clinical trials || endpoints in clinical trials on solid tumors – objective response
TRANSCRIPT
197
CHAPTER
Clinical TrialsDOI:
© 2012 Elsevier Inc. All rights reserved.2012
10.1016/B978-0-12-391911-3.00011-6
I. INTRODUCTION
Survival, as it applies to an individual study subject, and overall survival, as it applies to a population of study subjects, are clinical endpoints for oncology trials. Oncology clinical trials also use a number of surrogate endpoints, where these are used with the hope that they are prognostic for overall survival.
Surrogate endpoints in clinical trials on solid tumors include objective response, progression-free survival (PFS), time to progression (TTP), disease-free survival (DFS), time to distant metastasis (TDM), and biomarkers such as prostate-specific antigen (PSA) (1).
For use with populations of subjects, endpoints relating to PFS include median PFS, 6-month PFS, 2-year PFS, 5-year PFS, as well as the statistical parameter known as the hazard ratio.
For populations of subjects, endpoints that relate specifically to survival time include the endpoints of median overall survival, 6-month overall survival, 2-year over-all survival, 5-year overall survival, as well as the hazard ratio.
Median PFS and median overall survival refer to the average value from all study subjects or, at least, a number of subjects that are sufficient to provide the median value. Endpoints keyed to a specific time, such as 2-year PFS, refer not to any average value, but to the percent of all study subjects (in the entire study) experiencing that endpoint by the 2-year time point.
The following bullet points provide a context showing how this chapter fits into the next few chapters. While all of these are endpoints used in oncology, an under-standing of these will enable a better understanding of endpoints used in other dis-orders, for example immune diseases, infections, and metabolic diseases. This chapter concerns objective response, as indicated by the check mark.l Objective response ✓l Overall survival (OS)l Progression-free survival (PFS)l Time to progression (TTP)l Disease-free survival (DFS)l Time to distant metastasis (TDM).
Endpoints in Clinical Trials on Solid Tumors – Objective Response
11
1 Kelloff GJ, Bast RC Jr, Coffey DS, et al. Biomarkers, surrogate end points, and the acceleration of drug development for cancer prevention and treatment: an update prologue. Clin Cancer Res. 2004;10:3881–3884.
Clinical Trials198
Dhani et al. (2) Pazdur (3) Yothers (4) Mathoulin-Pelissier et al. (5) Saad and Katz (6) and Beckman (7) provide additional guidance on endpoints used in oncology clini-cal trials.
a. Objective response using RECIST criteriaIn a general statement about oncology, Grothey et al. (8) teach that the efficacy of a new oncology drug traditionally has been assessed by its ability to shrink exist-ing tumors and to prolong overall survival. Reliable data on tumor shrinkage can be obtained by small or large clinical trials, while reliable data on overall survival generally can only be obtained from large clinical trials. Tumor shrinkage can be easily measured in small trials, thus justifying further testing of the drug in a large clinical trial. In clini-cal practice, the observation of a tumor shrinkage, also called “response,” may convince the patient and the oncologist that the selected therapy is active against the cancer.
Objective response is an endpoint used in clinical trials on solid tumors. The term objective response refers to the size and number of the subject’s tumors. The earliest attempts to standardize tumor measurements were conducted by Moertel and Hanley during the 1960s and 1970s (9). At that time, palpitation and X-rays were used to assess tumor size. Since that time, more accurate imaging methods have been introduced and adopted, including computed tomography (CT), positron emission tomography (PET), and magnetic resonance imaging (MRI) (10).
Criteria for measuring tumor size and numbers are available from the World Health Organization (WHO) and the European Organization for Research and Treatment of Cancer (EORTC). In 1979, imaging was adopted for lesion measurement in the World Health Organization (WHO) criteria. However, because of some limitations of the WHO criteria, Response Evaluation Criteria in Solid Tumors (RECIST) was introduced in 2000. For reporting results from clinical trials, or for publications, the
2 Dhani N, Tu D, Sargent DJ, Seymour L, Moore MJ. Alternate endpoints for screening phase II studies. Clin Cancer Res. 2009;15:1873–1882.
3 Pazdur R. Endpoints for assessing drug activity in clinical trials. Oncologist. 2008;13 (suppl 2):19–21. 4 Yothers G. Toward progression-free survival as a primary end point in advanced colorectal cancer. J Clin Oncol.
2007;25:5153–5154. 5 Mathoulin-Pelissier S, Gourgou-Bourgade S, Bonnetain F, Kramar A. Survival end point reporting in randomized
cancer clinical trials: a review of major journals. J Clin Oncol. 2008;26:3721–3726. 6 Saad ED, Katz A. Progression-free survival and time to progression as primary end points in advanced breast cancer:
often used, sometimes loosely defined. Ann Oncol. 2009;20:460–464. 7 Beckman M. More clinical cancer treatments judged by progression-free rather than overall survival. J Natl Cancer
Inst. 99:1068–1069. 8 Grothey A, Hedrick EE, Mass RD, Sarkar S, Suzuki S, Ramanathan RK, et al. Response-independent survival benefit
in metastatic colorectal cancer: a comparative analysis of N9741 and AVF2107. J Clin Oncol. 2008;26:183–189. 9 Wahl RL, Jacene H, Kasamon Y, Lodge MA. From RECIST to PERCIST: evolving considerations for PET response
criteria in solid tumors. J Nucl Med. 2009;50(suppl 1):122S–150S.10 van Persijn van Meerten EL, Gelderblom H, Bloem JL. RECIST revised: implications for the radiologist. A review
article on the modified RECIST guideline. Eur Radiol. 2010;20:1456–1467.

Endpoints in Clinical Trials on Solid Tumors – Objective Response 199
response of tumors to therapy, in terms of tumor size and number, can be expressed by the RECIST criteria (11,12,13) as well as by the earlier set of criteria, the WHO response criteria (14,15). The RECIST criteria were created by the EORTC (16).
Figure 11.1 introduces the differences between the WHO criteria and the RECIST criteria (17). With the WHO criteria, a two-dimensional measure-ment is used. The longest diameter (A) and the longest perpendicular diameter (B) are obtained and multiplied. With RECIST criteria, only the longest diameter (A) is obtained. This is a one-dimensional measurement.
Figure 11.1 Radiologic image. Methods of tumor measurement according to the RECIST and WHO criteria. With the WHO criteria, the longest diameter (A) and the longest perpendicular diameter (B) are obtained and multiplied (2D measurement). With RECIST, only the longest diameter (A) is obtained (uni- or one-dimensional (1D) measurement)
11 Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–247.
12 Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92:205–216.
13 Schwartz LH, Bogaerts J, Ford R, et al. Evaluation of lymph nodes with RECIST 1.1. Eur J Cancer. 2009;45:261–267.
14 World Health Organization. Handbook for Reporting Results of Cancer Treatment. Geneva, Switzerland, World Health Organization, 1979, publication 48.
15 Park JO, Lee SI, Song SY, et al. Measuring response in solid tumors: comparison of RECIST and WHO response criteria. Jpn J Clin Oncol. 2003;33:533–537.
16 Suzuki C, Jacobsson H, Hatschek T, et al. Radiologic measurements of tumor response to treatment: practical approaches and limitations. Radiographics. 2008;28:329–344.
17 Suzuki C, Jacobsson H, Hatschek T, et al. Radiologic measurements of tumor response to treatment: practical approaches and limitations. Radiographics. 2008;28:329–344.

Clinical Trials200
The following provides further perspective regarding the endpoint of objec-tive response. According to Rubinstein et al. (18) in the era before RECIST criteria, the typical endpoint of the Phase II trials in oncology was objective tumor response (change in size and number of tumors). Unfortunately, for many diseases, such as lung, colon, breast, and renal cancers, objective tumor response failed to predict survival ben-efit (19). For other cancers, such as glioblastoma and prostate cancer, tumor response has proven difficult to measure. Hence, it is recognized that it is by no means automatic that objective response is the most appropriate endpoint for an oncology clinical trial.
In comments about clinical trials on melanoma, Korn et al. (20) found it has gen-erally not been the case that objective response is correlated with survival. Korn et al. (21) as well as Dy et al. (22) also point out that objective response is not a particu-larly sensitive reflection of the therapeutic effect of a class of drugs known as cytostatic drugs. Cytostatic drugs tend to result only in stabilization of the tumors. As a conse-quence, these authors concluded that overall survival and progression-free survival are better endpoints than objective response in trials of cytostatic drugs. This point was reiterated by Grothey et al. (23) who found that although objective change in tumor size is an important criterion for the treatment for solid tumors, this criterion may be more relevant as surrogate markers of drug efficacy for cytotoxic chemotherapy than for drugs that tend to have a more cytostatic effect, such as antibodies.
Objective response is often used with drugs that are cytotoxic agents (24). Rixe and Fojo (25) as well as Fleming et al. (26) describe how the efficacy of a cytostatic agent, which by its nature causes both tumor shrinkage and tumor stasis, is more easily detected by objective response, while efficacy of a cytotoxic agent, which by its nature causes mainly tumor stasis, is less easily detected by objective response. Cisplatin, and
18 Rubinstein L, Crowley J, Ivy P, Leblanc M, Sargent D. Randomized phase II designs. Clin Cancer Res. 2009;15:1883–1890.
19 Rubinstein L, Crowley J, Ivy P, Leblanc M, Sargent D. Randomized phase II designs. Clin Cancer Res. 2009;15:1883–1890.
20 Korn EL, Liu PY, Lee SJ, Chapman JA, et al. Meta-analysis of phase II cooperative group trials in metastatic stage IV melanoma to determine progression-free and overall survival benchmarks for future phase II trials. J Clin Oncol. 2008;26:527–534.
21 Korn EL, Liu PY, Lee SJ, Chapman JA, et al. Meta-analysis of phase II cooperative group trials in metastatic stage IV melanoma to determine progression-free and overall survival benchmarks for future phase II trials. J Clin Oncol. 2008;26:527–534.
22 Dy GK, Miller AA, Mandrekar SJ, et al. A phase II trial of imatinib (ST1571) in patients with c-kit expressing relapsed small-cell lung cancer: a CALGB and NCCTG study. Ann Oncol. 2005;16:1811–1816.
23 Grothey A, Hedrick EE, Mass RD, et al. Response-independent survival benefit in metastatic colorectal cancer: a comparative analysis of N9741 and AVF2107. J Clin Oncol. 2008;26:183–189.
24 Rubinstein L. E-mail of August 21, 2010.25 Rixe O, Fojo T. Is cell death a critical end point for anticancer therapies or is cytostasis sufficient? Clin Cancer Res.
2007;13:7280–7287.26 Fleming TR, Rothmann MD, Lu HL. Issues in using progression-free survival when evaluating oncology products.
J Clin Oncol. 2009;27:2874–2880.

Endpoints in Clinical Trials on Solid Tumors – Objective Response 201
other drugs that disrupt DNA metabolism, tend to be more cytotoxic, while sorafenib and flavopiridol may have properties that are more cytostatic (27).
The layperson may find it intuitively obvious that measuring tumor size and num-ber is the best way to determine efficacy of a drug, and for predicting long-term sur-vival. Unfortunately, attempts to find a correlation between objective response and overall survival, in the realm of solid tumors, are typically met with disappointment.
Figure 11.2 demonstrates some of the shortcomings of using objective response as a measure of drug efficacy. In the following hypothetical example, provided by Weber (28) a rapidly growing tumor (red in original) shrinks with therapy. But another tumor, a slowly growing tumor (green in original), continues to grow. At this point in time, the physician might conclude that the drug is effective against the rapidly growing tumor. However, as far as the patient is concerned, the drug provides no long-term benefit, because the rapidly growing tumor recovers from the toxic effects of the drug, and eventually is much larger than before. This hypothetical demonstrates why, for many oncology clinical trials, the endpoints of progression-free survival (PFS) and overall survival (OS) are typically chosen as primary endpoints, while objective response is used only as a secondary endpoint.
The following quotations provide a context for introducing the RECIST criteria. The examples are from breast cancer, colorectal cancer, lung cancer, and cancer of the head and neck. Endpoints that are objective response are emboldened. Definitions of the indicated subsets of objective response will then be disclosed.
10
9
8
7
5
4
3
2
1
0–1.0 –0.5 0 0.5 1.0 1.5 2.0
6
Time (y)
Tx
Tum
or d
iam
eter
(cm
)
Rapidly growing tumor (A)
Slowly growing tumor (B)
–33%
Figure 11.2 Tumor size versus years. This hypothetical diagram of tumor growth shows growth of a rapidly growing tumor (A) and growth of a slow growing tumor (B). Tx means treatment
28 Weber WA. Assessing tumor response to therapy. J Nucl Med. 2009;50:1S–10S.
27 Rixe O, Fojo T. Is cell death a critical end point for anticancer therapies or is cytostasis sufficient? Clin Cancer Res. 2007;13:7280–7287.
Clinical Trials202
In a study of breast cancer by Geyer et al. (29) the list of endpoints included objec-tive response, where this was classed as a secondary endpoint:
The primary end point was the time to progression, defined as the time from randomization to disease progression or death due to breast cancer. Secondary end points were progression-free survival, defined as the time from randomization to disease progression or death due to any cause; overall survival; the overall response rate;…complete response, partial response, or stable disease for at least 6 months.
In a study of colorectal cancer by Van Cutsem et al. (30) the list of endpoints included objective response, where this was classed as a secondary endpoint:
The primary end point was progression-free survival time, defined as the time from random-ization to disease progression or death from any cause within 60 days after the last tumor assessment or after randomization. Secondary end points included the overall survival time, the…complete response or partial response, defined as a response persisting for at least 28 days.
In a study of lung cancer, Shepherd et al. (31) included a list of primary endpoints and secondary endpoints:
The primary end point was overall survival. Secondary end points included progression-free sur-vival, overall response rate (complete and partial), duration of response, toxic effects, and quality of life. Responses were assessed with the use of the Response Evaluation Criteria in Solid Tumors (RECIST) criteria.
In a study of cancer of the head and neck, Vermorken et al. (32) provided an exten-sive list of endpoints, where the secondary endpoints included objective response:
The primary end point was overall survival, defined as the time from randomization to death. Secondary end points were progression-free survival (the time from randomization to the first radiologic confirmation of disease progression, or death from any cause within 60 days after the last assessment or randomization, whichever came first)…(a complete response, a partial response, or stable disease), the time to treatment failure (the time from randomization until the date of the first occurrence of one of the events specified in the protocol as constituting treat-ment failure).
Now, let us turn to the actual RECIST criteria. The RECIST criteria include the following subsets (33):
29 Geyer CE, Forster J, Lindquist D, et al. Lapatinib plus capecitabine for HER2-positive advanced breast cancer. New Engl J Med. 2006;355:2733–2743.
30 Van Cutsem E, Köhne CH, Hitre E, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. New Engl J Med. 2009;360:1408–1417.
31 Shepherd FA, Rodrigues Pereira J, Ciuleanu T, et al. Erlotinib in previously treated non-small-cell lung cancer. New Engl J Med. 2005;353:123–132.
32 Vermorken JB, Mesia R, Rivera F, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. New Engl J Med. 2008;359:1116–1127.
33 Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–247.

Endpoints in Clinical Trials on Solid Tumors – Objective Response 203
1. Complete Response (CR): Disappearance of all target lesions.2. Partial Response (PR): At least a 30% decrease in the sum of diameters of target
lesions, taking as reference the baseline sum diameters.3. Progressive Disease (PD): At least a 20% increase in the sum of diameters of target
lesions, taking as reference the smallest sum on study (this includes the baseline sum if that is the smallest on study). In addition to the relative increase of 20%, the sum must also demonstrate an absolute increase of at least 5 mm. The appearance of one or more new lesions is also considered progression.
4. Stable Disease (SD): Neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD, taking as reference the smallest sum diameters while on study.
b. Objective response – Demetri’s example of partial responseThe clinical trial of Demetri et al. (34) concerned gastrointestinal stromal tumors (GIST). Patients received imatinib, a small molecule that inhibits a small group of related tyrosine kinases, including the KIT receptor tyrosine kinase. The clinical trial contained two arms, where patients in arm A received 400 mg imatinib daily, and arm B received 600 mg imatinib daily.
There was no control group. But data from earlier clinical trials demonstrated that responses of this type of cancer to standard forms of chemotherapy were low. The documented objective response rate was 5%, and the overall survival in unresectable patients was less than 12 months (35). Subsequent clinical trials assessing the safety and efficacy of imatinib for GIST also did not contain any control group, for example the clinical trial of Heinrich et al. (36).
The following provides some background information regarding GIST. Most GISTs result from activating mutations in the KIT receptor tyrosine kinase, where this activating mutation is the mechanism responsible for about 85% of GIST patients. In about 8% of GIST patients, the mechanism responsible for the cancer is an activating mutation in a related enzyme, namely, platelet-derived growth factor receptor-alpha (PDGFRA) (37). The survival of metastatic GIST patients is dramatically improved by treatment with the KIT and PDGFRA inhibitor imatinib, a small molecule that
34 Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. New Engl J Med. 2002;347:472–480.
35 von Mehren M. E-mail of May 2, 2011.36 Heinrich MC, Owzar K, Corless CL, et al. Correlation of kinase genotype and clinical outcome in the North
American Intergroup Phase III Trial of imatinib mesylate for treatment of advanced gastrointestinal stromal tumor: CALGB 150105 Study by Cancer and Leukemia Group B and Southwest Oncology Group. J Clin Oncol. 2008;26:5360–5367.
37 Demetri GD, Heinrich MC, Fletcher JA, et al. Molecular target modulation, imaging, and clinical evaluation of gastrointestinal stromal tumor patients treated with sunitinib malate after imatinib failure. Clin Cancer Res. 2009;15:5902–5909.

Clinical Trials204
inhibits KIT and PDGFRA. Unfortunately, tumors eventually acquire resistance to imatinib due to evolution of mutations in these two enzymes (38).
The response of GIST to chemotherapy can be measured by imaging techniques, such as positron emission tomography (PET) or computed tomography (CT). PET works better in the context of GIST clinical trials. For PET imaging, the patient receives an infusion of [18F]fluoro-2-deoxyglucose. Objective response is accord-ing to the standard set forth by the Eastern Cooperative Oncology Group (ECOG). These guidelines state that a 25% reduction in the maximum standardized uptake value should be considered as the threshold for definition of partial response (39). These guidelines are not the same as the RECIST guidelines, but they are used in a similar manner. Interestingly, it has been found that when the RECIST criteria are used, the results do not predict the outcome of survival in response to chemotherapy while, in contrast, when the ECOG criteria are used, objective response does correlate with sur-vival outcome (40). Another publication, entitled “We Should Desist Using RECIST, at Least in GIST,” directly addressed the fact that the RECIST criteria result in poor correlations of objective response with survival (41).
The results from the clinical trial of Demetri et al. (42) are indicated in Table 11.1. The responses were assessed by PET scanning, followed by a confirmatory scan at least 28 days later. These results demonstrate that about half the subjects showed partial
Table 11.1 The Demitri study of gastrointestinal stromal tumorsNature of objective response (% of subjects)
400 mg imatinib 600 mg imatinib
Complete response 0% 0%Partial response 49.3 58.1Stable disease 31.5 24.3Progressive disease 16.4 10.8Could not be evaluated 2.7 6.8
38 Demetri GD, Heinrich MC, Fletcher JA, et al. Molecular target modulation, imaging, and clinical evaluation of gastrointestinal stromal tumor patients treated with sunitinib malate after imatinib failure. Clin Cancer Res. 2009;15:5902–5909.
39 Holdsworth CH, Badawi RD, Manola JB. CT and PET: early prognostic indicators of response to imatinib mesylate in patients with gastrointestinal stromal tumor. AJR Am J Roentgenol. 2007;189:W324–W330.
40 Holdsworth CH, Badawi RD, Manola JB. CT and PET: early prognostic indicators of response to imatinib mesylate in patients with gastrointestinal stromal tumor. AJR Am J Roentgenol. 2007;189:W324–W330.
41 Benjamin RS, Choi H, Macapinlac HA, et al. We should desist using RECIST, at least in GIST. J Clin Oncol. 2007;25:1760–1764.
42 Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. New Engl J Med. 2002;347:472–480.

Endpoints in Clinical Trials on Solid Tumors – Objective Response 205
response (partial shrinkage) while about a quarter of the subjects showed stable dis-ease. Only about 14% of the subjects experienced increases in tumor size. There were no significant differences in objective response between the two doses of imatinib. Figure 11.3 discloses representative PET scans (raw data) from one particular subject, where scans were taken at baseline after one month of imatinib treatment, and after 16 months of imatinib treatment. The figure reveals a dramatic reduction and near-disappearance of the pelvic-level signal arising from the tumors.
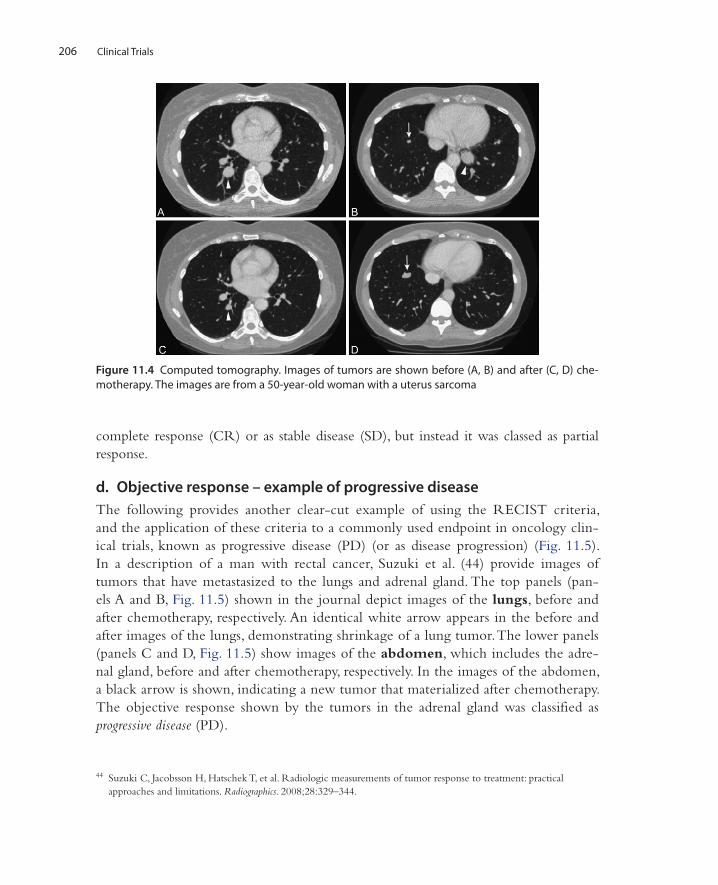
c. Objective response – van Meerten’s example of partial responseIn a description of lung tumors, occurring with the metastasis of uterine cancer, van Persijn van Meerten et al. (43) provide images of tumors assessed by objective response, according to the RECIST criteria. In Fig. 11.4, panels A and B show com-puted tomography scans before chemotherapy (baseline data), while panels C and D show scans after chemotherapy. The arrows in panels A and C point to target lesions, while the arrows in B and D point to non-target lesions. The term “target lesions” refers to spe-cific tumors that the investigator has decided to measure repeatedly during the course of the study.
All of the images are of lung tumors from the same woman being treated for uter-ine cancer. In comparing A and C, it is easy to see that the target lesion (arrow) has shrunk but has not disappeared. In comparing B and D, it is easy to see that one of the non-target lesions (arrow) has actually increased in size. The patient’s response was clas-sified as partial response (PR). In other words, the patient’s response was not classified as
43 van Persijn van Meerten EL, Gelderblom H, Bloem JL. RECIST revised: implications for the radiologist. A review article on the modified RECIST guideline. Eur Radiol. 2010;20:1456–1467.
Figure 11.3 Positron emission tomography (PET scan) of a subject with gastrointestinal stromal tumors during the course of treatment with imatinib. Baseline (left figure); 1 month chemotherapy (central figure); 16 months chemotherapy (right figure)
Clinical Trials206
complete response (CR) or as stable disease (SD), but instead it was classed as partial response.
d. Objective response – example of progressive diseaseThe following provides another clear-cut example of using the RECIST criteria, and the application of these criteria to a commonly used endpoint in oncology clin-ical trials, known as progressive disease (PD) (or as disease progression) (Fig. 11.5). In a description of a man with rectal cancer, Suzuki et al. (44) provide images of tumors that have metastasized to the lungs and adrenal gland. The top panels (pan-els A and B, Fig. 11.5) shown in the journal depict images of the lungs, before and after chemotherapy, respectively. An identical white arrow appears in the before and after images of the lungs, demonstrating shrinkage of a lung tumor. The lower panels (panels C and D, Fig. 11.5) show images of the abdomen, which includes the adre-nal gland, before and after chemotherapy, respectively. In the images of the abdomen, a black arrow is shown, indicating a new tumor that materialized after chemotherapy. The objective response shown by the tumors in the adrenal gland was classified as progressive disease (PD).
Figure 11.4 Computed tomography. Images of tumors are shown before (A, B) and after (C, D) che-motherapy. The images are from a 50-year-old woman with a uterus sarcoma
44 Suzuki C, Jacobsson H, Hatschek T, et al. Radiologic measurements of tumor response to treatment: practical approaches and limitations. Radiographics. 2008;28:329–344.

Endpoints in Clinical Trials on Solid Tumors – Objective Response 207
II. STUDIES CHARACTERIZING AN ASSOCIATION BETWEEN OBJECTIVE RESPONSE AND SURVIVAL
As detailed in the colorectal cancer study of Grothey et al. (45) the magnitude of objec-tive response may be correlated, at least to some extent, with the magnitude of overall survival. Buyse et al. (46) also reported a moderately good correlation between objec-tive response and survival for colorectal cancer. According to a personal communication from Dr. A. Grothey (47) a stronger correlation between objective response and over-all survival can be found from studies of testicular cancer. Also, excellent correlations
45 Grothey A, Hedrick EE, Mass RD, Sarkar S, Suzuki S, Ramanathan RK, et al. Response-independent survival benefit in metastatic colorectal cancer: a comparative analysis of N9741 and AVF2107. J Clin Oncol. 2008;26:183–189.
46 Buyse M, Thirion P, Carlson RW, et al. Relation between tumour response to first-line chemotherapy and survival in advanced colorectal cancer: a meta-analysis. The Lancet. 2000;356:373–378.
A B
C D
Figure 11.5 Objective response that is progressive disease. Images of lungs where rectal cancer has metastasized to the lungs (panels A and B) and to the adrenal gland (panels C and D). Panels A and B show computed tomography scans (lung window) obtained before (A) and after (B) treatment show multiple lung metastases. The target lesion (arrowhead) and many other lesions decreased in size after treatment. Panels C and D show computed tomography scans of the abdomen, obtained before (C) and after (D) treatment, show a new lesion in the adrenal gland after treatment (arrow in D)
47 Grothey A. E-mail of August 25, 2010.

Clinical Trials208
between objective response and overall survival occur with hematological cancers, for example the leukemias (48). Moreover, according to Benjamin et al. (49) objective response may be correlated with survival for gastrointestinal stromal tumors.
However, unfortunately, objective tumor response has generally been a poor sur-rogate for survival in most solid tumors (50). According to Sargent (51) improvements in objective response do not necessarily translate to overall survival benefit. And con-versely, it has been shown that, for example, patients with colon cancer still receive a benefit, in terms of overall survival, from a more effective treatment even if they do not show objective response (52).
III. AVOIDING CONFUSION WHEN USING OBJECTIVE RESPONSE AS AN ENDPOINT
The endpoint of objective response is potentially confusing, as listed below. These sources of confusion also apply to endpoints that rely on measurements of objective response, namely, the endpoints of progression-free survival (PFS) and time to progression (TTP).
a. Date for beginning objective response measurements in two study arms, relative to start date of treatment
When a clinical trial contains two study arms, confusion can result when assessments of objective response (in both arms) are not initiated on the same date (relative to the date of initiating drug treatment).
For example, consider the example of a cancer clinical trial involving two study arms, one receiving study drug and the other a control treatment. Let us say that the start date for assessing objective response of the study drug is delayed by two weeks, that is, delayed two weeks after the corresponding date for the control treatment.
For the sake of this hypothetical, assume that the true efficacies of both treatments (study drug, control treatment) are about the same. But in the situation where assess-ments of objective response for the study drug are delayed, for example, by two weeks, the clinical trial will conclude that the study drug works differently than the control treatment.
This particular situation was actually described in a study of melanoma compar-ing efficacy of temozolomide (study drug) and dacarbazine (control treatment) (53).
48 Hedrick EE. Personal communication, March 2, 2011.49 Benjamin RS, Choi H, Macapinlac HA, et al. We should desist using RECIST, at least in GIST. J Clin Oncol.
2007;25:1760–1764.50 Sargent DJ. E-mail of August 31, 2010.51 Sargent D. General and statistical hierarchy of appropriate biologic endpoints. Oncology. 2006;20(6 suppl 5):5–9.52 Sargent D. General and statistical hierarchy of appropriate biologic endpoints. Oncology. 2006;20(6 suppl 5):5–9.53 Middleton MR, Grob JJ, Aaronson N, et al. Randomized phase III study of temozolomide versus dacarbazine in the
treatment of patients with advanced metastatic malignant melanoma. J Clin Oncol. 2000;18:158–166.

Endpoints in Clinical Trials on Solid Tumors – Objective Response 209
Timing of objective response assessments in the two arms was initiated on different dates, relative to the start date for initiating treatment. Assessment of temozolomide efficacy was delayed by two weeks.
The efficacy of the study drug (temozolomide) appeared to be slightly better than efficacy of the active control (dacarbazine, DTIC). (The difference in start date for measuring objective response was not proven to be the source of this difference, but was only suggested as a cause.)
In the words of the authors, “DTIC treated patients underwent the first for-mal assessment for disease progression 2 weeks earlier than did temozolomide treated patients, which may have contributed to the difference observed in PFS” (54).
b. Where multiple measurements of objective response are taken, which measurement is used for analysis of efficacy?
Where duplicate measurements of objective response are taken, ambiguity can result where the publication does not clearly state which value, that is, which data collection, had been used for triggering the event of objective response. Typically, the second of the two measurements is confirmatory.
For example, in a clinical trial of melanoma, objective response (for every subject) was measured at two different time points. A personal communication from the inves-tigator settled the issue, revealing that the value reported in the publication was that from the second time point (55,56).
In another study of melanoma, multiple readings of objective response were taken, but the paper did not expressly state which reading from any given study subject was used for reporting objective response for that particular subject. Readings were taken after every eight-week cycle of therapy (57). A personal communication from the principal inves-tigator revealed that the reading providing the best result, for example greatest tumor shrinkage, was used for statistical analysis and for reporting in the publication, that is, “The object response rate is calculated based on the ‘best response’ of each individual patient. Complete responses are often durable, but partial responses are often not” (58,59). Thus, the reading that gave the best response was the reading used for assessing efficacy.
54 Middleton MR, Grob JJ, Aaronson N, et al. Randomized phase III study of temozolomide versus dacarbazine in the treatment of patients with advanced metastatic malignant melanoma. J Clin Oncol. 2000;18:158–166.
55 Tarhini AA, Kirkwood JM, Gooding WE, Cai C, Agarwala SS. Durable complete responses with high-dose bolus interleukin-2 in patients with metastatic melanoma who have experienced progression after biochemotherapy. J Clin Oncol. 2007;25:3802–387.
56 Agarwala SS. E-mail of September 8, 2010.57 Hwu WJ, Krown SE, Menell JH, et al. Phase II study of temozolomide plus thalidomide for the treatment of
metastatic melanoma. J Clin Oncol. 2003;21:3351–3356.58 Hwu WJ, Krown SE, Menell JH, et al. Phase II study of temozolomide plus thalidomide for the treatment of
metastatic melanoma. J Clin Oncol. 2003;21:3351–3356.59 Hwu WJ. E-mail of September 10, 2010.

Clinical Trials210
c. How is it possible to obtain a meaningful value for objective response, or for endpoints (PFS, TTP) that comprise objective response?
In assessing efficacy of an anti-cancer drug or radiation therapy, it might be expected that tumors begin to grow immediately after treatment. Hence, how is it logically possible for a typical clinical trial to report that the value for progression-free survival (PFS) was, for example, three months or perhaps five months? The answer is that objective response is measured according to the RECIST criteria, or a similar standard, which mandates that objective response (and endpoints that comprise objective response) is not triggered until there has occurred a specific increase in tumor size or number.
d. Objective response is reported in terms of a “rate” and also as a “percent”
In the text of publications in oncology, use the term “objective response rate” when referring to data from measuring tumor size and number. But in tables this “rate” has the unit of “percent.” This practice is potentially confusing, in view of the fact that the term “rate,” as it is used in chemistry and physics, entails the unit of time. But in oncol-ogy, the term “objective response rate” does not entail the unit of time. Instead, the term “objective response rate” means proportion or percent (60).
e. Drugs that are cytostatic and not cytotoxic may provide misleading results, where the endpoint of objective response is used
In a review of oncology endpoints, Dhani et al. (61) warned that, in the case of cer-tain drugs, the failure of the drug to provide an impressive objective response may give a misleading impression of eventual overall survival. The term RR means response rate, which is a subset of objective response. These authors referred to drugs having a very modest response rate, resulting in prolongation of progression-free survival (PFS) or overall survival (OS), suggesting that tumor stabilization rather than shrinkage may still result in clinical benefit. Dhani et al. (62) found that using response rate as a ‘‘go/no-go’’ criterion may lead to inappropriate termination of pursuit of the drug in ques-tion. A striking example is the putative Raf kinase and anti-vascular agent sorafenib in renal cell carcinoma and hepatocellular cancer, where response rates using the RECIST criteria were under 10%, conventionally a signal to abandon further devel-opment. But fortunately, subsequent clinical trials showed significant prolongation of both PFS and overall survival.
60 Eisenhauer E. E-mail of September 12, 2010.61 Dhani N, Tu D, Sargent DJ, Seymour L, Moore MJ. Alternate endpoints for screening phase II studies. Clin Cancer
Res. 2009;15:1873–1882.62 Dhani N, Tu D, Sargent DJ, Seymour L, Moore MJ. Alternate endpoints for screening phase II studies. Clin Cancer
Res. 2009;15:1873–1882.

Endpoints in Clinical Trials on Solid Tumors – Objective Response 211
f. Use of different criteria (standards) for objective response, and the availability of updated criteria
Yet another potential source of confusion, which can occur when comparing drug efficacies from different clinical trials, is the use of different standards for assessing objective response. As noted above, the available standards include the WHO criteria, and different, updated versions of the RECIST criteria. Potential confusion can also result when, during the course of a clinical trial, a new set of standards is issued, and where the investigators contemplate switching to the new standards. Yet another source of confusion is where more sensitive methods of tumor imaging become available. A more sensitive method of tumor imaging will have a direct effect on the ability to detect tumor progression. This issue is developed elsewhere in this textbook, in the material on the Will Rogers phenomenon.