complexed plasma elastase as an in vivo marker for leukocyte activation in antineutrophil...
TRANSCRIPT

1680 ARTHRITIS & RHEUMATISM Vol. 40, No. 9, September 1997, pp 1680-1684 0 1997, American College of Rheumatology
COMPLEXED PLASMA ELASTASE AS AN IN VIVO MARKER FOR LEUKOCYTE ACTIVATION IN ANTINEUTROPHIL CYTOPLASMIC
ANTIBODY -ASS 0 CIATED VAS CULITI S
M. HAUBITZ, P. SCHULZECK, S. SCHELLONG, M. SCHULZE, K. M. KOCH, and R. BRUNKHORST
Objective. It has been postulated that antineutro- phi1 cytoplasmic antibody (ANCA)-induced degranula- tion of primed granulocytes and monocytes is involved in the pathogenesis of ANCA-associated vasculitis. Since elastase is the major lysosomal protein released during leukocyte degranulation, we investigated cell activation in vivo in patients with ANCA-associated vasculitis by determining complexed plasma elastase levels.
Methods. Plasma elastase complexed with al- antitrypsin was measured in 20 patients with ANCA- associated vasculitis, using an immunoactivation assay. In parallel, C-reactive protein (CRP) and ANCA levels were determined and clinical disease activity was assessed.
Results. Complexed elastase levels were signifi- cantly elevated in patients with ANCA-associated vas- culitis who had not received immunosuppressive ther- apy (mean k SD 71.5 +: 22.6 pg/liter), compared with healthy volunteers (12.2 f 11.4 &liter; P < 0.001). Elastase decreased significantly after 2 weeks (46.5 f 26.8 &liter; P < 0.01) and further after 8-10 weeks of immunosuppressive treatment (28.1 f 13.4 &liter; P < 0.02), in correlation with decreasing vasculitis activity. Concomitantly, ANCA titers and CRP levels decreased.
Conclusion. These data support the theory that, by the release of lysosomal proteinases, leukocyte acti- vation may be involved in the pathogenesis of ANCA- associated vasculitis. In addition, plasma elastase may be used as a marker for disease activity.
Wegener’s granulomatosis (WG) and micro- scopic polyangiitis (MP) are systemic diseases that are characterized by a necrotizing pauci-immune vasculitis. WG mainly involves the upper and lower respiratory tract and the kidney. Although limited forms with no renal involvement are common in the early course of WG, the disease usually progresses to a generalized form. MP is characterized by necrotizing glomerulone- phritis, often together with pulmonary capillaritis. To date, the pathogenesis of WG and MP has only been theorized. It has been suggested that antineutrophil cytoplasmic antibodies (ANCA) may be involved in the pathogenesis, since there is a well-documented associa- tion between the presence of ANCA and these diag- noses (1-3). Furthermore, a positive correlation be- tween the ANCA level and disease activity has been shown (43). These findings are supported by in vitro data demonstrating that the binding of ANCA to surface-expressed proteinase 3 (PR3) or myeloperoxi- dase (MPO) of primed human neutrophils (6) can activate these cells to undergo a respiratory burst and degranulate (7), leading to endothelial cell injury. How- ever, the presence and role of degranulation products have not yet been investigated in vivo.
Elastase is the major lysosomal proteinase, gen- erated and released by activated granulocytes (8) and potentially also by monocytes (9). It is rapidly complexed in the circulation by antiproteinases, of which the most important is a,-antitrypsin. In the present study, we therefore evaluated in vivo granulocyte activation in patients with ANCA-associated vasculitis by measure- ment of a,-antitrypsin-complexed elastase in plasma.
M. Haubitz, MD, P. Schulzeck, MD, S. Schellong, MD, M. Schulze, MD, K. M. Koch, MD, R. Brunkhorst, MD: Medical School PATIENTS AND METHODS Hannover, Hannover, Germany.
Nephrology, Medizinische Hochschule, 30623 Hannover, Germany.
revised form April 23, 1997.
Address reprint requests to M. Haubitz, MD, Department of
Submitted for publication December 31, 1996; accepted in
Patients. Twenty patients (12 men and 8 women; mean age 50 years, range 17-80 years) with WG or MP and renal involvement were studied. Patients with bacterial or viral infections requiring antibiotic or antiviral therapy were ex-

PLASMA ELASTASE IN ANCA-ASSOCIATED VASCULITIS 1681
cluded. The diagnoses were made according to the definitions from the Chapel Hill International Consensus Conference (10). Diagnostic criteria for WG were a typical clinical presen- tation with involvement of the upper respiratory tract (as described in the American College of Rheumatology criteria for WG [ll]), together with positive classic ANCA (cANCA) and/or a granulomatous inflammation seen on histologic ex- amination. Diagnostic criteria for MP were a necrotizing pauci-immune vasculitis or glomerulonephritis of the small vessels without granuloma, together with positive perinuclear ANCA (pANCA) or cANCA. Eight patients (7 men and 1 woman; mean age 51 years, range 17-80 years) had WG (7 with cANCA [6 PR3-positive, 1 unknown antigen]; 1 with MPO- positive pANCA) and 12 patients ( 5 men and 7 women; mean age 50 years, range 20-71 years) had MP (10 with pANCA [all MPO-positive]; 2 with PR3-positive cANCA).
All patients were experiencing the first manifestation of the disease. The following organs were involved: kidney 100% (in 16 patients [12 with MP and 4 with WG], kidney biopsy showed a necrotizing pauci-immune glomerulonephri- tis), upper respiratory tract 40% (100% WG, 0% MP), lung 70% (63% WG, 75% MP), eyes 25% (50% WG, 8% MP), nervous system 20% (37.5% WG, 8% MP), intestinal tract 20% (12.5% WG, 25% MP), and skin 10% (25% WG, 0% MP). All patients had constitutional symptoms; 80% (75% WG, 83% MP) had myalgia and/or arthralgia. At diagnosis, creatinine values were 81-1,449 pmolesiliter, with a mean -C SD of 613 -+ 426 pmolesiliter (WG 583 5 435, MP 633 -t 438). Regarding potential a, -antitrypsin deficiency, no patient showed a reduction of a,-globulins on serum electrophoresis. Disease activity was assessed using the Birmingham vasculitis activity score (12), with the following modification: symptoms were recorded if they indicated the presence of active vasculi- tis, and not only, as described originally, if abnormalities were new or worsening. Thirty healthy volunteers served as controls.
Immunosuppressive therapy. With the exception of 1 patient who received cyclophosphamide 0.5 gmim’ 3 times every other week followed by an oral application (2 mg/kg), all patients were treated according to the following protocol: methylprednisolone 0.5 gm intravenously for 3 days, followed by prednisolone 1 mgikg orally, with tapering (reduction of 10 mgiweek) after 14 days; plus either (a) intravenous cyclo- phosphamide 0.75 gmim’ every fourth week (n = 13) (if creatinine clearance was <30 mliminute, intravenous cyclo- phosphamide was first given at 0.5 gmim’, with subsequent administration of 0.75 gm/m2 provided the leukocyte count was >4,0OO/p1) or (b) oral cyclophosphamide 2 mgikgiday (n = 6 ) (if creatinine clearance was <30 mliminute, oral cyclophospha- mide was first given at 1.5 mgkgiday).
Sample collection. Blood 4amples (2 ml anticoagulated [20 mM EDTA and 10 mM benzamidine] and 2 ml without any anticoagulant) were drawn before therapy and 2 weeks and 8-10 weeks after immunosuppressive treatment had been initiated. The samples were centrifuged (10 minutes at 1,700g) within 30 minutes and stored at -70°C until assayed. In addition, blood samples were collected during a relapse (6 patients) or during a rise in ANCA titer not followed by a relapse (6 patients). In patients who were undergoing hemo- dialysis, blood samples were obtained at least 24 hours after the last dialysis procedure.
Measurement of a,-antitrypsin-complexed plasma elastase. Complexed plasma elastase was measured as de- scribed by Neumann et al (13), after adaptation to a Hitachi 704 analyzer using an immunoassay (PMN Elastase immuno- assay; Merck, Darmstadt, Germany). The coefficient of varia- tion was 4% within one day and 4-1096 when comparing different days. The detection limit of the assay is 1 ngiml, and the standard curve is linear up to 320 ngiml.
ANCA determination. ANCA titers were determined using an indirect immunofluorescence technique with ethanol- fixed granulocytes as described by Nolle et a1 (5) . For autoan- tigen determination and quantification, a modified enzyme- linked immunosorbent assay (ELISA) technique described by Ludemann et a1 (14) was used. PR3 (Wieslander, Lund, Sweden) or MPO (Calbiochem Novabiochem, Bad Soden, Germany) were used as antigens, at concentrations of 2.5 pgiml and 1 pgiml, respectively. As a positive control, an aliquoted serum and/or a pooled positive standard serum, both diluted in 1:2 steps, were tested starting at a dilution of 1:1,000 (taken as 80 units) when PR3 was used as the antigen, and at a dilution of 1:2,000 (taken as 80 units) when MPO was used as the antigen. The ELISA values were taken from the optical density values obtained, by means of standard curves. ANCA values more than 2 standard deviations above the mean in 35 healthy volunteers were considered positive (>9 units for MPO-ANCA and >12 units for PR3-ANCA).
C-reactive protein determination. C-reactive protein (CRP) was measured nephelometrically (Behring, Marburg, Germany). The detection limit of the assay was 3-6 mgiliter. The upper limit for normal values was 8 mditer. For statistical analysis, values <6 mg/liter were calculated as 5 rngiliter.
Statistical analysis. Values are shown as the mean 2 SD. Paired values were compared using the Wilcoxon signed rank test, and unpaired values using the Mann-Whitney U test. P values less than 0.05 were considered significant.
RESULTS Patients with first manifestations of the disease.
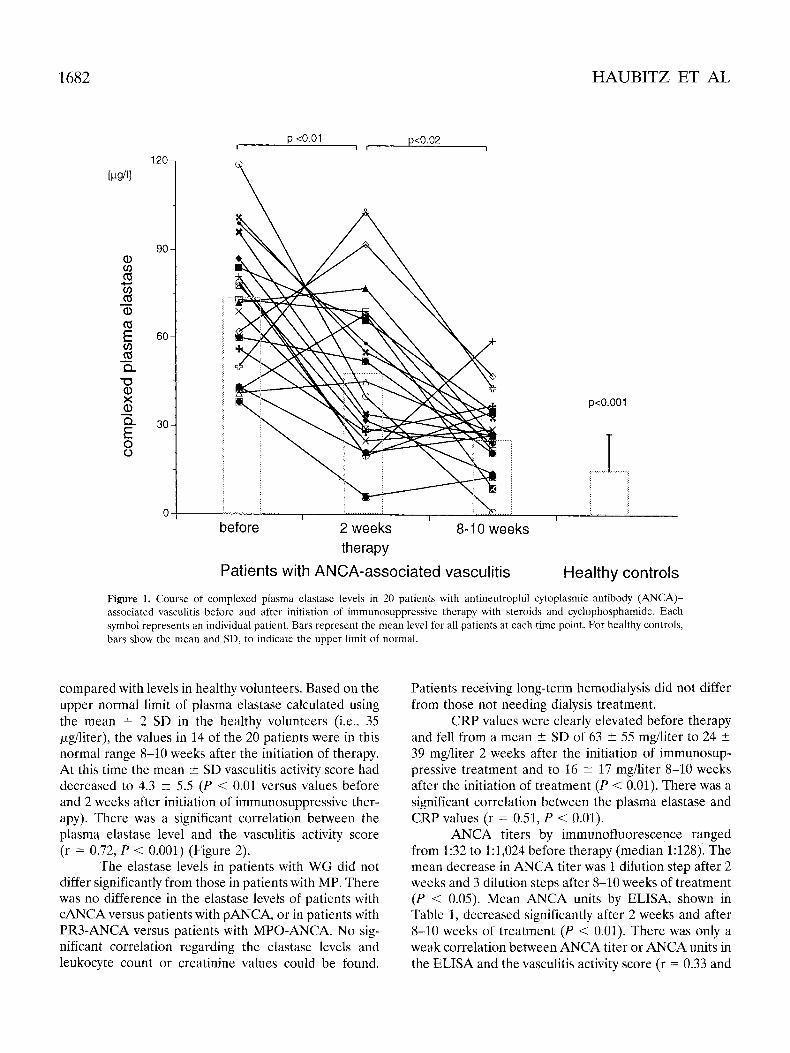
Complexed plasma elastase levels in patients with ANCA-associated vasculitis before immunosuppressive therapy were significantly elevated (mean 5 SD 71.5 t 22.6 pg/liter) compared with those in healthy volunteers (12.2 +- 11.4 pgiliter; P < 0.001) (Figure 1). Two weeks after the initiation of treatment, the values in patients had decreased significantly (46.5 +- 26.8 pg/liter; P < 0.01 compared with baseline), but were still significantly elevated compared with levels in healthy volunteers ( P < 0.001). Clinical symptoms had improved in 17 of the 20 patients, with a decrease in the vasculitis activity score from 25.3 t 6.0 to 14.7 2 5.4 (P < 0.01). Eight to 10 weeks after the initiation of treatment, the patients’ elastase values had further decreased significantly (28.1 ? 13.4 pdliter) compared with those before and 2 weeks after the beginning of immunosuppressive ther- apy (P < 0.02) (Figure I), but were still elevated
1682 HAUBITZ ET AL
p <0.01 p<0.02 I I , 1
p<o.o01
before 2 weeks 8-1 0 weeks therapy
Patients with ANCA-associated vasculitis Healthy controls Figure 1. Course of complexed plasma elastase levels in 20 patients with antineutrophil cytoplasmic antibody (ANCA)- associated vasculitis before and after initiation of immunosuppressive therapy with steroids and cyclophosphamide. Each symbol represents an individual patient. Bars represent the mean level for all patients at each time point. For healthy controls, bars show the mean and SD, to indicate the upper limit of normal.
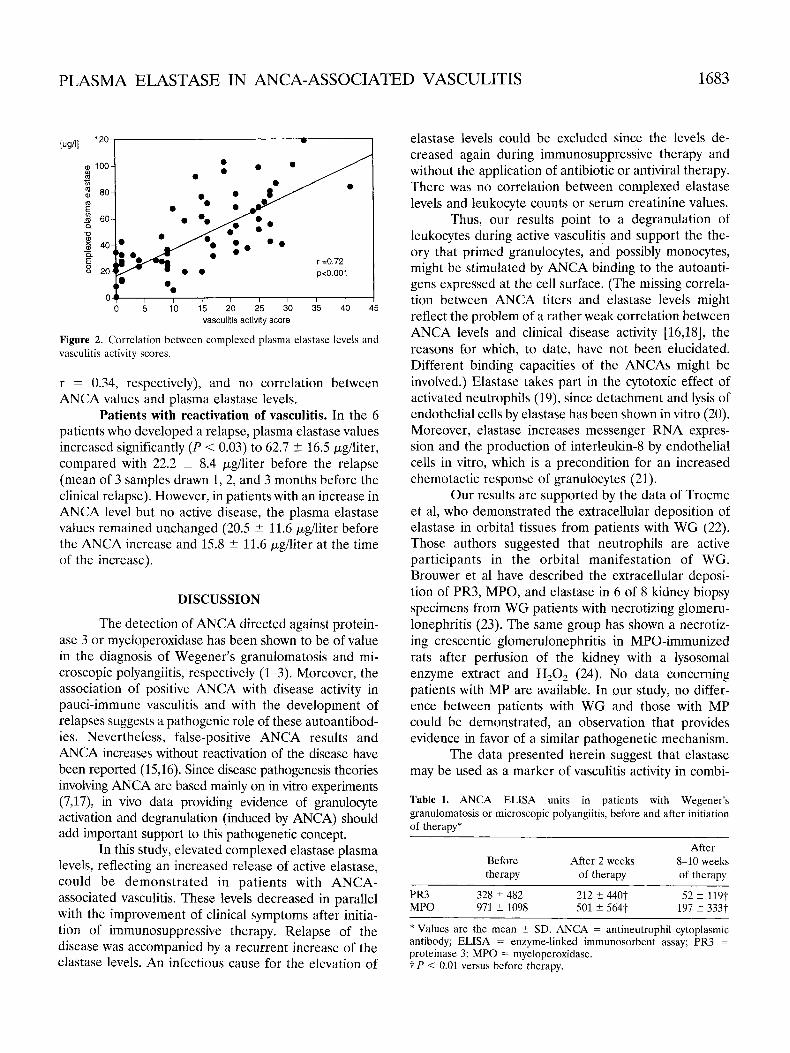
compared with levels in healthy volunteers. Based on the upper normal limit of plasma elastase calculated using the mean + 2 SD in the healthy volunteers (i.e., 3.5 pgiliter), the values in 14 of the 20 patients were in this normal range 8-10 weeks after the initiation of therapy. At this time the mean -+ SD vasculitis activity score had decreased to 4.3 ? 5.5 (P < 0.01 versus values before and 2 weeks after initiation of immunosuppressive ther- apy). There was a significant correlation between the plasma elastase level and the vasculitis activity score (r = 0.72, P < 0.001) (Figure 2).
The elastase levels in patients with WG did not differ significantly from those in patients with MP. There was no difference in the elastase levels of patients with cANCA versus patients with pANCA, or in patients with PR3-ANCA versus patients with MPO-ANCA. No sig- nificant correlation regarding the elastase levels and leukocyte count or creatinine values could be found.
Patients receiving long-term hemodialysis did not differ from those not needing dialysis treatment.
CRP values were clearly elevated before therapy and fell from a mean ? SD of 63 t 55 mg/liter to 24 ? 39 mg/liter 2 weeks after the initiation of immunosup- pressive treatment and to 16 -+ 17 mg/liter 8-10 weeks after the initiation of treatment (P < 0.01). There was a significant correlation between the plasma elastase and CRP values (r = 0.51, P < 0.01).
ANCA titers by immunofluorescence ranged from 1:32 to 1:1,024 before therapy (median 3:128). The mean decrease in ANCA titer was 1 dilution step after 2 weeks and 3 dilution steps after 8-10 weeks of treatment (P < 0.05). Mean ANCA units by ELISA, shown in Table 1, decreased significantly after 2 weeks and after 8-10 weeks of treatment (P < 0.01). There was only a weak correlation between ANCA titer or ANCA units in the ELISA and the vasculitis activity score (r = 0.33 and
PLASMA ELASTASE IN ANCA-ASSOCIATED VASCULITIS 1683
w 1
0 5 10 15 20 25 30 35 40 45 vasculitis activity score
Figure 2. Correlation between complexed plasma elastase levels and vasculitis activity scores.
r = 0.34, respectively), and no correlation between ANCA values and plasma elastase levels.
Patients with reactivation of vasculitis. In the 6 patients who developed a relapse, plasma elastase values increased significantly (P < 0.03) to 62.7 t 16.5 &liter, compared with 22.2 f- 8.4 pghter before the relapse (mean of 3 samples drawn 1,2, and 3 months before the clinical relapse). However, in patients with an increase in ANCA level but no active disease, the plasma elastase values remained unchanged (20.5 f- 11.6 pg/liter before the ANCA increase and 15.8 ? 11.6 pd i t e r at the time of the increase).
DISCUSSION
The detection of ANCA directed against protein- ase 3 or myeloperoxidase has been shown to be of value in the diagnosis of Wegener’s granulomatosis and mi- croscopic polyangiitis, respectively (1-3). Moreover, the association of positive ANCA with disease activity in pauci-immune vasculitis and with the development of relapses suggests a pathogenic role of these autoantibod- ies. Nevertheless, false-positive ANCA results and ANCA increases without reactivation of the disease have been reported (1 5,16). Since disease pathogenesis theories involving ANCA are based mainly on in vitro experiments (7,17), in vivo data providing evidence of granulocyte activation and degranulation (induced by ANCA) should add important support to this pathogenetic concept.
In this study, elevated complexed elastase plasma levels, reflecting an increased release of active elastase, could be demonstrated in patients with ANCA- associated vasculitis. These levels decreased in parallel with the improvement of clinical symptoms after initia- tion of immunosuppressive therapy. Relapse of the disease was accompanied by a recurrent increase of the elastase levels. An infectious cause for the elevation of
elastase levels could be excluded since the levels de- creased again during immunosuppressive therapy and without the application of antibiotic or antiviral therapy. There was no correlation between complexed elastase levels and leukocyte counts or serum creatinine values.
Thus, our results point to a degranulation of leukocytes during active vasculitis and support the the- ory that primed granulocytes, and possibly monocytes, might be stimulated by ANCA binding to the autoanti- gens expressed at the cell surface. (The missing correla- tion between ANCA titers and elastase levels might reflect the problem of a rather weak correlation between ANCA levels and clinical disease activity [16,18], the reasons for which, to date, have not been elucidated. Different binding capacities of the ANCAs might be involved.) Elastase takes part in the cytotoxic effect of activated neutrophils (19), since detachment and lysis of endothelial cells by elastase has been shown in vitro (20). Moreover, elastase increases messenger RNA expres- sion and the production of interleukin-8 by endothelial cells in vitro, which is a precondition for an increased chemotactic response of granulocytes (21).
Our results are supported by the data of Trocme et al, who demonstrated the extracellular deposition of elastase in orbital tissues from patients with WG (22). Those authors suggested that neutrophils are active participants in the orbital manifestation of WG. Brouwer et a1 have described the extracellular deposi- tion of PR3, MPO, and elastase in 6 of 8 kidney biopsy specimens from WG patients with necrotizing glomeru- lonephritis (23). The same group has shown a necrotiz- ing crescentic glomerulonephritis in MPO-immunized rats after perfusion of the kidney with a lysosomal enzyme extract and H,O, (24). No data concerning patients with MP are available. In our study, no differ- ence between patients with WG and those with MP could be demonstrated, an observation that provides evidence in favor of a similar pathogenetic mechanism.
The data presented herein suggest that elastase may be used as a marker of vasculitis activity in combi-
Table 1. ANCA ELISA units in patients with Wegener’s granulomatosis or microscopic polyangiitis, before and after initiation of therapy*
After After 2 weeks 8-10 weeks Before
therapy of therapy of therapy
MPO 971 2 1098 501 t 5647 197 5 333t PR3 328 5 482 212 ? 4407 52 -c 11Yt
* Values are the mean 2 SD. ANCA = antineutrophil cytoplasmic antibody; ELISA = enzyme-linked immunosorbent assay; PR3 = proteinase 3; MPO = myeloperoxidase. t P < 0.01 versus before therapy.
1684 HAUBITZ ET AL
nation with ANCA titers, since there is a strong corre- lation between plasma elastase levels and clinical disease activity. This may be helpful in differentiating “false” ANCA rises from “clinically relevant” ANCA rises with vasculitic activity. However, concomitant infectious complications have to be excluded, since they would lead to increased elastase levels as well. Furthermore, it must be kept in mind that increased elastase levels do not represent a specific diagnostic marker for ANCA- associated vasculitis, since elevated levels have previ- ously been found in other inflammatory or infectious diseases such as pancreatitis, inflammatory bowel dis- ease, rheumatoid arthritis, and sepsis (25-28).
In conclusion, increased complexed plasma elas- tase levels are present in patients with ANCA-associated vasculitis and active disease. Since elastase is liberated during granulocyte degranulation, our findings sup- port the notion that granulocyte activation is an important factor in the pathogenesis of ANCA-associated vasculitis.
REFERENCES 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Van der Woude FJ, Rasmussen N, Lobatto S, Wilk A, Permin H, van Es LA, van der Giessen M, van der Hem GK, The TH: Autoantibodies against neutrophils and monocytes: tool for diag- nosis and marker of disease activity in Wegener’s granulomatosis. Lancet 1:425-429, 1985 Falk RJ, Jennette JC: Anti-neutrophil cytoplasmic autoantibodies with specificity for myeloperoxidase in patients with systemic vasculitis and idiopathic necrotizing and crescentic glomerulone- phritis. N Engl J Med 318:1651-1657, 1988 Gross WL, Schmitt WH, Csernok E: ANCA and associated diseases: immunodiagnostic and pathogenetic aspects. Clin Exp Irnmunol91:1-12, 1993 Cohen Tervaert JW, van der Woude FJ, Fauci AS, Ambrus JL, Velosa J, Keane WF, Meijer S, van der Giessen M, van der Hem GK, The TH, Vallenberg GM: Association between active Wege- ner’s granulomatosis and anticytoplasmic antibodies. Arch Intern Med 149:2461-2465, 1989 Nolle B, Specks U, Ludemann J, Rohrbach MS, DeRemee RA, Gross WL: Anticytoplasmic autoantibodies: their immunodiagnostic value in Wegener’s granulomatosis. Ann Intern Med 111:28-40,1989 Csernok E, Ernst M, Schmitt W, Bainton DF, Gross WL: Acti- vated neutrophils express proteinase 3 on their plasma membrane in vitro and in vivo. Clin Exp Immunol 95:244-250, 1994 Falk RJ, Terrell RS, Charles LA, Jennette JC: Anti-neutrophil cytoplasmic autoantibodies induce neutrophils to degranulate and produce oxygen radicals in vitro. Proc Natl Acad Sci U S A
Ohlsson K, Ohlsson I: The extracellular release of granulocyte collagenase and elastase during phagocytosis and inflammatory processes. Scand J Haematol 19:145-152, 1977 Kargi HA, Campbell EJ, Kuhn C: Elastase and cathepsin G of human monocytes: heterogeneity and subcellular localization to peroxidase-positive granules. J Histochem Cytochem 38:1179- 1186, 1990 Jennette JC, Falk RJ, Andrassy K; Bacon PA, Churg J, Gross WL, Hagen EC, Hoffman GS, Hunder GG, Kallenberg CGB, McClus- key RT, Sinico RA, Rees AJ, van Es LA, Waldherr R, Wiik A. Nomenclature of systemic vasculitides: proposal of an interna- tional consensus conference. Arthritis Rheum 37:187-192, 1994
8714115-4119, 1990
11. Leavitt RY, Fauci AS, Bloch DA, Michel BA, Hunder GG, Arend WP, Calabrese LH, Fries JF, Lie JT, Lightfoot RW Jr, Masi AT, McShane DJ, Mills JA, Stevens MB, Wallace SL, Zvaifler NJ: The American College of Rheumatology 1990 criteria for the classifi- cation of Wegener’s granulomatosis. Arthritis Rheum 33:1101- 1107, 1990
12. Luqmani RA, Bacon PA, Moots RJ, Janssen BA, Pall A, Emery P, Savage C, Adu D: Birmingham Vasculitis Activity Score (BVAS) in systemic necrotizing vasculitis. QJM 87:671-678, 1994
13. Neumann S, Gunzer G, Hennrich N, Lang H: “PMN elastase assay”: enzyme immunoassay for human polymorphonuclear elas- tase complexed with oil-proteinase inhibitor. J Clin Chem Bio- chem 22:693-697, 1984
14. Ludemann J, Utecht B, Gross WL: Detection and quantitation of anti-neutrophil cytoplasmic antibodies in Wegener’s granulomato- sis by ELISA using affinity-purified antigen. J Immunol Methods
15. Koderisch J, Andrassy K, Rassmussen N, Hartmann M, Tilgen W: “False positive” anti-neutrophil cytoplasmic antibodies in HIV infection. Lancet 335: 1227-1228, 1990
16. Kerr GS, Fleisher TA, Hallahan CW, Leavitt RY, Fauci AS, Hoffman GS: Limited prognostic value of changes in antineutro- phi1 cytoplasmic antibody titer in patients with Wegener’s granu- lomatosis. Arthritis Rheum 36:365-371, 1993
17. Savage CO, Pottinger BE, Gaskin G, Pusey CD, Pearson JD: Autoantibodies developing to myeloperoxidase and proteinase 3 in systemic vasculitis stimulate neutrophil cytotoxicity toward cul- tured endothelial cells. Am J Pathol 141:335-342, 1992
18. Gordon M, Luqmani RA, Adu D, Greaves I, Richards N, Michael J, Emery P, Howie AJ, Bacon, PA: Relapses in patients with a systemic vasculitis. QJM 86:779-789, 1993
19. Phan SH, Gannon DE, Ward PA, Karmiol S: Mechanism of neutrophil-induced xanthine dehydrogenase to xanthin oxidase conversion in endothelial cells: evidence of a role for elastase. Am J Respir Cell Mol Biol 6:270-278, 1992
20. Ballieux BE, Hiemstra PS, Klar MN, Hagan EC, van Es LA, van der Woude F, Daha MR: Detachment and cytolysis of human endothelid cells by proteinase 3. Eur J Immunol24:3211-3215, 1994
21. Berger SP, Seelen MAJ, Hiemstra PS, Heemskerk E, van der Woude FJ, Daha MR: The neutrophil enzymes proteinase 3 and elastase enhance the production of IL-8 by endothelial cells in culture. J Am Soc Nephrol 7594-701, 1996
22. Trocme SD, Bartley GB, Campbell RJ, Gleich GJ, Leiferman KM: Eosinophil and neutrophil degranulation in ophthalmic lesions of Wegener’s granulomatosis. Arch Ophthalmol109:1585-1589,1991
23. Brouwer E, Huitema MG, Mulder AH, Heeringa P, van Goor H, Tervaert, JWC, Weening JJ, Kallenberg CGM: Neutrophil activa- tion in vitro and in vivo in Wegener’s granulomatosis. Kidney Int 45:1120-1131, 1994
24. Brouwer E, Huitema MG, Klok PA, de Weerd H, Tervaert JWC, Weening JJ, Kallenberg CGM: Antimyeloperoxidase-associated proliferative glomerulonephritis: an animal model. J Exp Med
25. Lasson A, Balldin G, Ohlsson K: Leucocyte elastase oil-proteinase inhibitor complexes may diagnose pancreatic abscesses early. Scand J Clin Lab Invest 21:220-221, 1986
26. Adeyemi EO, Neumann S, Chadwick VS, Hodgson HJF, Pepys MB: Circulating human elastase in patients with inflammatory diseases. Gut 26:1300-1306, 1985
27. Kuramitsu K, Yoshida A Plasma and synovial fluid levels of granulocytal elastase-alpha-1-protease inhibitor complex in pa- tients with rheumatoid arthritis. Rheumatol Tnt 10:51-56, 1990
28. Nuijens JH, Abbink JJ, Wachtfogel YT, Colman RW, Eermberg A, Dors D, Kamp AJ, Strackvan Schiindel RJ, Thus LG, Hack CE: Plasma elastase oil-antitrypsin and lactoferrin in sepsis: evidence for neutrophils as mediators in fatal sepsis. J Lab Clin Med
114:167-174, 1988
177:905-914, 1993
119:159-168, 1992