clinical/practice placements educator’s …€¦ · clinical/practice placements educator’s...
TRANSCRIPT
CLINICAL/PRACTICE PLACEMENTS EDUCATOR’S HANDBOOK
BSc Occupational Therapy and
Physiotherapy
EDUCATOR’S NAME……………………………………… REGISTRATION NO……………………………. University of Southampton School of Health Sciences
FOREWORD The Clinical/Practice organising team has designed this handbook. It assists clinical/practice education supervisors who work with students of the Allied Health Professions from the University of Southampton, School of Health Sciences. We purposely describe the clinicians and practitioners who deliver the clinical/practice education component of the programme as Clinical/Practice Education Supervisors as this reflects the School’s preferred approach to placement supervision including multiple models, team and split supervision. The purpose of the handbook is to provide information in a “user friendly” way to enable clinical/practice education supervisors to fulfil the expectations and responsibility of this role. Learning outcomes and assessment forms for all clinical/practice placements are included to enable clinical/practice education supervisors to see how the expectations and requirements of students and supervisors progress throughout the programme. It is sub-divided into sections: Programme Structure and Curriculum, Support and Education, Roles and Expectations, and Placement Learning Outcomes. The final section includes general information given directly to our students prior to commencing there clinical/practice placements. Effective communication and liaison between clinical/practice placements, clinical/practice education supervisors, students and School staff is essential in establishing a sound-working baseline. We hope this handbook facilitates this communication and look forward to working with you.
CONTENTS COURSE STRUCTURE AND CURRICULUM Course Structure and Curriculum Educational Focus Academic Modules of Study Overview Of Academic Year Clinical/Practice Education CLINICAL/PRACTICE EDUCATION SUPERVISOR SUPPORT AND DEVELOPMENT What do we offer you? Registration Study Days Briefing Sessions Locality Contacts Accreditation Education and Development EVALUATION Evaluation Evaluation Form CLINICAL/PRACTICE EDUCATION SUPERVISOR ROLES AND EXPECTATIONS What do we expect from you? Supervision Dealing with important issues Assessment Placement Hours PLACEMENT MODULE PROFILES Introduction Learning Outcomes Objectives Definitions Module Profile Resume (Assessment) Form GENERAL INFORMATION Preparation for placement Insurance & Safety Lone Working Position Statement Accident & Incident Reporting Sickness Reporting Mental Health Concerns Contact Numbers APPENDICES Appendix 1 Manual Handling Appendix 2 Reporting Mental Health Concerns Appendix 3 Clinical/Practice Placements for Disabled Students Appendix 4 Valid Consent to Examination and Treatment Appendix 5 Placement Mark Calculation Appendix 6 Physiotherapy placements Appendix 7 Academic year structures Appendix 8 Course Structure
COURSE STRUCTURE AND CURRICULUM STRUCTURE AND CURRICULUM The School of Health Sciences provides interdisciplinary educational programmes. Occupational therapists, physiotherapists and podiatrists emerge as distinct professionals from their programmes. The School has chosen a modular curriculum as its base for learning, which means the programmes are made up of a series of freestanding modules of study. These modules are linked together to form a coherent programme and each have clearly designed, achievable learning outcomes and assessments. The School provides variable programmes of study that provide opportunities for students’ choice in learning and enhances their motivation to learn. Within all the undergraduate programmes there are two types of modules:
Joint Modules - students receive common core teaching, but theory and activities are specific to professional groups.
Profession Specific Modules – students engage in separate subject areas. Also included is the Inter-professional Learning Programme [IPL], a core inter-professional educational component to pre-registration health professional programmes at both Southampton and Portsmouth Universities. EDUCATIONAL FOCUS Within the undergraduate programmes modules are graded and divided into 3 Levels which students complete in a three or five year period – the latter applicable to the part time study route. For students on the 3 year programme one level is completed within one academic year. Whereas, for students on the 5 year programme levels one and two take place over 4 years with level takes place over two semesters with an additional longer placement period. Level one is ‘student focused’ which means that the students learn about themselves and develop their basic skills. They reflect on their own experiences, learn how to learn, and develop learning strategies in the context of professional practice. The development of analytical thinking and basic research skills is essential for their own studies, and self management and time management are addressed to assist them with planning and organisation of workload. They develop key skills relevant to professional practice; from communication to basic interventions. Level two is ‘client focused’ and a major component is clinical/practice education and the preparation of students for the range of professional practice. Clinical/practice experience is scheduled in two 6 week blocks [10 week blocks for negotiating students taking their placements part-time], so that students can reflect on both their academic work in the clinical/practice environment and can appraise and integrate their practical experiences into subsequent learning in the School. Students also develop the skills to motivate and empower patients/clients and explore how statutory and ethical frameworks influence the management of patients/clients. Level three is ‘service focused’ so that as students progress towards qualification they understand their role within the health and social care systems and can function effectively and efficiently. Their clinical/practice placement(s), at level 3 consolidates and extends their knowledge and expertise to the level of practice required of a newly qualified therapist. They contribute to professional knowledge
by carrying out a clinical research project and present their findings in an organised manner. CLINICAL/PRACTICE EDUCATION The School “is committed to developing competent, reflective practitioners who are equipped with a range of professional and interpersonal skills to work in a diverse and changing health care system” and recognises that clinical/practice education has a fundamental role to play in this process. Over a three or five year period the School must ensure that students receive a span of clinical/practice experience as directed by the professional bodies. Clinical/practice is a time for developing hands-on skills. Students have the opportunity to integrate theory with practice, develop a range of professional skills and learn to work with different team members. They explore how their own attitudes and values fit within those of their profession and identify their own ethical and moral position within the boundary of their profession’s rules and guidelines. Structure of Clinical/Practice Education Each clinical/practice placement has its own learning outcomes and assessment criteria that reflect the developmental nature of the course. Placement A focuses on students’ observation and reflection about the role of the occupational therapist, physiotherapist and other key health workers. The student completes one week in a clinical area. The length of Placements B – D vary from five to ten weeks on the full-time programme and six to twelve part time-time, or equivalent weeks on the part time programme. To achieve maximum continuous integration of theoretical and practical knowledge, students experience Clinical/Practice Placements throughout the three levels of the programme; thus enabling theory to inform practice and also for practice to inform theory. For example: In Level 1 physiotherapy students study profession specific modules in which they explore the theoretical and scientific basis of physiotherapy practice and develop general manual skills in preparation for Clinical/Practice Placement B. During Placement B, students apply the skills learned and thus further increase their expertise. These experiences together serve as a foundation for clinical context and clinical management modules studied in Level 2. During these modules students reflect on their earlier clinical experiences and build on them in preparation for Placements C1 and C2. Occupational Therapy students study two OT practice modules in Level 1: ‘Understanding and Action’ and ‘OT Performance and Domains’, during which they develop skills for a variety of client groups. These skills are applied during Placement B and are foundation skills for clinical modules studied in Level 2. This process of initial exploration in School and application and elaboration during clinical/practice placements, followed by reflection and further investigation in School is continuous for all students throughout the programmes.
CLINICAL/PRACTICE EDUCATION SUPERVISOR SUPPORT AND DEVELOPMENT WHAT DO WE OFFER YOU? The School develops effective and efficient relationships with clinical/practice placements and clinical/practice education supervisors in the following ways: Registration. To ensure information reaches clinical/practice education supervisors. Briefing sessions. A series of these are held prior to each placement to allow new clinical/practice education supervisors working with our students to understand the philosophy of the School and practice the assessment process prior to having their first students. Locality contacts and visits. School tutors establish and maintain contact with clinical/practice placements and clinical/practice education supervisors within specific geographical areas. There is a commitment by the Locality Contact from school to visit students and clinical/practice education supervisors during each graded clinical/practice placement. Study days. Organised to focus on current clinical/practice education issues, and provide the opportunity for clinical/practice education supervisors and tutors to meet. Educational workshops. A series of workshops are regularly run to facilitate the professional development of clinical/practice education supervisors and promote good standards of practice. Accreditation. Clinical/practice placements and clinical/practice education supervisors/and or co-ordinators of practice placements voluntarily work with the School to validate opportunities available to students in the workplace. Practice Educator website. The website provides information on issues pertinent to practice education, eg courses, events, items of interest; plus provides access to resources to assist you in your role as practice educator. It also provides another means of having your questions answered. These aspects are now discussed in more detail to increase clinical/practice education supervisors’ awareness and understanding of the opportunities available.
REGISTRATION All qualified therapists are eligible to register with the School. This includes experienced therapists, junior/basic grades and part-time staff. The Registration can be viewed either as:
• expressing an interest in clinical/practice education supervision, with a commitment to working with students in the future;
• confirmation of a wish to take responsibility for clinical/practice education supervision in the immediate future.
REGISTRATION IS NOT ACCREDITATION Interest in Clinical/Practice: Therapists who initially express an interest in clinical/practice education can register as a clinical/practice education supervisor at any time. Clinical/Practice Education Supervisor: Therapists who register as a clinical/practice education supervisor should discuss this with their line manager and/or clinical team, prior to contacting the School. This enables line managers/clinical team to advise and support their development as educators as part of their CPD appraisal and personal development plan. Clinical/Practice education supervisors who work directly with our students are expected to register, as this ensures that information and newsletters are automatically forwarded to them. They also receive a Clinical/Practice Education Supervisor’s Handbook and a registration number, which means that handbooks can be traced to individuals and updated as and when necessary. Current copies of the Handbook are also accessible on the Practice Educator’s Website All registered clinical/practice education supervisors, whether experienced or not, are invited to become accredited with the School and are assisted in using their prior learning and experience in the process. The following registration procedure is implemented:
1. Therapists register by completing the registration form and forwarding this to the Clinical/Practice Secretary, School of Health Sciences, University of Southampton, Highfield, Southampton SO17 1BJ.
2. The application is acknowledged as soon as possible after receipt. 3. The School notifies the clinical/practice education supervisor of his/her
registration number. In summary, the School:
1. notifies and invites registered therapists to study days, workshops, and educational events;
2. provides regular updates and information through a newsletter related to clinical/practice education, e.g. curriculum development, as and when appropriate;
3. provides a personalised clinical/practice education supervisor handbook related to A, B, C and D placements, for all supervisors working directly with our students;
4. provides accreditation guidelines for clinical/practice education supervisors, co-ordinators and centres;
5. seeks advice and surveys therapists’ views on all things related to clinical/ practice education, e.g. assessment of students, through feedback to locality contacts, during study days or by postal questionnaire.
BRIEFING SESSIONS Clinical/Practice education supervisors who are new to working with Southampton students are required to attend a briefing session prior to receiving their first student. These sessions are carried out at the School or in specific localities according to the circumstances. The aim is to increase awareness and understanding of the School’s philosophy, programme content and use of clinical/practice assessment form. Case studies based on ‘hypothetical’ students are used so that clinical/practice education supervisors can practice using the School’s assessment forms. This provides opportunity for clinical/practice education supervisors to grade the case studies, discuss the outcomes and check their understanding with peers. It also provides the School with important information about whether the assessment form is being used consistently to grade and assess students. STUDY DAYS During the year the School organises events for clinical/practice education supervisors who work with our students. Issues specifically related to students are covered, e.g. preparation of students prior to placement and assessment reports; curriculum development and redesign. School tutors meet with clinical/practice education supervisors informally during the day. There is an opportunity to share and discuss general issues related to clinical/practice education and the School encourages clinical/practice education supervisors to identify areas of interest and topics for inclusion in the programme. LOCALITY CONTACT VISITS Clinical/Practice placements cover a large geographical area. This area has been subdivided into localities to which a School tutor is allocated as a locality contact with designated responsibility for liaison with departments, seniors and supervisors within the specific area. They have responsibility for developing links with the service, clinical/practice education supervisors, for visiting the student/s on placement within their designated locality and assisting with the accreditation process. In some localities, clinical/practice placements are provided for both occupational therapy and physiotherapy students. A locality contact from the School, will be assigned by the Clinical/Practice Education Coordinators from each profession. Locality Contacts visit students on placement at least once during each placement. A physiotherapy team tutor is responsible for visiting a physiotherapy student and an occupational therapy team tutor for visiting an occupational therapy student. The Locality Contact contacts the clinical/practice education supervisor to organise a suitable time for a visit. These visits are carried out to:
1. gather information from both students and supervisors about experience and skills gained up to the point of the visit and to review the programme and objectives for the placement;
2. ensure the experience on offer in the placement is used to the best advantage;
3. ask advice on behalf of the School on preparation and skills needed for the placement;
4. give positive feedback to both student and supervisor on achievements to date;
5. where necessary, check out whether the student is encountering any difficulties and take action as appropriate;
6. support the supervisor in the task of educating the student through information, advice and initiating other actions;
7. facilitate the transfer of learning from units to placement and vice versa when the opportunity presents itself;
8. assist supervisors with the accreditation process. In exceptional circumstances, it may be necessary to pay an additional visit where the supervisor or student requests this. The locality contact is asked to try to get an outline of the situation from both parties so that they can make the relevant preparations – such as liaising with the module co-ordinator or a member of the Clinical/Practice Organising Team, before meeting the situation. Whenever possible, the locality contact:
1. sees the student and clinical/practice supervisor individually; 2. sees the student and clinical/practice supervisor together, if appropriate.
Please call the practice placement administrator or [email protected] if you wish to make contact with your locality contact to discuss issues or to arrange an earlier or additional visit.
ACCREDITATION Accreditation is the adopted term to describe the formal act by which the School recognises the competence and continuing good practice of the Clinical/ Practice Education Supervisors, Co-ordinators and Centres The School is committed to developing competent, reflective practitioners and recognises that clinical/practice education has a fundamental role to play in this process. The responsibility for ensuring that standards of practice are met in clinical/practice education is the shared responsibility of the School, who prepare students for clinical/practice, services who provide the environment in which students gain experience and individual therapists who directly assist students to develop professional skills. The School accreditation system has been designed to reflect the guidelines published by the relevant professional bodies; ACE from the CSP and APPLE from the COT. For more information see the Practice Educator website. In order to provide a balanced approach, the School accredits:
• Clinical/practice education supervisors who directly supervise students • Co-ordinators who select, plan and develop placements • Centres who develop staff in order to provide clinical/practice placements.
There are separate guidelines focusing around nine standards for each of the above categories. We are primarily interested in accrediting individual clinical/practice education supervisors, as accreditation status applies wherever the supervisor works, now or in the future. To quote from the guidelines: The School wishes to establish a partnership with therapists and departments who share responsibility for educating students and believes that providing an accreditation framework is one way of valuing the role of the ‘clinical/practice education supervisor’. As the clinical/practice education supervisor role demands great flexibility in practice, so these guidelines should be used flexibly, with individuals working at their own pace and level of development. The standards are a useful resource for therapists who are involved in educating students, regardless of whether they choose to become accredited or not. As recipients of clinical/practice education, students are expected to take an active part in the process and the School values their contribution. The School introduces students to the accreditation process and assists them to develop a role within it. In the same way as theoretical knowledge and practical skills development, their understanding of the accreditation process will develop as they progress through the course. First year students may not be as skilled at providing feedback and testimony as a third year student.
AUTHORISED/ACCREDITED STATUS Any therapist or service can register with the School and become “authorised” to work with students. When authorised clinical/practice education supervisors, co-ordinators and centres have acquired experience of working with Southampton students, they are eligible to become accredited with the School. It is envisaged that this process will gradually develop over the coming months/years. The clinical/practice education supervisor, co-ordinator or centre does not need to have undergone a formal accreditation process in order to provide clinical/practice experience for our students. At present the only requirement is for a clinical/practice education supervisor to have attended the clinical briefing session. The School values existing accreditation schemes and therapists/services accredited by another school can use this knowledge and experience should they wish to become accredited with Southampton. Portfolio Development There are a variety of mechanisms that enable individuals to develop and demonstrate competence and good practice. The method adopted by the School is Portfolio Development and information about this is available on request. EDUCATION AND DEVELOPMENT The School provides a development programme for clinical/practice education supervisors, where a series of workshops are repeated on a regular basis throughout the year. Each workshop relates directly to a specific standard in the accreditation guidelines and covers a range of subjects such as supervision and teaching skills, assessment and evaluation of clinical/practice experience. The workshops are designed to assist clinical/practice education supervisors to develop sound practical supervision skills and to increase awareness of the clinical educator role. An introduction to the Accreditation system and developing a portfolio are included in the programme to assist clinical/practice placements and clinical/practice education supervisors. Notification of workshops and events held in the School and booking for courses are provided through the practice educator website. Priority is given to clinical/practice education supervisors who are actively involved with Southampton students when places on workshops are limited. Whenever possible requests from clinical/practice education supervisors to hold workshops in localities are accommodated. The School encourages clinical/practice placements to develop in-service education programmes within localities and offers assistance with organisation and teaching. External educational programmes provided within trusts are seen as complementing any programme provided by the School.

EVALUATION The School is keen to develop an effective system for evaluating clinical/practice education. This involves the supervisor, locality contact and student in the following: Student – Supervisor Feedback (During the placement) The evaluation form is designed to assist in the feedback process between student and supervisor throughout the placement. This form is sent out with the official assessment report form, but need not be returned to the School with the final report. It is for your own information and development. Locality Contact keeps a central record of their visit[s] to a placement. Supervisor provides feedback to the School through their locality contact (during and after placement). Student Feedback (after the placement) Students are debriefed on their return from placement. They identify and discuss their experience in peer groups. The focus for this debriefing is threefold;
• how the programme has prepared them for their clinical experience; • how they have prepared themselves and • the experience of the placement itself.
They provide feedback to the School about the placement and subsequently the School reports back to the providers either on request or through annual statements. Clinicians study afternoons often involve focus groups that are held to collect supervisor views and develop ideas on aspects of clinical/practice education and practice, preparation for placement and curriculum content. Each year, the clinical/practice team is engaged in activity to explore one or more aspects of clinical/practice, e.g. the use of locality contact visits, preparation of students for moving and handling, models of supervision, placement allocation models. These investigations give the School valuable information that can be used to enhance the practice of clinical/practice education.
CLINICAL/PRACTICE EDUCATION SUPERVISOR ROLE AND EXPECTATIONS WHAT DO WE EXPECT FROM YOU? The School has high expectations of clinical/practice placements. The following expectations are based on the standards of practice currently provided by the College of Occupational Therapists and the Chartered Society of Physiotherapy. For experienced clinical/practice education supervisors this will be familiar ground, however for those taking a student for the first time it is understandable that time and some assistance is needed to acclimatise to the requirements. Clinical/Practice Education Supervisor Role It is expected that the clinical/practice education supervisor:
1. has sufficient experience and expertise to facilitate students’ professional development and will have a minimum of 2 years post-qualification experience prior to taking a student on a graded placement;
2. registers with the University of Southampton School of Health Sciences; 3. attends a briefing session prior to receiving their first student; 4. provides sufficient information to assist students to comply with the
objectives of the placement; 5. is responsible for the personal and professional development of students
during the period of the placement; 6. assists students to identify and overcome personal and professional
obstacles, unexpected incidents and generally how to cope with the pressures of the workplace;
7. creates a learning environment which promotes the development of students’ level of professional competence;
8. has sufficient experience and expertise to assist students to fulfil the learning outcomes of the placement;
9. ensures the quality of the learning experience for students; 10. follows the guidelines provided by the School in the assessment of students’
knowledge, performance and professional competence.
SUPERVISION The School expects that a named clinical/practice education supervisor will be overall responsible for a student although more than one or a team may share the responsibility for the personal and professional development of the student/s during the period of the placement. This involves the provision of support and encouragement on a regular weekly basis and assistance in how to deal with the pressures of clinical work. In order to achieve good standards of practice it is expected that clinical/practice education supervisors understand the concept and principles of supervision and apply these when developing a working relationship with the student. The following instructions have been given to the students: A supervision relationship is possibly the best way of ensuring that you have the opportunity to reflect on your development as a trainee professional. You will have a named clinical/practice education supervisor in each of your clinical/practice placements, although other members of the clinical team may facilitate much of the placement learning. The supervisor will normally be a qualified therapist who has responsibility for meeting with you regularly, e.g. once a week, on a one-to-one basis to discuss and reflect upon the content and process of your work and to provide you with feedback and support. The clinical/practice education supervisor may have responsibility for more than one student. The format and style of supervision will depend upon the preference of your supervisor and yourself. This may also be influenced by the requirements and limitations of the clinical area. You will find that your supervisor will adopt different roles, and will focus on a variety of issues during each placement. Firstly, there will be an educative element where you will explore therapeutic interventions with patients/clients, e.g. why and how you carry out clinical work. Secondly, you will need support and encouragement to cope with the pressures of dealing with disease and distress and discussion with your clinical/practice education supervisor could be an important outlet for your own feelings and emotions. Finally, your supervisor will be managing the clinical situation in order to ensure that your work is appropriate and falls within defined standards of care for patients/clients and the service. You will need to draw up an informal agreement or learning contract with your supervisor about the most effective approach or balance of approaches to adopt. It is your responsibility to let your clinical/practice education supervisor know what your needs are. Supervisors notice many things, but may need some assistance in understanding your position.

DEALING WITH IMPORTANT ISSUES The majority of students develop steadily during their clinical/practice placements. A motivated student, with assistance from their clinical/practice education supervisor, has relatively trouble free experiences and successfully overcomes any problems as and when they occur. However, a small percentage of students experience great personal and professional difficulties, often when least expected, as a result of exposure to the pressures of clinical work. The reality that clinical/practice placements do not always run smoothly is brought to students’ attention during clinical preparation sessions and in their clinical/practice handbook. The following instructions have been given to students: There may be times when you and your supervisor do not agree on a particular professional issue which might be stressful or anxiety provoking. Try looking at the issue from your supervisor’s point of view within the context of that particular setting – local factors can affect how particular things are done or presented. Listen to feedback without being defensive. You may find that you have two ways to approach an issue whereas before you had only one. On the other hand, you may have to agree to differ, as some aspects of professional practice rest on opinion rather than verifiable fact. It only needs to become a big issue if it conflicts with your own duty of care to a particular patient/client. You must not do what you believe to be harmful, or cause harm by anything which you leave undone. This situation is very rare, and we need to hear from you as soon as possible should it ever occur in your placement. It is not feasible to prepare students for every eventuality. However, clinical/practice education supervisors need to be aware of a range of issues so that the symptoms can be recognised quickly. These important issues might include:
1. a student’s apparent lack of interest or commitment, 2. a student’s lack of ability and possible failure to reach the required standard, 3. shortness of time available for a student to modify his/her performance, 4. how a student copes with disease and distress, 5. an under/over confident student, 6. a student who demonstrates unprofessional or unsafe behaviour, 7. how a student copes with personal and family issues alongside clinical work, 8. a student who is frequently off sick, withdrawn or extremely tired/fatigued.
Students at any stage of training are affected and often a key to dealing with situations is prompt action by clinical/practice education supervisors. This places great demands on supervisors’ time, energy and confidence, and it is recommended that they establish a personal support network, either within the department/clinical team or through the School’s locality contact system. The School needs to be kept informed of any problems as early as possible so that assistance and support can be offered in good time.
ASSESSMENT The School expects clinical/practice education supervisors to follow the guidelines provided in the assessment of students’ knowledge, performance and professional competence. This involves assisting the student to attain and develop their competence in the clinical area, recognising competence and appraising the student’s performance through continuous and summative assessment. If continuous feedback is clear, with a written report at half way, the full-time report should not be a surprise to the student. It is recommended, indeed expected where more than one member of the team is involved, that clinical/practice education supervisors consult colleagues and the other members of the clinical team before finalising half way/full-time reports. The School can provide support and advice to students and supervisors throughout the process. The School does not require a copy of the half way report, though it is essential to contact the School if the student is experiencing difficulty. The half way grade should be noted alongside the full-time grade and the final report forwarded to the Clinical/Practice Secretary within one week of completion of the placement. The following instructions have been given to the students: Assessment of your performance by your clinical/practice education supervisors is an integral part of clinical/practice education. Its purpose is to ensure that you are developing your professional skills and are operating competently within the clinical/practice setting. Much of the feedback will be informal, e.g. instruction whilst in action, regular supervision sessions and discussion of cases. The formal assessment is seen as an extension of this learning process and will take place at least twice during the placement, i.e. half way and full-time reports. For these assessments, the clinical/practice education assessment forms will be used. PLACEMENT HOURS On the full-time programmes the School expects that students will work for the same time per week as the normal contracted hours of a full-time therapist. This will include the half-day study period. The hours recorded for a placement are the normal full-time contracted hours of a therapist under Agenda for Change, ie 37.5. Days lost through sickness or absence should be recorded on the assessment form. On the part time programme students may undertake placements on a part-time basis. Where this is the case this will be negotiated individually between the placement provider, practice placement co-ordinator and student. On part-time placements students will normally work three days a week and the hours per week will be equivalent to 0.6 of the full-time hours, ie 22.5.
Level 1 – Placements A&B INTRODUCTION This section focuses on Placement A, providing information about expectations, objectives and the assessment form. EXPECTATIONS Placement A consists of 1 week (3 days if undertaken on a part time programme) of observation towards the end of Semester 1, Year 1. This placement gives the students an opportunity to relate the communication strategies and professional frames of reference they have learned in their first semester to what happens in the clinical/practice setting. The student spends the majority of the time directly observing their clinical/practice education supervisor. The important part of the feedback at this stage is advice on strategies for settling into new areas and developing a professional approach to patients/clients and colleagues. It is envisaged that the student will use his/her clinical/practice education supervisor’s job description and/or a description of their role, as a resource for their Communication and Frames of Reference report in which module content is linked to clinical/practice experience. The student can and should be used in the same way as an Assistant during this placement. They should also have the opportunity to observe another professional in action so that they can explore and compare professional roles. The assessment report focuses on the student’s ability to observe and communicate, with opportunity for the supervisor to advise on the student’s future practice. OBJECTIVES The student fulfils the placement learning outcomes by:
- observing the role and activities of the clinical/practice education supervisor - identifying and developing his/her own role within the team setting: - carry out daily tasks and assist patients/clients and team members as
directed by the supervisor - establish professional relationships with patients/clients and team members
as necessary to carry out learning objectives - discuss observations and findings with the supervisor - find and follow safety policies and procedures used in the placement
Students may ask about the approaches and frames of reference used in your area. With this in mind, you may find the following useful: DEFINITIONS These are the definitions we will be using during the module: NB If you are reading other texts remember to check the Author’s definition, as these words are used to mean different things by different writers, Paradigm Provides a single statement of the fundamental principles and philosophy on which a profession is based. Frame of Reference A framework which draws together the unifying theories and hypotheses of an area of study or practice and sets boundaries to and foundations for, the construction of models and approaches.

Model A statement of an organised and synthesised body of knowledge which demonstrate relationships between elements within the model, between theory and practice, and co-ordinates the application of relevant approaches and techniques. Approach Describes a set of ideas and actions which provide the therapist with a particular focus which will lead to the selection of specific assessments, media, treatment techniques, or a style of relationship with the patient or client.
PLACEMENTS B, C AND D INTRODUCTION These placements provide the opportunity for students to develop professional and clinical skills. A similar assessment report has been devised for use in all the placements, with emphasis placed on safe practice, interpersonal skills, clinical skills and management skills. The wording of the assessment reports has been graded in a way that reflects the expected growth and ability of the student. Physiotherapy students must aquire skills and experience in the core areas of physiotherapy practice, and in acute and community environments i.e. Musculoskeletal, Acute/Respiratory care, Non-Acute care and Neurology. These placements are divided into five or six week blocks [or their part-time equivalent] according to the programme concerned. It is important that Occupational therapy students acquire a balance of practice experience of mental health/learning disability and physical specialities within hospital, community and social services settings. CASE STUDIES During each placement (B, C and D) students prepare a written case study on at least one patient/client or research a topic. This provides reference material for use in School, an example of treatment or intervention or the evidence base within that particular area. It provides evidence of the students’ understanding of the needs of the patient/client, appreciation of the occupational therapy/physiotherapy process and the evidence base, the skills involved, and a grasp of the place of occupational therapy/physiotherapy within the operation of a multidisciplinary team. The student may be required to present a summary of the case study or the chosen topic within the placement to colleagues and/or other staff. Whilst this may seem daunting, it gives the student further experience of public presentation and an opportunity to discuss issues with other therapists. It might be a useful means of discussing current practice or sharing their view of patients/clients needs. Each area has its own needs and requirement for layout of the study. Therefore, one fixed method would be inappropriate. However, these are some content guidelines for a case study. Each case study includes:
• demographic details such as age and sex • social background such as social network, socio-economic markers, cultural
setting • history of presenting problem – what does the patient/client see as the
difficulty and how did he/she come to be in contact with occupational therapy/ physiotherapy.
• current interventions by others, such as medical and social work staff • assessment, including process of collecting data and formulating problems
planning intervention • intervention • outcome of intervention • current status and future plans • other agencies and their involvement/influence

The above are not necessarily section headings, but will feature in the content. Content may include items not covered above. The student also relates information to modules covered where possible. STUDY TIME AND TUTORIALS On full-time placements students need time to reflect on their experiences. Therefore it is recommended that one half day per week, or equivalent, be allocated for personal study. This provides opportunity for background reading, planning, preparation and evaluation. Study time should be included and recorded as part of the student’s total working hours. Students are expected to manage their own study time, however guidance from clinical/practice education supervisors about relevant topics and resources such as libraries or quiet rooms where they can work is appropriate. Part time placement students should be offered study time, it is suggested that one half day every two weeks would support the students in their personal study. The School favours students’ involvement in seminars, lectures and in-service education held within the clinical/practice environment. Profession specific tutorials by clinical/practice education supervisors effectively increase students’ knowledge and understanding and are much appreciated by students. The format and frequency of study time and in-service education is at the discretion of the clinical/practice education supervisor.
PLACEMENT B Progress in performance: During this placement, the student progresses from observation of the role of the supervising occupational therapist/physiotherapist/podiatrist to participation in the work of the supervising occupational therapist/physiotherapist/podiatrist. OBJECTIVES 1. Safety The student:
• follows the Health and Safety policies used by the placement; • contributes towards providing a safe environment for patients/clients, carers
and the general public; • plans, where reasonable, how to deal with the risks affecting a patient/client
in carrying out a therapeutic programme. 2. Interpersonal Skills The student:
• is aware of a range of communication needs among different patients/but needs guidance in meeting these needs;
• begins to relate theoretical knowledge and teaching strategies to the therapeutic situation;
• keeps accurate records of clinical intervention as requested and under supervisory guidance;
• communicates effectively with other team members under supervisory guidance.
3. Clinical Skills The student:
• collects information and carries out patient/client assessment with; guidance from the supervisor
• shows ability to discuss with the supervisor the assessment method, assessment findings and possible development of an action plan;
• uses supervisor guidance to implement the action plan, as far as it is reasonable and safe for the student to do so;
• shows regard for the patient’s/client’s position in respect of privacy, dignity and personal needs;
• shows ability to discuss with the supervisor the outcome of the action plan implementation and, where appropriate, the implications for future action or discharge.
4. Management Skills The student:
• takes his/her share in the daily tasks of the placement with guidance as necessary;
• shows insight into when he/she needs help from the supervisor or other staff; • presents a professional appearance and behaviour which facilitates the
therapeutic objectives towards which he/she is working; • organises himself/herself to be in the right place at the right time,
appropriately prepared for the task in hand; • shows an awareness of the policies and procedures operating in the
placement in as far as they have an obvious effect on the patients/client with whom the student is in contact.
PLACEMENTS C1 & C2 PLACEMENT C Progress in Performance: During this placement, the student progresses with this patient/client group from participation in the work of the supervising occupational therapist/physiotherapist/podiatrist to taking responsibility for his/her own caseload. OBJECTIVES 1. Safety The student:
• follows the Health and Safety policies used by the placement • contributes towards providing a safe environment for patients/clients, carers
and the general public • plans, where reasonable, how to deal with the risks affecting a patient/ client
in carrying out a therapeutic programme. 2. Interpersonal Skills The student:
• uses, where possible, the patient’s/client’s own perceived requirements of the student therapist to foster a therapeutic relationship
• relates different teaching strategies/approaches to the needs of different groups (patient/client groups, carers, public)
• keeps accurate, appropriate records of clinical intervention • uses knowledge of therapeutic progress to participate appropriately in team
decision making 3. Clinical Skills The student:
• shows an integration of current experience with prior learning • routinely collects information and carries out patient/client assessment with
some prompting as necessary • shows an understanding of the reasons for assessment method choice, and
the implications of assessment outcomes for planning intervention • implements action plans with the supervisor prompting as necessary • shows regard for the patient’s/client’s position in respect of privacy, dignity
and personal needs • relates outcomes of therapeutic intervention to modification of action plans,
recommendations for future action, or formulation of plan for discharge. 4. Management Skills The student:
• routinely shares in the general tasks of the placement • develops an appropriate balance between confidence in own abilities and
recognising when assistance is required • maintains a professional approach which facilitates an appropriate working
relationship with patients/clients and other team members • identifies and begins to use appropriate personnel, service and resources
available to patients/clients • demonstrates attention to relevant policies and procedures used within the
placement.
PLACEMENT D OBJECTIVES 1. Safety The student:
• follows the Health and Safety policies used by the department; • contributes towards providing a safe environment for patients/clients, carers
and the general public; • plans, where reasonable, how to deal with the risks affecting a patient/client
in carrying out a therapeutic programme. 2. Interpersonal Skills The student:
• varies his/her approach to suit the needs of each individual – patient/client, carer, other team members, and the public;
• uses teaching strategies appropriate to the needs of the individual patient/client, carer, other team member, and the public;
• maintains accurate, appropriate records of clinical intervention using these to share relevant information with the patient/client and the multidisciplinary team, in keeping with the professional duty of confidentiality;
• operates as a full and effective member of the multidisciplinary team. 3. Clinical Skills The student:
• shows an integration of current experience with prior learning; • uses information collected and assessment outcomes to plan therapeutic
intervention; • demonstrates ability to justify choice and use of particular assessments and
therapeutic interventions; • involves the patient/client and/or carers in clinical decision making whenever
practicable; • shows regard for the patient’s/client’s position in respect of privacy, dignity
and personal needs; • evaluates the outcomes of intervention, modify or close the action plan as
appropriate and implement a plan for discharge where appropriate. 4. Management Skills The student:
• routinely shares in the general tasks of the placement; organises own time and patient/client contact time;
• identifies and uses personnel, service and material resources available to the client;
• shows awareness of costs involved in planned interventions and relates individual patient/client need to financial resources available to the service;
• identifies and uses resources for personal learning and clinical support within the service;
• demonstrates an appreciation of the impact of relevant legislation on service operation.
GENERAL INFORMATION PREPARATION FOR PLACEMENTS Compulsory sessions held prior to the students beginning clinical/practice placements cover topics such as Moving and Handling, Health and Safety, professional behaviour and expectations. This work is closely linked to professional practice and, in addition, students are expected to prepare themselves by carrying out background reading about the patient/client group and treatment techniques. The following instructions have been given to the students: “The modules you complete in School form the major part of your preparation for placements. For instance, your professional skills will be tested in your first year and you will need to pass (i.e. demonstrate your competence in those skills) before you can progress to your first major clinical/practice placement, which is Placement B. When you know the type of placement you are going to, you will do some background reading about that particular patient/client group, team members’ roles, relevant techniques of assessment, and professional intervention.” For Placements B, C and D: “At least 2 weeks before you are due to go on placement, write to your supervisor introducing yourself and asking whether there is any particular preparation you can make. Your supervisor will be able to give you further details about accommodation, facilities on site, any special uniform requirements and anything unusual about travel arrangements. The School should have this kind of basic information to give you, but it is always possible that changes have happened which we do not know about and so it is useful to ask the supervisor in advance whether there is anything he/she wants you to know!” For all students: “Check in your letter, or with your supervisor if necessary, what time you are expected to arrive on the first morning. After that first morning, you will be expected to follow the pattern of hours set by the supervisor, which may include evening sessions if that is normal for the area. If your personal responsibilities preclude this, let your tutor know in your personal review.”
INSURANCE Students are covered by University insurance when they are at the University and in the clinical/practice placement setting as long as they are undertaking activity for which they have been trained and under the supervision of their practice placement supervisor. The practice placement provider has been asked to agree to accept vicarious liability for the actions of the students whilst on placement. The agreement is recorded as part of the service level agreement with the practice placement provider. SAFETY The School recognises the importance of safe practice and incorporates this aspect directly into the clinical/practice placement assessment report. These issues are discussed during the clinical briefing sessions and the School ensures that students:
• are instructed in current moving and handling techniques • attend Health and Safety lectures • are instructed in first aid and basic life support • are advised to receive clear guidance, during clinical/practice placement
induction, of the consent for treatment policy, lone working policy, accident and incident reporting policy (including needle stick injuries if appropriate to the placement) and have clear comprehension of their role as a student in adhering to them within the clinical/practice placement setting
• are responsible for their own car insurance and safe travel when travelling to Placements
The following instructions have been given to the students: “Never attempt anything in the clinical/practice setting for which you have not been trained or in which you do not feel confident of a safe outcome for your patient/client. Likewise, never disregard an instruction from your supervisor. Follow the policies and procedures used by the department in which you are on placement. Rehabilitation is a risky business for your clients – someone who is learning to walk again after a stroke is clearly at greater risk of falling than he/she was before the stroke. Part of the professional judgement you will be learning is to balance risk against benefit and to manage risks as safely as possible for your patients/clients. Especially in the early stages, your supervisor will be more aware of the risks inherent in the activities you undertake with your patients/ clients and his/her instructions will be protecting you as well as the patient/ client. It may be that your supervisor believes you have practised a technique when you have not. If you are asked to do something with a patient/client which is strange to you, then refuse politely and explain why. Your supervisor can practice it with you and then you can carry out his/her instructions. You are covered by insurance for accident, but what has been outlined above is negligence – a much more serious matter which leaves both you, and possibly the School, open to legal retribution. It must also be obvious that we cannot allow a student who has shown him/herself to be negligent to continue on the course. This passage is not supposed to instil you with fear and dread of ever touching a patient/client, but it is necessary to be clear that you have responsibility to play your own part in ensuring the safety of the patients/clients in your care. Finally, you are required to attend certain health and safety sessions during the first year, which will ensure that you are prepared, for instance, for moving and handling safely. These sessions are compulsory and we cannot allow you into the clinical setting without having done them.
The sessions comprise: • Clinical briefing; including resuscitation and lone working policy advice • Health and Safety & Moving and Handling.
Finally, insurance cover for yourself comes through the University and the Professional bodies. If you take a car out on practice, the insurance cover does not extend to this. Do not take patients/clients out in your car and, if you use it to get yourself to your destination and/or to carry equipment, check that your own car insurance covers this.” LONE WORKING POSITION STATEMENT Lone working is an integral part of clinical work for many therapists. Students undertaking their clinical/practice placements may have the opportunity for lone working. However, the individual student must be assessed to be competent on all skills (communication/clinical/managerial) required to undertake lone working, and be confident in their knowledge and implementation of the local lone working policy. Risk assessment should be carried out according to local policy. It is therefore not expected that students will undertake lone working in the initial weeks of their clinical/practice placement. ACCIDENT OR INCIDENT ON PLACEMENT Accidents or incidents may occur despite your best efforts as a supervisor and compliance with risk assessment/management implementation. Each clinical/practice placement setting will have clear policies and procedures to follow in the event of an accident or incident (including “Needlestick injuries”). The Clinical/Practice Assessment form front page makes specific reference to any accident or incident and requests that you forward all completed forms with the assessment form. Where an accident or incident has occurred in response to unsafe practice or requires the student to take a period of sick leave please inform your locality contact as soon as possible. The following instructions have been given to the students: “If you are involved in an accident or incident on placement, please take advantage of any staff member in the immediate vicinity but make sure your supervisor knows as soon as possible. There will be policies and procedures to follow to manage and record the incident. Follow the guidance given by your supervisor. You will be required to complete the organisation’s ‘Accident/Incident’ form. This is normal practice for all staff and students within a health and social care organisation. A copy of the completed form will be forwarded to the clinical practice office for our records and so that we can ensure your and future student’s safety. Your supervisor has been made aware of this requirement.” SICKNESS The School ensures that students have clear guidelines to follow should they become ill during clinical/practice placements. Students are expected to inform their clinical/practice education supervisors immediately they become ill and provide a self- certificate for the first 6 days. A doctor’s certificate is required from the 7th day. This is sent directly to their supervisors, who then forward this to the Clinical/Practice Secretary at the School. Students may require emergency health care whilst on placement resulting from, for instance, an accident at work. Serious and sudden need can be dealt with through the local casualty department (e.g. cuts and fractures). In some cases, work related health problems may be dealt with by the local Occupational Health Department. However, health care needs may be less dramatic
or serious but still an issue (e.g. infections) during clinical/practice placements. Students may need to see a GP. For this reason, during the 6 and 12 week placements students will be expected to sign on as visitors with the GP practice nearest to their accommodation. The following instructions have been given to the students: “Hopefully, you will go through this course in a hale and hearty condition. However, you will be in contact with a number of infective agents with which your immune system is unfamiliar – the problem with hospitals is that they are full of sick people, with a few infective agents that are beyond anyone’s system to combat. There are some things you must do to safeguard yourself and others:
1. Co-operate with the initial medical check up – you have got to be safe to go out on practice. If you have any problem which could affect your safety, patient/client care during placement, or requires extra planning on placement, see your course leader about sending a health and special requirements note to your clinical/practice education supervisor.
2. You must have been vaccinated for Hepatitis B (etc). It is unlikely you would catch any of these things, but take the maximum precautions available to minimise any episodes of illness.
3. In areas where you may come into contact with some of the more untreatable conditions, such as HIV, there will be procedures to contain the infective agent and to protect you. FOLLOW THEM.
4. In some areas, even a slight infection can be dangerous to others. If you feel off colour, let your supervisor know, so that he or she can decide if you are safe to continue that day. If you are told to leave the area, then just go. We ensure that you have more than the minimum hours and it will take a long absence to put you in danger of needing a further placement. Assessment will take your absence into account and each situation will be judged on its own merit.”
Should you fall sick, you need to let your supervisor know that same working day. For the first 6 days you need to fill in a self-certification form that your supervisor will return to us. From the seventh day you will need a doctor’s certificate that your supervisor will send on to us. If the sickness is serious enough to warrant medical attention, we would like to hear directly from you as well as receiving the medical certificate from your supervisor. Call the Clinical/Practice Secretary on 023 8059 7041. It may be that your supervisor falls sick. Your supervisor’s manager is the first in line of call. In your first placement you will need daily supervision, but as your course progresses there will be flexibility about how much time you can spend alone and what tasks you can undertake. However, you must always have access to a qualified therapist. It may be that your supervisor’s manager or a delegate member of staff can Reorganise your programme to deal with the situation. If the situation looks set to continue for some time or it is not possible to reorganise your programme to cope, we would like to hear from you and your supervisor’s manager. Again, call the profession specific administrator. REPORTING MENTAL HEALTH CONCERNS The Department of Health published “Mental Health and Employment in the NHS” in October 2002. School guidance has been developed from the Department of Health’s document and the University of Southampton’s “The Management of Acute

Mental Health Emergencies”. The University of Southampton published its Mental Health Policy in 2002. One of the principles is “to ensure that all employees and students who experience mental health difficulties are treated fairly, sensitively and with respect, and are offered the support that they need to deal with their particular situation. The School of Health Professions and Rehabilitation Science has a responsibility under the Special Educational Needs and Disability Act 2001 to avoid discriminating against students with disabilities, including mental illness. If a student’s behaviour gives you cause for concern, do not worry about whether you are qualified to decide whether or not they have a mental health condition; your concern is sufficient cause, so contact the university locality contact immediately either by telephone or through the AHP Assistant for practice placements on 023 8059 8835 or [email protected]. Also contact your Occupational Health department for local assistance. It is the responsibility of the GP with whom the student is registered to provide professional support and care in incidents of mental illness. Whilst students are advised to register with a local GP for each placement of more than 6 weeks duration, their compliance with this advice may be limited. If you consider the student is showing signs of an acute mental health emergency you should attempt to discover the identity of the student’s GP, and, where this is known, report your concerns to the GP. Alternatively contact your Occupational Health department immediately and report your concerns to the locality contact immediately. Whilst you should limit the amount of information you reveal to external sources in order to protect the student’s confidentiality, it is entirely appropriate to inform services of any information that may be relevant to their evaluation of the situation. Do not contact the student’s family or friends unless specifically requested to do so by the student in person. The Duty of Confidentiality under the Data Protection Act 1998 is limited by the Duty of Care that we have to students and staff. The duty of care takes precedence where there are serious concerns about an individual’s mental or physical health or for the safety of others to serious risk from that person. The University recognises an acute mental health emergency may consist of any of the following: • The person is considered to be an immediate danger to themselves • The person is considered to be an immediate danger to others • The person is exhibiting extreme distress • The person is neglecting their own health (e.g. neglecting medication, self care or failing to eat adequately) such that they may trigger a crisis Please contact the University if you have any concerns and for further advice.

TO ALL OUR CLINICAL/FIELDWORK SUPERVISORS: We look forward to working with you in the future. If you have any queries regarding this handbook or clinical/practice placements in general, please do not hesitate to e-mail [email protected]
APPENDIX 1 MOVING AND HANDLING ADVICE Dear Supervisor, The following information is relevant to the current intake of students. By the time our students reach you for their clinical/practice placement, they will have completed their moving and handling training. This will include;
Basic biomechanics Normal movement Core moving and handling principles/skills Legislation Risk assessment
Students are also aware of handling techniques which are now considered unsafe and should not be used in clinical practice. These are:
Drag/under-arm holding Australian Lift Through-arm/top and tail lift Cradle/orthodox lift Manually lifting from the floor Manually lifting from the bath Placing patients/clients’’ arms around or near the handlers neck Basic Biomechanics
This is divided into the theory and practical application of the following principles;
Planes & axes Centre of gravity, line of gravity and base of support Stability Friction Forces and Levers
Core Moving and Handling Skills Students are taught core moving and handling skills under the following key headings;
General moving and handling (1) – handling inanimate loads and use of transfer equipment to assist non weight bearing patients/clients.
General moving and handling (2) – assisting a person to move in and out of a chair,walking and getting up from the floor following a fall
Hoisting Moving people in bed Management of the falling person, plus strategies for falls prevention.
All handling principles have been cross-referenced to the BackCare ‘Guide to the Handling of People’ (5th edition) where possible. In each area, normal movement and biomechanics is considered within the context of the moving and handling principles being taught. Students spend one half day in each of the above areas, receiving instruction and supervision in the relevant, current safe handling practices. Simple case studies are used to reinforce the principles taught. Revision time is programmed into the module to allow students to practice the principles/techniques learnt. Tutors are available on request to assist with revision. Students attend a one hour session in small groups, on complex handling which involves learning and practicing management of the falling person. Students are closely supervised during this session.
Assessment Students are assessed in all the theoretical principles taught in the module in a written extended matching questions paper. Moving and handling skills are assessed in a practical exam where students may be examined in a combination of any manoeuvres learnt in the moving and handling module. The following is a list of practices taught, with the relevant reference from the ‘Guide to the Handling of People’ (5th edition) where appropriate. General Moving and Handling • Assisting a person to move forward/backward and position themselves in a chair (Ch.14) • Assisting a person from sitting to standing and vice versa, with and without the use of a handling belt. (Ch.12) • Transfers (Ch.14) (Note: the use of a turntable as shown on page 166 is not taught as it is felt this technique puts students at risk of injury due to lack of clinical judgement skills.) • Assisted walking (Ch.13) • The falling and fallen person. (Ch.17) Hoisting • Hoisting a person from the floor. (Ch.17) • Hoisting a person between bed and chair and between chairs. (Chapters 14 & 15) • Moving a person in bed using a hoist. (Ch.15) Moving People in Bed • Helping a person in/out of bed. (Ch.15) • Helping a person to sit up in bed – one carer. (Ch.15) • Helping a person to sit up in bed (Ch.15) • Assisting a person to move up the bed in sitting and through sitting on the edge of the bed (not illustrated in the 5th edition) • Rolling/turning/positioning a conscious person in bed. (Ch.16) • Rolling/turning/positioning an unconscious person in bed. (Ch.16) Managing the falling person Students are taught and closely supervised in the practice of assisting a falling person to the floor. Principles of counter-force/balance and friction are emphasised for this manoeuvre. (NOTE: the technique is slightly different to that shown in the Guide to the Handling of People, however the basic principle of not holding the person or arresting the fall is the same) Moving and Handling Equipment
Turntables (hard and soft) Transfer Boards Rope Ladders Patient Handling Slings (only recommended for moving people forward in a
chair, or used by 2 carers to assist a person to sit up in bed as an interim strategy).
Patient Handling Belts Slide Sheets (low friction rollers) removed after manoeuvre. One way glide sheets Hand Blocks Arjo, Oxford and LIKO Hoists Quick-fit, Quick-fit deluxe and Access slings

Stedy Electric Stand Aids Mangar Elk
We endeavour to provide a comprehensive introduction to these subjects at good staff student ratios. We acknowledge however, that in many areas of clinical practice, our students may lack specific skills particular to your field of work. Our aim is to provide the students with basic skills and we ask that you offer additional training if necessary, to enable them to meet your service requirements. Students are told not to participate in moving and handling activities which they feel may put themselves or patients/clients at risk. If this raises issues while the students are on placement, please feel free to ring Maggie Bracher on the number below. If a student fails their moving and handling exam prior to placement B, they will undertake an individual review session with the unit co-ordinator or relevant other. As with the review of failures in other practical exams at this time, the staff member undertakes a risk assessment to consider whether the student presents a risk to patients, colleagues or themselves. If such a risk is considered to exist the student will not be allowed to go on placement until they successfully complete the resits of the relevant practical exam[s]. Where there is not considered to be a risk and the student goes on placement you will still receive a letter informing you of the situation and asking you to ensure supervision during any moving and handling procedures to assure yourself of their competence, and ensure safety for both the student and patient/client. This should not influence the overall assessment of the student’s performance while on placement unless they are clearly showing signs of unsafe practice. If you would like to discuss this further at any time during the placement, please feel free to ring Maggie Bracher on Tel: 023 8059 5086
APPENDIX 2 REPORTING MENTAL HEALTH CONCERNS Dear Supervisor The Department of Health published “Mental Health and Employment in the NHS” in October 2002 and the University of Southampton also published its Mental Health Policy in 2002. The guidance outlined in this appendix has been developed from the Department of Health’s document and the University of Southampton’s “The Management of Acute Mental Health Emergencies”. One of the University of Southampton’s principles is “to ensure that all employees and students who experience mental health difficulties are treated fairly, sensitively and with respect, and are offered the support that they need to deal with their particular situation. The School of Health Sciences has a responsibility under the Special Educational Needs and Disability Act 2001 to avoid discriminating against students with disabilities, including mental illness. If a student’s behaviour gives you cause for concern, do not worry about whether you are qualified to decide whether or not they have a mental health condition; your concern is sufficient cause, so contact the university locality contact immediately either by telephone or through the AHP Practice Placement Assistant on 023-8059-8835 or [email protected]. Also contact your Occupational Health department for local assistance. It is the responsibility of the GP with whom the student is registered to provide professional support and care in incidents of mental illness. Whilst students are advised to register with a local GP for each placement of more than 6 weeks duration, their compliance with this advice may be limited. If you consider the student is showing signs of an acute mental health emergency you should attempt to discover the identity of the student’s GP, and, where this is known, report your concerns to the GP. Alternatively contact your Occupational Health department immediately and report your concerns to the locality contact immediately. Whilst you should limit the amount of information you reveal to external sources in order to protect the student’s confidentiality, it is entirely appropriate to inform services of any information that may be relevant to their evaluation of the situation. Do not contact the student’s family or friends unless specifically requested to do so by the student in person. The Duty of Confidentiality under the Data Protection Act 1998 is limited by the Duty of Care that we have to students and staff. The duty of care takes precedence where there are serious concerns about an individual’s mental or physical health or for the safety of others to serious risk from that person. The University recognises an acute mental health emergency may consist of any of the following:
The person is considered to be an immediate danger to themselves The person is considered to be an immediate danger to others The person is exhibiting extreme distress The person is neglecting their own health (e.g. neglecting medication, self care or
failing to eat adequately) such that they may trigger a crisis Please contact your locality contact immediately should you have any concerns and they will then advise you further, in conjunction with GP and Occupational Health advice, about whether the student will be able to continue with the placement or should be withdrawn on health grounds.
APPENDIX 3 CLINICAL/PRACTICE PLACEMENTS FOR DISABLED STUDENTS The School of Health Sciences and Clinical/Practice Placement providers are required to adhere to the Disability Discrimination Act (DDA) (2002) with particular reference to part IV, which specifically refers to special educational needs and disability. The School of Health Sciences must also adhere to The Quality Assurance Agency (QAA) for Higher Education’s Code of Practice relating to students with disabilities to ensure that such students have a learning experience comparable to their peers. The DDA defines disability as any physical or mental impairment that has a substantial and long-term adverse effect on his/her ability to carry out normal day-today activities. Long-term is defined as in excess of 1 year. Even if there is recovery or the problem improves the student is defined as being disabled. Physical or mental impairment includes:
Physical disabilities Sensory impairments Dyslexia Severe disfigurements Autistic spectrum disorders Mental health difficulties Medical conditions e.g. epilepsy, diabetes etc
The legislation has been put in place to prevent discrimination, which is defined as treating disabled people “less favourably” than other people for a reason relating to their disability without justification. In addition failing to make reasonable adjustment when disabled people are placed at a serious disadvantage compared to other people, for a reason relating to their disability. Reasonable adjustment is dependent on each individual student’s circumstances and may include:
Changes to the institutional procedures Adapting the curriculum Providing additional support Training staff Changing the physical environment
These adjustments need to be considered in relation to clinical/practice placement environments. The School’s Admissions Teams work closely with the Clinical/Practice Placement Co-ordinators and communicate clearly the expected needs of any prospective student once a place has been offered. On entry to the School the student completes a health declaration form and once they have had a satisfactory occupational health check the Clinical/Placement Coordinators will discuss, with clinical/practice placement providers, the needs of each individual student in order to ensure they achieve the required clinical/practice hours to be licensed to practice on graduation. Health and Social Care Organisations who have provided clinical/practice placements in the past are approached initially since the support networks and “adjustments” required are already in place. Where possible the student will be placed in one Health or Social Care Organisation for all their placements if that organisation can provide the breadth of placements required. Previous disabled students have identified positive benefits of such single organisation placements as beneficial.

When going on placement students do not have to disclose their disability, unless safety is compromised. Information cannot be shared between the academic institution and the placement provider without the students consent. Whilst the University is responsible for ensuring the suitability of the placement and funding any adjustments within the placement environment which are seen to be reasonable e.g. additional hardware /software etc or a support worker on placement, the placement providers also have a duty under part III of the DDA to make reasonable adjustments in order to prevent discrimination against disabled people who have access to their services. The COT and CSP have produced guidance to academic institutions, clinicians and practitioners and further information is available on their respective websites www.cot.org.uk www.csp.org.uk The Quality Assurance Agency for Higher Education, Code of Practice, Students with Disabilities can be reviewed at http://www.qaa.ac.uk/public/COP/COPswd/contents.htm
APPENDIX 4 VALID CONSENT TO EXAMINATION AND TREATMENT Clinical/Practice Placements: Consent for Examination and/or Treatment Consent, by patients/clients, to examination and treatment is a core principle underpinning clinical practice. The Health Professions Council outlines in its Standards of conduct, performance and ethics. Your duties as a registrant: 2003, that “You must get informed consent to give treatment (except in an emergency)”, and since the incorporation of the European Convention of Human Rights into English Law as the Human Rights Act, treatment without informed consent is a potential breach of the act under article eight. Informed consent suggests that all and or complete information has been provided including all possible outcomes of any intervention that is proposed. Whilst this may be the intention, if challenged the information given may be incomplete and therefore open to possible litigation. Recent Department of Health advice to all professions has suggested a change in terminology from informed consent to valid consent. Patient’s and clients have a fundamental legal and ethical right to determine what happens to their own bodies. Valid consent to treatment is therefore absolutely central in all forms of healthcare. The Department of Health states that consent is a patient’s agreement for a health professional to provide care. For consent to be valid, the patient must:
Be competent to take the particular decision Have received sufficient information to take it; and Not be acting under duress
The patient’s actual consent to examination or treatment is only the end point of the whole consent process. This process includes the provision of information, discussion and decision-making. The health professional carrying out the assessment or treatment is ultimately responsible for ensuring that the patient is genuinely consenting to what is being done. If the process of seeking consent is to be a meaningful one, refusal must be one of the patient or client’s options. A competent adult is entitled to refuse any treatment, except in circumstances governed by the Mental Health Act 1983. The situation for children is more complex and you should refer to the Department of Health’s Seeking consent: Working with children. Patients and clients need sufficient information before they can decide whether to give their consent and if a patient or client is not offered as much information as they reasonably need, and in a form they can understand then their consent may not be valid. It is a health professional’s own responsibility:
To ensure that when they require colleagues to seek consent on their behalf they are confident that the colleague is competent to do so; and
To work within their competence and not to agree to perform tasks which exceed that competence.
Therefore, when or if students are asked to seek consent to examination and/or treatment it is the responsibility of the Clinical/Practice Education Supervisor to ensure that the student is competent to do so. The Department of Health has issued a number of guidance documents on consent that are available at

www.doh.gov.uk/consent and should be reviewed in conjunction with the regulatory and individual professional bodies guidance.
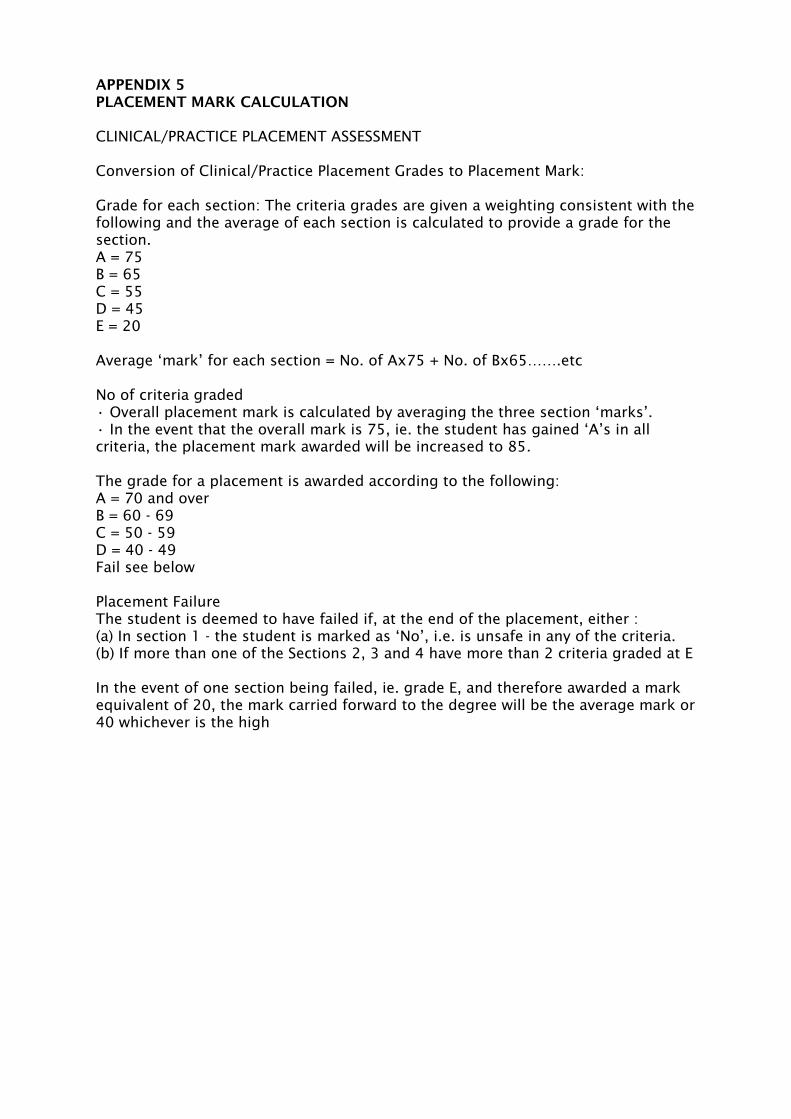
APPENDIX 5 PLACEMENT MARK CALCULATION CLINICAL/PRACTICE PLACEMENT ASSESSMENT Conversion of Clinical/Practice Placement Grades to Placement Mark: Grade for each section: The criteria grades are given a weighting consistent with the following and the average of each section is calculated to provide a grade for the section. A = 75 B = 65 C = 55 D = 45 E = 20 Average ‘mark’ for each section = No. of Ax75 + No. of Bx65…….etc No of criteria graded • Overall placement mark is calculated by averaging the three section ‘marks’. • In the event that the overall mark is 75, ie. the student has gained ‘A’s in all criteria, the placement mark awarded will be increased to 85. The grade for a placement is awarded according to the following: A = 70 and over B = 60 - 69 C = 50 - 59 D = 40 - 49 Fail see below Placement Failure The student is deemed to have failed if, at the end of the placement, either : (a) In section 1 - the student is marked as ‘No’, i.e. is unsafe in any of the criteria. (b) If more than one of the Sections 2, 3 and 4 have more than 2 criteria graded at E In the event of one section being failed, ie. grade E, and therefore awarded a mark equivalent of 20, the mark carried forward to the degree will be the average mark or 40 whichever is the high
PROGRESSION AND WEIGHTING OF ASSESSMENTS
Assessments are varied throughout the three levels of the programme to provide students with the opportunities to express their knowledge, attitudes and skills in different ways.
In the same way that the modules become more challenging over the three levels, so the assessments are progressively more complex.
Level 1 The assessment tasks are quite structured and students are required to carry out specific instructions. All summative assessments are compulsory. Whilst none of these assessments contribute to the honours classification, successful completion of these assessments is required to continue into Level 2 of the course. Level 2 Level 2 students begin to take more responsibility for selecting and organising the material presented in the assessments. All summative assessments are compulsory and contribute towards the honours classification. Level 3 There are no unseen assessments at Level 3 as the students have some freedom in choosing the topics/areas that will be evaluated. All summative assessments are compulsory and contribute towards the honours classification.
ADDITIONAL INFORMATION ABOUT PHYSIOTHERAPY PLACEMENTS It is not expected that you will be exposed to all common conditions, use all the usual physiotherapy interventions or be exposed to every type of context in which patients are managed. The priority is to ensure that you are familiar with and competent in the principles of assessment, planning, management and evaluation relevant to the area so that you can apply them in new and different situations in the future. As a consequence, these skills can be developed in a range of different contexts as long as there is exposure to a sufficient number and range of symptoms/problems/cases. The following gives a guide as to what that could include and what opportunities the learning experience could provide in each particular area of practice. PLACEMENT B – Neuromusculoskeletal 1 (6 Weeks) You will normally work with adult patients with simple musculoskeletal problems. You may work in in-patient or out-patient settings or both, e.g. T&O, orthopaedics, M/S outpatients, rheumatology [or Elderly Care, General Rehab for part-time students]. You should develop and apply a variety of assessment, planning, treatment and evaluation skills, and may involve treatment approaches that include: Joint mobilisation, Soft tissue techniques, Muscle strengthening, Electrotherapy, Gait re-education, Pain relief. Part-time students will only be able to use the approaches you have covered in year 1 of your programme. Your approach is to involve the patient throughout the therapeutic process in order to achieve an optimal functional outcome. Opportunities for you to broaden your experience are welcomed. These may include:
• attendance at theatre (orthopaedic procedures) • attendance at orthopaedic clinics, both uni- and multi-professional • involvement with paediatric orthopaedic patients • participation in home visits or other community interventions • involvement with related professional groups
PLACEMENT C1, C2, D1 and D2 These placements provide you with a variety of clinical experience. C Placements consist of two distinct blocks of 6 weeks each, named C1 and C2. The C1 Placement occurs in the first semester and C2 in the second semester of the second year, normally after Easter. The D Placements are two distinct blocks of 5 weeks each, named D1 and D2. These are two consecutive placements. The Placement D1 occurs at the end of semester 1 and D2 at the beginning of Semester 2 in the third year. PLACEMENTS C1 AND C2 – Acute/Non-acute/Neuro (6 weeks each) [may include neuromusculoskeletal 1 for part-time students] During C Placements, you will experience any two of the following:
Acute – Cardio –respiratory care OR Non-acute care/Special Client Groups OR Neurological Rehabilitation
* See Definitions below for detailed information PLACEMENTS D1 AND D2 – Neuromusculoskeletal 2/Acute/Non-acute/Neuro (5 weeks each)
One of these will be Neuromusculoskeletal 2; the other will be the one of the following that you haven’t yet completed:
Acute – Cardio –respiratory care Non-acute care/Special Client Groups Neurological Rehabilitation
DEFINITIONS NON-ACUTE CARE/SPECIAL CLIENT GROUPS You will work with patients in any of a range of settings, e.g. community hospital, rehabilitation unit, school, hospice, residential home, domiciliary, or with specialist client groups such as Older People, Learning Disabilities, Mental Health, Palliative Care/Oncology, Paediatrics, Women’s Health etc. You will learn to adapt and vary your core skills to suit the context and/or client group. These may include: modification of assessment/treatment techniques according to the environment or client group; education, advice and support to patients/clients and carers; multidisciplinary working/networking in the community setting or client group; personal safety during community based practice or with the particular client group. NEUROLOGICAL REHABILITATION It is not expected that you will be exposed to all common conditions, use all the usual physiotherapy interventions or be exposed to every type of context in which patients with neurological conditions are managed. The priority is to ensure that you are familiar with and competent in the principles of neurological assessment, planning and management so that you can apply them in new and different situations in the future. As a consequence, these skills can be developed in a range of different contexts as long as there is exposure to a sufficient number and range of symptoms/problems. NB: Normally it is expected that you will be exposed to adults with neurological problems but it may be combined with experience of other client groups, e.g. Paediatrics. Experience: Neurological rehabilitation focuses on diseases and trauma to the Central Nervous System i.e. the brain and spinal cord. Your learning is about the management of symptoms and not conditions i.e. an understanding of spasticity within the context of different conditions e.g. MS, CVA, spinal cord injury, brain injury. Learning also focuses on the movement disorders associated with neurological symptoms and how therapists can re-educate normal movement patterns. The main neurological symptoms you have been taught are concerned with upper motor neurone syndrome i.e. central nervous system disease/damage. These include spasticity, flexor/extensor spasms, dysynergic movement patterns, associated reactions, weakness, loss of dexterity. Management of conditions is taught broadly as acute and progressive again within the context of its application to symptoms. On placement it is important that you assess and treat a variety of neurological symptoms but not necessarily a variety of conditions. Physiotherapy skills to include: Assessment skills relative to:
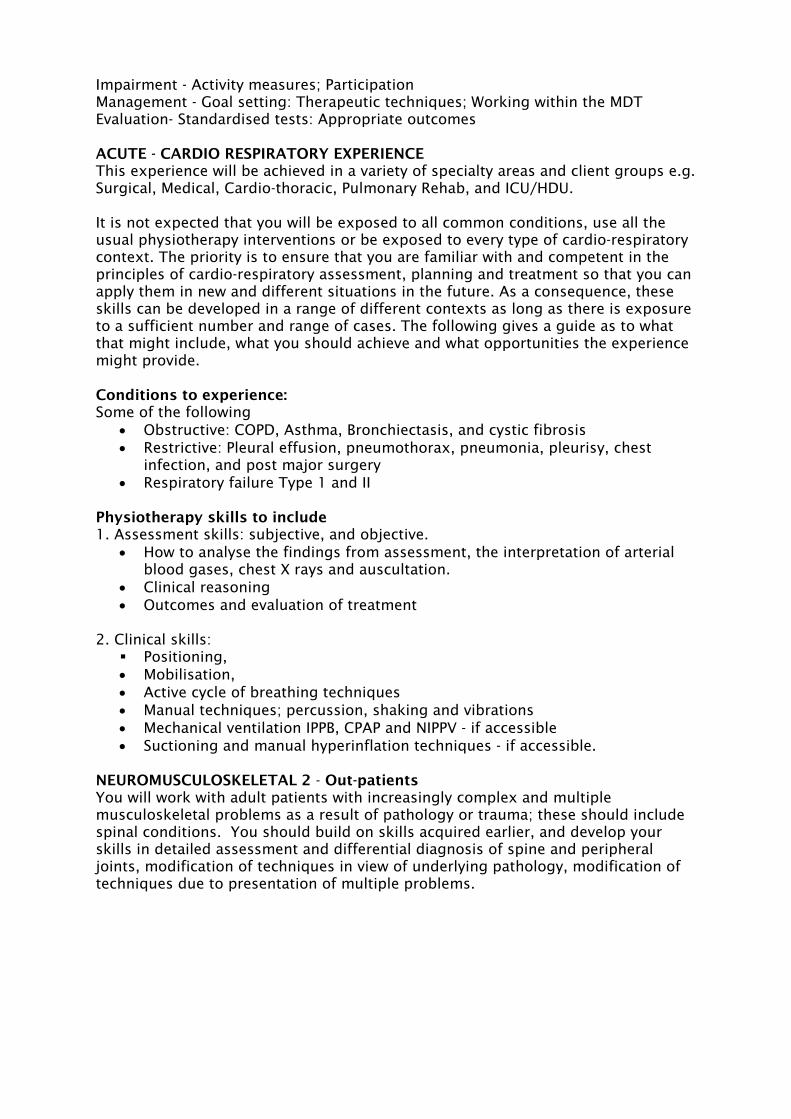
Impairment - Activity measures; Participation Management - Goal setting: Therapeutic techniques; Working within the MDT Evaluation- Standardised tests: Appropriate outcomes ACUTE - CARDIO RESPIRATORY EXPERIENCE This experience will be achieved in a variety of specialty areas and client groups e.g. Surgical, Medical, Cardio-thoracic, Pulmonary Rehab, and ICU/HDU. It is not expected that you will be exposed to all common conditions, use all the usual physiotherapy interventions or be exposed to every type of cardio-respiratory context. The priority is to ensure that you are familiar with and competent in the principles of cardio-respiratory assessment, planning and treatment so that you can apply them in new and different situations in the future. As a consequence, these skills can be developed in a range of different contexts as long as there is exposure to a sufficient number and range of cases. The following gives a guide as to what that might include, what you should achieve and what opportunities the experience might provide. Conditions to experience: Some of the following
• Obstructive: COPD, Asthma, Bronchiectasis, and cystic fibrosis • Restrictive: Pleural effusion, pneumothorax, pneumonia, pleurisy, chest
infection, and post major surgery • Respiratory failure Type 1 and II
Physiotherapy skills to include 1. Assessment skills: subjective, and objective.
• How to analyse the findings from assessment, the interpretation of arterial blood gases, chest X rays and auscultation.
• Clinical reasoning • Outcomes and evaluation of treatment
2. Clinical skills:
Positioning, • Mobilisation, • Active cycle of breathing techniques • Manual techniques; percussion, shaking and vibrations • Mechanical ventilation IPPB, CPAP and NIPPV - if accessible • Suctioning and manual hyperinflation techniques - if accessible.
NEUROMUSCULOSKELETAL 2 - Out-patients You will work with adult patients with increasingly complex and multiple musculoskeletal problems as a result of pathology or trauma; these should include spinal conditions. You should build on skills acquired earlier, and develop your skills in detailed assessment and differential diagnosis of spine and peripheral joints, modification of techniques in view of underlying pathology, modification of techniques due to presentation of multiple problems.
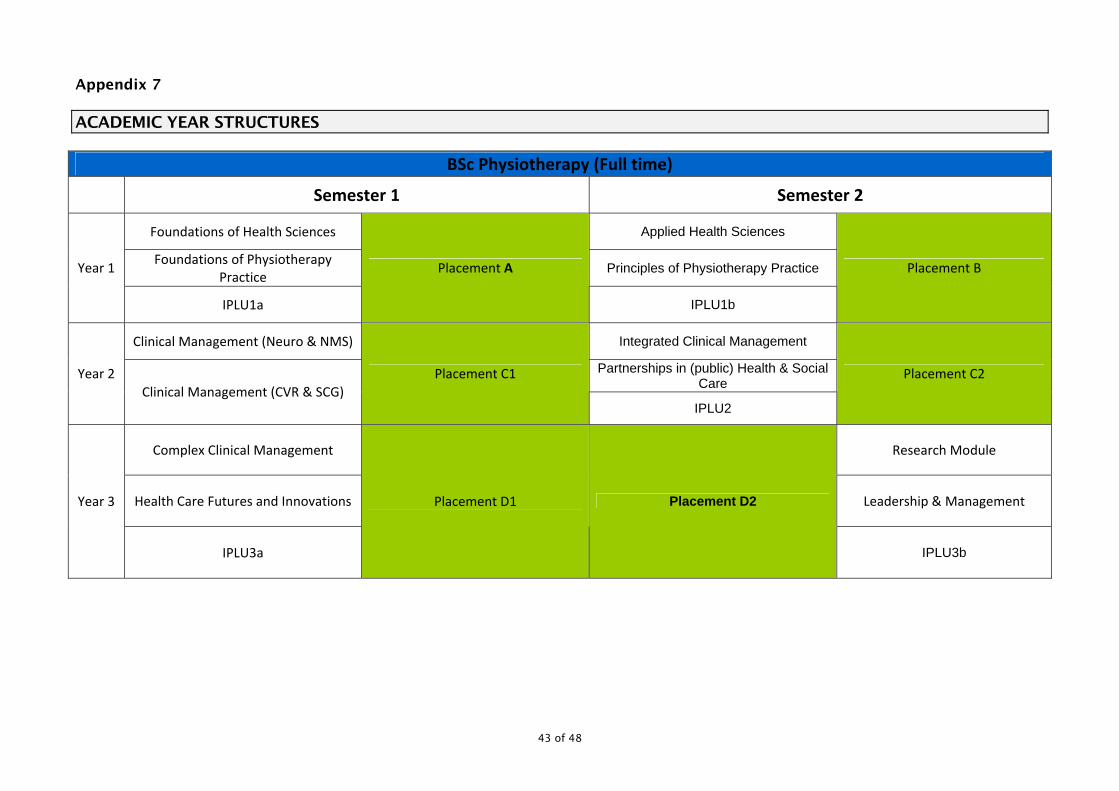
43 of 48
Appendix 7 ACADEMIC YEAR STRUCTURES
BSc Physiotherapy (Full time)
Semester 1 Semester 2
Foundations of Health Sciences Applied Health Sciences
Foundations of Physiotherapy Practice
Principles of Physiotherapy Practice Year 1
IPLU1a
Placement A
IPLU1b
Placement B
Clinical Management (Neuro & NMS) Integrated Clinical Management
Partnerships in (public) Health & Social Care
Year 2 Clinical Management (CVR & SCG)
Placement C1
IPLU2
Placement C2
Complex Clinical Management Research Module
Health Care Futures and Innovations Leadership & Management Year 3
IPLU3a
Placement D1 Placement D2
IPLU3b
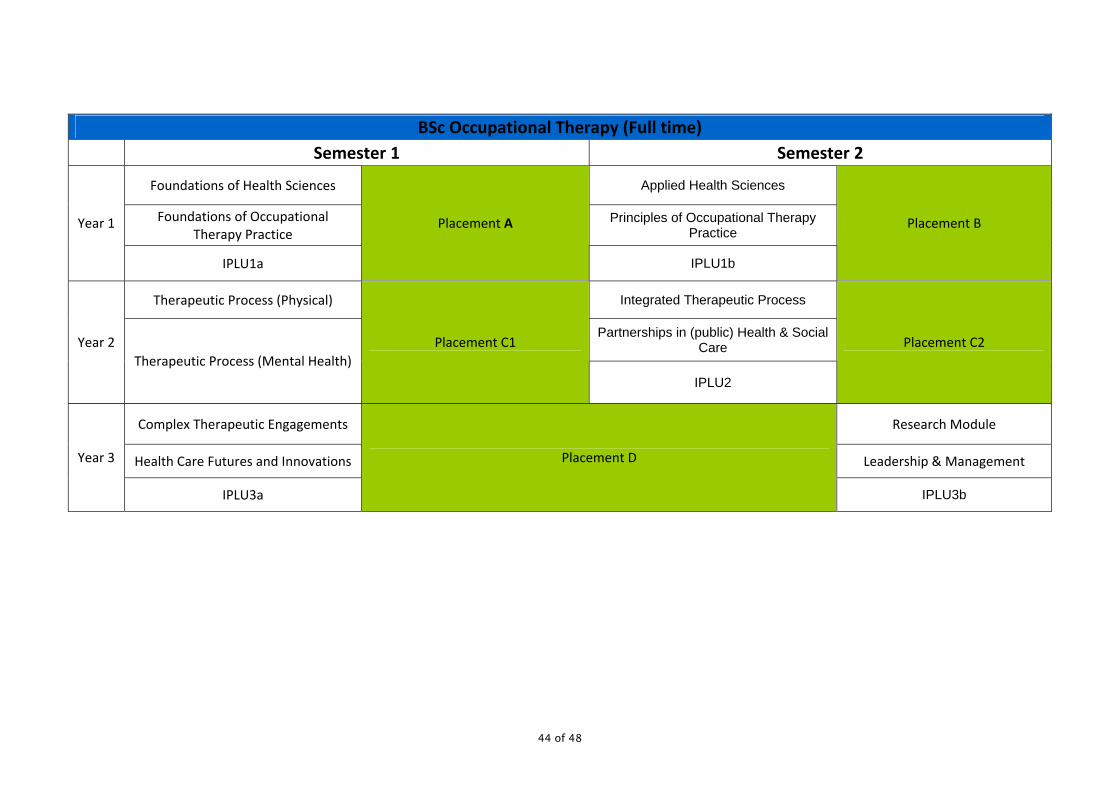
44 of 48
BSc Occupational Therapy (Full time) Semester 1 Semester 2
Foundations of Health Sciences Applied Health Sciences
Foundations of Occupational Therapy Practice
Principles of Occupational Therapy Practice
Year 1
IPLU1a
Placement A
IPLU1b
Placement B
Therapeutic Process (Physical) Integrated Therapeutic Process
Partnerships in (public) Health & Social Care Year 2
Therapeutic Process (Mental Health) Placement C1
IPLU2
Placement C2
Complex Therapeutic Engagements Research Module
Health Care Futures and Innovations Leadership & Management Year 3
IPLU3a
Placement D
IPLU3b
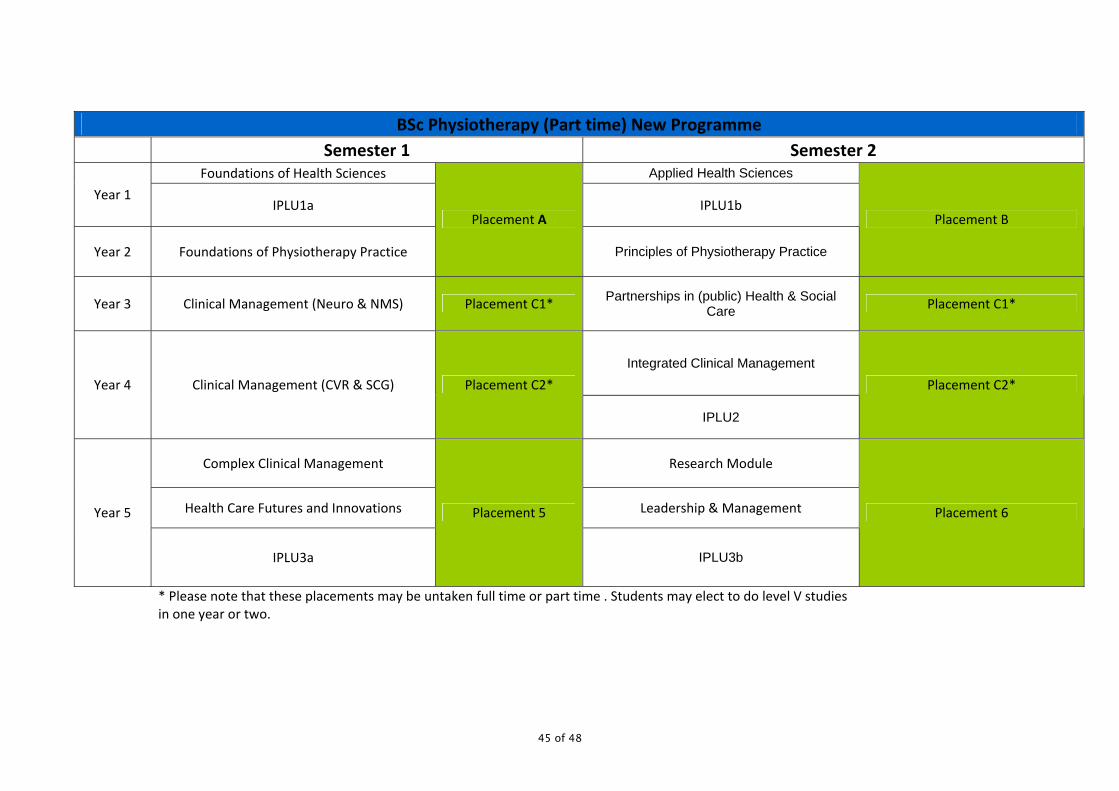
45 of 48
BSc Physiotherapy (Part time) New Programme Semester 1 Semester 2
Foundations of Health Sciences Applied Health Sciences Year 1
IPLU1a IPLU1b
Year 2 Foundations of Physiotherapy Practice
Placement A
Principles of Physiotherapy Practice
Placement B
Year 3 Clinical Management (Neuro & NMS) Placement C1* Partnerships in (public) Health & Social Care Placement C1*
Integrated Clinical Management Year 4 Clinical Management (CVR & SCG) Placement C2*
IPLU2
Placement C2*
Complex Clinical Management Research Module
Health Care Futures and Innovations Leadership & Management Year 5
IPLU3a
Placement 5
IPLU3b
Placement 6
* Please note that these placements may be untaken full time or part time . Students may elect to do level V studies in one year or two.

46 of 48
BSc Occupational Therapy (Part time) New Programme Semester 1 Semester 2
Year 1 Foundations of Health Sciences Applied Health Sciences
IPLU1a IPLU1b
Year 2 Foundations of Occupational Therapy
Practice
Placement A
Principles of Occupational Therapy Practice
Placement B
Year 3 Therapeutic Process (Physical) Placement C1* Partnerships in (public) Health & Social Care Placement C1*
Integrated Therapeutic Process Year 4 Therapeutic Process (Mental Health) Placement C2*
IPLU2
Placement C2*
Complex Therapeutic Engagements Research Module
Health Care Futures and Innovations Leadership & Management Year 5
IPLU3a
Placement D
IPLU3b
Placement D
* Please note that these placements may be untaken full time or part time. Students may elect to do level V studies in one year or two.
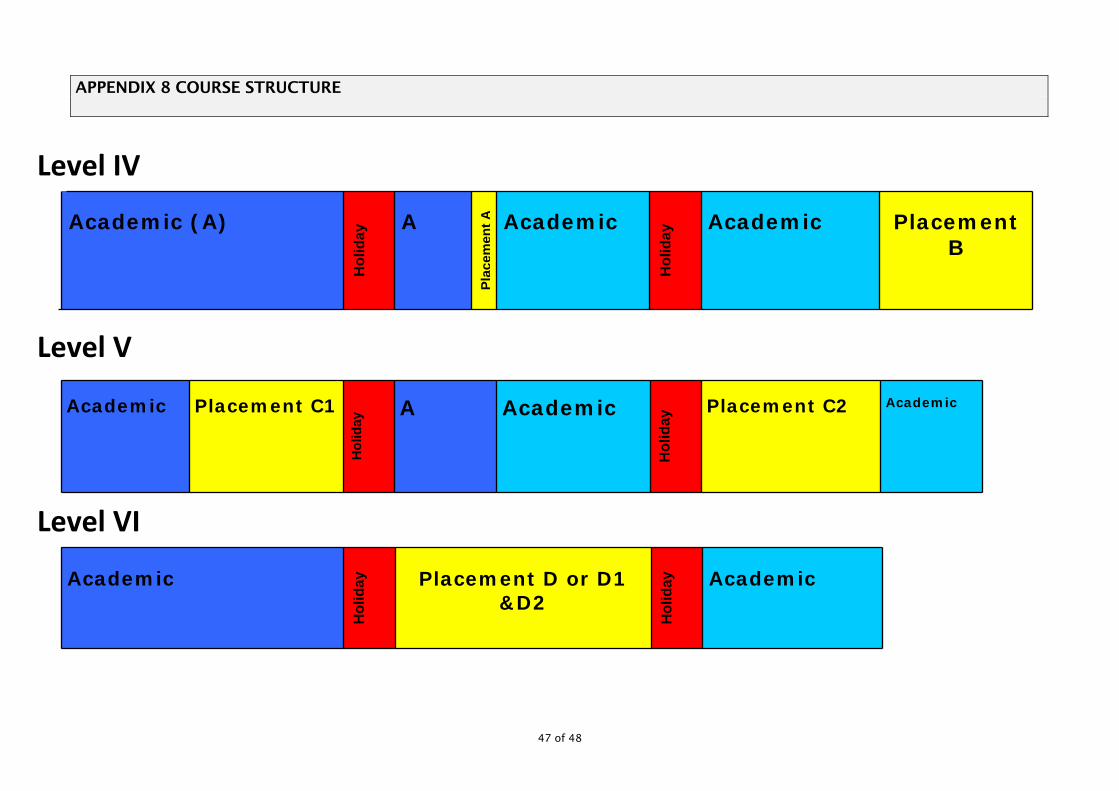
47 of 48
APPENDIX 8 COURSE STRUCTURE
Academic (A)
Hol
iday
A
Plac
emen
tA
Academic
Hol
iday
Academic
Placement B
Academic
Placement C1
Hol
iday
A
Academic
Hol
iday
Placement C2
Academic
Academic
Hol
iday
Placement D or D1
&D2
Hol
iday
Academic
Level IV
Level V
Level VI
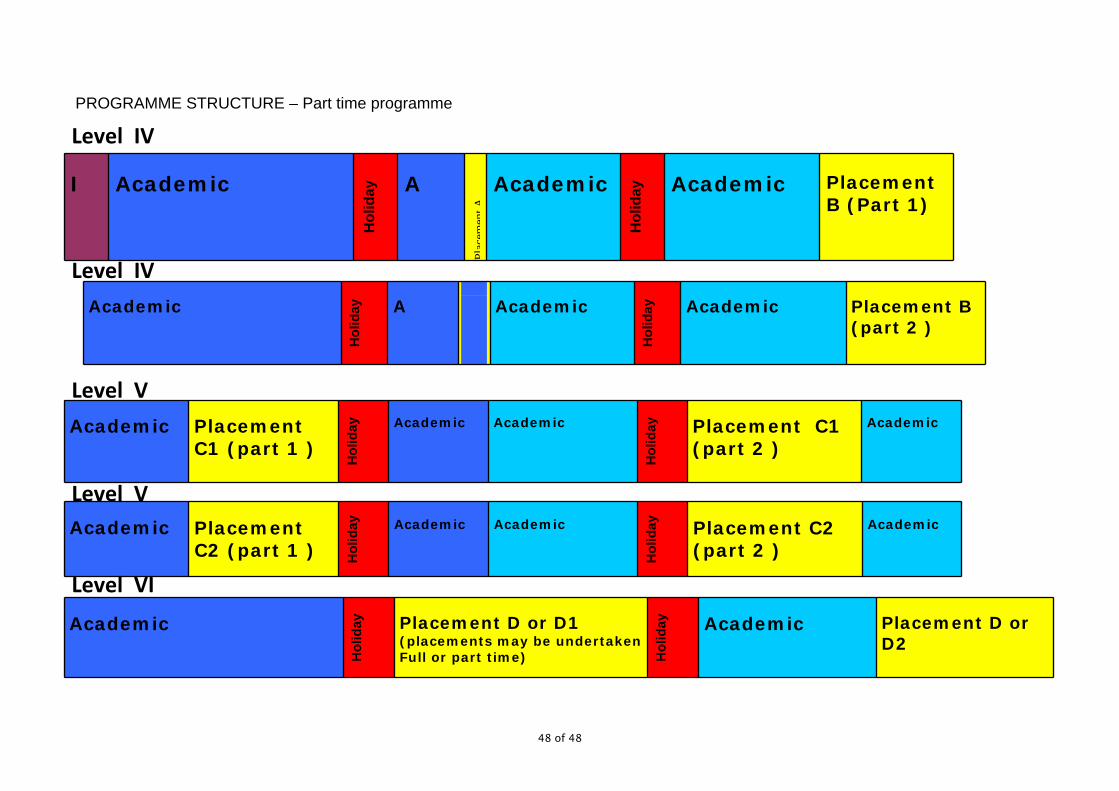
48 of 48
PROGRAMME STRUCTURE – Part time programme
I
Academic
Hol
iday
A
Plac
emen
tA
Academic
Hol
iday
Academic
Placement B (Part 1)
Academic
Hol
iday
A
Academic
Hol
iday
Academic
Placement B (part 2 )
Academic
Placement C1 (part 1 )
Hol
iday
Academic
Academic
Hol
iday
Placement C1 (part 2 )
Academic
Academic
Placement C2 (part 1 ) H
olid
ay
Academic
Academic
Hol
iday
Placement C2 (part 2 )
Academic
Academic
Hol
iday
Placement D or D1 (placements may be undertaken Full or part time) H
olid
ay
Academic
Placement D or D2
Level IV
Level IV
Level V
Level V
Level VI