considerations for evzio® (naloxone) and suboxone...
TRANSCRIPT
Considerations for Evzio® (naloxone) and Suboxone® (buprenorphine and
naloxone) Use
Laura Broder, MD
Dr. Broder indicated no potential conflict of interest to this presentation. She does not intend to discuss any
unapproved/investigative use of a commercial product/device.
Objectives
• Naloxone: how to prescribe it and who needs it
• Buprenorphine: pharmacology, side effects, and contraindications
• Special considerations for buprenorphine use
• Office-based opioid treatment
Naloxone
Steve’s Law
• Named after Steve Rummler, who died of an overdose in Minnesota in 2011
• Provides immunity to those who call 911
• Allows law enforcement and the public to access and administer naloxone
• Providers can prescribe to third parties if they may witness an overdose
• prescribetoprevent.org
Naloxone Prescribing
• Naloxone is an opioid antagonist used to treat opioid overdoses
• Should be prescribed to anyone at risk for an overdose• History of overdose• Any suspicion of non-medical use• On methadone or buprenorphine (Suboxone®)• Taking the equivalent of 50 mg of morphine or more per day• Age >65, Smoking, COPD, emphysema, asthma, sleep apnea, respiratory
infection, or other respiratory illness or potential obstruction, renal dysfunction, hepatic disease, cardiac illness, HIV/AIDS
• Known or suspected concurrent alcohol use• Concurrent benzodiazepine or other sedative prescription• Known recent suicidal ideation
Naloxone Prescribing
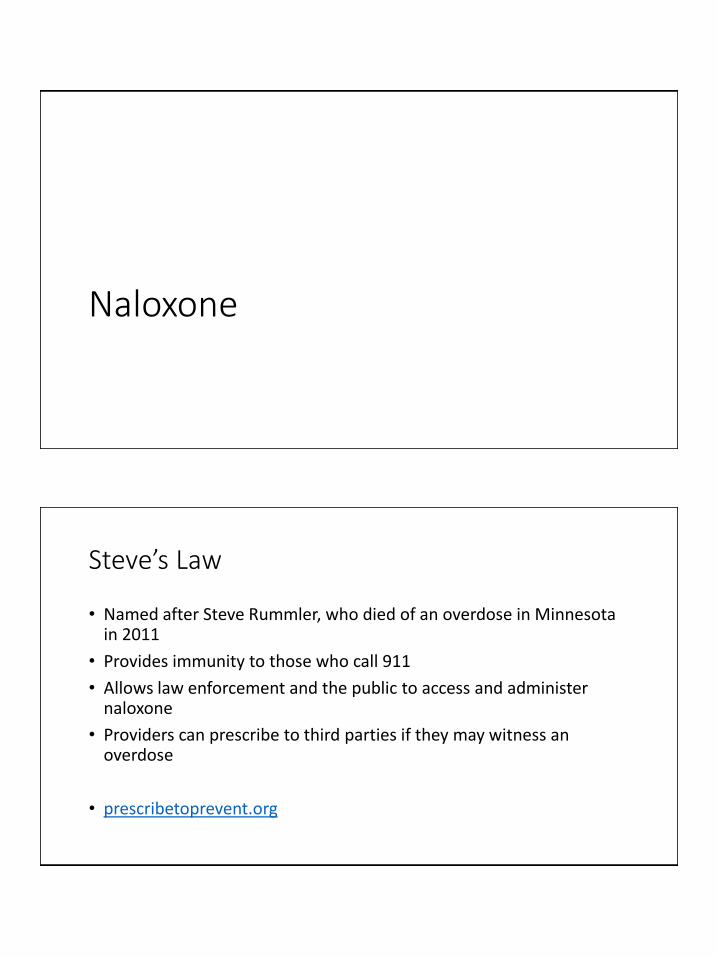
• Narcan® Nasal Spray• Very easy
• Relatively inexpensive • ($75 for 2)
• 4mg/0.1mL
• 2 per package
• Spray 0.1mL into one nostril
• May repeat with second device in 2-3 minutes if little or no response
Naloxone Prescribing
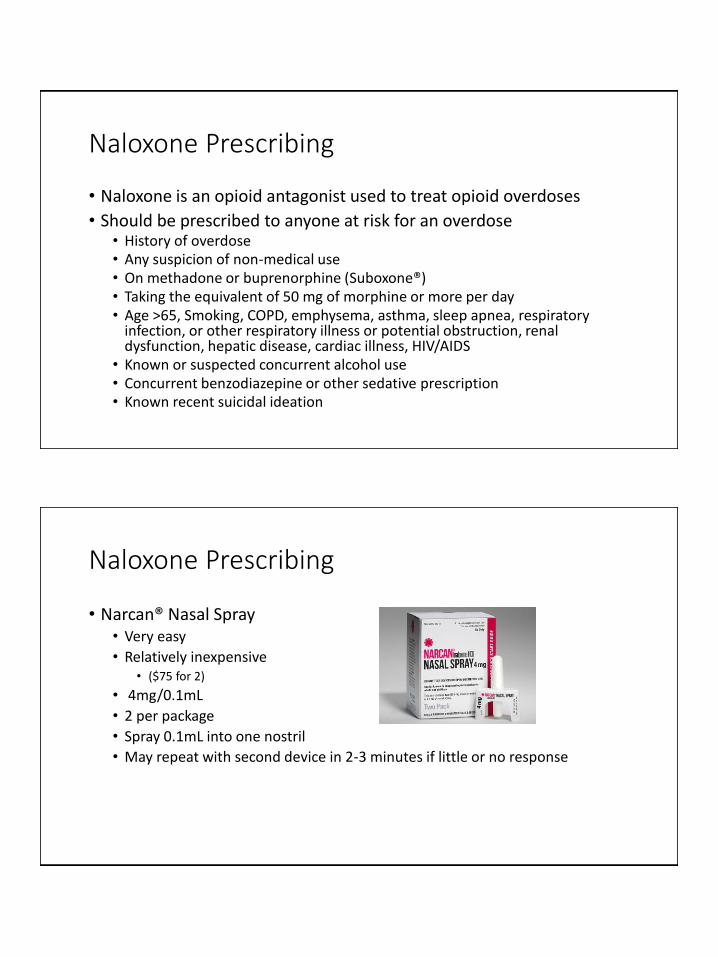
• Evzio® Auto-Injector• Very Easy
• 0.4mg/4mL
• 2 per box (and trainer)
• Very expensive• $3-4,000
• Button speaks directly to you
• Inject into outer thigh as directed by English voice-prompt system. Place black side firmly on outer thigh and depress and hold for 5 seconds. Repeat with second device in 2-3 minutes if no or minimal response
Naloxone Prescribing
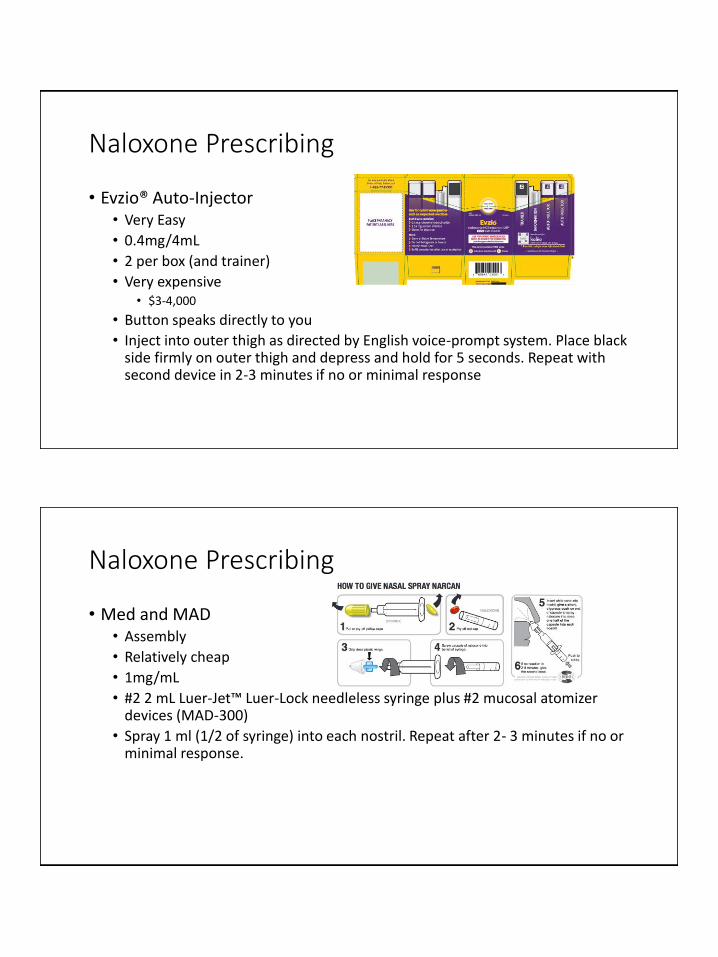
• Med and MAD• Assembly
• Relatively cheap
• 1mg/mL
• #2 2 mL Luer-Jet™ Luer-Lock needleless syringe plus #2 mucosal atomizer devices (MAD-300)
• Spray 1 ml (1/2 of syringe) into each nostril. Repeat after 2- 3 minutes if no or minimal response.
Naloxone Prescribing
• Med and Needle• Assembly
• Very cheap
• 0.4mg/mL
• #2 single-use 1 ml vials PLUS #2 3 mL syringe w/ 23-25 gauge 1-1.5 inch IM needles
• Inject 1 mL in shoulder or thigh. Repeat after 2-3 minutes if no or minimal response
Suboxone® (Buprenorphine and Naloxone)
Intro to Buprenorphine
• Buprenorphine is a partial opioid agonist used in treatment of opioid use disorder and chronic pain
• Suboxone® is a combination of buprenorphine and naloxone• Zubsolv® sublingual tablet
• Suboxone® sublingual film
• Bunavail™ buccal film
• Generics
• Naloxone is ineffective when used sublingually or orally but has excellent bio-availability when injected, blocking the high and potentially precipitating withdrawal from full opioid agonists
Intro to Buprenorphine
• Slow onset, long-acting μ opioid partial agonist• Relieves withdrawal from other opioids• Controls cravings
• Effects increase only to a certain point with increased dose, and level off at moderate doses (less abuse)
• Ceiling effect on respiratory depression
• Mildly reinforcing (improves treatment adherence)
• Very high affinity for and slow dissociation from μ receptors• Buprenorphine partially or totally blocks the effects of abusable opioids, such as
heroin and oxycodone• Can precipitate withdrawal
Indications for Buprenorphine: Opioid Use Disorder• Problematic pattern of opioid use leading to clinically significant
impairment or distress – DSM 5 criteria
• Heroin addicts
• Prescription opioid abuse• Obtaining pills illegally
• Fabricating or exaggerating pain
• Legitimate pain but using pills in excess of what is needed to treat the pain
Why Use Buprenorphine
• Buprenorphine has been shown in multiple studies to be as effective as methadone in suppressing opioid misuse
• Ceiling effect for respiratory depression with buprenorphine
• Somewhat less risk of abuse compared to methadone
• Methadone can only be prescribed by specially accredited opioid treatment programs for the treatment of opioid use disorder
• With extra training, non-addiction specialists can obtain a waiver from the DEA to prescribe buprenorphine to treat opioid use disorder• 8 hours for physicians, 24 hours for NPs and PAs
Pharmacokinetics
• Bioavailability depends on route of administration• Oral: Rapidly metabolized
• Transmucosal: Skips first-pass metabolism
• Primarily metabolized in GI tract and the liver, using the CYP 3A4 system
• Most metabolites are excreted fecally rather than renally -> relatively safe for patients with renal insufficiency
Effects of Buprenorphine
• Buprenorphine treatment maintains physical dependence
• Tolerance and physical dependence develop more slowly but patients still experience withdrawal• Somewhat less severe than withdrawal from a full agonist, however,
withdrawal from buprenorphine still can be severe and prolonged even with a taper
• Relapse rates after tapering from buprenorphine are very high
Buprenorphine Side Effects
• Safe when used as indicated.
• Side effects are rare, usually minor, and similar to side effects of other opioids. Some of the most commonly reported side effects of Suboxone® include:• Headaches• Withdrawal syndrome (Consider whether withdrawal may have been precipitated)• Pain• Nausea and vomiting• Constipation• Insomnia• Sweating• Numb mouth and painful tongue
Buprenorphine Side Effects
• An evaluation of waiver programs found that only 0.4% inducted onto buprenorphine ever experienced severe adverse reactions. The specific reactions reported were:• Withdrawal (n=103)
• Allergic reactions (12)
• Respiratory depression (9)
• Drug interactions (9)
• Liver problems (2)
• Renal insufficiency or aggravation of it (2)
• Unspecified (80)
Buprenorphine Side Effects
• Other less common side effects seen in opioids are also seen with buprenorphine• Sleep disordered breathing. • Included in several safety warnings for all opioids
• Serotonin syndrome• Adrenal insufficiency• Decreased sex hormone levels with chronic use • Less common with buprenorphine compared to other full agonist opioids
Contraindications
• Patients who have suffered a head injury or have intracranial lesions.
• Patients with a history of hypersensitivity to buprenorphine.
• Patients with elevated liver function testing 3-5 times greater than normal.
• Patients with moderate to severe hepatic impairment.
• Patients who indicate benzodiazepine abuse.
• Patients with at risk alcohol use or alcohol use disorder.
Drug Interactions
• Benzodiazepines, alcohol, sedative-hypnotics, tranquilizers, other opioids, muscle relaxants, gabapentin
• Anticholinergics (including inhaled)
• Drugs metabolized by the CYP 3A4 system:• Azole antifungals
• Macrolide antibiotics
• HIV protease inhibitors
• Antidepressants (e.g., fluoxetine, fluvoxamine, and amitriptyline)
• Antiseizure meds (e.g., phenobarbital, carbamazepine, phenytoin)
• Rifampicin
Special Populations
• Pregnancy: Use buprenorphine only
• Adolescents: Adolescents who are over age 16 and have had opioid use disorder for a year or more may be suitable for office-based treatment
• Elderly: May be used in elderly; consider lower dose
Phases of Buprenorphine Treatment
• Induction: Start buprenorphine treatment when the patient is in an appropriate state of withdrawal and to find the patient’s ideal daily dose (minimizes both side effects and drug craving).
• Stabilization: Eliminate opioid use other than buprenorphine. Continues until your patient is no longer experiencing withdrawal symptoms or intense cravings.
• Maintenance: Continue daily dose of buprenorphine to prevent relapse. Likely indefinite.
Office-Based Opioid Treatment in Primary Care• There is a large, unmet need for treatment of opioid use disorder.
• Only 10 to 15% of individuals who have opioid use disorder receive treatment
• Incorporating treatment into primary care increases availability and accessibility of treatment.• Reaches patients who would otherwise not seek treatment
• It’s effective
Prevalence of Buprenorphine Use
• Approximately 36,000 providers were waivered to prescribe buprenorphine at the end of 2016 (around 6% of the physicians and surgeons in the US)
• There are more than twice as many people maintained on buprenorphine as methadone
• 9.3 million buprenorphine prescriptions were filled in the U.S. in 2012
Special Considerations – Chronic Pain
• Many patients with opioid use disorder have chronic pain
• An ASAM Consensus Panel on buprenorphine treatment determined that there is insufficient data to recommend the use of buprenorphine for the treatment of acute or chronic pain in patients with a history of opioid use disorder
• A panel of experienced prescribers noted that patients having continuing chronic pain and opioid use disorder can be more challenging to treat in office-based opioid treatment
• Twice daily dosing may help
Special Considerations – Postoperative or Acute Pain• Continue buprenorphine
• Provide regional anesthesia, increase the buprenorphine dose, add a high-potency opioid such as fentanyl (1 mg Suboxone® = 75-90 mg morphine)
If Your Patient is on Buprenorphine…
• They will (should) likely be on it indefinitely
• There are many medication interactions
• Be aware of common side effects (e.g., constipation)
• Be aware of potential serious adverse events (sedation, hepatitis)
• Special considerations for acute pain (injuries, accidents, surgery)• Probably will be managed by buprenorphine prescriber
• High enough doses of full opioid agonists will work
• Concurrent psychosocial treatment is very important
If You Want to Prescribe Buprenorphine…
• Non-addiction specialists can obtain a waiver to prescribe• 8 hours for physicians (online)
• https://www.samhsa.gov/medication-assisted-treatment/training-resources/buprenorphine-physician-training
• 24 hours for NPs and PAs (in process) – may take initial 8 hours online now• pcssmat.org
• Must have capacity to provide or refer patients for counseling
• Can prescribe buprenorphine for hospitalized patients without a DEA waiver
Resources/References
• steverummlerhopefoundation.org
• Prescribetoprevent.org
• Substance Abuse and Mental Health Services: www.samhsa.gov
• Provider’s Clinical Support System for Medication Assisted Therapy: pcssmat.org
• Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Mattick et al. Cochrane Database Syst Rev. 2014 Feb 6;(2):CD002207
• A Review of Buprenorphine Diversion and Misuse: The Current Evidence Base and Experiences from Around the World. Lofwall and Walsh. J Addict Med. 2014 Sep-Oct; 8(5): 315–326.
• Donaher PA, Welsh C. Managing opioid addiction with buprenorphine. American Family Physician. 2006; 73(9): 1573-8. Available at: http://www.aafp.org/afp/2006/0501/p1573.html
• Tzschentke TM. Behavioral pharmacology of buprenorphine, with a focus on preclinical models of reward and addiction. Psychopharmacology (Berl). 2002; 161(1): 1-16. Available at: https://www.ncbi.nlm.nih.gov/pubmed/11967625
• Fiellin DA, Schottenfeld RS, Cutter CJ, et al. Primary care-based buprenorphine taper vs maintenance therapy for prescription opioid dependence: A randomized clinical trial. JAMA Internal Medicine. 2014; 174(12): 1947-1954. Available at: http://archinte.jamanetwork.com/article.aspx?articleid=1916910
• Weiss RD, Potter JS, Fiellin DA, Byrne M, Connery HS, Dickinson W, Gardin J, Griffin ML, Gourevitch MN, Haller DL, Hasson HL, Huang Z, Jacobs P, Kosinski AS, Lindblad R, McCance-Katz EF, Provost SE, Selzer J, Somoza EC, Sonne SC, Ling W. Adjunctive Counseling During Brief and Extended Buprenorphine-Naloxone Treatment for Prescription Opioid Dependence. Arch Gen Psychiatry. 2012; 68(12): 1238-1246. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3470422/
• Dunn KE, Sigmon SC, Strain EC, et al.. The association between outpatient buprenorphine detoxification duration and clinical treatment outcomes: a review. Drug Alcohol Depend. 2011; 119(1-2): 1-9. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21741781
• Reckitt Benckiser Pharmaceuticals Inc. Suboxone Prescribing Information. Reckitt Benckiser Pharmaceuticals. 2014. Available at: http://www.suboxone.com/content/pdfs/prescribing-information.pdf
• Stanton A, Mcleod C, Luckey B, Kissin W, Sonnefeld LJ. SAMHSA/CSAT Evaluation of the Buprenorphine Waiver Program. Paper presented at: 37th Annual Medical- Scientific Conference of the American Society of Addiction Medicine. 2006. Available at: http://www.samhsa.gov/sites/default/files/programs_campaigns/medication_assisted/evaluation-buprenorphine-waiver-program-study-overview.pdf
• Food and Drug Administration (FDA). Buprenorphine Drug Label. NDA 20-732, NDA 20-733. 2010.
• Kraus ML, Alford DP, Kotz MM, et al. Statement of the American Society of Addiction Medicine Consensus Panel on the Use of Buprenorphine in Office-Based Treatment of Opioid Addiction.. Journal of Addiction Medicine . 2011; 5(4): 254-263. Available at: http://www.asam.org/docs/advocacy/use-of-buprenorphine-in-office-based-treatment-of-opioid-addiction.pdf
• Johnson RE, Strain EC, Amass L. Buprenorphine: how to use it right. Drug Alcohol Depend. 2003; 70(suppl 2): S59-S77. Available at: https://www.ncbi.nlm.nih.gov/pubmed/12738351
• Alford DP, Labelle CT, Kretsch N, Bergeron A, Winter M, Botticelli M, Samet JH. Collaborative care of opioid-addicted patients in primary care using buprenorphine: five-year experience. Archives of Internal Medicine. 2011; 171(5): 425-31.
• Arfken CL, Johanson CE, di Menza S, Schuster CR. Expanding treatment capacity for opioid dependence with office-based treatment with buprenorphine: National surveys of physicians. J Subst Abuse Treat. 2010; 39(2): 96-104.
• Mintzer IL, Eisenberg M, Terra M, MacVane C, Himmelstein DU, Woolhandler S. Treating opioid addiction with buprenorphine-naloxone in community-based primary care settings. Ann Fam Med. 2007; 5(2): 146-50.
• SAMHSA. Physician and Program Data. SAMHSA Medication Assisted Treatment. 2017. Available at: https://www.samhsa.gov/programs-campaigns/medication-assisted-treatment/physician-program-data
• Renner J (Chair), Saxon A, Levounis P. Buprenorphine Update and Evolving Standards of Care. IPS: The Mental Health Services Conference, New York City. 2015; Oct 8-11: . Available at: http://www.psychiatry.org/File%20Library/Psychiatrists/Meetings/IPS-TheMentalHealthServicesConference/IPS-Program-Guide.pdf
• Anaesth Intensive Care 2013; 41: 222-230. Pain relief and opioid requirements in the first 24 hours after surgery in patients taking buprenorphine and methadone opioid substitution therapy P E. MACINTYRE*, R. A. RUSSELLf, K. A. N. USHER*, M. GAUGHWIN§, C. A. HUXTABLE