cervical cancer screening, diagnosis and treatment ... · cervical cancer screening, diagnosis and...
TRANSCRIPT

Cervical Cancer Screening, Diagnosis and TreatmentInterventions for Racial and Ethnic Minorities: A Systematic Review
Susan B. Glick, MD1, Amanda R. Clarke, MPH2,3, Anita Blanchard, MD4, and Amy K. Whitaker, MD, MS4
1Department of Medicine, Section of General Internal Medicine, University of Chicago, Chicago, IL, USA; 2Robert Wood Johnson FoundationFinding Answers: Disparities Research for Change National Program Office, Chicago, IL, USA; 3Center for Health and the Social Sciences,University of Chicago, Chicago, IL, USA; 4Department of Obstetrics and Gynecology, University of Chicago, Chicago, IL, USA.
OBJECTIVES: To systematically review the literature todetermine which interventions improve the screening,diagnosis or treatment of cervical cancer for racial and/or ethnic minorities.DATA SOURCES: Medline on OVID, Cochrane Registerof Controlled Trials, CINAHL, PsycINFO and CochraneSystematic Reviews.STUDY ELIGIBILITY CRITERIA, PARTICIPANTS ANDINTERVENTIONS: We searched the above databases fororiginal articles published in English with at least oneintervention designed to improve cervical cancer pre-vention, screening, diagnosis or treatment that linkedparticipants to the healthcare system; that focused onUS racial and/or ethnic minority populations; and thatmeasured health outcomes. Articles were reviewed todetermine the population, intervention(s), and out-comes. Articles published through August 2010 wereincluded.STUDY APPRAISAL AND SYNTHESIS METHODS: Oneauthor rated the methodological quality of each of theincluded articles. The strength of evidence was assessedusing the criteria developed by the GRADE WorkingGroup.45,46
RESULTS: Thirty-one studies were included. Thestrength of evidence is moderate that telephone supportwith navigation increases the rate of screening forcervical cancer in Spanish- and English-speaking pop-ulations; low that education delivered by lay healtheducators with navigation increases the rate of screen-ing for cervical cancer for Latinas, Chinese Americansand Vietnamese Americans; low that a single visit forscreening for cervical cancer and follow up of anabnormal result improves the diagnosis and treatmentof premalignant disease of the cervix for Latinas; andlow that telephone counseling increases the diagnosisand treatment of premalignant lesions of the cervix forAfrican Americans.LIMITATIONS: Studies that did not focus on racialand/or ethnic minority populations may have beenexcluded. In addition, this review excluded interven-tions that did not link racial and ethnic minorities tothe health care system. While inclusion of these studiesmay have altered our findings, they were outside thescope of our review.CONCLUSIONS AND IMPLICATIONS OF KEYFINDINGS: Patient navigation with telephone supportor education may be effective at improving screening,diagnosis, and treatment among racial and ethnic
minorities. Research is needed to determine the appli-cability of the findings beyond the populations studied.
KEY WORDS: cervical cancer; disparities; minority health; equity;
intervention.
J Gen Intern Med 27(8):1016–32
DOI: 10.1007/s11606-012-2052-2
© Society of General Internal Medicine 2012
INTRODUCTION
Though cervical cancer is a preventable illness, US womencontinue to develop this disease and to die from it. In 2011,12,710 US women were expected to be diagnosed with and4290 women to die from cervical cancer.1 The burden ofcervical cancer is not shared equally among women of allraces and ethnicities. While the age-adjusted incidence rateof cervical cancer for all US women is 8.1 per 100,000women per year,1 Latinas have a significantly higherincidence of cervical cancer (11.1 per 100,000 women), asdo African-American women (10.0 per 100,000).2 Theincidence is five times higher among Vietnamese Americanwomen than white women.3
In addition, the mortality from cervical cancer is higher forAfrican-American women (4.4 per 100,000 women), Latinas(3.1 per 100,000), and Native Americans/Native Alaskans(3.4 per 100,000), than it is for whites (2.2 per 100,000) andAsians/Pacific Islanders (2.1 per 100,000).1,4–6 Mortalityfrom cervical cancer shows geographic variation in the US,with higher mortality rates among African-Americans in theDeep South, Latinas on the Texas-Mexico border, whitewomen in Appalachia, rural New York State and northernNew England, Native Americans living in the NorthernPlains, and Native Alaskans.3 The mortality rate amongforeign-born women is increasing, especially in the South.3
Because premalignant cervical disease progresses slowlyto malignancy and is easily detected and treated, thecontinued existence of cervical cancer and the disparitiesin cervical cancer rates in the US are concerning. Humanpapillomavirus (HPV), a sexually transmitted infection, isimplicated as the cause of almost all cervical cancerworldwide, so interventions that promote safe sexual
1016

practices and HPV vaccination should theoretically elimi-nate the incidence of cervical cancer.7 In addition, becausethe Papanicolaou (Pap) smear is a safe, low cost andrelatively noninvasive screening test for cervical cancer,interventions targeted at increasing screening uptake andpromotion of follow-up after abnormal screening shoulddecrease the incidence of cervical cancer as well. Finally,because members of different racial and ethnic groups tendto achieve similar outcomes when they receive similartreatment, interventions that promote equal care andtreatment should decrease mortality from cervical cancer.8
Unfortunately, the continued existence of cervical cancer andthe disparities noted in its incidence and mortality suggest thatthese interventions have not been wholly successful. Amongthose newly diagnosed with cervical cancer, 30–60 % havenever had a screening test.47,48 Up to 15 % have hadinadequate follow up after an abnormal Pap smear.48 Sixty toeighty percent of women diagnosed with advanced cervicalcancer have not had a screening test within the past 5 years.49,50
Interventions that maximize the prevention, screening, diagno-sis or treatment of cervical cancer are critical to eradicate thisdisease. Currently, there exists no consolidated evaluation ofthe intervention research literature to determine which inter-
ventions improve cervical cancer prevention, screening, diag-nosis or treatment for racial or ethnic minorities in the US. Thepurpose of this systematic review is to fill that gap.
METHODS
Data Sources and Searches
We conducted a systematic review of the English languageliterature to assess studies that described and evaluatedinterventions with the potential to improve cervical cancerprevention, screening, diagnosis or treatment for racial and/or ethnic minorities in the United States. We conducted anelectronic search of the following five databases from theirinception through August 2010: MEDLINE on OVID, TheCochrane Register of Controlled Trials, CINAHL, Psy-cINFO, and Cochrane Systematic Reviews. We used anidentical search strategy for each database (see Text Box 1).In addition, we searched the reference sections of relevantreview articles as well as all included studies for additionalmanuscripts. This review does not have a publishedprotocol and therefore, was not registered.
Study Selection and Data Extraction
Titles and abstracts were reviewed by one author to determineeligibility for inclusion. Eligible studies had to meet all fiveinclusion criteria: 1) represent an original study; 2) include atleast one intervention designed to improve cervical cancerprevention, screening, diagnosis or treatment that linkedparticipants to the healthcare system; 3) present data for racialand/or ethnic minority populations in the US; 4) measuredirect outcomes such as HPV vaccination (cervical cancerprevention), Pap tests (cervical cancer screening), follow up
of abnormal Pap smears (cervical cancer diagnosis ortreatment of premalignant disease of the cervix) or treatmentof cervical cancer; and 5) report findings in English. We didnot include conference abstracts or unpublished studies.Articles not meeting inclusion criteria were reviewed by asecond author. When possible, disagreements were resolvedby discussion; when this was not possible, a third authorevaluated the title and abstract. Articles not recommended forexclusion were then reviewed in full. Following full textreview, those articles that did not meet all five inclusion
Text Box 1. Search Strategy
1017Glick et al.: Cervical Cancer Interventions for MinoritiesJGIM
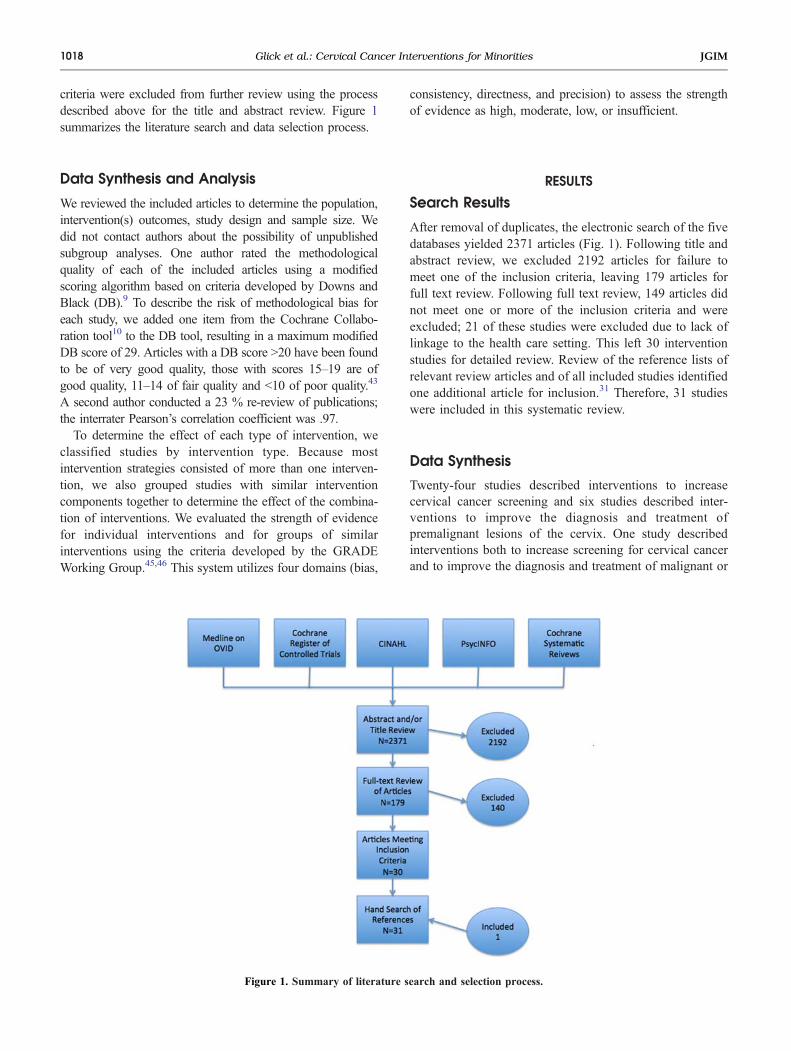
criteria were excluded from further review using the processdescribed above for the title and abstract review. Figure 1summarizes the literature search and data selection process.
Data Synthesis and Analysis
We reviewed the included articles to determine the population,intervention(s) outcomes, study design and sample size. Wedid not contact authors about the possibility of unpublishedsubgroup analyses. One author rated the methodologicalquality of each of the included articles using a modifiedscoring algorithm based on criteria developed by Downs andBlack (DB).9 To describe the risk of methodological bias foreach study, we added one item from the Cochrane Collabo-ration tool10 to the DB tool, resulting in a maximum modifiedDB score of 29. Articles with a DB score >20 have been foundto be of very good quality, those with scores 15–19 are ofgood quality, 11–14 of fair quality and <10 of poor quality.43
A second author conducted a 23 % re-review of publications;the interrater Pearson’s correlation coefficient was .97.To determine the effect of each type of intervention, we
classified studies by intervention type. Because mostintervention strategies consisted of more than one interven-tion, we also grouped studies with similar interventioncomponents together to determine the effect of the combina-tion of interventions. We evaluated the strength of evidencefor individual interventions and for groups of similarinterventions using the criteria developed by the GRADEWorking Group.45,46 This system utilizes four domains (bias,
consistency, directness, and precision) to assess the strengthof evidence as high, moderate, low, or insufficient.
RESULTS
Search Results
After removal of duplicates, the electronic search of the fivedatabases yielded 2371 articles (Fig. 1). Following title andabstract review, we excluded 2192 articles for failure tomeet one of the inclusion criteria, leaving 179 articles forfull text review. Following full text review, 149 articles didnot meet one or more of the inclusion criteria and wereexcluded; 21 of these studies were excluded due to lack oflinkage to the health care setting. This left 30 interventionstudies for detailed review. Review of the reference lists ofrelevant review articles and of all included studies identifiedone additional article for inclusion.31 Therefore, 31 studieswere included in this systematic review.
Data Synthesis
Twenty-four studies described interventions to increasecervical cancer screening and six studies described inter-ventions to improve the diagnosis and treatment ofpremalignant lesions of the cervix. One study describedinterventions both to increase screening for cervical cancerand to improve the diagnosis and treatment of malignant or
Figure 1. Summary of literature search and selection process.
1018 Glick et al.: Cervical Cancer Interventions for Minorities JGIM
premalignant lesions of the cervix.42 No studies describedinterventions to improve HPV vaccination.
Quality Assessment
Of the studies of interventions to improve screening forcervical cancer in racial and ethnic minority popula-tions, one was of very good quality,14 ten were of goodquality,15,22,23,32–36,39,40 12 were of fair quality,12,13,16–21,25,37,38,41 and one was of poor quality.26 Of thestudies of interventions to improve the diagnosis andtreatment of premalignant disease of the cervix, three were ofgood quality27–29 and three were of fair quality.24,30,31 Thesingle study that included both types of interventions was offair quality.42 The average modified DB score of includedarticles was 15 (range 9–23). In comparison, for a recentgroup of systematic reviews of interventions to reducedisparities, the average DB score was 18 out of a maximumscore of 27 points.11
Types of Interventions Examined
Of the 25 studies evaluating interventions to improve the rateof screening for cervical cancer, eight included a singleintervention12,17,32–34,38,40,42 and 17 included multiple inter-ventions.13–16,18–23,25,26,35–37,39,41 The most common inter-ventions were educational materials and education programs.Nineteen interventions included educational materi-als12,13,15,16,18–23,25,26,32,33,36,37,39–41 and 15 included educa-tion programs.15,16,18,19,21–23,25,26,35–37,39,41 Seveninterventions included navigation (including assistance sched-uling appointments, finding low-cost sources of care and withtransportation),13–15,22,23,35,36 five included strategies to pro-vide low-cost screening,16,21,26,37,42 five included strategies toimprove access to screening,17,18,21,34,38,39 four includedreminders for healthcare providers,18–20,25,41 four includedadvertisements,22,25,26,39 four included office policies andprocedures (such as protocols or tracking systems),18,25,26,41
three included telephone counseling or support,13,14,20 twoincluded feedback for providers on screening rates,18,41 andone included upgraded equipment.18
Of the seven studies evaluating interventions to improve thediagnosis and treatment of premalignant disease of the cervixin minority populations, two involved telephone counsel-ing.27,28 One study created a streamlined process for cervicalcancer screening and follow up of abnormalities29; oneincluded intensive follow up and/or vouchers for reduced-cost care30; and one included a personalized letter andpamphlet and/or an audiovisual presentation and/or transpor-tation incentives.31 One study included written educationalmaterials, education programs, and messages in the media24;and one evaluated the Breast and Cervical Cancer Preventionand Treatment Act of 2000, which authorized Medicaidexpansion to cover treatment of patients screened under the
Breast and Cervical Cancer Mortality Prevention Act andfound to have an abnormal Pap smear.42
Impact of Interventions to Increase Screening
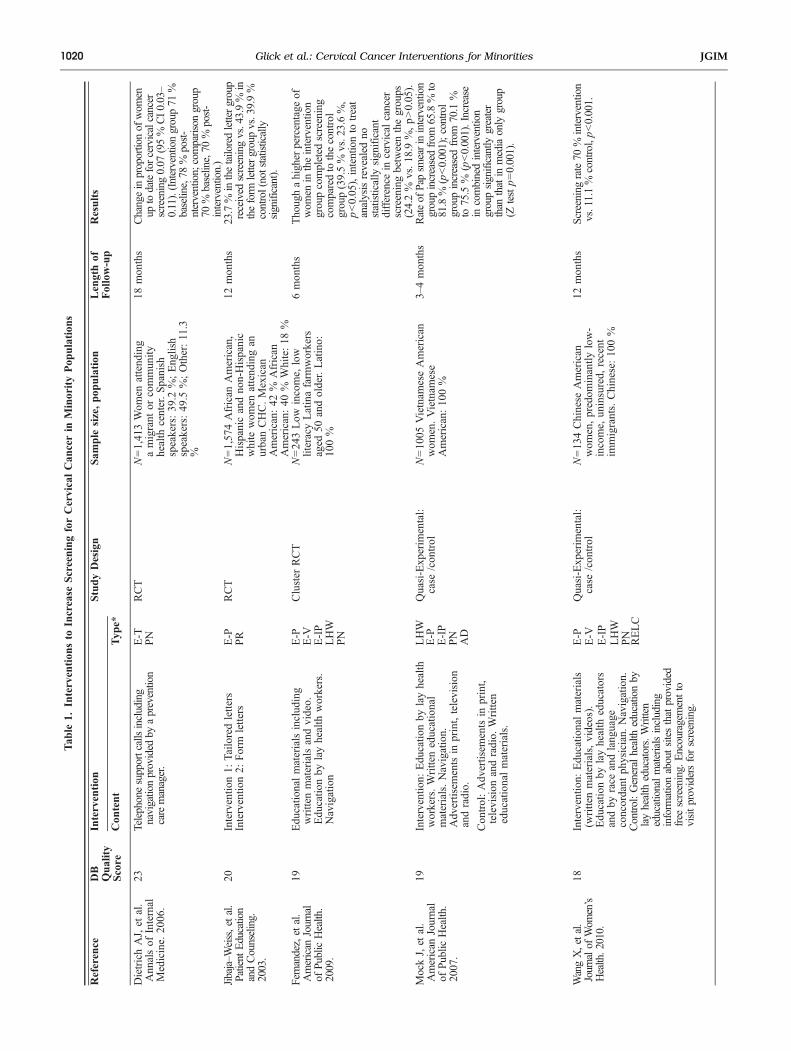
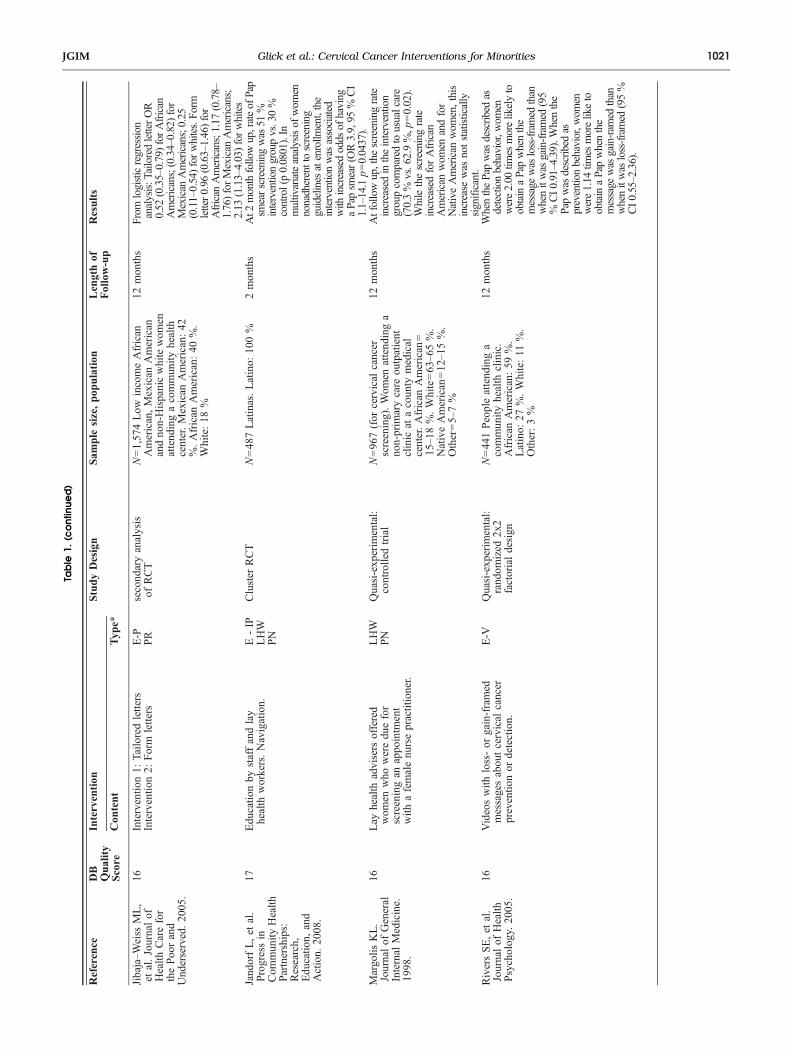
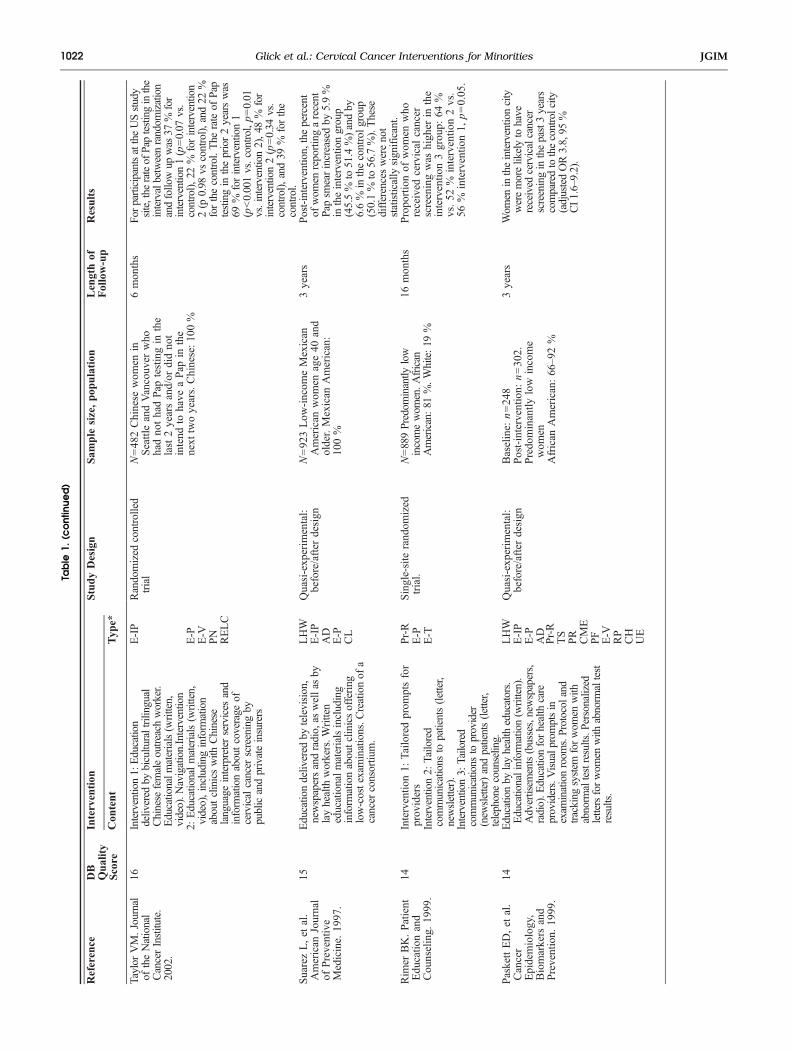
Of the eight studies that included a single intervention, fourevaluated the effect of educational materials alone toincrease the rate of screening for cervical cancer in minoritypopulations.12,32,33,40 For two of these studies, the educa-tional materials consisted of letters32,40; for the other twostudies, the intervention consisted of videos.12,33 Overall,Jibaja–Weiss found an increase in the rate of screening forcervical cancer for patients who received a form letter(43.9 % form letter vs. 39.9 % control), though not forpatients who received a tailored letter (23.7 % tailored lettervs. 39.9 % control).40 However, this difference was notstatistically significant. After examining the findings bypatient race and ethnicity, Jibaja–Weiss found a statisticallysignificant decrease in the rate of screening for cervicalcancer for African American, Mexican American and whitewomen who received a tailored letter.32 While white womenwho received a form letter experienced increased odds ofscreening (OR 2.13, 95 % CI 1.13–4.03); African Americanand Mexican American patients did not (for AfricanAmericans, OR 0.96, 95 % CI 0.63–1.46; for MexicanAmericans, OR 1.17, 95 % CI 0.78–1.76). Rivers found thatwhen the Pap smear was described as detection behavior, agroup of African American, Latino and white women weretwice as likely to obtain a Pap smear when the message wasloss-framed than when it was gain-framed (95 % CI 0.91–4.39).33 When the Pap smear was described as preventionbehavior, women were no more likely to obtain a Pap smearwhen the message was gain-framed than when it was loss-framed (OR 1.14, 95 % CI 0.55–2.36).33 Yancey showededucational videos to a sample of low income AfricanAmerican, Latina and white women in a clinic waitingroom. She found the proportion of women seen in the clinicreceiving screening was higher during intervention weeksthan during control weeks (clinic 1: 26.9 % intervention vs.19.4 % control, p=0.01; clinic 2 14.6 % interventionvs.10.3 % control, p=0.02).12 Because of the inconsistenteffect of the interventions, the strength of evidence thateducational materials improve screening for cervical cancerin minority populations is insufficient (Tables 1 and 2).Of the remaining four studies that addressed a single
intervention to improve screening for cervical cancer in racialor ethnic minority populations,17,34,38,42 each evaluated theimpact of a unique intervention. Margolis evaluated theimpact of using lay health advisers to offer women due forscreening an appointment with a female nurse practitioner.34
Because of the moderate risk of bias given this single studythat utilized a quasi-experimental design and the lack of astatistically significant impact for minority populations, thestrength of evidence is insufficient that offering women an
1019Glick et al.: Cervical Cancer Interventions for MinoritiesJGIM
Tab
le1.
Intervention
sto
Increase
ScreeningforCervicalCan
cerin
MinorityPop
ulation
s
Reference
DB
Quality
Score
Intervention
StudyDesign
Sam
ple
size,pop
ulation
Lengthof
Follow-up
Results
Con
tent
Typ
e*
DietrichAJ,et
al.
Ann
alsof
Internal
Medicine.
2006
.
23Telephonesupportcallsincluding
navigationprovided
byaprevention
caremanager.
E-T
RCT
N=1,41
3Wom
enattend
ing
amigrant
orcommun
ityhealth
center.Spanish
speakers:39
.2%;Eng
lish
speakers:49
.5%;Other:11.3
%
18mon
ths
Changeinproportionof
wom
enup
todateforcervicalcancer
screening0.07
(95%
CI0.03–
0.11).(Interventiongroup71
%baseline,78
%post-
ntervention;comparison
group
70%
baseline,70
%post-
intervention.)
PN
Jibaja–W
eiss,etal.
Patient
Education
andCounseling.
2003.
20Interventio
n1:
Tailoredletters
E-P
RCT
N=1,57
4African
American,
Hispanicandno
n-Hispanic
white
wom
enattend
ingan
urbanCHC.Mexican
American:42
%African
American:40
%White:18
%
12mon
ths
23.7%
inthetailoredlettergroup
received
screeningvs.43.9%
intheform
lettergroupvs.39.9%
control(notstatistically
significant).
Interventio
n2:
Form
letters
PR
Fernandez,etal.
American
Journal
ofPublicHealth.
2009.
19Edu
catio
nalmaterialsinclud
ing
writtenmaterialsandvideo.
Edu
catio
nby
layhealth
workers.
Navigation
E-P
Cluster
RCT
N=24
3Low
income,
low
literacyLatinafarm
workers
aged
50andolder.Latino:
100%
6mon
ths
Thoughahigher
percentage
ofwom
enin
theinterventio
ngroupcompleted
screening
comparedto
thecontrol
group(39.5%
vs.23.6%,
p<0.05),intentionto
treat
analysisrevealed
nostatistically
significant
difference
incervical
cancer
screeningbetweenthegroups
(24.2%
vs.18.9
%,p>0.05).
E-V
E-IP
LHW
PN
MockJ,et
al.
American
Journal
ofPu
blic
Health
.2007.
19Interventio
n:Edu
catio
nby
layhealth
workers.Writteneducational
materials.Navigation.
Adv
ertisem
entsin
print,television
andradio.
LHW
Quasi-Exp
erim
ental:
case
/con
trol
N=10
05Vietnam
eseAmerican
wom
en.Vietnam
ese
American:10
0%
3–4mon
ths
Rateof
Papsm
earinintervention
groupincreasedfrom
65.8%
to81.8%
(p<0.001);control
groupincreasedfrom
70.1
%to
75.5
%(p<0.001).Increase
incombinedintervention
groupsignificantly
greater
than
thatin
mediaonly
group
(Ztestp=0.001).
Con
trol:Adv
ertisem
entsin
print,
television
andradio.
Written
educationalmaterials.
E-P
E-IP
PN
AD
WangX,etal.
Journalof
Wom
en’s
Health.2010.
18Interventio
n:Edu
catio
nalmaterials
(writtenmaterials,videos).
Edu
catio
nby
layhealth
educators
andby
race
andlang
uage
concordant
physician.
Navigation.
E-P
Quasi-Exp
erim
ental:
case
/con
trol
N=13
4Chinese
American
wom
en,predom
inantly
low-
income,
uninsured,
recent
immigrants.Chinese:10
0%
12mon
ths
Screeningrate70
%intervention
vs.11.1%
control,p<0.001.
Contro
l:Generalhealth
educationby
layhealth
educators.Written
educationalmaterialsincluding
inform
ationaboutsitesthatprovided
free
screening.
Encouragementto
visitprovidersforscreening.
E-V
E-IP
LHW
PN
RELC
1020 Glick et al.: Cervical Cancer Interventions for Minorities JGIM
Table
1.(c
ontinue
d)
Reference
DB
Quality
Score
Intervention
StudyDesign
Sam
ple
size,pop
ulation
Lengthof
Follow-up
Results
Con
tent
Typ
e*
Jibaja–W
eiss
ML,
etal.Journalof
Health
Carefor
thePoo
rand
Und
erserved.20
05.
16Interventio
n1:
Tailo
redletters
E-P
second
aryanalysis
ofRCT
N=1,57
4Low
incomeAfrican
American,Mexican
American
andno
n-Hispanicwhitewom
enattend
ingacommun
ityhealth
center.Mexican
American:42
%.African
American:40
%.
White:18
%
12mon
ths
From
logisticregression
analysis:T
ailoredletterOR
0.52
(0.35–0.79)forAfrican
Americans;(0.34–0.82)for
Mexican
Americans;0.25
(0.11–0.54)forwhites.Form
letter0.96
(0.63–1.46)for
African
Americans;1.17
(0.78–
1.76)forMexican
Americans;
2.13
(1.13–4.03)forwhites
Interventio
n2:
Form
letters
PR
Jand
orfL,et
al.
Progressin
Com
mun
ityHealth
Partnerships:
Research,
Edu
catio
n,and
Action.
2008
.
17Edu
catio
nby
staffandlay
health
workers.Navigation.
E-IP
Cluster
RCT
N=48
7Latinas.Latino:
100%
2mon
ths
At2
monthfollowup,rateof
Pap
smearscreeningwas
51%
interventiongroupvs.30%
control(p0.0801).In
multivariateanalysisof
wom
ennonadherenttoscreening
guidelines
atenrollm
ent,the
interventionwas
associated
with
increasedodds
ofhaving
aPapsm
ear(OR3.9,95
%CI
1.1–14.1p=0.0437).
LHW
PN
Margo
lisKL.
Journalof
General
Internal
Medicine.
1998
.
16Lay
health
advisers
offered
wom
enwho
weredu
efor
screeningan
appo
intm
ent
with
afemalenu
rsepractitioner.
LHW
Quasi-exp
erim
ental:
controlledtrial
N=96
7(for
cervical
cancer
screening).Wom
enattend
inga
non-prim
arycare
outpatient
clinic
atacoun
tymedical
center.African
American
=15–1
8%.White=63–6
5%.
NativeAmerican
=12–1
5%.
Other=5–7%
12mon
ths
Atfollowup,the
screeningrate
increasedintheintervention
groupcomparedtousualcare
(70.3%
vs.62.9%,p
=0.02).
Whilethescreeningrate
increasedforAfrican
American
wom
enandfor
NativeAmerican
wom
en,this
increase
was
notstatistically
significant.
PN
RiversSE,et
al.
Journalof
Health
Psycholog
y.20
05.
16Videoswith
loss-or
gain-framed
messagesabou
tcervical
cancer
preventio
nor
detection.
E-V
Quasi-exp
erim
ental:
rand
omized
2x2
factorialdesign
N=44
1Peopleattend
inga
commun
ityhealth
clinic.
African
American:59
%.
Latino:
27%.White:11
%.
Other:3%
12mon
ths
WhenthePapwas
describ
edas
detectionbehavior,w
omen
were2.00
times
morelikelyto
obtainaPapwhenthe
message
was
loss-framed
than
whenitwas
gain-framed
(95
%CI0.91–4.39).W
henthe
Papwas
describ
edas
preventionbehavior,w
omen
were1.14
times
moreliketo
obtainaPapwhenthe
message
was
gain-ram
edthan
whenitwas
loss-framed
(95%
CI0.55–2.36).
1021Glick et al.: Cervical Cancer Interventions for MinoritiesJGIM
Table
1.(c
ontinue
d)
Reference
DB
Quality
Score
Intervention
StudyDesign
Sam
ple
size,pop
ulation
Lengthof
Follow-up
Results
Con
tent
Typ
e*
Taylor
VM.Journal
oftheNational
CancerInstitute.
2002.
16Intervention1:Education
delivered
bybiculturaltrilingual
Chinese
femaleoutreach
worker.
Educationalm
aterials(written,
video).N
avigation.Intervention
E-IP
Randomized
controlled
trial
N=48
2Chinese
wom
enin
SeattleandVancouv
erwho
hadno
thadPap
testingin
the
last2yearsand/or
didno
tintend
tohave
aPap
inthe
next
twoyears.Chinese:10
0%
6mon
ths
ForparticipantsattheUSstudy
site,the
rateof
Paptestinginthe
intervalbetweenrandom
ization
andfollowup
was
37%
for
intervention1(p=0.07
vs.
control),22
%forintervention
2(p
0.98
vscontrol),and
22%
forthecontrol.The
rateof
Pap
testingin
theprior2yearswas
69%
forintervention1
(p<0.001vs.control,p=0.01
vs.intervention2),48
%for
intervention2(p=0.34
vs.
control),and39
%forthe
control.
2:Educationalmaterials(written,
video),includinginform
ation
aboutclinicswith
Chinese
language
interpreterservices
and
inform
ationaboutcoverage
ofcervicalcancer
screeningby
publicandprivateinsurers
E-P
E-V
PN
RELC
SuarezL,et
al.
American
Journal
ofPreventive
Medicine.
1997
.
15Educatio
ndeliv
ered
bytelevision,
newspapersandradio,as
wellasby
layhealth
workers.W
ritten
educationalm
aterialsincluding
inform
ationaboutclin
icsoffering
low-costexaminations.C
reationof
acancer
consortiu
m.
LHW
Quasi-exp
erim
ental:
before/after
design
N=92
3Low
-incom
eMexican
American
wom
enage40
and
older.Mexican
American:
100%
3years
Post-interventio
n,thepercent
ofwom
enreportingarecent
Papsm
earincreasedby
5.9%
intheinterventiongroup
(45.5%
to51.4%)andby
6.6%
inthecontrolg
roup
(50.1%
to56.7%).These
differenceswerenot
statistically
significant.
E-IP
AD
E-P
CL
Rim
erBK.Patient
Edu
catio
nand
Cou
nseling.
1999
.
14Interventio
n1:
Tailoredprom
ptsfor
prov
iders
Pr-R
Single-site
rand
omized
trial.
N=889Predom
inantly
low
incomewom
en.African
American:81
%.White:19
%
16mon
ths
Propo
rtionof
wom
enwho
received
cervical
cancer
screeningwas
high
erin
the
interventio
n3grou
p:64
%vs.52
%interventio
n2vs.
56%
interventio
n1,
p=0.05
.
Intervention2 :
Tailored
communications
topatients(letter,
newsletter).
E-P
Intervention3:
Tailored
communications
toprovider
(new
sletter)andpatients(letter,
telephonecounseling.
E-T
PaskettED,et
al.
Cancer
Epidemiology,
Biomarkers
and
Prevention.
1999
.
14Educationby
layhealtheducators.
Educationalinformation(written).
Advertisem
ents(busses,newspapers,
radio).E
ducationforhealthcare
providers.Visualpromptsin
exam
inationroom
s.Protocoland
tracking
system
forwom
enwith
abnorm
altestresults.P
ersonalized
lettersforwom
enwith
abnorm
altest
results.
LHW
Quasi-exp
erim
ental:
before/after
design
Baseline:
n=24
83years
Wom
enintheinterventioncity
weremorelikelytohave
received
cervicalcancer
screeninginthepast3years
comparedtothecontrolcity
(adjustedOR3.8,95
%CI1.6–9.2).
E-IP
Post-interventio
n:n=30
2.E-P
Predo
minantly
low
income
wom
enAD
African
American:66–9
2%
Pr-R
TS
PR
CME
PF
E-V
RP
CH
UE
1022 Glick et al.: Cervical Cancer Interventions for Minorities JGIM
Table
1.(c
ontinue
d)
Reference
DB
Quality
Score
Intervention
StudyDesign
Sam
ple
size,pop
ulation
Lengthof
Follow-up
Results
Con
tent
Typ
e*
Bastani
R,et
al.
Med
Care.
2002
.14
Contin
uing
medicaleducationfor
health
care
providers(w
orkshops,
meetin
gs).Referralforms,chart
reminderstam
ps,new
sletter,
feedback
onscreeningratesfor
providers.Educatio
nalm
aterials
forpatients(w
ritten,videos).Clin
iclevelchanges
(protocolsforfollo
wup
ofabnorm
alPap
smearsandfor
routinescreening,increasedclinic
hours,im
proved
staffing,upgraded
equipm
ent).
Quasi-experim
ental:
longitu
dinal
nonequivalentcontrol
groupdesign,w
ithindependentrandom
samples
before
andafter
interventio
n
N=18
,642
Predo
minantly
low
incomewom
en.Latino:
57%;African
American:
15%;White:14
%;Other:
14%
2.5years
The
rateof
screeningforcervical
cancerincreasedforthe
interventionsitesvs.contro
lsitesatboththehospital
(adjustedOR3.06,95%
CI
2.07–4.54)
andthecommunity
healthcenterlevels(adjusted
OR2.34,95%
CI1.05–5.23).
Noeffectwas
seen
inthepublic
healthcenters(adjustedOR
1.00,95%
CI0.63–1.56).
OrnsteinSM.
Journalof
Fam
ilyPractice.
1991
.
14Writtenphysicianreminders,
patient
remindersor
both.
Educatio
nsessions
forphysicians,
ahealth
maintenance
flow
sheet,
andchartaudits
inboth
interventio
nandcontrolsites.
Pr-R
Quasi-exp
erim
ental:
before/after
design
Patients:baseline:n=7397;
African
American:61
%;
White:38
%;Other:2%;
Physicians:N=49;race/
ethnicity
datanotcollected
12mon
ths
Allsitesshow
edadecrease
inpercentage
ofpatients
compliantwith
screeningfor
cervicalcancer:physician
reminders-2.1%,p
=0.12;
patient
reminders-4.5
%,p=
0.001,
both
reminders-0.8
%,
p=0.60;control-0.9
%,
p=0.54).
P-R
E-IP
TS
Yancey.
Preventive
Medicine.
1995
.14
Six
videos
abou
tcervical
and
breastcancer
preventio
nwere
show
ncontinuo
usly
inthe
waitin
groom
sof
twoclinics.
E-V
Quasi-exp
erim
ental:
one-week-on
-1-w
eek-
offstud
ydesign
N=1,74
4Predo
minantly
low
incomewom
en.
6mon
ths
The
proportionof
wom
enseen
intheclinicreceivingscreening
was
significantly
higherduring
interventionweeks
than
during
controlw
eeks
(clinic1:26.9%
interventionvs.19.4%
control,
p=0.01;clinic214.6
%interventionvs.10.3%
control,
p=0.02).
Latino:
65%
African
American:21
%White:10
%Other:4%
Ngu
yenBH,et
al.
Journalof
Cancer
Edu
catio
n.20
00.
13Ph
ysicianremindersystem
,health
educationmaterialsforphysicians
togive
patients(w
ritten,videos),
continuing
medicaleducationfor
physicians
includingwritten
materialswith
inform
ationabout
low-costo
ptions
forcare,
newslettersforphysicians,and
access
toinform
ationaboutcancer
treatm
entand
research
for
physicians.
Pr-R
Rando
mized
controlled
trialof
physicians.
Physician
s:n=20
;Vietnam
ese:
100%
3year
intervention
period;post
intervention
followup
notreported
Inmultiv
ariableanalysis,
physicians
intheinterventio
ngrouphadahigher
performance
rateof
cervical
cancer
screeningthan
controls
(p=.004).
E-P
E-V
CME
1023Glick et al.: Cervical Cancer Interventions for MinoritiesJGIM
Table
1.(c
ontinue
d)
Reference
DB
Quality
Score
Intervention
StudyDesign
Sam
ple
size,pop
ulation
Lengthof
Follow-up
Results
Con
tent
Typ
e*
Sox
CH,et
al.
Journalof
Com
mun
ityHealth
.19
99.
13Com
munity
health
aidestrainedto
perform
cervicalcancer
screening.
CHW
Quasi-exp
erim
ental:
before/after
design
N=8villageswith
1098
wom
en;NativeAlaskan:
100%
12mon
ths
The
proportionof
wom
enreceivingaPaptestduring
the
baselineandfollowup
periods
increasedintheintervention
group(0.44+/-0.04
to0.48
+/-
0.05),butnotinthecontrol
group(0.42+/-0.04
to0.39
+/-
0.02).The
change
inproportionbetween
interventionandcontrolgroups
was
notstatisticallysignificant
(p=0.37).
Beach,et
al.
Cancer
Epidemiology,
Biomarkers
and
Prevention.
2007
13Langu
age-concordant
teleph
one
supp
ortforwom
enno
tup
-to-date
onscreening,
includ
ingnavigatio
n.Writteneducationalmaterialswere
mailedto
patients.
RELC
Quasi-exp
erim
ental:
second
aryanalysisof
data
from
arand
omized
controlledtrial
N=1,34
6Predo
minantly
low
incomewom
en18
mon
thsor
until
fully
up-to-date
with
screening
(whichever
camefirst)
For
allwom
en,increased
up-to-date
status
forcervical
cancer
screeningin
interventio
ngrou
pvs.con
trol
grou
p(adjustedOR1.73
,95
%CI1.31
–2.27).Greater
benefitforSpanish-speaking
wom
en(adjustedOR2.18
,95
%CI1.52–3
.13).
E-T
Spanish
speakers:63
%PN
Eng
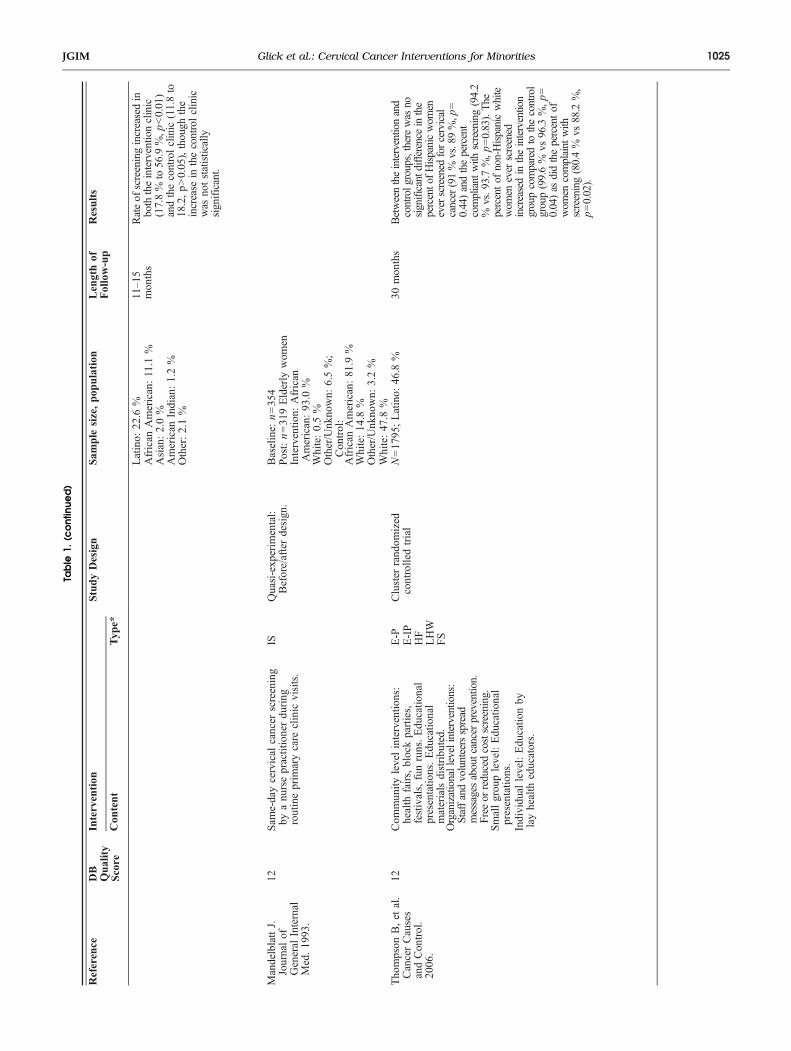
lishspeakers:37
%E-P
Gotay
CC,et
al.
Preventive
Medicine.
2000
.
13Edu
catio
nby
layhealth
educators.
Edu
catio
nalmaterials(w
ritten,
audiov
isual).Vou
chersforfree
screening.
Accessto
awom
en’s
clinic
with
alayhealth
educator
inattend
ance.
LHW
E-IP
Quasi-exp
erim
ental:
prospectivecoho
rtstud
y,usingpo
pulatio
n-based
teleph
onesurveysto
assess
screeningbefore
andafterinterventio
n
N=67
8;NativeHaw
aiians:
100%
3years
The
prop
ortio
nof
wom
encompliant
with
screening
increasedsign
ificantly
(59%
to67
%,p<0.05
)in
the
interventio
ncommun
itybu
tno
tin
thecontrolcommun
ity(63to
64%,p>0.05
).
E-P
E-V
PN
V
Lantz
PM,et
al.
Wom
en’sHealth
Issues.20
09.
12Medicaidexpansionto
cover
treatm
entforpatientsthroug
hthe
BreastandCervicalCancer
PreventionandTreatmentAct
of20
00.
PQuasi-exp
erim
ental:fixed
effects,retrospective
long
itudinaltim
eseries
design
.
N=45
,321
;White:61
.1%
5yearsprior
tothe
interventio
nand5years
afterthe
interventio
n
Propo
rtionof
peop
lescreened
who
hadan
abno
rmal
Pap
test
decreasedforblackwom
enfrom
1995
–00to
2001
–05
(11.9%
to10
.6%,p<0.05
;andincreasedforHispanic
wom
en(22.4%
to22
.7%,p<0.05
).
1024 Glick et al.: Cervical Cancer Interventions for Minorities JGIM
Table
1.(c
ontinue
d)
Reference
DB
Quality
Score
Intervention
StudyDesign
Sam
ple
size,pop
ulation
Lengthof
Follow-up
Results
Con
tent
Typ
e*
Latino:
22.6
%11–15
mon
ths
Rateof
screeningincreasedin
both
theinterventio
nclinic
(17.8%
to56.9%,p
<0.01)
andthecontrolclinic
(11.8to
18.2,p>0.05),though
the
increase
inthecontrolclinic
was
notstatistically
significant.
African
American:11.1
%Asian:2.0%
American
Indian:1.2%
Other:2.1%
MandelblattJ.
Journalof
General
Internal
Med.19
93.
12Sam
e-daycervical
cancer
screening
byanu
rsepractitionerdu
ring
routineprim
arycare
clinic
visits.
ISQuasi-exp
erim
ental:
Before/afterdesign
.Baseline:
n=35
4Post:n=31
9Elderly
wom
enInterventio
n:African
American:93
.0%
White:0.5%
Other/Unk
nown:
6.5%;
Con
trol:
African
American:81
.9%
White:14
.8%
Other/Unk
nown:
3.2%
Tho
mpson
B,et
al.
CancerCauses
andCon
trol.
2006
.
12Com
mun
itylevelinterventio
ns:
health
fairs,blockparties,
festivals,funruns.Edu
catio
nal
presentatio
ns.Edu
catio
nal
materialsdistribu
ted.
E-P
Cluster
rand
omized
controlledtrial
N=17
95;Latino:
46.8
%30
mon
ths
Betweentheinterventionand
controlgroups,therewas
nosignificantdifference
inthe
percentofHispanicwom
eneverscreened
forcervical
cancer(91%
vs.89%,p
=0.44)andthepercent
compliant
with
screening(94.2
%vs.93.7
%,p=0.83).The
percentof
non-Hispanicwhite
wom
enever
screened
increasedin
theintervention
groupcomparedto
thecontrol
group(99.6%
vs96.3
%,p=
0.04)as
didthepercentof
wom
encomplaint
with
screening(80.4%
vs88.2
%,
p=0.02).
Organizationallevelinterventions:
Staffandvolunteersspread
messagesaboutcancerprevention.
Free
orreducedcostscreening.
E-IP
White:47
.8%
Smallgrou
plevel:Edu
catio
nal
presentatio
ns.
HF
Individu
allevel:Edu
catio
nby
layhealth
educators.
LHW
FS
1025Glick et al.: Cervical Cancer Interventions for MinoritiesJGIM
Table
1.(c
ontinue
d)
Reference
DB
Quality
Score
Intervention
StudyDesign
Sam
ple
size,pop
ulation
Lengthof
Follow-up
Results
Con
tent
Typ
e*
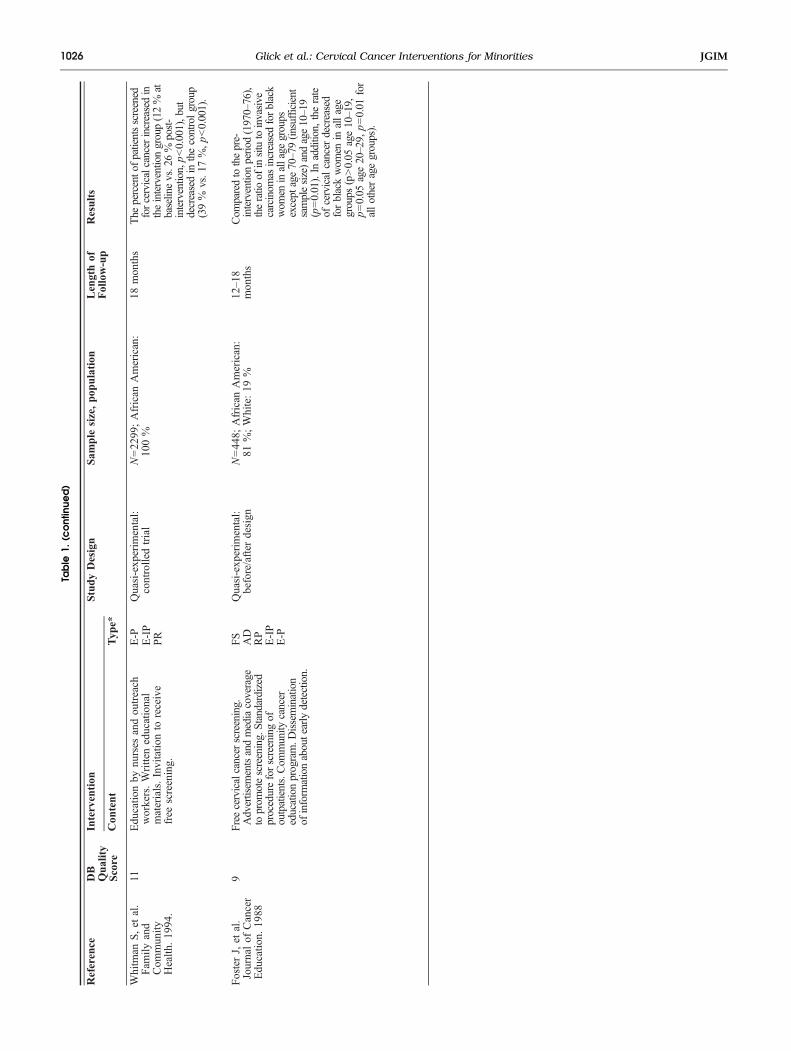
Whitm
anS,et
al.
Fam
ilyand
Com
mun
ityHealth
.19
94.
11Edu
catio
nby
nurses
andou
treach
workers.Writteneducational
materials.Invitatio
nto
receive
free
screening.
E-P
Quasi-exp
erim
ental:
controlledtrial
N=22
99;African
American:
100%
18mon
ths
The
percentofpatientsscreened
forcervicalcancerincreasedin
theinterventiongroup(12%
atbaselinevs.26%
post-
intervention,p<0.001),but
decreasedin
thecontrolgroup
(39%
vs.17
%,p<0.001).
E-IP
PR
FosterJ,et
al.
Journalof
Cancer
Edu
catio
n.19
88
9Free
cervicalcancerscreening.
Advertisem
entsandmediacoverage
toprom
otescreening.Standardized
procedureforscreeningof
outpatients.Com
munity
cancer
educationprogram.D
issemination
ofinform
ationaboutearlydetection.
FS
Quasi-exp
erim
ental:
before/after
design
N=44
8;African
American:
81%;White:19
%12–1
8mon
ths
Com
paredtothepre-
interventionperiod
(1970–76),
theratio
ofinsitutoinvasive
carcinom
asincreasedforblack
wom
eninallage
groups
exceptage70–79(in
sufficient
samplesize)andage10–19
(p=0.01).In
addition,
therate
ofcervicalcancer
decreased
forblackwom
enin
allage
groups
(p>0.05
age10–19,
p=0.05
age20–29,
p=0.01
for
allotheragegroups).
AD
RP
E-IP
E-P
1026 Glick et al.: Cervical Cancer Interventions for Minorities JGIM

appointment with a female nurse practitioner increasesscreening for cervical cancer in minority populations (seeTables 1 and 2). The fair or poor quality of the three otherstudies that addressed a single intervention to improvescreening for cervical cancer in minority populations confersa high risk of bias. Therefore, the strength of evidence forthese interventions is also insufficient (see Tables 1 and 2).Of the studies that evaluated the impact of multiple
interventions, five included education delivered by layhealth workers plus navigation in combination with otherinterventions (educational materials and/or messages in themedia), on the rate of screening for cervical cancer.15,22,23,35,36
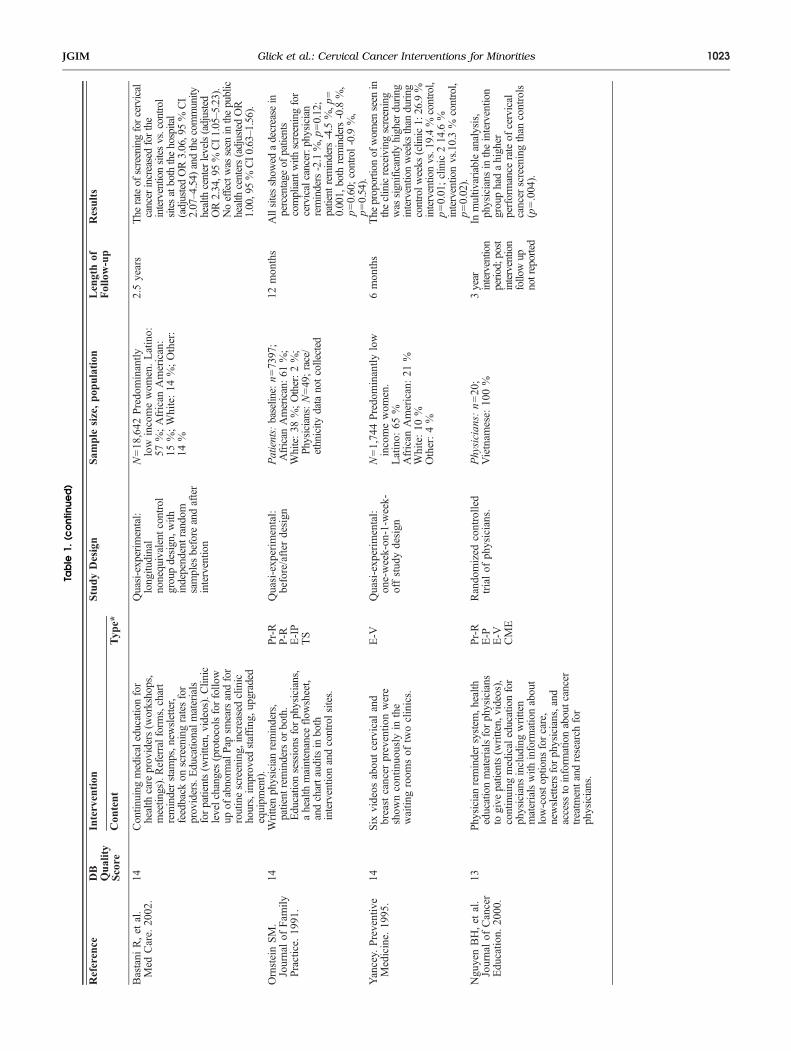
Compared to control, all found an increase in the rate ofscreening for cervical cancer with the intervention. Wangfound a 70 % rate of screening for cervical cancer with theintervention for Chinese American women compared to11.1 % for the control condition (p<0.001).23 Mock foundincreases in the rate of screening for cervical cancer forVietnamese women in both intervention and control groups(intervention 65.8 % to 81.8 %, p<0.001; control 70.1 % to75.5 %, p<0.001).22 The increase in the intervention groupwas significantly greater than that in the control (Z test p=0.001).22 Fernandez found that 39.5 % of Latinas in theintervention group completed screening compared to 23.6 %in the control group (p<0.05).36 However, intention to treatanalysis showed no significant difference in the rate ofscreening.36 Taylor found an increase in Pap testing forChinese women in the interval between randomization andthe follow up survey (37 % vs. 22 %); however, this findingwas not statistically significant.15 Jandorf also found anincrease in the rate of Pap smear screening following theintervention for Latinas that was not statistically significant(51 % vs. 30 %, p=0.0801).35 However, multivariate analysisrevealed a statistically significant adjusted odds ratio of 3.9
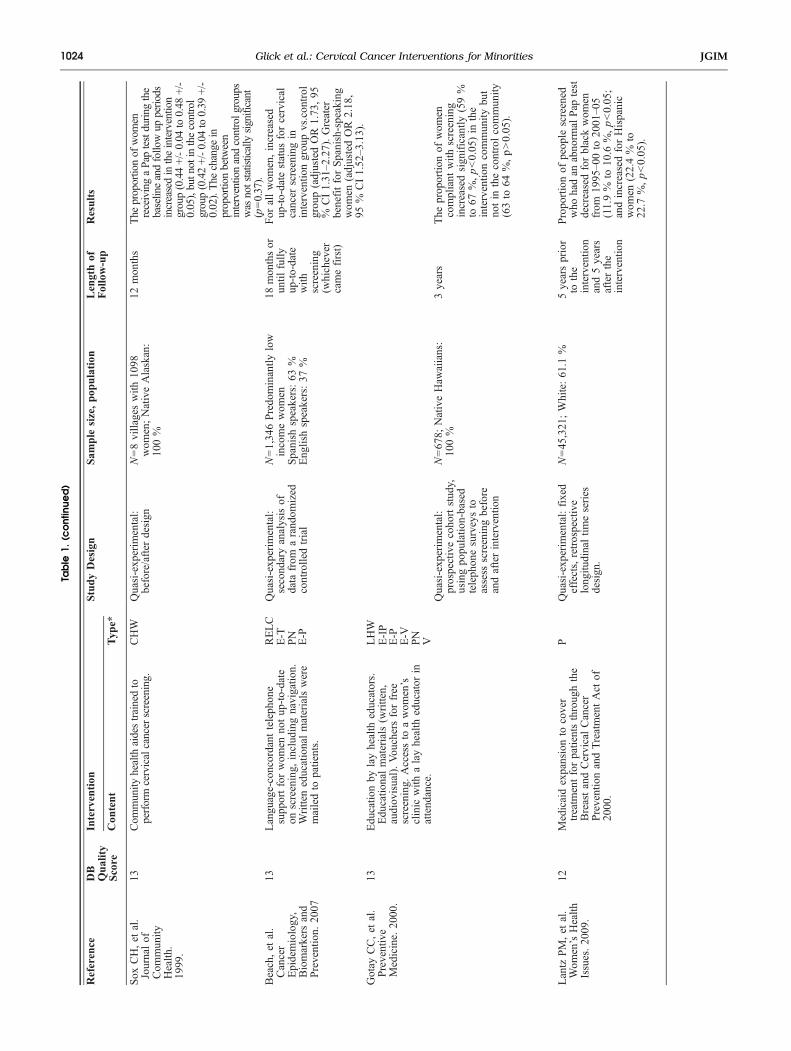
for the effect of the intervention on adherence to screening(95 % CI 1.1–14.1).35 Because of the low risk of bias due tothe presence of multiple good quality studies, the consistencyof study findings, and the imprecise estimates of effect, thestrength of evidence is low that education delivered by layhealth educators together with navigation increases the rate ofscreening for cervical cancer for minority populations(Tables 1 and 2).Two of the studies that evaluated the impact of multiple
interventions on screening for cervical cancer examined theeffect of navigation and telephone support.13,14 One of thesestudies also included written educational materials13; theother did not. Following the intervention, Dietrich found a7 % increase in the proportion of women up to date forcervical cancer screening (95 % CI 0.03–0.11).14 Similarly,Beach found an increase in the up-to-date status for cervicalcancer screening in the intervention group compared to thecontrol group (adjusted odds ratio 1.73, 95 % CI 1.31–2.27).13
The benefit was greater for Spanish-speaking women than forEnglish-speaking women (adjusted OR for Spanish-speakingwomen 2.18, 95 % CI 1.52–3.13; adjusted OR for English-speaking women 1.25, 95 % CI 0.81–1.91).13 Because of thelow risk of bias due to one randomized controlled trial of verygood quality, the consistency of study findings, and theprecise estimate of effect, the strength of evidence is moderatethat telephone support together with navigation increases therate of screening for cervical cancer for minority populations(Tables 1 and 2).The remaining studies that evaluated the impact of
multiple interventions on screening for cervical cancerexamined the effect of unique combinations of interven-tions.18–21,25,26,39,41 Due to the high risk of bias conferredby a single quasi-experimental study of good quality39 or asingle study of fair or poor quality,16,18–21,25,26,37,41 the
Table 2. Strength of Evidence for the Intervention on the Rate of Screening for Cervical Cancer
Intervention Strategy No. of Studies Risk of Bias Consistency Directness Precision Grade
Educational Materials 1 RCT and 3 Quasi-experimental Moderate Inconsistent Direct Imprecise InsufficientLay health advisers offered anappointment to women duefor screening
1 Quasi-experimental High Unknown Direct Imprecise Insufficient
Community health aides trainedto perform cervical cancerscreening
1 Quasi-experimental High Unknown Direct Imprecise Insufficient
Medicaid expansion to covertreatment for patients throughthe Breast and CervicalCancer Prevention andTreatment Act of 2000
1 Quasi-experimental High Unknown Direct Imprecise Insufficient
Same-day cervical cancerscreening by a nursepractitioner during routineprimary care clinic visits
1 Quasi-experimental High Unknown Direct Imprecise Insufficient
Lay health workers plusnavigation
1 RCT, 2 Cluster RCT,2 Quasi-Experimental
Low Consistent Direct Imprecise Low
Telephone support plusnavigation
1 RCT, 1 Quasi-experimental Low Consistent Direct Precise Moderate
1027Glick et al.: Cervical Cancer Interventions for MinoritiesJGIM
Tab
le3.
Intervention
sto
Improve
Follow
Upof
anAbnormal
Pap
SmearforMinorityPop
ulation
s
Reference
DB
Quality
Score
Intervention
StudyDesign
Sam
ple
size,
pop
ulation
Lengthof
Follow-up
Results
Con
tent
Typ
e
Brewster
WR,etal.
Journalof
the
American
medical
Association.
2005.
19Singlevisitfor
Papsm
earandfollo
wup
ofan
abnorm
alresult(H
GSIL,
AGUSor
carcinom
a).
S-T
RCT
N=3521;Latina:79.5
%singlevisit
6–12
mon
ths
Forw
omen
whosePapsm
earrevealedHGSIL/
AGUS,
88%
inthesinglevisitprogram
vs.
53%
intheusualcaregroupweretreated
within6monthsof
diagnosis(p=0.04);in
addition,63
%inthesinglevisitprogram
vs.
21%
intheusualcare
groupreturned
one
year
laterforrecommendedfollow
upPap
testing(p=0.02).
79.1%
usualcare;
White:
16.6%
singlevisit
16.4%
usualcare;
Other:
3.9%
sing
levisit
4.6%
usualcare
Lerman
C,etal.
Journalof
Clinical
Oncology.1992.
16Telephonecounselingtoincrease
adherencetofollowup
andtreatment
amongwom
ennoncom
pliantwith
theirfirstcolposcopy
appointment.
E-T
RCT
N=90;African
American:84.4
%Not
repo
rted
67%
intheinterventiongroupwereadherent
tocolposcopy
comparedto43
%inthe
controlgroup
(p<0.05).The
odds
ofadherenceto
colposcopy
were2.6tim
eshigher
fortheinterventiongroupthan
the
controlgroup(p<0.003).
Latino:
8.9%
White:6.7%
Miller.Journalof
the
NationalCancer
Institute.1997.
16Brieftelephonecounselingfollowing
anabnorm
alPapsm
earwith
orwithouta
boostercallpriorto
colposcopy.
E-T
Quasi-exp
erim
ental:
controlledtrial
N=82
8;African
American:86
%6mon
ths
Com
paredtotelephoneappointment
confirmation,telephonecounselingresulted
inincreasedadherencetotheinitial
colposcopy
appointment(76
%vs.68%,O
R1.50,95%
CI1.04–2.17),and
forattendance
atthe6-monthcolposcopy
appointment(61
%vs.36%,O
R2.70,95%
CI1.15–6.51).
Com
paredtotelephoneappointment
confirm
ation,standard
careresultedin
decreasedadherencetotheinitialcolposcopy
appointment(50
%vs.68%,O
R=0.47,95%
CI0.32–0.73)
anddidnotimpactadherence
torepeat(6
month)colposcopy.
Latino:
6%
White:6%
Other:2%
MarcusAC,et
al.
Medical
Care.
1992
.
14Personalized
follow-upletterand
pamphletoran
audiovisualprogram
onpapsm
earsor
transportation
incentives
(bus
passes/parking
perm
its).
PR
Quasi-exp
erim
ental:
2x2x
2factorial
N=20
44Predom
inantly
low
incomewom
en.
Hispanic41.4%
4mon
ths
Forthetransportationincentiveintervention,
theodds
ratio
ofreturningforfollowup
was
1.48
(95%
CI1.06–2.06).F
orthe
combinationpersonalized
form
letterand
audiovisualintervention,theodds
ratio
ofreturningforfollowup
was
2.30
(95%
CI
1.21–4.34).
E-P
Black
27.7
%
E-V
White
26.7
%
V
Asian
2.7%
Other
1.6%
1028 Glick et al.: Cervical Cancer Interventions for Minorities JGIM
Table
3.(c
ontinue
d)
Reference
DB
Quality
Score
Intervention
StudyDesign
Sam
ple
size,
pop
ulation
Lengthof
Follow-up
Results
Con
tent
Typ
e
LantzPM
,etal.
Wom
en’sHealth
Issues.2009.
12Medicaidexpansiontocover
treatmentfor
patientsthroughthe
Breastand
CervicalC
ancer
PreventionandTreatmentA
ctof
2000.
PQuasi-exp
erim
ental:
fixedeffects,
retrospective
long
itudinaltim
eseries
design
N=45
,321
;White:
61.1
%5yearspriorto
the
interventio
nand5
yearsafterthe
interventio
n.
The
numberof
days
todefinitivediagnosis
decreasedby
12.8%
forwhitewom
en.T
heaveragetim
ebetweenadiagnosisof
cervical
dysplasiaor
cancerandinitiationof
treatm
ent
increasedsignificantly
forBlack
and
Hispanicwom
en.T
heprobabilitythatBlack
wom
enwouldinitiatetreatmentw
ithin60
days
ofacervicalcancerdiagnosisdecreased
9%
(-0.094,95
%CI-0.178
to-0.01).
Latino:
22.6
%African
American:
11.1
%Asian:2.0%
American
Indian:
1.2%
Other:2.1%
MarcusAC,et
al.
11Intensivefollo
wup
,vo
uchers
orbo
th.
PR
Quasi-exp
erim
ental:
2×2factorial
N=14
53Predo
minantly
low
incomewom
en
4–6mon
ths
Com
paredtothecontrolcondition,theodds
ofreturningforfollowup
wereapproximately
50%
higherintheintensivefollowup
(OR
1.56,95%
CI1
.12–2.17,p
<0.01)andin
the
voucherconditions(OR1.50,95
%CI
1.09–2.05,
p<.01).The
combined
interventionwas
notsignificantly
relatedto
follow
upcare
aftertaking
into
accountthe
maineffectsof
both
interventions.
MedicalCare.1998.
V
Latino:
84%
African
American:
7.6%
White:5.8%
Other
2.6%
MichielutteR,etal.
Health
Education
Research.
1994.
11Messagesin
themedia.E
ducatio
nal
materials(w
ritten).E
ducatio
nfor
patientsandthecommunity.
Educatio
nforproviders
(presentations,w
rittenmaterials).
AD
Quasi-experim
ental:
singlegroup,
modifiedtrend
analysis.
N=87
8;African
12–1
8mon
ths
The
%of
blackwom
encompliantwith
follow
upandtreatmentofabnorm
alPaptests
increasedfrom
64%
pre-interventionto79
%post-intervention(p<0.001).
E-P
American:53
.1%
E-IP
White:46
.9%
*E-T=Educatio
ndelivered
bytelephone;PN=Patientnavigatio
n;E-P=Educatio
ndelivered
onprintm
aterials;P
R=Patientreminder;Pr-R=ProviderRem
inder;E-V=Educatio
ndelivered
inavideo;
E-IP=
Educatio
ndelivered
inperson;L
HW=Involvem
entofa
layhealthworker;AD=Public
advertisem
entsdelivered
inprint,television,orradio;RELC
=Patient-providerracial/ethnic/language
concordance;CL=
Learning
colla
borativeor
consortiu
m;TS
=Tracking
system
;CME=Contin
uing
medical
education;
PF=Perform
ance
feedback;RP=Revised
protocols;
CH=Changes
toclinic
hours;
UE=Upgraded
equipm
ent;CHW=Com
munity
Health
Workers;V
=Vouchersforcareor
relatedservices;P
=Changes
tonatio
nalorlocalpolicies;IS=Integrated
screening;HF=Health
fairs;FS=Freeor
lowcostscreening;
S-T=Screen-and-treat
inasinglevisit
1029Glick et al.: Cervical Cancer Interventions for MinoritiesJGIM

strength of evidence is insufficient that these combinationsof interventions improve the rate of screening for cervicalcancer in minority populations (Tables 1 and 2).
Interventions to Improve Diagnosisor Treatment
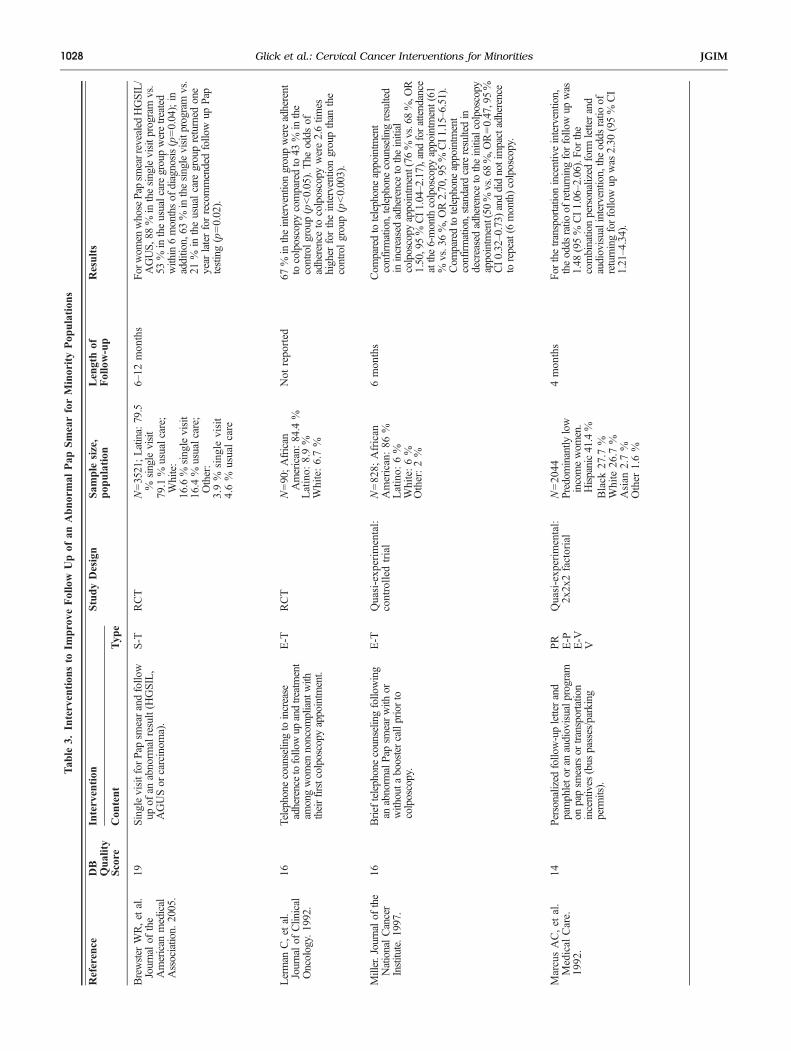
Of the seven studies that evaluated the impact of interventionsto improve the diagnosis or treatment of premalignant diseaseof the cervix, four evaluated the impact of a singleintervention27–29,42 and three evaluated the impact of acombination of interventions.24,30,31 In a randomized con-trolled trial, Brewster evaluated a single visit for bothscreening for cervical cancer and follow up of an abnormalresult (High-Grade Squamous Intraepithelial Lesion (HGSIL),Atypical Glandular Cells of Uncertain Significance (AGUS)or carcinoma).29 She found that for women whose Pap smearrevealed HGSIL/AGUS, 88 % in the intervention group weretreated within six months of diagnosis compared to 53 % inthe usual care group (p=0.04).29 Because of the low risk ofbias given the study design and quality for this single study,the direct measurement of outcomes, and the precision of theestimate, the strength of evidence is low that a single visit forscreening for cervical cancer and follow up of an abnormalresult results in improvement in the diagnosis and treatmentof premalignant disease of the cervix in minority populations(Tables 3 and 4).Two studies assessed the impact of telephone counseling
on the diagnosis and treatment of premalignant disease ofthe cervix.27,28 Compared to the control group, Lermanfound the odds of adherence to colposcopy were 2.6 timeshigher for the intervention group (p<0.003).27 Miller foundthat compared to telephone appointment confirmation,telephone counseling resulted in increased adherence tothe initial colposcopy appointment (76 % vs. 68 %, OR1.50, 95 % CI 1.04–2.17), and for attendance at the six-month colposcopy appointment (61 % vs. 36 %, OR 2.70,95 % CI 1.15–6.51).28 Given the moderate risk of bias dueto one randomized controlled trial and one quasi-experi-mental study of good quality, the consistency of thefindings, and the precision of the estimate, the strength ofevidence is low that telephone counseling increases thediagnosis and treatment of premalignant lesions of thecervix for minority women (Tables 3 and 4).
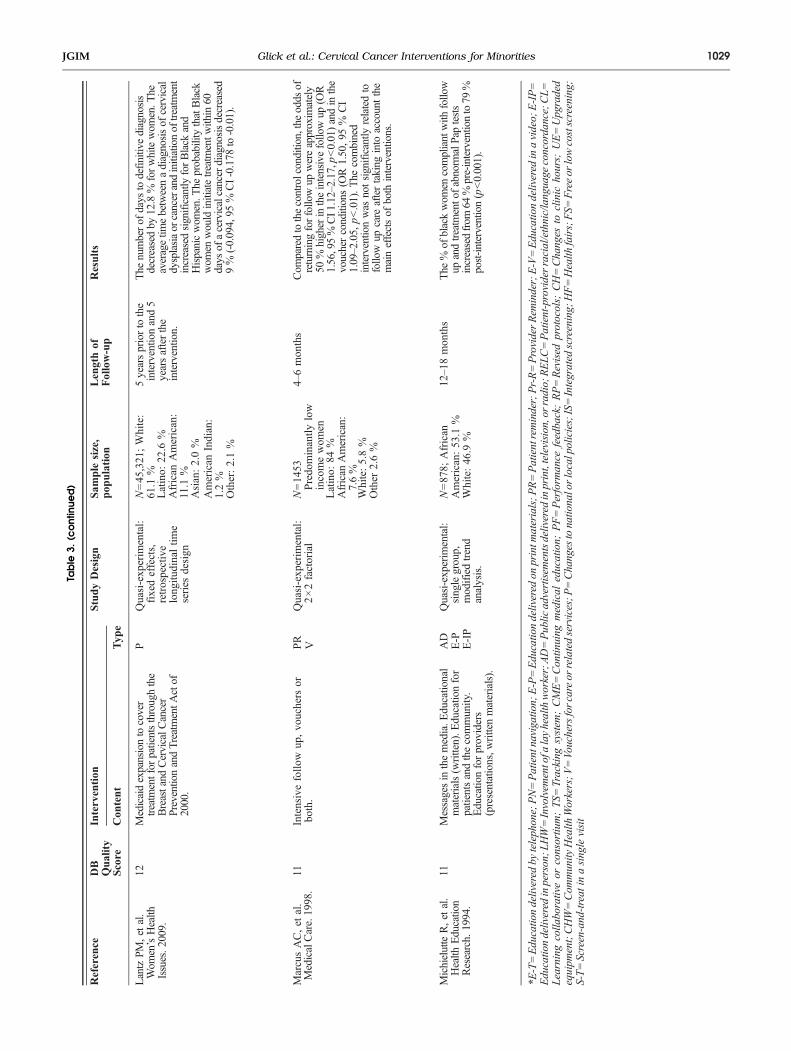
One study evaluated the impact of Medicaid expansion tocover treatment for patients diagnosed with malignant orpremalignant disease of the cervix through the NationalBreast and Cervical Cancer Early Detection Program.42 Dueto the high risk of bias conferred by a single quasi-experimental study of fair quality and the lack of precisionaround the estimates, the strength of evidence is insufficientthat this intervention improves the diagnosis or treatment ofpremalignant disease of the cervix in minority populations(Tables 3 and 4).The three studies that evaluated the impact of multiple
interventions on screening for cervical cancer examined theeffect of unique combinations of interventions.24,30,31 Dueto the high risk of bias conferred by a single quasi-experimental study of fair quality, the strength of evidenceis insufficient that these combinations of interventionsimprove the diagnosis or treatment of premalignant diseaseof the cervix in minority populations.
DISCUSSION
Summary of Results
This systematic review found a moderate strength ofevidence that telephone support with navigation increasesthe rate of screening for cervical cancer in minoritypopulations. The strength of evidence is low that educationdelivered by lay health educators with navigation increasesthe rate of screening for cervical cancer in minoritypopulations. For all of the other interventions andcombinations of interventions studied, the strength ofevidence is insufficient that these interventions improvethe rate of screening for cervical cancer in minoritypopulations.This systematic review also found a low strength of
evidence that a single visit for screening for cervical cancerand follow up of an abnormal result improves the diagnosisand treatment of premalignant disease of the cervix inminority populations. In addition, the strength of evidenceis low that telephone counseling increases the diagnosis andtreatment of premalignant lesions of the cervix for minoritywomen. For all of the other interventions and combinationsof interventions studied, the strength of evidence isinsufficient that these interventions improve the diagnosis
Table 4. Strength of Evidence for the Intervention on the Diagnosis and Treatment of Premalignant Disease of the Cervix
Intervention strategy No. of studies Risk of bias Consistency Directness Precision Grade
Single visit for screening andfollow up
1 RCT Low Unknown Direct Precise Low
Telephone counseling 1 RCT, 1 Quasi-experimental Moderate Consistent Direct Precise LowMedicaid expansion to covertreatment for patients throughthe Breast and Cervical CancerPrevention and TreatmentAct of 2000
1 Quasi-experimental High Unknown Direct Imprecise Insufficient
1030 Glick et al.: Cervical Cancer Interventions for Minorities JGIM

and treatment of premalignant lesions of the cervix forminority women.
Implications
For clinicians, administrators, policy makers and othersstriving to improve the rate of screening for cervical cancerin minority populations, telephone support with navigationand education programs by lay health educators withnavigation may be of benefit. Telephone support withnavigation has been shown to be effective for bothSpanish-speaking and English-speaking populations.13,14
Education programs led by lay health educators togetherwith navigation have been shown to be effective for Latina,Chinese and Vietnamese populations.22,23,36
A single visit for screening for cervical cancer and followup of an abnormal result may improve the diagnosis andtreatment of premalignant disease of the cervix for minoritypopulations, as may telephone counseling. A single visit forscreening and follow up was evaluated in a population thatwas predominantly Latina; therefore, its findings are mostapplicable to this group. Telephone counseling was evaluatedin a population that was predominantly African American;therefore, its conclusions are directly applicable to this group.
Limitations of the Systematic Review Process
Our search strategy may have overlooked studies that reporteddata on racial and ethnic minorities, but did not focus on thesepopulation groups. However, we feel this is unlikely becauseour search identified studies that focused on populations otherthan racial or ethnic minorities, such as women attending acommunity health clinic or low-income women.Because our aim was to evaluate the effectiveness of
interventions that linked participants to the health caresystem, we deliberately excluded 21 studies that failed to doso. While it is possible that inclusion of these studies wouldhave altered our findings, these studies were outside thescope of our systematic review.44
Though the original DB score has been validated and theuse of DB to categorize studies qualitatively has beendescribed,43 the use of this strategy to classify studies asvery good, good, fair or poor has not yet been validated.Therefore, it is possible that we have misclassified somestudies, especially those near the cut point for a qualitativescore. However, because we were conservative in ourestimate of risk of bias when determining the strength ofevidence, if misclassification were to have affected ourresults, it would have biased our findings toward the null.We neither searched for unpublished studies nor contacted
authors about potential unpublished subgroup analyses. Thus,the results of our review may be influenced by publicationbias and might bias our findings away from the null.
Recommendations for Future Research
While navigation seems a core element of the interventionsthat improve screening for cervical cancer in minoritypopulations, there is insufficient evidence to determinewhether navigation alone improves this outcome. Because asingle intervention may be more easily implemented and lesscostly than one that includes multiple elements, it isimportant to determine whether navigation alone improvesscreening for cervical cancer, as well as the added costs andbenefits of adding lay health education or telephone support.In addition, because the combination of navigation andeducation programs conducted by lay health educators havebeen inadequately studied in African Americans or NativeAmericans, future research should fill this gap. As navigationin conjunction with telephone support has been inadequatelystudied in populations that speak languages other thanEnglish or Spanish, further studies should confirm that thiscombination of interventions is effective in these populations.Interventions with the potential to improve the diagnosis
and treatment of premalignant lesions of the cervix areunderstudied. Future research should seek to extend thefindings of the Brewster study29 to additional populations,especially African Americans, Asian Americans and NativeAmericans. In addition, future research should confirm theeffect of telephone counseling in additional populations,notably Latinas, Asian Americans and Native Americans.
Funding Source: Support was provided by a grant from the RobertWood Johnson Foundation’s Finding Answers: Disparities Researchfor Change Program. The content is solely the responsibility of theauthors and does not necessarily represent the official views of theRobert Wood Johnson Foundation or of Finding Answers: DisparitiesResearch for Change Program.
Conflict of Interest: The authors declare that they do not have aconflict of interest.
Corresponding Author: Susan B. Glick, MD; Department ofMedicine, Section of General Internal Medicine, University ofChicago, Chicago, IL 60637, USA (e-mail: [email protected]).
REFERENCES1. Surveillance Epidemiology and End Results. SEER Stat Fact Sheet:
Cervix Uteri. Available at: http://seer.cancer.gov/statfacts/html/cervix.html. Accessed March 8, 2012.
2. U.S. Cancer Statistics Working Group. United States Cancer Statistics:1999–2007 Incidence and Mortality Web-based Report. Atlanta (GA):Department of Health and Human Services, Centers for Disease Controland Prevention, and National Cancer Institute; 2010.
3. Freeman HP, Wingrove BK. Excess Cervical Cancer Mortality: A Markerfor Low Access to Health Care in Poor Communities. Rockville, MD:National Cancer Institute, Center to Reduce Cancer Health Disparities,May 2005. NIH Pub. No. 05–5282.
4. Jemal A, et al. Cancer Statistics, 2004. CA Cancer J Clin. 2004;54:30–40.
5. American Cancer Society. Cancer Facts and Figures for Hispanics 2006–8. American Cancer Society 2006.
6. Howe HL, Wu X, Rus LA, et al. Annual report to the nation on the statusof cancer, 1975–2003, featuring cancer among US Hispanic/Latinopopulations. Cancer. 2006;107(8):1711–42.
1031Glick et al.: Cervical Cancer Interventions for MinoritiesJGIM

7. Walbloomers JMM. Human papillomavirus is a necessary cause ofinvasive cervical cancer worldwide. J Pathol. 1999;189(1):12–19.
8. Brawley O. Some perspective on black-white cancer statistics. CACancer J Clin. 2002;52:322–5.
9. Downs SH, Black N. The feasibility of creating a checklist for theassessment of the methodological quality both of randomized and non-randomised studies of health care interventions. J Epidemiol Commu-nity Health. 1998;52:377–384.
10. Higgins JPT, Green S (editors). Cochrane Handbook for SystematicReviews of Interventions Version 5.0.2 [updated September 2009]. TheCochrane Collaboration, 2009. Available at: www.cochrane-handbook.org. Accessed March 8, 2012.
11. Chin MH, Walters AE, Cook SC, Huang ES. Robert Wood JohnsonFoundation Finding Answers: Disparities Research for Change System-atic Review Leadership Team Health Disparities. Medical Care Researchand Review: Special Supplemental Issue. 2007;64(5) supplement.
12. Yancey AK, Walden L. Stimulating cancer screening among Latinas andAfrican-American women. A community case study. J Canc Educ.1994;9(1):46–52.
13. Beach ML, Flood AB, Robinson CM, Cassells AN, Tobin JN, Greene MA,et al. Can language-concordant prevention care managers improve cancerscreening rates? Canc Epidemiol Biomarkers Prev. 2007;16(10):2058–64.
14. Dietrich AJ, Tobin JN, Cassells A, Robinson CM, Greene MA, Sox CH,et al. Telephone care management to improve cancer screening amonglow-income women: a randomized, controlled trial. Ann Intern Med.2006;144(8):563–71.
15. Taylor VM, Hislop TG, Jackson JC, Tu S-P, Yasui Y, Schwartz SM, etal. A randomized controlled trial of interventions to promote cervicalcancer screening among Chinese women in North America. J NatlCancer Inst. 2002;94(9):670–7.
16. Whitman S, Lacey L, Ansell D, Dell J, Chen E, Phillips CW. Anintervention to increase breast and cervical cancer screening in low-incomeAfrican-American women. Fam Community Health. 1994;17(1):56–63.
17. Mandelblatt J, Traxler M, Lakin P, Thomas L, Chauhan P, MatseoaneS, et al. A nurse practitioner intervention to increase breast and cervicalcancer screening for poor, elderly black women. The Harlem Study Team.J Gen Intern Med. 1993;8(4):173–8.
18. Bastani R, Berman BA, Belin TR, Crane LA, Marcus AC, Nasseri K, etal. Increasing cervical cancer screening among underserved women in alarge urban county health system: can it be done? What does it take?Med Care. 2002;40(10):891–907.
19. Nguyen BH, Nguyen K, McPhee SJ, Nguyen AT, Tran DQ, JenkinsCNH. Promoting cancer prevention activities among Vietnamese physi-cians in California. J Canc Educ. 2000;15(2):82–5.
20. Rimer BK, Conaway M, Lyna P, Glassman B, Yarnall KS, Lipkus I, etal. The impact of tailored interventions on a community health centerpopulation. Patient Educ Couns. 1999;37(2):125–40.
21. Gotay CC, Banner RO, Matsunaga DS, Hedlund N, Enos R, Issell BF, etal. Impact of a culturally appropriate intervention on breast and cervicalscreening among native Hawaiian women. Prev Med. 2000;31(5):529–37.
22. Mock J, McPhee SJ, Nguyen T, Wong C, Doan H, Lai KQ, et al.Effective lay health worker outreach and media-based education forpromoting cervical cancer screening among Vietnamese Americanwomen. Am J Public Health. 2007;97(9):1693–700.
23. Wang X, Fang C, Tan Y, Liu A, Ma GX. Evidence-based intervention toreduce access barriers to cervical cancer screening among underservedChinese American women. J Wom Health. 2010;19(3):463–9. 15409996.
24. Michielutte R, Dignan M, Bahnson J, Wells HB. The Forsyth CountyCervical Cancer Prevention Project–II. Compliance with screeningfollow-up of abnormal cervical smears. Health Educ Res. 1994;9(4):421–32.
25. Paskett ED, Tatum CM, D'Agostino R Jr, Rushing J, Velez R,Michielutte R, et al. Community-based interventions to improve breast andcervical cancer screening: results of the Forsyth County Cancer Screening(FoCaS) Project. Canc Epidemiol Biomarkers Prev. 1999;8(5):453–9.
26. Foster JD, Holland B, Louria DB, Stinson L. In situ/invasive cervicalcancer ratios: impact of cancer education and screening. J Canc Educ.1988;3(2):121–5.
27. Lerman C, Hanjani P, Caputo C, Miller S, Delmoor E, Nolte S, et al.Telephone counseling improves adherence to colposcopy among lower-income minority women. J Clin Oncol. 1992;10(2):330–3.
28. Miller SM, Siejak KK, Schroeder CM, Lerman C, Hernandez E, HelmCW. Enhancing adherence following abnormal Pap smears among low-income minority women: a preventive telephone counseling strategy. JNatl Cancer Inst. 1997;89(10):703–8.
29. Brewster WR, Hubbell FA, Largent J, Ziogas A, Lin F, Howe S, et al.Feasibility of management of high-grade cervical lesions in a single visit:a randomized controlled trial. Jama. 2005;294(17):2182–7.
30. Marcus AC, Kaplan CP, Crane LA, Berek JS, Bernstein G,Gunning JE, et al. Reducing loss-to-follow-up among women withabnormal Pap smears. Results from a randomized trial testing anintensive follow-up protocol and economic incentives. Med Care.1998;36(3):397–410.
31. Marcus AC, Crane LA, Kaplan CP, Reading AE, Savage E, Gunning J,et al. Improving adherence to screening follow-up among women withabnormal pap smears: results from a large clinic-based trial of threeintervention strategies. Med Care. 1992;30(3):216–30.
32. Jibaja–Weiss ML, Volk RJ, Smith QW, Holcomb JD, Kingery P.Differential effects of messages for breast and cervical cancer screening.J Health Care Poor Underserved. 2005;16(1):42–52.
33. Rivers SE, Salovey P, Pizarro DA, Pizarro J, Schneider TR. Messageframing and Pap test utilization among women attending a communityhealth clinic. J Heal Psychol. 2005;10(1):65–77.
34. Margolis KL, Lurie N, McGovern PG, Tyrrell M, Slater JS. Increasingbreast and cervical cancer screening in low-income women. J Gen InternMed. 1998;13(8):515–21.
35. Jandorf L, Bursac Z, Pulley L, Trevino M, Castillo A, Erwin DO. Breastand cervical cancer screening among Latinas attending culturallyspecific educational programs. Prog Community Health Partnersh.2008;2(3):195–204.
36. Fernandez ME, Gonzales A, Tortolero-Luna G, Williams J, Saavedra-Embesi M, Chan W, et al. Effectiveness of Cultivando la Salud: a breastand cervical cancer screening promotion program for low-incomeHispanic women. Am J Public Health. 2009;99(5):936–43.
37. Thompson B, Coronado G, Chen L, Islas I. Celebremos la salud! acommunity randomized trial of cancer prevention (United States). CancCauses Contr. 2006;17(5):733–46.
38. Sox CH, Dietrich AJ, Goldman DC, Provost EM. Improved access towomen's health services for Alaska natives through community healthaide training. J Community Health. 1999;24(4):313–23.
39. Suarez L, Roche RA, Pulley LV, Weiss NS, Goldman D, Simpson DM.Why a peer intervention program for Mexican-American women failed tomodify the secular trend in cancer screening. Am J Prev Med. 1997;13(6):411–7.
40. Jibaja–Weiss ML, Volk RJ, Kingery P, Smith QW, Holcomb JD.Tailored messages for breast and cervical cancer screening of low-incomeand minority women using medical records data. Patient Educ Couns.2003;50(2):123–32.
41. Ornstein SM, Garr DR, Jenkins RG, Rust PF, Arnon A. Computer-generated physician and patient reminders. Tools to improve popula-tion adherence to selected preventive services. J Fam Pract. 1991;32(1):82–90.
42. Lantz PM, Soliman S. An evaluation of a Medicaid expansion for cancercare: the Breast and Cervical Cancer Prevention and Treatment Act of2000. Wom Health Issues. 2009;19(4):221–31.
43. Peek ME, Cargill A, Huang ES. Diabetes health disparities: asystematic review of health care interventions. Med Care Res Rev.2007;64:101S–156S.
44. Chin MH, Clarke AR, Nocon RS, Casey AA, Goddu AP, Keesecker NM,Cook SC. A Roadmap and Best Practices for Organizations to ReduceRacial and Ethnic Disparities in Health Care. J Gen Intern Med. 2012;doi:10.1007/s11606-012-2082-9.
45. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality ofevidence and strength of recommendations. BMJ 2008;336:924–926
46. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, SchunemannHJ. GRADE: what is “quality of evidence” and why is it important toclinicians? BMJ 2008;336:995–998.
47. Carmichael JA, Jeffrey JF, Steele HD, Ohlke ID. The cytologic historyof 245 patients developing invasive cervical carcinoma. Am J ObstetGynecol. 1984;148(5):685–90.
48. Janerich DT, Hadjimichael O, Schwartz PE, Lowell DM, Meigs JW,Merino MJ, Flannery JT, Polednak AP. The screening histories ofwomen with invasive cervical cancer, Connecticut. Am J Public Health.1995;85(6):791–4.
49. American Cancer Society. Cancer Prevention & Early Detection Facts &Figures 2011. Atlanta: American Cancer Society; 2011.
50. Centers for Disease Control and Prevention. [Surveillance of Screening-Detected Cancers (Colon and Rectum, Breast, and Cervix) — UnitedStates, 2004–2006]. MMWR 2010; 59(No. SS-9): 2.
1032 Glick et al.: Cervical Cancer Interventions for Minorities JGIM