clinical evidence of parietal cortex dysfunction and correlation … · clinical evidence of...
TRANSCRIPT
ORIGINAL ARTICLE
Clinical evidence of parietal cortex dysfunction and correlationwith extent of allodynia in CRPS type 1H. Cohen1,2,3, C. McCabe1,5, N. Harris3,4, J. Hall1,5, J. Lewis1, D.R. Blake1,3
1 Royal National Orthopaedic Hospital, Stanmore, UK
2 The Royal National Hospital for Rheumatic Diseases, Bath, UK
3 University of Bath, UK
4 Bath Institute of Medical Engineering, UK
5 University of the West of England, Bristol, UK
CorrespondenceHelen Cohen
E-mail: [email protected]
Funding sourcesDr Cohen was supported by Arthritis
Research UK (Grant No. 17573).
Conflicts of interestNo conflict of Interest has been declared by
the authors.
Accepted for publication23 July 2012
doi:10.1002/j.1532-2149.2012.00213.x
Abstract
Background: Unusual symptoms such as digit misidentification andneglect-like phenomena have been reported in complex regional painsyndrome (CRPS), which we hypothesized could be explained by parietallobe dysfunction.Methods: Twenty-two patients with chronic CRPS attending anin-patient rehabilitation programme underwent standard neurologicalexamination followed by clinical assessment of parietal lobe functionand detailed sensory testing.Results: Fifteen (68%) patients had evidence of parietal lobe dysfunction.Six (27%) subjects failed six or more test categories and demonstrated newclinical signs consistent with their parietal testing impairments, whichwere impacting significantly on activities of daily living. A higher incidencewas noted in subjects with >1 limb involvement, CRPS affecting thedominant side and in left-handed subjects.
Eighteen patients (82%) had mechanical allodynia covering 3–57.5% ofthe body surface area. Allochiria (unilateral tactile stimulation perceivedonly in the analogous location on the opposite limb), sensory extinction(concurrent bilateral tactile stimulation perceived only in one limb),referred sensations (unilateral tactile stimulation perceived concurrently inanother discrete body area) and dysynchiria (unilateral non-noxioustactile stimulation perceived bilaterally as noxious) were present in somepatients. Greater extent of body surface allodynia was correlated withworse parietal function (Spearman’s rho = -0.674, p = 0.001).Conclusion: In patients with chronic CRPS, detailed clinical examinationmay reveal parietal dysfunction, with severity relating to the extent ofallodynia.
1. Introduction
Complex regional pain syndrome (CRPS) can arisesecondarily to trauma and spontaneously in theabsence of injury or inflammation. Many differentmechanisms may drive the pain, and there is increas-ing evidence for the role of central mechanisms(Marinus et al., 2011).
CRPS patients may complain of symptoms such asfeelings of ‘foreignness’ (Förderreuther et al., 2004),distorted body image (Moseley, 2005) and body dys-morphic features (Lewis et al., 2007). Neglect-like phe-nomena (Galer and Jensen, 1999), dysexecutive andglobal cognitive processing impairment (Libon et al.,2010), and finger misidentification (Förderreutheret al., 2004) have been reported. Deficits in tactile
527Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters

processing of the affected limb can be defined by thespace in which the limb resides, suggesting that a typeof spatial neglect may occur in CRPS (Moseley et al.,2009). This constellation of symptoms and signs isreminiscent of those seen in patients with parietal lobelesions (e.g., hemineglect, dyspraxia, somatoparaphre-nia; denial of ownership of a limb).
Evidence is emerging for the role of the parietalcortex in the neurocognitive dysfunction observed inCRPS (Maihofner and Peltz, 2011). Functional mag-netic resonance imaging studies suggest involvementof posterior (Maihöfner et al., 2007) and inferior(Gieteling et al., 2008) parietal cortex in motor dys-function. Positron emission tomography (PET)studies have shown increased regional blood flow inthe parietal cortex (Shiraishi et al., 2006; Wu et al.,2006), which decreased after treatment (Wu et al.,2006). Magnetoencephalography responses duringtactile processing showed defective posterior parietalcortex (PPC) activation, with the authors suggestingthat this might be associated with neglect-like symp-toms (Vartiainen et al., 2008). PPC involvement hasalso been implicated in studies of functional imagingof allodynia (Maihöfner et al., 2006), and is sug-gested by work showing impaired function on alaterality task (Schwoebel et al., 2001; Moseley,2005) or with estimation of hand size (Peltz et al.,2011).
Studies using different techniques have demon-strated evidence of representational change in CRPS(Juottonen et al., 2002; Vartiainen et al., 2008). Neu-roplastic cortical reorganization correlates with the
intensity of CRPS pain and the extent of mechanicalhyperalgesia (Maihöfner et al., 2003), with mean painintensity (Pleger et al., 2004) and with tactile impair-ment (Pleger et al., 2006). The parietal cortex isinvolved in the perception of pain (Duncan andAlbanese, 2003), particularly in the region of thelateral sulcus (sylvian fissure) (Treede et al., 2000).Other work has demonstrated parallel processing ofnociceptive information in the primary SI and second-ary SII somatosensory cortex (Lin and Forss, 2002;Liang et al., 2011) and in the somatotopic organizationof pain in SI and SII (Bingel et al., 2004).
We postulated that in CRPS, cortical network dis-ruption may involve the parietal cortex; such patientsmay have greater neuroplastic representationalchanges. We hypothesized that some CRPS patientswould (1) demonstrate clinical evidence of parietallobe dysfunction and (2) CRPS patients with parietaldysfunction would have more extensive areas ofmechanical allodynia.
2. Methods
2.1 Participants
Consecutive CRPS patients attending a 2-weekin-patient rehabilitation programme at the RoyalNational Hospital for Rheumatic Diseases, Bath, UK,underwent sensory testing and detailed clinical assess-ment of parietal function. The sample size reported isbased on the number of subjects available within a6-month data collection period. All patients fulfilledInternational Association for the Study of Pain (IASP)diagnostic criteria for CRPS (Harden et al., 2007). Allpatients provided informed consent to participation inan overarching study into sensory integration, proprio-ception and autonomic responses in CRPS, which hadfull local ethics clearance (see Supporting InformationMethods S1). No patient had any other concurrentpathology that might impair sensation or higher centralperception of sensory stimuli (e.g., peripheral neuropa-thy, multiple sclerosis, prior history of cerebrovascularaccident) or significant visual impairment.
All the clinical testing was performed by one exam-iner (H. Cohen). The subject was seated comfortably,and told that they were undertaking a series of tests toexplore how well a particular part of the brain wasworking. It was explained that as this brain area isinvolved with putting a variety of different sensoryinformation together to make sense of our surround-ings, it would involve testing language, numeracy,drawing, touch and sense of body location.
What’s already known about this topic?• There is increasing neuroimaging evidence of
parietal lobe involvement in complex regionalpain syndrome (CRPS).
• Severe tactile allodynia and unusual symptomssuch as body dysmorphia and finger agnosiahave also been documented.
What does this study add?• Clinical evidence was found for parietal lobe
dysfunction in chronic CRPS.• Cortical network dysfunction in CRPS may
involve parietal areas, and could provide a ratio-nal explanation for otherwise unusual symptomsand signs.
• The extent of tactile allodynia correlated withthe severity of parietal dysfunction, suggesting arole for maladaptive neuroplasticity.
Parietal lobe dysfunction in CRPS H. Cohen et al.
528 Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters
2.2 Clinical method
2.2.1 Sensory testing: tactile thresholds/screeningfor allodynia
For full testing protocol details, see Supporting Infor-mation Methods S1.
Semmes–Weinstein (SW) filaments were used toassess tactile thresholds and body areas affected bymechanical allodynia. Hyperaesthesia was defined aswhen the tactile threshold was lower on the affectedside and hypoaesthesia when it was higher. Allodyniawas defined as when a given normally non-noxiousSW filament (0.008–2 g target force; light touchrange) was reported as being painful on the affectedside and non-painful on the unaffected side. Forpatients in whom tactile stimulation with normallynon-noxious SW filaments was reported as painfulbilaterally, this was also classified as allodynic.
Allodynic areas were mapped onto a ‘Lund andBrowder’ (1944) burns chart to allow for quantifica-tion of the percentage of body surface area (%BSA)affected.
2.2.2 Parietal lobe testing
For full testing protocol details, see Supporting Infor-mation Methods S1.
During clinical appraisal of parietal lobe function,healthy controls do not make consistent mistakesacross multiple categories of testing. Minor infrequenterrors may occur due to distraction. Therefore, inorder to fail a test where a series of stimuli were given,the patient was allowed three mistakes in total beforebeing deemed to have failed that test. This allowed formistakes due to distraction or loss of concentration. Apatient who failed one or more tests within a categorywas classified as having failed that category.
Each subject performed a testing battery for each ofthe following categories:(1) Interlocking fingers screen (Moo et al., 2003).(2) Ideomotor apraxia (inability to correctly imitate
hand gestures and voluntarily pantomime tool use).(3) Conduction and nominal aphasia (intact
auditory comprehension but poor speech repetition;difficulty with recalling words or names).(4) Agraphia/alexia (inability to write and spell
when writing; inability to read).(5) Acalculia (inability to perform mathematical cal-
culations such as adding, subtracting, multiplying orstating which of two numbers is larger).(6) Astereognosis (inability to identify an object by
touch without visual input).
(7) Finger agnosia (inability to distinguish, name orrecognize the fingers with the patient’s own fingers,the fingers of others, and drawing and other represen-tations of fingers).(8) Dysgraphaesthesia (inability to recognize
numbers or letters traced on to the skin of the hand).(9) Right/left (R/L) disorientation (inability to distin-
guish right from left).(10) Constructional apraxia (inability to copy draw-ings or to manipulate objects to form patterns ordesigns).
2.3 Data analysis
2.3.1 Sensory testing
The percentage body surface area affected by allodyniawas calculated from the mapped mannequin using aLund and Browder burns chart.
2.3.2 Parietal testing
Two outcomes were recorded: (1) total test score (foreach test performed without error, a score of one pointwas allocated; the maximum total possible score accu-mulated across all 10 categories was 116 points);(2) category score/10 (the number of testing categoriespassed). Patients were classified as having parietal dys-function if they failed one or more of the 10 testingcategories.
The data are presented as percentages (actualnumber of subjects) and median values. Statisticalanalysis utilized non-parametric tests. For comparisonbetween subjects with and without parietal dysfunc-tion, the Mann–Whitney test was used, and for corre-lation analysis, the Spearman’s rho test.
3. Results
3.1 Patient demographics
Twenty-two patients (17 female) were assessed. Themean age was 45 years, range 27–63 years and meanCRPS duration 6.8 years, range 1–18 years (seeTable 1). Of the total cohort, 64% (n = 14) were onopiate medication, 64% (14) on neuromodulatory/antidepressant drugs and 41% (9) on both (Table 1).
Nine subjects had CRPS in an upper extremity, ninein a lower extremity, and four in an upper and lowerextremity. Ten had CRPS on the right side, 11 on theleft and 1 on both sides. Six patients reported that theywere left-handed, 15 right-handed and 1 ambidex-trous (Table 2).
H. Cohen et al. Parietal lobe dysfunction in CRPS
529Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters
Twelve patients had undergone brain imagingas part of their workup prior to referral to ourcentre, which did not demonstrate any significantabnormality.
3.2 Sensory testing
There was mechanical allodynia in 82% (n = 18) ofCRPS patients. The %BSA affected by allodyniaranged from 3% to 57.5%, with the median%BSA = 16% (Table 2). The area of sensory impair-ment was confined to the affected limb in 41% (9) andextended beyond the limb in 59% (13). There was nosignificant correlation between %BSA and diseaseduration.
The tactile threshold on the affected limb comparedwith the unaffected limb was lower (hyperaesthesia)
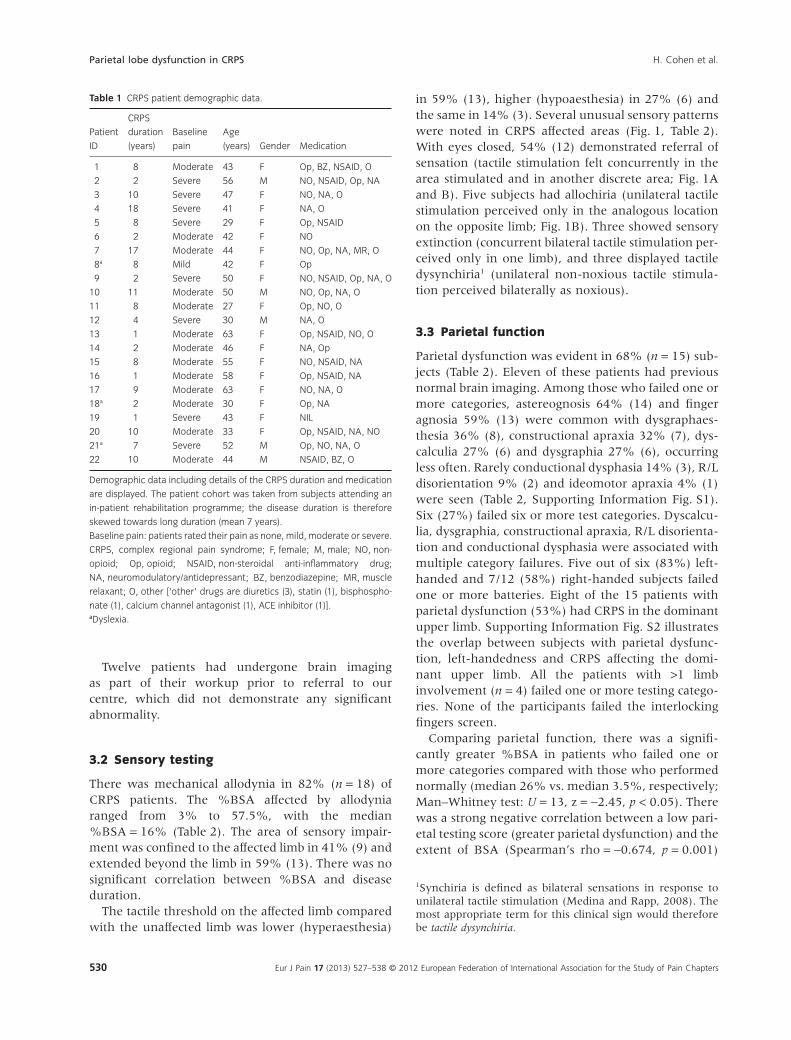
in 59% (13), higher (hypoaesthesia) in 27% (6) andthe same in 14% (3). Several unusual sensory patternswere noted in CRPS affected areas (Fig. 1, Table 2).With eyes closed, 54% (12) demonstrated referral ofsensation (tactile stimulation felt concurrently in thearea stimulated and in another discrete area; Fig. 1Aand B). Five subjects had allochiria (unilateral tactilestimulation perceived only in the analogous locationon the opposite limb; Fig. 1B). Three showed sensoryextinction (concurrent bilateral tactile stimulation per-ceived only in one limb), and three displayed tactiledysynchiria1 (unilateral non-noxious tactile stimula-tion perceived bilaterally as noxious).
3.3 Parietal function
Parietal dysfunction was evident in 68% (n = 15) sub-jects (Table 2). Eleven of these patients had previousnormal brain imaging. Among those who failed one ormore categories, astereognosis 64% (14) and fingeragnosia 59% (13) were common with dysgraphaes-thesia 36% (8), constructional apraxia 32% (7), dys-calculia 27% (6) and dysgraphia 27% (6), occurringless often. Rarely conductional dysphasia 14% (3), R/Ldisorientation 9% (2) and ideomotor apraxia 4% (1)were seen (Table 2, Supporting Information Fig. S1).Six (27%) failed six or more test categories. Dyscalcu-lia, dysgraphia, constructional apraxia, R/L disorienta-tion and conductional dysphasia were associated withmultiple category failures. Five out of six (83%) left-handed and 7/12 (58%) right-handed subjects failedone or more batteries. Eight of the 15 patients withparietal dysfunction (53%) had CRPS in the dominantupper limb. Supporting Information Fig. S2 illustratesthe overlap between subjects with parietal dysfunc-tion, left-handedness and CRPS affecting the domi-nant upper limb. All the patients with >1 limbinvolvement (n = 4) failed one or more testing catego-ries. None of the participants failed the interlockingfingers screen.
Comparing parietal function, there was a signifi-cantly greater %BSA in patients who failed one ormore categories compared with those who performednormally (median 26% vs. median 3.5%, respectively;Man–Whitney test: U = 13, z = -2.45, p < 0.05). Therewas a strong negative correlation between a low pari-etal testing score (greater parietal dysfunction) and theextent of BSA (Spearman’s rho = -0.674, p = 0.001)
1Synchiria is defined as bilateral sensations in response tounilateral tactile stimulation (Medina and Rapp, 2008). Themost appropriate term for this clinical sign would thereforebe tactile dysynchiria.
Table 1 CRPS patient demographic data.
Patient
ID
CRPS
duration
(years)
Baseline
pain
Age
(years) Gender Medication
1 8 Moderate 43 F Op, BZ, NSAID, O
2 2 Severe 56 M NO, NSAID, Op, NA
3 10 Severe 47 F NO, NA, O
4 18 Severe 41 F NA, O
5 8 Severe 29 F Op, NSAID
6 2 Moderate 42 F NO
7 17 Moderate 44 F NO, Op, NA, MR, O
8a 8 Mild 42 F Op
9 2 Severe 50 F NO, NSAID, Op, NA, O
10 11 Moderate 50 M NO, Op, NA, O
11 8 Moderate 27 F Op, NO, O
12 4 Severe 30 M NA, O
13 1 Moderate 63 F Op, NSAID, NO, O
14 2 Moderate 46 F NA, Op
15 8 Moderate 55 F NO, NSAID, NA
16 1 Moderate 58 F Op, NSAID, NA
17 9 Moderate 63 F NO, NA, O
18a 2 Moderate 30 F Op, NA
19 1 Severe 43 F NIL
20 10 Moderate 33 F Op, NSAID, NA, NO
21a 7 Severe 52 M Op, NO, NA, O
22 10 Moderate 44 M NSAID, BZ, O
Demographic data including details of the CRPS duration and medication
are displayed. The patient cohort was taken from subjects attending an
in-patient rehabilitation programme; the disease duration is therefore
skewed towards long duration (mean 7 years).
Baseline pain: patients rated their pain as none, mild, moderate or severe.
CRPS, complex regional pain syndrome; F, female; M, male; NO, non-
opioid; Op, opioid; NSAID, non-steroidal anti-inflammatory drug;
NA, neuromodulatory/antidepressant; BZ, benzodiazepine; MR, muscle
relaxant; O, other [‘other’ drugs are diuretics (3), statin (1), bisphospho-
nate (1), calcium channel antagonist (1), ACE inhibitor (1)].aDyslexia.
Parietal lobe dysfunction in CRPS H. Cohen et al.
530 Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters

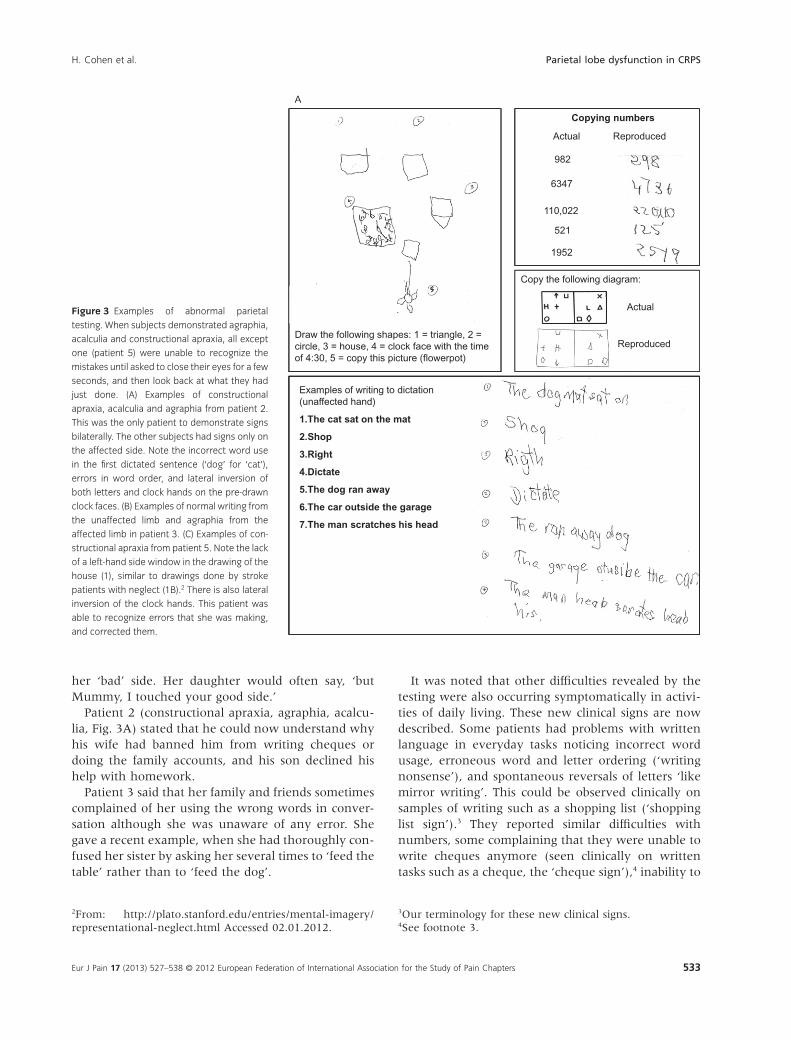
(i.e., low score, greater extent of allodynia, Fig. 2).Some examples of abnormal testing patterns are givenin Fig. 3 and Supporting Information Fig. S3. Therewas no statistically significant correlation betweendisease duration and parietal score.
Only 32% (n = 7) performed within normal param-eters on all 10 test batteries. The majority of subjectswith normal parietal function (n = 7) were right-handed (n = 5, 71%), 1 was left-handed and 1 ambi-dextrous. Five had unilateral involvement of a lowerlimb and 2 unilateral upper limb involvement (29%).Only 1/7 (14%) had CRPS affecting the dominantupper limb (Table 2).
3.4 Clinical observations
Patients demonstrating astereognosis described beingunable to detect the size, shape, weight, volume ortexture of the object and could therefore not guesswhat it might be. One patient used his thumb to tracethe edges of the objects presented. On being asked to
explain what they were doing, the patient respondedthat they were ‘tracing’ the object and ‘drawing it inthe mind’, to be able to try and guess what it might be.Patients unable to discriminate textures presented tothem also described having no idea of what it mightbe, unable to even state whether rough or smooth,soft or stiff.
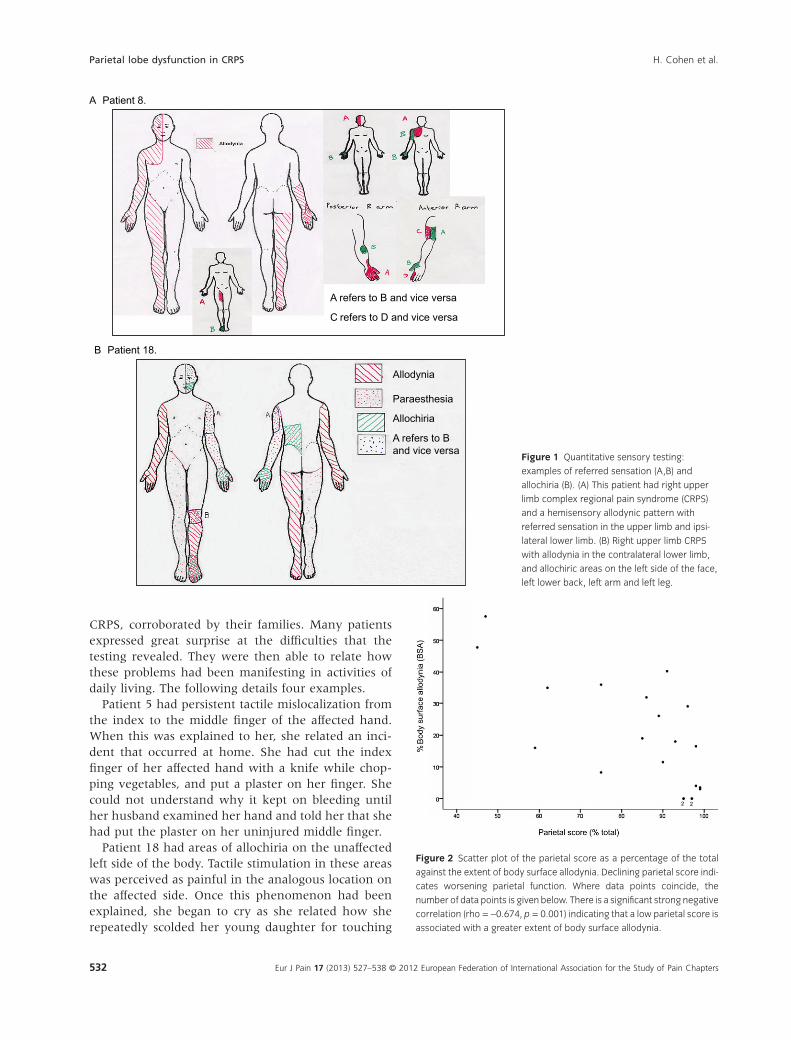
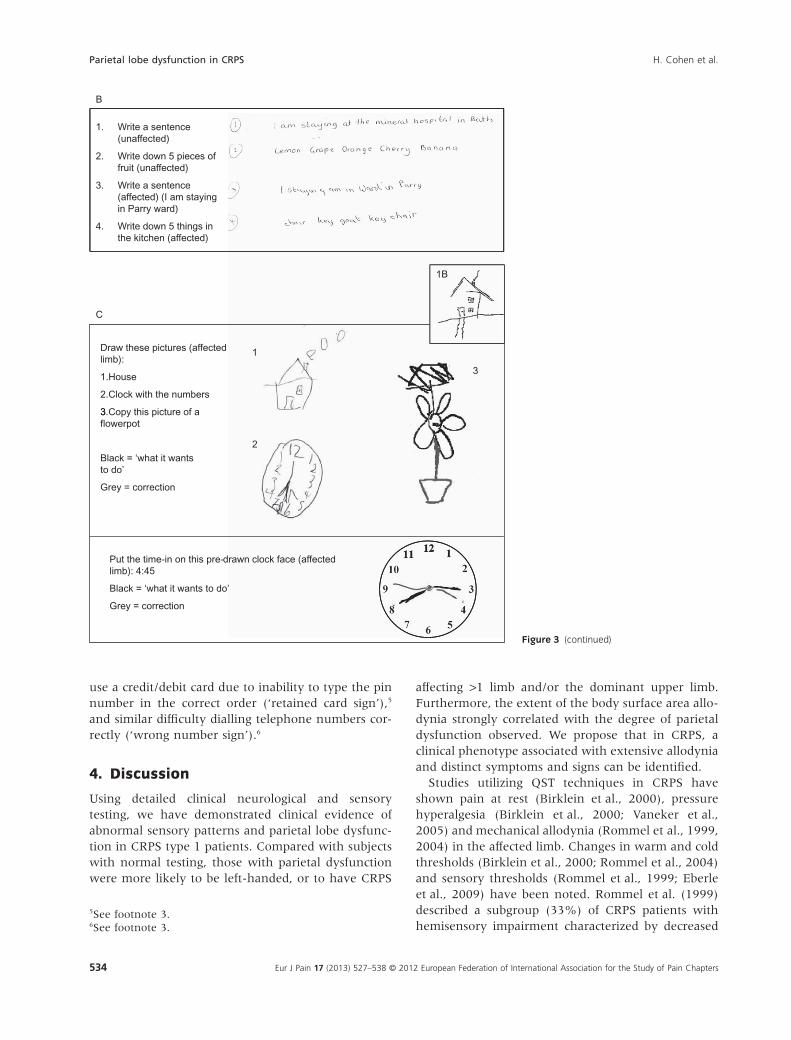
During written and drawing tasks, 5/7 patients wereunaware that any mistakes had been made. Of the fivesubjects that demonstrated constructional apraxia,four were unable to see the errors made until theirattention was distracted, and then refocused on thedrawings they had made (Fig. 3). A typical commentwas, ‘that is not what I did’, with the patient explain-ing that they were ‘doing it right in my head’ andconfused by what they saw on the page. Only one(patient 5) could recognize that errors were beingmade during execution of the task, and correctedthese (Fig. 3C).
None of the patients had any of the self-reporteddifficulties subsequently found prior to onset of their
Table 2 Quantitative sensory testing (QST) and parietal testing results.
Sensory testing Parietal testing
Patient ID Handed
CRPS
location %BSA Somaesthesia Total score %
Category
score/10 Category failed
1 R RA 47.75 R 45 1 IA, CDph, Ag, Ac, As, FA, Dg, RLD, CA
2 R RA 57.5 R 47 1 CDph, Ag, Ac, As, FA, Dg, CA
3 L LA 16 R, AC, SE 59 3 Ag, Ac, As, FA, Dg, RLD, CA
4 R LA RL 35 R, AC 62 4 Ag, Ac, As, FA, Dg, CA
5 L LA LL 36 R, AC, D, SE 75 4 Ag, Ac, As, FA, Dg, CA
6 R RL 8.25 R, AC 75 4 CDph, Ag, Ac, As, FA, CA
7 R LA 19 85 7 As, FA, CA
8 R RA RL 32 R 86 7 As, FA, Dg
9 R LL 26 R 89 8 As, FA
10 R RA 11.5 D 90 8 FA, Dg
11 L RL 40.25 R, D 91 8 As, FA
12 L RA 18 SE 93 8 As, Dg
13 R RA 0 95 8 As, FA
14 R RL 0 95 8 As, FA
15 L LA LL 29 R 96 9 As
16 R LL 0 R 97 10
17 R LA 0 97 10
18 R RA 15.25 R, AC 98 10
19 R/L LL 4 98 10
20 R LL 16.5 D 98 10
21 L LL 3.5 99 10
22 R LL 3 99 10
Results of QST and parietal testing for each patient are shown together with details of handedness and CRPS location. For sensory testing, the %BSA and
abnormal sensory patterns are detailed. The results of parietal testing are tabulated showing the parietal testing score as a percentage of total score,
number of categories that tested normally out of 10 and which categories were failed. CRPS, complex regional pain syndrome; R, right; L, left;
R/L, ambidextrous; RA, right arm; LA, left arm; RL, right leg; LL, left leg; R, right-handed; L, left-handed; %BSA, percentage of body surface allodynia;
somaesthesia, pattern of abnormal sensory findings; R, referred sensations; AC, allochiria; SE, sensory extinction; D, dysynchiria; IL, interlocking fingers;
IA, ideomotor apraxia; CDph, conduction dysphasia; Ag, agraphia; Ac, acalculia; As, astereognosis; FA, finger agnosia; Dg, dysgraphaesthesia;
RLD, right/left disorientation; CA, constructional apraxia.
H. Cohen et al. Parietal lobe dysfunction in CRPS
531Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters
CRPS, corroborated by their families. Many patientsexpressed great surprise at the difficulties that thetesting revealed. They were then able to relate howthese problems had been manifesting in activities ofdaily living. The following details four examples.
Patient 5 had persistent tactile mislocalization fromthe index to the middle finger of the affected hand.When this was explained to her, she related an inci-dent that occurred at home. She had cut the indexfinger of her affected hand with a knife while chop-ping vegetables, and put a plaster on her finger. Shecould not understand why it kept on bleeding untilher husband examined her hand and told her that shehad put the plaster on her uninjured middle finger.
Patient 18 had areas of allochiria on the unaffectedleft side of the body. Tactile stimulation in these areaswas perceived as painful in the analogous location onthe affected side. Once this phenomenon had beenexplained, she began to cry as she related how sherepeatedly scolded her young daughter for touching
A Patient 8.
A refers to B and vice versa
C refers to D and vice versa
B Patient 18.
Allodynia
Paraesthesia
A refers to B and vice versa
Allochiria
Figure 1 Quantitative sensory testing:
examples of referred sensation (A,B) and
allochiria (B). (A) This patient had right upper
limb complex regional pain syndrome (CRPS)
and a hemisensory allodynic pattern with
referred sensation in the upper limb and ipsi-
lateral lower limb. (B) Right upper limb CRPS
with allodynia in the contralateral lower limb,
and allochiric areas on the left side of the face,
left lower back, left arm and left leg.
Figure 2 Scatter plot of the parietal score as a percentage of the total
against the extent of body surface allodynia. Declining parietal score indi-
cates worsening parietal function. Where data points coincide, the
number of data points is given below. There is a significant strong negative
correlation (rho = -0.674, p = 0.001) indicating that a low parietal score is
associated with a greater extent of body surface allodynia.
Parietal lobe dysfunction in CRPS H. Cohen et al.
532 Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters
her ‘bad’ side. Her daughter would often say, ‘butMummy, I touched your good side.’
Patient 2 (constructional apraxia, agraphia, acalcu-lia, Fig. 3A) stated that he could now understand whyhis wife had banned him from writing cheques ordoing the family accounts, and his son declined hishelp with homework.
Patient 3 said that her family and friends sometimescomplained of her using the wrong words in conver-sation although she was unaware of any error. Shegave a recent example, when she had thoroughly con-fused her sister by asking her several times to ‘feed thetable’ rather than to ‘feed the dog’.
It was noted that other difficulties revealed by thetesting were also occurring symptomatically in activi-ties of daily living. These new clinical signs are nowdescribed. Some patients had problems with writtenlanguage in everyday tasks noticing incorrect wordusage, erroneous word and letter ordering (‘writingnonsense’), and spontaneous reversals of letters ‘likemirror writing’. This could be observed clinically onsamples of writing such as a shopping list (‘shoppinglist sign’).3 They reported similar difficulties withnumbers, some complaining that they were unable towrite cheques anymore (seen clinically on writtentasks such as a cheque, the ‘cheque sign’),4 inability to
2From: http://plato.stanford.edu/entries/mental-imagery/representational-neglect.html Accessed 02.01.2012.
3Our terminology for these new clinical signs.4See footnote 3.
Copying numbers
Actual Reproduced
A
982
6347
110,022
521521
1952
Copy the following diagram:
Actual
Examples of writing to dictation
Draw the following shapes: 1 = triangle, 2 = circle, 3 = house, 4 = clock face with the timeof 4:30, 5 = copy this picture (flowerpot)
Reproduced
(unaffected hand)
1.The cat sat on the mat
2.Shop
3.Right
4.Dictate
5.The dog ran away
6.The car outside the garage
7.The man scratches his head
Figure 3 Examples of abnormal parietal
testing. When subjects demonstrated agraphia,
acalculia and constructional apraxia, all except
one (patient 5) were unable to recognize the
mistakes until asked to close their eyes for a few
seconds, and then look back at what they had
just done. (A) Examples of constructional
apraxia, acalculia and agraphia from patient 2.
This was the only patient to demonstrate signs
bilaterally. The other subjects had signs only on
the affected side. Note the incorrect word use
in the first dictated sentence (‘dog’ for ‘cat’),
errors in word order, and lateral inversion of
both letters and clock hands on the pre-drawn
clock faces. (B) Examples of normal writing from
the unaffected limb and agraphia from the
affected limb in patient 3. (C) Examples of con-
structional apraxia from patient 5. Note the lack
of a left-hand side window in the drawing of the
house (1), similar to drawings done by stroke
patients with neglect (1B).2 There is also lateral
inversion of the clock hands. This patient was
able to recognize errors that she was making,
and corrected them.
H. Cohen et al. Parietal lobe dysfunction in CRPS
533Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters
use a credit/debit card due to inability to type the pinnumber in the correct order (‘retained card sign’),5
and similar difficulty dialling telephone numbers cor-rectly (‘wrong number sign’).6
4. Discussion
Using detailed clinical neurological and sensorytesting, we have demonstrated clinical evidence ofabnormal sensory patterns and parietal lobe dysfunc-tion in CRPS type 1 patients. Compared with subjectswith normal testing, those with parietal dysfunctionwere more likely to be left-handed, or to have CRPS
affecting >1 limb and/or the dominant upper limb.Furthermore, the extent of the body surface area allo-dynia strongly correlated with the degree of parietaldysfunction observed. We propose that in CRPS, aclinical phenotype associated with extensive allodyniaand distinct symptoms and signs can be identified.
Studies utilizing QST techniques in CRPS haveshown pain at rest (Birklein et al., 2000), pressurehyperalgesia (Birklein et al., 2000; Vaneker et al.,2005) and mechanical allodynia (Rommel et al., 1999,2004) in the affected limb. Changes in warm and coldthresholds (Birklein et al., 2000; Rommel et al., 2004)and sensory thresholds (Rommel et al., 1999; Eberleet al., 2009) have been noted. Rommel et al. (1999)described a subgroup (33%) of CRPS patients withhemisensory impairment characterized by decreased
5See footnote 3.6See footnote 3.
B
1. Write a sentence (unaffected)
2. Write down 5 pieces of fruit (unaffected)
3. Write a sentence (affected) (I am staying in Parry ward)
4. Write down 5 things in the kitchen (affected)
C
1B
Draw these pictures (affected limb):
1.House
2.Clock with the numbers
3 Copy this picture of a
1
3
Black = ‘what it wants to do’
Grey = correction
3.flowerpot
2
Put the time-in on this pre-drawn clock face (affected limb): 4:45
Black = ‘what it wants to do’
Grey = correction
Figure 3 (continued)
Parietal lobe dysfunction in CRPS H. Cohen et al.
534 Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters

temperature and pinprick sensation ipsilateral to theCRPS affected limb. The overall prevalence ofmechanical allodynia was 58% and mean diseaseduration was 4 years. Other studies report allodyniaprevalence of 30% (Birklein et al., 2000) and 11% (deMos et al., 2009), with mean disease durations of 6months and 6 years, respectively. In a follow-up study,Rommel et al. (2001) confirmed that 30% of CRPSpatients had hemisensory impairment. They weremore likely to have mechanical allodynia and hyper-algesia, and tended to have longer duration of CRPS.
The prevalence of mechanical allodynia for ourcohort was 82% and mean disease duration was 7years. Like Rommel and colleagues, we found a largepercentage of patients (59%) with sensory abnormali-ties extending beyond the affected limb. However, wefound no correlation between disease duration andextent of allodynia. This may be due to the smallsample size.
Referral of sensation (McCabe et al., 2003;Maihofner et al., 2006; Robinson et al., 2011) hasbeen previously documented in CRPS patients. Onlyone previous study (Förderreuther et al., 2004) haslooked for sensory extinction in a cohort of CRPSpatients (n = 114) and did not find any. However, thiswas an early CRPS cohort with a mean disease dura-tion of 6 months. While dysynchiria in CRPS has beenreported (Acerra and Moseley, 2005), it was a type ofvisuotactile dysynchiria induced by watching areflected image of the unaffected limb being touchedand feeling pain or paraesthesia at the correspondingsite on the affected limb. We have not found anypreviously published reports of allochiria (mislocationof sensory stimuli to the corresponding opposite halfof the body) (Meador et al., 1991) or pure tactile dys-ynchiria in CRPS.
While the parietal testing results are supportive ofparietal lobe dysfunction, our study had several limi-tations and further validation of this early pilot clinicalwork is required. Future work requires a larger studywith age/sex matched healthy controls and similarlymatched pain control groups, detailed neuropsycho-logical testing and neuroimaging. Our cohort was alonger duration, severely impaired group taken fromCRPS patients attending an in-patient rehabilitationprogramme. However, five patients with disease dura-tion of 2 years or less demonstrated parietal dysfunc-tion. Future work should encompass early CRPSpatients to establish whether disease duration is asignificant factor.
The parietal testing protocol required patients to usetheir upper limbs, so it is unsurprising that 11 out ofthe 15 with dysfunction had CRPS affecting an upper
limb. However, 4/15 had unilateral lower limbinvolvement showing that impaired testing is unlikelyto be an artefact of a protocol that needs subjects touse their upper limbs.
The pattern of parietal disturbance involves both theright and left parietal cortices, and superior and infe-rior lobules. Left parietal dysfunction can includefinger agnosia, astereognosis, dysgraphaesthesia, con-duction aphasia, R/L disorientation and agraphia.Right parietal dysfunction often causes constructionalapraxia (Joseph, 1990). Among subjects with three ormore category failures, both right- and left-sided dys-functions are apparent. Moseley et al. suggest anetwork of multisensory and homeostatic corticalareas may be responsible for maintaining a ‘body-matrix’ (Moseley et al., 2012). The parietal lobes areassociation cortices, and are likely to be part of such anetwork. The pattern of neuropsychological abnor-malities cannot be accounted for by an anatomicallesion, and may reflect a maladaptive failure to main-tain associative functional integrity. A similar mal-adaptive failure in the maintenance of global bodyconstructs has been proposed to explain the complex-ity of phantom limb pain (Giummarra et al., 2007)and body schema distortion described in CRPS (Lewiset al., 2010). For further discussion regarding aste-reognosis, constructional apraxia, dysgraphia andneglect, see Supporting Information Discussion S1.
A possible contributing mechanism may be disrup-tion in normal right-left hemispheric communication.Side to side hemispheric asymmetry in primary soma-tosensory cortical representation of the affected handin upper limb CRPS patients has been described(Pleger et al., 2004). A sustained shift leading to hemi-spheric representational asymmetry might perturbtranscallosal cross-referencing and interhemisphericcommunication. A case report of a CRPS patientwith neurophysiologic evidence of altered inter-hemispheric conduction lends credence to thisconcept, and its possible involvement in pathologicchronic pain (Forss et al., 2005).
When numbers of patients with CRPS affecting theirnon-dominant side are reviewed (n = 7), four (57%)had parietal dysfunction. Thirteen patients hadCRPS affecting their dominant side; 11 (85%) hadparietal dysfunction, suggesting a possible hemisphericdominance effect. For further discussion of handdominance and parietal function, see SupportingInformation Discussion S1.
Previously described clinical features in CRPS suchas digit misidentification (Förderreuther et al., 2004),agnosia for object orientation (Robinson et al., 2011)and neglect-like phenomena (Galer and Jensen, 1999;
H. Cohen et al. Parietal lobe dysfunction in CRPS
535Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters

Frettlöh et al., 2006; Lewis et al., 2007) are suggestiveof parietal lobe dysfunction in CRPS. Galer et al. useda self-administered questionnaire to enquire aboutneglect-like symptoms, reporting 84% of respondentsconfirmed the presence of at least one symptom (Galerand Jensen, 1999). Another study utilized a question-naire based upon the work of Galer et al. and admin-istered it to both CRPS patients and subjects withchronic limb pain of other origin. It was found thatwhile both groups reported neglect-like symptoms,this was significantly more frequent in the CRPSgroup, who reported more severe symptoms (Frettlöhet al., 2006). While Förderreuther et al. (2004) dem-onstrated impaired self-perception of the hand inCRPS, they did not find evidence for classic neglect.
A recent paper combined a standardized question-naire with neuropsychological (including parietalfunction), sensory and motor testing in patients withCRPS, chronic limb pain and healthy controls. It con-firmed that neglect-like phenomena can be found inboth CRPS and patients with chronic limb pain, butthat the two group scores were indistinguishable (Kolbet al., 2012). Moseley et al. have demonstrated a formof spatial neglect in CRPS. They found that by askingpatients to cross their limbs, tactile processing of theaffected limb could be affected (Moseley et al., 2009).Furthermore, prism adaptation to direct visiontowards the unaffected side has been demonstrated toalleviate pathologic pain in CRPS (Sumitani et al.,2007). Thus, CRPS patients may demonstrate aneglect-like syndrome.
Neuroimaging studies provide further evidence ofparietal involvement (Shiraishi et al., 2006; Wu et al.,2006; Maihöfner et al., 2007; Lebel et al., 2008;Vartiainen et al., 2008). A PET study of brush-evokedallodynia in healthy volunteers given intradermal cap-saicin demonstrated activation of the PPC (Wittinget al., 2001). Specific activation was seen in the con-tralateral Brodmann area 5/7 suggesting the impor-tance of this area to the processing of allodynia due toits multisensory input, role in conscious pain percep-tion and its neuroplastic properties. Reorganization inparietal areas other than S1 has been proposed ascontributing to synchiria in hands rendered anaes-thetic by stroke or neurosurgery (Sathian, 2000), andreferral of sensation in phantom limb patients (Floret al., 2000; Grusser et al., 2004). There is increasingevidence for the role of cortical plasticity in chronicpain, and that it may offer a potential therapeutictarget in rehabilitation (Moseley and Flor, 2012). Ourwork supports the concept that in CRPS patients withextensive allodynia, there may be cortical networkdisruption across widespread areas including the pari-
etal cortices. The extent of allodynia may reflect thedegree of neuroplasticity and thus explain the corre-lation with parietal dysfunction.
On a practical level, patients with constructionalapraxia, agraphia or acalculia may not be able to per-ceive mistakes made. They should be advised to asksomeone else to check written work or tasks involvingnumeracy. They may need to avoid writing chequesand consider using a ‘chip and signature card’ ratherthan a ‘chip and PIN’ number card.7 Use of the speeddial facility on telephones may overcome problemswith correctly dialling a number sequence. Those withdigit misidentification should be warned to check inju-ries carefully. Above all, the patient and their familyneed reassurance that these phenomena can occur,and that they are not ‘going mad’.
5. Conclusion
CRPS patients with extensive allodynia may also haveunusual sensory patterns and new clinical signs con-sistent with parietal lobe dysfunction, which is notapparent with standard neurological examination.
Author contributions
All authors discussed the results and commented on themanuscript.
Acknowledgements
We would like to thank and acknowledge all our patientsand healthy volunteers who gave up their time so freely.
References
Acerra, N.E., Moseley, G.L. (2005). Dysynchiria: Watching themirror image of the unaffected limb elicits pain on the affectedside. Neurology 65, 751–753.
Bingel, U., Lorenz, J., Glauche, V., Knab, R., Glascher, J., Weiller,C., Buchel, C. (2004). Somatotopic organization of humansomatosensory cortices for pain: A single trial fMRI study.Neuroimage 23, 224–232.
Birklein, F., Riedl, B., Sieweke, N., Weber, M., Neundorfer, B.(2000). Neurological findings in complex regional painsyndromes–analysis of 145 cases. Acta Neurol Scand 101, 262–269.
de Mos, M., Huygen, F.J., Hoeven-Borgman, M., Dieleman, J.P.,Ch Stricker, B.H., Sturkenboom, M.C. (2009). Outcome of thecomplex regional pain syndrome. Clin J Pain 25, 590–597.
7More information available on the Royal National Institutefor the Blind website (http://www.rnib.org).
Parietal lobe dysfunction in CRPS H. Cohen et al.
536 Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters
Duncan, G.H., Albanese, M.C. (2003). Is there a role for theparietal lobes in the perception of pain? Adv Neurol 93, 69–86.
Eberle, T., Doganci, B., Kramer, H.H., Geber, C., Fechir, M.,Magerl, W., Birklein, F. (2009). Warm and cold complexregional pain syndromes: Differences beyond skin tempera-ture? Neurology 72, 505–512.
Flor, H., Muhlnickel, W., Karl, A., Denke, C., Grusser, S., Kurth,R., Taub, E. (2000). A neural substrate for nonpainfulphantom limb phenomena. Neuroreport 11, 1407–1411.
Förderreuther, S., Sailer, U., Straube, A. (2004). Impaired self-perception of the hand in complex regional pain syndrome(CRPS). Pain 110(3), 756–761.
Forss, N., Kirveskari, E., Gockel, M. (2005). Mirror-like spread ofchronic pain. Neurology 65, 748–750.
Frettlöh, J., Huppe, M., Maier, C. (2006). Severity and specificityof neglect-like symptoms in patients with complex regionalpain syndrome (CRPS) compared to chronic limb pain of otherorigins. Pain 124, 184–189.
Galer, B.S., Jensen, M. (1999). Neglect-like symptoms in complexregional pain syndrome: Results of a self-administered survey.J Pain Symptom Manage 18(S3), 213–217.
Gieteling, E.W., van Rijn, M.A., de Jong, B.M., Hoogduin, J.M.,Renken, R., van Hilten, J.J., Leenders, K.L. (2008). Cerebralactivation during motor imagery in complex regional painsyndrome type 1 with dystonia. Pain 134, 302–309.
Giummarra, M.J., Gibson, S.J., Georgiou-Karistianis, N., Brad-shaw, J.L. (2007). Central mechanisms in phantom limbperception: The past, present and future. Brain Res Rev 54,219–232.
Grusser, S.M., Muhlnickel, W., Schaefer, M., Villringer, K.,Christmann, C., Koeppe, C., Flor, H. (2004). Remote activa-tion of referred phantom sensation and cortical reorganizationin human upper extremity amputees. Exp Brain Res 154,97–102.
Harden, R.N., Bruehl, S., Stanton-Hicks, M., Wilson, P.R. (2007).Proposed new diagnostic criteria for complex regional painsyndrome. Pain Med 8, 326–331.
Joseph, R. (1990). Neuropsychology, Neuropsychiatry, and BehavioralNeurology (Critical Issues in Neuropsychology) (New York: PlenumPress).
Juottonen, K., Gockel, M., Silen, T., Hurrir, H., Hari, R.F. (2002).Altered central sensorimotor processing in patients withcomplex regional pain syndrome. Pain 98, 315–323.
Kolb, L., Lang, C., Seifert, F., Maihofner, C. (2012). Cognitivecorrelates of ‘neglect-like syndrome’ in patients with complexregional pain syndrome. Pain 153, 1063–1073.
Lebel, A., Becerra, L., Wallin, D., Moulton, E.A., Morris, S.,Pendse, G., Jasciewicz, J., Stein, M., Aiello-Lammens, M.,Grant, E., Berde, C., Borsook, D. (2008). fMRI reveals distinctCNS processing during symptomatic and recovered complexregional pain syndrome in children. Brain 131, 1854–1879.
Lewis, J.S., Kersten, P., McCabe, C.S., McPherson, K.M., Blake,D.R. (2007). Body perception disturbance: A contribution topain in complex regional pain syndrome (CRPS). Pain 133,111–119.
Lewis, J.S., Kersten, P., McPherson, K.M., Taylor, G.J., Harris, N.,McCabe, C.S., Blake, D.R. (2010). Wherever is my arm?Impaired upper limb position accuracy in complex regionalpain syndrome. Pain 149, 463–469.
Liang, M., Mouraux, A., Iannetti, G.D. (2011). Parallel process-ing of nociceptive and non-nociceptive somatosensory infor-mation in the human primary and secondary somatosensory
cortices: Evidence from dynamic causal modeling of func-tional magnetic resonance imaging data. J Neurosci 31, 8976–8985.
Libon, D.J., Schwartzman, R.J., Eppig, J., Wambach, D., Brahin,E., Peterlin, B.L., Alexander, G., Kalanuria, A. (2010). Neu-ropsychological deficits associated with complex regional painsyndrome. J Int Neuropsychol Soc 16, 566–573.
Lin, Y.Y., Forss, N. (2002). Functional characterization of humansecond somatosensory cortex by magnetoencephalography.Behav Brain Res 135, 141–145.
Lund, C., Browder, N. (1944). The estimation of areas of burns.Surg Gynecol Obstet 79, 352–358.
Maihofner, C., Neundorfer, B., Birklein, F., Handwerker, H.O.(2006). Mislocalization of tactile stimulation in patients withcomplex regional pain syndrome. J Neurol 253, 772–779.
Maihofner, C., Peltz, E. (2011). CRPS, the parietal cortex andneurocognitive dysfunction: An emerging triad. Pain 152,1453–1454.
Maihöfner, C., Baron, R., DeCol, R., Binder, A., Birklein, F.,Deuschl, G., Handwerker, H.O., Schattschneider, J. (2007).The motor system shows adaptive changes in complexregional pain syndrome. Brain 130, 2671–2687.
Maihöfner, C., Handwerker, H.O., Birklein, F. (2006). Func-tional imaging of allodynia in complex regional pain syn-drome. Neurology 66, 711–717.
Maihöfner, C., Handwerker, H.O., Neundörfer, B., Birklein, F.(2003). Patterns of cortical reorganization in complex regionalpain syndrome. Neurology 61, 1707–1715.
Marinus, J., Moseley, G.L., Birklein, F., Baron, R., Maihofner, C.,Kingery, W.S., van Hilten, J.J. (2011). Clinical features andpathophysiology of complex regional pain syndrome. LancetNeurol 10, 637–648.
McCabe, C.S., Haigh, R.C., Halligan, P.W., Blake, D.R. (2003).Referred sensations in patients with complex regional painsyndrome type 1. Rheumatology 42, 1067–1073.
Meador, K.J., Allen, M.E., Adams, R.J., Loring, D.W. (1991).Allochiria vs allesthesia. Is there a misperception? Arch Neurol48, 546–549.
Medina, J., Rapp, B. (2008). Phantom tactile sensations modu-lated by body position. Curr Biol 18, 1937–1942.
Moo, L.R., Slotnick, S.D., Tesoro, M.A., Zee, D.S., Hart, J. (2003).Interlocking finger test: a bedside screen for parietal lobe dys-function. J. Neurol. Neurosurg. Psychiatry 74, 530–532.
Moseley, G.L. (2005). Distorted body image in complex regionalpain syndrome. Neurology 65, 773.
Moseley, G.L., Flor, H. (2012). Targeting cortical representationsin the treatment of chronic pain: A review. Neurorehabil NeuralRepair 26, 646–652.
Moseley, G.L., Gallace, A., Spence, C. (2009). Space-based, butnot arm-based, shift in tactile processing in complex regionalpain syndrome and its relationship to cooling of the affectedlimb. Brain 132, 3142–3151.
Moseley, G.L., Gallace, A., Spence, C. (2012). Bodily illusions inhealth and disease: Physiological and clinical perspectives andthe concept of a cortical ‘body matrix’. Neurosci Biobehav Rev36, 34–46.
Peltz, E., Seifert, F., Lanz, S., Muller, R., Maihofner, C. (2011).Impaired hand size estimation in CRPS. J Pain 12, 1095–1101.
Pleger, B., Ragert, P., Schwenkreis, P., Forster, A.F., Wilimzig, C.,Dinse, H., Nicolas, V., Maier, C., Tegenthoff, M. (2006). Pat-terns of cortical reorganization parallel impaired tactile dis-crimination and pain intensity in complex regional painsyndrome. Neuroimage 32, 503–510.
H. Cohen et al. Parietal lobe dysfunction in CRPS
537Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters

Pleger, B., Tegenthoff, M., Schwenkreis, P., Janssen, F., Ragert, P.,Dinse, H.R., Volker, B., Zenz, M., Maier, C. (2004). Meansustained pain levels are linked to hemispherical side-to-sidedifferences of primary somatosensory cortex in the complexregional pain syndrome I. Exp Brain Res 155, 115–119.
Robinson, G., Cohen, H., Goebel, A. (2011). A case of complexregional pain syndrome with agnosia for object orientation.Pain 152, 1674–1681.
Rommel, O., Gehling, M., Dertwinkel, R., Witscher, K., Zenz, M.,Malin, J.-P., Janig, W. (1999). Hemisensory impairment inpatients with complex regional pain syndrome. Pain 80,95–101.
Rommel, O., Malin, J.P., Janig, W., Zenz, M. (2004). [Clinicalfindings in patients with chronic complex regional pain syn-drome]. Anaesthesist 53, 965–977.
Rommel, O., Malin, J.P., Zenz, M., Janig, W. (2001). Quantitativesensory testing, neurophysiological and psychological exami-nation in patients with complex regional pain syndrome andhemisensory deficits. Pain 93, 279–293.
Sathian, K. (2000). Intermanual referral of sensation to anes-thetic hands. Neurology 54, 1866–1868.
Schwoebel, J., Friedman, R., Duda, N., Coslett, H.B. (2001). Painand the body schema: Evidence for peripheral effects onmental representations of movement. Brain 124, 2098–2104.
Shiraishi, S., Kobayashi, H., Nihashi, T., Kato, K., Iwano, S.,Nishino, M., Ishigaki, T., Ikeda, M., Kato, T., Ito, K., Kimura, T.(2006). Cerebral glucose metabolism change in patients withcomplex regional pain syndrome: A PET study. Radiat Med 24,335–344.
Sumitani, M., Rossetti, Y., Shibata, M., Matsuda, Y., Sakaue, G.,Inoue, T., Mashimo, T., Miyauchi, S. (2007). Prism adaptationto optical deviation alleviates pathologic pain. Neurology 68,128–133.
Treede, R.D., Apkarian, A.V., Bromm, B., Greenspan, J.D., Lenz,F.A. (2000). Cortical representation of pain: Functional char-acterization of nociceptive areas near the lateral sulcus. Pain87, 113–119.
Vaneker, M., Wilder-Smith, O.H., Schrombges, P., Man-Hermsen, I., Oerlemans, H.M. (2005). Patients initially diag-nosed as ‘warm’ or ‘cold’ CRPS 1 show differences in centralsensory processing some eight years after diagnosis: A quan-titative sensory testing study. Pain 115, 204–211.
Vartiainen, N.V., Kirveskari, E., Forss, N. (2008). Central process-ing of tactile and nociceptive stimuli in complex regional painsyndrome. Clin Neurophysiol 119, 2380–2388.
Witting, N., Kupers, R.C., Svensson, P., Arendt-Nielsen, L.,Gjedde, A., Jensen, T.S. (2001). Experimental brush-evokedallodynia activates posterior parietal cortex. Neurology 57,1817–1824.
Wu, C.T., Fan, Y.M., Sun, C.M., Borel, C.O., Yeh, C.C., Yang, C.P.,Wong, C.S. (2006). Correlation between changes in regionalcerebral blood flow and pain relief in complex regional painsyndrome type 1. Clin Nucl Med 31, 317–320.
Supporting Information
Additional Supporting Information may be found in theonline version of this article:
Figure S1. Pie chart showing the distribution of normaltesting and category failures among CRPS patients.Figure S2. A Venn diagram illustrating the overlap of CRPSpatients with parietal dysfunction, left-handedness and sub-jects with CRPS affecting their dominant upper limb.Figure S3. Examples of abnormal parietal testing. Examplesof constructional apraxia when copying a random geometricfigure using matchsticks. All subjects copied a different figureeasily and correctly using the unaffected hand.Methods S1. Addendum to Methods providing furtherexperimental details.Discussion S1. Addendum to discussion citing otherresearch and its relevance to this work.
Parietal lobe dysfunction in CRPS H. Cohen et al.
538 Eur J Pain 17 (2013) 527–538 © 2012 European Federation of International Association for the Study of Pain Chapters