comparative antihypertensive effects of enalapril maleate and hydrochlorothiazide, alone and in...
TRANSCRIPT
J C/in Pharmacol. 1983; 23:227-233.
ComparativeAntibypertensiveEffectsof EnalaprilMaleateandHydrochiorothiazide,Aloneandin Combination
PETER H. VLASSES, Pharm.D., HESCHI H. ROTMENSCH, M.D.,BRIAN N. SWANSON, Ph.D., JOHN D. IRVIN, M.D., Ph.D., ROBYN B. LEE, M.S.,
JANICE R. KOPLIN, R.N., and ROGER K. FERGUSON, M.D.Philadelphia, Penn., and West Point, Penn.
Abstract: Enalapril maleate isan investigational oral prodrug whose hydrolyzed diacidmetabolite is a potent angiotensin-converting enzyme inhibitor. Fourteen patientswith mild to moderate hypertension were evaluated after receiving placebo, and twoweeks of treatment with each of the following: enalapril maleate (20 mg b.i.d.), hy-drochlorothiazide (25 mg b.i.d.), and the two in combination. In comparison toplacebo, the magnitudes of the blood pressure reduction after enalapril and hydro-
chlorothiazide alone were comparable. The reduction in blood pressure following enala-pril was evident throughout the 12-hour dosing interval. The combination of enalapril
and hydrochlorothiazide resulted in a marked further reduction in blood pressure thatwas greater than that predicted from the responses to the individual drugs (P <0.05).Biochemical parameters confirmed inhibition of angiotensmn-converting enzyme dur-
ing enalapril treatment: serum angiotensmn-converting enzyme activity proved anexcellent monitor of compliance. Enalapril was generally well tolerated. Adverseeffects included symptomatic hypotension in three patients when enalapril was firstadded to hydrochlorothiazide and hyperesthesia of the oral mucosa without a loss oftaste in one patient on enalapril. Enalapril maleate alone and especially in combinationwith hydrochlorothiazide appears to be an effective, well-tolerated converting enzyme
inhibitor with at least a 12-hour duration of action.
NALAPRIL maleate, N-(1-S-1-carbeth- chemical structure of captopril may ac-
.J__4 oxy-3-phenylpropyl)-S-alanyl-S-pro- count for some of its adverse effects such as
line (MK-421), is an investigational oral skin rash, loss of taste, proteinuria, and
prodrug whose hydrolyzed diacid form is a leukopenia. Enalapril, which lacks this moi-
potent angiotensin-converting enzyme ety, may have a more favorable benefit-to-
(ACE) inhibitor. The efficacy of this new risk ratio.
class of agents in the treatment of hyper- In a previous pilot study,2 we compared
tension and congestive heart failure has the antihypertensive and humoral effects of
been widely documented with use of capto- 5-and 10-mg once-daily doses of enalapril ma-
pril, the first marketed oral ACE inhibitor.’ leate with those of hydrochlorothiazide in
However, the sulfhydryl moiety of the small groups of patients. The purpose of the
From the Division of Clinical Pharmacology, Depart- present study was to evaluate the effects ofment of Medicine, Jefferson Medical College, Thomas a larger dose of enalapril maleate (20 mgJefferson University, Philadelphia, Penn., and Merck .
Sharp and Dohme Research Laboratories, West Point, b:1.d.), hydrochiorothiazide, and their com-Penn. (Dr. Irvin and Ms. Lee). bination.
May-June 1983 227

VLASSES, ROTMENSCH. SWANSON, ETAL.
228
Methods
Patients
Fourteen patients with mild to moderate
hypertension (untreated, sitting diastolic
blood pressure between 95 and 120 mm Hg)
entered and completed the study. The pa-
tients (12 men, two women, aged 35 to 69
years) were judged to have essential hyper-
tension on the basis of a thorough history,
physical examination and laboratory eval-
uation. No patient had severe end-organ
involvement. No other medications were
consumed during the study period. The pa-
tients were instructed to follow a daily 100
mEq sodium, 80 mEq potassium diet which
they were asked to maintain throughout
the study.
Experimental Design
After at least a two-week no-treatment
washout period, all patients were admitted
to the Clinical Pharmacology Unit and re-
ceived a single dose of placebo. Supine and
seated blood pressures and pulse rates were
measured at hourly intervals for 12 hours
by an automatic device using the Doppler
principle (DINAMAP). Blood was collected
from a forearm intravenous catheter for de-
termination of serum electrolytes, plasma
renin activity (PRA), serum ACE activity,
and plasma aldosterone concentration
(PAC) before and at 4,12, and 24 hours after
placebo administration. Urine was col-
lected for 24 hours for electrolyte and pro-
tein determinations.
In the previous pilot study,2 the treat-
ments were allocated in a double-blind,
randomized crossover manner. In this
study, a single-blind fixed-sequence, con-
secutive treatment design was employed to
allow for a careful assessment of the acute
and chronic responses of enalapril maleate
as well as an evaluation of the safety of
instituting enalapril therapy in a patient
previously treated with hydrochlorothia-
zide. Thus, subsequent to the baseline
placebo evaluation, each patient received
consecutively 14 days of each of the follow-
ing treatments: 20 mg enalapril maleate
twice daily, 25 mg hydrochlorothiazide
twice daily, and the combination of en ala-
pril and hydrochlorothiazide in these doses.
All drug supplies were provided by Merck
Sharp & Dohme Research Laboratories.
The patients were admitted to the Unit on
days 1 and 14 of each treatment, and study
procedures were performed exactly as on
the placebo day. Patients were carefully
evaluated for side effects. Medication diar-
ies, pill counts, and ACE determinations
(on enalapril treatments) were used to
assess outpatient compliance.
Laboratory Analysis
PRA, at pH 7.4, and PAC were measured
by radioimmunoassay methods as pre-
viously described.34 ACE activity was meas-
ured by a modified radioenzymatic method
which assesses the percentage of hippuryl-glycylglycine substrate metabolized per
minute per milliliter of serum.5 In our
laboratory, normal values (mean ± S.D.) for
PRA, PAC, and ACE are 1.6 ± 0.4 ng/ml/hr,
11 ± 4 ng/dl, and 5.4 ± 0.3% metabolized!
min/ml, respectively.
Statistical Analysis
The mean seated diastolic blood pressure
(SDBP) for the group was calculated at the
various time points. In addition, the overall
treatment effect for the group was charac-
terized by the mean of the average SDBP
over 12 hours for each patient (1-12-hour
SDBP). Mean seated pulse rate was eval-
uated in a similar manner. The 1-12-hour
time period was selected to minimize the
effect of variability in the 0-hour (predrug)
values which were determined upon an in-
dividual’s arrival to the Clinical Pharma-
cology Unit; this 1-12-hour time period al-
lows a more precise comparison of drug
effects versus placebo response under com-
parable conditions.
Analysis of variance using a general lin-
ear models approach was used to test for
treatment effects and interactions after
The Journal of Clinical Pharmacology

0SO 105
I
EE
0.
SO 95-
‘I’
z
85
75
PLACEBO
HCTZ
ENALAPRIL
ENA/HCTZ
0 4 8 10 12
TIME (hours)
ENALAPRIL ANTIHYPERTENSIVE EFFECTS
May-June 1983 229
removing subject effects. The presence of a
significant interaction indicates that the
evaluated effect during combination treat-
ment differs from the additive sum of the
effects of the individual treatments. Dun-
can’s multiple range test was used for com-
parison of individual treatments. All tests
were two-tailed and performed at the a =
0.05 level of significance.
Results
Blood Pressure and Pulse Rate
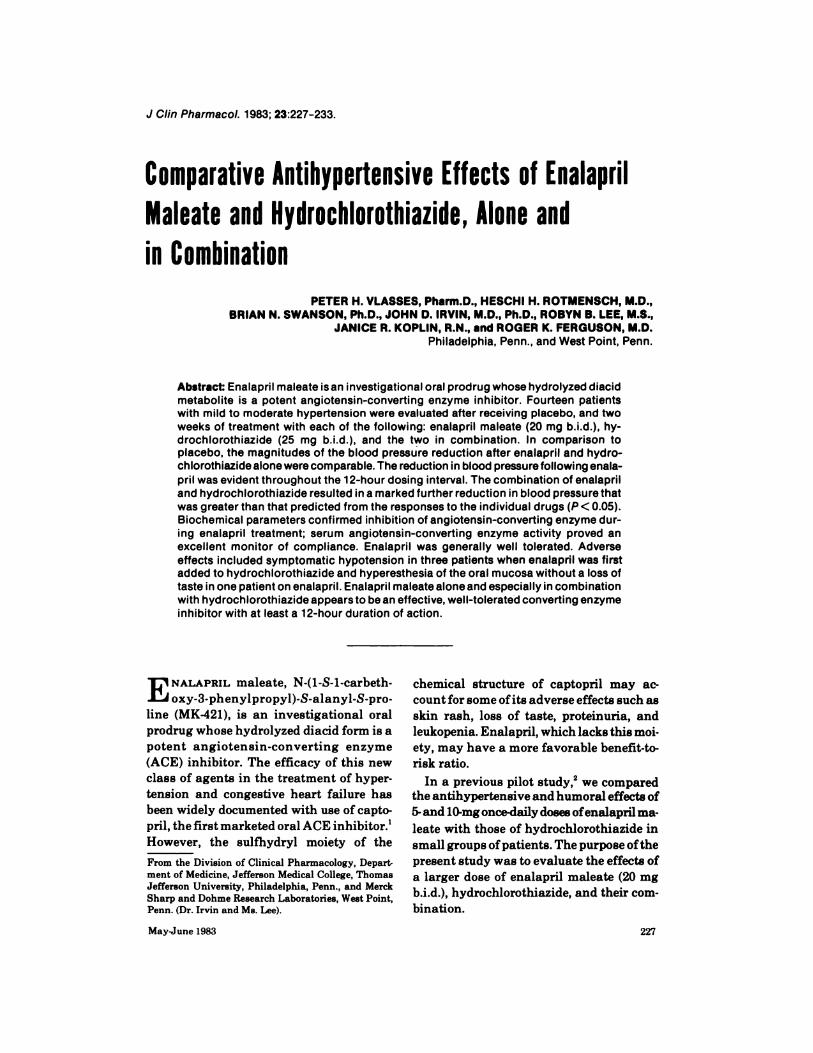
The time course of the mean SDBP for the
group after placebo and on the last day (day
14) of each treatment is depicted in Fig. 1.In
comparison to placebo, both enalapril ma-
leate and hydrochlorothiazide alone de-
creased mean SDBP significantly at most
time points. Mean (±S.D.) 1-12-hour SDBP
was 101 ± 5 mm Hg on placebo, 98 ± 8mm
Hg on enalapril, and 97 ± 8 mm Hg on
hydrochlorothiazide. The enalapril and
hydrochlorothiazide responses, though
small, differed significantly (P< 0.05) from
placebo but not from each other. Reduction
in mean SDBP with enalapril was evident
at 12 hours after dosing, and the days 1 and
14 responses were not significantly dif-
ferent.
In contrast, the mean SDBP on the com-
bination of enalapril and hydrochlorothia-
zide was significantly (P< 0.01) lower than
those on all other treatments at all time
points and persisted for 12 hours (Fig. 1).
The mean SDBP response on day 1 of com-
bination therapy (when enalapril was in-
itially added to hydrochlorothiazide) was
82± 7 mm Hg, which was not significantly
different from that on day 14 of this treat-
ment. Mean (±S.D.) 1-12-hour SDBP on day
14 was 85 ± 8 mm Hg, which was signifi-
cantly (P< 0.05) lower than those of all other
treatment. Blood pressure control (individ-
ual average 1-12-hour SDBP �90 mm Hg)
was achieved in two patients on enalapril,
in one on hydrochlorothiazide, and in 11
patients on the combination. Statistical
1 1 5-
ANTIHYPERTENSIVE EFFECTS OF ENALAPRIL,
HCTZ AND THEIR COMBINATION (n=14)
e
Fig. 1. Time course of the group (N = 14) mean seated diastolic blood
pressure (SDBP) after placebo (0 - - - 0) and on day 14 of treatment with
enalapril maleate (o-o), hydrochlorothiazide (s-s), and their combination(.-e) (refer to text for dosage).

8.
ENC
EN
.: .4’
E
00 4 12
25.
20.
N 15.SOC
V 10-
0.
5.
0.
1
10E
N
SOC
5.
0.
0 4 12
VLASSES, ROTMENSCH, SWANSON, ETAL.
230
BIOCHEMICAL EFFECTS OF ENALAPRIL,
HCTZ AND THEIR COMBINATION (n14)
TIME (hours)
Different from Placebo(s), Enalapril(t), All Treatments(#{149}) p’(0.05
Fig. 2. Changes in the group (N = 14) mean serum angiotensin-converting
enzyme (ACE) activity, plasma aldosterone concentration (PAC), and
plasma renin activity (PRA) at various times after treatment with placebo
(0 - - - 0) and on day 14 of enalapril maleate (0-0), hydrochlorothiazide
(s-.), and their combination (,-e) (refer to text for dosage).
analysis revealed a positive interaction (P
<0.01) between enalapril and hydrochioro-
thiazide when used in combination, indi-
cating an enhancement of the effect by the
combination. Similar treatment effects were
observed for mean supine diastolic as well
as mean sitting and supine systolic blood
pressures.
Mean (±S.D.) 1-12-hour seated pulse rate
(beats!min) was 78±9 on placebo and was
unchanged after enalapril either on day 1
(78 ± 10) orday 14(80 ± 12) of treatment. On
day 14 of hydrochiorothiazide, mean sit-
ting pulse rate was 84 ± 14, which was sig-
nificantly different from values on placebo.
On day 1 on the combination, though blood
pressure decreased markedly, no change in
pulse rate was evident (87 ± 14) in compari-
son to values on hydrochlorothiazide the
previous day. Interestingly, on day 14 of the
combination, though blood pressure re-
mained markedly decreased, the mean
pulse rate (80 ± 12) actually decreased in
relation to the value on hydrochlorothia-
zide and did not differ significantly from
placebo values.
Humoral and Electrolyte Effects
Mean ACE, PRA, and PAC before and at
various times after dosing on the last day of
each treatment are depicted in Fig. 2. Sig-
nificant marked decreases in mean ACE
(Fig. 2, left panel) at all time points in com-
parison to placebo values were seen on day
14 of treatment with both enalapril alone
and in combination with hydrochiorothia-
zide (P < 0.01). Mean ACE values during
hydrochlorothiazide treatment were com-
parable to those after placebo. In compari-
son to placebo, enalapril alone tended to
decrease mean PAC, while hydrochlorothi-
azide alone significantly increased this pa-
rameter (Fig. 2, middle panel). Mean PAC
on the combination returned toward, though
did not differ significantly from, placebo
values. Although increases in mean PRA
(Fig. 2, right panel) from placebo values
The Journal of Clinical Pharmacology

ENALAPRIL ANTIHYPERTENSIVE EFFECTS
May-June 1983 231
were seen with all treatments, only those
after combination therapy achieved statis-
tical significance. Humoral responses on
day 1 of treatment with enalapril, alone or
with hydrochiorothiazide, were similar to
those on day 14 of each treatment. No corre-
lation existed between the pretreatment
PRA and the change from placebo in 1-12-
hour SDBP after enalapril alone.
Mean serum electrolyte, uric acid, and
creatinine values on the morning of the last
day of each treatment are depicted in Table
I. In comparison to enalapril, hydrochioro-
thiazide resulted in decreases in serum pot-
assium and chloride concentrations and an
increase in serum uric acid concentrations.
The addition of enalapril to hydrochioro-
thiazide tended to reverse the changes in
serum potassium and chloride.
Adverse Effects
When enalapril was added to hydrochioro-
thiazide, three of the 14 patients ex-
perienced marked reductions in SDBP ac-
companied by dizziness. In one patient, the
symptoms resolved over the first 24 hours.
In the other two patients, because symp-
toms persisted, the daily dosage was de-
creased (20 mg enalapril and 25 mg hy-
drochlorothiazide) with subsequent im-
provement. The study data (Fig. 1) include
the responses of these patients at the lower
dosage, the character of which was similar
to that of other patients. Whether the dos-
age reduction in fact contributed to the im-
proved tolerance is unclear. One patient
experienced hyperesthesia (“scalded
mouth”) of the oral mucosa during treat-
ment with enalapril, both alone and in
combination with hydrochiorothiazide,
which resolved with discontinuation of
treatment.6 Two patients complained of de-
creased libido on all active treatments. No
skin rash, leukopenia, or proteinuria was
noted.
Discussion
In these patients, two weeks of treatment
with enalapril maleate or hydrochlorothia-
zide alone lowered SDBP comparably in
comparison to placebo. The mean reduc-
tions in SDBP from placebo values, though
significant, were modest. These responses,
especially with hydrochlorothiazide, may
be related to recruitment of an inherently
more resistant group of patients, the dura-
tion of treatment, or to the fact that treat-
ment effects were compared to the placebo
response (Fig. 1) rather than to the un-
treated SDBP. The mean blood pressure re-
sponses on days 1 and 14 of enalapril were
comparable, and the reduction in blood
pressure was evident throughout the 12-
hour dosing interval. In comparison to our
TABLE I
Mean Serum Electrolyte, Uric Acid, and Creatinine Concentrationson the Last Day of Each Treatments
TreatmentSodium
(mEq/liter)Potassium(mEq/liter)
Chloride(mEq/liter)
Uric acid(mg/dl)
Creatinine(mg/dl)
Placebo 144 3.9 109 5.5 1.1
Enalapril (20mg b.i.d.) 142 4.0 108 6.3 1.0
Hydrochlorothiazide
(25mg b.i.d.) 143 3.7” 103bb.,8...bb
Combination 143 3.9 106b 765*.bb
* a,aa = Different from enalapril, P< 0.05 and 0.01, respectively; b,bb = different from placebo, P <0.05 and 0.01,
respectively; c = different from combination, P < 0.05.

VLASSES, ROTMENSCH, SWANSON, ETAL.
232 The Journal of Clinical Pharmacology
experience with captopril at similar doses,
enalapril had a slower onset and a longer
duration of action.
Enalapril alone significantly lowered ACE
and tended to decrease PAC and increase
PRA. Measurement of serum ACE was an
excellent predictor of compliance with enal-
april treatment, either alone or in combi-
nation with hydrochlorothiazide. This
differs from captopril which chemically de-
grades rapidly after sample collection,
making measurement and interpretation of
serum ACE values difficult.9 Though the
biochemical effects observed are consistent
with angiotensin-converting enzyme inhi-
bition, the SDBP response to enalapril
alone was not related to the pretreatment
PRA. In combination, enalapril tended to
lower the increased PAC observed after hy-
drochlorothiazide alone. Interestingly, the
response to the enalapril!hydrochlorothia-
zide combination was of a greater magni-
tude than that predicted statistically from
the individual responses.
Theoretically, in the fixed-sequence, con-
secutive treatment design employed in this
study, the duration of treatment could have
contributed to an enhanced antihyperten-
sive response in the last treatment period.
Likewise, if the SDBP response to hydro-
chlorothiazide alone was not maximal after
two weeks of treatment, then the subse-
quent response to the combination with
enalapril may have appeared more than
additive. However, these factors do not
adequately explain the enhanced SDBP re-
sponse to enalapril/hydrochiorothiazide as
the blood pressure response was at least as
good on the first as on the last day of treat-
ment with the combination. Furthermore,
an enhanced effect of the combination of
enalapril and hydrochiorothiazide was
suggested in our previous double-blind,
randomized order of treatment pilot study
with lower doses of enalapril (5 and 10 mg
daily)2 indicating that the fixed-treatment
sequence of the present study is not the rea-
son for the enhanced effect.
One possible explanation for the enhanced
effect of the combination was that after in-
itial treatment with hydrochlorothiazide,
the blood pressure of these patients was
more dependent on the renin-angioten-
sin-aldosterone axis, as evidenced by the
increases in PRA and PAC. Thus, inhibi-
tion of this system with enalapril during
combination treatment might account for
the additional antihypertensive effect. It is
interesting to note, however, that the anti-
hypertensive effects of the combination of
captopril and hydrochiorothiazide, in our
previous experience7 and consistent with
the findings of others8’9 are additive and do
not suggest the enhanced response evident
for the combination of enalapril and hy-
drochiorothiazide in the present study. The
reason for this apparent discrepancy is un-
clear and warrants further investigation.
Several interesting differences were noted
between the effects of enalapril maleate
and hydrochlorothiazide. In comparison to
placebo values, sitting pulse rate increased
after hydrochiorothiazide, as commonly
seen after diuretic treatment, but was un-
changed after enalapril. More importantly,
when enalapril was added to hydrochloro-
thiazide, though blood pressure fell
markedly, heart rate did not increase
further. In fact, by day 14 of the combina-
tion treatment, although the blood pressure
reduction was maintained, heart rate had
actually decreased toward placebo values.
Whether this decrease in heart rate would
have accompanied the continued treatment
with hydrochiorothiazide or was caused by
enalapril is unclear. Of note, however, is
that the lack of effect of captopril on pulse
rate has been attributed in part to para-
sympathomimetic and/or sympatholytic
effects of this agent.1”#{176}
As expected, hydrochlorothiazide de-
creased serum potassium and chloride con-
centrations, presumably due in part to the
concomitant increase in serum aldosterone
concentrations. Enalapril alone had no ef-
fect on serum potassium and, in combina-
tion with hydrochlorothiazide, tended to
correct the electrolyte changes while

ENALAPRIL ANTIHYPERTENSIVE EFFECTS
May-June 1983 233
decreasing plasma aldosterone concentra-
tions. Hydrochlorothiazide, but not enala-
pril, increased serum uric acid concen-
trations.
During this short-term study, enalapril
maleate and hydrochiorothiazide were gen-
erally well tolerated; no skin rash, leukope-
nia, or proteinuria occurred. When enalapril
was added to hydrochlorothiazide, marked
symptomatic falls in blood pressure oc-
curred in three patients. Because of this,
careful monitoring is indicated when enal-
april is added to the regimen of diuretic
treated patients. However, in our previous
pilot study, when hydrochlorothiazide was
added to enalapril, a comparable SDBP re-
sponse to the combination resulted after
chronic treatment but the reduction was
more gradual and asymptomatic.2 Revers-
ible hyperesthesia of the oral mucosa oc-
curred in one patient during enalapril
treatment; this side effect has also been de-
scribed in captopril-treated patients in our
unit.2
References
1. Vlasses PH, Ferguson RK, Chatterjee
K. Captopril: clinical pharmacology
and benefit-to-risk ratio in hyperten-
sion and congestive heart failure.
Pharmacotherapy. 1982; 2:1-17.
2. Ferguson RK, Vlasses PH, Irvin JD,
Swanson BN, Lee RB. A comparative
pilot study of enalapril, a new con-
verting enzyme inhibitor, and hy-
drochlorothiazide in essential hyper-
tension. J Clin Pharmacol. 1982;
22:281-289.
3. Haber E, Koerner D, Page LB, Kliman
B, Purnode A. Application of a ra-
dioimmunoassay for angiotensin I to
the physiologic measurement of
plasma renin activity in normal
human subjects. J Clin Endocrinol.
1969; 29:1349-1355.
4. Ito T, Woo ,J, Haning R, Horton R. A
radioimmunoassay for aldosterone in
human peripheral plasma including a
comparison of alternate techniques. J
Clin Endocrinol. 1972; 34:106-112.
5. Swanson BN, Hichens M, Mojaverian
P, Ferguson RK, Viasses PH, Dudash
M. Angiotensin converting enzyme
activity in human serum: relation-
ship to enzyme inhibition in vivo and
in vitro. Res Comm Chem Path Phar-
macol. 1981; 33:525-536.
6. Vlasses PH, Sheaffer SL, Rotmensch
HH, Ferguson RK. “Scalded-mouth”
from angiotensin converting enzyme
inhibition. Br Med J. 1982; 284:
1672-1673.
7. Ferguson RK, Vlasses PH, Swanson
BN, Mojaverian P, Koplin JR. Com-
parison of the effects of captopril, diu-
retic and their combination in low-
and normal-renin essential hyperten-
sion. Life Sci. 1982; 30:59-65.
8. Johnston CI, McGrath BP, Millar JA,
Matthews PG. Long-term effects of
captopril (SQ 14225) on blood pres-
sure and hormone levels in essential
hypertension. Lancet. 1979; 2:
493-495.
9. Swartz SL, Williams GH, Hollenberg
NK, Crantz FR, Moore TJ, Levine L,
et al. Endocrine profile in the long-
term phase of converting-enzyme in-
hibition. Clin Pharmacol The rap.
1980; 28:499-508.
10. Imai Y, Abe K, Sato M, Haruyama T,
Hiwatari M, Goto T, et al. Evaluation
of the chronotropic property of capto-
pril in hypertensive patients. Am
Heart J. 1982; 104:1339-1345.
Requests for reprints to: Peter H. Vlasses, Pharm.D.,
Clinical Pharmacology (M-502), Thomas Jefferson
University, 11th and Walnut Streets, Philadelphia,Penn. 19107.