cochrane database of systematic reviews (reviews) || antihypertensive agents for preventing diabetic...
TRANSCRIPT
Antihypertensive agents for preventing diabetic kidney
disease (Review)
Lv J, Perkovic V, Foote CV, Craig ME, Craig JC, Strippoli GFM
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2012, Issue 12
http://www.thecochranelibrary.com
Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Figure 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
11DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
21CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
55DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 ACEi versus placebo/no treatment, Outcome 1 Normo- to micro- or macroalbuminuria. 57
Analysis 1.2. Comparison 1 ACEi versus placebo/no treatment, Outcome 2 All-cause mortality. . . . . . . . . 58
Analysis 1.3. Comparison 1 ACEi versus placebo/no treatment, Outcome 3 Doubling of SCr. . . . . . . . . 59
Analysis 1.4. Comparison 1 ACEi versus placebo/no treatment, Outcome 4 ESKD. . . . . . . . . . . . . 60
Analysis 1.5. Comparison 1 ACEi versus placebo/no treatment, Outcome 5 Adverse events. . . . . . . . . . 61
Analysis 1.6. Comparison 1 ACEi versus placebo/no treatment, Outcome 6 Blood pressure. . . . . . . . . . 62
Analysis 2.1. Comparison 2 ARB versus placebo/no treatment, Outcome 1 Normo- to micro- or macroalbuminuria. 63
Analysis 2.2. Comparison 2 ARB versus placebo/no treatment, Outcome 2 All-cause mortality. . . . . . . . . 64
Analysis 2.3. Comparison 2 ARB versus placebo/no treatment, Outcome 3 Doubling of SCr. . . . . . . . . 65
Analysis 2.4. Comparison 2 ARB versus placebo/no treatment, Outcome 4 ESKD. . . . . . . . . . . . . 66
Analysis 2.5. Comparison 2 ARB versus placebo/no treatment, Outcome 5 Adverse events. . . . . . . . . . 67
Analysis 2.6. Comparison 2 ARB versus placebo/no treatment, Outcome 6 Blood pressure. . . . . . . . . . 68
Analysis 3.1. Comparison 3 ACEi versus ARB, Outcome 1 Normo- to micro- or macroalbuminuria. . . . . . . 69
Analysis 3.2. Comparison 3 ACEi versus ARB, Outcome 2 All-cause mortality. . . . . . . . . . . . . . 69
Analysis 4.1. Comparison 4 ACEi versus CCB, Outcome 1 Normo to micro or macroalbuminuria. . . . . . . 70
Analysis 4.2. Comparison 4 ACEi versus CCB, Outcome 2 All-cause mortality. . . . . . . . . . . . . . 71
Analysis 4.3. Comparison 4 ACEi versus CCB, Outcome 3 Doubling of SCr. . . . . . . . . . . . . . . 72
Analysis 4.4. Comparison 4 ACEi versus CCB, Outcome 4 ESKD. . . . . . . . . . . . . . . . . . 73
Analysis 4.5. Comparison 4 ACEi versus CCB, Outcome 5 Blood pressure. . . . . . . . . . . . . . . . 74
Analysis 5.1. Comparison 5 Prevention of kidney disease: other agents, Outcome 1 ACEi + ARB versus ACEi. . . . 75
Analysis 5.2. Comparison 5 Prevention of kidney disease: other agents, Outcome 2 ACEi versus BB. . . . . . . 75
Analysis 5.3. Comparison 5 Prevention of kidney disease: other agents, Outcome 3 ACEi + CCB versus ACEi. . . 76
Analysis 5.4. Comparison 5 Prevention of kidney disease: other agents, Outcome 4 CCB versus placebo. . . . . . 76
76ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
80APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
88FEEDBACK . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
89WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
89HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
89CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
89DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
90INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iAntihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
[Intervention Review]
Antihypertensive agents for preventing diabetic kidney disease
Jicheng Lv1, Vlado Perkovic1, Celine V Foote1, Maria E Craig2, Jonathan C Craig3, Giovanni FM Strippoli3,4,5,6,7
1Renal and Metabolic Division, The George Institute for Global Health, Camperdown, Australia. 2Divison of Women’s and Children’s
Health, University of New South Wales, Kogarah, Australia. 3Cochrane Renal Group, Centre for Kidney Research, The Children’s
Hospital at Westmead, Westmead, Australia. 4Department of Emergency and Organ Transplantation, University of Bari, Bari, Italy.5Department of Clinical Pharmacology and Epidemiology, Mario Negri Sud Consortium, Santa Maria Imbaro, Italy. 6Sydney School
of Public Health, The University of Sydney, Sydney, Australia. 7Medical-Scientific Office, Diaverum, Lund, Sweden
Contact address: Giovanni FM Strippoli, [email protected].
Editorial group: Cochrane Renal Group.
Publication status and date: New search for studies and content updated (conclusions changed), published in Issue 12, 2012.
Review content assessed as up-to-date: 24 January 2011.
Citation: Lv J, Perkovic V, Foote CV, Craig ME, Craig JC, Strippoli GFM. Antihypertensive agents for preventing diabetic kidney
disease. Cochrane Database of Systematic Reviews 2012, Issue 12. Art. No.: CD004136. DOI: 10.1002/14651858.CD004136.pub3.
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Various blood pressure-lowering agents, and particularly inhibitors of the renin-angiotensin system (RAS), are widely used for people
with diabetes to prevent the onset of diabetic kidney disease (DKD) and adverse cardiovascular outcomes. This is an update of a
Cochrane review first published in 2003 and updated in 2005.
Objectives
This systematic review aimed to assess the benefits and harms of blood pressure lowering agents in people with diabetes mellitus and a
normal amount of albumin in the urine (normoalbuminuria).
Search methods
In January 2011 we searched the Cochrane Renal Group’s Specialised Register through contact with the Trials Search Co-ordinator.
Selection criteria
Randomised controlled trials (RCTs) comparing any antihypertensive agent with placebo or another agent in hypertensive or nor-
motensive patients with diabetes and no kidney disease (albumin excretion rate < 30 mg/d) were included.
Data collection and analysis
Two investigators independently extracted data on kidney and other patient-relevant outcomes (all-cause mortality and serious cardio-
vascular events), and assessed study quality. Analysis was by a random effects model was applied to analyse results which were expressed
as risk ratio (RR) and 95% confidence intervals (CI).
Main results
We identified 26 studies that enrolling 61,264 participants. Angiotensin-converting enzyme inhibitors (ACEi) reduced the risk of new
onset of microalbuminuria, macroalbuminuria or both when compared to placebo (8 studies, 11,906 patients: RR 0.71, 95% CI 0.56
to 0.89), with similar benefits in people with and without hypertension (P = 0.74), and when compared to calcium channel blockers
(5 studies, 1253 participants: RR 0.60, 95% CI 0.42 to 0.85). ACEi reduced the risk of death when compared to placebo (6 studies,
11,350 participants: RR 0.84, 95% CI 0.73 to 0.97). No effect was observed for angiotensin receptor blockers (ARB) when compared
1Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

to placebo for new microalbuminuria, macroalbuminuria or both (5 studies, 7653 participants: RR 0.90, 95% CI 0.68 to 1.19) or
death (5 studies, 7653 participants: RR 1.12, 95% CI 0.88 to 1.41); however, meta-regression suggested possible benefits from ARB for
preventing kidney disease in high risk patients. There was a trend towards benefit from use of combined ACEi and ARB for prevention
of DKD compared with ACEi alone (2 studies, 4171 participants: RR 0.88, 95% CI 0.78 to 1.00).The risk of cough was significantly
increased with ACEi when compared to placebo (6 studies, 11,791 patients: RR 1.84, 95% CI 1.24 to 2.72), however there was no
significant difference in the risk of headache or hyperkalaemia. There was no significant difference in the risk of cough, headache
or hyperkalaemia when ARB was to placebo. On average risk of bias was judged to be either low (27% to 69%) or unclear (i.e. no
information available) (8% to 73%). Blinding of participants, incomplete outcome data and selective reporting were judged to be high
in 23%, 31% and 31% of studies, respectively.
Authors’ conclusions
ACEi were found to prevent new onset DKD and death in normoalbuminuric people with diabetes, and could therefore be used in
this population. More data are needed to clarify the role of ARB and other drug classes in preventing DKD.
P L A I N L A N G U A G E S U M M A R Y
Drugs for preventing kidney disease in people with diabetes
Many people with diabetes (around 20% to 60%) are are affected by high blood pressure (hypertension) and need drugs (antihypertensive
agents) to treat this condition. These drugs also help to prevent development of kidney disease both in people with diabetes who have
normal blood pressure and those whose blood pressure is high. Many people with diabetic kidney disease (DKD) (20% to 40%) go
on to develop end-stage kidney disease (ESKD), and many others die from heart disease or other circulatory problems before ESKD
develops.
We reviewed the literature to determine the benefits and harms of antihypertensive treatment in people with diabetes who did not have
signs of kidney disease. We found 26 studies involving 61,264 participants that compared antihypertensive drugs with placebo (an
neutral agent with no therapeutic benefits or harms), no treatment, and other antihypertensive drugs. A family of drugs called ACEi
(angiotensin-converting enzyme inhibitors) has been shown to prevent new onset of kidney disease and reduce the numbers of deaths
in people with diabetes who have normal levels of albumin in their urine compared with placebo or calcium channel blocking drugs.
We found no significant effect from angiotensin receptor blocker (ARB) drugs on either development of ESKD or death.
Subgroup analyses that suggested similar benefits from ARB for people with type 2 diabetes who were at high risk of heart disease or
should be interpreted cautiously. Direct comparison of ACEi and ARB in this population showed no difference in preventing DKD.
The benefits of ACEi are consistent, and ACEi could be the first choice intervention for primary prevention of DKD.
B A C K G R O U N D
Description of the condition
Diabetes is a major global epidemic and responsible for most diag-
noses of end-stage kidney disease (ESKD). Diabetes is also a ma-
jor cause of death in many countries (IDF 2009; USRDS 2009).
Diabetic kidney disease (DKD) (also called diabetic nephropathy)
develops slowly, and the first clinically-evident feature of kidney
involvement is often development of microalbuminuria (urinary
albumin excretion > 30 mg/d). DKD occurs in 20% to 40% of
patients within 10 to 15 years of diabetes onset and typically pro-
gresses to macroalbuminuria before kidney function starts to de-
cline. Micro- and macroalbuminuria are both risk factors for kid-
ney failure, cardiovascular disease and death (Ninomiya 2009; Ritz
1999; Ruggenenti 1997).
Description of the intervention
Hypertension and proteinuria contribute to a progressive dete-
rioration of kidney function in patients with DKD (Hasslacher
1985; Mogensen 1976) and most antihypertensive agents are used
both for the treatment of hypertension and in an effort to slow
2Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

the progression of kidney damage in patients with DKD. Antihy-
pertensive agents used in this scenario include angiotensin-con-
verting enzyme inhibitors (ACEi), angiotensin receptor blockers
(ARB), calcium channel blockers (CCBs), beta-blockers and di-
uretics. These have been used both alone or in combination.
How the intervention might work
For patients with established DKD, inhibitors of the renin-an-
giotensin system (RAS) have been shown to retard progressive
kidney impairment and prevent ESKD onset (Strippoli 2004).
Based on data from completed studies, most guideline groups have
recommended the use of ACEi or angiotensin receptor block-
ers (ARB) equally in patients who have diabetes with micro- or
macroalbuminuria, interchangeably (Table 1).
Why it is important to do this review
Our original review suggested that ACEi may reduce the risk of
nephropathy developing in normoalbuminuric patients with dia-
betes (Strippoli 2005). However, relatively few data were available
about the effects of other classes of antihypertensives at that time,
which contributed to some persisting uncertainty. A number of
new studies have examined the efficacy of blood pressure lowering
for the primary prevention of DKD, albeit with conflicting results
(ADVANCE Study 2009; DIRECT Studies 2009; RASS Study
2002; TRANSCEND Study 2009). This updated systematic re-
view was therefore undertaken to evaluate the relative effects of
blood pressure lowering agents on the primary prevention of new-
onset kidney disease in patients who have diabetes.
O B J E C T I V E S
The objectives of this review were to assess the effects of antihy-
pertensive agents for prevention of diabetes in people with kidney
disease who were normoalbuminuric. We aimed to evaluate:
1. the benefits and harms of different antihypertensive agents
such as ACEi, ARB, calcium channel blockers (CCB), beta-
blockers (BB), and diuretics in preventing DKD in diabetic
patients without kidney disease (defined as an albumin excretion
rate < 30 mg/d, that is, no microalbuminuria);
2. if combination therapy with different antihypertensive
agents was better than monotherapy with a single agent if study
data were available; and
3. the variation of effects of interventions according to:
◦ diabetes type 1 or type 2
◦ duration of diabetes at initiation of antihypertensive
treatment (time of study entry)
◦ presence or absence of hypertension.
M E T H O D S
Criteria for considering studies for this review
Types of studies
Any randomised controlled trials (RCTs) and quasi-RCTs (RCTs
in which allocation to treatment was obtained by alternation, use of
alternate medical records, date of birth or other predictable meth-
ods) that evaluated the effect of any antihypertensive agent admin-
istered to diabetic patients who did not have kidney disease (de-
fined as an albumin excretion rate < 30 mg/d on a timed specimen
confirmed with three serial measurements) were included. Studies
in non-diabetic patients were excluded. Studies that were under-
taken in populations with mixed-causation hypertension and in-
cluded a proportion of diabetic patients were included if the raw
data relating to diabetic patients could be obtained from the study
investigators.
Types of participants
Adults aged 18 years and over with type 1 or type 2 diabetes, with-
out diagnoses of kidney disease, and who were normoalbumin-
uria, and irrespective of blood pressure status. Normoalbuminuria
was defined as an albumin excretion rate < 30 mg/d on a timed
specimen confirmed with three serial measurements.
Types of interventions
Antihypertensive agents compared with placebo, no treatment or
another antihypertensive agent for prevention of DKD, irrespec-
tive of class, administered at any dose and for a duration of at least
six months.
Types of outcome measures
• Number of patients who develop microalbuminuria/
macroalbuminuria
◦ progression from normo- to micro or
macroalbuminuria
◦ Albuminuria (mg/24 h or µg/min), macroalbuminuria
(mg/24 h or µg/min) or proteinuria (mg/24 h) at end of
treatment or change between beginning and end of treatment
• Death
◦ all-cause mortality
3Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

◦ cardiovascular
• Doubling of serum creatinine
• ESKD
• Blood pressure (mm Hg) (systolic, diastolic, mean arterial
pressure (MAP)) at end of treatment or change between the
beginning and end of treatment
• Adverse events (as reported by the studies)
• Lipid profile
• Glycaemic control (HbA1c%)
• Urinary albumin/creatinine ratio (mg albumin/mmol
creatinine)
Search methods for identification of studies
For this review update we searched the Cochrane Renal Group’s
Specialised Register (24 January 2011) through contact with the
Trials’ Search Co-ordinator using search terms relevant to this
review.
The Cochrane Renal Group’s Specialised Register contains studies
identified from:
1. Quarterly searches of the Cochrane Central Register of
Controlled Trials CENTRAL
2. Weekly searches of MEDLINE OVID SP
3. Handsearching of renal-related journals and the
proceedings of major renal conferences
4. Searching of the current year of EMBASE OVID SP
5. Weekly current awareness alerts for selected renal journals
6. Searches of the International Clinical Trials Register
(ICTRP) Search Portal and ClinicalTrials.gov.
Studies contained in the Specialised register are identified through
search strategies for CENTRAL, MEDLINE, and EMBASE based
on the scope of the Cochrane Renal Group. Details of these strate-
gies as well as a list of handsearched journals, conference proceed-
ings and current awareness alerts are available in the specialised
register section of information about the Cochrane Renal Group.
See Appendix 1 for search terms used in strategies for this review.
The original search strategies can be found in Strippoli 2005.
Data collection and analysis
Selection of studies
Two authors (original review GFMS, MC; review update JL, CF)
undertook selection of studies. Authors independently assessed
retrieved abstracts, and wherever necessary the full text of studies,
to determine which satisfied the inclusion criteria. Disagreements
were resolved in all cases by discussion among author teams.
Data extraction and management
Data extraction was carried out by the same authors independently
using standard data extraction forms. It was planned that any stud-
ies reported in non-English language journals would be translated
before assessment. Where more than one report of one study ex-
isted, the reports were grouped together and the report with most
complete data was used in the analyses. Where relevant outcomes
were only published in other reports these data was used.
Assessment of risk of bias in included studies
For this review update the following items were independently
assessed by two authors using the risk of bias assessment tool (
Higgins 2011) (see Appendix 2).
• Was there adequate sequence generation (selection bias)?
• Was allocation adequately concealed (selection bias)?
• Was knowledge of the allocated interventions adequately
prevented during the study (detection bias)?
◦ Participants and personnel
◦ Outcome assessors
• Were incomplete outcome data adequately addressed
(attrition bias)?
• Are reports of the study free of suggestion of selective
outcome reporting (reporting bias)?
• Was the study apparently free of other problems that could
put it at a risk of bias?
Measures of treatment effect
Data entry was carried out by two authors (original review GFMS,
MC; review update: JL, CF). For dichotomous outcomes results
were expressed as risk ratio (RR) with 95% confidence intervals
(CI). Where continuous scales of measurement were used to assess
the effects of treatment (microalbuminuria, blood pressure) the
mean difference (MD) was used.
Dealing with missing data
Any further information required from the original author was
requested by written correspondence (e.g. emailing and/or writing
to corresponding author/s) and any relevant information obtained
in this manner was included and noted in the Characteristics of
included studies table.
Assessment of heterogeneity
Heterogeneity was analysed using a Chi² test on N-1 degrees of
freedom, with an alpha of 0.05 used for statistical significance and
with the I² test (Higgins 2003). I² values of 25%, 50% and 75%
correspond to low, medium and high levels of heterogeneity.
4Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Assessment of reporting biases
It was planned that if sufficient RCTs were identified, an attempt
would be made to examine for publication bias using a funnel plot
(Higgins 2011). It was also planned that when different treatment
options had not been compared directly within available RCTs,
conclusions on relative efficacy would be based on indirect com-
parisons where applicable (Bucher 1997; Song 2000). STATA ver-
sion 10.0 was used to test for interaction.
Data synthesis
Data were pooled using the random-effects model but the fixed-
effect model was also used to investigate robustness of the model
chosen and susceptibility to outliers.
Subgroup analysis and investigation of heterogeneity
Subgroup analyses were used to explore possible sources of hetero-
geneity. Heterogeneity among participants could be related to age,
baseline presence or absence of hypertension, renal pathology and
glycaemic control. Heterogeneity in treatments could be related to
dose and duration of therapies administered to study participants.
These aspects were analysed and tabulated or computed when-
ever applicable. Adverse effects were tabulated and assessed using
descriptive techniques because of differences among the various
agents investigated. Where possible, the risk difference with 95%
CI was calculated for each adverse effect, either compared with no
treatment or another agent.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
Results of the search
The literature search identified 5073 articles, of which 4748
were excluded after title and abstract review (Figure 1). Full-text
assessment of 325 potentially eligible reports identified 26 el-
igible studies (143 publications) enrolling 61,264 patients, in-
cluding 33,735 who were normoalbuminuric at baseline (ABCD
Study 2002; ABCD-2V Study 2004; ADVANCE Study 2009;
Baba 2001; BENEDICT Study 2004; CALM II Study 2005;
Chan 1992; Crepaldi 1995; DIRECT Studies 2009 (DIRECT-
Prevent 1, DIRECT-Protect 1, DIRECT-Protect 2); EUCLID
Study 1997; FACET Study 1998; HOPE Study 2000; Joglekar
1998; Kavgaci 2002; Kvetny 2001; Lin 1995; ONTARGET Study
2008; Perrin 2008; RASS Study 2002; Ravid 1998; ROADMAP
Study 2009; Scognamiglio 1997; TRANSCEND Study 2009;
Tuominen 1998; UKPDS Study 1998; Velussi 1996).
5Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
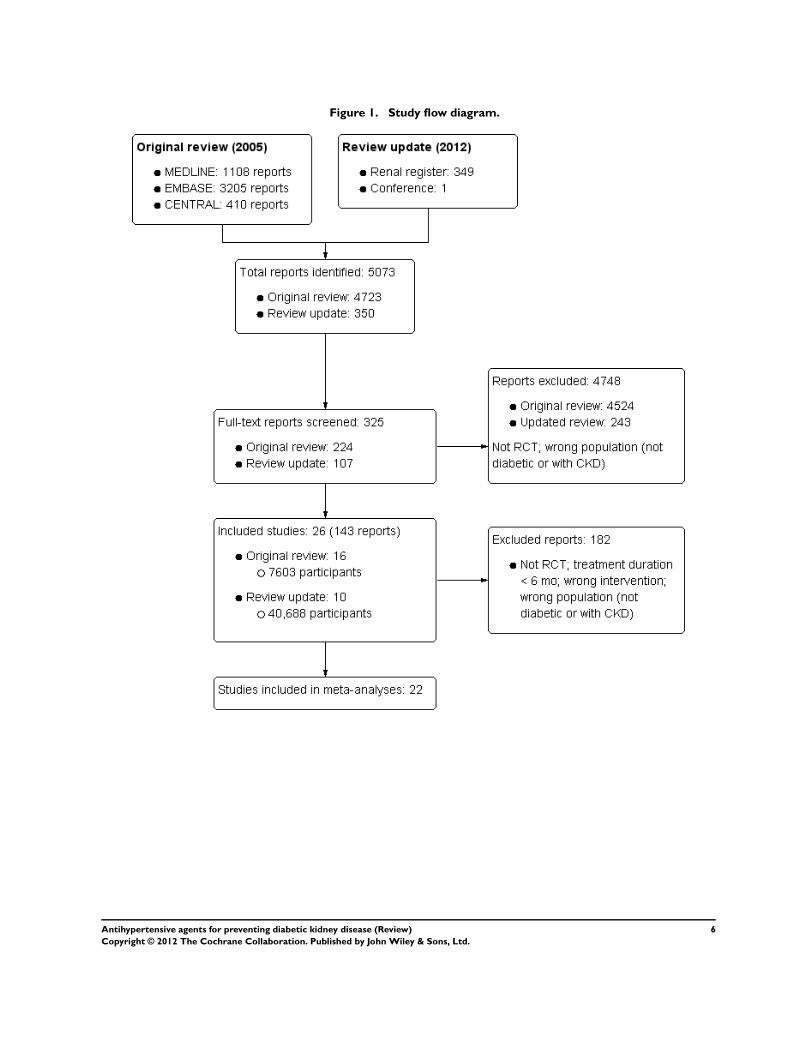
Figure 1. Study flow diagram.
6Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Included studies
Supplemental data on design features and outcomes were asked
of all authors of the studies. Authors of the 16 studies that en-
rolled both patients with and without kidney disease were also
asked for data sets of normoalbuminuric patients only, with 12
replying to our requests (ADVANCE Study 2009; Baba 2001;
CALM II Study 2005; Chan 1992; HOPE Study 2000; Kvetny
2001; ONTARGET Study 2008; RASS Study 2002; Ravid 1998;
TRANSCEND Study 2009; Tuominen 1998; Velussi 1996). Un-
fortunately, several studies did not contain any raw data or data
in an extractable format, only summary statistics and overall esti-
mates of the results. These studies therefore could not contribute
to our analyses, in particular to the meta-analyses.
The characteristics of the populations and interventions of
the studies included in this systematic review are presented in
Characteristics of included studies.
• Nine studies or study arms (16,463 patients) compared
ACEi versus placebo or no treatment
• Seven studies or study arms (1804 patients) compared
ACEi versus CCBs
• Four studies (10,517 patients) compared ARB versus
placebo
• Three studies or study arms (17,436 patients) compared
ACEi versus ARB
• One study compared ACEi with beta-blockers (1148
patients)
• Two studies combined ACEi and ARB and compared to
ACEi or ARB (25,695 patients)
• One study combined ACEi and CCB and compared to
ACEi, CCB or placebo (901 patients)
• One study compared ACEi to alpha-blockers (89 patients)
• Two studies compared CCB with placebo (5831 patients).
Most studies enrolled only type 2 diabetic patients (17 studies;
26,342 patients; DIRECT-Prevent 1); seven studies only enrolled
type 1 diabetic patients (2921 patients; DIRECT-Protect 1 and
DIRECT-Protect 2); one study enrolled both type 1 and type 2
diabetic patients (74 patients) and type of diabetes was unknown
in three studies (16,921 patients). Fifteen studies enrolled mixed
populations of normo- and micro-macroalbuminuric subjects.
Follow-up ranged from six to 72 months.
Cointerventions for blood glucose control were administered in
all but one study but the agents used were often not specified.
In general, tight control of blood glucose was addressed with end
of treatment values of HbA1c reported in 20 studies and ranging
between 5% and 9%.
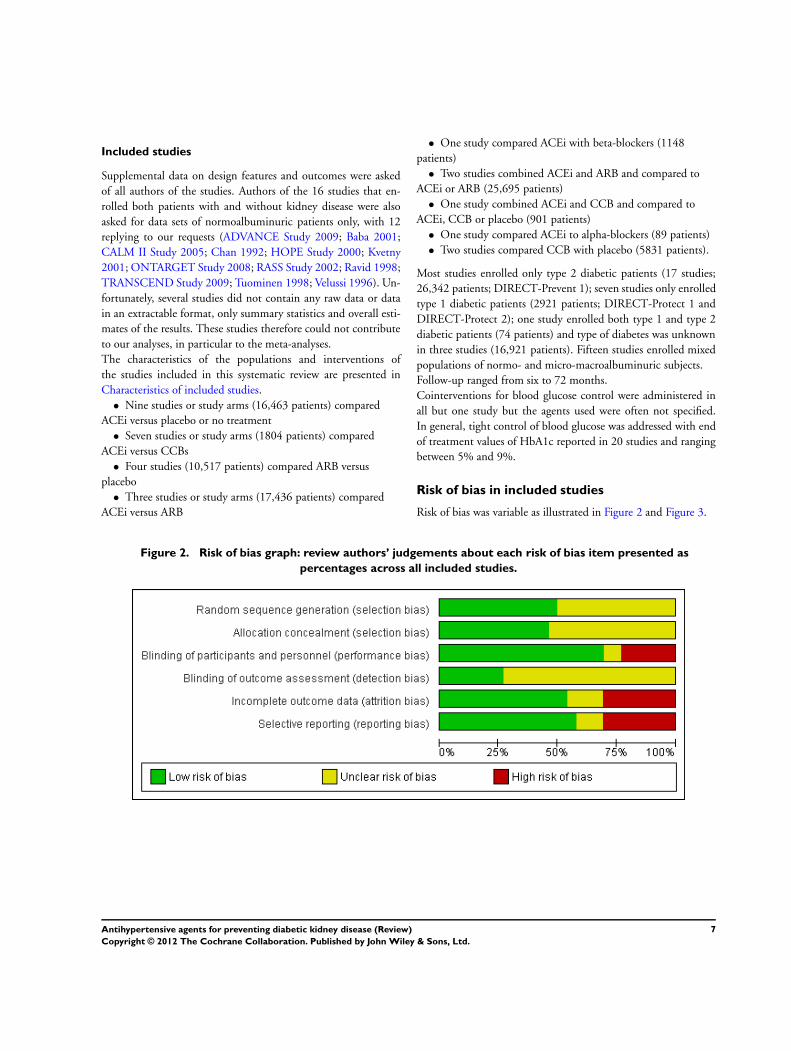
Risk of bias in included studies
Risk of bias was variable as illustrated in Figure 2 and Figure 3.
Figure 2. Risk of bias graph: review authors’ judgements about each risk of bias item presented as
percentages across all included studies.
7Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
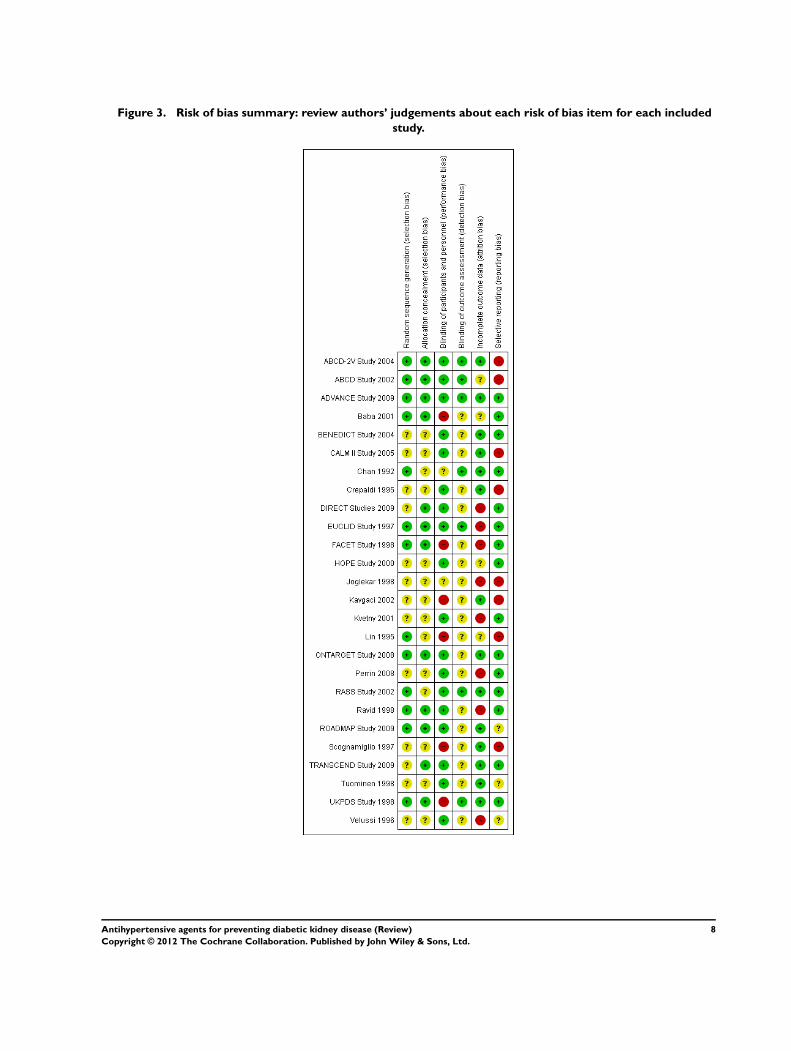
Figure 3. Risk of bias summary: review authors’ judgements about each risk of bias item for each included
study.
8Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Allocation
Random sequence generation
Random sequence generation was judged to be of low risk in 13/
26 (50%) studies (ABCD-2V Study 2004; ABCD Study 2002;
ADVANCE Study 2009; Baba 2001; Chan 1992; EUCLID Study
1997; FACET Study 1998; Lin 1995; ONTARGET Study 2008;
RASS Study 2002; Ravid 1998; ROADMAP Study 2009; UKPDS
Study 1998) and unclear in 13/26 studies (BENEDICT Study
2004; CALM II Study 2005; Crepaldi 1995; DIRECT Studies
2009; HOPE Study 2000; Joglekar 1998; Kavgaci 2002; Kvetny
2001; Perrin 2008; Scognamiglio 1997; TRANSCEND Study
2009; Tuominen 1998; Velussi 1996).
Allocation concealment
Allocation concealment was judged to be of low risk in 12/
26 (46%) studies (ABCD-2V Study 2004; ABCD Study 2002;
ADVANCE Study 2009; Baba 2001; DIRECT Studies 2009;
EUCLID Study 1997; FACET Study 1998; ONTARGET Study
2008; Ravid 1998; ROADMAP Study 2009; TRANSCEND
Study 2009; UKPDS Study 1998) and unclear in 14/26 (54%)
studies (BENEDICT Study 2004; CALM II Study 2005; Chan
1992; Crepaldi 1995; HOPE Study 2000; Joglekar 1998; Kavgaci
2002; Kvetny 2001; Lin 1995; Perrin 2008; RASS Study 2002;
Scognamiglio 1997; Tuominen 1998; Velussi 1996).
Blinding
Blinding of participants and personnel (performance bias) was
judged to be of low risk in 18/26 (69%) studies (ABCD-2V Study
2004; ABCD Study 2002; ADVANCE Study 2009; BENEDICT
Study 2004; CALM II Study 2005; Crepaldi 1995; DIRECT
Studies 2009; EUCLID Study 1997; HOPE Study 2000; Kvetny
2001; ONTARGET Study 2008; Perrin 2008; RASS Study 2002;
Ravid 1998; ROADMAP Study 2009; TRANSCEND Study
2009; Tuominen 1998; Velussi 1996); unclear in 2/26 (8%) stud-
ies (Chan 1992; Joglekar 1998); and of high risk in 6/26 (23%)
studies (Baba 2001; FACET Study 1998; Kavgaci 2002; Lin 1995;
Scognamiglio 1997; UKPDS Study 1998).
Blinding of outcome assessors (detection bias) was judged to be of
low risk in 7/26 (27%) studies (ABCD-2V Study 2004; ABCD
Study 2002; ADVANCE Study 2009; Chan 1992; EUCLID
Study 1997; RASS Study 2002; UKPDS Study 1998), and un-
clear in 19/26 (73%) studies (Baba 2001; BENEDICT Study
2004; CALM II Study 2005; Crepaldi 1995; DIRECT Studies
2009; FACET Study 1998; HOPE Study 2000; Joglekar 1998;
Kavgaci 2002; Kvetny 2001; Lin 1995; ONTARGET Study
2008; Perrin 2008; RASS Study 2002; Ravid 1998; ROADMAP
Study 2009; Scognamiglio 1997; TRANSCEND Study 2009;
Tuominen 1998; Velussi 1996).
Incomplete outcome data
Incomplete data was judged to be of low risk in 14/26 (54%)
studies (ABCD-2V Study 2004; ADVANCE Study 2009;
BENEDICT Study 2004; CALM II Study 2005; Chan 1992;
Crepaldi 1995; Kavgaci 2002; ONTARGET Study 2008; RASS
Study 2002; ROADMAP Study 2009; Scognamiglio 1997;
TRANSCEND Study 2009; Tuominen 1998; UKPDS Study
1998); unclear in 4/26 (15%) studies (ABCD Study 2002; Baba
2001; HOPE Study 2000; Lin 1995); and of high risk in 8/26
(31%) studies (DIRECT Studies 2009; EUCLID Study 1997;
FACET Study 1998; Joglekar 1998; Kvetny 2001; Perrin 2008;
Ravid 1998; Velussi 1996).
Selective reporting
Incomplete data was judged to be of low risk in 15/26 (57%)
studies (ADVANCE Study 2009; Baba 2001; BENEDICT Study
2004; Chan 1992; DIRECT Studies 2009; EUCLID Study
1997; FACET Study 1998; HOPE Study 2000; Kvetny 2001;
ONTARGET Study 2008; Perrin 2008; RASS Study 2002; Ravid
1998; TRANSCEND Study 2009; UKPDS Study 1998); un-
clear in 3/26 (12%) studies (ROADMAP Study 2009; Tuominen
1998; Velussi 1996); and of high risk in 8/26 (31%) studies
(ABCD-2V Study 2004; ABCD Study 2002; CALM II Study
2005; Crepaldi 1995; Joglekar 1998; Kavgaci 2002; Lin 1995;
Scognamiglio 1997).
Other potential sources of bias
Intention-to-treat analysis
Intention-to-treat analysis was used in 12/26 (43%) studies (Baba
2001; EUCLID Study 1997; HOPE Study 2000; ABCD-2V
Study 2004; ADVANCE Study 2009; DIRECT Studies 2009;
ONTARGET Study 2008; Perrin 2008; RASS Study 2002;
TRANSCEND Study 2009).
Loss to follow-up
The percentage of patients lost to follow-up ranged between 0%
and 17.2%.
9Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Effects of interventions
Prevention of microalbuminuria and
macroalbuminuria or both
ACEi versus placebo
Compared to placebo or no treatment, ACEi significantly reduced
the risk for new onset of microalbuminuria or macroalbuminuria
by 29% (Analysis 1.1 (8 studies, 11906 participants): RR 0.71,
95% CI 0.56 to 0.89, P = 0.004) with no evidence of heterogene-
ity in the magnitude of effect across the included studies (Chi² =
10.20, I² = 31%, P = 0.18). This analysis was dominated by the
ADVANCE Study 2009 which contributed 45.5% of the weight
to the summary estimate, but exclusion of this study did not sub-
stantially change the overall estimate (RR 0.63, 95% CI 0.48 to
0.83, P = 0.0009). Subgroup analysis and meta-regression revealed
a larger estimate of effect was reported in studies that were small,
did not have adequate allocation concealment or use intention-
to-treat analysis (P < 0.05, Table 2)
ARB versus placebo
Compared with placebo or no treatment, no significant effect on
new onset microalbuminuria or macroalbuminuria was observed
for ARB (Analysis 2.1 (5 studies, 7653 patients): RR 0.90, 95% CI
0.68 to 1.19, P = 0.45). There was some evidence of heterogeneity
in the effect across the included studies (Chi² = 11.16, I² = 56%,
P = 0.06). Subgroup analysis suggested a greater likelihood of
benefit in studies recruiting patients with previous cardiovascular
disease or risk factors, type 2 rather than type 1 diabetes, higher
baseline risk of albuminuria progression, and adequate allocation
concealment (P < 0.05, Table 2).
ACEi versus ARB
Only two studies compared between ACEi and ARB on new onset
albuminuria, and no clear difference was observed (Analysis 3.1
(2 studies, 4303 patients): RR 0.57, 95% CI 0.14 to 2.23, P =
0.42). There was evidence of heterogeneity in the magnitude of
effect between the two studies (Chi² = 6.76, I² = 85%, P = 0.009).
A third study (Kavgaci 2002) did not provide detailed data for
new onset albuminuria and could therefore not be included in the
meta-analysis.
Combination ACEi and ARB therapy
Two studies combined ACEi and ARB and compared to ACEi
alone (Analysis 5.1 (2 studies, 4171 patients): RR 0.88, 95% CI
0.73 to 1.00, P = 0.051). One of these studies (CALM II Study
2005) reported urinary albumin excretion levels remained stable
through the follow-up period.
ACEi versus other active agents
ACEi significantly reduced the risk for new onset of microalbu-
minuria or macroalbuminuria when compared to CCBs (Analysis
4.1 (5 studies, 1253 patients); RR 0.60, 95% CI 0.42 to 0.85, P =
0.004) with no evidence of heterogeneity (Chi² = 1.37, I² = 0.0%,
P = 0.71) .
There was no clear difference in the risk of new onset albuminuria
with ACEi compared with beta-blockers (Analysis 5.2 (1 study,
299 patients): RR, 1.01; 95% CI, 0.74 to 1.37), or ACEi plus
calcium channel blockers versus ACEi (Analysis 5.3 (1 study, 603
patients): RR 1.05, 95% CI 0.55 to 2.01), but the amount of data
available were limited.
CCBs versus placebo
Only one study compared a CCB (verapamil) with placebo and
no significant difference was seen in the risk of new onset microal-
buminuria (Analysis 5.4 (1 study, 603 patients): RR 1.19, 95%
CI 0.75 to 1.88).
All-cause mortality
Twelve studies provided information on the risk of death with
ACEi compared to placebo or no treatment. All-cause mortality
was reduced (Analysis 1.2 (6 studies, 11,350 patients): RR 0.84,
95% CI 0.73 to 0.97) in the ACEi group compared to those re-
ceiving placebo or no treatment, with no evidence of heterogeneity
(Chi² = 1.27, I² = 0%, P = 0.87). No clear reduction in the risk of
death was observed in the five studies (7653 patients) comparing
ARB with placebo or no treatment (Analysis 2.2: RR 1.36, 95%
CI 0.64 to 1.41) with no evidence of heterogeneity (Chi² = 2.66,
I² = 0%, P = 0.45). Similar rates of death were observed in a di-
rect comparison between ACEi and ARB (Analysis 3.2 (2 studies,
4303 patients): RR 1.02, 95% CI 0.85 to 1.22; I² = 0%). The risk
of death was also similar in the five studies (1284 patients) that
compared ACEi and CCBs (Analysis 4.2: RR 0.84, 95% CI 0.26
to 2.73; Chi² = 0.02, I² = 0%, P = 0.89).
Doubling of serum creatinine and progression to
ESKD
Very few patients in these studies progressed to the end point of
doubling of serum creatinine or ESKD. As a result, no significant
difference in the risk for doubling serum creatinine (Analysis 1.3
(5 studies, 10,749 patients): RR 0.77, 95% CI 0.39 to 1.49; Chi²
= 4.15, I² = 52%, P = 0.13) or ESKD (Analysis 1.4 (3 studies,
10,504 patients): RR 1.94, 95% CI 0.6 to 5.70; Chi² = 0.09, I²
= 0%, P = 0.76) was found with ACEi compared with placebo.
Pooled analysis for doubling serum creatinine or ESKD were not
able to be calculated from the studies of ACEi compared with
CCBs since no such events were reported in the four relevant
studies (680 patients).
10Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Three studies (6217 patients) comparing ARB with placebo
showed no significant reduction in the risk for doubling serum
creatinine (Analysis 2.3: RR 0.1.36, 95% CI 0.64 to 2.88). Only
four patients in one of these three studies progressed to ESKD
(Analysis 2.4).
Adverse effects
The risk of cough was significantly increased with ACEi compared
with placebo/no treatment (Analysis 1.5.1 (6 studies, 11,791 pa-
tients): RR 1.84, 95% CI 1.24 to 2.72; Chi² = 5.15, I² = 3%, P
= 0.40), whereas there was no significant difference for headache
(Analysis 1.5.2) and hyperkalaemia (Analysis 1.5.3).
No significant difference in the risk of cough, headache or hyper-
kalaemia was found for ARB compared to placebo (Analysis 2.5).
Blood pressure
Systolic BP was significantly lower in the ACEi group (Analysis
1.6.1 (2 studies, 7526 patients): MD -5.37 mm Hg, 95% CI -
7.12 to -3.62), and ARB group (Analysis 2.6.1 (2 studies, 1770
patients): MD -3.28 mm Hg, 95% CI -5.29 to -2.90) when com-
pared to placebo. CCB significantly lowered systolic BP when
compared to ACEi (Analysis 4.5.1 (2 studies, 430 participants):
MD 4.00 mm Hg, 95% CI -1.59 to 6.41).
Diastolic BP was significantly lower in the ACEi group (Analysis
1.6.2 (2 studies, 7526 patients): MD -1.50 mm Hg, 95% CI -
1.50 to -1.50), and ARB group (Analysis 2.6.2 (2 studies, 1770
patients): MD -2.00 mm Hg, 95% CI -2.64 to -1.36) when com-
pared to placebo. There was no significant difference between CCB
and ACEi (Analysis 4.5.2 (2 studies, 430 participants): MD 1.22
mm Hg, 95% CI -0.42 to 2.85).
Other outcomes
Lipid profile, glycaemic control and urinary albumin/creatinine
ratio were either poorly reported or not reported and we therefore
could not perform meta-analyses for these outcomes.
D I S C U S S I O N
Summary of main results
Individuals with diabetes who develop kidney disease are at in-
creased risk of kidney failure, cardiovascular events and death
(Ninomiya 2009; Perkovic 2008). Current treatments provide
modest benefits once kidney diease is established, so primary pre-
vention has been the focus of much attention in recent years
(DIRECT Studies 2009; RASS Study 2002; ROADMAP Study
2009; Parfrey 2009). This updated systematic review has several
times more data than a previous analysis, and has shown that ACEi
reduced the risk of new onset kidney disease by 29% and the risk
of death by 16% in people with diabetes. Clear renal benefits were
observed among individuals without hypertension at baseline, and
in comparison to CCBs. These effects are also consistent across
a broad spectrum of people with diabetes, including individuals
with type 1 or type 2 diabetes, with or without hypertension, and
in placebo controlled studies or those comparing ACEi to other
blood pressure agents. Other studies have suggested ACEi also
prevent new onset diabetic retinopathy in patients without albu-
minuria (EUCLID Study 1997; RASS Study 2002). In contrast
we were unable demonstrate similar overall benefits for ARB over-
all, although it remains possible that benefits may be present for
high risk individuals. These results suggest that ACEi could be
routinely considered for the primary prevention of microvascular
disease and death in people with diabetes regardless of blood pres-
sure levels, although further study is needed to evaluate the cost
effectiveness of this approach.
Potential biases in the review process
The main limitation of this study was that the effects of blood
pressure lowering agents on ESKD could not be ascertained, pos-
sibly due to the slowly progressive nature of DKD, and the re-
sultant low incidence of ESKD in the population. As the use of
ACEi in this population also reduced the risk of death from any
cause, the impact of this limitation for this drug class is likely to be
modest. It has been generally accepted that the onset of albumin-
uria precedes kidney failure and is thus a reliable sign of DKD,
but this notion has been challenged by reports of diabetic patients
with decreased renal function but without albuminuria (DIRECT
Studies 2009). Although observational studies show a strong and
graded relationship between albuminuria levels and the risk of de-
creasing GFR and the development of kidney failure (Adler 2003;
Gerstein 2001; Messent 1992). The available clinical studies have
not demonstrated that preventing microalbuminuria will neces-
sarily lead to reductions in kidney failure. This is mainly a result
of the slow rate of decline in kidney function in diabetes, meaning
that very long follow up would be required in people with diabetes
and normoalbuminuria (Levey 2009). Further study is needed to
confirm whether the prevention of microalbuminuria would lead
to fewer kidney failure or cardiovascular events (Klausen 2004).
Agreements and disagreements with otherstudies or reviews
ACEi and ARB have been recommended interchangeably in most
guidelines for the treatment of people with diabetes (Table 1).The
available data, summarized in this review, suggest that the benefits
of ACEi for the prevention of DKD as well as death were clear,
while as for ARB no clear effects on mortality was observed and
11Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

renal benefits were only found in subgroup analyses. ACEi were
also superior to calcium channel blockers in head to head compar-
isons, but little data was available for other drug classes. Studies in
people with DKD have identified clear benefit for ARB in the pre-
vention of ESKD, but have similarly failed to show any benefit for
cardiovascular outcomes or death (Strippoli 2004).Other studies
have also demonstrated consistent preventive effects of ARB on
diabetic retinopathy (Chaturvedi 2008; RASS Study 2002; Sjølie
2008). Caution is required in interpreting potential differences in
the effects of ACEi and ARB. Most ARB studies (DIRECT Studies
2009; RASS Study 2002) in this meta-analysis recruited mainly
normotensive patients at low renal and vascular risk, so event rates
were modest limiting study power. Metaregression also identified
baseline renal and cardiovascular risk as a significant effect modi-
fier for ARB in the prevention of kidney disease, with evidence of
benefit in high risk individuals that was similar in magnitude to
that reported for ACEi. The likelihood of similar effects of the two
classes is further supported by the results of the large ONTARGET
Study 2008 in which a head-to-head comparison demonstrated
that ARB and ACEi were equivalent for the prevention of DKD
in individuals at high cardiovascular risk, and that also suggested
additional benefit for new onset albuminuria when the two classes
of drugs were combined (ONTARGET Study 2008). The consis-
tency of effect demonstrated for ACEi, as well as the clear mortal-
ity benefits observed, suggest that these agents should be the first
choice for the primary prevention intervention of DKD, while
ARB appear a reasonable alternative in high risk individuals who
are unable to tolerate ACEi.
Another finding in this meta-analysis was that the benefits for pri-
mary prevention of DKD were similar in people with and without
hypertension at baseline, so that ACEi were effective even among
groups that are considered normotensive. As RAS blockade has
already been proven to be effective at preventing ESKD in indi-
viduals with established DKD (Strippoli 2004), these results sug-
gest that ACEi are likely to be beneficial for all individuals with
diabetes who are able to tolerate these agents.
Treatment with ACEi could therefore be recommended in nor-
moalbuminuric patients with diabetes for at least two purposes:
the primary prevention of kidney disease, as well as reduction in
the risk of death in this population. ACEi may be used in prefer-
ence to ARB based on the stronger data available for this class of
agents. If these data are applied to a broad population of people
with diabetes, the large excess burden of morbidity and mortality
suffered by these individuals may be substantially reduced.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
Our data therefore suggest that ACEi could prevent new onset
kidney disease and also reduce the risk of death in diabetics with
normoalbuminuria so should be the treatment of choice in this
population.
Implications for research
Future studies of antihypertensive agents in diabetic patients with
no kidney disease should report microalbuminuria and other re-
nal outcomes as well as the usually reported outcomes - all-cause
mortality and cardiovascular endpoints.
A C K N O W L E D G E M E N T S
We acknowledge the editorial and administrative support of
Narelle Willis and Gail Higgins, trial search coordinators of the
Cochrane Renal Group, provided search strategies for this review.
We are particularly indebted to Janice Pogue and the HOPE in-
vestigators; Michael Mauer and the RASS investigators; Drs An-
dersen, Ravid, Kvetny, Tuominen, Baba, Velussi, and Lin, who
provided data of normoalbuminuric patients with diabetes in their
study or information about study design and conduct upon re-
quest.
R E F E R E N C E S
References to studies included in this review
ABCD-2V Study 2004 {published data only}
Estacio RO, Coll JR, Tran ZV, Schrier RW. Effect of
intensive blood pressure control with valsartan on urinary
albumin excretion in normotensive patients with type 2
diabetes. American Journal of Hypertension 2006;19(12):
1241–8. [MEDLINE: 17161769]
Estacio RO, Esler A, Lundgren R, Schrier RW. Aggressive
blood pressure control with valsartan in normotensive Type
2 diabetic patients results in regression of albuminuria.
[abstract]. Journal of the American Society of Nephrology
2004;15(Oct):568A.
ABCD Study 2002 {published data only}
Estacio RO, Jeffers B, Biggerstaff S, Schrier RW. Effects of
a calcium channel antagonist versus an ace inhibitor on
diabetic nephropathy [abstract]. Journal of the American
Society of Nephrology 1998;9(Program & Abstracts):114A.
Estacio RO, Jeffers BW, Gifford N, Schrier RW. Effect
of blood pressure control on diabetic microvascular
complications in patients with hypertension and type
2 diabetes. Diabetes Care 2000;23(Suppl 2):B54–64.
12Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
[MEDLINE: 10860192]
Estacio RO, Jeffers BW, Hiatt WR, Biggerstaff SL, Gifford
N, Schrier RW. The effect of nisoldipine as compared with
enalapril on cardiovascular outcomes in patients with non-
insulin-dependent diabetes and hypertension. New England
Journal of Medicine 1998;338(10):645–52. [MEDLINE:
9486993]
Estacio RO, Mehler P, Esler A, Schrier RW. Aggressive
lowering of blood pressure in normotensive type 2
diabetic patients: beneficial effects on stroke, progression
of retinopathy and nephropathy [abstract]. Journal of
the American Society of Nephrology 2001;12(Program &
Abstracts):146A.
Estacio RO, Savage S, Nagel NJ, Schrier RW. Baseline
characteristics of participants in the Appropriate Blood
Pressure Control in Diabetes trial. Controlled Clinical Trials
1996;17(3):242–57. [MEDLINE: 8877260]
Estacio RO, Schrier RW. Antihypertensive therapy in type
2 diabetes: implications of the appropriate blood pressure
control in diabetes (ABCD) trial. American Journal of
Cardiology 1998;82(9B):9R–14R. [MEDLINE: 9822137]
Savage S, Estacio RO, Jeffers B, Schrier RW. Urinary
albumin excretion as a predictor of diabetic retinopathy,
neuropathy, and cardiovascular disease in NIDDM. Diabetes
Care 1996;19(11):1243–8. [MEDLINE: 8908388]∗ Schrier RW, Estacio RO, Esler A, Mehler P. Effects of
aggressive blood pressure control in normotensive type 2
diabetic patients on albuminuria, retinopathy and strokes.
Kidney International 2002;61(3):1086–97. [MEDLINE:
11849464]
Schrier RW, Estacio RO, Jeffers B. Appropriate Blood
Pressure Control in NIDDM (ABCD) Trial. Diabetologia
1996;39(12):1646–54. [MEDLINE: 8960857]
Stabler SP, Estacio R, Jeffers BW, Cohen JA, Allen
RH, Schrier RW. Total homocysteine is associated
with nephropathy in non-insulin-dependent diabetes
mellitus. Metabolism: Clinical & Experimental 1999;48(9):
1096–101. [MEDLINE: 10484047]
ADVANCE Study 2009 {published data only}
ADVANCE Collaborative Group. ADVANCE--Action in
Diabetes and Vascular Disease: patient recruitment and
characteristics of the study population at baseline. Diabetic
Medicine 2005;22(7):882–8. [MEDLINE: 15975103]
ADVANCE Collaborative Group, Patel A, MacMahon S,
Chalmers J, Neal B, Billot L, et al.Intensive blood glucose
control and vascular outcomes in patients with type 2
diabetes. New England Journal of Medicine 2008;358(24):
2560–72. [MEDLINE: 18539916]
ADVANCE Management Committee. Study rationale
and design of ADVANCE: action in diabetics and vascular
disease - preterax and diamicron MR controlled evaluation.
Diabetologia 2001;44(9):1118–20. [MEDLINE:
11596665]
Anonymous. Rationale and design of the ADVANCE
study: a randomised trial of blood pressure lowering and
intensive glucose control in high-risk individuals with type 2
diabetes mellitus. Action in Diabetes and Vascular Disease:
PreterAx and DiamicroN Modified-Release Controlled
Evaluation. Journal of Hypertension - Supplement 2001;19
(4):S21–8. [MEDLINE: 11848259]
Chalmers J. ADVANCE Study: objectives, design and
current status [Etude ADVANCE : objectifs, protocole
et état actuel]. Drugs 2003;63 Spec No. 1:39–44.
[MEDLINE: 12708881]
de Galan BE, Ninomiya T, Perrovic V, Pillai A, Patel A,
Neal AC, et al.Renoprotective effects of blood pressure
lowering with perindopril-indapamide below current targets
in people with type 2 diabetes mellitus: Results of the
ADVANCE trial [abstract]. Diabetes 2008;57(Suppl 1):
A218–9.∗ de Galan BE, Perkovic V, Ninomiya T, Pillai A, Patel A,
Cass A, et al.Lowering blood pressure reduces renal events in
type 2 diabetes. Journal of the American Society of Nephrology
2009;20(4):883–92. [MEDLINE: 19225038]
Heerspink HJ, Ninomiya T, Perkovic V, Woodward M,
Zoungas S, Cass A, et al.Effects of a fixed combination of
perindopril and indapamide in patients with type 2 diabetes
and chronic kidney disease. European Heart Journal 2010;
31(23):2888–96. [MEDLINE: 20501479]
Jardine M, Ninomiya T, Perkovic V, Woodward M, Pillai
A, Cass A, et al.Predictive baseline factors for major
renal events: a proportional hazards model based on the
Advance Study [abstract]. Journal of the American Society of
Nephrology 2008;19(Abstracts Issue):543A.
Ninomiya T, Zoungas S, Neal B, Woodward M, Patel
A, Perkovic V, et al.Efficacy and safety of routine blood
pressure lowering in older patients with diabetes: results
from the ADVANCE trial. Journal of Hypertension 2010;28
(6):1141–9. [MEDLINE: 20486273]
Patel A, MacMahon S, Chalmers J, Neal B, Woodward M,
Billot L, et al.Effects of a fixed combination of perindopril
and indapamide on macrovascular and microvascular
outcomes in patients with type 2 diabetes mellitus (the
ADVANCE trial): a randomised controlled trial. Lancet
2007;370(9590):829–40. [MEDLINE: 17765963]
Perkovic V, de Galan B, Chalmers J, Ninomiya T, Patel A,
Cass A, et al.Renoprotection with perindopril-indapamide
below current recommended blood pressure targets in
patients with type 2 diabetes mellitus: results of the
ADVANCE trial [abstract]. Nephrology 2008;13(Suppl 3):
A121.
Perkovic V, Ninomiya T, de Galan BE, Zoungas S, Cass A,
Patel A, et al.Joint effects of routine blood pressure lowering
and intensive glucose control in the ADVANCE trial
[abstract no: LB-002]. American Society of Nephrology
(ASN) Renal Week; 2008 Nov 4-9; Philadelphia, PA. 2008.
Perkovic V, Zoungas S, Heerspink HL, Woodward M,
Jun M, Cass A, et al.Intensive glucose lowering and end
stage kidney disease - new data from the ADVANCE trial
[abstract]. Nephrology 2011;16(Suppl 1):42.
Poulter NR. Blood pressure and glucose control in subjects
with diabetes: new analyses from ADVANCE. Journal of
Hypertension - Supplement 2009;27(1):S3–8. [MEDLINE:
13Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
19483505]
Zoungas S, de Galan BE, Ninomiya T, Grobbee D, Hamet
P, Heller S, et al.Combined effects of routine blood pressure
lowering and intensive glucose control on macrovascular and
microvascular outcomes in patients with type 2 diabetes:
New results from the ADVANCE trial. Diabetes Care 2009;
32(11):2068–74. [MEDLINE: 19651921]
Baba 2001 {published data only}
Baba S, The J-MIND Study Group. Nifedipine and
enalapril equally reduce the progression of nephropathy in
hypertensive type 2 diabetics. Diabetes Research & Clinical
Practice 2001;54(3):191–201. [MEDLINE: 11689274]
BENEDICT Study 2004 {published data only}
BENEDICT G. The BErgamo NEphrologic DIabetes
Complications Trial (BENEDICT): design and baseline
characteristics. Controlled Clinical Trials 2003;24(4):
442–61. [MEDLINE: 12865039]
De Cosmo S, Motterlini N, Prudente S, Pellegrini F,
Trevisan R, Bossi A, et al.Impact of the PPAR-gamma2
Pro12Ala polymorphism and ACE inhibitor therapy
on new-onset microalbuminuria in type 2 diabetes:
evidence from BENEDICT. Diabetes 2009;58(12):2920–9.
[MEDLINE: 19720797]
Remuzzi G, Macia M, Ruggenenti P. Prevention and
treatment of diabetic renal disease in type 2 diabetes:
the BENEDICT study. Journal of the American Society
of Nephrology 2006;17(4 Suppl 2):S90–7. [MEDLINE:
16565256]
Ruggenenti P, Fassi A, Ilieva AP, Iliev IP, Chiurchiu C,
Rubis N, et al.Effects of verapamil added-on trandolapril
therapy in hypertensive type 2 diabetes patients with
microalbuminuria: the BENEDICT-B randomized trial.
Journal of Hypertension 2011;29(2):207–16. [MEDLINE:
21243736]∗ Ruggenenti P, Fassi A, Parvanova Ilieva A, Bruno
Petrov Iliev I, Brusegan V, Rubis N, et al.Preventing
microalbuminuria in type 2 diabetes. New England
Journal of Medicine 2004;351(19):1941–51. [MEDLINE:
15516697]
Ruggenenti P, Iliev I, Costa GM, Parvanova A, Perna A,
Giuliano GA, et al.Preventing left ventricular hypertrophy
by ACE inhibition in hypertensive patients with type 2
diabetes: a prespecified analysis of the Bergamo Nephrologic
Diabetes Complications Trial (BENEDICT). Diabetes Care
2008;31(8):1629–34. [MEDLINE: 18443191]
Ruggenenti P, Perna A, Ganeva M, Ene-Iordache B,
Remuzzi G, BENEDICT Study Group. Impact of blood
pressure control and angiotensin-converting enzyme
inhibitor therapy on new-onset microalbuminuria in type
2 diabetes: a post hoc analysis of the BENEDICT trial.
Journal of the American Society of Nephrology 2006;17(12):
3472–81. [MEDLINE: 17082240]
Ruggenenti P, Remuzzi G. Primary prevention of renal
failure in diabetic patients: the Bergamo Nephrologic
Diabetes Complication Trial. Journal of Hypertension -
Supplement 1998;16(1):S95–7. [MEDLINE: 9534106]
CALM II Study 2005 {published data only}
Andersen NH, Knudsen ST, Poulsen PL, Poulsen SH,
Helleberg K, Eiskjaer H, et al.Dual blockade with
candesartan cilexetil and lisinopril in hypertensive patients
with diabetes mellitus: rationale and design. Journal of
the Renin-Angiotensin-Aldosterone System 2003;4(2):96–9.
[MEDLINE: 12806591]∗ Andersen NH, Poulsen PL, Knudsen ST, Poulsen SH,
Eiskjaer H, Hansen KW, et al.Long-term dual blockade
with candesartan and lisinopril in hypertensive patients with
diabetes: the CALM II study. Diabetes Care 2005;28(2):
273–7. [MEDLINE: 15677778]
Knudsen ST, Andersen NH, Poulsen SH, Eiskjaer H,
Hansen KW, Helleberg K, et al.Pulse pressure lowering
effect of dual blockade with candesartan and lisinopril vs.
high-dose ACE inhibition in hypertensive type 2 diabetic
subjects: a CALM II study post-hoc analysis. American
Journal of Hypertension 2008;21(2):172–6. [MEDLINE:
18188164]
Chan 1992 {published data only}
Chan JC, Cockram CS, Nicholls MG, Cheung CK,
Swaminathan R. Comparison of enalapril and nifedipine
in treating non-insulin dependent diabetes associated with
hypertension: one year analysis. BMJ 1992;305(6860):
981–5. [MEDLINE: 1458144]∗ Chan JC, Ko GT, Leung DH, Cheung RC, Cheung MY,
So WY, et al.Long-term effects of angiotensin-converting
enzyme inhibition and metabolic control in hypertensive
type 2 diabetic patients. Kidney International 2000;57(2):
590–600. [MEDLINE: 10652036]
Chan JC, Nicholls MG, Cheung CK, Law LK, Swaminathan
R, Cockram CS. Factors determining the blood pressure
response to enalapril and nifedipine in hypertension
associated with NIDDM. Diabetes Care 1995;18(7):
1001–6. [MEDLINE: 7555530]
Chan JC, Yeung VT, Leung DH, Tomlinson B, Nicholls
MG, Cockram CS. The effects of enalapril and nifedipine
on carbohydrate and lipid metabolism in NIDDM. Diabetes
Care 1994;17(8):859–62. [MEDLINE: 7956631]
Crepaldi 1995 {published data only}
Crepaldi G, Carraro A, Brocco E, Adezati L, Andreani
D, Bompiani G, et al.Hypertension and non-insulin-
dependent diabetes. Acta Diabetologica 1995;32(3):203–8.
[MEDLINE: 8590792]
DIRECT Studies 2009 {published data only}∗ Bilous R, Chaturvedi N, Sjolie AK, Fuller J, Klein R,
Orchard T, et al.Effect of candesartan on microalbuminuria
and albumin excretion rate in diabetes: three randomized
trials. Annals of Internal Medicine 2009;151(1):11-20, W3-
4. [MEDLINE: 19451554]
Bilous RW, Parving H, Nishi C. DIRECT-Renal: The effect
of the angiotensive type 1 receptor blocker candesartan
on the development of microalbuminuria in type 1 and
type 2 diabetes [abstract]. Journal of the American Society of
Nephrology 2008, (Abstracts Issue).
Chaturvedi N, Porta M, Klein R, Orchard T, Fuller J,
Parving HH, et al.Effect of candesartan on prevention
14Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(DIRECT-Prevent 1) and progression (DIRECT-Protect
1) of retinopathy in type 1 diabetes: randomised, placebo-
controlled trials. Lancet 2008;372(9647):1394–402.
[MEDLINE: 18823656]
Chaturvedi N, Sjoelie AK, Svensson A, DIRECT
Programme Study Group. The DIabetic Retinopathy
Candesartan Trials (DIRECT) Programme, rationale and
study design. Journal of the Renin-Angiotensin-Aldosterone
System 2002;3(4):255–61. [MEDLINE: 12584669]
Hirsch HH, Tuncer M, Friman S, Wiececk A, Citterio
F, Klinger M, et al.Prospective study of polyomavirus
BK viruria and viremia in de novo renal transplantation
[abstract]. American Journal of Transplantation 2005;5
(Suppl 11):272.
Hirsch HH, Vincenti F, Friman S, Wiecek A, Pescovitz MD,
Jenssen T, et al.Polomarvirus BK viruria and viremia in de
novo renal transplantation comparing cyclosporine and
tacrolimus: a multivariate analysis for the DIRECT Study
[abstract]. Journal of the American Society of Nephrology
2009, (Abstract Issue):85–6.
Jenssen T, Campistol J, Uchida K, Pescovitz M, Citterio F.
Insulin release and insulin sensitivity in patients developing
glucose abnormalities post-transplant: the relative effects of
tacrolimus and cyclosporine [abstract]. American Journal of
Transplantation 2006;6(Suppl 2):356.
Jenssen T, Campistol J, Uchida K, Pescovitz M, Citterio
F, DIRECT Study Group. Insulin release and insulin
sensitivity in patients developing glucose abnormalities
post-transplant: the relative effects of tacrolimus and
cyclosporine [abstract]. Journal of the American Society of
Nephrology 2006;17(Abstracts):233A.
Marchetti P, Tuncer M, Wiecek A, Chadban S, El-Shahawy
M, Budde K, et al.Steroid dose affects risk of glucose
metabolism abnormalities differently with cyclosporine
or tacrolimus in renal transplant recipients [abstract].
American Journal of Transplantation 2006;6(Suppl 2):357.
Marchetti P, Vincenti F, Jenssen T, Friman S. 6-month results
from randomized, international trial of cyclosporine versus
tacrolimus in de novo renal transplant patients: progression
of pre-existing diabetes and glucose abnormalities [abstract].
Transplant International 2007;20(Suppl 2):114.
Rostaing L, Vincenti F, Friman S, Scheuermann E,
DIRECT Study Group. Glucose metabolism disorders
after renal transplantation: results of an international,
randomized trial comparing cyclosporine versus tacrolimus
[abstract]. Journal of the American Society of Nephrology
2006;17(Abstracts):231A.
Rostaing L, Vincenti F, Friman S, Scheuermann E, Rostaing
L. Glucose metabolism disorders after renal transplantation:
results of an international, randomized trial comparing
cyclosporine versus tacrolimus [abstract]. American Journal
of Transplantation 2006;6(Suppl 2):83.
Sjolie AK, Klein R, Porta M, Orchard T, Fuller J, Parving
HH, et al.Effect of candesartan on progression and
regression of retinopathy in type 2 diabetes (DIRECT-
Protect 2): a randomised placebo-controlled trial. Lancet
2008;372(9647):1385–93. [MEDLINE: 18823658]
Sjolie AK, Porta M, Parving HH, Bilous R, Klein R,
DIRECT Programme Study Group. The DIabetic
REtinopathy Candesartan Trials (DIRECT) Programme:
baseline characteristics. Journal of the Renin-Angiotensin-
Aldosterone System 2005;6(1):25–32. [MEDLINE:
16088848]
Vincenti F, Friman S, Scheuermann E, Rostaing L,
Jenssen T, Campistol JM, et al.Results of an international,
randomized trial comparing glucose metabolism disorders
and outcome with cyclosporine versus tacrolimus.
American Journal of Transplantation 2007;7(6):1506–14.
[MEDLINE: 17359512]
Vincenti F, Pescovitz MD, El-Shahawy M. Glucose
metabolism disorders in non-white renal transplant patients
receiving cyclosporine or tacrolimus in an international,
randomized trial [abstract]. Transplant International 2007;
20(Suppl 2):115.
Vincenti F, Rostaing L, DIRECT (Diabetes Incidence
after REnal Transplantation: Neoral C2 monitoring
versus Tacrolimus) investigators. Rationale and design
of the DIRECT study: a comparative assessment of the
hyperglycemic effects of tacrolimus and cyclosporine
following renal transplantation. Contemporary Clinical
Trials 2005;26(1):17–24. [MEDLINE: 15837449]
Vincenti F, Tuncer M, Castagneto M, Klinger M, Friman
S, Scheuermann EH, et al.Prospective, multicenter,
randomized trial to compare incidence of new-onset diabetes
mellitus and glucose metabolism in patients receiving
cyclosporine microemulsion versus tacrolimus after de novo
kidney transplantation. Transplantation Proceedings 2005;
37(2):1001–4. [MEDLINE: 15848604]
Vincenti F, Tuncer M, Castagneto M, Klinger M, Friman
S, Scheuermann EH, et al.Prospective, multicenter,
randomized trial to compare incidence of new-onset diabetes
mellitus and glucose metabolism in patients receiving
cyclosporine microemulsion versus tacrolimus after de novo
kidney transplantation [abstract]. Transplantation 2004;78
(2):141.
EUCLID Study 1997 {published data only}
Chaturvedi N, Sjolie AK, Stephenson JM, Abrahamian
H, Keipes M, Castellarin A, et al.Effect of lisinopril
on progression of retinopathy in normotensive people
with type 1 diabetes. The EUCLID Study Group.
EURODIAB Controlled Trial of Lisinopril in Insulin-
Dependent Diabetes Mellitus. Lancet 1998;351(9095):
28–31. [MEDLINE: 9433426]∗ Chaturvedi N, Stevenson J, Fuller JH, Rottiers R, Ferriss B,
Karamanos B, et al.Randomised placebo-controlled trial of
lisinopril in normotensive patients with insulin-dependent
diabetes and normoalbuminuria or microalbuminuria. The
EUCLID Study Group. Lancet 1997;349(9068):1787–92.
[MEDLINE: 9269212]
Fuller JH, Anzalone D and EUCLID Study Group. Renal
effect of lisinopril in insulin dependent diabetes mellitus
(IDDM) without hypertension [abstract]. Journal of the
15Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
American Society of Nephrology 1996;7(9):1357.
Penno G, Chaturvedi N, Talmud PJ, Cotroneo P, Manto A,
Nannipieri M, et al.Effect of angiotensin-converting enzyme
(ACE) gene polymorphism on progression of renal disease
and the influence of ACE inhibition in IDDM patients:
findings from the EUCLID Randomized Controlled Trial.
EURODIAB Controlled Trial of Lisinopril in IDDM.
Diabetes 1998;47(9):1507–11. [MEDLINE: 9726242]
Schalkwijk CG, Chaturvedi N, Twaafhoven H, van
Hinsbergh VW, Stehouwer CD, EUCLID Study
Group. Amadori-albumin correlates with microvascular
complications and precedes nephropathy in type 1 diabetic
patients. European Journal of Clinical Investigation 2002;32
(7):500–6. [MEDLINE: 12153550]
Sjolie AK, Chaturvedi N, Fuller J. Effect of lisinopril
on progression of retinopathy and microalbuminuria in
normotensive subjects with insulin-dependent diabetes
mellitus. Ugeskrift for Laeger 1999;161(7):949–52.
[MEDLINE: 10051804]
FACET Study 1998 {published data only}
Tatti P, Pahor M, Byington RP, Di Mauro P, Guarisco R,
Strollo G, et al.Outcome results of the Fosinopril Versus
Amlodipine Cardiovascular Events Randomized Trial
(FACET) in patients with hypertension and NIDDM.
Diabetes Care 1998;21(4):597–603. [MEDLINE:
9571349]
HOPE Study 2000 {published data only}
Anonymous. The HOPE (Heart Outcomes Prevention
Evaluation) Study: the design of a large, simple randomized
trial of an angiotensin-converting enzyme inhibitor
(ramipril) and vitamin E in patients at high risk of
cardiovascular events. The HOPE study investigators.
Canadian Journal of Cardiology 1996;12(2):127–37.
[MEDLINE: 8605634]
Gerstein HC. Diabetes and the HOPE study: implications
for macrovascular and microvascular disease. International
Journal of Clinical Practice 2001;117(Suppl):8–12.
[MEDLINE: 21572783]
Gerstein HC, Bosch J, Pogue J, Taylor DW, Zinman B,
Yusuf S. Rationale and design of a large study to evaluate
the renal and cardiovascular effects of an ACE inhibitor and
vitamin E in high-risk patients with diabetes. The MICRO-
HOPE Study. Microalbuminuria, cardiovascular, and
renal outcomes. Heart Outcomes Prevention Evaluation.
Diabetes Care 1996;19(11):1225–8. [MEDLINE:
8908384]
Gerstein HC, Pogue J, Mann JF, Lonn E, Dagenais GR,
McQueen M, et al.The relationship between dysglycaemia
and cardiovascular and renal risk in diabetic and non-
diabetic participants in the HOPE study: a prospective
epidemiological analysis. Diabetologia 2005;48(9):
1749–55. [MEDLINE: 16059716]∗ Heart Outcomes Prevention Evaluation (HOPE) Study
Investigators. Effects of ramipril on cardiovascular and
microvascular outcomes in people with diabetes mellitus:
results of the HOPE study and MICRO-HOPE substudy.
Lancet 2000;335(9200):253–9. [MEDLINE: 10675071]
Hoogwerf BJ, Young JB. The HOPE study. Ramipril
lowered cardiovascular risk, but vitamin E did not.
Cleveland Clinic Journal of Medicine 2000;67(4):287–93.
[MEDLINE: 10780101]
Lamy A, Yusuf S, Pogue J, Gafni A, Heart Outcomes
Prevention Evaluation Investigators. Cost implications
of the use of ramipril in high-risk patients based on the
Heart Outcomes Prevention Evaluation (HOPE) study.
Circulation 2003;107(7):960–5. [MEDLINE: 12600907]
Lonn E, Mathew J, Pogue J, Johnstone D, Danisa K,
Bosch J, et al.Relationship of electrocardiographic left
ventricular hypertrophy to mortality and cardiovascular
morbidity in high-risk patients. European Journal of
Cardiovascular Prevention & Rehabilitation 2003;10(6):
420–8. [MEDLINE: 14671464]
Lonn E, Yusuf S, Hoogwerf B, Pogue J, Yi Q, Zinman B, et
al.Effects of vitamin E on cardiovascular and microvascular
outcomes in high-risk patients with diabetes: results of the
HOPE study and MICRO-HOPE substudy. Diabetes Care
2002;25(11):1919–27. [MEDLINE: 12401733]
Mann JF, Gerstein HC, Pogue J, Bosch J, Yusuf S. Renal
insufficiency (RI) as predicator of cardiovascular (CV)
outcomes and impact of ramipril: the HOPE study
[abstract]. Journal of the American Society of Nephrology
2000;11(Sept):156A.
Mann JF, Gerstein HC, Pogue J, Bosch J, Yusuf S. Renal
insufficiency as a predictor of cardiovascular outcomes and
the impact of ramipril: the HOPE randomized trial. Annals
of Internal Medicine 2001;134(8):629–36. [MEDLINE:
11304102]
Mann JF, Gerstein HC, Yi QL, Franke J, Lonn EM,
Hoogwerf BJ, et al.Progression of renal insufficiency in type
2 diabetes with and without microalbuminuria: results of
the Heart Outcomes and Prevention Evaluation (HOPE)
randomized study. American Journal of Kidney Diseases
2003;42(5):936–42. [MEDLINE: 14582037]
Mann JF, Gerstein HC, Yi QL, Lonn EM, Hoogwerf BJ,
Rashkow A, et al.Development of renal disease in people at
high cardiovascular risk: results of the HOPE randomized
study. Journal of the American Society of Nephrology 2003;14
(3):641–7. [MEDLINE: 12595499]
Mann JF, Lonn EM, Yi Q, Gerstein HC, Hoogwerf BJ,
Pogue J, et al.Effects of vitamin E on cardiovascular outcomes
in people with mild-to-moderate renal insufficiency: results
of the HOPE study. Kidney International 2004;65(4):
1375–80. [MEDLINE: 15086477]
Mann JF, Yi QL, Sleight P, Dagenais GR, Gerstein HC,
Lonn EM, et al.Serum potassium, cardiovascular risk, and
effects of an ACE inhibitor: results of the HOPE study.
Clinical Nephrology 2005;63(3):181–7. [MEDLINE:
15786818]
Mathew J, Sleight P, Lonn E, Johnstone D, Pogue J, Yi
Q, et al.Reduction of cardiovascular risk by regression of
electrocardiographic markers of left ventricular hypertrophy
by the angiotensin-converting enzyme inhibitor ramipril.
Circulation 2001;104(14):1615–21. [MEDLINE:
16Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
11581138]
McQueen MJ, Lonn E, Gerstein HC, Bosch J, Yusuf S.
The HOPE (Heart Outcomes Prevention Evaluation) Study
and its consequences. Scandinavian Journal of Clinical and
Laboratory Investigation Supplement 2005;240:143–56.
[MEDLINE: 6112972]
Sleight P, Yusuf S, Pogue J, Tsuyuki R, Diaz R, Probstfield
J, et al.Blood-pressure reduction and cardiovascular
risk in HOPE study. Lancet 2001;358(9299):2130–1.
[MEDLINE: 11784631]
Smieja M, Gnarpe J, Lonn E, Gnarpe H, Olsson G, Yi Q, et
al.Multiple infections and subsequent cardiovascular events
in the Heart Outcomes Prevention Evaluation (HOPE)
Study. Circulation 2003;107(2):251–7. [MEDLINE:
12538424]
Veres A, Fust G, Smieja M, McQueen M, Horvath
A, Yi Q, et al.Relationship of anti-60 kDa heat shock
protein and anti-cholesterol antibodies to cardiovascular
events. Circulation 2002;106(22):2775–80. [MEDLINE:
12451002]
Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais
G. Effects of an angiotensin-converting-enzyme inhibitor,
ramipril, on cardiovascular events in high-risk patients. The
Heart Outcomes Prevention Evaluation Study Investigators.
New England Journal of Medicine 2000; Vol. 342, issue 3:
145–53. [MEDLINE: 10639539]
Joglekar 1998 {published data only}
Joglekar SJ, Nanivadekar AS. A randomized, controlled,
multicenter study to compare prazosin GITS with enalapril
in hypertensive patients with diabetes mellitus. Bombay
Hypertension Study Group. Journal of the Association of
Physicians of India 1998;Suppl 1:52–62. [MEDLINE:
11233387]
Kavgaci 2002 {published data only}
Kavgaci H, Sahin A, Onder EH, Erem C, Ozdemir F.
The effects of losartan and fosinopril in hypertensive type
2 diabetic patients. Diabetes Research & Clinical Practice
2002;58(1):19–25. [MEDLINE: 12161053]
Kvetny 2001 {published data only}
Kvetny J, Gregersen G, Smith Pedersen R. Randomized
placebo-controlled trial of perindopril in normotensive,
normoalbuminuric patients with type 1 diabetes mellitus.
Qjm 2001;94(2):89–94. [MEDLINE: 11181984]
Lin 1995 {published data only}
Lin M, Yang YF, Chiang HT, Lee D, Wang SP, Chang MS,
et al.Beneficial effects of angiotensin-converting enzyme
inhibitors on cardiovascular and renal functions in patients
with hypertension and diabetes. Acta Cardiologica Sinica
1995;11(1):30–8. [EMBASE: 1995122137]
ONTARGET Study 2008 {published data only}
Barzilay JI, Gao P, O’Donnell M, Mann JF, Anderson
C, Fagard R, et al.Albuminuria and decline in cognitive
function: The ONTARGET/TRANSCEND studies.
Archives of Internal Medicine 2011;171(2):142–50.
[MEDLINE: 21263104]
Cukierman-Yaffe T, Gerstein HC, Anderson C, Zhao
F, Sleight P, Hilbrich L, et al.Glucose intolerance and
diabetes as risk factors for cognitive impairment in people
at high cardiovascular risk: results from the ONTARGET/
TRANSCEND research programme. Diabetes Research &
Clinical Practice 2009 Mar;83(3):387–93. [MEDLINE:
19157618]
Gallieni M, Cozzolino M, Brancaccio D, Giovannini M.
Renal outcomes in the ONTARGET study. Lancet 2008;
372(9655):2019–21. [MEDLINE: 19070732]
Mancia G, Schumacher H, Redon J, Verdecchia P,
Schmieder R, Jennings G, et al.Blood pressure targets
recommended by guidelines and incidence of cardiovascular
and renal events in the Ongoing Telmisartan Alone and
in Combination With Ramipril Global Endpoint Trial
(ONTARGET). Circulation 2011;124(16):1727–36.
[MEDLINE: 21947289]∗ Mann JF, Schmieder RE, McQueen M, Dyal L,
Schumacher H, Pogue J, et al.Renal outcomes with
telmisartan, ramipril, or both, in people at high vascular
risk (the ONTARGET study): a multicentre, randomised,
double-blind, controlled trial. Lancet 2008;372(9638):
547–53. [MEDLINE: 18707986]
Mann JF, Schmieder RE, McQueen MM, Dyal L,
Schumacher H, Pogue J, et al.Renal outcomes with
telmisartan, ramipril, or both in people at high vascular risk:
results from the ONTARGET trial [abstract]. Journal of the
American Society of Nephrology 2008;17(Abstracts Issue):
48A.
Mann JF, Schmieder RE, McQueen MM, Dyal L,
Schumacher H, Pogue J, et al.Renal outcomes with
telmisartan, ramipril, or both in people at high vascular risk:
results from the ONTARGET trial [abstract]. Journal of the
American Society of Nephrology 2008;19(Abstracts Issue):
48A.
Narayanan RM, Chi LS, Choo LL, Ying YL, Fang SC.
Renal outcomes in the ONTARGET study. Lancet 2008;
372(9655):2020–1. [MEDLINE: 19070735]
Nonoguchi H, Nanami M, Hasuike Y, Kuragano T,
Nakanishi T. Renal outcomes in the ONTARGET study.
Lancet 2008;372(9655):2019–20. [MEDLINE: 19070731]
ONTARGET Investigators, Yusuf S, Teo KK, Pogue J, Dyal
L, Copland I, et al.Telmisartan, ramipril, or both in patients
at high risk for vascular events. New England Journal of
Medicine 2008;358(15):1547–59. [MEDLINE: 8378520]
Ruilope LM, Redon J, Schmieder R. Cardiovascular risk
reduction by reversing endothelial dysfunction: ARBs, ACE
inhibitors, or both? Expectations from the ONTARGET
Trial Programme. Vascular Health & Risk Management
2007;3(1):1–9. [MEDLINE: 17583170]
Schmieder RE, Mann JFE, Dyal L, Pogue J, Copland I,
Teo KK, et al.ONTARGET: cardiovascular outcome in
patients at high cardiovascular risk and with chronic kidney
disease (CKD) [abstract]. Journal of the American Society of
Nephrology 2008;19(Abstracts Issue):309A.
Sleight P. Clinical evidence from ONTARGET: the value
of an angiotensin II receptor blocker and an angiotensin-
converting enzyme inhibitor. Journal of Hypertension
- Supplement 2009;27(Suppl 5):S23–9. [MEDLINE:
17Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
19587551]
Sleight P, Redon J, Verdecchia P, Mancia G, Gao P, Fagard
R, et al.Prognostic value of blood pressure in patients with
high vascular risk in the Ongoing Telmisartan Alone and in
combination with Ramipril Global Endpoint Trial study.
Journal of Hypertension 2009;27(7):1360–9. [MEDLINE:
19506526]
Teo K, Yusuf S, Sleight P, Anderson C, Mookadam F, Ramos
B, et al.Rationale, design, and baseline characteristics of
2 large, simple, randomized trials evaluating telmisartan,
ramipril, and their combination in high-risk patients: the
Ongoing Telmisartan Alone and in Combination with
Ramipril Global Endpoint Trial/Telmisartan Randomized
Assessment Study in ACE Intolerant Subjects with
Cardiovascular Disease (ONTARGET/TRANSCEND)
trials. American Heart Journal 2004;148(1):52–61.
[MEDLINE: 15215792]
Wetzels JF. Renal outcomes in the ONTARGET study.
Lancet 2008;372(9655):2020–1. [MEDLINE: 19070734]
Perrin 2008 {published data only}
Perrin NE, Jaremko GA, Berg UB. The effect of candesartan/
placebo treatment on renal function and morphology in
diabetes type 1 [abstract]. Journal of the American Society of
Nephrology 2007;18(Abstracts):327A.∗ Perrin NE, Jaremko GA, Berg UB. The effects of
candesartan on diabetes glomerulopathy: a double-blind,
placebo-controlled trial. Pediatric Nephrology 2008;23(6):
947–54. [MEDLINE: 18270751]
RASS Study 2002 {published and unpublished data}
Donnelly S, Goodyear P, Ly J, Klein R, Moss S, Sinsiko A, et
al.Renal biopsy complications in the RASS study [abstract].
Journal of the American Society of Nephrology 2005;16:559A.
Donnelly S, Sinaiko A, Strand T, Zinman B, Drummond
K, Gardiner R, et al.Effects of renin angiotensin system
(RAS) blockade on diabetic nephropathy (DN)-a primary
prevention trial: study design and baseline results [abstract].
Journal of the American Society of Nephrology 2002;13
(Program & Abstracts):651A.
Katavetin P, Katavetin P. Renal and retinal effects of enalapril
and losartan in type 1 diabetes. New England Journal of
Medicine 2009;361(14):1410–1. [MEDLINE: 19802919]
Mauer M, Strand T, Zinman B, Gardiner R, Suissa S,
Sinaiko A, et al.The Renin Angiotensin System Study
(RASS): compliance in a long-term kidney biopsy based
diabetic nephropathy (DN) primary prevention trial in
Type 1 diabetes mellitus (T1DM) patients (pts) [abstract].
Journal of the American Society of Nephrology 2005;16:554A.
Mauer M, Zinman B, Gardiner R, Drummond KN, Suissa
S, Donnelly SM, et al.ACE-I and ARBs in early diabetic
nephropathy. Journal of the Renin-Angiotensin-Aldosterone
System 2002;3(4):262–9. [MEDLINE: 12584670]∗ Mauer M, Zinman B, Gardiner R, Suissa S, Sinaiko A,
Strand T, et al.Renal and retinal effects of enalapril and
losartan in type 1 diabetes. New England Journal of Medicine
2009;361(1):40–51. [MEDLINE: 19571282]
Robiner WN, Yozwiak JA, Bearman DL, Strand TD,
Strasburg KR. Barriers to clinical research participation in a
diabetes randomized clinical trial. Social Science & Medicine
2009;68(6):1069–74. [MEDLINE: 19167143]
Suissa S. Renin angiotensin system study (RASS) of diabetic
nephropathy. (study protocol).
Tamsma JT. Renal and retinal effects of enalapril and
losartan in type 1 diabetes. New England Journal of Medicine
2009;361(14):1410. [MEDLINE: 19797291]
Ravid 1998 {published data only}
Ravid M, Brosh D, Levi Z, Bar-Dayan Y, Ravid D,
Rachmani R. Use of enalapril to attenuate decline in renal
function in normotensive, normoalbuminuric patients with
type 2 diabetes mellitus: a randomized, controlled trial.
Annals of Internal Medicine 1998;128(12 Pt 1):982–8.
[MEDLINE: 9625684]
ROADMAP Study 2009 {published data only}∗ Haller H, Ito S, Izzo JL, Januszewicz A, Katayama S,
Menne J, et al.Olmesartan for the delay or prevention
of microalbuminuria in type 2 diabetes. New England
Journal of Medicine 2011;364(10):907–17. [MEDLINE:
21388309]
Haller H, Viberti GC, Mimran A, Remuzzi G, Rabelink
AJ, Ritz E, et al.Preventing microalbuminuria in patients
with diabetes: rationale and design of the Randomised
Olmesartan and Diabetes Microalbuminuria Prevention
(ROADMAP) study. Journal of Hypertension 2006;24(2):
403–8. [MEDLINE: 16508590]
Haller HG, Viberti GV, Ritz E, Ruilope LM, Rabelink
TJ, for the ROADMAP Steering Committee Members.
Prevention of albuminuria and cardiovascular morbidity
with olmesartan, the ROADMAP trial. ASN Renal Week.
2009:LB–005.
Januszewicz A, Ritz E, Viberti G, Mimran A, Rabelink
AJ, Rump LC, et al.Office and ambulatory pulse
pressure--association with clinical characteristics and
cardiovascular risk factors in normoalbuminuric patients
with type 2 diabetes (ROADMAP study). Journal of
Human Hypertension 2011;25(11):679–85. [MEDLINE:
21150933]
Menne J, Izzo JL Jr, Ito S, Januszewicz A, Katayama S,
Chatzykirkou C, et al.Prevention of microalbuminuria in
patients with type 2 diabetes and hypertension. Journal of
Hypertension 2012;30(4):811–8. [MEDLINE: 22418908]
Ritz E, Viberti GC, Ruilope LM, Rabelink AJ, Izzo JL
Jr, Katayama S, et al.Determinants of urinary albumin
excretion within the normal range in patients with type
2 diabetes: the Randomised Olmesartan and Diabetes
Microalbuminuria Prevention (ROADMAP) study.
Diabetologia 2010;53(1):49–57. [MEDLINE: 19876613]
Scognamiglio 1997 {published data only}
Scognamiglio R, Nosadini R, Marin M, Nisti S, Fasoli G,
Palisi M, et al.Evaluation of the efficacy and tolerability of
nitrendipine in reducing both pressure and left ventricular
mass in hypertensive type 2 diabetic patients. Diabetes Care
1997;20(8):1290–2. [MEDLINE: 9250456]
TRANSCEND Study 2009 {published data only}
Barzilay JI, Gao P, O’Donnell M, Mann JF, Anderson
C, Fagard R, et al.Albuminuria and decline in cognitive
18Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
function: The ONTARGET/TRANSCEND studies.
Archives of Internal Medicine 2011;171(2):142–50.
[MEDLINE: 21263104]
Cukierman-Yaffe T, Gerstein HC, Anderson C, Zhao
F, Sleight P, Hilbrich L, et al.Glucose intolerance and
diabetes as risk factors for cognitive impairment in people
at high cardiovascular risk: results from the ONTARGET/
TRANSCEND research programme. Diabetes Research
& Clinical Practice 2009;83(3):387–93. [MEDLINE:
19157618]
Held C, Gerstein HC, Yusuf S, Zhao F, Hilbrich L,
Anderson C, et al.Glucose levels predict hospitalization for
congestive heart failure in patients at high cardiovascular
risk. Circulation 2007;115(11):1371–5. [MEDLINE:
17339550]∗ Mann JF, Schmieder RE, Dyal L, McQueen MJ,
Schumacher H, Pogue J, et al.Effect of telmisartan on renal
outcomes: a randomized trial. Annals of Internal Medicine
2009;151(1):1–10. [MEDLINE: 19451556]
Telmisartan Randomised AssessmeNt Study in ACE
iNtolerant subjects with cardiovascular Disease
(TRANSCEND) Investigators. Yusuf S. Teo K. Anderson
C. Pogue J. Dyal L, et al.Effects of the angiotensin-receptor
blocker telmisartan on cardiovascular events in high-
risk patients intolerant to angiotensin-converting enzyme
inhibitors: a randomised controlled trial. Lancet 2008;372
(9644):1174–83. [MEDLINE: 18757085]
Teo K, Yusuf S, Sleight P, Anderson C, Mookadam F, Ramos
B, et al.Rationale, design, and baseline characteristics of
2 large, simple, randomized trials evaluating telmisartan,
ramipril, and their combination in high-risk patients: the
Ongoing Telmisartan Alone and in Combination with
Ramipril Global Endpoint Trial/Telmisartan Randomized
Assessment Study in ACE Intolerant Subjects with
Cardiovascular Disease (ONTARGET/TRANSCEND)
trials. American Heart Journal 2004;148(1):52–61.
[MEDLINE: 15215792]
Tuominen 1998 {published data only}
Tuominen JA, Ebeling P, Koivisto VA. Long-term
lisinopril therapy reduces exercise-induced albuminuria in
normoalbuminuric normotensive IDDM patients. Diabetes
Care 1998;21(8):1345–8. [MEDLINE: 9702445]
UKPDS Study 1998 {published data only}
Anonymous. UK Prospective Diabetes Study (UKPDS).
VIII. Study design, progress and performance. Diabetologia
1991;34(12):877–90. [MEDLINE: 1778353]∗ Holman R, Turner R, Stratton I, Cull C, Frighi V, Manley
S, et al.Efficacy of atenolol and captopril in reducing risk
of macrovascular and microvascular complications in type
2 diabetes: UKPDS 39. UK Prospective Diabetes Study
Group. BMJ 1998;317(7160):713–20. [MEDLINE:
9732338]
UK PDS Group. Intensive blood-glucose control with
sulphonylureas or insulin compared with conventional
treatment and risk of complications in patients with
type 2 diabetes (UKPDS 33). UK Prospective Diabetes
Study (UKPDS) Group. Lancet 1998;352(9131):837–53.
[MEDLINE: 9742976]
UK PDS Group. Tight blood pressure control and risk
of macrovascular and microvascular complications in type
2 diabetes: UKPDS 38. UK Prospective Diabetes Study
Group. BMJ 1998;317(7160):703–13. [MEDLINE:
9732337]
Velussi 1996 {published data only}
Velussi M, Brocco E, Frigato F, Zolli M, Muollo B, Maioli
M, et al.Effects of cilazapril and amlodipine on kidney
function in hypertensive NIDDM patients. Diabetes 1996;
45(2):216–22. [MEDLINE: 8549868]
References to studies excluded from this review
ALLHAT 2002 {published data only}
ALLHAT Officers and Coordinators for the ALLHAT
Collaborative Research Group. The Antihypertensive
and Lipid-Lowering Treatment to Prevent Heart Attack
Trial. Major outcomes in high-risk hypertensive patients
randomized to angiotensin-converting enzyme inhibitor or
calcium channel blocker vs diuretic: The Antihypertensive
and Lipid-Lowering Treatment to Prevent Heart Attack Trial
(ALLHAT). JAMA 2002;288(23):2981–97. [MEDLINE:
12479763]
Messerli HF. Implications of discontinuation of doxazosin
arm of ALLHAT. Antihypertensive and Lipid-Lowering
Treatment to Prevent Heart Attack Trial. Lancet 2000;355
(9207):863–4. [MEDLINE: 10752699]
CAPPP 1999 {published data only}
Hansson L, Lindholm LH, Niskanen L, Lanke J, Hedner
T, Niklason A, et al.Effect of angiotensin-converting-
enzyme inhibition compared with conventional therapy on
cardiovascular morbidity and mortality in hypertension: the
Captopril Prevention Project (CAPPP) randomised trial.
Lancet 1999;353(9153):611–6. [MEDLINE: 10030325]
Hansson 1999 {published data only}
Hansson L, Lindholm LH, Ekbom T, Dahlof B, Lanke
J, Schersten B, et al.Randomised trial of old and new
antihypertensive drugs in elderly patients: cardiovascular
mortality and morbidity the Swedish Trial in Old Patients
with Hypertension-2 study. Lancet 1999;354(9192):
1751–6. [MEDLINE: 10577635]
HOT 1998 {published data only}
Hansson L, Zanchetti A, Carruthers SG, Dahlof B, Elmfeldt
D, Julius S, et al.Effects of intensive blood-pressure lowering
and low-dose aspirin in patients with hypertension:
principal results of the Hypertension Optimal Treatment
(HOT) randomised trial. Lancet 1998;351(9118):1755–62.
[MEDLINE: 9635947]
INSIGHT 2000 {published data only}
Brown MJ, Palmer CR, Castaigne A, de Leeuw PW,
Mancia G, Rosenthal T, et al.Morbidity and mortality
in patients randomised to double-blind treatment with
a long-acting calcium-channel blocker or diuretic in the
International Nifedipine GITS study: Intervention as a
Goal in Hypertension Treatment (INSIGHT). Lancet 2000;
356(9227):366–72. [MEDLINE: 10972368]
19Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
NORDIL 2000 {published data only}
Hansson L, Hedner T, Lund-Johansen P, Kjeldsen SE,
Lindholm LH, Syvertsen JO, et al.Randomised trial of
effects of calcium antagonists compared with diuretics and
beta-blockers on cardiovascular morbidity and mortality
in hypertension: the Nordic Diltiazem (NORDIL) study.
Lancet 2000;356(9227):359–65. [MEDLINE: 10972367]
Tuomilehto 1999 {published data only}
Tuomilehto J, Rastenyte D, Birkenhager WH, Thijs L,
Antikainen R, Bulpitt CJ, et al.Effects of calcium-channel
blockade in older patients with diabetes and systolic
hypertension. Systolic Hypertension in Europe Trial
Investigators. New England Journal of Medicine 1999;340
(9):677–84. [MEDLINE: 10053176]
Additional references
ADA 2010
American Diabetes Association. Standards of Medical Care
in Diabetes-2010. Diabetes Care 2010;33(Suppl 1):S11–61.
[MEDLINE: 14693929]
Adler 2003
Adler AI, Stevens RJ, Manley SE, Bilous RW, Cull CA,
Holman RR. Development and progression of nephropathy
in type 2 diabetes: The United Kingdom Prospective
Diabetes Study (UKPDS 64). Kidney International 2003;63
(1):225–32. [MEDLINE: 12472787]
Bucher 1997
Bucher HC, Guyatt GH, Griffith LE, Walter SD. The
results of direct and indirect treatment comparisons in meta-
analysis of randomized controlled trials. Journal of Clinical
Epidemiology 1997;50(6):683–91. [MEDLINE: 9250266]
CDA 2008
Canadian Diabetes Association Clinical Practice Guidelines
Expert Committee. Canadian Diabetes Association
2008 clinical practice guidelines for the prevention and
management of diabetes in Canada. Canadian Journal of
Diabetes 2008; Vol. 32, issue Suppl 1:S1–S201.
Chadban 2010
Chadban S, Howell M, Twigg S, Thomas M, Jerums G,
Cass A, et al.Prevention and management of chronic kidney
disease in type 2 diabetes. Nephrology 2010;15:S162–94.
[DOI: 10.1111/j.1440-1797.2010.01240.x]
Chaturvedi 2008
Chaturvedi N, Porta M, Klein R, Orchard T, Fuller J,
Parving HH, et al.Effect of candesartan on prevention
(DIRECT-Prevent 1) and progression (DIRECT-Protect
1) of retinopathy in type 1 diabetes: randomised, placebo-
controlled trials. Lancet 2008;372(9647):1394–402.
[MEDLINE: 18823656]
Chobanian 2003
Chobanian AV, Bakris GL, Black HR, Cushman WC,
Green LA, Izzo JL Jr, et al.The Seventh Report of the Joint
National Committee on Prevention, Detection, Evaluation,
and Treatment of High Blood Pressure: the JNC 7 report.
JAMA 2003;289(19):2560–72. [MEDLINE: 12748199]
ESH-ESC 2007
Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard
R, Germano G, et al.2007 ESH-ESC Practice Guidelines
for the Management of Arterial Hypertension: ESH-ESC
Task Force on the Management of Arterial Hypertension.
Journal of Hypertension 2007;25(9):1751–62. [MEDLINE:
17762635]
Gerstein 2001
Gerstein HC, Mann JF, Yi Q, Zinman B, Dinneen SF,
Hoogwerf B, et al.Albuminuria and risk of cardiovascular
events, death, and heart failure in diabetic and nondiabetic
individuals. JAMA 2001;286(4):421–6. [MEDLINE:
11466120]
Hasslacher 1985
Hasslacher C, Ritz E, Terpstra J, Gallasch G, Kunowski G,
Rall C. Natural history of nephropathy in type I diabetes.
Relationship to metabolic control and blood pressure.
Hypertension 1985;7(6 Pt 2):74–8. [MEDLINE: 4077240]
Higgins 2003
Higgins JP, Thompson SG, Deeks JJ, Altman DG.
Measuring inconsistency in meta-analyses. BMJ 2003;327
(7414):557–60. [MEDLINE: 12958120]
Higgins 2011
Higgins JPT, Green S (editors). Cochrane Handbook
for Systematic Reviews of Interventions Version 5.1.0
[updated March 2011]. The Cochrane Collaboration,
2011. Available from www.cochrane-handbook.org.
IDF 2009
International Diabetes Federation. IDF Diabetes Atlas.
http://www.idf.org/diabetesatlas/ (accessed 26 September
2012).
KDOQI 2007
American Kidney Foundation. KDOQI clinical practice
guidelines and clinical practice recommendations for
diabetes and chronic kidney disease. http://www.kidney.org/
professionals/KDOQI/guideline˙diabetes/guide3.htm
(accessed 26 September 2012).
Klausen 2004
Klausen K, Borch-Johnsen K, Feldt-Rasmussen B, Jensen
G, Clausen P, Scharling H, et al.Very low levels of
microalbuminuria are associated with increased risk of
coronary heart disease and death independently of renal
function, hypertension, and diabetes. Circulation 2004;110
(1):32–5. [MEDLINE: 15210602]
Levey 2009
Levey AS, Cattran D, Friedman A, Miller WG, Sedor
J, Tuttle K, et al.Proteinuria as a surrogate outcome in
CKD: report of a scientific workshop sponsored by the
National Kidney Foundation and the US Food and Drug
Administration. American Journal of Kidney Diseases 2009;
54(2):205–26. [MEDLINE: 19577347]
Messent 1992
Messent JW, Elliott TG, Hill RD, Jarrett RJ, Keen H,
Viberti GC. Prognostic significance of microalbuminuria
in insulin-dependent diabetes mellitus: a twenty-three year
20Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
follow-up study. Kidney International 1992;41(4):836–9.
[MEDLINE: 1513106]
Mogensen 1976
Mogensen CE. Progression of nephropathy in long-
term diabetics with proteinuria and effect of initial anti-
hypertensive treatment. Scandinavian Journal of Clinical &
Laboratory Investigation 1976;36(4):383–8. [MEDLINE:
959756]
Ninomiya 2009
Ninomiya T, Perkovic V, de Galan BE, Zoungas S, Pillai
A, Jardine M, et al.Albuminuria and kidney function
independently predict cardiovascular and renal outcomes in
diabetes. Journal of the American Society of Nephrology 2009;
20(8):1813–21. [MEDLINE: 19443635]
Parfrey 2009
Parfrey PS. Angiotensin-receptor blockers in the prevention
or treatment of microalbuminuria. Annals of Internal
Medicine 2009;151(1):63–5. [MEDLINE: 19581647]
Perkovic 2008
Perkovic V, Verdon C, Ninomiya T, Barzi F, Cass A, Patel
A, et al.The relationship between proteinuria and coronary
risk: a systematic review and meta-analysis. PLoS Medicine
/ Public Library of Science 2008;5(10):e207. [MEDLINE:
18942886]
Ritz 1999
Ritz E, Orth SR. Nephropathy in patients with type 2
diabetes mellitus. New England Journal of Medicine 1999;
341(15):1127–33. [MEDLINE: 10511612]
Ruggenenti 1997
Ruggenenti P, Remuzzi G. The diagnosis of renal
involvement in non-insulin-dependent diabetes mellitus.
Current Opinion in Nephrology & Hypertension 1997;6(2):
141–5. [MEDLINE: 9146975]
Sjølie 2008
Sjølie AK, Klein R, Porta M, Orchard T, Fuller J, Parving
HH, et al.Effect of candesartan on progression and
regression of retinopathy in type 2 diabetes (DIRECT-
Protect 2): a randomised placebo-controlled trial. Lancet
2008;372(9647):1385–93. [MEDLINE: 18823658]
Song 2000
Song F, Glenny AM, Altman DG. Indirect comparison
in evaluating relative efficacy illustrated by antimicrobial
prophylaxis in colorectal surgery. Controlled Clinical Trials
2000;21(5):488–97. [MEDLINE: 11018565]
Strippoli 2004
Strippoli GF, Craig M, Deeks JJ, Schena FP, Craig JC.
Effects of angiotensin converting enzyme inhibitors and
angiotensin II receptor antagonists on mortality and renal
outcomes in diabetic nephropathy: systematic review. BMJ
2004;329(7370):828–31. [MEDLINE: 15459003]
USRDS 2009
U S Renal Data System. USRDS 2009 Annual Data Report:
Atlas of Chronic Kidney Disease and End-Stage Renal
Disease in the United States, National Institutes of Health,
National Institute of Diabetes and Digestive and Kidney
Diseases, Bethesda, MD, 2009. http://www.usrds.org/
atlas09.aspx (accessed 25 September 2012).
Williams 2004
Williams B, Poulter NR, Brown MJ, Davis M, McInnes
GT, Potter JF, et al.British Hypertension Society guidelines
for hypertension management 2004 (BHS-IV): summary.
BMJ 2004;328(7440):634–40. [MEDLINE: 15016698]
References to other published versions of this review
Strippoli 2003
Strippoli GFM, Craig M, Schena FP, Craig JC.
Antihypertensive agents for preventing diabetic kidney
disease. (Protocol). Cochrane Database of Systematic Reviews
2003, Issue 2. [DOI: 10.1002/14651858.CD004136]
Strippoli 2005
Strippoli GF, Craig M, Craig JC. Antihypertensive agents
for preventing diabetic kidney disease. Cochrane Database
of Systematic Reviews 2005, Issue 4. [DOI: 10.1002/
14651858.CD004136.pub2]∗ Indicates the major publication for the study
21Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
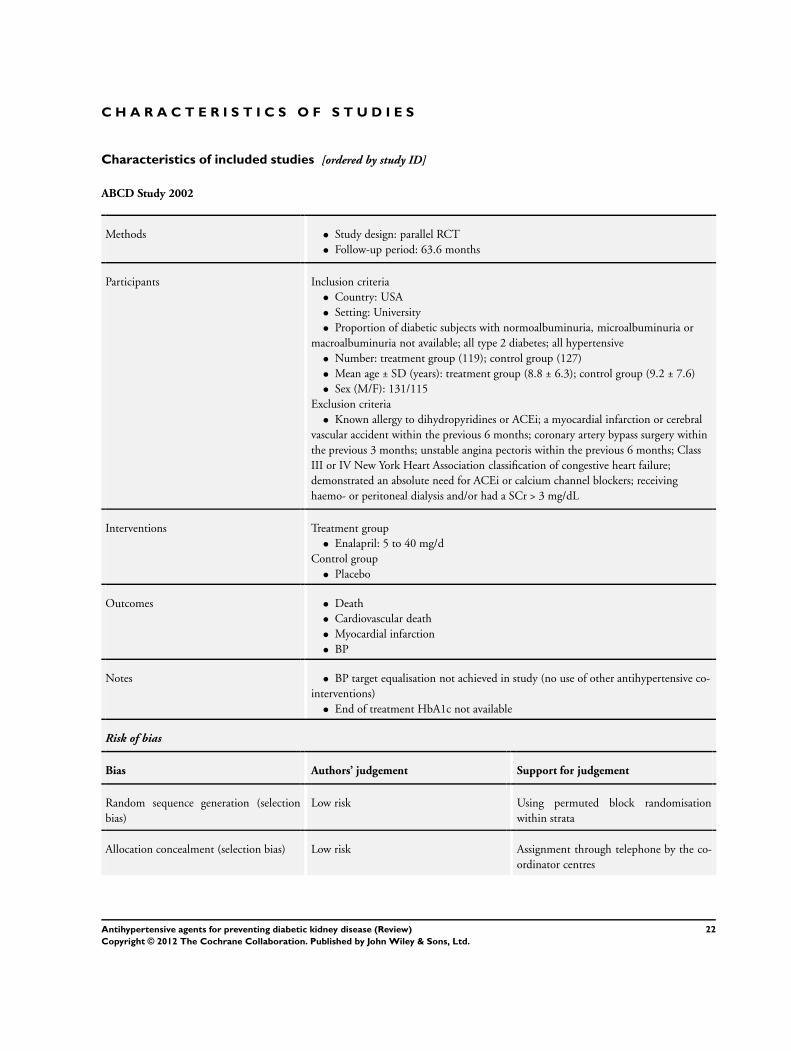
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
ABCD Study 2002
Methods • Study design: parallel RCT
• Follow-up period: 63.6 months
Participants Inclusion criteria
• Country: USA
• Setting: University
• Proportion of diabetic subjects with normoalbuminuria, microalbuminuria or
macroalbuminuria not available; all type 2 diabetes; all hypertensive
• Number: treatment group (119); control group (127)
• Mean age ± SD (years): treatment group (8.8 ± 6.3); control group (9.2 ± 7.6)
• Sex (M/F): 131/115
Exclusion criteria
• Known allergy to dihydropyridines or ACEi; a myocardial infarction or cerebral
vascular accident within the previous 6 months; coronary artery bypass surgery within
the previous 3 months; unstable angina pectoris within the previous 6 months; Class
III or IV New York Heart Association classification of congestive heart failure;
demonstrated an absolute need for ACEi or calcium channel blockers; receiving
haemo- or peritoneal dialysis and/or had a SCr > 3 mg/dL
Interventions Treatment group
• Enalapril: 5 to 40 mg/d
Control group
• Placebo
Outcomes • Death
• Cardiovascular death
• Myocardial infarction
• BP
Notes • BP target equalisation not achieved in study (no use of other antihypertensive co-
interventions)
• End of treatment HbA1c not available
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Using permuted block randomisation
within strata
Allocation concealment (selection bias) Low risk Assignment through telephone by the co-
ordinator centres
22Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
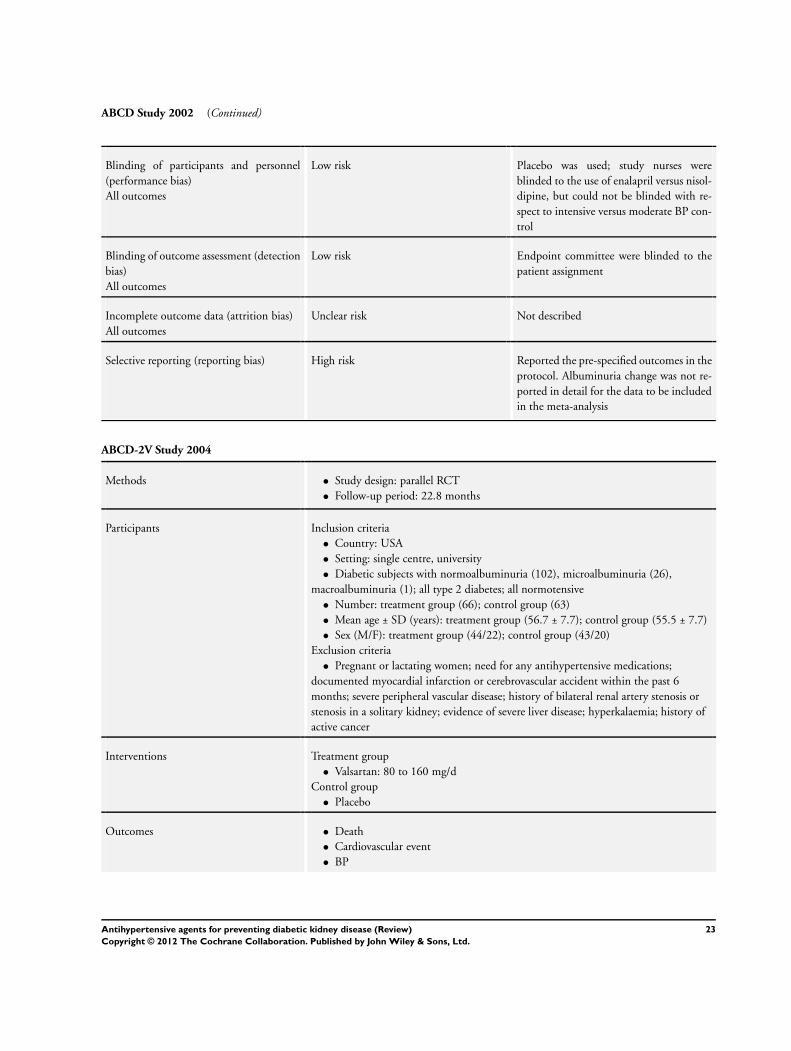
ABCD Study 2002 (Continued)
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Placebo was used; study nurses were
blinded to the use of enalapril versus nisol-
dipine, but could not be blinded with re-
spect to intensive versus moderate BP con-
trol
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Endpoint committee were blinded to the
patient assignment
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Not described
Selective reporting (reporting bias) High risk Reported the pre-specified outcomes in the
protocol. Albuminuria change was not re-
ported in detail for the data to be included
in the meta-analysis
ABCD-2V Study 2004
Methods • Study design: parallel RCT
• Follow-up period: 22.8 months
Participants Inclusion criteria
• Country: USA
• Setting: single centre, university
• Diabetic subjects with normoalbuminuria (102), microalbuminuria (26),
macroalbuminuria (1); all type 2 diabetes; all normotensive
• Number: treatment group (66); control group (63)
• Mean age ± SD (years): treatment group (56.7 ± 7.7); control group (55.5 ± 7.7)
• Sex (M/F): treatment group (44/22); control group (43/20)
Exclusion criteria
• Pregnant or lactating women; need for any antihypertensive medications;
documented myocardial infarction or cerebrovascular accident within the past 6
months; severe peripheral vascular disease; history of bilateral renal artery stenosis or
stenosis in a solitary kidney; evidence of severe liver disease; hyperkalaemia; history of
active cancer
Interventions Treatment group
• Valsartan: 80 to 160 mg/d
Control group
• Placebo
Outcomes • Death
• Cardiovascular event
• BP
23Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
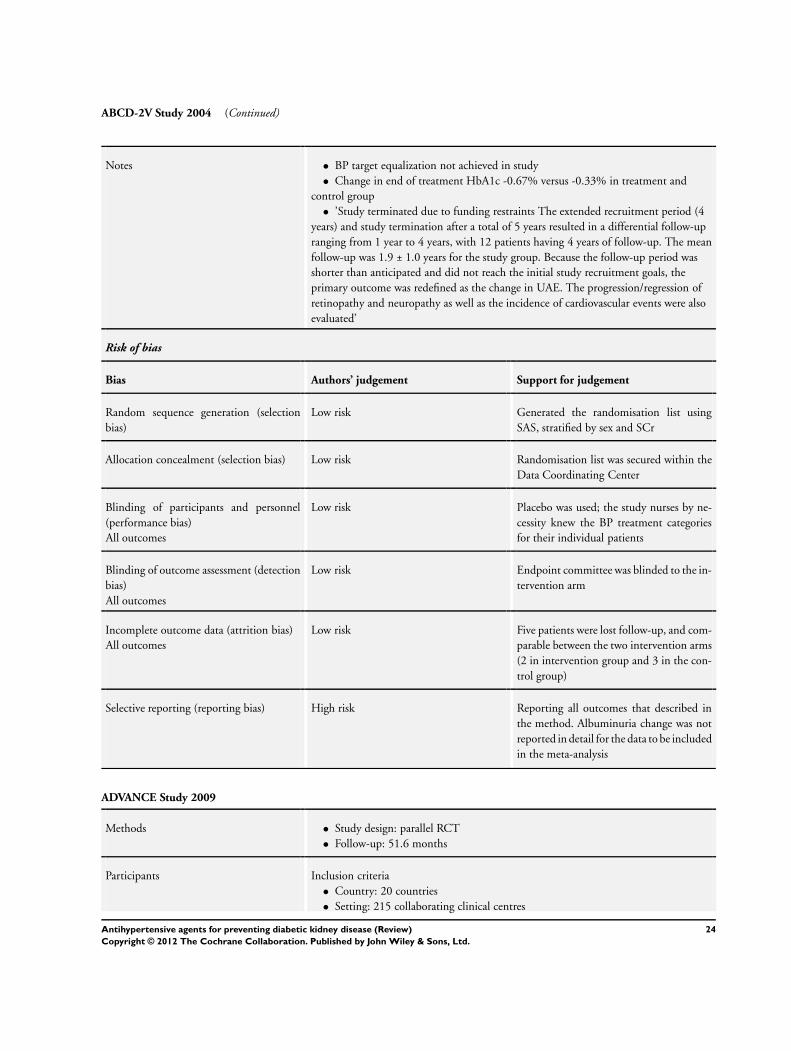
ABCD-2V Study 2004 (Continued)
Notes • BP target equalization not achieved in study
• Change in end of treatment HbA1c -0.67% versus -0.33% in treatment and
control group
• ’Study terminated due to funding restraints The extended recruitment period (4
years) and study termination after a total of 5 years resulted in a differential follow-up
ranging from 1 year to 4 years, with 12 patients having 4 years of follow-up. The mean
follow-up was 1.9 ± 1.0 years for the study group. Because the follow-up period was
shorter than anticipated and did not reach the initial study recruitment goals, the
primary outcome was redefined as the change in UAE. The progression/regression of
retinopathy and neuropathy as well as the incidence of cardiovascular events were also
evaluated’
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Generated the randomisation list using
SAS, stratified by sex and SCr
Allocation concealment (selection bias) Low risk Randomisation list was secured within the
Data Coordinating Center
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Placebo was used; the study nurses by ne-
cessity knew the BP treatment categories
for their individual patients
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Endpoint committee was blinded to the in-
tervention arm
Incomplete outcome data (attrition bias)
All outcomes
Low risk Five patients were lost follow-up, and com-
parable between the two intervention arms
(2 in intervention group and 3 in the con-
trol group)
Selective reporting (reporting bias) High risk Reporting all outcomes that described in
the method. Albuminuria change was not
reported in detail for the data to be included
in the meta-analysis
ADVANCE Study 2009
Methods • Study design: parallel RCT
• Follow-up: 51.6 months
Participants Inclusion criteria
• Country: 20 countries
• Setting: 215 collaborating clinical centres
24Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
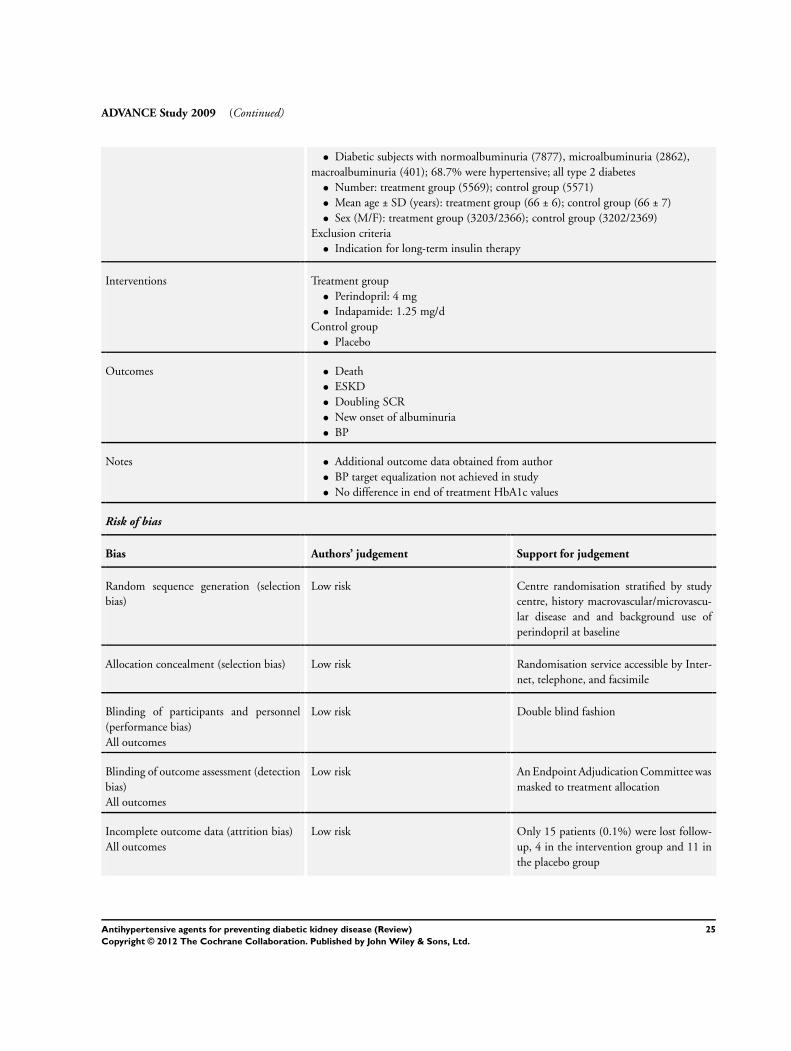
ADVANCE Study 2009 (Continued)
• Diabetic subjects with normoalbuminuria (7877), microalbuminuria (2862),
macroalbuminuria (401); 68.7% were hypertensive; all type 2 diabetes
• Number: treatment group (5569); control group (5571)
• Mean age ± SD (years): treatment group (66 ± 6); control group (66 ± 7)
• Sex (M/F): treatment group (3203/2366); control group (3202/2369)
Exclusion criteria
• Indication for long-term insulin therapy
Interventions Treatment group
• Perindopril: 4 mg
• Indapamide: 1.25 mg/d
Control group
• Placebo
Outcomes • Death
• ESKD
• Doubling SCR
• New onset of albuminuria
• BP
Notes • Additional outcome data obtained from author
• BP target equalization not achieved in study
• No difference in end of treatment HbA1c values
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Centre randomisation stratified by study
centre, history macrovascular/microvascu-
lar disease and and background use of
perindopril at baseline
Allocation concealment (selection bias) Low risk Randomisation service accessible by Inter-
net, telephone, and facsimile
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Double blind fashion
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk An Endpoint Adjudication Committee was
masked to treatment allocation
Incomplete outcome data (attrition bias)
All outcomes
Low risk Only 15 patients (0.1%) were lost follow-
up, 4 in the intervention group and 11 in
the placebo group
25Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
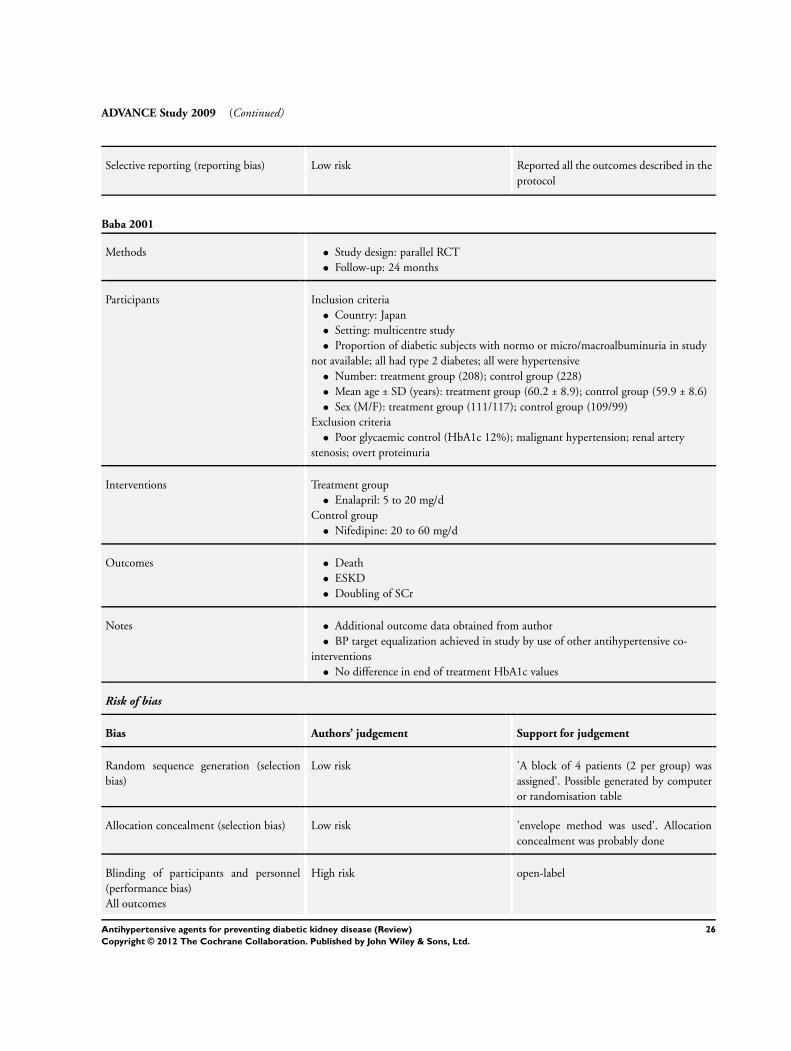
ADVANCE Study 2009 (Continued)
Selective reporting (reporting bias) Low risk Reported all the outcomes described in the
protocol
Baba 2001
Methods • Study design: parallel RCT
• Follow-up: 24 months
Participants Inclusion criteria
• Country: Japan
• Setting: multicentre study
• Proportion of diabetic subjects with normo or micro/macroalbuminuria in study
not available; all had type 2 diabetes; all were hypertensive
• Number: treatment group (208); control group (228)
• Mean age ± SD (years): treatment group (60.2 ± 8.9); control group (59.9 ± 8.6)
• Sex (M/F): treatment group (111/117); control group (109/99)
Exclusion criteria
• Poor glycaemic control (HbA1c 12%); malignant hypertension; renal artery
stenosis; overt proteinuria
Interventions Treatment group
• Enalapril: 5 to 20 mg/d
Control group
• Nifedipine: 20 to 60 mg/d
Outcomes • Death
• ESKD
• Doubling of SCr
Notes • Additional outcome data obtained from author
• BP target equalization achieved in study by use of other antihypertensive co-
interventions
• No difference in end of treatment HbA1c values
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk ’A block of 4 patients (2 per group) was
assigned’. Possible generated by computer
or randomisation table
Allocation concealment (selection bias) Low risk ’envelope method was used’. Allocation
concealment was probably done
Blinding of participants and personnel
(performance bias)
All outcomes
High risk open-label
26Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
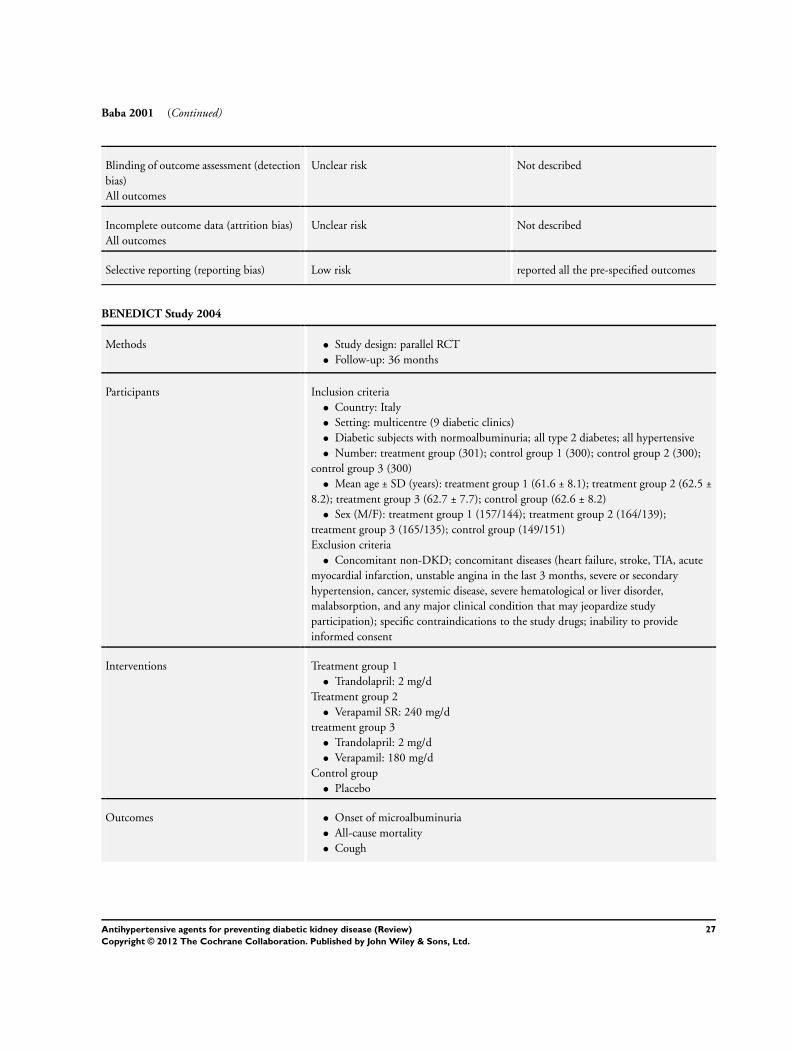
Baba 2001 (Continued)
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Not described
Selective reporting (reporting bias) Low risk reported all the pre-specified outcomes
BENEDICT Study 2004
Methods • Study design: parallel RCT
• Follow-up: 36 months
Participants Inclusion criteria
• Country: Italy
• Setting: multicentre (9 diabetic clinics)
• Diabetic subjects with normoalbuminuria; all type 2 diabetes; all hypertensive
• Number: treatment group (301); control group 1 (300); control group 2 (300);
control group 3 (300)
• Mean age ± SD (years): treatment group 1 (61.6 ± 8.1); treatment group 2 (62.5 ±
8.2); treatment group 3 (62.7 ± 7.7); control group (62.6 ± 8.2)
• Sex (M/F): treatment group 1 (157/144); treatment group 2 (164/139);
treatment group 3 (165/135); control group (149/151)
Exclusion criteria
• Concomitant non-DKD; concomitant diseases (heart failure, stroke, TIA, acute
myocardial infarction, unstable angina in the last 3 months, severe or secondary
hypertension, cancer, systemic disease, severe hematological or liver disorder,
malabsorption, and any major clinical condition that may jeopardize study
participation); specific contraindications to the study drugs; inability to provide
informed consent
Interventions Treatment group 1
• Trandolapril: 2 mg/d
Treatment group 2
• Verapamil SR: 240 mg/d
treatment group 3
• Trandolapril: 2 mg/d
• Verapamil: 180 mg/d
Control group
• Placebo
Outcomes • Onset of microalbuminuria
• All-cause mortality
• Cough
27Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
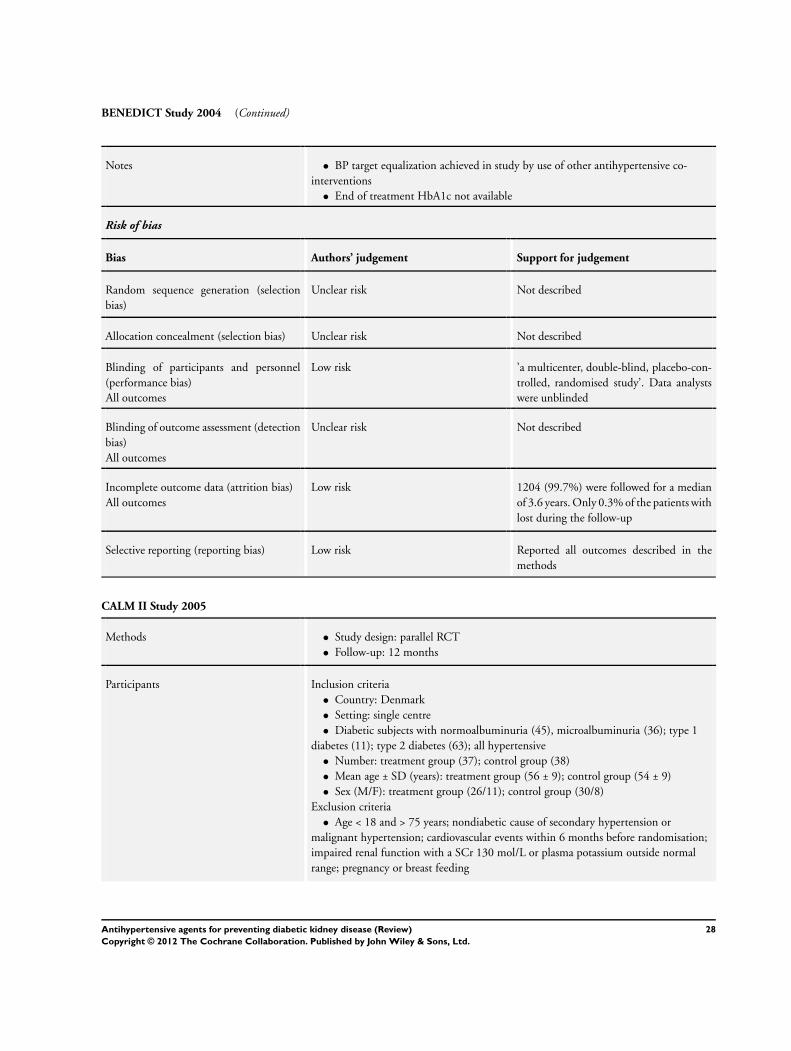
BENEDICT Study 2004 (Continued)
Notes • BP target equalization achieved in study by use of other antihypertensive co-
interventions
• End of treatment HbA1c not available
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not described
Allocation concealment (selection bias) Unclear risk Not described
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk ’a multicenter, double-blind, placebo-con-
trolled, randomised study’. Data analysts
were unblinded
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
Low risk 1204 (99.7%) were followed for a median
of 3.6 years. Only 0.3% of the patients with
lost during the follow-up
Selective reporting (reporting bias) Low risk Reported all outcomes described in the
methods
CALM II Study 2005
Methods • Study design: parallel RCT
• Follow-up: 12 months
Participants Inclusion criteria
• Country: Denmark
• Setting: single centre
• Diabetic subjects with normoalbuminuria (45), microalbuminuria (36); type 1
diabetes (11); type 2 diabetes (63); all hypertensive
• Number: treatment group (37); control group (38)
• Mean age ± SD (years): treatment group (56 ± 9); control group (54 ± 9)
• Sex (M/F): treatment group (26/11); control group (30/8)
Exclusion criteria
• Age < 18 and > 75 years; nondiabetic cause of secondary hypertension or
malignant hypertension; cardiovascular events within 6 months before randomisation;
impaired renal function with a SCr 130 mol/L or plasma potassium outside normal
range; pregnancy or breast feeding
28Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
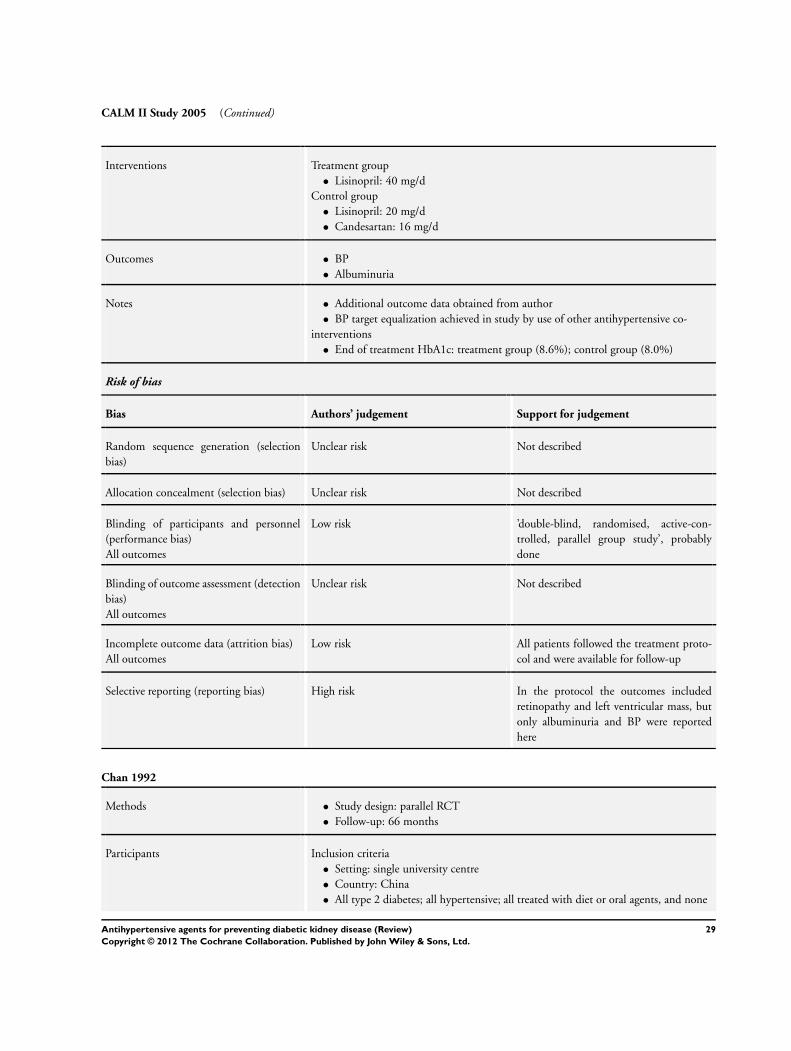
CALM II Study 2005 (Continued)
Interventions Treatment group
• Lisinopril: 40 mg/d
Control group
• Lisinopril: 20 mg/d
• Candesartan: 16 mg/d
Outcomes • BP
• Albuminuria
Notes • Additional outcome data obtained from author
• BP target equalization achieved in study by use of other antihypertensive co-
interventions
• End of treatment HbA1c: treatment group (8.6%); control group (8.0%)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not described
Allocation concealment (selection bias) Unclear risk Not described
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk ’double-blind, randomised, active-con-
trolled, parallel group study’, probably
done
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
Low risk All patients followed the treatment proto-
col and were available for follow-up
Selective reporting (reporting bias) High risk In the protocol the outcomes included
retinopathy and left ventricular mass, but
only albuminuria and BP were reported
here
Chan 1992
Methods • Study design: parallel RCT
• Follow-up: 66 months
Participants Inclusion criteria
• Setting: single university centre
• Country: China
• All type 2 diabetes; all hypertensive; all treated with diet or oral agents, and none
29Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Chan 1992 (Continued)
were receiving insulin treatment or lipid-lowering drugs at the time of recruitment
• Number: treatment group (50); control group (52)
◦ Normoalbuminuria: treatment group (20); control group (24)
◦ Microalbuminuria: treatment group (21); control group (15)
• Mean age ± SD (years): treatment group (60 ± 9.3); control group (56.2 ± 9.9)
• Sex (M/F): treatment group (20/30); control group (21/31)
Exclusion criteria
• Receiving insulin; history of non-DKD; SCr ≥ 200 mol/L; plasma potassium
concentration ≥ 5 mmol/L; cardiac failure; any concurrent systemic disease; receiving
treatment for any concomitant disorder
Interventions Treatment group
• Enalapril: 10-40 mg/d
Control group
• Nifedipine SF: 40-80 mg/d
Outcomes • Death
• BP
• Albuminuria
Notes • BP target equalisation achieved in study by use of other antihypertensive co-
interventions
• End of treatment HbA1c: treatment group (7.6%); control group (7.1%)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk ’according to a random allocation sched-
ule. A schedule of 102 allocation numbers
corresponding to similarly numbered drug
supplies was provided for this purpose.’ No
description of how random sequence was
produced
Allocation concealment (selection bias) Unclear risk No description of how allocation was per-
formed
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Patients blinded; blinding of investigators
not stated
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk “staff measuring BP and biochemical in-
dices were blinded to treatment.”
Incomplete outcome data (attrition bias)
All outcomes
Low risk Detailed description of the reasons of the 9
patients (8.8%) who did not finish follow-
up
30Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
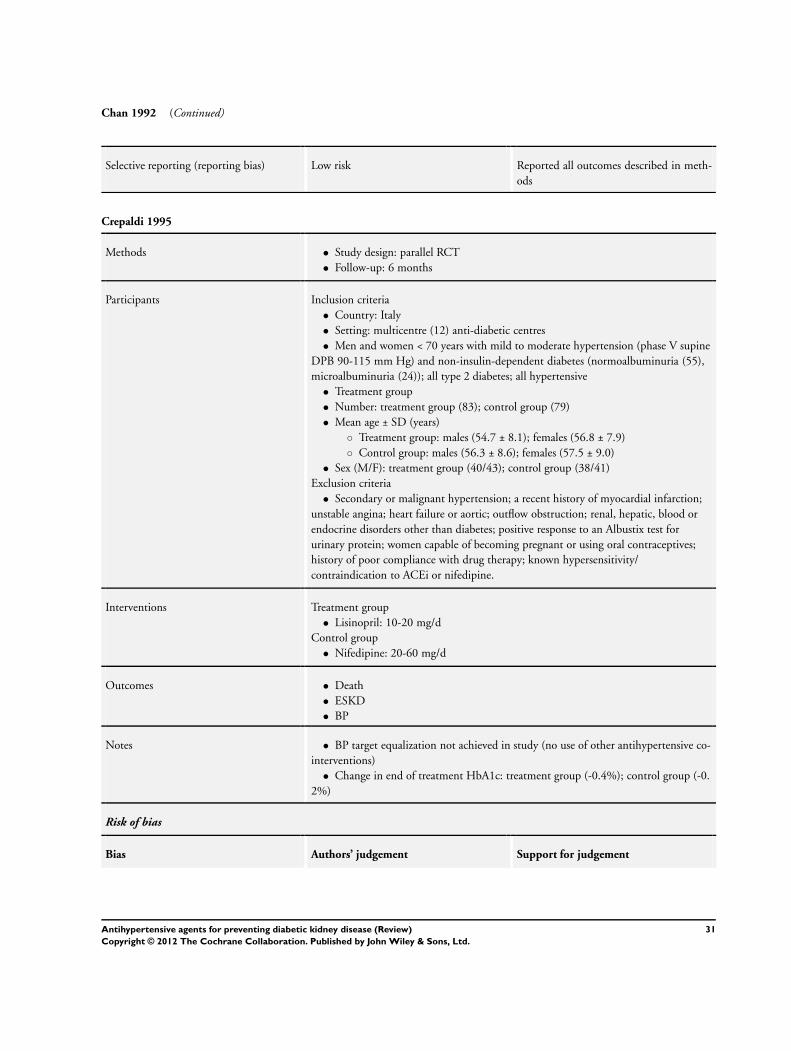
Chan 1992 (Continued)
Selective reporting (reporting bias) Low risk Reported all outcomes described in meth-
ods
Crepaldi 1995
Methods • Study design: parallel RCT
• Follow-up: 6 months
Participants Inclusion criteria
• Country: Italy
• Setting: multicentre (12) anti-diabetic centres
• Men and women < 70 years with mild to moderate hypertension (phase V supine
DPB 90-115 mm Hg) and non-insulin-dependent diabetes (normoalbuminuria (55),
microalbuminuria (24)); all type 2 diabetes; all hypertensive
• Treatment group
• Number: treatment group (83); control group (79)
• Mean age ± SD (years)
◦ Treatment group: males (54.7 ± 8.1); females (56.8 ± 7.9)
◦ Control group: males (56.3 ± 8.6); females (57.5 ± 9.0)
• Sex (M/F): treatment group (40/43); control group (38/41)
Exclusion criteria
• Secondary or malignant hypertension; a recent history of myocardial infarction;
unstable angina; heart failure or aortic; outflow obstruction; renal, hepatic, blood or
endocrine disorders other than diabetes; positive response to an Albustix test for
urinary protein; women capable of becoming pregnant or using oral contraceptives;
history of poor compliance with drug therapy; known hypersensitivity/
contraindication to ACEi or nifedipine.
Interventions Treatment group
• Lisinopril: 10-20 mg/d
Control group
• Nifedipine: 20-60 mg/d
Outcomes • Death
• ESKD
• BP
Notes • BP target equalization not achieved in study (no use of other antihypertensive co-
interventions)
• Change in end of treatment HbA1c: treatment group (-0.4%); control group (-0.
2%)
Risk of bias
Bias Authors’ judgement Support for judgement
31Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
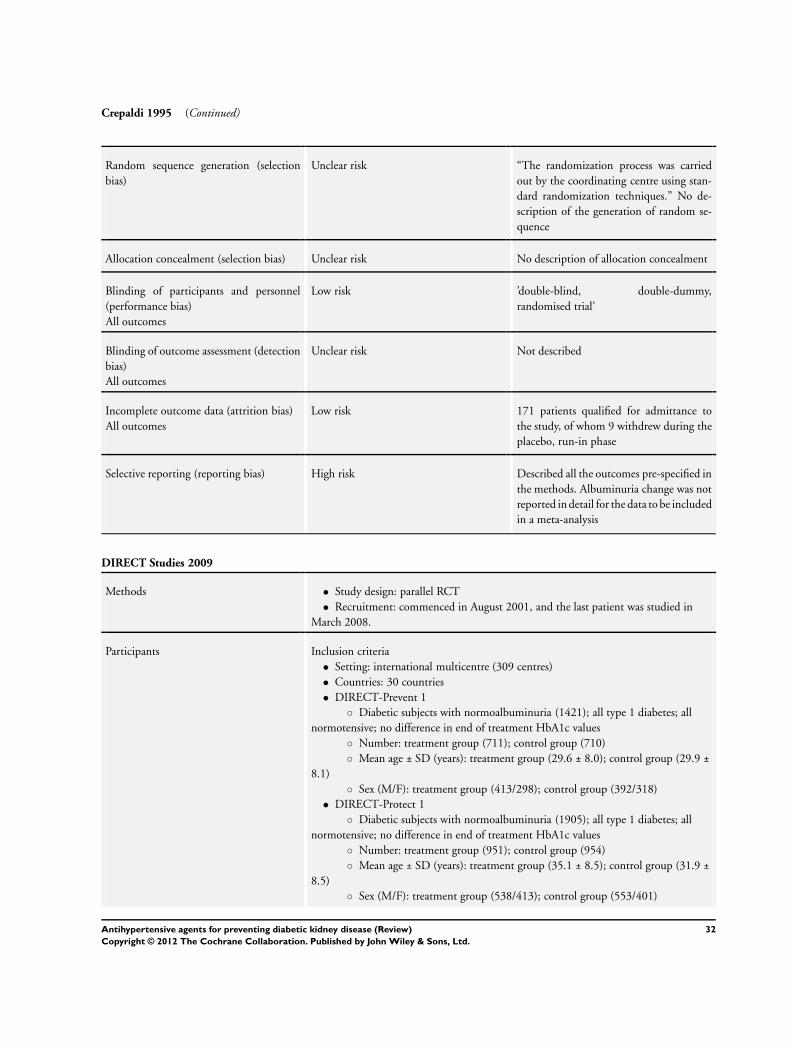
Crepaldi 1995 (Continued)
Random sequence generation (selection
bias)
Unclear risk “The randomization process was carried
out by the coordinating centre using stan-
dard randomization techniques.” No de-
scription of the generation of random se-
quence
Allocation concealment (selection bias) Unclear risk No description of allocation concealment
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk ’double-blind, double-dummy,
randomised trial’
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
Low risk 171 patients qualified for admittance to
the study, of whom 9 withdrew during the
placebo, run-in phase
Selective reporting (reporting bias) High risk Described all the outcomes pre-specified in
the methods. Albuminuria change was not
reported in detail for the data to be included
in a meta-analysis
DIRECT Studies 2009
Methods • Study design: parallel RCT
• Recruitment: commenced in August 2001, and the last patient was studied in
March 2008.
Participants Inclusion criteria
• Setting: international multicentre (309 centres)
• Countries: 30 countries
• DIRECT-Prevent 1
◦ Diabetic subjects with normoalbuminuria (1421); all type 1 diabetes; all
normotensive; no difference in end of treatment HbA1c values
◦ Number: treatment group (711); control group (710)
◦ Mean age ± SD (years): treatment group (29.6 ± 8.0); control group (29.9 ±
8.1)
◦ Sex (M/F): treatment group (413/298); control group (392/318)
• DIRECT-Protect 1
◦ Diabetic subjects with normoalbuminuria (1905); all type 1 diabetes; all
normotensive; no difference in end of treatment HbA1c values
◦ Number: treatment group (951); control group (954)
◦ Mean age ± SD (years): treatment group (35.1 ± 8.5); control group (31.9 ±
8.5)
◦ Sex (M/F): treatment group (538/413); control group (553/401)
32Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

DIRECT Studies 2009 (Continued)
• DIRECT-Protect 2
◦ Diabetic subjects with normoalbuminuria (1905); all type 2 diabetes; 62%
with hypertensive; no difference in end of treatment HbA1c values
◦ Number: treatment group (951); control group (954)
◦ Mean age ± SD (years): treatment group (56.9 ± 7.6); control group (56.8 ±
7.9)
◦ Sex (M/F): treatment group (466/485); control group (482/472)
Exclusion criteria
• Cataract or media opacity; angle closure glaucoma; history of retinopathy; history
or presence of clinical significant macular oedema; history or evidence of
photocoagulation of the retina; other retinal conditions which may mask assessment;
pregnant or lactating women or women of child bearing potential not practicing an
adequate method of contraception; need of treatment with ACEi; haemodynamically
significant aortic or mitral valve stenosis; known renal artery stenosis or kidney
transplantation; hypersensitivity to study drug; severe concomitant disease which may
interfere with the assessment of the patient; malignancy
Interventions Treatment group
• Candesartan: 16 mg/d increasing to 32 mg/d
Control group
• Placebo
Outcomes • Death
• New onset albuminuria
• BP
• headache
• hyperkalaemia
Notes • Supported By AstraZeneca and Takeda
• Statistical staff at AstraZeneca and Takeda did analyses according to the intention-
to-treat principle. The 2-sided P values were calculated without any adjustment for
multiple comparisons
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Randomisation into the three studies was
conducted based on primary grading of the
baseline photographs, using the ETDRS
severity scale.The patients are to be evalu-
ated in the correct study based on the final
grading of the photographs
No description of random sequence gener-
ation
Allocation concealment (selection bias) Low risk “randomly assigned eligible patients cen-
trally using an interactive voice-response
system”
33Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
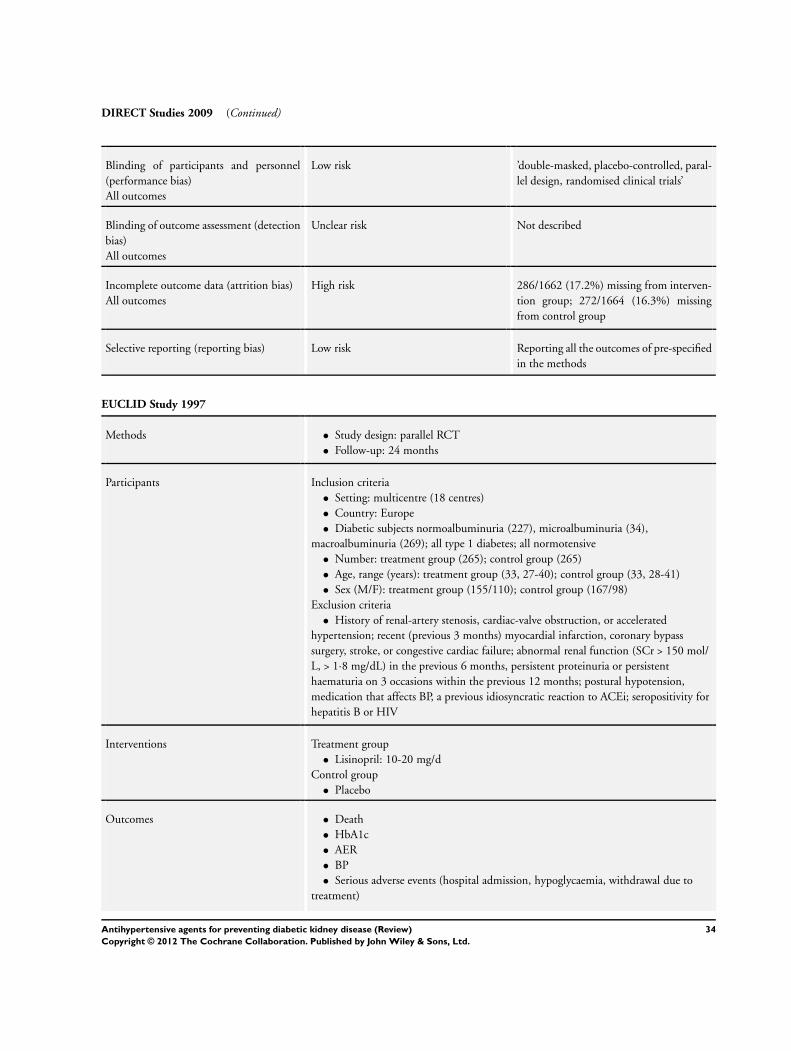
DIRECT Studies 2009 (Continued)
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk ’double-masked, placebo-controlled, paral-
lel design, randomised clinical trials’
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
High risk 286/1662 (17.2%) missing from interven-
tion group; 272/1664 (16.3%) missing
from control group
Selective reporting (reporting bias) Low risk Reporting all the outcomes of pre-specified
in the methods
EUCLID Study 1997
Methods • Study design: parallel RCT
• Follow-up: 24 months
Participants Inclusion criteria
• Setting: multicentre (18 centres)
• Country: Europe
• Diabetic subjects normoalbuminuria (227), microalbuminuria (34),
macroalbuminuria (269); all type 1 diabetes; all normotensive
• Number: treatment group (265); control group (265)
• Age, range (years): treatment group (33, 27-40); control group (33, 28-41)
• Sex (M/F): treatment group (155/110); control group (167/98)
Exclusion criteria
• History of renal-artery stenosis, cardiac-valve obstruction, or accelerated
hypertension; recent (previous 3 months) myocardial infarction, coronary bypass
surgery, stroke, or congestive cardiac failure; abnormal renal function (SCr > 150 mol/
L, > 1·8 mg/dL) in the previous 6 months, persistent proteinuria or persistent
haematuria on 3 occasions within the previous 12 months; postural hypotension,
medication that affects BP, a previous idiosyncratic reaction to ACEi; seropositivity for
hepatitis B or HIV
Interventions Treatment group
• Lisinopril: 10-20 mg/d
Control group
• Placebo
Outcomes • Death
• HbA1c
• AER
• BP
• Serious adverse events (hospital admission, hypoglycaemia, withdrawal due to
treatment)
34Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
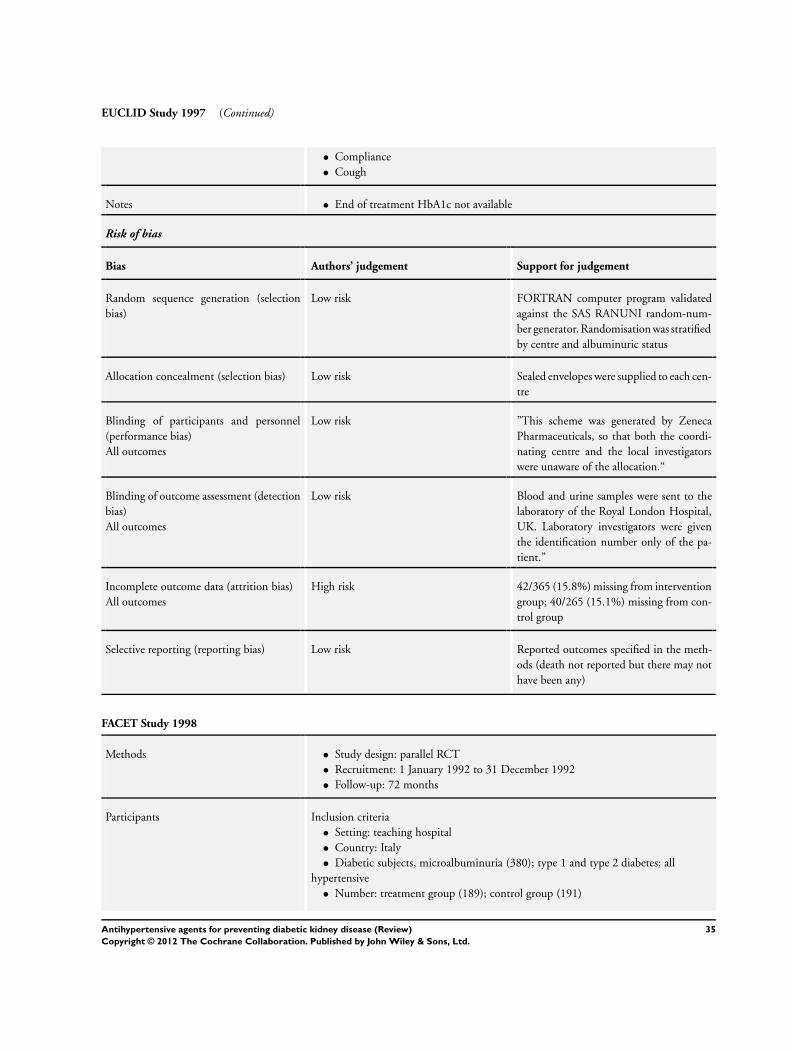
EUCLID Study 1997 (Continued)
• Compliance
• Cough
Notes • End of treatment HbA1c not available
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk FORTRAN computer program validated
against the SAS RANUNI random-num-
ber generator. Randomisation was stratified
by centre and albuminuric status
Allocation concealment (selection bias) Low risk Sealed envelopes were supplied to each cen-
tre
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk ”This scheme was generated by Zeneca
Pharmaceuticals, so that both the coordi-
nating centre and the local investigators
were unaware of the allocation.“
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Blood and urine samples were sent to the
laboratory of the Royal London Hospital,
UK. Laboratory investigators were given
the identification number only of the pa-
tient.”
Incomplete outcome data (attrition bias)
All outcomes
High risk 42/365 (15.8%) missing from intervention
group; 40/265 (15.1%) missing from con-
trol group
Selective reporting (reporting bias) Low risk Reported outcomes specified in the meth-
ods (death not reported but there may not
have been any)
FACET Study 1998
Methods • Study design: parallel RCT
• Recruitment: 1 January 1992 to 31 December 1992
• Follow-up: 72 months
Participants Inclusion criteria
• Setting: teaching hospital
• Country: Italy
• Diabetic subjects, microalbuminuria (380); type 1 and type 2 diabetes; all
hypertensive
• Number: treatment group (189); control group (191)
35Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

FACET Study 1998 (Continued)
• Mean age ± SD (years): treatment group (10.7 ± 9.96); control group (63.3 ± 5.
52)
• Sex (M/F): treatment group (120/69); control group (106/85)
Exclusion criteria
• history of coronary heart disease, stroke, or any other morbid condition with poor
prognosis; SCr > 1.5 mg/dL; a microalbuminurialevel > 40 ug/min; use of lipid
lowering drugs, aspirin, or antihypertensive agents other than diuretics and beta-
blockers
Interventions Treatment group
• Fosinopril: 20 mg/d
Control group
• Amlodipine: 10 mg/d
Outcomes • Death
• Myocardial infarction
• BP
• Albuminuria
Notes • BP target equalization not achieved in study (despite use of other antihypertensive
co-interventions)
• End of treatment HbA1c: treatment group (8.7%); control group (8.5%)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Computer-generated random number se-
quence
Allocation concealment (selection bias) Low risk Adequate
Blinding of participants and personnel
(performance bias)
All outcomes
High risk Open-label design
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
High risk 17/189 (9.0%) missing from treatment
group; 23/191(12.0%) missing from con-
trol group
Selective reporting (reporting bias) Low risk Reported all outcomes specified in the
methods
36Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
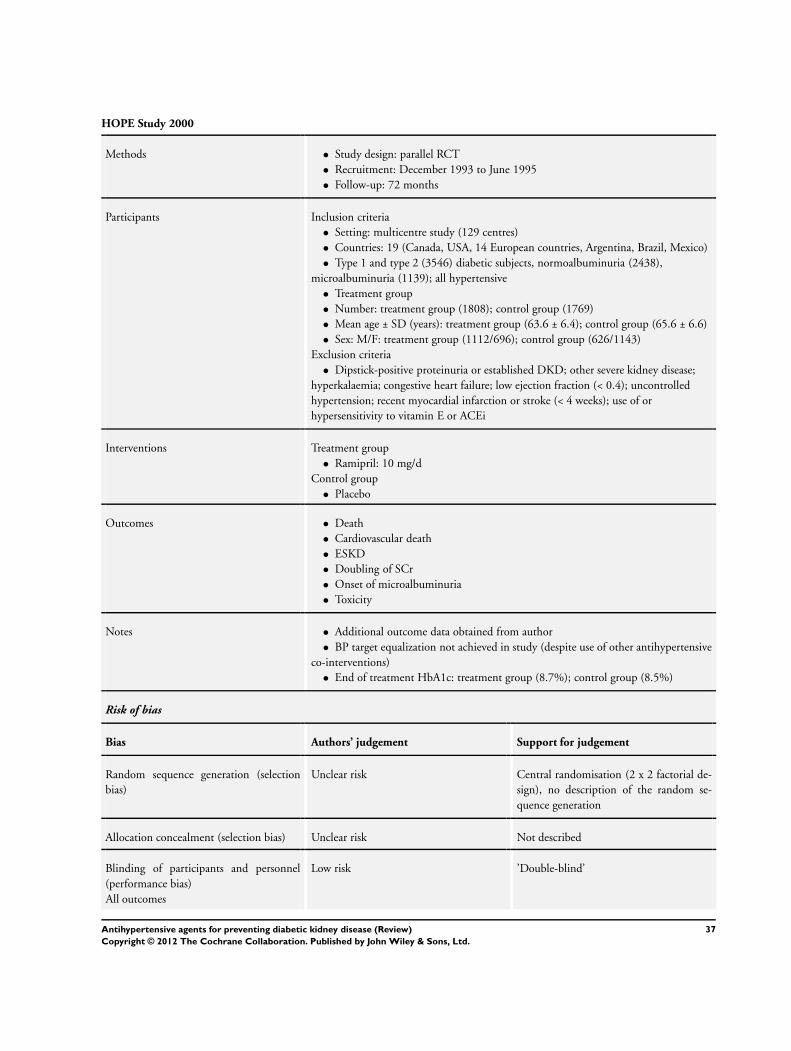
HOPE Study 2000
Methods • Study design: parallel RCT
• Recruitment: December 1993 to June 1995
• Follow-up: 72 months
Participants Inclusion criteria
• Setting: multicentre study (129 centres)
• Countries: 19 (Canada, USA, 14 European countries, Argentina, Brazil, Mexico)
• Type 1 and type 2 (3546) diabetic subjects, normoalbuminuria (2438),
microalbuminuria (1139); all hypertensive
• Treatment group
• Number: treatment group (1808); control group (1769)
• Mean age ± SD (years): treatment group (63.6 ± 6.4); control group (65.6 ± 6.6)
• Sex: M/F: treatment group (1112/696); control group (626/1143)
Exclusion criteria
• Dipstick-positive proteinuria or established DKD; other severe kidney disease;
hyperkalaemia; congestive heart failure; low ejection fraction (< 0.4); uncontrolled
hypertension; recent myocardial infarction or stroke (< 4 weeks); use of or
hypersensitivity to vitamin E or ACEi
Interventions Treatment group
• Ramipril: 10 mg/d
Control group
• Placebo
Outcomes • Death
• Cardiovascular death
• ESKD
• Doubling of SCr
• Onset of microalbuminuria
• Toxicity
Notes • Additional outcome data obtained from author
• BP target equalization not achieved in study (despite use of other antihypertensive
co-interventions)
• End of treatment HbA1c: treatment group (8.7%); control group (8.5%)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Central randomisation (2 x 2 factorial de-
sign), no description of the random se-
quence generation
Allocation concealment (selection bias) Unclear risk Not described
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk ’Double-blind’
37Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

HOPE Study 2000 (Continued)
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Not described
Selective reporting (reporting bias) Low risk Reported all outcomes specified in the
methods
Joglekar 1998
Methods • Study design: parallel RCT
• Follow-up: 6 months
Participants Inclusion criteria
• Setting: multicentre (20)
• Country: India
• Proportion with normoalbuminuria, microalbuminuria or macroalbuminuria not
available; all type 2 diabetes; all hypertensive
• Treatment group
• Number: treatment group (48); control group (41)
• Mean age ± SD (years): treatment group (54.7 ± 11.6); control group (53.4 ± 11.
6)
• Sex (M/F): treatment group (17/12); control group (19/12)
Exclusion criteria: not stated
Interventions Treatment group
• Enalapril: 5-10 mg/d
Control group
• Prazosin GITS: 2.5-5 mg/d
Outcomes • Cough
• GFR
Notes • BP target equalization not achieved in study (no use of other antihypertensive co-
interventions)
• End of treatment HbA1c not available
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Random sequence generation not de-
scribed
Allocation concealment (selection bias) Unclear risk No description of allocation concealment
38Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Joglekar 1998 (Continued)
Blinding of participants and personnel
(performance bias)
All outcomes
Unclear risk Not described
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
High risk 17/48 missing from intervention group;
12/41 missing from control group
Selective reporting (reporting bias) High risk Albuminuria change was not reported in
detail for the data to be included in a meta-
analysis
Kavgaci 2002
Methods • Study design: parallel RCT
• Follow-up: 6 months
Participants Inclusion criteria
• Setting: single centre
• Country: Turkey
• Diabetic subjects, normoalbuminuria (18), microalbuminuria (15); all type 2
diabetes; all hypertensive
• Number: treatment group (20); control group (13)
• Median age, range (years): treatment group (49, 41-62); control group (59, 40-66)
• Sex (M/F): treatment group (9/11); control group (4/19)
Exclusion criteria
• Albuminuria level > 300 mg/d; CCr < 100 mL/min; patients taking ACEi and
ARB
Interventions Treatment group
• Fosinopril: 10 mg/d
Control group
• Losartan: 50 mg/d
Outcomes • changes in albuminuria
Notes • BP target equalization achieved in study by use of other antihypertensive co-
interventions
• End of treatment HbA1c 7.57 versus 6.58% in treatment and control group
Risk of bias
Bias Authors’ judgement Support for judgement
39Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
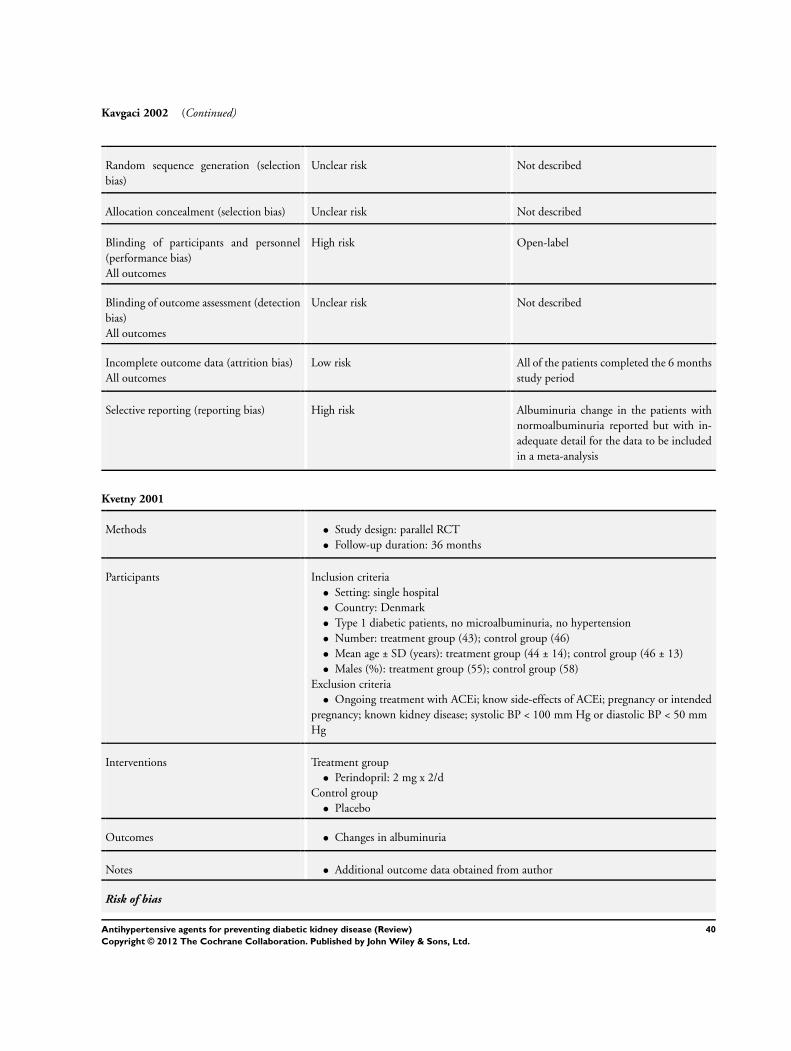
Kavgaci 2002 (Continued)
Random sequence generation (selection
bias)
Unclear risk Not described
Allocation concealment (selection bias) Unclear risk Not described
Blinding of participants and personnel
(performance bias)
All outcomes
High risk Open-label
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
Low risk All of the patients completed the 6 months
study period
Selective reporting (reporting bias) High risk Albuminuria change in the patients with
normoalbuminuria reported but with in-
adequate detail for the data to be included
in a meta-analysis
Kvetny 2001
Methods • Study design: parallel RCT
• Follow-up duration: 36 months
Participants Inclusion criteria
• Setting: single hospital
• Country: Denmark
• Type 1 diabetic patients, no microalbuminuria, no hypertension
• Number: treatment group (43); control group (46)
• Mean age ± SD (years): treatment group (44 ± 14); control group (46 ± 13)
• Males (%): treatment group (55); control group (58)
Exclusion criteria
• Ongoing treatment with ACEi; know side-effects of ACEi; pregnancy or intended
pregnancy; known kidney disease; systolic BP < 100 mm Hg or diastolic BP < 50 mm
Hg
Interventions Treatment group
• Perindopril: 2 mg x 2/d
Control group
• Placebo
Outcomes • Changes in albuminuria
Notes • Additional outcome data obtained from author
Risk of bias
40Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
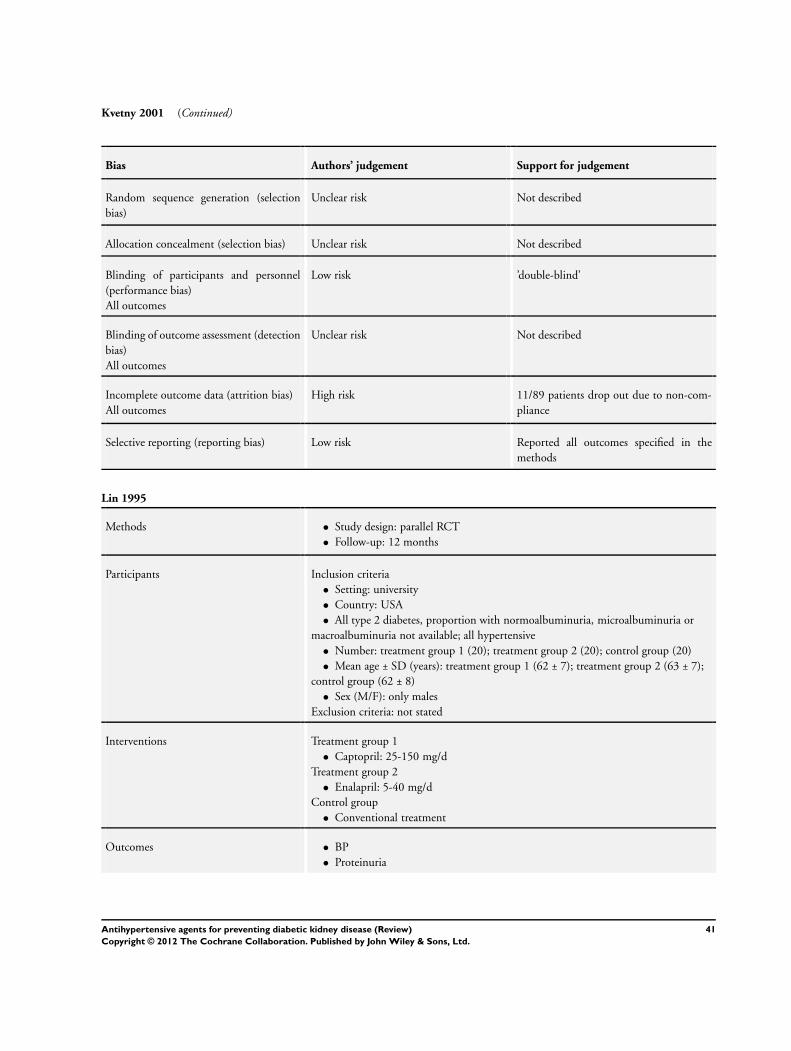
Kvetny 2001 (Continued)
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not described
Allocation concealment (selection bias) Unclear risk Not described
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk ’double-blind’
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
High risk 11/89 patients drop out due to non-com-
pliance
Selective reporting (reporting bias) Low risk Reported all outcomes specified in the
methods
Lin 1995
Methods • Study design: parallel RCT
• Follow-up: 12 months
Participants Inclusion criteria
• Setting: university
• Country: USA
• All type 2 diabetes, proportion with normoalbuminuria, microalbuminuria or
macroalbuminuria not available; all hypertensive
• Number: treatment group 1 (20); treatment group 2 (20); control group (20)
• Mean age ± SD (years): treatment group 1 (62 ± 7); treatment group 2 (63 ± 7);
control group (62 ± 8)
• Sex (M/F): only males
Exclusion criteria: not stated
Interventions Treatment group 1
• Captopril: 25-150 mg/d
Treatment group 2
• Enalapril: 5-40 mg/d
Control group
• Conventional treatment
Outcomes • BP
• Proteinuria
41Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
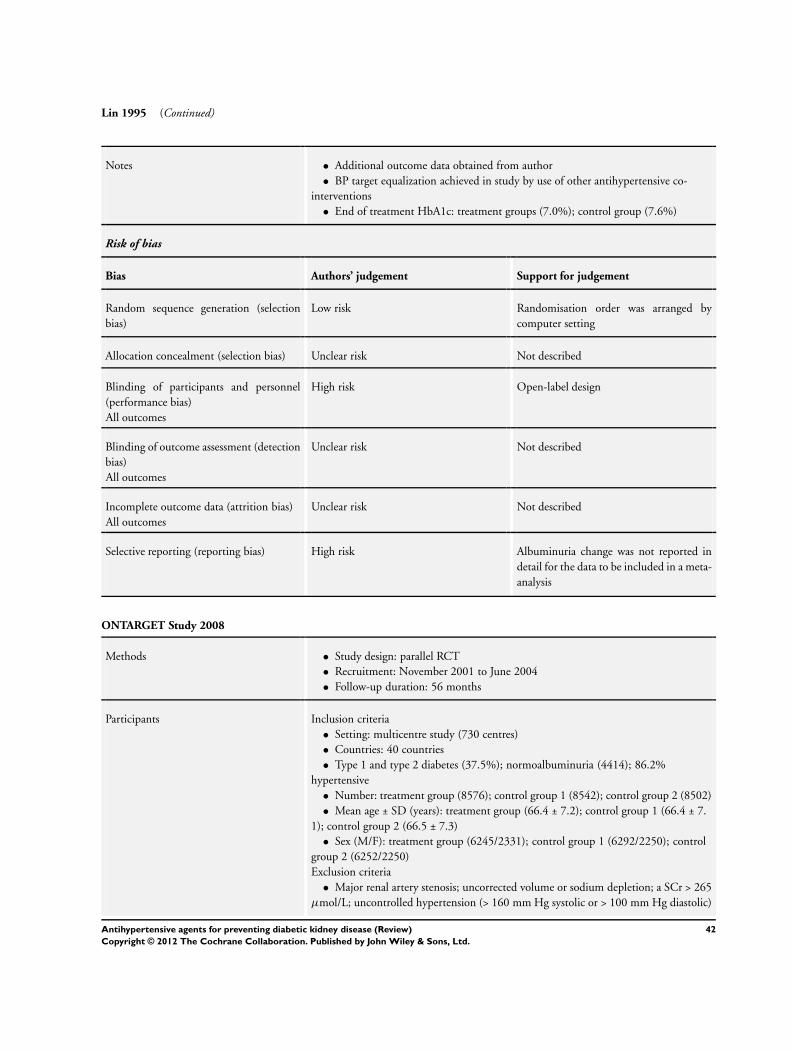
Lin 1995 (Continued)
Notes • Additional outcome data obtained from author
• BP target equalization achieved in study by use of other antihypertensive co-
interventions
• End of treatment HbA1c: treatment groups (7.0%); control group (7.6%)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Randomisation order was arranged by
computer setting
Allocation concealment (selection bias) Unclear risk Not described
Blinding of participants and personnel
(performance bias)
All outcomes
High risk Open-label design
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
Unclear risk Not described
Selective reporting (reporting bias) High risk Albuminuria change was not reported in
detail for the data to be included in a meta-
analysis
ONTARGET Study 2008
Methods • Study design: parallel RCT
• Recruitment: November 2001 to June 2004
• Follow-up duration: 56 months
Participants Inclusion criteria
• Setting: multicentre study (730 centres)
• Countries: 40 countries
• Type 1 and type 2 diabetes (37.5%); normoalbuminuria (4414); 86.2%
hypertensive
• Number: treatment group (8576); control group 1 (8542); control group 2 (8502)
• Mean age ± SD (years): treatment group (66.4 ± 7.2); control group 1 (66.4 ± 7.
1); control group 2 (66.5 ± 7.3)
• Sex (M/F): treatment group (6245/2331); control group 1 (6292/2250); control
group 2 (6252/2250)
Exclusion criteria
• Major renal artery stenosis; uncorrected volume or sodium depletion; a SCr > 265
µmol/L; uncontrolled hypertension (> 160 mm Hg systolic or > 100 mm Hg diastolic)
42Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
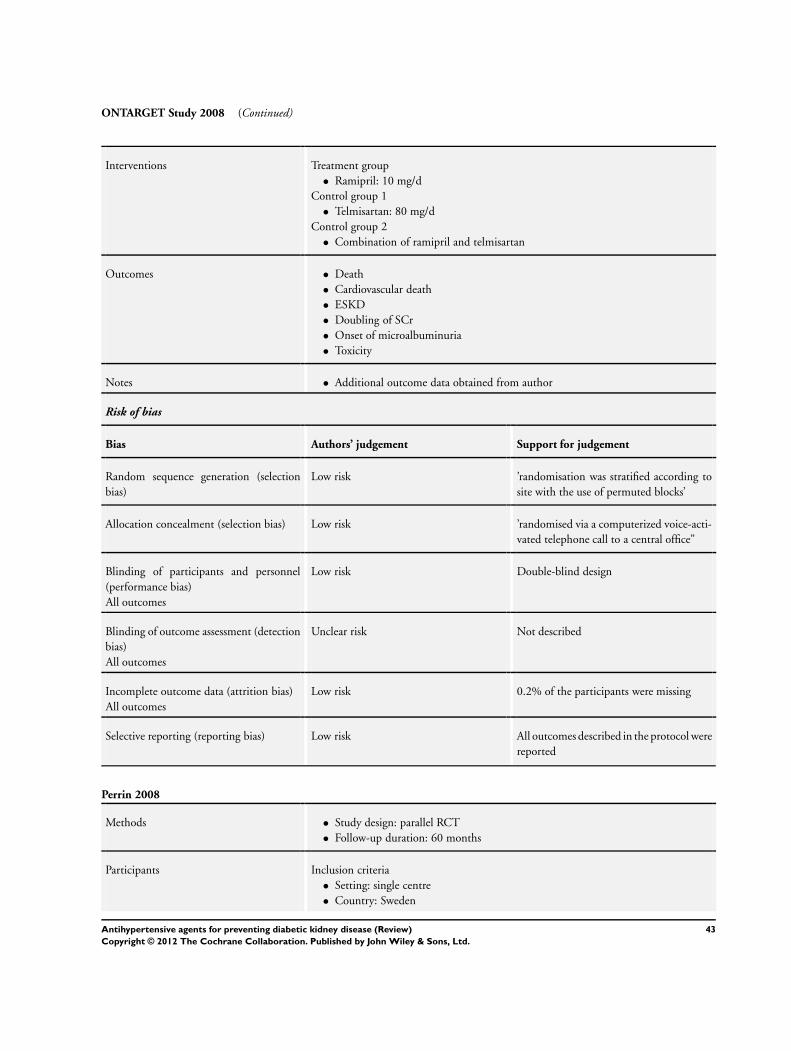
ONTARGET Study 2008 (Continued)
Interventions Treatment group
• Ramipril: 10 mg/d
Control group 1
• Telmisartan: 80 mg/d
Control group 2
• Combination of ramipril and telmisartan
Outcomes • Death
• Cardiovascular death
• ESKD
• Doubling of SCr
• Onset of microalbuminuria
• Toxicity
Notes • Additional outcome data obtained from author
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk ’randomisation was stratified according to
site with the use of permuted blocks’
Allocation concealment (selection bias) Low risk ’randomised via a computerized voice-acti-
vated telephone call to a central office”
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Double-blind design
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
Low risk 0.2% of the participants were missing
Selective reporting (reporting bias) Low risk All outcomes described in the protocol were
reported
Perrin 2008
Methods • Study design: parallel RCT
• Follow-up duration: 60 months
Participants Inclusion criteria
• Setting: single centre
• Country: Sweden
43Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
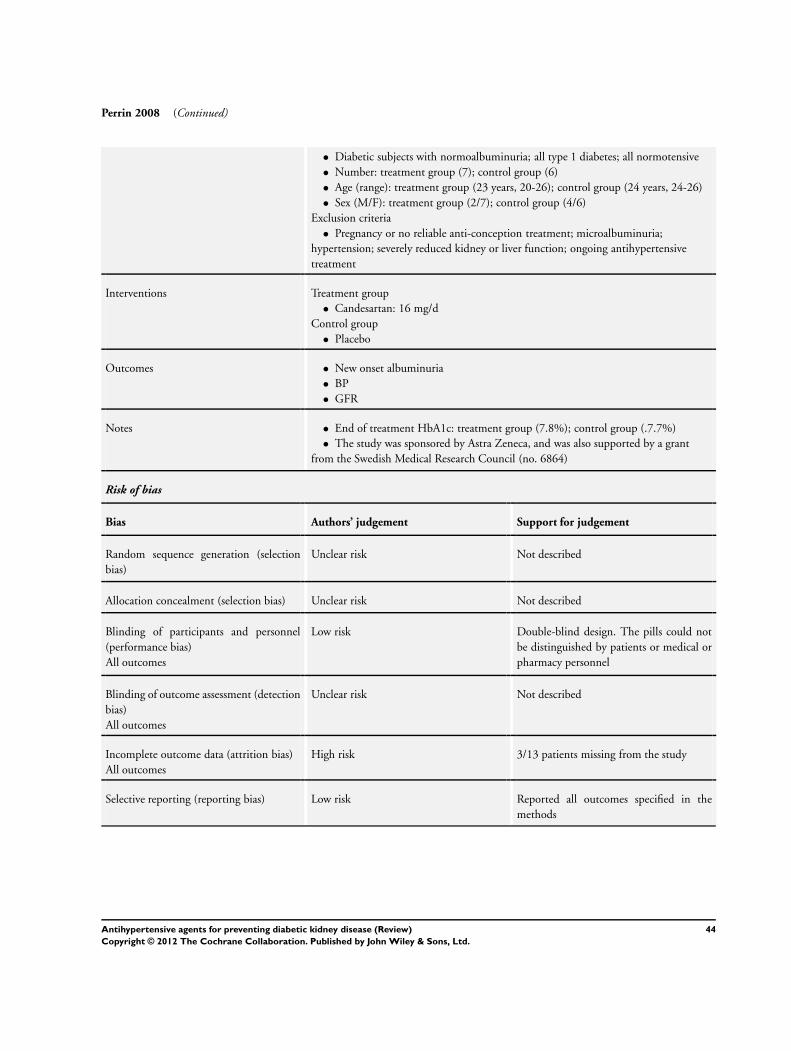
Perrin 2008 (Continued)
• Diabetic subjects with normoalbuminuria; all type 1 diabetes; all normotensive
• Number: treatment group (7); control group (6)
• Age (range): treatment group (23 years, 20-26); control group (24 years, 24-26)
• Sex (M/F): treatment group (2/7); control group (4/6)
Exclusion criteria
• Pregnancy or no reliable anti-conception treatment; microalbuminuria;
hypertension; severely reduced kidney or liver function; ongoing antihypertensive
treatment
Interventions Treatment group
• Candesartan: 16 mg/d
Control group
• Placebo
Outcomes • New onset albuminuria
• BP
• GFR
Notes • End of treatment HbA1c: treatment group (7.8%); control group (.7.7%)
• The study was sponsored by Astra Zeneca, and was also supported by a grant
from the Swedish Medical Research Council (no. 6864)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not described
Allocation concealment (selection bias) Unclear risk Not described
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Double-blind design. The pills could not
be distinguished by patients or medical or
pharmacy personnel
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
High risk 3/13 patients missing from the study
Selective reporting (reporting bias) Low risk Reported all outcomes specified in the
methods
44Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
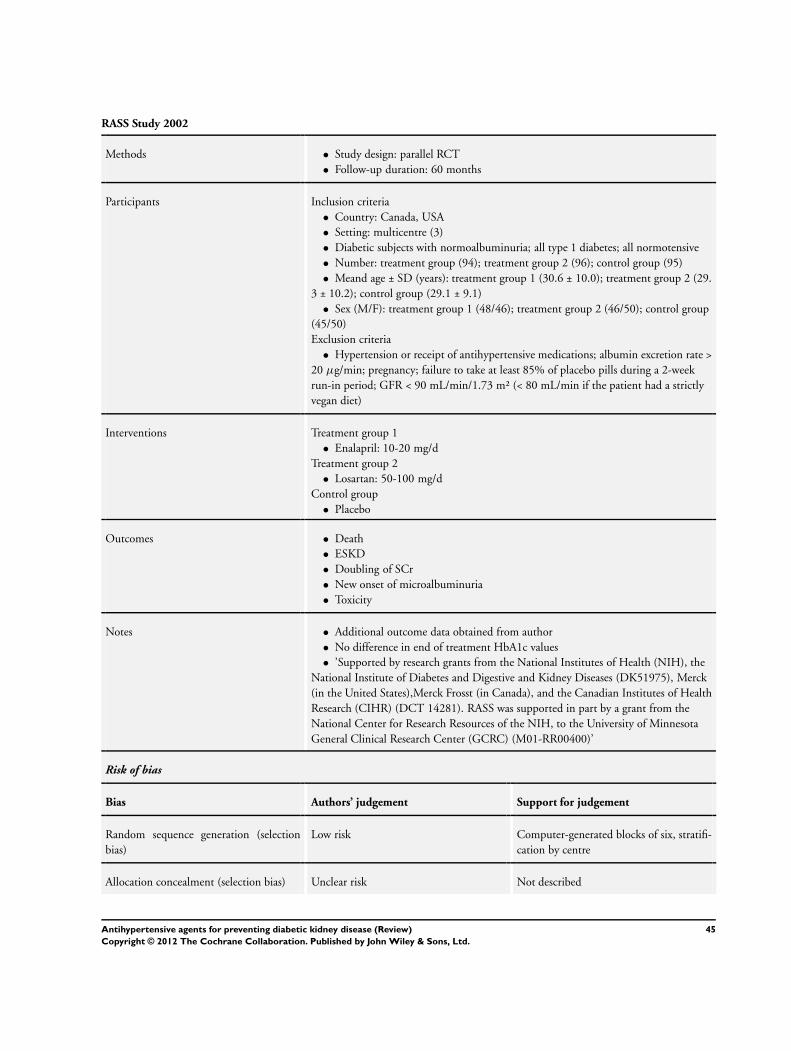
RASS Study 2002
Methods • Study design: parallel RCT
• Follow-up duration: 60 months
Participants Inclusion criteria
• Country: Canada, USA
• Setting: multicentre (3)
• Diabetic subjects with normoalbuminuria; all type 1 diabetes; all normotensive
• Number: treatment group (94); treatment group 2 (96); control group (95)
• Meand age ± SD (years): treatment group 1 (30.6 ± 10.0); treatment group 2 (29.
3 ± 10.2); control group (29.1 ± 9.1)
• Sex (M/F): treatment group 1 (48/46); treatment group 2 (46/50); control group
(45/50)
Exclusion criteria
• Hypertension or receipt of antihypertensive medications; albumin excretion rate >
20 µg/min; pregnancy; failure to take at least 85% of placebo pills during a 2-week
run-in period; GFR < 90 mL/min/1.73 m² (< 80 mL/min if the patient had a strictly
vegan diet)
Interventions Treatment group 1
• Enalapril: 10-20 mg/d
Treatment group 2
• Losartan: 50-100 mg/d
Control group
• Placebo
Outcomes • Death
• ESKD
• Doubling of SCr
• New onset of microalbuminuria
• Toxicity
Notes • Additional outcome data obtained from author
• No difference in end of treatment HbA1c values
• ’Supported by research grants from the National Institutes of Health (NIH), the
National Institute of Diabetes and Digestive and Kidney Diseases (DK51975), Merck
(in the United States),Merck Frosst (in Canada), and the Canadian Institutes of Health
Research (CIHR) (DCT 14281). RASS was supported in part by a grant from the
National Center for Research Resources of the NIH, to the University of Minnesota
General Clinical Research Center (GCRC) (M01-RR00400)’
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Computer-generated blocks of six, stratifi-
cation by centre
Allocation concealment (selection bias) Unclear risk Not described
45Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
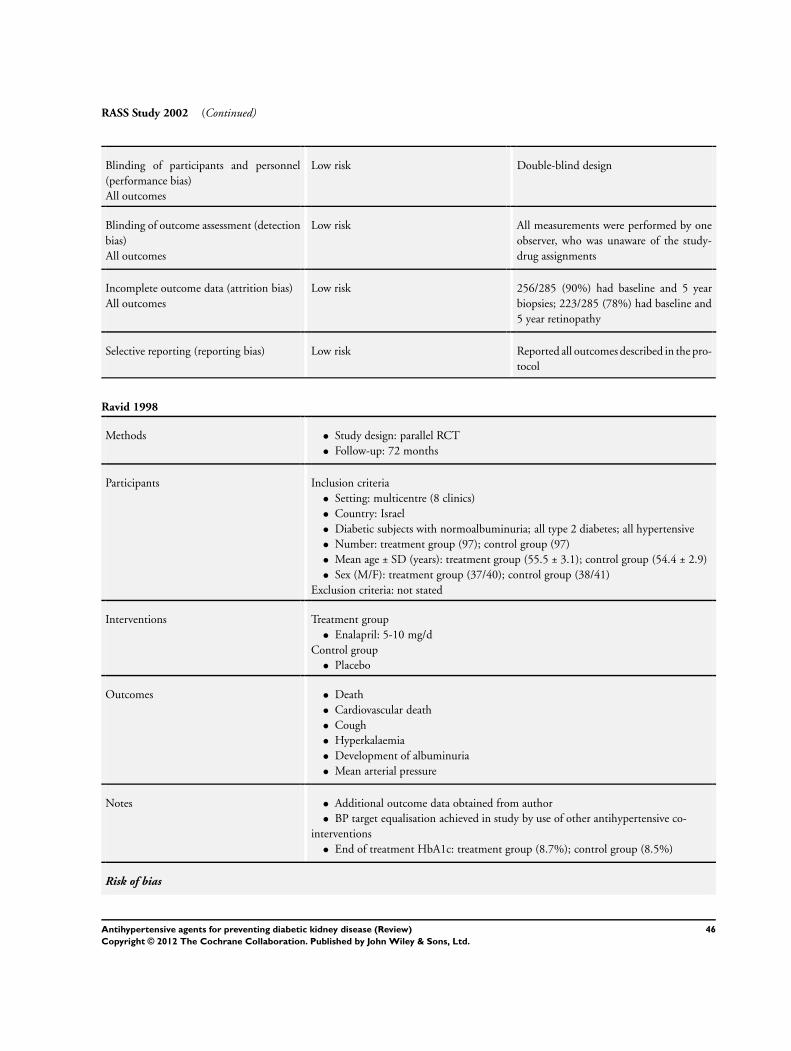
RASS Study 2002 (Continued)
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Double-blind design
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk All measurements were performed by one
observer, who was unaware of the study-
drug assignments
Incomplete outcome data (attrition bias)
All outcomes
Low risk 256/285 (90%) had baseline and 5 year
biopsies; 223/285 (78%) had baseline and
5 year retinopathy
Selective reporting (reporting bias) Low risk Reported all outcomes described in the pro-
tocol
Ravid 1998
Methods • Study design: parallel RCT
• Follow-up: 72 months
Participants Inclusion criteria
• Setting: multicentre (8 clinics)
• Country: Israel
• Diabetic subjects with normoalbuminuria; all type 2 diabetes; all hypertensive
• Number: treatment group (97); control group (97)
• Mean age ± SD (years): treatment group (55.5 ± 3.1); control group (54.4 ± 2.9)
• Sex (M/F): treatment group (37/40); control group (38/41)
Exclusion criteria: not stated
Interventions Treatment group
• Enalapril: 5-10 mg/d
Control group
• Placebo
Outcomes • Death
• Cardiovascular death
• Cough
• Hyperkalaemia
• Development of albuminuria
• Mean arterial pressure
Notes • Additional outcome data obtained from author
• BP target equalisation achieved in study by use of other antihypertensive co-
interventions
• End of treatment HbA1c: treatment group (8.7%); control group (8.5%)
Risk of bias
46Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
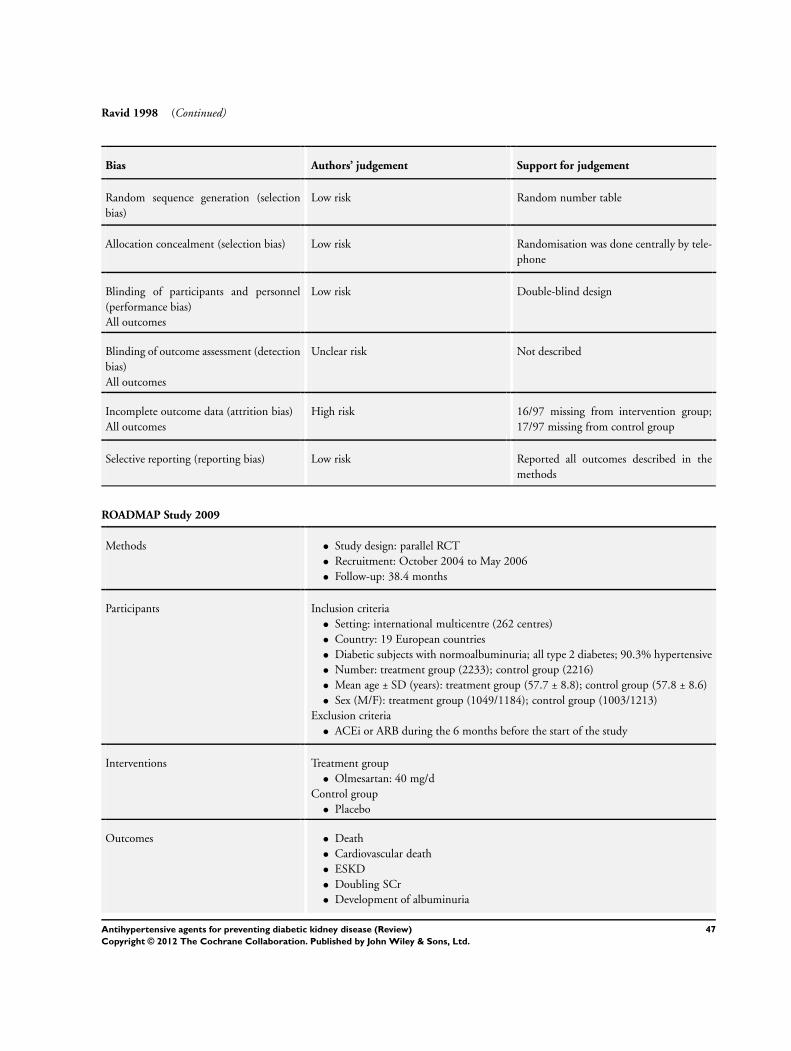
Ravid 1998 (Continued)
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Random number table
Allocation concealment (selection bias) Low risk Randomisation was done centrally by tele-
phone
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Double-blind design
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
High risk 16/97 missing from intervention group;
17/97 missing from control group
Selective reporting (reporting bias) Low risk Reported all outcomes described in the
methods
ROADMAP Study 2009
Methods • Study design: parallel RCT
• Recruitment: October 2004 to May 2006
• Follow-up: 38.4 months
Participants Inclusion criteria
• Setting: international multicentre (262 centres)
• Country: 19 European countries
• Diabetic subjects with normoalbuminuria; all type 2 diabetes; 90.3% hypertensive
• Number: treatment group (2233); control group (2216)
• Mean age ± SD (years): treatment group (57.7 ± 8.8); control group (57.8 ± 8.6)
• Sex (M/F): treatment group (1049/1184); control group (1003/1213)
Exclusion criteria
• ACEi or ARB during the 6 months before the start of the study
Interventions Treatment group
• Olmesartan: 40 mg/d
Control group
• Placebo
Outcomes • Death
• Cardiovascular death
• ESKD
• Doubling SCr
• Development of albuminuria
47Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

ROADMAP Study 2009 (Continued)
Notes • BP target equalisation achieved in study by use of other antihypertensive co-
interventions
• ’The sponsor (Daiichi Sankyo) had no role in the design or conduct of the study,
but representatives of the sponsor served as nonvoting members of the steering
committee’
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk Randomisation list produced by PRA using
SAS software
Allocation concealment (selection bias) Low risk Sealed envelopes used in randomisation al-
location
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Double-blind design
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
Low risk 51/2233 lost from intervention group; 57/
2216 lost from control group
Selective reporting (reporting bias) Unclear risk Reported all outcomes described in the pro-
tocol
Scognamiglio 1997
Methods • Study design: parallel RCT
• Follow-up period: 36 weeks
Participants Inclusion criteria
• Setting: not described
• Country: Italy
• Diabetic subjects with normoalbuminuria; all type 1 diabetes; all hypertensive
• Number: treatment group (36); control group (37)
• Mean age ± SD (years): treatment group (58.7 ± 6.9); control group (57.3 ± 6.7)
• Sex (M/F): treatment group (26/10); control group (29/8)
Exclusion criteria: not stated
Interventions Treatment group
• Captopril: 50-100 mg/d
Control group
• Nitrendipine: 20-40 mg/d
48Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
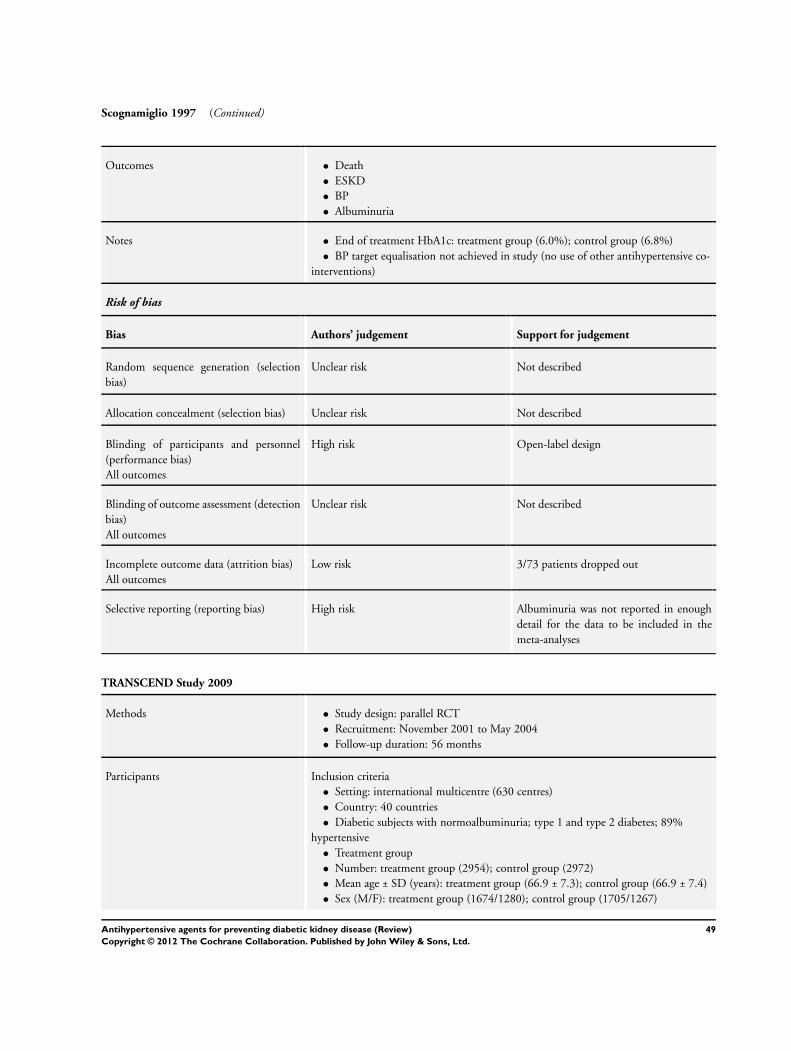
Scognamiglio 1997 (Continued)
Outcomes • Death
• ESKD
• BP
• Albuminuria
Notes • End of treatment HbA1c: treatment group (6.0%); control group (6.8%)
• BP target equalisation not achieved in study (no use of other antihypertensive co-
interventions)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not described
Allocation concealment (selection bias) Unclear risk Not described
Blinding of participants and personnel
(performance bias)
All outcomes
High risk Open-label design
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
Low risk 3/73 patients dropped out
Selective reporting (reporting bias) High risk Albuminuria was not reported in enough
detail for the data to be included in the
meta-analyses
TRANSCEND Study 2009
Methods • Study design: parallel RCT
• Recruitment: November 2001 to May 2004
• Follow-up duration: 56 months
Participants Inclusion criteria
• Setting: international multicentre (630 centres)
• Country: 40 countries
• Diabetic subjects with normoalbuminuria; type 1 and type 2 diabetes; 89%
hypertensive
• Treatment group
• Number: treatment group (2954); control group (2972)
• Mean age ± SD (years): treatment group (66.9 ± 7.3); control group (66.9 ± 7.4)
• Sex (M/F): treatment group (1674/1280); control group (1705/1267)
49Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

TRANSCEND Study 2009 (Continued)
Exclusion criteria
• Needed an ARB; hypersensitive or intolerant to ARB; heart failure, significant
valvular or cardiac outflow tract obstruction, constrictive pericarditis complex
congenital heart disease, unexplained syncope, planned cardiac surgery, cardiac
revascularization in the previous 3 months; systolic BP ≥ 160 mm Hg; heart
transplantation; subarachnoid haemorrhage; known significant renal artery stenosis;
SCr levels > 265 mol/L (3.0 mg/dL); hepatic dysfunction.
Interventions Treatment group
• Telmisartan: 80 mg/d
Control group
• Placebo
Outcomes • Death
• Cardiovascular death
• ESKD
• Doubling of SCr
• Onset of microalbuminuria
• Toxicity
Notes • Additional outcome data obtained from author
• ’Boehringer Ingelheim funded the study. The steering committee designed and
oversaw the study and had the final decision on the contents of the manuscript. All
data were received, checked, and analyzed independently at the coordinating center at
McMaster University.’
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk ’randomisation was stratified according to
site with the use of permuted blocks’
Allocation concealment (selection bias) Low risk randomised via a computerized voice-acti-
vated telephone call
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Double-blind design ’All participants and
trial investigators were blinded to random-
ized treatment’
’Unblinded data were made available exclu-
sively to the independent data safety and
monitoring board by a statistician who was
independent of the trial’
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
50Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
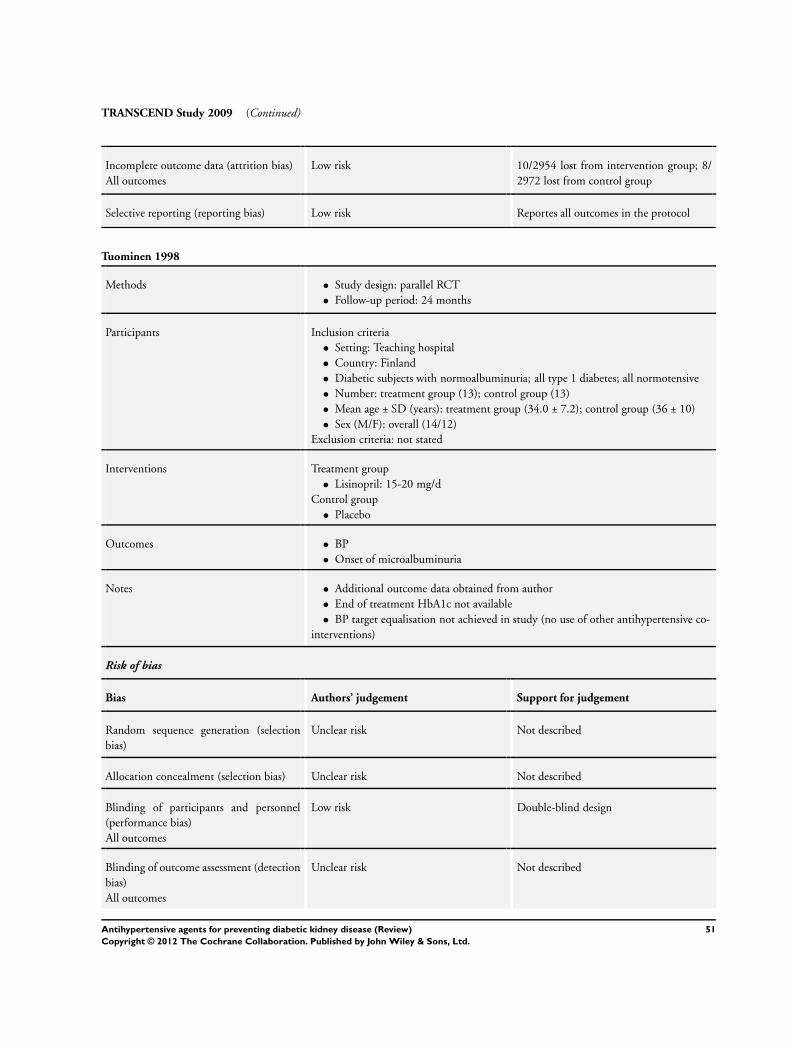
TRANSCEND Study 2009 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Low risk 10/2954 lost from intervention group; 8/
2972 lost from control group
Selective reporting (reporting bias) Low risk Reportes all outcomes in the protocol
Tuominen 1998
Methods • Study design: parallel RCT
• Follow-up period: 24 months
Participants Inclusion criteria
• Setting: Teaching hospital
• Country: Finland
• Diabetic subjects with normoalbuminuria; all type 1 diabetes; all normotensive
• Number: treatment group (13); control group (13)
• Mean age ± SD (years): treatment group (34.0 ± 7.2); control group (36 ± 10)
• Sex (M/F): overall (14/12)
Exclusion criteria: not stated
Interventions Treatment group
• Lisinopril: 15-20 mg/d
Control group
• Placebo
Outcomes • BP
• Onset of microalbuminuria
Notes • Additional outcome data obtained from author
• End of treatment HbA1c not available
• BP target equalisation not achieved in study (no use of other antihypertensive co-
interventions)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not described
Allocation concealment (selection bias) Unclear risk Not described
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Double-blind design
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
51Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
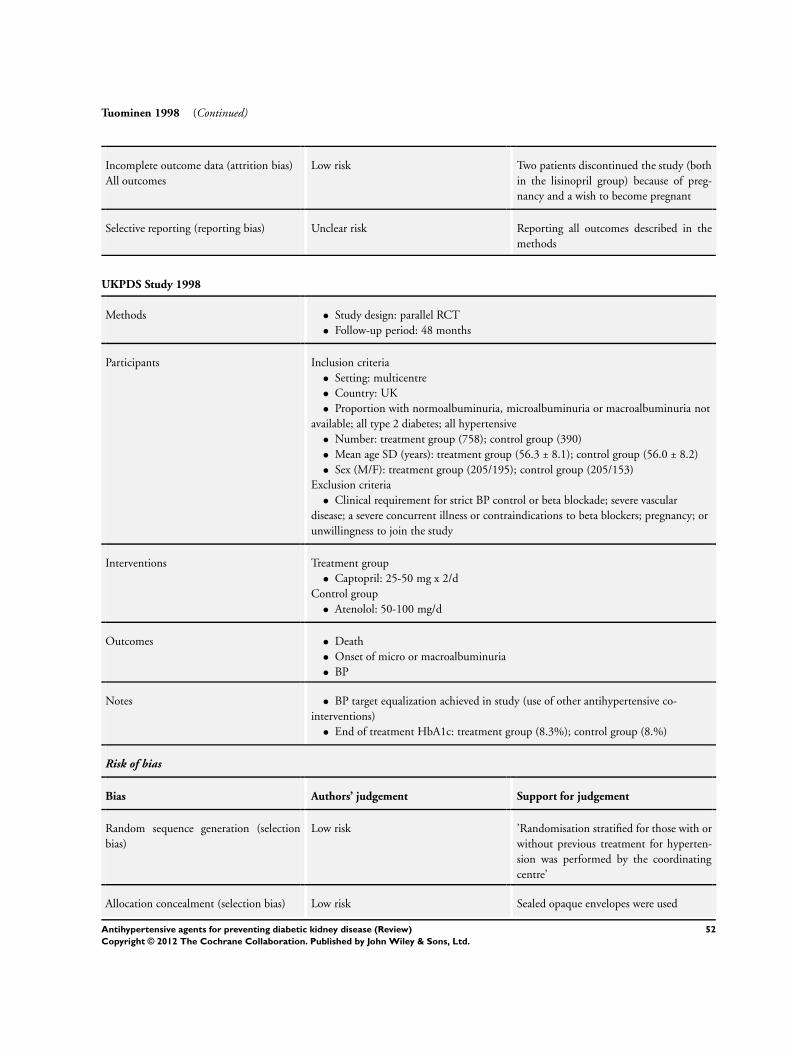
Tuominen 1998 (Continued)
Incomplete outcome data (attrition bias)
All outcomes
Low risk Two patients discontinued the study (both
in the lisinopril group) because of preg-
nancy and a wish to become pregnant
Selective reporting (reporting bias) Unclear risk Reporting all outcomes described in the
methods
UKPDS Study 1998
Methods • Study design: parallel RCT
• Follow-up period: 48 months
Participants Inclusion criteria
• Setting: multicentre
• Country: UK
• Proportion with normoalbuminuria, microalbuminuria or macroalbuminuria not
available; all type 2 diabetes; all hypertensive
• Number: treatment group (758); control group (390)
• Mean age SD (years): treatment group (56.3 ± 8.1); control group (56.0 ± 8.2)
• Sex (M/F): treatment group (205/195); control group (205/153)
Exclusion criteria
• Clinical requirement for strict BP control or beta blockade; severe vascular
disease; a severe concurrent illness or contraindications to beta blockers; pregnancy; or
unwillingness to join the study
Interventions Treatment group
• Captopril: 25-50 mg x 2/d
Control group
• Atenolol: 50-100 mg/d
Outcomes • Death
• Onset of micro or macroalbuminuria
• BP
Notes • BP target equalization achieved in study (use of other antihypertensive co-
interventions)
• End of treatment HbA1c: treatment group (8.3%); control group (8.%)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Low risk ’Randomisation stratified for those with or
without previous treatment for hyperten-
sion was performed by the coordinating
centre’
Allocation concealment (selection bias) Low risk Sealed opaque envelopes were used
52Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
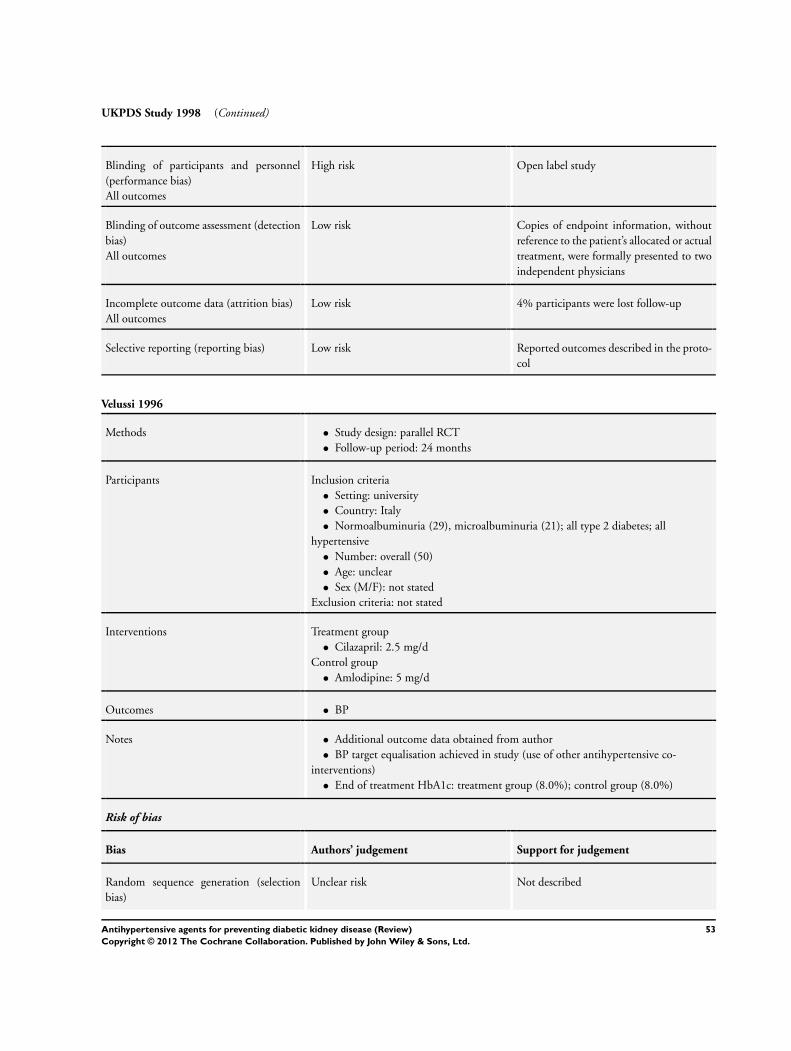
UKPDS Study 1998 (Continued)
Blinding of participants and personnel
(performance bias)
All outcomes
High risk Open label study
Blinding of outcome assessment (detection
bias)
All outcomes
Low risk Copies of endpoint information, without
reference to the patient’s allocated or actual
treatment, were formally presented to two
independent physicians
Incomplete outcome data (attrition bias)
All outcomes
Low risk 4% participants were lost follow-up
Selective reporting (reporting bias) Low risk Reported outcomes described in the proto-
col
Velussi 1996
Methods • Study design: parallel RCT
• Follow-up period: 24 months
Participants Inclusion criteria
• Setting: university
• Country: Italy
• Normoalbuminuria (29), microalbuminuria (21); all type 2 diabetes; all
hypertensive
• Number: overall (50)
• Age: unclear
• Sex (M/F): not stated
Exclusion criteria: not stated
Interventions Treatment group
• Cilazapril: 2.5 mg/d
Control group
• Amlodipine: 5 mg/d
Outcomes • BP
Notes • Additional outcome data obtained from author
• BP target equalisation achieved in study (use of other antihypertensive co-
interventions)
• End of treatment HbA1c: treatment group (8.0%); control group (8.0%)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selection
bias)
Unclear risk Not described
53Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Velussi 1996 (Continued)
Allocation concealment (selection bias) Unclear risk Not described
Blinding of participants and personnel
(performance bias)
All outcomes
Low risk Double-blinded double-dummy design
Blinding of outcome assessment (detection
bias)
All outcomes
Unclear risk Not described
Incomplete outcome data (attrition bias)
All outcomes
High risk 6/50(12%) participants missing from the
study
Selective reporting (reporting bias) Unclear risk Reported all outcomes described in the
methods
ACEi - angiotensin-converting enzyme inhibitor; ARB - angiotensin receptor blockers; BP - blood pressure; DKD - diabetic kidney
disease; ESKD - end-stage kidney disease; SCr - serum creatinine
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
ALLHAT 2002 Baseline data on kidney disease were not available, so that we were not able to separate out the data of diabetic
patients with normoalbuminuria and could not include these data in our main analyses
CAPPP 1999 Baseline data on kidney disease were not available, so that we were not able to separate out the data of diabetic
patients with normoalbuminuria and could not include these data in our main analyses
Hansson 1999 Baseline data on kidney disease were not available, so that we were not able to separate out the data of diabetic
patients with normoalbuminuria and could not include these data in our main analyses
HOT 1998 Baseline data on kidney disease were not available, so that we were not able to separate out the data of diabetic
patients with normoalbuminuria and could not include these data in our main analyses
INSIGHT 2000 Baseline data on kidney disease were not available, so that we were not able to separate out the data of diabetic
patients with normoalbuminuria and could not include these data in our main analyses
NORDIL 2000 Baseline data on kidney disease were not available, so that we were not able to separate out the data of diabetic
patients with normoalbuminuria and could not include these data in our main analyses
Tuomilehto 1999 Baseline data on kidney disease were not available, so that we were not able to separate out the data of diabetic
patients with normoalbuminuria and could not include these data in our main analyses
54Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
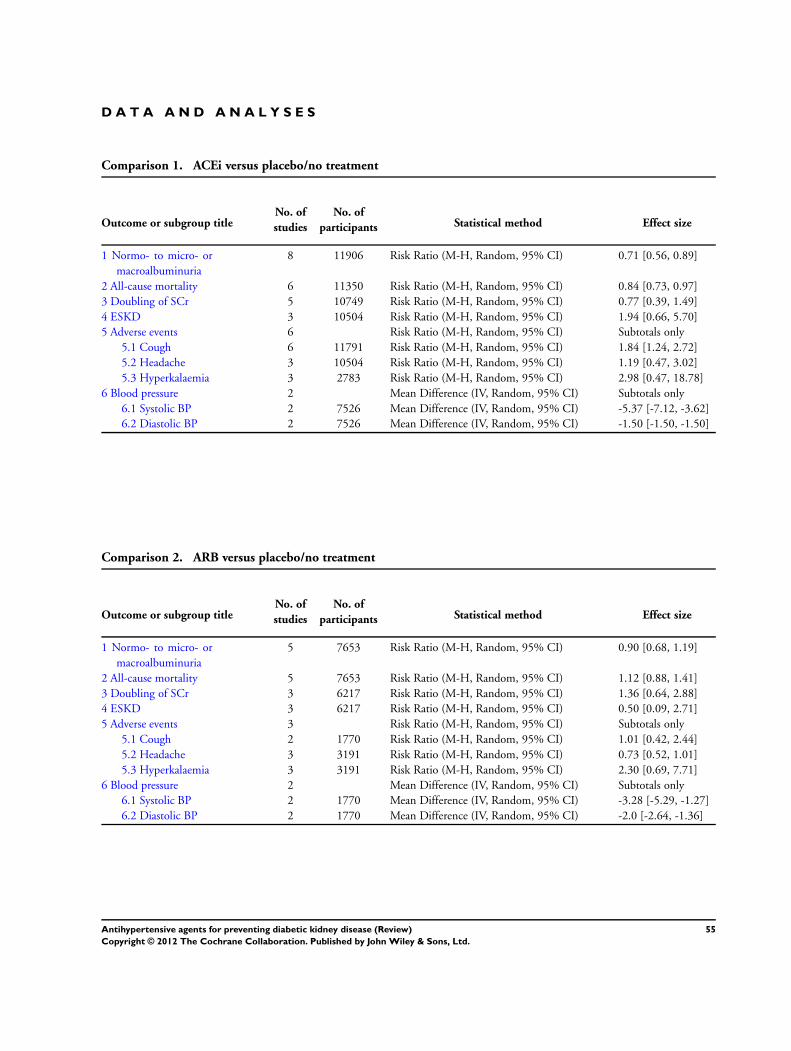
D A T A A N D A N A L Y S E S
Comparison 1. ACEi versus placebo/no treatment
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Normo- to micro- or
macroalbuminuria
8 11906 Risk Ratio (M-H, Random, 95% CI) 0.71 [0.56, 0.89]
2 All-cause mortality 6 11350 Risk Ratio (M-H, Random, 95% CI) 0.84 [0.73, 0.97]
3 Doubling of SCr 5 10749 Risk Ratio (M-H, Random, 95% CI) 0.77 [0.39, 1.49]
4 ESKD 3 10504 Risk Ratio (M-H, Random, 95% CI) 1.94 [0.66, 5.70]
5 Adverse events 6 Risk Ratio (M-H, Random, 95% CI) Subtotals only
5.1 Cough 6 11791 Risk Ratio (M-H, Random, 95% CI) 1.84 [1.24, 2.72]
5.2 Headache 3 10504 Risk Ratio (M-H, Random, 95% CI) 1.19 [0.47, 3.02]
5.3 Hyperkalaemia 3 2783 Risk Ratio (M-H, Random, 95% CI) 2.98 [0.47, 18.78]
6 Blood pressure 2 Mean Difference (IV, Random, 95% CI) Subtotals only
6.1 Systolic BP 2 7526 Mean Difference (IV, Random, 95% CI) -5.37 [-7.12, -3.62]
6.2 Diastolic BP 2 7526 Mean Difference (IV, Random, 95% CI) -1.50 [-1.50, -1.50]
Comparison 2. ARB versus placebo/no treatment
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Normo- to micro- or
macroalbuminuria
5 7653 Risk Ratio (M-H, Random, 95% CI) 0.90 [0.68, 1.19]
2 All-cause mortality 5 7653 Risk Ratio (M-H, Random, 95% CI) 1.12 [0.88, 1.41]
3 Doubling of SCr 3 6217 Risk Ratio (M-H, Random, 95% CI) 1.36 [0.64, 2.88]
4 ESKD 3 6217 Risk Ratio (M-H, Random, 95% CI) 0.50 [0.09, 2.71]
5 Adverse events 3 Risk Ratio (M-H, Random, 95% CI) Subtotals only
5.1 Cough 2 1770 Risk Ratio (M-H, Random, 95% CI) 1.01 [0.42, 2.44]
5.2 Headache 3 3191 Risk Ratio (M-H, Random, 95% CI) 0.73 [0.52, 1.01]
5.3 Hyperkalaemia 3 3191 Risk Ratio (M-H, Random, 95% CI) 2.30 [0.69, 7.71]
6 Blood pressure 2 Mean Difference (IV, Random, 95% CI) Subtotals only
6.1 Systolic BP 2 1770 Mean Difference (IV, Random, 95% CI) -3.28 [-5.29, -1.27]
6.2 Diastolic BP 2 1770 Mean Difference (IV, Random, 95% CI) -2.0 [-2.64, -1.36]
55Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
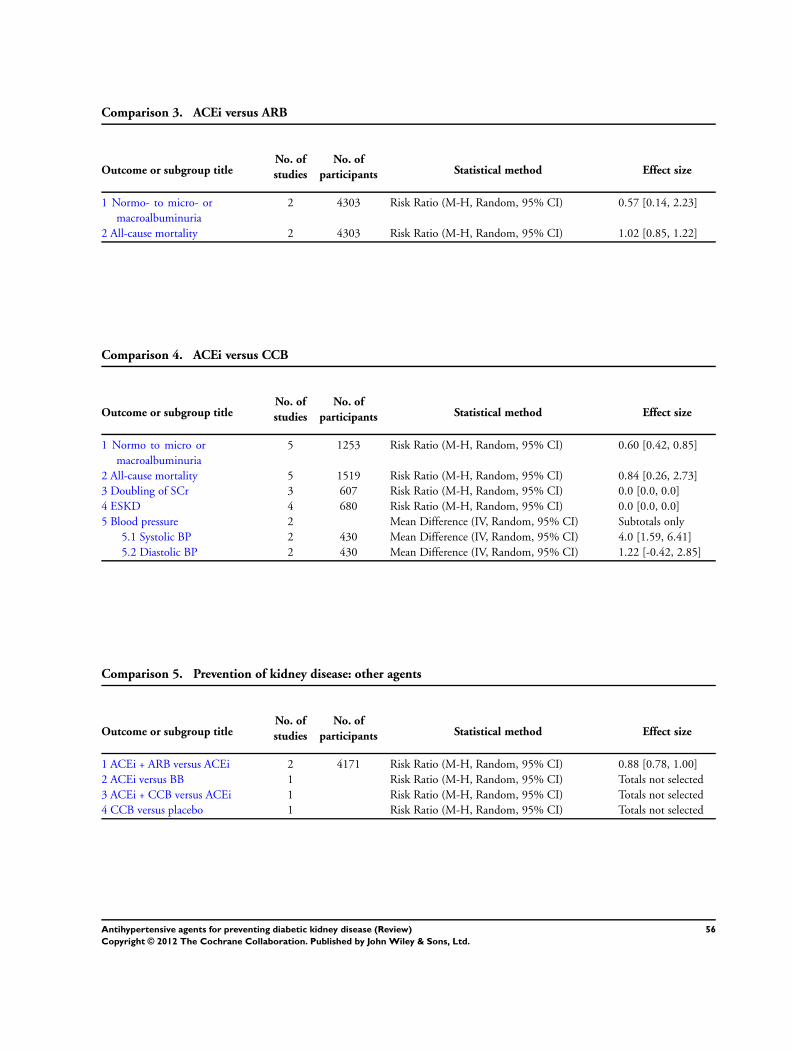
Comparison 3. ACEi versus ARB
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Normo- to micro- or
macroalbuminuria
2 4303 Risk Ratio (M-H, Random, 95% CI) 0.57 [0.14, 2.23]
2 All-cause mortality 2 4303 Risk Ratio (M-H, Random, 95% CI) 1.02 [0.85, 1.22]
Comparison 4. ACEi versus CCB
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Normo to micro or
macroalbuminuria
5 1253 Risk Ratio (M-H, Random, 95% CI) 0.60 [0.42, 0.85]
2 All-cause mortality 5 1519 Risk Ratio (M-H, Random, 95% CI) 0.84 [0.26, 2.73]
3 Doubling of SCr 3 607 Risk Ratio (M-H, Random, 95% CI) 0.0 [0.0, 0.0]
4 ESKD 4 680 Risk Ratio (M-H, Random, 95% CI) 0.0 [0.0, 0.0]
5 Blood pressure 2 Mean Difference (IV, Random, 95% CI) Subtotals only
5.1 Systolic BP 2 430 Mean Difference (IV, Random, 95% CI) 4.0 [1.59, 6.41]
5.2 Diastolic BP 2 430 Mean Difference (IV, Random, 95% CI) 1.22 [-0.42, 2.85]
Comparison 5. Prevention of kidney disease: other agents
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 ACEi + ARB versus ACEi 2 4171 Risk Ratio (M-H, Random, 95% CI) 0.88 [0.78, 1.00]
2 ACEi versus BB 1 Risk Ratio (M-H, Random, 95% CI) Totals not selected
3 ACEi + CCB versus ACEi 1 Risk Ratio (M-H, Random, 95% CI) Totals not selected
4 CCB versus placebo 1 Risk Ratio (M-H, Random, 95% CI) Totals not selected
56Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
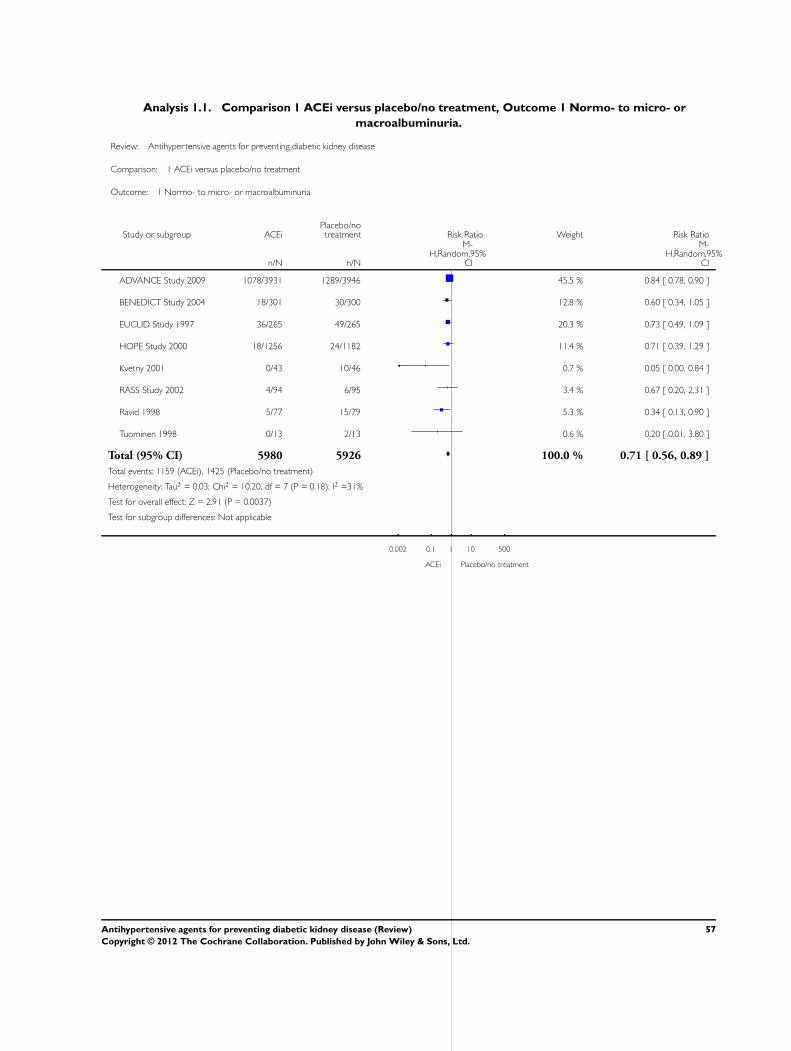
Analysis 1.1. Comparison 1 ACEi versus placebo/no treatment, Outcome 1 Normo- to micro- or
macroalbuminuria.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 1 ACEi versus placebo/no treatment
Outcome: 1 Normo- to micro- or macroalbuminuria
Study or subgroup ACEiPlacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
ADVANCE Study 2009 1078/3931 1289/3946 45.5 % 0.84 [ 0.78, 0.90 ]
BENEDICT Study 2004 18/301 30/300 12.8 % 0.60 [ 0.34, 1.05 ]
EUCLID Study 1997 36/265 49/265 20.3 % 0.73 [ 0.49, 1.09 ]
HOPE Study 2000 18/1256 24/1182 11.4 % 0.71 [ 0.39, 1.29 ]
Kvetny 2001 0/43 10/46 0.7 % 0.05 [ 0.00, 0.84 ]
RASS Study 2002 4/94 6/95 3.4 % 0.67 [ 0.20, 2.31 ]
Ravid 1998 5/77 15/79 5.3 % 0.34 [ 0.13, 0.90 ]
Tuominen 1998 0/13 2/13 0.6 % 0.20 [ 0.01, 3.80 ]
Total (95% CI) 5980 5926 100.0 % 0.71 [ 0.56, 0.89 ]
Total events: 1159 (ACEi), 1425 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.03; Chi2 = 10.20, df = 7 (P = 0.18); I2 =31%
Test for overall effect: Z = 2.91 (P = 0.0037)
Test for subgroup differences: Not applicable
0.002 0.1 1 10 500
ACEi Placebo/no treatment
57Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
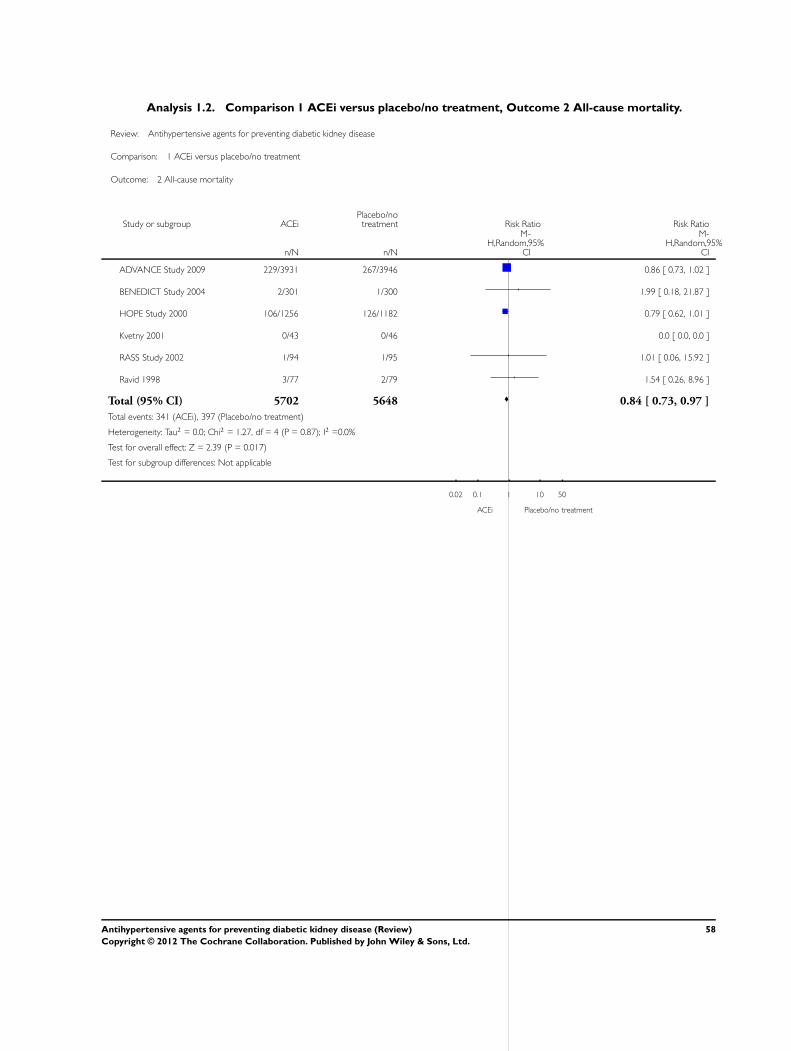
Analysis 1.2. Comparison 1 ACEi versus placebo/no treatment, Outcome 2 All-cause mortality.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 1 ACEi versus placebo/no treatment
Outcome: 2 All-cause mortality
Study or subgroup ACEiPlacebo/notreatment Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
ADVANCE Study 2009 229/3931 267/3946 0.86 [ 0.73, 1.02 ]
BENEDICT Study 2004 2/301 1/300 1.99 [ 0.18, 21.87 ]
HOPE Study 2000 106/1256 126/1182 0.79 [ 0.62, 1.01 ]
Kvetny 2001 0/43 0/46 0.0 [ 0.0, 0.0 ]
RASS Study 2002 1/94 1/95 1.01 [ 0.06, 15.92 ]
Ravid 1998 3/77 2/79 1.54 [ 0.26, 8.96 ]
Total (95% CI) 5702 5648 0.84 [ 0.73, 0.97 ]
Total events: 341 (ACEi), 397 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.0; Chi2 = 1.27, df = 4 (P = 0.87); I2 =0.0%
Test for overall effect: Z = 2.39 (P = 0.017)
Test for subgroup differences: Not applicable
0.02 0.1 1 10 50
ACEi Placebo/no treatment
58Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
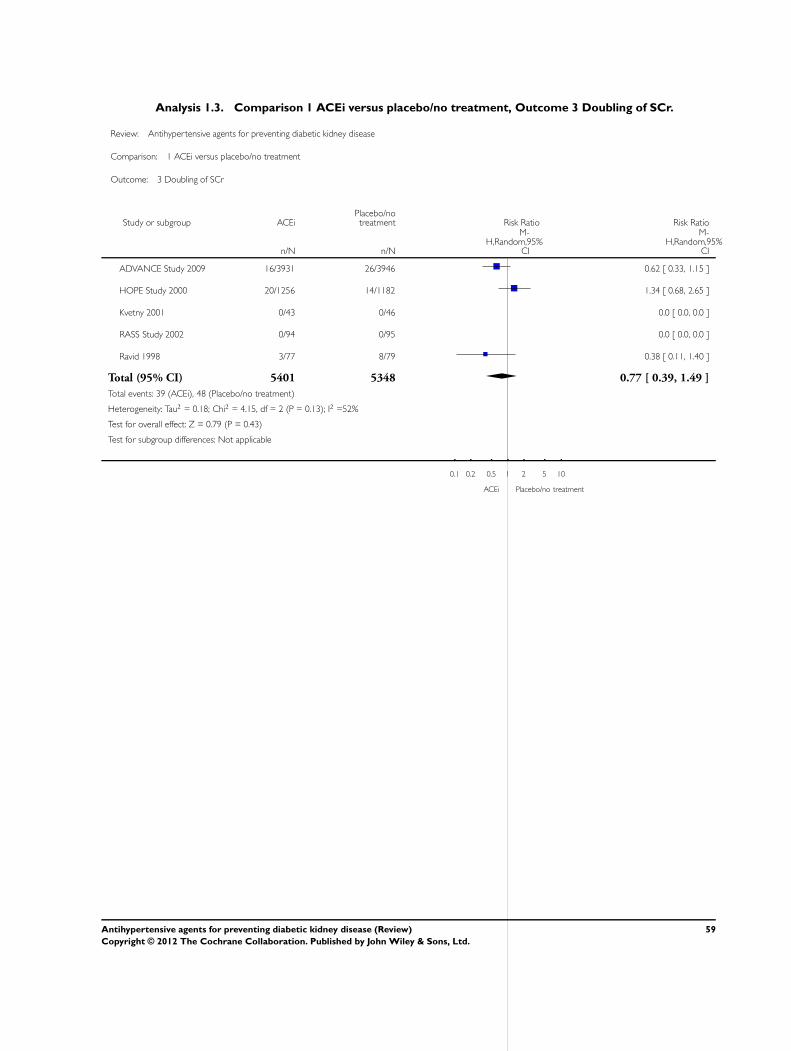
Analysis 1.3. Comparison 1 ACEi versus placebo/no treatment, Outcome 3 Doubling of SCr.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 1 ACEi versus placebo/no treatment
Outcome: 3 Doubling of SCr
Study or subgroup ACEiPlacebo/notreatment Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
ADVANCE Study 2009 16/3931 26/3946 0.62 [ 0.33, 1.15 ]
HOPE Study 2000 20/1256 14/1182 1.34 [ 0.68, 2.65 ]
Kvetny 2001 0/43 0/46 0.0 [ 0.0, 0.0 ]
RASS Study 2002 0/94 0/95 0.0 [ 0.0, 0.0 ]
Ravid 1998 3/77 8/79 0.38 [ 0.11, 1.40 ]
Total (95% CI) 5401 5348 0.77 [ 0.39, 1.49 ]
Total events: 39 (ACEi), 48 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.18; Chi2 = 4.15, df = 2 (P = 0.13); I2 =52%
Test for overall effect: Z = 0.79 (P = 0.43)
Test for subgroup differences: Not applicable
0.1 0.2 0.5 1 2 5 10
ACEi Placebo/no treatment
59Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
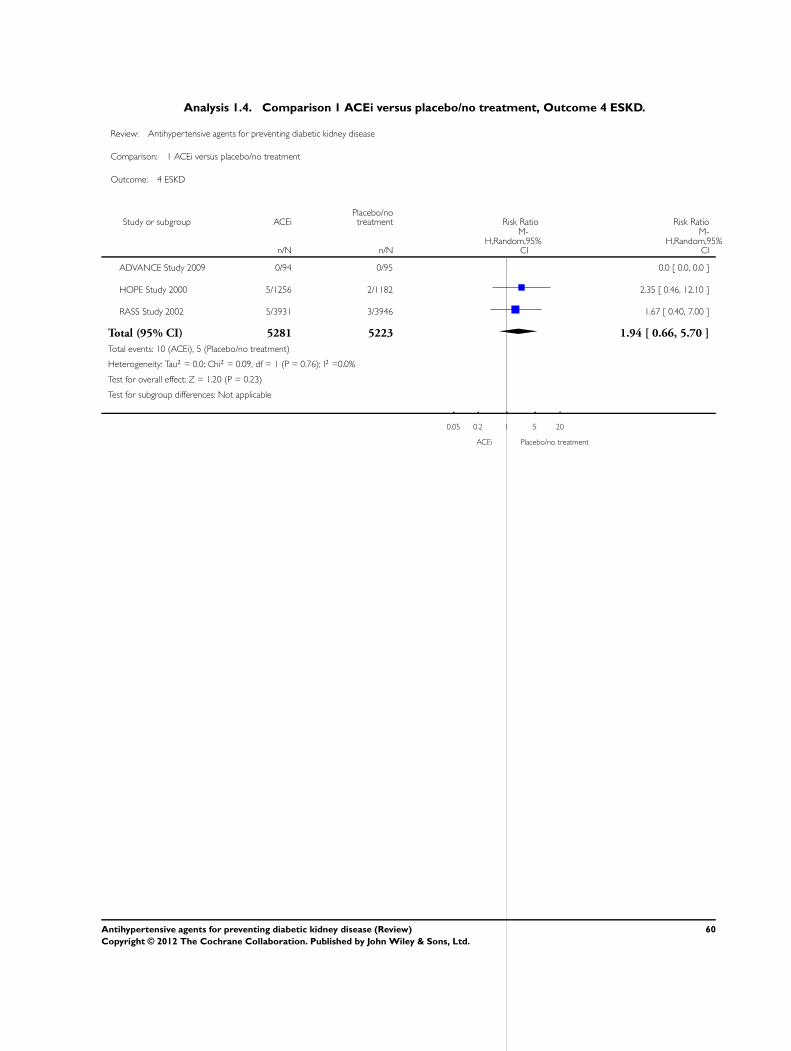
Analysis 1.4. Comparison 1 ACEi versus placebo/no treatment, Outcome 4 ESKD.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 1 ACEi versus placebo/no treatment
Outcome: 4 ESKD
Study or subgroup ACEiPlacebo/notreatment Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
ADVANCE Study 2009 0/94 0/95 0.0 [ 0.0, 0.0 ]
HOPE Study 2000 5/1256 2/1182 2.35 [ 0.46, 12.10 ]
RASS Study 2002 5/3931 3/3946 1.67 [ 0.40, 7.00 ]
Total (95% CI) 5281 5223 1.94 [ 0.66, 5.70 ]
Total events: 10 (ACEi), 5 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.09, df = 1 (P = 0.76); I2 =0.0%
Test for overall effect: Z = 1.20 (P = 0.23)
Test for subgroup differences: Not applicable
0.05 0.2 1 5 20
ACEi Placebo/no treatment
60Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.5. Comparison 1 ACEi versus placebo/no treatment, Outcome 5 Adverse events.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 1 ACEi versus placebo/no treatment
Outcome: 5 Adverse events
Study or subgroup ACEiPlacebo/notreatment Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
1 Cough
ADVANCE Study 2009 1/3931 3/3946 0.33 [ 0.03, 3.22 ]
BENEDICT Study 2004 4/301 2/300 1.99 [ 0.37, 10.80 ]
EUCLID Study 1997 21/265 7/265 3.00 [ 1.30, 6.94 ]
HOPE Study 2000 37/1256 24/1182 1.45 [ 0.87, 2.41 ]
RASS Study 2002 12/94 4/95 3.03 [ 1.01, 9.06 ]
Ravid 1998 4/77 2/79 2.05 [ 0.39, 10.88 ]
Subtotal (95% CI) 5924 5867 1.84 [ 1.24, 2.72 ]
Total events: 79 (ACEi), 42 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.01; Chi2 = 5.15, df = 5 (P = 0.40); I2 =3%
Test for overall effect: Z = 3.04 (P = 0.0024)
2 Headache
ADVANCE Study 2009 2/3931 2/3946 1.00 [ 0.14, 7.12 ]
HOPE Study 2000 8/1256 6/1182 1.25 [ 0.44, 3.61 ]
RASS Study 2002 0/94 0/95 0.0 [ 0.0, 0.0 ]
Subtotal (95% CI) 5281 5223 1.19 [ 0.47, 3.02 ]
Total events: 10 (ACEi), 8 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.04, df = 1 (P = 0.84); I2 =0.0%
Test for overall effect: Z = 0.37 (P = 0.71)
3 Hyperkalaemia
HOPE Study 2000 1/1256 0/1182 2.82 [ 0.12, 69.24 ]
RASS Study 2002 1/94 0/95 3.03 [ 0.13, 73.49 ]
Ravid 1998 1/77 0/79 3.08 [ 0.13, 74.39 ]
Subtotal (95% CI) 1427 1356 2.98 [ 0.47, 18.78 ]
Total events: 3 (ACEi), 0 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.00, df = 2 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 1.16 (P = 0.25)
0.01 0.1 1 10 100
ACEi Placebo/no treatment
61Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
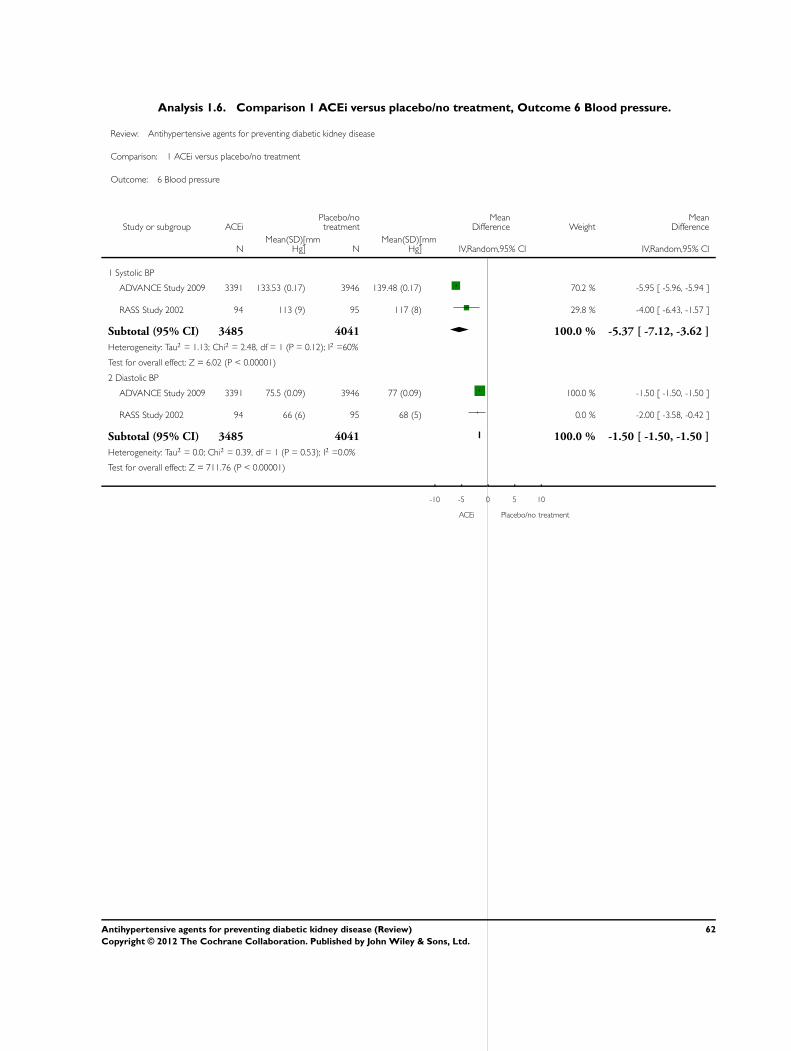
Analysis 1.6. Comparison 1 ACEi versus placebo/no treatment, Outcome 6 Blood pressure.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 1 ACEi versus placebo/no treatment
Outcome: 6 Blood pressure
Study or subgroup ACEiPlacebo/notreatment
MeanDifference Weight
MeanDifference
NMean(SD)[mm
Hg] NMean(SD)[mm
Hg] IV,Random,95% CI IV,Random,95% CI
1 Systolic BP
ADVANCE Study 2009 3391 133.53 (0.17) 3946 139.48 (0.17) 70.2 % -5.95 [ -5.96, -5.94 ]
RASS Study 2002 94 113 (9) 95 117 (8) 29.8 % -4.00 [ -6.43, -1.57 ]
Subtotal (95% CI) 3485 4041 100.0 % -5.37 [ -7.12, -3.62 ]
Heterogeneity: Tau2 = 1.13; Chi2 = 2.48, df = 1 (P = 0.12); I2 =60%
Test for overall effect: Z = 6.02 (P < 0.00001)
2 Diastolic BP
ADVANCE Study 2009 3391 75.5 (0.09) 3946 77 (0.09) 100.0 % -1.50 [ -1.50, -1.50 ]
RASS Study 2002 94 66 (6) 95 68 (5) 0.0 % -2.00 [ -3.58, -0.42 ]
Subtotal (95% CI) 3485 4041 100.0 % -1.50 [ -1.50, -1.50 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 0.39, df = 1 (P = 0.53); I2 =0.0%
Test for overall effect: Z = 711.76 (P < 0.00001)
-10 -5 0 5 10
ACEi Placebo/no treatment
62Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
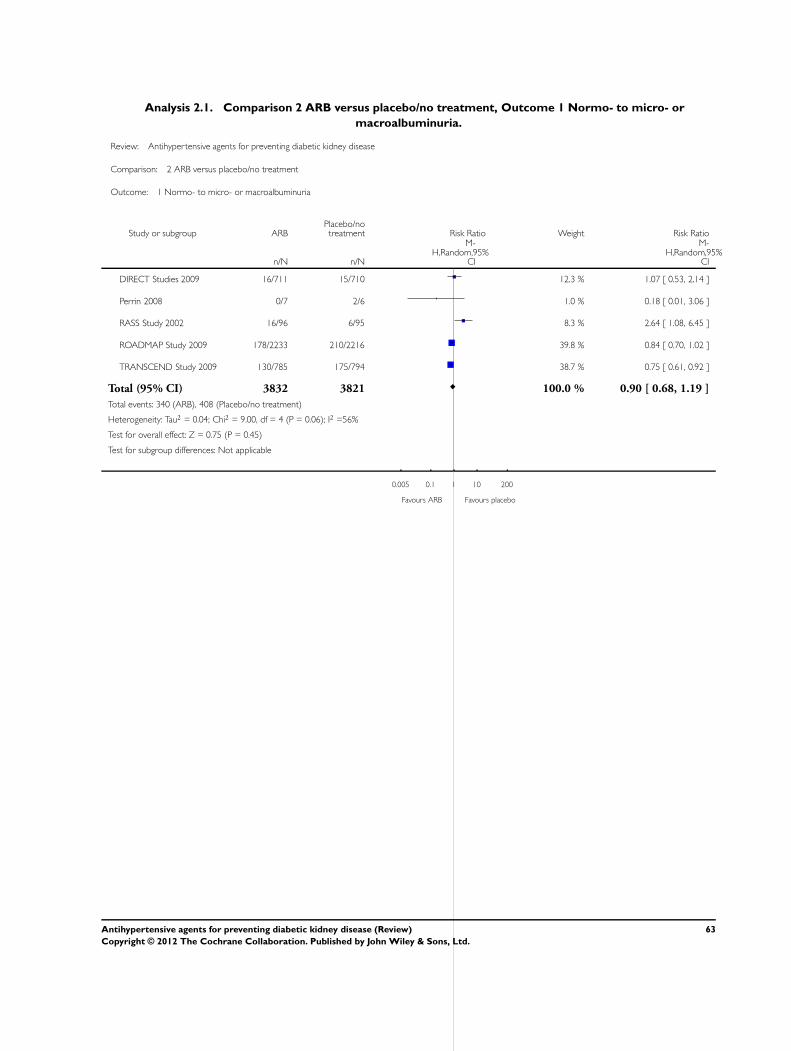
Analysis 2.1. Comparison 2 ARB versus placebo/no treatment, Outcome 1 Normo- to micro- or
macroalbuminuria.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 2 ARB versus placebo/no treatment
Outcome: 1 Normo- to micro- or macroalbuminuria
Study or subgroup ARBPlacebo/notreatment Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
DIRECT Studies 2009 16/711 15/710 12.3 % 1.07 [ 0.53, 2.14 ]
Perrin 2008 0/7 2/6 1.0 % 0.18 [ 0.01, 3.06 ]
RASS Study 2002 16/96 6/95 8.3 % 2.64 [ 1.08, 6.45 ]
ROADMAP Study 2009 178/2233 210/2216 39.8 % 0.84 [ 0.70, 1.02 ]
TRANSCEND Study 2009 130/785 175/794 38.7 % 0.75 [ 0.61, 0.92 ]
Total (95% CI) 3832 3821 100.0 % 0.90 [ 0.68, 1.19 ]
Total events: 340 (ARB), 408 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.04; Chi2 = 9.00, df = 4 (P = 0.06); I2 =56%
Test for overall effect: Z = 0.75 (P = 0.45)
Test for subgroup differences: Not applicable
0.005 0.1 1 10 200
Favours ARB Favours placebo
63Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
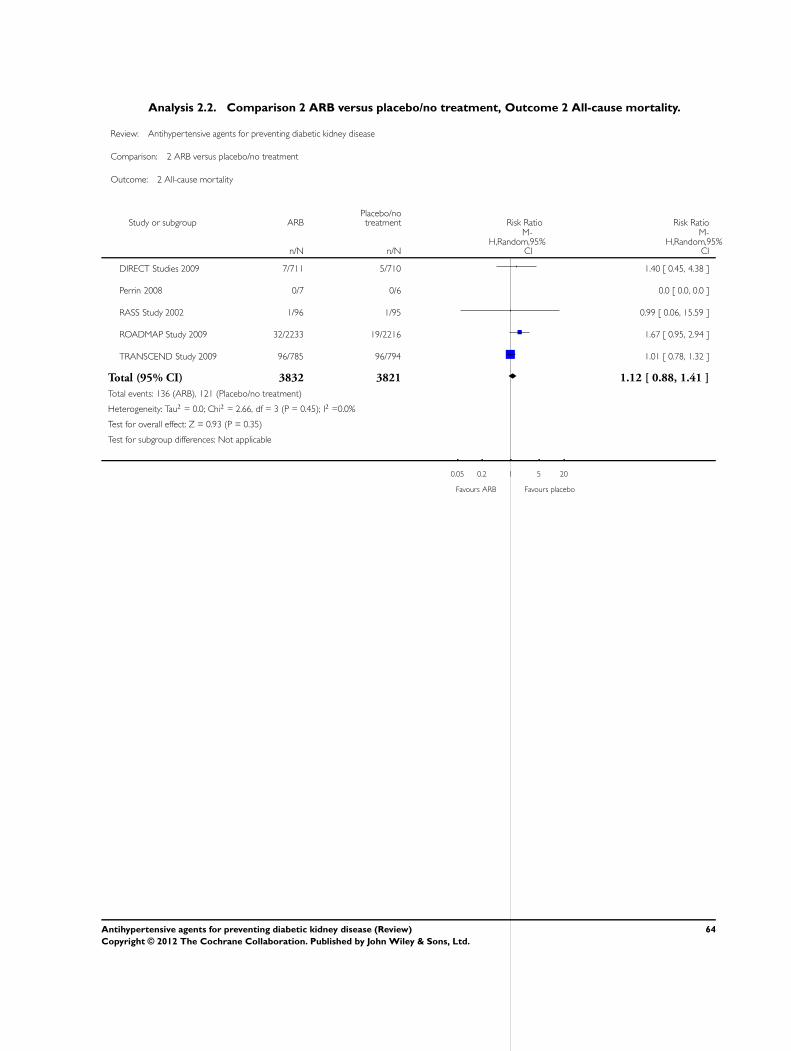
Analysis 2.2. Comparison 2 ARB versus placebo/no treatment, Outcome 2 All-cause mortality.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 2 ARB versus placebo/no treatment
Outcome: 2 All-cause mortality
Study or subgroup ARBPlacebo/notreatment Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
DIRECT Studies 2009 7/711 5/710 1.40 [ 0.45, 4.38 ]
Perrin 2008 0/7 0/6 0.0 [ 0.0, 0.0 ]
RASS Study 2002 1/96 1/95 0.99 [ 0.06, 15.59 ]
ROADMAP Study 2009 32/2233 19/2216 1.67 [ 0.95, 2.94 ]
TRANSCEND Study 2009 96/785 96/794 1.01 [ 0.78, 1.32 ]
Total (95% CI) 3832 3821 1.12 [ 0.88, 1.41 ]
Total events: 136 (ARB), 121 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.0; Chi2 = 2.66, df = 3 (P = 0.45); I2 =0.0%
Test for overall effect: Z = 0.93 (P = 0.35)
Test for subgroup differences: Not applicable
0.05 0.2 1 5 20
Favours ARB Favours placebo
64Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
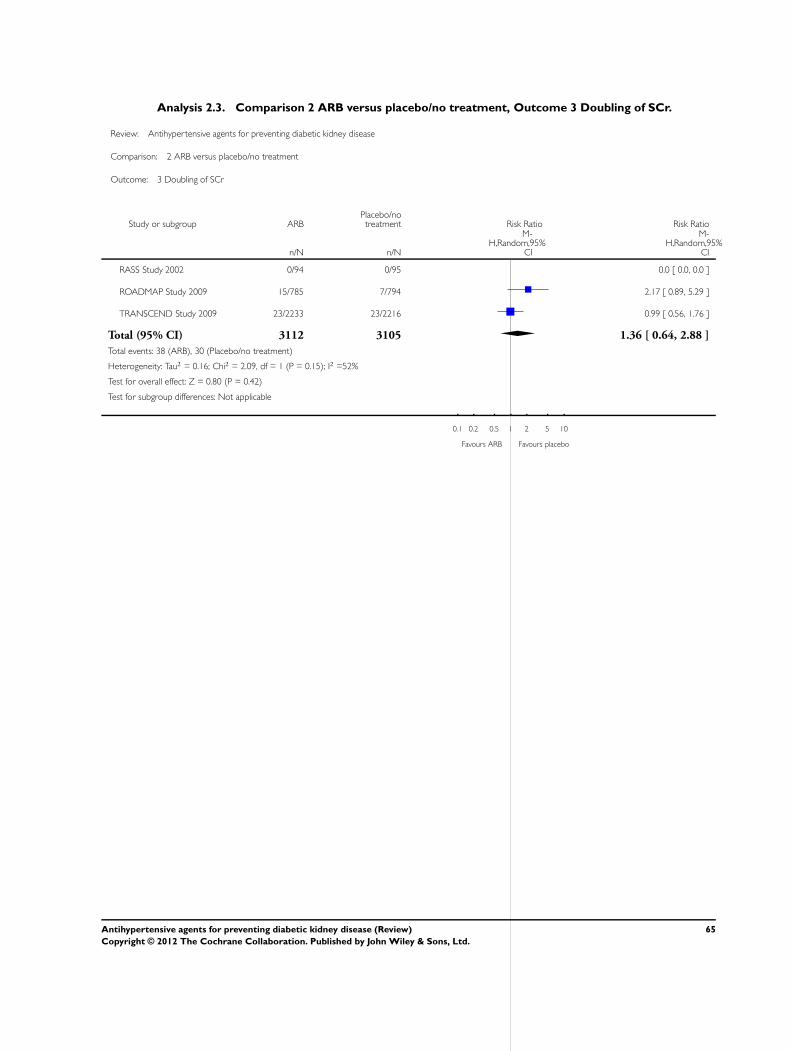
Analysis 2.3. Comparison 2 ARB versus placebo/no treatment, Outcome 3 Doubling of SCr.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 2 ARB versus placebo/no treatment
Outcome: 3 Doubling of SCr
Study or subgroup ARBPlacebo/notreatment Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
RASS Study 2002 0/94 0/95 0.0 [ 0.0, 0.0 ]
ROADMAP Study 2009 15/785 7/794 2.17 [ 0.89, 5.29 ]
TRANSCEND Study 2009 23/2233 23/2216 0.99 [ 0.56, 1.76 ]
Total (95% CI) 3112 3105 1.36 [ 0.64, 2.88 ]
Total events: 38 (ARB), 30 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.16; Chi2 = 2.09, df = 1 (P = 0.15); I2 =52%
Test for overall effect: Z = 0.80 (P = 0.42)
Test for subgroup differences: Not applicable
0.1 0.2 0.5 1 2 5 10
Favours ARB Favours placebo
65Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
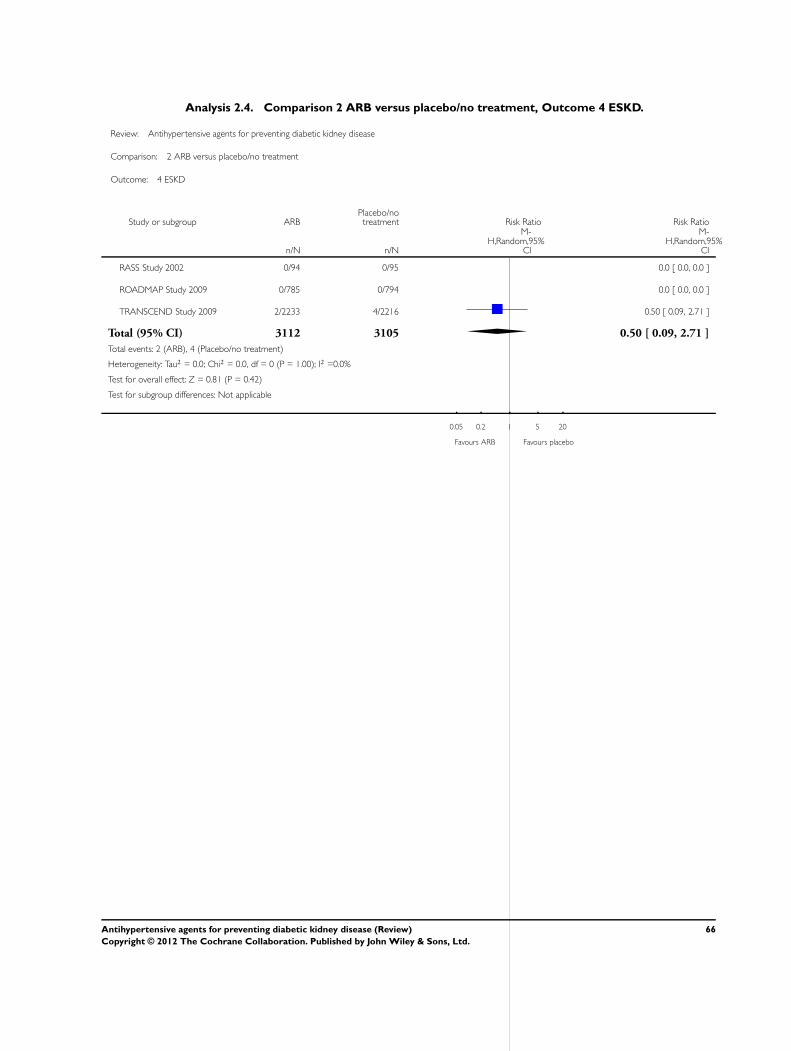
Analysis 2.4. Comparison 2 ARB versus placebo/no treatment, Outcome 4 ESKD.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 2 ARB versus placebo/no treatment
Outcome: 4 ESKD
Study or subgroup ARBPlacebo/notreatment Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
RASS Study 2002 0/94 0/95 0.0 [ 0.0, 0.0 ]
ROADMAP Study 2009 0/785 0/794 0.0 [ 0.0, 0.0 ]
TRANSCEND Study 2009 2/2233 4/2216 0.50 [ 0.09, 2.71 ]
Total (95% CI) 3112 3105 0.50 [ 0.09, 2.71 ]
Total events: 2 (ARB), 4 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.0, df = 0 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 0.81 (P = 0.42)
Test for subgroup differences: Not applicable
0.05 0.2 1 5 20
Favours ARB Favours placebo
66Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
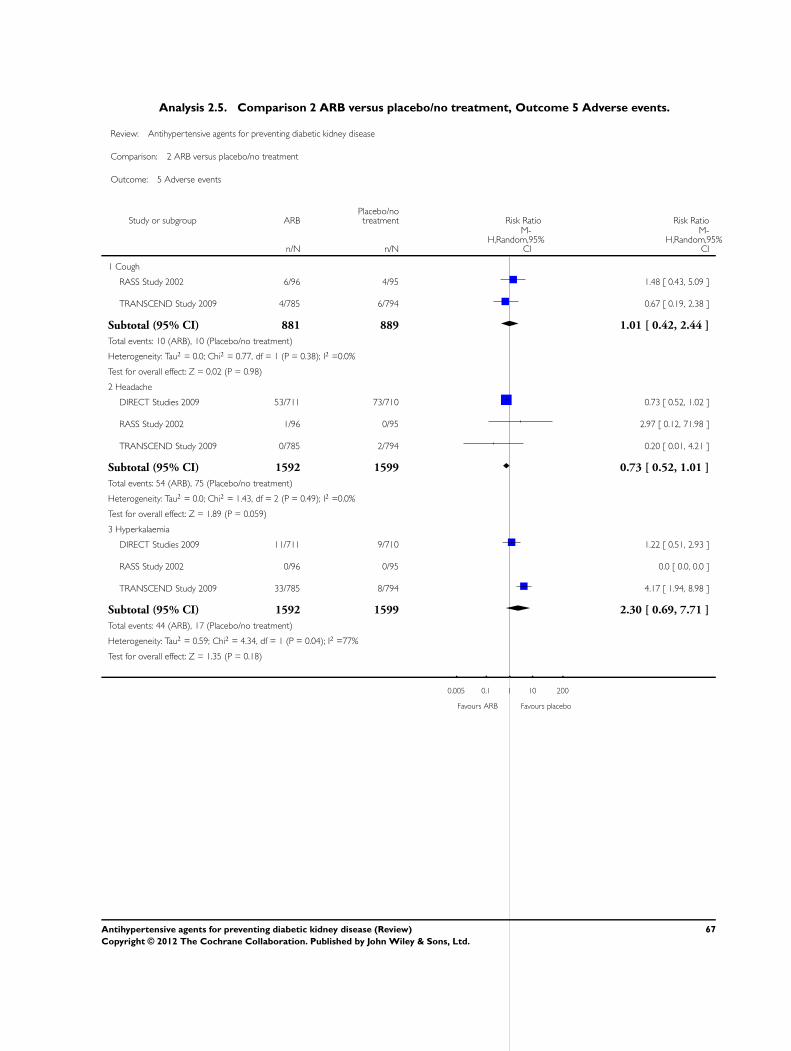
Analysis 2.5. Comparison 2 ARB versus placebo/no treatment, Outcome 5 Adverse events.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 2 ARB versus placebo/no treatment
Outcome: 5 Adverse events
Study or subgroup ARBPlacebo/notreatment Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
1 Cough
RASS Study 2002 6/96 4/95 1.48 [ 0.43, 5.09 ]
TRANSCEND Study 2009 4/785 6/794 0.67 [ 0.19, 2.38 ]
Subtotal (95% CI) 881 889 1.01 [ 0.42, 2.44 ]
Total events: 10 (ARB), 10 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.77, df = 1 (P = 0.38); I2 =0.0%
Test for overall effect: Z = 0.02 (P = 0.98)
2 Headache
DIRECT Studies 2009 53/711 73/710 0.73 [ 0.52, 1.02 ]
RASS Study 2002 1/96 0/95 2.97 [ 0.12, 71.98 ]
TRANSCEND Study 2009 0/785 2/794 0.20 [ 0.01, 4.21 ]
Subtotal (95% CI) 1592 1599 0.73 [ 0.52, 1.01 ]
Total events: 54 (ARB), 75 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.0; Chi2 = 1.43, df = 2 (P = 0.49); I2 =0.0%
Test for overall effect: Z = 1.89 (P = 0.059)
3 Hyperkalaemia
DIRECT Studies 2009 11/711 9/710 1.22 [ 0.51, 2.93 ]
RASS Study 2002 0/96 0/95 0.0 [ 0.0, 0.0 ]
TRANSCEND Study 2009 33/785 8/794 4.17 [ 1.94, 8.98 ]
Subtotal (95% CI) 1592 1599 2.30 [ 0.69, 7.71 ]
Total events: 44 (ARB), 17 (Placebo/no treatment)
Heterogeneity: Tau2 = 0.59; Chi2 = 4.34, df = 1 (P = 0.04); I2 =77%
Test for overall effect: Z = 1.35 (P = 0.18)
0.005 0.1 1 10 200
Favours ARB Favours placebo
67Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
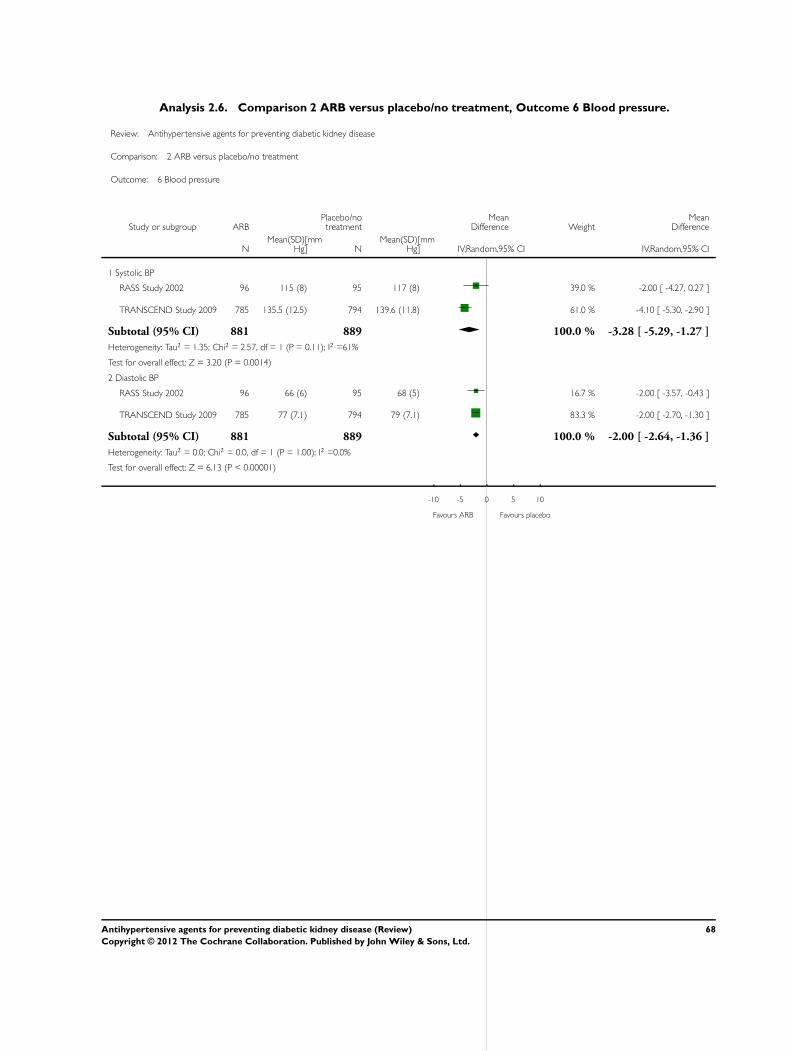
Analysis 2.6. Comparison 2 ARB versus placebo/no treatment, Outcome 6 Blood pressure.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 2 ARB versus placebo/no treatment
Outcome: 6 Blood pressure
Study or subgroup ARBPlacebo/notreatment
MeanDifference Weight
MeanDifference
NMean(SD)[mm
Hg] NMean(SD)[mm
Hg] IV,Random,95% CI IV,Random,95% CI
1 Systolic BP
RASS Study 2002 96 115 (8) 95 117 (8) 39.0 % -2.00 [ -4.27, 0.27 ]
TRANSCEND Study 2009 785 135.5 (12.5) 794 139.6 (11.8) 61.0 % -4.10 [ -5.30, -2.90 ]
Subtotal (95% CI) 881 889 100.0 % -3.28 [ -5.29, -1.27 ]
Heterogeneity: Tau2 = 1.35; Chi2 = 2.57, df = 1 (P = 0.11); I2 =61%
Test for overall effect: Z = 3.20 (P = 0.0014)
2 Diastolic BP
RASS Study 2002 96 66 (6) 95 68 (5) 16.7 % -2.00 [ -3.57, -0.43 ]
TRANSCEND Study 2009 785 77 (7.1) 794 79 (7.1) 83.3 % -2.00 [ -2.70, -1.30 ]
Subtotal (95% CI) 881 889 100.0 % -2.00 [ -2.64, -1.36 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 0.0, df = 1 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 6.13 (P < 0.00001)
-10 -5 0 5 10
Favours ARB Favours placebo
68Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
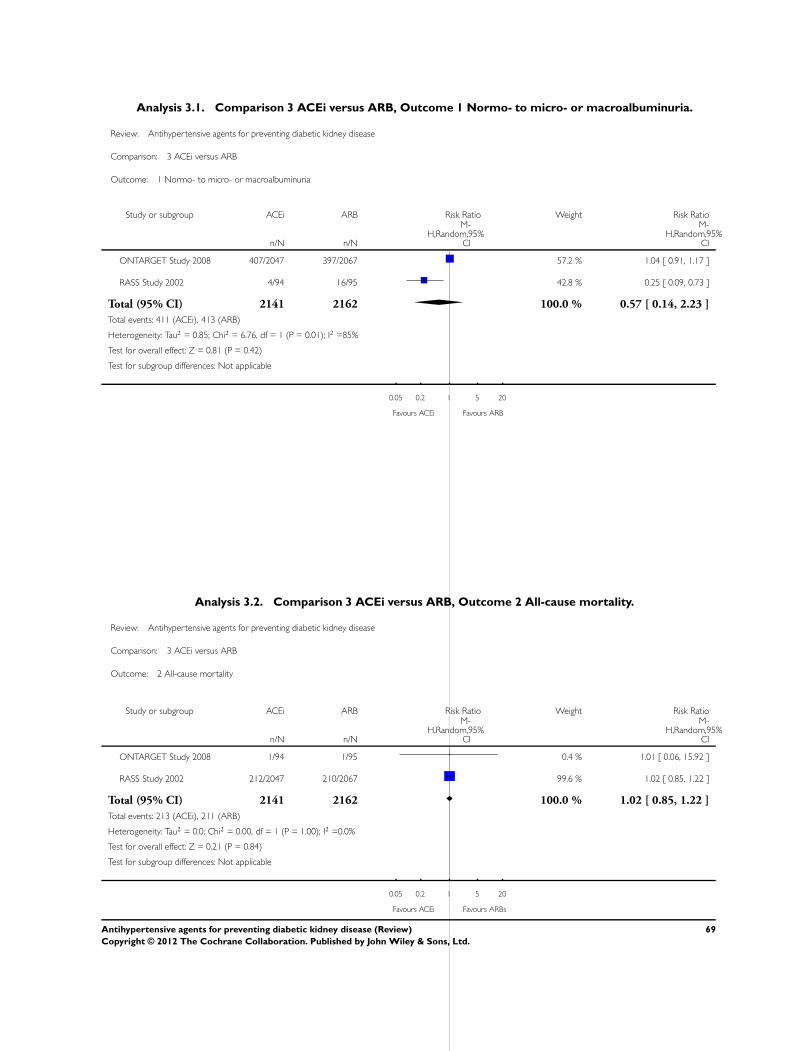
Analysis 3.1. Comparison 3 ACEi versus ARB, Outcome 1 Normo- to micro- or macroalbuminuria.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 3 ACEi versus ARB
Outcome: 1 Normo- to micro- or macroalbuminuria
Study or subgroup ACEi ARB Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
ONTARGET Study 2008 407/2047 397/2067 57.2 % 1.04 [ 0.91, 1.17 ]
RASS Study 2002 4/94 16/95 42.8 % 0.25 [ 0.09, 0.73 ]
Total (95% CI) 2141 2162 100.0 % 0.57 [ 0.14, 2.23 ]
Total events: 411 (ACEi), 413 (ARB)
Heterogeneity: Tau2 = 0.85; Chi2 = 6.76, df = 1 (P = 0.01); I2 =85%
Test for overall effect: Z = 0.81 (P = 0.42)
Test for subgroup differences: Not applicable
0.05 0.2 1 5 20
Favours ACEi Favours ARB
Analysis 3.2. Comparison 3 ACEi versus ARB, Outcome 2 All-cause mortality.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 3 ACEi versus ARB
Outcome: 2 All-cause mortality
Study or subgroup ACEi ARB Risk Ratio Weight Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
ONTARGET Study 2008 1/94 1/95 0.4 % 1.01 [ 0.06, 15.92 ]
RASS Study 2002 212/2047 210/2067 99.6 % 1.02 [ 0.85, 1.22 ]
Total (95% CI) 2141 2162 100.0 % 1.02 [ 0.85, 1.22 ]
Total events: 213 (ACEi), 211 (ARB)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.00, df = 1 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 0.21 (P = 0.84)
Test for subgroup differences: Not applicable
0.05 0.2 1 5 20
Favours ACEi Favours ARBs
69Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
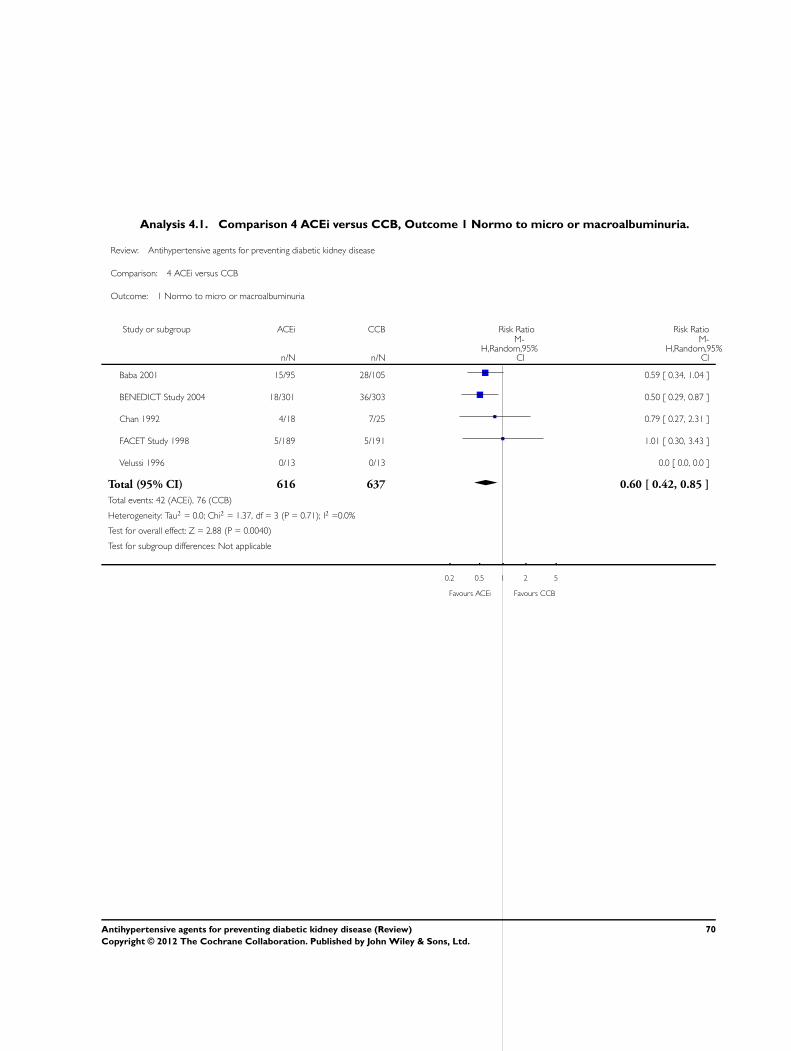
Analysis 4.1. Comparison 4 ACEi versus CCB, Outcome 1 Normo to micro or macroalbuminuria.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 4 ACEi versus CCB
Outcome: 1 Normo to micro or macroalbuminuria
Study or subgroup ACEi CCB Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
Baba 2001 15/95 28/105 0.59 [ 0.34, 1.04 ]
BENEDICT Study 2004 18/301 36/303 0.50 [ 0.29, 0.87 ]
Chan 1992 4/18 7/25 0.79 [ 0.27, 2.31 ]
FACET Study 1998 5/189 5/191 1.01 [ 0.30, 3.43 ]
Velussi 1996 0/13 0/13 0.0 [ 0.0, 0.0 ]
Total (95% CI) 616 637 0.60 [ 0.42, 0.85 ]
Total events: 42 (ACEi), 76 (CCB)
Heterogeneity: Tau2 = 0.0; Chi2 = 1.37, df = 3 (P = 0.71); I2 =0.0%
Test for overall effect: Z = 2.88 (P = 0.0040)
Test for subgroup differences: Not applicable
0.2 0.5 1 2 5
Favours ACEi Favours CCB
70Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
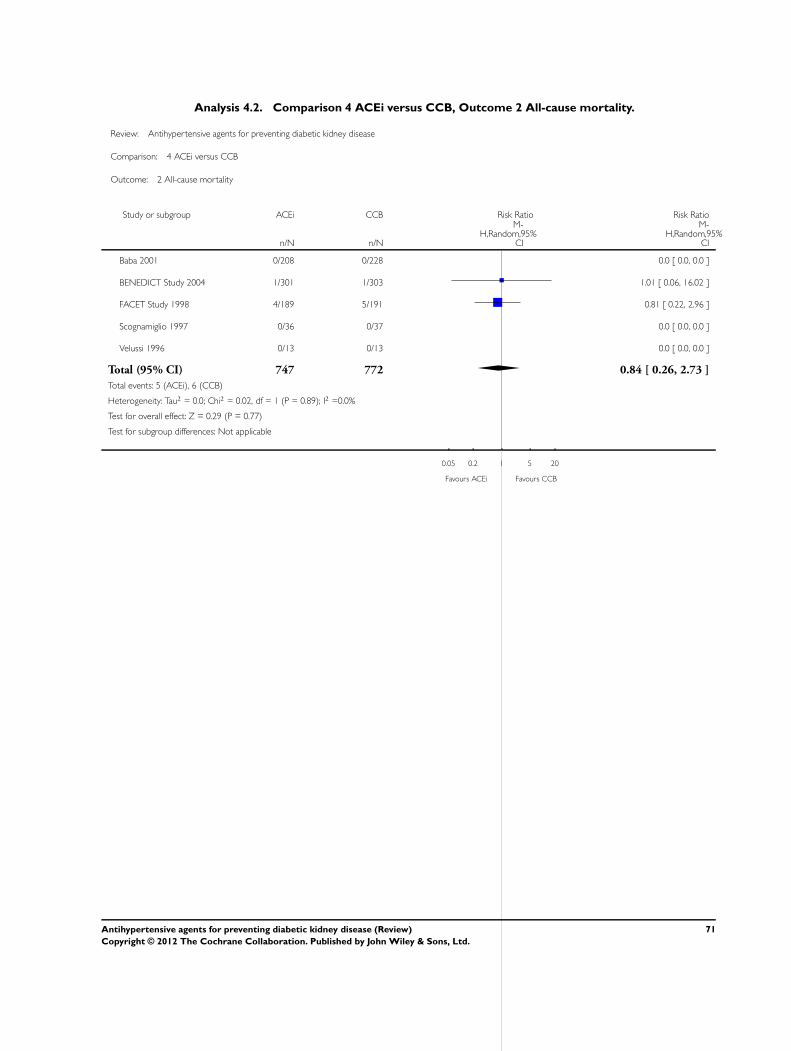
Analysis 4.2. Comparison 4 ACEi versus CCB, Outcome 2 All-cause mortality.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 4 ACEi versus CCB
Outcome: 2 All-cause mortality
Study or subgroup ACEi CCB Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
Baba 2001 0/208 0/228 0.0 [ 0.0, 0.0 ]
BENEDICT Study 2004 1/301 1/303 1.01 [ 0.06, 16.02 ]
FACET Study 1998 4/189 5/191 0.81 [ 0.22, 2.96 ]
Scognamiglio 1997 0/36 0/37 0.0 [ 0.0, 0.0 ]
Velussi 1996 0/13 0/13 0.0 [ 0.0, 0.0 ]
Total (95% CI) 747 772 0.84 [ 0.26, 2.73 ]
Total events: 5 (ACEi), 6 (CCB)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.02, df = 1 (P = 0.89); I2 =0.0%
Test for overall effect: Z = 0.29 (P = 0.77)
Test for subgroup differences: Not applicable
0.05 0.2 1 5 20
Favours ACEi Favours CCB
71Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
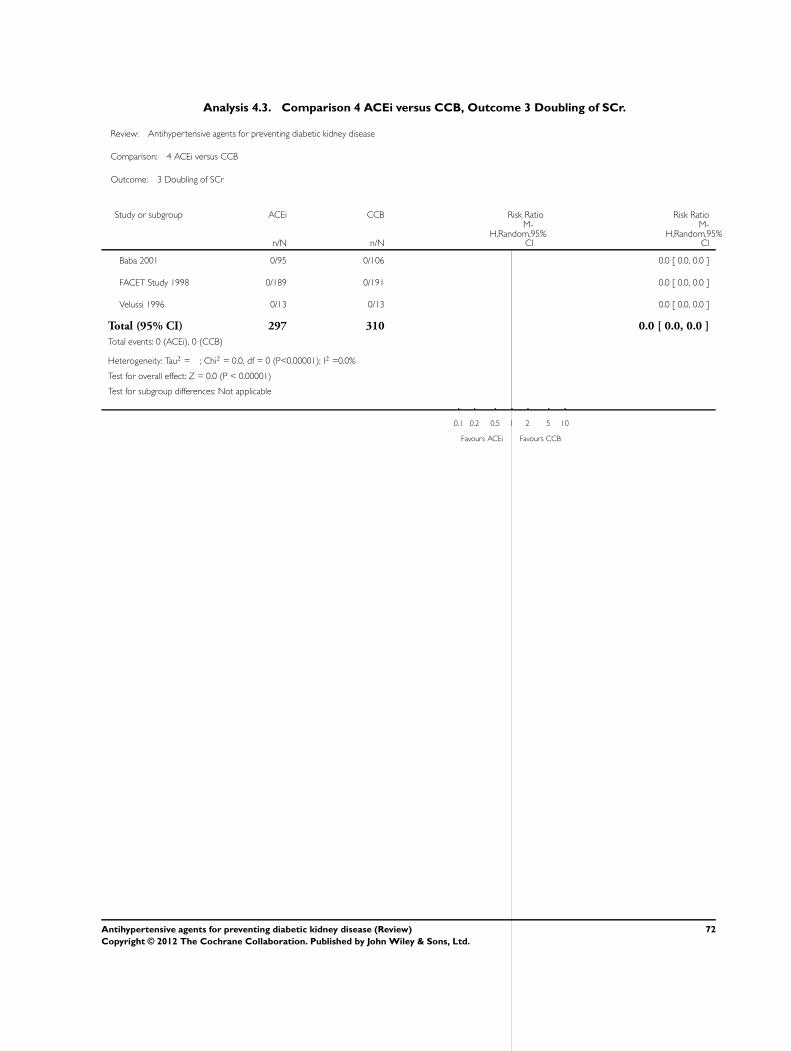
Analysis 4.3. Comparison 4 ACEi versus CCB, Outcome 3 Doubling of SCr.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 4 ACEi versus CCB
Outcome: 3 Doubling of SCr
Study or subgroup ACEi CCB Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
Baba 2001 0/95 0/106 0.0 [ 0.0, 0.0 ]
FACET Study 1998 0/189 0/191 0.0 [ 0.0, 0.0 ]
Velussi 1996 0/13 0/13 0.0 [ 0.0, 0.0 ]
Total (95% CI) 297 310 0.0 [ 0.0, 0.0 ]
Total events: 0 (ACEi), 0 (CCB)
Heterogeneity: Tau2 = ; Chi2 = 0.0, df = 0 (P<0.00001); I2 =0.0%
Test for overall effect: Z = 0.0 (P < 0.00001)
Test for subgroup differences: Not applicable
0.1 0.2 0.5 1 2 5 10
Favours ACEi Favours CCB
72Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
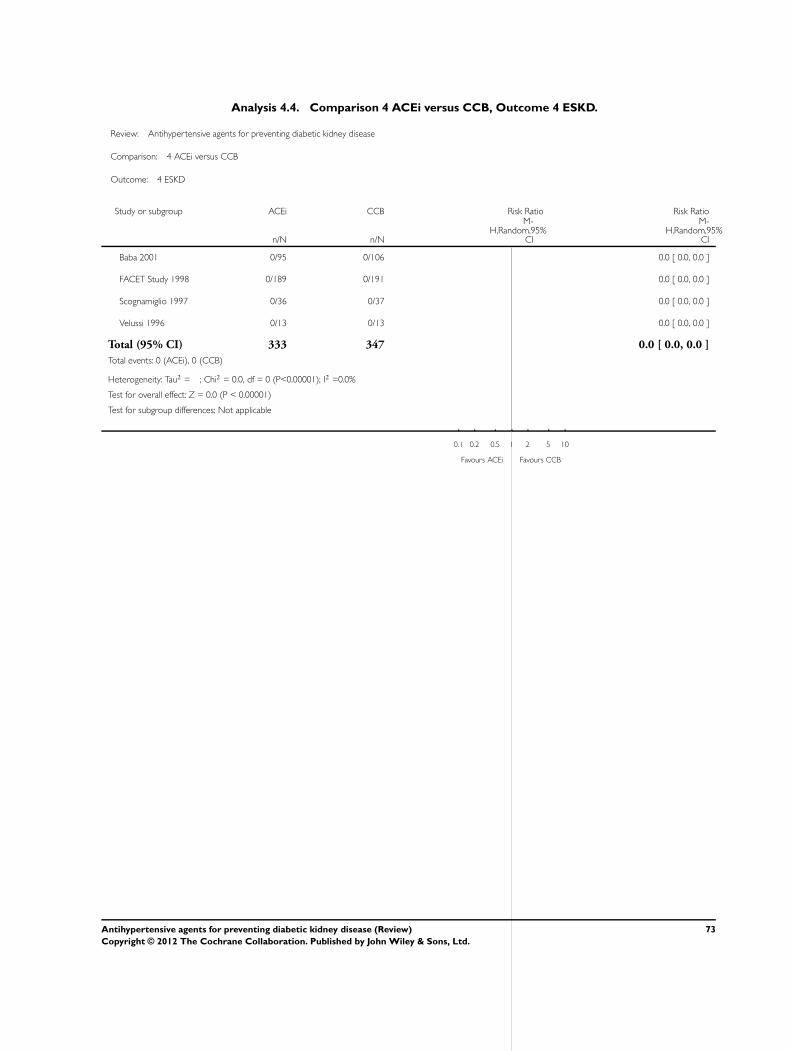
Analysis 4.4. Comparison 4 ACEi versus CCB, Outcome 4 ESKD.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 4 ACEi versus CCB
Outcome: 4 ESKD
Study or subgroup ACEi CCB Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
Baba 2001 0/95 0/106 0.0 [ 0.0, 0.0 ]
FACET Study 1998 0/189 0/191 0.0 [ 0.0, 0.0 ]
Scognamiglio 1997 0/36 0/37 0.0 [ 0.0, 0.0 ]
Velussi 1996 0/13 0/13 0.0 [ 0.0, 0.0 ]
Total (95% CI) 333 347 0.0 [ 0.0, 0.0 ]
Total events: 0 (ACEi), 0 (CCB)
Heterogeneity: Tau2 = ; Chi2 = 0.0, df = 0 (P<0.00001); I2 =0.0%
Test for overall effect: Z = 0.0 (P < 0.00001)
Test for subgroup differences: Not applicable
0.1 0.2 0.5 1 2 5 10
Favours ACEi Favours CCB
73Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
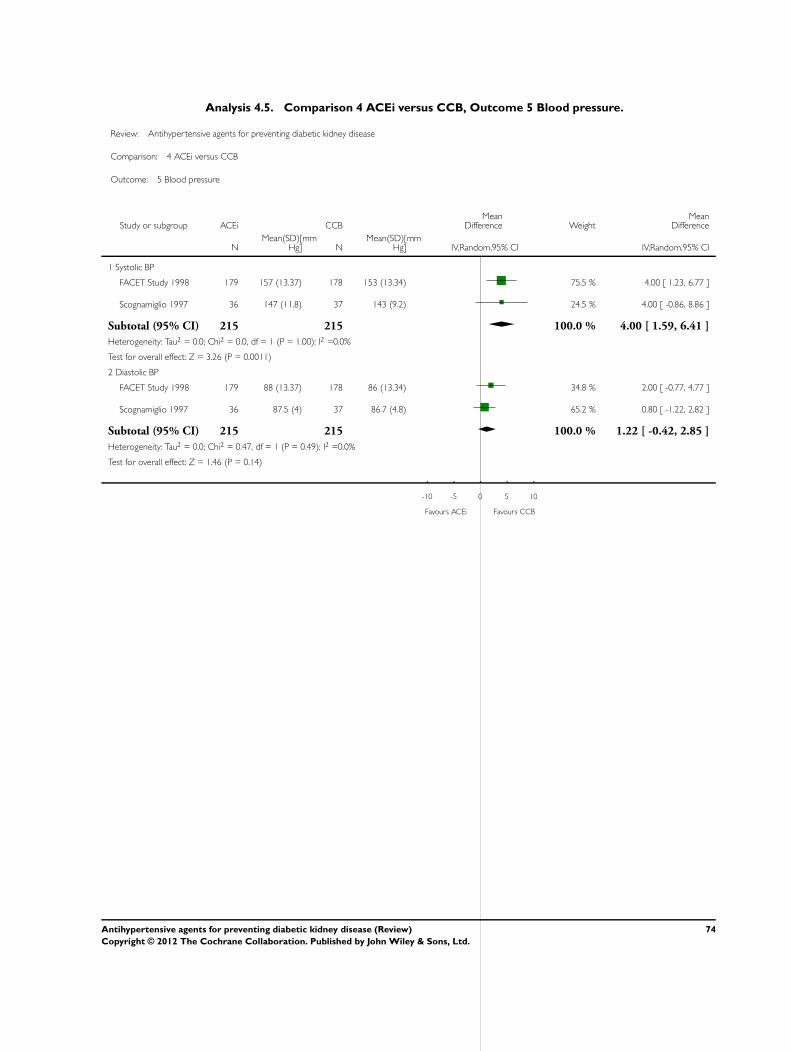
Analysis 4.5. Comparison 4 ACEi versus CCB, Outcome 5 Blood pressure.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 4 ACEi versus CCB
Outcome: 5 Blood pressure
Study or subgroup ACEi CCBMean
Difference WeightMean
Difference
NMean(SD)[mm
Hg] NMean(SD)[mm
Hg] IV,Random,95% CI IV,Random,95% CI
1 Systolic BP
FACET Study 1998 179 157 (13.37) 178 153 (13.34) 75.5 % 4.00 [ 1.23, 6.77 ]
Scognamiglio 1997 36 147 (11.8) 37 143 (9.2) 24.5 % 4.00 [ -0.86, 8.86 ]
Subtotal (95% CI) 215 215 100.0 % 4.00 [ 1.59, 6.41 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 0.0, df = 1 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 3.26 (P = 0.0011)
2 Diastolic BP
FACET Study 1998 179 88 (13.37) 178 86 (13.34) 34.8 % 2.00 [ -0.77, 4.77 ]
Scognamiglio 1997 36 87.5 (4) 37 86.7 (4.8) 65.2 % 0.80 [ -1.22, 2.82 ]
Subtotal (95% CI) 215 215 100.0 % 1.22 [ -0.42, 2.85 ]
Heterogeneity: Tau2 = 0.0; Chi2 = 0.47, df = 1 (P = 0.49); I2 =0.0%
Test for overall effect: Z = 1.46 (P = 0.14)
-10 -5 0 5 10
Favours ACEi Favours CCB
74Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
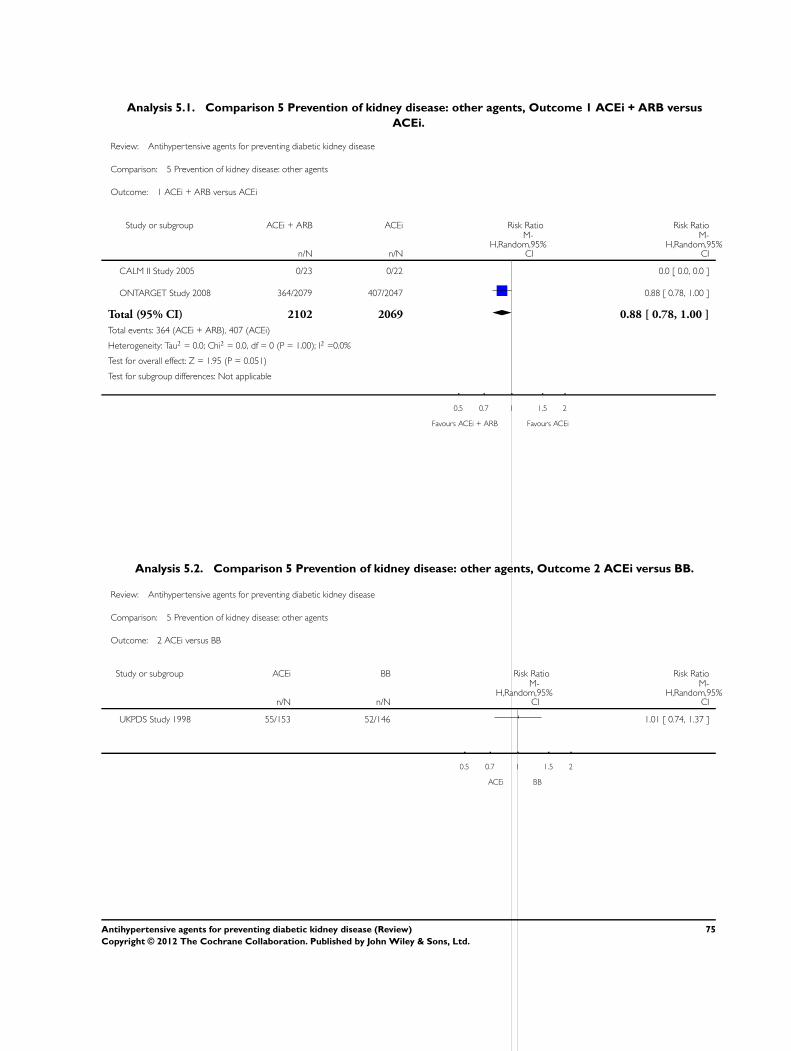
Analysis 5.1. Comparison 5 Prevention of kidney disease: other agents, Outcome 1 ACEi + ARB versus
ACEi.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 5 Prevention of kidney disease: other agents
Outcome: 1 ACEi + ARB versus ACEi
Study or subgroup ACEi + ARB ACEi Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
CALM II Study 2005 0/23 0/22 0.0 [ 0.0, 0.0 ]
ONTARGET Study 2008 364/2079 407/2047 0.88 [ 0.78, 1.00 ]
Total (95% CI) 2102 2069 0.88 [ 0.78, 1.00 ]
Total events: 364 (ACEi + ARB), 407 (ACEi)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.0, df = 0 (P = 1.00); I2 =0.0%
Test for overall effect: Z = 1.95 (P = 0.051)
Test for subgroup differences: Not applicable
0.5 0.7 1 1.5 2
Favours ACEi + ARB Favours ACEi
Analysis 5.2. Comparison 5 Prevention of kidney disease: other agents, Outcome 2 ACEi versus BB.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 5 Prevention of kidney disease: other agents
Outcome: 2 ACEi versus BB
Study or subgroup ACEi BB Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
UKPDS Study 1998 55/153 52/146 1.01 [ 0.74, 1.37 ]
0.5 0.7 1 1.5 2
ACEi BB
75Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
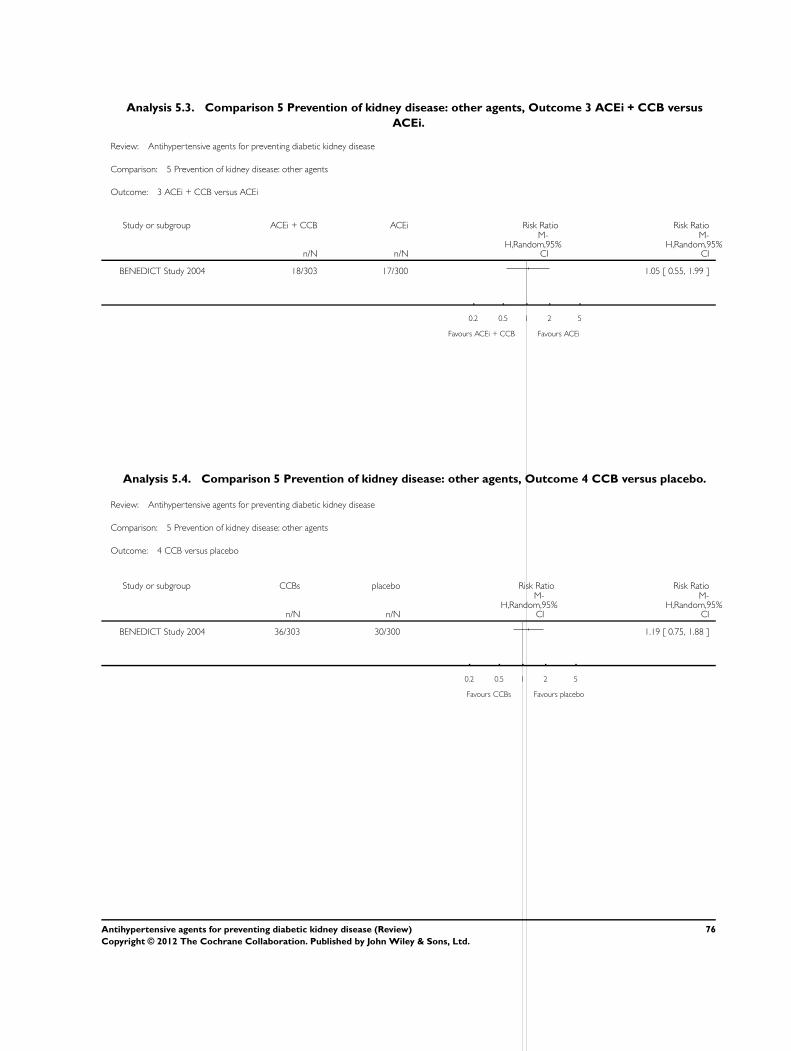
Analysis 5.3. Comparison 5 Prevention of kidney disease: other agents, Outcome 3 ACEi + CCB versus
ACEi.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 5 Prevention of kidney disease: other agents
Outcome: 3 ACEi + CCB versus ACEi
Study or subgroup ACEi + CCB ACEi Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
BENEDICT Study 2004 18/303 17/300 1.05 [ 0.55, 1.99 ]
0.2 0.5 1 2 5
Favours ACEi + CCB Favours ACEi
Analysis 5.4. Comparison 5 Prevention of kidney disease: other agents, Outcome 4 CCB versus placebo.
Review: Antihypertensive agents for preventing diabetic kidney disease
Comparison: 5 Prevention of kidney disease: other agents
Outcome: 4 CCB versus placebo
Study or subgroup CCBs placebo Risk Ratio Risk Ratio
n/N n/N
M-H,Random,95%
CI
M-H,Random,95%
CI
BENEDICT Study 2004 36/303 30/300 1.19 [ 0.75, 1.88 ]
0.2 0.5 1 2 5
Favours CCBs Favours placebo
76Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
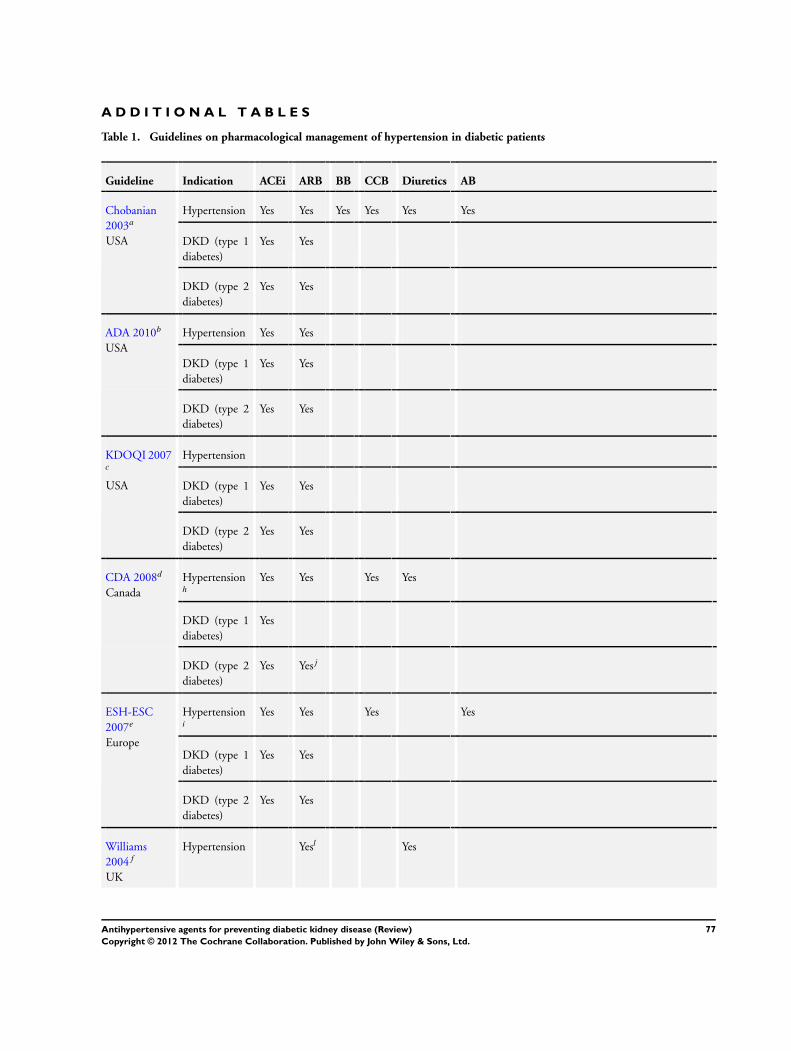
A D D I T I O N A L T A B L E S
Table 1. Guidelines on pharmacological management of hypertension in diabetic patients
Guideline Indication ACEi ARB BB CCB Diuretics AB
Chobanian
2003a
USA
Hypertension Yes Yes Yes Yes Yes Yes
DKD (type 1
diabetes)
Yes Yes
DKD (type 2
diabetes)
Yes Yes
ADA 2010b
USA
Hypertension Yes Yes
DKD (type 1
diabetes)
Yes Yes
DKD (type 2
diabetes)
Yes Yes
KDOQI 2007c
USA
Hypertension
DKD (type 1
diabetes)
Yes Yes
DKD (type 2
diabetes)
Yes Yes
CDA 2008d
Canada
Hypertensionh
Yes Yes Yes Yes
DKD (type 1
diabetes)
Yes
DKD (type 2
diabetes)
Yes Yesj
ESH-ESC
2007e
Europe
Hypertensioni
Yes Yes Yes Yes
DKD (type 1
diabetes)
Yes Yes
DKD (type 2
diabetes)
Yes Yes
Williams
2004f
UK
Hypertension Yesl Yes
77Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Guidelines on pharmacological management of hypertension in diabetic patients (Continued)
DKD (type 1
diabetes)
Yes
DKD (type 2
diabetes)
Yes
Chadban
2010g
Australia
Hypertension
DKD (type 1
diabetes)
Yes
DKD (type 2
diabetes)
Yes Yes
a Joint National Committee on Prevention, Diagnosis and Management of Hypertension; b American Diabetes Association; c Kidney
Disease Outcome Quality Initiative; d Canadian Diabetes Association; e European Society of Hypertension; f British Hypertension
Society; g Caring for Australians with Renal Impairment; h With special consideration given to ACEi or ARB; i A blocker of the
renin-angiotensin system should be a regular component of combination treatment and the one preferred when monotherapy is
sufficient; j Consensus for ARB use in type 1 diabetes; kUse calcium antagonists for hypertension when can be managed with
monotherapy; use any agent for hypertension which requires combination treatment; lIf intolerant to other agents
AB - alpha-blocker; ACEi - angiotensin-converting enzyme inhibitors; ARB - angiotensin receptor blockers; BB - beta-blockers; CCB
- calcium channel blockers; DKD - diabetic kidney disease
Table 2. Subgroup analysis of ACEi and ARB for preventing diabetic kidney disease
Vari-
ables
ACEi versus placebo ARB versus placebo ACEi versus CCB
Sub-
group
Studies RR
(95%
CI)
Het-
ero-
geneity
(P)
Sub-
group
Studies RR
(95%
CI)
Het-
ero-
geneity
(P)
Sub-
group
Studies RR
(95%
CI)
Het-
ero-
geneity
(P)
Nor-
moal-
bumin-
uria
≥ 500 4 0.84 (0.
79,0.
90)
0.023 ≥ 1500 4 0.86 (0.
76,0.
97)
0.089 ≥ 300 2 0.57 (0.
34,0.
96)
0.756
< 500 4 0.36 (0.
17,0.
79)
< 1500 3 1.30 (0.
49,3.
45)
< 300 3 0.63 (0.
38,1.
04)
Event
rate/
100
person-
years
≥ 5 4 0.76 (0.
54,1.
07)
0.059 ≥ 2.8 4 0.83 (0.
73,0.
94)
0.035 ≥ 2.0 3 0.57 (0.
39,0.
82)
0.378
78Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
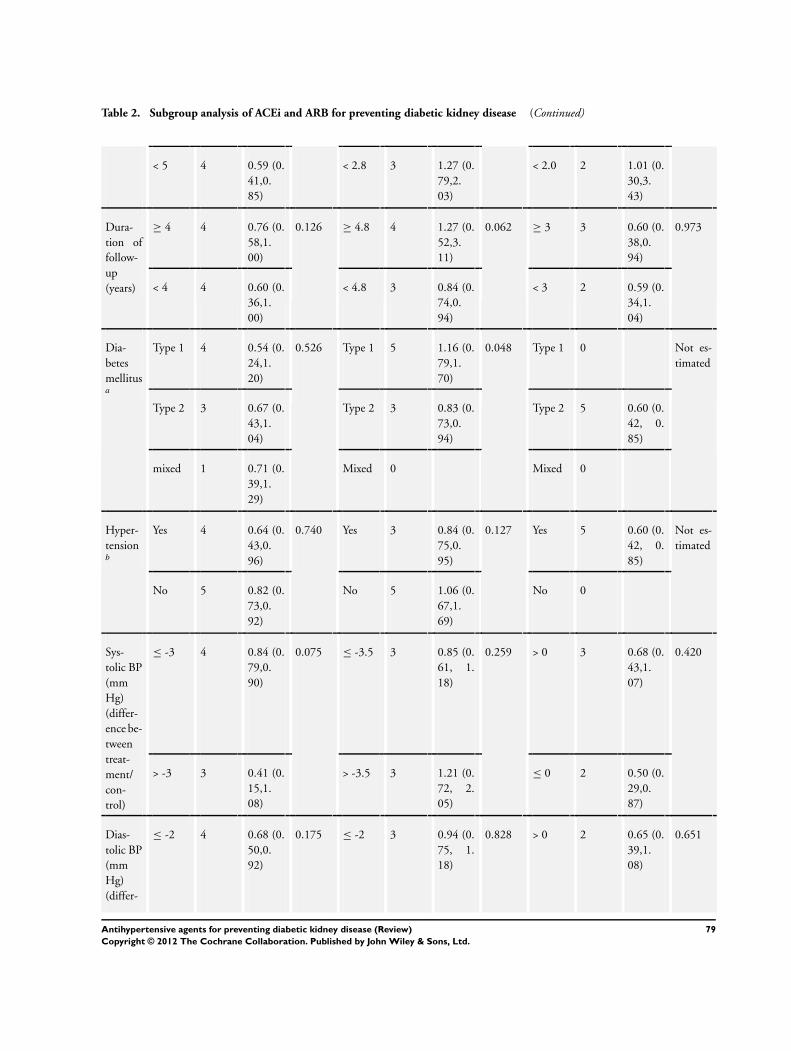
Table 2. Subgroup analysis of ACEi and ARB for preventing diabetic kidney disease (Continued)
< 5 4 0.59 (0.
41,0.
85)
< 2.8 3 1.27 (0.
79,2.
03)
< 2.0 2 1.01 (0.
30,3.
43)
Dura-
tion of
follow-
up
(years)
≥ 4 4 0.76 (0.
58,1.
00)
0.126 ≥ 4.8 4 1.27 (0.
52,3.
11)
0.062 ≥ 3 3 0.60 (0.
38,0.
94)
0.973
< 4 4 0.60 (0.
36,1.
00)
< 4.8 3 0.84 (0.
74,0.
94)
< 3 2 0.59 (0.
34,1.
04)
Dia-
betes
mellitusa
Type 1 4 0.54 (0.
24,1.
20)
0.526 Type 1 5 1.16 (0.
79,1.
70)
0.048 Type 1 0 Not es-
timated
Type 2 3 0.67 (0.
43,1.
04)
Type 2 3 0.83 (0.
73,0.
94)
Type 2 5 0.60 (0.
42, 0.
85)
mixed 1 0.71 (0.
39,1.
29)
Mixed 0 Mixed 0
Hyper-
tensionb
Yes 4 0.64 (0.
43,0.
96)
0.740 Yes 3 0.84 (0.
75,0.
95)
0.127 Yes 5 0.60 (0.
42, 0.
85)
Not es-
timated
No 5 0.82 (0.
73,0.
92)
No 5 1.06 (0.
67,1.
69)
No 0
Sys-
tolic BP
(mm
Hg)
(differ-
ence be-
tween
treat-
ment/
con-
trol)
≤ -3 4 0.84 (0.
79,0.
90)
0.075 ≤ -3.5 3 0.85 (0.
61, 1.
18)
0.259 > 0 3 0.68 (0.
43,1.
07)
0.420
> -3 3 0.41 (0.
15,1.
08)
> -3.5 3 1.21 (0.
72, 2.
05)
≤ 0 2 0.50 (0.
29,0.
87)
Dias-
tolic BP
(mm
Hg)
(differ-
≤ -2 4 0.68 (0.
50,0.
92)
0.175 ≤ -2 3 0.94 (0.
75, 1.
18)
0.828 > 0 2 0.65 (0.
39,1.
08)
0.651
79Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
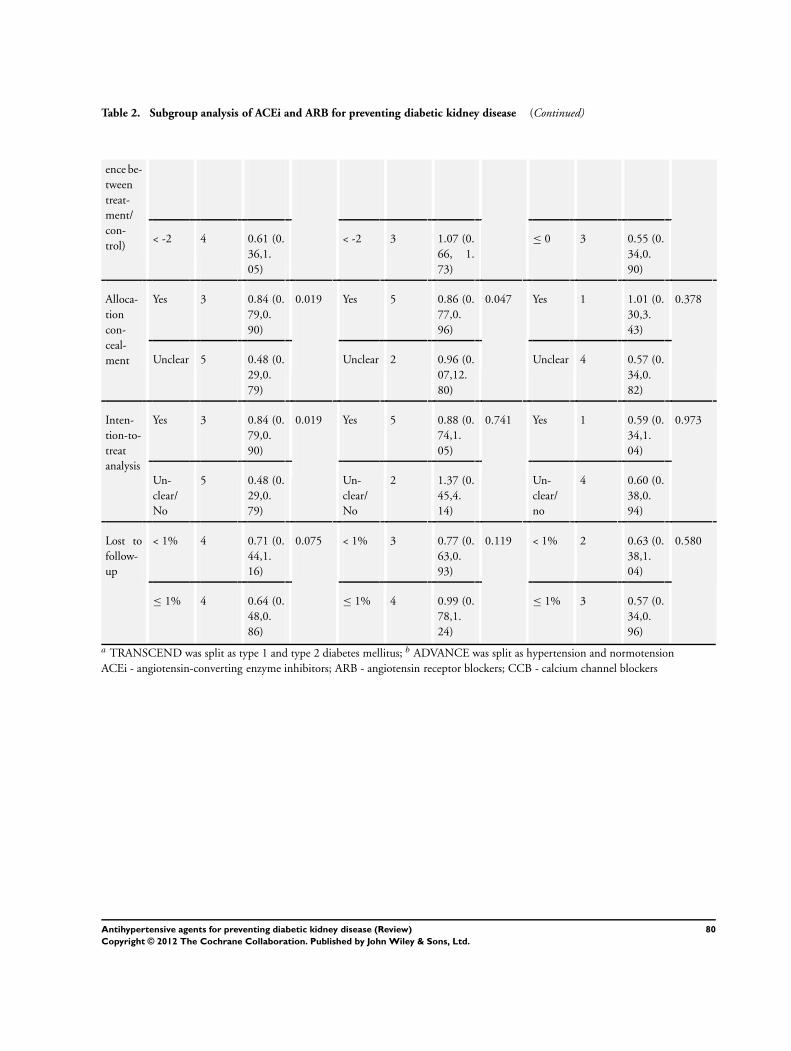
Table 2. Subgroup analysis of ACEi and ARB for preventing diabetic kidney disease (Continued)
ence be-
tween
treat-
ment/
con-
trol)< -2 4 0.61 (0.
36,1.
05)
< -2 3 1.07 (0.
66, 1.
73)
≤ 0 3 0.55 (0.
34,0.
90)
Alloca-
tion
con-
ceal-
ment
Yes 3 0.84 (0.
79,0.
90)
0.019 Yes 5 0.86 (0.
77,0.
96)
0.047 Yes 1 1.01 (0.
30,3.
43)
0.378
Unclear 5 0.48 (0.
29,0.
79)
Unclear 2 0.96 (0.
07,12.
80)
Unclear 4 0.57 (0.
34,0.
82)
Inten-
tion-to-
treat
analysis
Yes 3 0.84 (0.
79,0.
90)
0.019 Yes 5 0.88 (0.
74,1.
05)
0.741 Yes 1 0.59 (0.
34,1.
04)
0.973
Un-
clear/
No
5 0.48 (0.
29,0.
79)
Un-
clear/
No
2 1.37 (0.
45,4.
14)
Un-
clear/
no
4 0.60 (0.
38,0.
94)
Lost to
follow-
up
< 1% 4 0.71 (0.
44,1.
16)
0.075 < 1% 3 0.77 (0.
63,0.
93)
0.119 < 1% 2 0.63 (0.
38,1.
04)
0.580
≤ 1% 4 0.64 (0.
48,0.
86)
≤ 1% 4 0.99 (0.
78,1.
24)
≤ 1% 3 0.57 (0.
34,0.
96)
a TRANSCEND was split as type 1 and type 2 diabetes mellitus; b ADVANCE was split as hypertension and normotension
ACEi - angiotensin-converting enzyme inhibitors; ARB - angiotensin receptor blockers; CCB - calcium channel blockers
80Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
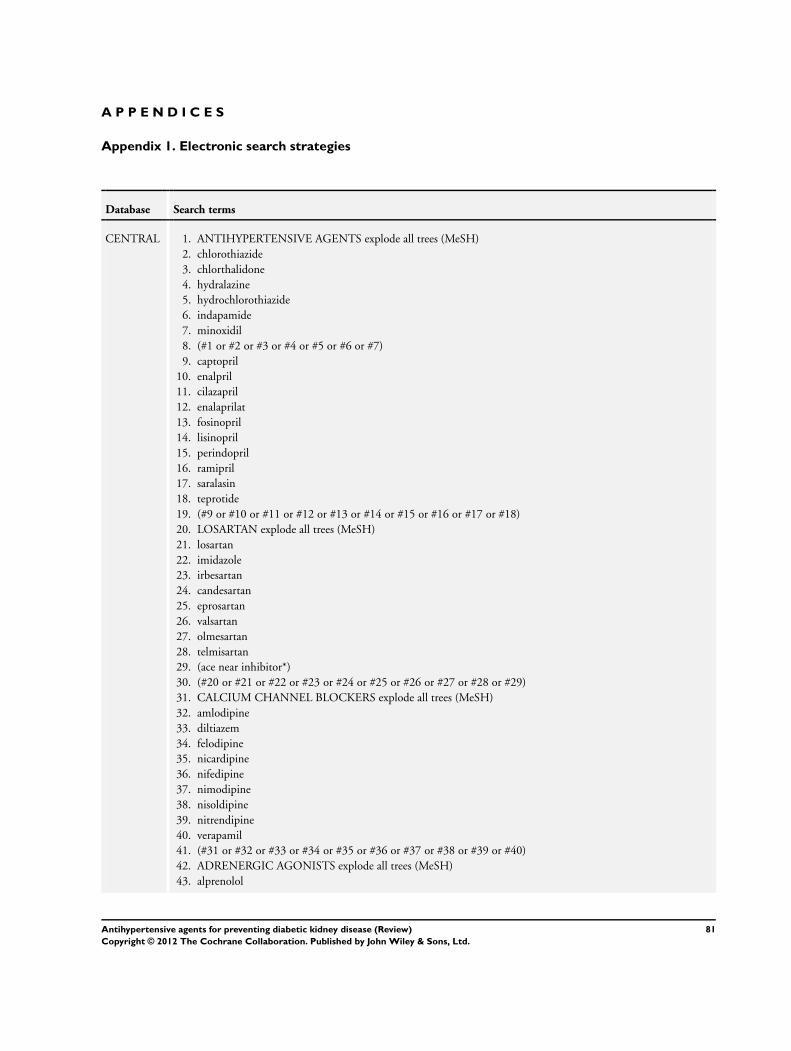
A P P E N D I C E S
Appendix 1. Electronic search strategies
Database Search terms
CENTRAL 1. ANTIHYPERTENSIVE AGENTS explode all trees (MeSH)
2. chlorothiazide
3. chlorthalidone
4. hydralazine
5. hydrochlorothiazide
6. indapamide
7. minoxidil
8. (#1 or #2 or #3 or #4 or #5 or #6 or #7)
9. captopril
10. enalpril
11. cilazapril
12. enalaprilat
13. fosinopril
14. lisinopril
15. perindopril
16. ramipril
17. saralasin
18. teprotide
19. (#9 or #10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 or #18)
20. LOSARTAN explode all trees (MeSH)
21. losartan
22. imidazole
23. irbesartan
24. candesartan
25. eprosartan
26. valsartan
27. olmesartan
28. telmisartan
29. (ace near inhibitor*)
30. (#20 or #21 or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29)
31. CALCIUM CHANNEL BLOCKERS explode all trees (MeSH)
32. amlodipine
33. diltiazem
34. felodipine
35. nicardipine
36. nifedipine
37. nimodipine
38. nisoldipine
39. nitrendipine
40. verapamil
41. (#31 or #32 or #33 or #34 or #35 or #36 or #37 or #38 or #39 or #40)
42. ADRENERGIC AGONISTS explode all trees (MeSH)
43. alprenolol
81Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
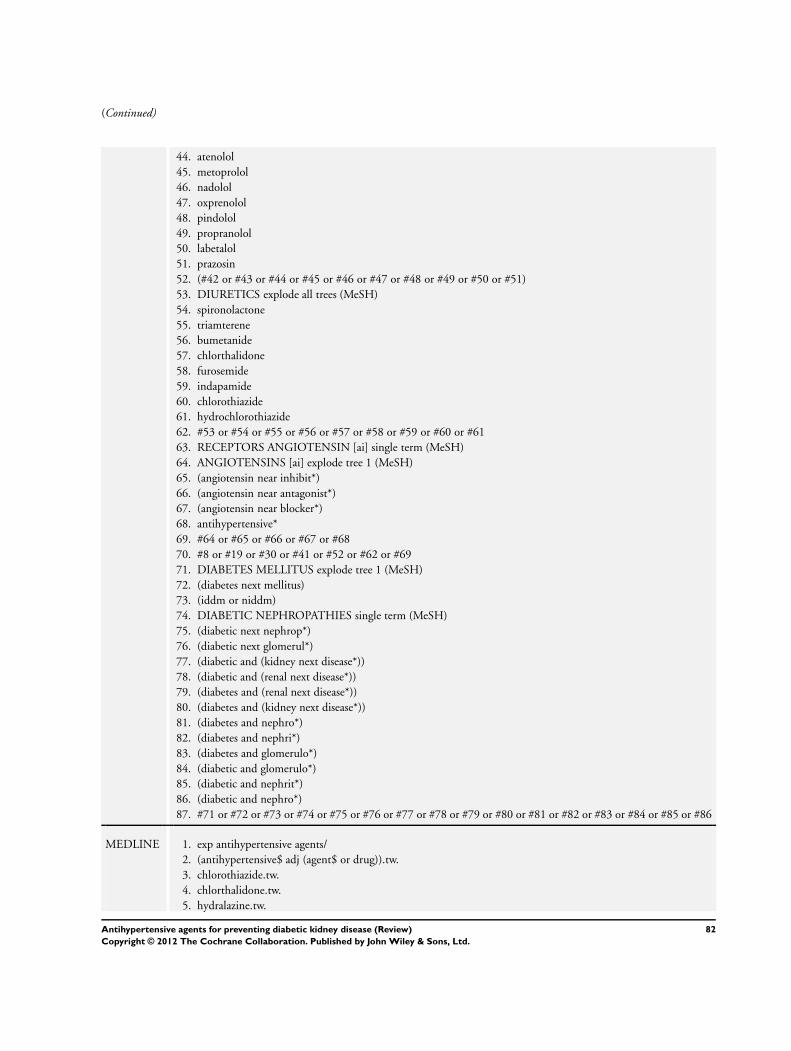
(Continued)
44. atenolol
45. metoprolol
46. nadolol
47. oxprenolol
48. pindolol
49. propranolol
50. labetalol
51. prazosin
52. (#42 or #43 or #44 or #45 or #46 or #47 or #48 or #49 or #50 or #51)
53. DIURETICS explode all trees (MeSH)
54. spironolactone
55. triamterene
56. bumetanide
57. chlorthalidone
58. furosemide
59. indapamide
60. chlorothiazide
61. hydrochlorothiazide
62. #53 or #54 or #55 or #56 or #57 or #58 or #59 or #60 or #61
63. RECEPTORS ANGIOTENSIN [ai] single term (MeSH)
64. ANGIOTENSINS [ai] explode tree 1 (MeSH)
65. (angiotensin near inhibit*)
66. (angiotensin near antagonist*)
67. (angiotensin near blocker*)
68. antihypertensive*
69. #64 or #65 or #66 or #67 or #68
70. #8 or #19 or #30 or #41 or #52 or #62 or #69
71. DIABETES MELLITUS explode tree 1 (MeSH)
72. (diabetes next mellitus)
73. (iddm or niddm)
74. DIABETIC NEPHROPATHIES single term (MeSH)
75. (diabetic next nephrop*)
76. (diabetic next glomerul*)
77. (diabetic and (kidney next disease*))
78. (diabetic and (renal next disease*))
79. (diabetes and (renal next disease*))
80. (diabetes and (kidney next disease*))
81. (diabetes and nephro*)
82. (diabetes and nephri*)
83. (diabetes and glomerulo*)
84. (diabetic and glomerulo*)
85. (diabetic and nephrit*)
86. (diabetic and nephro*)
87. #71 or #72 or #73 or #74 or #75 or #76 or #77 or #78 or #79 or #80 or #81 or #82 or #83 or #84 or #85 or #86
MEDLINE 1. exp antihypertensive agents/
2. (antihypertensive$ adj (agent$ or drug)).tw.
3. chlorothiazide.tw.
4. chlorthalidone.tw.
5. hydralazine.tw.
82Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
(Continued)
6. hydrochlorothiazide.tw.
7. indapamide.tw.
8. minoxidil.tw.
9. exp angiotensin converting enzyme inhibitors/
10. captopril.tw.
11. enalapril.tw.
12. cilazapril.tw.
13. enalaprilat.tw.
14. fosinopril.tw.
15. lisinopril.tw.
16. perindopril.tw.
17. ramipril.tw.
18. saralasin.tw.
19. teprotide.tw.
20. exp losartan/
21. losartan.tw.
22. imidazole$.tw.
23. irbesartan.tw.
24. candesartan.tw.
25. eprosartan.tw.
26. valsartan.tw.
27. olmesartan.tw.
28. telmisartan.tw.
29. (ace adj2 inhibitor$).tw.
30. (angiotensin adj2 receptor antagonist$).tw.
31. exp calcium channel blockers/
32. amlodipine.tw.
33. diltiazem.tw.
34. felodipine.tw.
35. nicardipine.tw.
36. nifedipine.tw.
37. nimodipine.tw.
38. nisoldipine.tw.
39. nitrendipine.tw.
40. verapamil.tw.
41. exp adrenergic beta-antagonists/
42. alprenolol.tw.
43. atenolol.tw.
44. metoprolol.tw.
45. nadolol.tw.
46. oxprenolol.tw.
47. pindolol.tw.
48. propranolol.tw.
49. exp adrenergic alpha-antagonists/
50. labetalol.tw.
51. prazosin.tw.
52. beta block$.tw.
53. exp diuretics/
83Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
(Continued)
54. spironolactone.tw.
55. triamterene.tw.
56. bumetanide.tw.
57. chlorthalidone.tw.
58. furosemide.tw.
59. indapamide.tw.
60. chlorothiazide.tw.
61. hydrochlorothiazide.tw.
62. or/1-61
63. exp diabetes mellitus/
64. diabetic nephropathies/
65. diabetic nephropath$.tw.
66. diabetic glomerulo$.tw.
67. ((diabetic or diabetes) and (kidney disease$ or renal disease$)).tw.
68. or/63-67
69. 62 and 68
EMBASE 1. exp antihypertensive agents/
2. (antihypertensive$ adj (agent$ or drug$)).tw.
3. (anti-hypertensive$ adj (agent$ or drug$)).tw.
4. chlorothiazide.tw.
5. chlorthalidone.tw.
6. hydralazine.tw.
7. hydrochlorothiazide.tw.
8. indapamide.tw.
9. minoxidil.tw.
10. losartan.tw.
11. imidazole$.tw.
12. irbesartan.tw.
13. candesartan.tw.
14. eprosartan.tw.
15. valsartan.tw.
16. olmesartan.tw.
17. telmisartan.tw.
18. exp angiotensin converting enzyme inhibitors/
19. (ace adj2 inhibitor$).tw.
20. (acei or ace-i).tw.
21. captopril.tw.
22. enalapril.tw.
23. fosinopril.tw.
24. lisinopril.tw.
25. perindopril.tw.
26. ramipril.tw.
27. saralasin.tw.
28. teprotide.tw.
29. exp Angiotensin 2 Receptor Antagonist/
30. exp Angiotensin Receptor Antagonist/
31. Angiotensin II Antagonist/
32. angiotensin II receptor antagonist$.tw.
84Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
(Continued)
33. angiotensin 2 receptor antagonist$.tw.
34. angiotensin II receptor block$.tw.
35. angiotensin 2 receptor block$.tw.
36. AT 2 receptor block$.tw.
37. AT 2 receptor antagon$.tw.
38. angiotensin receptor antagonist$.tw.
39. exp Calcium Channel Blockers/
40. amlodipine.tw.
41. diltiazem.tw.
42. felodipine.tw.
43. nicardipine.tw.
44. nifedipine.tw.
45. nimodipine.tw.
46. nisoldipine.tw.
47. nitrendipine.tw.
48. verapamil.tw.
49. exp adrenergic beta-antagonists/
50. alprenolol.tw.
51. atenolol.tw.
52. metoprolol.tw.
53. nadolol.tw.
54. oxprenolol.tw.
55. pindolol.tw.
56. propranolol.tw.
57. exp adrenergic alpha-antagonists/
58. labetalol.tw.
59. prazosin.tw.
60. beta block$.tw.
61. exp diuretics/
62. spironolactone.tw.
63. triamterene.tw.
64. bumetanide.tw.
65. furosemide.tw.
66. indapamide.tw.
67. or/1-66
68. exp Diabetes Mellitus/
69. diabetes mellitus.tw.
70. (IDDM or NIDDM).tw.
71. Diabetic Nephropathies/
72. diabetic nephrop$.tw.
73. diabetic glomerulo$.tw.
74. ((diabetic or diabetes) and (kidney disease$ or renal disease$ or nephro$ or nephrit$ or glomerulo$)).tw.
75. or/68-74
76. and/67,75
85Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Appendix 2. Risk of bias assessment tool
Potential source of bias Assessment criteria
Random sequence generation
Selection bias (biased allocation to interventions) due to inade-
quate generation of a randomised sequence
Low risk of bias: Random number table; computer random num-
ber generator; coin tossing; shuffling cards or envelopes; throwing
dice; drawing of lots; minimization (minimization may be imple-
mented without a random element, and this is considered to be
equivalent to being random)
High risk of bias: Sequence generated by odd or even date of birth;
date (or day) of admission; sequence generated by hospital or
clinic record number; allocation by judgement of the clinician; by
preference of the participant; based on the results of a laboratory
test or a series of tests; by availability of the intervention
Unclear: Insufficient information about the sequence generation
process to permit judgement
Allocation concealment
Selection bias (biased allocation to interventions) due to inade-
quate concealment of allocations prior to assignment
Low risk of bias: Randomisation method described that would not
allow investigator/participant to know or influence intervention
group before eligible participant entered in the study (e.g. central
allocation, including telephone, web-based, and pharmacy-con-
trolled, randomisation; sequentially numbered drug containers of
identical appearance; sequentially numbered, opaque, sealed en-
velopes)
High risk of bias: Using an open random allocation schedule (e.g. a
list of random numbers); assignment envelopes were used without
appropriate safeguards (e.g. if envelopes were unsealed or non-
opaque or not sequentially numbered); alternation or rotation;
date of birth; case record number; any other explicitly unconcealed
procedure
Unclear: Randomisation stated but no information on method
used is available
Blinding of participants and personnel
Performance bias due to knowledge of the allocated interventions
by participants and personnel during the study
Low risk of bias: No blinding or incomplete blinding, but the re-
view authors judge that the outcome is not likely to be influenced
by lack of blinding; blinding of participants and key study per-
sonnel ensured, and unlikely that the blinding could have been
broken
High risk of bias: No blinding or incomplete blinding, and the
outcome is likely to be influenced by lack of blinding; blinding
of key study participants and personnel attempted, but likely that
the blinding could have been broken, and the outcome is likely
to be influenced by lack of blinding
Unclear: Insufficient information to permit judgement
86Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Blinding of outcome assessment
Detection bias due to knowledge of the allocated interventions by
outcome assessors
Low risk of bias: No blinding of outcome assessment, but the review
authors judge that the outcome measurement is not likely to be
influenced by lack of blinding; blinding of outcome assessment
ensured, and unlikely that the blinding could have been broken
High risk of bias: No blinding of outcome assessment, and the
outcome measurement is likely to be influenced by lack of blind-
ing; blinding of outcome assessment, but likely that the blinding
could have been broken, and the outcome measurement is likely
to be influenced by lack of blinding
Unclear: Insufficient information to permit judgement
Incomplete outcome data
Attrition bias due to amount, nature or handling of incomplete
outcome data
Low risk of bias: No missing outcome data; reasons for missing
outcome data unlikely to be related to true outcome (for survival
data, censoring unlikely to be introducing bias); missing outcome
data balanced in numbers across intervention groups, with similar
reasons for missing data across groups; for dichotomous outcome
data, the proportion of missing outcomes compared with observed
event risk not enough to have a clinically relevant impact on the
intervention effect estimate; for continuous outcome data, plau-
sible effect size (difference in means or standardized difference in
means) among missing outcomes not enough to have a clinically
relevant impact on observed effect size; missing data have been
imputed using appropriate methods
High risk of bias: Reason for missing outcome data likely to be
related to true outcome, with either imbalance in numbers or rea-
sons for missing data across intervention groups; for dichotomous
outcome data, the proportion of missing outcomes compared with
observed event risk enough to induce clinically relevant bias in
intervention effect estimate; for continuous outcome data, plau-
sible effect size (difference in means or standardized difference in
means) among missing outcomes enough to induce clinically rel-
evant bias in observed effect size; ‘as-treated’ analysis done with
substantial departure of the intervention received from that as-
signed at randomisation; potentially inappropriate application of
simple imputation
Unclear: Insufficient information to permit judgement
Selective reporting
Reporting bias due to selective outcome reporting
Low risk of bias: The study protocol is available and all of the
study’s pre-specified (primary and secondary) outcomes that are of
interest in the review have been reported in the pre-specified way;
the study protocol is not available but it is clear that the published
reports include all expected outcomes, including those that were
pre-specified (convincing text of this nature may be uncommon)
87Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
High risk of bias: Not all of the study’s pre-specified primary out-
comes have been reported; one or more primary outcomes is re-
ported using measurements, analysis methods or subsets of the
data (e.g. subscales) that were not pre-specified; one or more re-
ported primary outcomes were not pre-specified (unless clear jus-
tification for their reporting is provided, such as an unexpected
adverse effect); one or more outcomes of interest in the review are
reported incompletely so that they cannot be entered in a meta-
analysis; the study report fails to include results for a key outcome
that would be expected to have been reported for such a study
Unclear: Insufficient information to permit judgement
Other bias
Bias due to problems not covered elsewhere in the table
Low risk of bias: The study appears to be free of other sources of
bias.
High risk of bias: Had a potential source of bias related to the spe-
cific study design used; stopped early due to some data-dependent
process (including a formal-stopping rule); had extreme baseline
imbalance; has been claimed to have been fraudulent; had some
other problem
Unclear: Insufficient information to assess whether an important
risk of bias exists; insufficient rationale or evidence that an iden-
tified problem will introduce bias
F E E D B A C K
ACEi compared to calcium channel blockers
Summary
There may be an error in the results section on the bottom of page 2. Under Angiotensin Converting Enzyme inhibitors vs. CCBs
(comparison 2) it says, “There was no statistically significant difference in the risk of development of kidney disease (micro or
macroalbuminuria) outcome 04, four trials, 1210 patients: RR 0.58, 95% CI 0.40 to 0.84) with ACEi compared to calcium channel
blockers.”
This seems to contradict both the data and the last sentence in the abstract “Compared to CCBs, ACEi significantly reduced progression
to microalbuminuria (four trials, 1210 patients: RR 0.58, 95% CI 0.40 to 0.84).”
Reply
To Dr Kripke and Dr Dressler:
The statistics are all correct, although the text describing them in the results section is wrong. It should read: “There was a statistically
significant reduction in the risk of development of kidney disease (micro or macroalbuminuria)....”
Dr Giovanni Strippoli
88Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Contributors
Dr Richard Dressler; Dr Clarissa Kripke
[email protected]; [email protected]
Family and General Preventive Medicine; Family Physician
W H A T ’ S N E W
Last assessed as up-to-date: 24 January 2011.
Date Event Description
8 November 2012 New search has been performed New studies and author team
1 August 2011 New citation required and conclusions have changed The updated review with more than 5 times of partic-
ipants has confirmed the effect with ACEi for the pri-
mary prevention of diabetic kidney disease and also re-
duction of all cause death, while no similar benefits of
angiotensin receptor blockers were observed
H I S T O R Y
Protocol first published: Issue 2, 2003
Review first published: Issue 4, 2005
Date Event Description
16 September 2008 Amended Converted to new review format.
C O N T R I B U T I O N S O F A U T H O R S
JL, VP, MC,CF, and GS were responsible for data collection, data analysis data interpretation, and preparation of the report. All authors
contributed to data interpretation and critical revision of the report.
89Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D E C L A R A T I O N S O F I N T E R E S T
Vlado Perkovic is supported by a fellowship from the Heart Foundation of Australia and a various grants from the Australian National
Health and Medical Research Council. He has received speakers fees from Roche, Servier and Astra Zeneca, funding for a clinical trial
from Baxter, and serves on Steering Committees for trials funded by Johnson and Johnson, Boehringer Ingelheim, Vitae and Abbott.
His employer conducts clinical trials funded by Servier, Johnson and Johnson, Roche and Merck.
Celine Foote has been supported by general research grants from both Amgen and the NHMRC. Both Amgen and the NHMRC have
played no part in the design, conduct and reporting of this research project.
JL has received grant support from Pfizer for hypertension research, and also is a recipient of a Research Fellowship supported by
Amgen.
I N D E X T E R M SMedical Subject Headings (MeSH)
Albuminuria [prevention & control]; Angiotensin Receptor Antagonists [∗therapeutic use]; Angiotensin-Converting Enzyme Inhibitors
[∗therapeutic use]; Antihypertensive Agents [∗therapeutic use]; Calcium Channel Blockers [∗therapeutic use]; Diabetic Nephropathies
[∗prevention & control]; Hypertension [drug therapy]; Randomized Controlled Trials as Topic
MeSH check words
Humans
90Antihypertensive agents for preventing diabetic kidney disease (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.