common skin problems
DESCRIPTION
Common skin problemsTRANSCRIPT
Common Skin Problems
Dr. Sanjeeva Hulangamuwa
Consultant Dermatologist
GH Chilaw
ECZEMA

Acute eczema

Dry Eczema

Infantile Eczema

Chronic Lichenified Eczema

Contact Dermatitis to rubber slippers
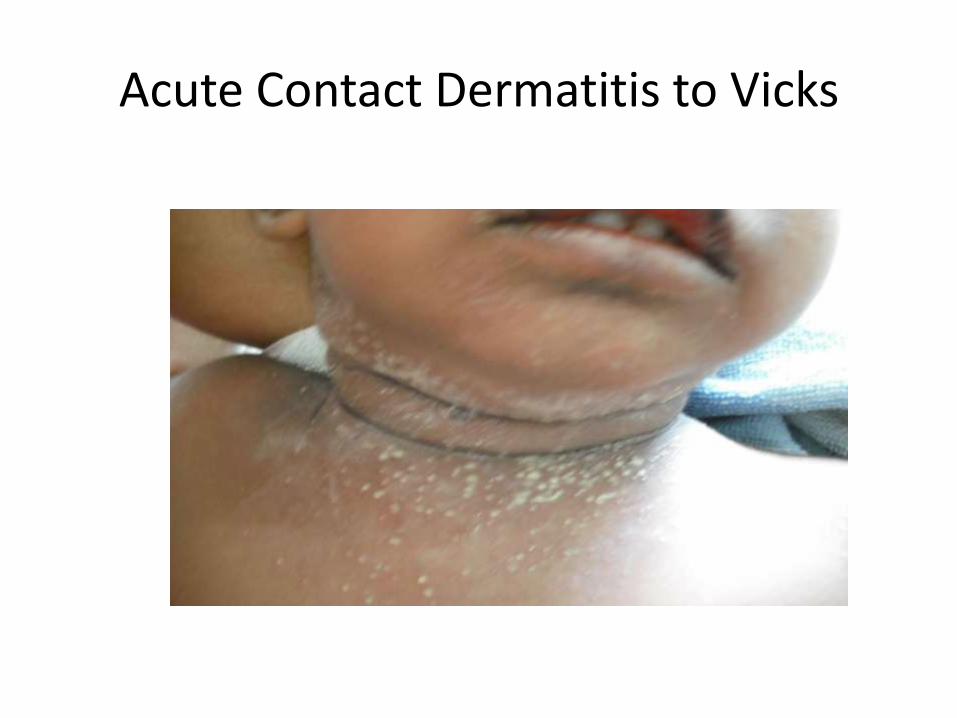
Acute Contact Dermatitis to Vicks
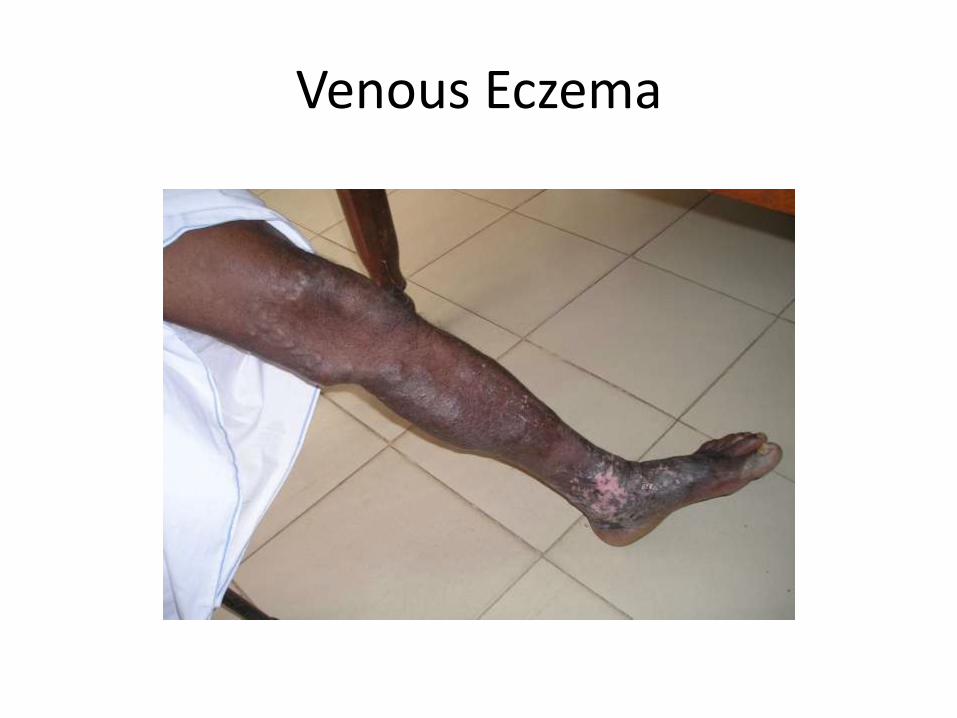
Venous Eczema

Eczema herpeticum

Eczema Symptoms and Signs
• Itchy skin patches
• Oozing ( weeping ) – acute stage
• Pigmentary changes
• Dry thick patches in chronic stages
• Recurrent attacks
• Can associated with asthma and allergic rhinitis
• Family members may have atopy
• Common sites –
face and flexures – infants and children
legs – adults
• Worsen with exposure to certain chemicals, dust, cement, fur,etc

Eczema (cont.)
Management
• Weepy areas - Condys ( potassium permangenate ) wash or compression
• Steroid creams – hydrocortisone, betamethasone, clobetasol
• Moisturizers – aquous cream, emulsifying ointment
• Oral antibiotics for acute infective eczemas
• Antihistamines for itching – chlorpheniramine, cetirizine, loratidine
• Avoid frequent washing and soaps
• Severe and resistant cases – prednisolone, azathioprine, methotrexate, ciclosporin
• Rule out immunodeficiency syndromes in severe eczemas in infants

Photodermatitis


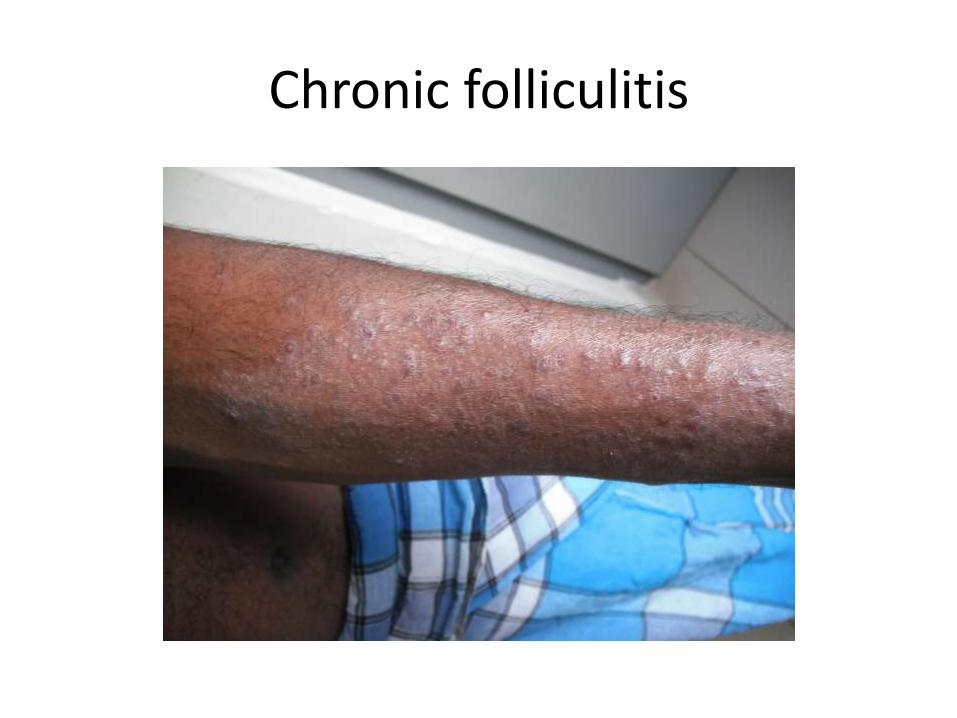
Chronic folliculitis

Seborrhoeic dermatitis

Chronic plaque psoriasis






Flexural Psoriasis in a baby

Erythrodermic Psoriasis

Psoriasis
• Thick scaly erythematous plaques
• Common sites - elbows, knees, umbilicus, scalp
In some pts. whole body is involved
• Scalp – scaling as in dandruff but severe
• Nail changes and arthritis occur in some patients
• Itching may or may not present
• Family history may be positive
• Rare presentations – pustular psoriasis and erythrodermic psoriasis
• Diagnosis - clinically

Psoriasis • Topical application –
steroid creams – hydrocortisone, betamethasone, clobetasol
coal tar
dithranol
moisturizers – aquous cream, emulsifying ointment, liquid paraffin
• Light therapy
PUVA ( Psoralen tablets + ultraviolet A )
Ultraviolet B
Solar PUVA – Expose to early morning sunlight 2h after taking the psoralen tablet

Psoriasis
• Systemic treatment
methotrexate, acitretin, ciclosporin,etc
• Newer therapies
Biological agents ( expensive )
INFECTIONS

Bacterial infections
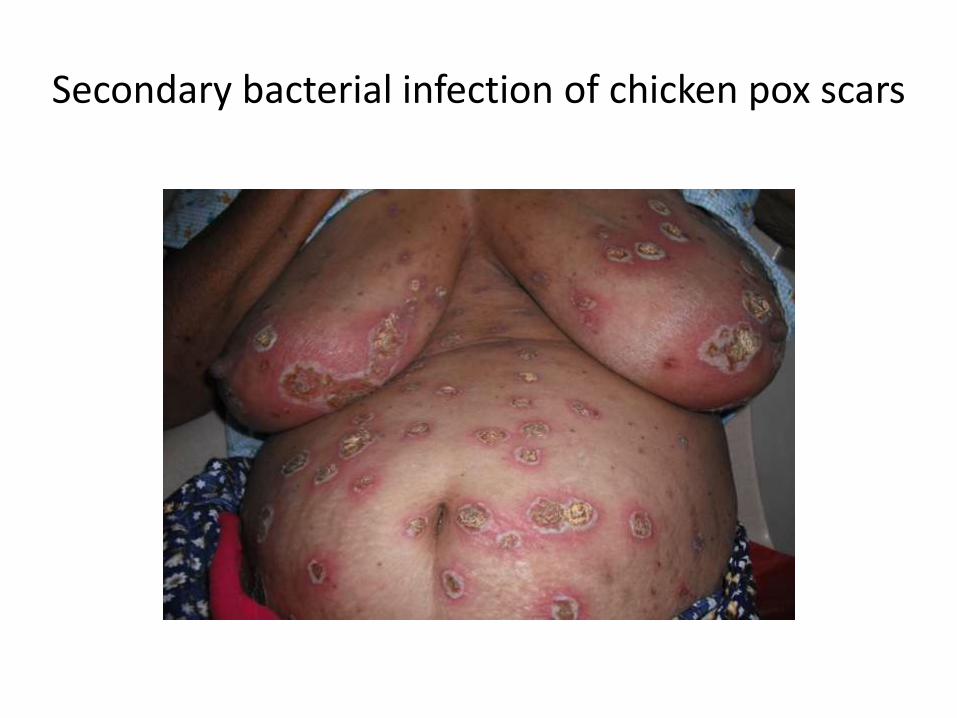
Secondary bacterial infection of chicken pox scars

Staphylococcal scalded skin syndrome



Staphylococcal scalded skin syndrome
• Common below 4y of age
• Irritable
• Refuse feeds
• Febrile
• Erythema and scaling around mouth, genital region and flexures
• Skin is tender
• Treatment
flucloxacillin
cloxacillin

Furuncles

Furuncles
• Common in preschool children
• Painful pustules and papules
• Some rupture and discharge pus
• Fever may occur
• Common on face and scalp
• Can be recurrent
• Treatment
oral – cloxacillin, erythromycin
topical – soframycin ( framycetin ), fucidic acid, mupirocin

Impetigo



Bullous impetigo

Impetigo
• Common in children
• Honey colored crusted plaques
• Sometimes blisters may occur ( bullous impetigo )
• Commonly occur peri-orificial ( around mouth, nose )
• Painful
• Appears suddenly in a few days
• Treatment Oral – cloxacillin
Topical – soframycin, fusidic acid, mupirocin creams

Other bacterial infections
• Eg; gram negative bacterial infections ( eg; pseudomonas )
anaerobic infections
MRSA ( methicillin resistant staphylococcus aureas )
secondary bacterial infection of skin lesions
( eg; chicken pox scars, eczema, scabies )
VIRAL INFECTIONS

Herpes simplex infection
Herpes simplex infection
• Common in immuno – compromised patients
Eg; AIDS, Diabetes, malnourished, etc
• Common sites – lips, genital area
• Presents with sudden eruption of painful grouped vesicles
• Genital herpes is a sexually transmitted disease
• Can be recurrent in some patients
Treatment • Aciclovir
• Topical or oral antibiotics to prevent secondary infections
Chicken pox


Chicken pox • Fever
• Body aches and pains
• Vesicular skin eruption
• Starts from head and gradually spreads to trunk and limbs
• Crusting occurs in 7-10 days
Complications • Common in adults and in immuno suppressed individuals
eg; pneumonia, secondary bacterial infection, myocarditis, thrombocytopenia, encephalitis, osteomyelitis, hepatitis
Treatment
• Aciclovir
• Antibiotics if needed
Chicken pox
• Chicken pox in pregnancy ( 1st trimester ) may lead to foetal abnormalities
Prevention varicella vaccine

Herpes zoster


Herpes Zoster
• Treatment
aciclovir
antibiotics if necessary for the secondary bacterial infection

Molluscum contagiosum

• Treatment
spontaneously resolves sometimes
larger lesions – prick with a sterile needle and extrude the
contents
trichloroacetic acid
electro cautery

Viral warts
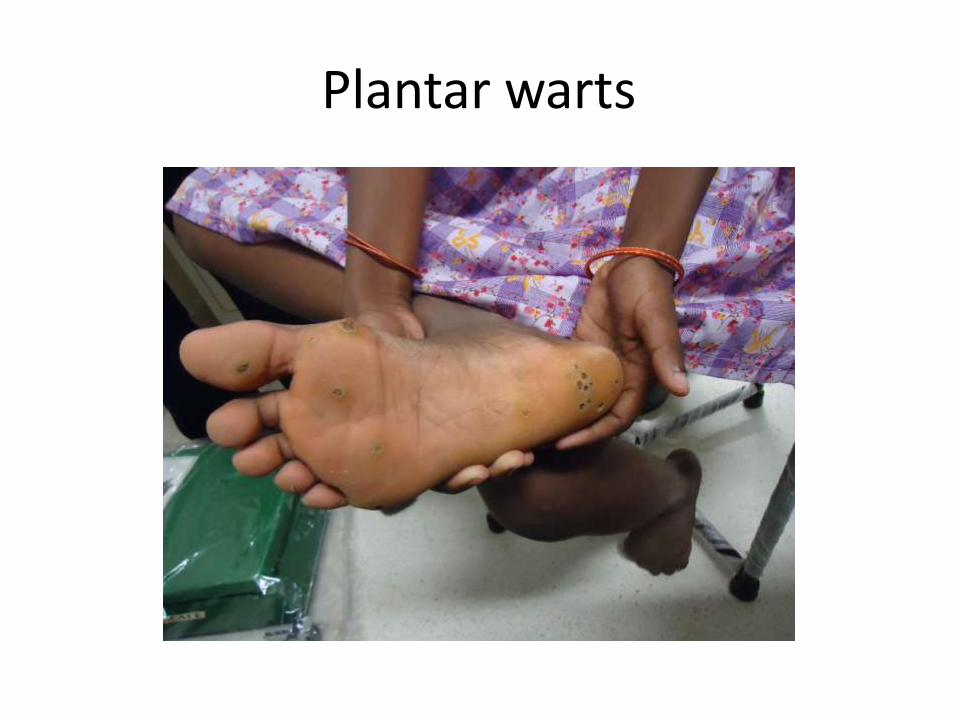
Plantar warts

Plane warts

Treatment
• Cryotherapy
• Electrocautery – in a few occasions
• 5% imiquimod – genital warts
• Wart implantation
• Hypnotherapy

Hand foot mouth disease

FUNGAL INFECTIONS

Tinea corporis

Tinea corporis


Tinea incognito

Tinea capitis

Kerion - due to zoophilic fungal infection

Tinea infections
• Reddish or skin colored patches
• Common sites – groins, buttocks, submammary areas, etc
• Annular or polycyclic
• Elevated edge
• Can be itchy
Treatment • Topical antifungals – miconazole, clotrimazole, terbinafine
• Oral antifungals – griseofulvin, terbinafine

Pityriasis versicolor
Treatment
• Ketoconazole – oral and topical
• Itraconazole – oral
• Fluconazole - oral
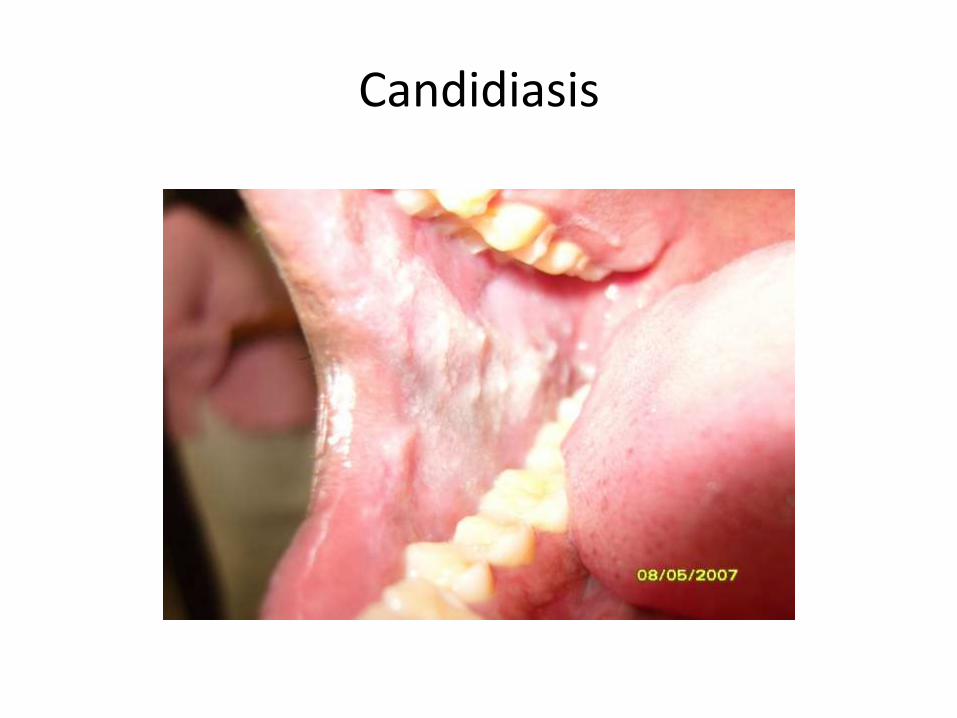
Candidiasis


Candidiasis • Common sites Oral mucosa, genital mucosa, flexural areas ( neck, groins ),
periungual ( around the nails )
• Precipitating conditions Diabetes mellitus, AIDS, other immuno suppressed pts,
Patients on prednisolone and broad spectrum antibiotics
Treatment
miconazole oral paste
2% ketoconazole cream
oral fluconazole, itraconazole

Chromoblastomycosis

Madura foot

Fungal infections
• There are so many other different fungal infections
• Some are deep fungal infections
• Needs skin biopsy and fungal cultures to diagnose them
• Needs prolong oral antifungal treatment

Parasitic infections

Scabies



Crusted scabies



Scabies • Very itchy skin condition
• Papular eruption
• Common sites are finger webs, genital region, abdomen and thighs
• Can lead to crusted scabies in neglected patients
Investigation Skin scrapings – will reveal the parasite – Sarcoptes scabei
• Treatment
5% Permethrin
Sulphar ointment
Benzyl benzoate
Should treat the family members at the same time

LEPROSY
• Caused by Mycobacterium Leprae
• Very slow growing bacterium
• Has a long incubation period before the onset of the clinical disease
• Common in over crowded places with poor ventilation

Tuberculoid Leprosy
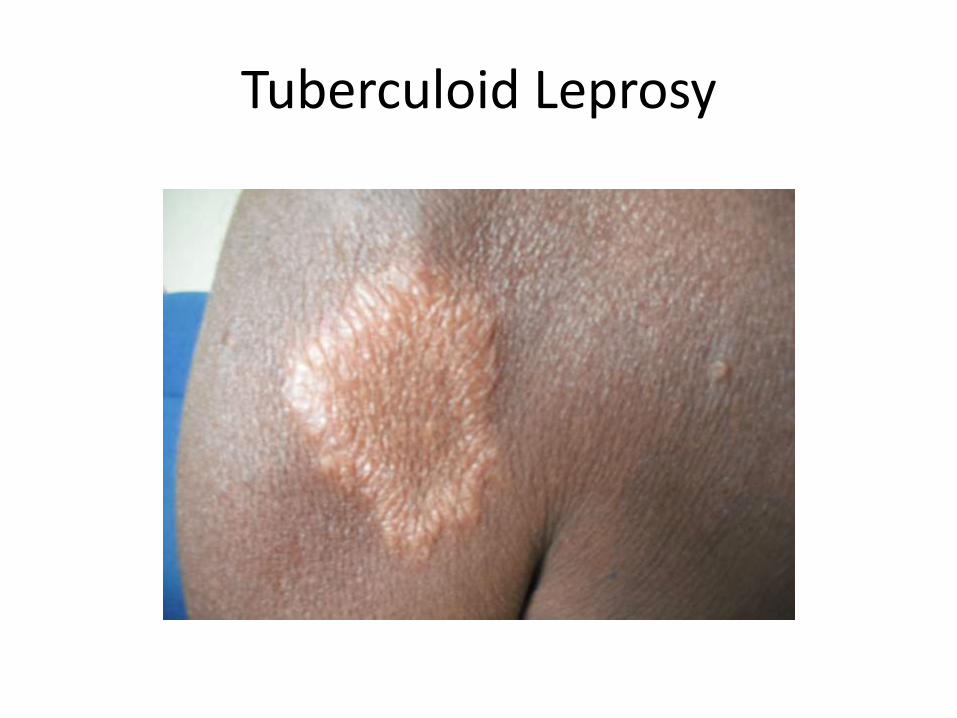
Tuberculoid Leprosy

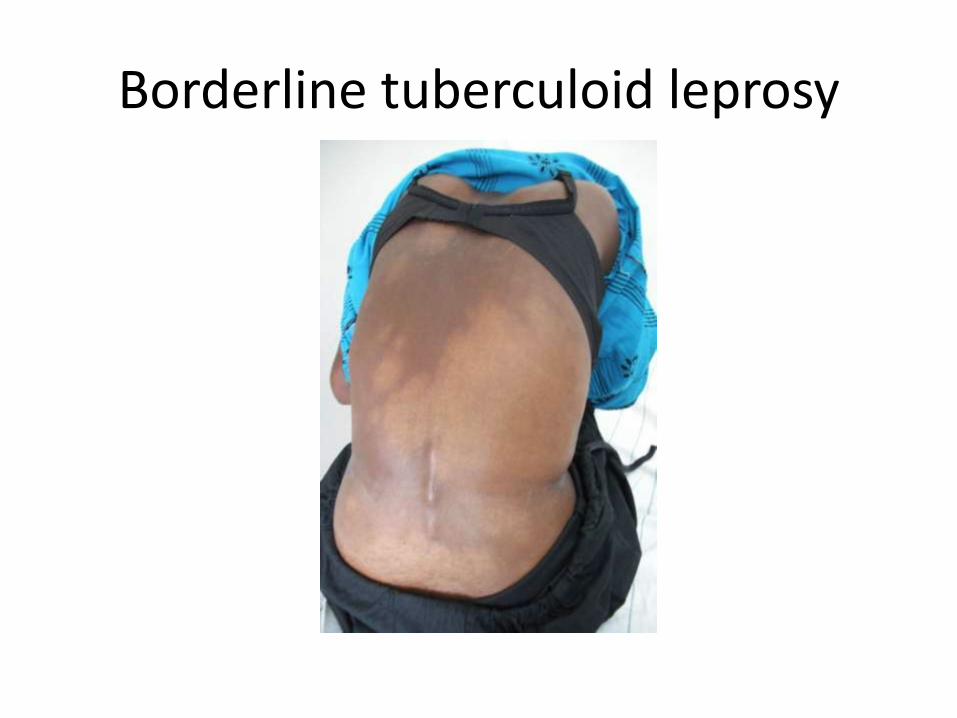
Borderline tuberculoid leprosy


Tuberculoid Leprosy • Presents with
Hypopigmented patches
Sensory impairment
Enlarged superficial nerves
Treatment • Multi drug treatment ( MDT – PB ) for 6months
( pauci bacillary )
Rifampicin
Dapsone
• However MDT ( MB ) for 12 months needed for some patients

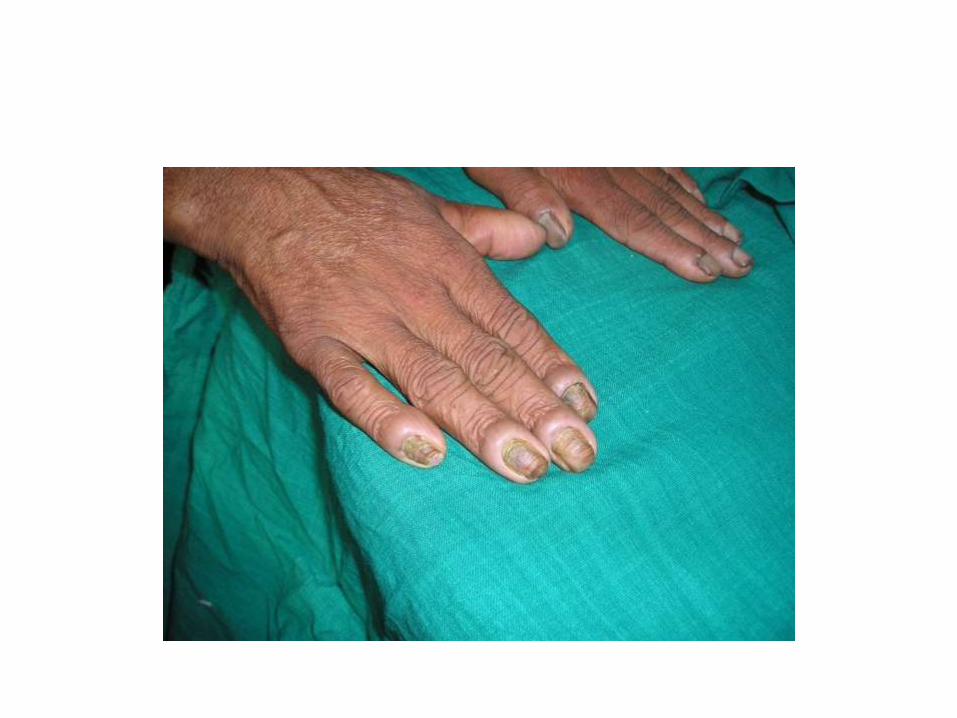
Lepromatous Leprosy

Lepromatous Leprosy • Can be infective to others
• Clinical Features
skin colored and erythematous nodules
Some have leonine facies
Infiltration of the ears
Peripheral neuropathy
Trophic ulcers
Certain internal organs could be involved
• Treatment
Multi drug treatment ( MDT – MB ) for 12months
( multi bacillary )
Rifampicin
Clofazimine
Dapsone


Ulnar claw hand

Trophic ulcers
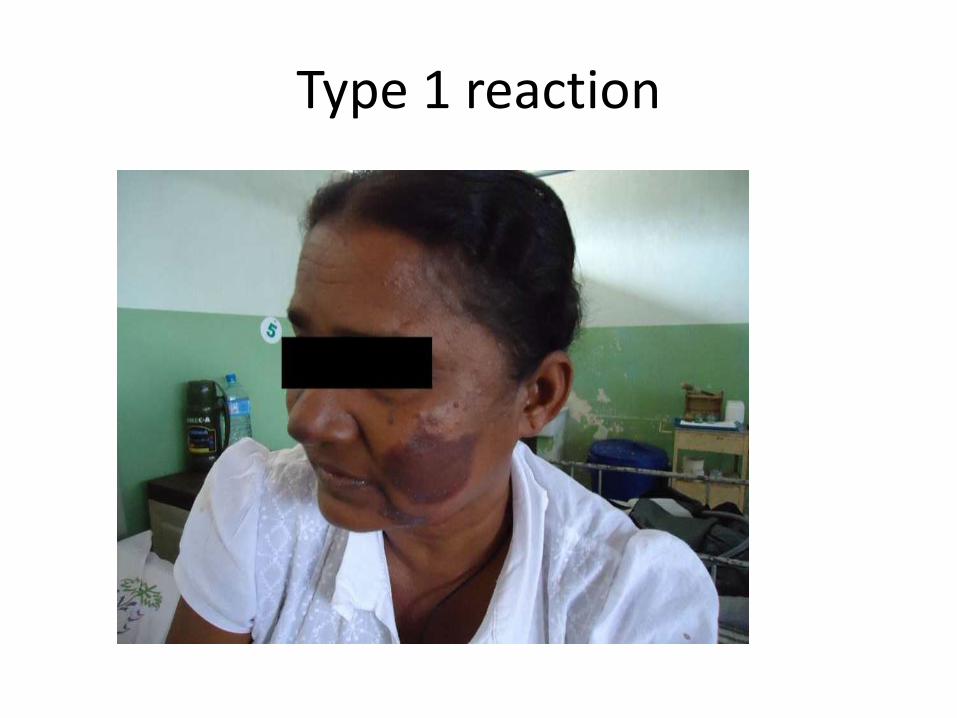
Type 1 reaction

ENL (type 2) reaction

Treatment – Lepra reactions
prednisolone
azathioprine
clofazimine
thalidomide
Cutaneous Tuberculosis (Skin TB) • Long standing non healing skin patches
• Various morphological patterns present
Investigations • Skin biopsy
• Mantoux test
• Chest Xray
• PCR studies
• T spot test
Treatment • Anti TB therapy

Verrucous TB

Scrofuloderma
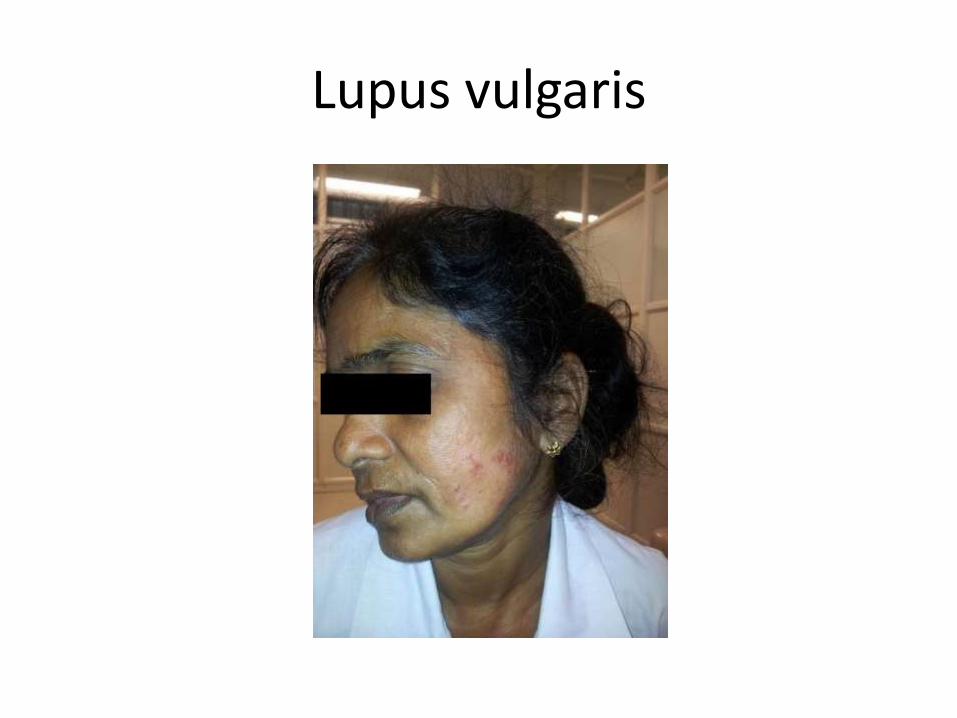
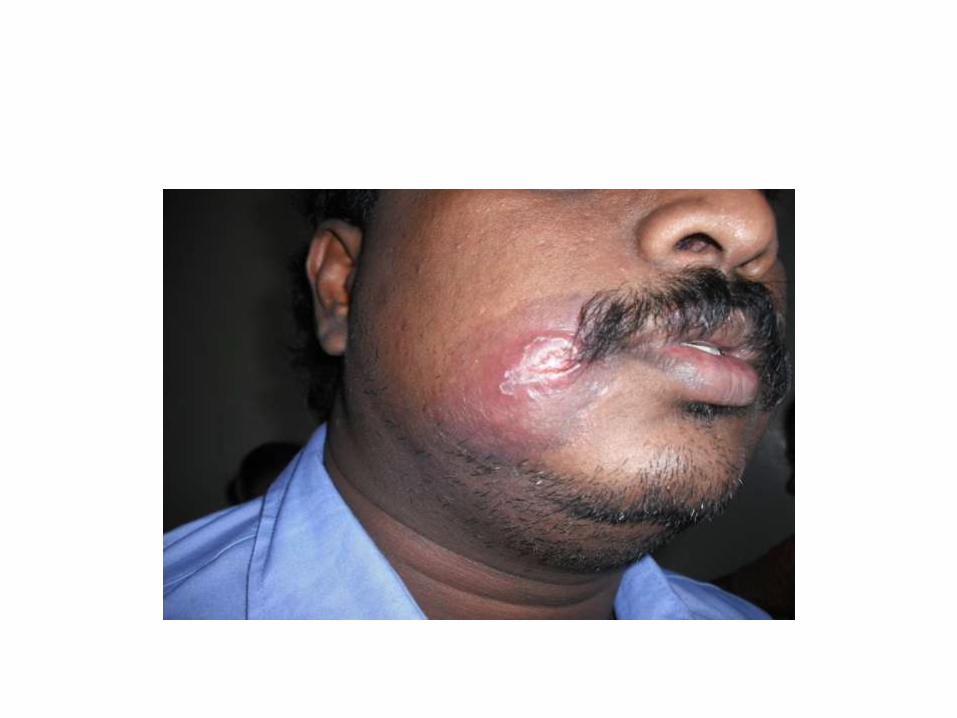
Lupus vulgaris

Cutaneous Leishmaniasis








Cutaneous Leishmaniasis
• Non healing volcano like skin lesions
• Occur on exposed areas of the body
• Common in certain parts of the country
North central province, southern province
Investigations Skin smears to identify the parasite
Skin biopsy for histology
Treatment Liquid nitrogen
Sodium stibo gluconate injection ( local / IM )

NUTRITIONAL
DEFICIENCIES

Zn deficiency

Zn deficiency
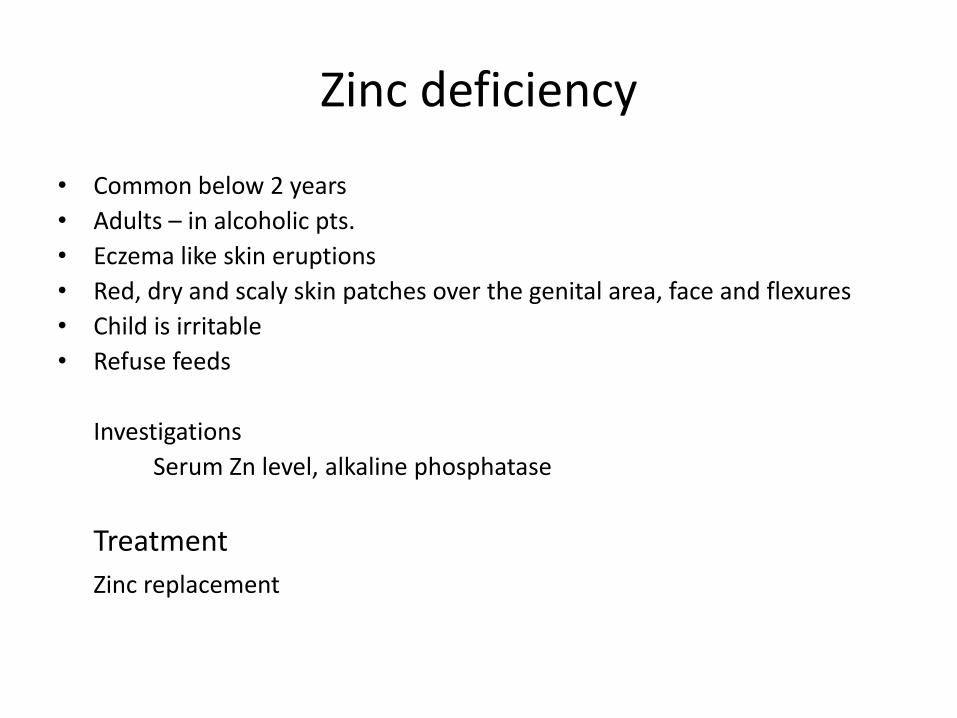
Zinc deficiency
• Common below 2 years
• Adults – in alcoholic pts.
• Eczema like skin eruptions
• Red, dry and scaly skin patches over the genital area, face and flexures
• Child is irritable
• Refuse feeds
Investigations
Serum Zn level, alkaline phosphatase
Treatment
Zinc replacement

Other nutritional deficiencies
• There are many other nutritional deficiencies which cause skin manifestations
Eg; Iron deficiency
Protein energy malnutrition
Biotin deficiency
Essential fatty acid deficiency
B12 deficiency
DRUG ERUPTIONS
Drug Eruptions
• Drug eruptions can present with various patterns
• Proper drug history is important in diagnosis
• Some are mild and some can be life threatening
• Internal organs can be affected in some drug reactions

Morbiliform type eruption

Urticaria

Fixed drug eruption

Striae due to prolong application of topical steroids

Stevens johnson syndrome


Toxic epidermal necrolysis



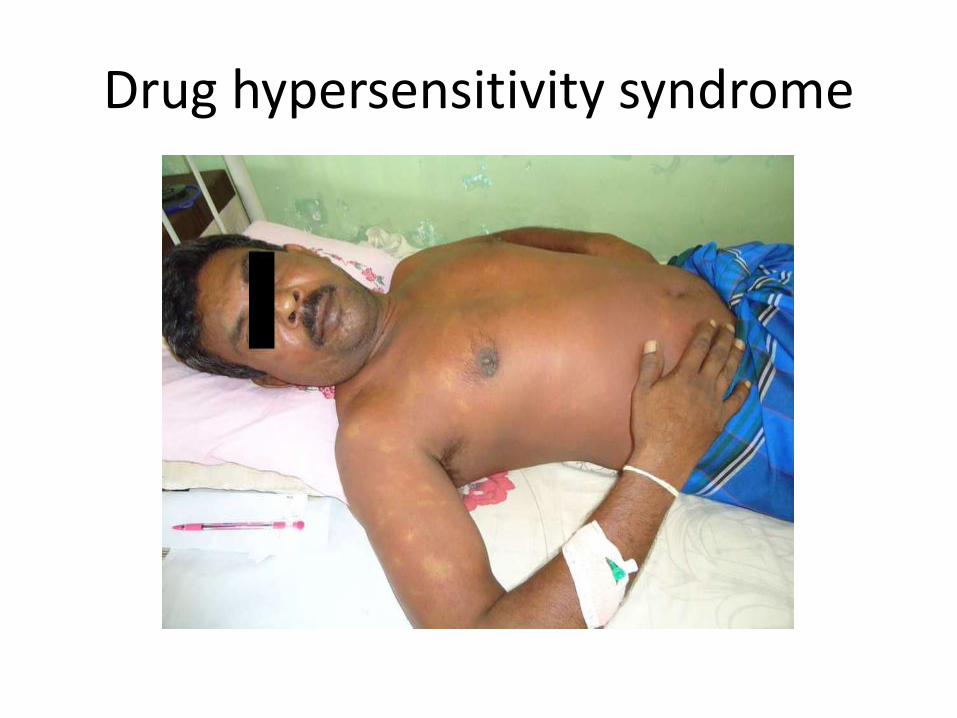
Drug hypersensitivity syndrome

Stevens johnson syndrome and toxic epidermal necrolysis
Can be life threatening Management stop the offending drug immediately monitor the vital functions investigate to detect the internal organ involvement (liver and kidney) skin care oral care eye care – urgent eye referral if eyes are involved increase hydration and fluid balance chart antibiotics to prevent secondary infection prednisolone and IV immunoglobulins sometimes antiepileptics

EXFOLIATIVE DERMATITIS



EXFOLIATIVE DERMATITIS
• More than 90% of the skin is involved
• Itching
• Erythema ( redness )
• Scaling
• Dehydration
• Low urine out put
• Aetiology
Common causes
Eczema, Psoriasis, Drugs, Lymphomas, etc
Treatment
Moisturizers – aquous cream, emulsifying ointment
liquid paraffin
Increase oral fluids and to maintain a fluid balance chart
High protein diet
Antibiotics if there are signs of infection
Antihistamines ( eg; chlorpheniramine ) for itching
skin biopsy
Need to find the aetiology and treat the cause
Needs regular follow up
ACNE


Hidradenitis suppurativa

Punch out & Ice pick Scars

Acne
• Very common skin problem
• Starts around puberty
• Chronic inflammation of the pilosebaceous units
• Clinical features
comedones, papules, pustules, cysts and scars
face, chest and upper back are usually involved
• Need to treat early to prevent unsighty scars

Treatment Depends on the sex, age, severity and extent of the disease
• Topical
benzoyl peroxide
antibiotic creams and lotions – erythromycin, clindamycin
retinoid creams and gels
• Oral
antibiotics – erythromycin, doxycyclines
hormonal – cyproterone acetate with ethynyl estradiol
isotretinoin ( most effective )
• Chemical peeling
salicylic acid and trichloroacetic acid

vasculitis
Vasculitis
• Inflammation of blood vessels
• Hall mark is the ‘palpable purpura’
• Erythematous papules and patches on dependent parts of the body
• Fever, arthralgia, abdominal pain, malaise, etc

Approach to the patient
Suspect vasculitis
Exclude non-vasculitic disorders that mimic vasculitis
Investigate to
establish vasculitis
evaluate the extent of the systemic involvement
look for underlying disorders

Sweets syndrome
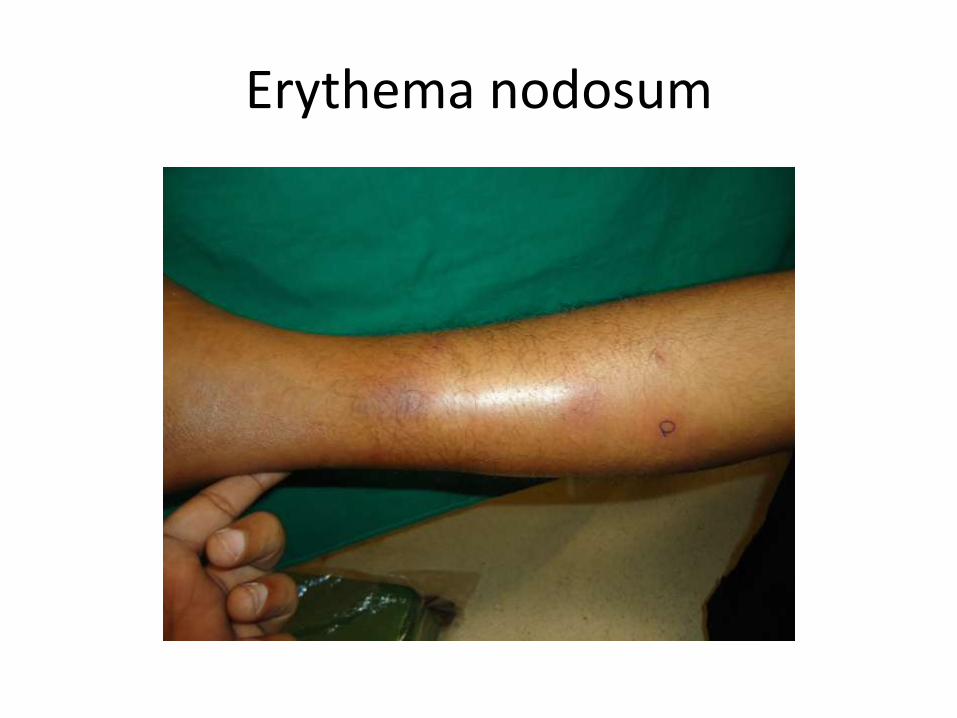
Erythema nodosum

SKIN CANCERS
Skin cancers
• Common in white skin individuals
• Rare in Asians
• Eg;
Basal cell carcinoma, Squamous cell carcinoma, Melanoma, etc
Risk factors
high sun exposure
white skin
family history
immunosupression
chronic ulcers and scarring
arsenic ingestion
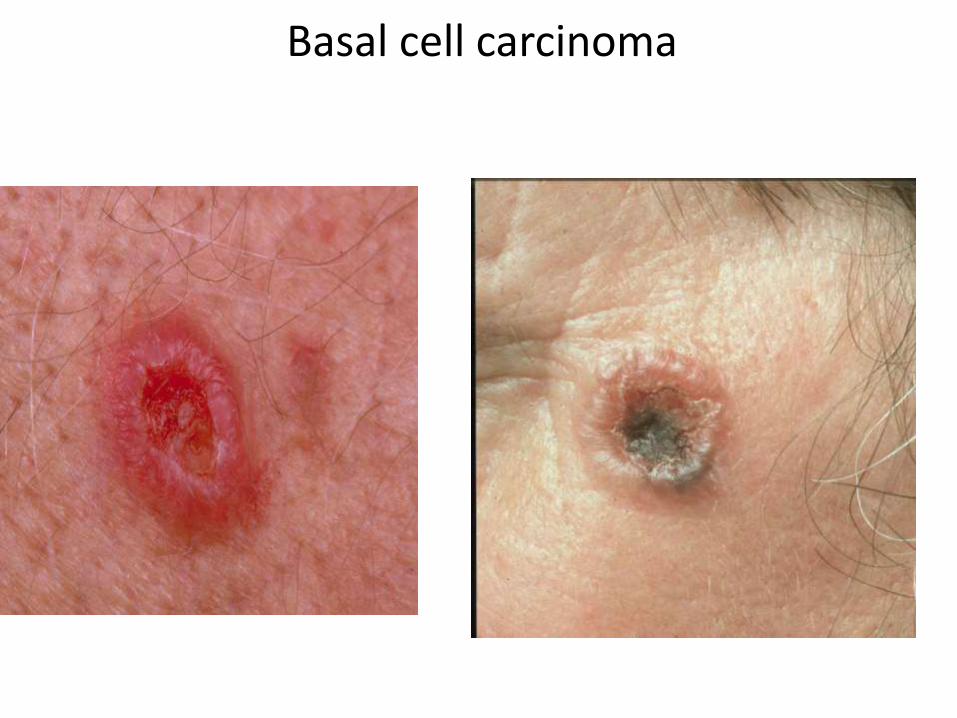
Basal cell carcinoma


Basal cell carcinoma

Squamous cell carcinoma

Squamous cell carcinoma

Malignant melanoma

Management
complete excision
radiotherapy
look for metastases ( local and distal spreading )

BLISTERING DISEASES
Causes of blisters
• Frictional
• Cold and Thermal injury
• Bullous Impetigo
• Diabetes
• Insect bites
• Drug reaction
• Herpes Simplex infection
• Chicken Pox, Herpes Zoster
• Epidermolysis Bullosa
• Autoimmune
Eg; Pemphigus, Pemphigoid

• There are many causes for blisters
• We must find the cause and treat
• Some conditions such as auto immune blistering disorders need special treatment and regular follow up

Pemphigus Vulgaris
Pemphigus Vulgaris • Flaccid blisters
• Easily ruptured and left with erosions
• Mouth, genital area and eyes can be involved
• Can be life threatening
• Common in Asians
Treatment
• Depends on the severity of the disease
• Mainstay of treatment is steroids
• IV dexamethasone and cyclophosphamide pulse therapy
• Antibiotics for the secondary infection
• Sometimes IV Immunoglobulins and plasmapharesis
Bullous Pemphigoid • Tense blisters
• Oral lesions are very rare
• Common in old age
• Incidence is high in west
• Less severe than Pemphigus
Treatment • Prednisolone
• Azathioprine
• Dapsone
• Tetracycline
• Topical steroids


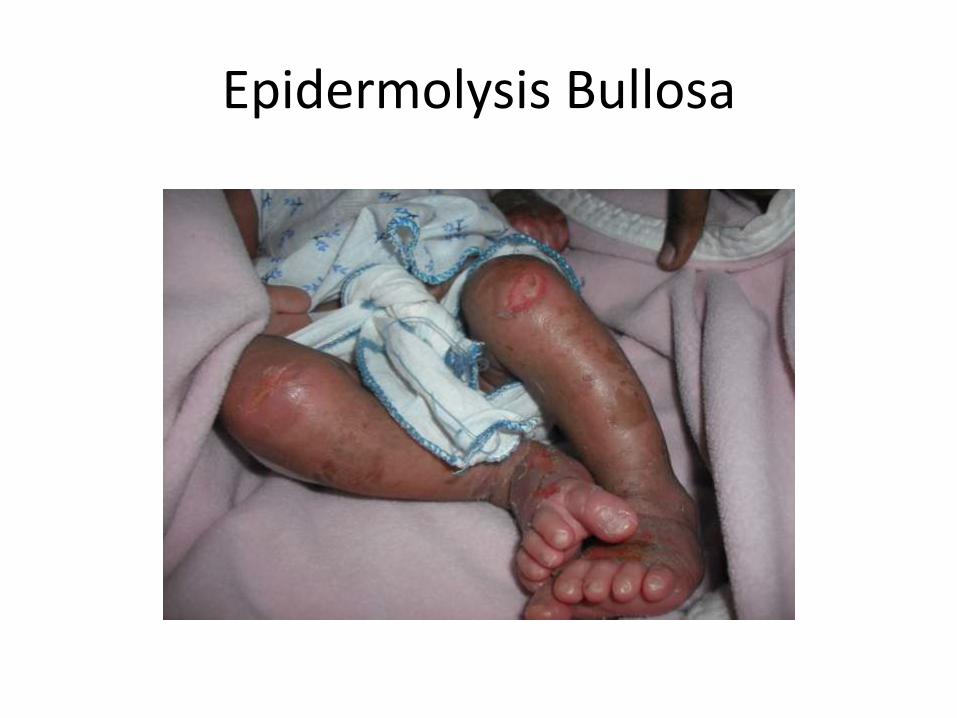
Epidermolysis Bullosa


Epidermolysis Bullosa
• Blisters appear on frictional sites
• These are mechanical blisters
• Exacerbates with sweating, hot and humid climates
Treatment • Prevention of repeated trauma
• Loose clothes
• Keep the skin dry and clean
• Minimal handling
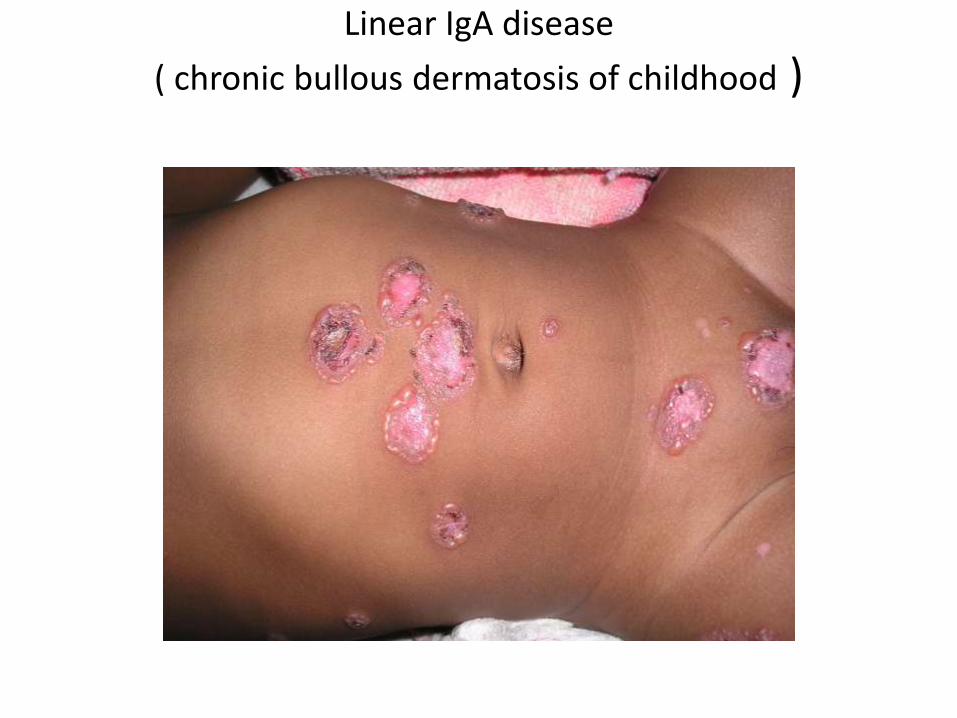
Linear IgA disease
( chronic bullous dermatosis of childhood )

Linear IgA disease
( chronic bullous dermatosis of childhood )


Linear IgA disease
( chronic bullous dermatosis of childhood ) • Tense blisters
• Mainly peri-orificial
( around mouth and genitalia )
• Oral mucosa can be involved
Treatment
• Dapsone
• prednisolone
DIABETES
SKIN MANIFESTATIONS
• Various systemic diseases including Diabetes Mellitus have skin manifestations
• Therefore skin features are important to detect underlying illnesses
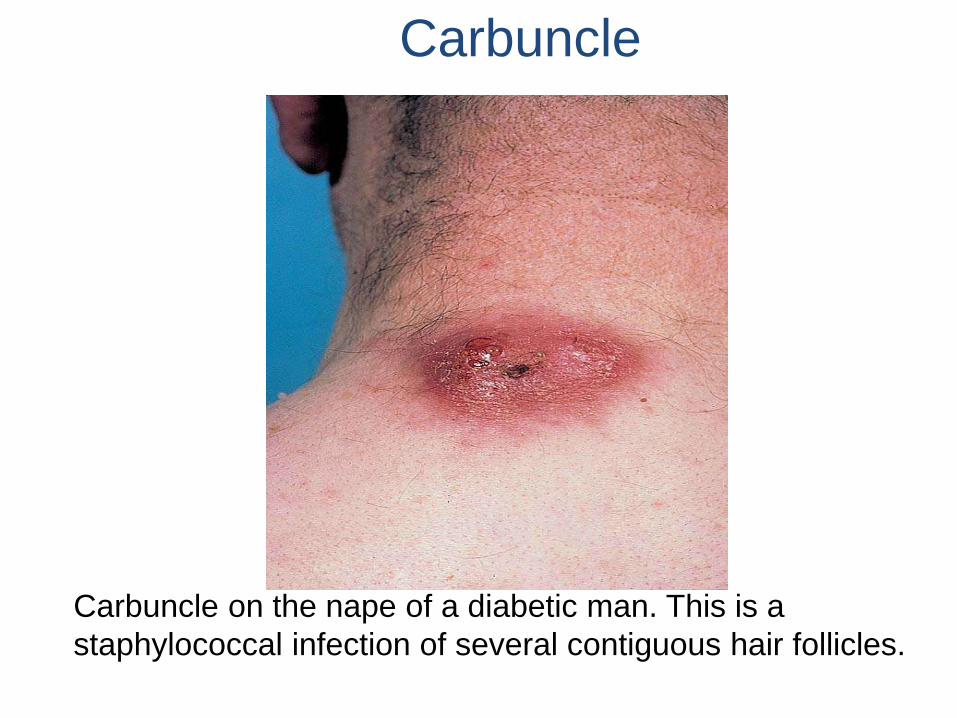
Carbuncle on the nape of a diabetic man. This is a
staphylococcal infection of several contiguous hair follicles.
Carbuncle

Diabetic Bulla

Older lesions of necrobiosis lipoidica are often pigmented as
well as obviously atrophic, but often lose the more inflamed
appearance of more recent lesions.
Necrobiosis Lipoidica

Melasma
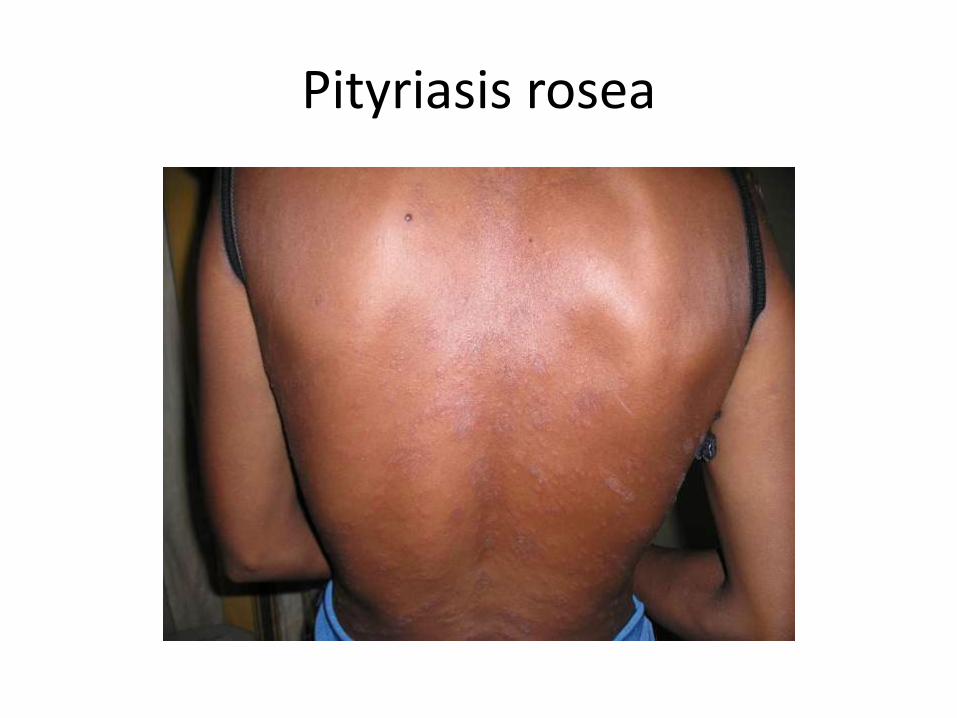
Pityriasis rosea
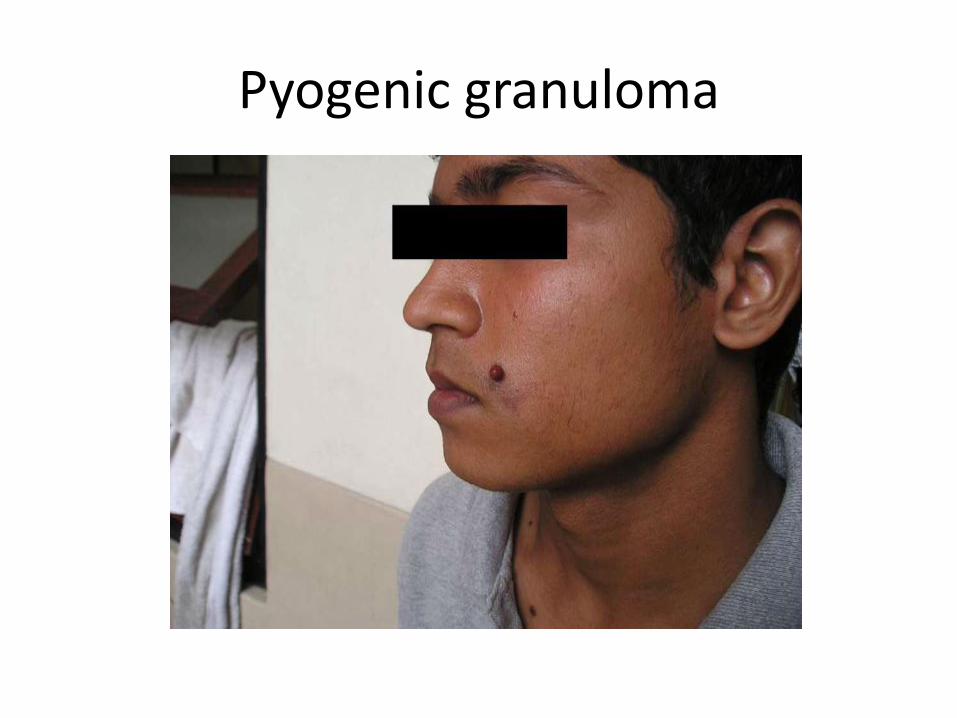
Pyogenic granuloma
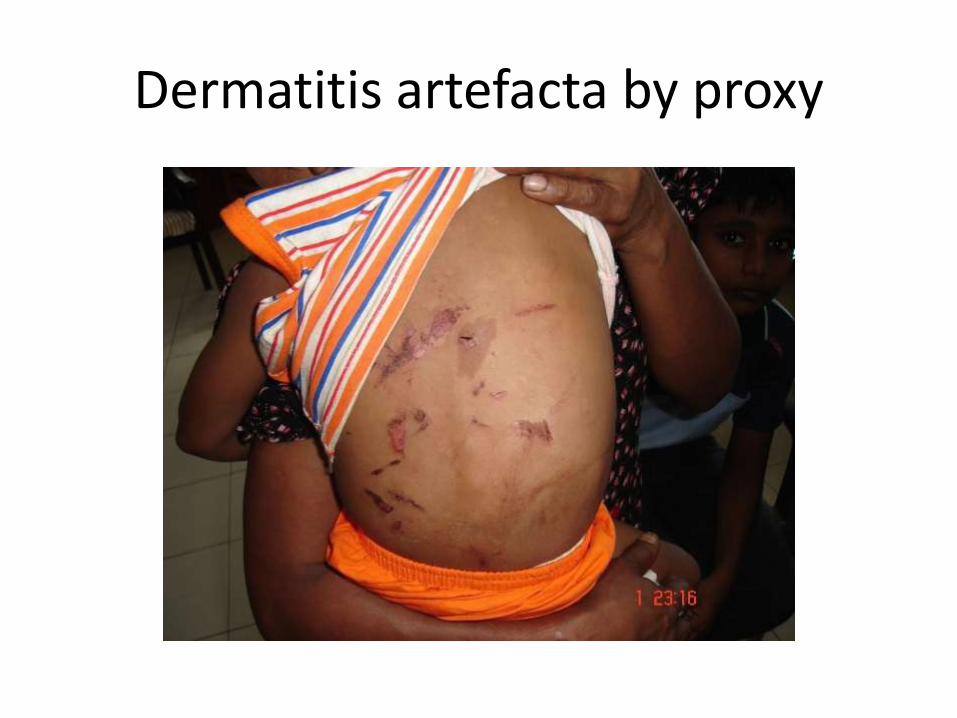
Dermatitis artefacta by proxy

Urticaria

Miliaria

Miliaria

Vitiligo

Lichen planus

Granuloma annulare
