“choosing wisely”? - centro bioetica · gf gensini received fees and research support from...
TRANSCRIPT
E’ possibile insegnare il
“CHOOSING WISELY”?
G. F. GENSINI
GF Gensini
received fees and research support from Astra Zeneca, Bayer, Boehringer
Ingelheim, Eli Lilly, GSK, Johnson&Johnson, Pfizer, Sanofi Aventis, Siemens, Sigma Tau and Sorin



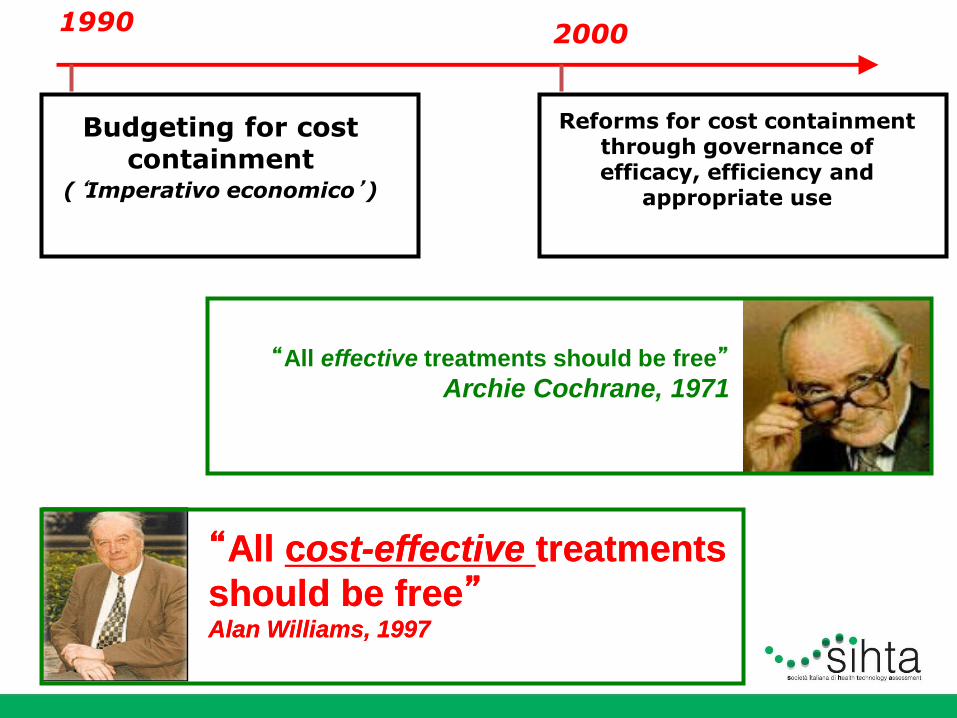
“All effective treatments should be free”
Archie Cochrane, 1971
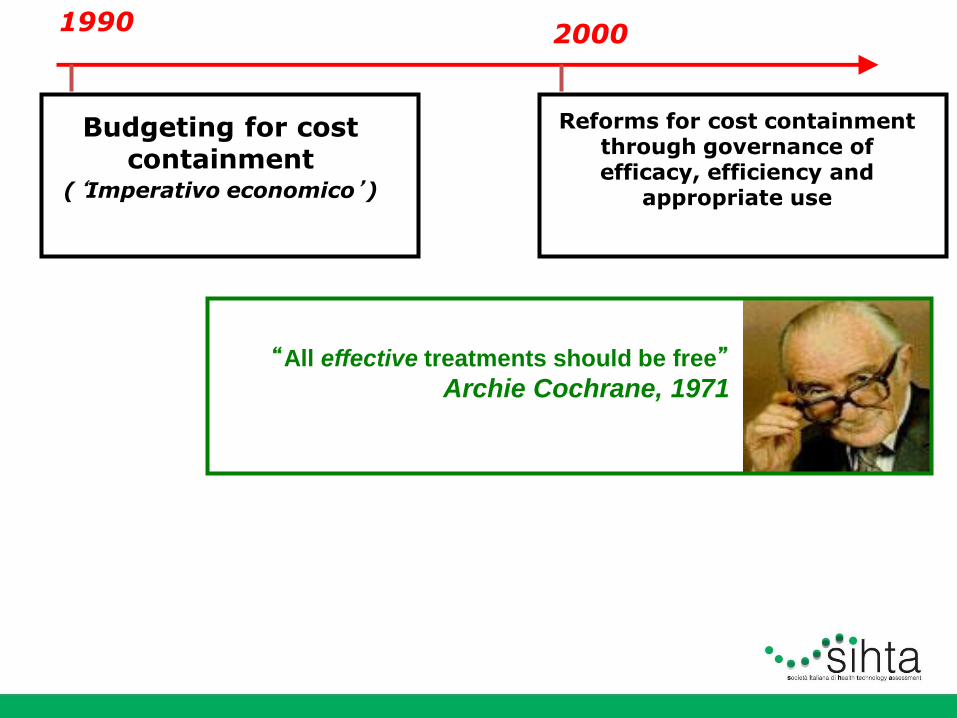
1990
Budgeting for cost containment
(‘Imperativo economico’)
2000
Reforms for cost containment through governance of efficacy, efficiency and
appropriate use
“All effective treatments should be free”
Archie Cochrane, 1971
1990
Budgeting for cost containment
(‘Imperativo economico’)
2000
Reforms for cost containment through governance of efficacy, efficiency and
appropriate use
“All effective treatments should be free”
Archie Cochrane, 1971
“All cost-effective treatments
should be free” Alan Williams, 1997
“All cost-effective treatments
should be free” Alan Williams, 1997
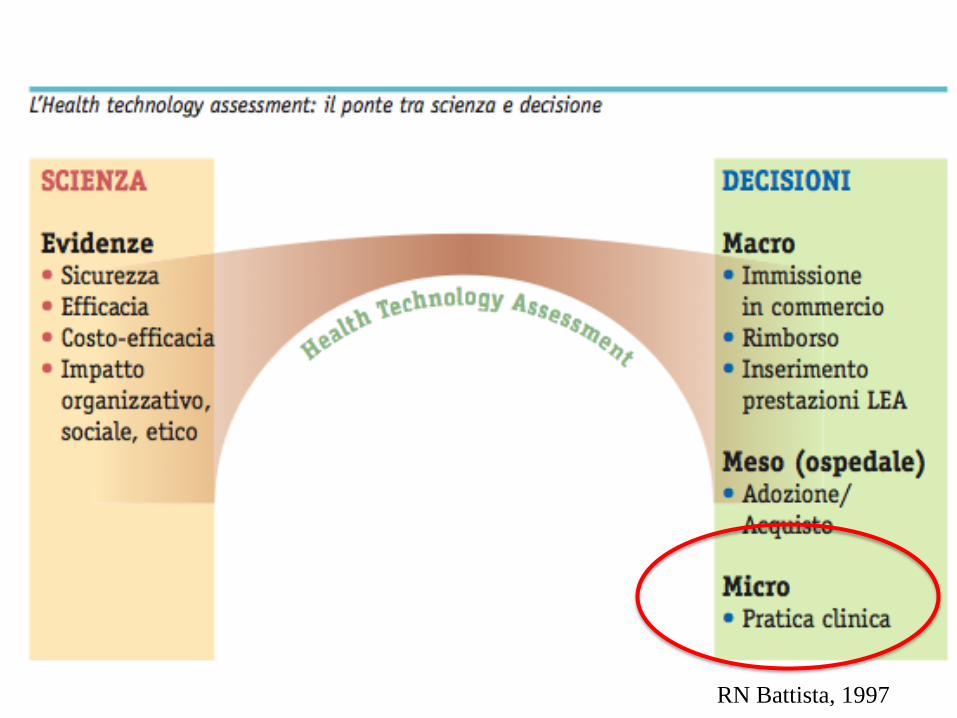
RN Battista, 1997

9
la storia del Technology Assessment
inizia da molto lontano… addirittura
…

10
…un senatore americano disse “…technical
information needed by policymakers is frequently not
available, or not in the right form. A policymaker
cannot judge the merits or consequences of a
technological program within a strictly technical
context. He has to consider social, economic, and
legal implication of any course of action…”
(U.S. Congress, House of Representatives, Congressman Emilio Daddario,
1967)
…nel 1967.. nel decidere se
inviare un uomo sulla luna…
• Qualità, equità, sostenibilità: quale equilibrio?
• Il contesto italiano: il riferimento dei LEA
• La qualità della assistenza sanitaria: tra ospedale e territorio
• L’individuo ed il sistema sanitario: come interagiscono?
• La carenza delle risorse: la percezione del clinico
• I programmi di miglioramento della qualità: pronti per il cambiamento?
• Le evidenze sulla efficienza dei programmi di cambiamento della cultura organizzativa nei contesti sanitari
• L’audit clinico come monitoraggio continuo della qualità
• Rischio clinico ed incident reporting
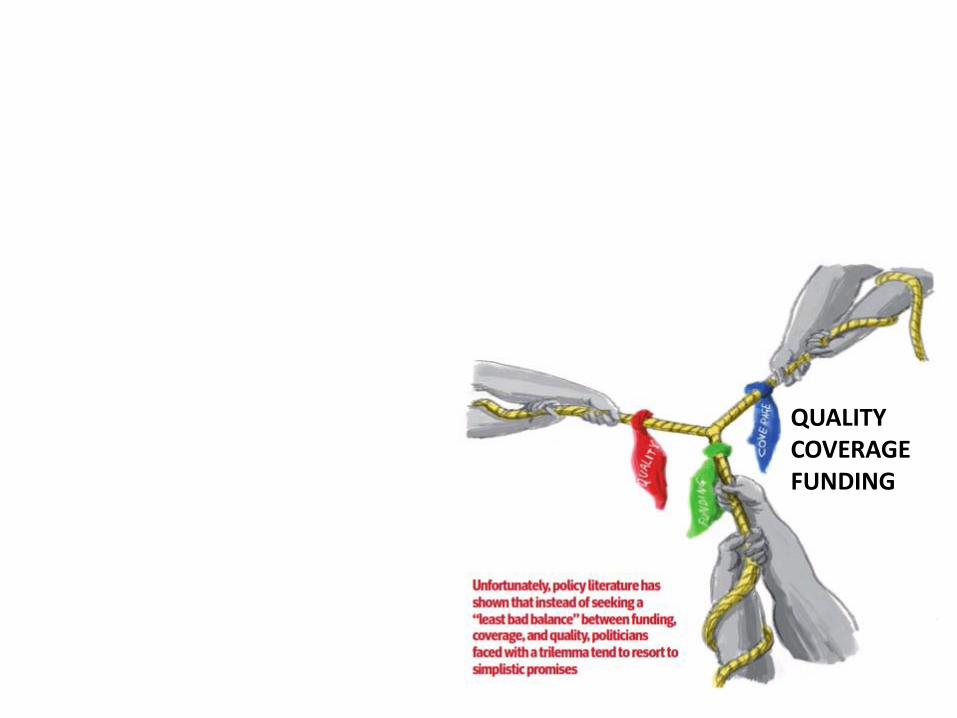
QUALITY COVERAGE FUNDING



La prospettiva britannica
>Ridurre l’eccesso di medicalizzazione
e la dipendenza dei pazienti dal sistema di
cura
>Smettere di utilizzare terapie non
costo-efficaci
>Ridurre i costi amministrativi
>Agire sulle aree di scarsa produttività
>Concordare gli indicatori
>Coinvolgere gli utenti e migliorarne le
conoscenze
>Ottenere migliori contratti con i fornitori
>Management dedicato ai programmi di
riduzione di spesa
QUALITY COVERAGE FUNDING

La prospettiva britannica
>Ridurre l’eccesso di medicalizzazione
e la dipendenza dei pazienti dal sistema di
cura
>Smettere di utilizzare
terapie non costo-efficaci >Ridurre i costi amministrativi
>Agire sulle aree di scarsa produttività
>Concordare gli indicatori
>Coinvolgere gli utenti e migliorarne le
conoscenze
>Ottenere migliori contratti con i fornitori
>Management dedicato ai programmi di
riduzione di spesa
QUALITY COVERAGE FUNDING
4 novembre 1992
http://ktclearinghouse.ca/cebm/
What is EBM?
Evidence-based medicine (EBM) is the integration of best research evidence with clinical expertise and patient values.

http://ktclearinghouse.ca/cebm/
What is EBM?
Evidence-based medicine (EBM) is the integration of best research evidence with clinical expertise and patient values.
by best research evidence we mean clinically relevant research, especially from patient centered clinical research into the accuracy and precision of diagnostic tests (including the clinical examination), the power of prognostic markers, and the efficacy and safety of therapeutic, rehabilitative, and preventive regimens.
http://ktclearinghouse.ca/cebm/
What is EBM?
Evidence-based medicine (EBM) is the integration of best research evidence with clinical expertise and patient values.
New evidence from clinical research both invalidates previously accepted diagnostic tests and treatments and replaces them with new ones that are more powerful, more accurate, more efficacious, and safer.

http://ktclearinghouse.ca/cebm/
What is EBM? Evidence-based medicine (EBM) is the integration of best research evidence with clinical expertise and patient values. by clinical expertise we mean the ability to use our clinical skills and past experience to rapidly identify each patient's unique health state and diagnosis, their individual risks and benefits of potential interventions, and their personal values and expectations.
http://ktclearinghouse.ca/cebm/
What is EBM? Evidence-based medicine (EBM) is the integration of best research evidence with clinical expertise and patient values. by patient values we mean the unique preferences, concerns and expectations each patient brings to a clinical encounter and which must be integrated into clinical decisions if they are to serve the patient.

LA MEDICINA CLASSICA
• Concetto di malattia • La medicina ha coniato il concetto di
‘malattia’ e aderisce a questo concetto nella sua attività.
• Le malattie definite come ontologie in medicina rappresentano il risultato di un processo di consenso talora recentemente esplicito, in precedenza più frequentemente implicito, relativamente alla definizione di un’ontologia.

• Il ragionamento diagnostico assume così le caratteristiche del riconoscimento di un’impronta digitale: si ricercano i punti di identità fra malattia conosciuta e situazione clinica del paziente e, quando i punti di identità superano un certo numero, si definisce la diagnosi (approccio euristico al problema).
LA MEDICINA CLASSICA
La medicina basata sulle evidenze, per sua natura, in generale ricerca e ottiene evidenze relative a malattie a definizione ontologica ben circoscritta, con studi clinici focalizzati su pazienti il più possibile privi di altre condizioni cliniche rilevanti che risulterebbero “confondenti” per le evidenze ricercate.

Scandinavian
Simvastatin Survival
Study (4S)
The Lancet, Vol 344, November 19, 1994

60
70
80
90
100
0 1 2 3 4 5 6
Simvastatin
Placebo
Coronary Death and Nonfatal MI
Years since randomization
% o
f p
ati
en
ts w
ith
ou
t e
ve
nts
34%
Risk Reduction
p<0.00001
The Lancet, Vol 344, November 19, 1994
Inclusion Criteria: Prior MI and/or angina pectoris

Baseline Characteristics
Mean age (years)-men
58.1 58.2
Mean age (years)-women
60.5 60.5
Angina only 21% 21%
MI only 62% 63%
Both angina and MI 17% 16%
Hypertension 26% 26% Smoker 27% 24%
TC (mg/dL) 260 260
LDL (mg/dL) 180 180
Placebo
(n=2223)
Simvastatin
(n=2221)
The Lancet, Vol 344, November 19, 1994

Holmes 2003
Importance of co-morbidity Prevalence and age trends for selected co-morbidities

• Progressivo invecchiamento della
popolazione
• Aumento dei pazienti con comorbilità
multiple - multimorbilità
• Queste categorie di pazienti sono
solitamente non incluse nei trial clinici
….in questi 20 anni che cosa
è cambiato
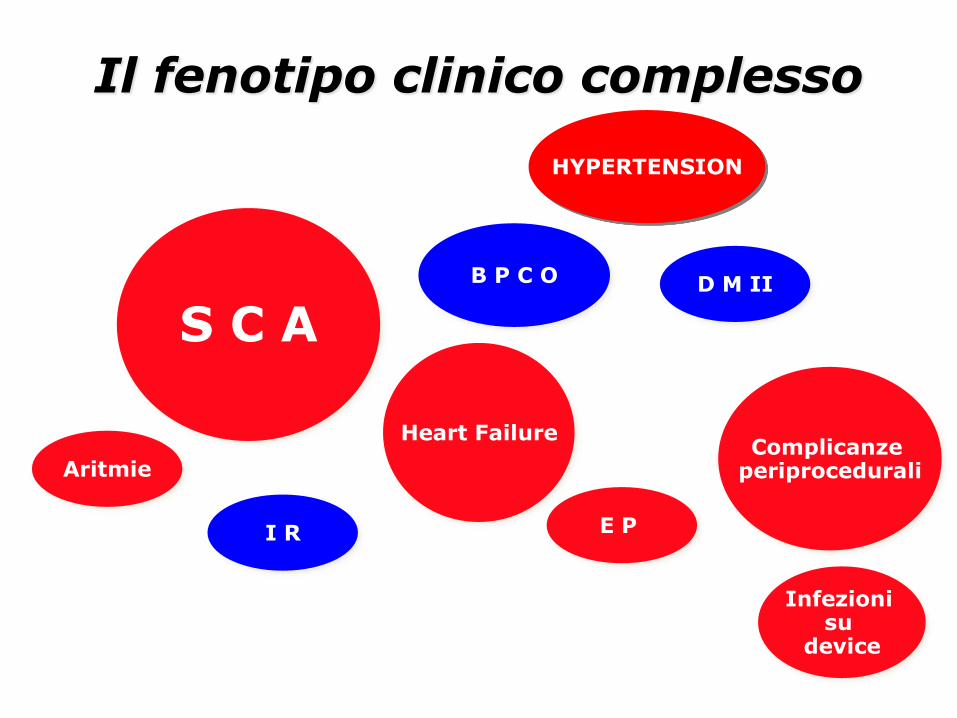
I R
S C A
B P C O
Heart Failure
E P
D M II
Aritmie
Infezioni su
device
Complicanze periprocedurali
Il fenotipo clinico complesso
HYPERTENSION
I R
ATRIAL FIBRILLATION
B P C O
Heart Failure
E P
D M II
Il fenotipo clinico complesso
HYPERTENSION
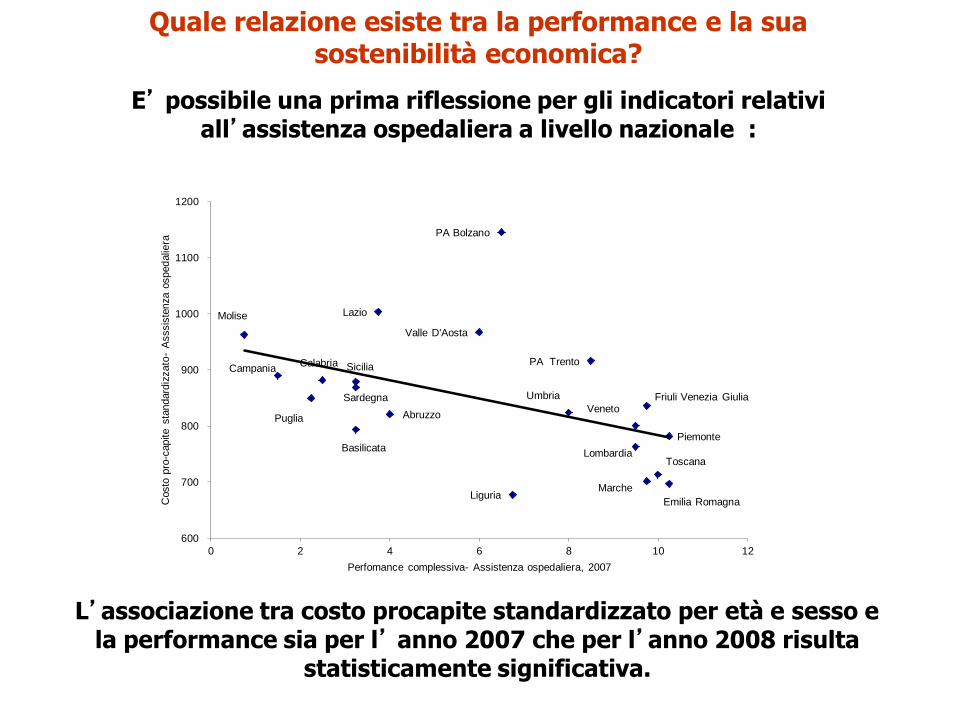
Quale relazione esiste tra la performance e la sua sostenibilità economica?
E’ possibile una prima riflessione per gli indicatori relativi all’assistenza ospedaliera a livello nazionale :
Piemonte
Valle D'Aosta
Lombardia
PA Bolzano
PA Trento
Veneto Friuli Venezia Giulia
Liguria Emilia Romagna
Toscana
Umbria
Marche
Lazio
Abruzzo
Molise
Campania
Puglia
Basilicata
Calabria Sicilia
Sardegna
600
700
800
900
1000
1100
1200
0 2 4 6 8 10 12
Costo
pro
-capite s
tandard
izzato
- A
sssis
tenza o
sped
alie
ra
Perfomance complessiva- Assistenza ospedaliera, 2007
L’associazione tra costo procapite standardizzato per età e sesso e la performance sia per l’ anno 2007 che per l’anno 2008 risulta
statisticamente significativa.
• The American College of Cardiology (ACC) released a list of ‘‘Five Things Physicians and Patients Should Question’’ in cardiology as part of Choosing Wisely which is an initiative of the American Board of Internal Medicine (ABIM) Foundation in partnership with Consumer reports.
• These were among 45 common tests and procedures recommended by nine medical specialty boards that should be performed less often.

The ACC list details the following five recommendations: 1. Don’t perform stress cardiac imaging or advanced non-invasive
imaging in the initial evaluation of patients without cardiac symptoms unless high-risk markers are present.
2. Don’t perform annual stress cardiac imaging or advanced non-invasive imaging as part of routine follow-up in asymptomatic
patients.
3. Don’t perform stress cardiac imaging or advanced non-invasive imaging as a pre-operative assessment in patients scheduled to undergo low-risk non-cardiac surgery.
4. Don’t perform echocardiography as routine follow-up for mild, asymptomatic native valve disease in adult patients with no change in signs or symptoms.
5. Don’t perform stenting of non-culprit lesions during percutaneous coronary intervention (PCI) for uncomplicated hemodynamically stable ST-segment elevation myocardial infarction (STEMI).
ACC Releases List of Five Tests/Procedures That May Be Overused or Misused as Part of Choosing Wisely Campaign
Patients were urged by these boards to question these
services if and when they are offered
first: stress tests or advanced noninvasive imaging should not be performed if there are no symptoms of heart disease or high-risk factors like diabetes or peripheral arterial disease are not present
Second:
cardiac imaging tests, particularly stress tests, should not be given as part of a routine annual follow up
in patients who have had no change in signs or symptoms

third:
cardiac imaging tests should not be given before performing low-risk surgery
that is not related to heart disease.

Fourth:
echocardiograms should not be used as routine follow-up care in adults with mild heart valve disease,
who have had no change in signs and symptoms.
• In addition to contributing to the rising costs of cardiovascular imaging, ordering stress myocardial perfusion imaging (MPI) tests for inappropriate indications adds to the radiation exposure of patients.
• The attention being directed at reducing the volume of cardiac imaging procedures that are inappropriate is occurring at a time when new imaging indications are emerging that may significantly impact on patient management and adherence to effective guideline-based therapy

Thus, the initiative by the ACC as part of the Choosing Wisely campaign to reduce the number of inappropriate cardiac imaging tests needs to be balanced by a willingness to approve new imaging tests if they impact favorably on clinical management and outcomes.
Da N. Dirindin
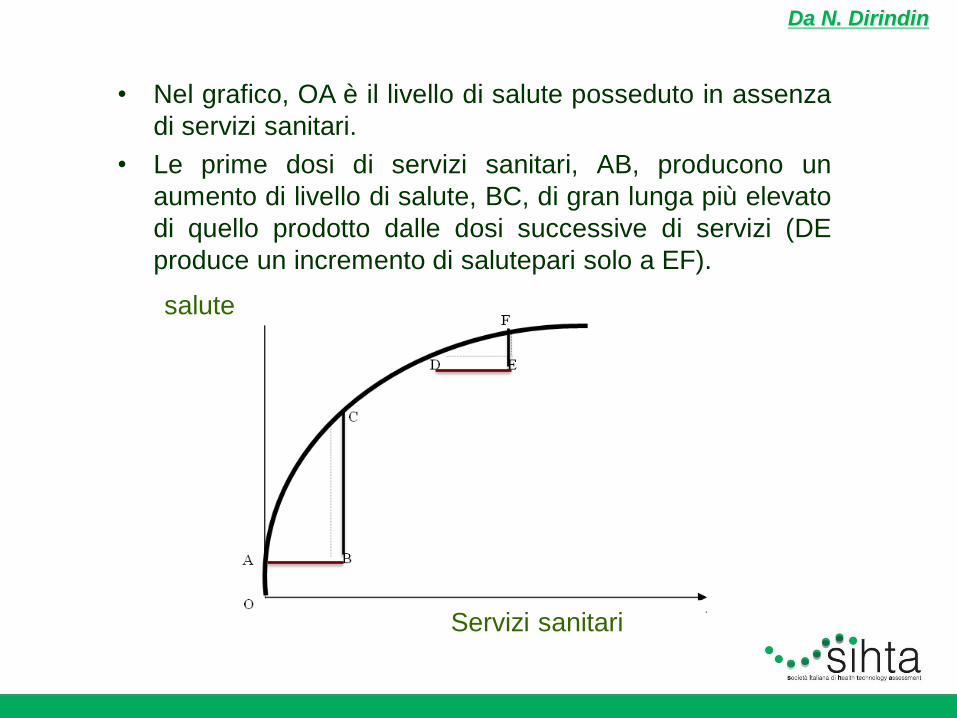
• Nel grafico, OA è il livello di salute posseduto in assenza
di servizi sanitari.
• Le prime dosi di servizi sanitari, AB, producono un
aumento di livello di salute, BC, di gran lunga più elevato
di quello prodotto dalle dosi successive di servizi (DE
produce un incremento di salutepari solo a EF).
salute
Servizi sanitari

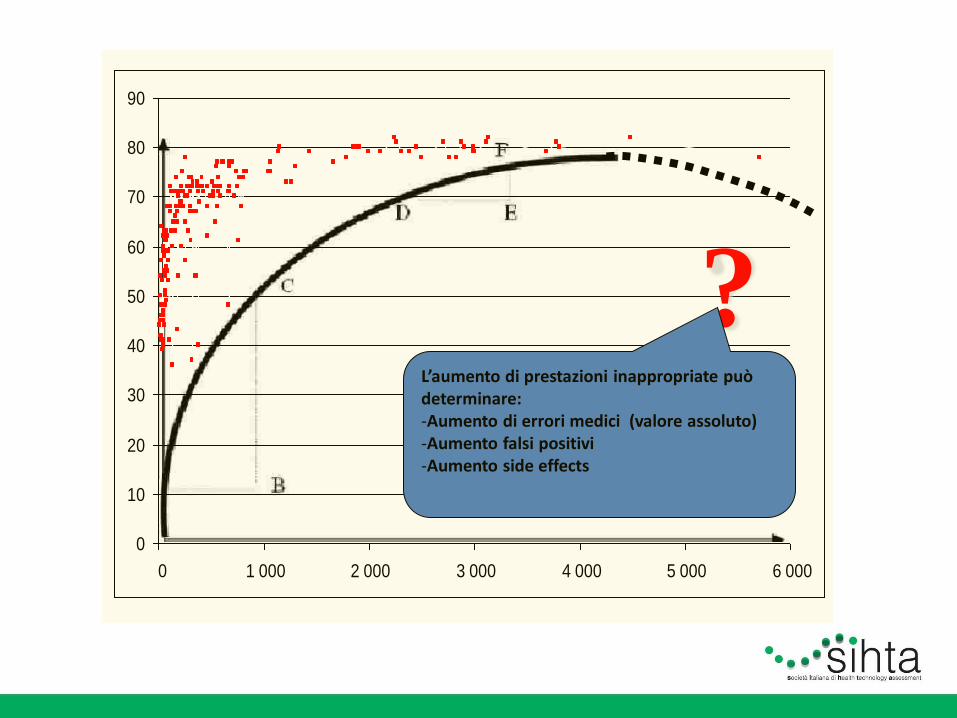
Dati OMS, 2003
0
10
20
30
40
50
60
70
80
90
0 1 000 2 000 3 000 4 000 5 000 6 000
? L’aumento di prestazioni inappropriate può determinare: -Aumento di errori medici (valore assoluto) -Aumento falsi positivi -Aumento side effects
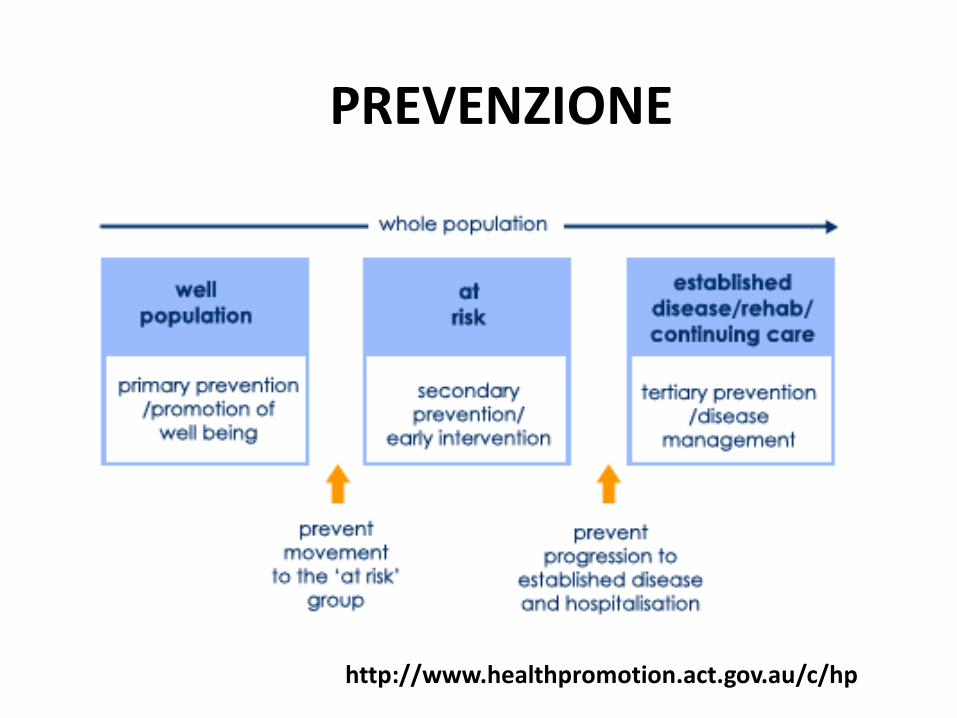
PREVENZIONE
http://www.healthpromotion.act.gov.au/c/hp
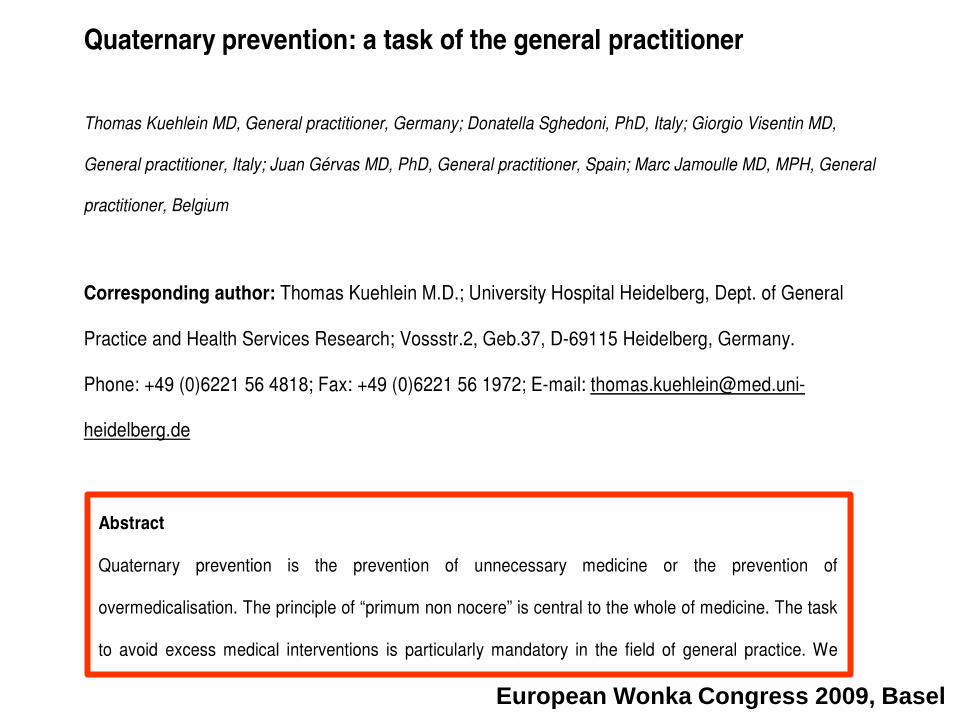
European Wonka Congress 2009, Basel

The main objection is the perception that ‘Choosing Wisely’ is the first collective effort on the part of professional medical societies to decide how to practise medicine on the basis of cost first and foremost.

BUT…

The ACC list details the following five recommendations: 1. Don’t perform stress cardiac imaging or advanced non-invasive
imaging in the initial evaluation of patients without cardiac symptoms unless high-risk markers are present.
2. Don’t perform annual stress cardiac imaging or advanced non-invasive imaging as part of routine follow-up in asymptomatic
patients.
3. Don’t perform stress cardiac imaging or advanced non-invasive imaging as a pre-operative assessment in patients scheduled to undergo low-risk non-cardiac surgery.
4. Don’t perform echocardiography as routine follow-up for mild, asymptomatic native valve disease in adult patients with no change in signs or symptoms.
5.Don’t perform stenting of non-culprit lesions during percutaneous coronary intervention (PCI) for uncomplicated hemodynamically stable ST-segment elevation myocardial infarction (STEMI).
ACC Releases List of Five Tests/Procedures That May Be Overused or Misused as Part of Choosing Wisely Campaign

Original Article Randomized Trial of Preventive Angioplasty in
Myocardial Infarction
David S. Wald, M.D., Joan K. Morris, Ph.D., Nicholas J. Wald, F.R.S., Alexander J. Chase, M.B., B.S., Ph.D., Richard J. Edwards, M.D., Liam O. Hughes, M.D., Colin Berry, M.B., Ch.B., Ph.D., Keith G. Oldroyd, M.D., for
the PRAMI Investigators
N Engl J Med
Volume 369(12):1115-1123 September 19, 2013
• Patients with acute STEMI were randomly assigned to undergo infarct-vessel-only PCI or preventive PCI (PCI to noninfarct arteries with stenoses).
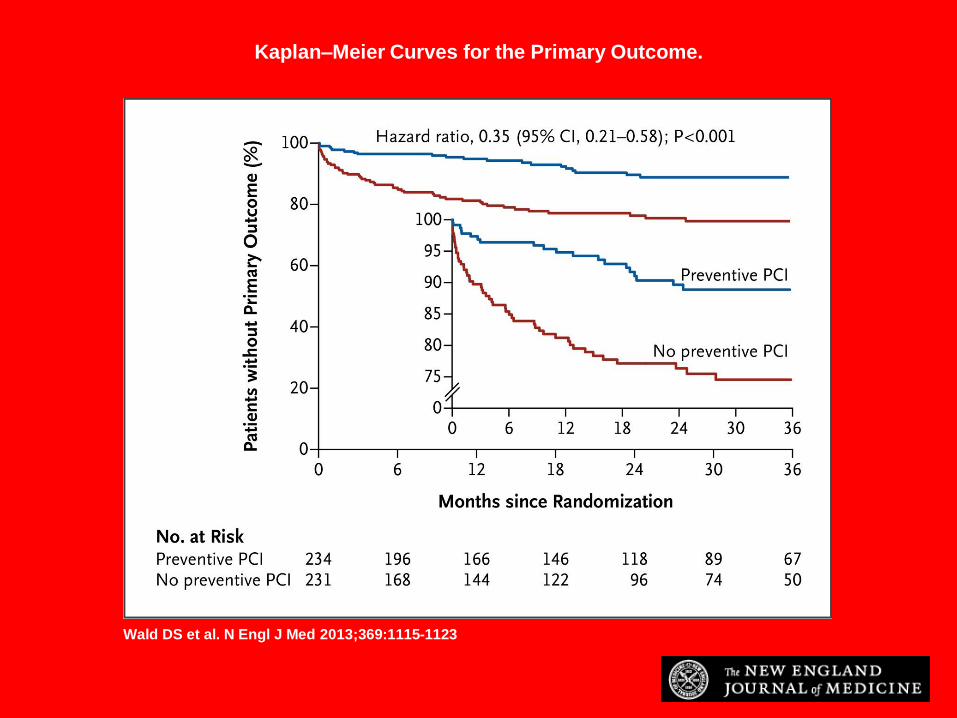
Kaplan–Meier Curves for the Primary Outcome.
Wald DS et al. N Engl J Med 2013;369:1115-1123
Conclusions
• In patients with STEMI and multivessel coronary artery disease undergoing infarct-artery PCI, preventive PCI in noninfarct coronary arteries with major stenoses significantly reduced the risk of adverse cardiovascular events, as compared with PCI limited to the infarct artery.
http://ktclearinghouse.ca/cebm/
What is EBM?
Evidence-based medicine (EBM) is the integration of best research evidence with clinical expertise and patient values.
by best research evidence we mean clinically relevant research, especially from patient centered clinical research into the accuracy and precision of diagnostic tests (including the clinical examination), the power of prognostic markers, and the efficacy and safety of therapeutic, rehabilitative, and preventive regimens. New evidence from clinical research both invalidates previously accepted diagnostic tests and treatments and replaces them with new ones that are more powerful, more accurate, more efficacious, and safer.
http://ktclearinghouse.ca/cebm/
What is EBM?
Evidence-based medicine (EBM) is the integration of best research evidence with clinical expertise and patient values.
by best research evidence we mean clinically relevant research, especially from patient centered clinical research into the accuracy and precision of diagnostic tests (including the clinical examination), the power of prognostic markers, and the efficacy and safety of therapeutic, rehabilitative, and preventive regimens. New evidence from clinical research both invalidates previously accepted diagnostic tests and treatments and replaces them with new ones that are more powerful, more accurate, more efficacious, and safer.

• La nostra struttura formativa è da decenni
tradizionalmente basata sulle ontologie e
su conoscenze evolute su basi strutturali e
classificative.
• I curricula sono stati approntati con il preciso
obiettivo di trasferire le conoscenze e le
competenze specifiche e settoriali generate
attraverso l’articolazione della medicina
nelle specialità, in linea con un approccio
riduzionistico.
• la visione sistemica è apparsa come una pericolosa ed a tratti inquietante modalità di allontanamento dalla rassicurante e ordinata capacità di analisi dello specialismo.
• La complessità pertanto è un tema sostanzialmente al momento non presente in modo organico nella formazione curriculare e post-curriculare.

4P medicine Predictive
Preventive
Personalized
Participatory
An Evolving Scenario Integrated Care supported by ICT
Efficient patient management Modulation of disease progress
ICT as enabler of a new model of care