community pharmacy benchmarking …...dr. nour hanah othman chief pharmacist hospital kuala lumpur...
TRANSCRIPT

COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division2
COMMUNITY PHARMACY BENCHMARKING GUIDELINESecond Edition2016
This benchmarking guideline serves as a set of standards that needs to be complied with for the purpose of community pharmacy practice set up, training activities (under-graduate / pre-registration), audits and complementing the licensing requirement. The facilities should project a professional image befitting the roles of community pharmacists without compromising the occupational and safety requirements.
A checklist on benchmarking audit of community pharmacies is also included in this edition to allow community pharmacies to conduct self-audits in order to ensure adherence to proper practice and requirements.
Pharmaceutical Services DivisionMinistry of Health MalaysiaLot 36, Jalan Universiti46350 Petaling JayaSelangor, Malaysia.
Website: www.pharmacy.gov.my
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 3
ACKNOWLEDGEMENT
Dr. Salmah binti BahriSenior Director of Pharmaceutical Services Division
Ministry of Health
Tn. Hj. Yunos bin ShaariPharmacy Board Malaysia
Ministry of Health
Fuziah Abdul RashidPharmacy Board Malaysia
Ministry of Health
Salwati Abd KadirPharmacy Board Malaysia
Ministry of Health
Hanisah ShafiePharmacy Board Malaysia
Ministry of Health
Datcayani a/p Ramadoo @ DevuduPharmacy Board Malaysia
Ministry of Health
Dr. Nour Hanah OthmanChief Pharmacist
Hospital Kuala Lumpur
Salbiah Mohd. SallehPharmacy Practice and Development Division
Ministry of Health

COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division4
Rosminah Mohd. DinPharmacy Practice and Development Division
Ministry of Health
Fatimah Abdul RahimPharmacy Practice and Development Division
Ministry of Health
Datin Dr. Faridah Aryani Md. YusofNational Pharmaceutical Regulatory Agency
Ministry of Health
Saimah Mat NoorPharmacy Practice and Development Division
Ministry of Health
Wan Mohaina Wan MohammadNational Pharmaceutical Regulatory Agency
Ministry of Health
Noraini MohamadPharmacy Practice and Development Division
Ministry of Health
Fatkhiah KhalilPharmacy Policy and Strategic Planning Division
Ministry of Health
Ainul Salhani Abdul RahmanPharmacy Policy and Strategic Planning Division
Ministry of Health
Rosliza LajisPharmacy Practice and Development Division
Ministry of Health
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 5
Nur Sufiza AhmadPharmacy Practice and Development Division
Ministry of Health
Nurul Adha OthmanPharmacy Practice and Development Division
Ministry of Health
Wan Utma Sapini Wan Abdul SamadPharmacy Practice and Development Division
Ministry of Health
Phuar Hsiao LingPharmacy Practice and Development Division
Ministry of Health
Hammira Abdul RazakPharmacy Practice and Development Division
Ministry of Health
Rosilawati AhmadNational Pharmaceutical Regulatory Agency
Ministry of Health
Nurul Fajar Mohd JamidNational Pharmaceutical Regulatory Agency
Ministry of Health
Azlina IsmailNational Pharmaceutical Regulatory Agency
Ministry of Health
Adnan SaliminPharmacy Enforcement Division
Ministry of Health
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division6
Asniza AliasPharmacy Enforcement Division
Ministry of Health
Hariah Mohd DerusPharmacy Enforcement Division
Ministry of Health
Siti Mariaton Abd MoksinPharmacy Enforcement Division
Ministry of Health
Amrahi BuangMalaysian Pharmaceutical Society (MPS)
Prof. Dr. Mohamed Azmi Ahmad HassaliSchool of Pharmaceutical Sciences
Universiti Sains Malaysia
Andrew TanMalaysian Pharmaceutical Society (MPS)
Datin Mariani Ahmad NizaruddinMalaysian Pharmaceutical Society (MPS)
Keh Song HockMalaysian Pharmaceutical Society (MPS)
Wan Hwei YenMalaysian Pharmaceutical Society (MPS)
Wong Sie SingMalaysian Community Pharmacy Guild (MCPG)
Lovy BehMalaysian Community Pharmacy Guild (MCPG)

COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 7
Loh Peng YeowMalaysian Community Pharmacy Guild (MCPG)
Hj. Abdul Rahman Lim AbdullahMalaysian Community Pharmacy Guild (MCPG)
Chin Kim LinMalaysian Community Pharmacy Guild (MCPG)
Ewe Kheng HuatPharmaceutical Association of Malaysia (PhAMA)
Cheah Ming LoongMalaysian Organisation of Pharmaceutical Industries (MOPI)
Sabrina HaronMalaysian Organisation of Pharmaceutical Industries (MOPI)
Lim Teng ChyuanMalaysian Association of Pharmaceutical Suppliers (MAPS)
Dr. Choe Tong SengMalaysian Association of Pharmaceutical Suppliers (MAPS)
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division8
TABLE OF CONTENTS
1.0 INTRODUCTION 09
2.0 MANAGEMENT 09
3.0 PREMISES 103.1 Location 103.3 Signboard & Advertisement 103.4 Facilities 113.5 Occupational and safety requirements: 123.6 References 15
4.0 PRACTICE 164.1 Service 164.2 Type of products 174.3 Personnel 174.4 Storage of medicines 184.5 Safety Measures 194.6 Record 194.7 Operating Hours 19
5.0 STANDARD OPERATING PROCEDURE 195.1 Counseling and Dispensing Medicines 195.2 Response to Minor Health Problems/Sales of
Pharmacy Medicines (Self-care) 195.3 Self-monitoring Devices 215.4 Health Screening 225.5 Extemporaneous Dispensing 225.6 Knowledge of Genuine and Counterfeit drugs, OTC and herbal supplements 23
Appendix I 25Appendix II 31Appendix III 32Appendix IV 33Appendix V 34Appendix VI 35
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 9
COMMUNITY PHARMACY BENCHMARKING GUIDELINE
1.0 INTRODUCTION
This benchmarking guideline serves as a set of standards that needs to be complied with for the purpose of community pharmacy practice set up, training activities (under-graduate / pre-registration), audits and complementing the licensing requirement.
The purpose of this guideline is to ensure the quality of the community pharmacy practice for the benefit of consumer/ patients.
For the purpose of this guideline, the community pharmacy is defined as a premise with at least one pharmacist holding a Type A license issued under the Poisons Act 1952 who can supply/sell poison either by retail only or by both retail and wholesale.
This guideline is subject to other laws/acts enforced in Malaysia.
2.0 MANAGEMENT
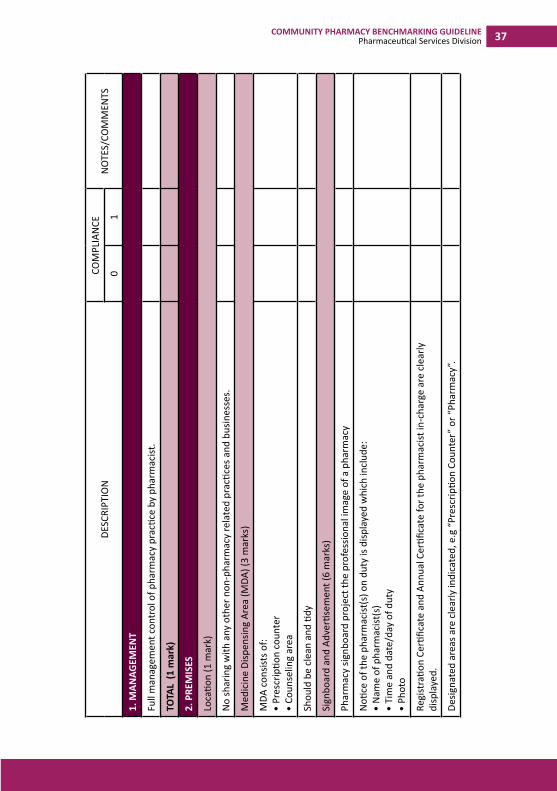
The community pharmacist should have full management control of the pharmacy practice.
The community pharmacist should:•• have full management control of the pharmacy practice•• have significant representation in executive board and
possess share equity•• inform any changes in shareholding to the Licensing
Officer and/or any other relevant authorities
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division10
3.0 PREMISES
3.1 Location
The premises are located within the management of the Local Council, where appropriate.
Pharmacies need to comply with the Local Authority laws.
The pharmacy premise cannot be shared with any other non-pharmacy related practices and businesses (including Multi-Level Marketing business)
Under certain circumstances where sharing of premise is unavoidable, the following conditions must be complied with:•• Full separation with no access allowed between the
different businesses in the same premises•• Should have different access points and clear signage•• Different business entities•• Each premise has its own staff
3.2 Medicine Dispensing Area (MDA)
The MDA should:•• be a minimum of 18 square meter (193 sq. ft) •• consist of:
ØPrescription counterØCounseling area ØMedicines preparation area (dry and wet
compounding)•• Screening tests area
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 11
3.3 Signboard & Advertisement Pharmacy signboard must project the professional image of a pharmacy.
No advertisement is permitted on any pharmacy signboard. This applies to signboards of both existing and new pharmacy businesses.
Any form of products advertisements displayed to public must be in accordance with the relevant legislations/guidelines.
The types of services offered should be displayed clearly inside the premises.
Examples of services are:•• Blood Glucose Test•• Certified Smoking Cessation Service Provider Program
(CSCSP)•• Urine Pregnancy Test•• Electronic blood pressure monitoring (Other service(s)
displayed is subjected to the relevant legislations)
Notice of the pharmacist(s) on duty to be displayed must include:•• Name of pharmacist(s)•• Time and date/day of duty•• Photo
Registration Certificate and Annual Certificate for the pharmacist in-charge should also be displayed clearly.
“No Smoking” and “No Vaping” signs must be displayed prominently to promote healthy lifestyle.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division12
Designated areas are indicated clearly, such as “Prescription Counter” or “Pharmacy”.
Pharmacies are encouraged to use the community pharmacy logo.
3.4 Facilities
Drugs and merchandises should be displayed in a neat and tidy manner thus projecting a professional image.
Pharmacist office (optional).
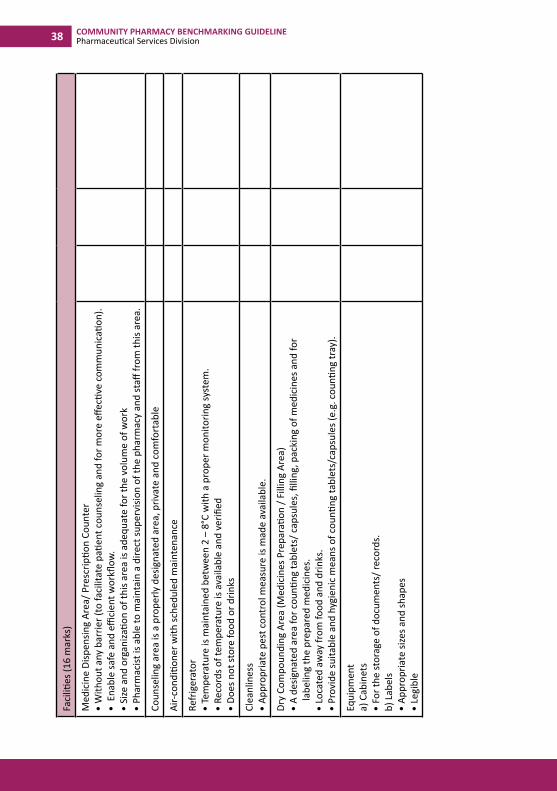
Medicine Dispensing Area/ Prescription Counter•• Preferably without any barrier to facilitate patient
counseling and for more effective communication.•• Enable safe and efficient workflow.•• Pharmacist should be able to maintain a direct supervision
of the pharmacy and staff from this area.•• Size and organization of this area should be adequate for
the volume of work. Counseling area must be a properly designated area, private and comfortable.•• If it is a room, the door should be made of half glass
Waiting area•• Comfortable with adequate space for customers.
Lighting and ventilation•• Ensure adequate lighting to reduce risk of medication
errors.•• Bright white fluorescent lights are preferred to filament.
Noise level•• Acceptable noise level - may have soft background music.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 13
Air-conditioner with scheduled maintenance to ensure the stability of medicines and for the comfort of staff and customers.
Refrigerator•• Should be maintained at temperature between 2 – 8°C
with a proper monitoring system.•• Daily temperature reading must be recorded and verified.•• Appropriate action should be taken to rectify any
problems identified.•• Do not store food or drinks in the refrigerator used for
the storage of medicines.
Cleanliness•• There should be appropriate pest control measure. •• Daily cleaning to maintain the pharmacy in a tidy and
dust free state.•• Regular cleaning of merchandise.•• Written cleaning procedures and schedules should be set
out and made available.
Medicines Preparation Area•• A washbasin with water supply should be available, other
than in the toilet.
a) “Wet Compounding Area” (for the purpose of extemporaneous preparations only)
•• A designated area with sink and water supply.•• Should be away from food and drinks.•• All working surfaces and shelves should have a smooth
impervious surface and washable material finishing.•• Wet compounding area must be equipped with the
following, if applicable:
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division14
i. Weighing scale- Regular verification and calibration by relevant
bodies are required to ensure reliability and efficiency
ii. Mortar and pestle - Must be maintained in good condition.
iii. Tile/glass slabs with spatula - Must be maintained in good condition.
iv. Measuring appliances - Must be maintained in good condition.
b) “Dry Compounding Area” •• A designated area for counting tablets/ capsules, filling
and packing of medicines. Also for labelling the prepared medicines.
•• Should be away from food and drinks.•• Provide suitable and hygienic means of counting tablets/
capsules (e.g. counting tray). Health Screening Area•• Equipped with appropriate equipment and devices.•• Equipment and devices in reliable conditions at all times.•• Water closet (optional)
Equipmenta) Computerized system (where available) preferably with
the following functions:•• Pharmacy Information Software •• Inventory/Stock keeping•• Printing of labels •• Printing of customer information leaflet•• Keeping of patient medication record •• Itemised billing with GST function•• Appropriate drug naming system
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 15
b) Printer (where available) preferably with the following functions:•• For the production of labels, leaflets or any printed
materials.
c) Cabinets•• For the storage of documents/ records.
d) Labels•• Appropriate sizes and shapes•• Preferably printed to prevent/ minimize errors due to
illegible •• handwriting
Other Requirements (optional)•• Entrance should be accessible to wheelchairs and
pushchairs.•• Pantry area for staff.•• Adequate toilet facilities, clean and in good condition.•• Arrangement must be made for the regular collection and
safe disposal of pharmaceutical waste and other refuse.
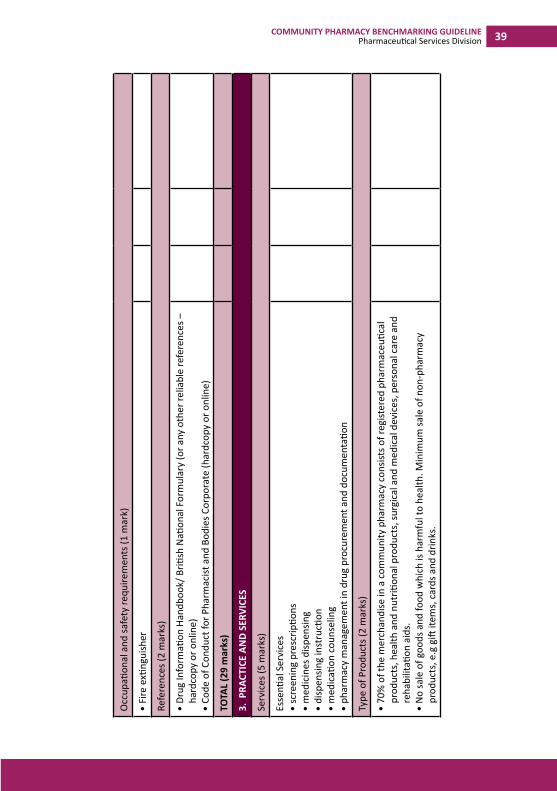
3.5 Occupational and safety requirements: The premises should be safe for the public and staff working in the pharmacy. Must comply with all statutory requirements where appropriate: •• Appropriate fire escape way•• Fire alarm •• Fire extinguisher •• Occupier’s indemnity
3.6 References The following references should be available:
•• British National Formulary or Australian Formulary•• Code of Conduct for Pharmacist and Bodies Corporate•• All relevant pharmacy legislations.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division16
Optional:
•• Martindale•• MIMS
4.0 PRACTICE
4.1 Service
Essential services•• Screening of prescription(s)•• Dispensing of medicines•• Compounding of medicines (patient specific)•• Counseling and advisory •• Monitoring and screening tests•• Pharmacy management in drug procurement•• Proper documentation
Optional ServicesMedication review and accredited pharmacy services including:•• Home Medication Review (HMR)•• Medication Therapy Adherence Clinic (MTAC) •• Certified Smoking Cessation Service Provider (CSCSP)•• Weight management •• Health screening•• Any other certified pharmaceutical care services
4.2 Type of products
70% of the merchandise in a community pharmacy should consist of registered pharmaceutical products, health and
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 17
nutritional products, surgical and medical devices, personal care and rehabilitation aids.
Sale of goods and food which is harmful to health is strictly prohibited. Non-pharmacy products, e.g gift items, cards and drinks, should be minimised.
4.3 Personnel
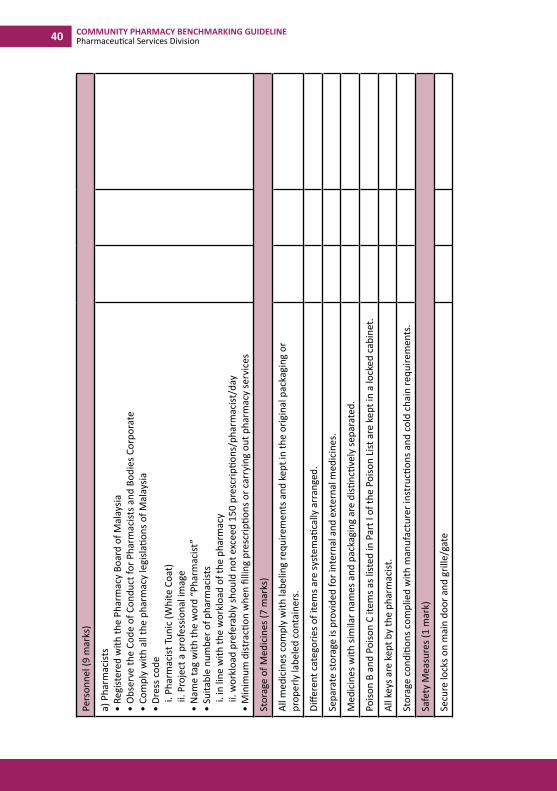
a) Pharmacists•• Registered with the Pharmacy Board of Malaysia•• Observe the Code of Conduct for Pharmacists and Bodies
Corporate•• Comply with all the pharmacy legislations of Malaysia•• Dress code
i. Pharmacist Tunic (White Coat) ii. Must project a professional image
•• Name tag should have the word “Pharmacist”•• Ratio of pharmacist to prescription should not exceed 80
to 100 prescriptions per pharmacist per day•• Notice and photograph of the pharmacist on duty must
be displayed with the duty hours
b) Pharmacy Assistants •• Diploma in Pharmacy are preferred•• Undergo structured training •• Suitable number of personnel
ØThe roles of the pharmacy assistant are to help in the preparation of medicines to be dispensed. They are not allowed to dispense scheduled poisons without a pharmacist.
4.4 Storage of medicines
All medicines must comply with labelling requirements and
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division18
should be kept in the original packaging or properly labeled containers.
Different categories of items should be systematically arranged.
Separate storage should be provided for internal and external medicines. Medicines with similar names and packaging should be distinctively separated to prevent dispensing errors.
All scheduled poisons under the Poisons Act 1952 must be stored in accordance with the legislations.
Poison B and Poison C items as listed in Part I of the Poison List should be kept in a locked cabinet to prevent access to customers and unauthorised personnel.
Psychotropic drugs/ dangerous drugs must be kept according to Regulations 24, Poison (Psychotropic Substances) Regulations 1989 whereas Dangerous Drugs should be kept according to Regulations 9(2) Dangerous Drugs Regulations 1952. A separate, safe and locked cabinet should be used for storage of psychotropic substances and dangerous drugs away from other goods/medicines.
All keys must be kept by the pharmacist.
Storage conditions must comply with manufacturer instructions and cold chain requirements where relevant.
Refer to Guidelines on Good Distribution Practice (GDP)
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 19
4.5 Safety Measures
•• Secure locks on main door and grille/gate.•• Secure locks on back doors and grille/gate if applicable.•• Electronically controlled locks may be utilised. •• Additional safety control such as video cameras and
alarm system are advisable.•• Policy for appropriate security should be arranged.•• To comply with relevant statutory requirements.
4.6 RecordRecords and documentations should be kept and updated systematically as stipulated by the law.
4.7 Operating Hours Minimum 40 hours/week with pharmacist
5.0 STANDARD OPERATING PROCEDURE
5.1 Counseling and Dispensing MedicinesRefer to Guide to Good Dispensing Practice (GDsP)
5.2 Response to Minor Health Problems/ Sales of Pharmacy Medicines (Self-care)
This applies to situations where the customer/patient comes to the pharmacy to consult the pharmacist on a minor health problem or request to purchase a pharmacy medicine or an over-the-counter medicine by name.
All pharmacy staff must be adequately trained. They should also know when to refer the customer to the pharmacist. Pharmacists and their staff must be aware of the potential of misuse for certain non-prescription medicines and should not supply when there are reasonable grounds for suspecting misuse/wrongful use.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division20
Pharmacy should have an area for confidential conversation with the patient/customer.
Pharmacists should counsel/ assess the health problem after obtaining sufficient information on the following:•• Who has the problem: if a child, the age of the child is
required•• What are the problems•• How long has the condition existed•• Action already taken•• Medicines already used for the problem•• Medical history: allergies, other existing health problems
and medication history•• To rule out possible underlying serious acute diseases•• When to refer to a medical practitioner or other health
professionals, with a referral note (refer to Appendix IV).
After the assessment, the pharmacist should:•• Differentiate minor ailments from major diseases•• Minimize risk factors and complications•• Offer appropriate advice (non-pharmacological and/or
pharmacological)•• Counsel patient/customer on the efficacy and safety of
the medicine(s) recommended•• Refer patient/customer to a medical practitioner or other
Health care professionals when appropriate.
When counseling patient:•• Make sure the patient knows/understands the objective
of the treatment.•• Go through the treatment as to why, what, when and
how to use The medicine(s).•• Advise on non-pharmacological treatment when
appropriate.•• Advise on possible side-effects and contraindications.•• If symptoms persist, the patient should be advised to see
a Medical practitioner with a referral note.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 21
Documentation Proper documentation should be maintained to fulfill legal and professional requirements. Preferably, the pharmacy should maintain patient medication record:•• To check the progress of the treatment and provide
information on the medical history of the patient.•• To be kept in pharmacy computer systems or in manual
records.•• Should be pertinent, accurate, up-to-date, stored
securely and treated as confidential and used only for the purpose for which it is obtained.
Labelling Refer to Guide to Good Dispensing Practice (GDsP)
5.3 Self-monitoring Devices
Pharmacist should give full information to the patients on the use of the self-monitoring devices and the frequency of measurement.
Patients may be asked to perform self-monitoring under the guidance of the pharmacist to ensure effective learning of the technique.
Encourage patients to document their own results. Help them to understand the results.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division22
5.4 Health Screening
All staff involved in providing the above service should be trained in the use of the monitoring devices and the procedures. They should also be aware of the limits of the tests provided.
The pharmacy must have a suitable area with facilities to perform the tests and provide counseling.
Ensure that the devices used are in good order.
Keep up to date with the latest development and know when to refer patients to medical practitioners. Before conducting the test, explain the procedure to the patient. Communicate test results to the patient in a manner in which he/she can understand and provide appropriate counseling.
5.5 Extemporaneous Dispensing
Ensure that the formula and intended method of preparation is correct. Requisite facilities and equipment for the preparation are available and maintained in good order. Ingredients must be sourced from reliable pharmaceutical supplier and be of a quality accepted for use in the preparation of the extemporaneous products.
All calculations, ingredients and quantities should be checked by a second person who is a pharmacist.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 23
Pharmacists must pay particular attention to substances that may be hazardous and require special handling techniques.The product must be suitably labeled with the necessary information, including special requirements for the safe handling and storage of the product including an expiry date.
Document the preparation and keep the records for at least 2 years. The records must include the formula, the ingredients and the quantities used, their source, batch number, expiry date, date of preparation and personnel involved in the preparation.
All documentations should be certified and duly stamped by a registered pharmacist with his/her registration number indicated. Refer to Guide to Good Dispensing Practice (GDsP) and Garispanduan Pembancuhan (Compounding) Persediaan Ekstemporanus Edisi 2015 Labelling Refer to Guide to Good Dispensing Practice (GDsP)
5.6 Knowledge of Genuine and Counterfeit drugs, OTC and herbal supplements
Pharmacist should only buy medicines from legitimate sources
Pharmacies must be equipped with the appropriate tool in order to ascertain if a product is genuine and registered with the competent authority.
Pharmacists must educate customers on how to identify
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division24
counterfeit medicines.
Pharmacists must be able to check the registration of a product through the National Pharmaceutical Regulatory Agency (NPRA) website.
Pharmacists must be aware of the latest information on de-registered products, products found containing adulterated ingredients, changes to product information and safety issues.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 25
Appendix I
1.0 OPTIONAL PROFESSIONAL SERVICES
1.1 Patient Medication Review (PM Review)
Patient Selection
Patient selection must have the following criteria:•• A PM Review can be conducted with patients on multiple
medications and those with long-term conditions.•• These regular PM Reviews, initiated by the pharmacist,
shall only be provided for patients who have been patronizing the pharmacy for the dispensing of prescriptions for at least the past three months.
•• PM Review can be conducted every 3 months after the last PM Review.
•• Self-referral by patients.•• Referral by medical practitioners.•• Referral by other health care professionals, e.g. nurses,
key workers and social services.•• Identified by the pharmacist as having problems
with medicine e.g. poor compliance, problems with administration and complicated medicine regimen.
Appointment
Schedule the appointments for the PM Review to be carried out. Give the patient an appointment card with the date and time.
Give patient an option for care giver to be present.
Inform the patient that the appointment will last for about 30 minutes.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division26
Inform the patient to bring their medicines including any complementary medicines, vitamins or any medicines they are taking regularly. A day before the review, remind the patient about his/her appointment.
Review Prior to the review:•• Prepare the pharmaceutical care plan.•• The pharmacist should be fully aware of the appropriate
use/ dose/ administration time/ side effects and major drug interactions of each medicine the patient is taking.
•• The pharmacist may need to refer to treatment guidelines as needed.
During the review:
•• Welcome patient and make the patient comfortable in the consultation area.
•• Explain the aims of the review.•• Explain the patient’s consent.•• Explain that the information will be shared with their GP
and a record will be kept in the pharmacy.•• Confirm and complete patient details on a PM Review
form (refer Appendix iv).•• Record the basic health data section of the form.•• For each medicine the pharmacist should consider the
following interventions:i. Advice on medicines usage (prescribed and
OTC), aiming to develop compliance;ii. Effective use of ‘when required’ medicines;
iii. Ensuring appropriate use of different medicine dosage forms (e.g. inhaler and soluble tablets);
iv. Advice on possible side effects;
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 27
v. Identification of items without adequate or correct dosage instructions;
vi. Identification of unwanted medicines (if patient is no longer taking their medicines);
vii. Identification of the need for a change of dosage form to facilitate effective usage;
viii. Suggestions of appropriate substitutes, if required;
ix. Proposals for dose optimization;x. Suggestions to improve patient’s clinical
outcome;xi. Advice on the use of any vitamins, complementary
medicines or self-purchased OTC medicines.
During the review, other health-related issues should be discussed such as:•• Practical problems in ordering, and obtaining their
medicines.•• General problems in taking and using medicines, e.g.
compliance charts.•• Health promotion advice where appropriate.•• Referral to other health care providers.
Complete the action plan•• The action plan will probably contain no more than 4 key
points.•• Discuss the action plan with the patient and get patient’s
consent •• Discuss with the patient information that requires follow-
up.
The PM review form shall be completed and a copy will be given to the patient at the end of the review.
Thank the patient and see him/her out.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division28
Post review:•• Send a copy of the review form to the patient’s GP •• Update the patient medication record.•• File all documents systematically and securely.•• Follow up on any actions you have agreed to do with the
patient.•• Record number of PM Reviews performed.
1.2 Health Promotion
Health promotion is the process of enabling people to have increased control over, and to improve their health. Community pharmacists can play a very important role in promoting, maintaining and improving the health of communities that they serve.
1.2.1 Smoking Cessation
•• Before providing this service, the pharmacists should have undergone the Certified Smoking Cessation Service Provider Program (CSCSP).
•• Pharmacists should apply the 5 A’s in the screening and assessment of customers:
Ask : Pharmacists should systematically identify all tobacco users among the customers who visit the pharmacy.
Advise : Pharmacists should strongly urge all tobacco users to quit.
Assess : Pharmacists must determine the willingness of the customers to make the quit attempt.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 29
Assist : If the customer is willing to quit, the pharmacist must help to devise an effective quit plan – provide practical counseling and recommend the use of approved pharmacotherapy.
Arrange : Pharmacists must also devise a follow-up plan to ensure the success of the quitting process.
•• For customers who have no intention to quit smoking, pharmacists should advise them of the possible health hazards of smoking. Pharmacists should provide them with leaflets and materials that they can take home to read. Customers should be assured of the pharmacist’s readiness to help them quit smoking.
•• If the customer is an ex-smoker (has not smoked for 6 months), the pharmacist should advise the customer on the dangers of relapse and offer solutions to overcome any potential problems.
•• If the patient is an ex-smoker (has not smoked for 12 months), the pharmacist should reinforce the benefits of cessation and help the customer to maintain smoke free.
•• Pharmacists should document the service provided and keep a record of the follow-ups for the individual customer in a prepared format to enable the service to be audited.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division30
1.2.2 Weight Management
•• Pharmacists intending to provide a weight management program should have a good understanding about obesity and the multi-disciplinary approach to weight management, which includes dieting, exercise, behavior modifications and recommendation of approved and suitable pharmacotherapy and/or evidence-based natural therapies.
•• Pharmacists and staff should offer to do a Body Mass Index (BMI) screening and a waist circumference measurement on potential customers.
•• If a more sophisticated weighing apparatus is available, measurements of total body fats, visceral fats and muscle mass would be more useful.
•• Pharmacists and staff should be able to interpret the results and explain the risks involved if one is overweight or obese.
•• Pharmacists should be able to recommend a weight reduction program suitable for the customer and design the proper follow-up visits in order to monitor the customer’s progress.
•• Customers who are overweight/ obese and who also have other co-morbidities such as diabetes, hypertension, hyperlipidemia, fatty liver, arthritis and gout should be encouraged to lose at least 5 to 10% of their body weight in order to reduce the risks associated with their weight. These customers may have to be referred to a physician if the need arises.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 31
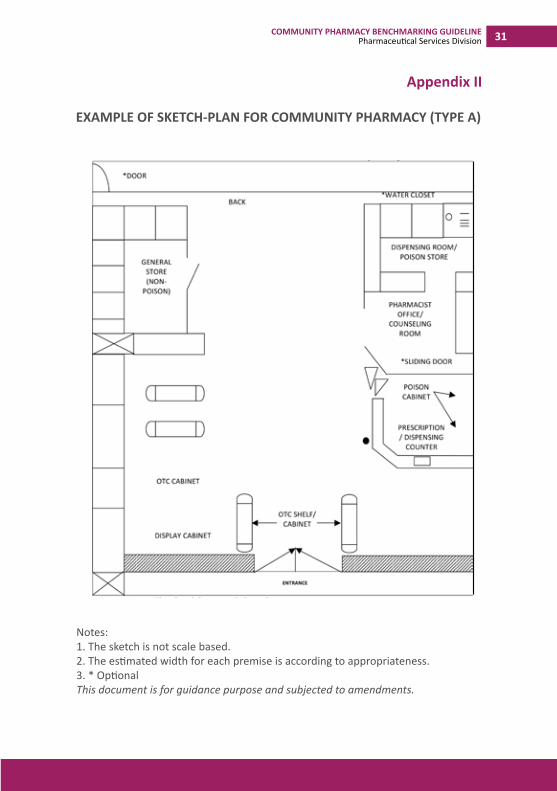
Notes:1. The sketch is not scale based.2. The estimated width for each premise is according to appropriateness. 3. * OptionalThis document is for guidance purpose and subjected to amendments.
Appendix II
EXAMPLE OF SKETCH-PLAN FOR COMMUNITY PHARMACY (TYPE A)
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division32
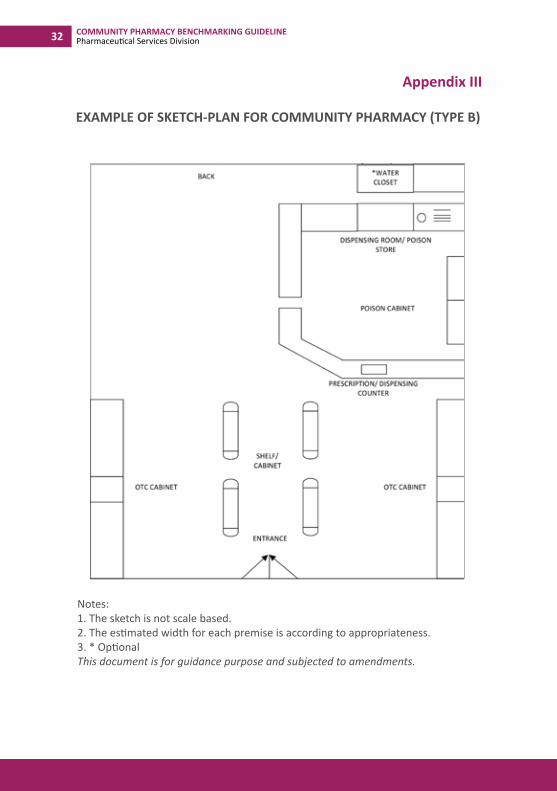
Notes:1. The sketch is not scale based.2. The estimated width for each premise is according to appropriateness. 3. * OptionalThis document is for guidance purpose and subjected to amendments.
Appendix III
EXAMPLE OF SKETCH-PLAN FOR COMMUNITY PHARMACY (TYPE B)
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 33
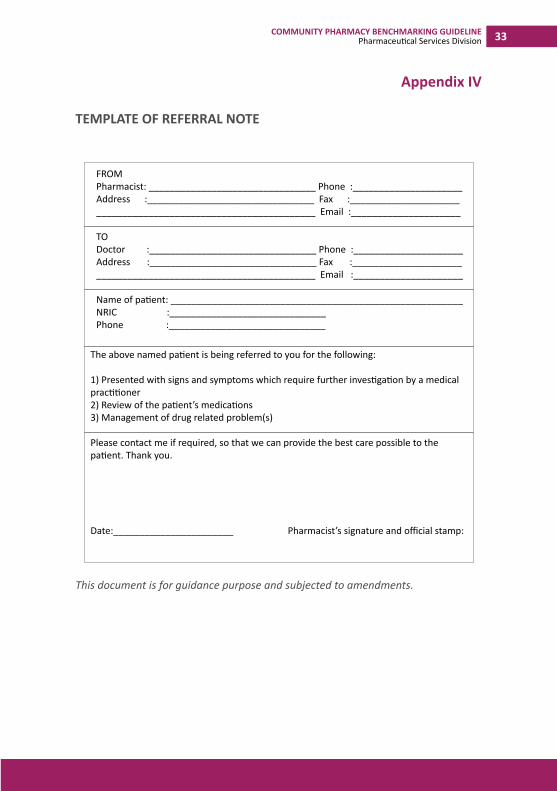
This document is for guidance purpose and subjected to amendments.
Appendix IV
TEMPLATE OF REFERRAL NOTE
FROMPharmacist: ________________________________ Phone :_____________________Address :________________________________ Fax :_______________________________________________________________ Email :_____________________
TODoctor :________________________________ Phone :_____________________Address :________________________________ Fax :_______________________________________________________________ Email :_____________________
Name of patient: ________________________________________________________NRIC :______________________________Phone :______________________________
The above named patient is being referred to you for the following:
1) Presented with signs and symptoms which require further investigation by a medical practitioner2) Review of the patient’s medications3) Management of drug related problem(s)
Please contact me if required, so that we can provide the best care possible to the patient. Thank you.
Date:_______________________ Pharmacist’s signature and official stamp:
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division34
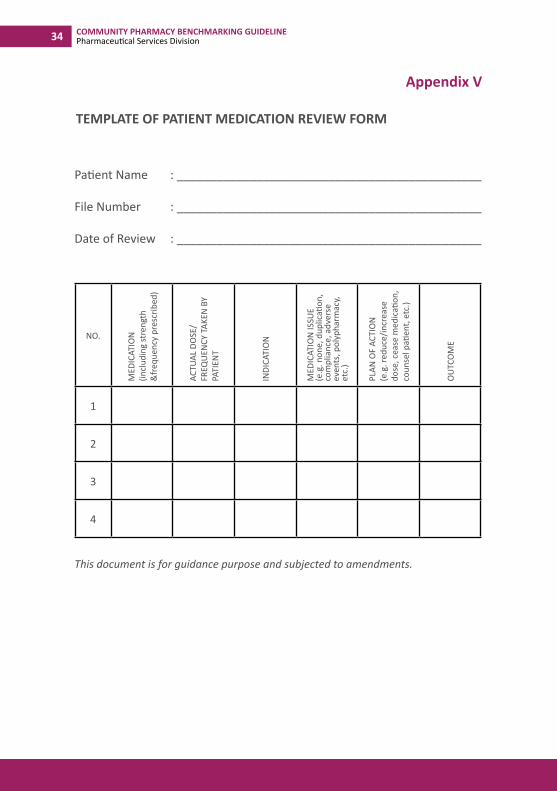
Patient Name : ______________________________________________ File Number : ______________________________________________
Date of Review : ______________________________________________
NO.
MED
ICAT
ION
(in
clud
ing
stre
ngth
&
freq
uenc
y pr
escr
ibed
)
ACTU
AL D
OSE
/ FR
EQU
ENCY
TAK
EN B
Y PA
TIEN
T
INDI
CATI
ON
MED
ICAT
ION
ISSU
E(e
.g. n
one,
dup
licati
on,
com
plia
nce,
adv
erse
ev
ents
, pol
ypha
rmac
y, et
c.)
PLAN
OF
ACTI
ON
(e.g
. red
uce/
incr
ease
do
se, c
ease
med
icati
on,
coun
sel p
atien
t, et
c.)
OU
TCO
ME
1
2
3
4
This document is for guidance purpose and subjected to amendments.
Appendix V
TEMPLATE OF PATIENT MEDICATION REVIEW FORM
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 35
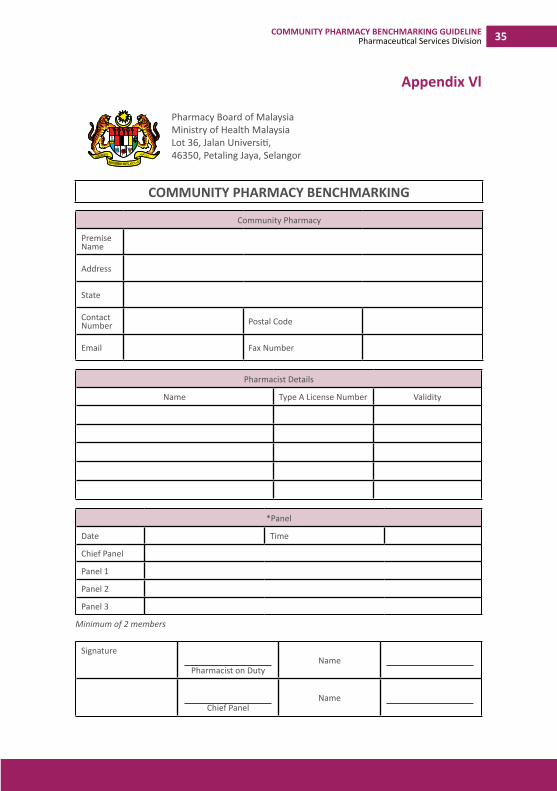
Appendix Vl
Community Pharmacy
Premise Name
Address
State
Contact Number Postal Code
Email Fax Number
Pharmacist Details
Name Type A License Number Validity
*Panel
Date Time
Chief Panel
Panel 1
Panel 2
Panel 3
Minimum of 2 members
Signature
Pharmacist on DutyName
Chief PanelName
Pharmacy Board of MalaysiaMinistry of Health MalaysiaLot 36, Jalan Universiti, 46350, Petaling Jaya, Selangor
COMMUNITY PHARMACY BENCHMARKING

SECT
ION
1: C
OM
PULS
ORY
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 37
DESC
RIPT
ION
COM
PLIA
NCE
NO
TES/
COM
MEN
TS0
1
1. M
ANAG
EMEN
T
Full
man
agem
ent c
ontr
ol o
f pha
rmac
y pr
actic
e by
pha
rmac
ist.
TOTA
L (1
mar
k)
2. P
REM
ISES
Loca
tion
(1 m
ark)
No
shar
ing
with
any
oth
er n
on-p
harm
acy
rela
ted
prac
tices
and
bus
ines
ses.
Med
icin
e Di
spen
sing
Area
(MDA
) (3
mar
ks)
MDA
con
sists
of:
• Pr
escr
iptio
n co
unte
r•
Coun
selin
g ar
ea
Shou
ld b
e cl
ean
and
tidy
Sign
boar
d an
d Ad
verti
sem
ent (
6 m
arks
)
Phar
mac
y sig
nboa
rd p
roje
ct th
e pr
ofes
siona
l im
age
of a
pha
rmac
y
Noti
ce o
f the
pha
rmac
ist(s
) on
duty
is d
ispla
yed
whi
ch in
clud
e:•
Nam
e of
pha
rmac
ist(s
)•
Tim
e an
d da
te/d
ay o
f dut
y•
Phot
o
Regi
stra
tion
Certi
ficat
e an
d An
nual
Cer
tifica
te fo
r the
pha
rmac
ist in
-cha
rge
are
clea
rly
disp
laye
d.
Desig
nate
d ar
eas a
re c
lear
ly in
dica
ted,
e.g
“Pr
escr
iptio
n Co
unte
r” o
r “Ph
arm
acy”
.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division38
Faci
lities
(16
mar
ks)
Med
icin
e Di
spen
sing
Area
/ Pre
scrip
tion
Coun
ter
• W
ithou
t any
bar
rier (
to fa
cilit
ate
patie
nt c
ouns
elin
g an
d fo
r mor
e eff
ectiv
e co
mm
unic
ation
).•
Ena
ble
safe
and
effi
cien
t wor
kflow
.•
Size
and
org
aniza
tion
of th
is ar
ea is
ade
quat
e fo
r the
vol
ume
of w
ork
• Ph
arm
acist
is a
ble
to m
aint
ain
a di
rect
supe
rvisi
on o
f the
pha
rmac
y an
d st
aff fr
om th
is ar
ea.
Coun
selin
g ar
ea is
a p
rope
rly d
esig
nate
d ar
ea, p
rivat
e an
d co
mfo
rtab
le
Air-c
ondi
tione
r with
sche
dule
d m
aint
enan
ce
Refr
iger
ator
• Te
mpe
ratu
re is
mai
ntai
ned
betw
een
2 –
8°C
with
a p
rope
r mon
itorin
g sy
stem
.•
Reco
rds o
f tem
pera
ture
is a
vaila
ble
and
verifi
ed•
Does
not
stor
e fo
od o
r drin
ks
Clea
nlin
ess
• Ap
prop
riate
pes
t con
trol
mea
sure
is m
ade
avai
labl
e.
Dry
Com
poun
ding
Are
a (M
edic
ines
Pre
para
tion
/ Fill
ing
Area
) •
A de
signa
ted
area
for c
ounti
ng ta
blet
s/ c
apsu
les,
filli
ng, p
acki
ng o
f med
icin
es a
nd fo
r la
belin
g th
e pr
epar
ed m
edic
ines
. •
Loca
ted
away
from
food
and
drin
ks.
• Pr
ovid
e su
itabl
e an
d hy
gien
ic m
eans
of c
ounti
ng ta
blet
s/ca
psul
es (e
.g. c
ounti
ng tr
ay).
Equi
pmen
t a)
Cab
inet
s•
For t
he st
orag
e of
doc
umen
ts/ r
ecor
ds.
b) L
abel
s•
Appr
opria
te si
zes a
nd sh
apes
• Le
gibl
e
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 39
Occ
upati
onal
and
safe
ty re
quire
men
ts (1
mar
k)
• Fi
re e
xting
uish
er
Refe
renc
es (2
mar
ks)
• Dr
ug In
form
ation
Han
dboo
k/ B
ritish
Nati
onal
For
mul
ary
(or a
ny o
ther
relia
ble
refe
renc
es –
ha
rdco
py o
r onl
ine)
• Co
de o
f Con
duct
for P
harm
acist
and
Bod
ies C
orpo
rate
(har
dcop
y or
onl
ine)
TOTA
L (2
9 m
arks
)
3. P
RACT
ICE
AND
SERV
ICES
Serv
ices
(5 m
arks
)
Esse
ntial
Ser
vice
s•
scre
enin
g pr
escr
iptio
ns•
med
icin
es d
ispen
sing
• di
spen
sing
inst
ructi
on•
med
icati
on c
ouns
elin
g•
phar
mac
y m
anag
emen
t in
drug
pro
cure
men
t and
doc
umen
tatio
n
Type
of P
rodu
cts (
2 m
arks
)
• 70
% o
f the
mer
chan
dise
in a
com
mun
ity p
harm
acy
cons
ists o
f reg
ister
ed p
harm
aceu
tical
pr
oduc
ts, h
ealth
and
nut
rition
al p
rodu
cts,
surg
ical
and
med
ical
dev
ices
, per
sona
l car
e an
d re
habi
litati
on a
ids.
• N
o sa
le o
f goo
ds a
nd fo
od w
hich
is h
arm
ful t
o he
alth
. Min
imum
sale
of n
on-p
harm
acy
prod
ucts
, e.g
gift
item
s, c
ards
and
drin
ks.
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division40
Pers
onne
l (9
mar
ks)
a) P
harm
acist
s•
Regi
ster
ed w
ith th
e Ph
arm
acy
Boar
d of
Mal
aysia
• O
bser
ve th
e Co
de o
f Con
duct
for P
harm
acist
s and
Bod
ies C
orpo
rate
• Co
mpl
y w
ith a
ll th
e ph
arm
acy
legi
slatio
ns o
f Mal
aysia
• Dr
ess c
ode
i. Ph
arm
acist
Tun
ic (W
hite
Coa
t)ii.
Pro
ject
a p
rofe
ssio
nal i
mag
e•
Nam
e ta
g w
ith th
e w
ord
“Pha
rmac
ist”
• Su
itabl
e nu
mbe
r of p
harm
acist
si.
in li
ne w
ith th
e w
orkl
oad
of th
e ph
arm
acy
ii. w
orkl
oad
pref
erab
ly sh
ould
not
exc
eed
150
pres
crip
tions
/pha
rmac
ist/d
ay•
Min
imum
dist
racti
on w
hen
fillin
g pr
escr
iptio
ns o
r car
ryin
g ou
t pha
rmac
y se
rvic
es
Stor
age
of M
edic
ines
(7 m
arks
)
All m
edic
ines
com
ply
with
labe
ling
requ
irem
ents
and
kep
t in
the
orig
inal
pac
kagi
ng o
r pr
oper
ly la
bele
d co
ntai
ners
.
Diffe
rent
cat
egor
ies o
f ite
ms a
re sy
stem
atica
lly a
rran
ged.
Sepa
rate
stor
age
is pr
ovid
ed fo
r int
erna
l and
ext
erna
l med
icin
es.
Med
icin
es w
ith si
mila
r nam
es a
nd p
acka
ging
are
disti
nctiv
ely
sepa
rate
d.
Poiso
n B
and
Poiso
n C
item
s as l
isted
in P
art I
of t
he P
oiso
n Li
st a
re k
ept i
n a
lock
ed c
abin
et.
All k
eys a
re k
ept b
y th
e ph
arm
acist
.
Stor
age
cond
ition
s com
plie
d w
ith m
anuf
actu
rer i
nstr
uctio
ns a
nd c
old
chai
n re
quire
men
ts.
Safe
ty M
easu
res (
1 m
ark)
Secu
re lo
cks o
n m
ain
door
and
gril
le/g
ate
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 41
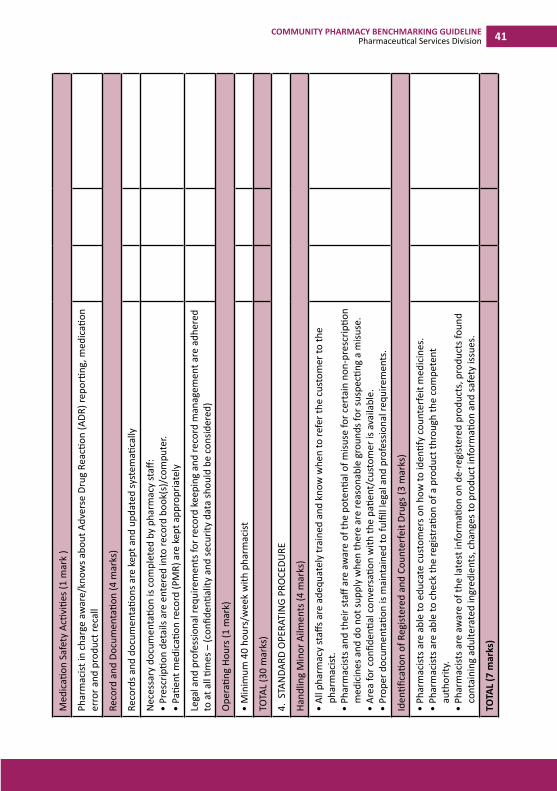
Med
icati
on S
afet
y Ac
tiviti
es (1
mar
k )
Phar
mac
ist in
cha
rge
awar
e/kn
ows a
bout
Adv
erse
Dru
g Re
actio
n (A
DR) r
epor
ting,
med
icati
on
erro
r and
pro
duct
reca
ll
Reco
rd a
nd D
ocum
enta
tion
(4 m
arks
)
Reco
rds a
nd d
ocum
enta
tions
are
kep
t and
upd
ated
syst
emati
cally
Nec
essa
ry d
ocum
enta
tion
is co
mpl
eted
by
phar
mac
y st
aff:
• Pr
escr
iptio
n de
tails
are
ent
ered
into
reco
rd b
ook(
s)/c
ompu
ter.
• Pa
tient
med
icati
on re
cord
(PM
R) a
re k
ept a
ppro
pria
tely
Lega
l and
pro
fess
iona
l req
uire
men
ts fo
r rec
ord
keep
ing
and
reco
rd m
anag
emen
t are
adh
ered
to
at a
ll tim
es –
(con
fiden
tialit
y an
d se
curit
y da
ta sh
ould
be
cons
ider
ed)
Ope
ratin
g Ho
urs (
1 m
ark)
• M
inim
um 4
0 ho
urs/
wee
k w
ith p
harm
acist
TOTA
L (3
0 m
arks
)
4. S
TAN
DARD
OPE
RATI
NG
PRO
CEDU
RE
Hand
ling
Min
or A
ilmen
ts (4
mar
ks)
• Al
l pha
rmac
y st
affs a
re a
dequ
atel
y tr
aine
d an
d kn
ow w
hen
to re
fer t
he c
usto
mer
to th
e ph
arm
acist
.•
Phar
mac
ists a
nd th
eir s
taff
are
awar
e of
the
pote
ntial
of m
isuse
for c
erta
in n
on-p
resc
riptio
n m
edic
ines
and
do
not s
uppl
y w
hen
ther
e ar
e re
ason
able
gro
unds
for s
uspe
cting
a m
isuse
.•
Area
for c
onfid
entia
l con
vers
ation
with
the
patie
nt/c
usto
mer
is a
vaila
ble.
• Pr
oper
doc
umen
tatio
n is
mai
ntai
ned
to fu
lfill
lega
l and
pro
fess
iona
l req
uire
men
ts.
Iden
tifica
tion
of R
egist
ered
and
Cou
nter
feit
Drug
s (3
mar
ks)
• Ph
arm
acist
s are
abl
e to
edu
cate
cus
tom
ers o
n ho
w to
iden
tify
coun
terfe
it m
edic
ines
.•
Phar
mac
ists a
re a
ble
to c
heck
the
regi
stra
tion
of a
pro
duct
thro
ugh
the
com
pete
nt
auth
ority
.•
Phar
mac
ists a
re a
war
e of
the
late
st in
form
ation
on
de-r
egist
ered
pro
duct
s, p
rodu
cts f
ound
co
ntai
ning
adu
ltera
ted
ingr
edie
nts,
cha
nges
to p
rodu
ct in
form
ation
and
safe
ty is
sues
.
TOTA
L (7
mar
ks)
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division42
SECT
ION
2: O
PTIO
NAL
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 43
DESC
RIPT
ION
COM
PLIA
NCE
NO
TES/
COM
MEN
TS0
1
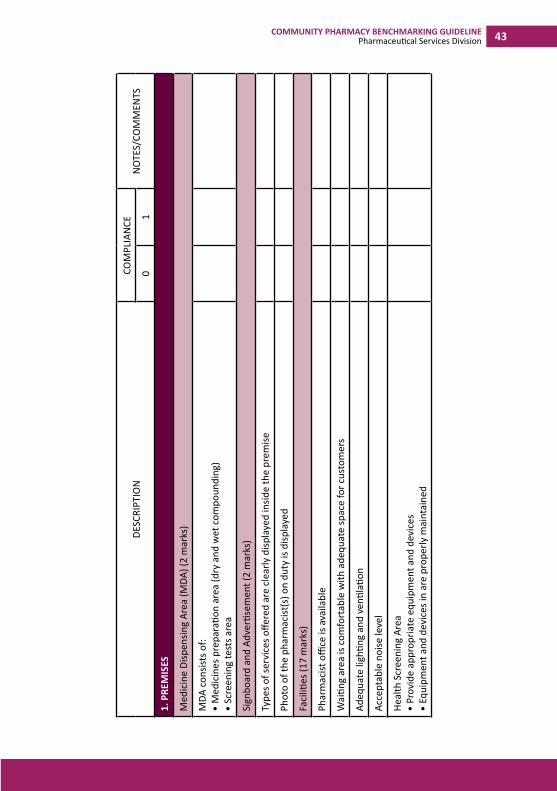
1. P
REM
ISES
Med
icin
e Di
spen
sing
Area
(MDA
) (2
mar
ks)
MDA
con
sists
of:
• M
edic
ines
pre
para
tion
area
(dry
and
wet
com
poun
ding
)•
Scre
enin
g te
sts a
rea
Sign
boar
d an
d Ad
verti
sem
ent (
2 m
arks
)
Type
s of s
ervi
ces o
ffere
d ar
e cl
early
disp
laye
d in
side
the
prem
ise
Phot
o of
the
phar
mac
ist(s
) on
duty
is d
ispla
yed
Faci
lities
(17
mar
ks)
Phar
mac
ist o
ffice
is a
vaila
ble
Wai
ting
area
is c
omfo
rtab
le w
ith a
dequ
ate
spac
e fo
r cus
tom
ers
Adeq
uate
ligh
ting
and
venti
latio
n
Acce
ptab
le n
oise
leve
l
Heal
th S
cree
ning
Are
a•
Prov
ide
appr
opria
te e
quip
men
t and
dev
ices
•
Equi
pmen
t and
dev
ices
in a
re p
rope
rly m
aint
aine
d
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division44
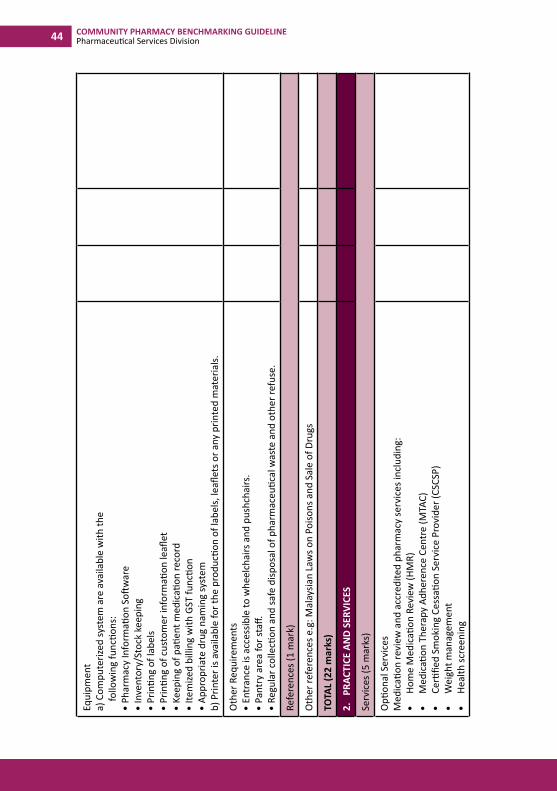
Equi
pmen
t a)
Com
pute
rized
syst
em a
re a
vaila
ble
with
the
fo
llow
ing
func
tions
:•
Phar
mac
y In
form
ation
Soft
war
e•
Inve
ntor
y/St
ock
keep
ing
• Pr
intin
g of
labe
ls•
Prin
ting
of c
usto
mer
info
rmati
on le
aflet
• Ke
epin
g of
pati
ent m
edic
ation
reco
rd•
Item
ized
billi
ng w
ith G
ST fu
nctio
n•
Appr
opria
te d
rug
nam
ing
syst
emb)
Prin
ter i
s ava
ilabl
e fo
r the
pro
ducti
on o
f lab
els,
leafl
ets o
r any
prin
ted
mat
eria
ls.
Oth
er R
equi
rem
ents
• En
tran
ce is
acc
essib
le to
whe
elch
airs
and
pus
hcha
irs.
• Pa
ntry
are
a fo
r sta
ff.•
Regu
lar c
olle
ction
and
safe
disp
osal
of p
harm
aceu
tical
was
te a
nd o
ther
refu
se.
Refe
renc
es (1
mar
k)
Oth
er re
fere
nces
e.g
: Mal
aysia
n La
ws o
n Po
isons
and
Sal
e of
Dru
gs
TOTA
L (2
2 m
arks
)
2.
PRAC
TICE
AN
D SE
RVIC
ES
Serv
ices
(5 m
arks
)
Opti
onal
Ser
vice
sM
edic
ation
revi
ew a
nd a
ccre
dite
d ph
arm
acy
serv
ices
incl
udin
g:•
H
ome
Med
icati
on R
evie
w (H
MR)
•
Med
icati
on T
hera
py A
dher
ence
Cen
tre
(MTA
C)
•
Cer
tified
Sm
okin
g Ce
ssati
on S
ervi
ce P
rovi
der (
CSCS
P)•
W
eigh
t man
agem
ent
•
Hea
lth sc
reen
ing
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 45
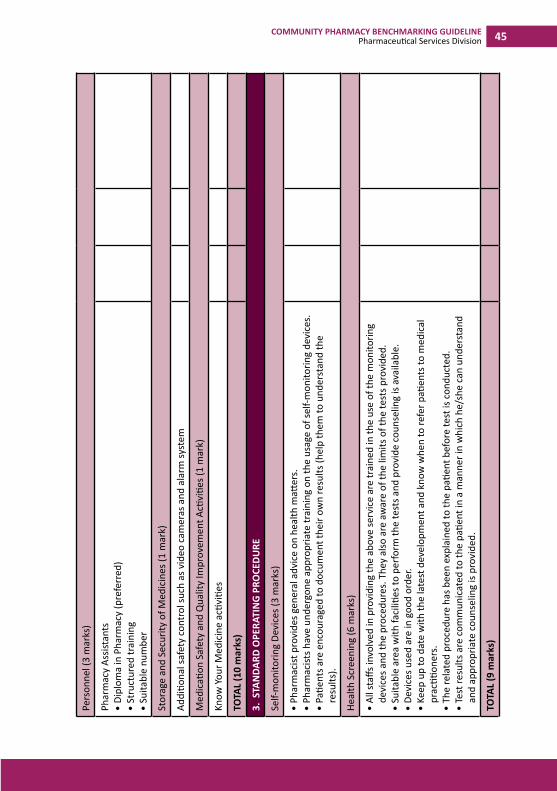
Pers
onne
l (3
mar
ks)
Phar
mac
y As
sista
nts
• Di
plom
a in
Pha
rmac
y (p
refe
rred
)•
Stru
ctur
ed tr
aini
ng•
Suita
ble
num
ber
Stor
age
and
Secu
rity
of M
edic
ines
(1 m
ark)
Addi
tiona
l saf
ety
cont
rol s
uch
as v
ideo
cam
eras
and
ala
rm sy
stem
Med
icati
on S
afet
y an
d Q
ualit
y Im
prov
emen
t Acti
vitie
s (1
mar
k)
Know
You
r Med
icin
e ac
tiviti
es
TOTA
L (1
0 m
arks
)
3. S
TAN
DARD
OPE
RATI
NG
PRO
CEDU
RE
Self-
mon
itorin
g De
vice
s (3
mar
ks)
• Ph
arm
acist
pro
vide
s gen
eral
adv
ice
on h
ealth
matt
ers.
• Ph
arm
acist
s hav
e un
derg
one
appr
opria
te tr
aini
ng o
n th
e us
age
of se
lf-m
onito
ring
devi
ces.
• Pa
tient
s are
enc
oura
ged
to d
ocum
ent t
heir
own
resu
lts (h
elp
them
to u
nder
stan
d th
e re
sults
).
Heal
th S
cree
ning
(6 m
arks
)
• Al
l sta
ffs in
volv
ed in
pro
vidi
ng th
e ab
ove
serv
ice
are
trai
ned
in th
e us
e of
the
mon
itorin
g de
vice
s and
the
proc
edur
es. T
hey
also
are
aw
are
of th
e lim
its o
f the
test
s pro
vide
d.•
Suita
ble
area
with
faci
lities
to p
erfo
rm th
e te
sts a
nd p
rovi
de c
ouns
elin
g is
avai
labl
e.•
Devi
ces u
sed
are
in g
ood
orde
r.•
Keep
up
to d
ate
with
the
late
st d
evel
opm
ent a
nd k
now
whe
n to
refe
r pati
ents
to m
edic
al
prac
tition
ers.
• Th
e re
late
d pr
oced
ure
has b
een
expl
aine
d to
the
patie
nt b
efor
e te
st is
con
duct
ed.
• Te
st re
sults
are
com
mun
icat
ed to
the
patie
nt in
a m
anne
r in
whi
ch h
e/sh
e ca
n un
ders
tand
an
d ap
prop
riate
cou
nsel
ing
is pr
ovid
ed.
TOTA
L (9
mar
ks)
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division46
SECT
ION
3: C
OM
PULS
ORY
(if se
rvic
e/pr
oduc
t(s)
ava
ilabl
e)
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 47
DESC
RIPT
ION
COM
PLIA
NCE
NO
TES/
COM
MEN
TS0
1
1. P
REM
ISES
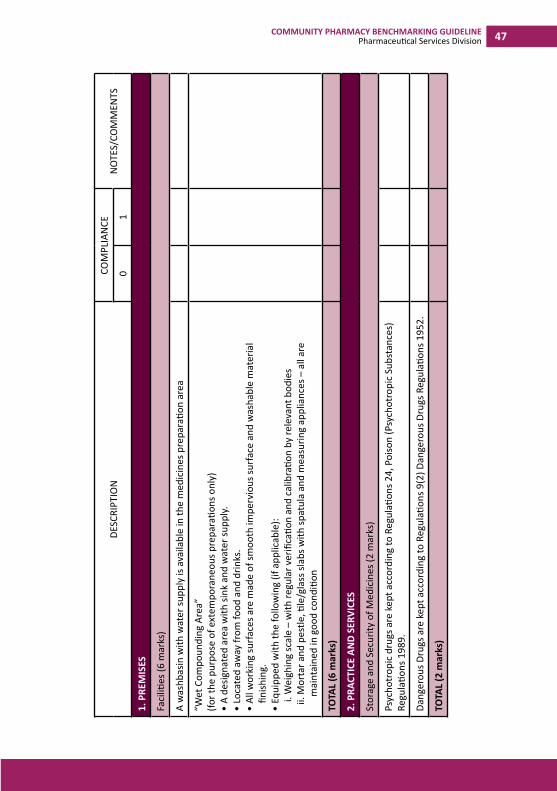
Faci
lities
(6 m
arks
)
A w
ashb
asin
with
wat
er su
pply
is a
vaila
ble
in th
e m
edic
ines
pre
para
tion
area
“Wet
Com
poun
ding
Are
a”
(for t
he p
urpo
se o
f ext
empo
rane
ous p
repa
ratio
ns o
nly)
• A
desig
nate
d ar
ea w
ith si
nk a
nd w
ater
supp
ly.•
Loca
ted
away
from
food
and
drin
ks.
• Al
l wor
king
surf
aces
are
mad
e of
smoo
th im
perv
ious
surf
ace
and
was
habl
e m
ater
ial
finish
ing.
• Eq
uipp
ed w
ith th
e fo
llow
ing
(if a
pplic
able
):i.
Wei
ghin
g sc
ale
– w
ith re
gula
r ver
ifica
tion
and
calib
ratio
n by
rele
vant
bod
ies
ii. M
orta
r and
pes
tle, ti
le/g
lass
slab
s with
spat
ula
and
mea
surin
g ap
plia
nces
– a
ll ar
e m
aint
aine
d in
goo
d co
nditi
on
TOTA
L (6
mar
ks)
2. P
RACT
ICE
AND
SERV
ICES
Stor
age
and
Secu
rity
of M
edic
ines
(2 m
arks
)
Psyc
hotr
opic
dru
gs a
re k
ept a
ccor
ding
to R
egul
ation
s 24,
Poi
son
(Psy
chot
ropi
c Su
bsta
nces
) Re
gula
tions
198
9.
Dang
erou
s Dru
gs a
re k
ept a
ccor
ding
to R
egul
ation
s 9(2
) Dan
gero
us D
rugs
Reg
ulati
ons 1
952.
TOTA
L (2
mar
ks)
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division48
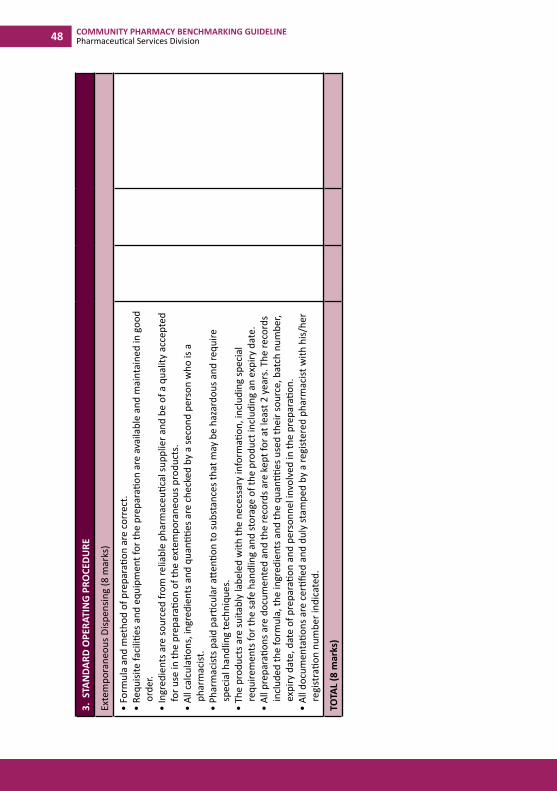
3. S
TAN
DARD
OPE
RATI
NG
PRO
CEDU
RE
Exte
mpo
rane
ous D
ispen
sing
(8 m
arks
)
• Fo
rmul
a an
d m
etho
d of
pre
para
tion
are
corr
ect.
• Re
quisi
te fa
ciliti
es a
nd e
quip
men
t for
the
prep
arati
on a
re a
vaila
ble
and
mai
ntai
ned
in g
ood
orde
r.•
Ingr
edie
nts a
re so
urce
d fr
om re
liabl
e ph
arm
aceu
tical
supp
lier a
nd b
e of
a q
ualit
y ac
cept
ed
for u
se in
the
prep
arati
on o
f the
ext
empo
rane
ous p
rodu
cts.
• Al
l cal
cula
tions
, ing
redi
ents
and
qua
ntitie
s are
che
cked
by
a se
cond
per
son
who
is a
ph
arm
acist
.•
Phar
mac
ists p
aid
parti
cula
r atte
ntion
to su
bsta
nces
that
may
be
haza
rdou
s and
requ
ire
spec
ial h
andl
ing
tech
niqu
es.
• Th
e pr
oduc
ts a
re su
itabl
y la
bele
d w
ith th
e ne
cess
ary
info
rmati
on, i
nclu
ding
spec
ial
requ
irem
ents
for t
he sa
fe h
andl
ing
and
stor
age
of th
e pr
oduc
t inc
ludi
ng a
n ex
piry
dat
e.•
All p
repa
ratio
ns a
re d
ocum
ente
d an
d th
e re
cord
s are
kep
t for
at l
east
2 y
ears
. The
reco
rds
incl
uded
the
form
ula,
the
ingr
edie
nts a
nd th
e qu
antiti
es u
sed
thei
r sou
rce,
bat
ch n
umbe
r, ex
piry
dat
e, d
ate
of p
repa
ratio
n an
d pe
rson
nel i
nvol
ved
in th
e pr
epar
ation
.•
All d
ocum
enta
tions
are
cer
tified
and
dul
y st
ampe
d by
a re
gist
ered
pha
rmac
ist w
ith h
is/he
r re
gist
ratio
n nu
mbe
r ind
icat
ed.
TOTA
L (8
mar
ks)
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 49
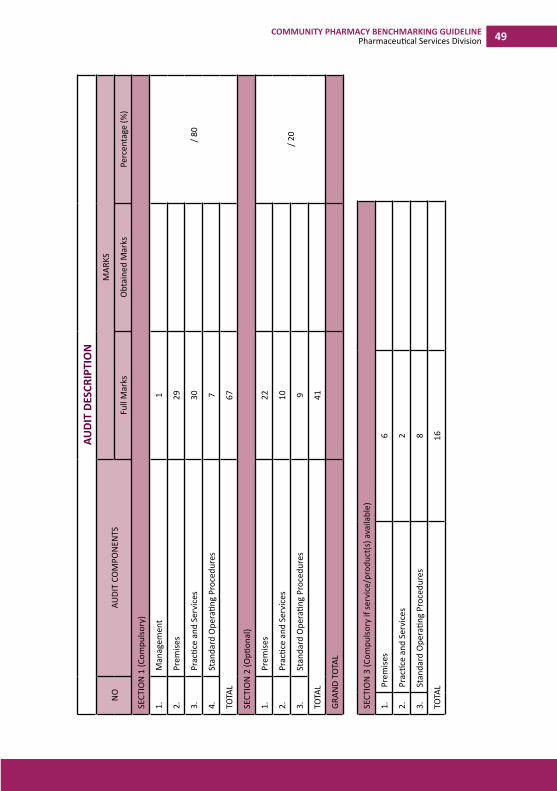
AUDI
T DE
SCRI
PTIO
N
NO
AUDI
T CO
MPO
NEN
TSM
ARKS
Full
Mar
ksO
btai
ned
Mar
ksPe
rcen
tage
(%)
SECT
ION
1 (C
ompu
lsory
)
1.M
anag
emen
t1
/
80
2.Pr
emise
s29
3.Pr
actic
e an
d Se
rvic
es30
4.St
anda
rd O
pera
ting
Proc
edur
es7
TOTA
L67
SECT
ION
2 (O
ption
al)
1.Pr
emise
s22
/ 20
2.Pr
actic
e an
d Se
rvic
es10
3.St
anda
rd O
pera
ting
Proc
edur
es9
TOTA
L41
GRAN
D TO
TAL
SECT
ION
3 (C
ompu
lsory
if se
rvic
e/pr
oduc
t(s)
ava
ilabl
e)
1.Pr
emise
s6
2.Pr
actic
e an
d Se
rvic
es2
3.St
anda
rd O
pera
ting
Proc
edur
es8
TOTA
L16
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division50
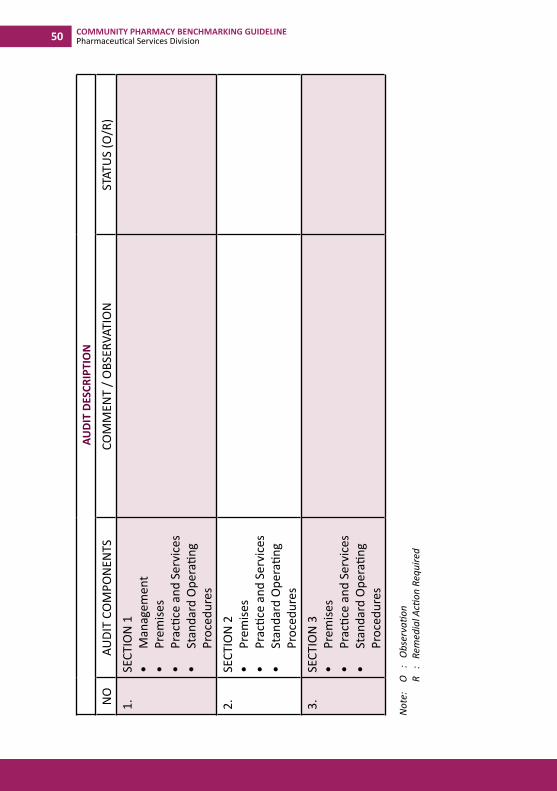
AUDI
T DE
SCRI
PTIO
N
NO
AUDI
T CO
MPO
NEN
TSCO
MM
ENT
/ OBS
ERVA
TIO
NST
ATU
S (O
/R)
1.SE
CTIO
N 1
• M
anag
emen
t•
Prem
ises
• Pr
actic
e an
d Se
rvic
es•
Stan
dard
Ope
ratin
g Pr
oced
ures
2.SE
CTIO
N 2
• Pr
emise
s•
Prac
tice
and
Serv
ices
• St
anda
rd O
pera
ting
Proc
edur
es3.
SECT
ION
3•
Prem
ises
• Pr
actic
e an
d Se
rvic
es•
Stan
dard
Ope
ratin
g Pr
oced
ures
Not
e:
O
: O
bser
vatio
n
R
:
Rem
edia
l Acti
on R
equi
red
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division 51
Auditor’s Comment
Remedial Action/s Required
COMMUNITY PHARMACY BENCHMARKING GUIDELINEPharmaceutical Services Division52
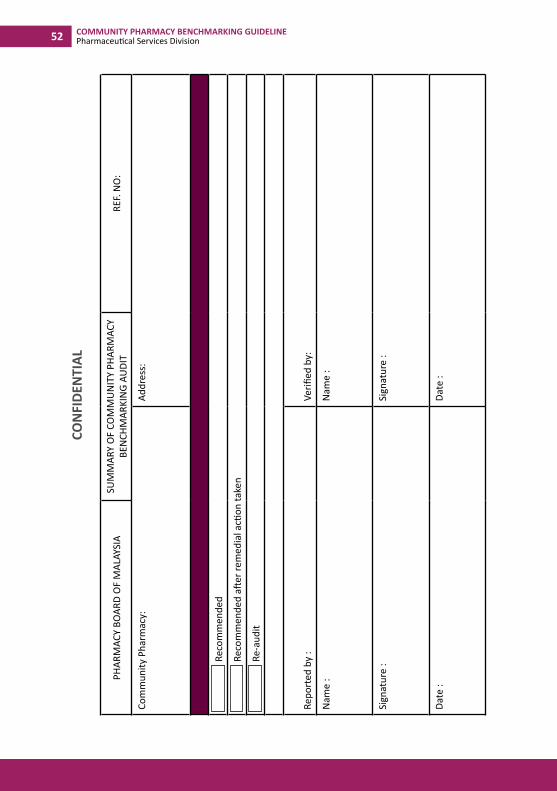
CON
FIDE
NTI
AL
PHAR
MAC
Y BO
ARD
OF
MAL
AYSI
ASU
MM
ARY
OF
COM
MU
NIT
Y PH
ARM
ACY
BEN
CHM
ARKI
NG
AUDI
TRE
F. N
O:
Com
mun
ity P
harm
acy:
Addr
ess:
Re
com
men
ded
Re
com
men
ded
after
rem
edia
l acti
on ta
ken
Re
-aud
it
Repo
rted
by
:Ve
rified
by:
Nam
e :
Nam
e :
Sign
atur
e :
Sign
atur
e :
Date
:Da
te :