cigarette smoking, alcohol consumption and risk of systemic lupus erythematosus
TRANSCRIPT
http://lup.sagepub.com/Lupus
http://lup.sagepub.com/content/23/6/537The online version of this article can be found at:
DOI: 10.1177/0961203313501400
2014 23: 537LupusSU Takvorian, JF Merola and KH Costenbader
Cigarette smoking, alcohol consumption and risk of systemic lupus erythematosus
Published by:
http://www.sagepublications.com
can be found at:LupusAdditional services and information for
http://lup.sagepub.com/cgi/alertsEmail Alerts:
http://lup.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Apr 24, 2014Version of Record >>
at PORTLAND STATE UNIV on September 13, 2014lup.sagepub.comDownloaded from at PORTLAND STATE UNIV on September 13, 2014lup.sagepub.comDownloaded from
Lupus (2014) 23, 537–544
http://lup.sagepub.com
SPECIAL ARTICLE
Cigarette smoking, alcohol consumption and risk of systemic
lupus erythematosus
SU Takvorian1, JF Merola2 and KH Costenbader1,31Department of Medicine; 2Department of Dermatology; and 3Division of Rheumatology, Immunology and Allergy, Brigham and Women’s
Hospital, Harvard Medical School, Boston, MA, USA
Systemic lupus erythematosus (SLE) is a complex multisystem autoimmune disease whosepathogenesis is thought to involve both genetic and environmental factors. It is possiblethat common environmental exposures, such as cigarette smoking and alcohol consumption,might modify risk of disease development in certain individuals. Here we aim to review theepidemiologic evidence related to the association of cigarette smoking, alcohol consumptionand the risk of developing SLE. A growing body of evidence suggests that cigarette smokingconfers a short-term increased risk of SLE in genetically susceptible individuals. On the otherhand, alcohol consumption in moderate doses may have a protective effect against the devel-opment of SLE, although this is still debated. We also have reviewed proposed mechanisticexplanations underlying the role of cigarette smoking and alcohol consumption in SLEpathogenesis. Lupus (2014) 23, 537–544.
Key words: Systemic lupus erythematosus; risk factors; environmental exposure
Introduction
Systemic lupus erythematosus (SLE) is a complexmultisystem autoimmune disease whose pathogen-esis remains incompletely understood. The currentparadigm is that environmental exposures triggerthe development of disease and disease phenotypein genetically susceptible individuals.1 Twin con-cordance studies, commonly used to quantify therole of gene inheritance in disease susceptibility,suggest an important role for environmental aswell as genetic factors in SLE susceptibility, withconcordance rates between monozygotic twins ran-ging from 11% to 57%.2
Although SLE is a rare disease, it is possible thatexposures linked to its susceptibility could be quitecommon, related to dose and duration of exposureor specific gene-environment interactions. Twosuch common exposures that have been studied inseveral epidemiologic studies are cigarette smokingand alcohol consumption. Cigarette smoking hasconsistently been found to be strongly associated
with the development of rheumatoid arthritis(RA), but its role in the pathogenesis of SLE isless well understood.3,4 Alcohol consumption, ahabit that often accompanies smoking, may protectagainst the development of SLE, although this isstill debated.5
The purpose of this article is to review the exist-ing literature pertaining to the association of cigar-ette smoking, alcohol consumption and the risk ofdeveloping SLE. We also aim to explore potentialmechanisms by which these environmental factorsmight be involved in the pathogenesis of SLE.
Methods
We performed a comprehensive literature search onPubMed for all years available through February2013, using the following search terms: ‘‘smoking,’’‘‘cigarette,’’ ‘‘alcohol’’ and ‘‘risk factor,’’ eachmatched with ‘‘systemic lupus.’’ We restricted oursearch to studies of humans, published in English.This generated 924 results, of which 224 pertainedto smoking as a risk factor and 78 pertained toalcohol as a risk factor. We excluded case reportsand case series from our analysis, as well as reviews,
Correspondence to: Samuel Takvorian, Brigham and Women’s
Hospital, 75 Francis Street, Boston, MA 02115, USA.
Email: [email protected]
! The Author(s), 2013. Reprints and permissions: http://www.sagepub.co.uk/journalsPermissions.nav 10.1177/0961203313501400
at PORTLAND STATE UNIV on September 13, 2014lup.sagepub.comDownloaded from
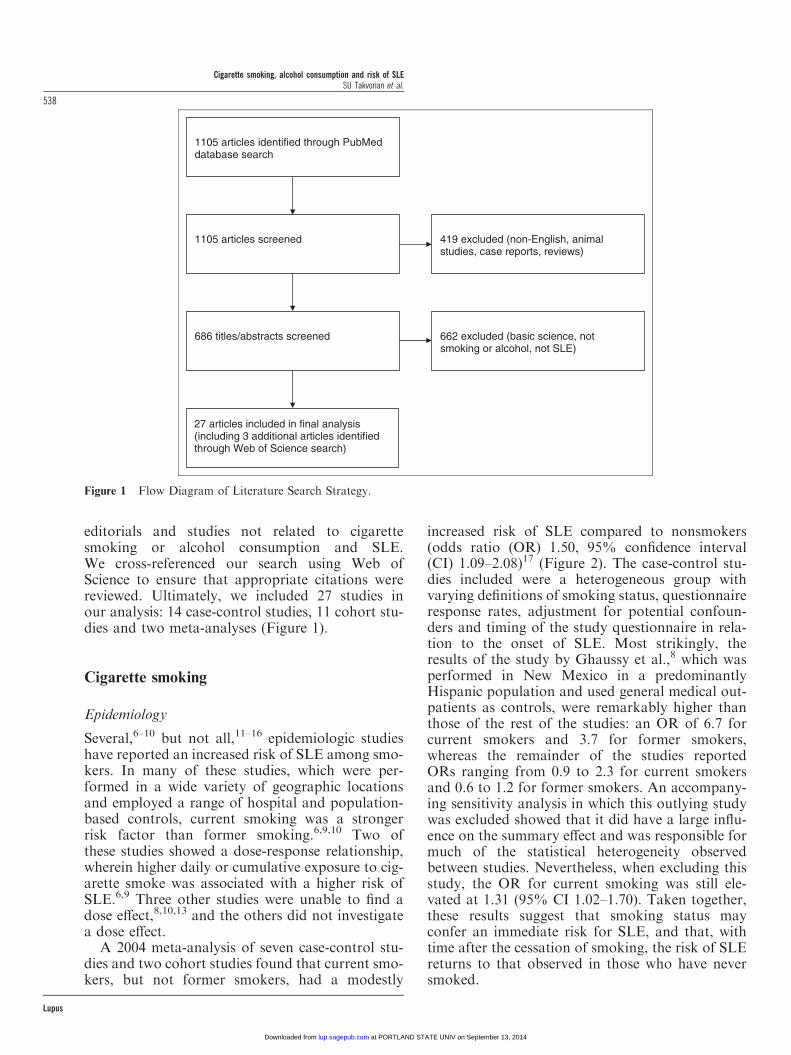
editorials and studies not related to cigarettesmoking or alcohol consumption and SLE.We cross-referenced our search using Web ofScience to ensure that appropriate citations werereviewed. Ultimately, we included 27 studies inour analysis: 14 case-control studies, 11 cohort stu-dies and two meta-analyses (Figure 1).
Cigarette smoking
Epidemiology
Several,6–10 but not all,11–16 epidemiologic studieshave reported an increased risk of SLE among smo-kers. In many of these studies, which were per-formed in a wide variety of geographic locationsand employed a range of hospital and population-based controls, current smoking was a strongerrisk factor than former smoking.6,9,10 Two ofthese studies showed a dose-response relationship,wherein higher daily or cumulative exposure to cig-arette smoke was associated with a higher risk ofSLE.6,9 Three other studies were unable to find adose effect,8,10,13 and the others did not investigatea dose effect.
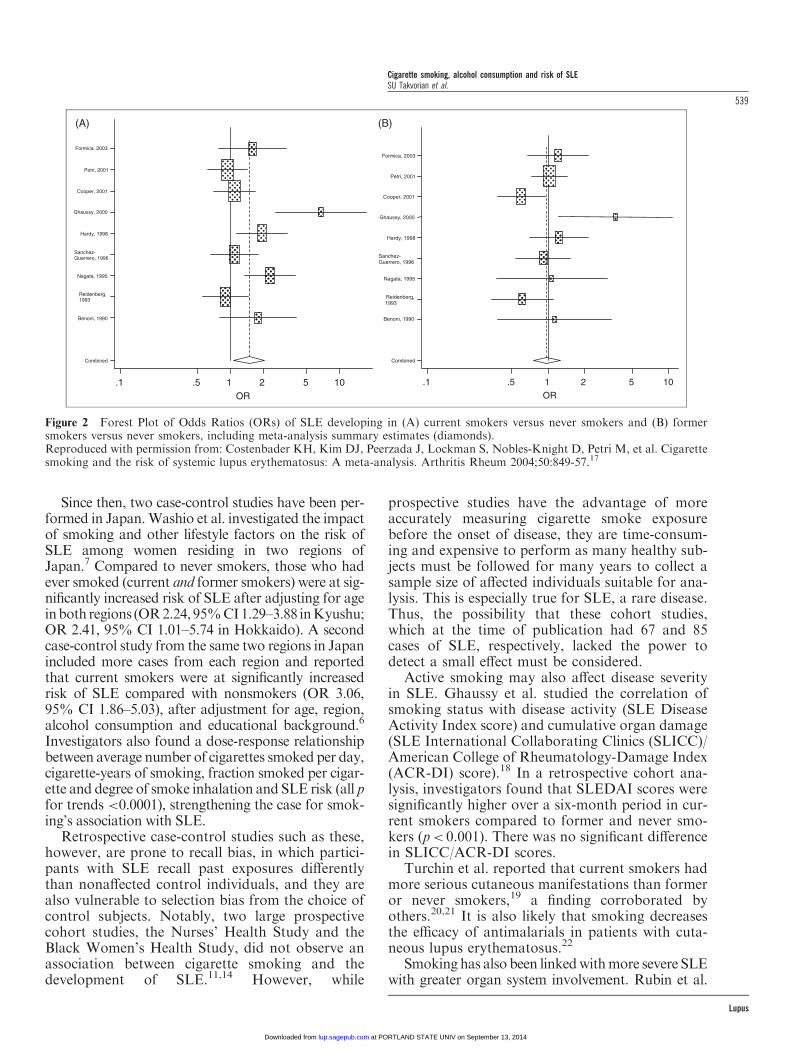
A 2004 meta-analysis of seven case-control stu-dies and two cohort studies found that current smo-kers, but not former smokers, had a modestly
increased risk of SLE compared to nonsmokers(odds ratio (OR) 1.50, 95% confidence interval(CI) 1.09–2.08)17 (Figure 2). The case-control stu-dies included were a heterogeneous group withvarying definitions of smoking status, questionnaireresponse rates, adjustment for potential confoun-ders and timing of the study questionnaire in rela-tion to the onset of SLE. Most strikingly, theresults of the study by Ghaussy et al.,8 which wasperformed in New Mexico in a predominantlyHispanic population and used general medical out-patients as controls, were remarkably higher thanthose of the rest of the studies: an OR of 6.7 forcurrent smokers and 3.7 for former smokers,whereas the remainder of the studies reportedORs ranging from 0.9 to 2.3 for current smokersand 0.6 to 1.2 for former smokers. An accompany-ing sensitivity analysis in which this outlying studywas excluded showed that it did have a large influ-ence on the summary effect and was responsible formuch of the statistical heterogeneity observedbetween studies. Nevertheless, when excluding thisstudy, the OR for current smoking was still ele-vated at 1.31 (95% CI 1.02–1.70). Taken together,these results suggest that smoking status mayconfer an immediate risk for SLE, and that, withtime after the cessation of smoking, the risk of SLEreturns to that observed in those who have neversmoked.
1105 articles identified through PubMed database search
662 excluded (basic science, not smoking or alcohol, not SLE)
686 titles/abstracts screened
419 excluded (non-English, animal studies, case reports, reviews)
1105 articles screened
27 articles included in final analysis (including 3 additional articles identified through Web of Science search)
Figure 1 Flow Diagram of Literature Search Strategy.
Cigarette smoking, alcohol consumption and risk of SLESU Takvorian et al.
538
Lupus
at PORTLAND STATE UNIV on September 13, 2014lup.sagepub.comDownloaded from
Since then, two case-control studies have been per-formed in Japan.Washio et al. investigated the impactof smoking and other lifestyle factors on the risk ofSLE among women residing in two regions ofJapan.7 Compared to never smokers, those who hadever smoked (current and former smokers) were at sig-nificantly increased risk of SLE after adjusting for ageinbothregions (OR2.24,95%CI1.29–3.88 inKyushu;OR 2.41, 95% CI 1.01–5.74 in Hokkaido). A secondcase-control study from the same two regions in Japanincluded more cases from each region and reportedthat current smokers were at significantly increasedrisk of SLE compared with nonsmokers (OR 3.06,95% CI 1.86–5.03), after adjustment for age, region,alcohol consumption and educational background.6
Investigators also found a dose-response relationshipbetween average number of cigarettes smoked per day,cigarette-years of smoking, fraction smoked per cigar-ette and degree of smoke inhalation and SLE risk (all pfor trends <0.0001), strengthening the case for smok-ing’s association with SLE.
Retrospective case-control studies such as these,however, are prone to recall bias, in which partici-pants with SLE recall past exposures differentlythan nonaffected control individuals, and they arealso vulnerable to selection bias from the choice ofcontrol subjects. Notably, two large prospectivecohort studies, the Nurses’ Health Study and theBlack Women’s Health Study, did not observe anassociation between cigarette smoking and thedevelopment of SLE.11,14 However, while
prospective studies have the advantage of moreaccurately measuring cigarette smoke exposurebefore the onset of disease, they are time-consum-ing and expensive to perform as many healthy sub-jects must be followed for many years to collect asample size of affected individuals suitable for ana-lysis. This is especially true for SLE, a rare disease.Thus, the possibility that these cohort studies,which at the time of publication had 67 and 85cases of SLE, respectively, lacked the power todetect a small effect must be considered.
Active smoking may also affect disease severityin SLE. Ghaussy et al. studied the correlation ofsmoking status with disease activity (SLE DiseaseActivity Index score) and cumulative organ damage(SLE International Collaborating Clinics (SLICC)/American College of Rheumatology-Damage Index(ACR-DI) score).18 In a retrospective cohort ana-lysis, investigators found that SLEDAI scores weresignificantly higher over a six-month period in cur-rent smokers compared to former and never smo-kers (p< 0.001). There was no significant differencein SLICC/ACR-DI scores.
Turchin et al. reported that current smokers hadmore serious cutaneous manifestations than formeror never smokers,19 a finding corroborated byothers.20,21 It is also likely that smoking decreasesthe efficacy of antimalarials in patients with cuta-neous lupus erythematosus.22
Smoking has also been linkedwithmore severe SLEwith greater organ system involvement. Rubin et al.
(A) (B)
Figure 2 Forest Plot of Odds Ratios (ORs) of SLE developing in (A) current smokers versus never smokers and (B) formersmokers versus never smokers, including meta-analysis summary estimates (diamonds).Reproduced with permission from: Costenbader KH, Kim DJ, Peerzada J, Lockman S, Nobles-Knight D, Petri M, et al. Cigarettesmoking and the risk of systemic lupus erythematosus: A meta-analysis. Arthritis Rheum 2004;50:849-57.17
Cigarette smoking, alcohol consumption and risk of SLESU Takvorian et al.
539
Lupus
at PORTLAND STATE UNIV on September 13, 2014lup.sagepub.comDownloaded from

found that among SLE patients current smokers hadmore episodes of pleuritis, peritonitis and neuro-psychiatric symptoms than former or never smokers.23
Ward et al. observed that among patients with lupusnephritis, those who smoked had accelerated develop-ment of end-stage renal disease.24 However, the inci-dence of lupus nephritis itself was not associated withsmoking exposure in a separate study.25 Smoking isalso associated with higher odds of thromboticevents26 and avascular necrosis27 among SLEpatients.
Pathogenesis
While the pathogenic role of smoking in neoplastic,pulmonary and cardiovascular disease has beenwell studied, less is known about its mechanisticrole in autoimmune disease.3,28 Cigarette smokecontains numerous potentially toxic components,including tars, nicotine, carbon monoxide andpolycyclic aromatic hydrocarbons. Exposure tosuch toxins, or their reactive metabolites, can dir-ectly damage endogenous proteins and DNA. Infact, cigarette smoke contains 1014–1016 free rad-icals per puff—including reactive aldehydes, quin-ones and benzo(a)pyrene—which induce oxidativestress,29,30 implicated in the pathogenesis of SLE.31
Cigarette smoke also induces epigenetic changes,some of which could modulate genes involved inpathways of inflammation and autoimmunity, per-haps triggering SLE.32,33 Finally, exposure to cig-arette smoke has harmful effects on both humoraland cell-mediated immunity. Cigarette smoke aug-ments production of numerous pro-inflammatorycytokines such as tumor necrosis factor (TNF)-alpha, interleukin (IL)-1, IL-6, IL-8 and granulo-cyte macrophage colony-stimulating factor(GM-CSF) and decreases levels of anti-inflamma-tory cytokines such as IL-10.34
In a retrospective analysis of 140 ever-smokersand 270 nonsmokers with SLE, Freemer et al.found an association between current smokingand the presence of anti-double-stranded DNA(anti-dsDNA) antibodies.35 Compared to neversmokers, current smokers were more likely tohave dsDNA antibody seropositivity (OR 4.0,95% CI 1.6–10.4). Former smokers, however,were not at increased risk for these antibodies com-pared to nonsmokers.
While this finding contradicted that of an earlierstudy,23 which found a negative associationbetween smoking and immunoglobulin G (IgG)anti-DNA autoantibodies both in human andmurine SLE, it provided another mechanistic
explanation for the role of smoking in SLE. In anaccompanying editorial, it was hypothesized thatthe increased apoptosis that is a known effect ofcigarette smoking could account for the generationof autoantibodies in smokers.36Active smokingmay cause DNA damage and the formation ofDNA adducts, which are more immunogenic thanundamaged DNA, and may induce autoimmunityin genetically susceptible individuals. The estimatedhalf-life of these adducts is nine to 13 weeks, pos-sibly explaining the observed association of currentbut not past smoking with increased risk of SLE.37
Alternatively, as cigarette smoke promotes aninflux of short-lived inflammatory cells into thelungs and impairs the capabilities of residentmacrophages to clear inflammatory debris, anti-dsDNA antibodies may be the result of ineffectiveclearance of apoptotic pulmonary material.36
The role of smoking in SLE may parallel its rolein the pathogenesis of RA, another systemic auto-immune disease for which smoking is a known riskfactor. A recent meta-analysis of 16 observationalstudies found that the risk of developing RA wasabout twice and 1.3 times greater for male andfemale smokers, respectively, compared to nonsmo-kers.38 Klareskog et al. demonstrated that smokingand pulmonary inflammation both lead toincreased citrullination of peptides in the lungs,with subsequent immune reactions to citrullinatedproteins occurring in genetically susceptible indi-viduals (e.g. human leukocyte antigen (HLA)-DRB1 shared epitope positive).39 Thus, smokingmay give rise to similar primary events in both dis-eases—activation of innate immunity and apop-tosis—triggering distinct forms of autoimmunitydepending on genetic predisposition.28
Mechanistic evidence implicating smoking inSLE pathogenesis is provided by three case-controlstudies from Japan, exploring potential gene-envir-onment interactions. Kiyohara et al. found thatsmokers carrying N-acetyltransferase 2 polymorph-isms, responsible for hepatic detoxification of aro-matic amines by acetylation, were at significantlyincreased risk of SLE (OR 2.34, 95% CI 1.21–4.52) compared with the rapid acetylatorgenotype.40 Likewise, smokers with a genotype pro-moting greater production of reactive oxygen spe-cies due to CYP1A1 polymorphisms had higherrisk of SLE (OR 9.72, 95% CI 2.73–34.6) comparedto nonsmokers with the predominant genotype.41 Itwas estimated that 60% of the excess risk for SLEin smokers was due to the additive interactionbetween the two factors. Finally, it appears thatcertain polymorphisms in the TNF receptor super-family, member 1B (TNFRSF1B) may confer excess
Cigarette smoking, alcohol consumption and risk of SLESU Takvorian et al.
540
Lupus
at PORTLAND STATE UNIV on September 13, 2014lup.sagepub.comDownloaded from
risk of SLE in smokers (OR 1.56, 95% CI 0.99–2.47).42 It was estimated that 49% of the excessrisk of SLE in smokers with the gene polymorph-ism was additive.
Alcohol consumption
Epidemiology
Several epidemiologic studies have investigated therelationship between alcohol consumption and riskof developing SLE, yielding conflicting results.Hardy et al., in a case-control study from theUnited Kingdom (UK), were the first to report astatistically significant inverse association and dose-response relationship between alcohol consumptionand SLE susceptibility, suggesting a possible pro-tective effect.9 Two subsequent studies have corro-borated this finding.6,12 The first was a case-controlstudy from Sweden, in which consumption of>150 g/month was compared with none, and sub-jects’ alcohol consumption was defined as the max-imum monthly consumption before SLE (or indexdate for controls). In this study, alcohol consump-tion was strongly protective against SLE (ORadj
0.2, 95% CI 0.1–0.5).12
In Japan, a case-control study involving 171 SLEcases and 492 unmatched controls found that light/moderate alcohol consumption was inversely asso-ciated with SLE risk, irrespective of type of alco-holic beverage consumed.6 These findings clarifiedan earlier analysis by Washio et al. from the samepopulation, which produced conflicting results.7
Investigators initially found a dose-response effectin the Kyushu region, wherein higher-frequencydrinkers were at increased odds of developingSLE, but this association was not seen in theHokkaido region. When investigators reanalyzedthe association in their later study,6 using nondrin-kers as a reference category instead of subjects whodrank <1 day per week, they found that light(<1 day per week) and moderate (one to threedays per week) drinkers had a significantlydecreased risk of SLE (OR 0.38, 95% CI 0.19–0.76). This association was not seen among heavydrinkers (four to seven days per week), but per-sisted after adjustment for age, region, smokingstatus and educational background.
Other investigations, however, including twocase-control studies8,10 and a prospective cohortanalysis,11 found no statistically significant associ-ations between alcohol consumption and SLE sus-ceptibility. However, it should be noted thatNagata et al., in their case-control study from
Japan, found a nonsignificant inverse trendbetween alcohol consumption and SLE risk com-pared to never drinkers (OR 0.52, 95% CI 0.25–1.06 for weekly drinking; OR 0.57, 95% CI 0.19–1.71 for daily drinking).10 Furthermore, the onlyprospective study assessing alcohol as a riskfactor for SLE was limited by a very smallnumber of incident SLE cases in the BlackWomen’s Health Study at the time (67 cases) andused a one-time baseline alcohol assessment.11
These inconsistent findings may further repre-sent population differences with respect to typesand patterns of alcohol consumption, selectionbias, recall bias or uncontrolled confounding.Additionally, there could be bias of existent diseaseon the exposure behavior with post-SLE onsetchanges in alcohol consumption leading to a spuri-ous inverse association. A recent case-controlstudy conducted via the Internet found evidence sug-gestive of such protopathic bias.43 While the studyfound that current drinking status was inverselyassociated with SLE risk in a dose-dependent fash-ion, alcohol consumption before SLE diagnosis wasnot associated with risk of SLE. Furthermore, caseswere more likely to quit drinking either before orafter diagnosis than were controls.
In a meta-analysis of six case-control studies andone cohort study assessing the relationship betweenalcohol and SLE risk, Wang et al. found an overallsignificantly protective effect when all studiesincluding patients with SLE treated for less thanten years were examined (OR 0.72, 95% CI 0.55–0.95).44 While this effect was absent when examin-ing patients with SLE treated for less than fiveyears, a sensitivity analysis suggested that thestudy of Washio et al.,7 described above, dispropor-tionately influenced the subgroup’s odds estimate.When excluding this study, which used a more lib-eral reference point than the other studies included,a significant protective effect was observed (OR0.66, 95% CI 0.49–0.89). These results are hard tointerpret, but taken together suggest a possible pro-tective effect of moderate alcohol consumption onthe development of SLE.
Pathogenesis
While ethanol contains many anti-inflammatorycompounds, the exact mechanisms by which itmight protect against SLE remain speculative.45
Alcohol consumption, like cigarette smoking, hasbeen found to cause epigenetic changes, resulting inaltered gene expression that might affect immunehomeostasis.33 Extensive evidence suggests thatethanol has dose-dependent immunomodulatory
Cigarette smoking, alcohol consumption and risk of SLESU Takvorian et al.
541
Lupus
at PORTLAND STATE UNIV on September 13, 2014lup.sagepub.comDownloaded from

properties, wherein moderate use is associated withattenuated inflammation and heavy use is asso-ciated with increased inflammation.46 Thus, moder-ate doses of alcohol might decrease susceptibility toinflammatory diseases by modulating synthesis andrelease of pro-inflammatory cytokines. For exam-ple, moderate alcohol consumption inhibits pro-duction of the pro-inflammatory cytokine IL-6,which is observed at high levels in patients withSLE and may be implicated in diseasepathogenesis.47
A similar anti-inflammatory effect has beenimplicated in RA, where multiple epidemiologicstudies have suggested that moderate alcohol con-sumption is protective against development of RAand disease progression.48–50 Using blood samplesfrom the prospective Nurses’ Health Study, Luet al. found that alcohol consumption had aU-shaped association with IL-6 levels in preclinicalRA patients (and thus was decreased at moder-ate doses), and that soluble TNF receptor IIlevels were negatively associated with daily alcoholconsumption.51
While some question the biologic plausibility ofalcohol’s protective effect in SLE,43 light to moder-ate alcohol intake has been demonstrated to haveprotective effects against several inflammatory dis-eases, including RA and cardiovascular disease.52
Whether the cardioprotective mechanisms of alco-hol may be at work in SLE remains to bedetermined.
Conclusion
It is widely believed that interactions between gen-etic and environmental factors contribute to thedevelopment of SLE. While genetic factors arebeing elucidated, epidemiologic studies have identi-fied several important environmental exposureslinked to SLE susceptibility. Two of these expos-ures, cigarette smoking and alcohol consumption,were reviewed here.
Several case-control studies across a variety ofpatient populations have shown that smokers, par-ticularly current smokers, have an increased risk ofdeveloping SLE. While this trend was not observedin two prospective cohort studies, both were ham-pered by small numbers of SLE cases at the time. Ameta-analysis revealed a small but significantlyincreased risk of SLE among current smokers, butnot former smokers. Further studies have shownthat cigarette smoking is associated with worse dis-ease activity and severity, including more extensive
organ system involvement. Given smoking’s harm-ful effects on the immune system, as well as itsimmunogenicity, it is biologically plausible that itmight contribute to autoimmune susceptibility, ashas been established for RA.
Alcohol consumption, a habit that oftenco-occurs with cigarette smoking, has been lesswell studied with respect to SLE risk. Few case-con-trol studies have directly investigated alcohol as arisk factor for SLE, yielding conflicting results.Three of these showed alcohol consumption to besignificantly protective against SLE in moderatedoses, but others did not find a significant associ-ation. A recent meta-analysis provided amoderatelyprotective summary estimate when all studies wereincluded. Since it is possible that patients in whomSLE has already developed tend not to drink asmuch as healthy controls, the possibility of proto-pathic bias must be considered. No published stu-dies have assessed the association between long-termalcohol consumption and future SLE risk in the set-ting of a well-controlled, large prospective cohortstudy. Thus, while the literature suggests that mod-erate alcohol consumption might be linked withdecreased SLE susceptibility, the evidence for thisprotective effect remains limited.
Cigarette smoking and alcohol consumption aretwo highly prevalent and potentially modifiableexposures, and thus represent areas ripe for clinicalintervention and are deserving of further investiga-tion. Future studies, including both prospectivecohort analyses and in vitro and animal studies,are necessary to mitigate the recall and selectionbias inherent in case-control studies, and to furtherunpack the biological mechanisms underlying theeffect of these exposures on inflammation and auto-immunity. Until such studies are performed, con-tinued counseling regarding smoking cessation forall patients is always warranted, and we would notrecommend against light to moderate alcoholconsumption.
Funding
This research received no specific grant from anyfunding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None of the authors has any conflicts of interest todisclose.
Cigarette smoking, alcohol consumption and risk of SLESU Takvorian et al.
542
Lupus
at PORTLAND STATE UNIV on September 13, 2014lup.sagepub.comDownloaded from

References
1 Zandman-Goddard G, Solomon M, Rosman Z, Peeva E, ShoenfeldY. Environment and lupus-related diseases. Lupus 2012; 21: 241–250.
2 Bogdanos DP, Smyk DS, Rigopoulou EI, et al. Twin studies inautoimmune disease: Genetics, gender and environment.J Autoimmun 2012; 38: J156–J169.
3 Costenbader KH, Karlson EW. Cigarette smoking and auto-immune disease: What can we learn from epidemiology? Lupus2006; 15: 737–745.
4 Costenbader KH, Karlson EW. Cigarette smoking and systemiclupus erythematosus: A smoking gun? Autoimmunity 2005; 38:541–547.
5 Sofat N, Keat A. Alcohol intake in rheumatic disease: Good orbad? Rheumatology (Oxford) 2002; 41: 125–128.
6 Kiyohara C, Washio M, Horiuchi T, et al. Cigarette smoking,alcohol consumption, and risk of systemic lupus erythematosus:A case-control study in a Japanese population. J Rheumatol2012; 39: 1363–1370.
7 Washio M, Horiuchi T, Kiyohara C, et al. Smoking, drinking,sleeping habits, and other lifestyle factors and the risk of systemiclupus erythematosus in Japanese females: Findings from the KYSSstudy. Mod Rheumatol 2006; 16: 143–150.
8 Ghaussy NO, Sibbitt Jr WL, Qualls CR. Cigarette smoking, alco-hol consumption, and the risk of systemic lupus erythematosus: Acase-control study. J Rheumatol 2001; 28: 2449–2453.
9 Hardy CJ, Palmer BP, Muir KR, Sutton AJ, Powell RJ.Smoking history, alcohol consumption, and systemic lupuserythematosus: A case-control study. Ann Rheum Dis 1998; 57:451–455.
10 Nagata C, Fujita S, Iwata H, et al. Systemic lupus erythematosus:A case-control epidemiologic study in Japan. Int J Dermatol 1995;34: 333–337.
11 Formica MK, Palmer JR, Rosenberg L, McAlindon TE. Smoking,alcohol consumption, and risk of systemic lupus erythematosus inthe Black Women’s Health Study. J Rheumatol 2003; 30:1222–1226.
12 Bengtsson AA, Rylander L, Hagmar L, Nived O, Sturfelt G. Riskfactors for developing systemic lupus erythematosus: A case-control study in southern Sweden. Rheumatology (Oxford) 2002;41: 563–571.
13 Cooper GS, Dooley MA, Treadwell EL, St Clair EW, GilkesonGS. Smoking and use of hair treatments in relation to risk ofdeveloping systemic lupus erythematosus. J Rheumatol 2001; 28:2653–2656.
14 Sanchez-Guerrero J, Karlson EW, Colditz GA, Hunter DJ, SpeizerFE, Liang MH. Hair dye use and the risk of developing systemiclupus erythematosus. Arthritis Rheum 1996; 39: 657–662.
15 Reidenberg MM, Drayer DE, Lorenzo B, et al. Acetylation pheno-types and environmental chemical exposure of people with idio-pathic systemic lupus erythematosus. Arthritis Rheum 1993; 36:971–973.
16 Benoni C, Nilsson A, Nived O. Smoking and inflammatory boweldisease: Comparison with systemic lupus erythematosus. A case-control study. Scand J Gastroenterol 1990; 25: 751–755.
17 Costenbader KH, Kim DJ, Peerzada J, et al. Cigarette smokingand the risk of systemic lupus erythematosus: A meta-analysis.Arthritis Rheum 2004; 50: 849–857.
18 Ghaussy NO, Sibbitt Jr W, Bankhurst AD, Qualls CR. Cigarettesmoking and disease activity in systemic lupus erythematosus.J Rheumatol 2003; 30: 1215–1221.
19 Turchin I, Bernatsky S, Clarke AE, St-Pierre Y, Pineau CA.Cigarette smoking and cutaneous damage in systemic lupus erythe-matosus. J Rheumatol 2009; 36: 2691–2693.
20 Piette EW, Foering KP, Chang AY, et al. Impact of smoking incutaneous lupus erythematosus. Arch Dermatol 2012; 148:317–322.
21 Boeckler P, Cosnes A, Frances C, Hedelin G, Lipsker D.Association of cigarette smoking but not alcohol consumptionwith cutaneous lupus erythematosus. Arch Dermatol 2009; 145:1012–1016.
22 Ezra N, Jorizzo J. Hydroxychloroquine and smoking in patientswith cutaneous lupus erythematosus. Clin Exp Dermatol 2012; 37:327–334.
23 Rubin RL, Hermanson TM, Bedrick EJ, et al. Effect of cigarettesmoke on autoimmunity in murine and human systemic lupus ery-thematosus. Toxicol Sci 2005; 87: 86–96.
24 Ward MM, Studenski S. Clinical prognostic factors in lupus neph-ritis. The importance of hypertension and smoking. Arch InternMed 1992; 152: 2082–2088.
25 McAlindon T, Giannotta L, Taub N, D’Cruz D, Hughes G.Environmental factors predicting nephritis in systemic lupus ery-thematosus. Ann Rheum Dis 1993; 52: 720–724.
26 Ho KT, Ahn CW, Alarcon GS, et al. Systemic lupus erythematosusin a multiethnic cohort (LUMINA): XXVIII. Factors predictive ofthrombotic events. Rheumatology (Oxford) 2005; 44: 1303–1307.
27 Mont MA, Glueck CJ, Pacheco IH, Wang P, Hungerford DS, PetriM. Risk factors for osteonecrosis in systemic lupus erythematosus.J Rheumatol 1997; 24: 654–662.
28 Klareskog L, Padyukov L, Alfredsson L. Smoking as a trigger forinflammatory rheumatic diseases. Curr Opin Rheumatol 2007; 19:49–54.
29 Pryor WA, Stone K. Oxidants in cigarette smoke. Radicals, hydro-gen peroxide, peroxynitrate, and peroxynitrite. Ann N Y Acad Sci1993; 686: 12–27. discussion 27–28.
30 Church DF, Pryor WA. Free-radical chemistry of cigarette smokeand its toxicological implications. Environ Health Perspect 1985;64: 111–126.
31 Wang G, Pierangeli SS, Papalardo E, Ansari GA, Khan MF.Markers of oxidative and nitrosative stress in systemic lupus ery-thematosus: Correlation with disease activity. Arthritis Rheum2010; 62: 2064–2072.
32 Costenbader KH, Gay S, Alarcon-Riquelme ME, Iaccarino L,Doria A. Genes, epigenetic regulation and environmental factors:Which is the most relevant in developing autoimmune diseases?Autoimmun Rev 2012; 11: 604–609.
33 Mathers JC, Strathdee G, Relton CL. Induction of epigenetic alter-ations by dietary and other environmental factors. Adv Genet 2010;71: 3–39.
34 Arnson Y, Shoenfeld Y, Amital H. Effects of tobacco smoke onimmunity, inflammation and autoimmunity. J Autoimmun 2010;34: J258–J265.
35 Freemer MM, King Jr TE, Criswell LA. Association of smokingwith dsDNA autoantibody production in systemic lupus erythema-tosus. Ann Rheum Dis 2006; 65: 581–584.
36 Majka DS, Holers VM. Cigarette smoking and the risk of systemiclupus erythematosus and rheumatoid arthritis. Ann Rheum Dis2006; 65: 561–563.
37 Mooney LA, Santella RM, Covey L, et al. Decline of DNAdamage and other biomarkers in peripheral blood following smok-ing cessation. Cancer Epidemiol Biomarkers Prev 1995; 4: 627–634.
38 Sugiyama D, Nishimura K, Tamaki K, et al. Impact of smoking asa risk factor for developing rheumatoid arthritis: A meta-analysisof observational studies. Ann Rheum Dis 2010; 69: 70–81.
39 Klareskog L, Stolt P, Lundberg K, et al. A new model for anetiology of rheumatoid arthritis: Smoking may trigger HLA-DR(shared epitope)-restricted immune reactions to autoantigens mod-ified by citrullination. Arthritis Rheum 2006; 54: 38–46.
40 Kiyohara C, Washio M, Horiuchi T, et al. Cigarette smoking,N-acetyltransferase 2 polymorphisms and systemic lupus erythe-matosus in a Japanese population. Lupus 2009; 18: 630–638.
41 Kiyohara C, Washio M, Horiuchi T, et al. Riskmodification by CYP1A1 and GSTM1 polymorphisms in theassociation of cigarette smoking and systemic lupus erythemato-sus in a Japanese population. Scand J Rheumatol 2012; 41:103–109.
42 Kiyohara C, Washio M, Horiuchi T, et al. Cigarette smoking,STAT4 and TNFRSF1B polymorphisms, and systemic lupus ery-thematosus in a Japanese population. J Rheumatol 2009; 36:2195–2203.
43 Wang J, Kay AB, Fletcher J, Formica MK, McAlindon TE.Alcohol consumption is not protective for systemic lupus erythe-matosus. Ann Rheum Dis 2009; 68: 345–348.
Cigarette smoking, alcohol consumption and risk of SLESU Takvorian et al.
543
Lupus
at PORTLAND STATE UNIV on September 13, 2014lup.sagepub.comDownloaded from

44 Wang J, Pan HF, Ye DQ, Su H, Li XP. Moderate alcohol drinkingmight be protective for systemic lupus erythematosus: A systematicreview and meta-analysis. Clin Rheumatol 2008; 27: 1557–1563.
45 Imhof A, Froehlich M, Brenner H, Boeing H, Pepys MB, KoenigW. Effect of alcohol consumption on systemic markers of inflam-mation. Lancet 2001; 357: 763–767.
46 Goral J, Karavitis J, Kovacs EJ. Exposure-dependent effects ofethanol on the innate immune system. Alcohol 2008; 42: 237–247.
47 Ripley BJ, Goncalves B, Isenberg DA, Latchman DS, Rahman A.Raised levels of interleukin 6 in systemic lupus erythematosus cor-relate with anaemia. Ann Rheum Dis 2005; 64: 849–853.
48 Kallberg H, Jacobsen S, Bengtsson C, et al. Alcohol consumptionis associated with decreased risk of rheumatoid arthritis: Resultsfrom two Scandinavian case-control studies. Ann Rheum Dis 2009;68: 222–227.
49 Pedersen M, Jacobsen S, Klarlund M, et al. Environmental riskfactors differ between rheumatoid arthritis with and without auto-antibodies against cyclic citrullinated peptides. Arthritis Res Ther2006; 8: R133.
50 Nissen MJ, Gabay C, Scherer A, Finckh A. The effect of alcoholon radiographic progression in rheumatoid arthritis. ArthritisRheum 2010; 62: 1265–1272.
51 Lu B, Solomon DH, Costenbader KH, Keenan BT, Chibnik LB,Karlson EW. Alcohol consumption and markers of inflammationin women with preclinical rheumatoid arthritis. Arthritis Rheum2010; 62: 3554–3559.
52 Corrao G, Bagnardi V, Zambon A, La Vecchia C. A meta-analysisof alcohol consumption and the risk of 15 diseases. Prev Med 2004;38: 613–619.
Cigarette smoking, alcohol consumption and risk of SLESU Takvorian et al.
544
Lupus
at PORTLAND STATE UNIV on September 13, 2014lup.sagepub.comDownloaded from