control measures for physicians' fee payments under provincial health insurance schemes
TRANSCRIPT

Control Measures for Physicians' Fee Payments Under Provincial Health Insurance SchemesAuthor(s): R. Després, R. G. Murray, A. W. Titus, N. Yourechuck and A. P. RudermanSource: Canadian Journal of Public Health / Revue Canadienne de Sante'e Publique, Vol. 62, No.4 (July/August 1971), pp. 271-284Published by: Canadian Public Health AssociationStable URL: http://www.jstor.org/stable/41984951 .
Accessed: 18/06/2014 14:35
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
Canadian Public Health Association is collaborating with JSTOR to digitize, preserve and extend access toCanadian Journal of Public Health / Revue Canadienne de Sante'e Publique.
http://www.jstor.org
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions
Control Measures for Physicians' Fee Payments
Under Provincial Health Insurance Schemes
R. Després, R. G. Murray, m.d., A. W. Titus, m.d., and N. Yourechuck. Edited by A. P. Ruderman1, ph.d.
A symposium on management problems in fee payment under provincial health insurance schemes was held during the annual meeting of the Cana- dian Public Health Association in Toronto in April 1971. While the original planning of the program was undertaken by the Medical Care Section of the CPHA, the subject reflected the growing interest in managerial aspects of health administration of the newly-formed Organization and Administration of Health Services Division of CPHA.
Since the theme is of wide general interest , the four papers presented at the symposium are reproduced below in somewhat condensed form , together with a brief summary of the discussion that followed. It is hoped that readers with responsibilities as claims managers , assessors and con- sultants in the different provinces will also find this exchange of views helpful in their own work , and that the general membership of the CPHA will obtain some useful insights into this field. The papers are presented in alphabetical order by province.
By way of introduction of the authors Mr. Després is President of the Quebec Health Insurance Board. Dr. Murray is Chairman of the Saskatche- wan Medical Care Insurance Commission , Dr. Titus is Medical Director of Maritime Medical Care, Ine ., Mr. Yourechuck is Director of Claims of the Manitoba Health Services Commission , and Dr. Ruderman is Professor of Health Administration, School of Hygiene, University of Toronto.
MANITOBA
'THE payment of fees by the Manitoba Health Services Commission is the respon-
sibility of the Claims Department, and the claims, on receipt, are handled by the Coding Section of that Department. Claims are sort- ed into fields of practice for coding (surgery, pediatrics, internal medicine, etc.) and each field of practice is assigned to a unit within
1. Address reprint requests to Dr. A. P. Ruderman, Professor of Health Administration, School of Hygiene, University of Toronto, Toronto 5, Ontario.
the Section, so that the clerks become famil- iar with a limited number of fields. They can often recognize inconsistencies by observa- tion and bring them to the attention of the medical assessors. The medical assessors -
physicians employed part-time under a ses- sional agreement - then observe the pat- terns of inconsistency and, if they are unable to justify them medically, ask the Medical Review Committee for a complete review of the physicians concerned.
271
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions

Some types of inconsistencies which have been detected through this method of obser- vation are (a) abnormal number of consulta- tions between physicians; (b) abnormal num- ber of higher-fee immediate-response calls by a physician, as distinct from routine house calls; (c) abnormal laboratory pattern - e.g. the same series of tests regardless of condi- tion; (d) assistants' fees being claimed for procedures such as tonsillectomies, adenoidec- tomies and endoscopies.
It must be emphasized that the clerk is re- quired to make only a clerical judgment and not a medical one. If the medical assessors can justify the observed pattern, the claims are re-entered into the system for normal processing.
The "investigate" area of the Claims De- partment is staffed by three employees more senior than the claims coders, and in this area, as well as in coding, observation plays a big part in spotting possible abuse. The sen- ior employees review services which cannot be dealt with automatically by the computer because the indications are ambiguous and may require clerical interpretation or medical judgment for appropriate disposal.
Audit Confirmation The Audit Confirmation Program was ini-
tiated in early 1970 to obtain consumer con- firmation of physicians' claims. The first statements that went out to consumers were for all services rendered by opted-in physi- cians in the months of January and February 1970. In the case of opted-out physicians, the patients routinely receive monthly statements attached to their reimbursement cheque. Fol- lowing this once-only total coverage, the Commission sent confirmation statements to a random sample of 10 per cent of patients each month.
Patient Questionnaires A Medical Review Committee studied the
various patient complaints that had been re- vealed by the audit confirmation procedure. As a result, certain physicians were more
closely scrutinized by the Committee. On the recommendation of the Review Committee, the Commission flooded the service areas of these physicians, using a questionnaire with a stamped addressed envelope and inviting reg- istrants to reply. As a result of this audit, most patients confirmed the service claims of their physicians. Only 65 of some 2,000 pa- tients questioned some of the services claimed. Most of the queries had a simple ex- planation - e.g. names of physicians not recognized by the patient were usually those who performed X-ray or laboratory services at the request of the family doctor. On some occasions when a house call was billed, and the patient claimed that the physician had never made the call, it related to a special call to a hospital out-patient department which was allowable as a house call.
In the few cases where there were com- plaints which warranted investigation, the pa- tients made it clear that they had replied in confidence and did not want their names re- vealed in the course of the investigation. This is understandable because many patients live in localities with only one doctor and, in the interests of their families, are afraid to com- plain and worsen the doctor-patient relation- ship. The patient feels that he may be deny- ing his family medical attention in some fu- ture emergency.
As a result, the replies are kept confiden- tial and are kept on file by the secretary of the Review Committee for use if the physi- cian in question is interviewed.
The comments of patients make it clear that the public is more concerned with assur- ing access to medical care in case of need than with controlling costs. Patients are not sharply aware of the cost of medical services when a third party makes payment on their behalf.
Statistical Records In the absence of active patient support,
the Medical Review Committee obtains most of its information from statistical records. The mam tools are the chi-square test
272 Canadian Journal of Public Health Vol. 62
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions

(comparing observed with expected occur- rences), the use of patterns or profiles of practice, and the analysis of costs separately for each field of practice, ranking physicians in each field in descending order of cost for purposes of comparison. These methods serve only to bring a physician to the atten- tion of the Committee for review. The com- mittee then must search for a justification or clinical explanation of the deviation from normal. If they are unable to do so they will invite the physician under review to attend a meeting and explain. In the case of a satis- factory explanation, the procedure stops at this point. If no satisfactory explanation is given, the physician may be told to improve his pattern or be subject to a taxing formula.
To date the Manitoba Health Services Commission has not had occasion to apply the taxing formula. It has, however, re- covered approximately $4,000 from one phy- sician for services admittedly charged incor- rectly. The review process is a slow one, sometimes taking several meetings before a recommendation is made and carried through, and if a decision to tax a physician were to be reached, the legislation allows the decision to be appealed to an arbitration board. Taxing actions may be applied with less reluctance in the future, since, for the first time in the history of the Committee, a lay person has been named to membership.
Assessment and Benefit Policy Committee In addition to the measures outlined
above, an Assessment and Benefit Policy Committee was formed early in 1970. It con- sists of the medical director, the claims man- ager, the two medical assessors, a data-proc- essing and statistical specialist, and a secre- tary. This committee is concerned with claims involving complex assessment and
with benefit policy and interpretation. ' The
work of this committee has cleared up many gray areas of submission and assessment, and the information has been communicated to the medical profession through general bulle- tins and personal letters. Bulletins have been issued on such general subjects as the dis- tinction between immediate-response calls and routine house calls, allergy desensitiza- tion and office visits, and psychotherapy by persons other than psychiatrists. Letters are sent to individual doctors in an attempt to correct individual problem areas.
The integration of hospital and medical in- surance also has alerted the Commission to various areas where there may be a duplica- tion of payments. The area of diagnostic services in hospitals and health units is pres- ently being studied. In addition, this integra- tion makes possible immediate access to phy- sician and hospital claims for matching pur- poses, and the comparison of the two has produced interesting results.
The physician services or physician rela- tions department has been particularly valua- ble in dealing with and hopefully preventing abuse. Members of this department of the Commission make routine visits to doctors and receptionists and discuss proper claims submission and interpretations. They bring to the attention of physicians errors or oddities in claims. As a result doctors' offices are well informed and cannot use the excuse of cleri- cal error to explain discrepancies in their medicare billings to a review committee.
The medical review committee feels very strongly that there is no excuse for careless claiming - in their opinion a claim card is a blank cheque and therefore careless, incor- rect, or excessive billing could be construed to be fraud and should be dealt with ac- cordingly.
July/August 1971 Physicians' Fee Payments 273
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions
NOVA SCOTIA
MEDICARE in Nova Scotia is administered by Maritime Medical Care Incorporated (MMC), a physician-sponsored health insur- ance plan, which had twenty years' experi- ence in this field prior to medicare. It carries out its administrative duties under policy de- cisions laid down by a government-appointed Medical Care Insurance Commission which is directly responsible to the Minister of Health. From the onset of medicare in Nova Scotia there has been excellent liaison be- tween the Commission, the Medical Society and MMC and this, by means of joint com- mittees and liaison or negotiating bodies, has brought about the profession's acceptance of, and participation in, many control proce- dures.
Identification of Problems Requiring Controls The past experience of MMC made it pos-
sible to identify most of the types of abuse that were likely to occur. The biggest job, at the onset, was to convert the manual process- ing of some 60,000 claims per month to computer processing of upwards of 220,000 claims per month - and still identify abu- sers. An effective computer program has been set up, supplemented by the work of some highly trained manual assessors. Never- theless changes are constantly being made in both areas as new types of abuses are uncov- ered.
The main areas of abuse, in broad terms, have been physician overservicing, overutili- zation by patients, fraud or attempted fraud, and miscellaneous abuses. The first three of these are well-recognized abuses in all plans, but in the miscellaneous area one finds costly abuses that are not so easily recognized or controlled.
For example, (1) a physician may claim for all members of a family on a house call when, in fact, only one member is examined. A similar situation may occur with patients in a nursing or rest home. (2) Members of a
group or clinic practice engage in frequent consultations and trading-around of patients. (3) Misuse of fee schedule code numbers -
submitting for a more major procedure than was performed. (4) Uninsured services charged under insured services codes, e.g. tubal ligation billed as appendectomy; pierc- ing of ears billed as treatment of otitis exter- na. (5) Late submission of claims in hopes they can't be assessed against patient histories for duplication. (6) Doctor refers everything out to confreres and treats very little himself. This way he can see many more patients dur- ing an office session and generate high in- come on volume alone. (7) Duplicate claim- ing from medicare and from the Workmen's Compensation Board or other insurance agency, e.g. life insurance examinations.
These, then, are some of the more subtle means by which abuse of a plan can and does occur and new ones are constantly com- ing to light. The difficulty is to identify them - particularly when nearly 80 to 85 per cent of the claims, if correctly made out by the physicians, can be automatically processed and paid through the computer without being examined by a human eye at all.
Overservicing by the Physician The number of services rendered by a phy-
sician, in relation to any given illness, is in the control of that physician - exclusive of the first visit which is patient-initiated. It is a primary rule of medicare plans to insure only medically necessary services. The physician is expected to govern his services accordingly. Unfortunately, this is not always the case. Therefore, some method of determining the cut-off point that is fair and acceptable to all concerned - doctor, patient, and plan - must be set up. There are many reasons for over-servicing, some of which are justified in the doctor's view, and some which are plainly not justified as they are done merely to gen- erate income and do not contribute to the
274 Canadian Journal of Public Health Vol. 62
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions
quality of care of the patient. Whatever the reason, be it the doctor's pattern of practice or for monetary reasons, controls are neces- sary.
Nova Scotia has built up the following progression of controls in regard to this prob- lem:
Computer Programming. The computer is programmed to reject all claims showing more than a certain number of services ren- dered a given patient in a given period of time, for a given diagnosis. These rejects, along with a complete "print-out" of that pa- tient's past history, are then examined man- ually by specially trained assessors who will exercise some judgment as to the medical ne- cessity for the volume of services claimed, Often the physician has written a note of ex- planation on his card which the computer cannot interpret. If no explanation is given, the assessor will look at the number of serv- ices claimed in relation to the diagnosis giv- en. If, in her opinion, the services appear ex- cessive, the assessor will then refer the claim to one of the medical directors for further judgment and possible referral to a Taxing Committee that can penalize the physician by lowering the amount reimbursed on claims.
The computer is also programmed, where possible, to reject claims which do not meet assessment rules laid down by the provincial tariff approved by the Commission. These claims also require manual assessing.
Medical Directors. Medical directors exam- ine unjustified claims referred by the assessor and give medical judgment based on their medical experience and knowledge. They may reduce the number of calls charged and return the claim to the system for payment, or they may retain it for the opinion of a Medical Taxing Committee. Also going to this Committee are claims appealed by physi- cians unwilling to accept any reduction ap- plied up to this stage by the manual or pro- fessional assessors.
The Medical Taxing Committee estab- lished by Maritime Medical Care, Incorpo-
rated, consists of five active practising physi- cians. Two are family practitioners, two are surgeons and one an internist. The committee also has a roster of specialist consultants who can be called upon to advise on a particular problem relating to their specialty. The com- mittee meets monthly and the problems con- sidered range from overservicing and overu- tilization to complicated cases and new pro- cedures not yet listed in the tariff. It reviews appeals from staff medical assessment deci- sions. Records are kept of each decision made and are tabulated for reference in han- dling similar cases in future for the sake of consistency. The physician concerned is also notified of the decision by letter. Very few physicians have exercised their right of ap- peal.
One of the main tasks of the Taxing Com- mittee is to seek out services which could be judged not to be medically necessary. These are refused payment, and the control feature lies in the hope that the physician will in turn charge these directly to the patient, thus making both a physician who is overservic- ing, or a patient who is overutilizing the plan, realize their responsibility in using the plan for necessary treatment only.
Any physician or patient who feels unfair- ly dealt with by any of the foregoing assess- ments may appeal, in writing, to the Presi- dent of Maritime Medical Care. He will have the case reviewed by the Board of Directors. If they can't resolve the problem, the whole matter is referred to the Commission which has the final say.
Medical Advisory Committee This is a priority committee of the Board
of Directors of MMC. Its six members are appointed by the Medical Society of Nova Scotia. Its present function is to deal with more serious aspects of claiming patterns, i.e. other than overservicing by a doctor or over- utilization by a patient, and advise the Board of its findings. It can only deal with matters referred to it by the Board and the
July/ August 1971 Physicians' Fee Payments 275
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions
Board is required to report, at least semi-an- nually, the activities of the Committee to the Commission and the Medical Society. The medicare administrators are tied into this committee by having the Medical Director or Associate Medical Director of MMC act as its permanent secretary.
Such a committee was necessary in Nova Scotia mainly because membership in the provincial medical society is not compul- sory. Therefore, if organized medicine is to play its part in any disciplinary function un- der the plan, such a committee gives the pro- vincial society, through its appointees, power to deal with all physicians - not only its own members.
The Medical Advisory Committee is now taking on new aspects of responsibility. Its duties now include studies of physicians' pro- files and patterns of practice with the object of using these reports not only as a control procedure but also to see if there is some way in which they can be used to improve the quality of medical care provided to resi- dents of Nova Scotia. This is a research pro- ject only in its infancy. The medical school is also attempting to find a way of using medi- care statistics, through physician pattern-of- practice studies, to enable the school to pin- point areas where a given physician may need further postgraduate training in a par- ticular aspect of his practice, to his and his patients' advantage. This type of research, which can accrue from well planned medi- care statistics, has tremendous possibilities in controlling spiraling costs by producing bet- ter doctors who will deliver medical services more efficiently.
Miscellaneous Controls The Act and Regulations include other
controls which are deterrents to abuse, such as (1) fines for providing misinformation; (2) power to expel from the plan a physician who continually breaks the rules; (3) presen- tation of claims for payment within one year from date of service; (4) special assessment
rules negotiated with the Nova Scotia Medi- cal Society which in effect alter the preamble of the Society's fee schedule; (5) resident eli- gibility controls; and (6) late filing penalty. Each of these, in its own way, acts to control abuse.
In addition to controls under the Act, as- sessment rules, and committees, a good pro- gram of professional relations serves as a control as well. If Medicare representatives keep the doctors informed of changes in rules or fees, visit them, talk to them, and are fair in assessments, abuses will diminish. The Medical Director or Associate Director at- tend all provincial branch medical society meetings where any complaints can be met "head on" and one can personally confront a particular physician with whom the plan may be having problems. Regional seminars are also conducted periodically for physicians' office staff at which medicare staff try to learn their problems and straighten them out. We feel this sort of co-operation has prevent- ed many things that would go on and become abuses of the plan.
Overutilization The patients who use physicians' services
unnecessarily include, among others, neurot- ics, psychotics, and drug addicts. Attempts to curtail these people cause "open mike" wires to start humming, and letters to flow, espe- cially to politicians.
An "overuse letter" is employed in this sit- uation which has been very carefully worded to avoid any possible offence. It merely points out to the patient that, because of the pattern of excessive physician services being claimed, the plan will in future specially re- view all claims and will only accept for pay- ment those deemed medically necessary. The remainder can be billed directly*, to him by his physician. This letter is only used when the attending physician requests it be sent or has expressed his opinion that a certain patient is abusing his services.
Drug addicts are being identified by medi-
276 Canadian Journal of Public Health Vol. 62
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions

care, as are individuals who run from doctor to doctor. One is recorded as attending eight physicians in one day. Medicare plans may have a responsibility in notifying all physi- cians concerned in such cases in an attempt to control such abuses. Perhaps this is an area where liaison of the medicare plans with public health departments might be of some benefit.
Fraud Fraud and attempts to defraud the plan
must always be watched for. Major fraud, once discovered and proven, poses no prob- lem. Such cases are simply turned over to the provincial Attorney General's Depart- ment to confirm the findings, and only the Minister of Health can give the go-ahead to prosecute. Minor misdemeanours, as noted earlier, are dealt with by the Medical Advi- sory Committee. A random sample audit of claims is used to identify those physicians who are misusing the plan. An audit letter asking the patient to confirm or deny services paid for by the plan is sent out to one per cent of claims. The rate of reply to these letters is presently running at better than 80 per cent. When a denial is received, it is checked out very carefully by the Special Services and Audit Department. Such a deni- al may prompt a concentrated audit of that physician's practice and a special in-depth study of his profile and pattern of practice.
This system of auditing may not be the best and we know it has many drawbacks; however, it is economical to operate and is effective even if only psychologically; for the physicians know it is in effect on a regular basis. This system also has the backing of the provincial medical society.
Controls on Public Usage Needed Before concluding this discussion, I would
like to make a few general remarks in regard to control procedures as they apply to gov- ernment operated medicare plans. I might add that these are my own views and not necessarily shared by the Commission. I be-
lieve we have put far too much emphasis on building up controls on the physicians who, for the most part, I find to be basically hon- est. We have not gone far enough in finding politically and publicly acceptable methods to control abusing patients.
Too much onus is being placed on the physician to control his patients himself. I don't believe he is always in a position to do this without the danger of being accused of malpractice, carelessness, or lack of interest in his patients' welfare, and this could seriously upset the doctor-patient relationship. I be- lieve government through some of its organi- zations, such as public health departments, medicare commissions, etc., will some day have to "bite the bullet" and evolve some sort of controls applying to the public's usage of medical and surgical services - be they po- litically expedient or not. It is a well-known fact that payment for health services is one of the biggest items of government budgets wherever such plans exist. Such controls must be fairly applied to allow the physician to continue to provide a high level of quality care to his patient with dignity and respect to both: otherwise, the plan fails.
Other Reasons for High Income Physicians Just because a physician is earning a high
income under medicare does not always mean something is "rotten in Denmark." Some physicians are more highly organized and experienced than others and can, there- fore, deliver health care more efficiently than others. Others work harder. Adjusting fees in a fee schedule will never correct these dis- crepancies under a fee-for-service system of payment, yet they are the ones everyone no- tices and public reaction to high physician in- comes may put the whole principle of fee- for-service in clanger. "Formula payments" and a salary system have already been men- tioned in some circles. I believe that the day will come when we will have better record linkage with other government agencies pres- ently paying doctors for health services, in- cluding the Workmen's Compensation
July/ August 1971 Physicians' Fee Payments 277
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions
Boards, Department of Veterans Affairs, and insurance companies. These agencies present- ly pay for certain physician services apart from medicare when, in fact, medicare may have already paid for the same service. One suggestion has been that medicare process the physicians' claims for these bodies, thus preventing double payments.
Another type of control is being discussed and that is to put a time factor on each type of service a doctor performs. Thus, he would be able to claim only a fixed number of serv- ices per day. I don't see this system as ever being accepted by the medical profession, al- though it is not without merit, particularly for certain services.
Conclusion In conclusion I would defend our rather
elaborate control measures, which I have out- lined very briefly, with the statement that "it's not what you catch, it's what you pre- vent" that is important. We can always calcu- late how much we catch but we will never know how much we have prevented. For ex- ample, in our first fiscal year total claims paid were approximately $750,000.00 less than the total value of claims submitted. Our control procedures were largely responsible for this significant saving, and I've no doubt new forms of controls will be formed as new abuses come to light.
QUEBEC
UNIVERSAL Health Insurance came into force in Quebec on November 1, 1970. To carry out this legislation, the administrative machinery required had to be based on the most modern management concepts with a view to maximum efficiency.
The Quebec Health Insurance Board was established in June 1969, and was assigned the task of implementing the Health Insur- ance Plan. The Board has developed an or- ganization and has designed systems that en- able it to administer the Plan efficiently and that may be readily modified to adapt to new situations. Before dealing with the subject of management problems in fee payment, it is essential to provide a general outline of the internal structure of the Board so that the rest may be more easily understood.
The Quebec Health Insurance Board is a public corporation, made up of 14 members representing various sectors of the popula- tion. The President of the Board is also Gen- eral Manager. The organizational structure
consists of seven main managerial divisions. Secretariat and Legal Affairs, responsible for all legal matters; Operations , responsible for the entire process of claims assessment and payment; Professional Affairs, responsible for advising the Board in matters pertaining to carrying out the Plan and for co-ordinat- ing the Board's activities with health profes- sionals. Research and statistics come under this Division; Administration and Finance, which acts in an advisory capacity and which co-ordinates all matters dealing with account- ing, budgeting, treasury, financial analyses, and auxiliary services; Personnel, which is re- sponsible for recruitment, selection and hir- ing of staff, industrial relations, human re- source planning, and training; Public Rela- tions, whose main responsibility consists in providing information and publicity services; and Pharmaceutical Affairs, which will ad- minister the drug assistance program that is expected to come into effect during 1971.
Among the various systems involved, the claims processing system is a most up-to-date
278 Canadian Journal of Public Health Vol. 62
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions

one which involves the use of modern data processing and computer equipment that is used from the moment claims are received up to the issuing of payment to the health professionals.
The Board has some 1,200 employees to meet the needs of more than 6,000,000 bene- ficiaries and close to 9,000 health profession- als. It has a daily processing capacity of about 120,000 claims, covering more than 35,000,000 medical acts per year.
The operation of a plan such as the Que- bec Health Insurance Plan, especially at the beginning, calls for continuous adjustment. As well as providing a high degree of flexibil- ity within its internal structures and numer- ous systems, it was necessary to provide, just as in any other well-organized body, certain mechanisms for the prevention, detection, and correction of possible abuses within a so- cial measure of such broad scope as universal health insurance - possible abuses on the part of the beneficiary as well as on the part of those dispensing insured services.
The Power of Enquiry Bill 8, which established the Quebec Uni-
versal Health Insurance Plan, gives the Board the powers of enquiry into any matter within its competence. These powers are conferred upon the Board both with regard to the bene- ficiary and those who dispense insured serv- ices. It should also be noted that the agree- ments concluded between the Minister of So- cial Affairs and the various organizations representing the health professionals contain provisions with a view to eliminating certain abuses from the outset.
For example, committees for the assess- ment of claims are formed for each profes- sional group. By means of these committees, many questions are answered regarding fees claimed for complex procedures and in re- spect to professional practices considered to be quantitatively abnormal. The committees also recommend to the Board to inform the College of the professional in question on the
facts concerning any abuses of a quantitative nature or concerning professional ethics.
The agreements also provide mechanisms for submitting grievances. They make provi- sion for the formation of councils of arbitra- tion to which any health professional may have recourse if he feels that his rights have been encroached upon. Moreover, the agree- ments provide for the formation of joint commissions made up of representatives of the Minister of Social Affairs and of the or- ganizations representing the health profes- sionals. The purpose of these commissions is to supervise the application of the agree- ments, to prevent abuses in the provision and consumption of insured services, and tó pre- vent any imbalance between the income of professionals of the same category.
Financial Management and Professional Practice
With regard to the role of the Quebec Health Insurance Board, a distinction must be made between professional practice and the administration of the Health Insurance Plan. The Board has no right to interfere in the standards of professional practice. Any problem of this nature is referred to the Col- lege that licensed the professional in question to practise, and only this College is empow- ered to look into such matters as standards of professional practice.
The role of the Board does not consist, therefore, in controlling professional activity, but rather in assessing claims submitted for payment after insured services have been ren- dered to beneficiaries.
On the administrative level, since the Board was entrusted with the administration of public funds, it must see to it that these funds are used in keeping with the Act, the Regulations and the Agreements.
Verification System With this in view, the Board has designed
a system to ensure that the payments made to the health professionals correspond exactly to
July/ August 1971 Physicians' Fee Payments 279
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions

the services rendered, as well as to the bene- ficiaries on whose behalf the Board has paid the claims.
This system consists of sampling claims al- ready paid. A form is sent to the person whose name is written on the claim chosen, to inform him of the services paid on his be- half and rendered on a given date. At the same time, the beneficiary is asked to inform the Board of any inaccuracy he may notice. Approximately one per cent of claims paid by the Board will be sent to beneficiaries. This will be done through a predetermined sampling method that will cover all health professionals over a two-year period.
In this entire process the Board ensures that the confidentiality of the medical act performed is respected. Even the nature of the services rendered is never stated precise- ly. Moreover, enquiries are made in such a way as to respect fully the personal privacy of those concerned.
This verification has but one purpose - that of supplying the Board with an adequate method of obtaining such indications as may enable it to detect possible error or abuse. There is no question of the Board passing judgment on the basis of fragmentary infor- mation. However, should a serious doubt ex- ist, the Board must continue to investigate in order to certify the authenticity of the infor- mation obtained.
Inquiry Service The Board has set up an Inquiry Service
whose primary responsibility is to examine complaints from beneficiaries and to verify the authenticity of any anomalies detected through the payments system. The principal complaints or anomalies concern: demands for extra payments or supplementary fees; fees claimed for services not rendered; non- participating professionals who fail to advise their patients; beneficiaries claiming for serv- ices supposedly rendered outside the province but not actually received.
The Inquiry Service must, first of all,
make sure that complaints or anomalies are substantiated by facts before beginning any investigation with a view to producing proof. When proof is completed, the file is studied by the Board and the Board decides on the measures to be taken in accordance with the judicial recourse provided in the Act.
Needless to add, the investigators, in carry- ing out their work, must use caution in order to avoid causing prejudice to any party what- soever.
Practice Profile The verification system and the inquiry
service constitute the direct means of coun- teracting abuse. There are also built-in mech- anisms in the Board's administrative machin- ery whose mere existence enables the Board to curb excessive practices. Under the Profes- sional Affairs Division, an operational unit has been created to study and analyze the practice profile of the health professionals.
This latter service will prove to be of inval- uable assistance in enlightening those re- sponsible for repressing possible abuses. By means of practice profiles a certain number of anomalies might be detected. It could hap- pen that certain abnormal practice patterns would be discovered regarding a given pro- fessional or a group of professionals.
The analysis of such patterns by the Board will, no doubt, result in the submission of cases to the College of the professional in question or to one of the joint commissions.
The practice profiles of all the profession- als of the province to whom the Board pays fees are analyzed by health professionals who, themselves, are employees of the Board. With regard to detection of abuse, these pro- fessionals work in close co-operation with the heads of the Inquiry Service and of the serv- ice in charge of the payments veritification system.
To sum up, the Board has elaborated a method which enables it to ensure, in a real- istic manner, that payments of fees issued to health professionals are actually due. At the
280 Canadian Journal of Public Health Vol. 62
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions
same time, the Board is perfectly aware of the delicate role it has to play in the matter because of the implications of such controls when dealing with the health professionals.
These methods of verification and control throw no shadow on the good faith of the health professionals; their only purpose is to
prevent abuse and to ensure efficient admin- istration.
The repression of abuse and fraud is not, however, our first preoccupation. Our main objective is to carry out the Health Insurance Plan in keeping with the Act, Regulations, and the Agreements.
SASKATCHEWAN
ANY insuring agency has the right to ex- pect that the service claimed for payment is the service given. On the surface this would seem to be an easy problem. However, while it may be obvious that an office call that was claimed was in truth only a telephone call, or that the office call merely involved a patient dropping in to pick up a prescription, what about the complete examination that only took three minutes? - or when the patient stated that he was never completely un- dressed? - or when only heart, chest, and mouth were examined? These are one set of problems that confront the insuring agency.
The larger and more complex problem is the one where there is no disagreement that the service was given, but the quantity is in dispute - the so-called overservicing - which has yet to be satisfactorily defined, if that is possible.
Probably the smallest problem, and yet the loudest heard in some areas, is overutilization by beneficiaries.
In view of these and related problems, the Saskatchewan Medical Care Insurance Com- mission has for a number óf years conducted both general and special verification for in- sured services paid by it to providers of serv- ices. These operations are conducted by both computer and manual methods.
General Verification The routine or general verification, which
is carried out throughout the province, is done on computer equipment. The computer is programmed to print out verifications of a wide range of services, including such vol- ume items as visits, consultations, and specif- ic procedures. Every other month 16,000 families have claims verified through them. A family could have up to a maximum of 10 lines of service verified. An example of the computer verification report is shown in Fig- ure 1.
Special Verification Special verifications are undertaken as
manual operations by the staff of the Com- mission. They are usually indicated where disagreements of an increased frequency have been noted in the general verification program, i.e., it may be detected that, on the general verification program, a number of beneficiaries disagree whether they have or have not had a complete examination; this might lead the Commission to institute a spe- cial verification on complete examinations for the doctor concerned.
For the special verification program to be effective, it is essential that close co-ordina- tion be maintained among all elements con- ducting the verification operation.
July/ August 1971 Physicians' Fee Payments 281
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions
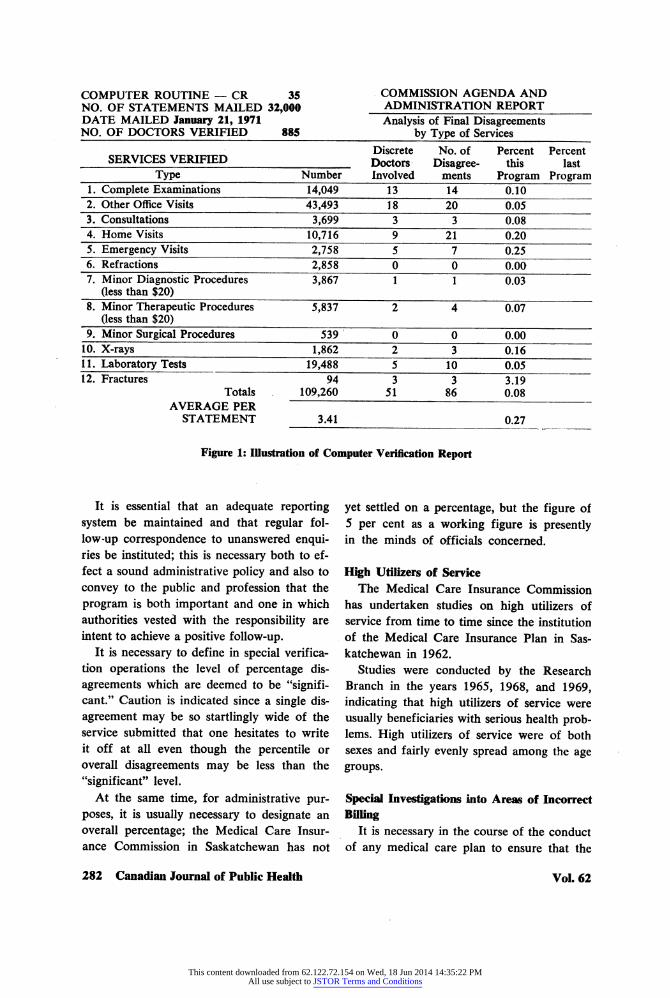
COMPUTER ROUTINE - CR 35 COMMISSION AGENDA AND NO. OF STATEMENTS MAILED 32,000 ADMINISTRATION REPORT DATE MAILED January 21, 1971 Analysis of Final Disagreements NO. OF DOCTORS VERIFIED 885 by Type of Services
_ „ Discrete No. of Percent Percent SERVICES _ „ VERIFIED Doctors Disagree- this last
Type Number Involved ments Program Program 1. Complete Examinations 14,049 13 14 0.10 2. Other Office Visits 43,493 YS 20 0.05 3. Consultations 3,699 3 3 0.08 4. Home Visits 10,716 9^ 21 0.20 5. Emergency Visits 2,758 5 7 0.25 6. Refractions 2,858 0 0 Q.QQ 7. Minor Diagnostic Procedures 3,867 1 1 0.03
(less than $20) 8. Minor Therapeutic Procedures 5,837 2 4 0.07
(less than $20) 9. Minor Surgical Procedures 539 0 0 0.00 10. X-rays 1,862 2 3 (Ū6 11. Laboratory Tests 19,488 5 10 Q.Q5 12. Fractures 94 3 3 3.19
Totals 109,260 51 86 0.08 AVERAGE PER
STATEMENT 3.41 027
Figure 1: Illustration of Computer Verification Report
It is essential that an adequate reporting system be maintained and that regular fol- low-up correspondence to unanswered enqui- ries be instituted; this is necessary both to ef- fect a sound administrative policy and also to convey to the public and profession that the program is both important and one in which authorities vested with the responsibility are intent to achieve a positive follow-up.
It is necessary to define in special verifica- tion operations the level of percentage dis- agreements which are deemed to be "signifi- cant." Caution is indicated since a single dis- agreement may be so startlingly wide of the service submitted that one hesitates to write it off at all even though the percentile or overall disagreements may be less than the "significant" level.
At the same time, for administrative pur- poses, it is usually necessary to designate an overall percentage; the Medical Care Insur- ance Commission in Saskatchewan has not
yet settled on a percentage, but the figure of 5 per cent as a working figure is presently in the minds of officials concerned.
High Utilizers of Service The Medical Care Insurance Commission
has undertaken studies on high utilizers of service from time to time since the institution of the Medical Care Insurance Plan in Sas- katchewan in 1962.
Studies were conducted by the Research Branch in the years 1965, 1968, and 1969, indicating that high utilizers of service were usually beneficiaries with serious health prob- lems. High utilizers of service were of both sexes and fairly evenly spread among the age groups.
Special Investigations into Areas of Incorrect Billing
It is necessary in the course of the conduct of any medical care plan to ensure that the
282 Canadian Journal of Public Health Vol. 62
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions
service which is billed for is the type of serv- ice which has in fact been rendered. It was of interest in Saskatchewan to note that a con- siderable number of services were billed to the Commission purporting to indicate that blood sugar and blood urea determinations had been performed by a laboratory glass- ware-technology method when in fact they had been done on pre-packaged paper deter- minative strips. As a result of this investiga- tion it was noted that a considerable number of physicians had billed the Commission for a sum of approximately $17,000, this sum was subsequently recovered.
Incorrect Use of Nursing Home Billing Pat- terns
Items which have caused concern to the Medical Care Insurance Commission in Sas- katchewan are home visit items which are billed for visiting patients in special-care homes or nursing homes.
One interesting study revealed a very high degree of billing by one particular physician
in which he billed for all patients at full rate ($9.00) rather than the rate which should have existed, first patient at $9.00, subse- quent patients at $4.00. This investigation led to a recovery of about $1,700.00.
Profiles Physicians' profiles, which were imple-
mented in December 1964, are based upon payments made by the Medical Care Insur- ance Commission and reports received from hospital out-patient departments, non-hospi- tal facilities, and the provincial laboratory for beneficiaries under the plan. A total of 70 characteristics are analyzed for 28 groups of physicians.
The computer is programmed so that all physicians who vary by two or more standard deviations of their group mean with respect to one or more of (1) approved amount per patient, (2) generated approved amount per patient, and (3) generated services, will be re- ferred to the College of Physicians and Sur- geons of Saskatchewan for review.
DISCUSSION
In the general discussion, the importance of good personal relations between the health insurance program and the medical profes- sion was emphasized. This had worked to the advantage of the health insurance programs in Manitoba and Nova Scotia in particular. In Manitoba, the provincial government had used the pre-existing physician-sponsored Manitoba Medical Services program as the government's agent during the first year of medicare, and had subsequently absorbed the agency into the Manitoba Health Services Commission. Mr. Yourechuck, for example, was able to benefit from the goodwill built up under the physician-sponsored plan and
explain to the medical profession that good billing procedure and adherence to Commis- sion rules was in their own best interest.
In Nova Scotia, the pre-existing physician- sponsored Maritime Medical Services, Inc. simply carried on as before in an administra- tive sense, though now reporting to the Nova Scotia Medical Care Insurance Commission. The Nova Scotia experience in court con- trasted to that of Saskatchewan, where a criminal prosecution for fraud had led to the acquittal of the defendant although there re- mained a good prospect of recovering much of the money in question through a separate action under different rules of evidence. The
July/ August 1971 Physicians' Fee Payments 283
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions

original Saskatchewan payment procedures had not set a time limit for presentation of claims, and it was felt that the case in ques- tion would likely not have arisen under the newly-adopted twelve-month time limit.
There was general agreement that comput- erized profiles and patterns of practice were an invaluable administrative tool, and it was noted that similar profiles were being devel- oped in Ontario and other provinces that had not contributed papers to the symposium. The handling of cases uncovered through the profile technique varied from province to province, and the willingness of provincial colleges of physicians and surgeons to take responsibility for disciplinary procedures also varied.
There was a general reluctance to use pen- al sanctions, and a number of instances were cited of the effect of personal letters and in- terviews on both physicians and patients who were felt to have overserviced or overutilized. The older provincial programs such as that of Saskatchewan had, over the years, had more occasion to use penal sanctions - the most common being reimbursement at a low- er rate of claims felt to involve overservicing.
All the participating provinces had a
roughly similar system of handling claims, starting with machine processing and assess- ment under simple rules that could be pro- grammed into the computers, followed by manual assessment of cases where the com- puter could not make a decision and cleri- cal rather than medical judgment was in- volved, with referral of the remaining un- solved problems to medical assessors and fi- nally to a medical review committee, with various appeal procedures stipulated.
Finally, cases were noted in several provinces where overutilization had, on in- vestigation, turned out to arise from psycho- logical problems of the patient. Patient atti- tudes were also important in verifying over- servicing, and some questions were raised about the long-run effectiveness of direct mail inquiries to patients, once the first flush of interest in new provincial health care pro- grams had worn off. In the long run, so long as the public at large did not feel a sense of personal financial involvement and were more interested in maintaining good physi- cian-patient relations, internal administrative procedures were likely to prove more useful than those that had to depend on patient co- operation.
284 Canadian Journal of Public Health Vol. 62
This content downloaded from 62.122.72.154 on Wed, 18 Jun 2014 14:35:22 PMAll use subject to JSTOR Terms and Conditions