changes in corneal thickness, curvature, and anterior chamber depth during the menstrual cycle
TRANSCRIPT

Changes in corneal thickness, curvature, and anteriorchamber depth during the menstrual cycle
Hassan Hashemi,*{ MD; Shiva Mehravaran,* MD; Farhad Rezvan,* MD
ABSTRACT N RESUME
Objective: To determine the variations in corneal thickness values, keratometry readings, and anterior chamberdepths (ACD) during the menstrual cycle of young women using the noncontact Scheimpflug imaging technique.
Design: Prospective cohort study.Participants: Fourteen women with regular menstrual cycles who were not taking contraceptive pills were enrolled
and had measurements taken every other day during a full menstrual cycle, starting from the first day. None usedcontact lenses or regular medication, and none had systemic disease or history of eye surgery.
Methods: The thickness at the centre, superior, inferior, temporal, nasal, and thinnest point of the cornea, the kerato-metry readings, and the ACD values measured with the Pentacam were recorded. We used data on days 1, 3, and 5 ofthe studied cycle, and counting backwards, 2, 4, 6, 12, 14, and 16 days before the first day of the next cycle.
Results: Themean differences between 2 points of time were not statistically significant (p. 0.05) for any variable. Themean difference between any 2 paired thickness measurements was less than 5.0 mm.
Conclusions:Contrary to our expectations and previous findings using ultrasound pachymetry, we found no clinicallyor statistically significant differences between the repeated measurements with the Pentacam. This could indicatethat the Pentacam is a clinical tool with less variability when performing serial measurements and follow-up exam-inations.
Objet : Etablir les variations de l’epaisseur corneenne, des lectures keratometriques et de la profondeur de la chambreanterieure (PCA) pendant le cycle menstruel des jeunes femmes selon la technique d’imagerie sans contact deScheimpflug.
Nature : Etude prospective de cohortes.Participantes :Quatorze femmes ayant des cycles menstruels normaux et ne prenant pas de pilule contraceptive ont
ete inscrites a l’etude. Les mesures ont ete prises a tous les deux jours pendant le cycle menstruel entier, a compterde la premiere journee. Aucune n’a utilise de verres de contact ni de medicaments reguliers et aucune n’avait demaladie systemique ni d’antecedents de chirurgie oculaire.
Methodes : Lesmesures de l’epaisseur au centre, aux parties superieure, inferieure, temporale, nasale et aux points lesplus minces de la cornee, les lectures keratometriques et la PCA ont ete relevees avec la Pentacam. Les donneesutilisees etaient celles des jours 1, 3 et 5 du cycle a l’etude, et les comptes a rebours 2, 4, 6, 12, 14 et 16 jours avant lepremier jours du cycle suivant.
Resultats : Les ecarts moyens entre 2 moments n’etaient pas statistiquement significatifs (p . 0,05) pour toutes lesvariables. L’ecart moyen entre 2 paires d’epaisseurs etait moins de 5,0 mm.
Conclusions :Contrairement a nos attentes et aux donnees precedentes de la pachymetrie a l’ultrason, nous n’avonspas trouve d’ecart cliniquement ou statistiquement significatif entre les mesures reprises avec la Pentacam. Celapourrait indiquer que la Pentacam est un outil clinique qui a moins de variabilite pour effectuer des mesures en serieet des examens de suivi.
The corneal thickness can be measured through a vari-ety of techniques, the gold standard of which is ultra-
sonography.1,2 There are several disadvantages to theultrasonic pachymetry technique that limit its accuracyand clinical value. These include the need for topical anaes-thesia, contact of a probe with the cornea and the assoc-iated risk of infection, the potential for inaccuratepositioning of the probe due to lack of fixation and gazecontrol, estimating the thickness of only a single point witheach contact, and the difficulty of performing scanningpachymetry to find abnormally thin areas of the cornea.2–4
The measurements may also be affected by variations in
sound speed with changes in tissue hydration, which maybe a result of hormonal changes during a regular menstrualcycle.The menstrual cycle is a collection of phases occurring
during the beginning of one menstrual flow to the begin-ning of the next. The first phase of a cycle is known as thefollicular phase, which lasts approximately 14 days. Thefollicular phase begins with menstrual flow, which occursduring the first few days, and is followed by increasinglevels of estrogen. At the ovulation phase, there is a pre-ovulatory estradiol surge, and then a mature follicleis released. The third and last phase of the cycle is the
From *the Noor Ophthalmology Research Center, Noor Eye Hospital; and{the Farabi Eye Hospital, Tehran University of Medical Sciences, Tehran,
Iran
Originally received Mar. 26, 2009. Revised June 7, 2009
Accepted for publication Sep. 29, 2009
Published online Jan. 13, 2010
Correspondence to Shiva Mehravaran, MD, Noor Ophthalmology Research
Center, #106 Esfandiar Blvd., Vali’asr Ave., Tehran 19686, Iran;
This article has been peer-reviewed. Cet article a ete evalue par les pairs.
Can J Ophthalmol 2010;45:67–70
doi:10.3129/i09-222
CAN J OPHTHALMOL—VOL. 45, NO. 1, 2010 67
luteal phase, when there are rising levels of progesteroneand estrogen. During a menstrual cycle, there are alsofluctuations in the levels of the luteinizing hormone andthe follicle-stimulating hormone, which are released fromthe pituitary gland.The hormonal changes during a menstrual cycle are
physiologic factors that may affect the corneal topography,curvature, and thickness; these are thought to be consistentwith changes in estrogen levels.5 However, results of studieson the correlation between ocular and hormonal variablesare not consistent. The present study was designed toinvestigate the changes in corneal thickness and curvature,as well as the anterior chamber depth (ACD), during themenstrual cycle, using a noncontact Scheimpflug imag-ing device, the Pentacam (Oculus Optikgerate, GmbH,Wetzlar, Germany).
METHODS
Young women were recruited from among hospital staffwho had volunteered to participate in the study. The par-ticipants had regular menstrual cycles, midcycle and pre-menstrual symptoms, and were not taking contraceptivepills. None of the participants used contact lenses or regu-lar medication, and none had systemic disease or a historyof eye trauma or surgery.During the pilot study, 2 right eye and 1 left eye Penta-
cam acquisitions were done on 33 volunteers to test therepeatability of the measurements and determine the cor-relations between right and left eye measurements. Theoriginal study began 4weeks later, and 14 participants wereinstructed to have 1 right eye measurement every other dayduring a full menstrual cycle starting from the first day.They were asked tomark their calendars to keep a record ofthe cycle.All tests were done with the Pentacam between 1:00 and
2:00 PM to avoid any possible diurnal fluctuations6 andensure that the participants had been awake for more than3 hours. The collected data included pachymetry mea-sures, simulated keratometry readings, and ACD readings.The pachymetry data included the thickness of the cornea
in the centre and at the thinnest point, as well as the super-ior, inferior, temporal, and nasal cornea, 3.0mm from thecentre.The study protocol was approved by the Institutional
Review Board of Noor Ophthalmology Research Center.The nature of the study was explained to all volunteers, andthe participants consented to take part during the entirestudy period, have the necessary examinations, and informthe researchers of any changes in their menstrual cycle.In the analyses, the Bland–Altman method was used
to express repeatability and the 95% limits of agree-ment (LoA). Correlation between contralateral eyes wasdetermined by the Pearson correlation coefficient. Varia-tions within subjects and between tests for each variablewere assessed through repeated measures analysis of vari-ance. A p value ,0.05 was considered significant. Resultsare presented as means and standard deviations.
RESULTS
The mean age of the participants was 28.6 (SD 2.6,range 25–33) years, and the mean cycle duration was28.1 (SD 2.9, range 24–34) days.Pachymetry, keratometry, and ACD data from same-
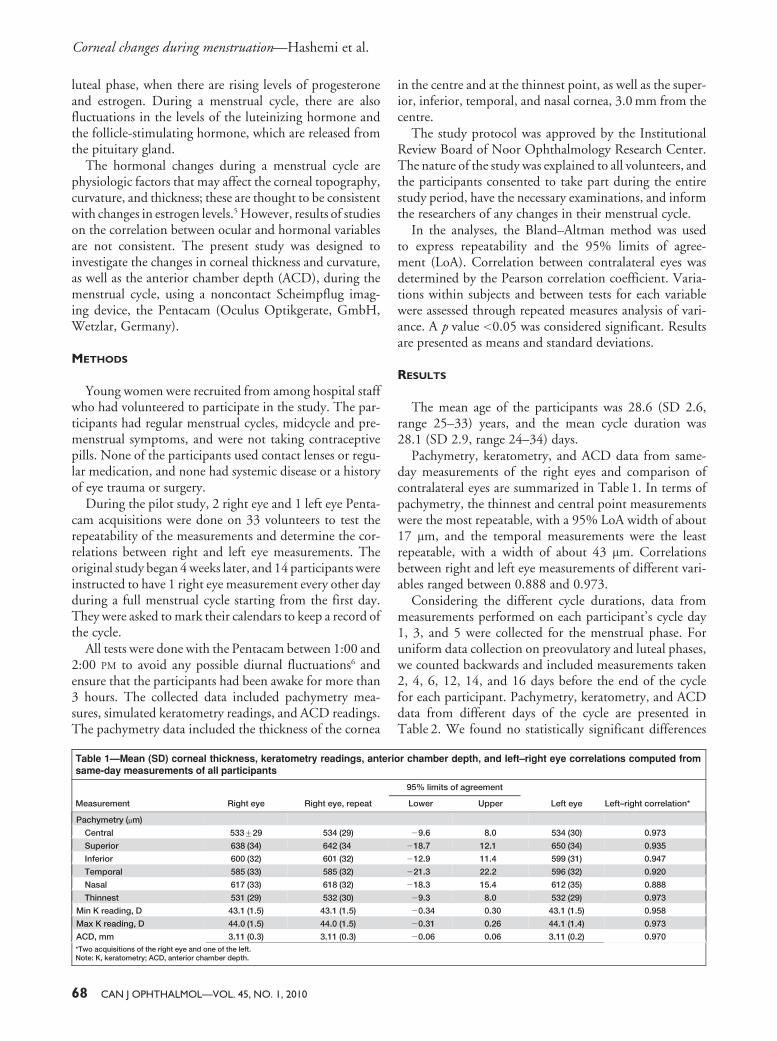
day measurements of the right eyes and comparison ofcontralateral eyes are summarized in Table 1. In terms ofpachymetry, the thinnest and central point measurementswere the most repeatable, with a 95% LoA width of about17 mm, and the temporal measurements were the leastrepeatable, with a width of about 43 mm. Correlationsbetween right and left eye measurements of different vari-ables ranged between 0.888 and 0.973.Considering the different cycle durations, data from
measurements performed on each participant’s cycle day1, 3, and 5 were collected for the menstrual phase. Foruniform data collection on preovulatory and luteal phases,we counted backwards and included measurements taken2, 4, 6, 12, 14, and 16 days before the end of the cyclefor each participant. Pachymetry, keratometry, and ACDdata from different days of the cycle are presented inTable 2. We found no statistically significant differences
Table 1—Mean (SD) corneal thickness, keratometry readings, anterior chamber depth, and left–right eye correlations computed fromsame-day measurements of all participants
Measurement Right eye Right eye, repeat
95% limits of agreement
Left eye Left–right correlation*Lower Upper
Pachymetry (mm)
Central 533¡29 534 (29) 29.6 8.0 534 (30) 0.973
Superior 638 (34) 642 (34 218.7 12.1 650 (34) 0.935
Inferior 600 (32) 601 (32) 212.9 11.4 599 (31) 0.947
Temporal 585 (33) 585 (32) 221.3 22.2 596 (32) 0.920
Nasal 617 (33) 618 (32) 218.3 15.4 612 (35) 0.888
Thinnest 531 (29) 532 (30) 29.3 8.0 532 (29) 0.973
Min K reading, D 43.1 (1.5) 43.1 (1.5) 20.34 0.30 43.1 (1.5) 0.958
Max K reading, D 44.0 (1.5) 44.0 (1.5) 20.31 0.26 44.1 (1.4) 0.973
ACD, mm 3.11 (0.3) 3.11 (0.3) 20.06 0.06 3.11 (0.2) 0.970
*Two acquisitions of the right eye and one of the left.Note: K, keratometry; ACD, anterior chamber depth.
Corneal changes during menstruation—Hashemi et al.
68 CAN J OPHTHALMOL—VOL. 45, NO. 1, 2010
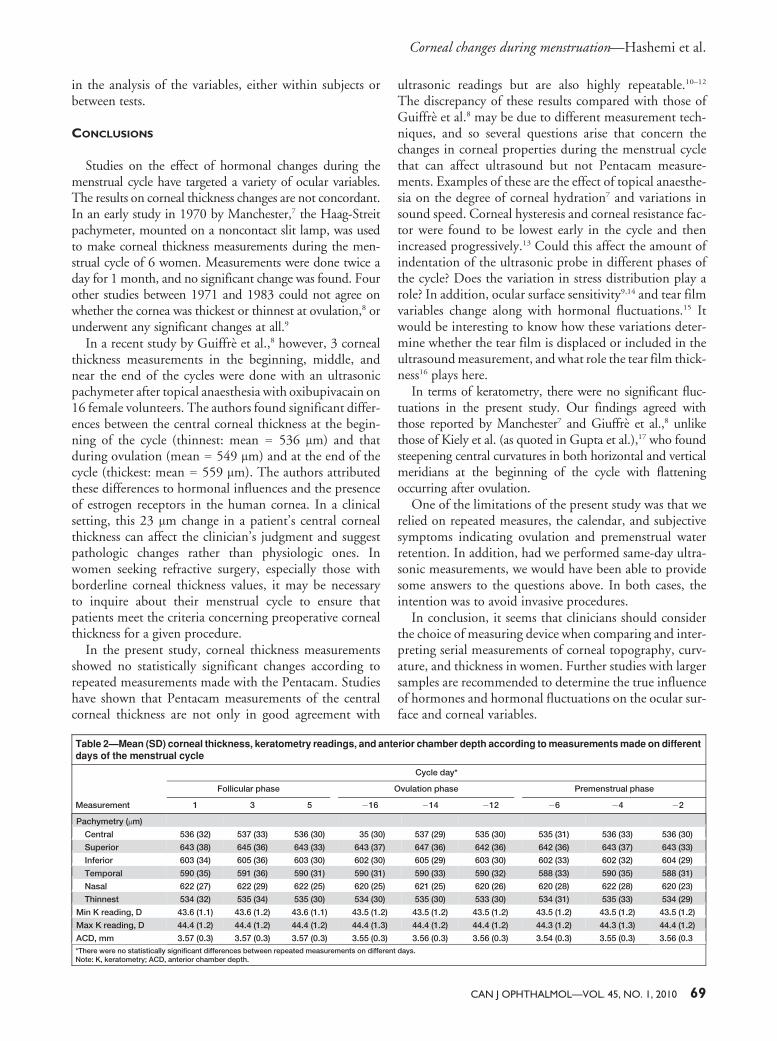
in the analysis of the variables, either within subjects orbetween tests.
CONCLUSIONS
Studies on the effect of hormonal changes during themenstrual cycle have targeted a variety of ocular variables.The results on corneal thickness changes are not concordant.In an early study in 1970 by Manchester,7 the Haag-Streitpachymeter, mounted on a noncontact slit lamp, was usedto make corneal thickness measurements during the men-strual cycle of 6 women. Measurements were done twice aday for 1 month, and no significant change was found. Fourother studies between 1971 and 1983 could not agree onwhether the cornea was thickest or thinnest at ovulation,8 orunderwent any significant changes at all.9
In a recent study by Guiffre et al.,8 however, 3 cornealthickness measurements in the beginning, middle, andnear the end of the cycles were done with an ultrasonicpachymeter after topical anaesthesia with oxibupivacain on16 female volunteers. The authors found significant differ-ences between the central corneal thickness at the begin-ning of the cycle (thinnest: mean 5 536 mm) and thatduring ovulation (mean 5 549 mm) and at the end of thecycle (thickest: mean 5 559 mm). The authors attributedthese differences to hormonal influences and the presenceof estrogen receptors in the human cornea. In a clinicalsetting, this 23 mm change in a patient’s central cornealthickness can affect the clinician’s judgment and suggestpathologic changes rather than physiologic ones. Inwomen seeking refractive surgery, especially those withborderline corneal thickness values, it may be necessaryto inquire about their menstrual cycle to ensure thatpatients meet the criteria concerning preoperative cornealthickness for a given procedure.In the present study, corneal thickness measurements
showed no statistically significant changes according torepeated measurements made with the Pentacam. Studieshave shown that Pentacam measurements of the centralcorneal thickness are not only in good agreement with
ultrasonic readings but are also highly repeatable.10–12
The discrepancy of these results compared with those ofGuiffre et al.8 may be due to different measurement tech-niques, and so several questions arise that concern thechanges in corneal properties during the menstrual cyclethat can affect ultrasound but not Pentacam measure-ments. Examples of these are the effect of topical anaesthe-sia on the degree of corneal hydration7 and variations insound speed. Corneal hysteresis and corneal resistance fac-tor were found to be lowest early in the cycle and thenincreased progressively.13 Could this affect the amount ofindentation of the ultrasonic probe in different phases ofthe cycle? Does the variation in stress distribution play arole? In addition, ocular surface sensitivity9,14 and tear filmvariables change along with hormonal fluctuations.15 Itwould be interesting to know how these variations deter-mine whether the tear film is displaced or included in theultrasoundmeasurement, andwhat role the tear film thick-ness16 plays here.In terms of keratometry, there were no significant fluc-
tuations in the present study. Our findings agreed withthose reported by Manchester7 and Giuffre et al.,8 unlikethose of Kiely et al. (as quoted in Gupta et al.),17 who foundsteepening central curvatures in both horizontal and verticalmeridians at the beginning of the cycle with flatteningoccurring after ovulation.One of the limitations of the present study was that we
relied on repeated measures, the calendar, and subjectivesymptoms indicating ovulation and premenstrual waterretention. In addition, had we performed same-day ultra-sonic measurements, we would have been able to providesome answers to the questions above. In both cases, theintention was to avoid invasive procedures.In conclusion, it seems that clinicians should consider
the choice of measuring device when comparing and inter-preting serial measurements of corneal topography, curv-ature, and thickness in women. Further studies with largersamples are recommended to determine the true influenceof hormones and hormonal fluctuations on the ocular sur-face and corneal variables.
Table 2—Mean (SD) corneal thickness, keratometry readings, and anterior chamber depth according tomeasurementsmade on differentdays of the menstrual cycle
Measurement
Cycle day*
Follicular phase Ovulation phase Premenstrual phase
1 3 5 216 214 212 26 24 22
Pachymetry (mm)
Central 536 (32) 537 (33) 536 (30) 35 (30) 537 (29) 535 (30) 535 (31) 536 (33) 536 (30)
Superior 643 (38) 645 (36) 643 (33) 643 (37) 647 (36) 642 (36) 642 (36) 643 (37) 643 (33)
Inferior 603 (34) 605 (36) 603 (30) 602 (30) 605 (29) 603 (30) 602 (33) 602 (32) 604 (29)
Temporal 590 (35) 591 (36) 590 (31) 590 (31) 590 (33) 590 (32) 588 (33) 590 (35) 588 (31)
Nasal 622 (27) 622 (29) 622 (25) 620 (25) 621 (25) 620 (26) 620 (28) 622 (28) 620 (23)
Thinnest 534 (32) 535 (34) 535 (30) 534 (30) 535 (30) 533 (30) 534 (31) 535 (33) 534 (29)
Min K reading, D 43.6 (1.1) 43.6 (1.2) 43.6 (1.1) 43.5 (1.2) 43.5 (1.2) 43.5 (1.2) 43.5 (1.2) 43.5 (1.2) 43.5 (1.2)
Max K reading, D 44.4 (1.2) 44.4 (1.2) 44.4 (1.2) 44.4 (1.3) 44.4 (1.2) 44.4 (1.2) 44.3 (1.2) 44.3 (1.3) 44.4 (1.2)
ACD, mm 3.57 (0.3) 3.57 (0.3) 3.57 (0.3) 3.55 (0.3) 3.56 (0.3) 3.56 (0.3) 3.54 (0.3) 3.55 (0.3) 3.56 (0.3
*There were no statistically significant differences between repeated measurements on different days.Note: K, keratometry; ACD, anterior chamber depth.
Corneal changes during menstruation—Hashemi et al.
CAN J OPHTHALMOL—VOL. 45, NO. 1, 2010 69

The authors wish to thank Miss F. Jafari and Miss S. Bigdeli for their
valuable assistance in conducting the project. The authors have no pro-
prietary or commercial interest in any materials discussed in this article.
REFERENCES
1. Iskander NG, Anderson Penno E, Peters NT, Gimbel HV,Ferensowicz M. Accuracy of Orbscan pachymetry measure-ments and DHG ultrasound pachymetry in primary laser in
situ keratomileusis and LASIK enhancement procedures.J Cataract Refract Surg 2001;27:681–5.
2. Chakrabarti HS, Craig JP, BrahmaA,Malik TY,McGheeCN.Comparison of corneal thickness measurements using ultra-
sound and Orbscan slit-scanning topography in normal andpost-LASIK eyes. J Cataract Refract Surg 2001;27:1823–8.
3. Javaloy J, VidalMT,Villada JR, Artola A, Alio JL. Comparisonof four corneal pachymetry techniques in corneal refractive
surgery. J Refract Surg 2004;20:29–34.4. Sallet G. Comparison of optical and ultrasound central corneal
pachymetry. Bull Soc Belge Ophtalmol 2001;281:35–8.5. Liu Z, Yang X, Zhang M. Topography of the normal cornea.
In: Wang M, ed. Corneal Topography in the Wavefront Era:A Guide for Clinical Application. Thorofare, NJ: Slack, Inc;2006:80.
6. Lattimore MR Jr, Kaupp S, Schallhorn S, Lewis R 4th. Orbs-
can pachymetry: implications of a repeated measures anddiurnal variation analysis. Ophthalmology 1999;106:977–81.
7. Manchester PT Jr. Hydration of the cornea. Trans AmOphthalmol Soc 1970;68:425–61.
8. Giuffre G, Di Rosa L, Fiorino F, Bubella DM, Lodato G.Variations in central corneal thickness during the menstrualcycle in women. Cornea 2007;26:144–6.
9. Riss B, Binder S, Riss P, Kemeter P. Corneal sensitivity during
the menstrual cycle. Br J Ophthalmol 1982;66:123–6.10. Lackner B, Schmidinger G, Pieh S, Funovics MA, Skorpik C.
Repeatability and reproducibility of central corneal thickness
measurement with Pentacam, Orbscan, and ultrasound.Optom Vis Sci 2005;82:892–9.
11. Barkana Y, Gerber Y, Elbaz U, et al. Central corneal thickness
measurement with the Pentacam Scheimpflug system, opticallow-coherence reflectometry pachymeter, and ultrasoundpachymetry. J Cataract Refract Surg 2005;31:1729–35.
12. HashemiH,Mehravaran S. Central corneal thicknessmeasure-
ment with Pentacam, Orbscan II, and ultrasound devicesbefore and after laser refractive surgery for myopia. J CataractRefract Surg 2007;33:1701–7.
13. Alfonso R. The ocular response analyzer continues to expandour understanding of ocular disease. Ophthalmology WebCommunity. Available at: http://www.ophthalmologyweb.com/
Spotlight.aspx?spid523&aid5255. Accessed June 23, 2008.14. Millodot M, Lamont A. Influence of menstruation on corneal
sensitivity. Br J Ophthalmol 1974;58:752–6.15. Versura P, Fresina M, Campos EC. Ocular surface changes
over the menstrual cycle in women with and without dry eye.Gynecol Endocrinol 2007;23:385–90.
16. King-Smith PE, Fink BA, Fogt N, Nichols KK, Hill RM,
Wilson GS. The thickness of the human precorneal tear film:evidence from reflection spectra. Invest Ophthalmol Vis Sci2000;41:3348–59.
17. Gupta PD, Johar K Sr, Nagpal K, Vasavada AR. Sex hormonereceptors in the human eye. Surv Ophthalmol 2005;50:274–84.
Keywords: corneal topography, menstruation, menstrual cycle,anterior chamber
Corneal changes during menstruation—Hashemi et al.
70 CAN J OPHTHALMOL—VOL. 45, NO. 1, 2010