combined chelation of lead (ii) by deferasirox and deferiprone in rats as biological model
TRANSCRIPT
Combined chelation of lead (II) by deferasiroxand deferiprone in rats as biological model
F. Dahooee Balooch • S. J. Fatemi •
M. Iranmanesh
Received: 6 November 2013 / Accepted: 22 November 2013 / Published online: 6 December 2013
� Springer Science+Business Media New York 2013
Abstract In order to investigate the capability of
two chelators deferasirox (DFX or ICL670) and
deferiprone (L1) in removing lead from the body, the
present research was performed. Two does levels of 40
and 80 mg/kg body weight of lead (II) chloride was
given to rats as biological model for 45 days. After
45 days, some toxicity symptoms were observed in
rats such as loss of hair and weight, appearance of red
dots around eyes, weakness and irritability. After lead
application, chelation therapy with DFX and L1 as
mono and combined (DFX, L1 and DFX ? L1) was
done for 10 days. After chelation therapy, lead level in
different tissues reduced. The combined chelation
therapy results showed that these chelators are able to
remove lead from the body and toxicity symptoms
decreased. The combined therapy results (DFX ? L1)
show higher efficacy and lower toxicity compared to
single therapies.
Keywords Lead toxicity � Chelation therapy �Deferasirox � Deferiprone � Rats
Introduction
The excessive amount of pollutants such as heavy
metals in animal feed and feed stuffs are often due to
human actions, resulting from either agricultural,
industrial production, accidental or deliberate misuse
(Mohamed et al. 2009; Aboul-Enein et al. 2010; El-
Beltagi et al. 2010; Afify and El-Beltagi 2011). Lead
(Pb) is a heavy metal with no apparent biological
function. Lead is one of the toxic metals, it is
dangerous to most human body organ if exposure
exceed to tolerable levels. Lead can affect individuals
of any age, but it has a disproportionate effect on
children because their behavioral patterns place them
at higher risk for exposure to lead. Their bodies absorb
a larger percentage of the lead that they ingest and they
exhibit lead toxicity at lower level for exposure than
adults do. Accumulation of lead produces damaging
effects in the hematopoietical, hematic, renal and
gastrointestinal system (Ibrahim et al. 2012). The
chemical agents exposed in the work places affect
various organ and tissue systems, leading to chronic
diseases. Today, lead that is widely found in the nature
and has an increasing use with the industrial advance-
ments is used in printing, rubber, batteries, ceramics,
dye, porcelain manufacturing, accumulator industry
and as a gasoline additive. Especially, the workers of
these industrial branches, persons exposed to lead
environmentally develop disorders in the functions of
vital organs such as brain and kidneys related to the
toxic impact of lead (Hinc Y ilmaz et al. 2012).
F. D. Balooch � S. J. Fatemi (&)
Department of Chemistry, Faculty of Sciences, Shahid
Bahonar University of Kerman, 22 Bahman Blvd,
76169 Kerman, Iran
e-mail: [email protected]
M. Iranmanesh
Department of Chemistry, Faculty of Sciences, Islamic
Azad University, Kerman Branch, Kerman, Iran
123
Biometals (2014) 27:89–95
DOI 10.1007/s10534-013-9689-0
Because of the size and charge similarities, Pb can
substitute Ca and can be deposited in the bone.
Especially, Children are susceptible to Pb-exposure
because the developing skeletal system requires high
calcium levels. Lead deposited in the bone is not
harmful, but may cause nephrotoxicity, neurotoxicity,
and hypertension (Kennish 1992). One of the major
concepts regarding the toxicity of heavy metals is
attributed to their ability to generate reactive oxygen
species (ROS), which cause oxidative stress (Ding
et al. 2001; Pande et al. 2001; Villeda-Hernandez et al.
2001; Hsu and Guo 2002) and consequently enhance
lipid peroxidation, decrease the saturated fatty acids
and increase the unsaturated fatty acid contents of
membranes (Malecka et al. 2001). Many authors
propose that the formation of free radicals is the most
important molecular mechanism of the lead toxicity
(Navarro-Moreno et al. 2009). Several studies have
shown that Pb can accumulate in the brain when its
concentration in the blood is elevated (Sansar et al.
2011). Only 1 h after intestinal absorption, lead
accumulates in bone, kidney, liver and other organs
(Navarro-Moreno et al. 2009). The toxicity of lead is
closely related to age, sex, and route of exposure level
of intake, solubility, metal oxidation state, retention
percentage, and duration of exposure, frequency of
intake, absorption rate, mechanisms and efficiency of
excretion. Lead has been associated with various
forms of cancer, nephrotoxicity, central nervous
system effects and cardiovascular diseases in human
(Ibrahim et al. 2012). In view of these considerations,
there is urgent need for development of a mechanism
for removal of toxic metal ions from the body.
Chelation therapy is the most effective way in
removing toxic element from the body. This kind of
treatment involves the use of chelating drugs that
coordinate to metal ion for the potentially fatal
conditions. These chelators increase the excretion
and subsequent depletion of transition metal in
biological system (Tubafard et al. 2010). In this
procedure, chelators are added to the blood through a
vein or administered orally in order to remove toxic
elements. Clinical investigations of some chelators in
removing various toxic metals in rats have been
previously published by Fatemi et al. (Amiri et al.
2007; Fatemi et al. 2007, 2009, 2012; Saljooghi and
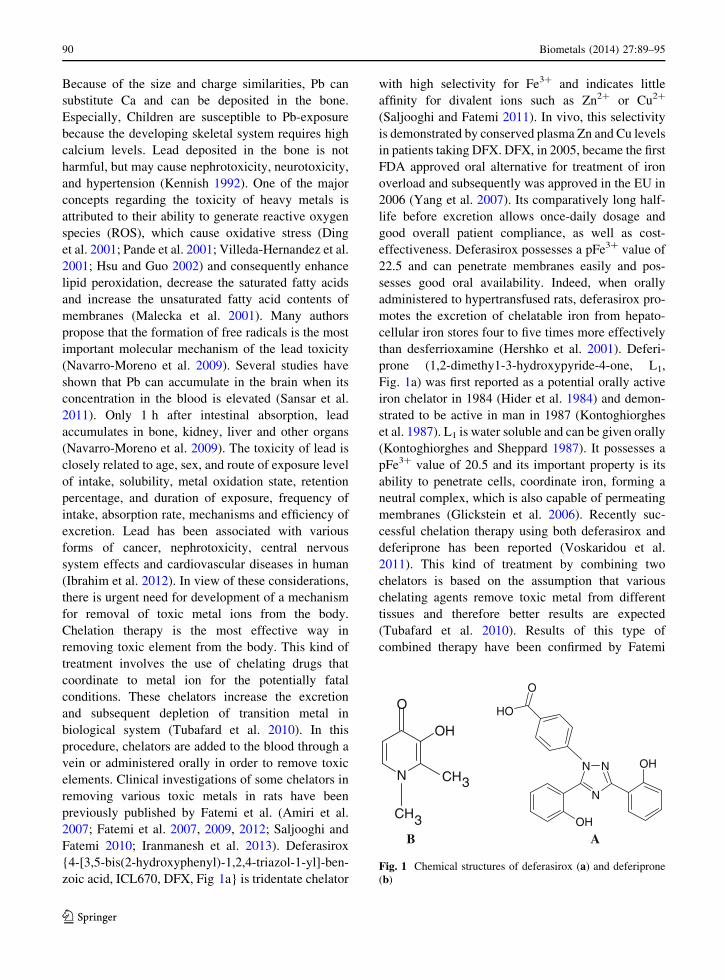
Fatemi 2010; Iranmanesh et al. 2013). Deferasirox
{4-[3,5-bis(2-hydroxyphenyl)-1,2,4-triazol-1-yl]-ben-
zoic acid, ICL670, DFX, Fig 1a} is tridentate chelator
with high selectivity for Fe3? and indicates little
affinity for divalent ions such as Zn2? or Cu2?
(Saljooghi and Fatemi 2011). In vivo, this selectivity
is demonstrated by conserved plasma Zn and Cu levels
in patients taking DFX. DFX, in 2005, became the first
FDA approved oral alternative for treatment of iron
overload and subsequently was approved in the EU in
2006 (Yang et al. 2007). Its comparatively long half-
life before excretion allows once-daily dosage and
good overall patient compliance, as well as cost-
effectiveness. Deferasirox possesses a pFe3? value of
22.5 and can penetrate membranes easily and pos-
sesses good oral availability. Indeed, when orally
administered to hypertransfused rats, deferasirox pro-
motes the excretion of chelatable iron from hepato-
cellular iron stores four to five times more effectively
than desferrioxamine (Hershko et al. 2001). Deferi-
prone (1,2-dimethy1-3-hydroxypyride-4-one, L1,
Fig. 1a) was first reported as a potential orally active
iron chelator in 1984 (Hider et al. 1984) and demon-
strated to be active in man in 1987 (Kontoghiorghes
et al. 1987). L1 is water soluble and can be given orally
(Kontoghiorghes and Sheppard 1987). It possesses a
pFe3? value of 20.5 and its important property is its
ability to penetrate cells, coordinate iron, forming a
neutral complex, which is also capable of permeating
membranes (Glickstein et al. 2006). Recently suc-
cessful chelation therapy using both deferasirox and
deferiprone has been reported (Voskaridou et al.
2011). This kind of treatment by combining two
chelators is based on the assumption that various
chelating agents remove toxic metal from different
tissues and therefore better results are expected
(Tubafard et al. 2010). Results of this type of
combined therapy have been confirmed by Fatemi
NN
N
OH
OH
O
HO
N
OH
O
CH
CH
3
3 A B
Fig. 1 Chemical structures of deferasirox (a) and deferiprone
(b)
90 Biometals (2014) 27:89–95
123

et al. (2011, 2012) (Amiri et al. 2007; Tubafard and
Fatemi, 2008). The aim of present study was to
investigate the capability of DFX and L1 as chelating
agents in chelating and removing lead from the body.
Testing was performed by using a chronic poisoning
model on rats after lead application.
Experimental
Apparatus
Measurement of lead and iron in various tissues were
performed by a Varian flame atomic absorption
spectrometer (FAAS). A microwave oven, model
CEM MDS 200, was used to elimination the water
content present in organs and to facilitate digestion.
Also a Mettler analytical balance Model AE 160 was
used in this research.
Maintenance of the animals
Male Wistar rats were obtained from Kerman Neuro-
science Research center (Kerman, Iran). They kept in
animal house at this Center. The animals were kept
under a controlled light: dark (12:12 h) schedule at
23 ± 1 �C and humidity 50 %. The rats were divided
randomly to control and treated groups and were
maintained in well-cleaned sterilized cages. This
research was allowed by the ethics committee of
Shahid Bahonar University and Kerman Neuroscience
Research Center (Kerman, Iran).
Materials
Lead (II) chloride, L1 and other materials were
purchased from Merck Chemicals Co. and DFX was
purchased from Novartis Co. (Basel, Switzerland).
Methods
In our study, lead at two doses of 40 and 80 mg/kg
body weight was given to rats for 45 days.
In order to investigate side effects of different doses
of lead and evaluate abilities of chelators (DFX and
L1) in removing various doses of lead, we used two
doses of this metal (low and high doses). Animals were
classified as follows (Table 1): the first group (control
group) was given normal food and distilled water to
drink. Rats in this group were killed at the end of lead
administration (day 45). The concentrations of lead
and iron in tissues in control group were compared
with the groups that received lead and chelators. The
treated groups (low and high doses drinking of lead)
were given water containing 40 and 80 mg Pb2?/kg
body weight, respectively. The given dose volume for
rats was calculated based upon their weight. The
control group involved five animals and each of
treated groups had 25 animals. After 45 days, intox-
ication signs appeared and low and high doses groups
were divided to 5 sub-groups: 1. Before chelation
therapy 2. Without chelation therapy 3. Single therapy
with DFX 4. Single therapy with L1 and 5. Combined
therapy with DFX ? L1. In order to compare the lead
and iron concentrations in tissues, before and after
chelation therapy, one group was selected as before
chelation therapy group (vehicle). The rats, in this
group, were anesthetized with ether vapors and were
killed. Kidney, heart, liver, intestine and spleen
samples were weighed, dried and collected for deter-
mination of lead and iron content. In order to
investigate the effect of passing time in removing
lead from rat organs, without chelation therapy group
was selected. In order to investigate the capability of
two chelators (DFX and L1) to remove lead from the
body, chelation therapy was done. Chelators were
given immediately after lead application for 10 days.
Chelators DFX and L1 were given orally as single and
combined therapies. Doses of DFX and L1 were 140
and 300 mg/kg body weight, respectively. Lead
toxicity symptoms appeared in rats, were removed in
short term after drug application. Experiments were
done on 7-week-old Wistar male rats. There wasn’t
notable difference between the groups in the initial
body weight of the rats (mean 230 g), but at the end of
lead application test, those given lead in their diet had
remarkable weight loss (Table 2). Investigation of the
weights in this study indicates that dietary treatment
affected the food intake, whereby rats given normal
diet consumed more food than those given lead. At the
end of chelation therapy, animals were killed and
tissues were taken, dried and collected for determina-
tion of Pb and Fe concentrations. The samples were
put in an oven at 60 �C for 3 days. Then 1 g of each
samples were digested by 1 ml of HNO3. After
digestion, the solutions were vaporized with the
addition of 0.5 ml of H2O2 under the hood. After-
wards, the fragment was diluted with distilled water to
Biometals (2014) 27:89–95 91
123

10 ml volume. Determination of lead and iron in
samples were performed by atomic absorption spec-
trometry. The values are expressed as mean values (at
least three separate determinations) ± standard error
of mean (SEM). The data were subjected to statistical
analysis by Student’s t test; P \ 0.05 was considered
significant.
Result
Comparison of the animals weights indicates that dietary
treatment affects the food intake, whereby animals given
normal diet consumed more food than those given lead. A
significant difference between control and treated groups
was observed. Results of lead raising and iron reduction
in organs of treated groups were statistically different.
The lead accumulation in tissues at the 80 mg/kg dose
(high dose group) was greater than the group at 40 mg/kg
(low dose group). The toxicity symptoms appeared after
45 days of lead administration. Lead toxicity signs in
animals were observed as follows: appearance of red dots
around eyes, weakness, irritability, flaccid, decline
weight and loss of hair. Also, our results shown, as lead
concentration increased in tissues, iron concentration
decreased. The maximum amount of lead accumulation
was found in kidney followed by liver and spleen. After
the chelation therapy, the obtained results indicated that
present lead concentration in all tissues was significantly
reduced and the toxicity signs also decreased. There is
statistical difference between DFX and L1 in reducing the
amount of lead in various tissues. The t-test was applied
to the results assuming the certified values were the true
values. When we compared single therapy efficiencies of
chelators in this study, DFX was more effective in
decreasing lead level in all tissues, whereas, L1 was to be
more effective in kidneys. Comparison of single and
combined therapy shows combined group (DFX ? L1)
is more effective in reducing the lead concentration in all
tissues. The effects of chelators (DFX and L1) application
on lead concentration in the various tissues are shown in
Tables 3 and 4.
The difference between iron concentrations before
and after chelation therapies is remarkable. Iron
concentration was lowest in the group that had the
highest lead level, which is probably due to an
interference that could take place by lead through iron
uptake mechanism. Furthermore, iron concentration
after chelation therapy significantly decreased thus,
consumption of iron tablet is recommended to return
iron level to its normal state. Combination of deferasi-
rox ? deferiprone shows more efficiency in decreasing
iron level. The results of iron concentrations before and
after chelation therapies are shown in Tables 5 and 6. In
order to investigate the spontaneous elimination of lead
from the body by the biological system, one group was
treated without chelation therapy (Mohamed et al. 2009;
Navarro-Moreno et al. 2009). Removal of lead by the
biological system in this group is not noticeable.
Discussion
In order to investigate the abilities of DFX and L1
chelators in removing lead from the body, the
Table 1 Classification of animals
Control group
All
rats
Low and/or high lead
doses drinking
group
Before chelation therapy
Without chelation therapy
(vehicle)
Single therapy with DFX
(140 mg/kg body weight)
Single therapy with L1
(300 mg/kg body weight)
Combined therapy with DFX
(70 mg/kg body
weight) ? L1 (150 mg/kg
body weight)
Table 2 Body weights over 45 days for rats in different groups
Group Control Low dose drinking High dose drinking
Initial body weighta (g) 227 ± 6 (5) (1 day) 225 ± 4 (5) (1 day) 230 ± 6 (5) (1 day)
Final body weighta (g) 285 ± 5 (5) (45 day) 260 ± 7 (5) (47 day) 257 ± 4 (5) (47 day)
Values are mean for the number of observation in parenthesesa Mean of five determination ± standard deviation
92 Biometals (2014) 27:89–95
123
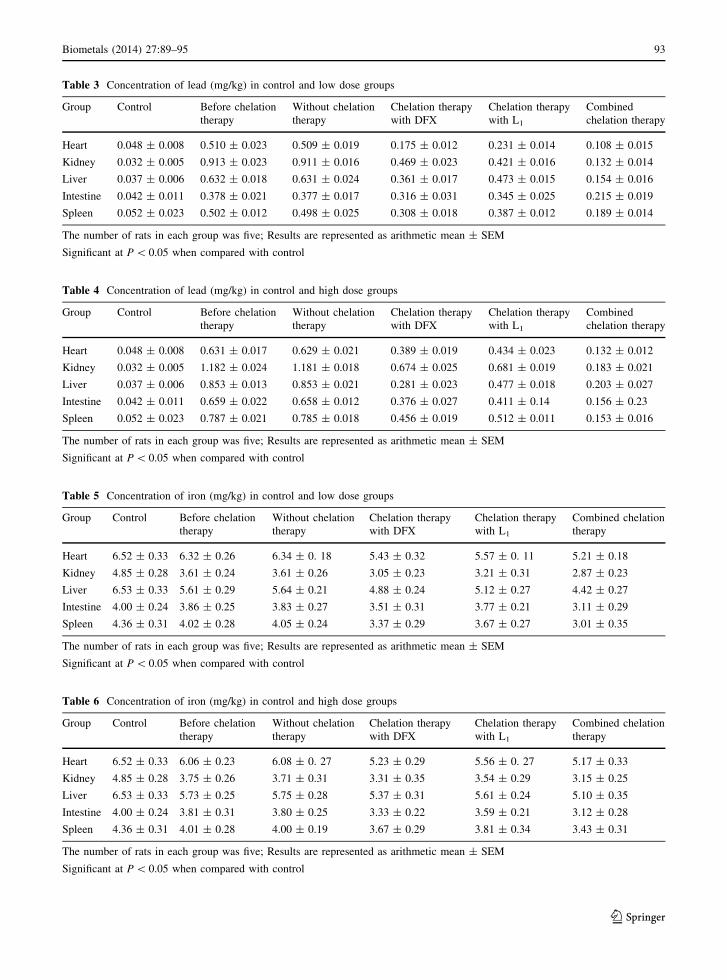
Table 3 Concentration of lead (mg/kg) in control and low dose groups
Group Control Before chelation
therapy
Without chelation
therapy
Chelation therapy
with DFX
Chelation therapy
with L1
Combined
chelation therapy
Heart 0.048 ± 0.008 0.510 ± 0.023 0.509 ± 0.019 0.175 ± 0.012 0.231 ± 0.014 0.108 ± 0.015
Kidney 0.032 ± 0.005 0.913 ± 0.023 0.911 ± 0.016 0.469 ± 0.023 0.421 ± 0.016 0.132 ± 0.014
Liver 0.037 ± 0.006 0.632 ± 0.018 0.631 ± 0.024 0.361 ± 0.017 0.473 ± 0.015 0.154 ± 0.016
Intestine 0.042 ± 0.011 0.378 ± 0.021 0.377 ± 0.017 0.316 ± 0.031 0.345 ± 0.025 0.215 ± 0.019
Spleen 0.052 ± 0.023 0.502 ± 0.012 0.498 ± 0.025 0.308 ± 0.018 0.387 ± 0.012 0.189 ± 0.014
The number of rats in each group was five; Results are represented as arithmetic mean ± SEM
Significant at P \ 0.05 when compared with control
Table 4 Concentration of lead (mg/kg) in control and high dose groups
Group Control Before chelation
therapy
Without chelation
therapy
Chelation therapy
with DFX
Chelation therapy
with L1
Combined
chelation therapy
Heart 0.048 ± 0.008 0.631 ± 0.017 0.629 ± 0.021 0.389 ± 0.019 0.434 ± 0.023 0.132 ± 0.012
Kidney 0.032 ± 0.005 1.182 ± 0.024 1.181 ± 0.018 0.674 ± 0.025 0.681 ± 0.019 0.183 ± 0.021
Liver 0.037 ± 0.006 0.853 ± 0.013 0.853 ± 0.021 0.281 ± 0.023 0.477 ± 0.018 0.203 ± 0.027
Intestine 0.042 ± 0.011 0.659 ± 0.022 0.658 ± 0.012 0.376 ± 0.027 0.411 ± 0.14 0.156 ± 0.23
Spleen 0.052 ± 0.023 0.787 ± 0.021 0.785 ± 0.018 0.456 ± 0.019 0.512 ± 0.011 0.153 ± 0.016
The number of rats in each group was five; Results are represented as arithmetic mean ± SEM
Significant at P \ 0.05 when compared with control
Table 5 Concentration of iron (mg/kg) in control and low dose groups
Group Control Before chelation
therapy
Without chelation
therapy
Chelation therapy
with DFX
Chelation therapy
with L1
Combined chelation
therapy
Heart 6.52 ± 0.33 6.32 ± 0.26 6.34 ± 0. 18 5.43 ± 0.32 5.57 ± 0. 11 5.21 ± 0.18
Kidney 4.85 ± 0.28 3.61 ± 0.24 3.61 ± 0.26 3.05 ± 0.23 3.21 ± 0.31 2.87 ± 0.23
Liver 6.53 ± 0.33 5.61 ± 0.29 5.64 ± 0.21 4.88 ± 0.24 5.12 ± 0.27 4.42 ± 0.27
Intestine 4.00 ± 0.24 3.86 ± 0.25 3.83 ± 0.27 3.51 ± 0.31 3.77 ± 0.21 3.11 ± 0.29
Spleen 4.36 ± 0.31 4.02 ± 0.28 4.05 ± 0.24 3.37 ± 0.29 3.67 ± 0.27 3.01 ± 0.35
The number of rats in each group was five; Results are represented as arithmetic mean ± SEM
Significant at P \ 0.05 when compared with control
Table 6 Concentration of iron (mg/kg) in control and high dose groups
Group Control Before chelation
therapy
Without chelation
therapy
Chelation therapy
with DFX
Chelation therapy
with L1
Combined chelation
therapy
Heart 6.52 ± 0.33 6.06 ± 0.23 6.08 ± 0. 27 5.23 ± 0.29 5.56 ± 0. 27 5.17 ± 0.33
Kidney 4.85 ± 0.28 3.75 ± 0.26 3.71 ± 0.31 3.31 ± 0.35 3.54 ± 0.29 3.15 ± 0.25
Liver 6.53 ± 0.33 5.73 ± 0.25 5.75 ± 0.28 5.37 ± 0.31 5.61 ± 0.24 5.10 ± 0.35
Intestine 4.00 ± 0.24 3.81 ± 0.31 3.80 ± 0.25 3.33 ± 0.22 3.59 ± 0.21 3.12 ± 0.28
Spleen 4.36 ± 0.31 4.01 ± 0.28 4.00 ± 0.19 3.67 ± 0.29 3.81 ± 0.34 3.43 ± 0.31
The number of rats in each group was five; Results are represented as arithmetic mean ± SEM
Significant at P \ 0.05 when compared with control
Biometals (2014) 27:89–95 93
123

distribution of lead was carried out and amount of
accumulation and toxic effects of lead on rats as
biological model was studied. In this study, a short-
term experimental model was used to speed up the
preliminary testing procedure. Lead is disharmonic
element with contexture of body. In contrast to other
vital elements such as zinc and selenium, tissues of
body identify lead as poison. Most of lead content
accumulate in kidney and liver. Chelation therapy is
one of the most effective ways to remove toxic metals
from the biological system. It has been reported that
the chelating agents having higher stability constants
with a metal in aqueous solution may also prove
successful in reducing the body burden of the metal
(Iranmanesh et al. 2013). Many studies have now
reported the high absorption/distribution, long-term
efficacy and safety of deferasirox and deferiprone in
removing some toxic metal ions and treating iron
overload in patients with b–thalassaemia major (Cap-
pellini 2008; Neufeld 2006; Hoffbrand et al. 2003).
After administration of chelators, the lead content
reduced, which shows that both of chelators (DFX, L1)
increases the removal of lead in tissues and also
toxicity symptoms were decreased. A comparison of
the results obtained from with and without chelation
therapies indicate that combined therapy (DFX ? L1)
enhances the removal of lead from rat organs consid-
erably and treat the side effects and general toxicity
symptoms caused by lead. Also, the toxicity and side
effects of combined therapy are lower than single
therapy. At present, combination therapy with deferi-
prone and desferrioxamine, that is highly selective for
iron(III) under biological conditions (pFe3? = 26.6),
is reported to be the most effective treatment for many
patients (Galanello et al. 2010). Desferrioxamine with
a higher pFe3? values acting as a sink. Presumably
deferasirox, also possessing a higher pFe3? values
than deferiprone, behaves in a similar manner.
Recently successful chelation therapy using both
deferasirox and deferiprone has been reported (Vosk-
aridou et al. 2011). In order for a chelating agent to
exert its pharmacological effect, a drug must be able to
reach the target sites at sufficient concentration. Each
of chelators (DFX and L1) has a different target tissue;
therefore, combination of them can help to remove
lead from various tissues effectively. The combined
therapy procedure is likely to increase metal excretion,
target specific metal tissues, minimize side effects (by
virtue of the use of lower doses) and improve
compliance. L1 by virtue of its bidentate nature and
the ability for iron(III) at neutral pH values, is highly
concentration dependent and at relatively low con-
centrations (\5 lM) the iron deferiprone complex will
donate iron to competing ligands (Devanur et al. 2008)
such as deferasirox. DFX, by virtue of its small size
and the ability to penetrate cells (Ma et al. 2012), has
capability of efficiency scavenging excess iron. By
considering of these characteristics, combination of
these chelators is more effective than single one in
removing of lead from rat organs. The important
finding that deferiprone leaves tissue iron at a level
close to normal is fundamental and would suggest that
the proposed use of this chelator will not be highly
toxic. The reason for this important observation is that
deferiprone is able to redistribute iron in mammals
(Evans et al. 2012). From the previous results obtained
by Fatemi et al. (2011, 2012) (Amiri et al. 2007;
Tubafard and Fatemi 2008) and our present results, it
can be concluded that two chelators (DFX ? L1) are
more effective as combined therapy than single
therapy in removal of lead from the body. Therefore,
DFX ? L1 combination seems to be a promising drug
of lead-mobilizing agent. This study might be effec-
tive for preliminary testing of the ability of chelating
agent in removing lead. Therefore after essential
preclinical experiments, this could be suggested for
human administration.
References
Aboul-Enein AM, AbouElella FN, Abdullah ES (2010) Moni-
toring of some organochlorines and organophosphorus
residues in imported and locally raised chicken and bovine
muscles in Egypt. J Appl Sci Res 6(6):600–608
Afify AMR, El-Beltagi HS (2011) Effect of the insecticide cy-
anophos on liver function in adult male rats. Fresen Envi-
ron Bull 20(4a):1084–1088
Amiri A, Fatemi SJ, Fatemi SN (2007) Removal of thallium by
combining desferrioxamine and deferiprone chelators in
rats. Biometals 20(2):159–163
Cappellini MD (2008) Long-term efficacy and safety of defer-
asirox. Blood Rev 22:35–41
Devanur LD, Neubert H, Hider RC (2008) The fenton activity of
iron(III) in the presence of deferiprone. J Pharm Sci
97:1454–1467
Ding Y, Gonick HC, Vaziri ND, Liang K, Wei L (2001) Lead-
induced hypertension. III. Increased hydroxyl radical pro-
duction. Am J Hypertens 14(2):169–173
El-Beltagi HS, Mohamed AA, Rashed MM (2010) Response of
antioxidative enzymes to cadmium stress in leaves and
94 Biometals (2014) 27:89–95
123
roots of radish (Raphanus sativus L.). Not Sci Biol
2(4):76–82
Evans RW, Kong X, Hider RC (2012) Iron mobilization from
transferrin by therapeutic iron chelating agents. Biochim
Biophys Acta 1820:282–290
Fatemi SJ, Amiri A, Bazargan MH, Tubafard S, Fatemi SN
(2007) Clinical evaluation of desferrioxamine (DFO) for
removal of thallium ions in rat. Int J Artif Org 30:902–905
Fatemi SJ, Tubafard S, Nadi B (2009) Evaluation of the effect of
cadmium on rat organs and investigation of diethyl car-
bamate as an oral drug in treatment of cadmium toxicity.
Med Chem Res 18(3):179–186
Fatemi SJ, Sh Saljooghi A, Dahooee BF, Iranmanesh M, Gol-
bafn MR (2011) Chelation of cadmium by combining
deferasirox and deferiprone in rats. Toxicol Ind Health
27(4):371–377
Fatemi SJ, Saljooghi AS, Balooch FD, Iranmanesh M, Golbafan
MR (2012) Removal of cadmium by combining deferasi-
rox and desferrioxamine chelators in rats. Toxicol Ind
Health 28(1):35–41
Galanello R, Agus A, Campus S, Danjou F, Giardina PJ, Grady
RW (2010) Combined iron chelation therapy. Ann NY
Acad Sci 1202:79–86
Glickstein H, BenEl R, Link G, Breuer W, Konijn AM, Hershko
C, Nick H, Cabantchik ZI (2006) Action of chelators in
iron-loaded cardiac cells: accessibility to intracellular labile
iron and functional consequences. Blood 108:3195–3203
Hershko C, Konijn AM, Nick HP, Breuer W, Cabantchik ZI,
Link G (2001) ICL670A: a new synthetic oral chelator:
evaluation in hypertransfused rats with selective radioiron
probes of hepatocellular and reticuloendothelial iron stores
and in iron-loaded rat heart cells in culture. Blood
97(4):1115–1122
Hider RC, Kontoghiorghes G, Silver J (1984) Pharmaceutical
compositions. UK patent 2,118,176A
Hinc Y ilmaz MD, Alper Keten MD, Emre Karacaoglu MD,
Engin Tutkun MD, Ramazan Akcan MD (2012) Analysis
of the hematological and biochemical parameters related to
lead intoxication. J Forensic Legal Med 19(8):452–454
Hoffbrand AV, Cohn A, Hershko C (2003) Role of deferiprone
in chelation therapy for transfusional iron overload. Blood
102:17–24
Hsu PC, Guo YL (2002) Antioxidant nutrients and lead toxicity.
Toxicology 180(1):33–44
Ibrahim NM, Eweis EA, El-Beltagi HS, Abdel-Mobdy YE
(2012) Effect of lead acetate toxicity on experimental male
albino rat. Asian Pac J Trop Biomed 2(1):41–46. doi:10.
1016/S2221-1691(11)60187-1
Iranmanesh M, Fatemi SJ, Ebrahimpour R, Dahooee FB (2013)
Chelation of chromium (VI) by combining deferasirox and
deferiprone in rats. Biometals 26(3):465–471
Kennish MJ (1992) Ecology of estuaries: anthropogenic effects.
CRC Press, Boca Raton. ISBN 9780849380419
Kontoghiorghes GJ, Sheppard L (1987) Simple synthesis of the
potent chelators 1-alkyl-3- hydroxy-2-mehylpyrid-4-ones.
Inorg Chim Acta 136:111–112
Kontoghiorghes GJ, Aldouri MA, Hoffbrand AV (1987)
Effective chelation of iron in beta thalassaemia with the
oral chelator 1,2-dimethyl-3-hydroxypyrid-4-one. Br Med
J 295:1509–1512
Ma Y, Zhou T, Kong X, Hider RC (2012) Chelating agents for
the treatment of systemic iron overload. Curr Med Chem
19:2816–2827. doi:10.2174/092986712800609724
Malecka A, Jarmuszkiewicz W, Tomaszewska B (2001) Anti-
oxidative defense to lead stress in sub cellular compart-
ments of pea root cells. Acta Biochim Pol 48:687–698
Mohamed AA, El-Beltagi HS, Rashed MM (2009) Cadmium
stress induced change in some hydrolytic enzymes, free
radical formation and ultrastructural disorders in radish
plant. Electron J Environ Agric Food Chem 8(10):967–983
Navarro-Moreno LG, Quintanar-Escorza MA, Gonzalez S,
Mondragon R, Cerbon-Solorzano J, Valdes J, Calderon-
Salinas JV (2009) Effects of lead intoxication on intercel-
lular junctions and biochemical alterations of the renal
proximal tubule cells. Toxicol In Vitro 23(7):1298–1304
Neufeld EJ (2006) Oral chelators deferasirox and deferiprone
for transfusional iron overload in thalassemia major: new
data, new questions. Blood 107(9):3436–3441
Pande M, Mehta A, Pant BP, Flora SJ (2001) Combined
administration of a chelating agent and an antioxidant in
the prevention and treatment of acute lead intoxication in
rats. Environ Toxicol Pharm 9(4):173–184
Saljooghi AS, Fatemi SJ (2010) Clinical evaluation of Defer-
asirox for removal of cadmium ions in rat. Biometals
23(4):707–712
Saljooghi AS, Fatemi SJ (2011) Removal of thallium by def-
erasirox in rats as biological model. J Appl Toxicol
31(2):139–143
Sansar W, Ahboucha S, Gamrani H (2011) Chronic lead
intoxication affects glial and neural systems and induces
hypoactivity in adult rat. Acta Histochem 113(6):601–607.
doi:10.1016/j.acthis.2010.06.005
Tubafard S, Fatemi SJ (2008) Chelation of bismuth by com-
bining desferrioxamine and deferiprone in rats. Toxicol Ind
Health 24(4):235–240
Tubafard S, Fatemi SJ, Saljooghi AS, Torkzadeh M (2010)
Removal of vanadium by combining desferrioxamine and
deferiprone chelators in rats. Med Chem Res 19:854–863.
doi:10.1007/s00044-009-9235-3
Villeda-Hernandez J, Barroso-Moguel R, Mendez-Armenta M,
Nava-Ruiz C, Huerta-Romero R, Rios C (2001) Enhanced
brain regional lipid peroxidation in developing rats
exposed to low level lead acetate. Brain Res Bull
55(2):247–251
Voskaridou E, Christoulas D, Terpos E (2011) Successful che-
lation therapy with the combination of deferasirox and
deferiprone in a patient with thalassaemia major and per-
sisting severe iron overload after single-agent chelation
therapies. Br J Haematol 154:654–656
Yang LP, Keam SJ, Keating GM (2007) Deferasirox: a review of
its use in the management of transfusional chronic iron
overload. Drugs 67(15):2211–2230
Biometals (2014) 27:89–95 95
123