corneal curvatures in premature infants
TRANSCRIPT

VOL. 98, NO. 5 LETTERS TO THE JOURNAL 627
dosage of 30 mg/day was gradually decreased. The patient's visual acuity improved to 20/40 and only a faint corneal nebula was ultimately visible.
Standard immunologie testing demonstrated a reduction in circulating T helper cells with an inverted ratio of T helper to T suppressor cells. This immunologie deficiency persisted from the time of the acute infection until the patient was tested again four months later. We believe that the abnormalities in cellular immune function were consistent with an underlying cellular immune disturbance, which may have played a part in the development of the fungal keratitis. Although the serum minimum inhibitory concentration of the antifungal drugs was inadequate to control the infection, the high concentration made available by topical administration would have been adequate to control the fungal infection locally. The repeated corneal scrapings probably also helped to reduce the bulk of fungal inoculum, and may have contributed to the favorable outcome.
CORNEAL CURVATURES IN PREMATURE INFANTS
P A U L B. D O N Z I S , M.D. , M I C H A E L S. INSLER, M.D. , AND R O B E R T A. G O R D O N , M.D.
Department of Ophthalmology, Tulane University School of Medicine.
Inquiries to Michael S. Insler, M. D., Department of Ophthalmology, Tulane Medical Center, 1430 Tulane Ave., New Orleans, LA 70112.
The use of infant donor corneas in keratoplasty as a method to induce a myopic shift has been confirmed by several investigations.1,2 Most recently, Pias
ter and Breaud3 reported on using newborn donor corneas as an alternative low-risk approach to correct refractive errors in an aphakic eye undergoing penetrating keratoplasty. The final kerato-metric power noted in the recipient depended on the gestational age of the donor infant cornea. Additionally, donor corneas from children 1 year old failed to produce markedly increased keratomet-ric powers. This led us to study the longitudinal change in corneal curvature in a group of premature newborns. Twelve eyes of six premature infants, ranging from 28 weeks to 34 weeks of gestational age at birth were examined during a three-month period. Each patient underwent an ocular examination (while in the newborn nursery) that included cycloplegic retinoscopy, ophthal-moscopy, and keratometric power determination. None of the infants had any ocular disease, any serious illness, or any developmental delay. The weight of each infant was within the normal range for the gestational age.
The Table shows the initial and follow-up mean spherical keratometric power in each of the six cases. The Figure plots the changing values obtained in our study. As noted, the corneal curvature was steepest in the youngest premature newborn and decreased significantly with age.
Our examination showed the rapid Ion-
Figure (Donzis, Insler, and Gordon). Plot of initial and follow-up corneal powers in premature infants.
628 AMERICAN JOURNAL OF OPHTHALMOLOGY NOVEMBER, 1984
Patient No., Sex, Age (yrs)
1, F, 37 2, F, 31
3, F, 21
4, F, 31
5, F, 25 6, F, 26
7, F, 23
8, F, 28
9, F, 25
10, F, 21
Systemic Illness
No No
Yes
No
Yes No
No
Yes
No
No
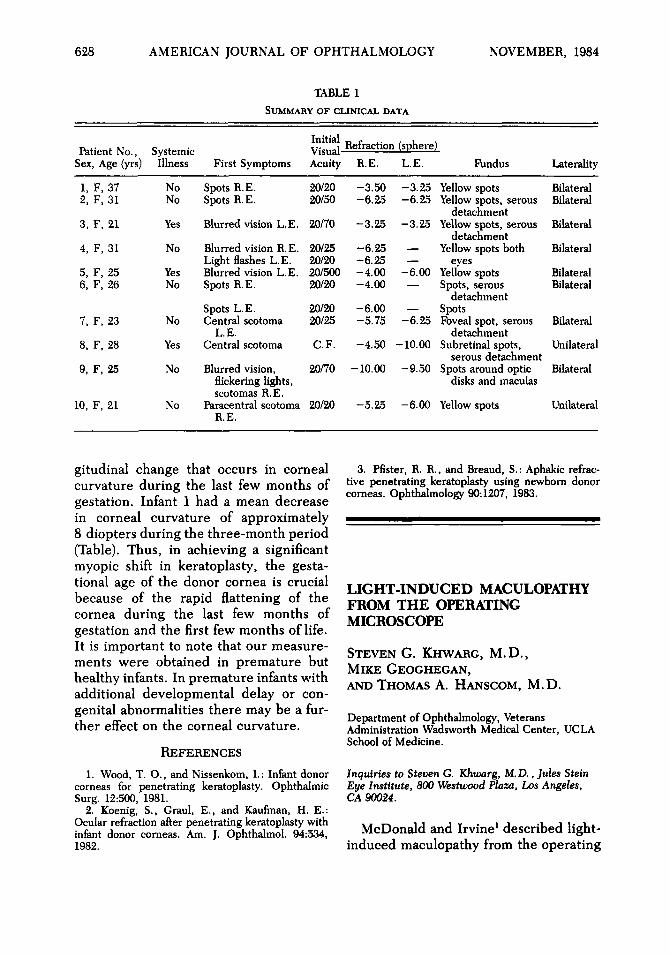
TABLE 1 SUMMARY OF CLINICAL DATA
First Symptoms
Spots R.E. Spots R.E.
Blurred vision L.E.
Blurred vision R.E. Light flashes L.E. Blurred vision L.E. Spots R.E.
Spots L.E. Central scotoma
L.E. Central scotoma
Blurred vision, flickering lights, scotomas R.E.
Paracentral scotoma R.E.
Initial Visual-Acuity
20/20 20/50
20/70
20/25 20/20 20/500 20/20
20/20 20/25
C F .
20/70
20/20
Refraction R.E.
-3.50 -6.25
-3.25
-6.25 -6.25 -4.00 -4.00
-6.00 -5.75
-4.50
-10.00
-5.25
(sphere L.E.
-3.25 -6.25
-3.25
— —
-6.00 —
— -6.25
-10.00
-9.50
-6.00
) Fundus
Yellow spots Yellow spots, serous
detachment Yellow spots, serous
detachment Yellow spots both
eyes Yellow spots Spots, serous
detachment Spots Foveal spot, serous
detachment Subretinal spots,
serous detachment Spots around optic
disks and maculas
Yellow spots
Laterality
Bilateral Bilateral
Bilateral
Bilateral
Bilateral Bilateral
Bilateral
Unilateral
Bilateral
Unilateral
gitudinal change that occurs in corneal curvature during the last few months of gestation. Infant 1 had a mean decrease in corneal curvature of approximately 8 diopters during the three-month period (Table). Thus, in achieving a significant myopic shift in keratoplasty, the gesta-tional age of the donor cornea is crucial because of the rapid flattening of the cornea during the last few months of gestation and the first few months of life. It is important to note that our measurements were obtained in premature but healthy infants. In premature infants with additional developmental delay or congenital abnormalities there may be a further effect on the corneal curvature.
REFERENCES 1. Wood, T. O., and Nissenkom, I.: Infant donor
corneas for penetrating keratoplasty. Ophthalmic Surg. 12:500, 1981.
2. Koenig, S., Graul, E., and Kaufman, H. E.: Ocular refraction after penetrating keratoplasty with infant donor corneas. Am. J. Ophthalmol. 94:534, 1982.
3. Pfister, R. R., and Breaud, S.: Aphakic refractive penetrating keratoplasty using newborn donor corneas. Ophthalmology 90:1207, 1983.
LIGHT-INDUCED MACULOPATHY FROM THE OPERATING MICROSCOPE
STEVEN G. KHWARG, M.D., MIKE GEOGHEGAN, AND THOMAS A. HANSCOM, M.D.
Department of Ophthalmology, Veterans Administration Wadsworth Medical Center, UCLA School of Medicine.
Inquiries to Steven G Khwarg, M. D., Jules Stein Eye Institute, 800 Westwood Plaza, Los Angeles, CA 90024.
McDonald and Irvine1 described light-induced maculopathy from the operating