characterization of occult hepatitis b virus infection from blood
TRANSCRIPT

1
Characterization of Occult Hepatitis B virus Infection from Blood Donors in 1
China 2
3
Xin Zheng1†, Xianlin Ye
2†, Ling Zhang
1, Wenjing Wang
1, Lifang Shuai
3, Anqi Wang
1, 4
Jinfeng Zeng2, Daniel Candotti
4, Jean-Pierre Allain
5,1, Chengyao Li
1* 5
1 Department of Transfusion Medicine, Southern Medical University, Guangzhou, 6
China. 7
2 Shenzhen Blood Centre, Shenzhen, China 8
3 Guangzhou Military Centre of Disease Control, Guangzhou, China 9
4 National Health Service Blood & Transplant, Cambridge Blood Centre, Cambridge, 10
England 11
5 Department of Hematology, University of Cambridge, Cambridge, UK 12
13
† Both authors contributed equally to this work. 14
Potential conflict of interest: Nothing to report. 15
Running title: Characteristics of Chinese OBI 16
* Correspondence to Professor Chengyao Li, Department of Transfusion Medicine, 17
Southern Medical University, Guangzhou, China. Email: [email protected]; 18
Phone/Fax: +86 20 61648466; or Professor Jean-Pierre Allain, Department of 19
Hematology, University of Cambridge, Cambridge Blood Centre, Long Road, 20
Cambridge CB2 2PT, United Kingdom. Email: [email protected]; Phone: +44 1223 21
588044. Fax: +44 1223 588155. 22
23
Copyright © 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved.J. Clin. Microbiol. doi:10.1128/JCM.00145-11 JCM Accepts, published online ahead of print on 16 March 2011
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

2
Abstract word count: 199 1
Text word count (excluding title page, footnote page, abstract, reference, tables and 2
figures): 2,913 3
Inserts: 6 (containing 4 tables with notes and 2 figures with separate legends) 4
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

3
Abstract 1
Prevalence and characteristics of occult hepatitis B virus infection (OBI) of genotypes 2
B and C prevalent in China have not been extensively explored. Characterization of 3
OBIs from Chinese blood donors was based on clinical, serological, follow-up testing 4
and sequence analyses. Twenty-eight samples from 165,371 HBsAg negative plasmas 5
were confirmed HBsAg-/DNA+, of which 22 were classified as OBIs and six as 6
window period infections. OBI yield was 1:7,517 in blood donors, whose ages ranged 7
between 20 and 45 years (median 28). OBI donors had normal ALT levels and low 8
viral loads ranging between un-quantifiable and 178 IU/ml (median 14 IU/ml). 9
Sequences from 21 BCP/PC, five whole genomes and two additional pre-S/S from 10
OBIs were compared to genotypes B and C HBsAg+ reference strains. 86% (6/7) 11
OBIs were genotype C. Deletions, insertions, stop codons and substitutions were 12
detected in 15/21 (71%) core regulatory elements of OBIs. Critical mutations were 13
found in core of 5/5 OBIs in parallel with random substitutions in pre-S/S proteins 14
from 6/7 (86%) OBIs. Critical mutations in core regulatory elements and core proteins 15
might affect OBI genotype B and C strain replication. Few S protein substitutions 16
suggest a minor role of the host immune defences in OBI occurrence. 17
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

4
Introduction 1
2
Hepatitis B virus (HBV) infection is a major threat to human health worldwide, 3
especially to people living in developing countries. HBV carriers with detectable 4
surface antigen (HBsAg) are estimated over 300 millions globally, while there are 5
around 100 millions of HBV infected individuals in mainland China (12). HBV 6
serological testing is widely used in controlling the risk of HBV transmission among 7
people who donate blood or have health examination in China. However, some studies 8
recently showed HBV DNA at low levels detected in HBsAg negative individuals, 9
some of them transmitting HBV infections in recipients of blood transfusion (10). 10
Occult hepatitis B virus infection (OBI) is defined as the detection of HBV-DNA in 11
the serum or liver tissue of patients who test negative for HBsAg (15). Currently, the 12
testing for HBsAg is performed for screening of HBV infection in blood donors in 13
China but not nucleic acid testing (NAT). 14
Characterization of OBIs of genotypes A1, A2, D and E from European and African 15
blood donors was recently published in comparison with wild type HBV. The 16
mechanisms for generating OBIs were mainly related to either imperfect immune 17
control or to genetic viral defects and appeared largely genotype-dependent (1, 4). 18
However, analysis of OBIs of genotypes B and C prevalent in Southeast Asia and 19
China has not been extensively explored, particularly, in terms of molecular 20
characterization (14, 18). 21
This study provides new information regarding the prevalence and the molecular 22
analysis of OBIs of genotypes B and C from asymptomatic blood donors tested in 23
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

5
Shenzhen, China. 1
2
PATIENTS AND METHODS 3
4
Blood center and sample screening. Donor blood samples were collected by the 5
Shenzhen blood center between August 2003 and December 2009. Donor plasmas 6
were individually screened twice for HBsAg, anti-HCV and anti-HIV antibodies using 7
domestic and international commercial enzyme immunoassays (EIA), including 8
Xiamen Xinchuang HBsAg EIA (Xiamen Xinchuang Scientific Ltd, Xiamen, China) 9
and Abbott Auszyme HBsAg (Abbott Laboratories, Abbott Park, IL, USA), Sino-10
America Huamei anti-HCV EIA (Sino-America Huamei Biotechnology Ltd, Luoyang, 11
China) and Ortho anti-HCV EIA kit (Ortho-Clinical Diagnostics, Inc., Raritan, NJ, 12
USA), Zhuhai Lizhu anti-HIV EIA (Zhuhai Lizhu Biotechnology Ltd, Zhuhai, China) 13
and Melia anti-HIV-1 and 2 EIA (Organon Teknika, Boxtel, The Netherlands). The 14
level of alanine aminotransferase (ALT) was also measured for each blood sample 15
with ReflotronPlus assay (Roche Diagnostics, Mannheim, Germany). 16
17
Nucleic acid testing. Donor plasmas negative for HBsAg, anti-HCV and anti-HIV 18
were tested individually for nucleic acids of HBV, HCV and HIV-1 with Roche 19
COBAS ampliscreen assay (Roche), Kehua Real-time PCR assay (Kehua 20
Biotechnology Ltd., Shanghai, China) or Procleix Ultrio assay (Novartis, Emeryville, 21
CA, USA). 22
23
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

6
Serological testing. HBsAg reactivity was confirmed with a highly sensitive 1
chemiluminescent microplate immunoassay (CMIA), (ARCHITECT HBsAg assay, 2
Abbott laboratories) used according to manufacturer’s instructions. Anti-HBs, HBeAg, 3
anti-HBe and anti-HBc were detected with Kehua HBV EIAs (Kehua). Anti-HBs was 4
quantified in IU/L with anti-HBs electrochemiluminescence immunoassay (Roche). 5
6
HBV DNA quantification, amplification and sequencing. HBV DNA load was 7
determined by qPCR as described (4, 21). Viral DNA was extracted from 0.4 to 1.0mL 8
of plasma (HighPure, Roche). HBV basic core promoter/precore region (BCP/PC 9
nucleotide (nt) 1679-1973), whole genome minus 53bp (nt 1804-1856) in the precore 10
region (3162bp), pre-S/S region (nt 2802-1020) were amplified using the nested-PCRs 11
sequentially to obtain either whole genome or fragments of HBV genome (5, 21). 12
Whole genome amplicons were cloned in pMD20-T vector (TaKaRa Biotechnology 13
Ltd., Dalian, China) and fragments of pre-S/S were cloned in the original TA cloning 14
kit, respectively. Amplified BCP/PC products and 2-6 clones were sent for sequencing 15
to Shanghai Invitrogen Co Ltd (Guangzhou, China). 16
The 2nd
WHO International Standard for HBV DNA (National Institute for 17
Biological Standards and Control, Potters Bar, UK) containing 5Х105 IU per vial 18
(NIBSC code: 97/750) was kindly provided by Mr. Qingtao Song (Xiamen Xinchuang) 19
for quantification of HBV DNA. 20
21
Occult HBV DNA analyses. Alignment and phylogenetic analyses were performed 22
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

7
on a consensus sequence from each OBI plasma sample using the neighbor-joining 1
(NJ) method and pre-S/S (1201bp) sequences (4). Control HBV wild type sequences 2
were mostly Chinese strains obtained from HBsAg+ strains selected in GeneBank 3
database. Accession numbers for genotype B were: AB205119, AB287329, AP011084, 4
AY167089, D00300, DQ448620, DQ448625, DQ993703, DQ993709, EU305548, 5
EU306701, EU306705, EU306706, FJ386582, FJ386642 and FJ787444; for genotype 6
C: AP011098, DQ089793, DQ478899, DQ478900, DQ993691, DQ993692, 7
DQ993693, EU306720, EU306721, EU916238, EU916240, EU939540, EU939652, 8
FJ386575, FJ386576, FJ386627, FJ386685, FJ562218, FJ562232, FJ562244, X04615, 9
X75656 and X75665. 10
Diversity was defined as the mean value for pair-wise difference of sequence 11
between OBI and HBV wild-type consensus sequences within the same group, 12
calculated as the number of nucleotide or amino acid differences between two 13
individual sequences (4). 14
15
Statistical analyses. SPSS software (version 13.0) was used for statistical analyses. 16
Categorical variables were compared by using Fisher’s exact test and, for continuous 17
variables, the non-parametric Mann–Whitney test. 18
19
RESULTS 20
21
Sample classification and characterization. A total of 165,371 donor plasma 22
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

8
samples from Shenzhen Blood Center were screened as HBsAg negative with one 1
international and one domestic commercial EIA kits. Thirty-three plasmas were 2
detected as HBV DNA+ by individual sample NAT. Twenty-eight of 33 plasmas were 3
confirmed as HBsAg-/DNA+ by the CMIA for HBsAg and nested PCR for BCP/PC. 4
20/33 blood donors with index samples HBsAg-/DNA+ were recalled for follow-up 5
testing of HBV infection markers 2 to 221 days after index donation. 6
A total of 22/28 index samples with HBsAg-/DNA+ were classified as OBIs (Table 7
1). Sero-marker negative SZ2 and SZ9 donors tested positive for HBV DNA by 8
Roche PCR-ELISA and nested PCR in follow-up samples and were classified as 9
seronegative or primary OBIs (1, 15). Donor SZ25 with negative sero-markers were 10
found reactive for both anti-HBs and anti-HBe 25 days post index and was classified 11
as OBI. The other 19 samples were confirmed as OBIs by serological markers or 12
follow-up testing. SZ90 and SZ99 were high-level anti-HBs+ only (>428IU/L) and 13
were HBV vaccinated six months and three years prior to blood donation, respectively. 14
Four index samples (SZ14, SZ17, SZ23 and SZ200) with no serological markers 15
and a viral load >200 IU/ml were confirmed HBV window period infections 16
following seroconversion to HBsAg or HBeAg (1st-WP) (Table 2). Two samples (SZ4 17
and SZ12) carrying anti-HBe+ and anti-HBc+ seroconverted to HBsAg and were 18
classified as secondary window period infections (2nd
-WP). Sample SZ3 with both 19
anti-HBe+ and anti-HBc+ was initially classified as HBsAg- by two EIAs, but was 20
weakly reactive (0.13IU/ml) by CMIA and was re-classified as chronic infection. 21
Sample SZ24 being HBsAg- but HBeAg+ was considered chronic infection. Samples 22
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

9
SZ13, SZ20 and SZ21 carrying either anti-HBs+ or anti-HBc+ but HBV DNA not-1
confirmed by BCP/PC nested PCR were considered false positive. 2
The prevalence of confirmed OBI was 1:7,517 (22/165,371) in Shenzhen blood 3
donors (Table 1). All 22 cases were between 20 and 45 years old (median 28 years) 4
and had normal ALT level (<40IU/L). Seventeen samples (77.3%) were anti-HBc+, 7 5
(31.8%) anti-HBs+ (5 with anti-HBc) and 5 (22.7%) anti-HBe+ (all with anti-HBc), 6
and three (13.6%) had all sero-markers negative at initial testing, respectively. Viral 7
load of OBIs ranged between un-quantifiable (considered < 1IU/ml) and 178.4IU/ml 8
(median 14.4IU/ml). There was no significant difference in viral load between anti-9
HBs or anti-HBe positive and negative OBIs (p=0.798 or p=0.903). 10
Phylogenetic analysis of five full-length genome (SZ5, SZ6, SZ7, SZ16 and SZ19) 11
and two additional pre-S/S (SZ26 and SZ92) sequences identified one (14.3%) 12
genotype B (OBIB) and six (85.7%) genotype C (OBIC) OBIs (Table 1). 13
Analyses of regulatory elements of occult HBV sequences. The consensus 14
nucleotide sequences of regulatory elements from OBIB or OBIC were compared to 15
consensus sequences from 16 genotype B or 23 genotype C HBsAg+ strains, 16
respectively. Promoters (pre-S1, pre-S2/S, core and X proteins), regulatory sequences 17
(core upstream regulatory sequence, CURS; direct repeat sequences, DR), enhancers 18
(ENH) and negative regulatory element (NRE) were analyzed. DR1, DR2 and NRE 19
were conserved. Significantly higher mean diversity was observed in SP and ENH 20
regulatory elements from OBIC (p≤0.004-0.0001) but not in CURS, BCP and XP 21
sequences between OBIC and HBsAg+ strains (p=0.025-0.846) (Table 3). 22
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

10
Mutations were observed in CURS and BCP regions in 71.4% (15/21) OBIs, but 1
less frequently in HBsAg+ control sequences (Table 4). 13/21 (61.9%) OBIs 2
presented CURS (indicate first and last nt) mutations, deletion, insertion, single or 3
multiple substitutions. OBIs SZ22 and SZ92 had one nucleotide deletion at the same 4
nt 1689 site; OBI SZ9 had an insertion of “C” at nt 1716. A total of 11 mutations were 5
detected in the CURS region of 11 OBIs, and were present in several strains at nt 6
1727, 1730, 1703, 1719 and 1726. In the BCP region, mutations were detected at six 7
sites in 8/21 (38.1%) OBIs, including G1742A (SZ5 and SZ15), A1752G (SZ5, SZ15, 8
SZ16 and SZ18), A1762T/G1764A (SZ6), G1799C or C1799G (SZ5, SZ16, SZ19 and 9
SZ92) and A1846T (SZ91). 10
In the epsilon domain eight OBI strains had mutations but only T1893A (SZ99) had 11
a possible structural impact on the bulge formation. 12
13
Analyses of occult HBV core, X, envelope and polymerase proteins. Seven OBI 14
amino acid (aa) sequences were aligned with the genotype B or genotype C HBsAg+ 15
control strains. The mean number of aa substitutions in pre-C/C, pre-S/S and Pol 16
regions from OBIC was higher than in wild type strains (P≤0.013-0.0001) (Table 3). 17
In the pre-core region of five OBIs, SZ7 had a V17F mutation, SZ16 had a stop 18
codon at aa 28. Critical mutations in the core region of all five OBIs associated with B 19
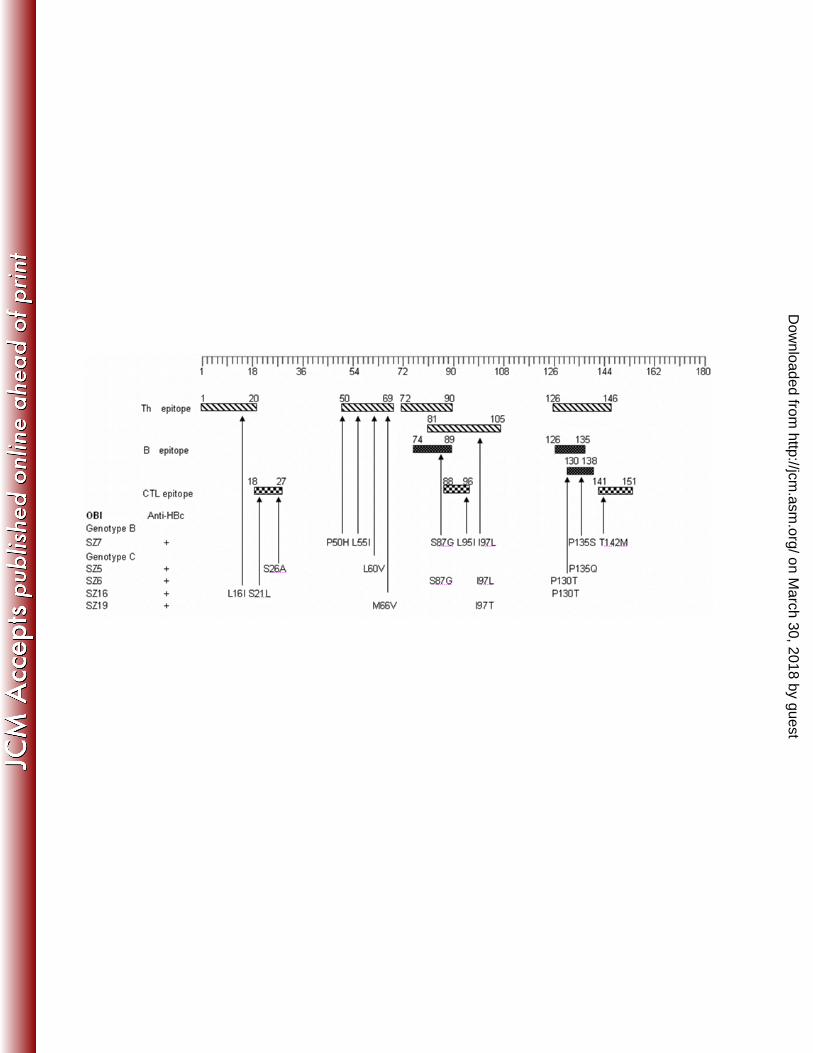
cell, T helper (Th) cell and cytotoxic T lymphocyte (CTL) epitopes might 20
theoretically influence immunological HBV epitope recognition (Fig. 1) (3, 16). The 21
common mutations I97L/T (SZ7, SZ6 and SZ19), P130T/S (SZ6 and SZ16), S87G 22
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

11
(SZ7 and SZ6), P135S/Q (SZ7 and SZ5) were found in 5/5 (100%) core regions of 1
OBIs. Specific substitutions L16I, S21L, S26A, P50H, L55I, L60V, M66V, L95I or 2
T142M were present in the core regions of all sequenced OBIs but not of WP or 3
chronic infection wild type HBV strains. 4
In the X region, a mutation of A1762T in BCP led to a substitution of K130M in 5
SZ6. Mutation V88A/N was detected in SZ6 and SZ19, and V5L and Q87G in SZ19. 6
One nucleotide deletion at nt 1689 and insertion at nt 1716 in the CURS regions 7
caused X protein ORF shift and abberant translation in OBIs SZ22, SZ92 and SZ9. 8
Mutations in the pre-S/S region of OBIs were examined with regard to the known 9
epitopes of CTL, Th and B cells and the major hydrophilic region (MHR) and “a” 10
determinant (Fig. 2) (4, 7, 14). OBI MHR and “a” regions were relatively conserved 11
and no hotspot mutations were found. Few mutations occurred at sites of subtype 12
conversion of adw and adr corresponding to genotype B and C. Substitutions sI110L 13
and sI126T were found in samples SZ7 (OBIB) and SZ5 and SZ6 (OBIC) and A159V 14
in SZ7 was presumably related to subtype (Fig. 2D). SZ5 presented substitutions 15
sT118M and sW165R in MHR. Frequent substitutions were observed in OBI S 16
protein aa 2-5 in 4/7 (57%) (SZ7, SZ16, SZ19, SZ26), middle position aa 88-104 17
within CTL epitope clusters 9 and 10 in 4/7 (57%) OBIs (Fig. 2C), and C-terminus aa 18
210-225 within the CTL epitope clusters 13 and 14 in 6/7 (85.7%) OBIs (Figure 2D). 19
Similarly, frequent substitutions were found in pre-S2 protein at initial position aa 5-9 20
within CTL epitope cluster 2 overlapping B-cell epitope cluster 8 from 5/7 (71.4%) 21
OBIs (Figure 2B). SZ7 and SZ5 had a pre-S2 mutated start codon. SZ92 had two 22
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

12
mutations (pre-sI84V and pre-sA90V) in pre-S1 that were also found in SZ7, SZ5, 1
SZ6 and SZ16 (Fig. 1A). 2
The mass random substitutions in polymerase regions of OBIC were observed at the 3
frequency of 11-47 (Table 3), and no well documented hotspot mutations were found 4
in YMDD and FLLA motifs. 5
6
DISCUSSION 7
8
The prevalence of HBsAg in the Chinese population has declined to 7.2% due to 9
nationwide HBV vaccination, but approximately 100 millions of HBV chronically 10
infected individuals live in China (12). The new issue of occult HBV infection 11
uncovered by NAT has become a concern in transfusion and in patients although little 12
is known of OBI in China where genotype B and genotype C are dominant (12, 18). 13
The epidemiology of HBV infection in Shenzhen blood donor population is 14
somewhat reflective of that in China as a whole, except for a lower prevalence of 15
HBsAg (12). The prevalence of OBIs in Shenzhen was therefore expected lower than 16
average in China, but the frequency of 1:7,517 was similar to those reported (median 17
1:9,819 and 1:8,209) in European or South African blood donors (1, 4). This is 18
surprising considering a lower prevalence in Europe and similar in South Africa. In 19
Hong Kong, close geographically from Shenzhen, 80 OBI cases were identified in 20
357,440 blood donations or 1:4,468 using the Novartis Ultrio screening method in 21
individual donations. This apparently higher frequency might be related to a higher 22
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
13
sensitivity of the screening method (6). 1
The ratio of male and female OBI donors was 3.4:1 (17:5). The 28 years median 2
age of OBI donors reflected the blood donor population in Shenzhen, but was 3
considerably younger than European OBI of genotype A2 or D and genotype A1 4
South African donors (1, 4). As elsewhere, OBI donors had normal ALT, viral load 5
below 200 IU/ml (median 14.4IU/ml) and carried anti-HBc+ (77.3%) with anti-HBs 6
or anti-HBs+ only (9%). Compared to European data, associated anti-HBc and anti-7
HBs appears less frequent in Shenzhen’s donors but primary OBI more frequent (4). 8
The availability of follow-up samples from 20/30 samples was of considerable help 9
to insure the classification of samples and inform the donors, separating OBIs from 10
WP and doubtful chronic infections and, within OBIs, distinguishing primary OBIs 11
from other types (Tables 1 and 2). Among the latter, follow-up data showed the 12
relative stability of HBV DNA detectability and load (Table 1). 13
Genomic amplification was relatively unsuccessful (12/30 for pre-S/S) in relation 14
with low, often not quantifiable, viral load. Therefore, genotype was determined in 15
only 27% of OBIs. 16
Mutations in core regulatory elements involved in viral replication were described 17
previously (8, 13). Compared to HBsAg+ strains, deletions, insertions and 18
substitutions at single or multiple sites were observed in OBI CURS and BCP (15/21) 19
(Table 4). Mutations A1752G and A1762T (5 OBIs) were found in TATA box-like 20
regulatory elements (TA1-4). Mutation of dual A1762T/G1764A was only found in 21
one OBIC (SZ6) a lower frequency than reported in OBIE (44.4%) (21). Synthesis of 22
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

14
both pregenomic and 5’-terminally extended precore RNA are controlled by the core 1
regulatory elements including ENH2, CURS and BCP, which, considering the 2
overlapping arrangement of ORFs, every single mutation can influence more than one 3
function of the corresponding nucleotide sequence during viral RNA transcription. 4
Mutations in core regulatory elements of OBIs decreasing or abolishing viral 5
replication, RNA transcription or production of pre-C/C and secreted HBe, might be 6
responsible for low viral load in OBIB and OBIC. 7
The mutations of core protein in HBV infection have been reported associated with 8
not only severe liver disease but also low secretion of HBV virions and immune 9
escape epitopes at Th and CTL levels (3, 11, 16). Mutations of OBI core proteins (Fig. 10
1) showing aa substitutions in the CTL epitope clusters 18-27, 88-96 and 141-151 11
might constitute escape epitopes and contribute to the persistence of HBV infection 12
despite reducing viral fitness (16). The CTL epitope 18-27 is restricted by HLA-A2 13
but the potential impact of substitutions at position 21 and 26 is not known (2). 14
Similarly, CTL epitopes 88-96 and 141-151 are restricted by HLA-A11 and HLA-15
Aw68, respectively (9). Substitution L60V (SZ5) was previously described as related 16
to low-level production of HBV virions [16]. Mutations of I97L/T and P130T 17
identified in 60% (3/5) and 40% (2/5) OBIs. I97L was reported responsible for 18
secretion of immature HBV core, but this phenomenon could be offset by P130T 19
mutation (18, 19). 20
The function of X protein could be influenced by the deletion, insertion and 21
substitutions of core regulatory elements (Table 4), because the X gene overlaps with 22
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

15
the enhancer and core promoter regions. Two important domains between aa 52-65 1
and 88-154 of HBx have enhancing effect on HBV transcription and replication (17). 2
At the protein level, substitution K130M caused by mutation A1762T in BCP (SZ6) 3
was observed; other substitutions V5L, Q87G and V88A/N were involved in 40% (2/5) 4
OBIs (SZ19 and SZ6), V88A/N and K130M were located in the functional domains 5
of the X protein, but their specific effect on HBV replication is not identified. 6
In the present study, the diversity of Pre-S1 and Pre-S2 at the nucleotide and protein 7
levels of OBIs genotype B and C was significantly higher than in control HBsAg+ 8
strains (p<0.0001) (Table 3). However, most mutations appeared random substitutions. 9
In contrast, the MHR of OBIB and OBIC was essentially wild type, particularly in 10
loops 3 and 4 (Fig.2D). This pattern does not suggest a major impact of immune 11
selection in genotype B and C OBIs although a small number of cases were examined 12
in contrast with findings in European genotype A2 and D but rather similar to findings 13
in African genotype A1 or E OBIs (1, 4). 14
The relatively high frequency of critical mutations in the pre-core/core region 15
potentially affecting viral replication and the virtual absence of mutations affecting 16
the pre-S and S proteins suggest that the main mechanism leading to OBI in Shenzhen 17
might rather be poor viral replication than ineffective immune control. 18
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

16
Acknowledgements 1
This work was supported by the National Basic Research Program of China (973 2
program No. 2007CB512901 and 2010CB530204) and Guangdong Research 3
Initiating Funding for talent from overseas. 4
We thank the staffs of Shenzhen Blood Center and Mr. Qingtao Song for their 5
contribution to the study. 6
7
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

17
References 1
1. Allain, J. P., D. Belkhiri, M. Vermeulen, R. Crookes, R. Cable, A. Amiri, R. 2
Reddy, A. Bird, D. Candotti. 2009. Characterization of occult hepatitis B virus 3
strains in South African blood donors. Hepatology 49:1868-76. 4
2. Bertoletti, A., A. Costanzo, F. V. Chisari, M. Levrero, M. Artini, A. Sette, A. 5
Penna, T. Giuberti, F. Fiaccadori, C. Ferrari. 1994. Cytotoxic T lymphocyte 6
response to a wild type hepatitis B virus epitope in patients chronically infected 7
by variant viruses carrying substitutions within the epitope. J. Exp. Med. 8
180:933-43. 9
3. Bozkaya, H., B. Ayola, A. S. Lok. 1996. High rate of mutations in the hepatitis B 10
core gene during the immune clearance phase of chronic hepatitis B virus 11
infection. Hepatology 24:32–37. 12
4. Candotti, D., P. Grabarczyk, P. Ghiazza, R. Roig, N. Casamitjana, P. 13
Iudicone, M. Schmidt, A. Bird, R. Crookes, E. Brojer, M. Miceli, A. Amiri, C. 14
Li, J. P. Allain. 2008. Characterization of occult hepatitis B virus from blood 15
donors carrying genotype A2 or genotype D strains. J. Hepatol. 49:537-47. 16
5. Candotti, D., O. Opare-Sem, H. Rezvan, F. Sarkodie, J. P. Allain. 2006. 17
Molecular and serological characterization of hepatitis B virus in deferred 18
Ghanaian blood donors with and without elevated alanine amino transferase. J. 19
Viral Hepatitis 13: 715-24. 20
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

18
6. Choi, W. C., D. Candotti, C. K. Chan, E. Chua, J. P. Allain, C. K. Lin. 2009. 1
Window period and occult HBV infection among blood donor population in 2
Hong Kong. Abstract p.114. ISBT Congress, Nagoya. 3
7. Desmond, C. P., A. Bartholomeusz, S. Gaudieri, P. A. Revill, S. R. Lewin. 4
2008. A systematic review of T-cell epitopes in hepatitis B virus: identification, 5
genotypic variation and relevance to antiviral therapeutics. Antivir. Ther. 13:161-6
75. 7
8. Guarnieri, M., K. H. Kim, G. Bang, J. Li, Y. Zhou, X. Tang, J. Wands, S. 8
Tong. 2006. Point mutations upstream of hepatitis B virus core gene affect DNA 9
replication at the step of core protein expression. J. Virol. 80:587-95. 10
9. Khakoo, S.I., R. Ling, I. Scott, A. I. Dodi, T. J. Harrison, G. M. Dusheiko, J. 11
A. Madrigal. 2000. Cytotoxic T lymphocyte responses and CTL epitope escape 12
mutation in HBsAg, anti-HBe positive individuals. Gut 47:137-43. 13
10. Kleinman, S. H., N. Lelie, M. P. Busch. 2009. Infectivity of human 14
immunodeficiency virus-1, hepatitis C virus, and hepatitis B virus and risk of 15
transmission by transfusion. Transfusion 49:2454-89. 16
11. Le Pogam, S., T. T. Yuan, G. K. Sahu, S. Chatterjee, C. Shih. 2000. Low-level 17
secretion of human hepatitis B virus virions caused by two independent, 18
naturally occurring mutations (P5T and L60V) in the capsid protein. J. Virol. 19
74:9099-105. 20
12. Liang, X., S. Bi , W. Yang, L. Wang, G. Cui, F. Cui, Y. Zhang, J. Liu, X. Gong, 21
Y. Chen, F. Wang, H. Zheng, F. Wang, J. Guo, Z. Jia, J. Ma, H. Wang, H. 22
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
19
Luo, L. Li, S. Jin, S. C. Hadler, Y. Wang. 2009. Epidemiological serosurvey of 1
hepatitis B in China--declining HBV prevalence due to hepatitis B vaccination. 2
Vaccine 27:6550-7. 3
13. Liu, C. J., Y. M. Jeng, C. L. Chen, H. R. Cheng, P.J. Chen, T. C. Chen, C. H. 4
Liu, M. Y. Lai, D. S. Chen, J. H. Kao. 2009. Hepatitis B virus basal core 5
promoter mutation and DNA load correlate with expression of hepatitis B core 6
antigen in patients with chronic hepatitis B. J. Infect. Dis.199:742-9. 7
14. Mu, S. C., Y. M. Lin, G. M. Jow, B. F. Chen. 2009. Occult hepatitis B virus 8
infection in hepatitis B vaccinated children in Taiwan. J. Hepatol. 50:264-72. 9
15. Raimondo, G., J. P. Allain, M. R. Brunetto, M. A. Buendia, D. S. Chen, M. 10
Colombo, A. Craxì, F. Donato, C. Ferrari, G. B. Gaeta, W. H. Gerlich, M. 11
Levrero, S. Locarnini, T. Michalak, M. U. Mondelli, J. M. Pawlotsky, T. 12
Pollicino, D. Prati, M. Puoti, D. Samuel, D. Shouval, A. Smedile, G. 13
Squadrito, C. Trépo, E. Villa, H. Will, A. R. Zanetti, F. Zoulim. 2008. 14
Statements from the Taormina expert meeting on occult hepatitis B virus 15
infection. J. Hepatol. 49:652-7. 16
16. Sendi, H., M. Mehrab-Mohseni, S. Shahraz, H. Norder, S. M. Alavian, B. 17
Noorinayer, M. R. Zali, P. Pumpens, H. L. Bonkovsky, L. O. Magnius. 2009. 18
CTL escape mutations of core protein are more frequent in strains of HBeAg 19
negative patients with low levels of HBV DNA. J. Clin. Virol. 46:259-64. 20
17. Tang, H., L. Delgermaa, F. Huang, N. Oishi, L. Liu, F. He, L. Zhao, S. 21
Murakami. 2005. The transcriptional transactivation function of HBx protein is 22
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

20
important for its augmentation role in hepatitis B virus replication. J. Virol. 1
79:5548-56. 2
18. Yuan, Q., S. H. Ou, C. R. Chen, S. X. Ge , B. Pei, Q. R. Chen, Q. Yan, Y. C. 3
Lin, H. Y. Ni, C. H. Huang, A. E. Yeo, J. W. Shih, J. Zhang, N. S. Xia. 2010. 4
Molecular Characteristics of Occult Hepatitis B Virus from Blood Donors in the 5
southeast China. J. Clin. Microbiol. 48:357-62. 6
19. Yuan, T. T., C. Shih. 2000. A frequent, naturally occurring mutation (P130T) of 7
human hepatitis B virus core antigen is compensatory for immature secretion 8
phenotype of another frequent variant (I97L). J. Virol. 74:4929-32. 9
20. Yuan, T. T., P. C. Tai, C. Shih. 1999. Subtype-independent immature secretion 10
and subtype-dependent replication deficiency of a highly frequent, naturally 11
occurring mutation of human hepatitis B virus core antigen. J. Virol. 73:10122-8. 12
21. Zahn, A., C. Li, K. Danso, D. Candotti, S. Owusu-Ofori, J. Temple, J. P. 13
Allain. 2008. Molecular characterization of occult hepatitis B virus in genotype 14
E-infected subjects. J. Gen. Virol. 89:409-18. 15
16
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

21
TABLE 1. Characterization of OBIs from China Shenzhen blood donors 1
A
ge ALT Serological Test VL
(IU/mSamples Gender HBsAg
Anti-
HBc
Anti-
HBs HBeAg Anti-HBe IU/ml
Genome
(Genotype)
SZ2 M 26 12 0.03 Neg Neg Neg Neg <1 BCP/PC
+2d Neg Neg Neg Neg Neg Pos
SZ9 M 33 5 0.02 Neg Neg Neg Neg <1 BCP/PC
+2d Neg Neg Neg Neg Neg Pos
SZ25 M 22 8 0.01 Neg Nega Neg Neg
a 15.2 BCP/PC
+25d Neg Neg Pos Neg Pos Pos
SZ1 M 30 31 0.03 Pos Neg Neg Neg 32.5 BCP/PC
+17d Neg Pos Neg Neg Neg 18.2
+45d Neg Pos Neg Neg Neg 27.3
+64d Neg Pos Neg Neg Neg 30.2
SZ5 M 37 8 0.02 Pos Neg Neg Pos 13.6 Whole (C)
+18d Neg Pos Neg Neg Pos ND
+33d Neg Pos Neg Neg Pos 6.8
+53d Neg Pos Neg Neg Pos ND
SZ6 F 30 10 0.04 Pos Nega Neg Neg 23.1 Whole(C)
+14d Neg Pos Neg Neg Neg 95
+22d Neg Pos Neg Neg Neg 48.6
+41d Neg Pos Pos Neg Neg 29.1
SZ7 F 37 11 0.03 Pos Neg Neg Neg 57.9 Whole (B)
+21d Neg Pos Neg Neg Pos 50
+47d Neg Pos Neg Neg Pos 27.9
+61d Neg Pos Neg Neg Pos 41.3
SZ10 M 24 18 0.02 Pos 44.39 Neg Neg <1 BCP/PC
SZ11 M 25 11 0.02 Pos >1000 Neg Neg 26.8 BCP/PC
+7d Neg Pos Pos Neg Neg 7.5
+15d Neg Pos Pos Neg Neg ND
+25d Neg Pos Pos Neg Neg ND
SZ15 M 29 15 0.03 Pos Nega Neg Neg
a 19.5 BCP/PC
+15d Neg Pos Neg Neg Neg ND
+930d Neg Pos Neg Neg Pos 7.5
+955d Neg Pos Pos Neg Pos ND
SZ16 M 22 30 0.02 Pos 73.36 Neg Nega 28.9 Whole (C)
+162d Neg Pos Pos Neg Neg ND
+464d Neg Neg Pos Neg Pos Pos
SZ18 M 20 8 0.01 Pos Neg Neg Neg <1 BCP/PC
SZ19 F 21 9 0.02 Pos 10.33 Neg Neg 69.2 Whole (C)
+68d Neg Pos Pos Neg Neg ND
+105d Neg Pos Pos Neg Neg ND
SZ22 M 45 21 0.02 Pos Neg Neg Nega 6.8 BCP/PC
+35d Neg Pos Neg Neg Pos Pos
SZ26 M 28 10 0.02 Pos 9.83 Neg Pos 17.4 PreS/S (C)
SZ27 F 20 9 0.01 Pos Neg Neg Pos <1 BCP/PC
SZ28 M 35 26 0.01 Pos Neg Neg Neg <1
SZ29 M 42 22 0.01 Pos Neg Neg Pos 178.4 BCP/PC
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

22
1
ALT level (IU/L) was tested by ReflotronPlus (Roche) in Nanfang hospital, 2
Guangzhou, China. Serological markers of HBV except HBsAg were detected 3
initially by Kehua HBV EIA assays and re-tested by ARCHITECT HBsAg in Nanfang 4
hospital. HBsAg <0.05 was considered negative. Anti-HBs+ was quantified in IU/L 5
by the cobas Anti-HBs electrochemiluminescence immunoassay (Roche) in Nanfang 6
hospital. VL, viral load was quantified by QPCR against an international HBV 7
standard. VL <1 indicates samples with no Ct value but confirmed by nested PCR. 8
OBI genomes were amplified by nested PCRs and sequenced by Invitrogen. Whole 9
genome or fragments of HBV DNA were amplified by the nested PCRs and 10
genotyping was phylogenetically performed from pre-S/S sequences aligned with 11
references. ND, not done. 12
a indicate seroconversion during follow-up. 13
b Donors of index sample SZ90 and SZ99 were vaccinated 6 and 36 months prior 14
index, respectively. 15
16
17
18
SZ91 M 35 4 0.02 Pos Neg Neg Pos <1 BCP/PC
SZ92 F 26 9 0.03 Pos Neg Neg Neg 25 PreS/S(C)
SZ90b M 22 6 0.02 Neg 714.2 Neg Neg <1 BCP/PC
SZ99b M 28 7 0.01 Neg 428.5 Neg Neg <1 BCP/PC
Median 28 10 14.4
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

23
TABLE 2. Classification of HBV DNA yield index samples other than OBIs 1
Symbols in the Table as the note of Table 1. 2
3
4
5
6
7
8
9
Serological Test VL
Samples Sex Age ALT
HBsAg Anti-HBc Anti-HBs HBeAg Anti-HBe (IU/ml)
Genome
& Genotype
1st-WP
SZ14 F 24 24 0.02a Neg Neg Neg Neg 224.6 BCP/PC
+12d Neg Neg Neg Neg Neg 262
+38d Pos Neg Neg Neg Neg 121
+47d Neg Pos Pos Neg Neg ND
SZ17 M 26 18 0.02 Neg Neg Nega Neg 925.5 Whole (C)
+45d Neg Neg Neg Pos Pos 23.2
SZ23 M 19 13 0.03a Neg Neg Neg Neg 675 Whole (B)
+13 Pos Neg Neg Neg Neg 23
+20 Pos Pos Neg Neg Neg 2429
+127 Neg Neg Neg Pos Pos 85
SZ200 F 41 10 0.04 Neg Nega Neg
a Neg 283.8 Whole (B)
+5d Neg Neg Pos Pos Pos 732
2nd-WP/chronic
SZ4 M 29 23 0.02a Pos Neg Neg Pos 51.8 BCP/PC
+21 Neg Pos Neg Neg Pos ND
+45 Pos Pos Neg Neg Pos ND
+91 Pos Pos Neg Neg Pos ND
+156 pos Pos Neg Neg Pos ND
SZ12 M 25 22 0.03a Pos Neg Neg Pos <1
+8 Pos Pos Neg Neg Pos Pos
SZ3 M 42 11 0.13a Pos Neg
a Neg Pos 266.1 Whole (B)
+38 Pos Pos Neg Neg Pos 323.2
+60 Neg Pos Pos Neg Pos ND
+121 Neg Pos Pos Neg Pos ND
+166 Neg Pos Pos Neg Pos ND
+221 Neg Pos Pos Neg Pos ND
SZ24 F 19 11 0.01a Pos 27.61 Pos Neg 7321 Whole (C)
False pos
SZ13 M 34 20 0.02 Pos Neg Neg Neg Neg
SZ20 F 21 18 0.03 Neg Pos Neg Neg Neg
SZ21 F 28 25 0.02 Neg Pos Neg Neg Neg
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

24
TABLE 3. Intra- and inter-group diversity analyses between OBIC and HBsAg+ 1
sequences 2
Regulatory elements
Protein
Genome
region
OBIC
N=4
HBsAg+
N=23
P value Genome
region
OBIC
N=4
HBsAg+
N=23
P value
ENH1 6.0 (4-9) 2.8 (0-10) 0.004 Pre-S/S 11.7(2-22)a 3.6(0-14) <0.0001
SP1 14.5(4-23) 6.2 (1-19) <0.0001 Pre-S1 4.3 (2-7) 0.7 (0-3) <0.0001
SP2 9.0 (5-17) 2.7 (0-9) <0.0001 Pre-S2 0.7 (0-1) 0.9 (0-7) 0.630
S 7.0 (0-14) 1.9 (0-6) <0.0001
ENH2 6.0 (4-10) 2.7 (0-7) 0.001 MHR 0.7 (0-3) 0.4 (0-1) 0.322
CURS 3.0 (2-4) 1.3 (0-4) 0.025 Pre-C/C 3.5 (2-5) 1.5 (0-5) 0.013
BCP 1.5 (0-3)a 1.4 (0-4) 0.846 Pol 23.3(11-47) 8.9(2-35) <0.0001
Pol (RT) 4.5 (2-7) 1.5 (0-5) 0.001
XP 2.5 (1-3) 2.2 (0-5) 0.713 X 8.0 (5-15) 3.0 (0-7) <0.0001
Regions with regulatory functions in HBV are presented separately. SP1 (nt2219-2780) 3
and SP2 (nt2809-3152), promoters for pre-S1 and pre-S2/S; XP (nt1239-1376), 4
promoter for X region; CURS (nt1643-1741), core upstream regulatory sequence; 5
BCP (nt1742-1849), basal core promoter; ENH2 (nt1627-1774), enhancer II; ENH1 6
(nt1071-1238), enhancer I. MHR, major hydrophilic region of S protein; Pol = 7
polymerase; Pol (RT) = reverse transcriptase; X, HBx. Average intra-group diversity 8
was calculated as the number of nucleotide or aa substitution differences between OBI 9
and reference sequences. The range for frequency of nt or aa substitutions is in 10
parentheses. N, number of complete sequences from OBIC or references used in 11
analysis. The difference of mean diversity between OBIC and reference sequences was 12
calculated as p value by Fisher’s Exact test. 13
a N=6 for BCP and pre-S/S regions from OBIC. 14
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

25
TABLE 4. Site mutations in core promoter of OBIs 1
Positions of mutation sites within CURS (nt1643-1741) and BCP (nt 1742-1849) are 2
presented according to nt numbering from EcoR1. NA, not available for nt1643-1678 3
from BCP/PC amplicons of 16 OBIs. HBsAg+ B/C represents the nt consensus of 4
genotype B or C (B/C) reference strains, their average diversity rates are 0.82% and 5
1.4%, respectively. The site mutations of OBIs were indicated at genotype B/C 6
positions of references. Consensus at site nt1752 was 95.7% (22/23) nucleotide A 7
within genotype C and 43.8% (7/16) A or 56.2% (9/16) G within genotype B. 8
a Italic C indicates an insertion of nt C of OBI SZ9. 9
b × Indicates deletions from OBI SZ22 and SZ92.10
Region CURS (nt1643-1741) BCP (nt1742-1849)
Position
1 6 5 2
1 6 7 3
1 6 7 9
1 6 8
9
1 7 0 3
1 7 0 8
1 7 1 6
1 7 1 8
1 7 1 9
1 7 2 5
1 7 2 6
1 7 2 7
1 7 3 0
1 7 4 2
1 7 5 2
1 7 6 2
1 7 6 4
1 7 9 9
1 8 4 6
HBsAg+ B/C G/
A T/
C A A A T T T G A C/
A T/
A G/
C G A A G G/
C A
SZ2 NA G T G
SZ5 (C) /T /G A G /G
SZ6 (C) G T /G T A
SZ7 (B) A/
SZ9 a NA C
SZ10 NA
SZ11 NA C
SZ15 NA A G
SZ16 (C) /C /T /G G /G
SZ18 NA G
SZ19 (C) /G /T /T /G /G
SZ22 b NA ×
SZ25 NA
SZ26 (C) NA T
SZ27 NA
SZ28 NA A
SZ29 NA
SZ90 NA
SZ91 NA G T
SZ92 (C) NA × /T /G /G
SZ99 NA
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

26
Legends 1
Fig. 1 Mutations in core proteins of OBIs corresponding to immune epitope 2
clusters of CTL, B and Th cells. Epitope clusters were from previous descriptions in 3
HBV infections (3, 16). OBI mutations in the core regions are shown; arrows indicate 4
the epitope clusters. The scale represents aa length of HBV core protein. The numbers 5
at both ends of epitopes indicate the start and end aa positions for each epitope. 6
7
Fig. 2 Alignments of deduced amino acid sequences of pre-S/S from OBIs 8
compared to consensus sequence of genotype B or C HBsAg+ strain. Alignments 9
of pre-S/S were examined for (A) Pre-S1, (B) pre-S2, (C) S and (D) MHR and “a” 10
region within the S protein. Numbered symbols indicate epitope clusters on top of 11
reference sequence (4, 7, 14). Aa identification is with one letter code. Dashes indicate 12
identity with the reference consensus sequence for genotype B or C shown on top of 13
each sequence. Aa “K” in bold in the reference sequence indicates HBV serotype 14
specific aa. MHR aa mutations in italics may affect serotype or subtype of HBV. 15
on March 30, 2018 by guest
http://jcm.asm
.org/D
ownloaded from