concord hospital - bureau of health · pdf filecompanion publication. ... concord gosford...
TRANSCRIPT

July 2009 – June 2012
Returns to acute care and mortality for five clinical conditions2
Condition This period
July 2000 – June 2003 July 2003 – June 2006 July 2006 – June 2009 July 2009 – June 2012
Average length of stay (days)3
Space for chart
Pneumonia
Hip fracture surgery
Concord Hospital
Time series
Acute myocardial
infarction (AMI)
Ischaemic stroke
Congestive heart
failure (CHF)
05
1015202530354045
Length
of
sta
y
Acute myocardial infarction
Ischaemic stroke Congestive heart failure Pneumonia Hip fracture surgery
Range across NSW hospitals NSW This hospital
Higher than expected No different than expected Lower than expected Not reported
This profile reports risk-standardised readmission ratios (RSRRs) and risk-standardised mortality ratios (RSMRs). The
ratios take into account differences across hospitals in terms of case mix and volumes of patients, and results are
reported as either: higher than expected; no different than expected; or lower than expected. The performance dashboard
below summarises ratio results for five conditions over a 12 year period together with length of stay information for July
2009 – June 2012. Subsequent pages provide information to support interpretation of the RSRR. Readmissions are
defined as returns to acute care1 and results describe the age profile and comorbidity profile of patients; the number who
returned to acute care within 30 days of discharge; and reasons, location and timing of returns to acute care.
RSRR
RSMR
RSRR
RSMR
RSRR
RSRR
RSMR
RSRR
RSMR
RSRR
RSMR
RSRR
RSMR
RSRR
RSRR
RSMR
RSRR
RSMR
Bureau of Health Information | Concord Hospital 1

NOTES:
1. For patients whose acute hospitalisation ends with discharge home, a return to acute care involves readmission to hospital; while
for patients whose acute hospitalisation ends with a 'discharge' to non-acute care, a return involves a move back into an acute
care setting regardless of whether they physically left the hospital.
2. The “Not reported” category is used when there were fewer than 50 index cases admitted in the time period. Risk-standardised
mortality ratios have been taken from the BHI publication The Insights Series: 30-day mortality following hospitalisation, five
clinical conditions, NSW, July 2009 – 2012 and further information about this measure can be found there. RSRR outlier status is
determined using funnel plot control limits of 95% and 99.8%.
3. For calculation of average length of stay, index admissions that were transferred in from, or transferred out to, another acute care
hospital were excluded. Unreasonably long episodes are trimmed on the basis of the Diagnosis Related Group (DRG) of the
episode. The trim point is the third quartile plus 1.5 x the interquartile range of all in-scope episodes in each DRG.
4. Discharge destinations are based on the mode of separation of the index case. For episodes coded as 'Discharged by hospital' or
'Discharged on leave', patients are considered to be destined for their place of usual residence. All other modes of separation are
deemed to indicate a discharge destination other than a patient‟s place of usual residence.
5. Age of the patient at admission for the index case is used. Percentages may not add to 100% due to rounding.
6. Comorbidities are identified from the hospital discharge records using the Elixhauser comorbidity set (plus dementia) with a one
year look-back from the admission date of the index case. Percentage labels have been rounded to the nearest integer.
7. Results for hospitals with <1 expected return to acute care (readmission) within 30 days are not shown.
8. Peer hospitals are identified according to the NSW Ministry of Health‟s peer grouping as of 30 June 2011. Hospitals with fewer
than 50 index cases are not shown.
9. Hospitals are classified as urban and regional/rural using the geocoded address of the hospital assigned to ABS statistical areas
(SA2) and the Australian remoteness index for areas. Further information can be found in this report's Spotlight on Measurement
companion publication.
10.Reasons for return to acute care are classified according to a draft specification made available to the BHI by the Australian
Institute of Health and Welfare. Principal diagnoses for the return to acute care episode, are stratified as: the same as the index
hospitalisation; related to that of the index hospitalisation; potentially related to hospital care (i.e. complications and adverse
events) using various time horizons; and, other reasons. Percentages may not add to 100% due to rounding.
Further information can be found in this report's Spotlight on Measurement companion publication.
Data source: SAPHaRI, Centre for Epidemiology and Evidence, NSW Ministry of Health.
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 2
This hospital NSW
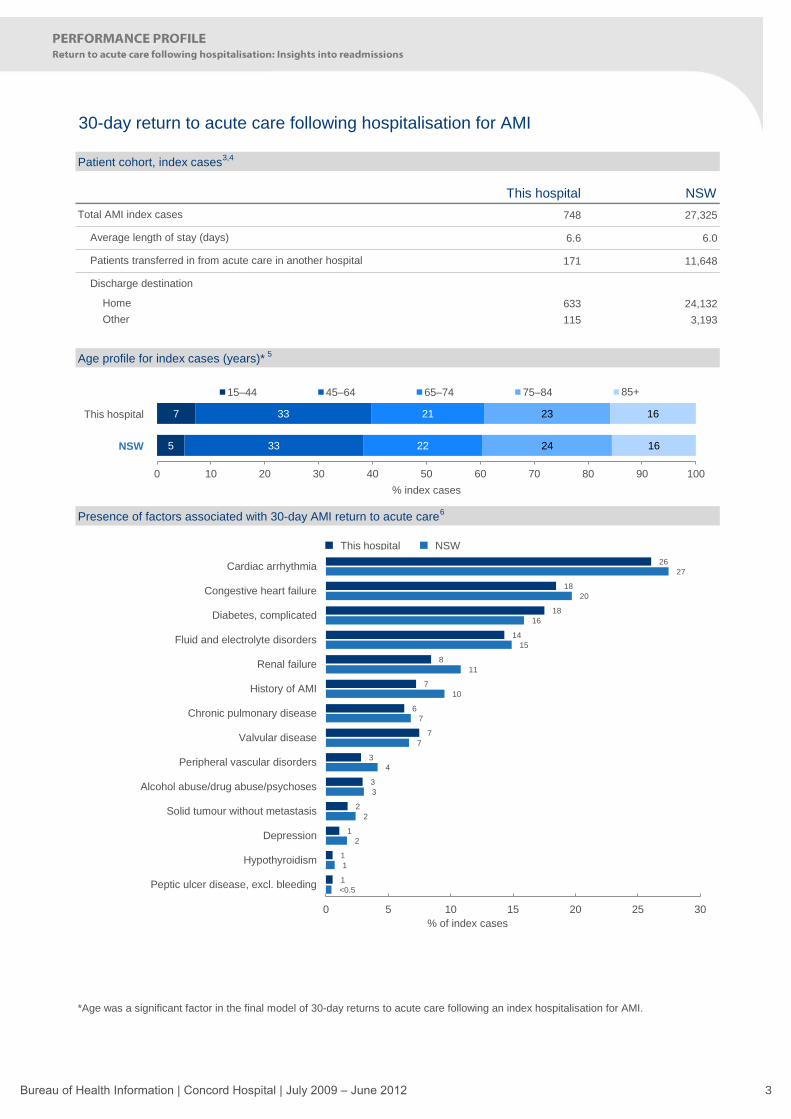
748 27,325
6.6 6.0
171 11,648
633 24,132
115 3,193
*Age was a significant factor in the final model of 30-day returns to acute care following an index hospitalisation for AMI.
Presence of factors associated with 30-day AMI return to acute care6
space for chart
30-day return to acute care following hospitalisation for AMI
Patient cohort, index cases3,4
Total AMI index cases
Age profile for index cases (years)* 5
Other
Home
Average length of stay (days)
Patients transferred in from acute care in another hospital
Discharge destination
space for chart5
7
33
33
22
21
24
23
16
16
0 10 20 30 40 50 60 70 80 90 100
% index cases
15–44 45–64 65–74 75–84 85+
This hospital
NSW
26
18
18
14
8
7
6
7
3
3
2
1
1
1
27
20
16
15
11
10
7
7
4
3
2
2
1
<0.5
0 5 10 15 20 25 30
Cardiac arrhythmia
Congestive heart failure
Diabetes, complicated
Fluid and electrolyte disorders
Renal failure
History of AMI
Chronic pulmonary disease
Valvular disease
Peripheral vascular disorders
Alcohol abuse/drug abuse/psychoses
Solid tumour without metastasis
Depression
Hypothyroidism
Peptic ulcer disease, excl. bleeding
% of index cases
This hospital NSW
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 3

Hospital level AMI RSRR by number of expected returns to acute care (readmissions)7
space for chart
space for chart
30-day return to acute care following hospitalisation for AMI
Observed and expected 30-day returns to acute care, grouped with peers8
Hospital-specific RSRRs report the ratio of actual or „observed‟ number of returns to acute care to the „expected‟
number of returns. A competing risk regression model draws on the NSW patient population‟s characteristics and
outcomes to estimate the expected number of returns for each hospital, given the characteristics of its patients. An
RSRR less than 1.0 indicates lower-than-expected returns to acute care, and a ratio higher than 1.0 indicates higher-
than-expected returns. Small deviations from 1.0 are not considered to be meaningful. Funnel plots with 95% and
99.8% control limits around the NSW rate are used to identify outliers.
0 50 100 150 200 250 300 350
Calvary Mater Newcastle
Bankstown / Lidcombe
St Vincent's
Concord
Gosford
Royal North Shore
Nepean
Prince of Wales
St George
Wollongong
John Hunter
Royal Prince Alfred
Liverpool
Westmead
Number of 30-day returns to acute care
This hospital,observed returns
Peer group hospital,observed returns
Expected returns to acutecare (based on model)
RSRR 0.81
NSW
0
0.5
1
1.5
2
2.5
3
0 50 100 150 200 250 300
Ris
k-s
tandard
ised r
eadm
issio
n r
atio
(O
bserv
ed/E
xpecte
d)
Expected number of returns to acute care (readmissions) within 30 days
This hospital
Other hospital
99.8% limit (3SD)
95% limit (2SD)
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 4

This hospital NSW
101 4,453
77 3,042
24 1,411
21
3
0
Distribution of reasons for returns to acute care
Number of, and reasons for, returns to acute care following hospitalisation for AMI, by days post discharge
Returned to a different hospital
Of these:
To an urban public hospital
30-day return to acute care following hospitalisation for AMI
Location of returns to acute care9
Returned to the hospital where acute care was completed
Total returns to acute care following AMI index hospitalisation
To a private hospital
Reasons for and time to returns to acute care10
space for chart
space for chart
To a regional or rural public hospital
14
11
33
36
8
11
8
1
20
18
18
24
0 10 20 30 40 50 60 70 80 90 100
% returns to acute care
Principal diagnosis Condition related to principal diagnosis Potentially related to hospital care (relevant at any time)
Potentially related to hospital care (time sensitive, ≤ 7 days post discharge)
Potentially related to hospital care (time sensitive, 8–30 days post discharge)
Other condition
This hospital
NSW
5 3
1 2
13 15
7
1
3 3
3
2
1
10
2
6
9
5
8
2
0
5
10
15
20
25
30
35
40
1–7 days 8–14 days 15–21 days 22–30 days
Num
ber
of re
turn
s to a
cute
care
Days post discharge
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 5

Bureau of Health Information | Concord Hospital | July 2009 – June 2012 6

This hospital NSW
470 12,776
10.2 9.5
30 1,713
237 6,772
233 6,004
space for chart
*Age was not a significant factor in the final model of 30-day returns to acute care following an index hospitalisation for ischaemic
stroke.
Discharge destination
Home
Other
Age profile for index cases (years)* 5
space for chart
Presence of factors associated with 30-day ischaemic stroke return to acute care6
Patients transferred in from acute care in another hospital
30-day return to acute care following hospitalisation for ischaemic stroke
Patient cohort, index cases3,4
Total ischaemic stroke index cases
Average length of stay (days)
4
3
20
18
23
21
32
34
21
24
0 10 20 30 40 50 60 70 80 90 100
% index cases
15–44 45–64 65–74 75–84 85+
This hospital
NSW
35
19
6
8
6
4
1
0
32
15
7
6
4
4
1
<0.5
0 5 10 15 20 25 30 35 40
Cardiac arrhythmia
Fluid and electrolyte disorders
Renal failure
Dementia
Weight loss
Chronic pulmonary disease
Metastatic cancer
AIDS/HIV
% of index cases
This hospital NSW
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 7

space for chart
30-day return to acute care following hospitalisation for ischaemic stroke
Hospital-specific RSRRs report the ratio of actual or „observed‟ number of returns to acute care to the „expected‟
number of returns. A competing risk regression model draws on the NSW patient population‟s characteristics and
outcomes to estimate the expected number of returns for each hospital, given the characteristics of its patients. An
RSRR less than 1.0 indicates lower-than-expected returns to acute care, and a ratio higher than 1.0 indicates higher-
than-expected returns. Small deviations from 1.0 are not considered to be meaningful. Funnel plots with 95% and
99.8% control limits around the NSW rate are used to identify outliers.
Hospital level ischaemic stroke RSRR by number of expected returns to acute care (readmissions)7
space for chart
Observed and expected 30-day returns to acute care, grouped with peers8
Calvary Mater Newcastle
St Vincent's
Prince of Wales
Concord
Bankstown / Lidcombe
Nepean
Royal North Shore
Royal Prince Alfred
Gosford
Westmead
John Hunter
Wollongong
St George
Liverpool
0 20 40 60 80 100 120
Number of 30-day returns to acute care
This hospital,observed returns
Peer group hospital,observed returns
Expected returns to acutecare (based on model)
RSRR 0.90
NSW
0
0.5
1
1.5
2
2.5
3
0 50 100 150 200 250 300
Ris
k-s
tandard
ised r
eadm
issio
n r
atio
(O
bserv
ed/E
xpecte
d)
Expected number of returns to acute care (readmissions) within 30 days
This hospital
Other hospital
99.8% limit (3SD)
95% limit (2SD)
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 8

This hospital NSW
43 1,321
33 1,022
10 299
10
0
0
Distribution of reasons for returns to acute care
space for chart
Number of, and reasons for, returns to acute care following hospitalisation for ischaemic stroke, by days post discharge
Of these:
To an urban public hospital
To a regional or rural public hospital
To a private hospital
Reasons for and time to returns to acute care10
space for chart
Returned to a different hospital
30-day return to acute care following hospitalisation for ischaemic stroke
Location of returns to acute care9
Returned to the hospital where acute care was completed
Total returns to acute care following ischaemic stroke index hospitalisation
19
7
10
7
21
30
7
12
15
23
28
21
0 10 20 30 40 50 60 70 80 90 100
% returns to acute care
Principal diagnosis Condition related to principal diagnosis Potentially related to hospital care (relevant at any time)
Potentially related to hospital care (time sensitive, ≤ 7 days post discharge)
Potentially related to hospital care (time sensitive, 8–30 days post discharge)
Other condition
This hospital
NSW
1 2
1
1
1 4
3 5 1
5
5
1 4
1
4
3 1
0
2
4
6
8
10
12
14
16
1–7 days 8–14 days 15–21 days 22–30 days
Num
ber
of re
turn
s to a
cute
care
Days post discharge
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 9

Bureau of Health Information | Concord Hospital | July 2009 – June 2012 10

This hospital NSW
889 29,961
8.2 6.6
31 2,820
707 26,099
182 3,862
space for chart
*Age was a significant factor in the final model of 30-day returns to acute care following an index hospitalisation for congestive heart
failure.
Discharge destination
Home
Other
Age profile for index cases (years)*5
space for chart
Presence of factors associated with 30-day congestive heart failure return to acute care6
Patients transferred in from acute care in another hospital
30-day return to acute care following hospitalisation for congestive heart failure
Patient cohort, index cases3,4
Total congestive heart failure index cases
Average length of stay (days)
1
1
11
8
18
16
37
40
32
34
0 10 20 30 40 50 60 70 80 90 100
% index cases
15–44 45–64 65–74 75–84 85+
This hospital
NSW
62
40
39
32
30
16
32
13
11
52
38
30
27
22
21
16
8
8
0 10 20 30 40 50 60 70
Cardiac arrhythmia
History of congestive heart failure
Fluid and electrolyte disorders
Renal failure
Diabetes, complicated
Chronic pulmonary disease
Valvular disease
Coagulopathy
Deficiency anaemia
% of index cases
This hospital NSW
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 11

space for chart
30-day return to acute care following hospitalisation for congestive heart failure
Hospital-specific RSRRs report the ratio of actual or „observed‟ number of returns to acute care to the „expected‟
number of returns. A competing risk regression model draws on the NSW patient population‟s characteristics and
outcomes to estimate the expected number of returns for each hospital, given the characteristics of its patients. An
RSRR less than 1.0 indicates lower-than-expected returns to acute care, and a ratio higher than 1.0 indicates higher-
than-expected returns. Small deviations from 1.0 are not considered to be meaningful. Funnel plots with 95% and
99.8% control limits around the NSW rate are used to identify outliers.
Hospital level congestive heart failure RSRR by number of expected returns to acute care (readmissions)7
space for chart
Observed and expected 30-day returns to acute care, grouped with peers8
Sydney/Sydney Eye
Calvary Mater Newcastle
St Vincent's
Gosford
Royal North Shore
Wollongong
Nepean
Concord
Prince of Wales
Bankstown / Lidcombe
John Hunter
Royal Prince Alfred
St George
Liverpool
Westmead
0 50 100 150 200 250 300 350
Number of 30-day returns to acute care
This hospital,observed returns
Peer group hospital,observed returns
Expected returns to acutecare (based on model)
RSRR 0.93
NSW
0
0.5
1
1.5
2
2.5
3
0 50 100 150 200 250 300
Ris
k-s
tandard
ised r
eadm
issio
n r
atio
(O
bserv
ed/E
xpecte
d)
Expected number of returns to acute care (readmissions) within 30 days
This hospital
Other hospital
99.8% limit (3SD)
95% limit (2SD)
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 12

This hospital NSW
199 6,850
155 5,608
44 1,242
41
2
1
Distribution of reasons for returns to acute care
Number of, and reasons for, returns to acute care following hospitalisation for congestive heart failure, by days post discharge
space for chart
Of these:
To an urban public hospital
To a regional or rural public hospital
To a private hospital
Reasons for and time to returns to acute care10
space for chart
Returned to a different hospital
30-day return to acute care following hospitalisation for congestive heart failure
Location of returns to acute care9
Returned to the hospital where acute care was completed
Total returns to acute care following congestive heart failure index hospitalisation
37
40
11
8
6
7
7
13
19
16
19
17
0 10 20 30 40 50 60 70 80 90 100
% returns to acute care
Principal diagnosis Condition related to principal diagnosis Potentially related to hospital care (relevant at any time)
Potentially related to hospital care (time sensitive, ≤ 7 days post discharge)
Potentially related to hospital care (time sensitive, 8–30 days post discharge)
Other condition
This hospital
NSW
22 22 15
21
5 3
4
4
6
1 6
1
25
15
8 8
11
8
7 7
0
10
20
30
40
50
60
70
80
1–7 days 8–14 days 15–21 days 22–30 days
Num
ber
of re
turn
s to a
cute
care
Days post discharge
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 13

Bureau of Health Information | Concord Hospital | July 2009 – June 2012 14

This hospital NSW
892 42,777
7.6 6.1
46 4,358
700 37,971
192 4,806
space for chart
*Age and sex were significant factors in the final model of 30-day return to acute care following an index hospitalisation for pneumonia.
The percentage of index hospitalisations that were female patients at this hospital was 47% compared to 48% for NSW.
Discharge destination
Home
Other
Age profile for index cases (years)*5
space for chart
Presence of factors associated with 30-day pneumonia return to acute care6
Patients transferred in from acute care in another hospital
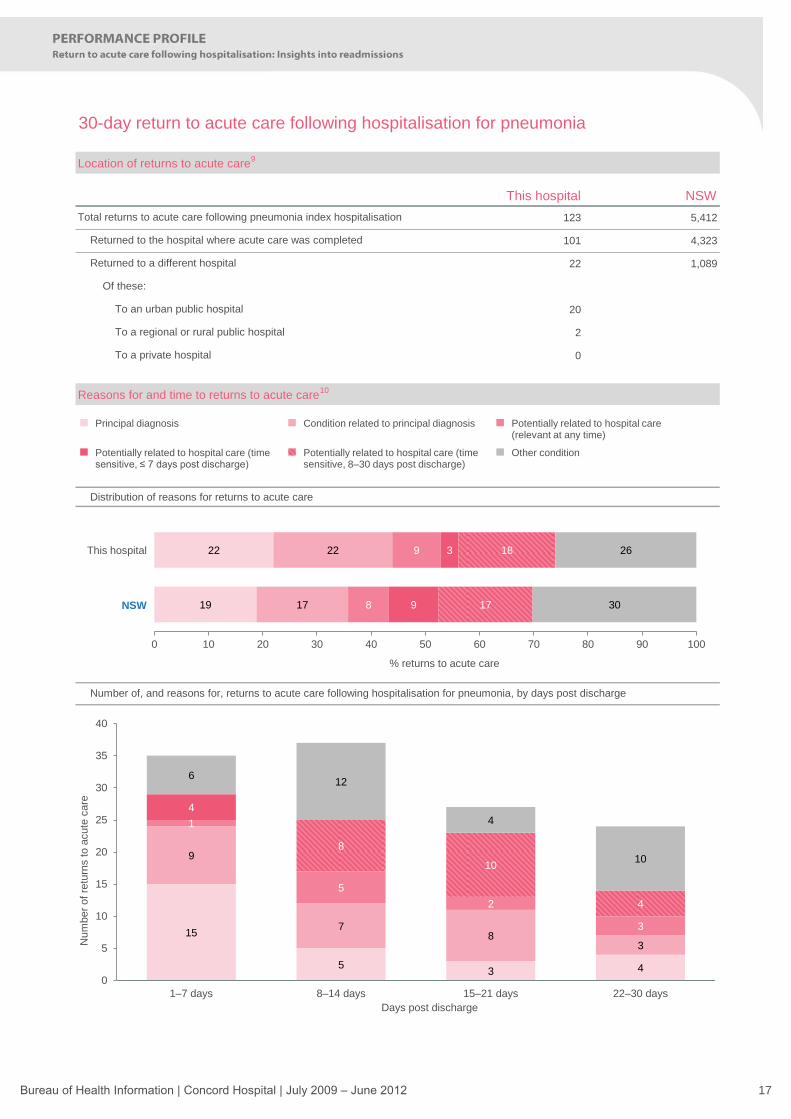
30-day return to acute care following hospitalisation for pneumonia
Patient cohort, index cases3,4
Total pneumonia index cases
Average length of stay (days)
15
11
22
17
18
18
26
28
19
26
0 10 20 30 40 50 60 70 80 90 100
% index cases
18–44 45–64 65–74 75–84 85+
This hospital
NSW
36
18
26
28
17
10
12
12
7
4
10
6
4
4
4
3
2
2
3
24
20
20
19
14
10
9
6
6
5
4
4
3
3
3
3
3
2
1
0 5 10 15 20 25 30 35 40
Fluid and electrolyte disorders
Chronic pulmonary disease
Cardiac arrhythmia
Hypertension, uncompl. or compl.
Congestive heart failure
History of pneumonia
Renal failure
Weight loss
Solid tumour without metastasis
Alcohol abuse/drug abuse/psychoses
Coagulopathy
Other neurological disorders
Pulmonary circulation disorders
Deficiency anaemia
Metastatic cancer
Depression
Diabetes, uncomplicated
Liver disease
Lymphoma
% of index cases
This hospital NSW
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 15

space for chart
30-day return to acute care following hospitalisation for pneumonia
Hospital-specific RSRRs report the ratio of actual or „observed‟ number of returns to acute care to the „expected‟
number of returns. A competing risk regression model draws on the NSW patient population‟s characteristics and
outcomes to estimate the expected number of returns for each hospital, given the characteristics of its patients. An
RSRR less than 1.0 indicates lower-than-expected returns to acute care, and a ratio higher than 1.0 indicates higher-
than-expected returns. Small deviations from 1.0 are not considered to be meaningful. Funnel plots with 95% and
99.8% control limits around the NSW rate are used to identify outliers.
Hospital level pneumonia RSRR by number of expected returns to acute care (readmissions)7
space for chart
Observed and expected 30-day returns to acute care, grouped with peers8
0 50 100 150 200 250 300
Sydney/Sydney Eye
Bankstown / Lidcombe
St Vincent's
Royal North Shore
John Hunter
Calvary Mater Newcastle
Gosford
Prince of Wales
Concord
Wollongong
Royal Prince Alfred
Nepean
Liverpool
St George
Westmead
Number of 30-day returns to acute care
This hospital,observed returns
Peer group hospital,observed returns
Expected returns to acutecare (based on model)
RSRR 0.93
NSW
0
0.5
1
1.5
2
2.5
3
0 50 100 150 200 250 300
Ris
k-s
tandard
ised r
eadm
issio
n r
atio
(O
bserv
ed/E
xpecte
d)
Expected number of returns to acute care (readmissions) within 30 days
This hospital
Other hospital
99.8% limit (3SD)
95% limit (2SD)
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 16
This hospital NSW
123 5,412
101 4,323
22 1,089
20
2
0
Distribution of reasons for returns to acute care
Number of, and reasons for, returns to acute care following hospitalisation for pneumonia, by days post discharge
space for chart
Of these:
To an urban public hospital
To a regional or rural public hospital
To a private hospital
Reasons for and time to returns to acute care10
space for chart
Returned to a different hospital
30-day return to acute care following hospitalisation for pneumonia
Location of returns to acute care9
Total returns to acute care following pneumonia index hospitalisation
Returned to the hospital where acute care was completed
19
22
17
22
8
9
9
3
17
18
30
26
0 10 20 30 40 50 60 70 80 90 100
% returns to acute care
Principal diagnosis Condition related to principal diagnosis Potentially related to hospital care (relevant at any time)
Potentially related to hospital care (time sensitive, ≤ 7 days post discharge)
Potentially related to hospital care (time sensitive, 8–30 days post discharge)
Other condition
This hospital
NSW
15
5 3 4
9
7 8
3
1
5
2
3
4
8
10
4
6 12
4
10
0
5
10
15
20
25
30
35
40
1–7 days 8–14 days 15–21 days 22–30 days
Num
ber
of
retu
rns to a
cute
care
Days post discharge
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 17

Bureau of Health Information | Concord Hospital | July 2009 – June 2012 18

This hospital NSW
462 14,035
12.3 12.1
22 3,141
56 4,888
406 9,147
space for chart
*Age and sex were significant factors in the final model of 30-day return to acute care following an index hospitalisation for hip fracture
surgery. The percentage of index hospitalisations that were female patients at this hospital was 73% compared to 73% for NSW.
Discharge destination
Home
Other
Age profile for index cases (years)*5
space for chart
Presence of factors associated with 30-day hip fracture surgery return to acute care6
Patients transferred in from acute care in another hospital
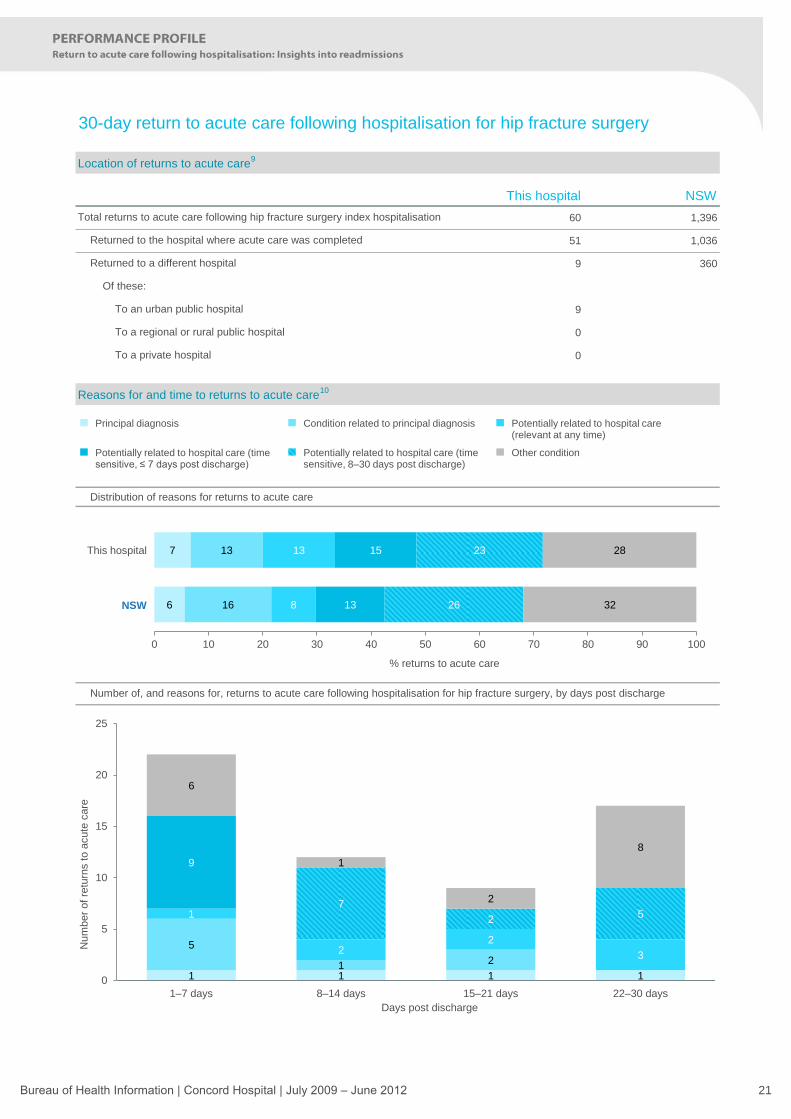
30-day return to acute care following hospitalisation for hip fracture surgery
Patient cohort, index cases3,4
Total hip fracture surgery index cases
Average length of stay (days)
6
5
12
8
35
35
48
53
0 10 20 30 40 50 60 70 80 90 100
% index cases
50–64 65–74 75–84 85+
This hospital
NSW
37
30
8
12
7
6
3
2
1
29
24
8
8
7
4
3
2
1
0 5 10 15 20 25 30 35 40
Fluid and electrolyte disorders
Dementia
Renal failure
Diabetes, complicated
Chronic pulmonary disease
Coagulopathy
Solid tumour without metastasis
Diabetes, uncomplicated
Liver disease
% of index cases
This hospital NSW
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 19

space for chart
30-day return to acute care following hospitalisation for hip fracture surgery
Hospital-specific RSRRs report the ratio of actual or „observed‟ number of returns to acute care to the „expected‟
number of returns. A competing risk regression model draws on the NSW patient population‟s characteristics and
outcomes to estimate the expected number of returns for each hospital, given the characteristics of its patients. An
RSRR less than 1.0 indicates lower-than-expected returns to acute care, and a ratio higher than 1.0 indicates higher-
than-expected returns. Small deviations from 1.0 are not considered to be meaningful. Funnel plots with 95% and
99.8% control limits around the NSW rate are used to identify outliers.
Hospital level hip fracture surgery RSRR by number of expected returns to acute care (readmissions)7
space for chart
Observed and expected 30-day returns to acute care, grouped with peers8
0 20 40 60 80 100 120
St Vincent's
Royal Prince Alfred
Liverpool
Bankstown / Lidcombe
Prince of Wales
Gosford
Concord
Royal North Shore
Westmead
St George
Wollongong
John Hunter
Nepean
Number of 30-day returns to acute care
This hospital,observed returns
Peer group hospital,observed returns
Expected returns to acutecare (based on model)
RSRR 1.21
NSW
0
0.5
1
1.5
2
2.5
3
0 50 100 150 200 250 300
Ris
k-s
tandard
ised r
eadm
issio
n r
atio
(O
bserv
ed/E
xpecte
d)
Expected number of returns to acute care (readmissions) within 30 days
This hospital
Other hospital
99.8% limit (3SD)
95% limit (2SD)
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 20
This hospital NSW
60 1,396
51 1,036
9 360
9
0
0
Distribution of reasons for returns to acute care
Number of, and reasons for, returns to acute care following hospitalisation for hip fracture surgery, by days post discharge
space for chart
Of these:
To an urban public hospital
To a regional or rural public hospital
To a private hospital
Reasons for and time to returns to acute care10
space for chart
Returned to a different hospital
30-day return to acute care following hospitalisation for hip fracture surgery
Location of returns to acute care9
Returned to the hospital where acute care was completed
Total returns to acute care following hip fracture surgery index hospitalisation
6
7
16
13
8
13
13
15
26
23
32
28
0 10 20 30 40 50 60 70 80 90 100
% returns to acute care
Principal diagnosis Condition related to principal diagnosis Potentially related to hospital care (relevant at any time)
Potentially related to hospital care (time sensitive, ≤ 7 days post discharge)
Potentially related to hospital care (time sensitive, 8–30 days post discharge)
Other condition
This hospital
NSW
1 1 1 1
5
1 2
1
2 2
3
9
7
2 5
6
1
2
8
0
5
10
15
20
25
1–7 days 8–14 days 15–21 days 22–30 days
Num
ber
of re
turn
s to a
cute
care
Days post discharge
Bureau of Health Information | Concord Hospital | July 2009 – June 2012 21

Bureau of Health Information | Concord Hospital | July 2009 – June 2012 22