colorectal neoplasms
TRANSCRIPT
COLORECTAL
NEOPLASMS
By
Dr. Abdul QadeerMBBS; FCPS; FICS
Assistant Professor in Surgery
King Faisal University College of Medicine
Kingdom of Saudi Arabia
OBJECTIVES
1. Clinical anatomy of colon & rectum
2. Physiology of colon
3. Colorectal polyps
4. Adenoma-carcinoma sequence
5. Classification of colorectal cancer
6. Signs & symptoms
7. Causes
8. Pathogenesis
OBJECTIVES (CONTD….)
9. Diagnosis
10. Prevention: Lifestyle, medication, screening
11. Management: surgery, chemotherapy,
radiation, palliative care
12. Prognosis
13. Follow-up
14. Epidemiology
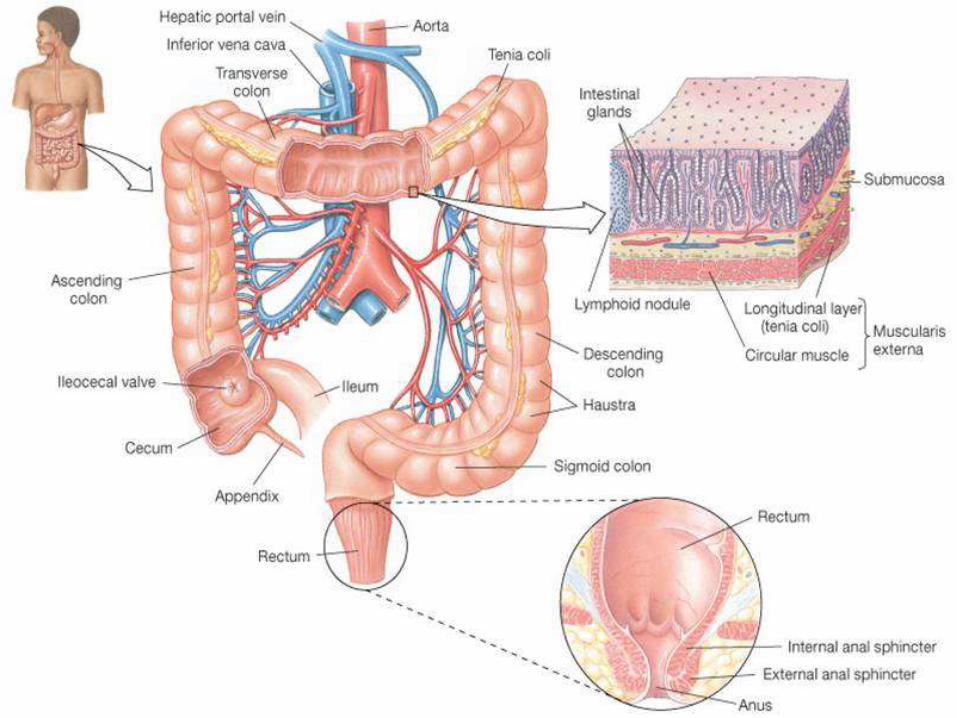
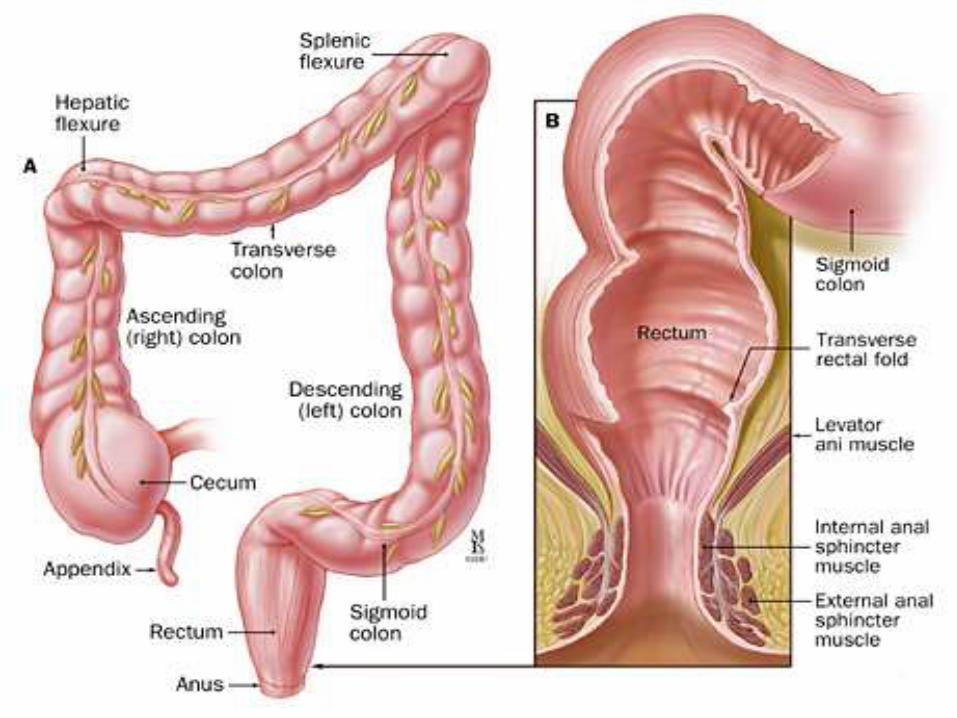
1. CLINICAL ANATOMY OF COLON & RECTUM
Large intestine (Colon & rectum) begins at ileo-caecal valve and extends up to the anus
Consists of:
1. Caecum (with appendix attached),
2. Ascending colon,
3. Hepatic flexure,
4. Transverse colon with attached greater omentum,
5. Splenic flexure,
6. Descending colon,
7. Sigmoid colon and
8. Rectum (begins at sacral promontry)
Transverse and sigmoid colon are mobile
Ascending, descending colon and rectum are
fixed
Apendices epiploicae
Taenia coli
Haustrations

ANATOMICAL RELATIONS
Posterior relations of cecum & ascending
colon are:
1. Right ureter
2. Right gonadal vessels
3. Duodenum
Posterior relations of left colon are:
1. Left ureter
2. Left gonadal vessels
3. Tail of pancreas
Rectum is 12-18 cm long in adults, encircled
by the puborectalis muscle, creating an
anorectal ring (120o)
It has three curves, 2 on right side and 1 on
left side
Theses curves make semicircular folds
(Houston’s valves) from inside
ANATOMICAL RELATIONS OF THE RECTUM
Its upper 1/3rd = peritoneum anteriorly +
laterally
Its middle 1/3rd = peritoneum anteriorly
Its lower 1/3rd = no peritoneum covering
Anteriorly = prostate/vagina separated by the
Denonvilliers’ fascia
Posteriorly = sacrum & coccyx separated by
Waldeyer’s fascia
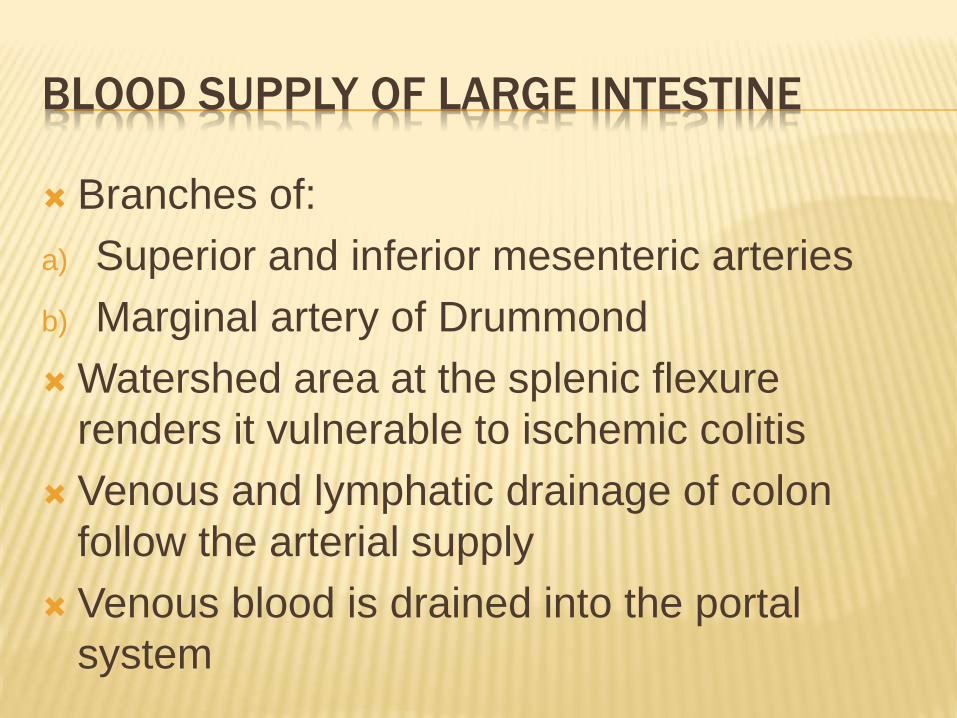
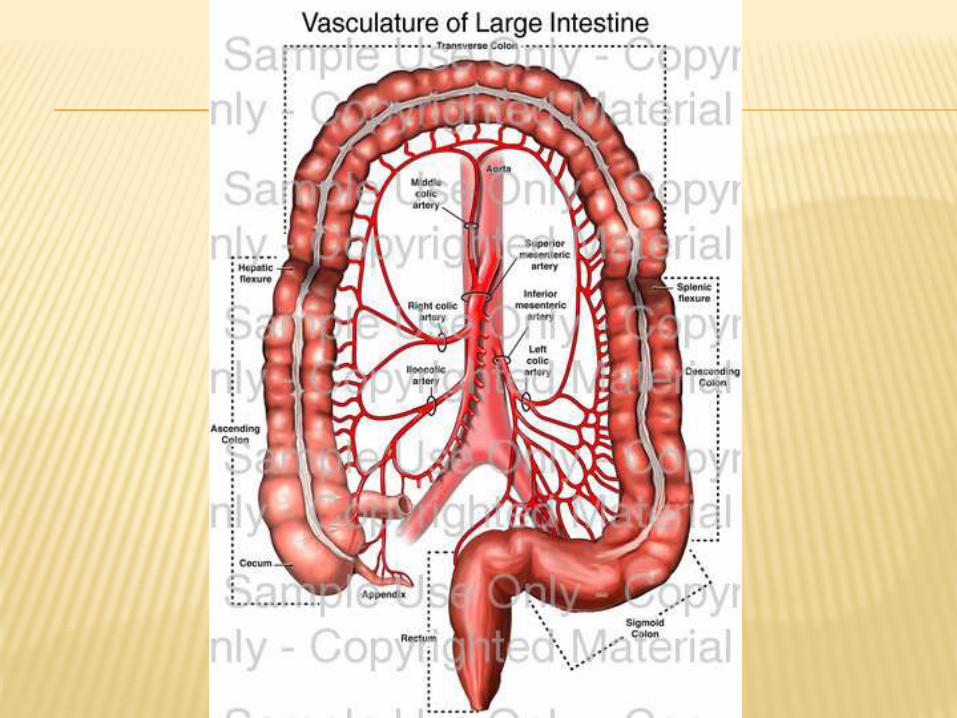
BLOOD SUPPLY OF LARGE INTESTINE
Branches of:
a) Superior and inferior mesenteric arteries
b) Marginal artery of Drummond
Watershed area at the splenic flexure
renders it vulnerable to ischemic colitis
Venous and lymphatic drainage of colon
follow the arterial supply
Venous blood is drained into the portal
system
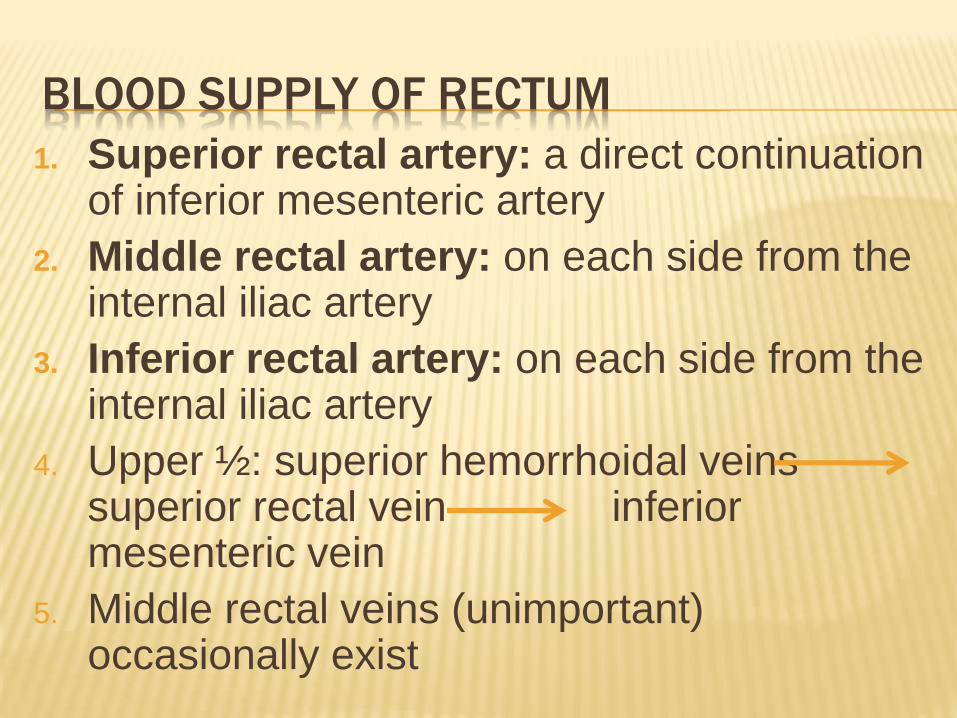
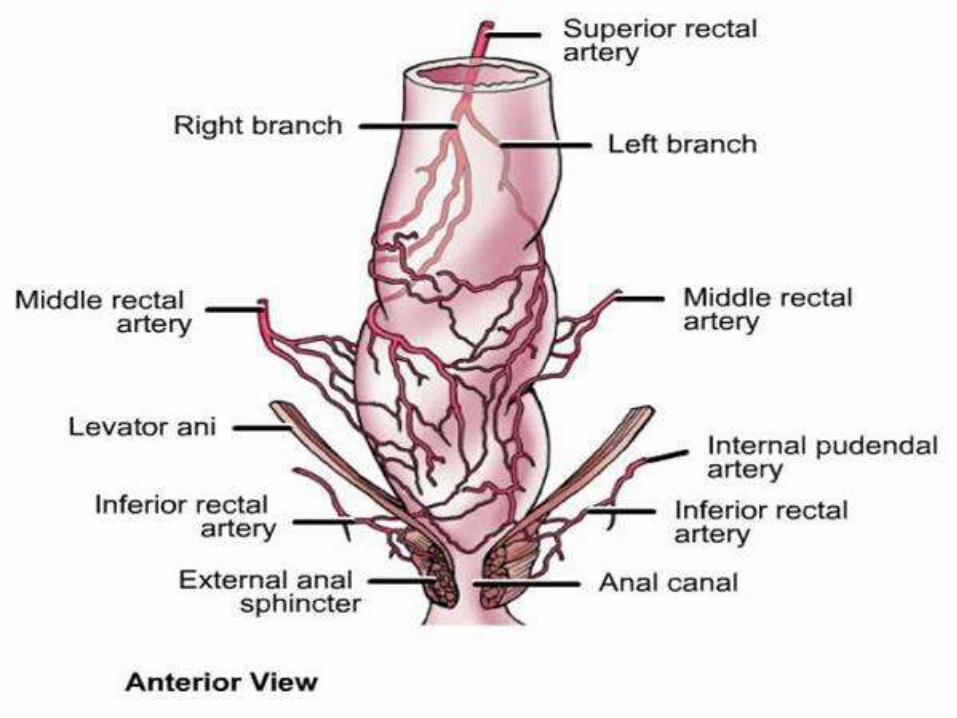
BLOOD SUPPLY OF RECTUM
1. Superior rectal artery: a direct continuation of inferior mesenteric artery
2. Middle rectal artery: on each side from the internal iliac artery
3. Inferior rectal artery: on each side from the internal iliac artery
4. Upper ½: superior hemorrhoidal veins superior rectal vein inferior mesenteric vein
5. Middle rectal veins (unimportant) occasionally exist
LYMPHATIC DRAINAGE OF RECTUM
Follow the upward route of superior rectal
vessels (the inferior mesenteric vessels),
hence important for surgical clearance in
malignancy
If it is blocked, then reverse flow may occur
to the nodes along with middle rectal vessels
or the inguinal region via inferior rectal
vessels
NERVE SUPPLY OF THE LARGE INTESTINE
Sympathetic nerves via splanchnic nerves
surrounding the superior and inferior
mesenteric arteries
Parasympathetic nerves via vagus and pelvic
splanchnic (S2-4) nerves
2. PYHSIOLOGY OF LARGE INTESTINE
Absorption of water is the principal function
of the colon
Out of 1000 ml of ileal contents, 150-250 is
excreted as feces.
Sodium is actively absorbed
Chloride and water are passively absorbed
by the sodium pump
A tiny amount of glucose, fatty acids, amino
acids and vitamins are also absorbed
Dietary fiber is fermented by normal colonic
microflora (anaerobes e.g. bacteroides and
bifidobacteria) producing short chain fatty
acids (SCFAs) e.g. butyrate which provides
fuel for colonic mucosa
Diversion of the fecal stream e.g. loop
ileostomy may cause diversion colitis
COLONIC MOTILITY
It is variable
Fecal residue reaches the caecum 4 hours,
and rectum 24 hours after meals
Some residue may still be passed after 4
days through the rectum
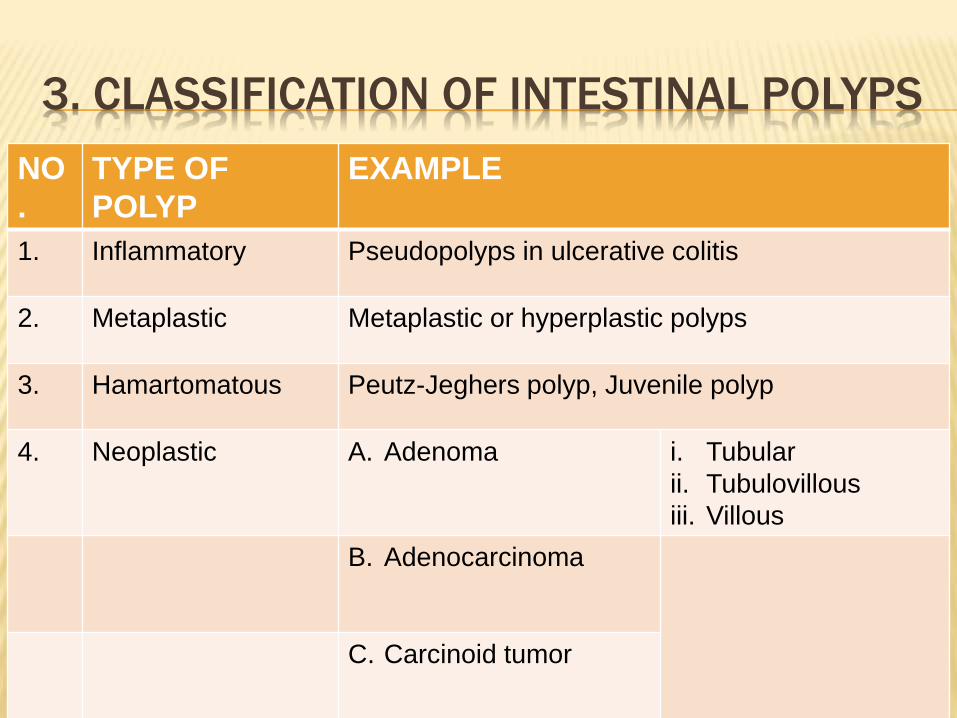
3. CLASSIFICATION OF INTESTINAL POLYPS
NO
.
TYPE OF
POLYP
EXAMPLE
1. Inflammatory Pseudopolyps in ulcerative colitis
2. Metaplastic Metaplastic or hyperplastic polyps
3. Hamartomatous Peutz-Jeghers polyp, Juvenile polyp
4. Neoplastic A. Adenoma i. Tubular
ii. Tubulovillous
iii. Villous
B. Adenocarcinoma
C. Carcinoid tumor
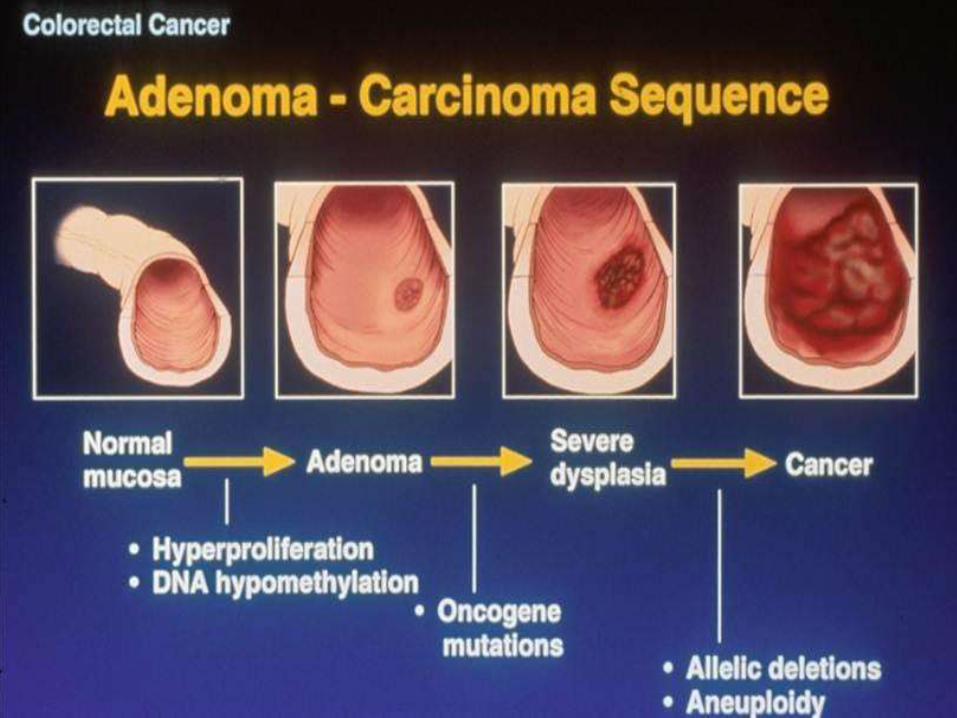
4. ADENOMA-CARCINOMA SEQUENCE
Colorectal cancer arises in a stepwise
progression from adenomas in which
increasing dysplasia in the adenoma is due
to an accumulation of genetic abnormalities.
This is known as adenoma-carcinoma
sequence
5. CLASSIFICATION OF COLORECTAL CANCER
Mostly adenocarcinomas
Rarely, carcinoid tumor, leiomyosarcomas
etc.
Colorectal cancers are staged by:
Duke’s staging
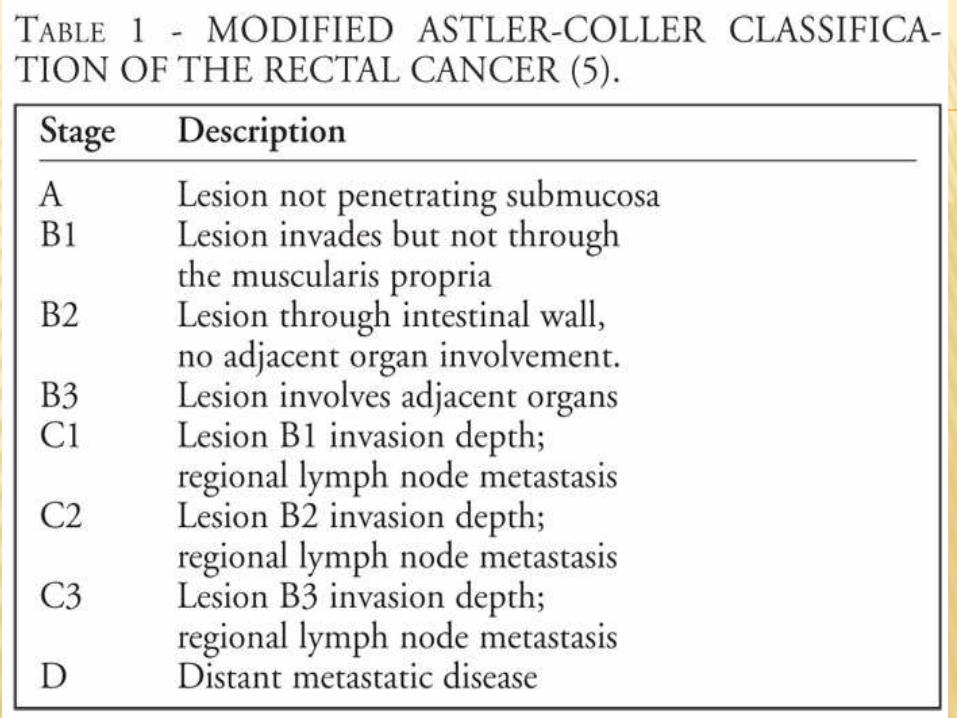
Astler-Coller staging
TNM staging
It is also graded into low (well-differentiated),
average and high (undifferentiated)
histological grades
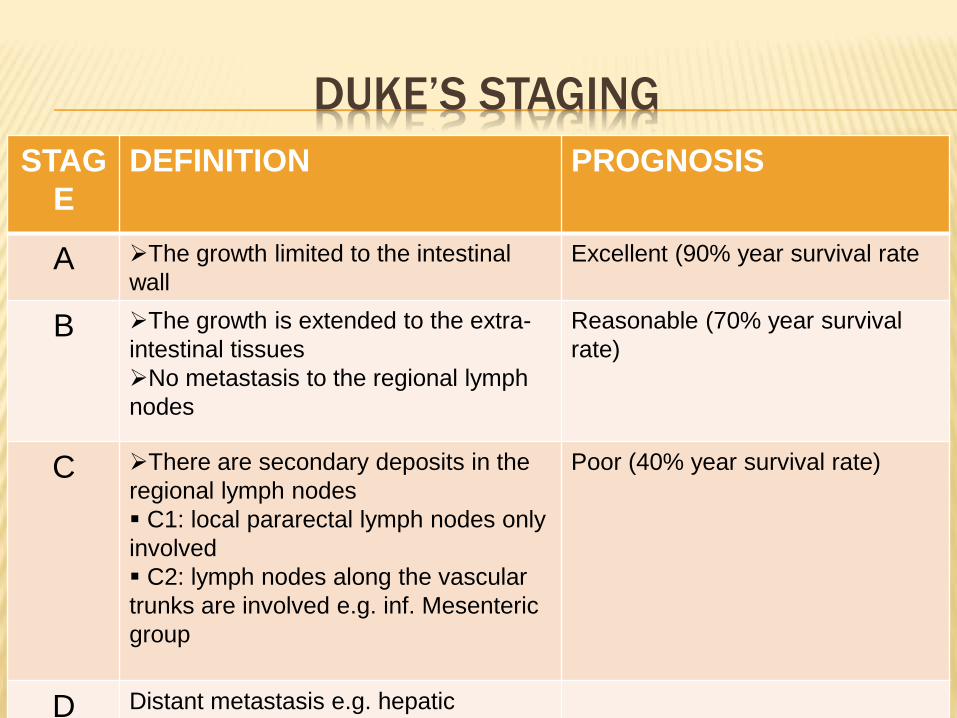
DUKE’S STAGING
STAG
E
DEFINITION PROGNOSIS
A The growth limited to the intestinal
wall
Excellent (90% year survival rate
B The growth is extended to the extra-
intestinal tissues
No metastasis to the regional lymph
nodes
Reasonable (70% year survival
rate)
C There are secondary deposits in the
regional lymph nodes
C1: local pararectal lymph nodes only
involved
C2: lymph nodes along the vascular
trunks are involved e.g. inf. Mesenteric
group
Poor (40% year survival rate)
D Distant metastasis e.g. hepatic
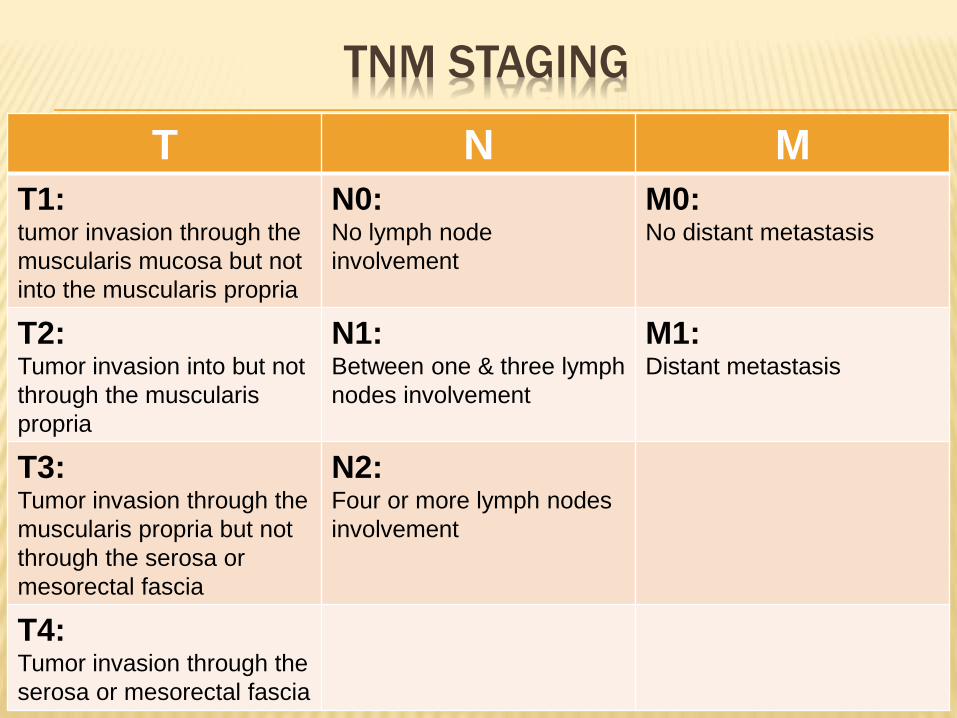
TNM STAGING
T N M
T1: tumor invasion through the
muscularis mucosa but not
into the muscularis propria
N0:No lymph node
involvement
M0:No distant metastasis
T2: Tumor invasion into but not
through the muscularis
propria
N1:Between one & three lymph
nodes involvement
M1:Distant metastasis
T3: Tumor invasion through the
muscularis propria but not
through the serosa or
mesorectal fascia
N2:Four or more lymph nodes
involvement
T4: Tumor invasion through the
serosa or mesorectal fascia
6. SIGNS & SYMPTOMS
Age: usually above 55
bleeding per rectum
Sense of incomplete defecation:
tenesmus, spurious diarrhea, bloody slime
Alteration in bowel habit: early morning
bloody diarrhea
Pain: a late symptom
Weight loss: suggests liver metastasis
7. ETIOLOGY
Adenoma-carcinoma sequence
Mutation of APC gene, K-ras gene, p53 gene
Diet: red meat, animal fat. Fiber is protective
Smoking
Alcohol
Long-standing ulcerative colitis & Crohn’sdisease
After cholecystectomy and ureterosigmoidostomy?
8. PATHOGENESIS
Macroscopically: 4 forms
1. Annular
2. Tubular
3. Ulcerative
4. Cauliflower
Microscopically:
1. Adenocarcinoma commonly
2. Lymphoma, GIST (leiomyosarcoma) rarely
SPREAD OF COLORECTAL CARCINOMA
1. Direct spread: longitudinal, transverse or
radial
2. Lymphatic spread
3. Hematogenous spread: commonly to the
liver, lungs, brian, bone, ovary, kidney are
rare
4. Transcoelomic spread: other structures
within the peritoneum e.g. omentum
9. DIAGNOSIS / INVESTIGATIONS
Screening: testing for fecal occult blood
followed by colonoscopy in 60-69 aged
people. A guaiac-based test is used which
detects the peroxidase like activity of fecal
hematin.
Endoscopy: fiberoptic, flexible
sigmoidoscopy / colonoscopy ± biopsy
Radiology: double-contrast barium enema
may show a filling defect. CT scan of
abdomen / chest
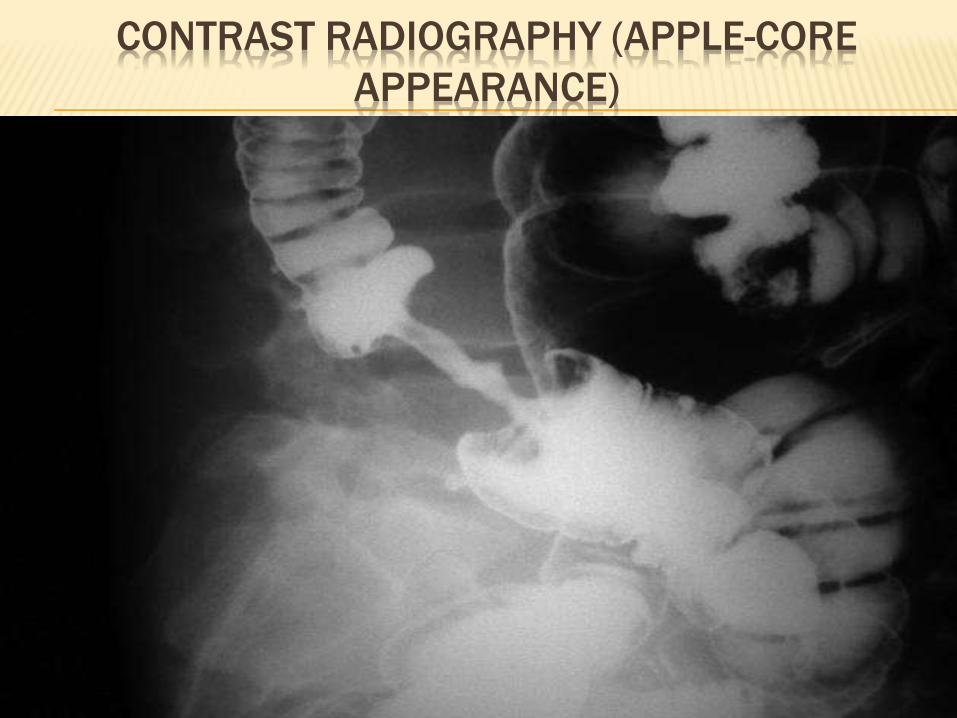
CONTRAST RADIOGRAPHY (APPLE-CORE
APPEARANCE)
10. PREVENTION
Change the dietary habits
Quit smoking and alcohol
Early diagnosis of intestinal polyps
11. MANAGEMENT (SURGERY)
Pre-operative preparation±
Prevention of thromboembolism by anti-
embolic stockings or s/c LMW heparin
Operations for colon:
1. Right hemicolectomy
2. Extended right hemicolectomy
3. Left hemicolectomy
4. Emergency surgery e.g. Hartmann’s
procedure
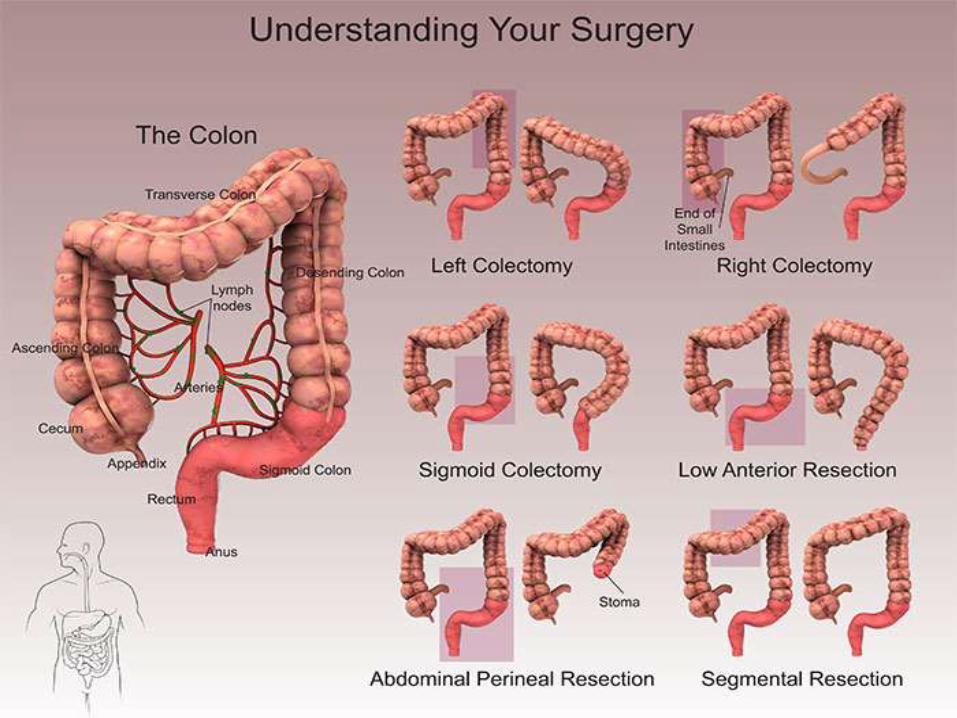
MANAGEMENT (SURGERY)
Operations for rectum:
1. Anterior resection
2. Abdomino-perineal excision of the rectum
3. Endoluminal stenting
4. Palliative colostomy/laser
5. Pelvic exenteration (Brunschwig’s
operation)
6. Liver resection

MANAGEMENT (CHEMOTHERAPY)
May be used combined with radiotherapy to
make the advanced tumor operable
5-FU as adjuvant therapy in node-positive
disease (Duke’s stage C/N1,2). It may be
combined with oxaliplatin
MANAGEMENT (RADIOTHERAPY)
Palliative irradiation for inoperable, painful
tumors
Brachyradiotherapy
12. PROGNOSIS (5-YEAR SURVIVAL RATE)
Overall 5-year survival for colorectal cancer
is 50%
Duke’s stage A: by surgical resection alone,
90%
Tumor spread beyond the bowel wall: 60-
70%
Tumor with lymph node metastasis: 30%
Metastatic disease: 10%
13. FOLLOW-UP
Surveillance colonoscopy
Regular imaging of liver (US, CTS) for
metastasis
Measurement of CEA
14. EPIDEMIOLOGY
In UK, colorectal cancer is second most
cause of cancer death
About 35000 patients are diagnosed with
colorectal cancer every year in UK; 1/3rd of
rectum and 2/3rd of colon
M:F = same
Less frequent in developing countries than in
industrialized countries