contrast induce nephropathy
TRANSCRIPT
Contrast Induce Nephropathy
Collage Of Medicine – Al-Qadisiya University Iraq
Done By :- Ziyad Salih
Index :
• Introduction
• Definition
• Epidemiology
• Pathophysiology
• Risk markers
• Risk score
• Contrast agents
• Management
INTRODUCTION
• CIN (CI -AKI ) it’s a leading cause of acute
kidney injury in hospitalized patients.
• Most frequent renal complication of
endovascular interventional procedures.
• Increases short and long term morbidity and
mortality.
• Treatment is limited to supportive measures
while awaiting the resolution of renal
impairement
QUESTIONS IN MIND
• How CIN occurs ?
• What is the definition of CIN ?
• Are contrast agents directly nephrotoxic ?
• How can it be prevented ?
• Will CIN be never having an effective
treatment ?
Historical view about contrast
• In 1906,Von Lichtenberg and Voelcker used
2% colloidal silver solution,for retrograde
pyelography studies.(toxic to kidneys,death).
• In 1920, Osborne and colleagues ,10% “NaI”
for Rx of syphilis, fortuiously found it to be
radiopaque ,excreted by kidneys.--first
pyelogram.
• 1924,Brooks – first angiogram (under GA).
Definition
• CI-AKI is defined by the Kidney Disease
Global Outcomes (KDIGO) guidelines as an :-
“…increase in serum creatinine of 0.5 mg/dL or
greater within 48 hours of contrast use or a
25% or greater increase from baseline serum
creatinine within 7 days”.
The serum creatinine usually increases within 24 -48hrs after contrast administration, peaks at 3 to 5 days,and returns to baseline in 1 -3 weeks.
Epidemiology
• According to the US FDA, the incidence of renal failure after contrast administration ,ranged from 0.6%to2.3%.
• However, rates of CIN maybe as high as 50%, depending on the presence of well characterized risk factors, the most important of which are baseline chronic renal insufficiency and DM.
Risk Factors
•Systolic blood pressure <80 mm Hg - 5 points•Intraarterial balloon pump– 5 points•Congestive heart failure (history of pulmonary edema .– 5 points
•Age >75 y - 4 points •Hematocrit level <39% for men and <35% for women -3 points•Diabetes - 3 points•Contrast media volume - 1 point for each 100 mL•Renal insufficiency - 4 points
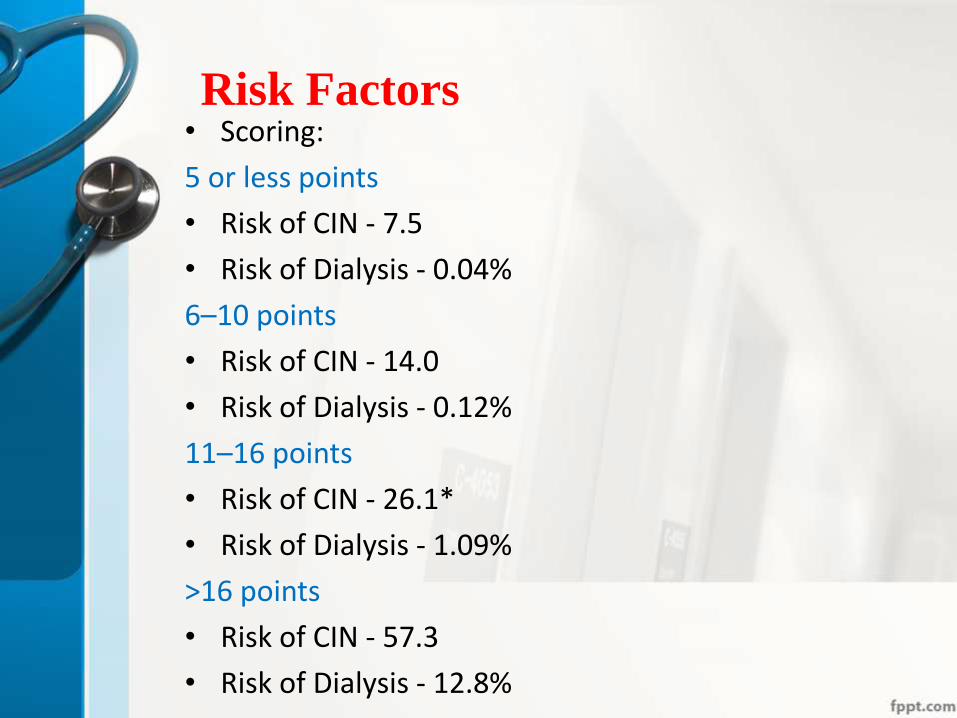
Risk Factors • Scoring:
5 or less points
• Risk of CIN - 7.5
• Risk of Dialysis - 0.04%
6–10 points
• Risk of CIN - 14.0
• Risk of Dialysis - 0.12%
11–16 points
• Risk of CIN - 26.1*
• Risk of Dialysis - 1.09%
>16 points
• Risk of CIN - 57.3
• Risk of Dialysis - 12.8%

Risk Factors
Or the CIN can be classified on the basis of GFR
• Low Risk: GFR> 60 ml/min
• Moderate Risk: GFR 30-59 ml/min
• High Risk: GFR < 30ml/min
Pathophysiology
• Not well understood until now , but there's theoretical explanation :-
1- tubular toxicity
2- microvascular alteration
3- oxidative stress
4- inflammation
5- protein precipitation
6- Regional Hypoxia
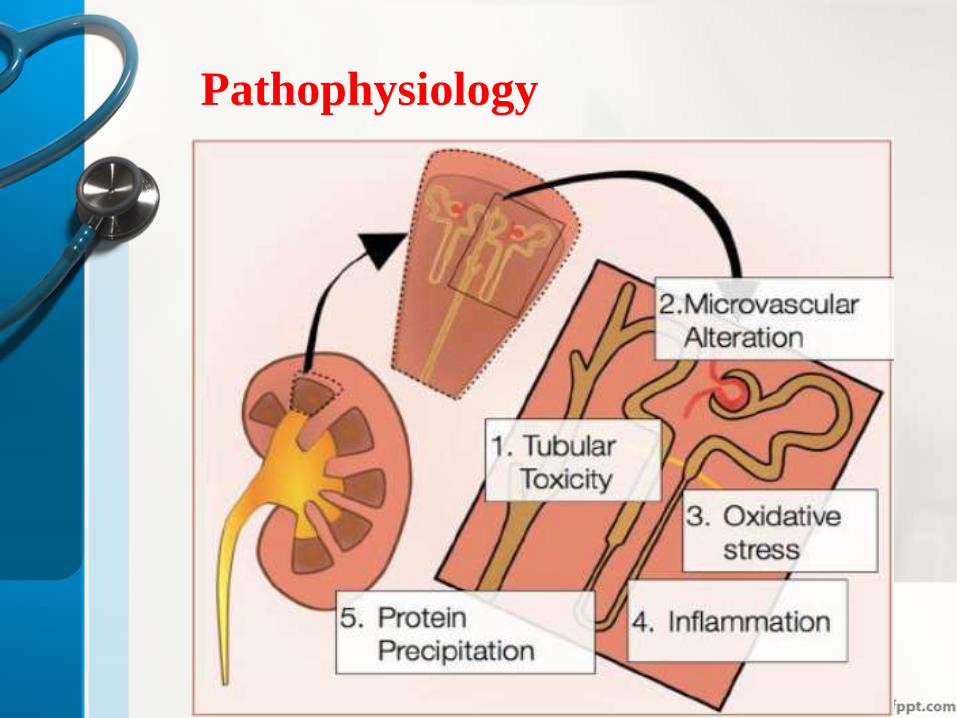
Pathophysiology

Important considerations in choosing a
contrast agent
• Its an important factor is to choose the appropriate contrast media depending on its harmful or beneficial effect
Types Of Contrast Media
A decreased incidence of contrast nephropathy appears to be associated with nonionic agents ,which, are either low osmolal or iso-osmolal
• SOLUBILITY Classified into ionic and nonionicgroups based on water solubility.
• OSMOLALITY ( High – Iso – Low )
• VISCOSITY ( High – Low )
How could hyperosmolality
cause nephropathy ?

How could hyperosmolality
cause nephropathy ?
Types Of Contrast Media
• So, recommended to use of either Isosmolaror Low Osmolar iodinated contrast media, rather than High Osmolar iodinated contrast media in patients at increased risk of CI-AKI.

Why we use Iso-Osmolar ?
• ISOSMOLAR Iodinated contrast media is recommended for the following groups of patients:
• –All high risk patients (eGFR<30 mL/min)
• –Dialysis patients
• –Moderate Risk (eGFR<60 mL/min) patients for intra-arterial procedures
Is there any role for drugs in CIN ?
• The use of some drugs that had been found to increase the posibility of Contrast induced nephropthy , through , their mechanism of action ..
The following drugs should be discontinued 24 hours before until 48 hours after contrast media administration
–NSAIDs
–Aminoglycosides
–Metformin
–Anti-virals(Acyclovir and Foscarnet)
–Amphotericin B
–High dose diuretics
–ACE-inhibitors
–ARBs

Clinical Manifestaion
• Contrast-induced nephropathy most commonly manifests as a nonoliguric and asymptomatic transient decline in renal function.
• The serum creatinine level begins to rise within 24 hr of contrast administration, usually peaks within 3–5 days, and returns to baseline within 10–14 day
Clinical Manifestaion
• Oliguric acute renal failure requiring hemodialysis can also occur. This condition presents with oliguria (24-hr urine volume < 400 mL) within 24 hr of contrast administration and typically persists for 2–5 days.
• Morbidity and mortality rates are significantly higher in this group of patients when compared with those who have nonoliguric renal failure
Investigations
o Urinary epithelial cell casts,
o debris,
o urate and calcium oxalate crystals
are nonspecific findings in contrast-induced nephropathy.
o Low urinary sodium and fractional excretion of sodium (< 1%) have been reported as being distinctive characteristics of this condition.

Diagnostic criteria for CIN
Diagnostic criteria for CIN
Exposure to contrast
Increase Sr.Creatinin
Prevention ….
o Hydration ... Hydraion ... And Hyrdraion
Hydration
o correct any decreases in renal blood flow by ensuring that intravascular volume is replete.
Hydration
• Simplest and most effective way of protecting
renal function.(decreases by 50% chance of
CI-AKI)
• Effect of contrast agents on kidney is
prolonged in dehydration.(RBF,GFR) … so
the hydration is very important .
Hydration
• How can I do a good hydration ?
• In which mean ?
• By any type of fluid ?
Hydration
ORAL: Low risk patients should be instructed to take 1-2 liters of water 12 hours before the procedure. Patients should be placed on NPO 4 hours before the procedure and IV fluids may be started if additional hydration is needed
Hydration
• While in High Risk patients …
IV Hydration : ≥ 1.0–1.5 ml/kg/h of NSS has to be administered for 3–12 hours before, and up to 6–12 hours after contrast media exposure.
• –Example: For a 60 kg patient, 60 –90 cc/hour for 3-12 hours prior to the procedure and up to 6-12 hours after the procedure.
Hydration
• In patients with poor systolic function OrChronic Renal failure use lower dose ( 0.5 ml/kg/hr )
Hydration
• Which type of I.V Fluids ?

Hydration
• Isotonic saline is superior to other types of fluids , since isotonic saline is a more effective volume expander.

NaHCo3
• Since alkalinization may protect against free radical injury, the possibility that sodium bicarbonate may be so important
• 3 ml/kg bolus (MAX 300 ml) 1 hour prior to procedure and 1 mL/kg/hour (MAX 100 ml/hr) during and for 6 hours post-procedure.
• Prepare = 150 meq of sodium bicarbonate in 850 ml of Dextrose

N-acetylcysteine
• There are great heterogeneity and conflicting results in the available clinical trials and study-analyses examining the effectiveness of acetylcysteine in the prevention of contrast nephropathy
• Being a precursor for glutathione synthesis, NAC has the potential to diminish oxidative stress by directly scavenging superoxide radicals and increasing intracellular glutathione.
N-acetylcysteine
Acetylcysteine Dosing :-
• Tolerating PO intake?
600-1200 mg capsules PO Q12h.
4 doses :-
2 doses pre-contrast and
2 doses post-contrast is optimal
• Emergent Procedure?
1 dose before and 3 doses post procedure is acceptable (Q12h x 4 doses total)
N-acetylcysteine
Acetylcysteine Dosing :-
For a high risk patient undergoing cardiac catheterization or PE protocol CT scan with no PO access
• IV Acetylcysteine?
600-1200 mg IV x 1 over 15 minutes, then 600-1200 mg PO q12h x 4 doses post-procedure .

Statins
• Statins may improve endothelial function,
• Reduce arterial stiffness, and reduce inflammation and oxidative stress.
• There are no sufficient data to support the use of statins for the prevention of contrast nephropathy.
Statins
Statins
• 2998 patients with type2 diabetes and CKD were assigned to receive rosuvastatin or to a control group prior to adiagnosticangiogram with or without percutaneous intervention.
• Patients assigned to rosuvastatin received 10 mg daily two days prior and three days after the scheduled procedure.
Contrast-induced was less common among patients assigned to rosuvastat incomparedwith control.
theophylline
• In a randomized study, prophylactic intravenous administration of theophylline 200mg reduced the incidence of CIN in 100 patients at risk ,as compared with placebo .
Calcium Channel Blocker
• In a small, randomized, placebo controlled study of 35 patients, eGFR was preserved in patients treated with nitrendipine but decreased in patients that received placebo.
Hemodialysis
• Iodinated contrast agents
are readily dialyzable.
• The plasma clearance of most modern contrast media is 50–70mL/min ,with more than 80% removed from the plasma within 4–5 hours of hemodialysis.
• Subsequent removal of CM is unlikely to stop the cascade of renal injury ,which would have already begun.
