children with esrd: they’re not little adults! with esrd- vogt.pdf · –c. lupus nephritis –d....
TRANSCRIPT

Children with ESRD:
They’re Not Little Adults!
Beth A. Vogt, MD
Rainbow Babies and
Children’s Hospital
Conflict of Interest/
Disclosure Statement
• I have no conflicts of interest to disclose
• I will not discuss off label use of drugs in my
presentation

Case: Ian
• 14 yr old teenage boy
• Born with posterior urethral valves and renal dysplasia
• Medically managed CKD until started PD at age 2 yrs
• Supported with G-tube feedings until age 6 yrs
• Living related donor transplantation from Mom at age 4.5 yrs
• Complications
– Rejection x 2
– Chronic low level EBV titer
– Recurrent sinusitis/URIs
– Short stature (height 5 ft, weight 86 lbs)
– Behavioral issues, school avoidance, adherence concerns
– Gradual loss of kidney function (Cr 2.2, eGFR 29 ml/min)
• Starting to plan for next step as allograft is failing after 10 yrs
Outline
• Causes of CKD/ESRD in children
• Medical issues
• Psychosocial issues
• Treatment options for children with ESRD
– Peritoneal dialysis
– Hemodialysis
– Transplantation

ESRD in Children
• Rare in children (9 per million)
• High burden of care
• Underlying causes of ESRD are very
different in children than in adults
– NOT diabetes and hypertension!
– Congenital conditions
– Glomerulonephritis
– Other

Congenital Kidney Disease
• 40% of pediatric ESRD
• Renal dysplasia– Poorly developed kidneys in utero
– May be associated with obstruction• Posterior urethral valves
– May be associated with a syndrome• Eagle Barrett syndrome (prune belly
syndrome)
– May be an isolated finding• Sarah Hyland (Haley Dunphy of Modern
Family)

Glomerular Disease
• 25% of pediatric ESRD
• Glomerulonephritis– Lupus nephritis
– MPGN
– IgA nephropathy
– HSP nephritis
– Vasculitis
• Steroid-resistant nephrotic syndrome– Infantile NS
– Focal segmental glomerulosclerosis• Alonzo Mourning, Sean Elliott, Gary Coleman
• Hereditary nephritis– Alport syndrome

Other Conditions
• Genetic disorders
– ARPKD
• h/o severe AKI– Former preemies
– ICU care• Sepsis
• BMT
• Cardiac surgery
• Cancer

Medical Issues

Measurement of
Kidney Function
• Serum creatinine (Cr)
• Affected by
– Age
– Muscle mass
– Creatinine supplements
• Cannot use MDRD, CKD-EPI formulas for eGFR
• Use Schwartz formula


Blood Pressure
• Adult norms
– < 120/80 Normal
– > 140/90 HTN
• Pediatric BP norms
– Age
– Height
– Gender
• Fourth Report BP table
• BP > 120/80 is always high in a child

5 yr old boy with
height at 5th
percentile

Normal:
BP < 104/65
PreHTN:
BP 104/65-
108/69
Stage 1 HTN:
BP > 108/69-
120/82
Stage 2 HTN:
BP > 120/82
Average BP:
90/50
Fourth Report on High BP in Children, Pediatrics 2004.

Anemia
• Lack of erythropoietin, +/- iron
• May be exacerbated by– Frequent lab tests
– Residual blood loss in HD circuit
– Uncontrolled CKD-MBD
• Microtainers can reduce blood loss
• EPO and Venofer (dosed per kg)
• Younger children may need higher doses of EPO
• Goal Hb 10-12 g/dl

Malnutrition
• Weight loss OR failure to
gain weight
• Multifactorial
• Often need oral, NG or G-
tube feedings
• Can help with catch up
growth
• Caution: obesity can occur if
weight gain without good
linear growth

Weight Gain Improves
with GT Feeds
CKD-MBD
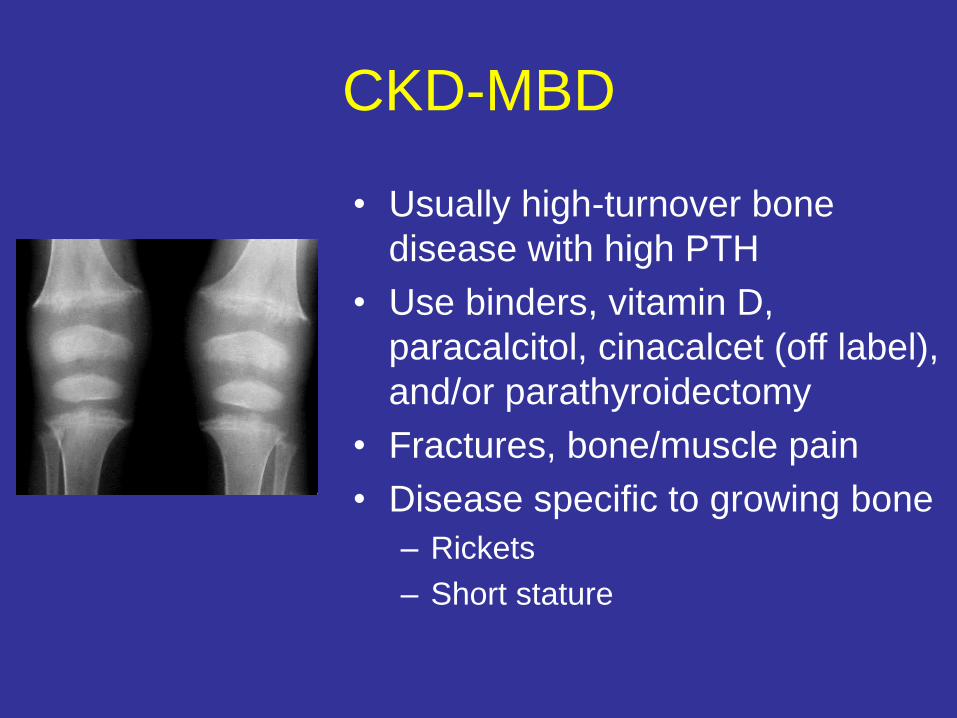
• Usually high-turnover bone
disease with high PTH
• Use binders, vitamin D,
paracalcitol, cinacalcet (off label),
and/or parathyroidectomy
• Fractures, bone/muscle pain
• Disease specific to growing bone
– Rickets
– Short stature
Short Stature
• >1/3 of kids on dialysis have short stature
• Multifactorial problem
– CKD-MBD
– Malnutrition
– Steroids
– Growth hormone (GH) resistance
• More of an issue with early onset CKD
• Treatment: nutrition, treat PTH and other
metabolic issues
• Recombinant GH
• Daily SQ injections given x years
• Track growth curve, height Z scores

Growth Improves with rGH

Cardiovascular Disease
• Growing focus of attention
• Usually does not manifest in
childhood years, but CV risk is
silently building
• 50% of kids on dialysis have LVH
• Treatment
– Tight BP control
– Fluid balance
– Treat anemia and CKD-MBD
– Surveillance echocardiograms

Psychosocial Issues

Quality of Life
• Multiple challenges for kids with ESRD
– Physical changes
– Need for medications
– Need for treatments
– Time spent away from school/peers
– Dependence on medical equipment
• Peds QOL scores are low and equal to
those of children with cancer!
Neurocognitive Concerns
• May have developmental delay, learning
disabilities
• IQ lower than in non-CKD/ESRD siblings
• Lower scores in
– Verbal performance
– Memory
– Executive function
– Problem solving

Psychological Concerns
• Issues with short stature, looking younger
than stated age
• Depression
• Fear/anxiety
• Needle phobia
• Family needs
• Non-adherence

Transition of Care
• Movement of patients from pediatric to
adult healthcare services
• Occurs between 18-21 years of age
• New problem created by improvement in
pediatric patient survival
• High risk time; requires a lot of
preparation; optimally “Transition Clinic”

Treatment Options for
Pediatric ESRD

Choosing an Option
for ESRD Treatment
• Pediatric Nephrologists usually follow their
patients from early stages of CKD
• Formal “options meeting” when patient
enters CKD 4 (GFR <30 ml/min)
– Discuss both dialysis options AND transplant
• Transplant almost always preferred in
children

Transplantation

Transplantation
• Preemptive transplantation is
treatment of choice!
• Only 20% of children are able
to get a preemptive transplant
– Size
– Lack of donor
– Late diagnosis
• Dialysis should be used as a
“bridge to transplant”

Benefits of Renal
Transplantation in Children
• Freedom from dialysis!
• Lower mortality/morbidity
• Improved growth
• Improved cognition and school performance
• More normal lifestyle

Special Considerations in
Pediatric Transplantation• Shorter waiting times
– Prioritized allocation to pediatric recipients
– Living donors
• Technical issues
– Smaller children
• Increased risk of infection (EBV, CMV, BK)
• Recurrent disease
• Adherence concerns (teens)

Peritoneal Dialysis

Peritoneal Dialysis
• Preferred dialysis modality for most children, particularly infants
• Technically easier, no needles
• Minimal interference with school and after-school activities
• Less restrictive diet
• Allows parents to provide their child’s care

Peritoneal Dialysis
• CCPD (rarely CAPD)
• Children are usually
high transporters
• Dwell volume
– 40 ml/kg
– 1100 ml/m2
• Treatment time
– 8 hrs; can be much
longer (12-13 hrs) in
infants

Peritonitis
• Peritonitis rate highest in youngest children
– < 1 yrs--1:15.3 months
– > 12 yrs--1:21.2 months
• Young children more likely to be hospitalized
• G-tube considerations
– Placement at a different time than PD catheter
– Placement as far as possible from PD catheter

Hemodialysis

Hemodialysis
• Less desirable dialysis
choice for children
– More restrictive diet
– Interrupts normal activities
– Access challenges
– Travel challenges
• Reserved for pediatric
patients with:
– PD failure
– Noncompliance issues
– Patient/family preference

Fistula
• Preferred access unless
– Weight < 20 kg
– Bridging to peritoneal
dialysis
– Expectation of transplant in
1 year
• Takes longer to mature
than in adults (> 4 months)

Graft
• Synthetic material
• Can be used in a
couple of weeks
• May be useful in
children with
smaller vessels

Tunneled Catheter
• Least desired access
• May be used in
– Children < 20 kg
– Bridging to PD
– Transplant expected in 6-12 mos
– Exhausted access
• Complications
– Infection
– Thrombosis
– Vessel stenosis
– Pro-inflammatory state
8F Medcomp 8-20 kg10F Medcomp Split 20-40 kg14F Medcomp Split >40 kg

Hemodialysis Equipment• Dialyzers
– F4 42 ml <20 kg
– F160 83 ml >20-80 kg
– F180 99 ml >80 kg
• Dialysis tubing– Neonatal 24 ml <10 kg
– Pediatric 67 ml 10-20 kg
– Adult 130 ml >20 kg
• Volume of dialyzer + tubing should be <10% of patient’s blood volume (80 ml/kg x wt x 0.1)
• 80 ml/kg x 18 kg x 0.1 = 144 ml
• F4 dialyzer (42 ml) + peds tubing (67 ml) = 109 ml
Circuit Priming• Needed in patients < 10 kg or
when circuit volume is >10%
of blood volume
• Prevents instability during
initiation of treatment
• Priming options
– Heparinized, diluted prbcs
from Blood Bank (hct 35%)
– 5% albumin
• Blood should not be returned
to patient at end of treatment

Hemodialysis Prescription
• Pediatric blood flow rate is
usually much lower than adult
blood flow rate
• For 18 kg patient, blood
flow18 x 5 = 90 ml/min
• Dialysate flow is usually 500
or 800 ml/min
• Treatments 3.5-4 hrs x 3
(may need 4x/week in
infants/toddlers)

Fluid Balance
• Dry weights are smaller and more
unusual values
– Ex. 10.5 kg
– Dry weights change with growth
• Fluid removal goals smaller and unusual
– Max removal for infant
– 10.5 kg x 13 ml/kg/hr x 3.5 hr = 480 ml
• Pre/post weights may involve
– Infant scale
– Staff supervision
• Errors have greater risk
• Blood volume monitoring helpful

Anticoagulation
• Heparin bolus
– Same scheme as adults
• Heparin infusion
– Occasionally used in infants, acute setting
• NS boluses q 30 min
– F4 100 ml flush
– All others 200 ml flush
Remember, smaller child, smaller dialyzer, smaller
flush volume

Medication Dosing
• Cannot use standard adult doses in children
• Children vs. adults
– Smaller size
– Increased volume of distribution
– Increased drug metabolism
• Drug dosing is usually in mg/kg
– Vancomycin 20 mg/kg x 18 kg = 360 mg
– Venofer load 1.4 mg/kg x 18 kg = 25 mg

Hemodialysis Adequacy
• KT/V goal > 1.2
• URR goal > 65%
• PCR goal higher in children than adults because of higher protein requirement for growing children
– < 6 mos >2.2
– 6 mos-3 yrs >1.8
– 4-6 yrs >1.5
– 7-10 yrs >1.2
– 11-14 yrs >1.0

Conclusions
• Children with ESRD are not little adults!
• Pediatric ESRD is due to congenital disorders and GN, not HTN and diabetes
• Cr and BP have age-adjusted norms
• Transplant is first choice, followed by PD then HD
• Medication doses, HD and PD Rx are all dosed by weight
• Special issues: growth, development, short stature, transition
• Risk of error is higher, particularly in infants
• Kids are resilient, and generally do well!

Questions

Question 1
• The most likely cause of ESRD in a 4 year
old boy is:
– A. Hypertensive nephrosclerosis
– B. Congenital kidney disease (renal dysplasia)
– C. Lupus nephritis
– D. Diabetic nephropathy
Question 2
• A 5 year old girl has a serum Cr of 1.0 mg/dl.
She most likely has:
– A. Normal kidney function
– B. End stage kidney disease
– C. Lab error
– D. Impaired kidney function

Question 3
• Which statement is true regarding pediatric
blood pressure?
– A. 120/80 is a normal BP for a 4 year old girl
– B. Children on dialysis can develop target organ
damage (LVH) but rarely have cardiac events
– C. Goal BP for all pediatric dialysis patients is
under 140/90
– D. Hypertension in a child is defined as BP > 50th
percentile
Question 4
• Which of the following is a manifestation of renal bone disease (CKD-MBD) seen only in children?
– A. Brown tumor
– B. Rickets
– C. Fractures
– D. Osteopenia

Question 5
• Which statement is correct regarding growth/nutrition in pediatric dialysis patients?
– A. Oral and G-tube dietary supplements may be needed to achieve nutritional goals
– B. Growth hormone injections are used to improve weight gain
– C. Dialysis patients cannot become obese
– D. Phosphate binders such as Renvela are not indicated in children

Question 6
• Which statement is true about pediatric dialysis patients?
– A. A mature 17 year old boy may sign himself off treatment early
– B. All pediatric HD patients have developmental delay
– C. Children on dialysis may transition to adult providers at age 16 years
– D. Pediatric dialysis patients have low QOL scores

Question 7
• The treatment of choice for children with
ESRD is:
– A. Chronic ambulatory peritoneal dialysis (CAPD)
– B. In center hemodialysis
– C. Kidney transplantation
– D. Chronic cycling peritoneal dialysis (CCPD)

Question 8
• Which of the following is true regarding pediatric hemodialysis access:
– A. Catheters are the preferred access in children to avoid needlestick pain
– B. Catheter choice is based on the child’s size/weight
– C. Fistulas mature more quickly in children than adults
– D. Fistulas are the preferred access in children < 20 kg

Question 9
• To prevent instability when initiating
hemodialysis, the total volume of the circuit
(dialyzer + tubing) should be:
– A. Less than 200 ml
– B. Less than 10% of the patient’s blood volume
– C. 10 ml/kg
– D. Less than 2% of the patient’s blood volume

Question 10
• All of the following are advantages of PD over
HD in children EXCEPT:
– A. Better school attendance
– B. No needles
– C. Fewer hours on dialysis machine
– D. Less restrictive diet
