corneal astigmatism after cataract extraction: a comparison of corneal and corneoscleral incisions
TRANSCRIPT
A C T A O P H T H A L M O L O G I C A V O L . 5 7 1 9 7 9
The Department of Ophthalmology (Heads: V . Dreyer, J. Edniund, E. Gregersen,
S. V . Kcssing. H . H. Seedorff), Rigshospitnkt, University of Cobenhagen
CORNEAL ASTIGMATISM AFTER CATARACT EXTRACTION
A Comparison of Corneal and Corneoscleral Incisions
BY
JOHN THYGESEN, PER REERSTED, HANS FLEDELIUS
and LElF CORYDON
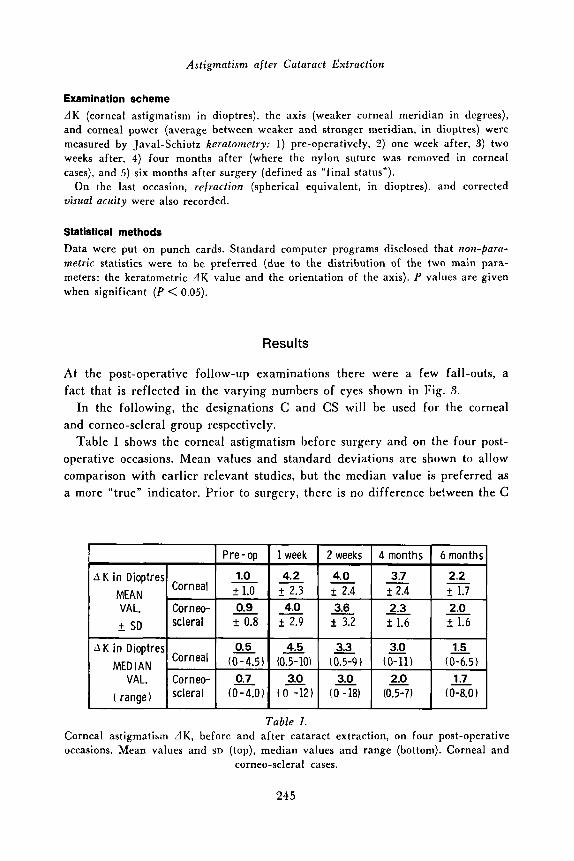
Corneal astigmatism after cataract surgery by way of corneal incision (C, n = 62) and corneo-scleral incision (CS, n = 61) was followed for six months. Corneal incisions were closed by continuous nylon 10-0 (7-25 loops, median 14). Corneo-scleral incisions were sutured with single knots (2-10, median value 5). Keratometric results in the C and CS groups are compared. Concerning the degree of astigmatism, pre-operative median values were 0.5 and 0.7 D, respectively. After one week they were 4.5 and 3.0 D; after two weeks 3.3 and 3.0 D; after four months 3.0 and 2.0 D; after six months (final status) 1.5 and 1.7 D, respectively. The differences between C and CS were not significant. For both, astigmatism after cataract surgery did not quite return to pre-operative levels. Concerning the axis (weaker meridian) of corneal astigmatism, the C cases retained their pre-operative distribution, while the CS cases showed the classical shift towards against-rule astigmatism. Final corrected visual acuity was of the same order in the C and CS group. Due to frequent shifts, also of the axis, it is recommended by early (pre- liminary) glass prescription not to correct the astigmatism, but to give only the best spherical correction.
Key words: cataract extraction - corneal incision - corneo-scleral incision - corneal astigmatism.
The material was presented to the Danish Ophthalmological Society April 15, 1975.
Received September 22, 1978.
243
J . Tliygesen, P . Reersted, H . Fledelizis and L. Corydon
During the last years a corneal incision (under the microscope) has found in- creasing use in our department in cataract surgery. Inevitably, discussion arose concerning the advantages and drawbacks as compared with the routine me- thod in use until then, namely, an ab externo corneo-scleral incision under a limbus-based conjunctival flap. I t thus appeared that corneal astigmatism was often high af ter a corneal incision, a t least initially, a n d apparently the patient had to wait longer for definitive glass prescription.
T o clarify these points, a consecutive series of cataract extraction by the two methods was followed for six months, a n d the results were compared. The degree of, a n d the change in post-operative corneal astigmatism is the subject of the present publication.
Materials and Methods
123 consecutive cataract extractions, from May to November 1976, were included in the study.
Excluded were only 1) cases in which keratometry was not possible due to pre- existing corneal pathology, and 2) patients where geography was inhibitory to follow- up (Greenland, Faroe Islands, remote parts of Denmark).
The bulk of the material was made up of senile and presenile cataracts, but there were also some complicated cataracts (uveitis, excessive mycpia, heterochromia). Cases with complications during surgery were not excluded.
Age of patients ranged from 33-91 years in the corneal and 54-85 years in the corneo-scleral group. There were 63 female and 60 male eyes; 67 right and 56 left eyes.
62 patients had a corneal incision and a continuous nylon 10-0 suture, except for six cases with single sutures (virgin silk, vicryl, dexon). The number of loops was 7-25, median value 14.
61 patients had a cornco-scIera1 incision under a limbus-based conjunctival flap. Single sutures were used in a number from 2 to 10, median value 5. Virgin silk was used in 33, vicryl in 22, and collagen in 6.
The incision was made ab externo, in two steps and angled; first with knife (usually razer-blade, perpendicular to surface to a depth of */3 of the cornea), and then with scissors. All cases but six were operated on under the microscope.
The operations were performed - usually in local anaesthesia - by members of the staff: a) Chief surgeons, 57 cases (38 corneal, 19 corneo-scleral), and b) Residents, 66 cases (24 corneal, 42 corneo-scleral).
There was a slight load of "heavy cases" in the corneal group (because, in general a corneal incision was chosen in cases where complications were expected). According- ly, vitreous loss occurred more often in this group (7/62) than in the corneo-scleral group (2161); a transitory rise in IOP (above 24 mmHg) was found in four and in one eye, respectively. There was one case of flat chamber after surgery (corneo-scleral incision) and one case of secondary haemorrhage (corneal incision). Clip lenses were implanted in seven corneal and in two corneo-scleral cases.
244
Astigmatism after Cataract Extraction
A K in Dioptres MEDIAN
Examination scheme dK (corneal astigmatism in dioptres), the axis (weaker corneal meridian in degrees), and corneal power (average between weaker and stronger meridian, in dioptres) were measured by Javal-Schi~tz keratomctry: 1) pre-operatively, 2) one week after, 3) two weeks after, 4) four months after (where the nylon suture was removed in corneal cases), and 5 ) six months after surgery (defined as “final status”).
On the last occasion, refraction (spherical equivalent, in dioptres). and corrected visual acuity were also recorded.
I
1.5 - 3.0 - 0.5 4.5 3.3 Corneal (0-4.5) (0x0) (0.5-9) (0-11) (0-6.5)
Statistical methods
Data were put on punch cards. Standard computer programs disclosed that non-pam- metric statistics were to be preferred (due to the distribution of the two main para- meters; the keratometric A K value and the orientation of the axis). P values are given when significant (P < 0.05).
Results
At the post-operative follow-up examinations there were a few fall-outs, a fact that is reflected in the varying numbers of eyes shown in Fig. 3.
In the following, the designations C and CS will be used for the corneal and corneo-scleral group respectively.
Table I shows the corneal astigmatism before surgery and on the four post- operative occasions. Mean values and standard deviations are shown to allow comparison with earlier relevant studies, but the median value is preferred as a more “true” indicator. Prior to surgery, there is no difference between the C
r I Pre-op I 1 week I 2 weeks I 4 months 1 6 months
A K in Dioptres MEAN
2.3 2.0 t SD f 1.6
VAL. I Corneo- I 0.7 I 3.0 I _3.0 I 2.0 I 1.7 I ( range) scleral (0-4.0) ( 0 -12) ( 0 -18) (0.5-7) (0-8.0)
Table I . Corneal astigmatism d K , before and after cataract extraction, on four post-operative occasions. Mean values and SD (top), median values and range (bottom). Corneal and
corneo-scleral cases.
245
J . Thygesen, P . Reersted, Ef. Fledelius and L. Corydon
60
5 40. W 0
20. n C .-
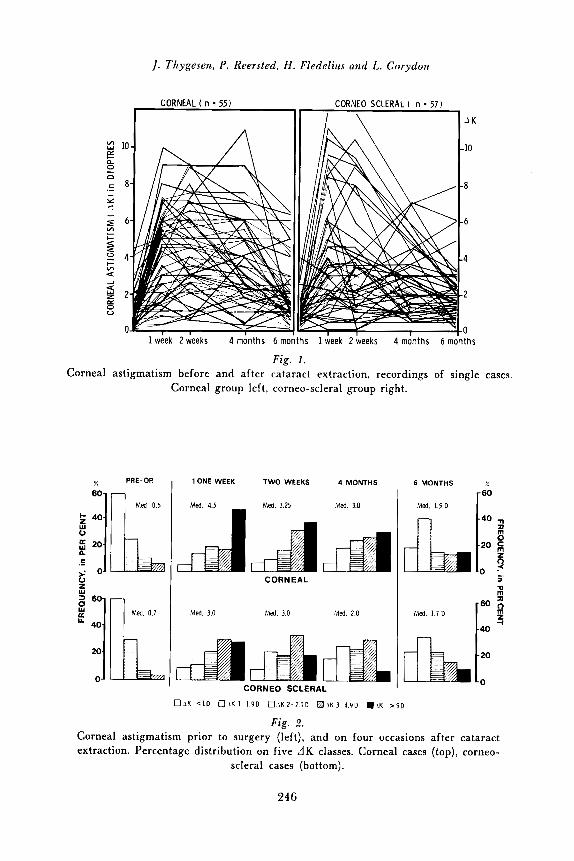
Fig. 1. Corneal astigmatism before and after cataract extraction, recordings of single cases.
Corneal group left, corneo-scleral group right.
- PRE-OP
1 Med. 0.5
1 ONE WEEK TWO WEEKS 4 MONTHS
Med. 4.5 Med. 3.25 Med. 3.0
CORNEAL
Med. 3.0 Med. 3.0 Med. 2.0
CORNEO SCLERAL
6 MONTHS
Med. 1.5 D
n TI m
Med. 1.7 0
40
t: 0 1 K <I0 OJKI 1 9 0 B I K 2 - 2 9 0 H J K 3 - 4 9 D .IK > 5 D
Fig. 2. Corneal astigmatism prior to surgery (left), and on four occasions after cataract extraction. Percentage distribution o n five J K classes. Corneal cases (top), corneo-
scleral cases (bottom).
246
:lstigmatism af ter Cataract Extraction
M 40 -
20 -
0 -
and CS group, and the same applies to the final A K value. The four months status, however, leaves the impression that CS cases achieve their final AK value somewhat earlier than the C cases.
The same is evident from Figs. 1 and 2, which show longitudinal recordings of single cases (Fig. 1) and percentage distributions (Fig. 2). In Fig. 1 , there is in the C group a rather high d K plateau until suture removal (after four months), while normalization occurs earlier among those with CS. According- ly, the darker (less favourable, high dK classes) columns of Fig. 2 show an abrupt increase in relation to surgery, followed by a gradual return to a dis- tribution which comes closer to the status before surgery.
Assessed by x 2 tests, there is no significant difference between C and CS on the five occasions, i. e. by vertical comparisons of the distributions shown in Fig. 2. By horizontal assessment - within the C and CS group respectively - there is a highly significant difference between the .4K distribution before surgery and at the final status (P < 0.001), and this applies to both groups. Corneal astigmatism thus does not return to preoperative levels.
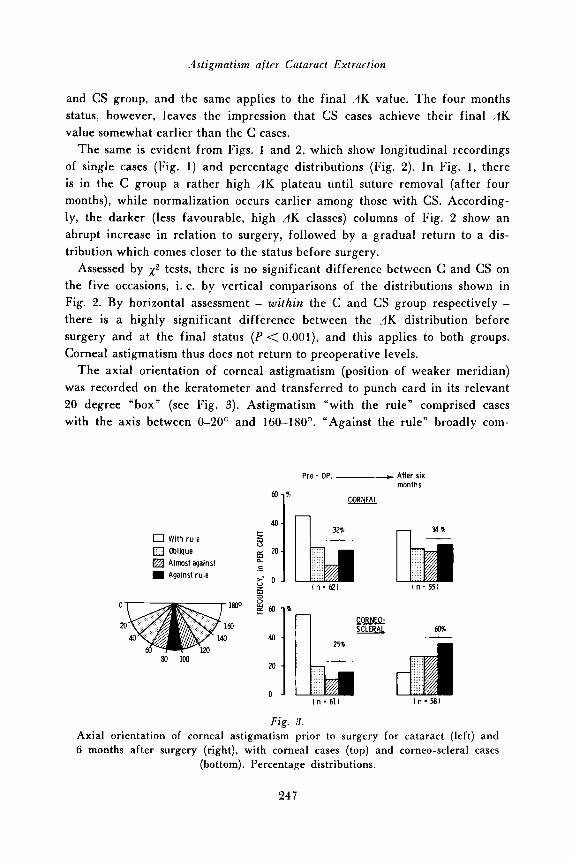
The axial orientation of corneal astigmatism (position of weaker meridian) was recorded on the keratometer and transferred to punch card in its relevant 20 degree “box” (see Fig. 3). Astigmatism “with the rule” comprised cases with the axis between 0-20’ and 160-180°. “Against the rule” broadly com-
CORNEO- SCLERAL
Pre - OP. -*After six months
CORNEAL
Fig. 3. Axial orientation of corneal astigmatism prior to surgery for cataract (left) and 6 months after surgery (right), with corneal cases (top) and corneo-scleral cases
(bottom). Percentage distributions.
24 7
J . Thygesen, P. Reersterl, H. Fledelius and L. Corydon
prised the zone 60-120°, but "against" in a narrow sense (90 f 10') is sepa- rated and specified with black in Fig. 3. Oblique astigmatism occupies the re- maining 2 x 40'.
Before surgery, about 50010 were "with rule", and there was no difference between C and CS groups. At the final status after six months, the change of axial orientation (distributions of Fig. 3) was not significant within the C group, which maintained a 11s share of "against rule" astigmatism. Conversely, there was a significant shift ( P < O . O O l ) in the CS group, with a marked re- duction in "with rule" astigmatism and a marked rise in the "against rule" fraction (from 25 to 60 O/O). The final C and CS status differ accordingly, but at only a 0.05 level.
The material enables us to give an answer to a practical question: Can glasses be prescribed early? Because, if significant changes occur in only a minor fraction, the major part of patients might have the benefit of an early full prescription. This, however, did not hold for any of the groups when single cases were followed (in contrast to the summary distributions of Fig. 3). As concerns dK, about 500/0 had changes exceeding 2 dioptres between day 14 after surgery and six months. Further, about fifty per cent showed an axial shift exceeding 20 degrees in the same period.
The above results are considered the main object of the present study. In addition, a summary mention will be given of some other data:
Corneal p o w e r (range 39.3-48.5 D) did not change much in relation to sur- gery. After exclusion of one eye with a presumed faulty recording (of 35.5 D, in the C group), the C cases had the mean value 43.28 D (SD 1.66) before sur- gery and 43.13 (sn 1.99) after six months. The corresponding CS values were 43.06 ( ~ ~ 1 . 6 6 ) and 43.09 D (SD 1.89).
Final corrected visual acuity was good in both groups, with values 2 619 in 84 O/O. Visual acuity 2 6/60 (pre-existing maculopathy, 2 cases; aphakic retinal detachment, 1 case) occurred in one eye with C and in two with CS.
There was no correlation between astigmatic error (dK) and final corrected visual acuity.
After exclusion of the nine eyes with clip lenses, the final refraction (spheri- cal equivalents) of C cases showed a significant shift ( P < 0.01) towards lower values when compared with the CS group. This is reflected also in the mean values of the two groups, being 1 1 . 1 D (sn 3.3) and 12.9 D (SD 1.5) respectively. As deducted from the aphakic refractive values, the C group thus entailed eight eyes that had high myopia prior to surgery, against only one eye in the CS group.
The final post-operative astigmatism showed no correlation (Spearmans rank) to pre-operative corneal astigmatism, age of patient, number of sutures, loops, or to visual acuity (vide supra).
248
Astigmatism after Cataract Extraction
Discussion
Advances in surgery (microsurgical techniques) and pharmacology (access to antibiotics and corticosteroids) have by and large eliminated the formerly dreaded severe complications of cataract extraction. Therefore, with the words of Troutman (1970), we can now ”begin to worry about the previously neglec- ted details. One area which has been ignored is the optical distorsion of the cornea randomly induced by current cataract incision and closure, over which chance still has the best control”.
This degree of “corneal distortion” is the sole subject of the present publica- tion, which does nol deal with other aspects of cataract surgery. Let it only be stated that a corneal incision has been used, because in general this is re- garded as being pretty safe (Corydon 1976; Corydon & Mackensen 1978), and especially so in eyes with expected complications to surgery (a fact that is also reflected by the greater share of heavy cases in the corneal group of the present material).
The ideal set-up for a comparison of the two cataract surgery incisions would be as follows: The same surgeon should perform the surgery in all cases, and with equal skill and experience as regards the two incisions to be compared. Allocation to the two techniques should be strictly at random. Regard should also be taken to type of knife and scissors, to suture material and technique, as well as to the age of the patient, sex, type of cataract, eye size, etc.
Such demands are hard to fulfil in a ciinical series. This is apparent from the present material, as well as those of earlier reports on the subject. W e managed to keep the unity of time and place, but a considerable number of eye surgeons were included, experienced as well as residents, and the tech- niques of wound closure varied. Corneal incisions were usually closed by a continuous nylon suture, while corneo-scleral incisions were sutured by single sutures, in a varying number and with different materials.
The present approach is therefore primarily practical-clinical and does not eliminate multifactorial hazards, but we still consider a comparison of the two methods as being justified. This may be supported i. a. by the fact that the corneal astigmatism after surgery by residents equalled the results gained by the chief surgeons. A similar experience was reported earlier by Bedrossian et al. (1969).
From our results, we may advance that the final degree of corneal astigma- tism showed no relation to the type of incision. Further, our 6-months-values equalled those of a quite recent German study (Steinbach & Gerhard 1978) with a set-up quite similar to the present one. In both studies, however, nor-
249

J . Thygesen. P . Reersterl, H . Fledeliiis and L. Corydon
malization seemed somewhat retarded in the group with corneal incision, due to the late removal of the non-absorbable nylon suture.
Concerning the axis of astigmatism, there is, however, a remarkable dif- ference between the two studies. Steinbach & Gerhardt (1978) found - for both incisions - a shift in axis from “with the rule” towards “against rule” (weaker meridian vertically). This is the classical experience gained since the Graefe incision was introduced, but it does not accord with more recent reports, that emphasise a more “natural tendency” (with rule) after corneal incision with a meticulous wound closure under the microscope. In our material, this was also evident. W e found a significant difference between the classical against-rule corneo-scleral cases and those with a corneal incision. The latter largely kept their original distribution of axial directions (Fig. 3).
The impact of the present study is that the end results concerning corneal astigmatism after the two different incisions were pretty similar, however, with the exception mentioned regarding the axis. This had but little influence on the functional end-result (which is corrected visual acuity). W e think - like Steinbach & Gerhardt (1978) - that both methods are, from an astigmate point of view, equally suited for cataract surgery. And further, modern microsurgical advances have now modified one of the classical dogmas about cataract sur- gery, that astigmatism will increase, the more corneal (nearer to vertex) the incision is located (Lundsgaard 1925).
It is tempting finally to quote another countryman, Edmund, who at the same meeting in 1925 stated that “Nature has a peculiar ability to let a, by external actions altered anatomy, return to its original norm”.
References
Bedrossian P. B., Sabater G. & Troutman R. C. (1969) Induced astigmatism us a result of surgery. South-African Intern. Ophthal. Sympos. 219-225. Butterworth, Washing- ton.
Corydon L. (1976) Kon~plikationen bei Katrzraktoperationen. Inaug. Diss., Freiburg. Corydon L. & Mackensen G. (1978) Progress in cataract surgery using microsurgical
Edmund C. (1925) net oftdmologiske Selskabs forhandlinger 194-1925 (Kbh. ) 23. Lundsgaard K. K. K. (1925) Den postoperative Astigmatisme. Det oftnlinologiske Sel-
skabs forhandlinger 1924-25 (Kbh. ) 16-28. Steinbach P.-D. & Gerhardt G. (1978) Postoperativer Astigmatismus und Visus nach
Kataraktextraktion bei unterschiedlichem operativem Vorgehen. Klin. Mbl. Augen- heilk. 172, 305-312.
Troutman R. C. (1970) Control of corneal astigmatism in cataract and corneal surgery. Trans. Pacific Coast Oto-Ophthnl. Soc. 51. 217-231.
technique. Actn ophthnl. (Kbh. ) 58, 53-66.
250
Astigmatism after Cataract Extraction
In addition, reference is made to essential contributions in a recent publication, Current Concepts in Cataract Surgery (Emery J. M. and Paton D., Eds., 1976. C. V. Mosby) which came to our knowledge after the present paper was finished.
Authors’ addresses: John Thygesen, Eye Dept., Hvidovre Hospital, Copenhagen, Ketteglrd AIIC, DK 2650 Hvidovre, Denmark.
Per Reersted, Eye Dept., Gentofte Hospital, DK 2900 Hellerup, Denmark.
25 1