chest and cvs radiology mocks fcps
TRANSCRIPT

Chest and CVS Radiology Mocks
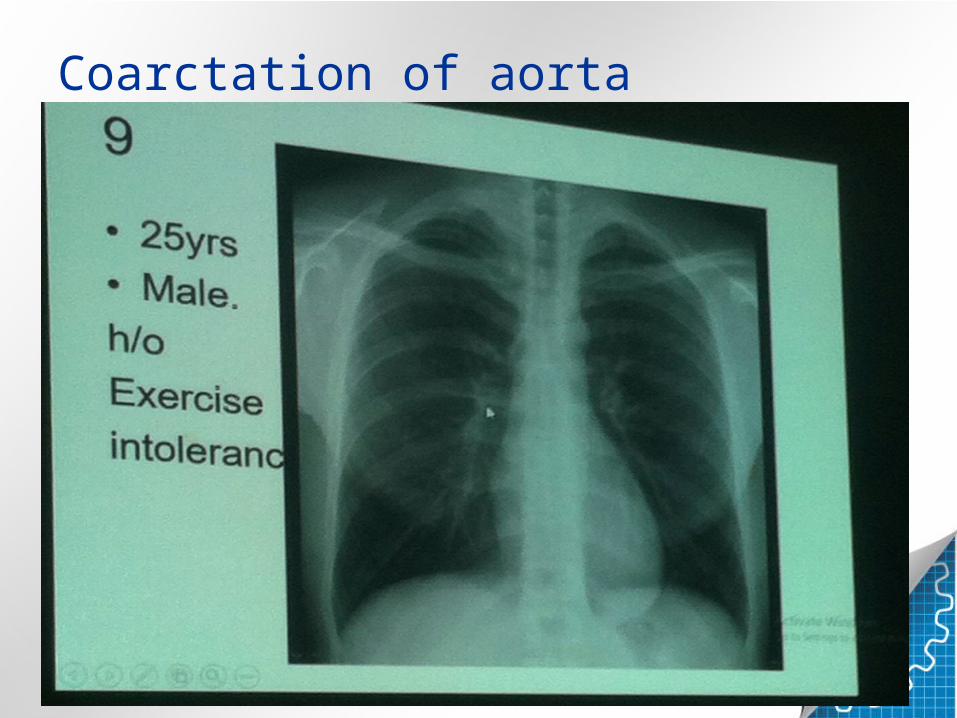
Coarctation of aorta

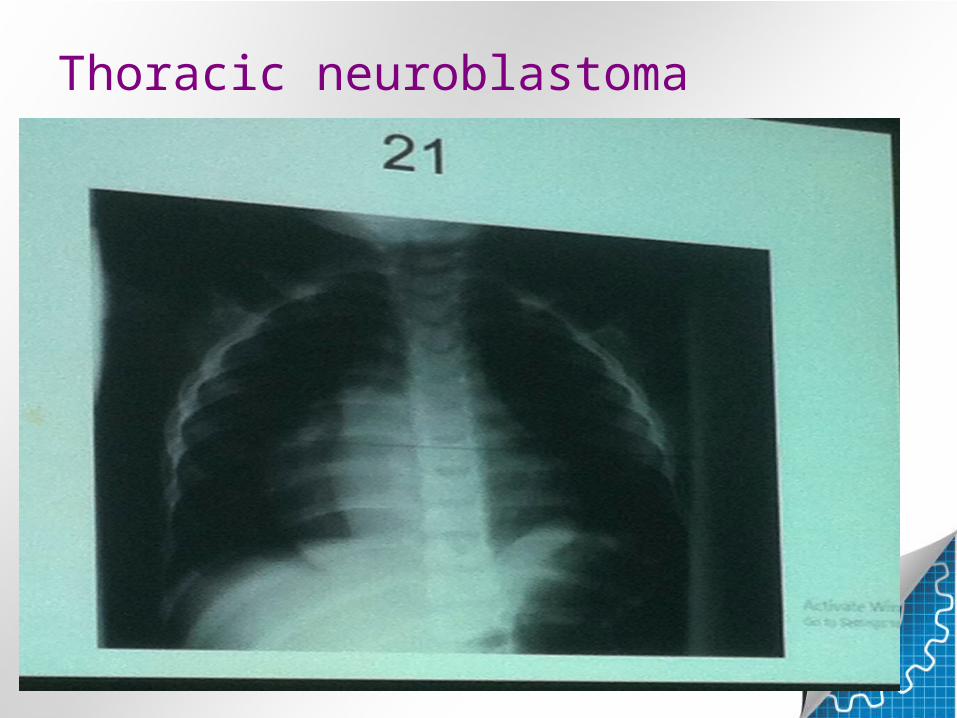
Thoracic neuroblastoma


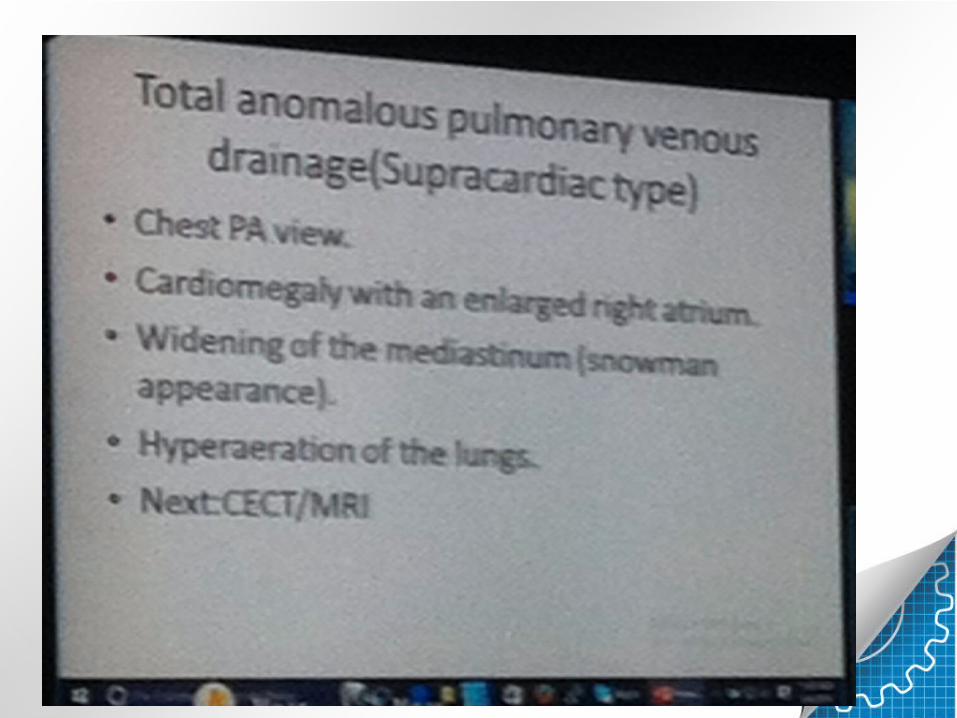
TAPVR

Scimitar Syndrome


Atherosclerotic aneurysm descending aorta

Solitary pulmonary nodule

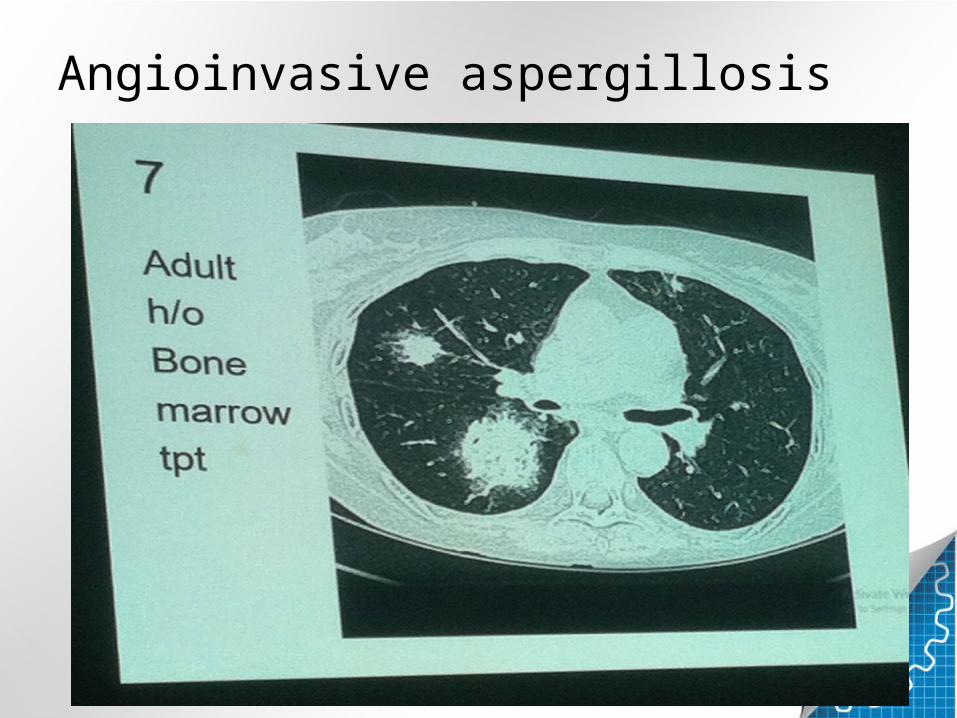
Angioinvasive aspergillosis

Lymphangitis carcinomatosa


Asbestosis


Anterior medistinal mass


IPF


Achalasia cardia
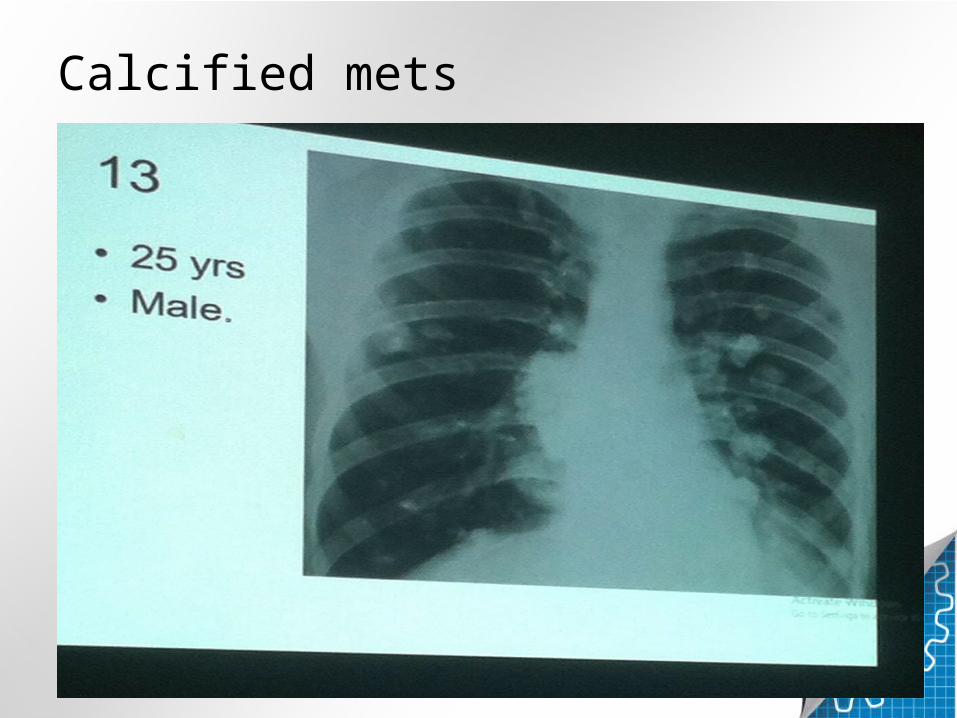
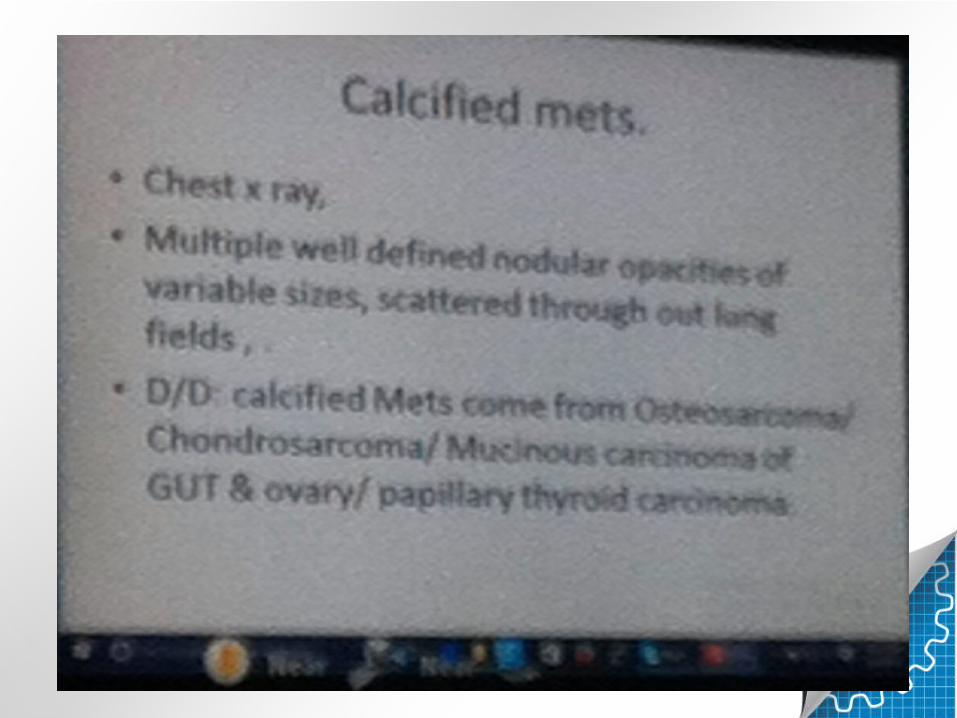
Calcified mets
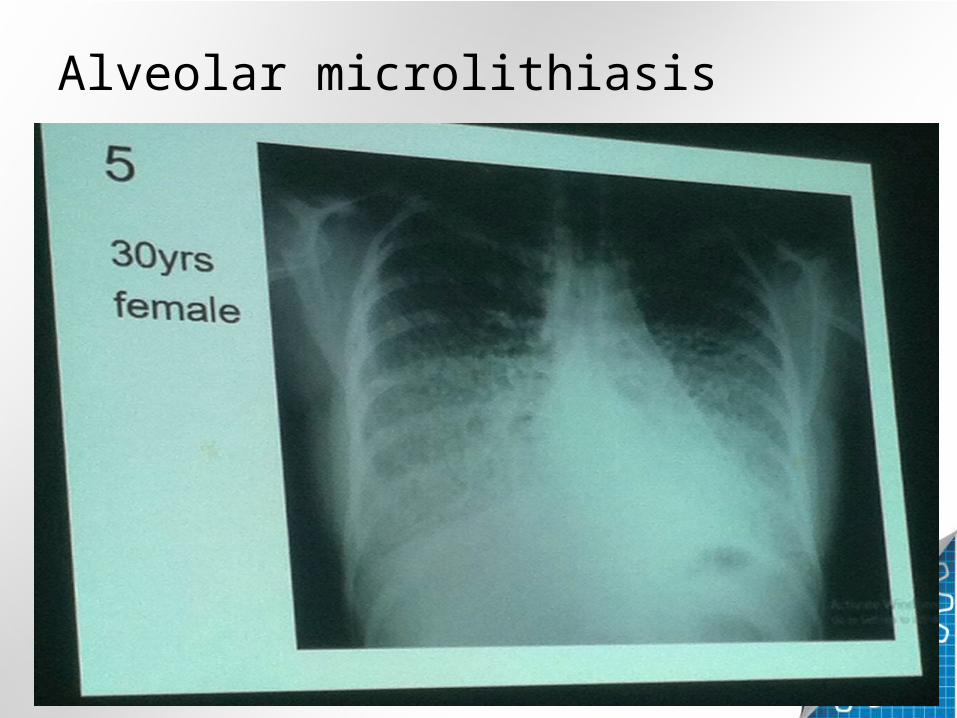
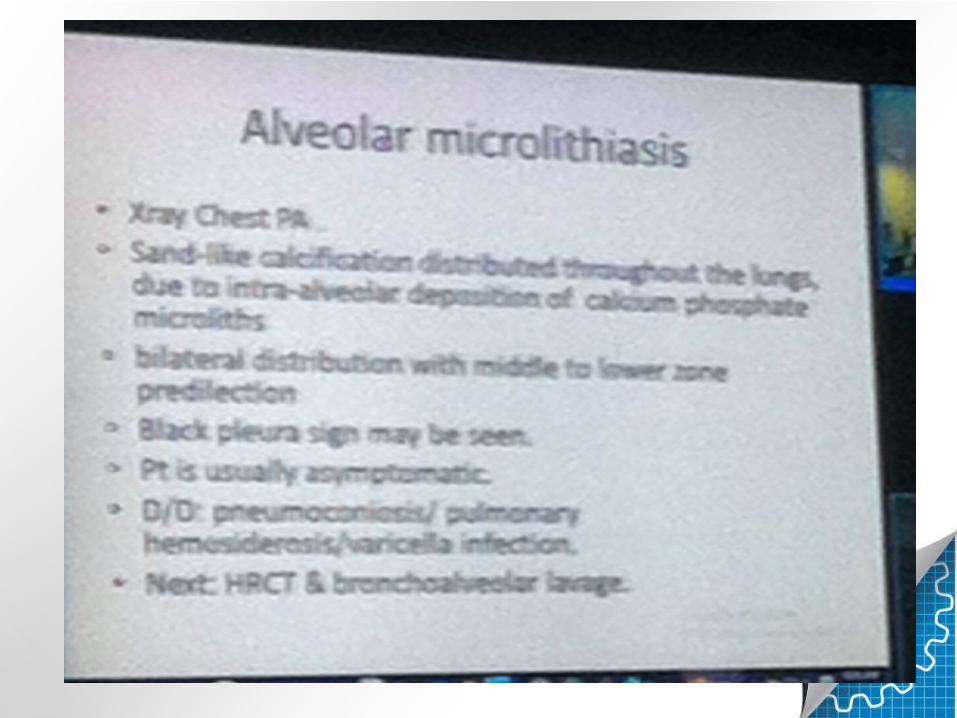
Alveolar microlithiasis

Bronchoceles
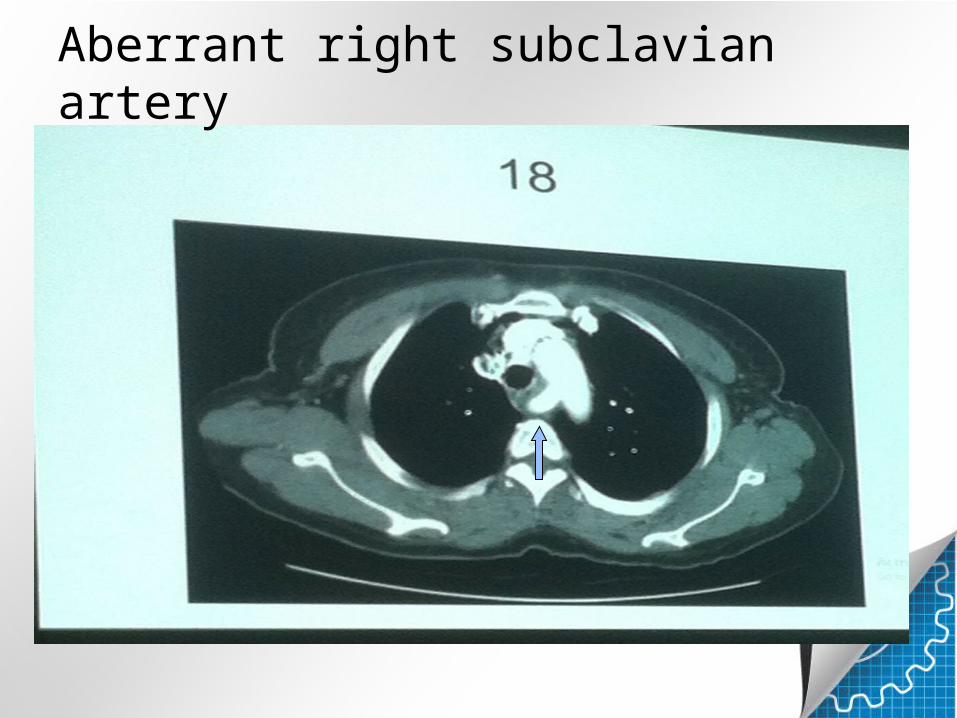
Aberrant right subclavian artery

Left upper lobe collapse

Centrilobular emphysema more in upper lobes


Intralobar sequestration


Hiatal hernia


ARDS


Mesothelioma

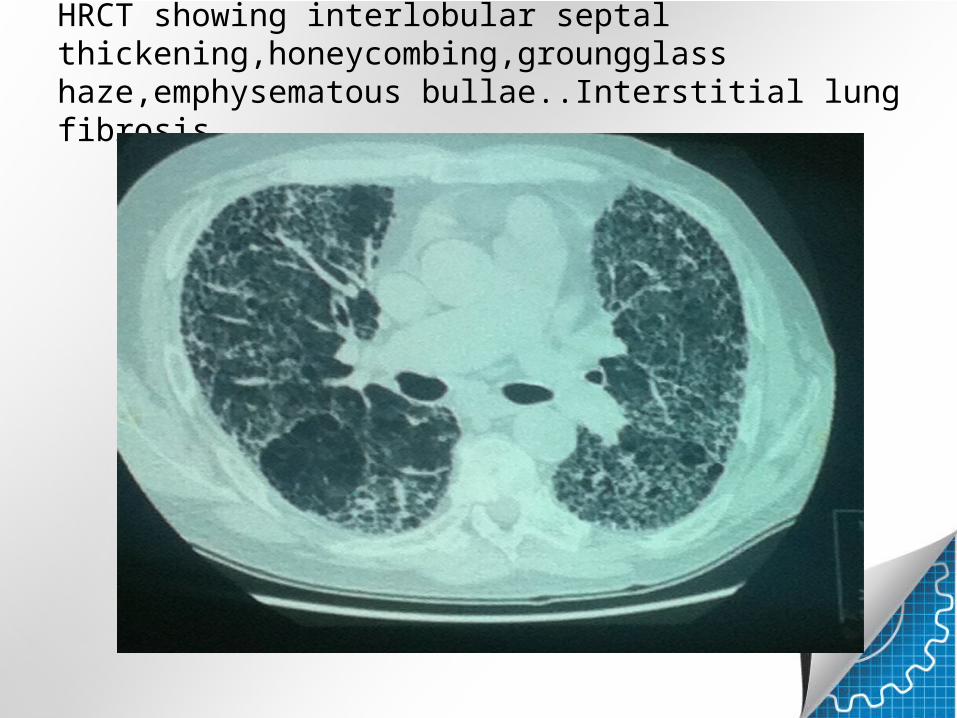
HRCT showing interlobular septal thickening,honeycombing,groungglass haze,emphysematous bullae..Interstitial lung fibrosis

Soft tissue density mass left hila with left upper lobe collapse and pull up of hilum wit raised hemidiaphragm
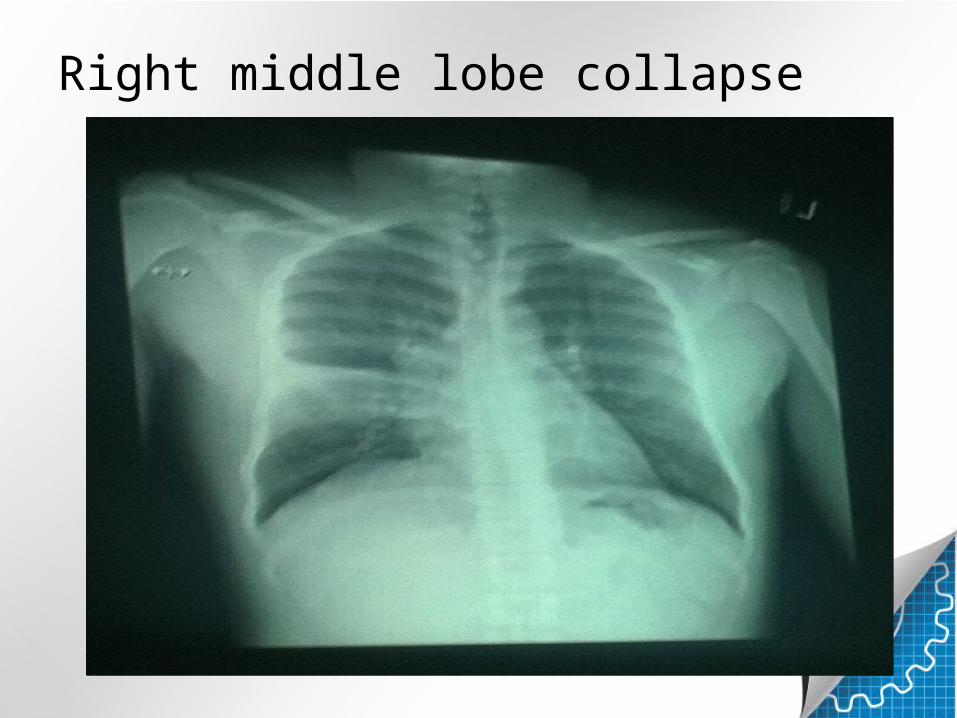
Right middle lobe collapse
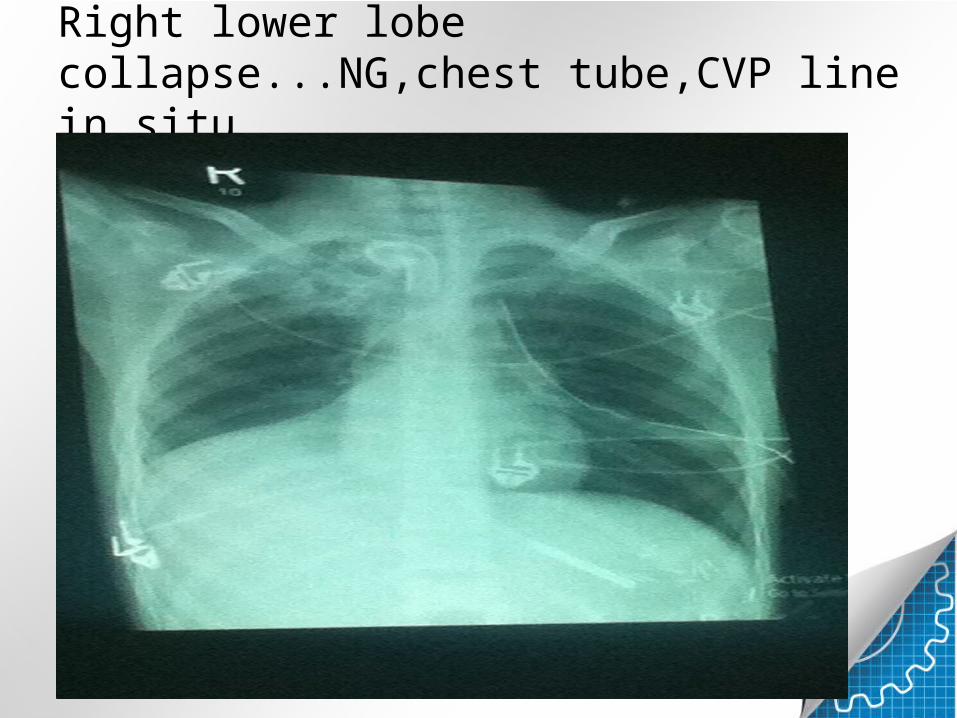
Right lower lobe collapse...NG,chest tube,CVP line in situ.
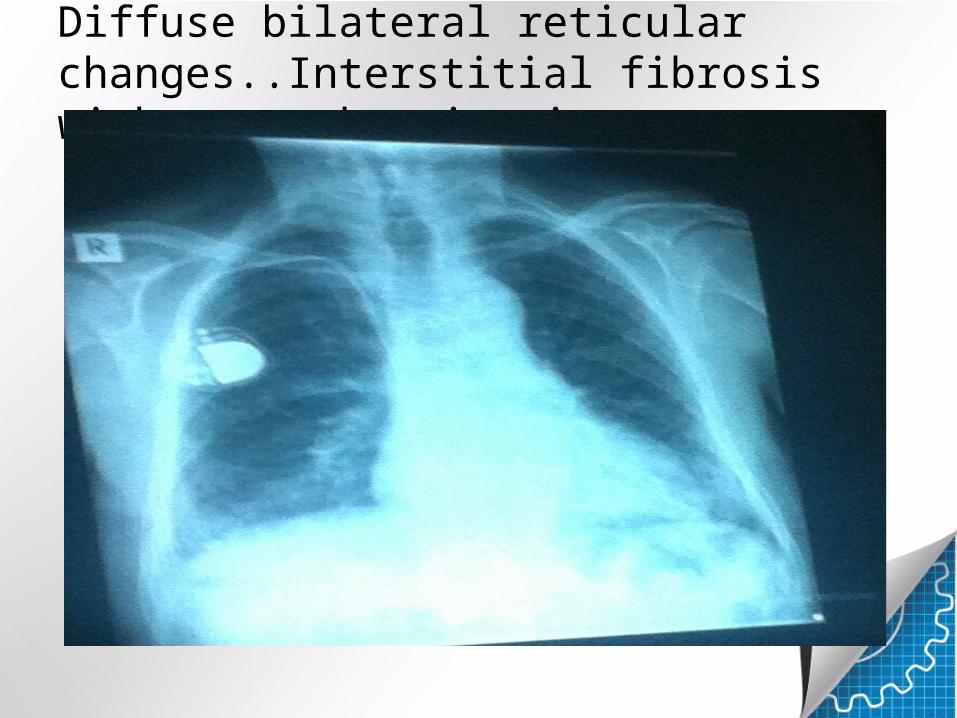
Diffuse bilateral reticular changes..Interstitial fibrosis with pacemaker in situ.
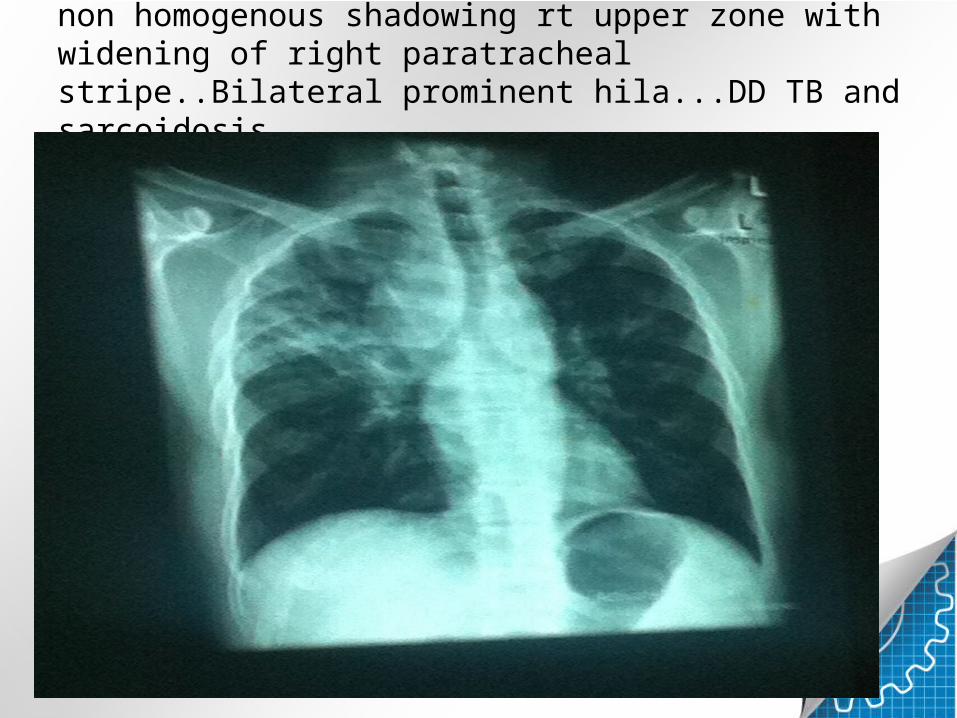
non homogenous shadowing rt upper zone with widening of right paratracheal stripe..Bilateral prominent hila...DD TB and sarcoidosis

Bilateral fibrocystic changes..left subcutaneous emphysema and left pneumothorax ..see it along medial border of left scapula...port a cath in situ......Cystic fibrosis with its complications

Port a cath• A catheter connects the
port to a vein. Under the skin, the port has a septum through which drugs can be injected and blood samples can be drawn many times, usually with less discomfort for the patient than a more typical "needle stick". Ports are used mostly to treat hematology and oncology patients
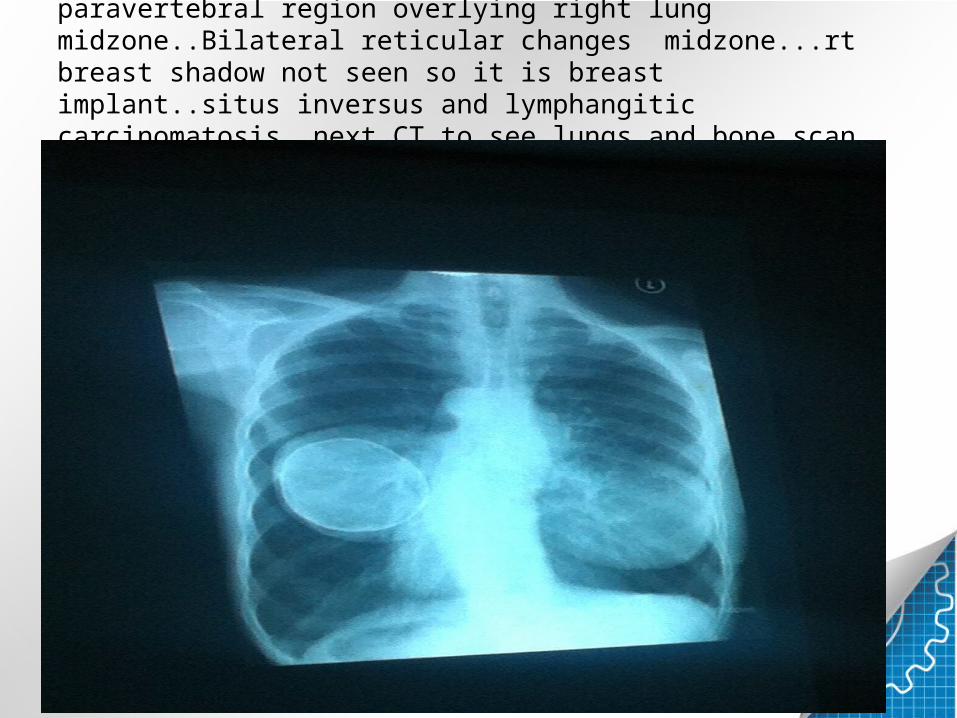
welldefined calcified rounded lesion in rt paravertebral region overlying right lung midzone..Bilateral reticular changes midzone...rt breast shadow not seen so it is breast implant..situs inversus and lymphangitic carcinomatosis..next CT to see lungs and bone scan for staging

Miliary mottling..DD tb ,mets,sarcoidosis

CTPA..saddle embolus ..Upto Which order branches are involved?

Consolidation/collapse rt upper lobe..NG tube in situ,,ETT malplaced

MLO and CC films..Architectural distortion and calcifications parallel to duct..no mass seen..plasma cell mastitis

Plasma cell mastitis pics from net..benign or malignant calcifications?distribution?
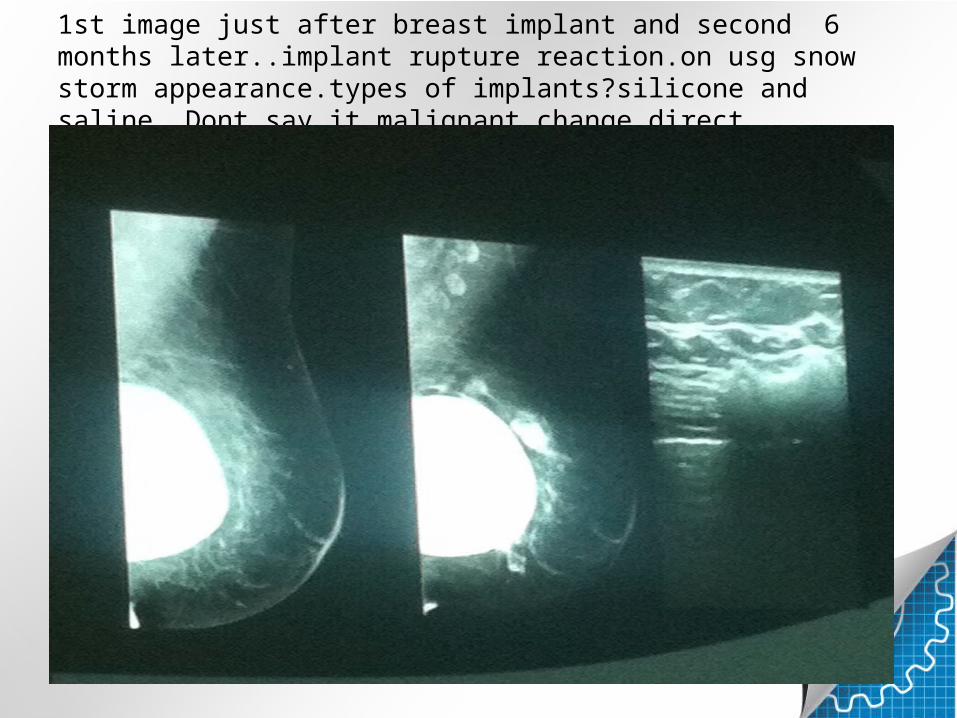
1st image just after breast implant and second 6 months later..implant rupture reaction.on usg snow storm appearance.types of implants?silicone and saline..Dont say it malignant change direct.


Presentation:Severe mitral valve regurgitation. Episodic, so-called "flash", pulmonary oedema.3 metallic butterfly-like clips (MitraClips) in the position of the mitral valve in a patient with cardiomegaly and defibrillating pacemaker.Case Discussion:MitraClip is a percutaneous system for treatment of patients with debilitating mitral regurgitation

Mitraclip

Rt aortic arch

CARDIOMEGALY WITH INCREASE PULMONARY VASCULARITY..asd CLOSURE DEVICE

ASD closure device

prominence of ascending aorta..Aortic stenosis further echo ..which mode?M mod e And CW mode,,continuous wave

Opaque left heithorax with erosion of left 1sr rib posteriorly...Pancoast tumor shifting medistinum to opposite side
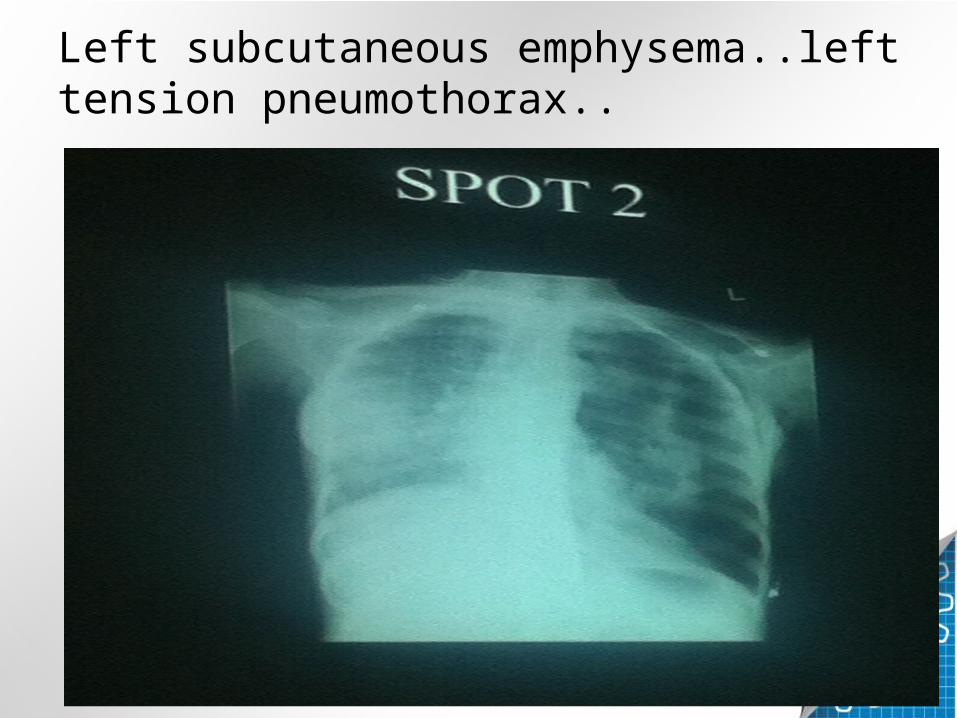
Left subcutaneous emphysema..left tension pneumothorax..

Hyperinflated left upper lobe..DD congenital lobar emphysema,foreign body,...In adults emphysematous changes or macleod syndrome..
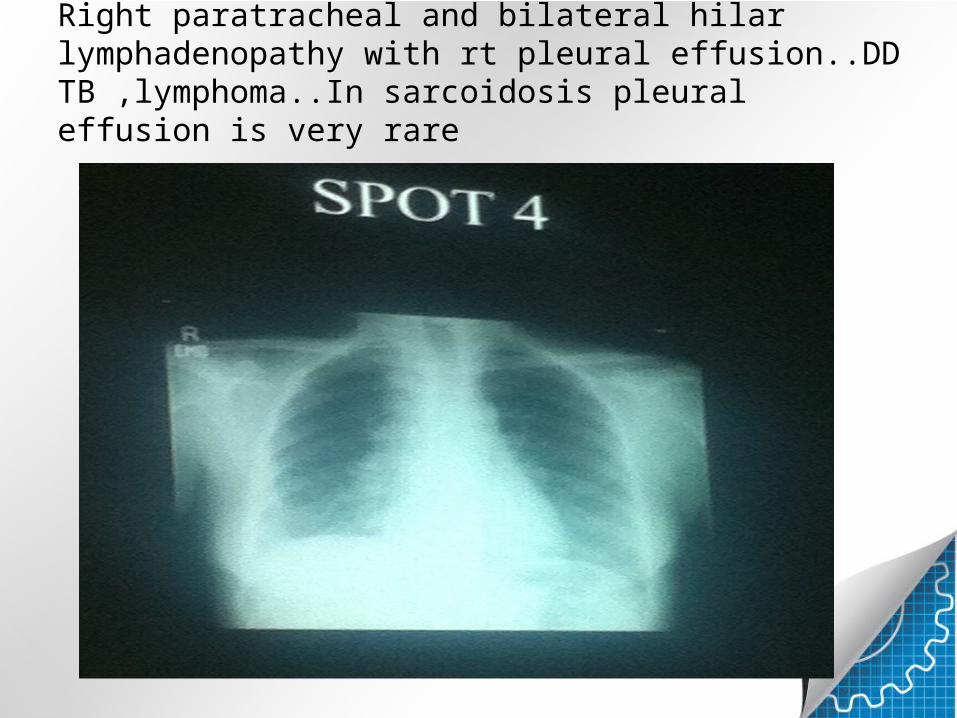
Right paratracheal and bilateral hilar lymphadenopathy with rt pleural effusion..DD TB ,lymphoma..In sarcoidosis pleural effusion is very rare

Bronchoceles..linear branching opacities radiating from rt hila

Bilateral reticular changes and calcified hilar lymphadenopathy..DD is sarcoidosis bcz mainly midzone involves..silicosis

TB cavity/necrotic neoplasm

Irregular soft tissue density mass at rt paerihilar region..next Ct showed mass in apical segment rt lower lobe

Bizarre shaped confluent opacities going towards hila with background emphysematous changes.....PMF..not mets they are well defined

Soft tissue opacity along rt cardiac border with foci of calcifications,,,AVM...complications of AVM?

Magnified view AVM embolized by coil
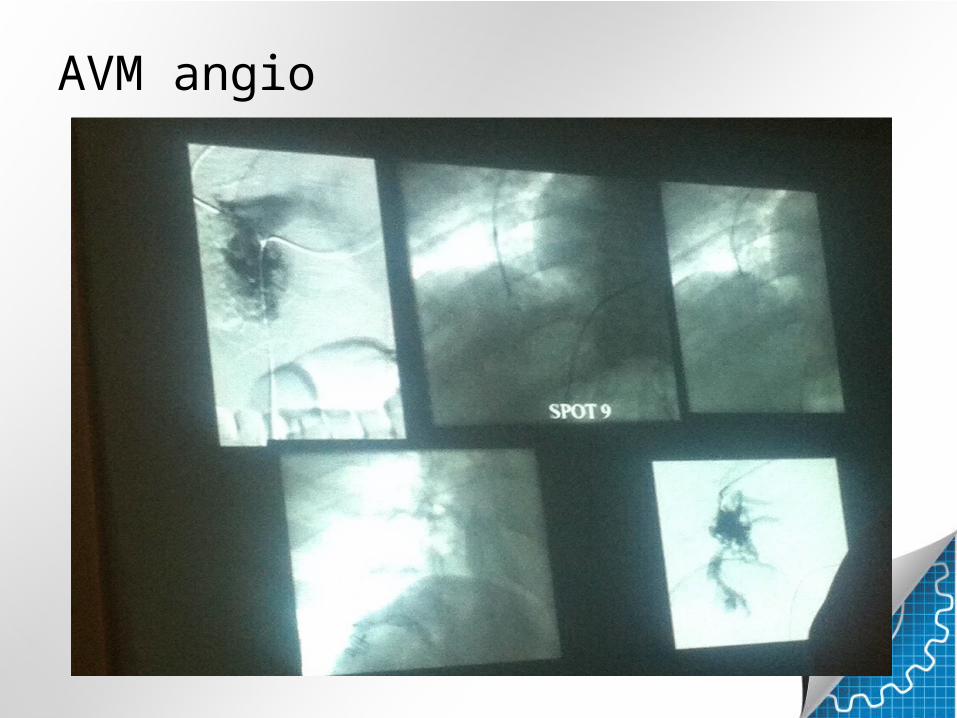
AVM angio
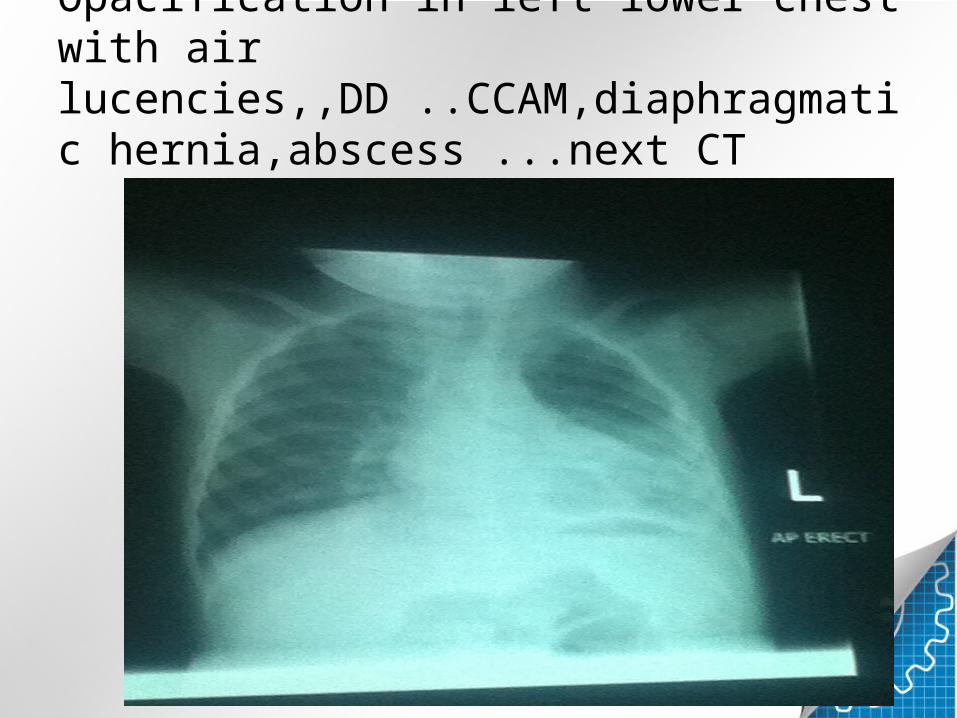
Opacification in left lower chest with air lucencies,,DD ..CCAM,diaphragmatic hernia,abscess ...next CT

CT showed multiple cystic spaces..CCAM

Opacification in right upper zone,rt heart border ,medial rt hemidiaphragm obscured ..with air bronchograms....,,Rt upper lobe,medial segment middle lobe,posterobasal segment lower lobe involved..multisegmental consoildation..pneumonia

Dissecting aortic aneurysmm.always tell its proximal and distal extent ,branches involved and which organ affected

Opacity with air crescent..aspergilloma right upper zone..cvp line and chest leads

miliary mottling,blunt left cp angle..tree in bud appearance apical region...DD is TB,mets...Not sarcoidosis it dont have random nodules
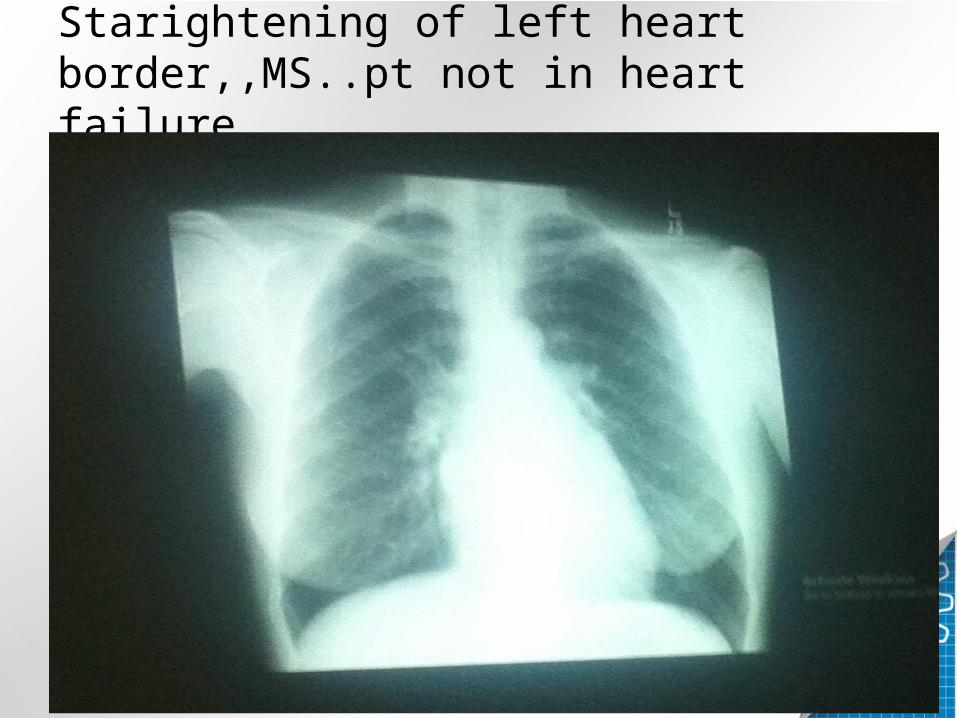
Starightening of left heart border,,MS..pt not in heart failure

Dilated aorta and peripheral calcification...aneurysm with left pleural effusion.Leaked AA

Enlarged tonsils and adnoids
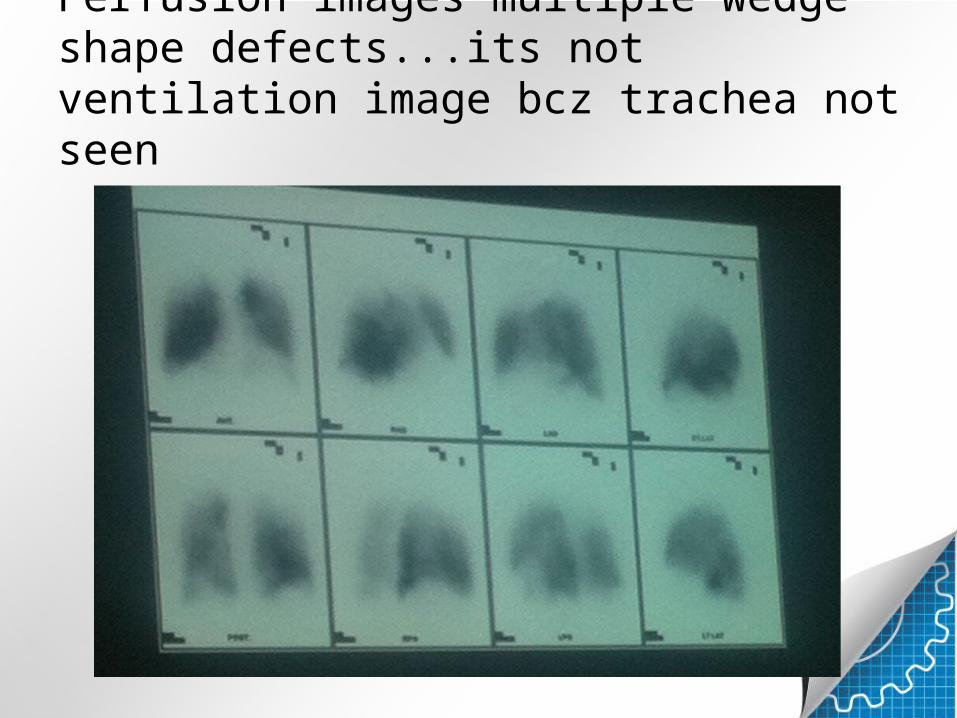
Perfusion images multiple wedge shape defects...its not ventilation image bcz trachea not seen
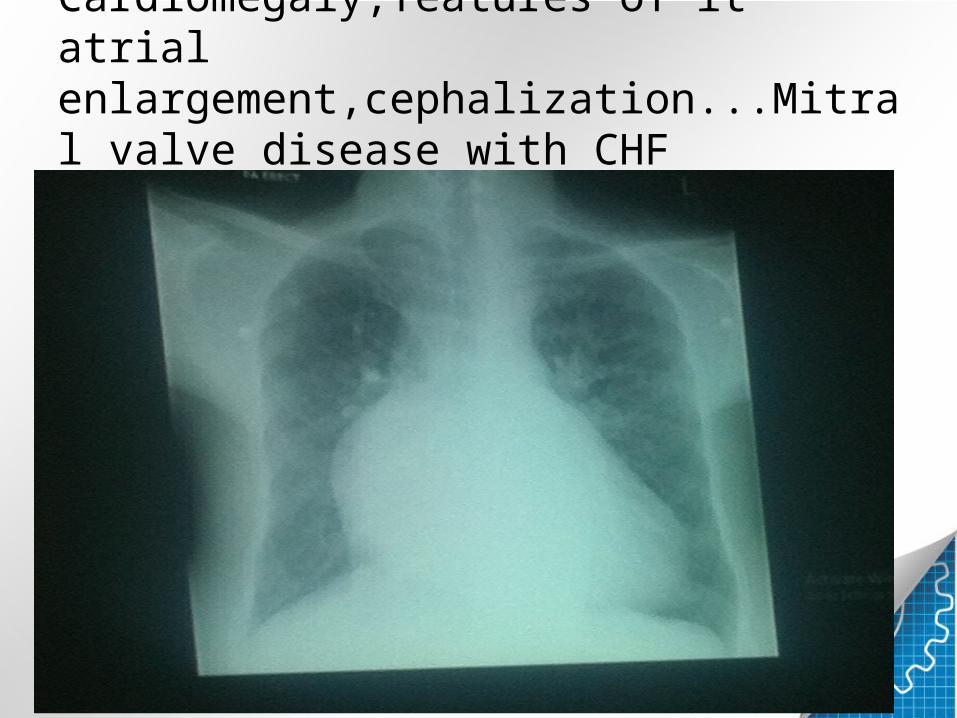
Cardiomegaly,features of lt atrial enlargement,cephalization...Mitral valve disease with CHF
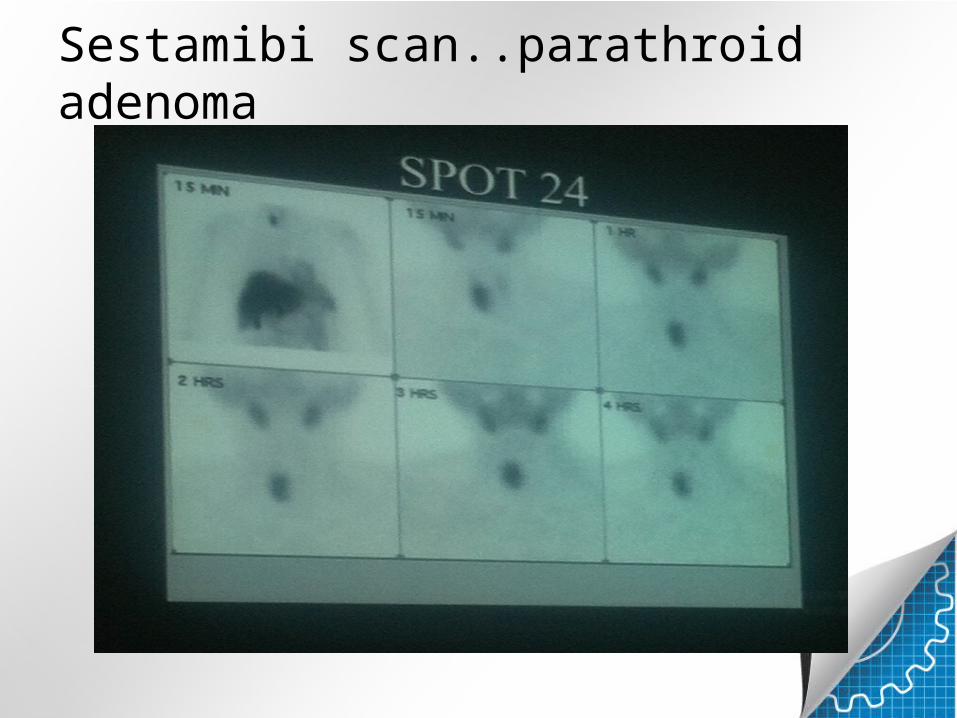
Sestamibi scan..parathroid adenoma
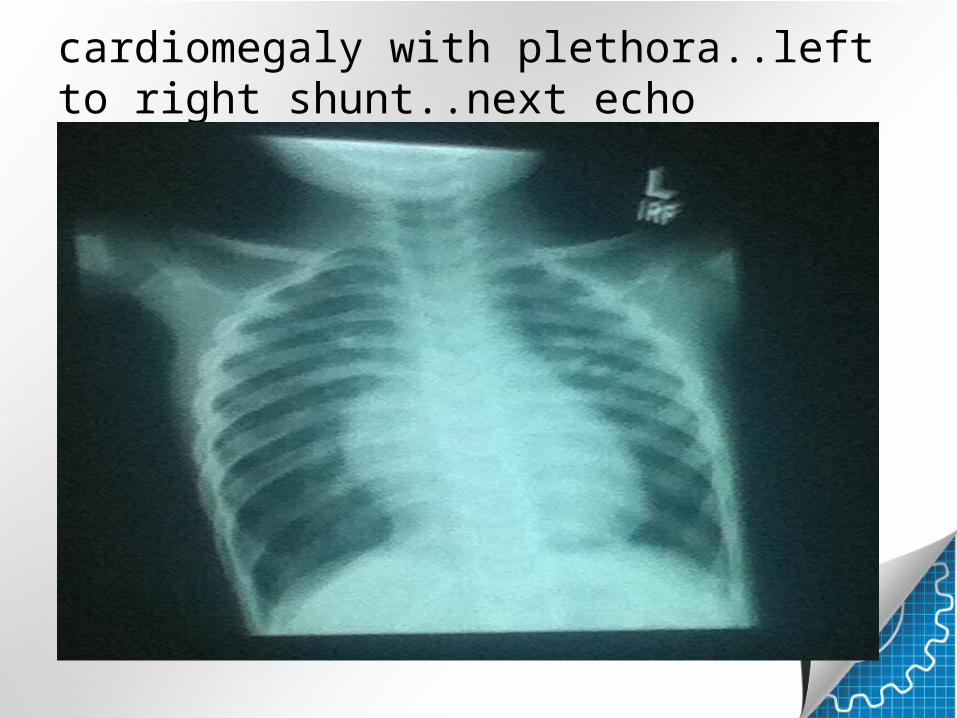
cardiomegaly with plethora..left to right shunt..next echo
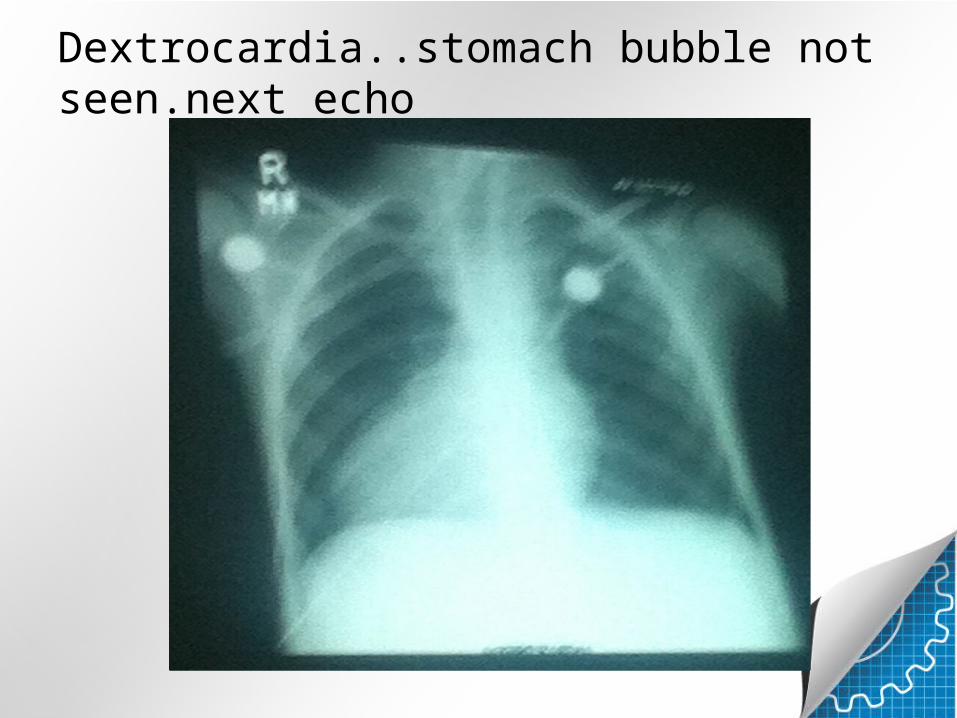
Dextrocardia..stomach bubble not seen.next echo

post op case..sternal wires .mediastinal drain,ETT,prosthetic mitral valve lying vertically..if it is in horizontal position then it will be
semilunar valves..cardiomegaly...