clinical practice indicators myocardial infarction (mi) · clinical practice indicators: myocardial...
TRANSCRIPT
Clinical Practice Indicators Myocardial Infarction (MI)
“From 1st symptoms to follow-up at 1 year”
March 2012
A method for improving the quality
of the patient’s care pathway
Pilot Programmes – Clinical Impact Division of Quality and Safety improvement in Health Care
Haute Autorité de Santé (HAS) – French National Authority for Health
& the national MI Task Force

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 2/85
Document placed online on 2 April 2009. This update is concerned with:
− bringing up to date bibliographic references on the subject of “Myocardial infarction”
− incorporating the French National MI Task Force feed-back (cf. MI Progress report for 2009,
HAS-BMJ Symposium, HAS Technical Meetings and Cardiovascular Plenaries 2009, 2010 and
2011)
− validation by professional consensus of the French National MI Task Force and participating
professional organisations.
This document was validated by the HAS Board in March 2012 © Haute Autorité de Santé – 2012

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 3/85
Table of Contents
1. Why these Clinical Practice Indicators (CPI)? ......................................................................... 5
2. Participatory approach: French National MI Task Force & HAS .......................................... 6
3. List of abbreviations................................................................................................................... 8
4. Review of practices, priority objectives and list of indicators for each stage.................... 10 Stage 1: From pain to reperfusion ........................................................................................... 11 Stage 2: From reperfusion to discharge from the healthcare establishment .................................. 11 Stage 3: Post-infarction follow-up at 1 year................................................................................ 12
5. Proposed CPI benchmarks for assessing the clinical quality of the myocardial infarction care cycle ................................................................................................................. 13
6. Fact sheets about clinical practice indicators ....................................................................... 14 1. Rate of calls to the emergency medical assistance as a first step in the acute phase..................... 14 2. Rate of appropriate treatment with platelet aggregation inhibitor .................................................. 15 3. Rate of treatment with morphine derivatives for intense pain ....................................................... 16 4. Rate of patients being referred directly to ICC............................................................................ 17 5. Rate of patients undergoing a reperfusion strategy in the acute phase ........................................ 18 6. Time to primary angioplasty in the acute phase ......................................................................... 19 7. Time to thrombolysis in the acute phase ................................................................................... 20 8. Rate of patients evaluated for left ventricular function while hospitalised ...................................... 21 9. Rate of patients with appropriate prescription for beta-blockers on discharge................................ 22 10. Rate of patients with appropriate prescription for platelet aggregation inhibitors on discharge ........ 23 11. Rate of patients with appropriate prescription for statin on discharge ........................................... 24 12. Rate of patients with appropriate prescription of ACEI on discharge............................................. 25 13. Rate of patients prescribed cardiovascular rehabilitation............................................................. 26 14. Rate of patients assisted with smoking cessation ....................................................................... 27 15. Rate of patients receiving specialist diabetes advice on severe hyperglycaemia ........................... 28 16. Rate of patients receiving information on using the emergency medical assistance ....................... 29 17. Rate of post-infarction patients investigated for chest pains and/or the use of nitrates ................... 30 18. Rate of post-infarction patients undergoing cardiovascular rehabilitation programmes ................... 31 19. Rate of patients whose blood pressure was monitored post-infarction.......................................... 32 20. Rate of patients evaluated for post-infarction tolerance to treatment ............................................ 33 21. Rate receiving information about the need for regular post-infarction physical exercise.................. 34 22. Rate of post-infarction patients monitored for active tobacco use................................................. 35 23. Rate having a lipid and blood glucose assessment 3 to 6 months post-infarction .......................... 36 24. Rate of patients having their weight monitored........................................................................... 37 25. Rate of patients having their post-infarction physical activity monitored 3 to 6 months
after discharge........................................................................................................................ 38 26. Rate of post-infarction patients examined for peripheral artery occlusive disease (PAOD).............. 39 27. Rate of patients receiving appropriate beta-blocker treatment at 1 year ......................................... 40 28. Rate of patients receiving appropriate aspirin treatment at 1 year.................................................. 41 29. Rate of patients receiving appropriate treatment with a platelet aggregation inhibitor (apart from
aspirin) at 1 year ..................................................................................................................... 42 30. Rate of patients receiving appropriate treatment with statin at 1 year............................................. 43 31. Rate of patients receiving appropriate treatment with a ACEI........................................................ 44 32. Rate of patients having their diet monitored ............................................................................... 45

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 4/85
33. Rate of cases involving correspondence between the primary care doctor and the cardiologist ...... 46 34. 30-day mortality rates Optional................................................................................................ 47
7. Risk and mortality scores ........................................................................................................ 48
8. List of proposed items for clinical practice indicators collection ....................................... 50
Appendix 1. Proposed tools ............................................................................................................. 54 1.1 Proposed case report forms................................................................................................. 54
1.1.1 Case report form for ACS in an outpatient setting – Transmission ......................................54 1.1.2 Case report form for A&E......................................................................................................55 1.1.3 Case report form for CARDIOLOGY.....................................................................................56 1.1.4 Ambulatory follow-up form – 1st year post-infarction............................................................57 1.1.5 Proposed shared report forms for “Assessment at 1 year post-infarction: indicators of results
and indicators of access to specialised programmes” ..........................................................59 1.2 Proposals for memos ........................................................................................................... 60
1.2.1 Optimal care pathway for the treatment of a suspected ACS ......................................... 60 1.2.2 Suspected ACS in an outpatient setting....................................................................... 60 1.2.3 For SAMU ................................................................................................................ 61 1.2.4 For SAMU and A&E................................................................................................... 62 1.2.5 For the Emergency Services ...................................................................................... 63 1.2.6 For Cardiology Departments....................................................................................... 64 1.2.7 Following an ACS: ACS and diabetes ......................................................................... 66 1.2.8 Following an ACS: ACS and smoking.......................................................................... 66
Appendix 2 – Literature search ........................................................................................................ 67
Appendix 3. Bibliographic references ............................................................................................. 70 3.1 HAS methodological references ............................................................................................... 70 3.2 Guidelines and other institutional studies and studies by healthcare agencies or professional
organisations on “Myocardial infarction and secondary prevention”.............................................. 71 3.3 “Myocardial infarction and secondary prevention” indicators........................................................ 76 3.4 Other publications................................................................................................................... 81

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 5/85
1. Why these Clinical Practice Indicators (CPI)?
Myocardial infarction is a public health issue about which there are very many regularly updated references both in France1 and abroad. Established good practice is implemented by healthcare professionals and care teams along the entire patient care cycle, including the specific ones developed by regional actors. In order to facilitate and to monitor the implementation of guidelines and the improvement of practices, practitioners from various disciplines working under the auspices of the HAS have together agreed on a common and shared base of Clinical Practice Indicators (CPI) that can be used to measure the optimal clinical pathway over the full patient care cycle – from the call to the emergency medical assistance 15 to the follow-up in outpatients of the “classic” acute myocardial infarction.2 Every discipline and every team in addition retains the capability of creating and retrieving other criteria better suited to their objectives or to their practice. CPIs are worked out on the basis of a collaborative, prospective approach, centred on the patient and his/her full care cycle and incorporating the 3 ESA quality dimensions (Efficacy, Safety and Access to the best care). Focusing on the key points of clinical practice, they enable their level of quality to be objectified. Their ultimate purpose is to help improve the quality and safety of care and the clinical impact for the patient throughout the full cycle of care. CPIs are produced and validated with directly involved health professionals and their professional organisations (HAS Method3). Information about implementation and feedback on practices are available on the HAS website.4 Thus this common base of indicators enables professionals to assess and compare their results and their approaches to care, a form of benchmarking designed to improve the actual benefit for the patients.5 This comparison can be beneficially enhanced by describing the populations studied. These CPIs also give institutions and decision-makers valid and consensual benchmarks for the clinical quality of the care cycle, and give patients useful information about the key benchmarks for good practice and for the results of care.
1 Appendix III B. Guidelines: 38, 40, 52, 61, 62, 65; C. Indicators: 115 and D. Other: 151 2 Definition: [acute coronary syndrome with ST elevation (ACS ST+) or with recent or presumed recent left bundle branch block (LBBB)] 3 Appendix III A. Method: 1, 2, 5, 6 4 Appendix III A. Method: 3; C. Indicators: 99, 107, 108, 109; D. Other: 149 5 Appendix III B. Guidelines: 3; D. Other: 150

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 6/85
2. Participatory approach: French National MI Task Force & HAS
The following professional bodies were invited to be involved in carrying out this programme: ANFIIDE, CEPPRAL, CFMU, CHEM, CMG, CNCF, CNCH, CNGE, CNPC, CNPEDMM, FMC No. 1, FNMF, LORFOMEC, RSSMG, SFC, SFDRMG, SFMG, SFMU, SFT, SFTG, UFCV, UNAFORMEC, UNR Santé and the representatives of the practice registries of E-MUST, of Chateauroux, and of Franche Comté, RICO, RESCA+31, REGLOR-SCA ST+, Oscar+, RESCUe network, RENAU-RESURCOR network, Rivarance network, the National Fast-MI Survey, the REACH Study and the Euroheart Survey. Contributors: Since 2008 Dr François-Xavier Ageron, A&E doctor, RENAU-RESURCOR, Annecy Dr Sophie Bataille, A&E doctor, E-MUST, Paris Dr Loïc Belle, cardiologist, RENAU-RESURCOR, SFC, CNCH, Annecy Dr Jean-Michel Bunel, GP, Maronne Prof. Bogdan Catargi, endocrinologist-diabetologist, Bordeaux Dr Sandrine Charpentier, A&E doctor, RESCA+ 31, Toulouse Prof Cyrille Colin, epidemiologist, CEPPRAL, Lyon Prof. Yves Cottin, cardiologist, RICO, Dijon Prof. Nicolas Danchin, cardiologist, SFC, Fast-MI, Indicqard, Paris Dr Valérie Debierre, A&E doctor, SFMU, Nantes Prof. Laurent Degos, President of HAS 2004-2010 Dr Jean-Louis Ducassé, A&E doctor, CFMU, Toulouse Dr Antoine Duclos, epidemiologist, CEPPRAL, Lyon Dr Annabel Dunbavand, medical adviser, FNMF Health Centres, Paris Dr Carlos El Khoury, A&E doctor, RESCUe, OSCAR+, Vienne Dr Patrick Goldstein, A&E doctor, SFMU, Lille Dr Etienne Hinglais, A&E doctor, CFMU, Paris Dr Thierry Laperche, cardiologist, Saint-Denis Dr Yves Le Noc, GP, SFDRMG, CMG, Doctor’s Guide Group, Nantes Dr Olivier Mayer, GP, Strasbourg Prof. François Schiele, cardiologist, Franche Comté Registry, Euroheart Survey, Besançon Dr Louis Soulat, A&E doctor, Central Châteauroux Registry Dr Christian Ziccarelli, cardiologist, UFCV, CNPC, Indicqard, Orléans
In 2010-2012 Dr Charles Autreaux, GP, Jolimetz Dr Marc Baudet, cardiologist, Maison du cœur, Dax Dr Jacques Berland, cardiologist, CNPC, CNCF, Rouen Dr Ivan Berlin, pharmacologist, smoking specialist, SFT Mireille Bucau, nurse specialising in therapeutic education, Dax Dr Simon Cattan, cardiologist, CNCH, Montfermeil Dr Tahar Chouihed, A&E doctor, REGLOR-SCA ST+ Registry, Nancy Dr Emmanuel Corbillon, SMACDAM, HAS Catherine Daugareil, nurse specialising in therapeutic education, Maison du cœur, Dax Eric Delezie, masseur/physiotherapist, CNOMK, Paris Dr Thierry Denolle, cardiologist, Rivarance Network, Dinard Dr Gilles Dentan, cardiologist, CNPC, Fontaine les Dijon Marielle Desmartin, dietician, Lyon Catherine Frerou, dietician, Rennes Dr Pascal Héricotte, cardiologist, URCET, Dax Dr Marie-Christine Iliou, cardiologist, SFC, Gers Prof. Patrick Jourdain, cardiologist, CNCH, Cergy Pontoise Prof. Véronique Kerlan, endocrinologist, CNPEDMM, Brest Brigitte Lecointre, ANFIIDE, Lyon Dr Béatrice Lemaitre, company doctor, SFT, Caen Dr Yann L’Hermitte, A&E doctor and HAS project manager, Paris Dr Jacques Migueres, GP, Paris Dr Jean-Michel Oriol, GP, HAS project manager, Septeme, Rhône Alpes Prof. François Paillard, cardiologist, Rennes Dr Eric Perchicot, cardiologist, CNPC, Cavaillon Dr Joel Petite, GP, HAS project manager, Franche Comté Marion Plétan, health manager, HAS project manager Dr Denis Pouchain, GP, CNGE, Paris Armelle Richard, nurse specialising in therapeutic education, Rivarance Network, Dinard Dr Pierre Sabouret, cardiologist, REACH, Paris Prof. Jeannot Schmidt, A&E doctor, SFMU, Clermont-Ferrand Dr Claude Sichel, GP, Carnoux en Provence Florent Teboul, masseur-physiotherapist, Villeneuve St Denis Prof. Daniel Thomas, cardiologist, smoking specialist, SFT Dr Michel Varroud-Vial, diabetologist, UNR Santé

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 7/85
HAS Coordination - Pilot Programmes- Clinical Impact Department: Dr Armelle Leperre-Desplanques, Head of Department; Dr Linda Banaei-Bouchareb, Lead Project Manager “Myocardial Infarction” Pilot Programme, Dr Carlos El-Khoury, Consultant “Myocardial Infarction”, Marie Erbault, Carole Micheneau, Dr Nathalie Riolacci, Deputy Head of Department. The literature search and monitoring were carried out by Virginie Henry (Documentalist) and Renée Cardoso (Assistant Documentalist), with the participation of Mireille Cecchin (Documentalist) of the HAS’s Communication and Publications Department, in conjunction with the Lead Project Manager reporting on the topic of myocardial infarction, Linda Banaei-Bouchareb.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 8/85
3. List of abbreviations
ACEI Angiotensin converting enzyme inhibitor ACS Acute coronary syndrome ACS ST+ Acute coronary syndrome with ST segment elevation A&E Accident and emergency department ADLF Association des Diététiciens de Langue Française [Association of French-Speaking Dieticians] AFDN Association Française des Diététiciens Nutritionnistes [French association of nutritional dieticians] AFSSAPS Agence Française de Sécurité Sanitaire des Produits de Santé [French Health Products Safety Agency] ALFEDIAM Association de Langue Française pour l'Etude du Diabète et des Maladies Métaboliques [French
language association for the study of diabetes and metabolic diseases] ANFIIDE Association Nationale Française des Infirmières et Infirmiers Diplômés et Etudiants [French National
Graduate and Student Nurses Association] APP Acute phase pathway ARA II Angiotensin receptor antagonist BASA Beta-blocker, Antiplatelet drugs or platelet aggregation inhibitor (aspirin and/or
clopidogrel/prasugrel/ticagrelor), Statin, ACEI or ARAII CARDIO-ARHIF
Registre de Cardiologie de l’Agence régionale d'hospitalisation d'Ile de France [Ile de France Regional Hospitalisation Agency Cardiology Registry]
CD Cardiology department CEPPRAL Coordination Pour L’évaluation Des Pratiques Professionnelles en santé en Rhône-Alpes [Coordination
for the evaluation of professional health practices in Rhône-Alpes] CFMU Collège Français de Médecine d'Urgence [French College of Emergency Medicine] CHEM Collège des Hautes Etudes en medicine [College of Higher Medical Studies] CMG Collège de la Médecine Générale [College of General Medicine] CMRE Chargés de Mission Régionaux pour l'Evaluation [Regional Project Leaders for Evaluation] CNCF Collège National des Cardiologues Français [French National College of Cardiologists] CNCH Collège National des Cardiologues Hospitaliers [French National College of Hospital Cardiologists] CNGE Collège National des Généralistes Enseignants [French National College of Generalist Teachers] CNOMK Conseil National de l'Ordre des Masseurs-Kinésitherapeutes [National Board of the Association of
Masseurs and Physiotherapists) CNPC Conseil National Professionnel de Cardiologie [French National Council for the Cardiology Profession] CNPEDMM Conseil National Professionnel d’Endocrinologie, Diabète et Maladies Métaboliques [French National
Professional Council for Endocrinology, Diabetes and Metabolic Diseases] CO Cardiologie ambulatoire [cardiology outpatients] CPI Clinical Practice Indicator CR Cardiovascular rehabilitation DDE Department of diabetology and endocrinology DO Diabétologie ambulatoire [diabetes outpatients] DREES Direction de la recherche, des études, de l’évaluation et des statistiques [Directorate for Research,
Surveys, Assessment and Statistics] E MUST Evaluation en Médecine d’urgence des stratégies thérapeutiques de l’infarctus du myocarde [Evaluation
in emergency medicine of therapeutic strategies for myocardial infarction] FMC No.1 Association Formation Médicale Continue n°1 [Association for continuous medical training No. 1] FNMF Fédération Nationale de la Mutualité Française [French National Federation of Mutual Companies] GP General Practitioner HCSP Haut Conseil de la Santé Publique [French High Council for Public Health] IC Interventional Cardiology INPES Institut National de Prévention et d'Education pour la Santé – [National Prevention and Health Education
Institute] INVS Institut de Veille Sanitaire [Health Monitoring Institute]
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 9/85
IRDES Institut de Recherche et Documentation en Economie de la Sante [Institute for Research and Information in Health Economics]
LBBB Left bundle branch block LORFOMEC Fédération Lorraine des Associations de Formation Médicale Continue [Lorraine Federation of
Associations for Continuous Medical Training] MI Myocardial infarction ORBI Observatoire Régional Breton sur l'Infarctus du Myocarde [Breton Regional Observational Study on
Myocardial Infarction] OSCAR+ Observatoire du Syndrome Coronarien Aigu du réseau RESCUe avec surélévation du segment ST
[Observational study on acute coronary syndrome of the RESCUe network with ST segment elevation] Pathway Patient’s care pathway in the health system PMP Paramedical professionals PPE Évaluation des Pratiques Professionnelles [Professional practice evaluation] RCFC Registre du réseau de cardiologie de Franche Comté [Franche Comté cardiology network registry] REACH Reduction of Atherothrombosis for Continued Health REGLOR-SCA ST+
REGistre LORrain des Syndromes Coronariens Aigus avec surélévation du segment ST [Lorraine registry of acute coronary syndromes with ST segment elevation]
RENAU RÉseau Nord Alpin des Urgences [North Alps Emergency Network] RESCA + 31 Recueil des SCA (Haute Garonne) [ACS Registry (Haute Garonne) RESCUe RÉSeau Cardiologie Urgence (Rhône-Alpes) [Emergency cardiology network (Rhône-Alpes)] RESURCOR Réseau des Urgences Coronaires (Rhône-Alpes) [Emergency coronary network (Rhône-Alpes)] RICO Registre des infarctus de Côte d'Or [Côte d’Or infarct registry] RSSMG Regroupement des sociétés savantes de Médecine Générale [Grouping of learned societies in general
medine] SAMU Service d’Aide Médicale Urgente [Emergency Medical Assistance - EMA] SFAR Société Française d’Anesthésie et de Réanimation – [French Society of Anaesthesia and Intensive
Care] SFC Société Française de Cardiologie [French Cardiology Society] SFD Société Française de Diabétologie – [French Language Diabetes Society] SFDRMG Société Française de Documentation et de Recherche en Médecine Générale [French Society for
Documentation and Research in General Medicine] SFGG Société Française de Gériatrie et Gérontologie – [French society for geriatrics and gerontology] SFMG Société française de médecine générale [French General Medical Society] SFMU Société française de médecine d’urgence [French Society for Emergency Medicine] SFT Société française de tabacologie [French society on Smoking Addiction] SFTG Société de formation thérapeutique du généraliste [Society for Therapeutic Education of General
Practitioners] SPI Blood Systolic Pressure Index SMUR Service Mobile d'Urgence et de Réanimation [Mobile Emergency and Resuscitation service] TA Tabacologie ambulatoire [Outpatient smoking clinic/consultation] UFCV Union de Formation et d'évaluation en médecine Cardio-Vasculaire [Union for Training and Assessment
in cardiovascular medicine] UNAFORMEC Union nationale des Associations de formation médicale continue [National union of associations for
continuous medical training] UNR Santé Union Nationale des Réseaux de santé [National union of health networks] URCET Unité de Rééducation Cardiaque et d'Éducation Thérapeutique [Cardiac rehabilitation and therapeutic
education unit] WHO World Health Organisation
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 10/85
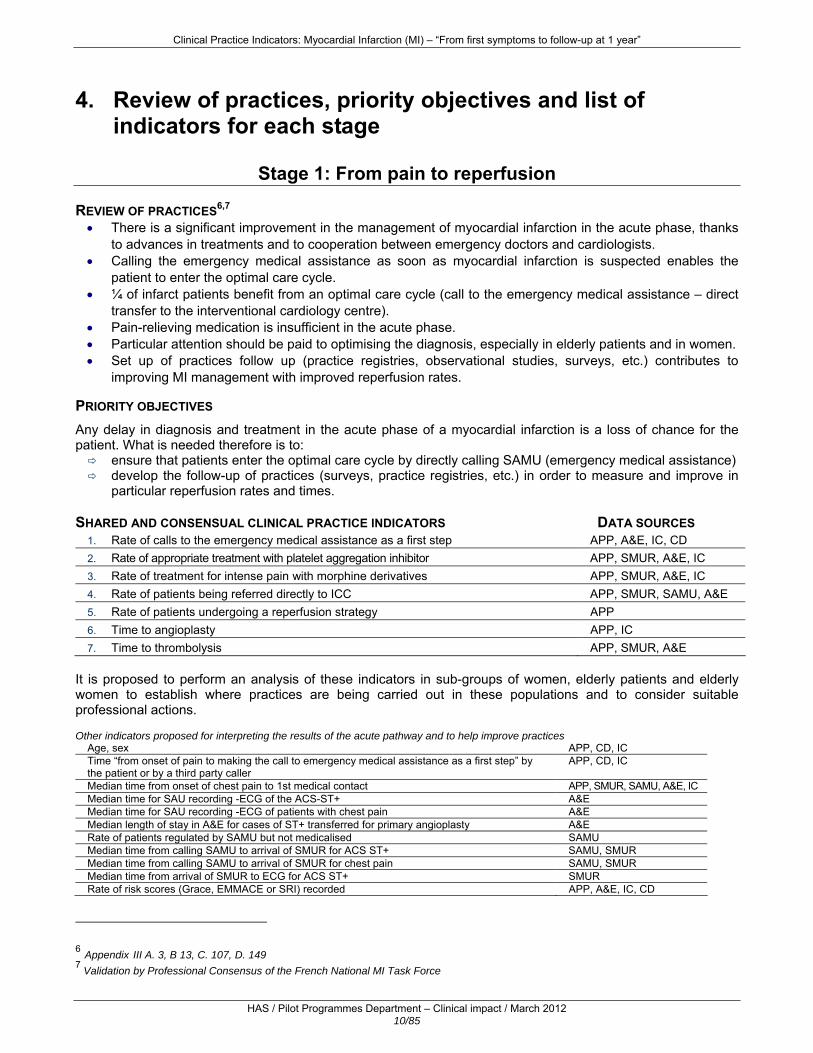
4. Review of practices, priority objectives and list of indicators for each stage
Stage 1: From pain to reperfusion
REVIEW OF PRACTICES6,7 • There is a significant improvement in the management of myocardial infarction in the acute phase, thanks
to advances in treatments and to cooperation between emergency doctors and cardiologists. • Calling the emergency medical assistance as soon as myocardial infarction is suspected enables the
patient to enter the optimal care cycle. • ¼ of infarct patients benefit from an optimal care cycle (call to the emergency medical assistance – direct
transfer to the interventional cardiology centre). • Pain-relieving medication is insufficient in the acute phase. • Particular attention should be paid to optimising the diagnosis, especially in elderly patients and in women. • Set up of practices follow up (practice registries, observational studies, surveys, etc.) contributes to
improving MI management with improved reperfusion rates. PRIORITY OBJECTIVES Any delay in diagnosis and treatment in the acute phase of a myocardial infarction is a loss of chance for the patient. What is needed therefore is to:
ensure that patients enter the optimal care cycle by directly calling SAMU (emergency medical assistance) develop the follow-up of practices (surveys, practice registries, etc.) in order to measure and improve in
particular reperfusion rates and times.
SHARED AND CONSENSUAL CLINICAL PRACTICE INDICATORS DATA SOURCES 1. Rate of calls to the emergency medical assistance as a first step APP, A&E, IC, CD 2. Rate of appropriate treatment with platelet aggregation inhibitor APP, SMUR, A&E, IC 3. Rate of treatment for intense pain with morphine derivatives APP, SMUR, A&E, IC 4. Rate of patients being referred directly to ICC APP, SMUR, SAMU, A&E 5. Rate of patients undergoing a reperfusion strategy APP 6. Time to angioplasty APP, IC 7. Time to thrombolysis APP, SMUR, A&E
It is proposed to perform an analysis of these indicators in sub-groups of women, elderly patients and elderly women to establish where practices are being carried out in these populations and to consider suitable professional actions. Other indicators proposed for interpreting the results of the acute pathway and to help improve practices
Age, sex APP, CD, IC Time “from onset of pain to making the call to emergency medical assistance as a first step” by the patient or by a third party caller
APP, CD, IC
Median time from onset of chest pain to 1st medical contact APP, SMUR, SAMU, A&E, IC Median time for SAU recording -ECG of the ACS-ST+ A&E Median time for SAU recording -ECG of patients with chest pain A&E Median length of stay in A&E for cases of ST+ transferred for primary angioplasty A&E Rate of patients regulated by SAMU but not medicalised SAMU Median time from calling SAMU to arrival of SMUR for ACS ST+ SAMU, SMUR Median time from calling SAMU to arrival of SMUR for chest pain SAMU, SMUR Median time from arrival of SMUR to ECG for ACS ST+ SMUR Rate of risk scores (Grace, EMMACE or SRI) recorded APP, A&E, IC, CD
6 Appendix III A. 3, B 13, C. 107, D. 149 7 Validation by Professional Consensus of the French National MI Task Force
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 11/85
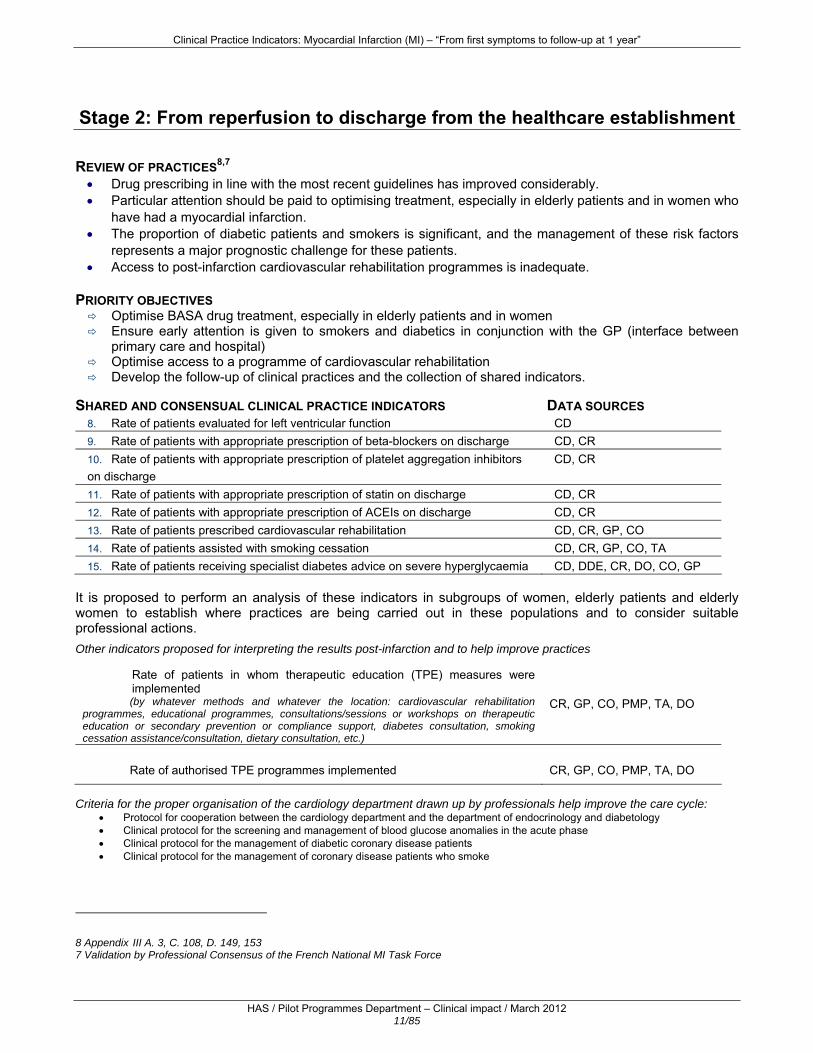
Stage 2: From reperfusion to discharge from the healthcare establishment
REVIEW OF PRACTICES8,7 • Drug prescribing in line with the most recent guidelines has improved considerably. • Particular attention should be paid to optimising treatment, especially in elderly patients and in women who
have had a myocardial infarction. • The proportion of diabetic patients and smokers is significant, and the management of these risk factors
represents a major prognostic challenge for these patients. • Access to post-infarction cardiovascular rehabilitation programmes is inadequate.
PRIORITY OBJECTIVES
Optimise BASA drug treatment, especially in elderly patients and in women Ensure early attention is given to smokers and diabetics in conjunction with the GP (interface between
primary care and hospital) Optimise access to a programme of cardiovascular rehabilitation Develop the follow-up of clinical practices and the collection of shared indicators.
SHARED AND CONSENSUAL CLINICAL PRACTICE INDICATORS DATA SOURCES
8. Rate of patients evaluated for left ventricular function CD 9. Rate of patients with appropriate prescription of beta-blockers on discharge CD, CR 10. Rate of patients with appropriate prescription of platelet aggregation inhibitors on discharge
CD, CR
11. Rate of patients with appropriate prescription of statin on discharge CD, CR 12. Rate of patients with appropriate prescription of ACEIs on discharge CD, CR 13. Rate of patients prescribed cardiovascular rehabilitation CD, CR, GP, CO 14. Rate of patients assisted with smoking cessation CD, CR, GP, CO, TA 15. Rate of patients receiving specialist diabetes advice on severe hyperglycaemia CD, DDE, CR, DO, CO, GP
It is proposed to perform an analysis of these indicators in subgroups of women, elderly patients and elderly women to establish where practices are being carried out in these populations and to consider suitable professional actions.
Other indicators proposed for interpreting the results post-infarction and to help improve practices Rate of patients in whom therapeutic education (TPE) measures were implemented (by whatever methods and whatever the location: cardiovascular rehabilitation
programmes, educational programmes, consultations/sessions or workshops on therapeutic education or secondary prevention or compliance support, diabetes consultation, smoking cessation assistance/consultation, dietary consultation, etc.)
CR, GP, CO, PMP, TA, DO
Rate of authorised TPE programmes implemented
CR, GP, CO, PMP, TA, DO
Criteria for the proper organisation of the cardiology department drawn up by professionals help improve the care cycle:
• Protocol for cooperation between the cardiology department and the department of endocrinology and diabetology • Clinical protocol for the screening and management of blood glucose anomalies in the acute phase • Clinical protocol for the management of diabetic coronary disease patients • Clinical protocol for the management of coronary disease patients who smoke
8 Appendix III A. 3, C. 108, D. 149, 153 7 Validation by Professional Consensus of the French National MI Task Force

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 12/85
Stage 3: Post-infarction follow-up at 1 year
REVIEW OF PRACTICES9,7 • The control of cardiovascular risk factors is inadequate • Post-infarction cardiovascular rehabilitation and therapeutic education programmes make an effective
contribution to the reduction of recurrences and deaths and to improving quality of life. • Myocardial infarction BASA treatment some time after discharge can be optimised • 30-day mortality has fallen by 60% in 15 years • It should be possible to reduce 1st-year post-myocardial infarction mortality even further.
PRIORITY OBJECTIVES FOR IMPROVING PROFESSIONAL PRACTICES Improve and evaluate the control of the risk factors in post-infarction patients Optimise the patient’s overall care cycle in conjunction with his/her primary care doctor: drug treatment,
non-drug treatment and patient education Develop the follow-up of clinical practices and the collection of shared indicators.
SHARED AND CONSENSUAL CLINICAL PRACTICE INDICATORS – DATA SOURCES
Short-term follow-up Data sources 16. Rate of patients receiving information on using the emergency medical assistance CR, GP, PMP, CO 17. Rate of patients investigated for chest pain and/or the use of nitrates GP, PMP, CO 18. Rate of patients undergoing cardiovascular rehabilitation programmes CR, CO, GP 19. Rate of patients whose blood pressure was monitored CR, GP, PMP, CO 20. Rate of patients evaluated for tolerance to BASA treatment GP, PMP, CO 21. Rate of patients receiving information about the need for regular physical exercise CR, GP, PMP, CO
Medium-term follow-up (3-6 months)
22. Rate of patients monitored for active tobacco use CR, GP, CO, PMP, TA 23. Rate of patients having a lipid and blood glucose assessment GP, CO, DO 24. Rate of patients having their weight monitored GP, CO, PMP 25. Rate of patients having their physical exercise monitored CR, GP, PMP, CO 26. Rate of patients examined for peripheral artery occlusion disease (PAOD) CR, GP, CO Follow-up at 1 year 27. Rate of patients receiving appropriate beta-blocker treatment CO, GP 28. Rate of patients receiving appropriate aspirin treatment CO, GP 29. Rate of patients receiving appropriate treatment with platelet aggregation inhibitor apart from aspirin
CO, GP
30. Rate of patients receiving appropriate treatment with statin CO, GP 31. Rate of patients receiving appropriate treatment with ACEI CO, GP 32. Rate of patients having their diet monitored CR, CO, GP, PMP 33. Rate of correspondence between the GP and the cardiologist at 1 year CO, GP
30-day post-myocardial infarction mortality rate, optional APP, CR, GP, CO
9 Appendix III A. 3, C. 109, D. 149, 153 7 Validation by Professional Consensus of the French National MI Task Force

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 13/85
5. Proposed CPI benchmarks for assessing the clinical quality∗ of the myocardial infarction care cycle
1
Pain - call emergency call centre
Reperfusion
5, 6, 7
Cardiovascular rehabilitation
28, 29, 30, 31, 32
DischargeReferral
Drug treatmentand non-drug treatment
Follow-up and monitoring of risk factorsLifestyle and dietary rulesContribution from patient
Acute ward
RISK
FACTO
RS
PRIM
ARY PREVEN
TION
IMPAC
TM
OR
TALITY -MO
RB
IDITY
ACCESS: CPI benchmarks - entry into the optimal emergency pathway by calling the emergency call centre (1)- direct referral to ICC (4)- cardiovascular rehabilitation (18)
EFFICACY – SAFETY: CPI benchmarks- reperfusion rates and times (5, 6, 7)- appropriate BASIC prescription on discharge (9, 10, 11, 12)- appropriate BASIC treatment at 1 year (28, 29, 30, 31, 32)
184
Assessment at 1 year
9, 10, 11, 12
∗ The evaluation concerns the 3 ESA quality dimensions: Efficacy, Safety and Access

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 14/85
6. Fact sheets about clinical practice indicators
1. Rate of calls to the emergency medical assistance as a first step in the acute phase
Rate of ACS ST+ or LBBB patients for whom SAMU was contacted as a first step
Numerator Number of ACS ST+ or LBBB* patients for whom SAMU was contacted as a first step on the appearance of the symptoms
Denominator Number of ACS ST+ or LBBB* patients with chest pains for less than 12
hours Data APP – A&E – IC – CD
For it to be capable of being interpreted at geographical area level, this indicator should cover patients taken into the care cycle by SAMU as well as those brought in by the emergency services or even those coming directly into cardiology (APP). This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification A prompt call to SAMU emergency medical assistance by the patient or
by a third-party caller enables a patient suspected of presenting an acute coronary syndrome to benefit from the best care pathway in terms of speed of diagnosis and treatment, thus helping to reduce mortality. Entry into the care pathway occurs as soon as SAMU takes the call.
This indicator has been validated by professional consensus of the French national MI Task Force Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 40, 61, 62, 65 C. Indicators 98, 107, 115 * Recent or presumed recent LBBB
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 15/85
2. Rate of appropriate treatment with platelet aggregation inhibitor
Appropriate prescription* of platelet aggregation inhibitor(s) in patients with ACS ST+ or LBBB**
Numerator Number of ACS ST+ or LBBB** patients with • aspirin and another platelet aggregation inhibitor●, or • only one platelet aggregation inhibitor apart from aspirin, if a contraindication is noted in the medical file, or the patient is already on aspirin or was put on aspirin by the 1st medical contact, or • aspirin alone if there is a contraindication to any other platelet aggregation inhibitor (in particular an unfavourable risk/benefit ratio noted in the medical file), or • no platelet aggregation inhibitor with contraindications noted in the medical file or patient refusal noted in the file
Denominator Total number of ACS ST+ or LBBB** patients Data APP – SMUR – A&E – IC – CD
For it to be capable of being interpreted at geographical area level, this indicator should cover patients taken into the care cycle by SAMU as well as those brought in by the emergency services or even those coming directly into cardiology (APP). This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification The use of platelet aggregation inhibitor(s) reduces mortality due to myocardial infarction.
Clopidogrel or Prasugrel or Ticagrelor are currently the platelet aggregation inhibitors used in combination with aspirin in the absence of any contraindications. There are calls for other platelet aggregation inhibitors validated in this indication to be placed on the market.
This indicator has been validated by professional consensus of the French national MI Task Force Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 18, 21, 31, 35, 37, 40, 49, 53 C. Indicators: 95, 107, 110, 112, 113, 114, 115, 117 D. Other: 129, 152, 175, 168 * “Appropriate” prescription refers to a prescription where there is a corresponding indication, and the lack of a prescription means there is a corresponding contraindication, or no indication or a refusal on the part of the patient. ** Recent or presumed recent LBBB
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 16/85
3. Rate of treatment with morphine derivatives for intense pain
Rate of ACS ST+ or LBBB* patients with persistent pain and VAS ≥ 60 mm or NS ≥ 6 treated with morphine derivatives
Numerator Number of ACS ST+ or LBBB* patients with persistent intense chest pain (VAS ≥ 60 mm or NS ≥ 6) treated with morphine derivatives
Denominator Number of ACS ST+ or LBBB* patients with persistent intense chest pain
(VAS ≥ 60 mm or NS ≥ 6) Data APP – SMUR – A&E – IC – CD
For it to be capable of being interpreted at geographical area level, this indicator should cover patients taken into the care cycle by SAMU as well as those brought in by the emergency services or even those coming directly into cardiology (APP).
This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification Management of pain in the acute phase of an ACS ST+ or LBBB is essential
from an ethical point of view, also because pain is associated with sympathetic activation, which produces vasoconstriction and increases the cardiac workload. Immediate recourse to titrated intravenous morphine derivatives is justified in cases of intense pain (VAS ≥ 60 mm or NS ≥ 6).
This indicator has been validated by professional consensus of the French national MI Task Force Additional information
Reference tools for the evaluation of pain in adults capable of communication are the visual analogue scale (VAS) and the numerical scale (NS), and when these cannot be used, the simple 5-point verbal scale.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 17, 28, 30, 37, 40 C. Indicators 103, 107
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 17/85
4. Rate of patients being referred directly to ICC
Rate of patients with ACS ST+ or LBBB* who have been referred directly to an interventional cardiology centre with available technical resources
Numerator Number of ACS ST+ or LBBB* (with chest pain less than 12 hours old) referred directly to a ICC with available technical resources for angioplasty
Denominator Number of ACS ST+ or LBBB* patients with chest pains for less than
12 hours Data APP – SMUR – SAMU – A&E
For it to be capable of being interpreted at geographical area level, this indicator should cover patients taken into the care cycle by SAMU as well as those brought in by the emergency services or even those coming directly into cardiology (APP).
This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audit of patient files in each sector.
Justification All patients with ACS ST+ or LBBB need to have an emergency coronary
thrombectomy. Therefore they need to be sent as soon as possible to an interventional cardiology centre for a diagnostic and interventional coronary angiography, irrespective of whether the thrombolysis had been performed or not. In particular, this indicator enables the optimal care path to be evaluated (call to SAMU – SMUR – direct transfer to ICC).
This indicator has been validated by professional consensus of the French national MI Task Force Références bibliographiques (Annexe III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 17, 37, 40 C. Indicators: 107, 115 D. Other: 126, 159 * Recent or presumed recent LBBB

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 18/85
5. Rate of patients undergoing a reperfusion strategy in the acute phase
Rate of patients with ACS ST+ or LBBB* patients taken into the care cycle within 12 hours following the start of symptoms and receiving early coronary reperfusion therapy Numerator Number of ACS ST+ or LBBB* patients receiving coronary
reperfusion therapy (angioplasty or thombolysis) within 12 hours following the start of symptoms
Denominator Number of ACS ST+ or LBBB* patients taken into the care cycle within 12 hours following the start of symptoms
Exclusion criteria:
Contraindications and non-indications to the reperfusion techniques justified in the medical file
Patient refusal
Data APP – For it to be capable of being interpreted at geographical area level, this indicator should cover patients taken into the care cycle by SAMU as well as those brought in by the emergency services or even those coming directly into cardiology (APP). This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification The advantage in terms of mortality and morbidity of early reperfusion (by angioplasty or thrombolysis) in patients with ACS ST+ is currently acknowledged unanimously. Any patient admitted to the care cycle within 12 hours after the start of symptoms should be given coronary reperfusion therapy, either by angioplasty or by thrombolysis.
This indicator has been validated by professional consensus of the French national MI Task Force
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 11, 17, 26, 29, 31, 37, 38, 40, 43 C. Indicators: 107, 112, 113, 114, 115, 117 * Recent or presumed recent LBBB

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 19/85
6. Time to primary angioplasty in the acute phase
The median time from first medical contact to the first balloon inflation/first thromboaspiration for ACS ST+ or LBBB* patients who have had an angioplasty Numerator Time between first medical contact (FMC) and the time of the first balloon expansion or
first thromboaspiration for patients who have had a primary angioplasty during the 12 hours following the start of the pain.
Exclusion criteria: postponement of the angioplasty for reasons documented in the medical file (temporary contraindication, patient refusal)
Denominator No denominator Data APP – IC
For it to be capable of being interpreted at geographical area level, this indicator should cover patients taken into the care cycle by SAMU as well as those brought in by the emergency services or even those coming directly into cardiology (APP). This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification The advantage in terms of mortality and morbidity of early reperfusion (by angioplasty or thrombolysis) in patients with ACS ST+ is currently acknowledged unanimously.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information
The FMC is the moment when the doctor first arrives at the point of care, enabling a qualifying ECG to be carried out and, if indicated, the administration of reperfusion therapy. The time when the qualifying ECG is carried out and the time when the first device for reopening the artery is introduced should be noted by the cardiologists, in addition to the time of the puncture usually collected (currently used techniques: balloon, thromboaspiration, direct stenting). It is nevertheless advisable to make a note of the following times: start of pain, arrival on site – first medical contact, qualifying ECG, arrival on the catheterisation ward. Primary angioplasty should be carried out:
if the time between the start of pain and the first medical contact is less than 2 hours and the time from FMC to balloon inflation/thromboaspiration is estimated at < 90 minutes if the time between the start of pain and the first medical contact is more than
2 hours and the time from FMC to balloon inflation/thromboaspiration is estimated at < 120 minutes
In all other cases, thrombolysis is recommended.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 17, 26, 29, 31, 37, 38, 40, 43, 49 C. Indicators: 70, 91, 92, 107, 112, 113, 114, 115, 117
* Recent or presumed recent LBBB
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 20/85
7. Time to thrombolysis in the acute phase
Median time from first medical contact to thrombolysis for patients ACS ST+ or LBBB* thrombolysed
Numerator Time from first medical contact (FMC) and the thrombolytic agent injection for patients having had thrombolysis within 12 hours of the start of pain.
Exclusion criteria: postponement of the thrombolysis for reasons documented in the medical file (temporary contraindication, patient refusal)
Denominator No denominator Data APP – SMUR – A&E
For it to be capable of being interpreted at geographical area level, this indicator should cover patients taken into the care cycle by SAMU as well as those brought in by the emergency services or even those coming directly into cardiology (APP).
This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification The advantage in terms of mortality and morbidity of early reperfusion (by
angioplasty or thrombolysis) in patients with ACS ST+ is currently acknowledged unanimously.
This indicator has been validated by professional consensus of the French national MI Task Force
Additional information
The FMC is the moment when the doctor first arrives at the point of care, enabling a qualifying ECG to be carried out and, if indicated, the administration of reperfusion therapy. The thrombolysis may be performed either in hospital or outside. The thrombolysis should be performed by an experienced team within less than 30 minutes after the first medical contact.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 17, 26, 29, 37, 38, 40, 43, 49 C. Indicators: 69, 90, 107, 112, 113, 114, 115, 117 * Recent or presumed recent LBBB

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 21/85
8. Rate of patients evaluated for left ventricular function while hospitalised
Rate of ACS ST+ or LBBB* patients having their left ventricular function assessed while hospitalised
Numerator ACS ST+ or LBBB* patients having their left ventricular function evaluated by echography, angiography or scintigraphy during their hospitalisation, recorded in the medical file.
Denominator Number of ACS ST+ or LBBB patients* Data CD – CR
This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification Evaluation of left ventricular function is recommended with all infarctions as it determines the treatment and the prognosis. If there is any left ventricular dysfunction, this will need to be re-evaluated later.
This indicator has been validated by professional consensus of the French national MI Task Force Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 17, 37 C. Indicators: 99, 108, 112, 113, 114, 115, 117 * Recent or presumed recent LBBB

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 22/85
9. Rate of patients with appropriate prescription for beta-blockers on discharge
Rate of ACS ST+ or LBBB* patients with appropriate** prescription for beta-blockers on discharge
Numerator Number of ACS ST+ or LBBB* patients
with a prescription for beta-blockers on discharge, or without a prescription for beta-blockers, with a contraindication
recorded in the medical file without a prescription for beta-blockers, with a documented
intolerance and a prescription for ivabradine or patient refusal recorded in the medical file
Denominator Number of ACS ST+ or LBBB* patients Data CD – CR
This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification Treatment with Beta-blockers reduces the mortality from myocardial infarction.
This indicator has been validated by professional consensus of the French national MI Task Force
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 9, 10, 17, 37, 38, 41 C. Indicators: 74, 99, 93, 108, 112, 113, 114, 115, 116, 117 * Recent or presumed recent LBBB ** “Appropriate” prescription refers to a prescription where there is a corresponding indication, and the lack of a prescription means there is a corresponding contraindication, or no indication or a refusal on the part of the patient.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 23/85
10. Rate of patients with appropriate prescription for platelet aggregation inhibitors on discharge Rate of ACS ST+ or LBBB* patients with appropriate** prescription for aspirin and/or another platelet aggregation inhibitor on discharge
Numerator Number of ACS ST+ or LBBB* patients with, on discharge, • aspirin and another platelet aggregation inhibitor●, or • only one platelet aggregation inhibitor apart from aspirin if a contraindication to aspirin is recorded in the medical notes, or • aspirin alone, if there is a contraindication to any other platelet aggregation inhibitor (in particular an unfavourable risk/benefit ratio noted in the medical file), or • no platelet aggregation inhibitor with contraindications or patient refusal recorded in the file
Denominator Total number of ACS ST+ or LBBB* patients
Data CD – CR This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification Taking this combination of treatments reduces the mortality from myocardial infarction.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information Clopidogrel or prasugrel or ticagrelor are currently the platelet aggregation
inhibitors recommended in combination with aspirin in the absence of any contraindications. There is a call for other platelet aggregation inhibitors validated in this indication to be placed on the market.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 18, 21, 31, 35, 37, 38, 49, 53 C. Indicators: 74, 99, 94, 108, 110, 112, 113, 114, 115, 117 D. Other: 120, 152 ** “Appropriate” prescription refers to a prescription where there is a corresponding indication, and the lack of a prescription means there is a corresponding contraindication, or no indication or a refusal on the part of the patient. * Recent or presumed recent LBBB

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 24/85
11. Rate of patients with appropriate prescription for statin on discharge Rate of ACS ST+ or LBBB* patients with appropriate** prescription for a statin on discharge
Numerator Number of ACS ST+ or LBBB* patients • with a prescription on discharge comprising a statin • without a prescription for a statin but with a contraindication or patient refusal recorded in the medical file
Denominator Number of ACS ST+ or LBBB* patients Data CD – CR
This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification Taking a statin reduces the risk of mortality and recurrences in
patients who have had a myocardial infarction. This indicator has been validated by professional consensus of the French national MI Task Force Additional information
Target objective in cases of dyslipidaemia: LDL-cholesterol < 1 g/l. Serious adverse events are uncommon (< 1%), consisting essentially of rhabdomyolysis and myalgia, elevated levels of transaminases (ASAT and ALAT) and CPK. Checking the transaminase levels is vital at least once during the three months following the start of the treatment. If the initial determination of the CPK level before the commencement of treatment is not scientifically justified (except in certain at-risk situations), any unexplained muscle symptom appearing during treatment should lead to a CPK determination. This monitoring applies to fibrates, statins and ezetimibe, either alone or in combination with statins.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 14, 17, 37, 38, 41, 44, 57 C. Indicators: 74, 99, 100, 108, 112, 113, 114, 115, 116, 117 * Recent or presumed recent LBBB ** “Appropriate” prescription refers to a prescription where there is a corresponding indication, and the lack of a prescription means there is a corresponding contraindication, or no indication or a refusal on the part of the patient.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 25/85
12. Rate of patients with appropriate prescription of angiotensin converting enzyme inhibitor on discharge Rate of ACS ST+ or LBBB* patients, with appropriate** prescription for ACEI or ARA-II
Numerator Number of ACS ST+ or LBBB* patients with altered left ventricular function • with a prescription for an angiotensin converting enzyme inhibitor or ARA-II if there is a contraindication to ACEIs (do not accept as a contraindication moderate renal insufficiency, i.e. a creatinine clearance > 30 ml/min) • without a prescription for an angiotensin converting enzyme inhibitor or ARA-II but with a contraindication to ACEIs and ARA-II, OR a patient refusal recorded in the medical file (do not accept as a contraindication moderate renal insufficiency, i.e. a creatinine clearance > 30 ml/min)
Denominator Number of ACS ST+ or LBBB* patients with altered left ventricular
function Data CD – CR
This collection can be prospective and continuous: practice registries, databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector
Justification Taking this treatment reduces serious cardiovascular events and mortality due to myocardial infarction, including in patients with altered left ventricular function.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information Aspects of monitoring treatment with ACEIs: blood potassium and blood
creatinine/creatinine clearance Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 17, 37, 38, 49 C. Indicators: 74, 97, 99, 108, 112, 113, 114, 115, 117 * Recent or presumed recent LBBB ** “Appropriate” prescription refers to a prescription where there is a corresponding indication, and the lack of a prescription means there is a corresponding contraindication, or no indication or a refusal on the part of the patient.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 26/85
13. Rate of patients prescribed cardiovascular rehabilitation Rate of MI patients* prescribed cardiovascular rehabilitation following a myocardial infarction
Numerator Number of MI patients*: - with a prescription for cardiovascular rehabilitation - without a prescription, with a documented contraindication or patient refusal
Denominator Number of MI* patients * ACS with ST+ or LBBB and non-ST+ ACS Data CD – CR CO, GP: First consultation with primary care doctor This collection can be prospective and continuous: practice registries, databases,
observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
This good practice indicator may be collected in a healthcare establishment or in the short term during post-infarction follow-up by the care team at the healthcare establishment, by the cardiologist, or by the primary care doctor; each discipline selects indicators pragmatically from among all the indicators with a view to improving their practice.
Justification Post-infarction cardiovascular rehabilitation improves the patient’s quality of life
and in the medium term results in a 26% reduction in cardiovascular mortality and a 20% reduction in mortality from all causes. A cardiovascular rehabilitation programme ensures patients access: to an exercice training programme, to therapeutic optimisation, to multidisciplinary therapeutic education and to the monitoring of risk factors. This full care cycle takes account of the patient’s mental state and his/her personal, social and family concerns.
This indicator has been validated by professional consensus of the French national MI Task Force
Additional information A cardiovascular rehabilitation programme is currently recommended with a high
level of proof for all patients after an acute coronary syndrome (Guidelines GERS-SFC, 2011) In practice, it is necessary to check that the risk has been stratified before entering the patient in an exercise training programme. In the absence of any complications, a stress evaluation under treatment, limited by the symptoms, may be carried out 5 to 7 days after the heart attack, while the maximal test, without treatment, requires a wait of 4 weeks.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 17, 19, 22, 23, 37, 48, 52, 55 C: Indicators: 82, 86 D. Other: 126, 134, 153, 156, 173
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 27/85
14. Rate of patients assisted with smoking cessation Rate of smoking MI patients offered assistance with smoking cessation following an MI
Numerator Rate of MI* patients who smoke offered assistance with smoking cessation following an MI: - smoking cessation prescribed AND appropriate prescription for nicotine replacements - OR patient refusal
Denominator Number of MI* patients who are smokers *ACS with ST+ or LBBB, non-ST+ ACS Data CD – CR
GP1, CO: First consultation with the GP or cardiologist TA: consultation with the smoking cessation outpatients clinic
This collection can be prospective and continuous: practice registries, databases, observational study or retrospective and targeted when carrying out a survey: audit of patient files in each sector. This good practice indicator may be collected in the relevant healthcare establishment or during the post-infarction follow-up in the short term, by the care team in the healthcare establishment, by the cardiologist, by the smoking cessation adviser and by the primary care doctor; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification Total and final cessation of the use of tobacco in all its forms decreases the risk of a recurrence of myocardial infarction and mortality, with the best cost/benefit ratio in cardiovascular prevention.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information Following an acute coronary syndrome, management of the process of quitting the use of tobacco should start as early as in the Coronary Intensive Care Unit. All patients who are smokers will be given information about the risks associated with tobacco use (cardiovascular risks in particular) and the expected benefits that come with quitting, and assistance with quitting tobacco use will be offered:
- Firstly, in dependent patients: nicotine replacements1 in the immediate aftermath of an ACS (patch, chewing-gum, lozenges, inhaler, chewing-tablets).
In practice, in the absence of specific guidelines and targeted studies on adapting treatment, the initial dose of nicotine to be prescribed is assessed on the basis of the daily cigarette consumption, with in practice 1 mg of nicotine/cigarette.
- Secondly: other type of medicinal aid to smoking cessation (bupropion LP, varenicline);2 - Complementary treatments if necessary: behavioural and cognitive therapies, anxiolytic and/or antidepressant
treatments. Comprehensive customised drug and non-drug monitoring in conjunction with the primary care doctor should be organised. 1 Flat-rate provision in accordance with the National Health Insurance list. http://www.ameli.fr/professionnels-de-sante/medecins/exercer-au-quotidien/prescriptions/substituts-nicotiniques.php 2buproprion LP, varenicline are medicinal products placed on the watchlist on 04 May 2011 http://sante-medecine.commentcamarche.net/faq/5225-la-liste-des-77-medicaments-mis-sous-surveillance-par-l-afssaps; buproprion does not qualify for National Health Insurance reimbursement
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 22, 36, 37, 41, 42, 45, 50, 52, 61, 62 C: Indicators: 96, 98, 99, 112, 113, 114, 115, 117 D. Other: 124, 153, 161
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 28/85
15. Rate of patients receiving specialist diabetes advice on severe hyperglycaemia Rate of MI patients* with severe hyperglycaemia (blood sugar > 180 mg/dl or 10.0 mmol/l - HbA1c ≥ 8%) receiving specialist diabetes advice following an MI Numerator Rate of MI patients* with severe hyperglycaemia (blood sugar > 180 mg/dl
or 10.0 mmol/l – HbA1c ≥ 8%) for whom specialist diabetes advice is requested OR where the patient refuses
Denominator Number of MI* patients with severe hyperglycaemia (HbA1c ≥ 8%)
*ACS with ST+ or LBBB, non-ST+ ACS Data CD – DDE – CR
GP – CO: First consultation with the primary care doctor or cardiologist DA: consultation with the diabetes specialist
This collection can be prospective and continuous: practice registries, databases, observational study or retrospective and targeted when carrying out a survey: audit of patient files in each sector. This good practice indicator may be collected in a healthcare establishment or, in the short term, during post-infarction follow-up by the care team at the healthcare establishment, by the cardiologist, by the diabetologist or by the primary care doctor; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification Immediately following a myocardial infarction and in the longer term,
monitoring of blood sugar levels is a major prognostic factor. This indicator has been validated by professional consensus of the French national MI Task Force
Additional information In metropolitan France, the prevalence among adults aged between 18 and 74 years of fasting hyperglycaemia and/or antidiabetic treatments (oral or insulin) is 4.7%, of which 1.3% are not treated with antidiabetics. A major increase in the prevalence of treated diabetes estimated at +5.7% per year was reported between 2000 and 2005, with an increase in geographical disparities in prevalence. Diabetic patients (known or discovered) should be subject to suitable drug and non-drug follow-up in conjunction with the primary care doctor. Very unbalanced diabetes (blood sugar > 180 mg/dl or 10.0 mmol/l – HbA1c ≥ 8%), is one of those clinical situations for which recourse to advice from a diabetes specialist is recommended (Consensus SFD-SFC, 2011).
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 20, 22, 23, 24, 25, 52, 61, 62, 67 C: Indicators: 72 D. Other: 133, 153, 172

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 29/85
16. Rate of patients receiving information on using the emergency medical assistance
Rate of post-infarction patients* receiving information about the signs suggestive of a myocardial infarction (recurrence) and about the need to call SAMU (the emergency medical assistance) if these signs appear
Numerator Number of post-infarction patients* informed about the signs suggestive of a myocardial infarction and of the need to call SAMU (emergency medical assistance) in the event of these signs occurring, making a note in the medical file.
Denominator Number of post-infarction patients* * ACS with ST+ or LBBB and non-ST+ ACS
Data GP: First consultation with primary care doctor CA, PMP: cardiologist and/or paramedical professionals attending to the
patient in the first year post-infarction CR: cardiovascular rehabilitation This collection can be prospective and continuous: practice registries,
databases, observational study or retrospective and targeted when carrying out a survey: audit of patient files in each sector.
This good practice indicator is valid throughout the post-infarction follow-up by the primary care doctor and by the cardiologist; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification The call to SAMU (emergency medical assistance) ensures that the patient enters the best care pathway in terms of speed of diagnosis and treatment, thus helping to reduce mortality.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information The post-infarction patient (and ideally his/her family and friends) should
be given information/training, by whatever means and in whatever location, on recognising the signs suggestive of a recurrence and the need to call SAMU (emergency medical assistance) in the event that these signs occur. This information/training forms part of the comprehensive drug and non-drug care cycle.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 38, 39, 40, 52, 61, 62, 65 C: Indicators: 98, 109, 115 D. Other: 153

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 30/85
17. Rate of post-infarction patients investigated for chest pain and/or the use of nitrates
Rate of post-infarction patients* having their medical history taken to detect any occurrence, since leaving the healthcare establishment, of chest pain(s) and/or the use of glyceryl trinitrate or nitrate
derivatives
Numerator Number of post-infarction patients* having their medical history taken to detect any occurrence, since leaving the healthcare establishment, of chest pain(s) and/or the use of glyceryl trinitrate or nitrate derivatives and noted in the medical file
Denominator Number of post-infarction patients*
* ACS with ST+ or LBBB and non-ST+ ACS
Data GP: First consultation with primary care doctor CO, PMP: cardiologist and/or paramedical personnel attending to the patient in
the first year post-infarction CR: cardiovascular rehabilitation This collection can be prospective and continuous: practice registries,
databases, observational study or retrospective and targeted when carrying out a survey: audit of patient files in each sector.
This good practice indicator is valid throughout the post-infarction follow-up by the primary care doctor, the paramedical professional or by the cardiologist; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification The occurrence of chest pain(s), whether or not they necessitated the use of nitrate derivatives, should be routinely investigated as they could be indicative of an insufficiency or a failure of treatment compliance or the possible recurrence of an acute coronary syndrome (ischaemia).
This indicator has been validated by professional consensus of the French national MI Task Force Additional information The post-infarction patient (and ideally his family and friends) should be given
information/training, by whatever means and in whatever location, on recognising the signs suggestive of a recurrence, as well as how to react appropriately in the event that these signs occur. This information/training forms part of the comprehensive drug and non-drug care path.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 19, 28, 37, 52, 61, 62, 65 C: Indicators: 103, 109 D. Other: 153

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 31/85
18. Rate of post-infarction patients undergoing cardiovascular rehabilitation programmes
Rate of post-infarction patients* undergoing cardiovascular rehabilitation programmes
Numerator Number of post-infarction patients* who have undergone a
cardiovascular rehabilitation programme while hospitalised or as an outpatient
Denominator Number of post-infarction patients*
*ACS with ST+ or LBBB, non-ST+ ACS
Data CR: cardiovascular rehabilitation CO – GP: First or second consultation with the cardiologist and/or the GP This collection can be prospective and continuous: practice registries,
databases, observational study or retrospective and targeted when carrying out a survey: audit of patient files in each sector.
This good practice indicator is valid throughout the post-infarction follow-up by the GP, the paramedical professional or by the cardiologist; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification Post-infarction cardiovascular rehabilitation allows 26% reduction in cardiovascular mortality and a 20% reduction in mortality from all causes. The cardiovascular rehabilitation programme ensures patients are afforded access: to a physical fitness programme, to therapeutic optimisation, to multidisciplinary therapeutic education and to the monitoring of risk factors. This full care cycle takes account of the patient’s mental state and his/her personal, social, family and job concerns and helps improve the patient’s quality of life.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information
A cardiovascular rehabilitation programme is currently recommended with a high level of proof for all patients after an acute coronary syndrome (Guidelines GERS-SFC, 2011) In practice, it is necessary to check that the risk has been stratified before entering the patient in an exercise training programme. In the absence of any complications, a stress evaluation under treatment, limited by the symptoms, may be carried out 5 to 7 days after the heart attack, while the maximal test, without treatment, requires a wait of 4 weeks
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 17, 19, 22, 23, 37, 39, 48, 52, 55, 61, 62, 65 C: Indicators: 68, 86, 82, 101, 109 D. Other: 134, 139, 144, 146, 153, 168, 173, 176

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 32/85
19. Rate of patients whose blood pressure was monitored post-infarction
Rate of post-infarction patients* whose blood pressure was monitored
Numerator Number of post-infarction patients* whose blood pressure is measured and monitored at each consultation
Denominator Number of post-infarction patients* *ACS with ST+ or LBBB, non-ST+ ACS
Data GP: consultation with the GP during the year post-infarction CO: consultation with the cardiologist CR: cardiovascular rehabilitation PMP: paramedical professionals involved in caring for the patient This collection can be prospective and continuous: practice registries, databases,
observational study or retrospective and targeted when carrying out a survey: audit of patient files in each sector.
This good practice indicator is valid throughout the post-infarction follow-up by the primary care doctor, the cardiologist or the paramedical professionals; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification Monitoring the blood pressure by way of secondary prevention helps reduce cardiovascular events and mortality.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information The treatment care path for cardiovascular risk depends on the GP, with the ability to call on the opinions of specialists (in particular cardiologists and endocrinologists). The blood pressure goal depends on the patient’s profile. The commonly accepted goal in France is an SBP < 140 mm Hg and a DBP < 90 mm Hg, and 135 mm Hg and DBP < 85 mm Hg with self-monitoring (national information campaign of January 2012, whose target between now and 2015 is that 70% of treated hypertensive patients will be controlled). A guide for healthcare professionals is available on the Internet (cf. Appendix III D. 135). Achieving the target requires, in particular, that patients also make a contribution, and that it be set in the context of an overall drug and non-drug care cycle. Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 9, 10, 27, 32, 33, 37, 38, 39, 41, 48, 52, 56, 61, 62, 65, 135 C: Indicators: 68, 72, 78, 98, 109, 116 D. Other: 135, 137, 153, 158, 128
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 33/85
20. Rate of post-infarction patients evaluated for tolerance to BASA treatment Rate of post-infarction patients* assessed for tolerance to BASA treatment
Numerator Rate of post-infarction patients* assessed for tolerance to BASA treatment Beta-blockers, Antiplatelet drugs or platelet aggregation inhibitors (aspirin and/or clopidogrel,
prasugrel, ticagrelor or another platelet aggregation inhibitor), Statins, ACEI or ARA-II Denominator Number of post-infarction patients* *ACS with ST+ or LBBB, non-ST+ ACS
Data GP: First GP consultation CR: cardiovascular rehabilitation CO +/- other medical professionals (geriatricians, etc.) involved in the care of the
patient PMP: Paramedical professionals involved in caring for the patient This collection can be prospective and continuous: practice registries, databases,
observational study or retrospective and targeted when carrying out a survey: audit of patient files in each sector.
This good practice indicator is valid throughout the post-infarction follow-up by the primary
care doctor and by all medical and paramedical professionals caring for these patients; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification Poor tolerance and ignorance about the treatment are just some of the
factors behind patients’ poor compliance that need to be investigated. Compliance is essential for the treatment to be effective. Achieving recommended treatment objectives should be seen in the context of an overall drug and non-drug care cycle.
This indicator has been validated by professional consensus of the French national MI Task Force Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 16, 38, 39, 41, 46, 52, 61, 62, 65 C: Indicators: 109, 116 D. Other: 145, 153 Professional Consensus of the French National MI Task Force
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 34/85
21. Rate of patients receiving information about the need for regular post-infarction physical exercise Rate of post-infarction patients* who have been informed about the need to engage in regular physical exercise at the first consultation Numerator Number of post-infarction patients* who have been given information about
the need to take appropriate regular physical exercise (except in the case of documented inability to take exercise and comorbidities)
Denominator Number of post-infarction patients* *ACS with ST+ or LBBB, non-ST+ ACS
Data GP: First GP consultation CR: Cardiovascular rehabilitation PMP: Paramedical professionals involved in caring for the patient CO: Consultation with the cardiologist in the first year post-infarction This collection can be prospective and continuous: practice registries, databases,
observational study or retrospective and targeted when carrying out a survey: audit of patient files in each sector.
This good practice indicator is valid throughout the post-infarction follow-up by the primary care doctor, the cardiologist or the paramedical professionals; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification Immediately after the infarction, the patient should be informed and reassured about his capacity for resuming an active life. A sedentary existence is a known factor in recurrence. Engaging in 30 minutes’ moderate physical exercise a day, adjusted for the patient’s age and general condition, reduces the risk of recurrence and mortality.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information Achieving the target requires, in particular, that patients also make a
contribution. It should be set in the context of an overall drug and non-drug care cycle.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 22, 37, 38, 39, 41, 42, 55, 61, 62, 65, 67 C: Indicators: 68, 82, 109, 116 D. Other: 153, 156
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 35/85
22. Rate of post-infarction patients monitored for active smoking Rate of post-infarction patients* investigated for active smoking Numerator Number of post-infarction patients* investigated for active smoking Denominator Number of post-infarction patients* *ACS with ST+ or LBBB, non-ST+ ACS Data CR: cardiovascular rehabilitation GP, CO: consultations with the primary care doctor in the first year post-infarction TA: outpatient consultation with the smoking cessation clinic PMP: paramedical professionals involved in the first year post-infarction This collection can be prospective and continuous: practice registries, databases,
observational study or retrospective and targeted when carrying out a survey: audit of patient files in each sector.
This good practice indicator is valid throughout the post-infarction follow-up by the GP, the paramedical professional, the smoking cessation clinic or by the cardiologist; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification Quitting smoking completely and for good reduces mortality by 36% and recurrences at 5 years by 32%, with the best cost/benefit ratio in cardiovascular prevention.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information In France, around 20% (or 430/2392) of the patients are still smokers 18 months after an ACS, and this percentage has remained virtually unchanged since 1995. Patients who still smoked were encouraged to stop using tobacco and support measures will be offered to them routinely. They will be given information about the risks associated with smoking (cardiovascular risks in particular) and the expected benefits that come with quitting, and assistance with smoking cessation will be offered:
- recommended drug treatment (nicotine replacements:1 patch, chewing-gum, lozenges, inhaler, chewing-tablets; other:2 bupropion LP, varenicline).
- non-drug support measures, and in some cases specialist counselling. 1 Flat-rate provision in accordance with the National Health Insurance list. http://www.ameli.fr/professionnels-de-sante/medecins/exercer-au-quotidien/prescriptions/substituts-nicotiniques.php 2buproprion LP, varenicline are drug products placed on the watchlist on 04 May 2011 2011 http://sante-medecine.commentcamarche.net/faq/5225-la-liste-des-77-medicaments-mis-sous-surveillance-par-l-afssaps; buproprion does not qualify for National Health Insurance reimbursement In practice, assessing the initial nicotine dose to prescribe may be simply determined from the daily number of cigarettes smoked: 1 mg of nicotine/cigarette. Nicotine replacement products will be adjusted depending on the efficacy of the treatment in terms of the reduction in the tobacco consumption, symptoms associated with quitting tobacco consumption and the patient’s tolerance/compliance. Comprehensive post-infarction follow-up seeks to ensure that the patient has quit smoking for good and is protected from exposure to passive smoking, regularly monitoring his/her weight and waist circumference, and providing information and training on diet and physical exercise. There are tools available, such as: the study by Berlin et al. from 2011, and the AHRQ guidelines updated in 2009, based on the 2008 clinical practice guidelines. Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 22, 36, 37, 38, 41, 45, 48, 50, 52, 59 C: Indicators: 68, 98, 109, 115, 116, 117 D. Other: 119, 121, 124, 128, 136, 153, 155, 167, 170
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 36/85
23. Rate of patients having a lipid and blood glucose assessment 3 to 6 months post-infarction
Rate of post-infarction patients* having their LDL-cholesterol and fasting blood glucose (and glycosylated haemoglobin (HbA1c) for diabetic patients) checked 3 to 6 months after discharge
Numerator Number of post-infarction patients* having their LDL-cholesterol and fasting blood-glucose (or HbA1c (glycosylated haemoglobin) in the case of diabetic patients) checked 3 to 6 months after discharge
Denominator Number of patients seen in consultation during the course of the year post-infarction*
*ACS with ST+ or LBBB, non-ST+ ACS Data GP, CA: consultations with the primary care doctor in the first year post-infarction
DA: consultation by the diabetes specialist in the first year post-infarction
This collection can be prospective and continuous: practice registries, databases, observational study or retrospective and targeted when carrying out a survey: audit of patient files in each sector.
Justification In post-infarction patients it is important to monitor the metabolic risk factors (LDL-cholesterol level < 1 g/l and HbA1c < 7% in diabetics) and to screen for possible diabetes. An HbA1c (glycosylated haemoglobin) level < 7% in the years following a diagnosis of diabetes is currently acknowledged as being associated with a reduction in microvascular, neurological, as well as macrovascular complications.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information Screening relies on investigation for lipid abnormalities, which determines the concentrations of TC, TG, HDL-C and LDL-C. Dyslipidaemia is defined by: HDL-C < 0.40 g/l (1 mmol/l), LDL-C > 1.60 g/l (4.1 mmol/l), TG > 1.5 g/l (1.7 mmol/l). An LDL-C level < 1 g/l is recommended by way of secondary prevention. The definition of diabetes currently accepted in France is that of the WHO. Published definitions:
- a blood sugar level higher than 1.26 g/l (7 mmol/l) after 8 hours’ fasting (WHO and ADA 2010) and checked twice; - or the presence of symptoms of diabetes (polyuria, polydypsia, weight loss) associated with a blood sugar level (in venous plasma) greater than or equal to 2 g/l (11.1 mmol/l) (WHO and ADA 2010); - or a blood sugar level greater than or equal to 2 g/l (11.1 mmol/l) 2 hours after a 75 g glucose drink (criteria proposed by the WHO and ADA 2010). - HbA1c ≥ 6.5% (ADA 2010, WHO 2011).
The target HbA1c in diabetics is customised according to age and the history of complications, to optimise the balance between the risk of developing complications in the future, the risk of severe hypoglycaemias, treatment constraints and the benefit of a quality of life that is acceptable to and by the patient. Post-infarction diabetes screening is carried out under stable conditions and in the context of the patient’s actual lifestyle and diet. Achieving the target requires, in particular, that patients also make a contribution, and that it be set in the context of an overall drug and non-drug care cycle. Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 14, 23, 24, 25, 37, 39, 44, 51, 52, 61, 62, 65 C. Indicators: 72, 80, 98, 109 D. Other: 169

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 37/85
24. Rate of patients having their weight monitored
Rate of post-myocardial infarction patients* whose weight is monitored Numerator Number of post-myocardial infarction patients* whose weight is
measured Denominator Number of post-infarction patients*
*ACS with ST+ or LBBB, non-ST+ ACS
Data GP, CO: consultations with the primary care doctor in the first year post-infarction
PMP: paramedical professionals involved in caring for the patient
This collection may be prospective and continuous (practice registries, databases, observational studies) or based on a snap sample (or retrospective in the case of a survey: auditing of medical files). This good practice indicator is valid throughout the post-infarction follow-up by the GP, the cardiologist or the paramedical professionals; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Rationale Any increase in body fat in the abdominal region increases the risk of developing other risk factors (hypertension, type 2 diabetes, dyslipidaemia), cardiovascular risk and mortality.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information Body weight should be measured regularly, at least three times in the post-infarction year. Height should be measured at the first consultation. The patient’s weight and height should be recorded in their medical file in order to calculate their BMI and monitor its development. Definitions in adults: overweight: BMI ≥ 25 kg/m2; obesity ≥ 30 kg/m2. If the BMI is between 25 and 35 kg/m2, it is recommended to measure the waist, half-way between the last rib and the top of the iliac crest. A large waist circumference, ≥ 80 cm in women and ≥ 94 cm in men, is a risk factor for diabetes and cardiovascular disease, regardless of the BMI. Recommended target in adults:
- overweight without any associated comorbidity or excessive waistline: avoid putting on additional weight - overweight with associated comorbidities: lose weight - obesity: weight loss by 5 to 15% at a rate of 1 to 2 kg per month; adjust by way of secondary prevention
according to the patient’s age, comorbidities and choice. The HAS has published practical leaflets on diet and physical exercise to help doctors provide guidance for their patients. Achieving the target requires, in particular, that patients also make a contribution, and that it be seen as part of a comprehensive long-term care cycle, together with the primary care doctor.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 15, 38, 42, 52, 61, 62 C: Indicators: 79, 98

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 38/85
25. Rate of patients having their post-infarction physical activity monitored 3 to 6 months after discharge Rate of post-infarction patients* having their physical activity assessed 3 to 6 months after discharge Numerator Number of post-infarction patients* whose physical activity is
assessed 3 to 6 months after discharge (except in the case of documented incapacity for physical activity and comorbidities)
Denominator Number of post-infarction patients* *ACS with ST+ or LBBB, non-ST+ ACS
Data GP: consultation with the GP during the first year post-infarction CO: consultation with the cardiologist in the first year post-infarction PMP: paramedical professionals involved in caring for the patient CR: cardiovascular rehabilitation This collection can be prospective and continuous: practice registries,
databases, observational study or retrospective and targeted when carrying out a survey: audit of patient files in each sector. This good practice indicator is valid throughout the post-infarction follow-up by the primary care doctor, the cardiologist or the paramedical professionals; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification A sedentary lifestyle is a known factor in recurrence. Engaging in 30 minutes’
moderate physical exercise a day, adjusted for the patient’s age and general condition, reduces the risk of recurrence of ACS and mortality.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information Achieving the target requires, in particular, that patients also make a
contribution. It should be set in the context of an overall drug and non-drug care cycle.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 22, 37, 38, 39, 41, 52, 55, 61, 62, 65, 67 C: Indicators: 68, 86, 109, 116 D. Other: 128, 168
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 39/85
26. Rate of post-infarction patients examined for peripheral artery occlusive disease (PAOD) Rate of post-infarction patients* examined for peripheral artery occlusive disease by measuring their systolic pressure index (SPI) Numerator Number of post-infarction patients* examined for peripheral artery occlusive
disease by measurement of their SPI Denominator Number of post-infarction patients*
*ACS with ST+ or LBBB, non-ST+ ACS Data GP, CO: consultations with the primary care doctor in the first year post-infarction CR: cardiovascular rehabilitation This collection can be prospective and continuous: practice registries, databases,
observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
This good practice indicator is valid throughout the post-infarction follow-up by the primary care doctor and by all medical and/or paramedical professionals caring for these patients; each discipline selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification Smoking is the primary risk factor for PAOD. Secondary prevention is useful and
effective for reducing cardiovascular risk of a low SPI and for improving the patient’s quality of life. Measuring the SPI is simple and quick and may be performed either in hospital or on an outpatient basis. It should be done routinely in patients aged from 40-50 years, especially after a myocardial infarction and/or in the presence of cardiovascular risk factors.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information The history-taking interview (looking for antecedents of clinical manifestations of ischaemia occurring either on effort or at rest, episodes of acute ischaemia, amputation) and clinical examination (feeling the pulse, measuring the SPI) all make it possible to assess the stage of the PAOD. The optimum care pathway for PAOD in post-infarction patients comprises: quitting smoking, prescribing statins to reduce the hypercholesterolaemia, antihypertensives for controlling the hypertension, including ACEI and ARA-II and platelet aggregation inhibitors, but also a balanced diet and a supervised physical rehabilitation and, ideally, therapeutic education. The stages of PAOD defined in the ALD 2007 guide are: • asymptomatic exercise ischaemia: SPI < 0.9 or lack of pulse with no clinical signs of ischaemia • symptomatic exercise ischaemia: SPI < 0.9 or lack of pulse with clinical signs of ischaemia • chronic permanent ischaemia: combination of decubitus pains or trophic disorders for at least two weeks, with an ankle systolic blood below 50 mm Hg or 30 mm Hg at the toe. This requires hospitalisation.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 58, 63, 64 C: Indicators: 85 D. Other: 165

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 40/85
27. Rate of patients receiving appropriate beta-blocker treatment at 1 year
Rate of post-infarction patients receiving appropriate* beta-blocker treatment 1 year after discharge from the healthcare establishment
Numerator Number of post-infarction patients 1 year after discharge from the healthcare establishment
with a prescription for beta-blocker, or without a prescription for beta-blocker, with a documented
contraindication (arteritis, diabetes or left ventricular dysfunction not acceptable as contraindications)
without a prescription for beta-blockers, with a documented intolerance and a prescription for ivabradine
or patient refusal recorded in the medical file
Denominator Number of patients surviving at 1 year post-infarction
Data GP: consultation with the GP at 1 year post-infarction CO: consultation with the cardiologist at 1 year post-infarction This collection can be prospective and continuous: practice registries,
databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification Long-term beta-blocker treatment after myocardial infarction has shown a gain in terms of morbidity and mortality and should be continued. A review of the patient’s appropriate prescription in conjunction with the cardiologist is proposed to assess the risk-benefit analysis.
This indicator has been validated by professional consensus of the French national MI Task Force
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 16, 37, 38, 39, 41, 42, 48, 61, 62, 65 C: Indicators: 68, 77, 105, 109, 116 D. Other: 128, 174
* “Appropriate” prescription refers to a prescription where there is a corresponding indication, and the lack of a prescription where there is a corresponding contraindication, or no indication or a refusal on the part of the patient.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 41/85
28. Rate of patients receiving appropriate aspirin treatment at 1 year
Rate of post-infarction patients with appropriate* aspirin treatment 1 year after discharge from the healthcare establishment
Numerator Number of post-infarction patients 1 year after discharge from the healthcare establishment
with a prescription for aspirin, or without a prescription for aspirin, with a documented
contraindication or patient refusal
Denominator Number of patients surviving at 1 year post-infarction
Data GP: consultation with the GP at 1 year post-infarction CO: consultation with the cardiologist at 1 year post-infarction This collection can be prospective and continuous: practice registries,
databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification Long-term treatment with aspirin has shown a gain in terms of
morbidity and mortality and should be continued for life. This indicator has been validated by professional consensus of the French national MI Task Force Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 16, 22, 37, 38, 39, 41, 42, 48, 61, 62, 65 C: Indicators: 68, 76, 98, 104, 109 D. Other: 128, 174
* “Appropriate” prescription refers to a prescription where there is a corresponding indication, and the lack of a prescription where there is a corresponding contraindication, or no indication or a refusal on the part of the patient.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 42/85
29. Rate of patients receiving appropriate treatment with a platelet aggregation inhibitor (apart from aspirin) at 1 year Rate of post-infarction patients receiving appropriate* treatment with a platelet aggregation inhibitor (apart from aspirin) 1 year after discharge from the healthcare establishment
Numerator Number of post-infarction patients at 1 year after discharge from the healthcare establishment with a prescription and an indication for a platelet aggregation inhibitor (apart
from aspirin), without a prescription for a platelet aggregation inhibitor (apart from aspirin), with
a documented contraindication or patient refusal without a prescription for a platelet aggregation inhibitor (apart from aspirin), in
the absence of an indication
Denominator Number of patients surviving at 1 year post-infarction
Data GP: consultations with the GP at 1 year post-infarction CO: consultation with the cardiologist at 1 year post-infarction This collection can be prospective and continuous: practice registries, databases,
observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification Reviewing the appropriate prescription for a platelet aggregation inhibitor makes it possible to assess, together with the cardiologist, the risk-benefit ratio of continuing the treatment beyond 1 year.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information Treatment with a platelet aggregation inhibitor (apart from aspirin) beyond one year is
envisaged if an active stent has been placed. Clopidogrel or prasugrel or ticagrelor are currently the platelet aggregation inhibitors used in combination with aspirin in the absence of any contraindications. There are calls for other platelet aggregation inhibitors validated in this indication to be placed on the market.
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 16, 21, 31, 35, 37, 38, 39, 41, 42, 48, 61, 62, 65 C: Indicators: 68, 76, 104, 109, 110, 116 D. Other: 123, 128, 148, 166, 174 * “Appropriate” prescription refers to a prescription where there is a corresponding indication, and the lack of a prescription where there is a corresponding contraindication, or no indication or a refusal on the part of the patient.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 43/85
30. Rate of patients receiving appropriate statin treatment at 1 year
Rate of post-infarction patients with appropriate* statin treatment 1 year after discharge from the healthcare establishment
Numerator Number of post-infarction patients 1 year after discharge from the healthcare establishment
with a prescription comprising a statin without a prescription for statin but with a documented
contraindication or patient refusal Denominator Number of patients surviving at one year post-infarction
Data GP: consultation with the GP at 1 year post-infarction CO: consultation with the cardiologist at 1 year post-infarction This collection can be prospective and continuous: practice registries,
databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification Taking a statin by way of secondary prevention reduces the risk of mortality and recurrences in patients who have had a myocardial infarction.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information Target objective in cases of dyslipidaemia: LDL-cholesterol < 1 g/l. Serious adverse events are uncommon (< 1%), consisting essentially of rhabdomyolysis and myalgia, elevated levels of transaminases (ASAT and ALAT) and CPK. Checking the transaminase levels is vital at least once during the three months following the start of the treatment. If the initial determination of the CPK level before the commencement of treatment is not scientifically justified (except in certain at-risk situations), any unexplained muscle symptom appearing during treatment should lead to a CPK determination. This monitoring applies to fibrates, statins and ezetimibe, either alone or in combination with statins. Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 16, 37, 38, 39, 41, 42, 44, 48, 57, 61, 62, 65 C: Indicators: 68, 98, 109, 116 D. Other: 128, 174
* “Appropriate” prescription refers to a prescription where there is a corresponding indication, and the lack of a prescription where there is a corresponding contraindication, or no indication or a refusal on the part of the patient.
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 44/85
31. Rate of patients receiving appropriate treatment with a ACEI
Rate of post-infarction patients receiving appropriate* treatment with Angiotensin converting enzyme inhibitor or ARA-II
Numerator Number of post-infarction patients 1 year after discharge from the healthcare establishment with a prescription for an ACEI, or ARA-II if ACEIs are
contraindicated without a prescription for either a ACEI or ARA-II, but with a
documented contraindication to ACEIs and to ARA-II or a patient refusal moderate renal insufficiency, i.e. creatinine clearance > 30 ml/min,
is not acceptable as a contraindication
Denominator Number of surviving patients at 1 year post-infarction with impairment of left ventricular function
Data GP: GP consultations in the first year post-infarction CO: consultation with the cardiologist in the first year post-infarction This collection can be prospective and continuous: practice registries,
databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification ACEI treatment reduces serious cardiovascular events and mortality
due to myocardial infarction. This indicator has been validated by professional consensus of the French national MI Task Force
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 16, 37, 38, 39, 41, 42, 48, 61, 62, 65 C: Indicators: 68, 72, 75, 109, 116 D. Other: 128, 174
* “Appropriate” prescription refers to a prescription where there is a corresponding indication, and the lack of a prescription where there is a corresponding contraindication, or no indication or a refusal on the part of the patient.
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 45/85
32. Rate of post-infarction patients having their diet monitored Rate of post-infarction patients whose diet is followed up at least once during the post-infarction year
Numerator Rate of post-infarction patients whose diet is followed up at least once
during the post-infarction year Denominator Number of post-infarction patients Data CR: cardiovascular rehabilitation GP: consultation with the GP during the first year post-infarction CO: consultation with the cardiologist in the first year post-infarction PMP: dieticians and paramedical professionals involved in caring for the patient This collection can be prospective and continuous: practice registries, databases,
observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector. This good practice indicator is valid throughout the post-infarction follow-up by the GP, the cardiologist and/or the paramedical professionals; each discipline or profession selected indicators pragmatically from among all the indicators with a view to improving their practice.
Justification As secondary prevention, following rules regarding lifestyle and diet (balanced diet, quitting
smoking, and physical exercise) improves the quality of life and reduces the risk of myocardial infarction recurring and mortality. The benefit to the patient starts in the first year of follow up and achieves a 22% reduction in mortality at 4.7 years. After the dietary assessment in the first year, an assessment every 1 or 2 years appears desirable to ensure that the recommended diet is being maintained.
This indicator has been validated by professional consensus of the French national MI Task Force Additional information Secondary prevention guidelines: limit the intake of saturated fatty acids; increase the consumption of omega 3 polyunsaturated fatty acids, increase the consumption of fruit and vegetables (fibre and natural micronutrients); limit dietary cholesterol with an omega 6/omega 3 ratio < 5 (ANC-Lipides 2010 – French recommended daily allowances), reduce salt consumption (< 6 g/day, PNNS – French national programme on nutrition and health, WHO), limit alcohol consumption to 1 or two glasses of wine or beer/day (French Cardiology Society) and do not encourage abstainers to consume alcohol, even in moderate quantities, on a regular basis, as any regular consumption places that person at risk of cancer from the first glass of wine (French National Cancer Institute). The High Council for Public Health encourages scientific research in order to define the risk attributable to the consumption of small quantities of alcohol in terms of cardiovascular disease and/or cancer and, if applicable, to examine the risk/benefit ratio of consuming small doses of alcohol (HCSP 2009). In diabetics, reduce the intake of fats, above all saturated fats and refined sugars. Patients’ active involvement in managing their risk factors is vital and they should be given customised education regarding diet, treatment compliance, weight watching and regular endurance training. In practice, dietary advice should be adjusted for age and the patient’s risk profile by emphasizing cardiovascular prevention in the case of young people, and a balanced diet and prevention of undernourishment in the case of the elderly. French dietary assessment tools have been published (e.g. validated questionnaire published by Laviole and Paillard. 2005 – a simplified questionnaire is in process of being drawn up by this team – or the score published by the team of Dr Héricotte, Sylvie Caspar-Bauguil et al. 2010 - Marc Baudet et al. 2006). Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 10, 12, 37, 38, 39, 41, 42, 47, 48, 52, 54, 60, 61, 62, 65, 66, 67, 141 C: Indicators: 68, 98, 109, 111, 116 D. Other: 122, 125, 128, 130, 131, 132, 142, 144, 157, 162, 164
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 46/85
33. Rate correspondence between the primary care doctor and the cardiologist for the post-infarction follow-up Rate of post-infarction patients* given a letter by their primary care doctor referring them for a visit to the cardiologist during the year post-infarction
Numerator Number of patients for whom the primary care doctor has written to the cardiologist prior to the check-up during the first year post-infarction*
Denominator Number of post-infarction patients* *ACS ST+ or LBBB, non-ST+ ACS
Data GP: consultation with the GP during the first year post-infarction CO: consultation with the cardiologist in the first year post-infarction
This collection can be prospective and continuous: practice registries,
databases, observational study, or retrospective and targeted when carrying out surveys: audits of patient files in each sector.
Justification Exchanging information is vital for coordinating follow-up and care, for sharing the patient’s progress, assessing the risk-benefit ratio for reviewing appropriate drug prescriptions (including platelet aggregation inhibitors other than aspirin) and non-drug prescriptions, and for referring the patient, if necessary, for specialist care.
This indicator has been validated by professional consensus of the French national MI Task Force
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 B. Guidelines: 65 C. Indicators: 98, 109

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 47/85
34. 30-day mortality rates Optional Rate of ACS ST+ or LBBB patients who died in the 30 days following initial admission to the healthcare establishment
Type of indicator: The indicator in question is a clinical impact indicator The mortality rate from all causes is a classic public health indicator that can be monitored for epidemiological purposes or for information purposes within a care team. The risk-adjusted 30-day mortality rate is an outcome indicator which conveniently complements the clinical practice indicators. However, collecting the mortality rate is a long and difficult task, as it necessitates following up patients after they have been discharged from the healthcare establishment. Moreover, for comparisons between teams (benchmarking), this rate has to be risk-adjusted, which requires the collection and processing of all the elements necessary for establishing an actual risk score. On account of these practical difficulties, the mortality rate is not used initially as a shared indicator of improvements in practices. The frequency of risk distribution, whatever scoring system is used, is an indispensable tool for qualifying and above all comparing the patients included. For teams wishing to collect this indicator, the Task Force proposes to use at least the Simple Risk Index (SRI) (cf. Appendix III. D, references 118, 163,140) With a view to improving practices, it would seem appropriate to analyse the mortality associated with cardiovascular events. The latter, after risk-adjustment, will make it possible to measure the impact in terms of mortality for the cardiovascular care cycle as a whole. This indicator should be interpreted with regard to survival and quality of life. This indicator has been validated by professional consensus of the French national MI Task Force
Numerator Number of ACS ST+ or LBBB* patients who died in the 30 days following initial admission to the healthcare establishment
Denominator Number of patients admitted with a diagnosis of myocardial infarction (ACS ST+ or LBBB*)
Data APP (acute phase care pathway).
This collection may be prospective and continuous (practice registries, databases, observational studies) or based on a snap sample (retrospective when conducting surveys: auditing of medical files). In order for this indicator to be interpretable and compared (over time or with a view to benchmarking), it should ideally be risk-adjusted (cf. following chapter “Risk and mortality scores”. Proposed use of risk scores for calculating the probability of death: 30-day mortality adjusted at least to the SRI or to EMMACE, hospital mortality adjusted to the GRACE score).
Bibliographic references (Appendix III) A. Method: 1, 2, 3, 4, 5, 6, 7, 8 C: Indicators: 73, 83, 84, 87, 88, 89, 102 D. Other: 109, 118, 163, 140 Professional Consensus of the French National MI Task Force * Recent or presumed recent LBBB

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 48/85
7. Risk and mortality scores
Many risk scores have been validated for myocardial infarction, including TIMI (Thrombolysis In Myocardial Infarction http://www.timi.org) (154, 147, 143, 138, 163), KILLIP (154), GRACE (Global Registry of Acute Coronary Events) (147, 143), EMMACE (Evaluation of the Methods and Management of Acute Coronary Events) (138) and SRI (Simple Risk Index) (163). The clinical value of using risk scores is to enable risk to be stratified (118) for the purpose of adapting treatment. Risk scores are based, at the very least, on such parameters as age, systolic blood pressure and heart rate. These scores also help in estimating theoretical/expected risk-adjusted mortality. This theoretical/expected mortality can be calculated per patient, and then estimated for the study population. A comparison can then be made between the theoretical/expected mortality and the actual/observed mortality. Three risk scores have been validated for cases of ACS ST+ and non-ST+ for many populations (140): GRACE (147, 143), EMMACE (138) and SRI (163).
Proposed use of risk scores for calculating the probability of death: Hospital mortality
GRACE (Global Registry of Acute Coronary Events) (147, 143) - Use the automatic calculator available online at www.outcomes-umassmed.org/grace/ - Individual risk: enter the data for each patient into the calculator. Each patient’s risk score and
probability of death is displayed automatically. - Collective risk: The probability of death of the population is obtained by calculating the mean of the
individual probabilities of death.
30-day mortality 1. EMMACE (Evaluation of the Methods and Management of Acute Coronary Events) (138)
- Use the logarithmic formula to directly calculate the 30-day probability of death (P30) (and not the risk score): P30 = 1/1+exp [-6.914+(0.081 × age)+(0.016 × heart rate)-(0.016 × SBP)]
- Individual risk: Enter the data for age, systolic blood pressure and heart rate for each patient in an Excel spreadsheet. By applying the formula the probability of death can be calculated for each patient.
- Collective risk: The probability of death of the population is obtained by calculating the mean of the individual probabilities of death.
2. SRI (Simple Risk Index)) (163)
- Use the formula: Heart rate (beats per minute) × (age/10)2/SBP (in mm Hg). - Individual risk: Enter the data for age, systolic blood pressure and heart rate for each patient in an
Excel spreadsheet. Apply the formula to calculate the risk score for each patient. The probability of death of each patient from the calculated risk score is obtained by referring to the table below:
Risk index Group risk 30-day death risk (absolute)
≤ 12.5 1 0.8 12.5-17.5 2 1.9 17.5-22.5 3 3.3 22.5-30 4 7.3
> 30 5 17.4
Table taken from the publication by Morrow et al. 2001 (163)
- Collective risk: The probability of death of the population is obtained by calculating the mean of the individual probabilities of death.
SBP: Systolic blood pressure

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 49/85
Interpreting risk-adjusted mortality rates – Discussion
With a view to improving practices, it would seem appropriate to analyse the mortality associated with cardiovascular events. After risk-adjustment, the latter will reflect the impact of cardiovascular care, excluding any associated comorbidities and/or accidents. The existence of a significant difference measured at 30 days between the actual mortality rate and the expected mortality rate should lead the professionals involved to analyse the principal stages of the patient’s management, from the first symptoms right until his/her death. The shared clinical practice indicators that measure the quality of clinical practices throughout the care cycle are very useful for this analysis, in terms of the time between the onset of pain and the medical treatment, starting reperfusion by whatever technique (thrombolysis or angioplasty), treatment received prior to hospital admission and treatments prescribed on discharge from the healthcare establishment and actually taken, the commencement of cardiovascular rehabilitation and therapeutic education and the patient’s adherence to a changed lifestyle (follow-up of drug and non-drug treatment, including quitting smoking, physical exercise, etc.). The analysis will reveal any areas of weakness, which will serve as a basis for remedial actions. The impact of these targeted actions will be measured by the changes in the clinical practice indicators in the care pathway, including the mortality rate. No comparison of the 30-day mortality rate can be made until after adjustment to the risk in the populations concerned (expected/observed at time T, between healthcare establishments at time T, any time comparison, etc.).
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 50/85
8. List of proposed items for clinical practice indicators collection
Admitted to the care cycle in the acute phase (pre-admission or post-admission) - Time of onset of pain/first symptoms - Call to SAMU emergency medical assistance in first instance (yes, no) - Time of call to SAMU emergency medical assistance - Time of arrival on scene - Time of first medical contact: in practice estimated by the time of the qualifying ECG - Type of ACS (ACS with ST+ or LBBB; non-ST+ ACS) - Patient put on aspirin (yes, no, CI, refused, patient already on platelet aggregation inhibitor) - Patient put on another platelet aggregation inhibitor: clopidogrel, prasugrel or ticagrelor (yes, no, CI, refused,
patient already on platelet aggregation inhibitor) - Evaluation of pain by VAS or NS (yes, no) - If VAS ≥ 60 mm or NS≥ 6, patient treated with morphine (yes, no, CI, refused) - Direct referral to an ICC with a technical support centre available (yes, no) - Arrival time at ICC or on catheterisation ward - Reperfusion given (yes, no, CI, refused) - Time of primary angioplasty: time of first balloon inflation or first thromboaspiration or direct stenting, and
otherwise puncture time - Thrombolytic agent injection time - Left ventricular ejection fraction (LVEF) in % (< or > 40%) - Evaluation of left ventricular function (echocardiography, angiography or scintigraphy) (yes, no) - LVEF altered (yes, no) - GRACE score calculated (yes, no) - Discharged with beta-blocker (yes, no, CI, intolerance, refused) - Discharged with ivabradine (yes, no, CI, intolerance, refused) - Discharged with aspirin (yes, no, CI, intolerance, refused) - Discharged with clopidogrel (yes, no, CI, intolerance, refused) - Discharged with statin (yes, no, CI, intolerance, refused) - Discharged with Angiotensin converting enzyme inhibitor (ACEI) (yes, no, CI, intolerance, refused) - Discharged with ARA-II (yes, no, CI, intolerance, refused) - Discharged with prescription for cardiovascular rehabilitation (yes, no, absolute CI, refused, lack of available
cardiovascular rehabilitation centre) - Active smoking (yes, no) - Number of cigarettes consumed per day: - Passive smoking (yes, no) - Prescription for smoking cessation products (yes, no, not applicable- patient is a non-smoker-) - Evaluation of the patient’s mental state (yes, no, refused) - Depression/anxiety diagnosed - Appropriate prescription for nicotine substitutes (yes, no, CI, not applicable -patient a non-smoker-, refused) - Blood glucose measured (yes, no) - Blood glucose value on admission: - Historical fasting blood glucose value: - HbA1c measured (yes, no) - Value of HbA1c: - Diabetes (yes, no) - Severe hyperglycaemia during or with regression of the ACS (yes, no) - Diabetologist’s advice requested in hospital or during the 3 months post-infarction (yes, no, not indicated,
refused) - Referred for specialist management in a hospital or post-infarction ambulatory setting: consultation with
smoking cessation clinic, diabetes clinic, dietician, therapeutic education, assistance with compliance or therapeutic education programme or cardiovascular rehabilitation programme (yes, no, not indicated, refused, not available)
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 51/85
Follow-up until 1 year post-infarction
Short-term follow-up - Date of myocardial infarction - Date of discharge from healthcare establishment - Type of myocardial infarction (ACS ST+, ACS with LBBB, non-ST+ ACS, unspecified) - Chest pain and/or nitrate use (yes, no) - Patient informed about signs suggestive of myocardial infarction (yes, no) - Patient informed of the need to call the emergency medical assistance if such signs occur (yes, no) - Cardiovascular rehabilitation programme arranged (yes, no, absolute CI, not available) - Fasting blood glucose tested (yes, no) - Fasting blood glucose value: - HbA1c measured (yes, no) - Value of HbA1c: - Diabetes (yes, no) - Severe hyperglycaemia during the ACS (yes, no) - Diabetologist’s advice requested in hospital or during the 3 months post-infarction (yes, no, not
indicated, refused) - Referred for specialist management in a hospital or ambulatory setting: consultation with smoking
cessation clinic, diabetes clinic, dietician, therapeutic education, assistance with compliance or therapeutic education programme or cardiovascular rehabilitation programme (yes, no, not indicated, refused, not available)
- Blood pressure measured during consultations (yes, no) - Patient shown how to measure own blood pressure (yes, no, refused) - Search for elements of tolerance to BASA treatment (beta-blocker or ivabradine, antiplatelet drugs /
platelet aggregation inhibitor (aspirin and/or clopidogrel or prasugrel or ticagrelor), statin, ACEI or ARA-II) (yes, no)
- Patient informed about the need to engage in regular physical exercise (yes, no, CI, refused) Medium-term follow-up (between 3 and 6 months post-infarction)
- Active smoking (yes, no) - Number of cigarettes consumed per day: - Plan to quit smoking (yes, no, not applicable -patient a non-smoker-) - Passive smoking (yes, no) - Prescription for smoking cessation products (yes, no, not applicable -patient is a non-smoker-) - Evaluation of the patient’s mental state (yes, no, refused) - Depression/anxiety diagnosed - Appropriate prescription for nicotine substitutes (yes, no, CI, not applicable –patient a non-smoker,
refused) - Referred for specialist management in a hospital or ambulatory setting: consultation with smoking
cessation clinic, diabetes clinic, dietician, therapeutic education, assistance with compliance or therapeutic education programme or cardiovascular rehabilitation programme (yes, no, not indicated, refused, not available)
- Height: - Weight: - BMI monitored (yes, no) - Waist circumference measured (yes, no) - Checked for peripheral artery occlusive disease (yes, no) - Systolic pressure index (SPI) measured (yes, no) - Fasting LDL cholesterol measured (yes, no) - Fasting blood glucose or glycosylated haemoglobin in a diabetics measured (yes, no) - Information about physical exercise (yes, no, done within the framework of a therapeutic education
setting) - stress ECG (yes, no, CI) - Patient engages in regular physical activity for at least 30 min per day (yes, no, CI, refused)
Follow-up at 1 year - Evaluation of LVEF (echocardiography, angiography or scintigraphy) (yes, no) - LVEF in %: (< or > 40%)

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 52/85
- LVEF altered (yes, no) - Treatment with beta-blocker (yes, no, CI, intolerance, refused) - Treatment with ivabradine (yes, no, CI, intolerance, refused) - Treatment with aspirin (yes, no, CI, intolerance, refused) - Treatment with another platelet aggregation inhibitor (clopidogrel, prasugrel or ticagrelor) (yes, no, CI,
intolerance, refused) - Treatment with ACEI (yes, no, CI, intolerance, refused) - Treatment with ARA-II (yes, no, CI, intolerance, refused) - Dietary assessment (including alcohol consumption) (yes, no, refused) - Correspondence between GP and cardiologist (yes, no)
At 30 days post-infarction - Patient died (yes, no, not known) - Date of death - Cause of death - Heart rate, age, systolic blood pressure documented (yes, no) - SRI (Simple Risk Index) calculated (yes, no) - Mortality adjusted for expected risk - Mortality adjusted for observed risk To interpret an observed mortality rate, it is essential to compare it with the expected mortality rate taking into account the risk factors of the study population. There are three valid risk scores. The most simple score can be calculated using the formula: SRI (Simple Risk Index) = Heart rate × (age/10)2/Systolic blood pressure. The corresponding expected mortality is obtained from a table (cf. section on “Risk and mortality scores”).
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 53/85
APPENDICES
All these tools are available and downloadable on the HAS website
www.has-sante.fr
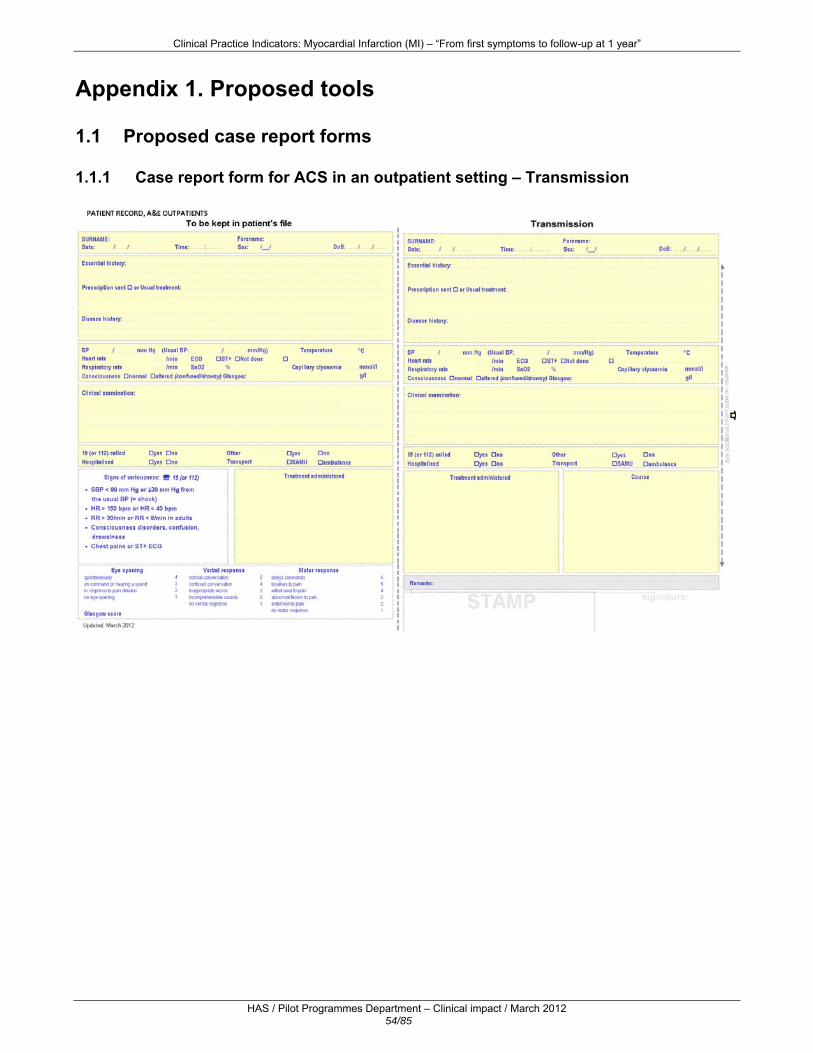
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 54/85
Appendix 1. Proposed tools
1.1 Proposed case report forms 1.1.1 Case report form for ACS in an outpatient setting – Transmission

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 55/85
1.1.2 Case report form for A&E
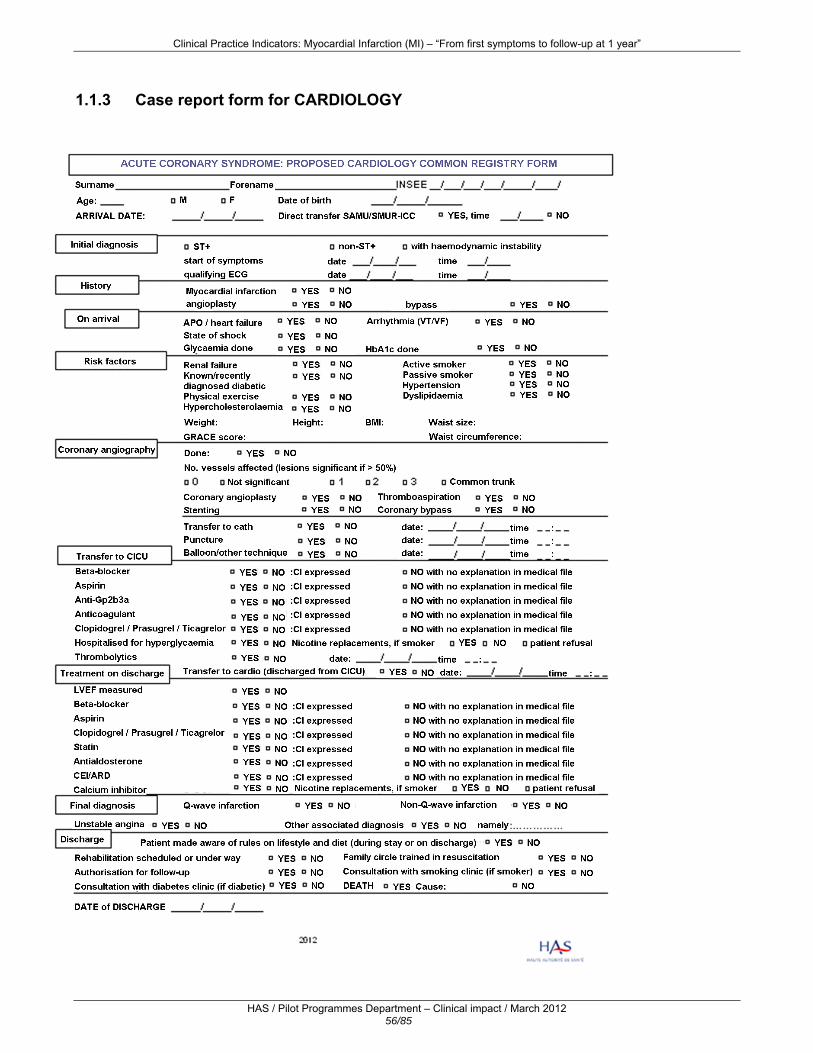
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 56/85
1.1.3 Case report form for CARDIOLOGY

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 57/85
1.1.4 Ambulatory follow-up form – 1st year post-infarction 1. Time since myocardial infarction (ACS ST+, ACS with LBBB, non-ST+ ACS)?
1 month 3 months 6 months
1 year > 1 year Not known
2. Do you know the signs suggestive of a recurring myocardial infarction?
Yes No
3. Do you know that the emergency services must be called immediately in the event of a recurrence?
Yes No
4. Have you felt any chest pains and/or have you taken any nitrate?
Yes No
Don’t know
5. Have you taken part in a cardiovascular rehabilitation programme?
Yes Time after infarction
No Don’t know
7. Active tobacco user
Yes - Number of cigarettes/day - Thinking of quitting
No - Never smoked - If quit, since when
8. Have you measured your weight?
Yes No
BMI calculated Waist circumference
measured 9. Screening for peripheral artery occlusive disease (PAOD)
Yes No
SPI measured
10. Blood pressure measured
Yes No 11. Blood glucose tested
Yes No 12. Lipid assessment carried out
Yes No 13. Do you do 30 minutes of regular physical exercise?
Yes No 14. Do you know about the post-infarction diet?
Yes No 15. Do you follow the instructions for the post-infarction diet?
Yes No
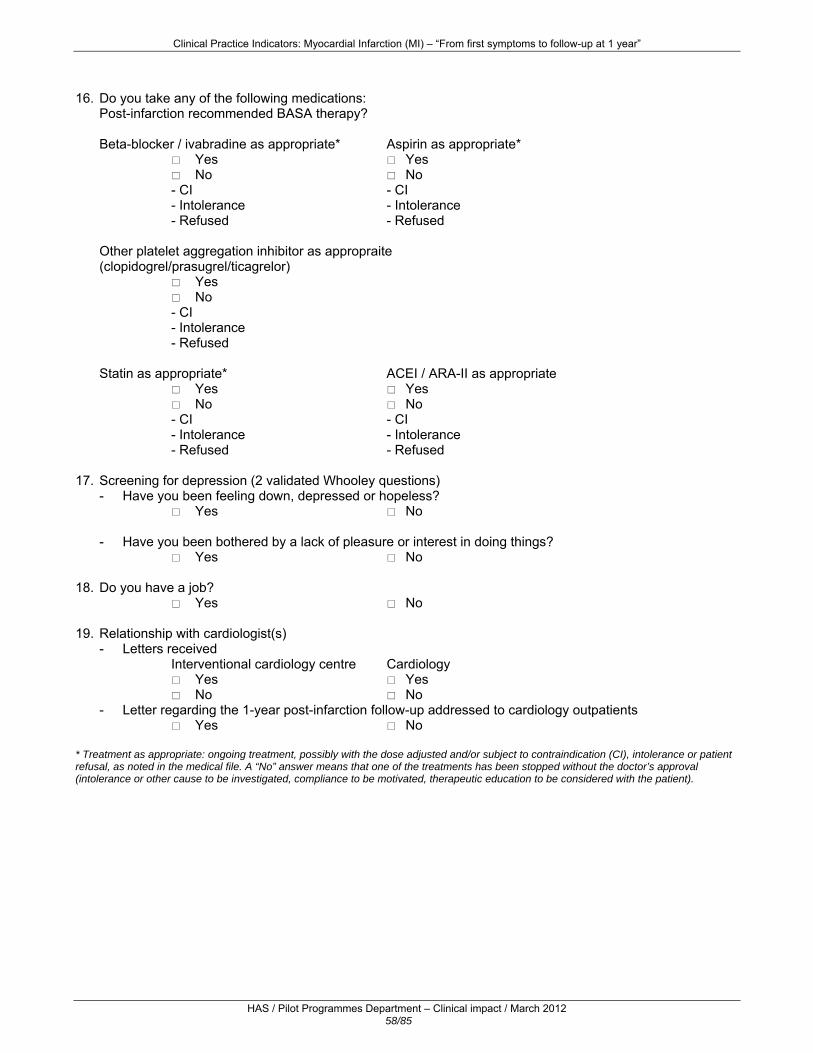
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 58/85
16. Do you take any of the following medications: Post-infarction recommended BASA therapy? Beta-blocker / ivabradine as appropriate* Aspirin as appropriate*
Yes No
- CI - Intolerance - Refused
Yes No
- CI - Intolerance - Refused
Other platelet aggregation inhibitor as appropraite (clopidogrel/prasugrel/ticagrelor)
Yes No
- CI - Intolerance - Refused
Statin as appropriate* ACEI / ARA-II as appropriate
Yes No
- CI - Intolerance - Refused
Yes No
- CI - Intolerance - Refused
17. Screening for depression (2 validated Whooley questions) - Have you been feeling down, depressed or hopeless?
Yes No - Have you been bothered by a lack of pleasure or interest in doing things?
Yes No 18. Do you have a job?
Yes No 19. Relationship with cardiologist(s) - Letters received
Interventional cardiology centre Yes No
Cardiology Yes No
- Letter regarding the 1-year post-infarction follow-up addressed to cardiology outpatients Yes No
* Treatment as appropriate: ongoing treatment, possibly with the dose adjusted and/or subject to contraindication (CI), intolerance or patient refusal, as noted in the medical file. A “No” answer means that one of the treatments has been stopped without the doctor’s approval (intolerance or other cause to be investigated, compliance to be motivated, therapeutic education to be considered with the patient).
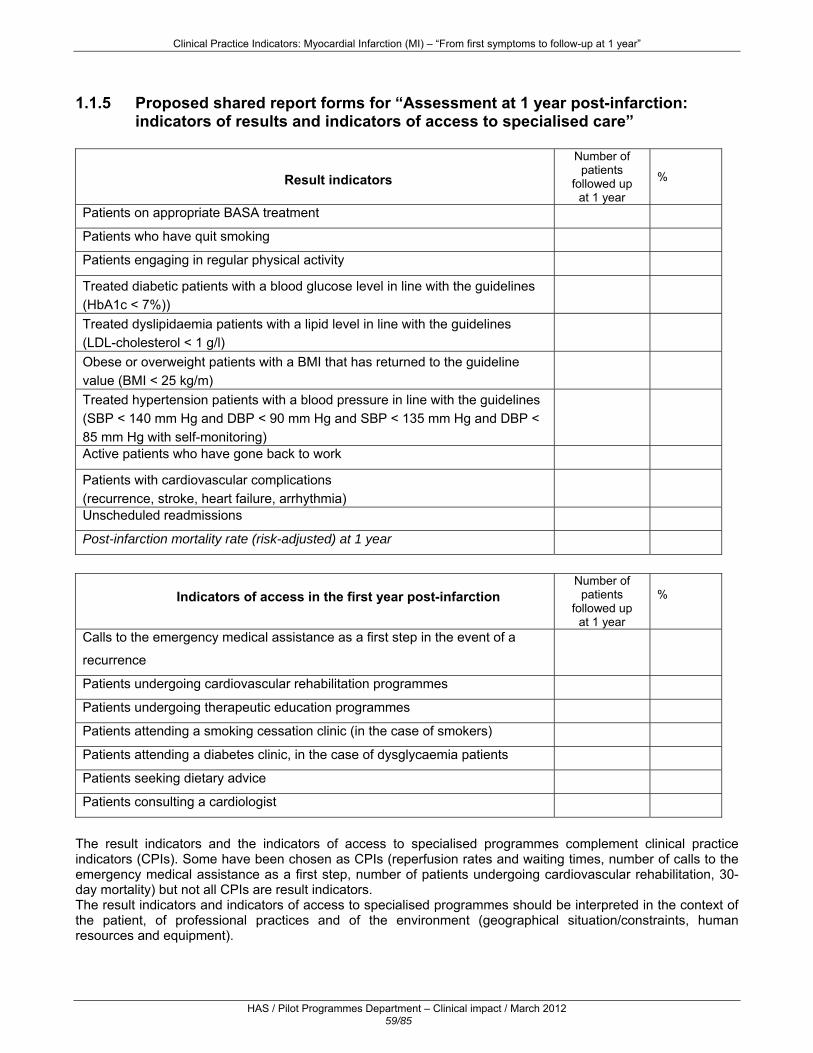
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 59/85
1.1.5 Proposed shared report forms for “Assessment at 1 year post-infarction:
indicators of results and indicators of access to specialised care”
Result indicators
Number of patients
followed up at 1 year
%
Patients on appropriate BASA treatment
Patients who have quit smoking
Patients engaging in regular physical activity
Treated diabetic patients with a blood glucose level in line with the guidelines (HbA1c < 7%))
Treated dyslipidaemia patients with a lipid level in line with the guidelines (LDL-cholesterol < 1 g/l)
Obese or overweight patients with a BMI that has returned to the guideline value (BMI < 25 kg/m)
Treated hypertension patients with a blood pressure in line with the guidelines (SBP < 140 mm Hg and DBP < 90 mm Hg and SBP < 135 mm Hg and DBP < 85 mm Hg with self-monitoring)
Active patients who have gone back to work
Patients with cardiovascular complications (recurrence, stroke, heart failure, arrhythmia)
Unscheduled readmissions
Post-infarction mortality rate (risk-adjusted) at 1 year
Indicators of access in the first year post-infarction
Number of patients
followed up at 1 year
%
Calls to the emergency medical assistance as a first step in the event of a
recurrence
Patients undergoing cardiovascular rehabilitation programmes
Patients undergoing therapeutic education programmes
Patients attending a smoking cessation clinic (in the case of smokers)
Patients attending a diabetes clinic, in the case of dysglycaemia patients
Patients seeking dietary advice
Patients consulting a cardiologist
The result indicators and the indicators of access to specialised programmes complement clinical practice indicators (CPIs). Some have been chosen as CPIs (reperfusion rates and waiting times, number of calls to the emergency medical assistance as a first step, number of patients undergoing cardiovascular rehabilitation, 30-day mortality) but not all CPIs are result indicators. The result indicators and indicators of access to specialised programmes should be interpreted in the context of the patient, of professional practices and of the environment (geographical situation/constraints, human resources and equipment).

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 60/85
1.2 Proposals for memos 1.2.1 Optimal care pathway for the treatment of a suspected ACS
1.2.2 Suspected ACS in an outpatient setting
Suspected ACShistory taking, clinical examination
Transmisson on arrival of SMUR
Treatment of a suspected ACS in outpatients
CALL TO SAMU Emergency call centre 15
112
+/- aspirin (150 to 325 mg)
+/- 12- or 18-lead ECG
1
HAUTE AUTORITÉ DE SANTÉ2012
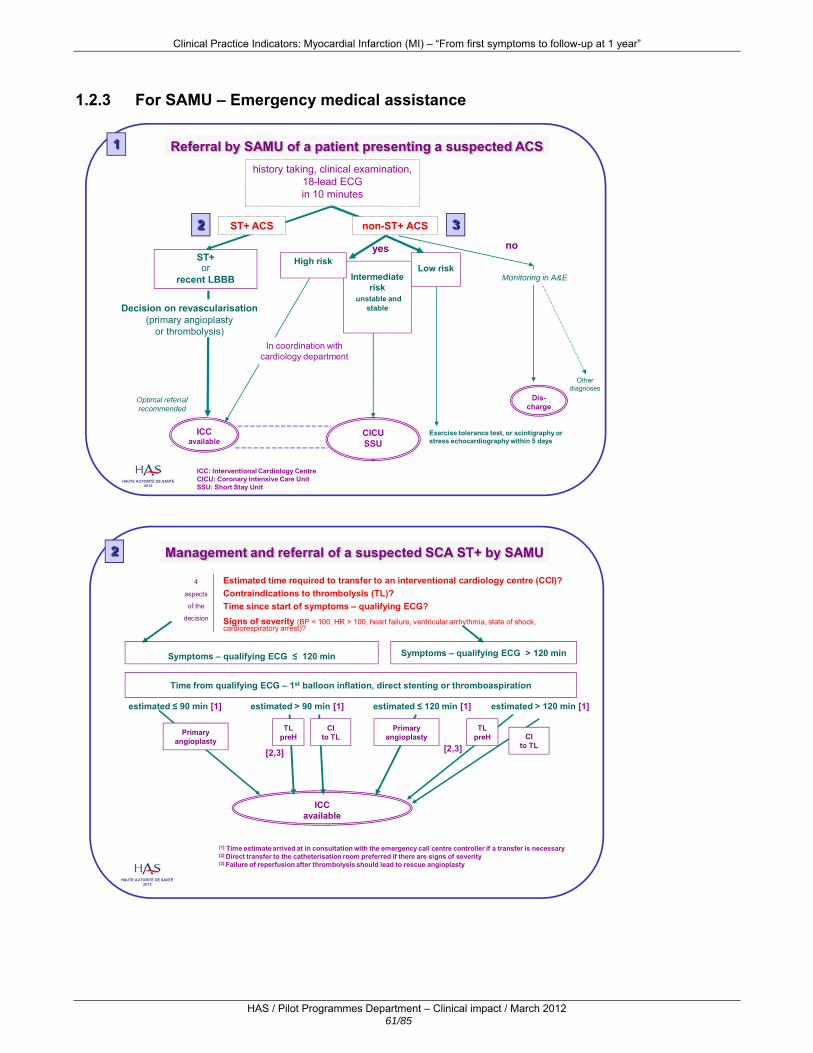
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 61/85
1.2.3 For SAMU – Emergency medical assistance
ST+or
recent LBBB
history taking, clinical examination,18-lead ECGin 10 minutes
ST+ ACS
Referral by SAMU of a patient presenting a suspected ACS
yes
non-ST+ ACS
ICCavailable
Intermediate risk
unstable and stable
CICUSSU
Optimal referral recommended
1
2 3
High riskLow risk
Exercise tolerance test, or scintigraphy or stress echocardiography within 5 days
Dis-charge
Monitoring in A&E
Otherdiagnoses
no
Decision on revascularisation(primary angioplasty
or thrombolysis)
ICC: Interventional Cardiology CentreCICU: Coronary Intensive Care UnitSSU: Short Stay Unit
In coordination with cardiology department
HAUTE AUTORITÉ DE SANTÉ2012
ICC available
TLpreH
Management and referral of a suspected SCA ST+ by SAMU
Estimated time required to transfer to an interventional cardiology centre (CCI)?Contraindications to thrombolysis (TL)?Time since start of symptoms – qualifying ECG?Signs of severity (BP < 100, HR > 100, heart failure, ventricular arrhythmia, state of shock, cardiorespiratory arrest)?
4
aspects
of the
decision
2
Time from qualifying ECG – 1st balloon inflation, direct stenting or thromboaspiration
Symptoms – qualifying ECG ≤ 120 min Symptoms – qualifying ECG > 120 min
estimated ≤ 90 min [1] estimated > 90 min [1]
TL preH
CI to TL
estimated ≤ 120 min [1] estimated > 120 min [1]
CI to TL
[2,3]
Primary angioplasty
Primary angioplasty
[1] Time estimate arrived at in consultation with the emergency call centre controller if a transfer is necessary[2] Direct transfer to the catheterisation room preferred if there are signs of severity[3] Failure of reperfusion after thrombolysis should lead to rescue angioplasty
[2,3]
HAUTE AUTORITÉ DE SANTÉ2012

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 62/85
1.2.4 For SAMU and A&E
Management and referral of a suspected non-ST+ ACS
ICC
Marker(s) for acute risk and/or abnormal ECG
Patients at high risk
• Refractory angina• Recurrent ischaemia (angina and 2-mm ST segment depression or T-wave inversion)• Left ventricular failure or state of shock• Ventricular arrhythmia
Unstable patientsat intermediate risk
• GRACE score > 140 and/or
• Elevated troponin (standard threshold defined according to the type of troponin)• Dynamic modification of the ST segment orT wave
Aspirin + Clopidogrel or other recommended antiaggregant + antithrombotic +/- anti-GPIIbIIIa (elevated troponin)
Stable patientsat intermediate risk
• Diabetes• Renal failure• LVEF < 40• MI or recent angioplasty• History of bypass surgery• Intermediate to high GRACE score
rare situation ≤ 5 %
within 24 hours
3
CICUSSU
Immediate transfer
within 72 hours
Low-risk patients•GRACE score < 140 and/or
• Normal troponin• No recurrent ischaemia• Stable haemodynamics• Normal ECG
Exercise stress test or scintigraphy or stress
echoradiographywithin 5 days
Absence of marker(s) for acute risk and/or normal ECG
CardiologyAspirin
Analgesia according to
VAS/NSAND
THE FRENCH NATIONAL MI TASK FORCE2012
Indications and contraindications for thrombolysis
Indications
•Prolonged precordial pain
for more than 30 min but less than 12 hoursresistant to nitrate derivatives
•Combined with typical electrocardiographic modifications:
ST segment elevation ≥ 1 mm in at least 2 standard leads, or
ST ≥ 2 mm in at least 2 contiguous precordial leads, or
recent left bundle branch block
ContraindicationsKnown haemorrhagic diathesis (coagulopathy)History of stroke, or severe injury to the central nervous system (aneurism, brain surgery)Recent severe trauma (less than 10 days): operation, childbirth, head injury, fracture, etc.Prolonged resuscitation Recent puncture of a noncompressible or intramuscular vesselSevere hypertension not controlled by any treatmentRecent bacterial endocarditis, pericarditis, aortic dissectionAcute pancreatitisGastric ulcers with recent or still very symptomatic bleedingSevere neoplasia increasing the risk of bleedingSevere liver diseaseLong-term anticoagulant treatment with anti-vitamin KSevere or potentially dangerous bleeding, whether manifest or recent
4
HAUTE AUTORITÉ DE SANTÉ2012

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 63/85
1.2.5 For the Emergency Services - A&E
ST+or
recent LBBB
ACS ST+
Referral by A&E of a patient with suspected ACS
yes
Non-ST+ ACS
ICCavailable
Stable and unstable
intermediate risk
CICUSSU
1
2 3
High riskLowrisk
Exercise stress test or scintigraphy or stress echoradiography within 5 days
Discharge
Monitoring in A&E
Other diagnoses
no
Decision on revascularisation(primary angioplasty or
thrombolysis)
In coordination with the cardiology department
Patient history, clinical examination
12/18-lead ECG to be performed within 10 minutes Triage nurse
Read immediately by a senior doctor
HAUTE AUTORITÉ DE SANTÉ2012
ICC available
TL
Management and referral of a suspected ACS ST+ to A&E
Estimated time required to transfer to an interventional cardiology centre (ICC)?Contraindications to thrombolysis (TL)?Time since start of symptoms - qualifying ECG?Signs of severity (BP < 100, HR > 100, heart failure, ventricular arrhythmia, state of shock, cardiorespiratory arrest)?
4
aspects
of the
decision
2
Time from qualifying ECG – 1st balloon inflation, direct stenting or thromboaspiration
Symptoms – qualifying ECG ≤ 120 min Symptoms – qualifying ECG > 120 min
estimated ≤ 90 min [1] estimated > 90 min [1]
TL CI to TL
estimated ≤ 120 min [1] estimated > 120 min [1]
CI to TL
[2,3]
Primary angioplasty
Primary angioplasty
[1] Time estimate arrived at in consultation with the emergency call centre controller if a transfer is necessary[2] Direct transfer to the catheterisation room preferred if there are any signs of severity[3] Failure of reperfusion after thrombolysis should lead to rescue angioplasty
[2,3]
HAUTE AUTORITÉ DE SANTÉ2012
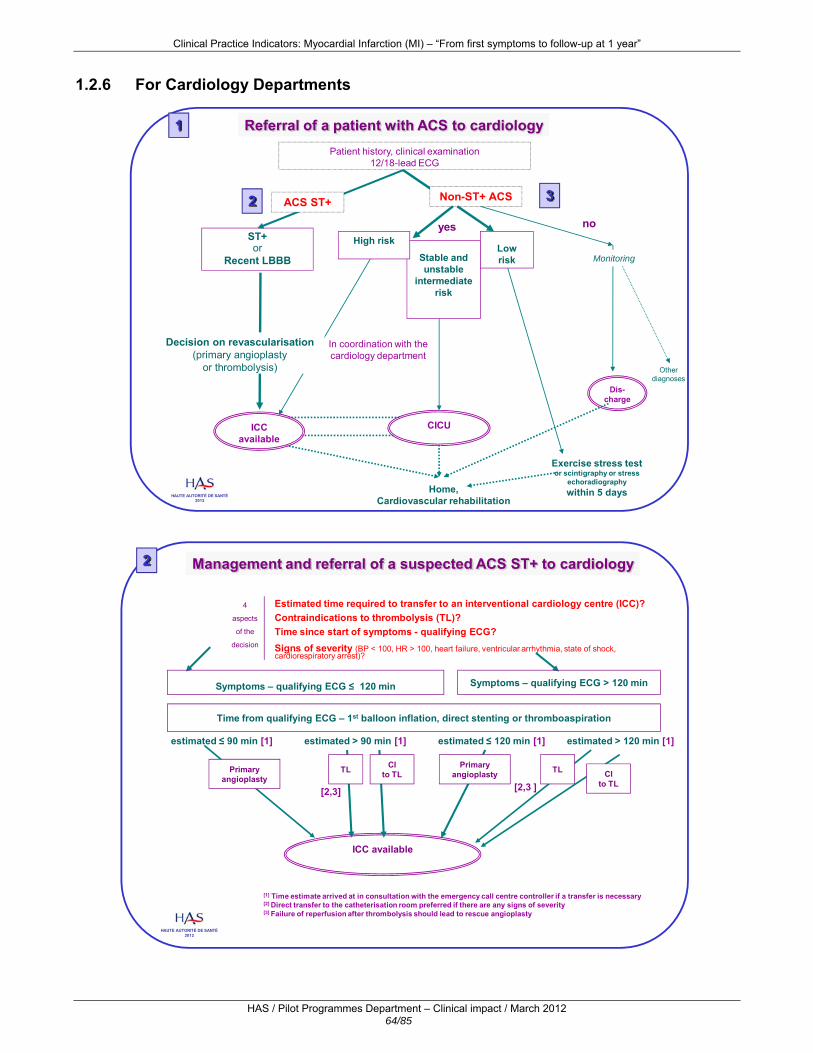
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 64/85
1.2.6 For Cardiology Departments
ST+or
Recent LBBB
ACS ST+
Referral of a patient with ACS to cardiology
yes
Non-ST+ ACS
Stable and unstable
intermediate risk
CICU
1
2 3
High riskLowrisk
Exercise stress test or scintigraphy or stress
echoradiographywithin 5 days
Dis-charge
Monitoring
Otherdiagnoses
no
Decision on revascularisation(primary angioplasty
or thrombolysis)
In coordination with the cardiology department
Patient history, clinical examination12/18-lead ECG
Home, Cardiovascular rehabilitation
ICCavailable
HAUTE AUTORITÉ DE SANTÉ2012
ICC available
TL
Management and referral of a suspected ACS ST+ to cardiology
Estimated time required to transfer to an interventional cardiology centre (ICC)?Contraindications to thrombolysis (TL)?Time since start of symptoms - qualifying ECG?Signs of severity (BP < 100, HR > 100, heart failure, ventricular arrhythmia, state of shock, cardiorespiratory arrest)?
4
aspects
of the
decision
2
Time from qualifying ECG – 1st balloon inflation, direct stenting or thromboaspiration
Symptoms – qualifying ECG ≤ 120 min Symptoms – qualifying ECG > 120 min
estimated ≤ 90 min [1] estimated > 90 min [1]
TL CI to TL
estimated ≤ 120 min [1] estimated > 120 min [1]
CI to TL
[2,3]
Primary angioplasty
Primary angioplasty
[1] Time estimate arrived at in consultation with the emergency call centre controller if a transfer is necessary[2] Direct transfer to the catheterisation room preferred if there are any signs of severity[3] Failure of reperfusion after thrombolysis should lead to rescue angioplasty
[2,3 ]
HAUTE AUTORITÉ DE SANTÉ2012

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 65/85
Management and referral of a suspected non-ST+ ACS to cardiology
ICC
Marker(s) for acute risk and/or abnormal ECG
Patients at high risk
• Refractory angina• Recurrent ischaemia (angina and 2-mm ST depression or inverse T-wave)• Left ventricular failure or state of shock• Ventricular arrhythmia
Unstable patientsat intermediate risk
•GRACE score > 140 and/or
• Elevated troponin (standard threshold defined according to the type of troponin)• Dynamic modification of the ST segment orT-wave
Aspirin + Clopidogrel or other recommended antiaggregant + antithrombotic +/- anti-GPIIbIIIa (elevated troponin)
Stable patientsat intermediate risk
• Diabetes• Renal failure• LVEF < 40• MI or recent angioplasty• History of bypass surgery• Intermediate to high GRACE score
rare situation ≤ 5 %
within 24 hours
CICUImmediate transfer
within 72 hours
Low-risk patients• GRACE score < 140 and/or
• Normal troponin• No recurrent ischaemia• Haemodynamically stable• Normal ECG DischargeOther diagnosis
Exercise stress test within 5 daysor scintigraphy or stress echoradiography
(as outpatient or as inpatient)
Assessment continued in cardiology
AspirinAnalgesiaaccordingto VAS/NS
Absence of marker(s) for acute risk and/or normal ECG
3
AND THE FRENCH NATIONAL MI TASK FORCE
2012
Significant coronary lesions> 50%
Non-significant coronary lesions
Coronary arteries angiographically normal
Surgery5%
Angioplasty45%
ACS confirmed ACS uncertain
Appropriate ASA
Anti-ischaemic drug treatmentBASIC: BB, ASA, Statin, CEI, and another appropriate AA [3]
Prevention and treatment of risk factors
Revascularisation not indicated
50%
Management based on coronary angiography 4
[1] lesions not justifying or not lending themselves to revascularisation, neither by surgery nor by angioplasty[2] virtually all angioplasties being done including placement of stents[3] the aggregation inhibitors currently used in combination with aspirin are: clopidogrel/prasugrel/ticagrelor
[1] [2]
HAUTE AUTORITÉ DE SANTÉ2012
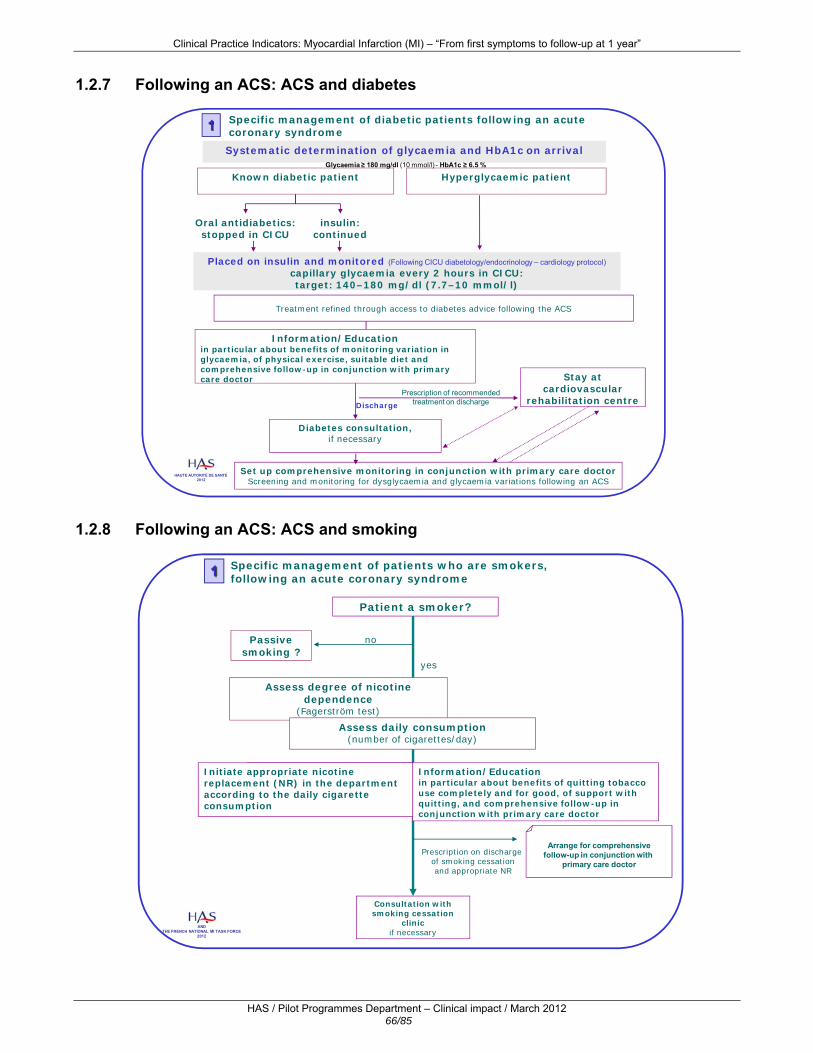
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 66/85
1.2.7 Following an ACS: ACS and diabetes
Systematic determination of glycaemia and HbA1c on arrival
Specific management of diabetic patients following an acute coronary syndrome
Placed on insulin and monitored (Following CICU diabetology/endocrinology – cardiology protocol)capillary glycaemia every 2 hours in CICU: target: 140–180 mg/dl (7.7–10 mmol/l)
Stay atcardiovascular
rehabilitation centre
Known diabetic patient Hyperglycaemic patient
Oral antidiabetics: stopped in CICU
insulin: continued
Diabetes consultation, if necessary
Discharge
Treatment refined through access to diabetes advice following the ACS
Glycaemia ≥ 180 mg/dl (10 mmol/l) - HbA1c ≥ 6.5 %
Information/Educationin particular about benefits of monitoring variation in glycaemia, of physical exercise, suitable diet and comprehensive follow-up in conjunction with primary care doctor
Prescription of recommendedtreatment on discharge
Set up comprehensive monitoring in conjunction with primary care doctorScreening and monitoring for dysglycaemia and glycaemia variations following an ACS
1
HAUTE AUTORITÉ DE SANTÉ2012
1.2.8 Following an ACS: ACS and smoking
Patient a smoker?
Specific management of patients who are smokers, following an acute coronary syndrome
Initiation de la substitution nicotinique dans le service
si nécessaire
no
yes
Consultation with smoking cessation
clinicif necessary
Arrange for comprehensivefollow-up in conjunction with
primary care doctorPrescription on discharge
of smoking cessationand appropriate NR
Assess degree of nicotine dependence
(Fagerström test)
Passive smoking ?
1
Assess daily consumption(number of cigarettes/day)
Information/Education in particular about benefits of quitting tobacco use completely and for good, of support with quitting, and comprehensive follow-up in conjunction with primary care doctor
Initiate appropriate nicotine replacement (NR) in the department according to the daily cigarette consumption
AND THE FRENCH NATIONAL MI TASK FORCE
2012

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 67/85
Appendix 2 – Literature search The updating of the literature search on the topic of myocardial infarction concentrated on the subjects10 and types of studies11 defined in agreement with the project manager and was limited to French and English-language publications for the period from 2009 to December 2011. Other works published between 1999 and 2009 were included in this update because they were specific to the context of the French care system and/or corresponded to reference studies. The following sources were searched:
for international literature: the Medline database and the Cochrane Library; for guidelines and indicators: websites publishing guidelines, the websites of learned societies
relevant to the area of research and sources specialising in indicators.
Bibliographical databases The strategy for searching bibliographic databases is formulated using, for each subject, either terms from a thesaurus (keywords) or free terms (from the title or summary). They are combined with the terms describing the types of studies. Table 1 presents the strategy used to search the Medline database. Table 1: Strategy for searching the Medline database Terms used
Period Number of references
01/2009 – 12/2011 474 Stage 1 (acute coronary syndrome OR myocardial infarction OR myocardial ischemia OR ((secondary
prevention OR risk factors) AND cardiovascular diseases))/de OR (acute coronary syndrome* OR myocardial infarct *)/ti
AND Stage 2 (guideline AND implementation))/ti,ab OR (program evaluation OR quality of health care OR
outcome and process assessment (health care) OR outcome assessment (health care) OR process assessment (health care) OR guideline adherence OR peer review, health care OR quality indicators, health care OR health care evaluation mechanisms OR utilization review OR clinical audit OR medical audit OR nursing audit OR quality assurance, health care OR total quality management OR reference standards OR health care quality, access, and evaluation OR benchmarking OR united states agency for healthcare research and quality OR management quality circles OR quality control OR accreditation OR registries)/de OR (quality OR pay-for-performance OR (indicator* AND (clinical* OR quality OR performance)) OR audit criteria OR core measure* OR program OR registry OR registries)/ti OR (quality improve*)/ti,ab
de: descriptor; ti: title; ab: abstract In all, 176 publications were included in this document:
8 methodological references, 60 guidelines and other works produced by institutions, health agencies or professional organisations, 49 references to indicators, 58 other types of publications.
10 Acute coronary syndrome, myocardial infarction, secondary prevention and risk factors in cardiovascular diseases. 11 Guidelines, professional consensus documents, good practice guides, chronic cindition guides, institutional reports and opinions, performance indicators, other types of health quality indicators and audit criteria, systematic reviews, meta-analyses, studies demonstrating the clinical impact of introducing good practice and/or programmes for controlling risk factors, including studies adapted to the French context, practice tools (questionnaires, scores, etc.).

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 68/85
Websites consulted Agence française de sécurité sanitaire des produits de santé – AFSSAPS Association de langue française pour l'étude du diabète et des maladies métaboliques – ALFEDIAM Bibliothèque interuniversitaire santé [Inter-university health library] – BIUS Bibliothèque médicale Lemanissier [Lemanissier medical library] Direction de la recherche, des études, de l’évaluation et des statistiques – DREES Evaluation des technologies de santé pour l'aide à la décision [Evaluation of health technologies as an aid to decision-making] – ETSAD Expertise collective INSERM [INSERM Collective Expert Opinion] Haut conseil de la santé publique – HCSP Institut de recherche et documentation en économie de la santé - IRDES Institut de veille sanitaire – INVS Institut national de prévention et d'éducation pour la santé – INPES Ministère du travail, de l’emploi et de la santé [Ministry of labour, employment and health] Mission nationale d’expertise et d’audit hospitaliers [National mission for expertise and hospital auditing] – MeaH Projet COMPAQH [Coordination pour la Mesure de la Performance et l’Amélioration de la Qualité Hospitalière – COMPAQH project Coordination for measuring performance and improving quality in hospitals] Société française d’anesthésie et de réanimation – SFAR Société Française de Cardiologie. Référentiel des bonnes pratiques cliniques en réadaptation cardiologique GERS-SFC, 2011 [French Cardiology Society. Guidelines for good clinical practice in cardiological rehabilitation] – GERS-SFC, 2011 Société française de gériatrie et gérontologie – SFGG Société française de médecine générale [French General Medical Society] – SFMG Adelaide Health Technology Assessment – AHTA Agency for Healthcare Research and Quality - AHRQ Alberta Heritage Foundation for Medical Research – AHFMR Alberta Medical Association – AMA American College of Cardiology – ACC American College of Physicians – ACP American Heart Association – AHA Australian Council on Healthcare Standards – ACHS Australian Institute of Health and Welfare – AIHW Blue Cross Blue Shield Association – BCBS California Technology Assessment Forum – CTAF Canadian Agency for Drugs and Technologies in Health – CADTH Canadian Task Force on Preventive Health Care – CTFPHC Centers for Disease Control and Prevention - CDC Centre fédéral d'expertise des soins de santé [Belgian Health Care Knowledge Centre] – KCE Centre for Clinical Effectiveness – CCE Centre for Reviews and Dissemination databases Clinical Evidence
Clinical Knowledge Summaries Clinical Resource and Audit Group CMA Infobase Cochrane Library College of Physicians and Surgeons of Alberta - CPSA Department of Health - DH European Medicines Agency – EMEA European Society of Cardiology – ESC Euroscan Food and Drug Administration – FDA Guideline Advisory Committee – GAC Guidelines and Protocols Advisory Committee – GPAC Guidelines Finder Guidelines International Network – GIN Heart Foundation Horizon Scanning Institut national d'excellence en santé et en services sociaux [National Institute for Excellence in Health and Social Services] – INESSS Institute for Clinical Evaluative Sciences – ICES Institute for Clinical Systems Improvement – ICSI Institute for Health Economics Alberta – IHE Institute for Healthcare Improvement – IHI International Quality Indicators Project – IQIP Intute Health & Life Sciences – INTUTE Joint Commission on Accreditation of Healthcare Organizations Maine health management coalition Medical Services Advisory Committee – MSAC National Committee for Quality Assurance – NCQA National Coordinating Centre for Health Technology Assessment – NCCHTA National Guideline Clearinghouse – NGC National Health and Medical Research Council – NHMRC National Health Service Information Centre National Health Service – NHS National Health Service Scotland National Horizon Scanning Centre – NHSC National Institute for Health and Clinical Excellence – NICE National Institutes of Health – NIH National Quality Measures Clearinghouse New Zealand Guidelines Group – NZGG New Zealand Health Technology Assessment – NZHTA Ontario Health Technology Advisory Committee – OHTAC Organisation for Economic Co-operation and Development – OECD QI Project Royal College of Physicians – RCP Health Canada Scottish Intercollegiate Guidelines Network – SIGN Singapore Ministry of Health The Clinical Indicators Support Team (NHS Scotland) Tripdatabase U.S. Preventive Services Task Force – USPSTF Veterans affairs, Dep. of Defense Clinical practice guidelines West Midlands Health Technology Assessment Collaboration – WMHTA Wisconsin Hospital Association World Health Organisation

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 69/85
Literature monitoring The abstracts from the following journals have been examined throughout the project:
- Archives of Cardiovascular Diseases, - British Medical Journal, - Chest, - Circulation, - European Heart Journal, - Journal of the American College of Cardiology, - Journal of the American Medical Association, - New England Journal of Medicine, - The Lancet.
In addition, Medline and the websites listed above were monitored until December 2011.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 70/85
Appendix 3. Bibliographic references
3.1 HAS methodological references (1-8) 1. Haute Autorité de Santé. HAS Collaboratives: A participatory method for improving professional practice.
2010 http://www.has-sante.fr/portail/upload/docs/application/pdf/2012-02/4_pages_collaboratives_eng_vf.pdf
2. Haute Autorité de Santé. Together, let us improve the quality in health care. Clinical Practice Indicators –
Efficacy Safety Access (Myocardial Infarction care pathway) 2009. http://www.has-sante.fr/portail/upload/docs/application/pdf/2011-03/english_ipc_vf.pdf
3. Haute Autorité de Santé, BMJ Group. Clinical impact of quality improvements, 19th April 2010, Nice, France.
Qual Safe Health Care 2010;19(3 Suppl 1).
4. Godlee F, Cabarrot P, Desplanques A, Smith J, Degos L. Foreword. Qual Safe Health Care 2010;19(1 Suppl 1):A1-A2.
5. Haute Autorité de Santé. Programmes d'amélioration des pratiques (PAP). Démarche générale d'élaboration
[Programme for the improvement of practices. General approach to development]. Saint-Denis La Plaine: HAS; 2008. http://www.has-sante.fr/portail/upload/docs/application/pdf/2008-07/pap-_upp_23-06-08.pdf
6. Haute Autorité de Santé. Registres, observatoires, bases de données et évaluation des pratiques
professionnelles [Registries, observational studies, databases and evaluation of professional practices]. Saint-Denis La Plaine: HAS; 2008. http://www.has-sante.fr/portail/jcms/c_667910/registres-observatoires-bases-de-donnees-et-epp-4-pages
7. Haute Autorité de Santé. Critères de qualité pour l'évaluation et l'amélioration des pratiques. Une interface
entre les recommandations et les démarches d'amélioration de la qualité [Quality criteria for the evaluation and improvement of practices. An interface between guidelines and approaches to quality improvement]. Saint-Denis La Plaine: HAS; 2007. http://www.has-sante.fr/portail/upload/docs/application/pdf/criteres_de_qualite_pour_levaluation_et_lamelioration_de_des_pratiques_professionnelles_-_synthese.pdf
8. Agence nationale d'accréditation et d’évaluation en santé. Évaluation d'un programme d'amélioration de la
qualité: Les enseignements de 60 projets dans les établissements de santé français [French national agency for health accreditation and evaluation. Evaluation of a quality improvement programme. Lessons learned from 60 projects in French healthcare establishments]. Paris: ANAES; 1999.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 71/85
3.2 Guidelines and other institutional studies and studies by healthcare agencies or professional organisations on “Myocardial infarction and secondary prevention” (9-67)
List of guidelines
Acronym Body Title of guidelines Year Document URL
9. ACCFTF/ AHA
American College of Cardiology Foundation Task Force / American Heart Association
Expert Consensus Document on Hypertension in the Elderly
2011 http://circ.ahajournals.org/content/123/21/2434.full.pdf+html?sid=3ca8c567-8c2c-4035-9997-d837b6055a4f
10. ACCF/AHA American College of Cardiology Foundation / American Heart Association
Secondary Prevention and Risk Reduction Therapy for Patients With Coronary and Other Atherosclerotic Vascular Disease: 2011 Update
2011 http://circ.ahajournals.org/content/124/22/2458.full.pdf+html
11. ACCF/AHA/ SCAI
American College of Cardiology Foundation / American Heart Association / Society for Cardiovascular Angiography and Interventions
Guideline for Percutaneous Coronary Intervention
2011 http://circ.ahajournals.org/content/early/2011/11/07/CIR.0b013e31823ba622.full.pdf+html
12. ADLF Association des diététiciens de langue française
Quick reference guide Dietary consultation with a dietician
2011 http://www.has-sante.fr/portail/upload/docs/application/pdf/dietary_consultation_-_quick_reference_guide_.pdf
13. AHA American Heart Association The American Heart Association's Recommendations for Expanding the Applications of Existing and Future Clinical Registries
2011 http://circ.ahajournals.org/content/123/19/2167.full.pdf+html
AFSSAPS Agence Française de Sécurité Sanitaire des Produits de Santé
Groupe de travail «antiagrégants plaquettaires» du comité de validation des recommandations de bonne pratique sur les produits de santé
2011 Mise en place en novembre 2011
14. ESC/EAS European Society of Cardiology, European Atherosclerosis Society
Guidelines for the Management of Dyslipidaemias
2011 http://www.escardio.org/guidelines-surveys/esc-guidelines/Pages/Dyslipidemias.aspx
15. HAS Haute Autorité de santé Quick reference guide Overweight and obesity in adults: first-line medical management
2011 http://www.has-sante.fr/portail/upload/docs/application/pdf/2012-10/overweight_and_obesity_in_adults_first_line_medical_management_version_anglaise.pdf
16. ICSI Institute for Clinical Systems Improvement
Stable Coronary Artery Disease 2011 http://www.icsi.org/coronary_artery_disease/coronary_artery_disease__stable_.html
17. ICSI Institute for Clinical Systems Improvement
Diagnosis and Treatment of Chest Pain and Acute Coronary Syndrome (ACS)
2011 http://www.icsi.org/acs_acute_coronary_syndrome/acute_coronary_syndrome_and_chest_pain__diagnosis_and_treatment_of_2.html
18. ICSI Institute for Clinical Systems Improvement
Antithrombotic Therapy Supplement
2011 http://www.icsi.org/antithrombotic_therapy_supplement__guideline__14045/antithrombotic_therapy_supplement__guideline_.html
19. NICE National Institute for Health and Clinical Excellence
Stable angina CG 126
2011 http://guidance.nice.org.uk/CG126
20. NICE National Institute for Health and Clinical Excellence
Hyperglycaemia in acute coronary syndromes CG 130
2011 http://www.nice.org.uk/nicemedia/live/13589/56817/56817.pdf

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 72/85
Acronym Body Title of guidelines Year Document URL
21. NICE National Institute for Health and Clinical Excellence
Ticagrelor for the treatment of acute coronary syndrome CG 236
2011 http://www.nice.org.uk/nicemedia/live/13588/56819/56819.pdf
22. SFC Société Française de Cardiologie
Référentiel des bonnes pratiques cliniques en réadaptation cardiologique GERS-SFC, 2011
2011 http://www.cardio-sfc.org/groupes/groupes/exercice-readaptation-sport/recommandations-readaptation/readaptation/sommaire/files/reco_referentiel_long.pdf/attachment_download/attachedFile
23. SFD/SFC Vergès B, Avignon A, Bonnet F, Catargi B, Cattan S, Cosson E, Ducrocq G, Elbaz M, Fredenrich A, Gourdy P, Henry P, Lairez O, Leguerrier AM, Monpère C, Moulin P, Vergès-Patois B, Roussel R, Steg G, Valensi P; Diabetes and Cardiovascular Disease study group of the Société francophone du diabète (SFD), in collaboration with the Société française de cardiologie (SFC).
Consensus statement on the care of the hyperglycaemic/diabetic patient during and in the immediate follow-up of acute coronary syndrome.
2011 Diabetes Metab. 2011 Dec 30. [Epub ahead of print] doi : 10.1016/j.diabet.2011.11.003
24. WHO World Health Organisation Use of glycated haemoglobin (HbA1c) in the diagnosis of diabetes mellitus
2011 http://www.who.int/diabetes/publications/report-hba1c_2011.pdf
25. ADA American Diabetes Association Executive Summary: Standards of Medical Care in Diabetes—2010
2010 http://care.diabetesjournals.org/content/33/Supplement_1/S4.full.pdf+html
26. ESC/EACTS European Society of Cardiology / European Association for Cardio-Thoracic Surgery
Guidelines on myocardial revascularization
2010 http://www.escardio.org/guidelines-surveys/esc-guidelines/GuidelinesDocuments/guidelines-revasc-FT.pdf
27. ESH European Society of Hypertension
ESH update of previous guideline 2010 http://www.ncbi.nlm.nih.gov/pubmed/20150842 Fagard R. Pol Arch Med Wewn. 2010;120(1-2):31-5.
28. NICE National Institute for Health and Clinical Excellence
Chest pain of recent onset: Assessment and diagnosis of recent onset chest pain or discomfort of suspected cardiac origin CG 95
2010 http://www.nice.org.uk/nicemedia/live/12947/47938/47938.pdf
29. OHTAC Ontario Health Technology Advisory Committee
Primary Angioplasty and Thrombolysis for the Treatment of Acute ST-Segment Elevated Myocardial Infarction - OHTAC Recommendation
2010 http://www.health.gov.on.ca/english/providers/program/ohtac/tech/recommend/rec_primary_angio_20100830.pdf
30. SFAR/SFMU Société française d’anesthésie et de réanimation / Société française de médecine d’urgence
Sédation et analgésie en structure d’urgence. Sedation and analgesia in emergency structure. (Réactualisation de la Conférence d’experts de la Sfar de 1999)
2010 http://www.sfar.org/_docs/articles/RFESdationAFARcorrig.pdf
31. ACC/AHA American College of Cardiology / American Heart Association
2009 Focused Updates: ACC/AHA Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction (Updating the 2004 Guideline and 2007 Focused Update) and ACC/AHA/SCAI Guidelines on Percutaneous Coronary Intervention (Updating the 2005 Guideline and 2007 Focused Update).
2009 http://circ.ahajournals.org/cgi/reprint/CIRCULATIONAHA.109.192663

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 73/85
Acronym Body Title of guidelines Year Document URL
32. Canadian Hypertension Education Program
The 2009 Canadian Hypertension Education Program recommendations for the management of hypertension: Part 1 – blood pressure measurement, diagnosis and assessment of risk
2009 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2707176/pdf/cjc25279.pdf
33. Canadian Hypertension Education Program
The 2009 Canadian Hypertension Education Program recommendations for the management of hypertension: Part 2--therapy.
2009 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2707169/pdf/cjc25287.pdf
34. HCSP Haut Conseil de santé publique Analyse des recommandations en matière de consommation d'alcool
2009 http://www.hcsp.fr/docspdf/avisrapports/hcspn20090701_alcool.pdf
35. NICE National Institute for Health and Clinical Excellence
Prasugrel for the treatment of acute coronary syndromes with percutaneous coronary intervention TA 182
2009 http://www.nice.org.uk/nicemedia/live/12324/45849/45849.pdf
36. US Public Health Service
US. Department of Health and Human Services. Public Health Service.
Clinical Practice Guideline Treating Tobacco Use and Dependence: 2008 Update
2008 http://www.surgeongeneral.gov/tobacco/treating_tobacco_use08.pdf.
37. ESC European Society of Cardiology
Management of acute Myocardial Infarction in patients presenting with ST-segment elevation
2008 http://www.escardio.org/guidelines-surveys/esc-guidelines/GuidelinesDocuments/guidelines-AMI-FT.pdf
38. SFC/FGG Société Française de Cardiologie - French Society of Cardiology / Société Française de Gériatrie et Gérontologie -French Society of Gerontology and Geriatrics
Consensus of the French Society of Gerontology and Geriatrics and the French Society of Cardiology for the management of coronary artery disease in older adults
2008 O. Hanon et al. Consensus of the French Society of Gerontology and Geriatrics and the French Society of Cardiology for the management of coronary artery disease in older adults. Archives of Cardiovascular Disease (2009) 102, 829—845
39. AHA/ ACCVPR
American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation
Core Components of Cardiac Rehabilitation/Secondary Prevention Programs: 2007 Update
2007 http://circ.ahajournals.org/cgi/reprint/115/20/2675
40. HAS/SFC/ SFMU
Haute Autorité de Santé / Société française de cardiologie / Société française de médecine d’urgence
Conférence de consensus [Consensus conference] Prise en charge de l'infarctus du myocarde à la phase aiguë en dehors des services de cardiologie.
2007 http://www.has-sante.fr/portail/jcms/c_484720/prise-en-charge-de-l-infarctus-du-myocarde-a-la-phase-aigue-en-dehors-des-services-de-cardiologie?xtmc=infarctus&xtcr=1
41. NICE National Institute for Health and Clinical Excellence
Secondary prevention in primary and secondary care for patients following a myocardial infarction CG48
2007 http://www.nice.org.uk/nicemedia/pdf/CG48NICEGuidance.pdf
42. WHO World Health Organization Prevention of Cardiovascular Disease, Pocket Guidelines for Assessment and Management of Cardiovascular Risk
2007 http://www.who.int/cardiovascular_diseases/guidelines/PocketGL.ENGLISH.AFR-D-E.rev1.pdf
43. AHA American Heart Association Recommendation to Develop Strategies to Increase the Number of ST-Segment–Elevation Myocardial Infarction Patients With Timely Access to Primary Percutaneous Coronary Intervention
2006 http://circ.ahajournals.org/cgi/reprint/113/17/2152
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 74/85
Acronym Body Title of guidelines Year Document URL
44. AFSSAPS Agence française de sécurité sanitaire des produits de santé
Prise en charge thérapeutique des patients dyslipidémiques
2005 http://www.soc-nephrologie.org/PDF/enephro/recommandations/Afssaps/2005/dyslipemie_argu.pdf
45. AFSSAPS Agence Française de Sécurité Sanitaire des Produits de Santé
Les stratégies thérapeutiques médicamenteuses et non médicamenteuses de l’aide à l’arrêt du tabac. Recommandations de bonne pratique.
2003 http://www.tabac-info-service.fr/data/pdf/tabarg.pdf
46. WHO World Health Organization World Health Organization. Adherence to long-term therapies. Evidence for action. Geneva:
2003 http://www.who.int/chp/knowledge/publications/adherence_full_report.pdf
List of other studies by institutions, health agencies and professional organisations
Acronym Body Title of guidelines Year Document URL
47. AHA American Heart Association The Importance of Population-Wide Sodium Reduction as a Means to Prevent Cardiovascular Disease and Stroke: A Call to Action From the American Heart Association
2011 http://www.medpagetoday.com/upload/2011/1/13/CIR.0b013e31820d0793v1.pdf
48. BMJ CE BMJ Clinical Evidence Systematic review Secondary prevention of ischaemic cardiac events
2011 http://clinicalevidence.bmj.com/ceweb/conditions/cvd/0206/0206-get.pdf
49. BMJ CE BMJ Clinical Evidence Systematic review Myocardial infarction (ST-elevation)
2011 http://clinicalevidence.bmj.com/ceweb/conditions/cvd/0202/0202-get.pdf
50. EMA European Medicines Agency Press release. European Medicines Agency confirms positive benefit/risk balance for Champix. Benefits as a smoking-cessation medicine outweigh slight reported cardiovascular events. July 2011
2011 http://www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2011/07/news_detail_001314.jsp&mid=WC0b01ac058004d5c1&jsenabled=true
51. HAS Haute Autorité de santé Leaflet on good practice in healthcare technology use Self-monitoring of blood glucose in type 2 diabetes: limited use for a target population
2011 http://www.has-sante.fr/portail/upload/docs/application/pdf/2011-12/good_practice_-_self-monitoring_blood_glucose_type_2_diabetes.pdf
52. HAS Haute Autorité de santé Scoping report Développement de la prescription de thérapeutiques non médicamenteuses validées
2011 http://www.has-sante.fr/portail/upload/docs/application/pdf/2011-06/developpement_de_la_prescription_de_therapeutiques_non_medicamenteuses_rapport.pdf
53. HAS Haute Autorité de santé HAS Opinion. Commission de la transparence. (Brilique – Ticagrelor)
2011 http://www.has-sante.fr/portail/upload/docs/application/pdf/2012-01/brilique_07-12-2011_avis_ct10968.pdf
54. AFSSA Agence française de sécurité sanitaire des aliments French Food Safety Agency
AFSSA– Request no. 2006-SA-0359 Opinion of the French Food Safety Agency on the update of French population reference intakes (ANCs) for fatty acids
2010 http://www.anses.fr/Documents/NUT2006sa0359EN.pdf
55. Cochrane Systematic review Home-based versus centre-based cardiac rehabilitation.
2010 Taylor RS, Dalal H, Jolly K, Moxham T, Zawada A. Home-based versus centre-based cardiac rehabilitation. Cochrane Database Syst Rev 2010;Issue 1.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 75/85
Acronym Body Title of guidelines Year Document URL
56. ESHTF European Society of Hypertension Task Force
Reappraisal of the European guidelines on hypertension management: the European Society of Hypertension Task Force document: a short review
2009 http://www.ish.org.il/2009GuidelinesESH.pdf
57. HAS Haute Autorité de santé Medical/economic evaluation Efficacité et efficience des hypolipémiants : une analyse centrée sur les statines
2010 http://www.has-sante.fr/portail/upload/docs/application/pdf/2010-07/synthese_efficacite_et_efficience_des_hypolipemiants_-_une_analyse_centree_sur_les_statines.pdf
58. HAS Haute Autorité de Santé List of procedures and services Artériopathie Oblitérante des Membres Inférieurs
2010
http://www.has-sante.fr/portail/upload/docs/application/pdf/liste_actes_presta_aomi_ald3.pdf
59. HCSP Haut Conseil de santé publique
Avis relatif aux moyens nécessaires pour relancer la lutte contre le tabagisme [Opinion on the necessary resources for relaunching the anti-smoking campaisn]
2010 http://www.hcsp.fr/docspdf/avisrapports/hcspa20100922_luttetabagisme.pdf
60. HCSP Haut Conseil de santé publique
Analyse des recommandations en matière de consommation d'alcool [Analysis of the guidelines on alcohol consumption]
2009 http://www.hcsp.fr/docspdf/avisrapports/hcspn20090701_alcool.pdf
61. HAS Haute Autorité de Santé Guide for doctors. Long-term conditions. Coronary heart disease.
2007 http://www.has-sante.fr/portail/upload/docs/application/pdf/2008-06/gm_mcoronarienne_anglais_web.pdf
62. HAS Haute Autorité de Santé Guide for patients 13. Long-term conditions. Coronary heart disease.
2007 http://www.has-sante.fr/portail/upload/docs/application/pdf/2008-06/08-098_gp_maladie_corona.pdf
63. HAS Haute Autorité de Santé Guide for doctors 3. Artériopathie oblitérante des membres inférieurs [Peripheral artery occlusive disease]
2007 http://www.has-sante.fr/portail/upload/docs/application/pdf/ald3_aomi_guide_cardiovasc_post_corrlemire_revuenp28avril__205.pdf
64. HAS Haute Autorité de Santé Guide for patients 3. Long-term conditions La prise en charge de votre artérite des membres inférieurs [Managing your lower limb arteritis]
2007 http://www.has-sante.fr/portail/upload/docs/application/pdf/2008-06/08-098_gp_maladie_corona_2008-06-16_14-30-47_587.pdf
65. HAS Haute Autorité de Santé Patient leaflet. Lutte contre l'infarctus : nous sommes tous concernés. Les réponses à vos questions [Beating infarction: it affects all of us. Your questions answered].
2007 http://www.has-sante.fr/portail/upload/docs/application/pdf/infarctus_myocarde_patient.pdf
66. HAS Haute Autorité de Santé Quick reference guide. Dietary consultation with a dietician.
2006 http://www.has-sante.fr/portail/upload/docs/application/pdf/dietary_consultation_-_quick_reference_guide_.pdf
67. Ministère de la santé et des solidarités. Health and Solidarity Ministry
Second National Nutrition and Health Programme – 2006-2010 – Actions and measures
2006 http://www.sante.gouv.fr/IMG/pdf/pnns2.pdf
Literature monitoring on the theme of infarction and secondary prevention is at your disposal on the HAS website, Pilot Programmes section, area devoted to myocardial infarction: http://www.has-sante.fr/portail/jcms/c_736856/ensemble-ameliorons-la-prise-en-charge-de-linfarctus-du-myocarde-idm

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 76/85
3.3 “Myocardial infarction and secondary prevention” indicators (68-117) List of publications relating to indicators, quality criteria, reports and analyses of quality measures
Acronym Body Document title Year Document URL
68. ACCF/AHA/AMA-PCPI
American College of Cardiology Foundation, American Heart Association, American Medical Association-Physician Consortium for Performance Improvement
Performance Measures for Adults With Coronary Artery Disease and Hypertension
2011 http://circ.ahajournals.org/content/124/2/248.full.pdf+html
69. ACHS Australian Council on Healthcare Standards
Acute myocardial infarction (AMI): percentage of patients with an AMI requiring thrombolysis who receive thrombolytic therapy within 1 hour of presentation to the emergency department, as their primary treatment, during the 6 month time period.
2011 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=32839
70. ACHS Australian Council on Healthcare Standards
Acute myocardial infarction (AMI): percentage of patients with an AMI who receive PTCA as their primary treatment and have balloon inflation within 1 hour of presentation to the emergency department, during the 6 month time period.
2011 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=32841
71. AFDN Association Française des Diététiciens Nutritionnistes
Critères de qualité pour l’évaluation et l’amélioration des pratiques professionnelles. Le soin diététique réalisé par un diététicien en établissement de santé
2011 http://www.afdn.org/fileadmin/pdf/soins-etbs-sante/soin-dietetique-ets-de-sante-ceapp.pdf
72. BMA British Medical Association Coronary heart disease indicators Summary of 2011/12 QOF indicator changes, points and thresholds
2011 http://www.bma.org.uk/images/summaryqofguidance2011_v3_tcm41-204734.pdf
73. DREES
Direction de la recherche, des études, de l’évaluation et des statistiques
JM. Januel. Studies and Research series – n°112 - Les méthodes d’ajustement dans les modèles d’évaluation de la mortalité hospitalière - Partie 1 - Étude descriptive. Document de travail
2011 http://www.sante.gouv.fr/IMG/pdf/serieetud112-4.pdf.
74. DREES – Compaq INSERM
Direction de la recherche, des études, de l’évaluation et des statistiques COordination de la Mesure de la Performance et Amélioration de la Qualité Institut national de la santé et de la recherche médicale
Analyse critique du développement d’indicateurs composites : le cas de l’infarctus du myocarde après la phase aiguë. Document de travail
2011 http://www.sante.gouv.fr/IMG/pdf/seriesource_method19.pdf
75. NHS IC National Health Service Information Centre
ACE inhibitor therapy for patients with myocardial infarction
2011 https://indicators.ic.nhs.uk/download/NCHOD/Specification/Spec_09O_607PC_10_V1.pdf
76. NHS IC National Health Service Information Centre
Antiplatelet / anti-coagulant therapy for patients with coronary heart disease
2011 https://indicators.ic.nhs.uk/download/NCHOD/Specification/Spec_09M_605PC_10_V1.pdf
77. NHS IC National Health Service Information Centre
Beta blocker therapy for patients with coronary heart disease
2011 https://indicators.ic.nhs.uk/download/NCHOD/Specification/Spec_09N_606PC_10_V1.pdf
78. NHS IC National Health Service Information Centre
Blood pressure in patients with coronary heart disease
2011 https://indicators.ic.nhs.uk/download/NCHOD/Specification/Spec_09K_603PC_10_V1.pdf
79. NHS IC National Health Service Information Centre
Body Mass Index 2011 https://indicators.ic.nhs.uk/download/NCHOD/Specification/Spec_02D_310VSP2_08_V1.pdf
80. NHS IC National Health Service Information Centre
Cholesterol levels in patients with coronary heart disease
2011 https://indicators.ic.nhs.uk/download/NCHOD/Specification/Spec_09L_604PC_10_V1.pdf
81. NHS IC National Health Service Information Centre
Deaths within 30 days of emergency admission to hospital: myocardial infarction
2011 https://indicators.ic.nhs.uk/download/NCHOD/Specification/Spec_09E_212ISR3AM_09_V1.pdf

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 77/85
Acronym Body Document title Year Document URL
82. NHS IC National Health Service Information Centre
Exercise testing / specialist referral for patients with newly diagnosed angina
2011 https://indicators.ic.nhs.uk/download/NCHOD/Specification/Spec_09I_601PC_10_V1.pdf
83. NHS IC National Health Service Information Centre
Mortality from acute myocardial infarction
2011 https://indicators.ic.nhs.uk/download/NCHOD/Specification/Spec_09B_055DR00++_09_V1.pdf
84. OECD Organisation for Economic Co-operation and Development
Health at a Glance: Europe 2012 2012 http://ec.europa.eu/health/reports/docs/health_glance_2012_en.pdf
85. ACCF/AHA/ACR/SCAI/ SIR/SVM/ SVN/SVS
American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures, American College of Radiology, Society for Cardiac Angiography and Interventions, Society for Interventional Radiology, Society for Vascular Medicine, Society for Vascular Nursing, Society for Vascular Surgery
Performance Measures for Adults With Peripheral Artery Disease
2010 http://circ.ahajournals.org/content/122/24/2583.long
86. AACVPR/ ACCF/AHA
American Association of Cardiovascular and Pulmonary Rehabilitation, American College of Cardiology Foundation, American Heart Association Task Force on Performance Measures
Performance Measures on Cardiac Rehabilitation for Referral to Cardiac Rehabilitation/Secondary Prevention Services
2010 http://content.onlinejacc.org/cgi/reprint/56/14/1159.pdf
87. AHRQ AHRQ quality indicators Acute myocardial infarction (AMI): mortality rate, without transfer cases
2010 http://qualitymeasures.ahrq.gov/content.aspx?id=26515
88. CIHI Canadian Institute for Health Information
Acute myocardial infarction (AMI): risk-adjusted rate of all cause in-hospital death occurring within 30 days of first admission to an acute care hospital with a diagnosis of AMI.
2010 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=15068
89. CMS Centers for Medicare & Medicaid Services
Acute myocardial infarction (AMI): hospital 30-day, all cause, risk-standardized mortality rate (RSMR) following AMI hospitalization.
2010 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=16299
90. CMS/Joint Commission
Centers for Medicare & Medicaid Services, The Joint Commission
Acute myocardial infarction: median time from hospital arrival to administration of fibrinolytic therapy in acute myocardial infarction (AMI) patients with ST-segment elevation or left bundle branch block (LBBB) on the electrocardiogram (ECG) performed closest to hospital arrival time.
2010 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=16246
91. CMS/Joint Commission
Centers for Medicare & Medicaid Services, The Joint Commission
Acute myocardial infarction: median time from hospital arrival to primary PCI in acute myocardial infarction (AMI) patients with ST-segment elevation or LBBB on the ECG performed closest to hospital arrival time.
2010 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=16248
92. CMS/Joint Commission
Centers for Medicare & Medicaid Services, The Joint Commission
Acute myocardial infarction: percent of patients receiving primary PCI during the hospital stay with a time from hospital arrival to PCI of 90 minutes or less.
2010 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=16249
93. CMS/Joint Commission
Centers for Medicare & Medicaid Services, The Joint Commission
Acute myocardial infarction: percent of patients who are prescribed a beta-blocker at hospital discharge.
2010 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=16245
94. CMS/Joint Commission
Centers for Medicare & Medicaid Services, The Joint Commission
Acute myocardial infarction: percent of patients who are prescribed aspirin at hospital discharge.
2010 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=16242
95. CMS/Joint Commission
Centers for Medicare & Medicaid Services, The Joint Commission
Acute myocardial infarction: percent of patients who received aspirin within 24 hours before or after hospital
2010 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=16241

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 78/85
Acronym Body Document title Year Document URL
arrival 96. CMS/Joint
Commission Centers for Medicare & Medicaid Services, The Joint Commission
Acute myocardial infarction: percent of patients with a history of smoking cigarettes who receive smoking cessation advice or counselling during the hospital stay.
2010 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=16244
97. CMS/Joint Commission
Centers for Medicare & Medicaid Services, The Joint Commission
Acute myocardial infarction: percent of patients with LVSD who are prescribed an ACEI or ARB at hospital discharge.
2010 http://qualitymeasures.ahrq.gov/content.aspx?f=rss&id=16243
98. HAS Haute Autorité de santé Indicateurs de pratique clinique AVC Clinical practice indicators. Stroke.
2010 http://www.has-sante.fr/portail/upload/docs/application/pdf/2010-06/ipc_avc_vf_22062010.pdf
99. HAS Haute Autorité de santé Indicateurs généralisés IDM à la sortie [General MI indicators on discharge] Indicateurs de qualité généralisés par la HAS en 2008 et en 2009 dans les établissements de santé. Synthèse et évolution – activité MCO – Infarctus du myocarde à la sortie
2010 http://www.has-sante.fr/portail/upload/docs/application/pdf/2010-12/ipaqss_analyse_descriptive_mco.pdf
100. ICSI Institute for Clinical Systems Improvement
Diagnosis and treatment of chest pain and acute coronary syndrome (ACS): percentage of AMI patients who receive a statin agent within 24 hours of arrival and at discharge from hospital for whom treatment is appropriate.
2010 http://www.qualitymeasures.ahrq.gov/content.aspx?id=34170&search=myocardial+infarction
101. ICSI Institute for Clinical Systems Improvement
Diagnosis and treatment of chest pain and acute coronary syndrome (ACS): percentage of patients with AMI who are using appropriate cardiac rehabilitation.
2010 http://www.qualitymeasures.ahrq.gov/content.aspx?id=34171&search=myocardial+infarction
102. ICSI Institute for Clinical Systems Improvement
Acute myocardial infarction (AMI): mortality rate.
2010 http://www.qualitymeasures.ahrq.gov/content.aspx?id=26500&search=myocardial+infarction
103. NICE National Institute for Health and Clinical Excellence - Audit criteria
Chest pain of recent onset: audit support CG 95
2010 http://www.nice.org.uk/nicemedia/live/12947/47973/47973.doc
104. BMA British Medical Association Coronary heart disease: the percentage of patients with coronary heart disease with a record in the previous 15 months that aspirin, an alternative anti-platelet therapy, or an anti-coagulant is being taken (unless a contraindication or side-effects are recorded)
2009 http://www.qualitymeasures.ahrq.gov/summary/summary.aspx?ss=1&doc_id=14460
105. BMA British Medical Association Coronary heart disease: the percentage of patients with coronary heart disease who are currently treated with a beta blocker (unless a contraindication or side-effects are recorded)
2009 http://www.qualitymeasures.ahrq.gov/content.aspx?id=27147&search=chd
106. HAS Haute Autorité de santé Indicateurs de pratique clinique Infarctus du myocarde Clinical practice indicators. Myocardial infarction.
2009 http://www.has-sante.fr/portail/upload/docs/application/pdf/2010-04/04_document_complet_indicateurs_idm_3_avril_09vf.pdf
107. HAS Haute Autorité de santé Together, let’s improve myocardial infarction management”. A progress report in 2009. Phase 1. From pain to reperfusion
2009 http://www.has-sante.fr/portail/upload/docs/application/pdf/2010-11/idm_etape_1_v5_en_vf.pdf
108. HAS Haute Autorité de santé Together, let’s improve myocardial infarction management”. A progress report in 2009. Phase 2. From reperfusion to hospital discharge
2009 http://www.has-sante.fr/portail/upload/docs/application/pdf/2010-11/idm_etape_2_v5_en_vf.pdf
109. HAS Haute Autorité de santé Together, let’s improve myocardial infarction management”. A progress
2009 http://www.has-sante.fr/portail/upload/docs/appli

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 79/85
Acronym Body Document title Year Document URL
report in 2009. Phase 3. Follow up after hospital discharge
cation/pdf/2010-11/idm_etape_3_v5_en_vf.pdf
110. NICE National Institute for Health and Clinical Excellence - Audit criteria
Acute coronary syndrome - prasugrel: audit support TA 182
2009 http://www.nice.org.uk/nicemedia/pdf/TA182AuditSupport.doc
111. ADLF-HAS Association des diététiciens de langue française Haute Autorité de santé
Consultation diététique réalisée par un Diététicien [Dietary consultation conducted by a dietician]. Série de critères de qualité pour l’évaluation et l’amélioration des pratiques professionnelles
2008
http://www.has-sante.fr/portail/upload/docs/application/pdf/liste_des_criteres_dietetique_-_pdf_2008_04_18__14_26_16_673.pdf
112. ACC/AHA American College of Cardiology / American Heart Association
Report ACC/AHA 2008 Performance Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
2008 http://circ.ahajournals.org/cgi/reprint/CIRCULATIONAHA.108.191099
113. ACC/AHA American College of Cardiology / American Heart Association
ACC/AHA 2008 Statement on Performance Measurement and Reperfusion Therapy
2008 http://circ.ahajournals.org/cgi/reprint/CIRCULATIONAHA.108.191100
114. ACC/AHA American College of Cardiology / American Heart Association
ACC/AHA 2008 Performance Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
2008 http://circ.ahajournals.org/cgi/reprint/CIRCULATIONAHA.108.191099
115. HAS Haute Autorité de santé 7 Evaluation of Professional Practice Programmes. ACS in ambulatory setting, SCA for SAMU, SCA for emergency departments, SCA for Cardiology, SCA and diabetes et SCA and tobacco, acute cardiac failure
2007 http://www.has-sante.fr/portail/jcms/c_864845/outils-pratiques-et-messages-cles-idm
116. NICE National Institute for Health and Clinical Excellence - Audit criteria
MI: secondary prevention: audit criteria CG 48
2007 http://www.nice.org.uk/nicemedia/pdf/word/AuditcriteriaFINAL.doc
117. ACC/AHA American College of Cardiology / American Heart Association
Clinical performance measures for adults with ST-elevation and non-ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Performance Measures on ST-Elevation and Non-ST-Elevation Myocardial Infarction)
2006 http://circ.ahajournals.org/content/113/5/732.full.pdf+html

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 80/85
Literature monitoring on the theme of infarction and secondary prevention is at your disposal on the HAS website, Pilot Programmes section, area devoted to myocardial infarction: http://www.has-sante.fr/portail/jcms/c_736856/ensemble-ameliorons-la-prise-en-charge-de-linfarctus-du-myocarde-idm
Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 81/85
3.4 Other publications (118-176) 118. Abou TJ, Buffet P, Lorgis L, Zeller M, Gonzalez S, L'Huillier I, et al. Scores de stratification du risque et
syndromes coronariens aigus [Risk stratification scores and acute coronary syndromes]. Ann Cardiol Angeiol 2005;54(4):157-60.
119. Auer R, Gaume J, Rodondi N, Cornuz J, Ghali WA. Efficacy of in-hospital multidimensional interventions of secondary prevention after acute coronary syndrome: a systematic review and meta-analysis. Circulation 2008;117(24):3109-17.
120. Baigent C, Blackwell L, Collins R, Emberson J, Godwin J, Peto R, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009;373(9678):1849-60.
121. Barnoya J, Glantz SA. Cardiovascular effects of secondhand smoke: nearly as large as smoking. Circulation 2005;111(20):2684-98.
122. Baudet M, Hericotte P, Daugareil C. Amélioration du pronostic des syndromes coronaires aigus dans les Landes par la modification de l'hygiène de vie. [Improvement of the prognosis of the acute coronary syndromes in Landes by lifestyle modifications.] Ann Cardiol Angeiol 2006;55(4):192-8.
123. Berger PB. Optimal duration of clopidogrel use after implantation of drug-eluting stents--still in doubt. N Engl J Med 2010;362(15):1441-3.
124. Berlin I, Jacob N, Coudert M, Perriot J, Schultz L, Rodon N. Adjustment of nicotine replacement therapies
according to saliva cotinine concentration: the ADONIS* trial-a randomized study in smokers with medical comorbidities. Addiction 2011;106(4):833-43.
125. Bibbins-Domingo K, Chertow GM, Coxson PG, Moran A, Lightwood JM, Pletcher MJ, et al. Projected effect of dietary salt reductions on future cardiovascular disease. N Engl J Med 2010;362(7):590-9.
126. Bourdillon F, Hagenmuller JB. Groupe filières de soins. Rapport final [Care pathway group. Final report]. Paris: AP-HP; 2009. http://cme.aphp.fr/docs-raps/folder.2008-06-09.2256396194/folder.2009-09-07.6879762710/folder.2009-11-17.7410952475/ploneexfileat.2009-11-18.0609486360/view?searchterm=fili%E8res%20de%20soins
127. Campbell NC. Secondary prevention clinics: improving quality of life and outcome. Heart 2004;90 Suppl 4:iv29-iv32.
128. Campbell SM, Ludt S, Van Lieshout J, Boffin N, Wensing M, Petek D, et al. Quality indicators for the prevention and management of cardiovascular disease in primary care in nine European countries. Eur J Cardiovasc Prev Rehabil 2008;15(5):509-15.
129. Cannon CP, Harrington RA, James S, Ardissino D, Becker RC, Emanuelsson H, et al. Comparison of ticagrelor with clopidogrel in patients with a planned invasive strategy for acute coronary syndromes (PLATO): a randomised double-blind study. Lancet 2010;375(9711):283-93.
130. Carsin M, Mahe G. Pourquoi devons-nous evaluer l'alimentation des sujets a risque vasculaire? [Why should vascular patients have a dietary assessment?] J Mal Vasc 2010;35(1):17-22.
131. Caspar-Bauguil S, Garcia J, Galinier A, Periquet B, Ferrieres J, Allenbach S, et al. Positive impact of long-term lifestyle change on erythrocyte fatty acid profile after acute coronary syndromes. Arch Cardiovasc Dis 2010;103(2):106-14.
132. Chow CK, Jolly S, Rao-Melacini P, Fox KA, Anand SS, Yusuf S. Association of diet, exercise, and smoking modification with risk of early cardiovascular events after acute coronary syndromes. Circulation

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 82/85
2010;121(6):750-8.
133. Cicek G, Uyarel H, Ergelen M, Ayhan E, Abanonu GB, Eren M, et al. Hemoglobin A1c as a prognostic marker in patients undergoing primary angioplasty for acute myocardial infarction. Coron Artery Dis 2011;22(3):131-7.
134. Clark AM, Hartling L, Vandermeer B, McAlister FA. Meta-analysis: secondary prevention programs for patients with coronary artery disease. Ann Intern Med 2005;143(9):659-72.
135. Comité français de lutte contre l'hypertension artérielle, Société Française Neuro-Vasculaire. Objectif 2015. 70% des hypertendus contrôlés [French committee against arterial hypertension, French neuro-vascular society. Goal for 2015: controlling 70% of hypertension patients]. Paris: CFLHTA; 2012. http://www.comitehta.org/wp-content/uploads/downloads/2012/01/cflhta_Obj2015-vDEF-0901-vWEB.pdf
136. Critchley JA, Capewell S. Mortality risk reduction associated with smoking cessation in patients with coronary heart disease: a systematic review. JAMA 2003;290(1):86-97.
137. Cushman WC, Evans GW, Byington RP, Goff DC, Jr., Grimm RH, Jr., Cutler JA, et al. Effects of intensive
blood-pressure control in type 2 diabetes mellitus. The ACCORD study group. N Engl J Med 2010;362(17):1575-85.
138. Dorsch MF, Lawrance RA, Sapsford RJ, Oldham J, Greenwood DC, Jackson BM, et al. A simple benchmark for evaluating quality of care of patients following acute myocardial infarction. Heart 2001;86(2):150-4.
139. Duarte FP, Haida A, Bousquet M, Richard L, Mauriege P, Guiraud T. Short-term impact of a 4-week intensive cardiac rehabilitation program on quality of life and anxiety-depression. Ann Phys Rehabil Med 2011;54(3):132-43.
140. Fayard M, Buttard P, Cusey-Sagnol I, Sagnol P, Salmi-Belmihoub S, Zeller M, et al. Le profil de risque dans l'infarctus du myocarde: une evaluation indispensable pour la comparaison des populations [Risk profile in myocardial infarction: an essential evaluation for comparing populations]. Ann Cardiol Angeiol (Paris) 2009;58(1):11-9.
141. Fédération nationale des observatoires régionaux de la santé. Harmoniser les études en nutrition. Un guide de bonnes pratiques pour les études régionales et locales [French national federation of regional health observational studies. Harmonising nutrition studies. A good practice guide for regional and local studies]. Paris: FNORS; 2009. http://www.fnors.org/uploadedFiles/publicationsFnors/guide_nutrition_fnors2009.pdf
142. Filion KB, El KF, Bielinski M, Schiller I, Dendukuri N, Brophy JM. Omega-3 fatty acids in high-risk cardiovascular patients: a meta-analysis of randomized controlled trials. BMC Cardiovasc Disord 2010;10:24.
143. Fox KA, Goodman SG, Anderson FA, Jr., Granger CB, Moscucci M, Flather MD, et al. From guidelines to clinical practice: the impact of hospital and geographical characteristics on temporal trends in the management of acute coronary syndromes. The Global Registry of Acute Coronary Events (GRACE). Eur Heart J 2003;24(15):1414-24.
144. Froger-Bompas C, Laviolle B, Guillo P, Letellier C, Ligier K, Daubert JC, et al. Sustained positive impact of a coronary rehabilitation programme on adherence to dietary guidelines. Arch Cardiovasc Dis 2009;102(2):97-104.
145. Girerd X, Hanon O, Angnostopoulos K, Ciupek C, Mourad JJ, Consoli S. Evaluation de l'observance du traitement antihypertenseur par un questionnaire: mise au point et utilisation dans un service spécialisé [Evaluation of compliance with antihypertensive treatment by questionnaire: development and use in a specialist department]. Presse Méd 2001;30(21):1044-8.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 83/85
146. Goel K, Lennon RJ, Tilbury RT, Squires RW, Thomas RJ. Impact of cardiac rehabilitation on mortality and cardiovascular events after percutaneous coronary intervention in the community. Circulation 2011;123(21):2344-52.
147. Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, Cannon CP, et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med 2003;163(19):2345-53.
148. Gurbel PA, Bliden KP, Butler K, Antonino MJ, Wei C, Teng R, et al. Response to ticagrelor in clopidogrel nonresponders and responders and effect of switching therapies: the RESPOND study. Circulation 2010;121(10):1188-99.
149. Haute Autorité de Santé. Plénière HAS cardioneurovasculaire. Plateformes professionnelles IDM et AVC. Indicateurs de pratique clinique [HAS plenary on neurocardiovascular disease. Professional platforms on MI and stroke. Clinical practice indicators]. Saint-Denis, 2 février 2011 http://www.has-sante.fr/portail/jcms/c_1023612/pleniere-has-cardioneurovasculaire-plateformes-professionnelles-idm-et-avc-indicateurs-de-pratique-clinique-saint-denis-2-fevrier-2011?xtmc=plénière&xtcr=1
150. Haute Autorité de Santé. Définition et exemples d'indicateurs de pratique clinique. Zoom - Certification & Actualités, n°3 Octobre-décembre 2011 [Definition and examples of clinical practice indicators. Zoom – Certification & topical news no. 3, October-December 2011]. http://www.has-sante.fr/portail/jcms/c_1103832/definition-et-exemples-dindicateurs-de-pratique-clinique
151. Haute Autorité de Santé. Coronaropathies. Dossier spécial « Cardiologie » 11 mai, Actualités & Pratiques 2011 [Coronary heart disease. Special report “Cardiology” 11 May, Topical news and practices 2011]. http://www.has-sante.fr/portail/jcms/c_1051695/coronaropathies
152. Hulot JS, Collet JP, Silvain J, Pena A, Bellemain-Appaix A, Barthelemy O, et al. Cardiovascular risk in
clopidogrel-treated patients according to cytochrome P450 2C19*2 loss-of-function allele or proton pump inhibitor coadministration: a systematic meta-analysis. J Am Coll Cardiol 2010;56(2):134-43.
153. Jacquat D, Morin A. Education thérapeutique du patient. Propositions pour une mise en oeuvre rapide et pérenne. Rapport au premier ministre. Assemblée Nationale [Patient therapeutic education. Proposals for rapid and annual implementation. Report to the prime minister. French National Assembly]; 2010. http://www.sante.gouv.fr/IMG/pdf/Rapport_Education_therapeutique_du_patient.pdf
154. Killip TI, Kimball JT. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am J Cardiol 1967;20(4):457-64.
155. Kotseva K, Wood D, De BG, De BD, Pyorala K, Keil U, et al. Cardiovascular prevention guidelines in daily practice: a comparison of EUROASPIRE I, II, and III surveys in eight European countries. Lancet 2009;373(9667):929-40.
156. Lavie CJ, Milani RV. Cardiac rehabilitation and exercise training in secondary coronary heart disease prevention. Prog Cardiovasc Dis 2011;53(6):397-403.
157. Laviolle B, Froger-Bompas C, Guillo P, Sevestre A, Letellier C, Pouchard M, et al. Relative validity and reproducibility of a 14-item semi-quantitative food frequency questionnaire for cardiovascular prevention. Eur J Cardiovasc Prev Rehabil 2005;12(6):587-95.
158. Law MR, Morris JK, Wald NJ. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ 2009;338:b1665.
159. Leurent G, Fougerou C, Pennec PY, Filippi E, Moquet B, Druelles P, et al. Door-to-balloon delays before primary angioplasty in the Regional Acute Myocardial Infarction Registry of Brittany. An analysis of the Observatoire Regional Breton sur l'Infarctus du myocarde (ORBI). Arch Cardiovasc Dis 2009;102(11):777-84.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 84/85
160. Mehta S. SCA Mehta SR. A randomized comparison of a clopidogrel high loading and maintenance dose regimen versus standard dose, and high versus low dose aspirin in 25000 patients with acute coronary syndromes: results of the CURRENT-OASIS 7 Trial. Congrès de l'European Society of Cardiology, session Hot Line I, 30 August 2009 http://www.theheart.org/displayItem.do?primaryKey=998041&type=ppt.
161. Meine TJ, Patel MR, Washam JB, Pappas PA, Jollis JG. Safety and effectiveness of transdermal nicotine patch in smokers admitted with acute coronary syndromes. Am J Cardiol 2005;95(8):976-8.
162. Mente A, de KL, Shannon HS, Anand SS. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch Intern Med 2009;169(7):659-69.
163. Morrow DA, Antman EM, Giugliano RP, Cairns R, Charlesworth A, Murphy SA, et al. A simple risk index for rapid initial triage of patients with ST-elevation myocardial infarction: an InTIME II substudy. Lancet 2001;358(9293):1571-5.
164. Mozaffarian D, Micha R, Wallace S. Effects on coronary heart disease of increasing polyunsaturated fat in place of saturated fat: a systematic review and meta-analysis of randomized controlled trials. PLoS Med 2010;7(3):e1000252.
165. Pande RL, Perlstein TS, Beckman JA, Creager MA. Secondary prevention and mortality in peripheral artery disease: National Health and Nutrition Examination Study, 1999 to 2004. Circulation 2011;124(1):17-23.
166. Park SJ, Park DW, Kim YH, Kang SJ, Lee SW, Lee CW, et al. Duration of dual antiplatelet therapy after
implantation of drug-eluting stents. N Engl J Med 2010;362(15):1374-82.
167. Pell JP, Haw S, Cobbe S, Newby DE, Pell AC, Fischbacher C, et al. Secondhand smoke exposure and survival following acute coronary syndrome: prospective cohort study of 1261 consecutive admissions among never-smokers. Heart 2009;95(17):1415-8.
168. Piepoli MF, Corra U, Benzer W, Bjarnason-Wehrens B, Dendale P, Gaita D, et al. Secondary prevention through cardiac rehabilitation: from knowledge to implementation. A position paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation. Eur J Cardiovasc Prev Rehabil 2010;17(1):1-17.
169. Ray KK, Seshasai SR, Wijesuriya S, Sivakumaran R, Nethercott S, Preiss D, et al. Effect of intensive control of glucose on cardiovascular outcomes and death in patients with diabetes mellitus: a meta-analysis of randomised controlled trials. Lancet 2009;373(9677):1765-72.
170. Rigotti NA, Munafo MR, Stead LF. Smoking cessation interventions for hospitalized smokers: a systematic review. Arch Intern Med 2008;168(18):1950-60.
171. Société française de santé publique. Propositions pour le PNNS 2011-2015 [French Society of Public Health. Proposals for PNNS 2011-2015]. Vandoeuvre-lès-Nancy: SFSP; 2010. http://www.sfsp.fr/publications/file/RapportfinalpropositionsPNNS5-11-2010.pdf
172. Squire IB, Nelson CP, Ng LL, Jones DR, Woods KL, Lambert PC. Prognostic value of admission blood glucose concentration and diabetes diagnosis on survival after acute myocardial infarction; Results from 4702 index cases in routine practice. Clin Sci (Lond) 2009.
173. Tabet JY, Meurin P, Teboul F, Tartiere JM, Weber H, Renaud N, et al. Determination of exercise training level in coronary artery disease patients on beta blockers. Eur J Cardiovasc Prev Rehabil 2008;15(1):67-72.
174. Vokó Z, de Brouwer S, Lubsen J, Danchin N, Otterstad JE, Dunselman PH, et al. Long-term impact of secondary preventive treatments in patients with stable angina. Eur J Epidemiol 2011;26(5):375-83.

Clinical Practice Indicators: Myocardial Infarction (MI) – “From first symptoms to follow-up at 1 year”
HAS / Pilot Programmes Department – Clinical impact / March 2012 85/85
175. Wallentin L, Becker RC, Budaj A, Cannon CP, Emanuelsson H, Held C, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2009;361(11):1045-57.
176. Yohannes AM, Doherty P, Bundy C, Yalfani A. The long-term benefits of cardiac rehabilitation on depression, anxiety, physical exercise and quality of life. J Clin Nurs 2010;19(19-20):2806-13.