corneal asphericity after refractive surgery when the munnerlyn formula is applied
TRANSCRIPT

98 J. Opt. Soc. Am. A/Vol. 21, No. 1 /January 2004 Jimenez et al.
Corneal asphericity after refractive surgery whenthe Munnerlyn formula is applied
Jose Ramon Jimenez, Rosario Gonzalez Anera, Jose Antonio Dıaz, and Francisco Perez-Ocon
Departamento de Optica, Facultad de Ciencias, Universidad de Granada, Granada 18071, Spain
Received April 2, 2003; revised manuscript received August 28, 2003; accepted September 8, 2003
We deduce a mathematical equation for corneal asphericity after refractive surgery when the Munnerlyn for-mula is used. For this, an analytical least-squares procedure is used. The equation explains the discrepan-cies found by different authors when the Munnerlyn formula or its paraxial approximation is used. Equationsfor corneal asphericity deduced here may be of clinical relevance, for example, in studying quantitatively therole of different factors (decentration, type of laser, optical role of the flap, wound healing, biomechanical ef-fects, technical procedures) during corneal ablation. © 2004 Optical Society of America
OCIS codes: 170.1020, 170.4470.
1. INTRODUCTIONIn recent years various experimental studies have beendone on corneal asphericity after refractive surgery1–5 aswell as on its implications in visual function and cornealaberrations. All the studies show notable increases inthe p factor for myopes1–4 but decreases (negative in-crease) for hyperopes.5 A number of authors have at-tempted to explain these results. One difficulty encoun-tered is that it is not possible to know exactly the ablationalgorithm to be applied during practical surgery, as thealgorithms are proprietary. Although most noncustom-ized-ablation algorithms rely on the Munnerlyn formula,most theoretical studies on refractive surgery use eitherthis formula or its paraxial approximation.
Recently Jimenez et al.6,7 provided an analytical equa-tion for corneal asphericity after surgery when theparaxial Munnerlyn formula is applied. According tothis equation, the p factor after surgery, p8, is given by
p8 5R83
R3p, (1)
where p is the presurgery p factor and R8 and R are thepostsurgery and presurgery radius, respectively. Thisequation can partially explain the notable increase in as-phericity for myopes6,7 (initially prolate or oblate) and thedecrease for hyperopes.8 In contrast, Gatinel et al.9 indi-cate that for prolate subjects, postsurgery asphericityshould be more prolate, explaining this discrepancy withexperimental data on factors that influence ablation suchas laser effects and biomechanical aspects. In theirstudy, these authors did a numerical analysis withoutproviding any equation; their analysis was based directlyon the Munnerlyn formula without paraxial approxima-tion.
In the present paper we study the discrepancies be-tween the above-mentioned two studies. For this, we cal-culate analytically the postsurgical corneal asphericitywhen the Munnerlyn formula is used without paraxial ap-proximation and compare this with the corneal aspheric-
1084-7529/2004/010098-06$15.00 ©
ity when the formula is approximated. From the analy-sis of the formulas deduced, we discuss the implications ofthe study with respect to clinical aspects of refractive sur-gery.
2. METHODSThe Munnerlyn formula for the ablation depth, s1( y), isgiven by10
s1~ y ! 5 ~R2 2 y2!1/2 2 ~R82 2 y2!1/2 1 ~R82 2 d2/4!1/2
2 ~R2 2 d2/4!1/2, (2)
where y is the radial distance from the optical axis, R8and R are the radius postsurgery and presurgery, respec-tively, and d is the ablation diameter.
The parabolic approximation11 of the Munnerlyn for-mula, s2( y), is given by
s2~ y ! 54Dy2
32
Dd2
3, (3)
where D is the number of diopters to correct. This equa-tion is deduced by using the first two terms of the seriesexpansion for the square root:
~1 1 x !1/2 > 1 1 x/2 2 x2/8. (4)
For Eq. (3), it is assumed that the refractive index ofthe cornea is 1.375 and that the number of diopters is re-lated to the radius, before and after surgery, by
D
0.3755
1
R82
1
R. (5)
A. Calculation of the Postsurgical Corneal Asphericityfor the Munnerlyn Formula: MathematicalProcedureWe will calculate the postsurgical corneal asphericity forthe Munnerlyn formula with a procedure similar to thatused by Jimenez et al.6,7 to deduce Eq. (1), using the
2004 Optical Society of America

Jimenez et al. Vol. 21, No. 1 /January 2004 /J. Opt. Soc. Am. A 99
paraxial approximation. This mathematical proceduregives an analytical equation from a least-squares analy-sis.
Initially, we shall consider a presurgical anterior cor-nea with a radius R and p factor p, the equation of whichverifies that of a conicoid:
z~ y ! 5R
p2
~R2 2 py2!1/2
p, (6)
with the z axis being the optical axis and y a spatial coor-dinate that indicates the height over the optic axis. Inour analysis, we will assume rotational symmetry,6–9 al-though our analysis could be valid for different meridians.The equation corresponding to the paraboloid ( p 5 0),given by
z~ y ! 5 y2/2R, (7)
will be analyzed below.To simulate the surgical procedure, we must add the ef-
fect of the ablation on the anterior cornea by addings1( y), as given by the Munnerlyn formula [Eq. (2)], toz( y) [Eq. (6)]. Therefore the anterior surface of the cor-nea after surgery, denoted z8( y), is given by
z8~ y ! 5 s1~ y ! 1 z~ y ! 5 ~R2 2 y2!1/2 2 ~R82 2 y2!1/2
1 ~R82 2 d2/4!1/2 2 ~R2 2 d2/4!1/2 1R
p
2~R2 2 py2!1/2
p. (8)
This equation does not verify the conicoid model butrather deviates; although the geometry of postsurgical an-terior cornea fails to verify the conicoid model, we shalldetermine the closest or most representative asphericityof the postsurgical cornea. As indicated above, we seekto find the conicoid that is mathematically closest to z8( y)and that would provide the postsurgical asphericity value(and that, for example, would be detected by a corneal to-pographer). This conicoid, z9( y), would be given by thefollowing equation,
z9~ y ! 5 z0 1R8
p82
~R82 2 p8y2!1/2
p8, (9)
where the parameters z0 (this parameter indicates theconicoid shift along the z axis), p8, and R8 are unknownand will be calculated by the least-squares method. Forthis, the following expression must be minimized6,7:
g~z0 , R8, p8! 5 E0
d/2
@z9~ y ! 2 z8~ y !#2dy. (10)
This procedure guarantees that the differences be-tween z8( y) and z9( y) are minimum, and it provides thep8 factor, the parameter of interest.
To minimize Eq. (10), we must find the points zmin ,Rmin8 and pmin8 that solve the equations
]/]z0@ g~z0, R8, p8!#~zmin , Rmin8 , pmin8 ! 5 0, (11a)
]/]R8@ g~z0, R8, p8!#~zmin , Rmin8 , pmin8 ! 5 0, (11b)
]/]p8@ g~z0, R8, p8!#~zmin , Rmin8 , pmin8 ! 5 0. (11c)
These (zmin , Rmin8 and pmin8 ) constitute the geometrical pa-rameters that will characterize the postsurgical cornea.
Replacing z8( y) and z9( y) in Eq. (10), we get
g~z0 , R8, p8! 5 E0
d/2H z0 1R8
p82
~R82 2 p8y2!1/2
p8
2 @~R2 2 y2!1/2 2 ~R82 2 y2!1/2
1 ~R82 2 d2/4!1/2 2 ~R2 2 d2/4!1/2#
2R
p1
~R2 2 py2!1/2
p J 2
dy. (12)
To minimize the above expression is complex; to attainan analytical solution, it is first necessary to perform cer-tain computations on the function g(z0 , R8, p8). The in-tegral given by Eq. (12) has six square roots, for which wewill substitute a series expansion given by
~1 1 x !1/2 > 1 1 x/2 2 x2/8. (13)
That is, we keep three terms of the series expansion. Asan example, we show the series expansion for one of theterms:
~R2 2 py2!1/2
p>
R
p2
y2
2R2
py4
8R3. (14)
Certain considerations must be taken into account re-garding this series expansion.6,7,12 Although this type ofseries expansion is mathematically justified, since ( y/R), 1, the paraxial approximation of the Munnerlyn for-mula, as remarked above, is achieved by the same seriesexpansion but with only two terms. The approximationwith only two terms, apart from being less exact, has se-rious limitations for the calculation of corneal asphericity.An examination of Eq. (14) indicates that the term y4 isproportional to p/(8R3), which includes the p factor. Ifonly two terms are used, the term y2 has 1/(2R) as a pro-portionality constant, and all the asphericity informationis lost,6,12 making it a rough approximation. To include athird term in the approximation eliminates this problemand provides numerical values very close to those foundwhen the square root is not expanded, as other studieshave shown.7
When we apply approximation (13) in all the rootsshown in Eq. (12), neglecting terms higher than y4, andafter some easy computations (a more exhaustive expla-nation can be found in other references6,7), we get the fol-lowing values for zmin , Rmin8 and pmin8 ;
zmin 5 R 2 R8 1 ~R82 2 d2/4!1/2
2 ~R2 2 d2/4!1/2, (15a)
Rmin8 5 R8, (15b)
pmin8 2 1 5R83
R3~ p 2 1 !. (15c)
The values of zmin and Rmin are expected; zmin repre-sents the conicoid shift in the optical axis given by Eq. (2)

100 J. Opt. Soc. Am. A/Vol. 21, No. 1 /January 2004 Jimenez et al.
when y 5 0 and Rmin8 coincide with the final radius se-lected in Eq. (2), applied to emmetropize the subject.
For the final asphericity, we get an equation [Eq. (15c)]that can be expressed in different forms. For Eq. (15c),
taking into account that p 5 Q 1 1 with Q being the cor-neal asphericity, we get
Qmin8 5R83
R3Q. (16)
A simplified mathematical procedure shows that Eqs.(15) and (16) are also valid for the paraboloid ( p 5 0).Note that Eqs. (15) and (16) do not depend on the opticalzone selected. This is because we studied the effect of theMunnerlyn formula on postsurgical corneal asphericityand on no other variables (as will be discussed below) thatalso influence corneal ablation.
3. RESULTS AND DISCUSSIONAn analysis of the p value and Q after surgery as given byEqs. (15) and (16) explains the results reported by Gatinelet al.9 With their numerical procedure, these authors
init. prolate 0 , p , 1, Q
init. oblate p . 1, Q
found that, in case of an initial prolate cornea, prolate-ness increased for myopes. According to Eqs. (15) and(16), and knowing that (R8/R)3 . 1 for a myopic subject(R8 . R), we get
The results of Eqs. (15) explain qualitatively the trendfound by Gatinel et al.9 and also explain that sphericalcorneas remain spherical after surgery, as these authorsindicate by their numerical method, since if p 5 1, thenp8 5 1 [Eqs. (15) and (16)].
On making a quantitative analysis of their results withthose provided by the formula deduced here, we foundthat the results fit very well. Figure 1 shows the resultsthat can be deduced with great agreement between thefigures by Gatinel et al.9 and those calculated from Eqs.(15) and (16). Figure 1 shows the values of the p8 factorafter surgery for the myopia values D 5 24 and D5 28 as a function of the presurgical p factor. We veri-fied that Eqs. (15) provided values very similar to thosegiven by the numerical method of Gatinel et al.,9 theequation deduced in the present paper having the advan-tage, in our opinion, of analytically predicting the value ofthe asphericity in a general way according to the initialvalues of radius, asphericity, and number of diopters tocorrect. The comparisons with other graphics of thework by Gatinel et al.9 also gave a very good fit.
0 ⇒R83
R3Q , Q ⇒ Q8 , Q , 0 increase prolateness,
0 ⇒R83
R3Q . Q ⇒ Q8 . Q . 0 increase oblateness.
,
.
Fig. 1. Postsurgical p8 factor for two myopia values, D 5 24 and D 5 28, as a function of the presurgery p factor when the Munnerlynformula is applied. Lines show the values calculated with Eqs. (15) and (16), and single points (triangles) are deduced from data fromthe numerical procedure proposed by Gatinel et al.9
Jimenez et al. Vol. 21, No. 1 /January 2004 /J. Opt. Soc. Am. A 101
Equations (15) are different from the equation deducedby use of the paraxial Munnerlyn formula with a similarmathematical procedure.6,7 For this case, from Eq. (1),we deduce that
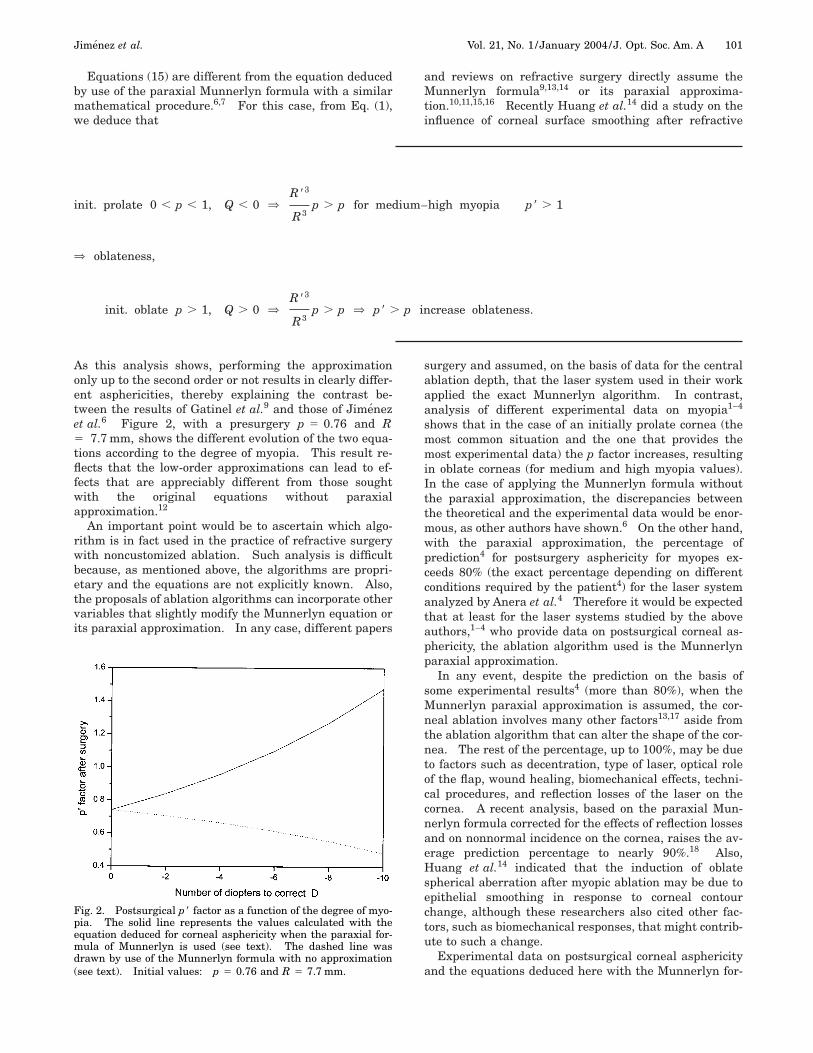
As this analysis shows, performing the approximationonly up to the second order or not results in clearly differ-ent asphericities, thereby explaining the contrast be-tween the results of Gatinel et al.9 and those of Jimenezet al.6 Figure 2, with a presurgery p 5 0.76 and R5 7.7 mm, shows the different evolution of the two equa-tions according to the degree of myopia. This result re-flects that the low-order approximations can lead to ef-fects that are appreciably different from those soughtwith the original equations without paraxialapproximation.12
An important point would be to ascertain which algo-rithm is in fact used in the practice of refractive surgerywith noncustomized ablation. Such analysis is difficultbecause, as mentioned above, the algorithms are propri-etary and the equations are not explicitly known. Also,the proposals of ablation algorithms can incorporate othervariables that slightly modify the Munnerlyn equation orits paraxial approximation. In any case, different papers
init. prolate 0 , p , 1, Q , 0 ⇒R83
R3p . p for medi
⇒ oblateness,
init. oblate p . 1, Q . 0 ⇒R83
R3p . p ⇒ p8 .
and reviews on refractive surgery directly assume theMunnerlyn formula9,13,14 or its paraxial approxima-tion.10,11,15,16 Recently Huang et al.14 did a study on theinfluence of corneal surface smoothing after refractive
surgery and assumed, on the basis of data for the centralablation depth, that the laser system used in their workapplied the exact Munnerlyn algorithm. In contrast,analysis of different experimental data on myopia1–4
shows that in the case of an initially prolate cornea (themost common situation and the one that provides themost experimental data) the p factor increases, resultingin oblate corneas (for medium and high myopia values).In the case of applying the Munnerlyn formula withoutthe paraxial approximation, the discrepancies betweenthe theoretical and the experimental data would be enor-mous, as other authors have shown.6 On the other hand,with the paraxial approximation, the percentage ofprediction4 for postsurgery asphericity for myopes ex-ceeds 80% (the exact percentage depending on differentconditions required by the patient4) for the laser systemanalyzed by Anera et al.4 Therefore it would be expectedthat at least for the laser systems studied by the aboveauthors,1–4 who provide data on postsurgical corneal as-phericity, the ablation algorithm used is the Munnerlynparaxial approximation.
In any event, despite the prediction on the basis ofsome experimental results4 (more than 80%), when theMunnerlyn paraxial approximation is assumed, the cor-neal ablation involves many other factors13,17 aside fromthe ablation algorithm that can alter the shape of the cor-nea. The rest of the percentage, up to 100%, may be dueto factors such as decentration, type of laser, optical roleof the flap, wound healing, biomechanical effects, techni-cal procedures, and reflection losses of the laser on thecornea. A recent analysis, based on the paraxial Mun-nerlyn formula corrected for the effects of reflection lossesand on nonnormal incidence on the cornea, raises the av-erage prediction percentage to nearly 90%.18 Also,Huang et al.14 indicated that the induction of oblatespherical aberration after myopic ablation may be due toepithelial smoothing in response to corneal contourchange, although these researchers also cited other fac-tors, such as biomechanical responses, that might contrib-ute to such a change.
Experimental data on postsurgical corneal asphericityand the equations deduced here with the Munnerlyn for-
–high myopia p8 . 1
increase oblateness.
um
p
Fig. 2. Postsurgical p8 factor as a function of the degree of myo-pia. The solid line represents the values calculated with theequation deduced for corneal asphericity when the paraxial for-mula of Munnerlyn is used (see text). The dashed line wasdrawn by use of the Munnerlyn formula with no approximation(see text). Initial values: p 5 0.76 and R 5 7.7 mm.

102 J. Opt. Soc. Am. A/Vol. 21, No. 1 /January 2004 Jimenez et al.
mula and those deduced with the paraxial approxi-mation6,7 can serve to ascertain which formula, or slightvariation thereof, should be used in a noncustomized pro-cedure. In addition, these equations, together with theprocedure of comparing data from theoretical predictionswith those of experimental predictions can be highly use-
ful from a clinical standpoint in studying the influence ofdifferent variables in refractive surgery.
Using this procedure, as indicated above, Jimenezet al.7 and Anera et al.18 demonstrated that, when addedto the ablation algorithms, an adjustment factor thattakes into account the effects of reflection losses and non-normal incidence on the cornea provides results for thecornea that more closely approach the experimental datafor myopic subjects. If we succeed in quantifying theo-retically the influence of any other of the above-mentioned variables that affect corneal ablation, we canverify whether the prediction fits the experimental re-sults. In this sense, the parameter corneal asphericity(although not highly correlated with visual performance,owing to the influence of other ocular surfaces19) can be ofgreat use, as it provides an average of corneal shape andis easily measured. It should be pointed out that the pro-cedure used by Huang et al.14 to analyze the effects ofcorneal-surface smoothing (comparison of experimentaldata with a theoretical prediction) resembles that used byAnera et al.,18 although Huang et al.14 did not study cor-neal asphericity. In both studies, it was crucial to as-sume that the Munnerlyn formula, or its paraxial ap-proximation, was applicable to the corneal ablation.
It is known that refractive surgery tends toward cus-tomized surgery, minimizing the aberrations of the eye(including the intraocular structures); for example, someof the new algorithms propose optimizing postsurgery cor-neal asphericity.20–24 In any case, noncustomized abla-tion remains highly useful for the study of refractive sur-gery from a practical standpoint. With customizedsurgery, in which the deviations with respect to the Mun-nerlyn formula or its paraxial approximation will be
init. prolate 0 , p ,
⇒ Q8 . Q decrease
init. oblate p . 1, Q
Considering the para
init. prolate 0 , p ,
⇒ p8 , p , 1 incre
init. oblate p . 1 ⇒
large, the difficulties in comparing the experimental re-sults with any modeling theory will be great if, as ex-pected, the algorithms are proprietary and it is not pos-sible to have access to them.
With respect to the data for hyperopia, with R8/R, 1, Eqs. (15) and (16) would indicate that
A discrepancy is also found between the two formulasfor initially prolate corneas. As in the case of myopia,the experimental data for hyperopia5 (at least for the la-ser system used by these authors), coincide with the trendshown by the paraxial approximation of Munnerlyn.8
4. CONCLUSIONSIn the present paper, we deduce a mathematical equationfor calculating the postsurgical corneal asphericity in thecase of applying the Munnerlyn formula without theparaxial approximation. This equation explains the re-sults reported by other authors indicating increased pro-lateness for initially prolate corneas when this equation isapplied. In addition, the equation deduced here shows amarked discrepancy with respect to the experimental re-sults for postsurgical corneal asphericity and to the equa-tion resulting from the application of the paraxial Mun-nerlyn formula.
From the analytical study of equations and experimen-tal data for corneal asphericity, we could deduce whetherthe Munnerlyn formula or its paraxial approximation, orslight deviations of either, are used in noncustomized ab-lation. Equations for corneal asphericity after surgerymay be of clinical relevance, for example, in studyingquantitatively the role of the different factors (such as de-centration, type of laser, optical role of the flap, woundhealing, biomechanical effects, technical procedures) dur-ing corneal ablation.
ACKNOWLEDGMENTWe thank David Nesbitt for translating the text intoEnglish. This research was supported by Ministerio deCiencia y Tecnologıa (Spain) grant BFM2003-1492.
Q , 0 ⇒R83
R3Q . Q
olateness (asphericity more positive),
0 ⇒ Q .R83
R3Q ⇒ 0 , Q8 , Q decrease oblateness.
approximation, Eq. (1), we get
⇒R83
R3p , p
prolateness (asphericity more negative),
3
p , p ⇒ p8 , p decrease oblateness.
1,
pr
.
xial
1
ase
R8
R3

Jimenez et al. Vol. 21, No. 1 /January 2004 /J. Opt. Soc. Am. A 103
The authors can be reached at [email protected].
REFERENCES1. J. T. Holladay, D. R. Dudeja, and J. Chang, ‘‘Functional vi-
sion and corneal changes after laser in situ keratomileusisdetermined by contrast sensitivity, glare testing, and cor-neal topography,’’ J. Cataract Refract. Surg. 25, 663–669(1999).
2. J. T. Holladay and J. A. Janes, ‘‘Topographic changes in cor-neal asphericity and effective optical zone after laser in situkeratomileusis,’’ J. Cataract Refract. Surg. 28, 942–947(2002).
3. E. Moreno-Barriuso, J. Merayo-Lloves, S. Marcos, R. Na-varro, L. Llorente, and S. Barbero, ‘‘Ocular aberrations be-fore and after myopic corneal refractive surgery: LASIK-induced changes measured with laser ray tracing,’’ Invest.Ophthalmol. Visual Sci. 42, 1396–1403 (2001).
4. R. G. Anera, J. R. Jimenez, L. Jimenez del Barco, J. Bermu-dez, and E. Hita, ‘‘Changes in corneal asphericity after la-ser in situ keratomileusis,’’ J. Cataract Refract. Surg. 29,762–768 (2003).
5. C. C. Chen, A. Izadshenas, A. A. Rana, and D. T. Azar, ‘‘Cor-neal asphericity after hyperopic laser in situ keratomileu-sis,’’ J. Cataract Refract. Surg. 28, 1539–1545 (2002).
6. J. R. Jimenez, R. G. Anera, and L. Jimenez del Barco,‘‘Equation for corneal asphericity after corneal refractivesurgery,’’ J. Refract. Surg. 19, 65–69 (2003).
7. J. R. Jimenez, R. G. Anera, L. Jimenez del Barco, and E.Hita, ‘‘Effect on laser-ablation algorithms of reflectionlosses and nonnormal incidence on the anterior cornea,’’Appl. Phys. Lett. 81, 1521–1523 (2002).
8. J. R. Jimenez, R. G. Anera, L. Jimenez del Barco, and E.Hita, ‘‘Predicting changes in corneal asphericity after hy-peropic laser in situ keratomileusis,’’ J. Cataract Refract.Surg. 29, 1468 (2003).
9. D. Gatinel, T. Hoang-Xuan, and D. T. Azar, ‘‘Determinationof corneal asphericity after myopia surgery with the exci-mer laser: a mathematical model,’’ Invest. Ophthalmol.Visual Sci. 42, 1736–1742 (2001).
10. C. R. Munnerlyn, S. J. Koons, and J. Marshall, ‘‘Photore-fractive keratotomy: a technique for laser refractive sur-gery,’’ J. Cataract Refract. Surg. 14, 46–52 (1988).
11. J. T. Lin, ‘‘Critical review on refractive surgical lasers,’’ Opt.Eng. 34, 668–675 (1995).
12. J. R. Jimenez, R. G. Anera, and L. Jimenez del Barco, ‘‘Ef-fect on visual function of approximations of the corneal-
ablation profile during refractive surgery,’’ Appl. Opt. 40,2200–2205 (2001).
13. D. Gatinel, J. Malet, T. Hoang-Xuan, and D. T. Azar,‘‘Analysis of customized corneal ablation: theoretical limi-tations of increasing negative asphericity,’’ Invest. Ophthal-mol. Visual Sci. 43, 941–948 (2002).
14. D. Huang, M. Tang, and R. Shekhar, ‘‘Mathematical modelof corneal surface smoothing after laser refractive surgery,’’Am. J. Ophthalmol. 135, 267–278 (2003).
15. M. Mrochen, M. Kaemmerer, P. Mierdel, and T. Seiler, ‘‘In-creased higher-order optical aberrations after laser refrac-tive surgery,’’ J. Cataract Refract. Surg. 27, 362–369 (2001).
16. A. W. Chang, A. C. Tsang, J. E. Contreras, P. D. Huynh, C.J. Calvano, T. C. Crnic-Rein, and E. H. Thall, ‘‘Corneal tis-sue ablation depth and the Munnerlyn formula,’’ J. Cata-ract Refract. Surg. 29, 1204–1210 (2003).
17. C. Roberts and W. Dupps, ‘‘Corneal biomechanics and theirrole in corneal ablative procedures,’’ in Customized CornealAblation: the Quest for Supervision, S. M. MacRae, R. R.Krueger, and R. A. Applegate, eds. (SLACK Inc., Thorofare,N.J., 2001), pp. 109–132.
18. R. G. Anera, J. R. Jimenez, L. Jimenez del Barco, and E.Hita, ‘‘Changes in corneal asphericity after laser refractivesurgery, including reflection losses and nonnormal inci-dence upon the anterior cornea,’’ Opt. Lett. 28, 417–419(2003).
19. R. A. Applegate, G. Hilmantel, H. C. Howland, E. Y. Tu, T.Starck, and E. J. Zayac, ‘‘Corneal first surface optical aber-rations and visual performance,’’ J. Refract. Surg. 16, 507–514 (2000).
20. T. Seiler, U. Genth, A. Holschbach, and M. Derse, ‘‘Asphericphotorefractive keratectomy with excimer laser,’’ Refract.Corneal Surg. 9, 166–172 (1993).
21. J. Schwiegerling and R. W. Snyder, ‘‘Corneal ablation at-terns to correct for spherical aberration in photorefractivekeratectomy,’’ J. Cataract Refract. Surg. 26, 214–221(2000).
22. S. MacRae, J. Schwiegerling, and R. W. Snyder, ‘‘Custom-ized and low spherical aberration corneal ablation design,’’J. Refract. Surg. (Suppl.) 15, S246–S248 (1999).
23. F. Manns, A. Ho, J. M. Parel, and W. Culbertson, ‘‘Ablationprofiles for wavefront-guided correction of myopia and pri-mary spheical aberration,’’ J. Cataract Refract. Surg. 28,766–774 (2002).
24. J. A. Dıaz, R. G. Anera, J. R. Jimenez, and L. Jimenez delBarco, ‘‘Optimum corneal asphericity of myopic eyes for re-fractive surgery,’’ J. Mod. Opt. 50, 1903–1915 (2003).