coeliac disease: effect of early feeding on the incidence of the disease
TRANSCRIPT
Coeliac disease: effect of early feeding on the
incidence of the disease
Olle Hernella, , Anneli Ivarssona,b, Lars Ake Perssonb
aPediatrics, Department of Clinical Sciences, Umea University, SE-901 85 Umea, SwedenbEpidemiology, Department of Public Health and Clinical Medicine, Umea University, Umea, Sweden
Abstract
Coeliac disease, also called permanent gluten sensitive enteropathy, has recently been recognised
as constituting a widespread health problem. Effective treatment involves the strict exclusion of
wheat, rye, barley and possibly also oats from the diet. Genetic susceptibility and the presence of
gluten in the diet are prerequisites for developing the disease. Sweden has recently experienced an
epidemic of coeliac disease in children below 2 years of age. Previously, considerable changes in
incidence over time have also been reported from England, Scotland and Ireland. Such obvious
changes in incidence over rather short time periods, in genetically stable populations, emphasise the
importance of environmental factors in the aetiology. Thus, most likely, the aetiology of coeliac
disease is multifactorial. However, further conclusive evidence is required to settle if environmental
factors, beyond presence of gluten in the diet, really influence the immunological process resulting in
the coeliac small intestinal lesion, or merely influence the clinical expression of the disease. The
search for contributing exposures has thus far focused on early feeding, suggesting that breast-
feeding duration and the amount of gluten consumed are of importance, and possibly also the age for
introducing gluten into the diet of infants. The pattern of causation may vary over time and between
countries, however, which may obscure the search for risk factors. Nevertheless, a challenging
possibility that needs to be explored is if coeliac disease can be delayed, or possibly even prevented
for an entire life span, by favourable dietary habits. D 2001 Elsevier Science Ireland Ltd. All rights
reserved.
Keywords: Breast-feeding; Children; Coeliac disease; Gluten consumption; Incidence; Infant feeding; Prevention
0378-3782/01/$ – see front matter D 2001 Elsevier Science Ireland Ltd. All rights reserved.
PII: S0378 -3782 (01 )00217 -1
* Corresponding author. Tel.: +46-90-785-21-21; fax: +46-90-12-37-28.
E-mail address: [email protected] (O. Hernell).
www.elsevier.com/locate/earlhumdev
*
Early Human Development 65 Suppl. (2001) S153–S160
1. Introduction
Coeliac disease, also called permanent gluten sensitive enteropathy, has recently been
recognised as constituting a widespread health problem. This is problematic, as in many
countries, gluten-containing cereals, i.e. wheat, rye, barley and possibly also oats, are an
important part of the diet. Further, when the disease is untreated, it is associated with a
number of complications related to malabsorption, e.g. diarrhoea and growth problems in
infancy and depression, osteoporosis and malignancies later in life [1,2]. A wide spectrum
of symptoms contributes to diagnostic difficulties, and in many countries, screening
studies have revealed that the majority of cases, both among children and adults, are
undiagnosed [3–9]. The diagnosis is ascertained by a small intestinal biopsy revealing an
enteropathy that resolves with a gluten-free diet [10]. Thus, an effective treatment is
available.
Coeliac disease is considered an immunological disease possibly of autoimmune type, but
with the antigen, i.e. gluten, identified. Genetic predisposition and the presence of gluten in
the diet are prerequisites for developing the small intestinal coeliac lesion, but the aetiology
is most likely multifactorial and also includes other environmental factors [11–13].
Dietary patterns during infancy have been the focus of research on such environmental
factors, especially breast-feeding duration and intake of gluten-containing cereals with
respect to age at introduction and amounts consumed [14–20]. However, there is thus far
no consensus concerning the role of these factors. Further, there is some question as to
whether oats should really be considered to contain gluten [21].
Symptomatic coeliac disease in childhood has been more common in Sweden than in
any other country [22], and furthermore, the incidence in children below 2 years of age has
varied considerably over time [23–25]. This has provided a unique opportunity to explore
any temporal relationship between changes in early feeding patterns and the changes in
incidence of the disease.
2. The Swedish epidemic of coeliac disease
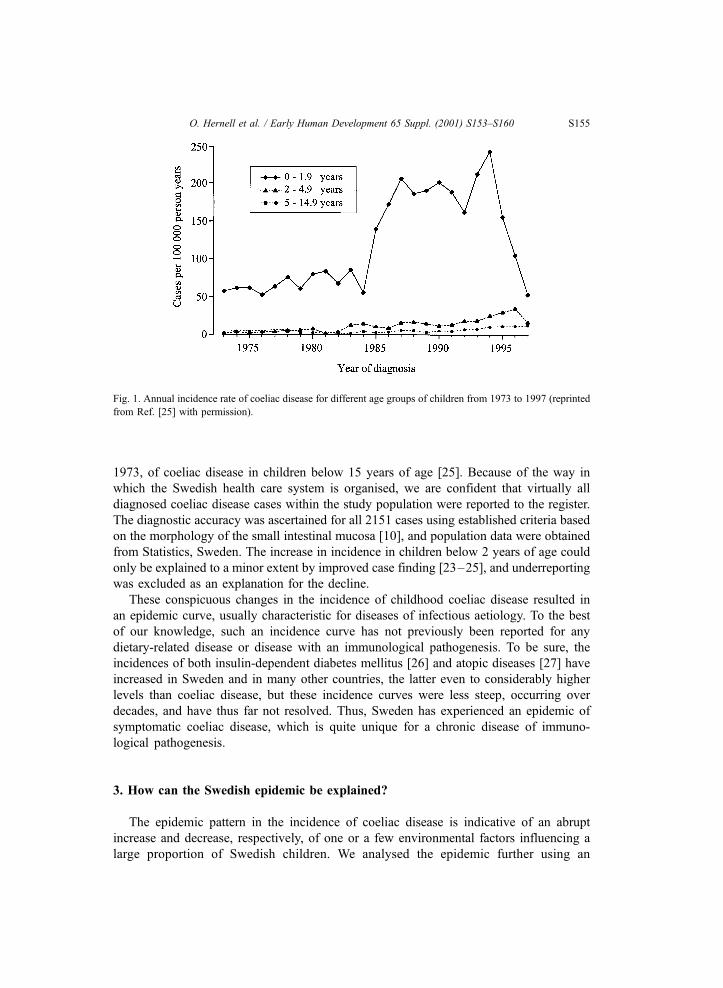
Starting in the mid-1980s, Sweden experienced an epidemic of symptomatic coeliac
disease (Fig. 1) [25]. From 1985 to 1987, the annual incidence rate in children below 2
years of age increased fourfold to 198 cases (95% CI 186–210)/100000 person years,
followed from 1995 and onward by a sharp decline to 51 cases (95% CI 36–70)/100000
person years in 1997, which is back to the level preceding the increase. The birth cohort of
1993 had the highest risk, with a cumulative incidence that by the age of 2 years, had
already reached 4.4 cases (95% CI 3.8–5.0)/1000 births, and by the age of 4 years, had
increased further to 5.0 cases (95% CI 4.4–5.7)/1000 births. In older children, the
incidence remained at a much lower level, albeit with a slow increase with time which
was probably due to improved case finding [25]. Also, in a follow-up continuing until
1998, no compensatory increase among older children has thus far been found (to be
published).
The findings reported above were derived from a population-based prospective
incidence register established in 1991, and from retrospective data collected back to
O. Hernell et al. / Early Human Development 65 Suppl. (2001) S153–S160S154
1973, of coeliac disease in children below 15 years of age [25]. Because of the way in
which the Swedish health care system is organised, we are confident that virtually all
diagnosed coeliac disease cases within the study population were reported to the register.
The diagnostic accuracy was ascertained for all 2151 cases using established criteria based
on the morphology of the small intestinal mucosa [10], and population data were obtained
from Statistics, Sweden. The increase in incidence in children below 2 years of age could
only be explained to a minor extent by improved case finding [23–25], and underreporting
was excluded as an explanation for the decline.
These conspicuous changes in the incidence of childhood coeliac disease resulted in
an epidemic curve, usually characteristic for diseases of infectious aetiology. To the best
of our knowledge, such an incidence curve has not previously been reported for any
dietary-related disease or disease with an immunological pathogenesis. To be sure, the
incidences of both insulin-dependent diabetes mellitus [26] and atopic diseases [27] have
increased in Sweden and in many other countries, the latter even to considerably higher
levels than coeliac disease, but these incidence curves were less steep, occurring over
decades, and have thus far not resolved. Thus, Sweden has experienced an epidemic of
symptomatic coeliac disease, which is quite unique for a chronic disease of immuno-
logical pathogenesis.
3. How can the Swedish epidemic be explained?
The epidemic pattern in the incidence of coeliac disease is indicative of an abrupt
increase and decrease, respectively, of one or a few environmental factors influencing a
large proportion of Swedish children. We analysed the epidemic further using an
Fig. 1. Annual incidence rate of coeliac disease for different age groups of children from 1973 to 1997 (reprinted
from Ref. [25] with permission).
O. Hernell et al. / Early Human Development 65 Suppl. (2001) S153–S160 S155

ecological study design, and explored any temporal relationship between changes in early
feeding patterns and the changes in disease occurrence [25].
National data were collected on the risk factors presently under debate, i.e. breast-
feeding duration and quantity of gluten-containing cereals consumed, and recommenda-
tions on when and how to introduce gluten into the diet of infants were also taken into
account. Changes in consumption of flour via the use of industrially produced follow-on
formulas were used as an estimate of changes in total gluten consumption.
Our results showed rapidly increasing incidence rates between 1985 and 1987 (Fig.
1). The time period of interest with respect to exposure was characterised by: (i) about
half the infants being breast-fed at 6 months of age, (ii) a twofold increase in the average
daily consumption of flour via the use of follow-on formula from 1981 to 1983 with
respect to the total amount of wheat, rye and barley, while the amount of oats decreased,
and (iii) a national recommendation at the end of 1982 to postpone introduction of gluten
from 4 to 6 months of age. The latter was in accordance with European recommenda-
tions [28].
The rapid decline in incidence rates started in 1995, and was still ongoing throughout
1997 (Fig. 1). The period of interest with respect to exposure was characterised by: (i) a
continuous increase from 54% to 76% in the proportion of infants still breast-fed at 6
months of age, (ii) the average daily consumption of flour via the use of follow-on formula
decreasing, starting in 1995, by one third with respect to the total amount of wheat, rye and
barley, while the amount of oats increased, and (iii) a change in the national recommen-
dation in the autumn of 1996 to the introduction of gluten into the diet in smaller amounts
from 4 months of age, preferably while the child is still being breast-fed.
Results based on this ecological approach must of course be interpreted with caution, as
they are not based on exposure data and disease risk on an individual level. The findings
are, however, compatible with the epidemic being a result, at least in part, of a change in
and interplay between amount of gluten given, age at introduction of gluten, and whether
breast-feeding was ongoing or not when gluten was introduced. Other factor(s) may also
have contributed, and the search for these should be intensified.
4. Comparison with England, Scotland and Ireland
Interestingly, a decline in the incidence of symptomatic coeliac disease was observed in
England, Scotland and Ireland in the 1970s, and according to some studies, this was also
preceded by an increase in incidence. In Ireland, the cumulative incidence for the whole
childhood period reached 2.5/1000 births followed by a decline to 0.4/1000 births [29],
and in England [30,31] and Scotland [11], the highest level reported was about 1/1000
births. Changes in infant feeding practices, in Britain promoted by a new recommendation
[32], were discussed as the likely explanation for the decline in incidence [11,29–31]. This
recommendation advocated breast-feeding for a minimum of 2 weeks, but preferably for
4–6 months, use of adapted infant formulas, avoidance of solids or adding cereals to the
milk in bottle feed before the age of 4 months. It is noteworthy that comparable changes in
infant feeding practices were also adopted in Sweden at this time, without any change in
incidence [33,34].
O. Hernell et al. / Early Human Development 65 Suppl. (2001) S153–S160S156

Hence, when the Swedish epidemic started in the mid-1980s, feeding practices in
agreement with the above-cited recommendation were well established; about half of the
infants were breast-fed for 6 months or longer, only adapted infant formulas were used,
and it was rare to introduce solids before 4 months of age. What differed, however, was the
Swedish custom of using gluten-containing follow-on formula, and this is still the case,
although since the early 1980s, the recommended age for introduction has been 6 months.
The incidence reached higher levels in Sweden, and the changes were more abrupt
compared to those in England, Scotland and Ireland. In both settings, changes in early
feeding patterns most likely explain, or at least contributed to the changes in incidence, but
beyond this, the similarities are not easily identified. What is most important, however, is
that such obvious changes in incidence over a rather short time period, and in populations
that are genetically stable, emphasise the significance of environmental factors in the
aetiology. However, the pattern of causation may vary over time and between countries,
which may obscure the search for risk factors.
5. Comparison with Finland
In the 1970s, Finland experienced a decreased incidence of coeliac disease in children
below 2 years of age, but this was counteracted by an increased incidence among school
children, with more vague symptoms [35]. Thus far, there are no indications that this is
happening in Sweden [25], but a longer follow-up will be needed before definite
conclusions can be made.
It is noteworthy, however, that the peak of the Swedish epidemic was reached by a birth
cohort that at 4 years of age already had a cumulative incidence of 5.0/1000 births (95% CI
4.4–5.7) [25], while in Finland, the highest level reported up to 16 years of age was 1.0/
1000 births (95% CI 0.64–1.4) [35]. This indicates that the proportion of children with
possibly preventable coeliac disease may be larger in Sweden than in Finland, provided
that genetic differences are not the explanation.
With the use of an augmented diagnostic approach among Finnish adults, a prevalence
of 2.7/1000 inhabitants (95% CI 2.4–3.0) was demonstrated [36]. It is unclear what
proportion of these individuals developed the coeliac small intestinal lesion already in
childhood but with delayed diagnosis, and what proportion developed the lesion as adults.
In both children and adults eating a normal gluten-containing diet, it has, however, been
demonstrated that a first small intestinal biopsy may show a normal mucosal villous
architecture, and later in life, a second biopsy may reveal mucosal findings compatible
with coeliac disease [37]. Thus, the coeliac small intestinal lesion does not necessarily
develop shortly after gluten-containing foods have been introduced into the diet of a
genetically susceptible individual. Hence, very likely, the prevalence of 2.7/1000 was the
result, at least in part, of individuals that developed the disease as adults. Even if this is
not the case, also when taking the confidence limits into account, this prevalence is still
below that for Swedish pre-school children during the peak of the epidemic. This
indicates a difference in exposure to environmental factor(s) of importance in the
aetiology, as it has not been possible to demonstrate a genetic difference as the likely
explanation [38].
O. Hernell et al. / Early Human Development 65 Suppl. (2001) S153–S160 S157

6. Conclusions
Coeliac disease has emerged as a public health problem. Genetic susceptibility and
presence of gluten in the diet are prerequisites for developing the disease. However,
obvious changes in incidence over rather short time periods, in genetically stable
populations, emphasise the importance of environmental factors in the aetiology. Thus,
most likely, the aetiology of coeliac disease is multifactorial. However, further conclusive
evidence is required to settle if environmental factors, beyond presence of gluten in the
diet, really influence the immunological process resulting in the coeliac small intestinal
lesion, or merely influence the clinical expression of the disease. The search for such
factors has thus far focused on early feeding, suggesting that breast-feeding duration and
the amount of gluten consumed are of importance, and possibly also the age for
introducing gluten into the diet of infants. The pattern of causation may vary over time
and between countries, however, which may obscure the search for risk factors. Never-
theless, a challenging possibility, that need to be explored, is if coeliac disease can be
delayed, or possibly even prevented for an entire life span, by favourable dietary habits.
Acknowledgements
We thank Susanne Walther, administrative assistant, Epidemiology, Department of
Public Health and Clinical Medicine, Umea University. Financial support from the
Swedish Council for Forestry and Agricultural Research, the Swedish Foundation for
Health Care Sciences and Allergy Research, the Swedish Foundation for Research on
Asthma and Allergy, and the Vasterbotten County Council, is gratefully acknowledged.
References
[1] Maki M, Collin P. Coeliac disease. Lancet 1997;349:1755–9.
[2] Murray JA. The widening spectrum of celiac disease. Am J Clin Nutr 1999;69:354–65.
[3] Grodzinsky E, Franzen L, Hed J, Strom M. High prevalence of celiac disease in healthy adults revealed by
antigliadin antibodies. Ann Allergy 1992;69:66–70.
[4] Catassi C, Fabiani E, Ratsch IM, Coppa GV, Giorgi PL, Pierdomenico R, et al. The coeliac iceberg in Italy: a
multicentre antigliadin antibodies screening for coeliac disease in school-age subjects. Acta Paediatr
1996;412:29–35 (Suppl).
[5] Johnston SD, Watson RGP, McMillan SA, Sloan J, Love AHG. Coeliac disease detected by screening is not
silent—simply unrecognized. QJM 1998;91:853–60.
[6] Not T, Horvath K, Hill ID, Partanen J, Hammed A, Magazzu G, et al. Celiac disease risk in the USA:
high prevalence of antiendomysium antibodies in healthy blood donors. Scand J Gastroenterol 1998;33:
494–8.
[7] Ivarsson A, Persson LA, Juto P, Peltonen M, Suhr O, Hernell O. High prevalence of undiagnosed coeliac
disease in adults: a Swedish population-based study. J Intern Med 1999;245:63–8.
[8] Meloni G, Dore A, Fanciulli G, Tanda F, Bottazzo GF. Subclinical coeliac disease in schoolchildren from
northern Sardinia [letter]. Lancet 1999;353:37.
[9] Csizmadia CGDS, Mearin ML, von Blomberg BME, Brand R, Verloove-Vanhorick SP. An iceberg of
childhood coeliac disease in the Netherlands [letter]. Lancet 1999;353:813–4.
O. Hernell et al. / Early Human Development 65 Suppl. (2001) S153–S160S158

[10] Walker-Smith JA, Guandalini S, Schmitz J, Shmerling DH, Visakorpi JK. Revised criteria for diagnosis of
coeliac disease. Report of working group of European society of paediatric gastroenterology and nutrition.
Arch Dis Child 1990;65:909–11.
[11] Logan RFA, Rifkind EA, Busuttil A, Gilmour HM, Ferguson A. Prevalence and ‘‘incidence’’ of celiac
disease in Edinburgh and the Lothian region of Scotland. Gastroenterology 1986;90:334–42.
[12] Ferguson A. New perspectives of the pathogenesis of coeliac disease: evolution of a working clinical
definition [editorial]. J Intern Med 1996;240:315–8.
[13] Sollid LM. Molecular basis of celiac disease. Annu Rev Immunol 2000;18:53–81.
[14] Auricchio S, Follo D, De Ritis G, Giunta A, Marzorati D, Prampolini L, et al. Does breast feeding protect
against the development of clinical symptoms of celiac disease in children? J Pediatr Gastroenterol Nutr
1983;2:428–33.
[15] Greco L, Auricchio S, Mayer M, Grimaldi M. Case control study on nutritional risk factors in celiac disease.
J Pediatr Gastroenterol Nutr 1988;7:395–9.
[16] Logan RFA. Epidemiology of coeliac disease. In: Marsh MN, editor. Coeliac disease. Oxford: Blackwell;
1992. p. 192–214.
[17] Maki M, Holm K, Ascher H, Greco L. Factors affecting clinical presentation of coeliac disease. Role of type
and amount of gluten-containing cereals in the diet. In: Auricchio S, Visakorpi JK, editors. Common food
intolerances: 1. Epidemiology of coeliac disease, vol. 2. Basel: Karger; 1992. p. 76–82.
[18] Ivarsson A, Hernell O, Stenlund H, Persson LA. Breast-feeding protects against celiac disease. Am J Clin
Nutr 2001; in press.
[19] Falth-Magnusson K, Franzen L, Jansson G, Laurin P, Stenhammar L. Infant feeding history shows distinct
differences between Swedish celiac and reference children. Pediatr Allergy Immunol 1996;7:1–5.
[20] Ascher H. The role of quantity and quality of gluten-containing cereals in the epidemiology of coeliac disease.
In: Maki M, Collin P, Visakorpi JK, editors. Coeliac disease: Proceedings of the seventh international sympo-
sium on coeliac disease, 1996, Tampere, Finland. Tampere: Coeliac Disease Study Group; 1997. p. 15–22.
[21] Schmitz J. Lack of oats toxicity in coeliac disease [editorial]. BMJ 1997;314:159–60.
[22] Greco L, Maki M, Di Donato F, Visakorpi JK. Epidemiology of coeliac disease in Europe and the Medi-
terranean area: a summary report on the multicentre study by the European society of paediatric gastro-
enterology and nutrition. In: Auricchio S, Visakorpi JK, editors. Common food intolerances: 1. Epidemiology
of coeliac disease, vol. 2. Basel: Karger; 1992. p. 25–44.
[23] Ascher H, Krantz I, Kristiansson B. Increasing incidence of coeliac disease in Sweden. Arch Dis Child
1991;66:608–11.
[24] Cavell B, Stenhammar L, Ascher H, Danielsson L, Dannaeus A, Lindberg T, et al. Increasing incidence of
childhood coeliac disease in Sweden. Results of a national study. Acta Paediatr 1992;81:589–92.
[25] Ivarsson A, Persson LA, Nystrom L, Ascher H, Cavell B, Danielsson L, et al. Epidemic of coeliac disease in
Swedish children. Acta Paediatr 2000;89:165–71.
[26] Diabetes Epidemiology Research International Group. Secular trends in incidence of childhood IDDM in 10
countries. Diabetes 1990;39:858–64.
[27] Bousquet J, Burney P. Evidence for an increase in atopic disease and possible causes. Clin Exp Allergy
1993;23:484–92.
[28] ESPGAN committee on nutrition. Guidelines on infant nutrition III. Recommendations for infant feeding.
Acta Paediatr Scand 1982;302:16–20 (Suppl).
[29] Gumaa SN, McNicholl B, Egan-Mitchell B, Connolly K, Loftus BG. Coeliac disease in Galway, Ireland
1971–1990. Ir Med J 1997;90:60–1.
[30] Dossetor JFB, Gibson AAM, McNeish AS. Childhood coeliac disease is disappearing [letter]. Lancet
1981;i:322–3.
[31] Challacombe DN, Mecrow IK, Elliott K, Clarke FJ, Wheeler EE. Changing infant feeding practices and
declining incidence of coeliac disease in West Somerset. Arch Dis Child 1997;77:206–9.
[32] Present-day practice in infant feeding. Report of a working party of the panel on child nutrition, Committee
on Medical Aspects of Food Policy, vol. 9. London: Her Majesty’s Stationery Office; 1974. p. 24–6.
[33] Lindberg T. Coeliac disease and infant feeding practices [letter]. Lancet 1981;i:449.
[34] Stenhammar L, Ansved P, Jansson G, Jansson U. The incidence of childhood celiac disease in Sweden. J
Pediatr Gastroenterol Nutr 1987;6:707–9.
O. Hernell et al. / Early Human Development 65 Suppl. (2001) S153–S160 S159

[35] Maki M, Holm K. Incidence and prevalence of coeliac disease in Tampere: coeliac disease is not disappear-
ing. Acta Paediatr Scand 1990;79:980–2.
[36] Collin P, Reunala T, Rasmussen M, Kyronpalo S, Pehkonen E, Laippala P, et al. High incidence and
prevalence of adult coeliac disease. Augmented diagnostic approach. Scand J Gastroenterol 1997;32:
1129–33.
[37] Maki M, Holm K, Koskimies S, Hallstrom O, Visakorpi JK. Normal small bowel biopsy followed by coeliac
disease. Arch Dis Child 1990;65:1137–41.
[38] Ascher H, Holm K, Kristiansson B, Maki M. Different features of coeliac disease in two neighbouring
countries. Arch Dis Child 1993;69:375–80.
O. Hernell et al. / Early Human Development 65 Suppl. (2001) S153–S160S160