clavicle fracture following tight rope fixation of acromioclavicular joint dislocation
TRANSCRIPT
CASE REPORT
Clavicle fracture following Tight Rope fixation ofacromioclavicular joint dislocation
Simon V. Ball *, Andrew Sankey, Carlos Cobiella
Injury Extra (2007) 38, 430—432
www.elsevier.com/locate/inext
Orthopaedic Department, University College Hospital, London, UK
Accepted 9 February 2007
Case report
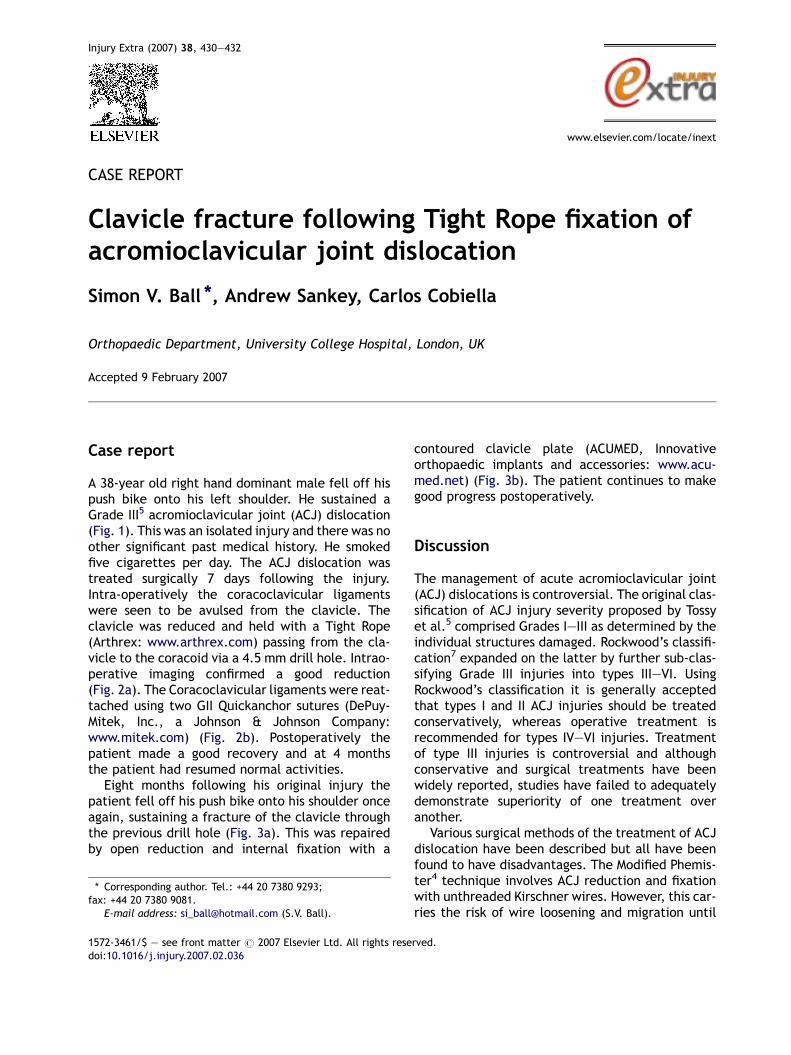
A 38-year old right hand dominant male fell off hispush bike onto his left shoulder. He sustained aGrade III5 acromioclavicular joint (ACJ) dislocation(Fig. 1). This was an isolated injury and there was noother significant past medical history. He smokedfive cigarettes per day. The ACJ dislocation wastreated surgically 7 days following the injury.Intra-operatively the coracoclavicular ligamentswere seen to be avulsed from the clavicle. Theclavicle was reduced and held with a Tight Rope(Arthrex: www.arthrex.com) passing from the cla-vicle to the coracoid via a 4.5 mm drill hole. Intrao-perative imaging confirmed a good reduction(Fig. 2a). The Coracoclavicular ligaments were reat-tached using two GII Quickanchor sutures (DePuy-Mitek, Inc., a Johnson & Johnson Company:www.mitek.com) (Fig. 2b). Postoperatively thepatient made a good recovery and at 4 monthsthe patient had resumed normal activities.
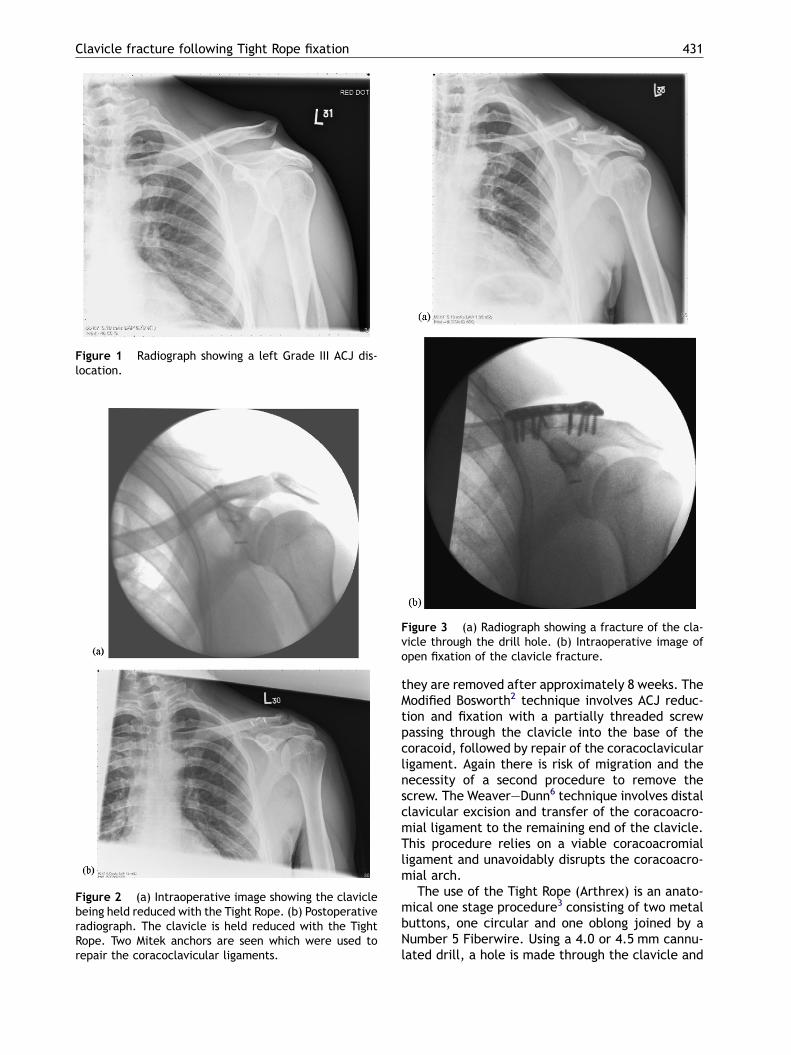
Eight months following his original injury thepatient fell off his push bike onto his shoulder onceagain, sustaining a fracture of the clavicle throughthe previous drill hole (Fig. 3a). This was repairedby open reduction and internal fixation with a
* Corresponding author. Tel.: +44 20 7380 9293;fax: +44 20 7380 9081.
E-mail address: [email protected] (S.V. Ball).
1572-3461/$ — see front matter # 2007 Elsevier Ltd. All rights resedoi:10.1016/j.injury.2007.02.036
contoured clavicle plate (ACUMED, Innovativeorthopaedic implants and accessories: www.acu-med.net) (Fig. 3b). The patient continues to makegood progress postoperatively.
Discussion
The management of acute acromioclavicular joint(ACJ) dislocations is controversial. The original clas-sification of ACJ injury severity proposed by Tossyet al.5 comprised Grades I—III as determined by theindividual structures damaged. Rockwood’s classifi-cation7 expanded on the latter by further sub-clas-sifying Grade III injuries into types III—VI. UsingRockwood’s classification it is generally acceptedthat types I and II ACJ injuries should be treatedconservatively, whereas operative treatment isrecommended for types IV—VI injuries. Treatmentof type III injuries is controversial and althoughconservative and surgical treatments have beenwidely reported, studies have failed to adequatelydemonstrate superiority of one treatment overanother.
Various surgical methods of the treatment of ACJdislocation have been described but all have beenfound to have disadvantages. The Modified Phemis-ter4 technique involves ACJ reduction and fixationwith unthreaded Kirschner wires. However, this car-ries the risk of wire loosening and migration until
rved.
Clavicle fracture following Tight Rope fixation 431
Figure 1 Radiograph showing a left Grade III ACJ dis-location.
Figure 2 (a) Intraoperative image showing the claviclebeing held reduced with the Tight Rope. (b) Postoperativeradiograph. The clavicle is held reduced with the TightRope. Two Mitek anchors are seen which were used torepair the coracoclavicular ligaments.
Figure 3 (a) Radiograph showing a fracture of the cla-vicle through the drill hole. (b) Intraoperative image ofopen fixation of the clavicle fracture.
they are removed after approximately 8 weeks. TheModified Bosworth2 technique involves ACJ reduc-tion and fixation with a partially threaded screwpassing through the clavicle into the base of thecoracoid, followed by repair of the coracoclavicularligament. Again there is risk of migration and thenecessity of a second procedure to remove thescrew. The Weaver—Dunn6 technique involves distalclavicular excision and transfer of the coracoacro-mial ligament to the remaining end of the clavicle.This procedure relies on a viable coracoacromialligament and unavoidably disrupts the coracoacro-mial arch.
The use of the Tight Rope (Arthrex) is an anato-mical one stage procedure3 consisting of two metalbuttons, one circular and one oblong joined by aNumber 5 Fiberwire. Using a 4.0 or 4.5 mm cannu-lated drill, a hole is made through the clavicle and

432 S.V. Ball et al.
the coracoid. The Tight Rope system is passedthrough, the dislocation is reduced and the systemsecured in place.1 The coracoclavicular ligamentsmay also be repaired using anchor sutures to addfurther stability. Postoperatively a sling is used for 4weeks with the patient only removing it for washingand elbow flexion and extension exercises. Phy-siotherapy is then commenced with movementslimited to below shoulder height. At 6 weeks fullactive motion is commenced. Heavy resistance workshould be avoided for 3 months after the operation.
To date there have been no reports into thebenefits and complications of the Tight Rope tech-nique for ACJ dislocations. It is thought that thebenefits are anatomical reduction with a minimallyinvasive approach and a one stage procedure. Herewe report a complication of this technique whichhas neither been described in the literature norreported to the manufacturers of the Tight Ropesystem (Arthrex). We recognise that there was sig-nificant trauma leading to the clavicle fracturehowever we do believe that surgeons should beaware that this technique may leave the patientsusceptible to clavicle fracture through the drillhole used. This theoretical increased risk is due tothe drill hole being occupied by non-absorbablematerial. It is however widely accepted that if adrill hole remains unoccupied it becomes mechani-cally insignificant after approximately 8 weeks. It istherefore not unreasonable to suggest that theTight Rope system should be removed once therehas been sufficient healing for the ACJ to no longerrequire mechanical assistance from the Tight Ropesystem to remain reduced. This is normally after 8—12 weeks. The Tight Rope may be removed via
arthroscopy and the procedure may be done as aday case. It is however a second procedure whichcontradicts the advert that the Tight Rope techni-que is a one stage procedure.
For optimal results we do recommend that theTight Rope system be removed as mentioned. We dohowever recognise that this has significant costimplications and the risk of fracture through theoccupied drill hole may be low. As the Tight Ropetechnique is used more commonly more data will beavailable and the risk may be more accuratelyquantified. In the meantime surgeons should beaware of this potential problem.
References
1. Arthrex. Arthroscopic Stabilisation of Acute AcromioclavicularJoint Dislocation using the Tight Rope System: Surgical Tech-nique, www.athrex.com.
2. Bosworth BM. Complete acromioclavicular dislocation. N Eng JMed 1949;41:221—5.
3. Hernegger GS, Kadletz R. Tight Rope — the revolutionaryanatomical fixation in acromioclavicular joint dislocation —a case report. Techniques Shoulder Elbow Surg 2006;7(2):86—8.
4. Phemister DB. The treatment of dislocation of acromioclavi-cular joint by open reduction and threaded-wire fixation. JBone Joint Surg 1942;24:166.
5. Tossy JD, Mead NC, Sigmond HM. Acromioclavicular separa-tions: useful and practical classification for treatment. ClinOrthopaed Relat Res 1963;28:111—9.
6. Weaver JK, Dunn HK. Treatment of acromioclavicular injuries,especially complete acromioclavicular separation. J BoneJoint Surg Am 1972;54A:1187—94.
7. Williams GR, Nguyen VD, Rockwood CA. Classification andradiographic analysis of acromioclavicular dislocations. ApplRadiol 1989;29—34.