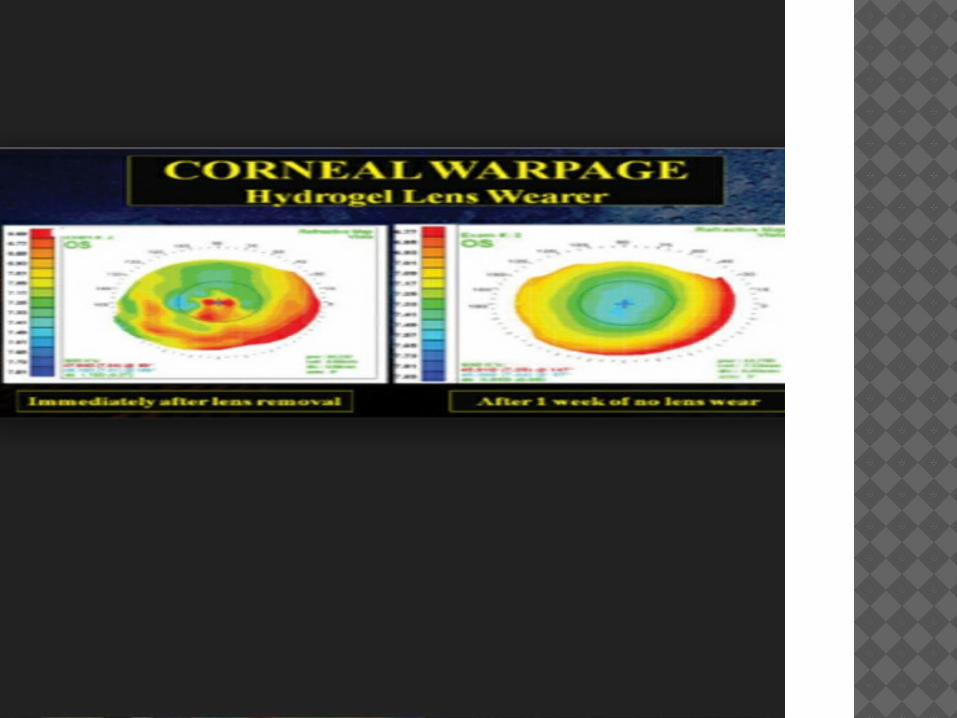
CONTACT LENS INDUCED CORNEAL WARPAGE Characterised by topograhic changes in
cornea following contact lens wear as a result of mechanical pressure exerted by lens
Usually 4 different form which occur alone or with one another
i.Peripheral steepeningii. Central flatteningiii. Furrow depressioniv. Central moulding

OTHER USES To guide removal of tight sutures after
corneal surgery Guide contact lens fitting Evaluate effect of keratographic
procedure