comparison of the anti-anginal efficacy of nicardipine and nifedipine in patients receiving...
TRANSCRIPT
Iniernatlonal Journal of Curdwlogv. 22 (1989) 357-363
Elsevier
357
IJC 00825
Comparison of the anti-angina1 efficacy of nicardipine and nifedipine in patients receiving atenolol: a randomized,
double-blind, crossover study
Hew? Douard, Bernard Mora and Jean-Paul Broustet
H6ptaf Cardiologique du Haut Leueque, merue de Mageffan, Pessac. France
(Received 1 April 1988; revision accepted 24 September 1988)
Douard H. Mora B, Broustet J-P. Comparison of the anti-angina1 efficacy of nicarpidine and nifedipine in patients receiving atenolol: a randomized, double-blind, crossover study. Int J Cardiol 1988;22:357-363.
The effects of oral nicardipine (40 mg) and nifedipine (20 mg) in combination with atenolol (100 mg) were compared with those of placebo, oral nitroglycerin (0.4 mg) and atenolol alone (100 mg) in 17 patients with stable effort angina. Patients performed symptom-limited, multistage, upright bicycle ergometric exercises with computer-assisted ECG analysis in bipolar lead CM5. Nicardipine and nifedipine were given double blind and in randomized order. In comparison with placebo (4818 f 2021 kpm), patients exercised longer and with a greater work load with nitroglycerin (5748 f 1711 kpm, P < O.OOl), the combinations of atenolol and nifedipine (6120 f 2274 kpm, P < 0.05), and atenolol and nicardipine (6671 k 2339 kpm, P < O.Ol), but not with atenolol alone (5305 f 1524 kpm, P = NS). The magnitude of ST-segment depression at peak exercise with placebo (3.22 + 1.72 mm) was dramatically reduced with nitroglycerin (1.39 f 1.87 mm) but less with atenolol alone (2.95 f 1.83 mm, P < 0.05) or the combinations of atenolol and nicardipine (3.05 f 1.51 mm, P= NS), and atenolol and nifedipine (2.45 k 1.25 mm, P < 0.001). Compared to the combination of atenolol and nifedipine, that of atenolol and nicardipine produced a significantly (P c 0.05) greater exercise tolerance (6671 f 2339 versus 6120 f 2274 kpm) but with a greater ST-segment depression at peak exercise (3.05 f 1.51 versus 2.45 + 1.29 mm, P < 0.01).
Key words: Nicardipine; Exercise test
Introduction generally be improved by giving a beta-blocker in combination with a calcium antagonist [l-5].
In many patients with angina pectoris, therapy There have been recent reports of the efficacy of
with a beta-blocker given in isolation is often nicardipine, a new calcium slow channel-blocking
insufficient, in which case exercise tolerance can drug [6-91, but never in combination with a beta- blocker. The purpose of the present study was to compare the combination of atenolol and nicardipine with that of atenolol and nifedipine. We sought to determine the efficacy of each com-
Correspondence to: Dr. H. Douard. Hapital Cardiologique bination compared to a beta-blocker and sublin-
du Haut Leveque. avenue de Magellan, 33604 Pessac, France. gual nitroglycerin alone as well as in combination.
0167-5273/89/$03.50 ‘cl 1989 Elsevier Science Publishers B.V. (Biomedical Division)

358
Patients studied
Methods TABLE 1
Protocol of the eight exercise tests performed by each patient.
Seventeen men aged 57.4 i 7.8 years (mean I standard deviation), with reproducible exertional angina pectoris were enrolled in the study. Each had a positive exercise tolerance test (with chest pain accompanied by horizontal or downsloping ST-segment depression of at least 1 mm or more in bipolar lead CM5). Exclusion criteria were as follows: peripheral vascular insufficiency, ortho- pedic impairment, severe hypertension (systolic > 200 mm Hg, diastolic > 100 mm Hg at rest), con- gestive heart failure, valvar disease. bundle branch block, atrioventricular block, pre-excitation syn- drome, and hepatic or renal dysfunction. All were in sinus rhythm; no patient had had coronary arterial bypass surgery or transluminal coronary angioplasty. Each patient had had at least two exercise tests before entering the study and was familiar with the test environment. All patients underwent selective coronary arteriography. within two weeks before or after enrollment. All had luminal diameter stenosis of 70% or more of at least one major coronary artery (3-vessel disease in six, 2-vessel disease in six and l-vessel disease in five); informed written consent was obtained from all patients at the time of study entry.
Protocol
No concomitant therapy was allowed, other than anticoagulants. Patients on previous anti- angina1 treatment underwent a wash-out phase (one month for arniodarone, two days for beta- blockers and calcium antagonists, and 24 hours for nitrates).
The study was carried out over three days: each patient underwent eight exercise tests (schedule and treatments are given in Table 1). The presen- tation of placebo, nicardipine and nifedipine was identical; placebo was administered single blind on Day 1 at 10.00 h. Nifedipine (20 mg) and nicardipine (40 mg) were administered in double- blind crossover fashion on Day 2 or 3 of the protocol at 10.00 h (1.5 h before exercise testing): atenolol(lO0 mg) was administered on Days 1 and
Time Day 1 Day 2 Day 3 (a.m.)
09.30 ATE (no. 3) ATE (no. 6) ATE + NTG ATE + NTG
(no. 4) (no. 7)
11.30 Placebo NIF (or NIC) NIC (or NIF)
(no. 1) +ATE (no. 5) +ATE (no. 8)
12.00 Pla + NTG
(no. 2)
ATE = atenolol: NIC = nicardipine; NIF= nifedipine; NTG
= sublingual nitroglycerin; Pla = placebo.
2 at 20.00 h (13.30 h before exercise testing). Five minutes after exercise tests 1. 3, and 6 a nitrog- lycerin spray (0.4 mg) was administered, followed 5 minutes later by exercise Tests 2, 4, and 7.
Efficiency equivalence of nicardipine and nifedipine dosages used were established from previous studies [6-91.
Exercise testing
Multistage upright bicycle ergometer testing was performed according to the exercise protocol of our laboratory [lo]. In summary, heart rate and blood pressure were recorded after the patient had been sitting on the bicycle for five minutes. Bi- polar lead CM5 was monitored continuously. The workload was increased by 30 watts every three minutes with a starting load of 30 watts: the patient pedalled at a constant rate of 60 r/mm; heart rate and ST-segment depression (measured 60 msec after the J point) were analyzed automati- cally (Marquette CASE) every three minutes, at peak exercise and every minute during the re- covery phase. Blood pressure was monitored every three minutes using a sphygmomanometer. Ex- ercise was continued until the occurrence of ex- haustion. angina. frequent ventricular ectopy, ab- sence of elevation or fall in blood pressure; in no case was testing stopped because of marked ST- segment depression.
Variables assessed
The following variables were measured (before breaking the randomization code) at rest and peak

359
TABLE 2
Analysis of variance showed no interaction or order effect
between the atenolol and nicardipine, and atenolol and
nifedipine combinations, but a significant treatment effect with
respect to exercise work, maximal ST-segment depression and
maximal heart rate.
Interaction Order effect Treatment
test effect
Rate-pressure t = 0.25 NS t = 0.20 NS t = 1.55 NS
product
Exercise work 2 = 1.88 NS t = 0.98 NS t = 2.42
(kpm) P i 0.05
Maximal ST-segment t = 0.91 NS t = 1.07 NS t = 3.89
depression P < 0.01
Maximal heart t=0.55NS t=1.88NS r=2.69
rate P < 0.02
exercise: heart rate, systolic blood pressure, rate- pressure product (heart rate X systolic pressure), total exercise tolerance (kpm), and ST-segment depression. Exercise work and ST-segment depres- sion were recorded when the heart rate reached 100 beats/min. Heart rate and ST-segment de- pression were recorded when the exercise level reached 3260 kpm (minimal workload reached by all patients).
Statistical analysis
Analysis of variance of total exercise tolerance and ischemic ST-segment depression indicated sig- nificant patient and treatment factors (P -c 0.001 in each case); two different treatments were there- fore compared by paired t-testing. Analysis of variance showed no significant test order effect (Table 2) with respect to the main parameters: rate-pressure product, exercise work, maximal ST depression, maximal heart rate (for Patients 1, 3, 6, 7, 9. 12, 14, and 16, the order was nicardipine and atenolol, followed by nifedipine plus atenolol with the reverse order for Patients 2. 4, 5, 8, 11, 13, and 14).
Results (Table 3)
Adverse effects
Patient compliance was excellent throughout the study with respect to treatment times and
exercise testing: no patient withdrew from the study; no adverse effects were noted except for an excessive fall in blood pressure in two patients following administration of sublingual nitro- glycerin before the second test.
The fall in blood pressure was probably pre- cipitated by diminished peripheral resistance fol-
lowing the first exercise test.
Cause of cessation
On placebo, all patients stopped exercise be- cause of angina. The percentage for cessation of pain was lower on the following combinations, atenolol and nitroglycerin (32%, P = NS); ateno- 101 and nicardipine (41%, P = NS), atenolol and nifedipine (23%, P < 0.05), than on single therapy
(nitroglycerin 53%, atenolol 53%).
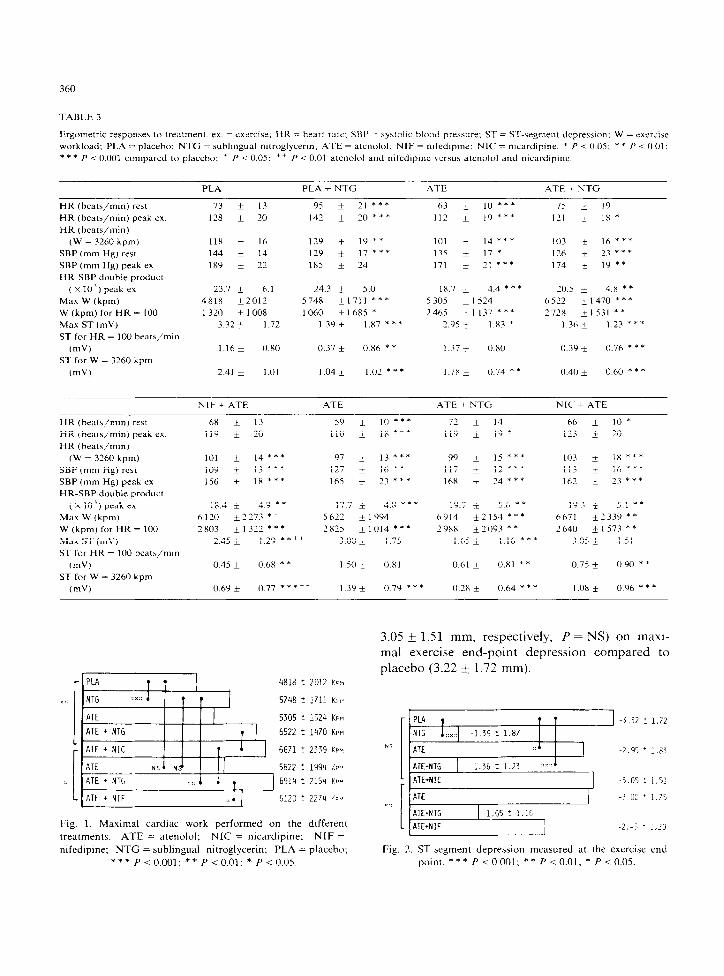
Exercise work (Fig. 1)
Compared to placebo (4818 k 2012 kpm), the improvement in performance was significant on nitroglycerin (5748 k 1711 kpm, P < 0.001) but not on atenolol (5622 i 1994 kpm. P = NS). This was probably due to the fact that the patients did not have very severe coronary arterial disease and were inhibited by beta-blocker-induced brady- cardia at the exercise end-point (110 + 118 beats/min).
The best performances (P < 0.01) were achieved on the combinations of atenolol and nitroglycerin (6914 k 2154 kpm) or atenolol and nicardipine (6671 f 2339 kpm), which were significantly more effective than atenolol and nifedipine (6120 * 2273 kpm, P < 0.05).
At a heart rate of 100 beats/mm, work perfor- mance was lower on nitroglycerin as the patients had not fully returned to their baseline state after the test on placebo. There was no significant dif- ference between beta-blockers alone or in combi- nation: all significantly improved work perfor- mance (from 2640 f 1573 to 2988 + 2093 kpm, P -c 0.01) compared to placebo (1320 k 1008 kpm), as a result of their bradycardia-inducing activity.
ST-segment depression (Fig. 2)
Atenolol alone or in combination with nicardipine had little or no effect (3.00 + 1.75 and
360
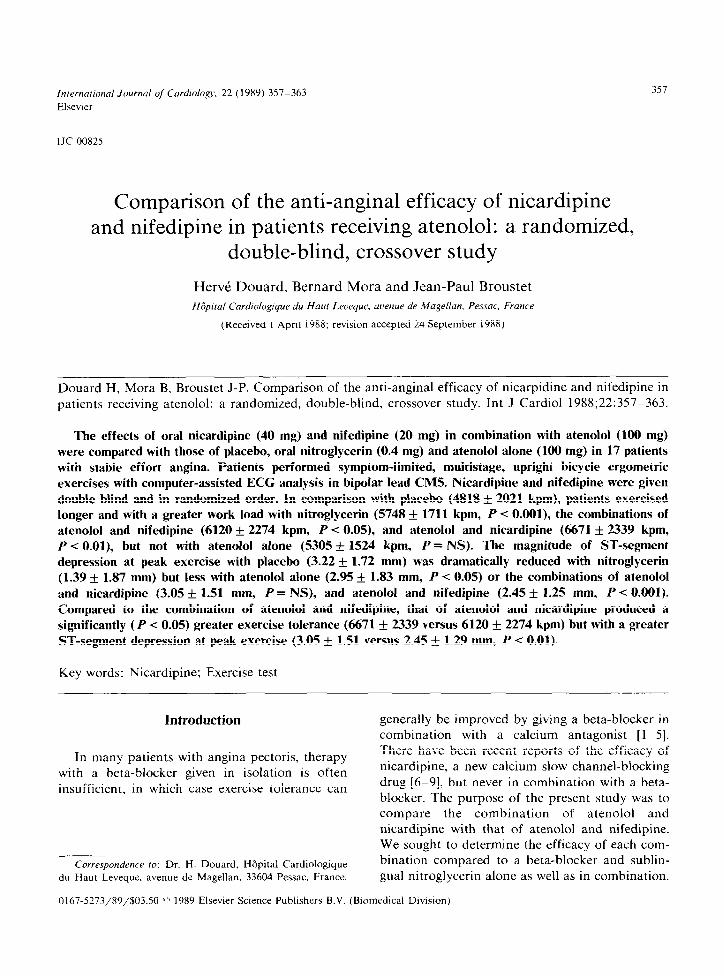
TABLE 3
Ergometric responsrs to treatment. ex. = sxucise: HR = heart rate: SBP = systoltc blood pressure: ST = ST-segment deprewon: W = exirraze
workload: PLA = placebo; NTG = suhllngual nitroglycerin; ATE = atenolol; NIF = nifedlpine: NIC = mcardipine. * P c 0.05; * * P c 0.01; * * * P < 0.001 compared to placebo: * P < 0.05; ++ I’ < 0.01 atenolol and nifedipmc versus atenolol and nicardipinu.
PLA PLA + NTG ATE ATE + NTG
HR (hrats/min) rat
HR (beata/min) peak ex.
HR (heats/mm)
(W = 3260 kpm)
SBP (mm Hg) rat
SBP (mm Hg) peak ex
HR.SBP double product
(x IO’) peak ex
Max W (kpm)
W (kpm) for HR = 100
Max ST (mV)
ST for HR = 100 hrats/min
(mV)
ST for W = 3260 kpm
(mV)
73 * 13
178 ? 20
95 f 21***
141 f 20 * * *
63 ir IO *** 75 + 19
112 f 19 *** 121 t IX *
11x i 16
144 i 14
189 i 22
17Y -i- 1Y **
129 i 17 ***
1x5 i 24
23.7 + 6.1 24.3 i 5.0
4818 f2012 5 748 *1711 ***
1 320 i 1008 1060 + 1685 *
3 32 * 1.12 139* I.87 ***
101 * 14 *** 103 + 16 ***
135 i 17 * 126 f 23 ***
171 i 2, A** 174 * 19 **
18.7 i 4.4 * * * 70.5 t 4.x **
5 305 * 1 524 6 522 + 1470 * * *
2465 ?I137 *** 2 72x +1531 **
2.Y5 + 1.83 * 13hI I.?? ***
1.16 + 0.x0 0.37 f 0.X6 * * 1.37 i 0.80 0.3’) i 0.76 * * *
2.41 i 1.01 I .04 + 1.02 *** 1.7x i 0.74 * * 0.40 I 0.60 * * *
NIF + ATE ATE ATE + NTG NIC’ + ATE
HR (hrats/min) rest
HR (beats/min) peak ex.
HR (brats/mm)
(W = 3260 kpm)
SBP (mm Hg) rest
SBP (mm Hg) peak ex
HR.SBP double product
(xlO’)prakex
Max W (kpm)
W (kpm) for HR = 100
Max ST (mV)
ST for HR = 100 heats/mln
CrnV)
ST for W = 3260 kpm
(rnV)
6X + 13 59 f 10 ***
119 * 20 + IIU + 1x ***
101 i 14 *** 97 + 13 ***
109 i 13 *** 127 * 16 **
156 k IX *** 165 i 23 ***
18.4 i 4.9 * * 17.7 * 4.x ***
6120 i2773 *’ 5 622 f 1994
2 803 *I322 *** 2 x25 t1014 ***
2.45 i 1.29 **++ 3.00 * 1.75
0.45 * 0.6X * * 1 so t 0.x1
72 * 14
119 * 1’) *
99 + 15 ***
117 * 12 ***
16X i 24 ***
19.7 + 56 **
6914 *2154 ***
2 YXX i2093 **
1 .h5 * 1.16 ***
U.61 + 0.x1 **
66 i IO*
123 i 20
103 + 1x ***
113 * 16 ***
162 i 73 ***
193 ?r 51**
6671 *2339 **
7 640 &- 1573 * *
3.05 * 1.51
0.75 f 0.90 * *
0.6Y k 0.77 ***** 1.3’) f 0.7Y *** 0.28 t 064 *** I .0x 2 O.Y6 * * *
4818 i_ 2012 tsn
3.05 + 1.51 mm, respectively, P = NS) on maxi- mal exercise end-point depression compared to placebo (3.22 + 1.72 mm).
5748 ? 1711 Kw
5305 ? 1524 KPM
6522 ? 1470 KPM
6671 ! 2339 KPY
5622 ? 1994 IKP
6914 : 2154 KPM
6120 : 2?74 Y:u
PLA , 1 1 -3.32 : 1.72
NTG 1::.::1 -1.39 2 1.87 1 1
N5
::::
i
ATE + NIF :.l 1
ATE+NTG -1.65 t 1.16
ATE+N IF -2.-i ! 1.25 Fig. 1. Maximal cardiac work performed on the
treatments. ATE = atenolol; NIC = nicardipine:
different NIF =
nifedipine; NTG = sublingual nitroglycerin; PLA = placebo;
* ** P < 0.001; ** P < 0.01: * P < 0.05. Fig. 1. ST-segment depression measured at the exercise end-
point. * * * P i 0 001: * * P i 0.01: * P < 0.05.

361
The greatest reduction in the electrocardio- graphic end-point of ischemia (P < 0.001) was achieved on nitroglycerin alone (1.39 + 1.87 mm) or in combination with atenolol (1.36 i 1.23 mm).
The “anti-ischemic potency” of a drug can be evaluated by measuring the ST depression at a given workload (3260 kpm); all test agents were active compared to placebo (2.41 f 1.01 mm), but the combination of atenolol and nitroglycerin was by far the most effective (0.40 + 0.60 mm, P -c 0.001). It was significantly superior to nitro- glycerin alone (1.04 i 1.02 mm, P -c O.Ol), and to the combinations of atenolol and nifedipine (0.69 k 0.77 mm, P -c 0.01) and atenolol and nicardi- pine (1.08 + 0.96 mm, P < 0.001).
At the same workload, the agent with the least depression-reducing effect was atenolol alone (1.78 + 0.74 mm).
Heart rate
At rest, a clear slowing was induced by atenolol compared to placebo: 59 k 10 versus 73 k 13 beats/min (P < 0.001).
On nitroglycerin alone, or in combination with atenolol. relative tachycardia was not caused just by the activity of nitroglycerin. In many cases, the patients had not fully returned to baseline status.
There was no significant difference between placebo and the combinations of atenolol and nicardipine or atenolol and nifedipine (66 _t 10 68 t_ 13 beats/min. respectively).
At the exercise end-point, the most significant increase in heart rate occurred on nitroglycerin (142 f 20 versus 128 + 20 beats/mm, P < 0.001). A highly significant reduction occurred with atenolol (112 Ifr 19 beats/mm, P < 0.001) and, to a lesser degree, with the combination of atenolol and nitroglycerin (121 f 18 beats/mm, P < 0.05).
There was no significant difference between placebo and the combinations of either atenolol and nicardipine or atenolol and nifedipine (121 + 20 and 119 f 20 beats/mm, respectively).
At the intermediate workload of 3240 kpm, the same time profiles were seen as at the exercise end-point: a very significant increase on nitro- glycerin (129 + 19 beats/min, P < 0.01); a very significant reduction on atenolol alone (101 k 144
beats/min, P -c 0.001). less so on atenolol and nitroglycerin (103 + 16 beats/mm, P < 0.001).
If there was no significant difference between atenolol and nitroglycerin (103 f 16 beats/min), atenolol and nicardipine (103 + 18 beats/min) or atenolol and nifedipine (101 & 14 beats/mm), all combinations induced significant bradycardia compared to placebo (P =c O.OOl), for the same given workload.
Systolic pressure
At rest, all test compounds significantly re- duced systolic pressure compared to placebo (144 + 14 mm Hg). The combinations of atenolol and nicardipine and atenolol and nifedipine did not differ significantly from one another (113 * 16 and 109 + 13 mm Hg, respectively) but were more effective than that of atenolol and nitroglycerin (126 & 13 mm Hg, P < 0.001) or atenolol alone (135 + 17 mm Hg, P -c 0.001).
At the exercise end-point. a significant dif- ference remained between atenolol and nitro- glycerin (174 f 19 mm Hg) and the combinations of atenolol and nicardipine (162 k 23 mm Hg) or atenolol and nifedipine (156 + 18 mm Hg, P < 0.001).
Heart rate-systolic pressure product
The above double product is an indirect reflec- tion of myocardial oxygen consumption. At the exercise end-point. the rate-pressure product was significantly reduced by all treatments (0.01 < P < 0.001). except nitroglycerin alone (24.3 i 5 versus 23.9 + 6.1). There was no difference be- tween the combinations of atenolol and nitrog- lycerin, atenolol and calcium-blocker or atenolol alone.
Discussion
Nicardipine is a dihydropyridine derivative structurally similar to nifedipine or nisoldipine [ll]. It acts as a vasodilator by affecting vascular smooth muscle, and has been shown to have effec- tive antihypertensive activity. Some studies have also reported its efficacy in the treatment of chronic stable angina, but never in combination

362
with beta-blockade [6-91. The value of such com- bination lies in the absence of any changes in sinus-node automaticity and atrioventricular con- duction induced by the calcium-channel blocker.
The protocol used in the present study is shorter than those generally used for the ergometric evaluation of anti-angina] agents. Some degree of muscle fatigue might be feared due to the close sequence of tests (eight exercise tests in three days per patient). The main limitation in all patients. however, was exertional angina in the absence of treatment (inclusion criterion) and peripheral muscle factors were probably little involved. On the other hand, a “training” effect from repeated testing might be feared in these patients, giving rise to spontaneous improvement in ergometric parameters [12,14]. Test reproducibility, evaluated by comparing the exercise tests performed on atenolol alone (nos. 3. 6) and atenolol + nitroglycerin (nos. 4, 7) was, nonetheless excellent. Thus, only eight paired r-tests of 36 were signifi- cant. Besides those due to first-order error. the differences were essentially in heart rate and sys- tolic pressure, the values of which were always lower on the second comparative test, indicating the probability of a cumulative dose effect of the beta-blocker. Nevertheless, no blood levels of atenolol were measured to confirm this hypothe- sis.
Conducting the tests at such short intervals, can also be justified by the very rapid elimination of nicardipine and nifedipine [3.5.6]. There are significant advantages to a short protocol. Treat- ment dosing is readily supervised. Patients are not lost to follow-up during the study. It eliminates any influence on the results of ergometric testing from coronary arterial disease and its possible deterioration over time. Exercise testing at a fixed time of day also eliminates factors due to circadian
variation. Work performance, reduction in ST depression
at the exercise end-point and maximal myocardial oxygen consumption, as estimated by the rate- pressure product, all significantly improved on monotherapy (nitroglycerin or beta-blockade) compared to placebo. Furthermore, additional im- provement occurred with the combination of nitroglycerin and beta-blockade or beta-blockade
and calcium antagonist, compared to anti-angina1 therapy using one drug alone. These results con- firm the value of anti-angina1 combination ther- apy in stable angina of effort [1,3.5].
Comparison between atenolol and nicardipine with atenolol and nifedipine
Although Table 2 shows no treatment-order interaction or order effect in the first four parame- ters analyzed (work performed, end-point ST de- pression. double product, maximal heart rate). it does show, at an approximately identical myocar- dial oxygen consumption, as evaluated by the double product, that the average work performed on atenolol and nicardipine (6671 + 2339 kpm) was significantly greater than that performed on atenolol and nifedipine (6120 i 2273 kpm, P < 0.05). The end-point of heart rate was significantly higher on atenolol and nicardipine (123 + 20 beats/min) than on atenolol and nifedipine (119 f 20 beats/min, P -c 0.02). The gain, however, was at the expense of a maximal depression that was also significantly greater (3.05 * 1.51 versus 2.45 + 1.25 mm, P < 0.01). Furthermore. ST-seg- ment depression measured at an equal workload was significantly greater (P < 0.01) on nicardipine than on nifedipine.
Comparison between the benefit of nicardipine and nitroglycerin in combination with atenolol
The most favorable mean parameter of the two exercise tests performed on atenolol and nitro- glycerin was used for comparison. Changes in the heart rate. systolic pressure and ST-segment at rest could not be used because the patients fre- quently performed the exercise test on nitro- glycerin and atenolol too soon after the test on atenolol alone. Work performed and rate-pressure product did not differ significantly, whereas work performed on atenolol and nifedipine (6120 k 2273 kpm) was significantly less than on atenolol and nitroglycerin (6914 f 2154 kpm, P < 0.01).
In contrast, ST-segment depression was very significantly less marked on atenolol and nitro- glycerin than on atenolol and nicardipine both at the exercise end-point (1.36 & 1.23 versus 3.05 +

363
1.51 mm, P < 0.001) and at an identical workload (0.28 k 0.64 versus 1.08 k 0.96 mm, P < 0.01). On atenolol and nicardipine, systolic blood pressure values were significantly lower at rest (113 -I_ 16 mm Hg) and at the exercise end-point (162 k 23 mm Hg) than on atenolol and nitroglycerin (126 k 13 mm Hg P -c 0.001; 174 f 19 mm Hg P < 0.01).
Combining nicardipine rather than sublingual nitroglycerin with atenolol thus appears less effec- tive from an anti-ischemic viewpoint, but prob- ably more effective from an anti-hypertensive viewpoint.
Conclusion
Nicardipine potentiates the effects of atenolol and allows patients much the same degree of exercise tolerance as that achieved with atenolol combined with sublingual nitroglycerin, a combi- nation which reliably produces an improvement in exercise tolerance and, more specifically, a reduc- tion in ST-segment depression, all the more strik- ing in that, for a given heart rate, depression is more marked on beta-blockers alone. On the other hand, improvement in ST-segment depression is less clear with atenolol and nicardipine than with atenolol and nitroglycerin.
Nicardipine significantly reduces systolic blood pressure both at rest and on exertion, suggesting that it probably lowers peripheral resistance. Compared to nifedipine (at an oral dose of 40 mg taken 1.5 h before exercise), nicardipine (20 mg) affords significantly greater exercise tolerance, un- explained by either a reduction in heart rate or blood pressure, but which is achieved at the ex- pense of increased ST-segment depression at the exercise end-point and an increased rate of angina-induced cessation. Thus, nicardipine as a complement to beta-blocker treatment for angina1 and probably hypertensive patients appears val- uable as judged from its acute administration al- though long-term studies are still required.
sorbide dinitrate in patients receiving propranolol: a dou- ble-blind study. Circulation 1983;68:568-575.
2 Hung J. Lamb IH. Connolly SJ. Jutzy KR, Gomis ML.
Schroeder JS. The effect of diltiazem and propranolol. alone and in combination, on exercise performance and left
ventricular function in patients with stable effort angina: a
double-blind, randomized, and placebo-controlled study.
Circulation 1983;68:560-567.
3 Morse JR, Nesto RW. Double-blind crossover comparison
of the antianginal effects of nifedipine and isosorbide di-
nitrate in patients with exertional angina receiving pro-
pranolol. J Am Co11 Cardiol 1985;6:1395-1401.
4 Schroeder JS. Hung J. Lamb IH, Connolly SJ, Jutzy KR.
Goris ML. Diltiazem and propranolol. alone and in combi-
nation, on exercise performance and left ventricular func-
tion in patients with stable effort angina: a double-blind.
randomized, and placebo-controlled study. Acta Pharmacol
Toxic01 1985:57(suppl 11):55-60. 5 Winniford MD. Fulton KL. Corbett JR. Croft CH. Hillis
LD. Propranolol-verapamil versus propranolol-nifedipine
in severe angina pectoris of effort: a randomized. double-
blind. crossover study. Am J Cardiol 1985;55:2Xll285.
6 Gelman JS. Feldman RL, Scott E, Pepine CJ. Nicardipine
for angina pectoris at rest and coronary arterial spasm. Am J Cardiol 19X5:56:232-236.
7 Khurmi NS, Bowles MJ, Subramanian VB. Raftery EB.
Short- and long-term efficacy of nicardipine. assessed by
placebo-controlled single- and double-blind crossover trials
in patients with chronic stable angina. J Am Co11 Cardiol
1984;4:908%917.
8 McGill D, McKenzie W, McCredie M. Comparison of
nicardipine and propranolol for chronic stable angina pec-
toris. Am J Cardiol 19X6:57:39-43.
9 Scheidt S. LeWinter MM. Hermanovich J. Venkataraman
K. Freedman D. Efficacy and safety of nicardipine for chronic, stable angina pectoris: a multicenter randomized
trial. Am J Cardiol 1986:5X:715-721.
10 Broustet JP. Emeriau JP, Guern P. Series E. Epreuve d’ef- fort en cardiologie. Rev Prat 1977;27:3129-3141.
11 Lam J, Chaitman BR, Crean P, Blum R, Waters DD. A
dose-ranging. placebo-controlled, double-blind trial of
nisoldipine in effort angina: duration and extent of anti-
angina1 effects. J Am Co11 Cardiol 1985;6:447-452.
12 Khurmi NS. Bowles MJ, Kohli RS. Raftery EB. Does
placebo improve indexes of effort-induced myocardial
ischemia? An objective study in 150 patients with chronic
stable angina pectoris. Am J Cardiol 19X6:57:907-911.
13 Weber JR. Problems associated with clinical evaluation of
antianginal medications. Am J Cardiol 1985:56:141-1X1. 14 Waters DD. McCans. JL. Crean PA. Serial exercise testing
in patients with effort angina: variable tolerance. fixed
threshold. J Am Co11 Cardiol 1985;6:1011-1015.
References
1 Bassan MM. Weiler-Ravel1 D, Shalev 0. Comparison of the antianginal effectiveness of nifedipine. verapamil and iso-