classification of receptors - meduni wien...classification of receptors 1. g protein coupled...
TRANSCRIPT

Classification of Receptors
1. G Protein coupled receptors epinephrine, serotonine, glucagon
2. Ion channel receptors acetylcholine receptor
3. Tyrosine kinase-linked receptors cytokine-receptor family
4. Receptors with intrinsic enzymatic activity the receptor has intrinsic catalytic activity receptor tyrosine kinases

Receptors with intrinsic enzymatic activity
1. Guanylatcyclase: GTP -> cGMP ANP: peptide hormone, atrium of the heart upon
Upon rising blood pressure – decreases vascular resistance via a cGMP dependent kinase
2. serin-threonine kinases: TGF –ß superfamily
growth inhibition, bone formation,
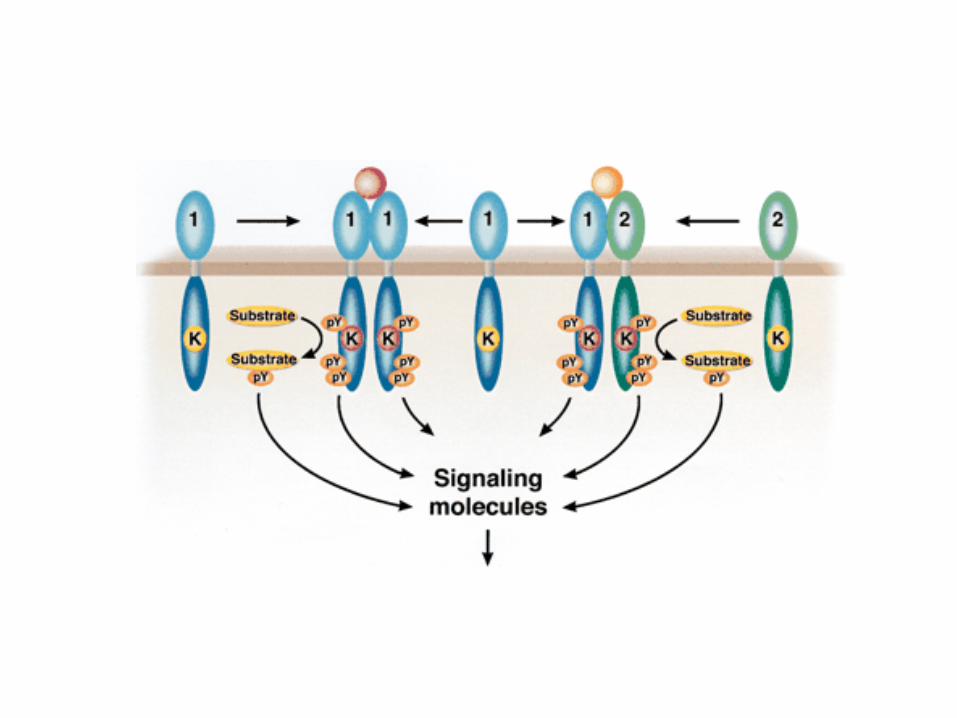
3. receptor tyrosine phosphatases: CD45, expressed on B and T lymphocytes
4. RTKs: EGFR, Insulin, VEGFR

The ANP Receptor

Receptors with intrinsic enzymatic activity
1. Guanylatcyclase: GTP -> cGMP ANP: peptide hormone, atrium of the heart upon
rising blood pressure – decreases vascular resistance via a cGMP dependent kinase
2. serin-threonine kinases: TGF –ß superfamily
growth inhibition, bone formation,
3. receptor tyrosine phosphatases: CD45, expressed on B and T lymphocytes
4. RTKs: EGFR, Insulin, VEGFR

cell type specific glykosylation
B220 B cell specific
CD45 exists in various isoforms
D1: active phosphatase highly conserved
D2: inactive required for
correct folding


Constitutive activation of CD45 leads to lymphoproliferation and autoimmunity in mice
Cell 2000, 103: 1059
Inactivation of CD45 leads to Severe combined Immuno Deficiency (SCID)
Nature Med 2000, 6:343
The hematopoietic-specific transmembrane protein tyrosine phosphatase CD45 functions to regulate Src kinases required for T- and B-cell antigen receptor signal transduction. So far, there have been no reports to our knowledge of a human deficiency in a tyrosine-specific phosphatase. Here, we identified a male patient with a deficiency in CD45 due to a large deletion at one allele and a point mutation at the other. The point mutation resulted in the alteration of intervening sequence 13 donor splice site. The patient presented at 2 months of age with severe combined immunodeficiency disease. The population of peripheral blood T lymphocytes was greatly diminished and unresponsive to mitogen stimulation. Despite normal B-lymphocyte numbers, serum immunoglobulin levels decreased with age. Thus, CD45 deficiency in humans results in T- and B-lymphocyte dysfunction.

Implications for Medicine
Inhibitors of CD45 have implications in transplant medicine – prevention of kidney rejection in mouse models has been proven microglial activation by ß-amyloid peptide can be prevented – Alzheimers disease the various specific activatio forms may allow for a relatively specific inhibition dependent on the indication

RTKs
NGF, PDGF, FGF, EGF, Insulin
regulate cell survival, proliferation, differentiation therefore found in cancer constitutive active RTKs
RTKs-ras as important signalling
cascade leading to cancer

ligand binds a dimer –
dimerization of the receptor –
activation of its kinase activity –
tyrosine phosphorylation of its own cytosolic domaine


RTKs are frequent targets in human cancer

Signalling Pathways in Cancer downstream of RTK

Sorafenib • Hemmt Serin/Threonin- und Rezeptor-Tyrosinkinasen • = Multikinasenhemmer • Greift in RAS-Signasltransduktionsweg ein, indem er RAF-Kinase (=
Serin/Threonin-Kinase) hemmt verminderte Proliferation von Tumorzellen
• Hemmt VEGF-Rezeptor keine Angiogenese keine Nährstoffversorgung kein Wachstum
• Hemmt PDGFR (Platelet-derived growth factor) • Hemmt c-KIT (stem-cell growth factor)

ErbB Protein Tyrosine Kinase Subfamily
EGF, TNFα, ΗΒ−ΕΓΦ
tyrosine kinase domain
dual cysteine cluster
Heregulin, NDF..
EGFR ErbB1 HER2
ErbB2 neu
HER3 ErbB3
HER4 ErbB4

EGFR/ErbB2 Heterodimer
P
P
P
P
P
P
P
Tyr877
Tyr1023 Tyr1112
Tyr1139
Tyr1221 Tyr1196
Tyr1248
NH2
COOH
membrane EGFR/ErbB1 ErbB2/HER2
Cbl Grb2
Shc
Chk
Src
Sos
Ras GTP
GDP Raf1
MEK
MAPK
Sustained MAPK activation: G0/ G1 progression, differentiation

Herceptin efficently inhibits Her2 signalling in breast cancer

The EGFR – a key element in receptor cross-talk:
signal transactivation

GPCR activates metalloproteinases The ADAMS


The IGF-receptor – a key molecule in cancer

Oncogenes that need an intact IGF-R signalling

VEGF
•VEGF is a homodimeric glycoprotein, binding to VEGF-Receptors on vaskular endothelial cells •Molecular weight: 45,000Da •VEGF plays a key role for the formation of blood vessels (Angiogenesis)
Ferrara N, et al. Endocr Rev 1997;18:4–25 VEGF = vascular endothelial growth factor

Die VEGF Familie und ihre Rezeptoren
Adapted from Ferrara N. Nat Med 2003;9:669–76
Migration, proliferation, permeability, DNA synthesis, survival
Lymphangiogenesis Angiogenesis
– P P– – P
P–
VEGF-A VEGF-B
PlGF
VEGFR-1
VEGF-A
VEGFR-2
VEGF-C VEGF-D
VEGFR-3
P–
P– P–
P– – P – P – P
– P

Angiogenesis contributes to Tumorigenesis, tumor growth and Metastasis
Modifiziert nach Poon RT-P, et al. J Clin Oncol 2001;19:1207–25
Schritte, bei denen Angiogenese eine Rolle bei der Tumorprogression spielt
Prämalignes Stadium
Maligner Tumor
Tumor- Wachstum
Gefäß- invasion
ruhende Mikrometastase
Offene Metastasierung
(Avaskulärer Tumor)
(Angiogenic switch)
(Vaskularisierter Tumor)
(Tumorzell- freisetzung)
(Streuung in entfernte Organe)
(Zweite Angiogenese)

The “angiogene switch” and Tumordevelopment
Modifiziert nach Bergers G, et al. Nat Rev Cancer 2002;3:401–10
Kleiner Tumor (1–2mm) • avaskulär • ruhend
größerer Tumor • vaskularisiert • Metastasierungspotential
Angiogenic switch führt zur Überexpression von pro-angiogenen Faktoren, wie zum Beispiel VEGF

VEGF overexpression correlates with a bad prognosis
Study Cancer n Tumours (%) Prognostic value
Gasparini, 1997 Breast 260 95 Relapse-free survival, overall survival
Toi, 1995 152 55 Increased vascular density and relapse-free survival
Imoto, 1998 Lung NSCLC 91 53 Overall survival
O’Byrne, 2000 NSCLC 223 47 Tumour size, vascular density
Volm, 1997 SCLC 109 59 Overall survival
Maeda, 2000 GI CRC 100 37 Overall prognosis
Amaya, 1997 CRC 136 43 Vascular density
Ishigami, 1998 CRC 60 100 Clinical stage, metastasis
Ogata, 2003 Oesophagus 92 24 Overall survival
Shih, 2000 Oesophagus 117 31 Overall survival
Paley, 1997 Ovarian 68 43 Disease-free survival
Yamamoto, 1997 70 97 Overall survival
Jacobsen, 2004 Renal 229 100 Tumour size and stage, survival
Aguayo, 2002 Haem. AML 58 100 Survival
Verstovsek, 2002 Haem. CML 184 100 Survival


Antiangiogenic therapy – a double edged sword

Classification of Receptors
1. G Protein coupled receptors epinephrine, serotonine, glucagon
2. Ion channel receptors acetylcholine receptor
3. Tyrosine kinase-linked receptors cytokine-receptor family
4. Receptors with intrinsic enzymatic activity the receptor has intrinsic catalytic activity receptor tyrosine kinases

D3
D2
D1
IL-6R
JAK JAK
IL-6
D3 D3
D2
D1
P P
Homo- or Hetero-Dimers
P
P
Y Y
SH2
SH2
P P
P P
gp130
IL-6
D3 D3
D2
D1
D2
D3
D1 IL-6
P P
P P Y
Y
SH2
SH2
IL-6 target genes STAT1/1 STAT1/3 STAT3/3
SH2
Tyrosine kinase-linked receptors cytokine-receptor family

Y Y Jak Jak P P
P P
IFN-α IFN-β IFN-γ
IL-2, -3, -4, -5, -7, -9, -13, -15 GM-CSF, Epo, Prl, GH, TPO
Jak1
Jak3 Jak2
Stat4 Stat5a Stat5b
Immuno- modulation
Stat6
Tyk2 Stat1 Stat2
Growth Inhibition Cell cycle arrest
Apoptosis
Jak1
Proliferation Survival
Differentiation Cancer
Progression
Stat3
Stat5b Stat5a
Jak1 Jak2

O´Shea J. et al., Ann. Rheum. Dis., 2013
Cytokine signaling and specificity

“An acquired mutation in JAK2 has been described in nearly all patients with the myeloproliferative disorder (MPD), polycythemia vera (PV), and half those with essential thrombocythemia (ET) and idiopathic myelofibrosis (IMF). The V617F mutation arises in a multipotent progenitor.”
James et al. Nature. 2005;434:1144-1148 Baxter et al. Lancet.2005;365:1054-1061 Levine et al. Cancer Cell. 2005;7:387-397 Kralovics et al. N Engl J Med. 2005;352:1779-1790
caJAK2 (V617F) STAT5 STAT5
Hyperactive tyrosine kinase signaling

The pseudokinase is a Serine/Threonine kinase
Ungureanu D. et al., and Bandaranayake RM et al., Nat. Struc. Mol. Biol., 2011 and 2012
The JAK2 kinase

The correct response of the target cell to cytokines
duration of response
normal response
C
magnitude of response
signal new signal
too strong
too long
too weak
too short
C
C
C
C C
C
excessive production of mediators
target cell
C C C
C
too many receptors
C C C
C
inefficient shut-down of the signal cascade
mediator-independent activation (mutations)
overshooting response of the target cell possible disease development
C

STATs have a unique C-terminal transactivation domain

Very similar DNA binding between STATs, but tissue specific transcriptional regulators
Kang et al., BMC Genomics, 2013
Genome-wide STAT binding validated the cytokine-dependent nature of STAT binding to DNA. STAT binding is primarily defined by the cell type and less so by the individual STAT protein. The number of binding sites greatly varied between different cell contexts. The total number of STAT enriched binding sites ranged from several hundred to one hundred thousand Overlap of common binding sites between STATs 3 and 5 in T cells exceeds binding between STAT5 in T cells and non-T cells.

STAT5a/5b
Flt-3L SCF
PDGF EGF
Insulin IGF-1 Leptin
Cytoplasm
Epo Tpo GH Prl
IL-2 IL-4 IL-7 IL-9
IL-13 IL-15 IL-21 TSLP
IL-3 GM-CSF IL-5
DNA loop
OSM IL-31
Tpo Tpo-R
Nucleus
Y
SH2 Y
SH2
STAT5a/5a
STAT5b/5b
BCR-ABL p185 BCR-ABL p210 v-ABL TEL-JAK1/2/3 TEL-PDGFRβ FIP1L1-PDGFRα etc.
amplified / mutated cytokine / growth factor response
Kit (D816V) Flt3-ITD
ErbB / EGFR truncated G-CSFR
MPL mutation v-MPL
AR GR ER PR
caJAK2 (V617F) caJAK2 (R683#) caJAK3 (A572V) caTYK2 (E957D)
STAT-Oligomers
The two faces of STAT5 activation
PY PY
membrane
HCK, SRC
GAB2 PI3K
AKT
survival cell cycle
progression
differentiation senescence
immunity metabolism

pYSTAT5 as a target in myeloproliferative neoplasms Kotecha et al. Cancer Cell, 2008
But: not validated and used clinically pYSTAT5 is a clinical biomarker in leukemia
Hoelbl et al., EMBO Mol Med, 2010
Yoshimoto et al., Blood, 2009 Reckzeh et al., Leukemia, 2012
Warsch et al., Blood, 2011
- the BCR/ABL oncogene is addicted to STAT5, but depends not on JAK2 or STAT3 - increased expression of STAT5A/B mRNA/protein is a mechanism for imatinib drug resistance
Flt3-ITD transformation requires STAT5 function
Yan et al., Blood, 2012 Walz et al., Blood, 2012 JAK2 V617F transformation requires STAT5 function
JAK1: V301I, T478A/S, S512L, R532C, V623A, R629_D630del, A634D, Q644H, Y652D, Y654F, V658F, D660H, S703I, S703G, R724H/Q, R755Q, M828T, R879S/C/H, T901R, G902E, L910P, Y999H… JAK2: I166T, G180A, D319N, I324S, F495V, T514A/M, N533D, F537-indelsΔIREED, I540-E543delinsKK, N542-E543del, R564Q/L, G571S/R/G, H578R, H606Q, H608N, L611V/S, V617F, C618R, D620E, L624P, R683G/K/T/S, R867Q, D873N, P933R… JAK3: P132T, L156P, R172W/Q, E183G, Q501H, M511T, L527P, A572V, A573V, R657Q, V722I, D846N, R887C, I933fs, R948C, S1008*, G1101R… TYK2: G36D, G36R, S47N, R243W, E315K, R425H, R565W, I684S, V713F, H732R, E957D, R1027H, I1112V…
Recurrent mutations in COSMIC database, many validated culminating into STAT5 activation (or/and pYSTAT3)
Roberts et al., NEJM, 2014 Ph-like ALL requires STAT5 function

Potential C-terminal GOF mutations in COSMIC database, some validated
76 mutations in STAT5B and 44 STAT5A
Punktmutationen in STAT5A/B Transkriptionsfaktoren
STAT5A: N522S, A630T, P636S, R649Q, D658E, R673H, R769C… STAT5B: S552F, R566Q, W573G, G592R, G592V, G596V, N609D, N609K, R618T, T628I, R638I, N642H, L643V, L643Q, P645S, D658G, Y665F, A714T, D727G, A729S, P736S, P736F, P736L, Q745H…

Mimic of cytokine signaling through STAT5 gain of function
magnitude of respone
too strong
too long
signal
Onishi et al., MCB, 1998 Moriggl et al., Cancer Cell, 2005 Harir et al., Blood, 2007 Li et al., Leukemia, 2007 Harir et al., Blood, 2008 Grebien et al., Blood, 2008 Baumgartner et al., Amer. J. Patho., 2010 Li et al., Blood, 2010 Li et al., Leukemia, 2010 Friedbichler et al., Blood, 2010
S710->F
Y 793 1 136
domain DNA binding SH2
693 725 779 S S
transactivation /pY-stability cS5a
duration of response
normal
STAT5a oligomerisation domain
786 Y 699 730
S
linker domain
S715->F
687
N642->H Y665->F Gain of function of STAT5b in Large Granular
Lymphocytic Leukemia patients Rajala HL et al., Blood, 2013
1 136
domain DNA binding SH2
transactivation /pY-stability cS5b STAT5b oligomerisation
domain linker
domain
687

Palmer DC and Restifo NP, Trends Immunology, 2009
Hypermethylation or genetic deletion of SOCS family members in cancer