clinical maintenance, new builds, renovations and ... · clinical . maintenance, new builds,...
TRANSCRIPT
Clinical
Maintenance, new builds, renovations and refurbishments Infection prevention and control implications SOP
Document Control Summary
Status: replacement Infection control implications for maintenance, new builds, renovations and refurbishments
Version: 1 Date: September 2016
Author/Owner: Judy Carr/ Kenny Laing
Approved by: Policy and Procedures Committee Date: 23 March 2017
Ratified: Policy and Procedures Committee Date: 23 March 2017
Related Trust Strategy and/or Strategic Aims
Provide high quality services, built on best known practice and evaluated through clear process and outcome measures
Implementation Date: December 2016
Review Date: December 2018
Key Words: New build, renovation, refurbishment, Infection Prevention and Control
Associated Policy or Standard Operating Procedures
Infection Prevention and control policy
2
Contents
1. Introduction ..................................................................................................................... 3
2. Purpose ............................................................................................................................ 3
3. Scope ............................................................................................................................... 3
4. Recommendations ............................................................................................................ 4
5. Planning ........................................................................................................................... 4
6. Construction and high risk maintenance ............................................................................ 5
7. Commissioning ................................................................................................................. 6
8. References ........................................................................................................................ 6
Appendix 1. Guidance on Infection Control Principles and Measures to be incorporated into New Builds Renovations and Refurbishments………………………………………………………………………7
Appendix 2. Infection control risk assessment during construction / refurbishment of a healthcare facility………………………………………………………………………………………………………………………………………………16
Appendix 3. – Infection Prevention and Control Checklist………………………………………………………………19
Change Control – Amendment History
Version Dates Amendments
3
1. Introduction It is recognised that the health care environment is a secondary reservoir for micro-organisms with the potential for infecting patients (NHS Estates Infection Control in a Built Environment 2013). Studies have suggested that bacteria can exist and survive in the environments with fixtures, fittings and furnishings acting as reservoirs of infection. Therefore it is essential to ensure that infection control and cleanliness issues are considered and implemented during the planning, designing and final construction stages of all new builds, renovations and refurbishments to minimise the cross infection risks that can be associated with the environment see Appendix 1.
The need to minimise the risk of cross-infection is important in mental health settings, but other factors such as ligature risk and the creation of a positive therapeutic environment will need to be taken into consideration when providing advice to these areas.
The guidance in this document follows the essential principles given in the Health and Social Act 2012: Code of Practice for health and adult social care on the prevention and control of infections and related guidance below
• Health Technical Memorandum 03-01 Part A and Part B – Heating and Ventilation Systems
• Health Building Note 00-09 Infection control in the built environment (2013)
• HCAI Code of Practice 2008
• Health Building Note 03-01 – ‘Adult acute mental health units’ and medium secure services
• Dementia Design Checklist NHS Scotland
2. Purpose This SOP outlines the Infection Prevention and Control (IPC) input required in new builds and air handling systems during the concept/ feasibility scoping and detailed planning stages of all new builds, renovation and refurbishment of old buildings as well as during the construction and commissioning stages. The Trust regards the health, safety and welfare of staff, patients and visitors as a serious issue. The Trust will work to ensure the environment is compatible with proper provisions of services to patients where health hazards are kept to a minimum.
3. Scope This document applies to all South Staffordshire and Shropshire employees and all those visiting the Trusts premises such as contractors, agency/bank/locum staff, students and volunteers.
4
4. Recommendations Creating/maintaining a non-clinical feel can be achieved by using furnishings/fittings that are manufactured especially for this setting and are easy to clean and maintain. For example, wood-effect vinyl can be used to create a less clinical environment, but cleanliness can be maintained.
In some specialties within mental health bedroom areas, porcelain basins and toilets would present a risk; alternatives such as resin or stainless steel should be considered. Cleaning of these materials should, however, be considered carefully.
There is no requirement for a clinical wash-hand basin in an en-suite bedroom. Alternative arrangements to provide healthcare staff with access to hand hygiene should be made.
There should be sufficient access to hand-hygiene facilities for staff. Clinical wash-hand basins should be sited only in supervised areas such as the clean utility room, treatment rooms and dirty utility room. Antimicrobial hand-rub should be provided. Where necessary, the use of patient wash-hand basins in en-suite rooms can be used with care to avoid recontamination of hands.
In secure mental health units, hand dryers or vandal-proof integral hand-wash dryers in communal toilets may provide a safer option for hand hygiene while encouraging those in the service to clean hands.
Single rooms can be used for source isolation.
Risk assessment should inform the storage of protective clothing, soap and paper towels, clinical waste receptacles etc. All fixtures and fittings should be anti-ligature (see Health Building Note 03-01 – ‘Adult acute mental health units’).
Assessment of the need for a macerator or bedpan washer-disinfector should be undertaken. If a specific dirty utility room is not required, alternative procedures should be in place for the disposal of body fluids and urine testing
5. Planning Within all new builds the standards set out in the must be complied with. Where possible the same principles must be applied to refurbishments and renovations of existing buildings. During the planning period, it is paramount that the health care environment is designed to facilitate effective cleaning and maintenance. The IPC team need to review the scheme design plans and drawings to ensure that the appropriate infection control measures have been incorporated. It is important that the IPC team and the chief executive officer sign-off each stage of the project. This will ensure that the control of infection is considered throughout; failure to assess infection control risk properly can lead to the expensive redesign later and expose the patient and healthcare worker to infection control hazards.
5
An infection control checklist for use during the different stages of a capital project is in Appendix 3
6. Construction and high risk maintenance Maintenance and construction work generates a significant amount of dust and debris. The dispersal of environmental micro-organisms during the construction stages can result in health care associated infection. For example fungal spores such as aspergillorosis can pose an increased risk to some patients of invasive fungal infections.
The following standard control measures to minimise dust and debris should be undertaken within all construction and maintenance work within an existing building:
• Windows, doors and roof spaces must be sealed to control dust • A restricted access entrance, lift and a hallway must be designated for the use of
the construction workers only and must not be used by patients, visitors or health care workers
• Debris must not be allowed to accumulate and must be removed as it is created. Debris must not be carried through patients’ areas and must be removed via the designated access points for the construction workers. Where construction work is being undertaken above ground floor level, debris should be removed via the window. Debris must be transported in sealed containers/bags or covered with a damp dust sheet.
• Regular vacuuming and cleaning of the construction site and surrounding areas must be undertaken. Where applicable, wet mopping of the area around the outside entrance to the site, corridor, lift etc must be undertaken daily or more frequently as required. Dust attracting mats should be placed at the entrance and exit of the work area (tacky mat).
As an integral part of all construction and high risk maintenance work, the following will be undertaken by the Project manager, Estates team and Infection control to identify the need for any additional infection control measure:
Risk Assessment This will identify any potential risks to patients within the environment and indicate any additional environmental control measures required to maintain patient safety such as movement of patients to other wards (see Appendix 2).
Documentation The outcome of the risk assessment and recommendations for the control measures will be produced in the form of written report and communicated to all the relevant parties prior to implementation of the scheme.
6
7. Commissioning Following completion of construction or high risk maintenance work, it is essential that the site is thoroughly deep cleaned by Hotel Services. The infection control team will need to undertake a site visit of any new build, renovation or refurbishment to enable any infection control issues to be addressed before the site is handed over.
The IPC team should also be involved in processes for:
• analysis of commissioning data; • transfer of facilities; • phased or staged occupation; storage and subsequent cleaning/disinfection of
any furniture or equipment; • approval of engineering commissioning data • commissioning tests (for example, water testing); • approval of engineering commissioning data for special ventilated isolation
room(s); • site visits; • staff orientation and training; • post-handover period; • decommissioning of redundant facilities; • period of handover to operational management; • confirming communication of procedures with internal and external
agencies/users (for example, ambulance service and patient information leaflets).
8. References • Health Technical Memorandum 03-01 Part A and Part B – Heating and Ventilation
Systems • Health Building Note 00-09 Infection control in the built environment (2013) • HCAI Code of Practice 2008 • Health Building Note 03-01 – ‘Adult acute mental health units’ and medium secure
services • Dementia Design Checklist NHS Scotland
7
Appendix 1
Guidance on Infection Control Principles and Measures to be incorporated into
New Builds Renovations and Refurbishments
Introduction This guidance provides a summary of principles and measures to be incorporated into new building developments, refurbishments and renovations. Issues to consider when designing a healthcare facility Design to eliminate reservoirs of infection: • Keep lines simple and clean, without unnecessary ornamentation. • Uses finishes that are impervious and seamless, as far as practicable. • Run hard flooring up the walls for a short distance to provide an easy-to-clean
coving. • Minimise dead-legs and blind ends in water systems, but in the original design
and as the systems are modified. • Ensure good ventilation, with appropriate ventilation rates where specified. • Consider “no-hands” operation of utilities (for example, sensor taps, automatic
lights, movement sensors for toiler flushes etc). • Consider “no-hands” operation of other facilities (for example, automatic doors,
proximity-sensors etc). • Consider enclosed blinds as an alternative to curtains at windows. • Discourage pests such as rats, pigeons etc by designing-out the places where
they nest or feed. • Design-in pest control such as fly screens, ultraviolet fly-killers etc.
Encourage desired behaviour (for example, tidiness, hand hygiene) • Provide sufficient space in all areas to allow for easy movement – including
movement of equipment and supplies. • Provide sufficient storage for each patient and for all supplies. Storage areas
should be enclosed. • Ensure proper segregation and management of waste, including clinical waste
from linen. • Provide sufficient general litter bins, including stub bins. • Provide bedside litter disposal facilities for patient use. • Design-out unnecessary horizontal surfaces (for example, window sills, waste-bin
lids) in order to discourage clutter. • Provide enough hand hygiene stations – both wash-hand basins and
antimicrobial handrub/wash dispensers. • Focus on efficient work flows – and design-in the appropriate facilities. • Plan for and deliver good separation of clean and dirty activities. • Provide sufficient space for storage and preparation of cleaning equipment and
materials, both for cleaning staff and ad-hoc use by non-cleaning staff. • Provide suitable facilities for local cleaning of equipment such as commodes, drip
stands etc. • Provide sufficient seating to discourage visitors sitting on beds, waste-bins etc.
8
Design for easy cleaning Good design can make cleaning immeasurably easier.
• Use robust finishes that resist staining, but which are also easy to clean. • Use hard flooring in all clinical areas, and use carpet sparingly in any patient or public
area. • Use dirt-trapper matting on all external entrances. • Where items must be removed for cleaning (for example, curtains, radiator covers,
ventilator grilles), make removal and replacement easy. • Ensure that all storage areas can be easily emptied for cleaning (for example, use
trolleys within storage bays or removable storage baskets within cupboards). • Use wall-hung WCs/wash-hand basins etc to allow floors to be cleaned easily. • Use bumper rails as necessary to prevent scuffing trolleys, beds etc. • Provide “easy-clean” computer keyboards, telephone etc.
Common Pitfalls There may be pressure to choose the cheapest products or design. Attention to whole-life costs, including the costs of cleaning, is important. Design that leaves the building exposed to unnecessary contamination, or which encourages poor practice, will cost more in the end.
Lay Outs In all schemes the workflow of the environment needs to be considered. Clean to dirty workflows need to be incorporated to ensure that the staff can practice safely and risks are reduced.
Single Rooms Single rooms should have en-suite toilet and bathroom facilities as well as hand wash facilities in the main room. Day Rooms The aesthetic appeal of the environment and psychological needs of the patients are important aspects to consider in the design of day rooms in conjunction with the infection control standards. However careful consideration must be given to the types of fixtures, fittings and soft furnishings incorporated into the scheme. It is important to ensure that storage cupboards are considered because day rooms often become overrun with pieces of equipment particularly large pieces of equipment which are difficult to store elsewhere – e.g. wheelchairs, hoist
Therapy Rooms It is important to ensure that the room is designed to the appropriate infection control standards e.g. furnishing, fixtures and fittings must be impervious to water. Therapy services tend to utilise large bulky types of patient equipment, therefore storage facilities within new builds must be sufficient to store clean equipment not in use. Where possible a separate dirty room should be available to enable used equipment to be segregated and cleaned in between each patient use. The IPC team will advise further on the appropriate facilities required within the separate room to ensure that the standards recommended within the DH decontamination agenda are met. Hand wash basins must be available within the therapy room and the number required will vary on the size of the room
9
and the number of therapists. Staff catering facilities must be in a separate room to the therapy and decontamination room.
Cleaning Cupboards Sufficient accommodation must be provided in the form of a separate room for cleaning equipment. The size and number required will depend on the activity and types of services provided within the area. All cleaning cupboards should have space for a slop hopper for the disposal of dirty water, a sink system to clean cleaning equipment, hand wash sink, sufficient storage racks for colour coded segregation of cleaning equipment and storage facilities for replenishments.
Dirty Utility / Sluices It is essential that ancillary areas are of an acceptable standard and appropriate size for purpose. The exact requirements will depend on the use of the area, the types of services accessing the area and the activities that will be undertaken within the area. Space and facilities for holding and reprocessing equipment must be incorporate. Separate, double sinks are required in sluice areas for the decontamination of equipment such as commodes, bed pan holders and patient wash bowls (NHS Estates’ HTM 2030). A separate clinical wash- hand basin should be provided.
Adequate storage facilities for equipment such as commodes, linen bag holders and Sterile Service Department (SSD) equipment awaiting return to SSD must be incorporated. Storage facilities for temporarily holding items for disposal must be included. Racking should be installed for disposable items such as bed pans and urinals.
Separate receivers such as slop hoppers should be provided for contaminated wastewater or blood and body fluids (HBN 36). Macerators are recommended for areas that have a heavy use of bedpans. Bed pan washers are not recommended for use due to ongoing maintenance and validation costs required within the NHS Estates HTM 2030 (washer-disinfectors).
Clean utility room The function of clinical rooms will vary. It is important to ensure that the room is designed to the appropriate infection control standards e.g. furnishings, fixtures and fittings must be impervious to water and adequate storage facilities provided. Hand was facilities must be available.
Treatment Room A treatment room may be required for in-patient examinations or investigations on the ward. There should be a hand washing sink and space to allow for the storage of equipment and sterile supplies.
Waiting Rooms, Entrances and Receptions The aesthetic appeal of a waiting room and the psychological needs of the patients are important aspects to consider in the design of this area in conjunction with the infection control standards. These areas have high throughputs and have the added impact of external elements. Therefore, consideration needs to be given to the durability of and ease
10
of cleaning any fixtures, fittings and furnishings incorporated into the scheme (please refer to these sections). Toilet facilities should be available within these areas for patients. Where possible, hand wash facilities should be incorporated for reception staff. Appropriate storage facilities need to considered within reception areas and notice boards should be kept to a minimum. Nappy-changing area Provision of a nappy changing area is a necessary in any healthcare facility. It should be in a separate room within accessible WCs used by visitors and outpatients and be provided with a fold down facility. Facilities for disposal of soiled nappies and for hand washing in the immediate environment are required.
Hand Hygiene Facilities see HTM 64 and HBN 00-02
Clinical wash – hand basin Designated hand wash facilities must be available in all clinical areas, sluices, decontamination rooms, public and staff toilets, cleaners’ storerooms and kitchen facilities (including staff rest rooms). Within mental health and learning disability settings there should be 1 hand wash facility for every 6 beds. Guidelines for the appropriate numbers of clinical wash hand basins in clinical areas are given in Health Building Note (HBN) 04-01
Alcohol hand rub stations / holders MUST NOT be situated within bathrooms and kitchens and should be kept to a minimum in all other areas, as staff are encouraged to wear a tottle.
Hand hygiene facilities should be easily visible and accessible and should not be obscured by curtain rails, doors, equipment etc.
Hand wash facilities should be designed for purpose and conform to the full guidance i.e.
• No overflow • No plug • Made from non-scratch material such as porcelain • Elbow operated or no touch sensor taps. Screw taps ate not acceptable. • Sink, large enough to allow adequate room for proper hand washing to take place
and curved to avoid splashing • Suitably sited, foot operated waste bins and wall mounted dispensers for
approved hand hygiene products; in most cases this will be a liquid soap. Placement of Hand hygiene products will be discussed with the IPC Team.
• Suitably sited wall mounted dispensers will be available for disposable paper towels in an approved presentation
• Have a sealed waterproof back splash to allow effective cleaning of all surfaces. • Hot – air dryers should not be used in clinical areas as warm air currents dry
hands slowly and can only be used by one individual at a time. This results in the temptation to dry hands on clothing. They are also noisy which would discourage staff hand washing when patients are sleeping
Non- clinical wash-hand basin
• All en-suite facilities should have a wash-hand basin
11
• All toilet facilities should have a hand wash basin • Tap outlets that are not sited above the waste pipe outlet to avoid
splashing of contamination from the waste pipe. • Have a sealed waterproof back splash to allow effective cleaning of all
surfaces Toilets All the toilets will have covered toilet paper dispensers that dispense single sheets of paper. Client toilets will be easy to maintain to render them hygienic and cleanable. Padded backrests with soft plastic covers should not be used
Visitor toilets These should provide enough space and have a high grade of finishes to maintain a good standard of hygiene. There should be provision of disposal facilities for sanitary waste in both women and mixed-sex toilets.
Linen Services and Storage Linen cupboards should be large enough to ensure that the linen is not stored on open trolleys. Cupboards should be situated in a place that is accessible for clinical use as well as for clean deliveries. Shelves within cupboards should be impervious to water and cleanable. Sufficient storage facilities should be allowed for in use linen skips and bags awaiting disposal. Used linen MUST NOT be stored within the same environment as clean linen or other clean products. Clear segregation of clean and dirty items must be maintained (NHS Estates HBN 4). Where laundrettes are provided in hospitals for long-stay patients, there must be a dedicated area specifically for laundering and not used for any other purpose. There must be segregation of clean and dirty linen, industrial standard washing machines and dryers and hand wash facilities dedicated for hand hygiene purposes. Changing and showering facilities for laundrette staff must be provided within any new building schemes.
Changing Facilities In all new builds, changing, showering and storage facilities for personal belongings must be provided for staff. Where possible these should be incorporated into any refurbishment or renovation work which involves the whole or a significant proportion of that site. However, this will need to be risk assessed as the need will depend on the size, types of services provided and activities of the site.
Kitchens and Beverage Areas Patients are particularly vulnerable to food-borne infections. Therefore it is essential to ensure that high standards are maintained within all food preparation facilities, storage and processing areas, distribution methods and servicing practices. All equipment, fixtures and fittings, finishes and facilities within ward kitchens, pantries, therapeutic kitchens and beverage areas must comply with the Food Safety Act 1990. Dedicated hand wash facilities must be incorporated.
12
The reprocessing of patient crockery and cutlery should be undertaken within a dishwasher.
For all new schemes or upgrades involving main catering kitchen, the Environmental Health Officer, Hotel Service managers and Infection control team must be involved in the planning and design meetings.
Staff Kitchens A suitable kitchen/pantry will be available and sited away from the clinical and dirty utility areas. Kitchen areas should be kept clean and tidy where domestic refrigerators are provided they must be clearly identified. Drugs and samples must not be stored in domestic refrigerators.
Storage Adequate provision of storage cupboards / facilities for clean and used items of equipment must be included in schemes particularly for large pieces of equipment such as mattresses, wheelchairs, hoists etc. Storage of equipment in sluices and bathrooms is inappropriate and must not occur. Storage facilities are often insufficient within new schemes and lead to both infection control and health and safety implications within the clinical area. Storage racks, boxes and shelving need to be accessible and easily cleaned. Storage space should be sufficient to discourage storing items on the floor. In larger builds such as community hospitals consideration should be given to incorporating larger equipment library stores. Storage cupboards placed on walls should be built up to the ceiling or have sloping surfaces to prevent items being put on top of cupboards and also to prevent a reservoir for dust to collect. Wardrobes/ bedside locker facilities must be of a design that adequately contains patient’s personal effects.
Lighting Natural lighting is preferred from windows. Privacy should be ensured for patient and staff by obscure glass Light fittings should be of a design which prevents buildup of dust e.g. no ledges or ridges. They should be positioned for easy access and frequent cleaning.
Finishes Carpets are not to be used in clinical areas. Evidence indicates that carpets are contaminated with infectious micro-organisms and have been well associated with outbreaks (Skoutelis et al, 194; Sarangi and Roswell 1995). Carpets are more difficult to keep clean and retain odours. If carpets are to be installed in day rooms, waiting areas etc then it is essential to ensure that the cleaning schedules are agreed upon and achievable before the carpet is placed. Hard floors that are impervious to water, sealed and non-slip must be incorporated into all other areas. Wood and tile floors must be avoided as they can be reservoirs for infection micro-organisms. Fixtures, fittings and hard surfaces should be easily accessible and easy to clean. High level surfaces should be avoided.
13
All soft furnishes such as chairs should be chosen with cleaning in mind. In all clinical areas, the designs should be smooth, non porous and water resistant. Blinds should be avoided in all clinical areas as they are difficult to clean and will not withstand disinfectants. Frosted glass or curtains are recommended. Curtains need to be made of material that can withstand temperatures above 65°C and they need to be incorporated in to room cleaning schedules. Doors and walls need to be smooth, hard and impervious surfaces. Ceilings need to be made of a material that is cleanable. False ceilings can be associated with the accumulation of dust, fungi and pests. Upon completion of building work, these should be checked to ensure that there is no unwanted material and that there is no access for pests. Electrical power sockets and light switches where possible should be flush mounted to avoid dust accumulation. NB All finishes must be able to withstand the use of cleaning and disinfection products that are recommended for use within Health Care Trusts.
Equipment The IPC team should be involved in decisions for new equipment for example paper towel dispensers, soap dispensers, to ensure that it is compatible with IPC requirements.
Water Systems Hot and cold water systems must comply with HTM 2027 and HTM 2040. Whilst work is being undertaken, it is important to ensure that water contamination does not occur and that the quality of water is not compromised. Water coolers must be fed from a main water supply and the drainage system attached to a main waste system. Ice making machines must only be installed for topical therapy purposes and not for oral consumption. Procurement of regular maintenance for ice making machines must be planned into the scheme.
Waste There are stringent legislations and guidelines for the management of all health care waste. Good design and space can minimise problems associated with inadequate storage, waster segregation and disposal (NHS Estates HTM 2065). Clinical bin lids do become contaminated with micro-organisms. Therefore bins that are purchased need to be easily cleaned and disinfected. Bins with a removable body are recommended to allow for adequate and easy cleaning. Bins should be foot operated only and have a lid with a mechanism that prevents it being operated by the hand. Appropriate storage facilities for waste should be incorporated into the design. Storage cupboards for waste situated at ward entrances must be designed into any new build schemes and where possible into any new renovation / refurbishment to prevent sluices becoming cluttered with waste waiting to be collected. These cupboards must only be use for the storage of waste and used linen. In other health care facilities such as clinics, all waste bags must be contained in lockable containers that comply with waste guidelines.
14
Air Handling Systems
Ventilation All rooms should be well ventilated to ensure the comfort of both patients and staff. For areas where it is absolutely necessary to install mechanical ventilation, ventilation systems should be designed in accordance with the requirements of Health Technical Memorandum 03-01 – ‘Specialised ventilation for healthcare .Air movement induced by any form of mechanical ventilation must flow from clean to dirty areas, where these areas can be defined. The design should allow for adequate flow of air into any spaces having only mechanical extract ventilation, via transfer grilles in doors or walls. However, such arrangements should avoid the introduction of un- tempered air and should not prejudice fire safety or privacy.
Internal design conditions The design conditions selected within patient areas must strike a balance between the comfort requirements of staff and patients, who often have very different levels of clothing and activity.
Minimum fresh-air requirements The dilution of body odours is the critical factor in determining ventilation requirements. Where natural ventilation or full fresh-air systems are used, all ventilation air will be fresh. Where odour dilution is the overriding factor, it is recommended that 10 litres per second per person should be taken as the minimum ventilation rate.
Limiting supply air conditions For most applications in healthcare buildings, it is the temperature differential between the supply and room air, rather than the actual temperature of the supply air, which is the critical factor. The maximum recommended supply-to-room-air temperature differential is: Summer cooling: –7 K Winter heating: +10 K. If a humidifier is fitted, it is necessary to keep supply-air humidity below 70% during winter in order to minimise the risk of condensation on cold surfaces.
Air purity In healthcare premises, the standard of filtration will depend on the activities within the occupied spaces. With the exception of specialist areas (for example manufacturing pharmacies), aerobiological requirements are not stringent, and filtration is only required to:
• Maintain hygienic conditions for the health and welfare of occupants, or for processes such as food preparation;
• Protect finishes, fabrics and furnishings in order to reduce redecoration costs; • Protect equipment either within the supply air system (that is, to prevent blocking of
coils), or in the space itself to prevent dust build-up.

15
Given that almost all viable particles originate from the occupants of a space and not from the incoming air, dilution is the more important factor aerobiologically. Therefore, for general areas a G4 filter is suitable.
Heating General space heating requirements may be met by a variety of systems including radiators and radiant panels, or within the air-conditioning system. Designers should ensure that the most appropriate method is employed with regard to the healthcare environment being provided If radiators are installed they need to be easily cleaned. Radiators and low surface systems which have narrow channels and groves should not be installed as they are very difficult to keep clean and free from dust. Radiators should be located under windows or against exposed walls. There should be space between the top of the radiator and the windowsill to prevent curtains reducing the output. There should be adequate space underneath to allow cleaning equipment to be used. Where possible, low surface temperature control covers need to be easily removed to enable cleaning of the actual radiator from all angles; top, back, front and underneath.
16
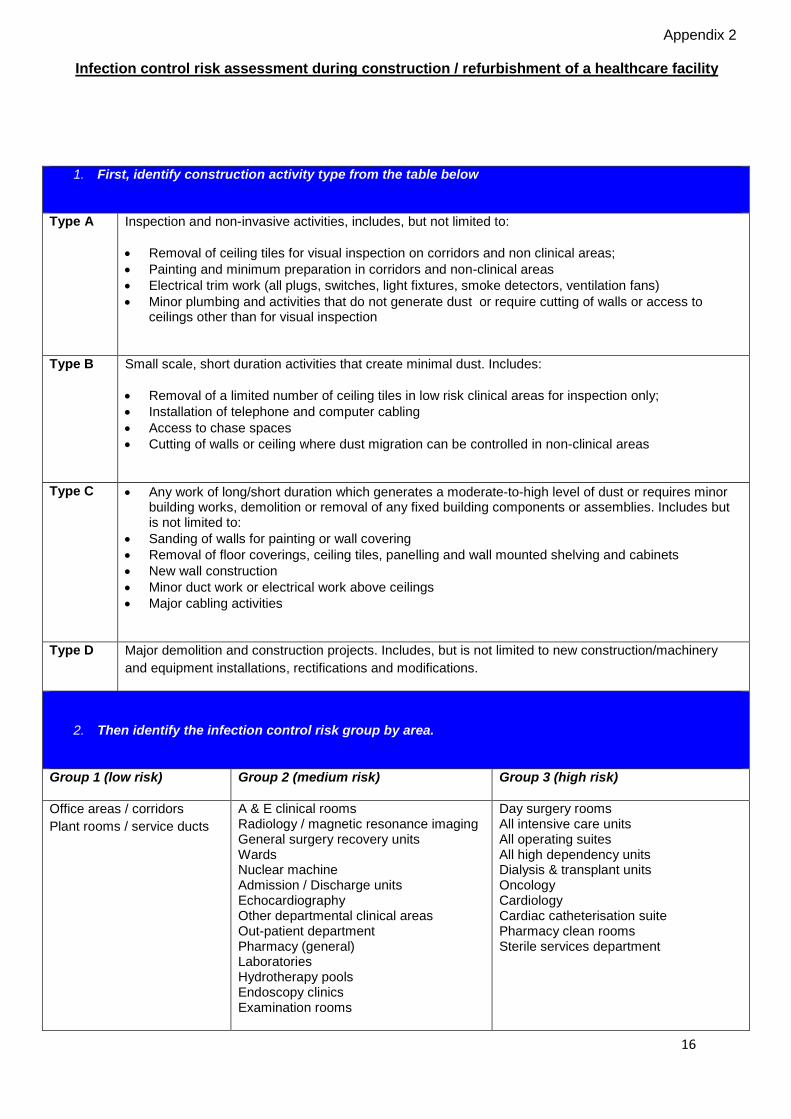
1. First, identify construction activity type from the table below
Type A Inspection and non-invasive activities, includes, but not limited to:
• Removal of ceiling tiles for visual inspection on corridors and non clinical areas; • Painting and minimum preparation in corridors and non-clinical areas • Electrical trim work (all plugs, switches, light fixtures, smoke detectors, ventilation fans) • Minor plumbing and activities that do not generate dust or require cutting of walls or access to
ceilings other than for visual inspection
Type B Small scale, short duration activities that create minimal dust. Includes:
• Removal of a limited number of ceiling tiles in low risk clinical areas for inspection only; • Installation of telephone and computer cabling • Access to chase spaces • Cutting of walls or ceiling where dust migration can be controlled in non-clinical areas
Type C • Any work of long/short duration which generates a moderate-to-high level of dust or requires minor building works, demolition or removal of any fixed building components or assemblies. Includes but is not limited to:
• Sanding of walls for painting or wall covering • Removal of floor coverings, ceiling tiles, panelling and wall mounted shelving and cabinets • New wall construction • Minor duct work or electrical work above ceilings • Major cabling activities
Type D Major demolition and construction projects. Includes, but is not limited to new construction/machinery and equipment installations, rectifications and modifications.
2. Then identify the infection control risk group by area.
Group 1 (low risk) Group 2 (medium risk) Group 3 (high risk)
Office areas / corridors Plant rooms / service ducts
A & E clinical rooms Radiology / magnetic resonance imaging General surgery recovery units Wards Nuclear machine Admission / Discharge units Echocardiography Other departmental clinical areas Out-patient department Pharmacy (general) Laboratories Hydrotherapy pools Endoscopy clinics Examination rooms
Day surgery rooms All intensive care units All operating suites All high dependency units Dialysis & transplant units Oncology Cardiology Cardiac catheterisation suite Pharmacy clean rooms Sterile services department
Appendix 2
Infection control risk assessment during construction / refurbishment of a healthcare facility
17
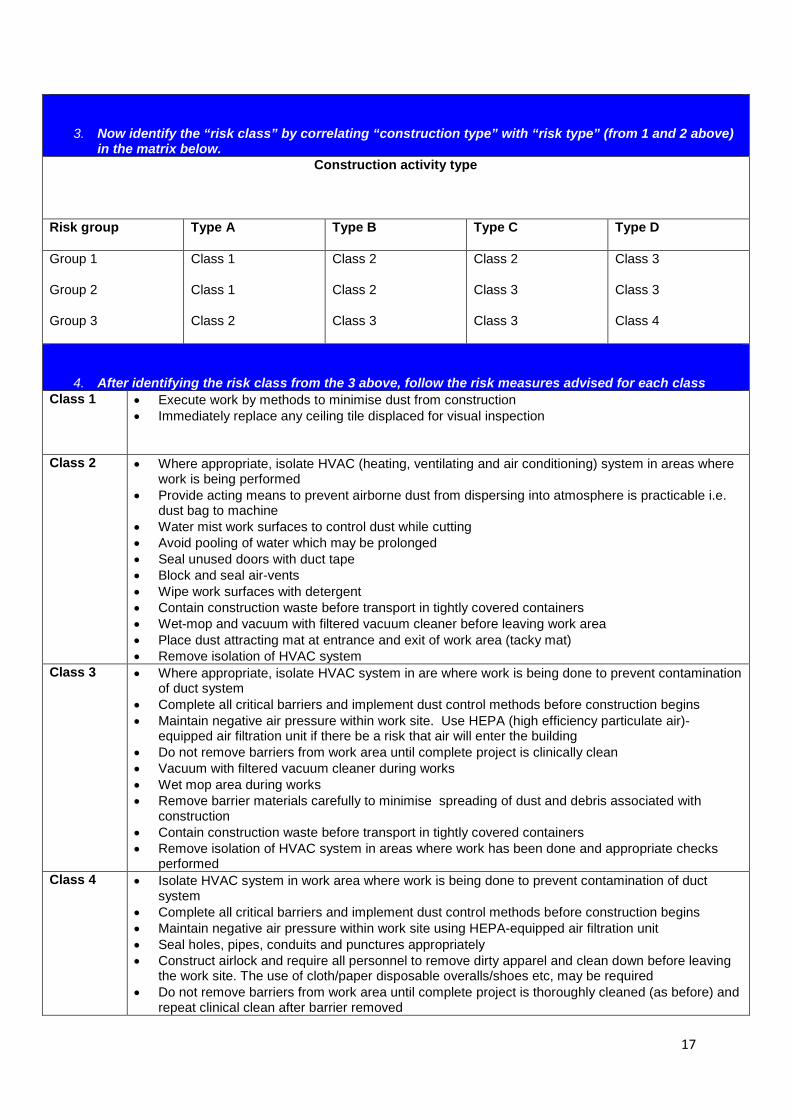
3. Now identify the “risk class” by correlating “construction type” with “risk type” (from 1 and 2 above) in the matrix below.
Construction activity type
Risk group Type A Type B Type C Type D
Group 1
Group 2
Group 3
Class 1
Class 1
Class 2
Class 2
Class 2
Class 3
Class 2
Class 3
Class 3
Class 3
Class 3
Class 4
4. After identifying the risk class from the 3 above, follow the risk measures advised for each class Class 1 • Execute work by methods to minimise dust from construction
• Immediately replace any ceiling tile displaced for visual inspection
Class 2 • Where appropriate, isolate HVAC (heating, ventilating and air conditioning) system in areas where work is being performed
• Provide acting means to prevent airborne dust from dispersing into atmosphere is practicable i.e. dust bag to machine
• Water mist work surfaces to control dust while cutting • Avoid pooling of water which may be prolonged • Seal unused doors with duct tape • Block and seal air-vents • Wipe work surfaces with detergent • Contain construction waste before transport in tightly covered containers • Wet-mop and vacuum with filtered vacuum cleaner before leaving work area • Place dust attracting mat at entrance and exit of work area (tacky mat) • Remove isolation of HVAC system
Class 3 • Where appropriate, isolate HVAC system in are where work is being done to prevent contamination of duct system
• Complete all critical barriers and implement dust control methods before construction begins • Maintain negative air pressure within work site. Use HEPA (high efficiency particulate air)-
equipped air filtration unit if there be a risk that air will enter the building • Do not remove barriers from work area until complete project is clinically clean • Vacuum with filtered vacuum cleaner during works • Wet mop area during works • Remove barrier materials carefully to minimise spreading of dust and debris associated with
construction • Contain construction waste before transport in tightly covered containers • Remove isolation of HVAC system in areas where work has been done and appropriate checks
performed Class 4 • Isolate HVAC system in work area where work is being done to prevent contamination of duct
system • Complete all critical barriers and implement dust control methods before construction begins • Maintain negative air pressure within work site using HEPA-equipped air filtration unit • Seal holes, pipes, conduits and punctures appropriately • Construct airlock and require all personnel to remove dirty apparel and clean down before leaving
the work site. The use of cloth/paper disposable overalls/shoes etc, may be required • Do not remove barriers from work area until complete project is thoroughly cleaned (as before) and
repeat clinical clean after barrier removed

18
• Vacuum work area with filtered vacuum cleaner • Wet mop area with detergent during works • Remove barrier materials carefully to minimise spreading of dust and debris associated with
construction • Contain construction waste before transport in tightly covered and sealed containers • Remove isolation of HVAC system in areas where work has been done and appropriate checks
performed
Appendix 3 – Infection Prevention and Control Checklist
Business Case Review
For non-clinical issues relating to the design, construction and fitting out of multi-bed rooms and associated areas
To be completed by the trust
Date:
Trust
Site
Project / scheme
Building / ward
Project manager for the trust / PCT
Business case or design stage to which this checklist / review applies
Completed by (for trust) Date:
Reviewed by Date:
Notes on scheme by local trust
The checklist has been informed by the Healthcare Commissions 2007 report ‘Investigation into outbreaks of Clostridium difficile at Maidstone and Tunbridge Wells NHS Trust’
General Notes
20
A This checklist is not exhaustive and is not intended to replace or be a substitute for central guidance and legislation. It is purely intended as a check on the more practical elements of the basic design and subsequent management inn relation to business case approval and associated tasks. The local IPC team may have its own specific requirements. Completion or use of this checklist by the designers should NOT be taken as proof of complying with Trust or NHS policies, guidance etc. Checks SHOULD be made for latest possible guidance or legislation is force whenever a design is undertaken.
B Items with an asterisk* below should also be considered in detail with regard to privacy and dignity issues and health and safety aspects (such as lifting and moving patients). See also the ‘Privacy and Dignity’ checklist.
C Although referred to below, this checklist is not intended to review cleaning regimes, clinical processes, clinical prescribing or performance of control of infection procedures.
D Reference is made in several; areas to small items of equipment such as gel dispensers and waste receptacles. Whilst not strictly building – or designed related, these are essential items of which should be allowed for in the design and therefore considered worthy of inclusion in this checklist.
E It is accepted that not all developments incorporate in-patient areas; however every area in a healthcare environment needs to consider infection control. As such, the relevant sections need to be considered and completed or shown as not applicable (N/A).
Part 1. Sign-off
The Control of Infection checklist / review SHOULD be signed off by the relevant parties before the scheme proceeds
Some of the roles below (not CEO) may be covered by a relevant trust director. If appropriate, a single sign-off, clearly stating which areas of responsibility are covered, may suffice.
21
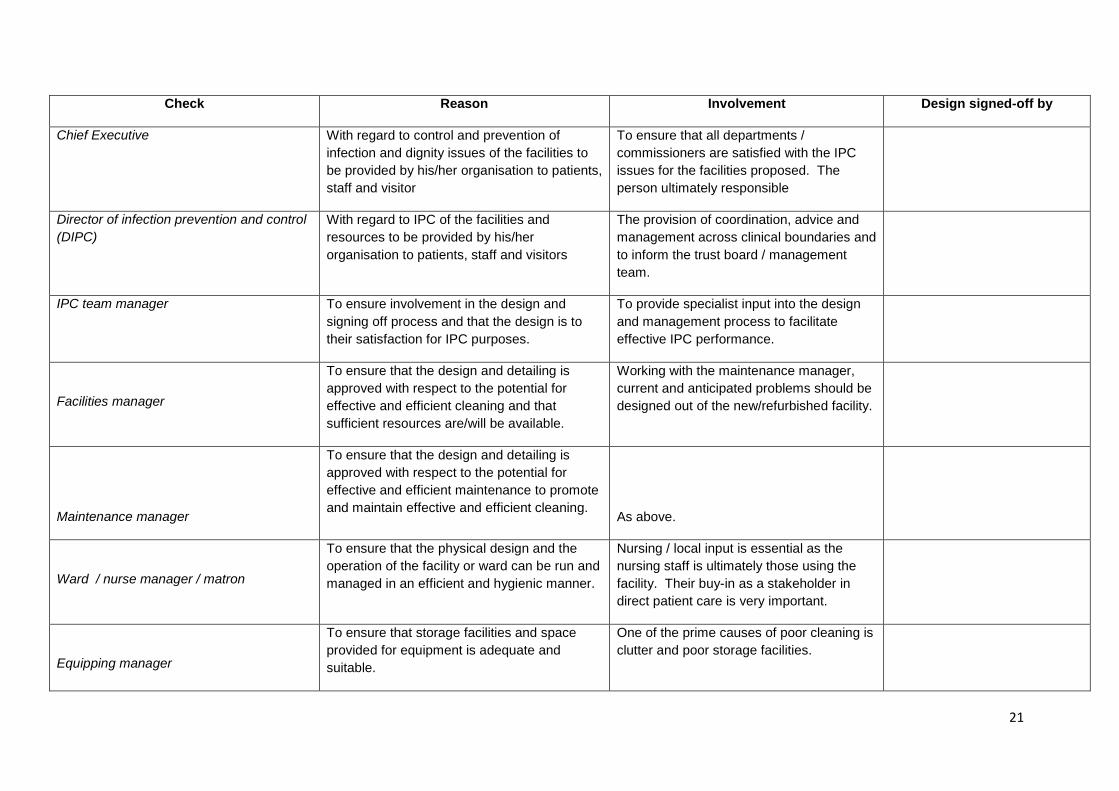
Check Reason Involvement Design signed-off by
Chief Executive With regard to control and prevention of infection and dignity issues of the facilities to be provided by his/her organisation to patients, staff and visitor
To ensure that all departments / commissioners are satisfied with the IPC issues for the facilities proposed. The person ultimately responsible
Director of infection prevention and control (DIPC)
With regard to IPC of the facilities and resources to be provided by his/her organisation to patients, staff and visitors
The provision of coordination, advice and management across clinical boundaries and to inform the trust board / management team.
IPC team manager To ensure involvement in the design and signing off process and that the design is to their satisfaction for IPC purposes.
To provide specialist input into the design and management process to facilitate effective IPC performance.
Facilities manager
To ensure that the design and detailing is approved with respect to the potential for effective and efficient cleaning and that sufficient resources are/will be available.
Working with the maintenance manager, current and anticipated problems should be designed out of the new/refurbished facility.
Maintenance manager
To ensure that the design and detailing is approved with respect to the potential for effective and efficient maintenance to promote and maintain effective and efficient cleaning.
As above.
Ward / nurse manager / matron
To ensure that the physical design and the operation of the facility or ward can be run and managed in an efficient and hygienic manner.
Nursing / local input is essential as the nursing staff is ultimately those using the facility. Their buy-in as a stakeholder in direct patient care is very important.
Equipping manager
To ensure that storage facilities and space provided for equipment is adequate and suitable.
One of the prime causes of poor cleaning is clutter and poor storage facilities.
22
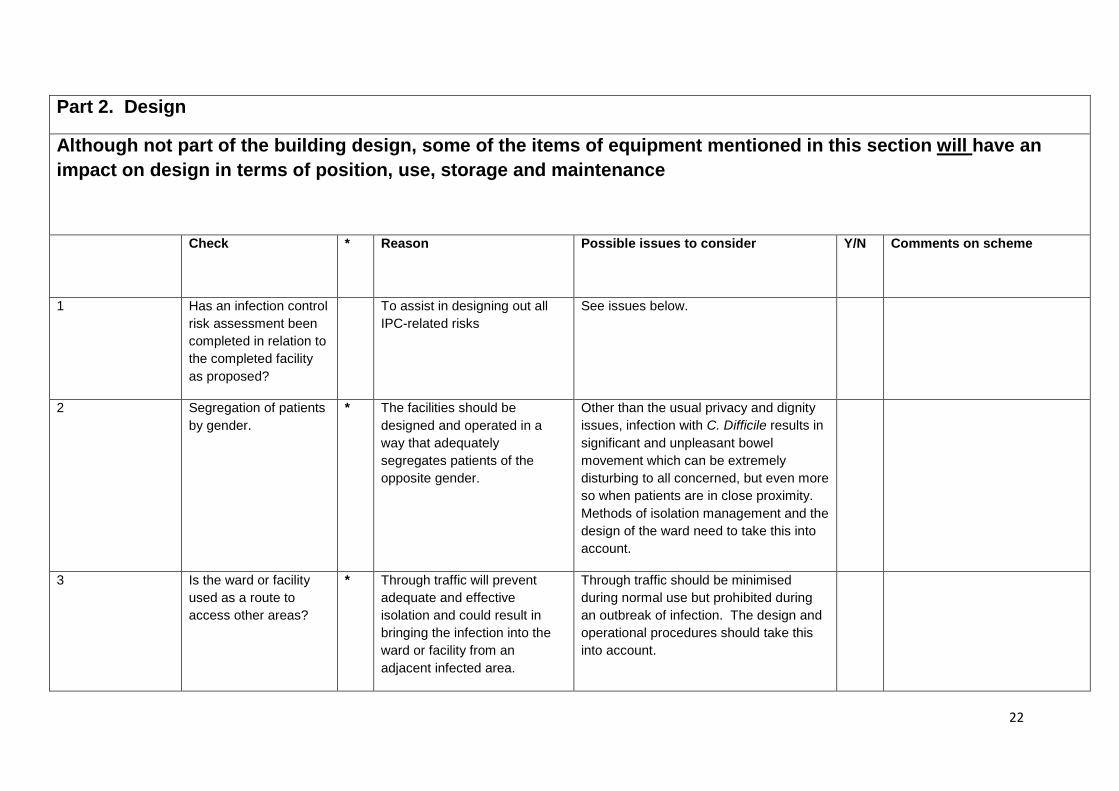
Part 2. Design
Although not part of the building design, some of the items of equipment mentioned in this section will have an impact on design in terms of position, use, storage and maintenance
Check
* Reason Possible issues to consider Y/N Comments on scheme
1 Has an infection control risk assessment been completed in relation to the completed facility as proposed?
To assist in designing out all IPC-related risks
See issues below.
2 Segregation of patients by gender.
* The facilities should be designed and operated in a way that adequately segregates patients of the opposite gender.
Other than the usual privacy and dignity issues, infection with C. Difficile results in significant and unpleasant bowel movement which can be extremely disturbing to all concerned, but even more so when patients are in close proximity. Methods of isolation management and the design of the ward need to take this into account.
3 Is the ward or facility used as a route to access other areas?
* Through traffic will prevent adequate and effective isolation and could result in bringing the infection into the ward or facility from an adjacent infected area.
Through traffic should be minimised during normal use but prohibited during an outbreak of infection. The design and operational procedures should take this into account.
23
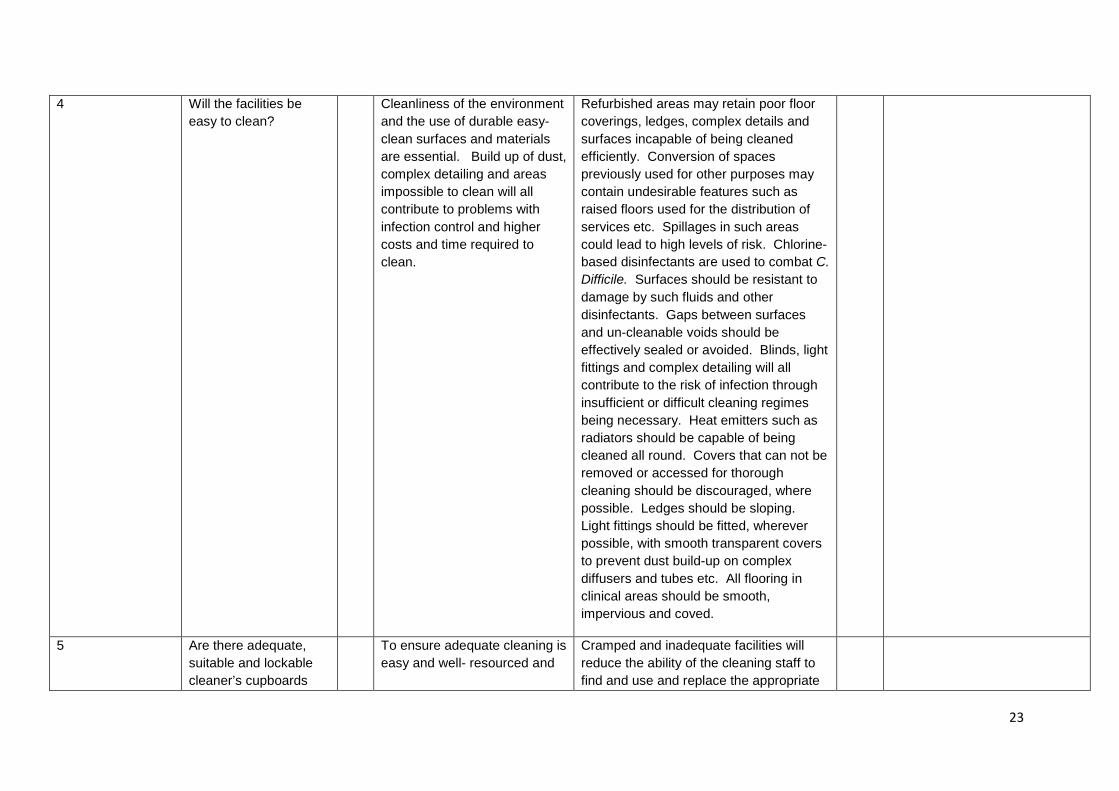
4 Will the facilities be easy to clean?
Cleanliness of the environment and the use of durable easy-clean surfaces and materials are essential. Build up of dust, complex detailing and areas impossible to clean will all contribute to problems with infection control and higher costs and time required to clean.
Refurbished areas may retain poor floor coverings, ledges, complex details and surfaces incapable of being cleaned efficiently. Conversion of spaces previously used for other purposes may contain undesirable features such as raised floors used for the distribution of services etc. Spillages in such areas could lead to high levels of risk. Chlorine-based disinfectants are used to combat C. Difficile. Surfaces should be resistant to damage by such fluids and other disinfectants. Gaps between surfaces and un-cleanable voids should be effectively sealed or avoided. Blinds, light fittings and complex detailing will all contribute to the risk of infection through insufficient or difficult cleaning regimes being necessary. Heat emitters such as radiators should be capable of being cleaned all round. Covers that can not be removed or accessed for thorough cleaning should be discouraged, where possible. Ledges should be sloping. Light fittings should be fitted, wherever possible, with smooth transparent covers to prevent dust build-up on complex diffusers and tubes etc. All flooring in clinical areas should be smooth, impervious and coved.
5 Are there adequate, suitable and lockable cleaner’s cupboards
To ensure adequate cleaning is easy and well- resourced and
Cramped and inadequate facilities will reduce the ability of the cleaning staff to find and use and replace the appropriate
24
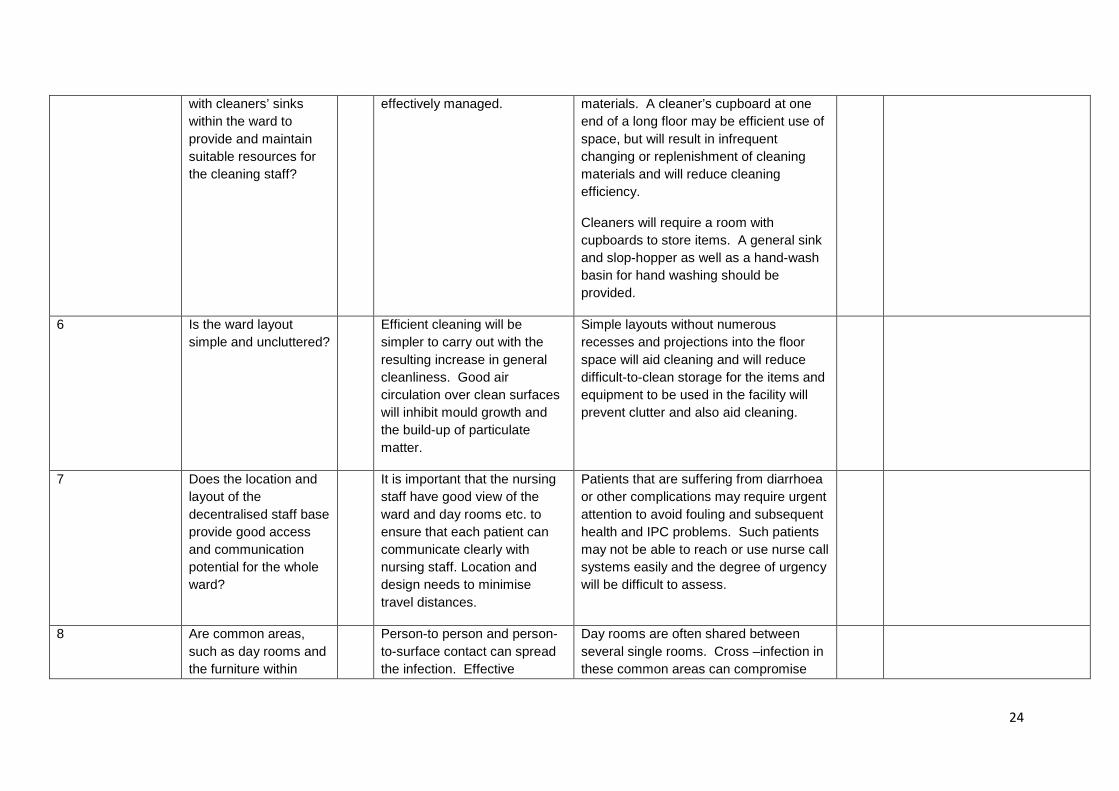
with cleaners’ sinks within the ward to provide and maintain suitable resources for the cleaning staff?
effectively managed. materials. A cleaner’s cupboard at one end of a long floor may be efficient use of space, but will result in infrequent changing or replenishment of cleaning materials and will reduce cleaning efficiency.
Cleaners will require a room with cupboards to store items. A general sink and slop-hopper as well as a hand-wash basin for hand washing should be provided.
6 Is the ward layout simple and uncluttered?
Efficient cleaning will be simpler to carry out with the resulting increase in general cleanliness. Good air circulation over clean surfaces will inhibit mould growth and the build-up of particulate matter.
Simple layouts without numerous recesses and projections into the floor space will aid cleaning and will reduce difficult-to-clean storage for the items and equipment to be used in the facility will prevent clutter and also aid cleaning.
7 Does the location and layout of the decentralised staff base provide good access and communication potential for the whole ward?
It is important that the nursing staff have good view of the ward and day rooms etc. to ensure that each patient can communicate clearly with nursing staff. Location and design needs to minimise travel distances.
Patients that are suffering from diarrhoea or other complications may require urgent attention to avoid fouling and subsequent health and IPC problems. Such patients may not be able to reach or use nurse call systems easily and the degree of urgency will be difficult to assess.
8 Are common areas, such as day rooms and the furniture within
Person-to person and person-to-surface contact can spread the infection. Effective
Day rooms are often shared between several single rooms. Cross –infection in these common areas can compromise
25
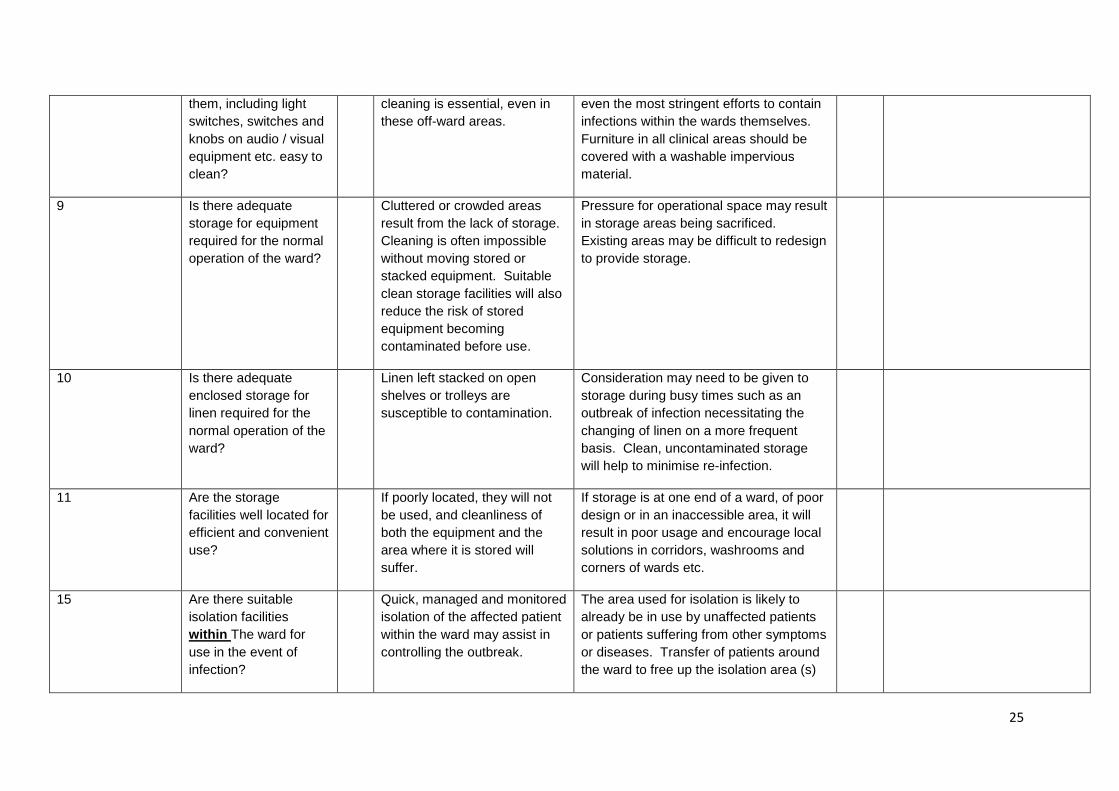
them, including light switches, switches and knobs on audio / visual equipment etc. easy to clean?
cleaning is essential, even in these off-ward areas.
even the most stringent efforts to contain infections within the wards themselves. Furniture in all clinical areas should be covered with a washable impervious material.
9 Is there adequate storage for equipment required for the normal operation of the ward?
Cluttered or crowded areas result from the lack of storage. Cleaning is often impossible without moving stored or stacked equipment. Suitable clean storage facilities will also reduce the risk of stored equipment becoming contaminated before use.
Pressure for operational space may result in storage areas being sacrificed. Existing areas may be difficult to redesign to provide storage.
10 Is there adequate enclosed storage for linen required for the normal operation of the ward?
Linen left stacked on open shelves or trolleys are susceptible to contamination.
Consideration may need to be given to storage during busy times such as an outbreak of infection necessitating the changing of linen on a more frequent basis. Clean, uncontaminated storage will help to minimise re-infection.
11 Are the storage facilities well located for efficient and convenient use?
If poorly located, they will not be used, and cleanliness of both the equipment and the area where it is stored will suffer.
If storage is at one end of a ward, of poor design or in an inaccessible area, it will result in poor usage and encourage local solutions in corridors, washrooms and corners of wards etc.
15 Are there suitable isolation facilities within The ward for use in the event of infection?
Quick, managed and monitored isolation of the affected patient within the ward may assist in controlling the outbreak.
The area used for isolation is likely to already be in use by unaffected patients or patients suffering from other symptoms or diseases. Transfer of patients around the ward to free up the isolation area (s)
26
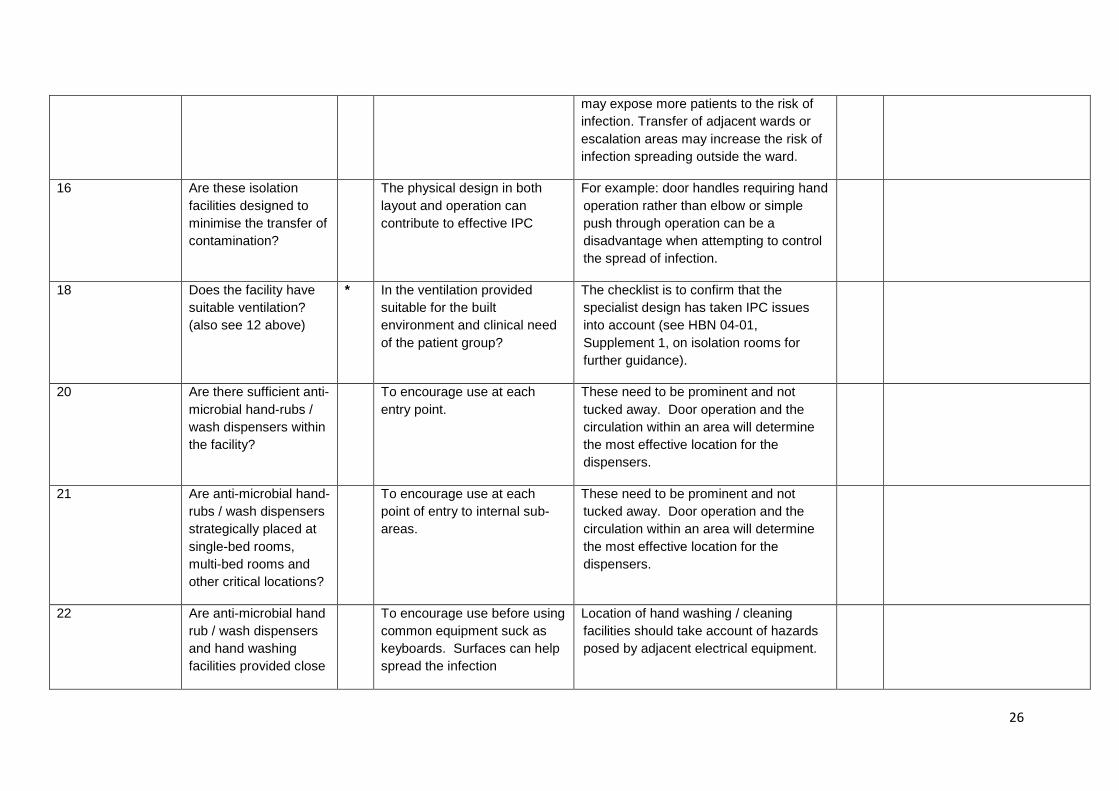
may expose more patients to the risk of infection. Transfer of adjacent wards or escalation areas may increase the risk of infection spreading outside the ward.
16 Are these isolation facilities designed to minimise the transfer of contamination?
The physical design in both layout and operation can contribute to effective IPC
For example: door handles requiring hand operation rather than elbow or simple push through operation can be a disadvantage when attempting to control the spread of infection.
18 Does the facility have suitable ventilation? (also see 12 above)
* In the ventilation provided suitable for the built environment and clinical need of the patient group?
The checklist is to confirm that the specialist design has taken IPC issues into account (see HBN 04-01, Supplement 1, on isolation rooms for further guidance).
20 Are there sufficient anti-microbial hand-rubs / wash dispensers within the facility?
To encourage use at each entry point.
These need to be prominent and not tucked away. Door operation and the circulation within an area will determine the most effective location for the dispensers.
21 Are anti-microbial hand-rubs / wash dispensers strategically placed at single-bed rooms, multi-bed rooms and other critical locations?
To encourage use at each point of entry to internal sub-areas.
These need to be prominent and not tucked away. Door operation and the circulation within an area will determine the most effective location for the dispensers.
22 Are anti-microbial hand rub / wash dispensers and hand washing facilities provided close
To encourage use before using common equipment suck as keyboards. Surfaces can help spread the infection
Location of hand washing / cleaning facilities should take account of hazards posed by adjacent electrical equipment.
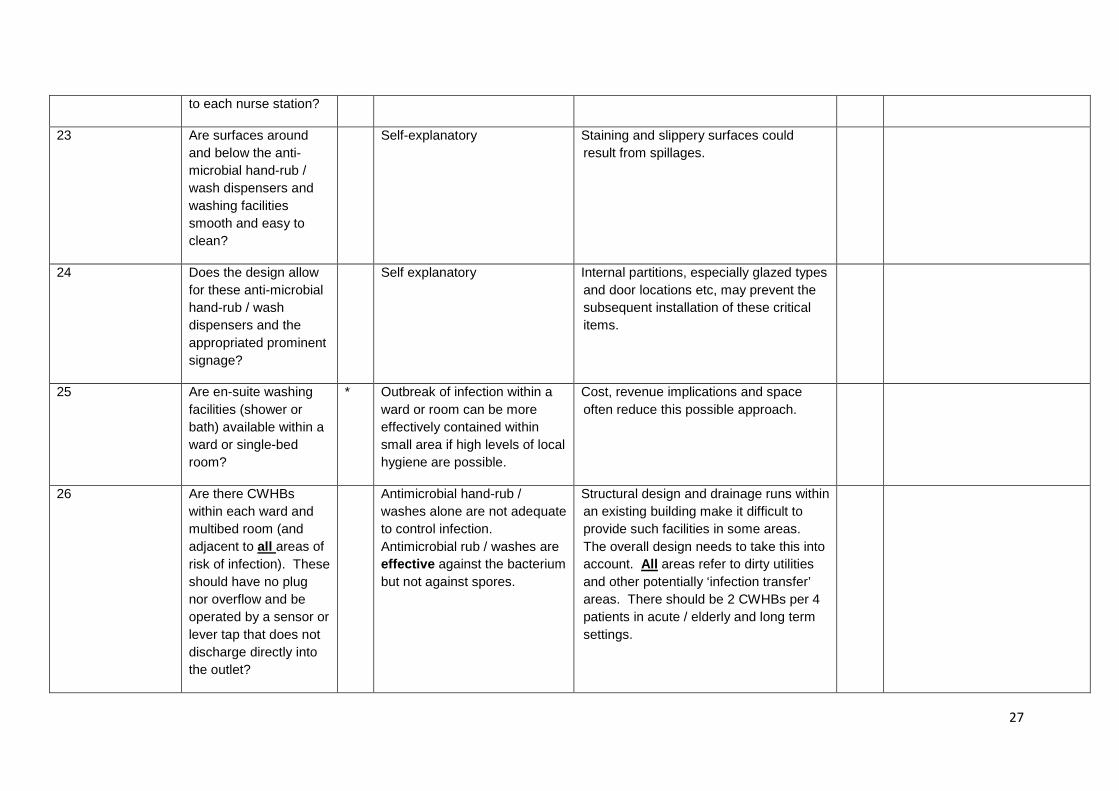
27
to each nurse station?
23 Are surfaces around and below the anti-microbial hand-rub / wash dispensers and washing facilities smooth and easy to clean?
Self-explanatory Staining and slippery surfaces could result from spillages.
24 Does the design allow for these anti-microbial hand-rub / wash dispensers and the appropriated prominent signage?
Self explanatory Internal partitions, especially glazed types and door locations etc, may prevent the subsequent installation of these critical items.
25 Are en-suite washing facilities (shower or bath) available within a ward or single-bed room?
* Outbreak of infection within a ward or room can be more effectively contained within small area if high levels of local hygiene are possible.
Cost, revenue implications and space often reduce this possible approach.
26 Are there CWHBs within each ward and multibed room (and adjacent to all areas of risk of infection). These should have no plug nor overflow and be operated by a sensor or lever tap that does not discharge directly into the outlet?
Antimicrobial hand-rub / washes alone are not adequate to control infection. Antimicrobial rub / washes are effective against the bacterium but not against spores.
Structural design and drainage runs within an existing building make it difficult to provide such facilities in some areas. The overall design needs to take this into account. All areas refer to dirty utilities and other potentially ‘infection transfer’ areas. There should be 2 CWHBs per 4 patients in acute / elderly and long term settings.

28
27 Is the plumbing designed to maintain suitable temperatures for both safety and control of the legionella spp?
To avoid injury from hot water and the potential risk of Legionella within the ward.
Installation of thermostatic valves and the avoidance of ‘dead legs’ (giving rise to standing water in pipe work) in the physical plumbing design.
28 Are there suitable liquid soap dispensers located adjacent to each wash basin?
Self-explanatory Ensure the wall behind the basin and around the soap dispenser is impermeable and easily cleaned. Should be of a wall-mounted cartridge design and not refillable.
29 Are there hygienic hand drying facilities and foot operated bins at all hand-washing locations? In accessible facilities, foot operated lidded bins are not appropriate – are alternatives in place?
Poor hand and lower arm washing may result in contamination being passed on to others through the drying media or the lid of the waste receptacle.
Paper towels, not tear-off rolls, are preferable. Paper towels requires in all clinical areas and toilets.
30 If en-suite toilet and washing facilities are not provided, are there adequate toilets and washing facilities within the ward to be designated for infected used (or more frequent cleaning) to help prevent infection of
Generally self explanatory If segregation of common use toilet facilities (not en-suite within a ward) is the solution during an outbreak of infection, how is this managed and are there processes in place to increase the cleaning regime and monitor the use / cleaning of the facilities?
29
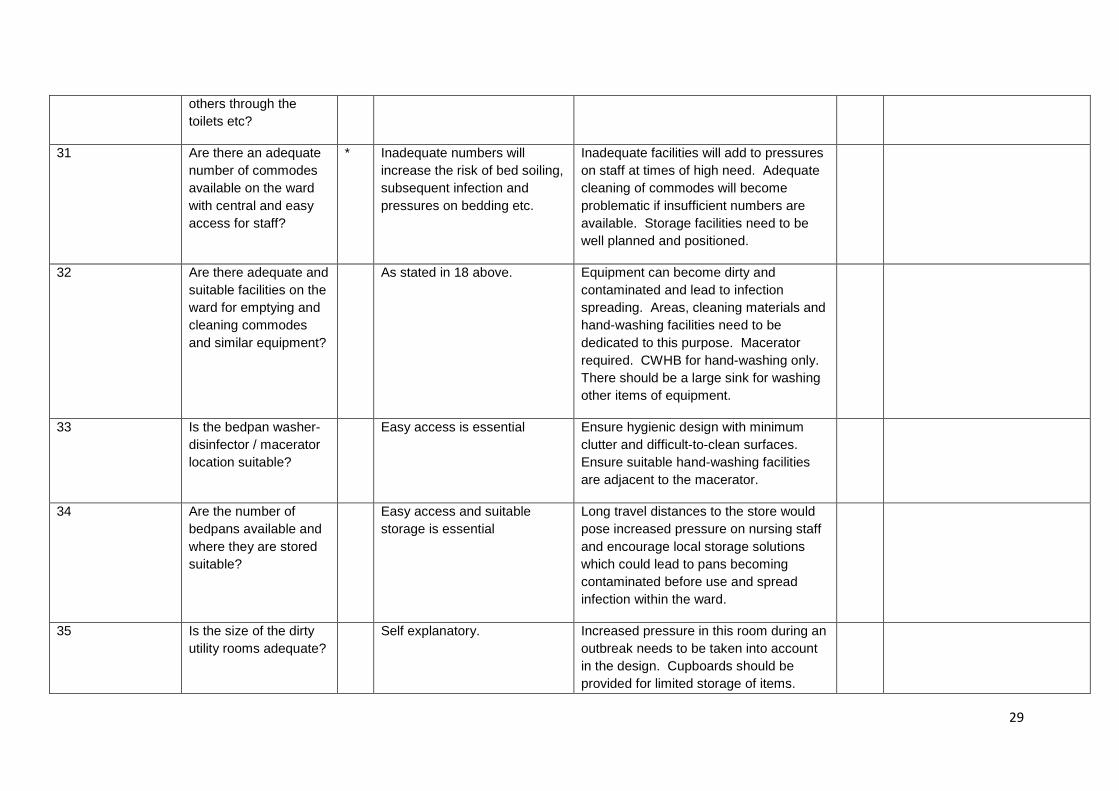
others through the toilets etc?
31 Are there an adequate number of commodes available on the ward with central and easy access for staff?
* Inadequate numbers will increase the risk of bed soiling, subsequent infection and pressures on bedding etc.
Inadequate facilities will add to pressures on staff at times of high need. Adequate cleaning of commodes will become problematic if insufficient numbers are available. Storage facilities need to be well planned and positioned.
32 Are there adequate and suitable facilities on the ward for emptying and cleaning commodes and similar equipment?
As stated in 18 above. Equipment can become dirty and contaminated and lead to infection spreading. Areas, cleaning materials and hand-washing facilities need to be dedicated to this purpose. Macerator required. CWHB for hand-washing only. There should be a large sink for washing other items of equipment.
33 Is the bedpan washer-disinfector / macerator location suitable?
Easy access is essential Ensure hygienic design with minimum clutter and difficult-to-clean surfaces. Ensure suitable hand-washing facilities are adjacent to the macerator.
34 Are the number of bedpans available and where they are stored suitable?
Easy access and suitable storage is essential
Long travel distances to the store would pose increased pressure on nursing staff and encourage local storage solutions which could lead to pans becoming contaminated before use and spread infection within the ward.
35 Is the size of the dirty utility rooms adequate?
Self explanatory. Increased pressure in this room during an outbreak needs to be taken into account in the design. Cupboards should be provided for limited storage of items.
30
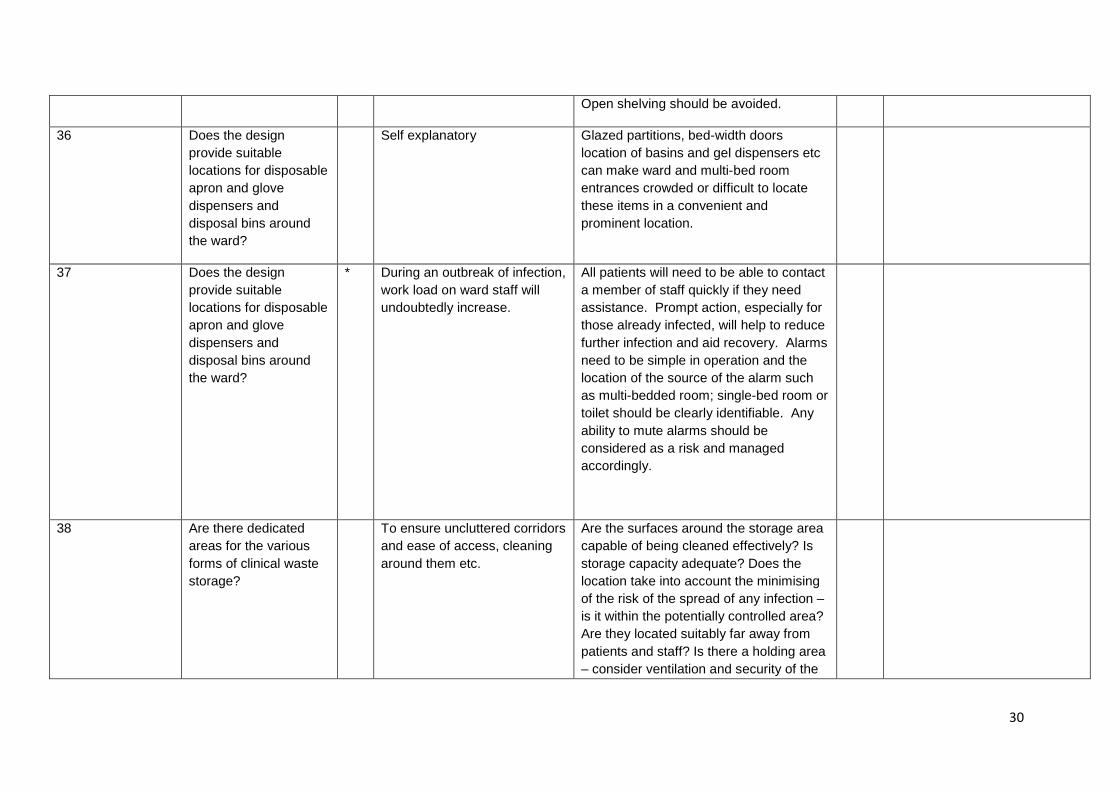
Open shelving should be avoided.
36 Does the design provide suitable locations for disposable apron and glove dispensers and disposal bins around the ward?
Self explanatory Glazed partitions, bed-width doors location of basins and gel dispensers etc can make ward and multi-bed room entrances crowded or difficult to locate these items in a convenient and prominent location.
37 Does the design provide suitable locations for disposable apron and glove dispensers and disposal bins around the ward?
* During an outbreak of infection, work load on ward staff will undoubtedly increase.
All patients will need to be able to contact a member of staff quickly if they need assistance. Prompt action, especially for those already infected, will help to reduce further infection and aid recovery. Alarms need to be simple in operation and the location of the source of the alarm such as multi-bedded room; single-bed room or toilet should be clearly identifiable. Any ability to mute alarms should be considered as a risk and managed accordingly.
38 Are there dedicated areas for the various forms of clinical waste storage?
To ensure uncluttered corridors and ease of access, cleaning around them etc.
Are the surfaces around the storage area capable of being cleaned effectively? Is storage capacity adequate? Does the location take into account the minimising of the risk of the spread of any infection – is it within the potentially controlled area? Are they located suitably far away from patients and staff? Is there a holding area – consider ventilation and security of the
31
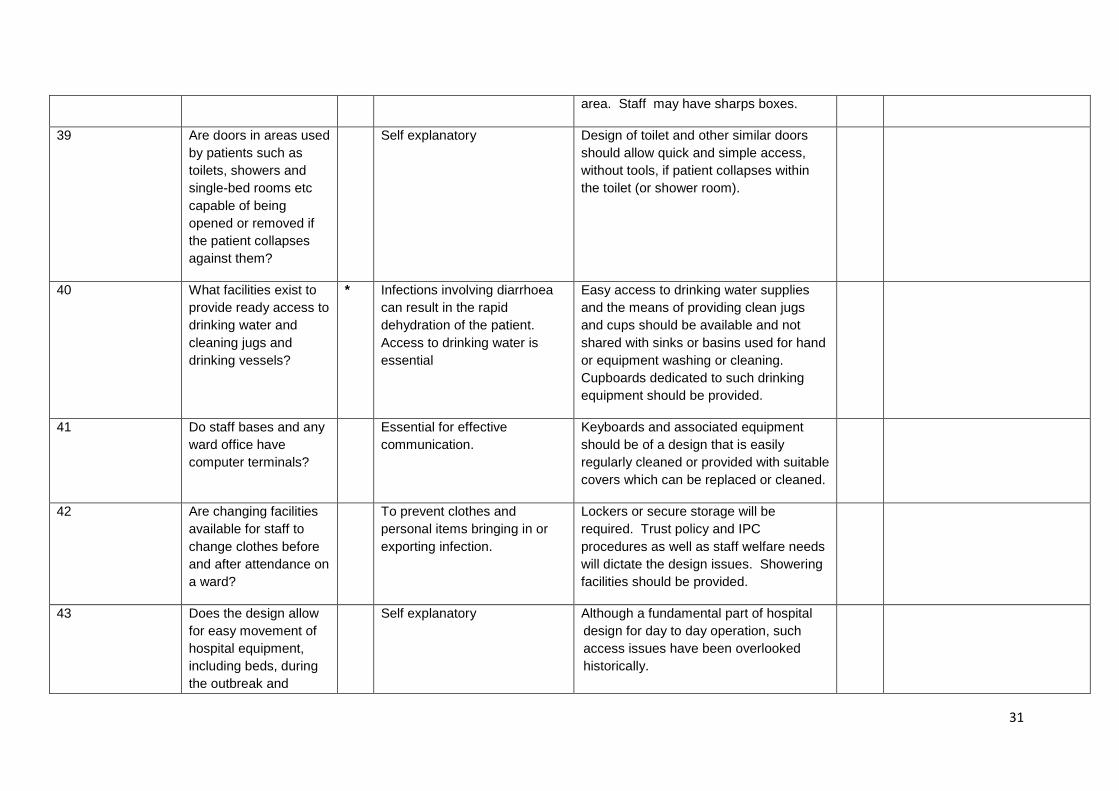
area. Staff may have sharps boxes.
39 Are doors in areas used by patients such as toilets, showers and single-bed rooms etc capable of being opened or removed if the patient collapses against them?
Self explanatory Design of toilet and other similar doors should allow quick and simple access, without tools, if patient collapses within the toilet (or shower room).
40 What facilities exist to provide ready access to drinking water and cleaning jugs and drinking vessels?
* Infections involving diarrhoea can result in the rapid dehydration of the patient. Access to drinking water is essential
Easy access to drinking water supplies and the means of providing clean jugs and cups should be available and not shared with sinks or basins used for hand or equipment washing or cleaning. Cupboards dedicated to such drinking equipment should be provided.
41 Do staff bases and any ward office have computer terminals?
Essential for effective communication.
Keyboards and associated equipment should be of a design that is easily regularly cleaned or provided with suitable covers which can be replaced or cleaned.
42 Are changing facilities available for staff to change clothes before and after attendance on a ward?
To prevent clothes and personal items bringing in or exporting infection.
Lockers or secure storage will be required. Trust policy and IPC procedures as well as staff welfare needs will dictate the design issues. Showering facilities should be provided.
43 Does the design allow for easy movement of hospital equipment, including beds, during the outbreak and
Self explanatory Although a fundamental part of hospital design for day to day operation, such access issues have been overlooked historically.
32
subsequent deep cleaning operation?
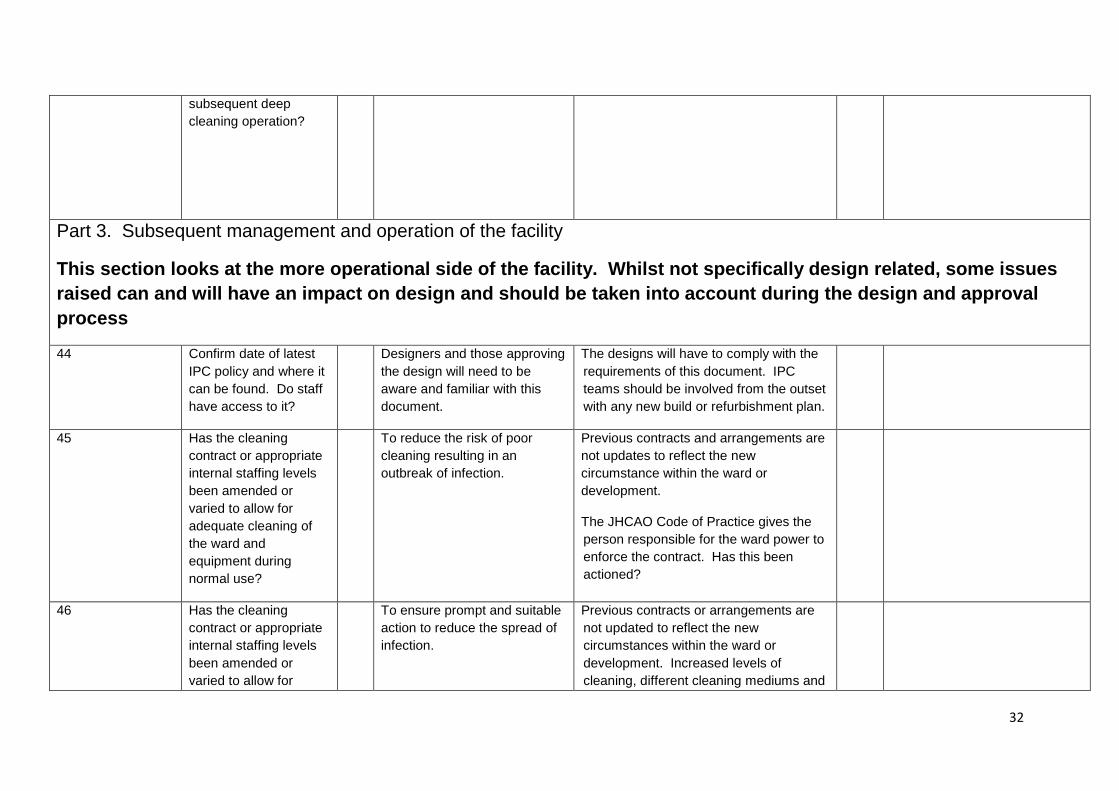
Part 3. Subsequent management and operation of the facility
This section looks at the more operational side of the facility. Whilst not specifically design related, some issues raised can and will have an impact on design and should be taken into account during the design and approval process
44 Confirm date of latest IPC policy and where it can be found. Do staff have access to it?
Designers and those approving the design will need to be aware and familiar with this document.
The designs will have to comply with the requirements of this document. IPC teams should be involved from the outset with any new build or refurbishment plan.
45 Has the cleaning contract or appropriate internal staffing levels been amended or varied to allow for adequate cleaning of the ward and equipment during normal use?
To reduce the risk of poor cleaning resulting in an outbreak of infection.
Previous contracts and arrangements are not updates to reflect the new circumstance within the ward or development.
The JHCAO Code of Practice gives the person responsible for the ward power to enforce the contract. Has this been actioned?
46 Has the cleaning contract or appropriate internal staffing levels been amended or varied to allow for
To ensure prompt and suitable action to reduce the spread of infection.
Previous contracts or arrangements are not updated to reflect the new circumstances within the ward or development. Increased levels of cleaning, different cleaning mediums and
33
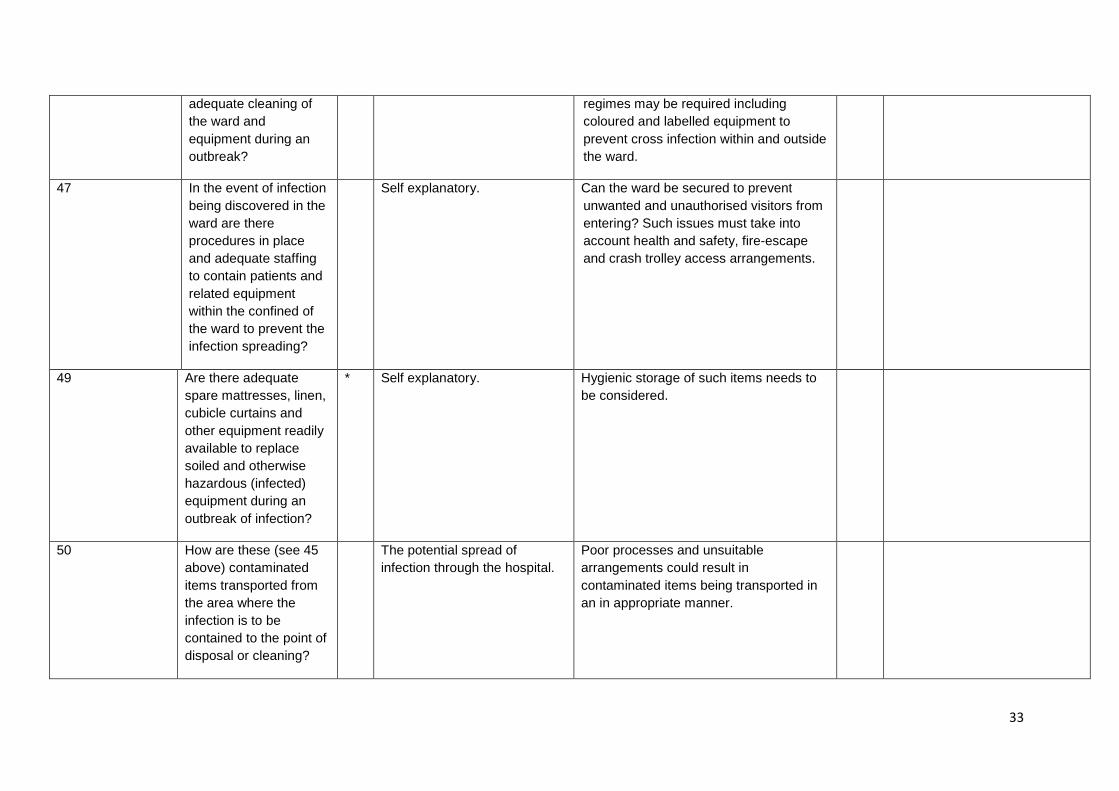
adequate cleaning of the ward and equipment during an outbreak?
regimes may be required including coloured and labelled equipment to prevent cross infection within and outside the ward.
47 In the event of infection being discovered in the ward are there procedures in place and adequate staffing to contain patients and related equipment within the confined of the ward to prevent the infection spreading?
Self explanatory. Can the ward be secured to prevent unwanted and unauthorised visitors from entering? Such issues must take into account health and safety, fire-escape and crash trolley access arrangements.
49 Are there adequate spare mattresses, linen, cubicle curtains and other equipment readily available to replace soiled and otherwise hazardous (infected) equipment during an outbreak of infection?
* Self explanatory. Hygienic storage of such items needs to be considered.
50 How are these (see 45 above) contaminated items transported from the area where the infection is to be contained to the point of disposal or cleaning?
The potential spread of infection through the hospital.
Poor processes and unsuitable arrangements could result in contaminated items being transported in an in appropriate manner.
34
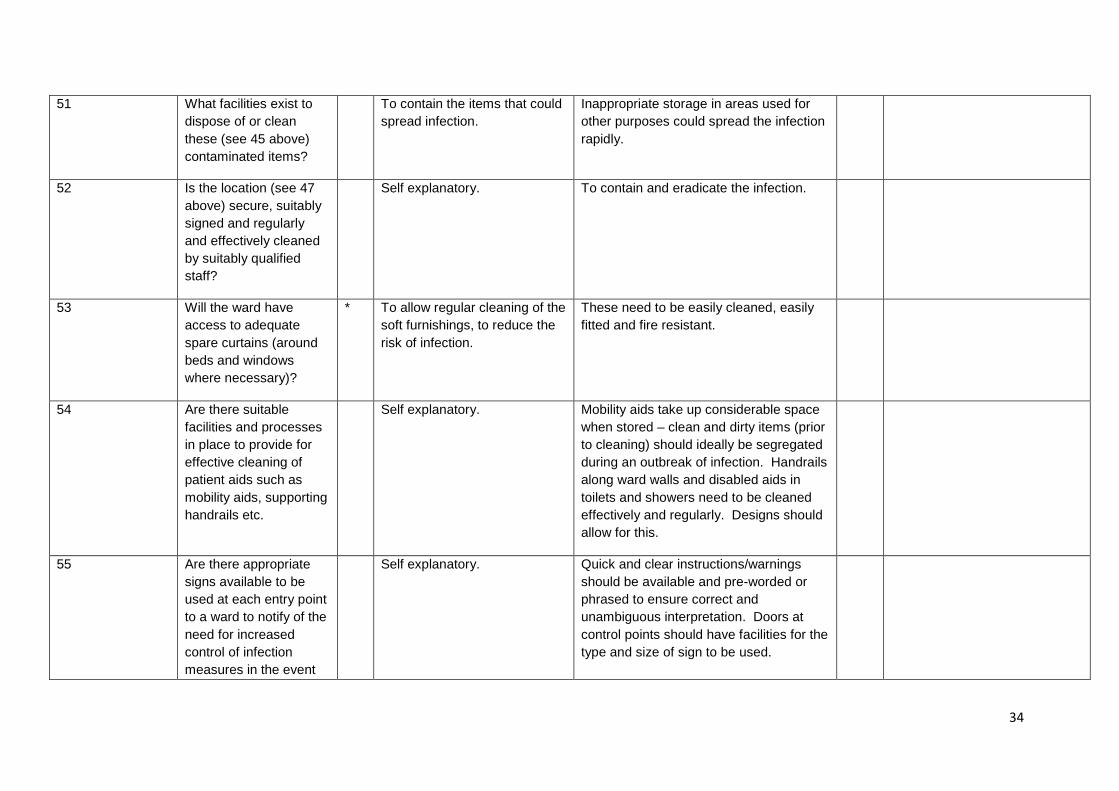
51 What facilities exist to dispose of or clean these (see 45 above) contaminated items?
To contain the items that could spread infection.
Inappropriate storage in areas used for other purposes could spread the infection rapidly.
52 Is the location (see 47 above) secure, suitably signed and regularly and effectively cleaned by suitably qualified staff?
Self explanatory. To contain and eradicate the infection.
53 Will the ward have access to adequate spare curtains (around beds and windows where necessary)?
* To allow regular cleaning of the soft furnishings, to reduce the risk of infection.
These need to be easily cleaned, easily fitted and fire resistant.
54 Are there suitable facilities and processes in place to provide for effective cleaning of patient aids such as mobility aids, supporting handrails etc.
Self explanatory. Mobility aids take up considerable space when stored – clean and dirty items (prior to cleaning) should ideally be segregated during an outbreak of infection. Handrails along ward walls and disabled aids in toilets and showers need to be cleaned effectively and regularly. Designs should allow for this.
55 Are there appropriate signs available to be used at each entry point to a ward to notify of the need for increased control of infection measures in the event
Self explanatory. Quick and clear instructions/warnings should be available and pre-worded or phrased to ensure correct and unambiguous interpretation. Doors at control points should have facilities for the type and size of sign to be used.
35
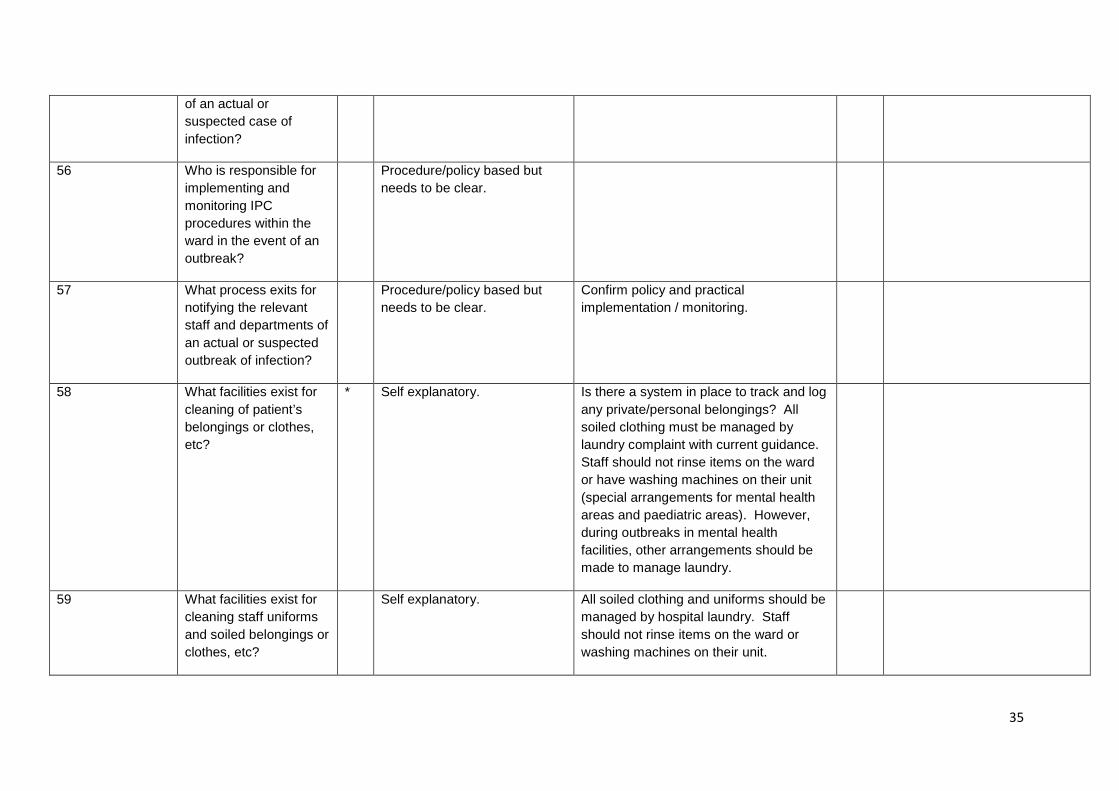
of an actual or suspected case of infection?
56 Who is responsible for implementing and monitoring IPC procedures within the ward in the event of an outbreak?
Procedure/policy based but needs to be clear.
57 What process exits for notifying the relevant staff and departments of an actual or suspected outbreak of infection?
Procedure/policy based but needs to be clear.
Confirm policy and practical implementation / monitoring.
58 What facilities exist for cleaning of patient’s belongings or clothes, etc?
* Self explanatory. Is there a system in place to track and log any private/personal belongings? All soiled clothing must be managed by laundry complaint with current guidance. Staff should not rinse items on the ward or have washing machines on their unit (special arrangements for mental health areas and paediatric areas). However, during outbreaks in mental health facilities, other arrangements should be made to manage laundry.
59 What facilities exist for cleaning staff uniforms and soiled belongings or clothes, etc?
Self explanatory. All soiled clothing and uniforms should be managed by hospital laundry. Staff should not rinse items on the ward or washing machines on their unit.
36
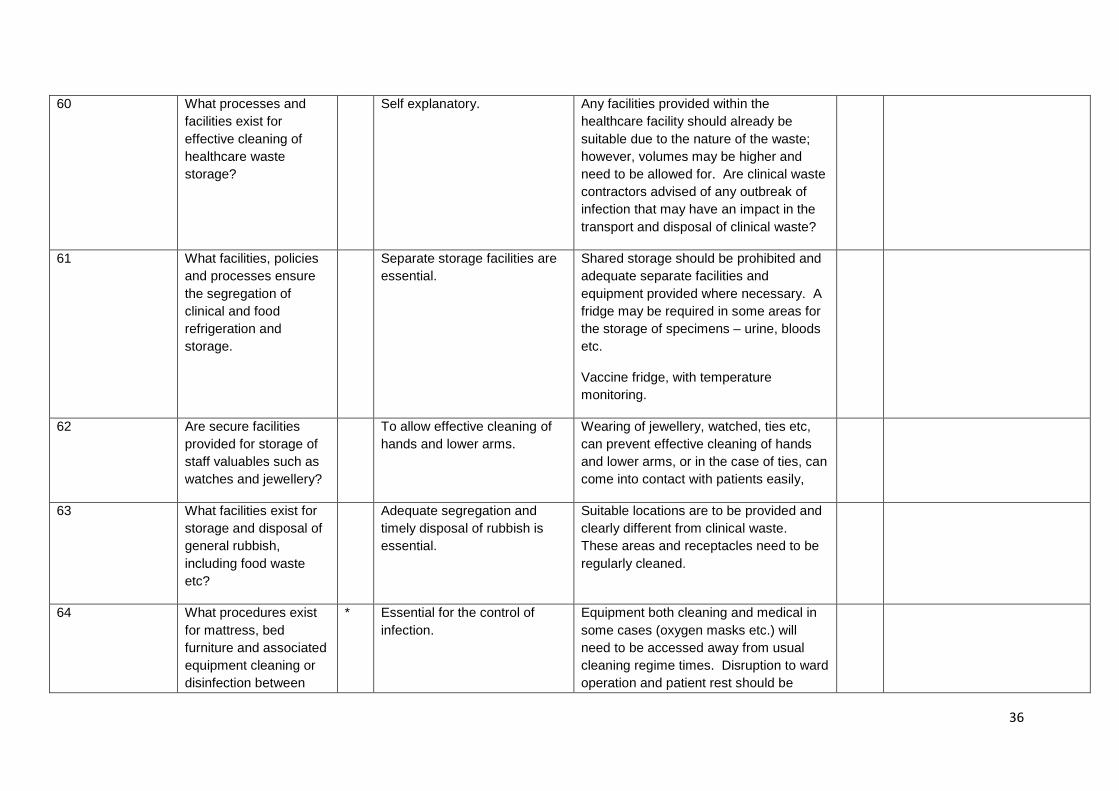
60 What processes and facilities exist for effective cleaning of healthcare waste storage?
Self explanatory. Any facilities provided within the healthcare facility should already be suitable due to the nature of the waste; however, volumes may be higher and need to be allowed for. Are clinical waste contractors advised of any outbreak of infection that may have an impact in the transport and disposal of clinical waste?
61 What facilities, policies and processes ensure the segregation of clinical and food refrigeration and storage.
Separate storage facilities are essential.
Shared storage should be prohibited and adequate separate facilities and equipment provided where necessary. A fridge may be required in some areas for the storage of specimens – urine, bloods etc.
Vaccine fridge, with temperature monitoring.
62 Are secure facilities provided for storage of staff valuables such as watches and jewellery?
To allow effective cleaning of hands and lower arms.
Wearing of jewellery, watched, ties etc, can prevent effective cleaning of hands and lower arms, or in the case of ties, can come into contact with patients easily,
63 What facilities exist for storage and disposal of general rubbish, including food waste etc?
Adequate segregation and timely disposal of rubbish is essential.
Suitable locations are to be provided and clearly different from clinical waste. These areas and receptacles need to be regularly cleaned.
64 What procedures exist for mattress, bed furniture and associated equipment cleaning or disinfection between
* Essential for the control of infection.
Equipment both cleaning and medical in some cases (oxygen masks etc.) will need to be accessed away from usual cleaning regime times. Disruption to ward operation and patient rest should be
37
uses by different patients, especially at night? (Terminal cleaning after patients vacates bed?
minimised. Location and type of cleaning equipment should be considered.
All furniture should be covered with a washable impervious material.
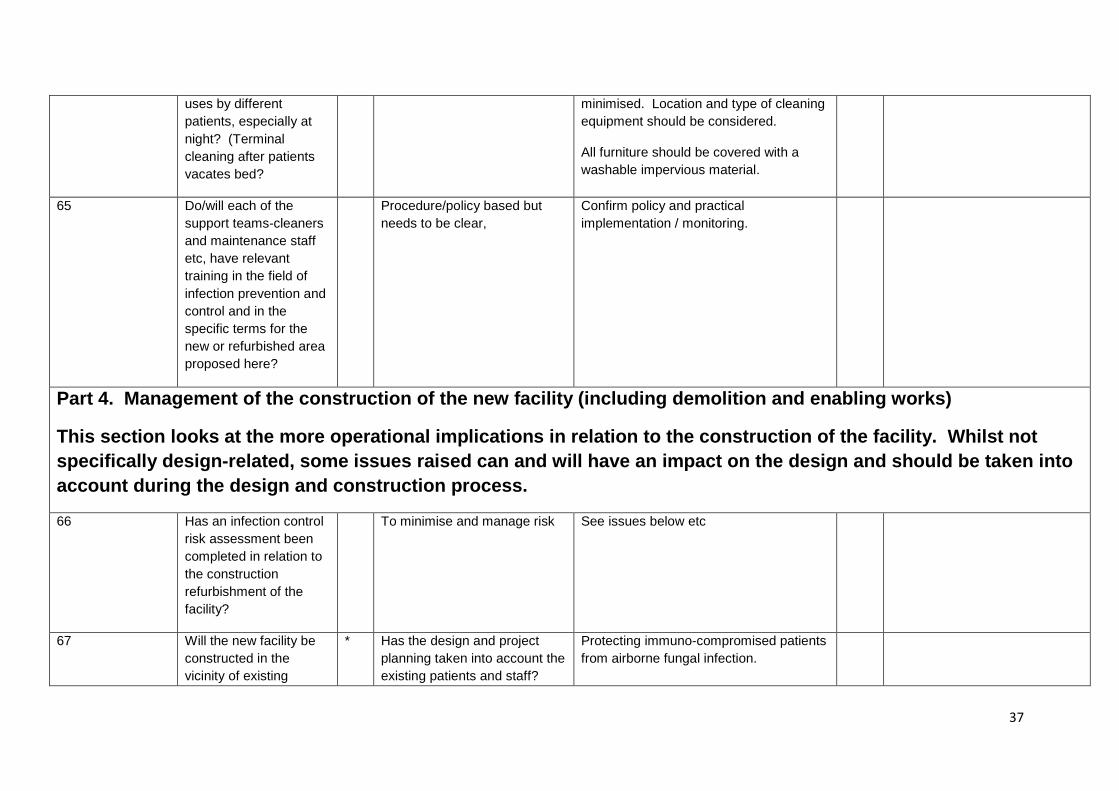
65 Do/will each of the support teams-cleaners and maintenance staff etc, have relevant training in the field of infection prevention and control and in the specific terms for the new or refurbished area proposed here?
Procedure/policy based but needs to be clear,
Confirm policy and practical implementation / monitoring.
Part 4. Management of the construction of the new facility (including demolition and enabling works)
This section looks at the more operational implications in relation to the construction of the facility. Whilst not specifically design-related, some issues raised can and will have an impact on the design and should be taken into account during the design and construction process.
66 Has an infection control risk assessment been completed in relation to the construction refurbishment of the facility?
To minimise and manage risk See issues below etc
67 Will the new facility be constructed in the vicinity of existing
* Has the design and project planning taken into account the existing patients and staff?
Protecting immuno-compromised patients from airborne fungal infection.
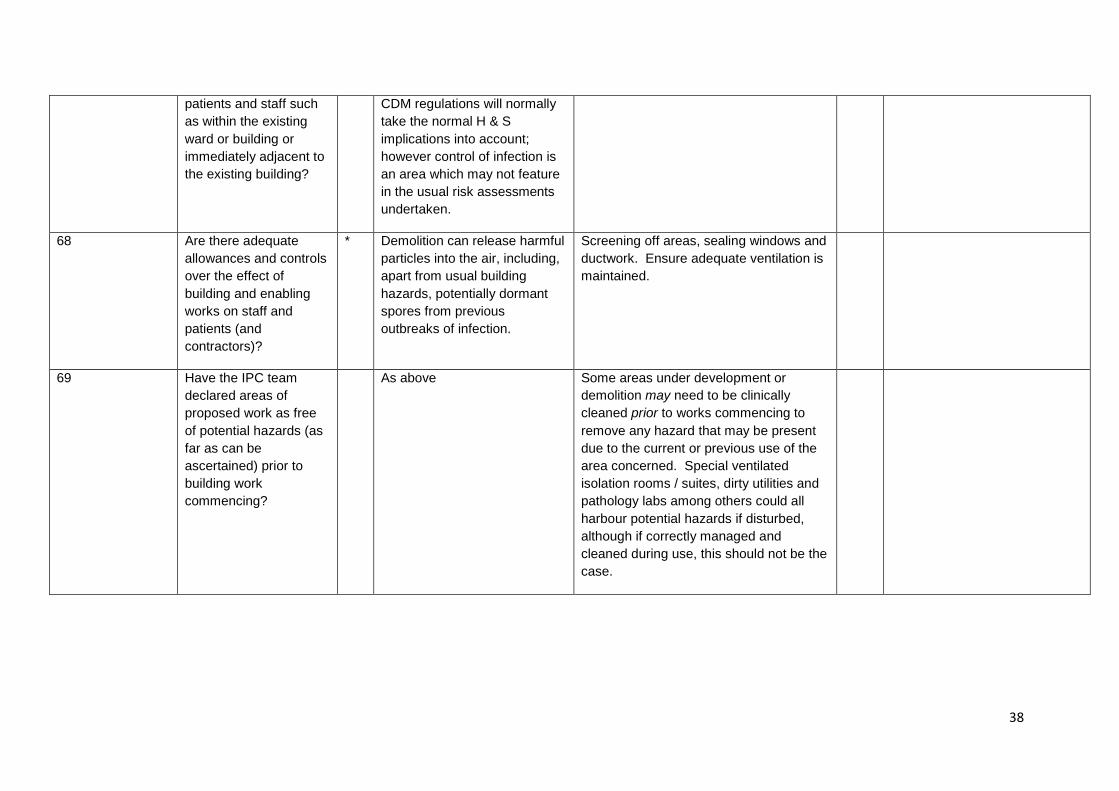
38
patients and staff such as within the existing ward or building or immediately adjacent to the existing building?
CDM regulations will normally take the normal H & S implications into account; however control of infection is an area which may not feature in the usual risk assessments undertaken.
68 Are there adequate allowances and controls over the effect of building and enabling works on staff and patients (and contractors)?
* Demolition can release harmful particles into the air, including, apart from usual building hazards, potentially dormant spores from previous outbreaks of infection.
Screening off areas, sealing windows and ductwork. Ensure adequate ventilation is maintained.
69 Have the IPC team declared areas of proposed work as free of potential hazards (as far as can be ascertained) prior to building work commencing?
As above Some areas under development or demolition may need to be clinically cleaned prior to works commencing to remove any hazard that may be present due to the current or previous use of the area concerned. Special ventilated isolation rooms / suites, dirty utilities and pathology labs among others could all harbour potential hazards if disturbed, although if correctly managed and cleaned during use, this should not be the case.

39
40