complex interventions to improve the health of people with limited literacy: a systematic review
TRANSCRIPT

Patient Education and Counseling 75 (2009) 340–351
Complex interventions to improve the health of people with limited literacy:A systematic review
Sarah Clement a,*, Saima Ibrahim b, Nicola Crichton b, Michael Wolf c, Gillian Rowlands b
a Health Service and Population Research Department (PO29), David Goldberg Centre, Institute of Psychiatry, London, UKb Institute of Primary Care and Public Health, Faculty of Health and Social Care, London South Bank University, London, UKc Institute for Healthcare Studies, Division of General Internal Medicine, Feinberg School of Medicine, Northwestern University, Chicago, USA
A R T I C L E I N F O
Article history:
Received 2 October 2008
Received in revised form 23 December 2008
Accepted 8 January 2009
Keywords:
Literacy
Numeracy
Complex interventions
Systematic review
Health literacy
A B S T R A C T
Objective: To evaluate the published literature on the effects of complex (multi-faceted) interventions
intended to improve the health-related outcomes of individuals with limited literacy or numeracy.
Methods: We undertook a systematic review of randomized and quasi-randomized controlled trials with
a narrative synthesis. The search strategy included searching eight databases from start date to 2007,
reference checking and contacting expert informants. After the initial screen, two reviewers
independently assessed eligibility, extracted data and evaluated study quality.
Results: The searches yielded 2734 non-duplicate items, which were reduced to 15 trials. Two
interventions were directed at health professionals, one intervention was literacy education, and 12
were health education/management interventions. The quality of the trials was mixed, 13/15 trials were
conducted in North America, and all focused on literacy rather than numeracy. 13/15 trials reported at
least one significant difference in primary outcome, all favoring the intervention group. Only 8/15 trials
measured direct clinical outcomes. Knowledge and self-efficacy were the class of outcome most likely to
improve.
Conclusion: A wide variety of complex interventions for adults with limited literacy are able to improve
some health-related outcomes.
Practice implications: This review supports the wider introduction of interventions for people with
limited literacy, particularly within an evaluation context.
� 2009 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at ScienceDirect
Patient Education and Counseling
journa l homepage: www.e lsev ier .com/ locate /pateducou
1. Introduction
Health literacy has been a focus for attention in North Americasince the 1990s and is now listed as one of the four key priorities inpublic health in the US [1]. More recently it has become recognizedas a health issue in Europe and elsewhere. For example, work hasbegun to appear in the British medical literature highlighting howhealth literacy is central to involving patients in their care and toreducing health inequalities [2]. Health literacy is a broad andcomplex concept, which has been defined in a number of waysincluding ‘‘the capacity to obtain, process and understand basichealth information and services needed to make appropriatehealth decisions’’ [3], ‘‘the cognitive and social skills whichdetermine the motivation and ability of individuals to gain accessto, understand and use information in ways which promote andmaintain good health’’ [4], and as ‘‘a critical empowerment
* Corresponding author at: Health Service and Population Research Department
(PO29), David Goldberg Centre, Institute of Psychiatry, King’s College London, De
Crespigny Park, London SE5 8AF, UK. Tel.: +44 20 7848 0739; fax: +44 20 7277 1462.
E-mail address: [email protected] (S. Clement).
0738-3991/$ – see front matter � 2009 Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.pec.2009.01.008
strategy to increase people’s control over their health, their abilityto seek out information and their ability to take responsibility’’ [5].
Literacy skills and numeracy skills are two key components ofthis wider concept of health literacy [6], and are the focus of thepresent review. One study has defined the reading element ofliteracy as the ability to understand texts and to obtain informationfrom different sources including signs and symbols [7], but a widerperspective would also include writing. Numeracy skills refer tothe ability to understand and use numerical, graphical andmathematical information [7]. A national survey of the literacyand numeracy skills of working age adults in England found that16% had limited literacy and 47% had limited numeracy [7]. Thereis no one agreed definition of what constitutes limited literacy, andour use of this term should simply be taken to mean having feweror lower literacy or numeracy skills than other people. Althoughliteracy levels are associated with education, ethnicity and age [8] anumber of studies have shown that having limited literacy ornumeracy skills acts as an independent risk factor for poor health[9–11], through medication errors [12,13] and poorer under-standing of disease and treatments [12]. A recent systematicreview of the relationship between literacy and health outcomes

S. Clement et al. / Patient Education and Counseling 75 (2009) 340–351 341
concluded that limited literacy is related to several adverse health-related variables, including knowledge about health and healthcare, hospitalization, global measures of health and some chronicdiseases [14]. Qualitative research has demonstrated the shameand practical difficulties that patients with limited literacy canexperience when interacting with the health care system, as wellas the coping strategies they employ to circumvent these [15,16].These findings have intensified the growing international recogni-tion of this highly prevalent problem and the need for action.
To date, researchers and practitioners have used a number ofapproaches to attempt to lessen the impact of limited literacy ornumeracy on health outcomes. Some of these strategies can betermed simple interventions, such as the use of simplified writtenlanguage, pictorial material, and audio/audio–visual resources.Other strategies are classified as complex interventions. A complexintervention is defined as one that ‘‘comprises of a number ofseparate elements which seem essential to the proper functioning ofthe intervention although the ‘‘active ingredient’’ of the interventionthat is effective is difficult to specify . . . The components will usuallyinclude behaviors, parameters of behaviors (e.g. frequency, timing),and methods of organizing and delivering those behaviors (e.g. typeof practitioner, setting) . . . [and] may be at the level of individualpatient care, . . . organizational or service modification’’ [17]. Acomplex interventions to improve the health of people with limitedliteracy or numeracy might, for example, provide health educationthrough a combination of verbal presentation, pictorial materialsand checking for understanding, or might have one primary elementthat is in itself multi-component or involves human interaction,such as literacy education. By contrast, examples of simpleinterventions in this field include the sole use of a pamphlet writtenin simplified language or the sole use of a DVD. Existing evidence hasdemonstrated that simple interventions responding to limitedliteracy, such as the use of audiotapes, have been met with variablesuccess with no consistent findings regarding whether thisintervention increases knowledge, produces behavior change orreduces distress [18]. We postulate that complex interventions arelikely to be needed to effectively tackle the complex health-relatedneeds of people with limited literacy or numeracy, a view which canalso be inferred from the work of others [2,19].
To our knowledge, no existing systematic review has beenconducted specifically focusing on complex interventions toimprove the health of people with limited literacy or numeracy.Coulter and Ellins [2,20] conducted a policy overview rather than asystematic review, and only a small part of the work examinedliteracy. One systematic review focused on one type of simpleintervention, namely audiotapes [18]. Pignone et al. [21] havesystematically reviewed a mix of interventions, the majority(n = 15) being simple and the minority (n = 5) complex. Theirreview was restricted to studies published in English, fromdeveloped countries, and those where a formal assessment ofliteracy had been made. Furthermore, only studies publishedbetween 1980 and 2003 were considered, and as health literacyresearch is a vastly expanding field, a significant number of studieswill have been published since 2003.
The aim of our review was to evaluate the published literatureon the effects of complex interventions intended to improve thehealth-related outcomes of people with limited literacy ornumeracy.
2. Methods
2.1. Search strategy
Eight electronic databases were searched: Medline (1966–);Cumulative Index to Nursing & Allied Health Literature (CINAHL,1982–); Cochrane Central Register of Controlled Trials (CENTRAL,
1800–); PsycINFO (1887–); SCOPUS database (1966–); BritishEducation Index (1975–); Educational Resources InformationCenter (ERIC, 1966–), and Australian Education Index (1979–).Searches were undertaken in March and April 2007 and eachdatabase was searched from its earliest date. No languagerestrictions were used. The search strategy for Medline usedsubject heading and textword searching, combining terms asfollows ($ indicates truncation): ((literacy-related terms, e.g.reading/, literac$) OR (numeracy-related terms, e.g. mathe-matics/, numera$) OR (educational terms, e.g. educationalstatus/)) AND (the set of terms for identifying clinical trials fromthe Cochrane Handbook [22]). The searches for the other databaseswere based on the Medline search strategy, but for the non-healthdatabases a set of health terms (e.g. health/, disorder$, patient$,nurs$) were added to limit the studies to those with relevance tohealth. Full details of the electronic searches are available as anelectronic supplementary file to this paper.
The reference lists of all studies included in our review, and ofother relevant reviews [20,21] were inspected to identify furtherpossible studies. Three groups of expert informants werecontacted: the authors of all of the included studies; researchersknown to be working in the field of health literacy; and the leads ofongoing studies in the area identified through searches on theNational Research Register, the Health Services Research Projectsin Progress database, and the Cochrane Central Register ofControlled Trials. The 78 expert informants were asked to identifyany published studies likely to meet the inclusion criteria that hadnot yet been included in the review.
2.2. Selection of studies
The titles and abstracts of the studies yielded by the searchwere screened to exclude those that clearly did not meet theinclusion criteria. Initially, 150 studies were independentlyscreened by two researchers (SI and SC) then discussed to aidreliability, with the remaining studies being screened by oneresearcher (SI). Full papers were obtained for papers not screenedout. Two researchers (SI and SC) independently assessed thesepapers against the inclusion criteria, with any differences ininclusion decisions being resolved via discussion, with a thirdresearcher (GR) acting as arbiter.
The inclusion criteria are shown in Table 1, and aimed to selectpublished papers reporting randomized controlled trials (RCTs) orquasi-randomized controlled trials of complex interventionsintended to improve outcomes for people with limited literacyor numeracy, which included at least one health-related outcome.
2.3. Data extraction, quality assessment and synthesis
Data on study characteristics, study quality and findings wereextracted independently by two researchers (SI and SC) fromunmasked publications. Any discrepancies were resolved viadiscussion and arbitration with GR and MW, and statistical issuesresolved with statistician NC.
The quality of the studies was assessed using the Delphi List[23], which we modified by deleting the two criteria relating toblinding of patients and professionals (as these are rarely possiblein the types of intervention reviewed here), and replacing themwith two criteria from the CONSORT statement [24], namelyinclusion of an a priori sample size calculation and of a participantflow diagram.
Statistical aggregation of findings was deemed inappropriategiven the variety of different measures of outcome used and therange of time periods to follow-up. Consequently a narrativeanalysis was undertaken with findings presented in tabular form,with supplementary data in the text. The synthesis covered both
Table 1Inclusion criteria.
Data type Primary research, quantitative data
Participants Adults (including adults consulting on behalf of dependents,
and professionals who may be the target of an intervention,
all participants on whom outcomes are reported must
be adult)
Setting Any
Health condition Any or none
Intervention � Complex intervention (more than one element) AND
intended to improve outcomes for people with limited
literacy/numeracy, evidenced by either:
� mention of literacy or numeracy in the description of
the population or
� mention of literacy or numeracy in the description of
the intervention
Comparator Any (active or inactive control)
Outcomes At least one of the following health-related outcomes
measured:
� Clinical outcomes (physical or psychological)
� Health knowledge
� Health behaviors
� Self-reported health status/quality of life
� Self-efficacy/confidence in relation to health/health
behavior
� Utilization of health care
� Health professional behavior
Study types � Randomized controlled trials
� Quasi-randomized controlled trials
Dissemination
type
Published journal paper
Fig. 1. Selection of studies for systematic review.
S. Clement et al. / Patient Education and Counseling 75 (2009) 340–351342
overall study populations and subgroup analyses performed ondata from participants with limited literacy/numeracy where thelatter has been reported by the study authors. We have restrictedour reporting of the effectiveness of the interventions at the finalfollow-up point and focused on outcomes defined by the trialists asprimary, although summary data are also presented on secondaryoutcomes. We were unable to report test-values to accompany p
values where these were missing from the original papers.
3. Results
3.1. Search results
The searches yielded 2734 non-duplicate items, which werereduced to 17 papers [25–41] reporting 15 trials, as described bythe flow diagram in Fig. 1. Eleven expert informants replied to therequest for additional studies, suggesting 46 studies, of which 10had already been screened out and 36 had not been previouslyidentified but were screened out or excluded as they did not meetinclusion criteria. References for all excluded studies are availablefrom the corresponding author.
3.2. Trial characteristics and study designs
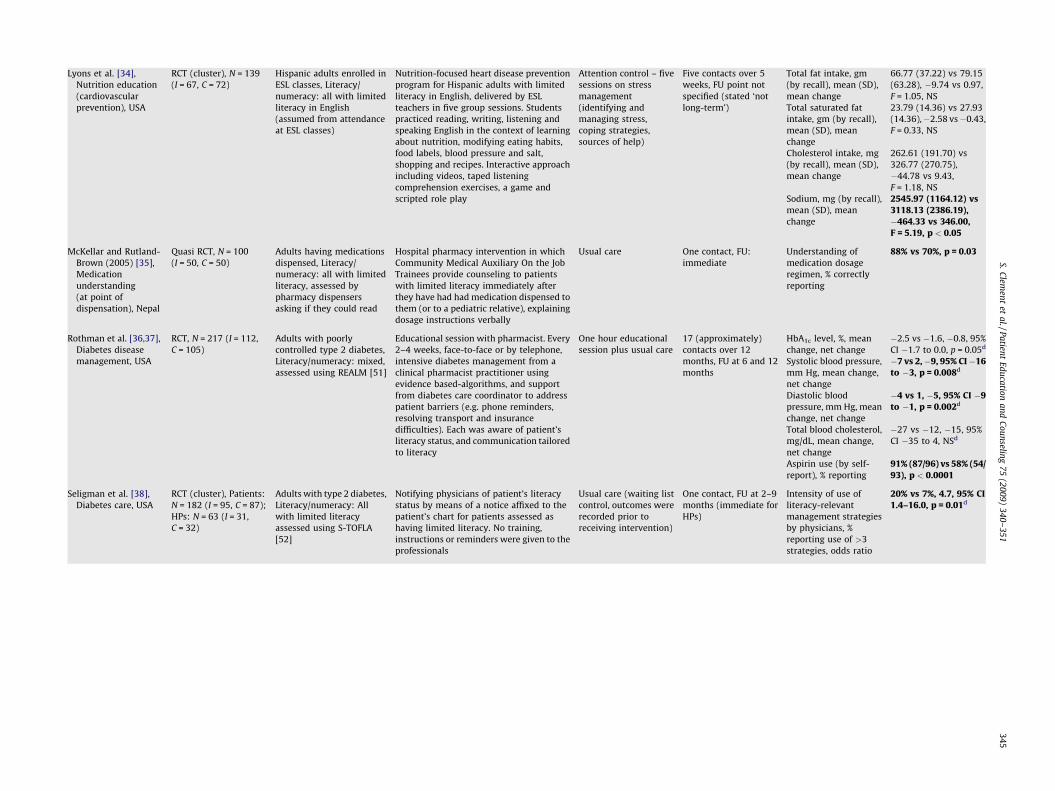
The trial characteristics, primary outcome(s) measured andresults for these primary outcomes are shown in Table 2.
Eleven of the studies were RCTs, the remaining four[25,28,32,35] being quasi-randomized trials, using alternation toallocate to groups. All were two-arm parallel-groups trials, and fivehad cluster designs [28,30,31,34,38]. Sample sizes ranged from 40to 2046 (median 160.5). In nine studies outcomes were measuredduring or immediately after the intervention [25,26,29,30,33,35–37,39–41], in one [34] duration of follow-up was unspecified, andin the remaining five the duration of post-intervention follow-upranged from 1 week [31] to 10.5 months [29] median 5.5 months.
3.3. Settings and populations
All but two [25,35] of the studies were conducted in the USA.Recruitment and interventions took place in outpatient settings infive of the studies [27,28,32,38–40]; in community settings inthree studies [30,31,34]; in three studies participants wererecruited in outpatients with the intervention being by telephoneand/or mail [26,29,36,37]; one study [25] took place in a maternityunit; one [35] took place in a hospital pharmacy; one recruited inthe community and provided the intervention in an outpatientsetting [33]; and one [41] did the converse.
The health issues that were studied included new born hearingscreening [25], hypertension [26], heart failure [27], colorectalcancer screening [28], nutrition education for cancer [29] andcardiovascular disease [30,31,33,34] prevention, medication adher-ence in chronic health conditions [32], general medication under-standing [35], diabetes disease management [36–38], HIVmedication adherence and knowledge [39,40], and depression [41].
Four studies [34,35,38,41] were restricted to individuals withlimited literacy/numeracy, the remainder having samples withmixed levels. The literacy levels of the study populations wereassessed in 11 trials [26–28,30,31,33,35–41] using a wide varietyof measures and cut-offs. The measures all focused primarily onreading ability rather than numeracy, although three studies usedmeasures with numeracy-relevant elements such as interpretingdosage information [27,38–40].
3.4. Interventions
The interventions are briefly described in Table 2, and fell intothree main categories: two were directed at health professionals[28,38], one was a literacy education intervention [41], and theremainder were health education/management interventions. Theinterventions differed widely on a number of dimensions such asthe extent to which they had been developed with limited literacy
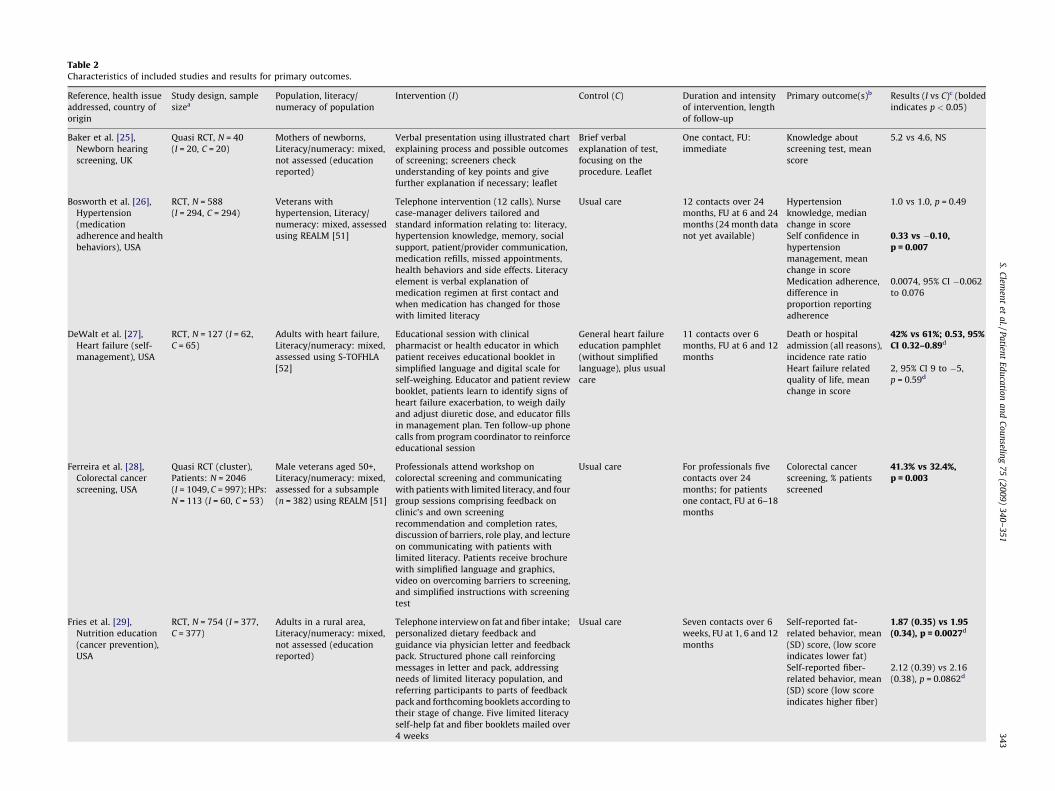
Table 2Characteristics of included studies and results for primary outcomes.
Reference, health issue
addressed, country of
origin
Study design, sample
sizea
Population, literacy/
numeracy of population
Intervention (I) Control (C) Duration and intensity
of intervention, length
of follow-up
Primary outcome(s)b Results (I vs C)c (bolded
indicates p < 0.05)
Baker et al. [25],
Newborn hearing
screening, UK
Quasi RCT, N = 40
(I = 20, C = 20)
Mothers of newborns,
Literacy/numeracy: mixed,
not assessed (education
reported)
Verbal presentation using illustrated chart
explaining process and possible outcomes
of screening; screeners check
understanding of key points and give
further explanation if necessary; leaflet
Brief verbal
explanation of test,
focusing on the
procedure. Leaflet
One contact, FU:
immediate
Knowledge about
screening test, mean
score
5.2 vs 4.6, NS
Bosworth et al. [26],
Hypertension
(medication
adherence and health
behaviors), USA
RCT, N = 588
(I = 294, C = 294)
Veterans with
hypertension, Literacy/
numeracy: mixed, assessed
using REALM [51]
Telephone intervention (12 calls). Nurse
case-manager delivers tailored and
standard information relating to: literacy,
hypertension knowledge, memory, social
support, patient/provider communication,
medication refills, missed appointments,
health behaviors and side effects. Literacy
element is verbal explanation of
medication regimen at first contact and
when medication has changed for those
with limited literacy
Usual care 12 contacts over 24
months, FU at 6 and 24
months (24 month data
not yet available)
Hypertension
knowledge, median
change in score
1.0 vs 1.0, p = 0.49
Self confidence in
hypertension
management, mean
change in score
0.33 vs �0.10,p = 0.007
Medication adherence,
difference in
proportion reporting
adherence
0.0074, 95% CI �0.062
to 0.076
DeWalt et al. [27],
Heart failure (self-
management), USA
RCT, N = 127 (I = 62,
C = 65)
Adults with heart failure,
Literacy/numeracy: mixed,
assessed using S-TOFHLA
[52]
Educational session with clinical
pharmacist or health educator in which
patient receives educational booklet in
simplified language and digital scale for
self-weighing. Educator and patient review
booklet, patients learn to identify signs of
heart failure exacerbation, to weigh daily
and adjust diuretic dose, and educator fills
in management plan. Ten follow-up phone
calls from program coordinator to reinforce
educational session
General heart failure
education pamphlet
(without simplified
language), plus usual
care
11 contacts over 6
months, FU at 6 and 12
months
Death or hospital
admission (all reasons),
incidence rate ratio
42% vs 61%; 0.53, 95%CI 0.32–0.89d
Heart failure related
quality of life, mean
change in score
2, 95% CI 9 to �5,
p = 0.59d
Ferreira et al. [28],
Colorectal cancer
screening, USA
Quasi RCT (cluster),
Patients: N = 2046
(I = 1049, C = 997); HPs:
N = 113 (I = 60, C = 53)
Male veterans aged 50+,
Literacy/numeracy: mixed,
assessed for a subsample
(n = 382) using REALM [51]
Professionals attend workshop on
colorectal screening and communicating
with patients with limited literacy, and four
group sessions comprising feedback on
clinic’s and own screening
recommendation and completion rates,
discussion of barriers, role play, and lecture
on communicating with patients with
limited literacy. Patients receive brochure
with simplified language and graphics,
video on overcoming barriers to screening,
and simplified instructions with screening
test
Usual care For professionals five
contacts over 24
months; for patients
one contact, FU at 6–18
months
Colorectal cancer
screening, % patients
screened
41.3% vs 32.4%,p = 0.003
Fries et al. [29],
Nutrition education
(cancer prevention),
USA
RCT, N = 754 (I = 377,
C = 377)
Adults in a rural area,
Literacy/numeracy: mixed,
not assessed (education
reported)
Telephone interview on fat and fiber intake;
personalized dietary feedback and
guidance via physician letter and feedback
pack. Structured phone call reinforcing
messages in letter and pack, addressing
needs of limited literacy population, and
referring participants to parts of feedback
pack and forthcoming booklets according to
their stage of change. Five limited literacy
self-help fat and fiber booklets mailed over
4 weeks
Usual care Seven contacts over 6
weeks, FU at 1, 6 and 12
months
Self-reported fat-
related behavior, mean
(SD) score, (low score
indicates lower fat)
1.87 (0.35) vs 1.95(0.34), p = 0.0027d
Self-reported fiber-
related behavior, mean
(SD) score (low score
indicates higher fiber)
2.12 (0.39) vs 2.16
(0.38), p = 0.0862d
S.C
lemen
tet
al./P
atien
tE
du
catio
na
nd
Co
un
seling
75
(20
09
)3
40
–3
51
34
3
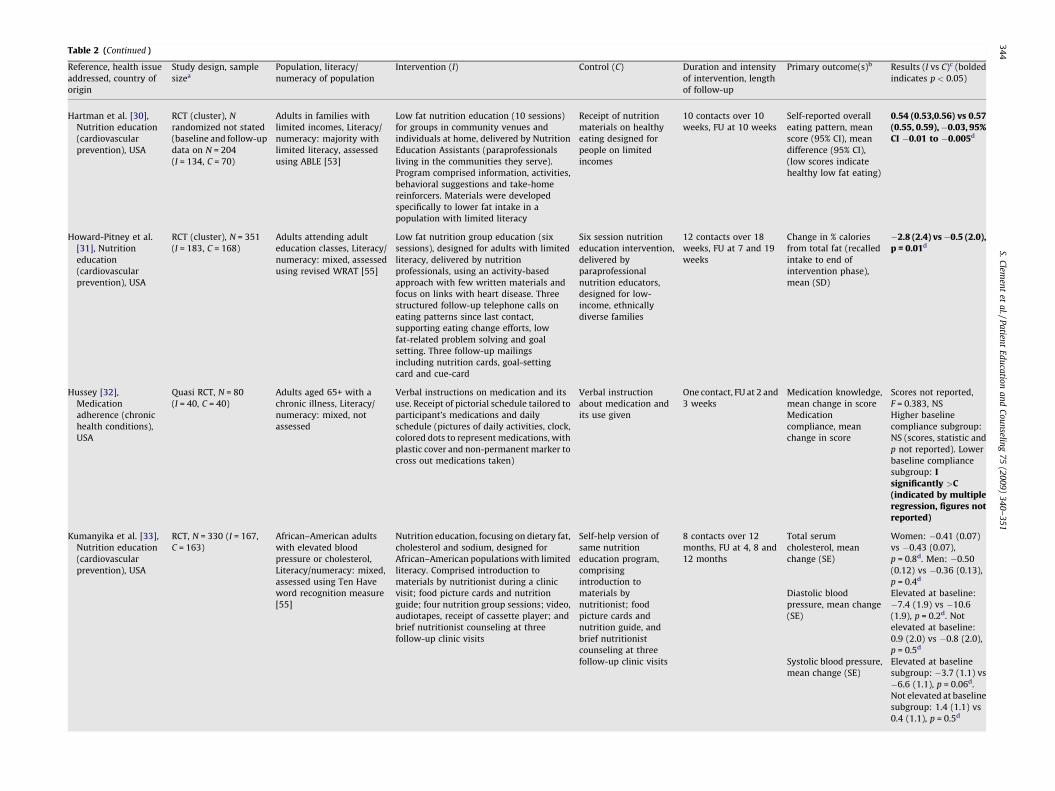
Table 2 (Continued )
Reference, health issue
addressed, country of
origin
Study design, sample
sizea
Population, literacy/
numeracy of population
Intervention (I) Control (C) Duration and intensity
of intervention, length
of follow-up
Primary outcome(s)b Results (I vs C)c (bolded
indicates p < 0.05)
Hartman et al. [30],
Nutrition education
(cardiovascular
prevention), USA
RCT (cluster), N
randomized not stated
(baseline and follow-up
data on N = 204
(I = 134, C = 70)
Adults in families with
limited incomes, Literacy/
numeracy: majority with
limited literacy, assessed
using ABLE [53]
Low fat nutrition education (10 sessions)
for groups in community venues and
individuals at home, delivered by Nutrition
Education Assistants (paraprofessionals
living in the communities they serve).
Program comprised information, activities,
behavioral suggestions and take-home
reinforcers. Materials were developed
specifically to lower fat intake in a
population with limited literacy
Receipt of nutrition
materials on healthy
eating designed for
people on limited
incomes
10 contacts over 10
weeks, FU at 10 weeks
Self-reported overall
eating pattern, mean
score (95% CI), mean
difference (95% CI),
(low scores indicate
healthy low fat eating)
0.54 (0.53,0.56) vs 0.57(0.55, 0.59),�0.03, 95%CI �0.01 to �0.005d
Howard-Pitney et al.
[31], Nutrition
education
(cardiovascular
prevention), USA
RCT (cluster), N = 351
(I = 183, C = 168)
Adults attending adult
education classes, Literacy/
numeracy: mixed, assessed
using revised WRAT [55]
Low fat nutrition group education (six
sessions), designed for adults with limited
literacy, delivered by nutrition
professionals, using an activity-based
approach with few written materials and
focus on links with heart disease. Three
structured follow-up telephone calls on
eating patterns since last contact,
supporting eating change efforts, low
fat-related problem solving and goal
setting. Three follow-up mailings
including nutrition cards, goal-setting
card and cue-card
Six session nutrition
education intervention,
delivered by
paraprofessional
nutrition educators,
designed for low-
income, ethnically
diverse families
12 contacts over 18
weeks, FU at 7 and 19
weeks
Change in % calories
from total fat (recalled
intake to end of
intervention phase),
mean (SD)
�2.8 (2.4) vs�0.5 (2.0),p = 0.01d
Hussey [32],
Medication
adherence (chronic
health conditions),
USA
Quasi RCT, N = 80
(I = 40, C = 40)
Adults aged 65+ with a
chronic illness, Literacy/
numeracy: mixed, not
assessed
Verbal instructions on medication and its
use. Receipt of pictorial schedule tailored to
participant’s medications and daily
schedule (pictures of daily activities, clock,
colored dots to represent medications, with
plastic cover and non-permanent marker to
cross out medications taken)
Verbal instruction
about medication and
its use given
One contact, FU at 2 and
3 weeks
Medication knowledge,
mean change in score
Scores not reported,
F = 0.383, NS
Medication
compliance, mean
change in score
Higher baseline
compliance subgroup:
NS (scores, statistic and
p not reported). Lower
baseline compliance
subgroup: Isignificantly >C(indicated by multipleregression, figures notreported)
Kumanyika et al. [33],
Nutrition education
(cardiovascular
prevention), USA
RCT, N = 330 (I = 167,
C = 163)
African–American adults
with elevated blood
pressure or cholesterol,
Literacy/numeracy: mixed,
assessed using Ten Have
word recognition measure
[55]
Nutrition education, focusing on dietary fat,
cholesterol and sodium, designed for
African–American populations with limited
literacy. Comprised introduction to
materials by nutritionist during a clinic
visit; food picture cards and nutrition
guide; four nutrition group sessions; video,
audiotapes, receipt of cassette player; and
brief nutritionist counseling at three
follow-up clinic visits
Self-help version of
same nutrition
education program,
comprising
introduction to
materials by
nutritionist; food
picture cards and
nutrition guide, and
brief nutritionist
counseling at three
follow-up clinic visits
8 contacts over 12
months, FU at 4, 8 and
12 months
Total serum
cholesterol, mean
change (SE)
Women: �0.41 (0.07)
vs �0.43 (0.07),
p = 0.8d. Men: �0.50
(0.12) vs �0.36 (0.13),
p = 0.4d
Diastolic blood
pressure, mean change
(SE)
Elevated at baseline:
�7.4 (1.9) vs �10.6
(1.9), p = 0.2d. Not
elevated at baseline:
0.9 (2.0) vs �0.8 (2.0),
p = 0.5d
Systolic blood pressure,
mean change (SE)
Elevated at baseline
subgroup: �3.7 (1.1) vs
�6.6 (1.1), p = 0.06d.
Not elevated at baseline
subgroup: 1.4 (1.1) vs
0.4 (1.1), p = 0.5d
S.C
lemen
tet
al./P
atien
tE
du
catio
na
nd
Co
un
seling
75
(20
09
)3
40
–3
51
34
4
Lyons et al. [34],
Nutrition education
(cardiovascular
prevention), USA
RCT (cluster), N = 139
(I = 67, C = 72)
Hispanic adults enrolled in
ESL classes, Literacy/
numeracy: all with limited
literacy in English
(assumed from attendance
at ESL classes)
Nutrition-focused heart disease prevention
program for Hispanic adults with limited
literacy in English, delivered by ESL
teachers in five group sessions. Students
practiced reading, writing, listening and
speaking English in the context of learning
about nutrition, modifying eating habits,
food labels, blood pressure and salt,
shopping and recipes. Interactive approach
including videos, taped listening
comprehension exercises, a game and
scripted role play
Attention control – five
sessions on stress
management
(identifying and
managing stress,
coping strategies,
sources of help)
Five contacts over 5
weeks, FU point not
specified (stated ‘not
long-term’)
Total fat intake, gm
(by recall), mean (SD),
mean change
66.77 (37.22) vs 79.15
(63.28), �9.74 vs 0.97,
F = 1.05, NS
Total saturated fat
intake, gm (by recall),
mean (SD), mean
change
23.79 (14.36) vs 27.93
(14.36),�2.58 vs�0.43,
F = 0.33, NS
Cholesterol intake, mg
(by recall), mean (SD),
mean change
262.61 (191.70) vs
326.77 (270.75),
�44.78 vs 9.43,
F = 1.18, NS
Sodium, mg (by recall),
mean (SD), mean
change
2545.97 (1164.12) vs3118.13 (2386.19),�464.33 vs 346.00,F = 5.19, p < 0.05
McKellar and Rutland-
Brown (2005) [35],
Medication
understanding
(at point of
dispensation), Nepal
Quasi RCT, N = 100
(I = 50, C = 50)
Adults having medications
dispensed, Literacy/
numeracy: all with limited
literacy, assessed by
pharmacy dispensers
asking if they could read
Hospital pharmacy intervention in which
Community Medical Auxiliary On the Job
Trainees provide counseling to patients
with limited literacy immediately after
they have had had medication dispensed to
them (or to a pediatric relative), explaining
dosage instructions verbally
Usual care One contact, FU:
immediate
Understanding of
medication dosage
regimen, % correctly
reporting
88% vs 70%, p = 0.03
Rothman et al. [36,37],
Diabetes disease
management, USA
RCT, N = 217 (I = 112,
C = 105)
Adults with poorly
controlled type 2 diabetes,
Literacy/numeracy: mixed,
assessed using REALM [51]
Educational session with pharmacist. Every
2–4 weeks, face-to-face or by telephone,
intensive diabetes management from a
clinical pharmacist practitioner using
evidence based-algorithms, and support
from diabetes care coordinator to address
patient barriers (e.g. phone reminders,
resolving transport and insurance
difficulties). Each was aware of patient’s
literacy status, and communication tailored
to literacy
One hour educational
session plus usual care
17 (approximately)
contacts over 12
months, FU at 6 and 12
months
HbA1c level, %, mean
change, net change
�2.5 vs �1.6, �0.8, 95%
CI �1.7 to 0.0, p = 0.05d
Systolic blood pressure,
mm Hg, mean change,
net change
�7 vs 2,�9, 95% CI�16to �3, p = 0.008d
Diastolic blood
pressure, mm Hg, mean
change, net change
�4 vs 1, �5, 95% CI �9to �1, p = 0.002d
Total blood cholesterol,
mg/dL, mean change,
net change
�27 vs �12, �15, 95%
CI �35 to 4, NSd
Aspirin use (by self-
report), % reporting
91% (87/96) vs 58% (54/93), p < 0.0001
Seligman et al. [38],
Diabetes care, USA
RCT (cluster), Patients:
N = 182 (I = 95, C = 87);
HPs: N = 63 (I = 31,
C = 32)
Adults with type 2 diabetes,
Literacy/numeracy: All
with limited literacy
assessed using S-TOFLA
[52]
Notifying physicians of patient’s literacy
status by means of a notice affixed to the
patient’s chart for patients assessed as
having limited literacy. No training,
instructions or reminders were given to the
professionals
Usual care (waiting list
control, outcomes were
recorded prior to
receiving intervention)
One contact, FU at 2–9
months (immediate for
HPs)
Intensity of use of
literacy-relevant
management strategies
by physicians, %
reporting use of >3
strategies, odds ratio
20% vs 7%, 4.7, 95% CI1.4–16.0, p = 0.01d
S.C
lemen
tet
al./P
atien
tE
du
catio
na
nd
Co
un
seling
75
(20
09
)3
40
–3
51
34
5
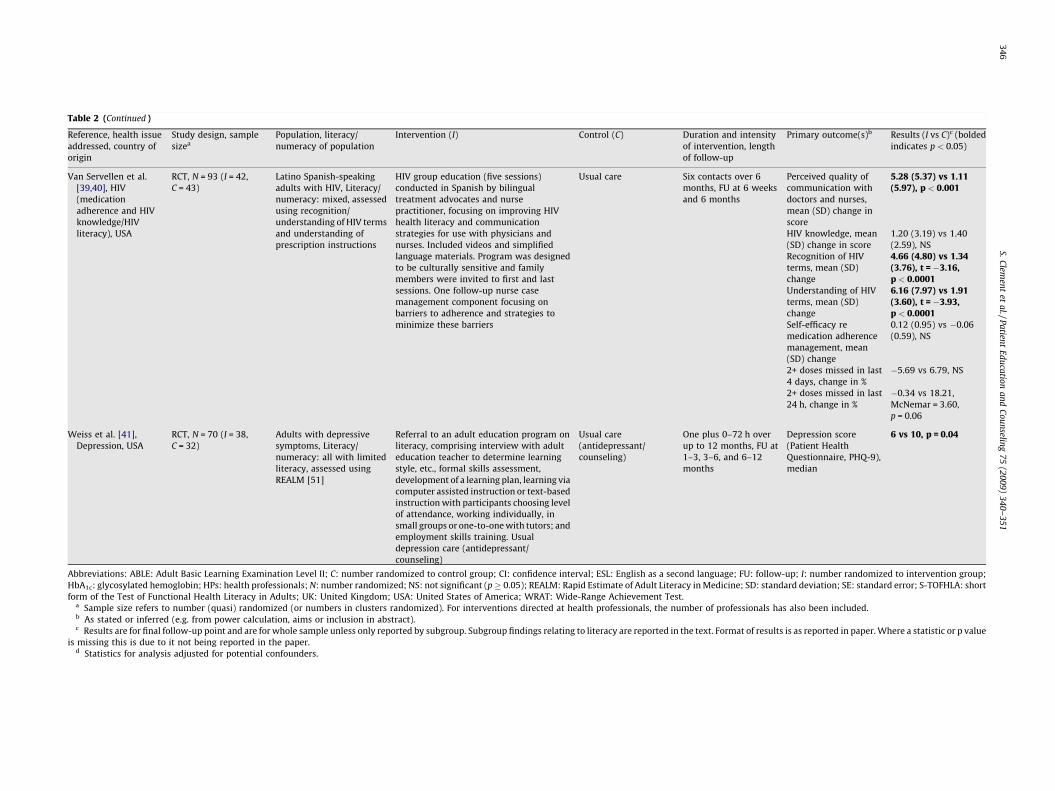
Table 2 (Continued )
Reference, health issue
addressed, country of
origin
Study design, sample
sizea
Population, literacy/
numeracy of population
Intervention (I) Control (C) Duration and intensity
of intervention, length
of follow-up
Primary outcome(s)b Results (I vs C)c (bolded
indicates p < 0.05)
Van Servellen et al.
[39,40], HIV
(medication
adherence and HIV
knowledge/HIV
literacy), USA
RCT, N = 93 (I = 42,
C = 43)
Latino Spanish-speaking
adults with HIV, Literacy/
numeracy: mixed, assessed
using recognition/
understanding of HIV terms
and understanding of
prescription instructions
HIV group education (five sessions)
conducted in Spanish by bilingual
treatment advocates and nurse
practitioner, focusing on improving HIV
health literacy and communication
strategies for use with physicians and
nurses. Included videos and simplified
language materials. Program was designed
to be culturally sensitive and family
members were invited to first and last
sessions. One follow-up nurse case
management component focusing on
barriers to adherence and strategies to
minimize these barriers
Usual care Six contacts over 6
months, FU at 6 weeks
and 6 months
Perceived quality of
communication with
doctors and nurses,
mean (SD) change in
score
5.28 (5.37) vs 1.11(5.97), p < 0.001
HIV knowledge, mean
(SD) change in score
1.20 (3.19) vs 1.40
(2.59), NS
Recognition of HIV
terms, mean (SD)
change
4.66 (4.80) vs 1.34(3.76), t = �3.16,p < 0.0001
Understanding of HIV
terms, mean (SD)
change
6.16 (7.97) vs 1.91(3.60), t = �3.93,p < 0.0001
Self-efficacy re
medication adherence
management, mean
(SD) change
0.12 (0.95) vs �0.06
(0.59), NS
2+ doses missed in last
4 days, change in %
�5.69 vs 6.79, NS
2+ doses missed in last
24 h, change in %
�0.34 vs 18.21,
McNemar = 3.60,
p = 0.06
Weiss et al. [41],
Depression, USA
RCT, N = 70 (I = 38,
C = 32)
Adults with depressive
symptoms, Literacy/
numeracy: all with limited
literacy, assessed using
REALM [51]
Referral to an adult education program on
literacy, comprising interview with adult
education teacher to determine learning
style, etc., formal skills assessment,
development of a learning plan, learning via
computer assisted instruction or text-based
instruction with participants choosing level
of attendance, working individually, in
small groups or one-to-one with tutors; and
employment skills training. Usual
depression care (antidepressant/
counseling)
Usual care
(antidepressant/
counseling)
One plus 0–72 h over
up to 12 months, FU at
1–3, 3–6, and 6–12
months
Depression score
(Patient Health
Questionnaire, PHQ-9),
median
6 vs 10, p = 0.04
Abbreviations: ABLE: Adult Basic Learning Examination Level II; C: number randomized to control group; CI: confidence interval; ESL: English as a second language; FU: follow-up; I: number randomized to intervention group;
HbA1c: glycosylated hemoglobin; HPs: health professionals; N: number randomized; NS: not significant (p � 0.05); REALM: Rapid Estimate of Adult Literacy in Medicine; SD: standard deviation; SE: standard error; S-TOFHLA: short
form of the Test of Functional Health Literacy in Adults; UK: United Kingdom; USA: United States of America; WRAT: Wide-Range Achievement Test.a Sample size refers to number (quasi) randomized (or numbers in clusters randomized). For interventions directed at health professionals, the number of professionals has also been included.b As stated or inferred (e.g. from power calculation, aims or inclusion in abstract).c Results are for final follow-up point and are for whole sample unless only reported by subgroup. Subgroup findings relating to literacy are reported in the text. Format of results is as reported in paper. Where a statistic or p value
is missing this is due to it not being reported in the paper.d Statistics for analysis adjusted for potential confounders.
S.C
lemen
tet
al./P
atien
tE
du
catio
na
nd
Co
un
seling
75
(20
09
)3
40
–3
51
34
6
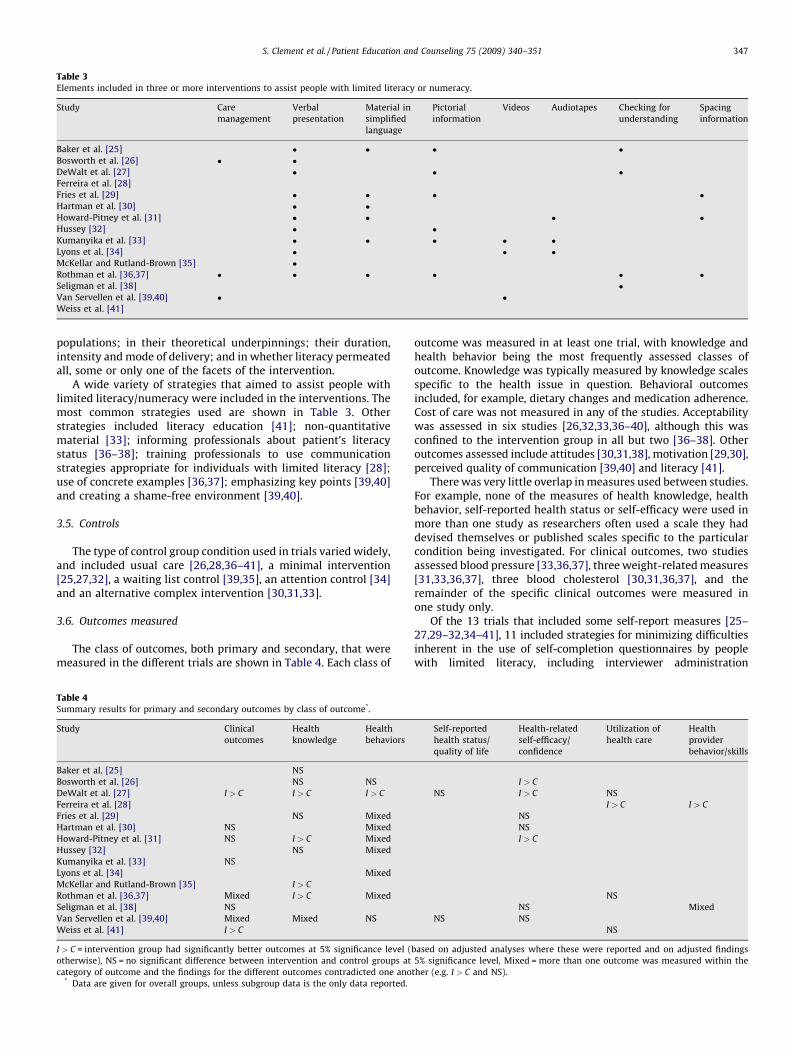
Table 3Elements included in three or more interventions to assist people with limited literacy or numeracy.
Study Care
management
Verbal
presentation
Material in
simplified
language
Pictorial
information
Videos Audiotapes Checking for
understanding
Spacing
information
Baker et al. [25] � � � �Bosworth et al. [26] � �DeWalt et al. [27] � � �Ferreira et al. [28]
Fries et al. [29] � � � �Hartman et al. [30] � �Howard-Pitney et al. [31] � � � �Hussey [32] � �Kumanyika et al. [33] � � � � �Lyons et al. [34] � � �McKellar and Rutland-Brown [35] �Rothman et al. [36,37] � � � � � �Seligman et al. [38] �Van Servellen et al. [39,40] � �Weiss et al. [41]
S. Clement et al. / Patient Education and Counseling 75 (2009) 340–351 347
populations; in their theoretical underpinnings; their duration,intensity and mode of delivery; and in whether literacy permeatedall, some or only one of the facets of the intervention.
A wide variety of strategies that aimed to assist people withlimited literacy/numeracy were included in the interventions. Themost common strategies used are shown in Table 3. Otherstrategies included literacy education [41]; non-quantitativematerial [33]; informing professionals about patient’s literacystatus [36–38]; training professionals to use communicationstrategies appropriate for individuals with limited literacy [28];use of concrete examples [36,37]; emphasizing key points [39,40]and creating a shame-free environment [39,40].
3.5. Controls
The type of control group condition used in trials varied widely,and included usual care [26,28,36–41], a minimal intervention[25,27,32], a waiting list control [39,35], an attention control [34]and an alternative complex intervention [30,31,33].
3.6. Outcomes measured
The class of outcomes, both primary and secondary, that weremeasured in the different trials are shown in Table 4. Each class of
Table 4Summary results for primary and secondary outcomes by class of outcome*.
Study Clinical
outcomes
Health
knowledge
Health
behaviors
Baker et al. [25] NS
Bosworth et al. [26] NS NS
DeWalt et al. [27] I > C I > C I > C
Ferreira et al. [28]
Fries et al. [29] NS Mixed
Hartman et al. [30] NS Mixed
Howard-Pitney et al. [31] NS I > C Mixed
Hussey [32] NS Mixed
Kumanyika et al. [33] NS
Lyons et al. [34] Mixed
McKellar and Rutland-Brown [35] I > C
Rothman et al. [36,37] Mixed I > C Mixed
Seligman et al. [38] NS
Van Servellen et al. [39,40] Mixed Mixed NS
Weiss et al. [41] I > C
I > C = intervention group had significantly better outcomes at 5% significance level (
otherwise), NS = no significant difference between intervention and control groups at
category of outcome and the findings for the different outcomes contradicted one ano* Data are given for overall groups, unless subgroup data is the only data reported.
outcome was measured in at least one trial, with knowledge andhealth behavior being the most frequently assessed classes ofoutcome. Knowledge was typically measured by knowledge scalesspecific to the health issue in question. Behavioral outcomesincluded, for example, dietary changes and medication adherence.Cost of care was not measured in any of the studies. Acceptabilitywas assessed in six studies [26,32,33,36–40], although this wasconfined to the intervention group in all but two [36–38]. Otheroutcomes assessed include attitudes [30,31,38], motivation [29,30],perceived quality of communication [39,40] and literacy [41].
There was very little overlap in measures used between studies.For example, none of the measures of health knowledge, healthbehavior, self-reported health status or self-efficacy were used inmore than one study as researchers often used a scale they haddevised themselves or published scales specific to the particularcondition being investigated. For clinical outcomes, two studiesassessed blood pressure [33,36,37], three weight-related measures[31,33,36,37], three blood cholesterol [30,31,36,37], and theremainder of the specific clinical outcomes were measured inone study only.
Of the 13 trials that included some self-report measures [25–27,29–32,34–41], 11 included strategies for minimizing difficultiesinherent in the use of self-completion questionnaires by peoplewith limited literacy, including interviewer administration
Self-reported
health status/
quality of life
Health-related
self-efficacy/
confidence
Utilization of
health care
Health
provider
behavior/skills
I > C
NS I > C NS
I > C I > C
NS
NS
I > C
NS
NS Mixed
NS NS
NS
based on adjusted analyses where these were reported and on adjusted findings
5% significance level, Mixed = more than one outcome was measured within the
ther (e.g. I > C and NS).

S. Clement et al. / Patient Education and Counseling 75 (2009) 340–351348
[29,30,32,34,35,38–41] developing measures suitable for popula-tions with limited literacy [36,37], selecting existing measures withproven suitability for such populations [31], and simplifying existingmeasures [27].
3.7. Effectiveness of interventions
The findings comparing primary outcomes for the totalpopulations studied in the trials are shown in Table 2. Statisticallysignificant differences in primary outcome measures were foundfor 13 of the 15 trials [26–32,34–41] all favoring the intervention.Eight [26,27,29,31,32,34,36,37,39,40] of these 13 trials had mixedresults finding significant positive findings for some primaryoutcomes and no significant differences between groups for otherprimary outcomes. Two trials [25,33] reported no statisticallysignificantly differences between groups for their primary out-comes. Nine of the fifteen trials [25,26,28–32,34,39,40], includingone of the trials that found no evidence of effect [25], failed toreport an a priori sample size calculation, consequently it is likelythat some of the trials will have been underpowered.
Summary data on effectiveness by class of health outcome forboth primary and secondary outcomes can be seen in Table 4. Fulldata on these outcomes is available from the correspondingauthor. Inspection of the table indicates that health knowledge andhealth-related self-efficacy were the classes of outcome that theinterventions were most likely to improve. Two studies comparedsatisfaction levels in the intervention and control groups, one inpatients [36,37] and one in physicians [38]. In Rothman et al.’sstudy [36,37] of diabetes management the intervention grouppatients were slightly more satisfied (Diabetes Treatment Satisfac-tion Questionnaire [42] possible range 10–36, difference in meanchange 3, 95% confidence interval 1–6). This is a small butstatistically significant improvement in patient satisfaction. InSeligman et al.’s trial of physician notification of patients’ limitedliteracy (without any physician training in the appropriatemanagement for such patients) [38] the intervention groupphysicians were significantly less satisfied with the consultationthan those in the control group (82% vs 96%, adjusted odds ratio0.2, 95% confidence interval 0.1–0.5, p < 0.001).
3.8. Effectiveness for limited literacy subgroups
Of the 11 trials involving participants with mixed literacy levels[25–33,36,37,39,40], four reported a subgroup analysis by literacy
Table 5Quality of included studies.
Reference Method of
randomization
performed?
Treatment
allocation
concealed?
Groups similar at
baseline regarding
important
prognostic
indicators?
Eligi
crite
spec
Baker et al. [25] No No Yes Yes
Bosworth et al. [26] Yes No Yes Yes
DeWalt et al. [27] Yes Yes No Yes
Ferreira et al. [28] No No Yes Yes
Fries et al. [29] Yes Unclear No Yes
Hartman et al. [30] Yes Unclear No Yes
Howard-Pitney et al. [31] Yes Unclear Yes No
Hussey [32] No No Yes Yes
Kumanyika et al. [33] Yes Yes No Yes
Lyons et al. [34] Yes Unclear Yes No
McKellar and
Rutland-Brown [35]
No No Unclear Yes
Rothman et al. [36,37] Yes No No Yes
Seligman et al. [38] Yes Unclear No Yes
Van Servellen et al. [39,40] Yes No No Yes
Weiss et al. [41] Yes No Yes Yes
[25,27,28,36,37]. None was specifically powered to detect differ-ences in subgroups.
Baker et al., in a study [25] on mother’s understanding of ahearing screening for newborns, found no difference in knowledgebetween the intervention and control groups for the overall sample(see Table 2). However, for the mothers with lower levels ofeducation, the intervention group had significantly higher knowl-edge scores (5.00 vs 3.38, p < 0.05).
In a study [27] investigating heart failure self-management,DeWalt et al. reported that for combined death or hospitalizationthere was a significant difference between the intervention andcontrol groups in the group with lower functional health literacy:incidence ratio rate (adjusted) 0.39, 95% confidence interval 0.16–0.91, but not in the higher literacy group: incidence ratio rate(adjusted) 0.56, 95% confidence interval 0.30–1.04. For quality of lifethere was no significant difference between the intervention andcontrol groups in either the low literacy subgroup (difference �1.6,95% confidence interval�15 to 12, p = 0.81) or in the higher literacygroup (difference �4.2, 95% confidence interval �14 to 6, p = 0.40).
In Ferreira et al.’s study [28] on colorectal cancer screening, inthe higher literacy group there was no significant difference inscreening rates between the intervention and control groups(39.0% vs 36.0%, p = 0.65). In contrast, patients with lower literacyin the intervention group were significantly more likely to havescreening than the controls (55.7% vs 30.0%, p = 0.002).
Rothman et al., investigating diabetes management, reportedno difference in Hemoglobin A1c (HbA1C) levels in the higherliteracy subgroup (adjusted difference �0.5%, 95% confidenceinterval�1.4% to 0.3%, p = 0.21), but in the lower literacy subgroupthe intervention group had a greater reduction in HbA1c levels(adjusted difference �1.4%, 95% confidence interval �2.3% to�0.6%, p < 0.001). For systolic blood pressure, differences werecomparable for patients with low and higher literacy [36,37].
3.9. Quality of studies
An overview of the quality of the trials using the modifiedDelphi List criteria can be seen in Table 5. Only five trials clearlymet six or more of the nine criteria [27,33,36–38,41] and five metthree or fewer [25,30,31,34,39,40]. The criteria most likely to beclearly met were specifying eligibility criteria, giving pointestimates and measures of variability and using randomization,and those least likely to be clearly met were concealment oftreatment allocation and blinding of outcome assessors.
bility
ria
ified?
Outcome
assessor
blinded for
all primary
outcomes?
Point estimates
and measure of
variability given
for all primary
outcomes?
Intention-
to-treat
analysis?
A priori
sample size
calculation
included?
Participant
flow diagram
included?
Unclear No Yes No No
Unclear Yes Unclear No No
No Yes Unclear Yes Yes
Unclear Yes No No Yes
Unclear Yes Unclear No Yes
Unclear Yes Unclear No No
Unclear Yes Unclear No No
Unclear No Yes No No
Yes Yes Unclear Yes No
Unclear Yes No No No
No Yes Yes Yes No
Yes Yes Yes Yes Yes
Unclear Yes Yes Yes Yes
Unclear Yes No No No
Yes No Yes Yes No

S. Clement et al. / Patient Education and Counseling 75 (2009) 340–351 349
Of the five cluster trials, one [28] was very limited by onlyhaving one cluster per group so intervention and cluster areconfounded. One of the cluster trials [34] made no mention ofadjusting for the design effect in the analysis.
Inspection of Tables 2 and 5 indicated that there was no evidentrelationship between the significance of primary outcomes andquality (assessed by either �6 vs �3 Delphi criteria clearly met orby randomized vs quasi-randomized trials).
4. Discussion and conclusions
4.1. Discussion
The evidence uncovered in this systematic review indicatesthat the complex interventions reviewed are effective in achievingimprovement in certain outcomes, but not all. The majority (13/15) of the trials reported positive change in at least one of theirprimary outcomes. Knowledge and self-efficacy were the classesout outcome most likely to improve. Health knowledge is anappropriate intermediate outcome to study, indicating successfuldelivery of an intervention. Improvements in knowledge alone area weak premise for implementing an intervention, however onlyone study [35] had knowledge improvement as its sole beneficialoutcome.
Of the two trials not reporting such change, one [25] did nottarget its intervention at a group anticipated to have manyparticipants with limited literacy, and its subgroup analysis ofthose with lower levels of education did find a significantintervention effect. The other [33] had a control condition thathad substantial elements likely to aid those with limited literacy. Inaddition, as it used a mixed literacy sample with no subgroupanalysis by literacy level, it is possible that there may have been amasked benefit specific to those with limited literacy. It should benoted, however, that some interventions may improve outcomesfor people regardless of literacy level, while others may be effectivesolely in low or high literacy populations. This issue merits furtherexploration in future research.
The only detrimental outcome reported was decreasedphysician satisfaction [38], an effect which might be amelioratedby extending the intervention to include training professionals onhow best to respond after receiving information that a patient haslimited literacy. Another possible detriment may be the additionalcost of the complex interventions for possibly significant but smallbenefit. The interventions varied widely in their intensity andduration, and consequently are likely to differ in their cost. Thesetwo issues highlight the importance of economic evaluation whichnone of the studies reviewed had undertaken.
The focus, scope and timing of our review differed from that ofPignone et al. [21] in that ours was restricted to complexinterventions and was a more recent review. Consequently itwas able to include the many studies published since 2003 andlargely because of this only a quarter (4/15) of our studiesoverlapped with those in the earlier review. Despite thesedifferences, our findings largely concur, with results eitherfavoring the intervention or there being no evidence of effect.Furthermore, both reviews found interventions were highlydiverse and the quality of the studies was varied. This resonateswith the findings of the Institute of Medicine’s overview [3] whichreported that studies evaluating complex health literacy inter-ventions produced variable results. Although our review had anarrower focus than the work of Coulter and Ellins [2], our findingsare broadly in line the conclusion of these authors that large gapsremain in our knowledge about how health literacy can beimproved [2].
There is increasing debate about definitions of, and conceptsinvolved in, health literacy. This review has focused on just two of
these, although many of the interventions included widerempowerment and/or community participation aspects. Furtherprimary and secondary research is needed to explore healthliteracy interventions from this wider conceptual framework.
In reviewing trials specifically on literacy and numeracy it wasapparent that all the interventions concentrated on reading ability,and none had numeracy as its primary focus, although onespecified using a non-quantitative approach [33], and another usedpictorial representations of medication regimens [32] which mayspecifically aid those with numeracy difficulties. The importance ofnumeracy skills and complex numeracy concepts in some areas ofmedicine, such as the concepts of absolute and relative risk used inadvice on screening tests, makes this an important area for futurestudy.
Results of the trial quality assessment, found that only a third(5/15) clearly met six or more of the nine quality criteria, and athird (5/15) met three or fewer. This may reflect poor trial designand conduct, such as the use of alternation and the non-blindedassessment of outcomes. Some of the quality findings may reflectpoor reporting, as there is empirical evidence that the reporting ofmethodological aspects of trials does not necessarily reflect theconduct of the trial [43]. The CONSORT statement was introducedin 1996 to improve the reporting of trials [44]. All but one [32] ofthe trials were published after its introduction, but nine trials didnot include an a priori sample size calculation and 10 did notinclude patient flow diagrams, indicating that the statement is notbeing optimally adhered to.
The review noted the complexity of self-reported outcomemeasurement with populations with limited literacy. Furtherresearch might address whether interviewer administration or thedevelopment and validation of low literacy-appropriate outcomemeasures is warranted. In the US work on the latter activity hasalready begun [45]. We noted that nearly half (7/15) of the trialshad not reported any clinical outcomes. Whilst outcomes such ashealth knowledge and health behavior are important, changes insuch variables do not necessarily translate into changes in health,as was the case in two trials reviewed [30,31].
We have highlighted the need for rigor in the design andreporting of trials using CONSORT guidelines [24]. Such trialswould benefit from including more clinical, quality of life, and costoutcomes, and longer post-intervention durations of follow-up.There is a relative dearth of trials of interventions directed athealth professionals, and future trials could usefully combine bothinforming practitioners of patient’s literacy status and training thepractitioners to optimally deliver care to such patients. Similarlywe found only one study on the health benefits of literacyeducation, which found it was beneficial for depression [41].Further research in this area may prove useful, particularly asanother study found a complex intervention incorporating literacyeducation improved depression [46]. Increasing literacy skills alsohas the theoretical potential for improving physical health, but thisdoes not appear to have been researched.
As complex interventions are particularly context-sensitive[47,48], there is a need for research to allow flexibility to localneeds [48], and to be undertaken in a wider variety of contexts thanthe current predominantly North American evidence base. Futureresearch might also usefully explore which of the complexinterventions’ components are the most effective in improvinghealth through qualitative studies conducted alongside or afterRCTs [17], or by integrating process evaluations, which may usequalitative or quantitative data or both, into RCTs [47]. Further-more, as not all social interventions can be tested in RCTs [49] andas some researchers see such trials as being inappropriate forevaluating health promotion interventions [50], there may be acase for future reviews in this area to include a wider range of studytypes beyond the controlled trial.

S. Clement et al. / Patient Education and Counseling 75 (2009) 340–351350
4.2. Strengths and limitations
A strength of this review is the comprehensive search andsystematic application of inclusion criteria, which yielded 15studies for in-depth review. Although not a replication of Pignoneet al.’s earlier systematic review [21], our review helps to updatethat review by its inclusion of 10 studies published since theseauthors conducted their searches [21]. Another strength is thedetailed data extraction and critical appraisal of studies, whichprovides a synthesis of the current state of evidence and may helpto guide future research.
The review’s main limitations are: unmasked screening andassessment of papers; the majority of the initial screen beingundertaken by one assessor; the possibility of publication bias,particularly as the review was limited to published material; therestriction to journal articles; and that family-focused interven-tions measuring both adult and child outcomes were excluded. Theinclusion of some papers which did not specifically assess literacycould be viewed as a strength in that it allowed a wider range ofstudies to be included, however, it can also be viewed as animportant limitation due to the non-use of validated measures ofliteracy or numeracy. To aid comparability, we recommend thatfuture studies use standardized measures of literacy and numeracywhenever possible. Another issue which can be perceived as eithera strength or a limitation is the restriction of the review to RCTs andquasi-RCTs, which enhances the rigor of the body of literatureconsidered, but excludes some quality studies undertaken in thisarea which used other study designs.
4.3. Practice implications
This review lends support to the wider introduction ofinterventions for people with limited literacy, particularly withinan evaluation context. The reason for this recommendation thatimplementation incorporates some evaluation is because ourfindings have a number of important caveats.
We cannot infer from the findings that it is necessarily theliteracy elements of the interventions which have produced thechanges as all were complex interventions and to some degreemulti-faceted, and none had a control group that was identicalapart from the literacy element.
The inferences about implications for practice that can be madefrom this review need to be considered in the light of the internalvalidity (scientific quality) of the trials. Table 5 shows that theinternal validity of the trials was of variable quality. The trialsreviewed also vary in their external validity (generalizability).Some were specifically designed to be relatively easy to implementin routine practice [26] whereas others are more resource intensive[36,37]. Further, the majority of the research was from the US,therefore cannot necessarily be generalized to other health andeducational contexts.
It is also important to consider the size of clinical changesfound. Four studies had primary clinical outcomes [27,33,36,37,41]and three of these reported statistically significant differencesbetween the intervention and control groups for these outcomes[27,36,37,41]. The size of the differences between groups appearsto be clinically meaningful.
4.4. Conclusions
In conclusion, the evidence in this systematic review suggeststhat there is a case for initiatives such as those reviewed beingintroduced more widely. The findings do not give a clear pictureabout which type of initiative is most likely to be effective as theinterventions were diverse and health-related outcomes improvedfor each of the major intervention types (health education/
management interventions, literacy education interventions, andthose directed at professionals). However, methodological short-comings and the mixed nature of some of the findings indicate thatinterventions would most appropriately be introduced in anevaluative or research context. Furthermore, given that some of theinterventions were quite highly resource intensive, and that withall complex interventions we do not know which are the key activeingredients, it will be important to design any initiative with care,drawing on both theoretical and empirical knowledge. This mightinclude careful consideration of evidence from studies of simpleinterventions, or the conduct of future research comparingcomplex interventions that differ in their constituent parts. Lastly,although this review focused on two specific aspects of healthliteracy (reading ability and numeracy) many of the interventionsincluded wider empowerment and/or community participationaspects, and the implementation of literacy/numeracy interven-tions might most usefully be embedded within this broaderapproach to health literacy.
Conflict of interest
None.
Acknowledgements
We thank those working in the field of health literacy whokindly sent us information about potentially relevant studies.
Funding: Sarah Clement was supported by a HEFCE ResearchCapability Fellowship; Saima Ibrahim was supported by a grantfrom STaRNet London, Department of Health. The funding sourceshad no role in the study design, in the collection, analysis, andinterpretation of data, in the writing of the report, or in the decisionto submit for paper for publication. The views expressed are thoseof the authors and do not necessarily reflect those of the fundingbodies.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, in
the online version, at doi:10.1016/j.pec.2009.01.008.
References
[1] United States Department of Health and Human Services. Public healthpriorities. Office of the Surgeon General, United States Department of Healthand Human Services. http://www.surgeongeneral.gov/publichealthpriorities.html; 2007.
[2] Coulter A, Ellins J. Effectiveness of strategies for informing, educating, andinvolving patients. Brit Med J 2007;335:24–7.
[3] Institute of Medicine. Health literacy: a prescription to end confusion.Washington, DC: The National Academic Press; 2004.
[4] Nutbeam D. Health promotion glossary. Health Promot Int 1998;13:349–64.[5] Kickbusch I, Wait S, Maag D. Navigating health: the role of health literacy.
London: Alliance for Health and the Future; 2005, http://ns1.siteground169.com/�healthan/healthandfuture/images/stories/Documents/navigating%20health%20-%20the%20role%20of%20health%20literacy.pdf.
[6] Baker DW. The meaning and the measure of health literacy. J Intern Med2006;21:878–83.
[7] Department for Education and Science. The skills for life survey: a nationalneeds and impact survey of literacy, numeracy and ICT skills. London: Depart-ment for Education and Skills; 2003, http://www.dfes.gov.uk/research/data/uploadfiles/RR490.pdf.
[8] Paasche-Orlow MK, Parker RM, Gazmararian JA, Nielson-Bohlman LT, Rudd RR.The prevalence of limited health literacy. J Gen Intern Med 2005;20:175–84.
[9] Baker DW, Parker RM, Williams MV, Clark WS. Health literacy and the risk ofhospital admission. J Gen Intern Med 1998;13:791–800.
[10] Wolf MS, Gazmararian JA, Baker DW. Health literacy and functional healthstatus among older adults. Arch Intern Med 2005;165:1946–52.
[11] Sudore RL, Yaffe K, Satterfield S, Harris TB, Mehta KM, Simonsick EM. Limitedliteracy and mortality in the elderly: the health, aging, and body compositionstudy. J Gen Intern Med 2006;21:806–12.
S. Clement et al. / Patient Education and Counseling 75 (2009) 340–351 351
[12] Williams MV, Baker DW, Parker RM, Nurss JR. Relationship of functional healthliteracy to patients’ knowledge of their chronic disease: a study of patientswith hypertension and diabetes. Arch Intern Med 1998;158:166–72.
[13] Wolf MS, Davis TC, Tilson HH, Bass PF, Parker RM. Misunderstanding ofprescription drug warning labels among patients with low literacy. Am JHealth-Syst Ph 2006;63:1048–55.
[14] DeWalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP. Literacy and healthoutcomes. J Gen Intern Med 2004;19:1228–39.
[15] Baker DW, Parker RM, Williams MV, Pitkin K, Parikh NS, Coates W, Imara M.The health care experiences of patients with low literacy. Arch Fam Med 1996;5:329–34.
[16] Wolf MS, Williams MV, Parker RM, Parikh NS, Nowlan AW, Baker DW. Patient’sshame and attitudes toward discussing the results of literacy screening. JHealth Commun 2007;12:721–32.
[17] Medical Research Council. A framework for development and evaluation ofRCTs for complex interventions to improve health. London: Medical ResearchCouncil; 2000, http://www.mrc.ac.uk/Utilities/Documentrecord/index.htm?d=MRC003372.
[18] Santo A, Laizner AM, Shohet L. Exploring the value of audiotapes for healthliteracy: a systematic review. Patient Educ Couns 2005;58:235–43.
[19] Paasche-Orlow MK, Schillinger D, Greene SM, Wagner EH. How health caresystems can begin to address the challenge of limited literacy. J Gen InternMed 2006;2:884–7.
[20] Coulter A, Ellins J. Improving health literacy. In: Patient-focused interventions:a review of the evidence. London: Picker Institute Europe; 2006 , http://www.pickereurope.org/Filestore/Publications/QEI_Review_AB.pdf.
[21] Pignone M, DeWalt DA, Sheridan S, Berkman, Lohr KN. Interventions toimprove health outcomes for patients with low literacy: a systematic review.J Gen Intern Med 2005;20:185–92.
[22] Higgins JPT, Green S, editors. Cochrane handbook for systematic reviews ofinterventions 4.2.6. The Cochrane Library. Chichester: John Wiley & Sons Ltd.;2006, http://www.cochrane.org/resources/handbook/hbook.htm.
[23] Verghagen AP, de Vet HCW, de Bie RA, Kessells AGH, Boers M, Bouter LM,Knipschild PG. The Delphi List: a criteria list for quality assessment ofrandomized clinical trials for conducting systematic reviews developed byDelphi consensus. J Clin Epidemiol 1998;51:1235–41.
[24] Moher D, Schulz KF, Altman DG. The CONSORT statement: revised recom-mendations for improving the quality of reports of parallel group randomizedtrials. BMC Med Res Method 2001;1:2.
[25] Baker H, Uus K, Bamford J, Marteau TM. Increasing knowledge about a screen-ing test: preliminary evaluation of a structured, chart-based, screener pre-sentation. Patient Educ Couns 2004;52:55–9.
[26] Bosworth HB, Olsen MK, Gentry P, Orr M, Dudley T, McCant F, Oddone EZ. Nurseadministered telephone intervention for blood pressure control: a patient-tailored multifactorial intervention. Patient Educ Couns 2005;57:5–14.
[27] DeWalt DA, Malone RM, Bryant ME, Kosnar MC, Corr KE, Rothman RL, Sueta CA,Pignone MP. A heart failure self-management program for patients of allliteracy levels: a randomized, controlled trial. BMC Health Serv Res 2006;6:30.
[28] Ferreira MR, Dolan NC, Fitzgibbon ML, Davis TC, Gorby N, Ladewski L, Lui D,Rademaker AW, Medio F, Schmitt BP, Bennett CL. Health care provider-directed intervention to increase colorectal cancer screening among veterans:results of a randomized controlled trial. J Clin Oncol 2005;23:1548–54.
[29] Fries E, Edinboro P, McClish D, Manion L, Bowen D, Beresford SAA, Ripley J.Randomized trial of a low-intensity dietary intervention in rural residents: theRural Physician Cancer Prevention Project. Am J Prev Med 2005;28:162–8.
[30] Hartman TJ, McCarthy PR, Park RJ, Schuster E, Kushi LH. Results of a commu-nity-based low-literacy nutrition education program. J Commun Health 1997;22:325–41.
[31] Howard-Pitney B, Winkleby MA, Albright CL, Bruce B, Fortmann SP. TheStanford Nutrition Action Program: a dietary fat intervention for low-literacyadults. Am J Public Health 1997;87:1971–6.
[32] Hussey LC. Minimizing effects of low literacy on medication knowledge andcompliance among the elderly. Clin Nurs Res 1994;3:132–45.
[33] Kumanyika SK, Adams-Campbell L, Van Horn B, Ten Have TR, Treu JA, Askov E,Williams J, Achterberg T, Zaghloul H, Monsegu D, Bright M, Stoy DB, Malone-Jackson M, Mooney D, Deiling S, Caulfield J. Outcomes of a cardiovascularnutrition counseling program in African–Americans with elevated bloodpressure or cholesterol level. J Am Diet Assoc 1999;99:1380–91.
[34] Lyons GK, Woodruff SI, Candelaria JI, Rupp JW, Elder JP. Effect of a nutritionintervention on macronutrient intake in a low English-proficient Hispanicsample. Am J Health Promot 1997;11:371–4.
[35] McKellar AT, Rutland-Brown W. Using community medical auxiliary traineesto improve dose understanding among illiterate hospital outpatients in ruralNepal. Trop Doct 2005;35:17–8.
[36] Rothman RL, DeWalt DA, Malone R, Bryant B, Shintani A, Crigler B, WeinbergerM, Pignone M. Influence of patient literacy on the effectiveness of a primarycare-based diabetes disease management program. J Amer Med Assoc 2004;292:1711–6.
[37] Rothman RL, Malone R, Bryant B, Shintani A, Crigler B, DeWalt DA, Dittus RS,Weinberger M, Pignone MP. A randomized trial of a primary care-baseddisease management program to improve cardiovascular risk factors andglycated hemoglobin levels in patients with diabetes. J Amer Med Assoc2005;118:276–84.
[38] Seligman HK, Wang FF, Palacios JL, Wilson CC, Daher C, Piette JD, Schillinger D.Physician notification of their diabetes patients’ limited health literacy: arandomised, controlled trial. J Gen Intern Med 2005;20:1001–7.
[39] Van Servellen G, Carpio F, Lopez M, Garcia-Teague L, Herrera G, Monterrosa F,Gomez R, Lombardi E. Program to enhance health literacy and treatmentadherence in low-income HIV-infected Latino men and women. AIDS PatientCare ST 2003;17:581–94.
[40] Van Servellen G, Nyamathi A, Carpio F, Pearce D, Garcia-Teague L, Herrera G,Lombardi E. Effects of a treatment adherence enhancement program on healthliteracy, patient–provider relationships, and adherence to HAART among low-income HIV-positive Spanish-speaking Latinos. AIDS Patient Care ST 2005;19:745–59.
[41] Weiss BD, Francis L, Senf JH, Heist K. Literacy education as treatment fordepression in patients with limited literacy and depression: a randomizedcontrolled trial. J Gen Intern Med 2006;21:823–8.
[42] Bradley C. Handbook of psychology and diabetes. London: Harwood AcademicPublishers; 1994.
[43] Soares HP, Daniels S, Kumar A, Clarke M, Scott C, Swann S, Djulbegovic B. Badreporting does not mean bad methods for randomized trials: observationalstudy of randomized controlled trials performed by the Radiation TherapyOncology Group. Brit Med J 2004;328:22–4.
[44] Begg CB, Cho MK, Eastwood S, Horton R, Moher D, Olkin I, Rennie D, Schulz KF,Simel DL, Stroup DF. Improving the quality of reporting of randomized con-trolled trials: the CONSORT statement. J Amer Med Assoc 1996;276:637–9.
[45] Reeve BB, Hayes RD, Bjorner JB, Cook KF, Crane PK, Teresi JA, Thissen D, RevickiDA, Weiss DJ, Hambleton RK, Liu H, Gershon R, Reise SP, Lai J, Cella D.Psychometric evaluation and calibration of health-related quality of life itembanks: plans for the Patient-Reported Outcomes Measurement InformationSystem (PROMIS). Med Care 2007;45:S22–31.
[46] Poresky RH, Daniels AM. Two-year comparison of income, education, anddepression among parents participating in regular Head Start of supplemen-tary Family Service Center Services. Psychol Rep 2001;88:787–96.
[47] Oakley A, Strange V, Bonell C, Allen E, Stephenson J, RIPPLE Study Team.Process evaluation in randomized controlled trials of complex interventions.Brit Med J 2006;332:413–6.
[48] Hawe P, Shiell A, Riley T. Complex interventions: how ‘‘out of control’’ can arandomized controlled trial be? Brit Med J 2004;328:1561–3.
[49] Thomson H, Hoskins R, Petticrew M, Ogilvie D, Craig N, Quinn T, Lindsay G.Evaluating the health effects of social interventions. Brit Med J 2004;328:282–5.
[50] World Health Organisation Europe. Health promotion evaluation: recommen-dations for policy makers. Copenhagen: WHO Working Group on HealthPromotional Evaluation; 1999.