clinical effectiveness of low-dose chlorthalidone (6.25 mg) + atenolol combination in stage i...
TRANSCRIPT
CURRENT MEDICAL RESEARCH AND OPINION�
VOL. 24, NO. 6, 2008, 1771–1779
0300-7995
doi:10.1185/03007990802118071
� 2008 Informa UK Ltd All rights reserved: reproduction in whole or part not permitted
ORIGINAL ARTICLE
Clinical effectiveness oflow-dose chlorthalidone(6.25 mg)Yatenololcombination in stage Ihypertensive patients: amulticenter, randomized,controlled studyA. Pareeka, N. Karnikb, S. B. Salagrec, S. D. Zaward,V. K. Joglekare, N. Chandurkara and G. S. Naika
a Ipca Laboratories Ltd, Mumbai, Indiab LTMM College & LTMG Hospital, Mumbai, Indiac Seth G.S. Medical College & KEM Hospital, Mumbai, Indiad Indira Gandhi Government Medical College, Nagpur, Indiae Grant Medical College & St. George Hospital, Mumbai, India
Key words: Amlodipine – Atenolol – Chlorthalidone – Stage I essential hypertension
ABSTRACT
Objective: To compare the efficacy and safety of low-dose
chlorthalidoneþ atenolol combination with atenolol and
atenololþ amlodipine combination in stage I hypertensive
patients uncontrolled on active run-in monotherapy.
Methods: Newly diagnosed stage I hypertensive patients
were randomized to active run-in monotherapy either
with atenolol 25 mg (98/300) or chlorthalidone 6.25 mg
(100/300) or amlodipine 2.5 mg (102/300). A total of
282/300 patients (atenolol 92, chlorthalidone 91,
amlodipine 99) completed the active run-in phase
successfully. Patients uncontrolled on active run-in
monotherapy (atenolol 33, chlorthalidone 45, amlodipine
47) received the study treatment, namely atenolol 50 mg
alone, chlorthalidone 6.25 mgþ atenolol 25 mg and
atenolol 25 mgþ amlodipine 2.5 mg, respectively. Efficacy
of the therapy was evaluated by BP measurement at
weeks 12 and 20 post-therapy.
Results: Post-active run-in monotherapies, the study
treatment groups showed a significant fall in mean SBP
and DBP from baseline ( p50.05). The mean fall in SBP
and DBP was comparable for study treatments (atenolol
50 mg, atenolol 25 mgþ chlorthalidone 6.25 mg and
atenolol 25 mgþ amlodipine 2.5 mg) ( p¼ 0.337 for SBP
and p¼ 0.054 for DBP) at week 12 and ( p¼ 0.744 for
SBP and p¼ 0.855 for DBP) at week 20; also, the
percentage of responders was comparable for the three
study treatment groups ( p¼ 0.799) indicating that the
low-dose chlorthalidoneþ atenolol combination is non-
inferior to the high-dose atenolol alone and atenololþ
amlodipine combination. No serious laboratory/clinical
adverse events were reported in this study.
Conclusion: Chlorthalidone 6.25 mg in combination with
atenolol 25 mg is effective and safe in stage I (JNC 7)
essential hypertensive patients. This low dose of
chlorthalidone could reduce dose-related concerns
over metabolic adverse effects and may lead to
wider usage of this proven antihypertensive agent in
combination therapy.
Address for correspondence: Anil Pareek, Medical Affairs and Clinical Research, IpcaLaboratories Ltd, 142 AB, Kandivli Industrial Estate, Kandivli (West), Mumbai 400 067, India.Tel.: þ91 022 66474747; Fax: 91 022 28686954; [email protected]
Paper 4517 1771
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mon
ash
Uni
vers
ity o
n 09
/24/
13Fo
r pe
rson
al u
se o
nly.

Introduction
Hypertension is an increasingly important public health
issue. In 1990 there were about 5.2 million deaths from
cardiovascular disease in economically developed
regions and about 9.1 million deaths in economically
developing countries. It has been predicted that by the
year 2020 there will be an increase of almost 75% in
global cardiovascular disease burden. Of the number of
risk factors responsible for the increase in cardiovascular
morbidity and mortality, high blood pressure is one of
the most important and independent risk factors,
affecting 24–36% of the adult population in developed
countries1. Hypertension is a well known risk factor for
causing acceleration of atherosclerosis. Recent guide-
lines for controlling hypertension emphasize greater
concerns for the prevention of cardiovascular diseases.
The Joint National Committee on Prevention,
Detection, and Treatment of High Blood Pressure
(JNC 7) guideline has now coined a new terminology,
‘pre-hypertension’, for individuals whose systolic blood
pressure is in the range 120–139 mmHg and diastolic
blood pressure in the range of 80–89 mmHg, as there is
a significant risk of atherosclerosis even at these blood
pressure levels. Hence there is a need for wider usage of
evidence-based therapies in patients with stage I
hypertension.
Evidence from the Antihypertensive and
Lipid-Lowering to prevent Heart Attack Trial
(ALLHAT)2–4 and other pivotal hypertension studies
like Hypertension Detection and Follow-up Program
(HDFP)5, Multiple Risk Factor Intervention Trial
(MRFIT)6, Systolic Hypertension in the Elderly
Program (SHEP)7 has established that thiazide-like
diuretics confer significant reduction in stroke and
cardiovascular events8. Given their strong record of
evidence, low cost and favorable tolerability, low-dose
thiazide-like diuretics are recommended as initial
therapy in most of the hypertensive patients and as
the foundation for multiple antihypertensive drug
regimens9. Chlorthalidone was commonly used in
1970s, but its use has sharply declined in the past
20 years. It is not known why the drug has fallen out of
favor. One of the reasons for its low usage is the
concerns over metabolic adverse effects10. These
concerns can be addressed to a great extent by use of
low-dose chlorthalidone.
The largest clinical trials, including Hypertension
Detection and Follow-up Program (HDFP), MRFIT,
Systolic Hypertension in the Elderly Program (SHEP),
and ALLHAT, primarily used chlorthalidone as the
initial therapy and more consistently showed reduc-
tions in cardiovascular events than did studies that
primarily used HCTZ.10 Chlorthalidone possesses a
distinct pharmacokinetic profile, it provides more
sustained BP reduction over 24 hours, and it has been
suggested that its longer duration of action might
provide greater antihypertensive effects, particularly
throughout nighttime hours11. Due to its higher
potency and longer duration of action, chlorthalidone
is effective in providing additional protection from
stroke and myocardial infarction during the early
morning BP surge11.
In a pilot study, the substitution of chlorthalidone
for HCTZ in patients with uncontrolled blood pressure
on stable doses of HCTZ for 6 months, was found to
reduce SBP by an additional 4–7 mmHg, which led to
achieving goal BP in 6 of the 19 patients11. Similarly, a
randomized, single-blind clinical trial showed that,
after 8 weeks, patients who were taking 25 mg/day
chlorthalidone experienced a greater reduction in
blood pressure than those taking 50 mg/day of
hydrochlorothiazide11.
Since chlorthalidone appeared to be more than twice
as potent as hydrochlorothiazide10, a low dose of
chlorthalidone, i.e. 6.25 mg once daily, was thought to
be adequate in providing blood pressure control and
at the same time reducing the metabolic adverse effects.
Despite several advances in treatment of hyperten-
sion, mild-to-moderate hypertension still remains
poorly controlled. This relates to multiple factors,
including low antihypertensive efficacy of single-drug
therapies, reluctance of primary care physicians to
modify or titrate initially-chosen therapy to obtain
target blood pressure, and poor compliance with
medication12.
More than two-thirds of hypertensive individuals
cannot be controlled on one drug and require two or
more antihypertensive agents selected from different
drug classes13–17. The Joint National Committee on
Prevention, Detection, and Treatment of High Blood
Pressure (JNC 7) report9, as well as the European
Society of Hypertension and Cardiology (ESH/ESC)18
and the German Hypertension League19, have stated
that a high proportion of hypertensives will require a
combination of two or more antihypertensive agents
to achieve the desired target blood pressure (BP).
Besides better efficacy, the combination of two anti-
hypertensive agents with complementary mechanisms
of action is associated with better tolerance, improved
compliance, a simple drug regimen and lower cost.
The purpose of this study was to investigate the
antihypertensive efficacy and safety of 20 weeks
of treatment with a low-dose combination of
chlorthalidone (6.25 mg) and the �-blocker atenolol
(25 mg) in comparison with a high dose of atenolol
(50 mg) and a commonly used �-blocker–calcium
channel blocker combination (atenolol 25 mg
1772 Low-dose chlorthalidone in stage I hypertension � 2008 Informa UK Ltd - Curr Med Res Opin 2008; 24(06)
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mon
ash
Uni
vers
ity o
n 09
/24/
13Fo
r pe
rson
al u
se o
nly.

and amlodipine 2.5 mg) in patients who were
uncontrolled on 4 weeks of active run-in on low-
dose monotherapies.
Study objective
The primary objective was to compare the mean fall in
systolic and diastolic blood pressure between the
chlorthalidone 6.25 mgþ atenolol 25 mg combination
with atenolol 50 mg alone and atenolol 25 mgþ
amlodipine 2.5 mg combination, administered once
daily in patients who were uncontrolled on 4 weeks of
active run-in monotherapies. The secondary objective
was to evaluate the number of responders in each
treatment group and to evaluate the safety of low-dose
chlorthalidone and its combination in patients with
stage I essential hypertension.
Patients and methods
Patients
Male and female patients aged 18 years and above were
eligible if they: were newly diagnosed with stage I
essential primary hypertension (BP 140–159/90–
99 mmHg as per JNC 7 criteria), were willing to sign
an informed consent form and were available for regular
follow-up. Patients with a known history of hypersen-
sitivity to chlorthalidone, atenolol, amlodipine or any
other component of the formulations were excluded
from the study. Patients with electrolyte imbalance,
abnormal hepatic and renal function were excluded
from the study. Patients with a recent cerebrovascular
accident, overt heart failure, AV block greater than first
degree, sinus bradycardia and severe aortic stenosis
were not enrolled in this study.
Pregnant and lactating women, and all females of
childbearing potential not practicing contraception
were not enrolled in this study.
Trial design
This was a randomized, comparative, multicenter,
open-label study, conducted at Seth G.S. Medical
College & KEM Hospital, Mumbai, LTMM College &
LTMG Hospital, Mumbai, Indira Gandhi Government
Medical College, Nagpur and Grant Medical College
and St. George Hospital, Mumbai. The study protocol
was approved by the hospital ethics committees of
each center. All the patients gave their written
informed consent to participate in the study
in accordance with the Declaration of Helsinki.
The execution and monitoring of the study was
conducted in accordance with the requirements of
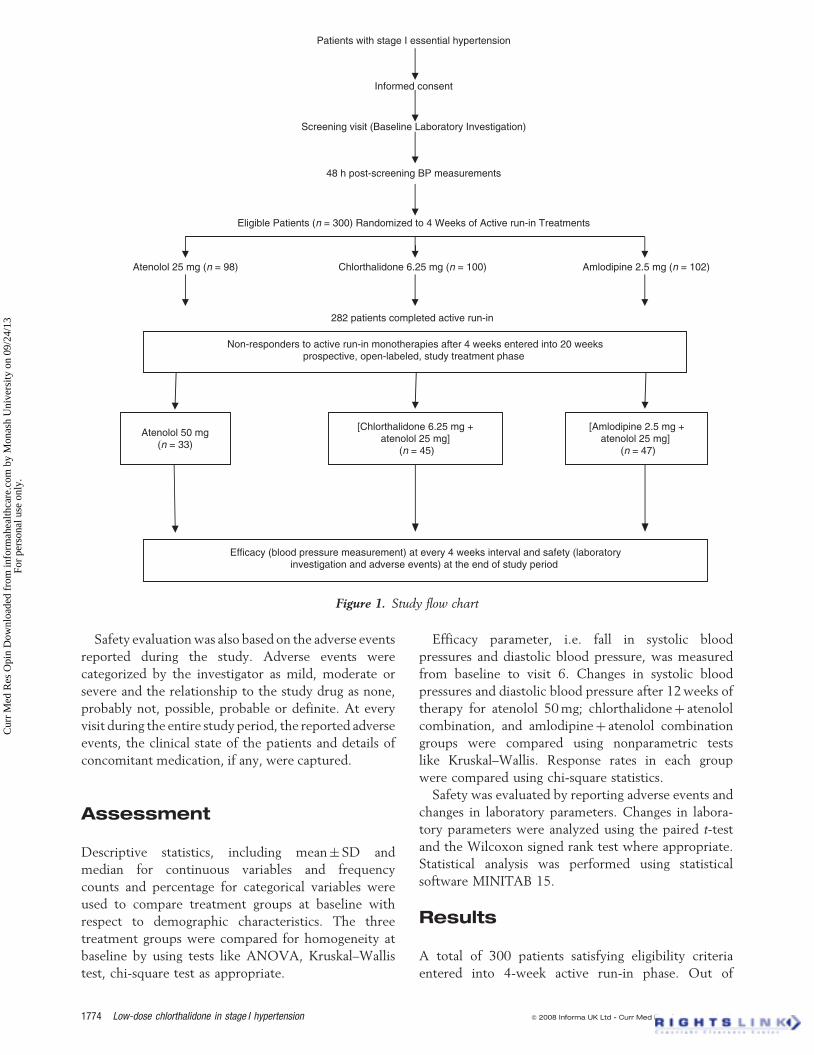
good clinical practice. Figure 1 depicts a flow chart of
the study design.
Treatment procedures
This outpatient study consisted of three phases:
(1) screening visit and 48 hours post-screening BP
measurements, (2) 4 weeks of active run-in treatment,
and followed by (3) 20 weeks of prospective
open-label, study treatment. During the screening visit,
patients’demographyandmedicalhistorywererecorded
and patients were screened for the eligibility criteria; 48
hours after the screening visit, BP measurements were
reconfirmed and eligible patients were randomized to
receive4 weeksofactiverun-inmonotherapywitheither
atenolol 25 mg, or chlorthalidone 6.25 mg, or amlodi-
pine 2.5 mg. Subsequently patients who were uncon-
trolled (SBP�140 mmHg and DBP�90 mmHg) on run-
in therapy entered into the 20 weeks’ study treatment
phase. Those patients who were uncontrolled on
atenolol 25 mg were shifted to atenolol 50 mg; those
uncontrolled on chlorthalidone were shifted to atenolol
25 mgþ chlorthalidone 6.25 mg combination, and those
uncontrolled on amlodipine monotherapy were shifted
to amlodipine 2.5 mg þ atenolol 25 mg fixed-dose
combination for the next 20 weeks. The study drugs
were administered orally once daily. Randomization
chartswereprovidedateachcenterbythesponsor.Study
medicationswereprovidedasasingle tablet tobetaken in
the morning. Patients were examined for adverse events
and BP measurements monthly for 6 months.
At each visit, patients’ blood pressure was measured
in the morning prior to taking medications.
The patients were not allowed to take any concomi-
tant antihypertensive medication or any other drug that
could interfere with the study drugs. At each visit, study
medication compliance was assessed by counting the
used and unused strips of study medications.
Efficacy of the therapy in treated patients was
evaluated by mean changes in systolic and diastolic
blood pressure at the end of 12 and 20 weeks from
baseline (after a 4 weeks of active run-in phase). The
percentage of responders at week 12 post-therapy
was used as a secondary efficacy parameter. Blood
pressure measurements were performed at each study
visit during the study period. Measurements were
performedinduplicate,2 minapart inthesittingposition
after 10 min rest, using a sphygmomanometer. Patients
were termed as responders if systolic BP was less than
140 mmHg and diastolic BP was less than 90 mmHg.
Patients who received at least one dose of the study
medication were evaluable for the safety assessment.
Blood samples were obtained at the baseline and at the
end of 6 months’ therapy to perform hematology and
biochemistry tests including complete blood count,
urine routine, ECG, serum electrolytes (Naþ, Cl�,
Kþ), fasting and postprandial blood sugar and lipid
profile (TG, TC).
� 2008 Informa UK - Curr Med Res Opin 2008; 24(06) Low-dose chlorthalidone in stage I hypertension Pareek et al. 1773
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mon
ash
Uni
vers
ity o
n 09
/24/
13Fo
r pe
rson
al u
se o
nly.
Safety evaluation was also based on the adverse events
reported during the study. Adverse events were
categorized by the investigator as mild, moderate or
severe and the relationship to the study drug as none,
probably not, possible, probable or definite. At every
visit during the entire study period, the reported adverse
events, the clinical state of the patients and details of
concomitant medication, if any, were captured.
Assessment
Descriptive statistics, including mean� SD and
median for continuous variables and frequency
counts and percentage for categorical variables were
used to compare treatment groups at baseline with
respect to demographic characteristics. The three
treatment groups were compared for homogeneity at
baseline by using tests like ANOVA, Kruskal–Wallis
test, chi-square test as appropriate.
Efficacy parameter, i.e. fall in systolic blood
pressures and diastolic blood pressure, was measured
from baseline to visit 6. Changes in systolic blood
pressures and diastolic blood pressure after 12 weeks of
therapy for atenolol 50 mg; chlorthalidoneþ atenolol
combination, and amlodipineþ atenolol combination
groups were compared using nonparametric tests
like Kruskal–Wallis. Response rates in each group
were compared using chi-square statistics.
Safety was evaluated by reporting adverse events and
changes in laboratory parameters. Changes in labora-
tory parameters were analyzed using the paired t-test
and the Wilcoxon signed rank test where appropriate.
Statistical analysis was performed using statistical
software MINITAB 15.
Results
A total of 300 patients satisfying eligibility criteria
entered into 4-week active run-in phase. Out of
Patients with stage I essential hypertension
Informed consent
Screening visit (Baseline Laboratory Investigation)
48 h post-screening BP measurements
Eligible Patients (n = 300) Randomized to 4 Weeks of Active run-in Treatments
Atenolol 25 mg (n = 98) Chlorthalidone 6.25 mg (n = 100) Amlodipine 2.5 mg (n = 102)
282 patients completed active run-in
Non-responders to active run-in monotherapies after 4 weeks entered into 20 weeksprospective, open-labeled, study treatment phase
Atenolol 50 mg(n = 33)
[Chlorthalidone 6.25 mg +atenolol 25 mg]
(n = 45)
[Amlodipine 2.5 mg +atenolol 25 mg]
(n = 47)
Efficacy (blood pressure measurement) at every 4 weeks interval and safety (laboratoryinvestigation and adverse events) at the end of study period
Figure 1. Study flow chart
1774 Low-dose chlorthalidone in stage I hypertension � 2008 Informa UK Ltd - Curr Med Res Opin 2008; 24(06)
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mon
ash
Uni
vers
ity o
n 09
/24/
13Fo
r pe
rson
al u
se o
nly.
300 patients, 98 patients were randomized to receive
active run-in therapy with atenolol 25 mg, 100 patients
received chlorthalidone 6.25 mg and the remaining
102 patients received amlodipine 2.5 mg.
Out of 300 patients, 282 patients (atenolol 92,
chlorthalidone 91, amlodipine 99) completed
the active run-in phase successfully. Five patients
from the atenolol group, nine patients from the
chlorthalidone group, and two patients from the
amlodipine group were lost to follow-up during
the active run-in period. One patient from the atenolol
group was withdrawn from the study due to protocol
violation, and one patient from the amlodipine group
due to adverse events.
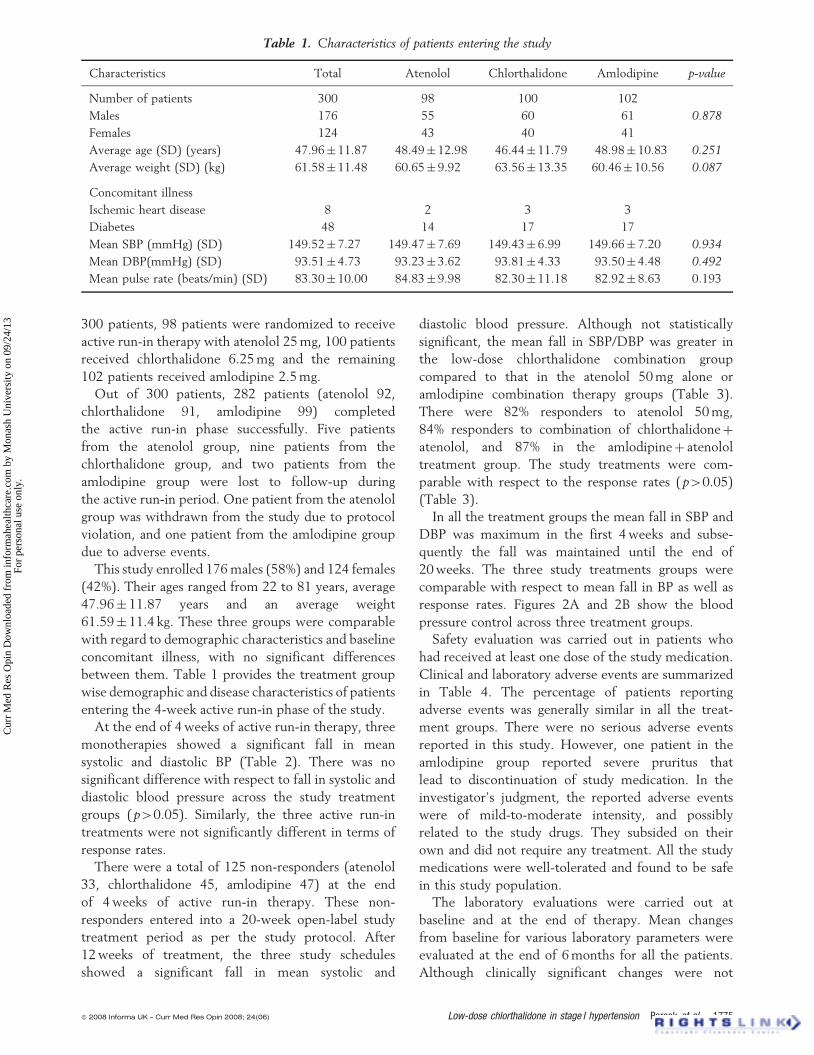
This study enrolled 176 males (58%) and 124 females
(42%). Their ages ranged from 22 to 81 years, average
47.96� 11.87 years and an average weight
61.59� 11.4 kg. These three groups were comparable
with regard to demographic characteristics and baseline
concomitant illness, with no significant differences
between them. Table 1 provides the treatment group
wise demographic and disease characteristics of patients
entering the 4-week active run-in phase of the study.
At the end of 4 weeks of active run-in therapy, three
monotherapies showed a significant fall in mean
systolic and diastolic BP (Table 2). There was no
significant difference with respect to fall in systolic and
diastolic blood pressure across the study treatment
groups (p40.05). Similarly, the three active run-in
treatments were not significantly different in terms of
response rates.
There were a total of 125 non-responders (atenolol
33, chlorthalidone 45, amlodipine 47) at the end
of 4 weeks of active run-in therapy. These non-
responders entered into a 20-week open-label study
treatment period as per the study protocol. After
12 weeks of treatment, the three study schedules
showed a significant fall in mean systolic and
diastolic blood pressure. Although not statistically
significant, the mean fall in SBP/DBP was greater in
the low-dose chlorthalidone combination group
compared to that in the atenolol 50 mg alone or
amlodipine combination therapy groups (Table 3).
There were 82% responders to atenolol 50 mg,
84% responders to combination of chlorthalidoneþ
atenolol, and 87% in the amlodipineþ atenolol
treatment group. The study treatments were com-
parable with respect to the response rates (p40.05)
(Table 3).
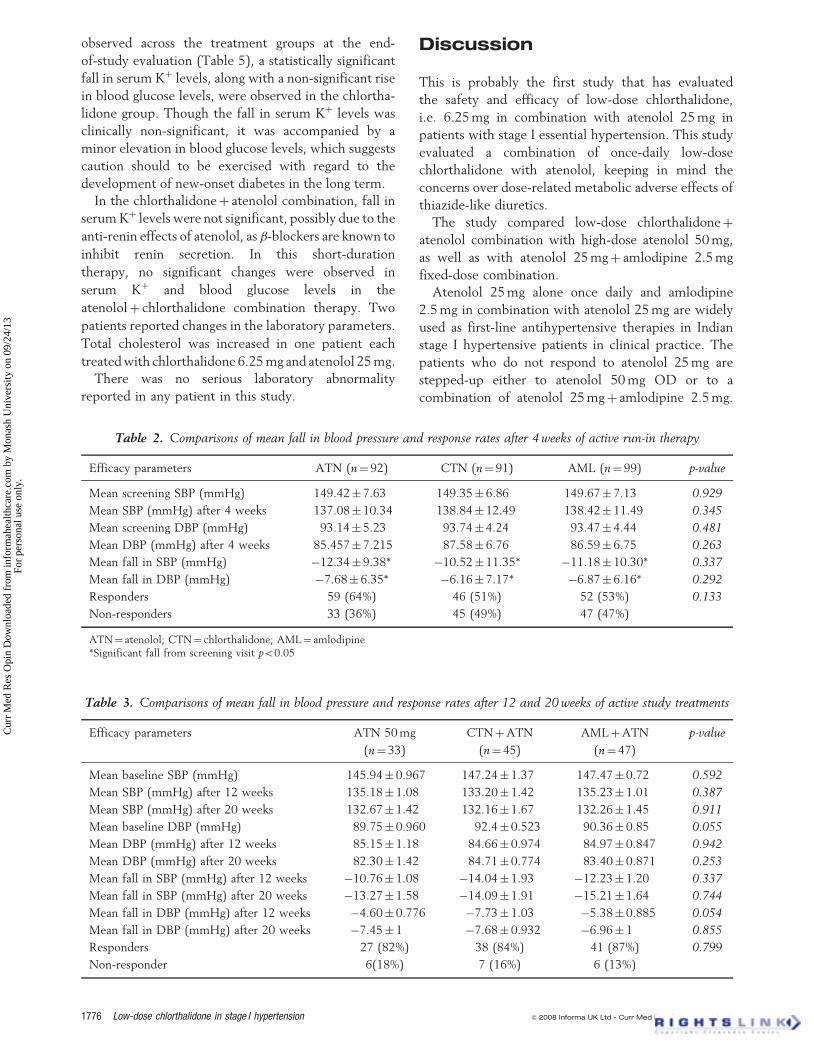
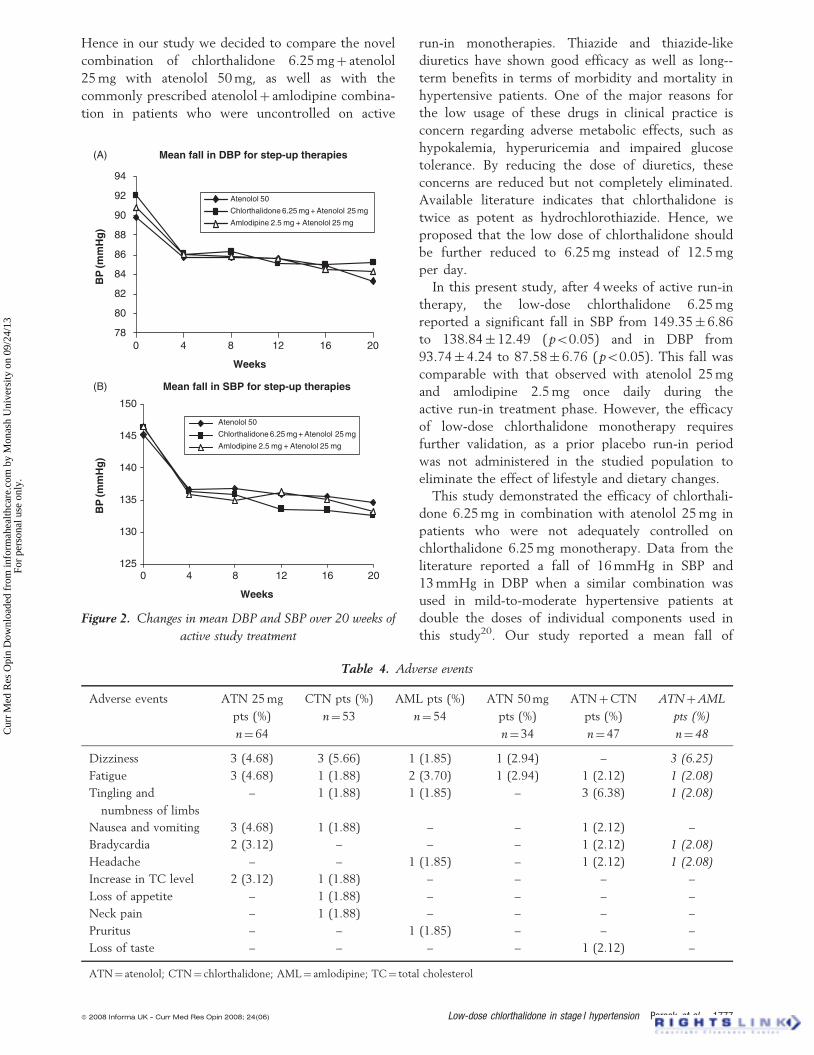
In all the treatment groups the mean fall in SBP and
DBP was maximum in the first 4 weeks and subse-
quently the fall was maintained until the end of
20 weeks. The three study treatments groups were
comparable with respect to mean fall in BP as well as
response rates. Figures 2A and 2B show the blood
pressure control across three treatment groups.
Safety evaluation was carried out in patients who
had received at least one dose of the study medication.
Clinical and laboratory adverse events are summarized
in Table 4. The percentage of patients reporting
adverse events was generally similar in all the treat-
ment groups. There were no serious adverse events
reported in this study. However, one patient in the
amlodipine group reported severe pruritus that
lead to discontinuation of study medication. In the
investigator’s judgment, the reported adverse events
were of mild-to-moderate intensity, and possibly
related to the study drugs. They subsided on their
own and did not require any treatment. All the study
medications were well-tolerated and found to be safe
in this study population.
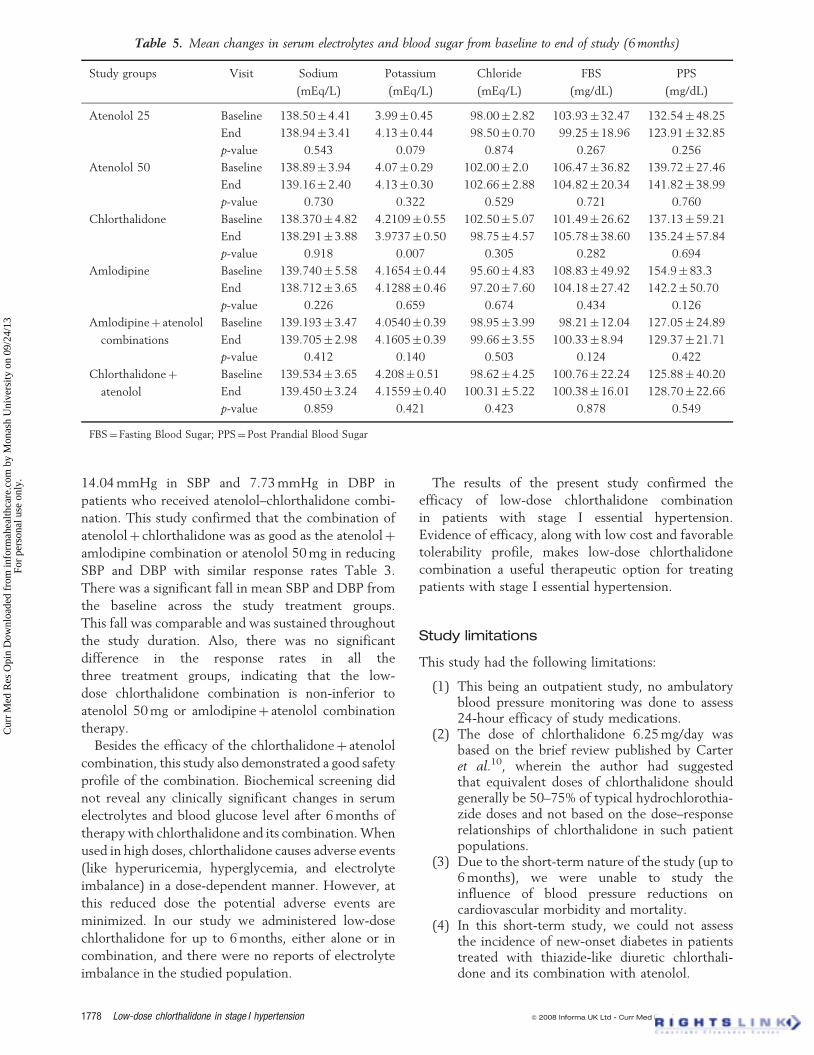
The laboratory evaluations were carried out at
baseline and at the end of therapy. Mean changes
from baseline for various laboratory parameters were
evaluated at the end of 6 months for all the patients.
Although clinically significant changes were not
Table 1. Characteristics of patients entering the study
Characteristics Total Atenolol Chlorthalidone Amlodipine p-value
Number of patients 300 98 100 102
Males 176 55 60 61 0.878
Females 124 43 40 41
Average age (SD) (years) 47.96� 11.87 48.49� 12.98 46.44� 11.79 48.98� 10.83 0.251
Average weight (SD) (kg) 61.58� 11.48 60.65� 9.92 63.56� 13.35 60.46� 10.56 0.087
Concomitant illness
Ischemic heart disease 8 2 3 3
Diabetes 48 14 17 17
Mean SBP (mmHg) (SD) 149.52� 7.27 149.47� 7.69 149.43� 6.99 149.66� 7.20 0.934
Mean DBP(mmHg) (SD) 93.51� 4.73 93.23� 3.62 93.81� 4.33 93.50� 4.48 0.492
Mean pulse rate (beats/min) (SD) 83.30� 10.00 84.83� 9.98 82.30� 11.18 82.92� 8.63 0.193
� 2008 Informa UK - Curr Med Res Opin 2008; 24(06) Low-dose chlorthalidone in stage I hypertension Pareek et al. 1775
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mon
ash
Uni
vers
ity o
n 09
/24/
13Fo
r pe
rson
al u
se o
nly.
observed across the treatment groups at the end-
of-study evaluation (Table 5), a statistically significant
fall in serum Kþ levels, along with a non-significant rise
in blood glucose levels, were observed in the chlortha-
lidone group. Though the fall in serum Kþ levels was
clinically non-significant, it was accompanied by a
minor elevation in blood glucose levels, which suggests
caution should to be exercised with regard to the
development of new-onset diabetes in the long term.
In the chlorthalidoneþ atenolol combination, fall in
serum Kþ levels were not significant, possibly due to the
anti-renin effects of atenolol, as �-blockers are known to
inhibit renin secretion. In this short-duration
therapy, no significant changes were observed in
serum Kþ and blood glucose levels in the
atenololþ chlorthalidone combination therapy. Two
patients reported changes in the laboratory parameters.
Total cholesterol was increased in one patient each
treated with chlorthalidone 6.25 mg and atenolol 25 mg.
There was no serious laboratory abnormality
reported in any patient in this study.
Discussion
This is probably the first study that has evaluated
the safety and efficacy of low-dose chlorthalidone,
i.e. 6.25 mg in combination with atenolol 25 mg in
patients with stage I essential hypertension. This study
evaluated a combination of once-daily low-dose
chlorthalidone with atenolol, keeping in mind the
concerns over dose-related metabolic adverse effects of
thiazide-like diuretics.
The study compared low-dose chlorthalidoneþ
atenolol combination with high-dose atenolol 50 mg,
as well as with atenolol 25 mgþ amlodipine 2.5 mg
fixed-dose combination.
Atenolol 25 mg alone once daily and amlodipine
2.5 mg in combination with atenolol 25 mg are widely
used as first-line antihypertensive therapies in Indian
stage I hypertensive patients in clinical practice. The
patients who do not respond to atenolol 25 mg are
stepped-up either to atenolol 50 mg OD or to a
combination of atenolol 25 mgþ amlodipine 2.5 mg.
Table 3. Comparisons of mean fall in blood pressure and response rates after 12 and 20 weeks of active study treatments
Efficacy parameters ATN 50 mg
(n¼ 33)
CTNþATN
(n¼ 45)
AMLþATN
(n¼ 47)
p-value
Mean baseline SBP (mmHg) 145.94� 0.967 147.24� 1.37 147.47� 0.72 0.592
Mean SBP (mmHg) after 12 weeks 135.18� 1.08 133.20� 1.42 135.23� 1.01 0.387
Mean SBP (mmHg) after 20 weeks 132.67� 1.42 132.16� 1.67 132.26� 1.45 0.911
Mean baseline DBP (mmHg) 89.75� 0.960 92.4� 0.523 90.36� 0.85 0.055
Mean DBP (mmHg) after 12 weeks 85.15� 1.18 84.66� 0.974 84.97� 0.847 0.942
Mean DBP (mmHg) after 20 weeks 82.30� 1.42 84.71� 0.774 83.40� 0.871 0.253
Mean fall in SBP (mmHg) after 12 weeks �10.76� 1.08 �14.04� 1.93 �12.23� 1.20 0.337
Mean fall in SBP (mmHg) after 20 weeks �13.27� 1.58 �14.09� 1.91 �15.21� 1.64 0.744
Mean fall in DBP (mmHg) after 12 weeks �4.60� 0.776 �7.73� 1.03 �5.38� 0.885 0.054
Mean fall in DBP (mmHg) after 20 weeks �7.45� 1 �7.68� 0.932 �6.96� 1 0.855
Responders 27 (82%) 38 (84%) 41 (87%) 0.799
Non-responder 6(18%) 7 (16%) 6 (13%)
Table 2. Comparisons of mean fall in blood pressure and response rates after 4 weeks of active run-in therapy
Efficacy parameters ATN (n¼ 92) CTN (n¼ 91) AML (n¼ 99) p-value
Mean screening SBP (mmHg) 149.42� 7.63 149.35� 6.86 149.67� 7.13 0.929
Mean SBP (mmHg) after 4 weeks 137.08� 10.34 138.84� 12.49 138.42� 11.49 0.345
Mean screening DBP (mmHg) 93.14� 5.23 93.74� 4.24 93.47� 4.44 0.481
Mean DBP (mmHg) after 4 weeks 85.457� 7.215 87.58� 6.76 86.59� 6.75 0.263
Mean fall in SBP (mmHg) �12.34� 9.38* �10.52� 11.35* �11.18� 10.30* 0.337
Mean fall in DBP (mmHg) �7.68� 6.35* �6.16� 7.17* �6.87� 6.16* 0.292
Responders 59 (64%) 46 (51%) 52 (53%) 0.133
Non-responders 33 (36%) 45 (49%) 47 (47%)
ATN¼ atenolol; CTN¼ chlorthalidone; AML¼ amlodipine*Significant fall from screening visit p50.05
1776 Low-dose chlorthalidone in stage I hypertension � 2008 Informa UK Ltd - Curr Med Res Opin 2008; 24(06)
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mon
ash
Uni
vers
ity o
n 09
/24/
13Fo
r pe
rson
al u
se o
nly.
Hence in our study we decided to compare the novel
combination of chlorthalidone 6.25 mgþ atenolol
25 mg with atenolol 50 mg, as well as with the
commonly prescribed atenololþ amlodipine combina-
tion in patients who were uncontrolled on active
run-in monotherapies. Thiazide and thiazide-like
diuretics have shown good efficacy as well as long--
term benefits in terms of morbidity and mortality in
hypertensive patients. One of the major reasons for
the low usage of these drugs in clinical practice is
concern regarding adverse metabolic effects, such as
hypokalemia, hyperuricemia and impaired glucose
tolerance. By reducing the dose of diuretics, these
concerns are reduced but not completely eliminated.
Available literature indicates that chlorthalidone is
twice as potent as hydrochlorothiazide. Hence, we
proposed that the low dose of chlorthalidone should
be further reduced to 6.25 mg instead of 12.5 mg
per day.
In this present study, after 4 weeks of active run-in
therapy, the low-dose chlorthalidone 6.25 mg
reported a significant fall in SBP from 149.35�6.86
to 138.84� 12.49 (p50.05) and in DBP from
93.74� 4.24 to 87.58� 6.76 (p50.05). This fall was
comparable with that observed with atenolol 25 mg
and amlodipine 2.5 mg once daily during the
active run-in treatment phase. However, the efficacy
of low-dose chlorthalidone monotherapy requires
further validation, as a prior placebo run-in period
was not administered in the studied population to
eliminate the effect of lifestyle and dietary changes.
This study demonstrated the efficacy of chlorthali-
done 6.25 mg in combination with atenolol 25 mg in
patients who were not adequately controlled on
chlorthalidone 6.25 mg monotherapy. Data from the
literature reported a fall of 16 mmHg in SBP and
13 mmHg in DBP when a similar combination was
used in mild-to-moderate hypertensive patients at
double the doses of individual components used in
this study20. Our study reported a mean fall of
Table 4. Adverse events
Adverse events ATN 25 mg
pts (%)
n¼ 64
CTN pts (%)
n¼ 53
AML pts (%)
n¼ 54
ATN 50 mg
pts (%)
n¼ 34
ATNþCTN
pts (%)
n¼ 47
ATNþAML
pts (%)
n¼ 48
Dizziness 3 (4.68) 3 (5.66) 1 (1.85) 1 (2.94) – 3 (6.25)
Fatigue 3 (4.68) 1 (1.88) 2 (3.70) 1 (2.94) 1 (2.12) 1 (2.08)
Tingling and
numbness of limbs
– 1 (1.88) 1 (1.85) – 3 (6.38) 1 (2.08)
Nausea and vomiting 3 (4.68) 1 (1.88) – – 1 (2.12) –
Bradycardia 2 (3.12) – – – 1 (2.12) 1 (2.08)
Headache – – 1 (1.85) – 1 (2.12) 1 (2.08)
Increase in TC level 2 (3.12) 1 (1.88) – – – –
Loss of appetite – 1 (1.88) – – – –
Neck pain – 1 (1.88) – – – –
Pruritus – – 1 (1.85) – – –
Loss of taste – – – – 1 (2.12) –
ATN¼ atenolol; CTN¼ chlorthalidone; AML¼ amlodipine; TC¼ total cholesterol
78
80
82
84
86
88
90
92
94
BP
(mm
Hg
)
(A)
125
130
135
140
145
150
0 4 8 16 20
BP
(mm
Hg
)
Atenolol 50
Chlorthalidone 6.25 mg + Atenolol 25 mg
Amlodipine 2.5 mg + Atenolol 25 mg
Atenolol 50
Chlorthalidone 6.25 mg + Atenolol 25 mg
Amlodipine 2.5 mg + Atenolol 25 mg
(B) Mean fall in SBP for step-up therapies
Mean fall in DBP for step-up therapies
Weeks
12
0 4 8 16 20
Weeks
12
Figure 2. Changes in mean DBP and SBP over 20 weeks of
active study treatment
� 2008 Informa UK - Curr Med Res Opin 2008; 24(06) Low-dose chlorthalidone in stage I hypertension Pareek et al. 1777
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mon
ash
Uni
vers
ity o
n 09
/24/
13Fo
r pe
rson
al u
se o
nly.
14.04 mmHg in SBP and 7.73 mmHg in DBP in
patients who received atenolol–chlorthalidone combi-
nation. This study confirmed that the combination of
atenololþ chlorthalidone was as good as the atenololþ
amlodipine combination or atenolol 50 mg in reducing
SBP and DBP with similar response rates Table 3.
There was a significant fall in mean SBP and DBP from
the baseline across the study treatment groups.
This fall was comparable and was sustained throughout
the study duration. Also, there was no significant
difference in the response rates in all the
three treatment groups, indicating that the low-
dose chlorthalidone combination is non-inferior to
atenolol 50 mg or amlodipineþ atenolol combination
therapy.
Besides the efficacy of the chlorthalidoneþ atenolol
combination, this study also demonstrated a good safety
profile of the combination. Biochemical screening did
not reveal any clinically significant changes in serum
electrolytes and blood glucose level after 6 months of
therapy with chlorthalidone and its combination. When
used in high doses, chlorthalidone causes adverse events
(like hyperuricemia, hyperglycemia, and electrolyte
imbalance) in a dose-dependent manner. However, at
this reduced dose the potential adverse events are
minimized. In our study we administered low-dose
chlorthalidone for up to 6 months, either alone or in
combination, and there were no reports of electrolyte
imbalance in the studied population.
The results of the present study confirmed the
efficacy of low-dose chlorthalidone combination
in patients with stage I essential hypertension.
Evidence of efficacy, along with low cost and favorable
tolerability profile, makes low-dose chlorthalidone
combination a useful therapeutic option for treating
patients with stage I essential hypertension.
Study limitations
This study had the following limitations:
(1) This being an outpatient study, no ambulatoryblood pressure monitoring was done to assess24-hour efficacy of study medications.
(2) The dose of chlorthalidone 6.25 mg/day wasbased on the brief review published by Carteret al.10, wherein the author had suggestedthat equivalent doses of chlorthalidone shouldgenerally be 50–75% of typical hydrochlorothia-zide doses and not based on the dose–responserelationships of chlorthalidone in such patientpopulations.
(3) Due to the short-term nature of the study (up to6 months), we were unable to study theinfluence of blood pressure reductions oncardiovascular morbidity and mortality.
(4) In this short-term study, we could not assessthe incidence of new-onset diabetes in patientstreated with thiazide-like diuretic chlorthali-done and its combination with atenolol.
Table 5. Mean changes in serum electrolytes and blood sugar from baseline to end of study (6 months)
Study groups Visit Sodium
(mEq/L)
Potassium
(mEq/L)
Chloride
(mEq/L)
FBS
(mg/dL)
PPS
(mg/dL)
Atenolol 25 Baseline 138.50� 4.41 3.99� 0.45 98.00� 2.82 103.93� 32.47 132.54� 48.25
End 138.94� 3.41 4.13� 0.44 98.50� 0.70 99.25� 18.96 123.91� 32.85
p-value 0.543 0.079 0.874 0.267 0.256
Atenolol 50 Baseline 138.89� 3.94 4.07� 0.29 102.00� 2.0 106.47� 36.82 139.72� 27.46
End 139.16� 2.40 4.13� 0.30 102.66� 2.88 104.82� 20.34 141.82� 38.99
p-value 0.730 0.322 0.529 0.721 0.760
Chlorthalidone Baseline 138.370� 4.82 4.2109� 0.55 102.50� 5.07 101.49� 26.62 137.13� 59.21
End 138.291� 3.88 3.9737� 0.50 98.75� 4.57 105.78� 38.60 135.24� 57.84
p-value 0.918 0.007 0.305 0.282 0.694
Amlodipine Baseline 139.740� 5.58 4.1654� 0.44 95.60� 4.83 108.83� 49.92 154.9� 83.3
End 138.712� 3.65 4.1288� 0.46 97.20� 7.60 104.18�27.42 142.2� 50.70
p-value 0.226 0.659 0.674 0.434 0.126
Amlodipineþ atenolol
combinations
Baseline 139.193� 3.47 4.0540� 0.39 98.95� 3.99 98.21� 12.04 127.05� 24.89
End 139.705� 2.98 4.1605� 0.39 99.66� 3.55 100.33� 8.94 129.37� 21.71
p-value 0.412 0.140 0.503 0.124 0.422
Chlorthalidoneþ
atenolol
Baseline 139.534� 3.65 4.208�0.51 98.62� 4.25 100.76� 22.24 125.88� 40.20
End 139.450� 3.24 4.1559� 0.40 100.31� 5.22 100.38� 16.01 128.70� 22.66
p-value 0.859 0.421 0.423 0.878 0.549
FBS¼Fasting Blood Sugar; PPS¼Post Prandial Blood Sugar
1778 Low-dose chlorthalidone in stage I hypertension � 2008 Informa UK Ltd - Curr Med Res Opin 2008; 24(06)
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mon
ash
Uni
vers
ity o
n 09
/24/
13Fo
r pe
rson
al u
se o
nly.

Conclusion
Low-dose chlorthalidone, i.e. 6.25 mg in combination
with atenolol 25 mg, is found to be effective and
safe in patients with stage I (JNC 7) essential
hypertension. The combination of low-dose chlortha-
lidoneþ atenolol is as effective as a combination of
amlodipineþ atenolol, as well as high-dose atenolol
monotherapy. If future clinical trials using chlorthali-
done 6.25 mg confirm its efficacy, then this dose could
reduce the concerns of metabolic adverse effects and
could lead to its wider usage in clinical practice.
Acknowledgements
Declaration of interest: This study was sponsored by
Ipca Laboratories Ltd., Mumbai, India. A. Pareek
and N.B. Chandurkar, who are employees of Ipca
Labs Ltd, were involved in the conceptualization,
coordination and execution of the study, at all the
centers. N.D. Karnik, S.B. Salagre, S.D. Zawar and
V.K. Joglekar, who were study investigators, did not
receive any financial benefit and declare that they
have no conflicts of interest of a declarable nature.
The authors thank S.R Kulkarni and G.S. Naik (of
Ipca Labs Ltd) for technical assistance and S.P. Dixit
(of Ipca Labs Ltd) for statistical analysis and data
management for this study. The authors would also
like to thank C.Y. Nimkar, who served as an external
consultant for statistical analysis.
References1. Scholze J, Bida M, Hansen A, et al. Initiation of hypertension
treatment with a fixed dose combination or its monocomponents– Does it really matter? Int J Clinical Pract 2006;60:265-74
2. The ALLHAT Officers and Coordinators for the ALLHATCollaborative Research Group. Major outcomes in high riskhypertensive patients randomized to angiotensin-convertingenzyme inhibitor or calcium channel blocker vs diuretic.The Antihypertensive and Lipid-Lowering Treatment toPrevent Heart Attack Trial. JAMA 2002;288:2981–97
3. Wright JT, Dunn JK, Cutler JA, et al. For the ALLHATCollaborative Research Group. Outcomes in hypertensive blackand nonblack patients treated with chlorthalidone, amlodipine,and lisinopril. JAMA 2005;293:1595-608
4. Psaty BM, Lumley T, Furberg CD, et al. Health outcomesassociated with various antihypertensive therapies used as first-line agents: a network meta-analysis. JAMA 2003;289:2534-44
5. Five-year findings of the hypertension detection and follow-upprogram. I. Reduction in mortality of persons with high
blood pressure, including mild hypertension. Hypertension
Detection and Follow-up Program Cooperative Group. JAMA
1979;242:2562–716. The Multiple Risk Factor Intervention Trial Research Group
(MRFIT). Mortality rates after 10.5 years for hypertensive
participants in the Multiple Risk Factor Intervention Trial.
Circulation 1990;82:1616–287. SHEP Cooperative Research Group. Prevention of stroke by
antihypertensive drug treatment in older persons with isolated
systolic hypertension. Final results of the Systolic Hypertension
in the Elderly Program (SHEP). JAMA 1991;265:3255–648. Neaton JD, Grimm RH, Prineas RJ, et al. For the Treatment
of Mild Hypertension Study Research Group. Treatment of
mild hypertension study. Final results. Treatment of Mild
Hypertension Study Research Group. JAMA 1993;270:713-249. Chobanian AV, Bakris GL, Black HR, et al. Joint National
Committee on Detection, Evaluation, and Treatment of High
Blood Pressure. The seventh report of the Joint National
Committee on Detection, Evaluation, and Treatment of High
Blood Pressure (JNC 7). JAMA 2003;289:2560-7210. Barry LC, Michael EE, Jerome DC. Hydrochlorothiazide versus
chlorthalidone: evidence supporting their interchangeability.
Hypertension 2004;43:4-911. Barry LC, Chris JG, Jennifer JG, et al. Comparative anti-
hypertensive effects of hydrochlorothiazide and chlorthalidone
on ambulatory and office blood pressure. Hypertension
2006;47:352-812. Ruzicka M, Leenen FH. Combination therapy as firstline
treatment of arterial hypertension. Can J Cardiol 2002;18:
1317-2713. Cushman WC, Ford CE, Cutler JA, et al. Success and
predictors of blood pressure control in diverse North
American settings: The Antihypertensive and Lipid-Lowering
Treatment to Prevent Heart Attack Trial (ALLHAT). J Clin
Hypertens 2002;4:393-40414. Hansson L, Zanchetti A, Carruthers SG, et al. Effects of
intensive blood-pressure lowering and low-dose aspirin in
patients with hypertension: principal results of the
Hypertension Optimal Treatment (HOT) randomized trial.
HOT Study Group. Lancet 1998;26:S80-215. Black HR, Elliot WJ, Grandits G, et al. Principal results of the
Controlled Onset Verapramil Investigation of Cardiovascular
End Points (CONVINCE) trial. JAMA 2003;289:2073-8216. Dahlof B, Devereux RB, Kjeldsen SE, et al. Cardiovascular
morbidity and mortality in the Losartan Intervention for
Endpoint Reduction in Hypertensive Study (LIFE): a rando-
mized trial against atenolol. Lancet 2002;359:995-100317. Materson BJ, Reda DJ, Cushman WC, et al. Single-drug
therapy for hypertension in men. A comparison of six
antihypertensive agents with placebo. The Department of
Veterans Affairs Cooperative Study Group on
Antihypertensive Agents. N Engl J Med 1993;328:914-2118. 2003 European Society of Hypertension – European Society
of Cardiology Guidelines for the management of arterial
hypertension. J Hypertens 2003;21:1011–5319. Zidek W. Hochdruckleitlinien iiberabeitet. Was ist
Praxisrelevant? MMW Fortschr Med 2004;1–2:16/37-8/1720. Curry RC Jr Schwartz KM, Urban PL. Atenolol and chlortha-
lidone therapy for hypertension: a double blind comparison.
South Med J 1988;81:1401-6, 1411
CrossRef links are available in the online published version of this paper:
http://www.cmrojournal.com
Paper CMRO-4517_4, Accepted for publication: 10 April 2008
Published Online: 9 May 2008
doi:10.1185/03007990802118071
� 2008 Informa UK - Curr Med Res Opin 2008; 24(06) Low-dose chlorthalidone in stage I hypertension Pareek et al. 1779
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mon
ash
Uni
vers
ity o
n 09
/24/
13Fo
r pe
rson
al u
se o
nly.