control and responsibility in addicted individuals: what do addiction neuroscientists and clinicians...
TRANSCRIPT

Control and Responsibility in Addicted Individuals:What do Addiction Neuroscientists and Clinicians Think?
Adrian Carter & Rebecca Mathews &
Stephanie Bell & Jayne Lucke & Wayne Hall
Accepted: 23 September 2013# Springer Science+Business Media Dordrecht 2013
Abstract Impaired control over drug use is a definingcharacteristic of addiction in the major diagnostic sys-tems. However there is significant debate about theextent of this impairment. This qualitative study exam-ines the extent to which leading Australian addictionneuroscientists and clinicians believe that addicted indi-viduals have control over their drug use and are respon-sible for their behaviour. One hour semi-structured in-terviews were conducted during 2009 and 2010 with 31Australian addiction neuroscientists and clinicians (10females and 21 males; 16 with clinical experience and15 with no clinical experience). Although many addic-tion neuroscientists and clinicians described uncon-trolled or compulsive drug use as characteristic of ad-diction, most were ambivalent about whether or notaddicted people could be said to have no control of theirdrug use. Most believed that addicted individuals havefluctuating levels of impaired control over their drug usebut they nonetheless believed that addicted persons wereresponsible for their behaviour, including criminal be-haviour engaged in to fund their drug use. Addictionwas not seen as exculpating criminal behaviour but as amitigating factor.
Keywords Addiction . Drug use . Control .
Responsibility . Compulsion . Attitudes . Qualitativeresearch
Introduction
Compulsive drug use and impaired control over druguse are defining features of addiction in the major sys-tems of classification [1–3]. Despite this, there is debatewithin the addictions field as to whether: 1) addictedpersons are able to exert control over their drug use andunder what circumstances; and 2) whether they shouldbe held fully responsible for criminal acts committed tofund their drug use.
Prominent neuroscientists at the National Institute onDrug Abuse (NIDA) have argued that the chronic use ofaddictive drugs “hijacks” the brains of addicted individ-uals so that they are driven to use drugs [4, 5]. Thedegree to which addicted individuals can control theirdrug use and take responsibility for their actions hasimportant clinical, ethical and legal implications for theway that we treat addicted persons, particularly thosewhose behaviour harms others or involves criminal acts.
Drug Use is a Choice: The Moral Model of Addiction
The traditional moral view of drug use is that drugusers voluntarily engage in drug use and hence shouldbe morally responsible for their drug use and for crim-inal acts involved in obtaining drugs or committedwhile intoxicated. To those who are sceptical of the
NeuroethicsDOI 10.1007/s12152-013-9196-6
A. Carter (*) :R. Mathews : S. Bell : J. Lucke :W. HallUniversity of Queensland Centre for Clinical Research,The University of Queensland, Herston Road, Brisbane,Queensland 4029, Australiae-mail: [email protected]
W. HallQueensland Brain Institute, The University of Queensland,Brisbane, Queensland 4072, Australia

idea of addiction, addiction is simply an excuse usedby drug users to evade responsibility for their unlawfulor socially deviant behaviour [7–10]. In Foddy andSavulescu’s liberal account of addiction [10], theyargue that decisions to use drugs are just like any otherdecisions that an individual makes about whether toengage in a rewarding behaviour, such as deciding toeat strawberries or carrots.
A number of arguments are offered in support of thisview. Drug use is, at least initially, a voluntary choice.Heavy drug use occurs in only a minority of those whouse drugs, most of whom stop using drugs withoutassistance [11–13]. Even putatively addicted drug usersengage in considerable planning to obtain and use theirdrug of choice and their drug use can be reduced bycontingency management programs that offer financialincentives for clean urine samples [14, 15]. Addictivedrug use is also influenced by changes in the price ofdrugs in ways that would be difficult to explain if indi-viduals’ behaviour were solely driven by impaired brainfunction [16]. According to these critics, the ability ofexternal factors to influence drug use suggests that itremains under some level of rational control and decisionmaking even in putatively “addicted” drug users.
Addiction as a Brain Disease
Clinicians who deal with addicted persons have longargued that addiction is a disease that robs affectedindividuals of their ability to control their drug use. Thisview was first advocated for alcoholism in the late 18thcentury and early 19th centuries by Benjamin Rush inthe USA and Thomas Trotter in the UK. A version ofthis model was promoted in the late 1930s by the foun-ders of Alcoholics Anonymous (AA) and later byJellinek [17]. In all of these cases, the idea that alcohol-ism and other forms of addiction were diseases was anhypothesis invoked to explain the persistence of alcoholand other drug use in the absence of a causal mecha-nism. Since then, a range of sophisticated models havebeen developed to explain how the chronic use of ad-dictive drugs can undermine some individual’s ability tocontrol their drug use (e.g. the incentive salience, rewardlearning, impaired impulse inhibition or allostasismodels of addiction). It is not possible to review all ofthese here. All of these models, however, share thecommon view that control over drug use is somehowimpaired – they differ on the precise neurobiological,psychological or behavioural mechanism that explains
this impairment. We have provided a more detailed ex-planation of the various models of addiction elsewhere.
Addiction neuroscientists have recently proposed thataddiction be thought of as a brain disease. They haveargued that their research provides plausible neurochem-ical hypotheses that explain how the chronic use ofaddictive drugs can undermine an individual’s ability tocontrol their drug use [2, 18, 19]. Animal models ofaddiction have identified changes in brain reward mech-anisms produced by chronic drug administration. Humanneuroimaging studies suggest that the brains of addictedand non-addicted persons differ in how they respond toaddictive drugs and drug-related stimuli [6, 20].Addicted individuals specifically exhibit abnormalitiesin brain regions involved in motivation, reward andinhibitory control [21, 22] and decision-making [23,24]. These differences seem to be related to the amountof drugs used, correlate with self-reported drug cravings,and often persist long after abstinence has been achieved.Twin and adoption studies also suggest that there is asubstantial genetic contribution to addiction vulnerability[25–27], with shared genes accounting for between 40%and 60 % of addiction liability [28, 29].
This evidence has prompted directors of themajor USdrug research institutes, such as NIDA and the NationalInstitute on Alcohol Abuse and Alcoholism (NIAAA), tostrongly advocate for a brain disease model of addiction[1, 18]. According to this model, prolonged drug useproduces enduring changes in brain function that persistafter abstinence has been achieved and undermine at-tempts to regain control over drug use [4, 30].
Implications of these Models of Addiction for Controland Responsibility
The degree to which addicted individuals are seen ascontrolling their drug use has implications for the waysin which they are treated by friends, families and thecourts in the case of drug-related criminal behaviour[31]. Those who see drug use as wholly a voluntarychoice believe that drug users should be held legallyresponsible for their behaviour, including harmful effectson others [8, 9, 32]. By contrast, the conception ofaddiction as “a chronic relapsing brain disease” couldbe seen as absolving addicted persons of legal responsi-bility for their drug use and any criminal acts and soshould be offered addiction treatment rather than a prisonsentence [33]. Indeed, according to some high profileadvocates of the brain disease view of addiction, the
A. Carter et al.

autonomy of some addicted individuals is so impairedthat we have a moral obligation to forcibly treat theiraddiction [34–37].
Given these competing views of addicted persons’control over their behaviour, it is important to know towhat extend these views are endorsed by addictionneuroscientists and clinicians. To what extent do addic-tion neuroscientists and clinicians who treat addictedpersons accept the brain disease model of addiction?What views do they hold about addicted persons’ con-trol over and responsibility for their drug use and crim-inal acts? To answer these questions, we conductedqualitative interviews with leading Australian addictionclinicians and neuroscientists about their views on ad-diction, whether addicted persons’ have control overtheir drug use and whether they should be held respon-sible for their drug use and for criminal behaviourengaged in to fund their drug use.
Methods
Sample and Recruitment
We recruited 31Australian addiction neuroscientists andclinicians (10 females and 21 males) using expert nom-inations or snowballing, searches of publications, andquota sampling methods. A database of Australian ad-diction neuroscientists and clinicians (developed by theauthors) was used to identify 48 potential participants ofwhom 31 (65 %) agreed to be interviewed. The averageage of the sample was 45 years (ranging from 29 to 65).All participants were involved in neuroscience researchon addiction in Australia at the time of recruitment. Thesample was divided into those who had either current orpast clinical experience in treating addicted persons(clinicians, n=16) and those without such experience(primarily addiction neuroscientists only, n=15). Theneuroscientists (n=15) included a behaviour geneticist(n=1), psychopharmacologists (n=2), human patholo-gists (n=1), animal researchers (n=7), and cognitiveneuroscientists/psychologists (n=4). The 16 addictionclinicians included psychiatrists (n=3), clinical psychol-ogists (n=11) and physicians (n=2). The majority of theclinicians treated persons addicted to opioids, alcoholand psychostimulants (n=14). Only two particpants re-ported treating behavioural addictions, such as compul-sive overeating. Ethics approval was obtained from The
University of Queensland Behavioural & Social Sci-ences Ethical Review Committee.
Qualitative Interviews and Coding
Participants took part in a one-hour semi-structuredinterview during 2009 and 2010. All participants wereprovided with an information sheet describing thestudy and gave informed consent: 26 interviews wereconducted face-to-face and 5 were conducted via tele-phone. The interview comprised open-ended questionsexploring participants’ views on the aetiology andnature of addiction, addicted individuals’ ability tocontrol their drug use, addicted persons’ responsibilityfor their drug use and any criminal behaviour, and theimpact of neuroscience research on the clinical treat-ment of addiction and public health policies. Thispaper reports on a subset of these themes. An analysisof participant views on the clinical treatment and be-haviour of addicted individuals is reported elsewhere.
All interviews were transcribed verbatim and codedin QSR NVivo (Doncaster, Australia) version 10 usingdescriptive thematic analysis [38]. A detailed codingstructure was developed by three members of the re-search team to reflect the primary themes emergingfrom the interview data. Two members of the researchgroup coded data for three primary themes: i) under-standing of addiction; ii) addicted individuals controlover their drug use; and iii) responsibility for their druguse and its associated behaviour. Data coded withineach primary theme was then revised to establish sec-ondary themes (see Table 1). An iterative approach wasused during coding in which new data that challengedthe existing coding structure were used to develop thesecondary themes until no new themes emerged. Athird member of the research group reviewed codeddata to ensure accurate coding and resolved any dis-crepancies between the two initial coders.
The authors also made a global assessment of wheth-er on balance each participant believed that addictedindividuals have: (i) control over their drug use, and(ii) are responsible for their behaviour. Two authors(RM,AC) independently assessed participants’ predom-inant view of both control and responsibility. Partici-pants were coded as either ‘Yes’ (have control or areresponsible) or ‘No’ (have no control or are not respon-sible) if they made a clear preference for a particularviewpoint. Those that discussed both sides of the argu-ment for control and responsibility were coded as
Control and Responsibility in Addicted Individuals
‘ambivalent’. Discrepancies in classification betweenthe two coders (RM, AC) were resolved by discussionto reach a consensus.
Results
Understandings of Addiction
Participants were first asked how they would describe ordefine addiction. Addiction was most often defined assome form of “loss of control” over drug use; often thisloss of control was described as “compulsive” (n=14).
“I would think of addiction as characterised by thecompulsive use of a substance and the lack ofcontrol over intake.” (Animal Researcher 3, male)
“The core feature of addiction is compulsive,repetitive use of drugs in the face of known harm.
I think that’s the real nub of it. Compulsive,uncontrollable.” (Animal Researcher 5, male)
Around a third of respondents (n=12) believed thataddiction was a multifactorial condition that shared acombination of two or more psychological/mental, bio-logical (including both genetic and neurobiological) orsocial factors.
“In terms of aetiology, well it’s obviously going tobe multifactorial and different. I mean the factorsare probably the same, but the blend in eachindividual is going to be different.” (AddictionPsychiatrist 2, male)
Small minorities of individuals defined addictionsolely by: changes in brain function or as a “braindisease” (n=5); a behavioural disorder (n=4); or definedit in terms of the harm or negative impact that drug usehad on an individual’s life (n=6). One respondent arguedthat addiction was largely a social construction.
Control over Drug Use and Behaviour in Addiction
Although nearly half defined addiction as a “loss ofcontrol” or a “compulsion”, they differed markedly intheir views about whether addicted individuals hadcontrol over their drug use, or if so, to what degree.Only 5 participants believed that some addicted indi-viduals had no control over their drug use, for example:
“Do I believe they have control over it? Person-ally, no. I believe that whatever’s happening inthe brain is so strong that they know that theyshouldn’t but for some reason they still do.”(Animal Researcher 4, female)
None of these participants had any clinical experi-ence treating addicted individuals and 4 did researchon animal models of addiction. One argued that indi-viduals who could control their drug use were notaddicted by definition.
“I think that there are some people who can juststop taking drugs, but I would consider thosepeople as not necessarily addicted to the drug.They might be drug takers but they’re not in myview drug addicted individuals.” (Animal Re-searcher 2, male)
The overwhelming majority of participants (n=26)believed that addicted individuals retained some con-trol over drug use, although they differed greatly in
Table 1 Primary and secondary themes emerging from analysis
Primary themes Secondary themes
1. Understandingof addiction
Definition of addiction
Loss of control/Compulsion
Multifactorial
Harmful drug use
Changes in brain function/“braindisease”
Social construction
2. Control Control as a characteristic of addiction
Overall view on ability to control
Have no control
Have control
Impaired control
Factors that influence ability to controldrug use
Individual variability
Stages or severity of dependence
Environment and social drivers
3. Responsibility Overall ratings
Are responsible for behaviour
Are not responsible for behaviour
Ambivalent
Legal responsibility
Mitigating factor
Therapeutic responsibility
A. Carter et al.
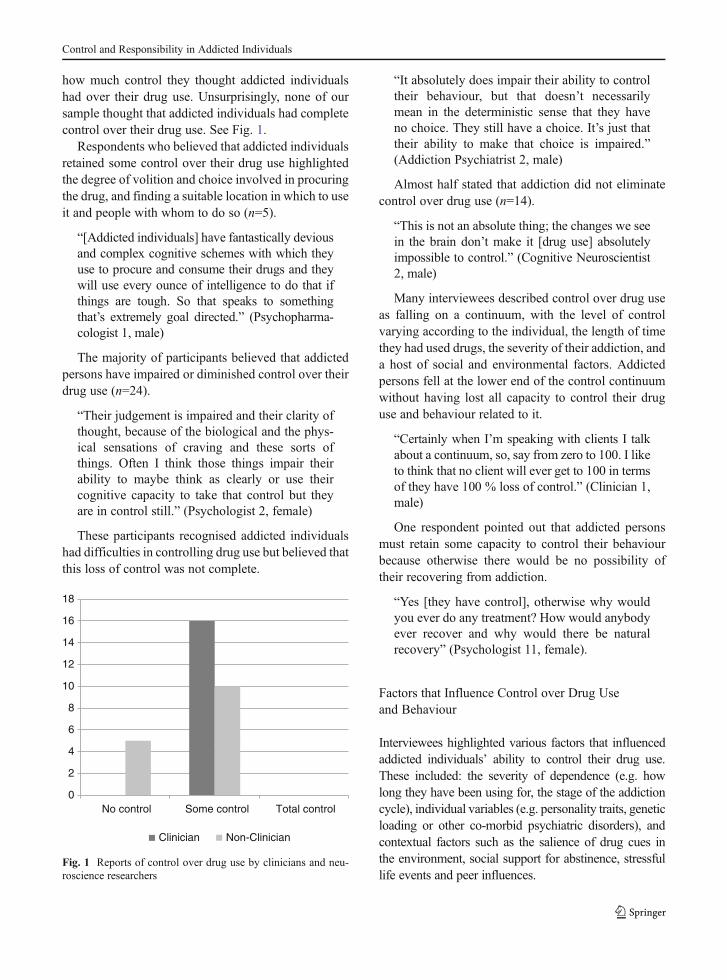
how much control they thought addicted individualshad over their drug use. Unsurprisingly, none of oursample thought that addicted individuals had completecontrol over their drug use. See Fig. 1.
Respondents who believed that addicted individualsretained some control over their drug use highlightedthe degree of volition and choice involved in procuringthe drug, and finding a suitable location in which to useit and people with whom to do so (n=5).
“[Addicted individuals] have fantastically deviousand complex cognitive schemes with which theyuse to procure and consume their drugs and theywill use every ounce of intelligence to do that ifthings are tough. So that speaks to somethingthat’s extremely goal directed.” (Psychopharma-cologist 1, male)
The majority of participants believed that addictedpersons have impaired or diminished control over theirdrug use (n=24).
“Their judgement is impaired and their clarity ofthought, because of the biological and the phys-ical sensations of craving and these sorts ofthings. Often I think those things impair theirability to maybe think as clearly or use theircognitive capacity to take that control but theyare in control still.” (Psychologist 2, female)
These participants recognised addicted individualshad difficulties in controlling drug use but believed thatthis loss of control was not complete.
“It absolutely does impair their ability to controltheir behaviour, but that doesn’t necessarilymean in the deterministic sense that they haveno choice. They still have a choice. It’s just thattheir ability to make that choice is impaired.”(Addiction Psychiatrist 2, male)
Almost half stated that addiction did not eliminatecontrol over drug use (n=14).
“This is not an absolute thing; the changes we seein the brain don’t make it [drug use] absolutelyimpossible to control.” (Cognitive Neuroscientist2, male)
Many interviewees described control over drug useas falling on a continuum, with the level of controlvarying according to the individual, the length of timethey had used drugs, the severity of their addiction, anda host of social and environmental factors. Addictedpersons fell at the lower end of the control continuumwithout having lost all capacity to control their druguse and behaviour related to it.
“Certainly when I’m speaking with clients I talkabout a continuum, so, say from zero to 100. I liketo think that no client will ever get to 100 in termsof they have 100 % loss of control.” (Clinician 1,male)
One respondent pointed out that addicted personsmust retain some capacity to control their behaviourbecause otherwise there would be no possibility oftheir recovering from addiction.
“Yes [they have control], otherwise why wouldyou ever do any treatment? How would anybodyever recover and why would there be naturalrecovery” (Psychologist 11, female).
Factors that Influence Control over Drug Useand Behaviour
Interviewees highlighted various factors that influencedaddicted individuals’ ability to control their drug use.These included: the severity of dependence (e.g. howlong they have been using for, the stage of the addictioncycle), individual variables (e.g. personality traits, geneticloading or other co-morbid psychiatric disorders), andcontextual factors such as the salience of drug cues inthe environment, social support for abstinence, stressfullife events and peer influences.
0
2
4
6
8
10
12
14
16
18
No control Some control Total control
Clinician Non-Clinician
Fig. 1 Reports of control over drug use by clinicians and neu-roscience researchers
Control and Responsibility in Addicted Individuals

Deficits in the capacity to exercise control were seenas increasing with the severity of addiction or the stageof addictive drug use.
“I think in the initial phases of use, probably notunder the acute intoxication phase, but if you’reexperimenting probably not much. I think as yougo down the track it becomes more and moredifficult to exercise control.” (Cognitive Neurosci-entist 1, male)
Participants believed that individuals who haveused drugs for longer periods of time develop neuro-logical changes that impair control over drug use.
“It depends on their length of substance abuse, interms of the way it affects the pre-frontal cortexand their ability to control their urges… I thinkthe longer a person is using then the less controlthat they will have.” (Clinician 1, male)
The majority of interviewees emphasized that con-trol over drug use fluctuated over time. They suggestedthat addicted individuals have much less control overtheir drug use during relapse or periods of binge drink-ing and drug use, and more control at other times.
“So it’s very dynamic. It changes minute to min-ute, you know, depending on the situation they’rein; how intoxicated or in withdrawal they are andwhat else is going on. So I don’t think it’s a staticquantity.” (Addiction Psychiatrist 2, male)
The dynamic nature of control over drug use wasalso believed to vary between individuals. Genetic orhereditary variables were highlighted by a number ofrespondents, while personality or behavioural styles(e.g. impulsivity or poor self-control) were believedto account for differences in the level of harm experi-enced by some drug users and difficulty experienced inabstaining from drug use.
“Some people cannot control it, some can. Her-oin is an interesting one because we come acrossheroin users [with] 30, 40 years’ of abuse, andthey’re able to control their use. They will tellyou, “If I can afford it, I’ll do heroin, if not, thenI’ll go to methadone” and they oscillate and theyfunction, they get a job and they are okay. Andyou can get ones that are completely a mess, theyjust sit on the street corner and they rob and stealand do whatever they can to get the habit.” (Be-haviour Geneticist 1, female)
The age of onset was also seen to be an importantfactor in an addicted individual’s prognosis, whileothers believed that the capacity for control was de-pendent on the substance used. Social environmentalfactors were believed to have a significant influence oncontrol over drug use (n=8).
“I think there are situational factors that increaseyour capacity for control and I think that for a lotof individuals it’s about making those situationalfactors different enough so that they can manageto not use.” (Psychologist 11, female)
Others thought that stressful life events and socialcues could undermine control.
“But what we know is that they have a dimin-ished level of control, that as you increase levelsof reward, that control gets worse. That if youstress them or you create an adverse event andthen provide a reward, that their control is reallypoor.” (Addiction Psychiatrist 1, male)
Responsibility for Drug Use
All participants believed that addicted individualsshould be held responsible, at least to some degree, fortheir drug use and drug-related crimes. Nobody weinterviewed believed that addiction absolved an affectedindividual from taking responsibility for their behaviour.
“Ultimately someone is engaging in a behaviourto seek a substance, to take a drug. The respon-sibility for that behaviour is not obviated by thefact, or reduced by the fact, that they’re a druguser.” (Animal Researcher 3, male)
“I don’t think having an addiction means that youshould not be held responsible for your actions.”(Psychologist 4, female)
The majority (n=23) believed that addiction did notreduce addicted individual’s responsibility for theiractions; 6 believed that addiction diminished but didnot abolish responsibility (ambivalent). These viewswere equally common among clinicians and non-clinicians. Two participants who did not answer thisquestion were excluded from the analysis. See Fig. 2.
A number of reasons were given for believing thatindividuals remain responsible for their drug use and itsconsequences. “Responsibility”was most often employedin a legal sense: that is, in terms of whether addicted
A. Carter et al.

individuals were able to understand and make autono-mous choices about their drug use, and were thereforeblameworthy for their actions. For some, addicted per-sons were responsible for their drug use in the same waythat any person was responsible for any other behaviourover which they had some agency and a capacity tochange.
“We are all responsible in our society, for our-selves, and our behaviour. Full stop.” (AddictionSpecialist 2, male)
Some believed that addicted persons were responsi-ble for their behaviour because their loss of control overtheir drug use and related behaviour was incomplete.
“I still think that there’s a high level of responsi-bility because even though of all of the differentfactors that claim to a person being addicted andchoosing to use drugs—see I even use the term‘choosing to’. I just don’t believe that it’s soautomatic, you know; that there’s not some ele-ment of free choice there, and I can understandthat it’s a struggle and it’s really, really difficultbut I don’t really accept that there’s nothing theycan do that—you know, they’re compelled to doit without having any control.” (Neuropsycholo-gist 1, female)
Others believed that while addiction interfered withdecision-making, they were responsible for the initialchoice to use drugs. Addicted individuals were there-fore responsible for any subsequent consequences of
these choices (e.g. activities in which they engaged inwhile intoxicated).
“Look, you don’t become addicted if you don’tuse very much; you have to use a fair bit tobecome addicted over a prolonged period of time.And yes, the person was responsible for that…youbear some responsibility for getting yourself in thesituation.” (Psychopharmacologist 2, male)
While participants generally believed that addictedpersons were responsible for their actions many none-theless believed that their drug use should be taken intoaccount when assessing their behaviour. “It is a reason,but it’s not an out.” (Psychologist 5, male).
“If I stole your video because I needed money fordrugs, versus I stole your video because I kind ofliked it, I think most people would be slightlymore sympathetic to the guy who was a drugaddict who stole it, because at least he wasn’tjust trying to enrich himself. He had a problem,and he was responding to that problem with anantisocial and unpleasant behaviour, but at least itwas not entirely just greed. So sometimes I thinkwe would accept some degree of diminishedresponsibility. So if he accepts that he stole yourvideo because of his drug problem and he’s will-ing to engage in treatment, or do something torectify that situation, we would accept that situa-tion. But he retains responsibility for stealing thevideo.” (Addiction Psychiatrist 3, male)
Participants also used “responsibility” in a therapeuticsense. That is, they saw addicted individuals as beingresponsible for making attempts to overcome their addic-tion and abstain from drug use in the future. Theserespondents highlighted the responsibility of addictedindividuals for future choices; the fact that it was up toaddicted individuals to make positive therapeutic choices.
“You’ve got to be able to say at some point, it isup to me to do something different, so ultimatelyyou’ve got to be able to take responsibility forthat. You’ve got to be able to say it’s somethingwithin me.” (Psychologist 11, female)
Discussion
Consistent with our earlier analyses of these data, very fewof the Australian addiction neuroscientists and clinicians
0
2
4
6
8
10
12
14
Not responsible Ambivalent Yes Responsible
Clinician Non-Clinician
Fig. 2 Reports of responsibility by clinician and neuroscienceresearchers
Control and Responsibility in Addicted Individuals

we interviewed defined addiction as a brain disease. Ad-diction was largely defined by behavioural changes indrug use, most notably a “loss of control” over or “com-pulsive” patterns of drug use. Despite most intervieweesseeing impaired control over drug use as characteristic ofaddiction, only a very small minority believed that addic-tion entailed a complete loss of control over drug use;none of the participants who believed this had any clinicalexperience with addicted individuals.
Research is needed to determine whether theseviews are shared by researchers and clinicians in otherWestern countries, such as the US, where there hasbeen greater emphasis placed on the brain diseasemodel of addiction by the leading funding agencies.It is not clear from our research whether the apparentambivalent or cautious attitude toward brain diseasemodels among Australian clinicians and scientists isunique to Australia, or reflects a more prevalent atti-tude amongst addiction clinicians and scientists. Theneuroscientists interviewed in this study were activelyengaged in neuroscience research and had published inthe area. It is unlikely that the ambivalent attitudesidentified in this and previous studies were due toignorance of neuroscience research on addiction. Itmight seem reasonable to assume that there is morewidespread support for the brain disease model in theUS, given that this model is heavily promoted by theUS agency that funds research on addiction. But it isalso possible that the brain disease model reflects theviews of NIDA spokespersons rather than the views ofall who work within the addictions field in the USA.
All of the clinicians we interviewed believed thataddicted individuals maintained some control over theirdrug use, even if their control was impaired. The clini-cians we interviewed were actively engaged in neuro-science research on addiction, and were knowledgeableabout the findings of neuroscience research and posi-tively disposed towards neurobiological explanations ofaddiction. This finding raises doubts about the claims ofsome commentators, such as Louis Charland [39] andPeter Cohen [40], that addiction neuroscientists believethat addiction entails a “loss of control” over drug use,because drug use “hijacks” the brain [e.g. 1, 4, 17]. Ourresearch suggests that statements about loss of control inaddiction made by addiction neuroscientists and clini-cians should not be interpreted in this strong sense. Italso suggests that our participants did not accept the strongform of the brain disease model of addiction that is advo-cated by NIDA [2, 18, 19]. The overwhelmingmajority, in
fact, believed that addicted individuals retained somelegally-relevant control over their drug use (see below).
While control over drug use was universally under-stood to be impaired, the level of impairment was seento vary with a range of factors that included: length andseverity of drug use, stage of addiction cycle, individualvariation due to genetic, psychological or inherited fac-tors, or early life experiences, and social contexts, par-ticularly stressful environments. The factors that under-mine decisions not to use drugs highlighted by partici-pants represent areas that are often targeted for thera-peutic intervention in treating someone with more re-fractory forms of addiction.
All participants believed that addicted individualswere both legally responsible for their drug-relatedbehaviour and therapeutically responsible for address-ing their addiction. Even the minority of participantswho believed that addicted individuals had no controlover their drug use believed that addicted individualsshould be held accountable for any criminal or harmfulacts that they had committed.
While addiction was not seen to abolish responsibil-ity, most participants believed that addiction mitigatedmoral responsibility for addiction-related behaviour.Such a view is consistent with the approach taken byAustralian drug courts which hold addicted individualsresponsible for addiction-related crimes, such as theft tofund a drug habit, but take addiction into account as amitigating factor at sentencing [31]. Participants alsoemphasised the necessity for addicted persons to taketherapeutic responsibility for overcoming their addictionby seeking treatment and abstaining from drug use in thefuture.
Limitations
This was an exploratory qualitative interview studywith a small sample of Australian addiction neurosci-entists and clinicians. It is not clear whether theseresults would apply to addiction clinicians and scien-tists in other countries.
Conclusion
Addiction neuroscientists and clinicians see loss ofcontrol over drug use as a defining characteristic ofaddiction, but nonetheless do not believe that addictedindividuals have no control over their drug use and
A. Carter et al.
associated behaviour. Most believed that addicted in-dividuals were ultimately responsible for their behav-iour but were prepared to recognise addiction as amitigating factor when setting penalties for criminaloffences committed by addicted offenders.
Acknowledgments This workwas supported byNational Healthand Medical Research Council fellowships awarded to Wayne Halland Adrian Carter [grant numbers 569738 and 628935].
Conflicts Interests The Authors declare that there is no conflictof interest.
References
1. Volkow, N.D., and T.K. Li. 2004. Drug addiction: the neu-robiology of behaviour gone awry. Nature Reviews Neuro-science 5: 963–970.
2. Baler, R.D., and N.D. Volkow. 2006. Drug addiction: theneurobiology of disrupted self-control. Trends in MolecularMedicine 12: 559–566.
3. American Psychiatric Association. 2000. Diagnostic andstatistical manual of mental disorders—Text revision(DSM-IV-TR). Washington, DC: American PsychiatricAssociation.
4. Dackis, C., and C. O’Brien. 2005. Neurobiology of addic-tion: treatment and public policy ramifications. Nature Neu-roscience 8: 1431–1436.
5. Volkow, N.D., and T.K. Li. 2005. The neuroscience of ad-diction. Nature Neuroscience 8: 1429–1430.
6. Carter, A., and W. Hall. 2012. Addiction neuroethics: thepromises and perils of neuroscience research on addiction.London: Cambridge University Press.
7. Davies, J.B. 1997. The myth of addiction, 2nd ed. Amster-dam: Harwood Academic.
8. Dalrymple, T. 2006. Romancing opiates: Pharmacologicallies and the addiction bureaucracy. New York: EncounterBooks.
9. Szasz, T.S. 1975. Ceremonial chemistry: The ritual perse-cution of drugs, addicts, and pushers. London: Routledge.
10. Foddy, B., and J. Savulescu. 2006. Addiction and autonomy:can addicted people consent to the prescription of their drugof addiction? Bioethics 20: 1–15.
11. Heyman, G. 2001. Is addiction a chronic, relapsing disease?In Drug addiction and drug policy the struggle to controldependence, eds. Heymann P and Brownsberger W, 81–117.Cambridge, Mass: Harvard University Press.
12. Heyman, G. 2009. Addiction: A disorder of choice. Cam-bridge: Harvard University Press.
13. Peele, S. 2004. The surprising truth about addiction. Psy-chology Today 37: 43.
14. Higgins, S.T., and N.M. Petry. 1999. Contingencymanagement—Incentives for sobriety. Alcohol Research &Health 23: 122–127.
15. Higgins, S.T. 2006. Extending contingency management tothe treatment of methamphetamine use disorders. AmericanJournal of Psychiatry 163: 1870–1872.
16. Room, R. 2007. Social policy and psychoactive substances.In Drugs and the future: Brain science, addiction and soci-ety, ed. D. Nutt, T. Robbins, G. Stimson, M. Ince, and A.Jackson, 337–358. London: Academic.
17. Jellinek, E.M. 1960. The disease concept of alcoholism.New Brunswick: Hillhouse Press.
18. Leshner, A.I. 1997. Addiction is a brain disease, and itmatters. Science 278: 45–47.
19. Volkow, N.D., and T.-K. Li. 2005. Drugs and alcohol:treating and preventing abuse, addiction and their med-ical consequences. Pharmacology & Therapeutics 108:3–17.
20. Garavan, H., A. Lingford-Hughes, T. Jones, P. Morris, J.Rothwell, and S. Williams. 2007. Neuroimaging. In Drugsand the future: Brain science, addiction and society, ed. D.Nutt, T. Robbins, G. Stimson, M. Ince, and A. Jackson, 285–314. London: Academic.
21. Ersche, K.D., P.S. Jones, G.B. Williams, A.J. Turton, T.W.Robbins, and E.T. Bullmore. 2012. Abnormal brain structureimplicated in stimulant drug addiction. Science 335: 601–604.
22. Volkow, N.D., J.S. Fowler, and G.J. Wang. 2003. Theaddicted human brain: insights from imaging studies. Jour-nal of Clinical Investigation 111: 1444–1451.
23. Bechara, A. 2005. Decision making, impulse control andloss of willpower to resist drugs: a neurocognitive perspec-tive. Nature Neuroscience 8: 1458–1463.
24. Jentsch, J.D., and J.R. Taylor. 1999. Impulsivity resultingfrom frontostriatal dysfunction in drug abuse: implicationsfor the control of behavior by reward-related stimuli. Psy-chopharmacology 146: 373–390.
25. True, W.R., H. Xian, J.F. Scherrer, P.A.F. Madden, K.K.Bucholz, A.C. Heath, S.A. Eisen, M.J. Lyons, J. Goldberg,and M. Tsuang. 1999. Common genetic vulnerability fornicotine and alcohol dependence in men. Archives of Gen-eral Psychiatry 56: 655–661.
26. Ball, D. 2008. Addiction science and its genetics. Addiction103: 360–367.
27. Goldman, D., G. Oroszi, and F. Ducci. 2005. The genetics ofaddictions: uncovering the genes. Nature Reviews Genetics6: 521–532.
28. Uhl, G.R., T. Drgon, C. Johnson, C.-Y. Li, C. Contoreggi, J.Hess, D. Naiman, and Q.-R. Liu. 2008. Molecular geneticsof addiction and related heritable phenotypes. Annals of theNew York Academy of Sciences 1141: 318–381.
29. Uhl, G.R., M.D. Li, J. Gelertner, W. Berrettini, and J. Pol-lock. 2004. Molecular genetics of addiction vulnerabilityand treatment responses. Neuropsychopharmacology 29:S26–S26.
30. McLellan, A.T., D.C. Lewis, C.P. O’Brien, and H.D. Kleber.2000. Drug dependence, a chronic medical illness: implicationsfor treatment, insurance, and outcomes evaluation. JAMA 284:1689–1695.
31. Hall, W., and A. Carter. 2012. How may neuroscience affectthe way that the criminal courts deal with addicted of-fenders? In Neuroscience and responsibility, ed. N. Vincent,279–298. London: Oxford University Press.
32. Satel, S. 1999. The fallacies of no-fault addiction. PublicInterest 99: 52–67.
Control and Responsibility in Addicted Individuals

33. Chandler, R.K., B.W. Fletcher, and N.D. Volkow. 2009.Treating drug abuse and addiction in the criminal jus-tice system: improving public health and safety. JAMA301: 183–190.
34. Caplan, A. 2008. Denying autonomy in order to create it: theparadox of forcing treatment upon addicts. Addiction 103:1919–1921.
35. Sullivan, M.A., F. Birkmayer, B.K. Boyarsky, R.J. Frances,J.A. Fromson, M. Galanter, F.R. Levin, C. Lewis, E.P. Nace,R.T. Suchinsky, J.S. Tamerin, B. Tolliver, and J. Westermeyer.2008. Uses of coercion in addiction treatment: clinical aspects.American Journal on Addictions 17: 36–47.
36. Marlowe, D.B. 2006. Depot naltrexone in lieu of incar-ceration: a behavioral analysis of coerced treatment for
addicted offenders. Journal of Substance Abuse Treatment31: 131–139.
37. Bell, S., A. Carter, R. Mathews, C. Gartner, J. Lucke, and W.Hall. 2013. Views of addiction neuroscientists and clinicianson the clinical impact of a brain disease model of addiction.Neuroethics 1–9.
38. Rhodes, T., and R. Coomber. 2010. Qualitative methods andtheory in addictions research. Addiction research methods,59–78. Oxford: Wiley Blackwell.
39. Charland, L.C. 2002. Cynthia’s dilemma: consenting to her-oin prescription. American Journal of Bioethics 2: 37–47.
40. Cohen, P.J. 2002. Untreated addiction imposes an ethical barto recruiting addicts for non-therapeutic studies of addictivedrugs. Journal of Law Medicine & Ethics 30: 73–81.
A. Carter et al.