certified professional soil scientist application incomplete ... or crime for which circumstances...
TRANSCRIPT

Certified ProfessionalSoil Scientist
CPSS
Certified Professional Soil ScientistApplication
In order to qualify for certification, one of the two points below must be met (for full CPSS certification, not APSS):
1. Hold a Bachelor’s degree in Soil Science or closely related Agricultural, Earth, or Environmental Science (e.g., a named option in Soil Science, minor in Soil Science) and 5 years of work experience.
Or2. Hold a MS or PhD degree in Soil Science or closely related Agricultural, Earth, or Environmental Science (e.g., a named option in Soil Science, minor in Soil Science) and 3 years of work experience.
If you are applying for the APSS, you must meet the education requirements above and be working toward the work experience requirement.
Note: Incomplete applications will be returned to the applicant without review.
As of February 1, 2012, all new applications received must be on the new application and meet the new requirements.

2
Application for Professional Certification5585 Guilford Road • Madison, WI 53711-5801 • (608) 268-4955 • FAX (608) 273-2081 • www.soils.org/certifications
Have you ever been charged, indicated or convicted of a felony, misdemeanor,or crime for which circumstances relate to being a soil scientist or soil classifier? ❑ Yes ❑ No If yes, attach an explanation.
5. FEES:
Application Fee $75
FEE ENCLOSED $ ______________________ (Fee is non-refundable)
MAKE CHECK PAYABLE TO: SOIL SCIENCE SOCIETY OF AMERICA (Payment must be in U.S. funds)
2. PERSONAL DATA (Completion of this section is optional. Informa tion re-garding specific individual members will not be released.)
Birthdate ______________________ Race ______________________
Citizenship _____________________ Gender ____________________
3. AREA OF CERTIFICATION APPLYING FOR
❑ Currently certified as __________________________ and applying for: (CCA, CCA-CPAg, APSS, or N/A)
Area of Certification
❑ Certified Professional Soil Scientist, CPSS ❑ Associate Professional Soil Scientist, APSS
4. DOCUMENTATION REQUIRED:
a. Completed Core Requirement Form documenting educational background in-cluding: institution, degree(s), major, and minor areas, and course work.
b. An Official Transcript of all academic credits and including verification of degree(s).
c. Completed Professional Experience Form. List all professional positions held, professional activities, and membership and offices held in professional and honorary societies.
d. Completed Core Summary Form.e. Resume.f. Signed and dated Code of Ethicsg. References: 1. For Certified Professional Applications refer to I.B.3. 2. For Associate Professional Applications refer to II.C.1.(3).
The following credit cards are accepted:
❑ MasterCard ❑ Visa ❑ Discover ❑ AMX
Card Number
Expiration Date
Cardholder’s Name
Please Print Name
Certified ProfessionalSoil Scientist
CPSS
1. APPLICANT’S NAME AND ADDRESSPlease print or type:
❑ Dr. ❑ Mr. ❑ Ms.
Last Name/Surname _______________________________________________________________________________________
First Name/Given Name _______________________________________ Middle Name _____________________________
Address _________________________________________________________________________________________________________________________________
Address __________________________________________________________________________ County (U.S. only) _______________________________________
City ________________________________________ State/Province ________________ Postal Code________________________ Country ______________________
Office Phone ______________________________ Home Phone ___________________________________ FAX ____________________________________________
Cell Phone _______________________________ Email ___________________________________________________________________________________________
Office Use Only
Certification No.
6. NAME TO BE PRINTED ON CERTIFICATE:
Degree following name: (choose only one)—optional
❑ BS ❑ BA ❑ MS ❑ PhD ❑ Other _________________
Last Name/Surname
First Name/Given Name
Middle Name

8. PLEASE LIST NAME AND ADDRESS OF PRESENT EMPLOYER:
9. DIRECTORY OF CONSULTANTS
A directory of certified individuals is located on the web at:http://www.soils.org/certification/directory/
Would you like to be included?
❑ Yes ❑ No
10. SIGNATURE
I hereby certify that all information submitted in support of this application is correct and true to the best of my knowledge and that all information re-garding this application will remain confidential. I have read and signed the Code of Ethics.
Date Signature of Applicant
3
7. PROFESSIONAL EXPERTISE:
Please choose one or more categories in which you can substantiate that you are technically and professionally qualified to practice. Place the category code that you feel the most technically and professionally qualified to prac-tice in the first choice and the next most qualified in the second choice and so on up to four choices.
1. __________ 2. __________ 3. __________ 4. __________
Acid-Sulfate Soils—S2Agricultural Administration—P3Agricultural Climatology—ElAgricultural Development—F2Agro-forestry—X0Agronomic Education—P1Agronomic Management—FlAgronomy (general)—AlBest Management Practices—F4Biometrics—A3Biotechnology—ClCell Biology—C2Computer Assisted Design—B5Computer Modeling—B4Computer Uses—BlConservation Education—P2Conservation Planning, Food Security
Act 1985—F5Comprehensive Nutrient Management—N4Conservation Tillage—D6Crop Breeding—JlCrop Chemistry—K5Crop Cytogenetics—J5Crop Ecology—L1Crop Genetics—J7Crop Marketing—L3Crop Metabolism—KlCrop Physiology—K3Crop Production—L4Crop Protection—L6Crop Quality—O1Crop Science—I1Crop Specialization–Cannery Crops—P4Crop Specialization–Corn—P5Crop Specialization–Cotton—P6Crop Specialization–Grazing—P7Crop Specialization–Rice—P8Crop Specialization–Small Grains—P9Crop Specialization–Soybean—Q2Crop Specialization–Tobacco—Q3Crop Specialization–Tree Fruit—Q4Crop Specialization–Vegetable—Q5Crop Specialization–Wheat—Q6Crop Utilization—O2Cytology—J3Digitized Mapping—B3Edaphology—U3Entomology—L9Environmental Protection—E3Environmental Regulation—E2Ethics—E9Farm Management—F6Farmland Preservation—F3Fertilizer Technology—YlFertilizer Use—Y3Floriculture—H3Floristry—H4Forages—N2Forest Soils—XlGarden Center Management—I7Genetics—J9Greenhouse Production—H2Ground Water Quality—G7Hazardous Waste Management—G2Horticulture (General)—H1Hydric Soils—R4Impact Assessment—E4Information Systems—B2International Agronomy—I4International Horticulture—I6Irrigation—RlIrrigation and Drainage—R2Labor Management—F7Land Classification—V8Land Management—DlLand Resource Analysis—V6
Land Resource Development—V7Land Use—D2Land Use Planning—D5Molecular Cytogenetics—C4Molecular Genetics—C3Nursery Management—I8Nutrient Management—N3Olericulture—H6Organic—O3Ornamental Horticulture—H9Pedology—U6Pest Management—L7Pesticide Use—L8Plant Breeding—J2Plant Chemistry—K6Plant Ecology—L2Plant Cytogenetics—J6Plant Cytology—J4Plant Genetics—J8Plant Metabolism—K2Plant Nutrition—UlPlant Pathology—I5Plant Physiology—K4Plant Propagation—K7Plant Taxonomy—K8Pollution Control—G6Pomology—H5Post-Harvest Physiology—H7Product R&D—W3Range Management—X6Range Soil Science—X3Reclamation—W8Regulatory Admin./Enforcement—E5Regulatory Compliance—E6Resource Conservation—D4Saline Soils—R5Seed Production—MlSeed Technology—M3Small Fruit Culture—I9Soil Biochemistry—TlSoil Chemistry—SlSoil Erosion Sediment Control—W5Soil Fertility—U2Soil Genesis—VlSoil Interpretations—V2Soil Management—W7Soil Microbiology—T2Soil Mineralogy—Z1Soil Morphology/Classification—V3Soil Physics—R3Soil Plant Analysis—U4Soil-Plant Correlation—U7Soil Science—Q1Soil-Water-Plant Relation—U5Soil Resource Inventory—V4Soil Survey—V5Soil and Waste Management—GlSoil and Water Conservation—W1Soil and Water Management—W2Statistical Analysis—B6Streambank Stabilization—W6Surface Mine Reclamation—W4Tissue Culture—C5Tropical Agriculture—I3Tropical Crops—I2Turfgrass Management—NlViticulture—H8Waste Disposal, On-site—G3Waste, Land Treatment/Applic.—G5Waste Management—G4Water Diversion and Control—W9Weed Control—LOWeed Science—L5Wetlands Identification—WOWildlife Management—X2Undefined, Other—Z9
If you have questions on completing this application,please contact Marta Krist at
or at 608-268-4955

4
I, the undersigned, agree to adhere to the above Code of Ethics.
Signature:_________________________________________________________ Date____________________________
Please Print Name__________________________________________________
Article I. Preamble1. The privilege of professional practice imposes obligations of
responsibility as well as professional knowledge. The Soil Science Society of America (SSSA) certifies the credentials of individu-als through the Soils Certifying Board, which is the national soil science certification board. Individuals who meet the requirements for soil science certification will receive the designation of Cer-tified Professional Soil Scientist (CPSS) or Certified Professional Soil Classifier (CPSC). The soil science certification program will only award the title of CPSS/CPSC to individuals who have met the examination, education, experience and ethics requirements as set forth by the SSSA Soils Certifying Board.
2. The Soils Certifying Board will award the title of CPSS to indi-viduals who meet the college education, experience, testing re-quirements, ethics and the continuing education requirements of the Soils Certifying Board. CPSC was no longer issued after 2011. Existing CPSC still apply.
3. A CPSS/CPSC, at the request of a client or employer, must disclose the information used to gain certification. CPSS/CPSC who know-ingly misrepresents their credentials will face disciplinary action.
Article II. Relation of Professional to the Public 1 A CPSS/CPSC shall avoid and discourage sensational, exaggerat-
ed, and/or unwarranted statements that might induce participation in unsound enterprises.
2 A CPSS/CPSC shall not give professional opinion or make a rec-ommendation without being as thoroughly informed as might rea-sonably be expected considering the purpose for which the opinion or recommendation is desired, and the degree of completeness of information upon which the opinion is based should be made clear.
3 A CPSS/CPSC shall not issue a false statement or false information even though directed to do so by employer or client.
Article III. Relation of Professional to Employer and Client
1. A CPSS/CPSC shall protect, to the fullest extent possible, the interest of his/her employer or client insofar as such interest is con-sistent with the law and professional obligations and ethics.
2. A CPSS/CPSC who finds that obligations to their employer or cli-ent conflict with their professional obligation or ethics should work to have such objectionable conditions corrected.
3. A CPSS/CPSC shall not use, directly or indirectly, an employer’s or client’s information in any way that would violate the confidence of the employer or client.
4. CPSS/CPSC retained by one client shall not accept, without the client’s written consent, an engagement by another if the interests of the two are in any manner conflicting.
5. A CPSS/CPSC who has made an investigation for any employer or client shall not seek to profit economically from the informa-tion gained, unless written permission to do so is granted or until it is clear that there can no longer be a conflict of interest with the original employer or client.
6. A CPSS/CPSC shall not divulge information given in confidence. 7. A CPSS/CPSC shall engage, or advise employer or client to en-
gage, and cooperate with other experts and specialists. 8. A CPSS/CPSC protects the interests of a client by recommending
only products and services that are in the best interest of the client and public.
9. A CPSS/CPSC protects his/her credibility by disclosing to clients how he/she will be compensated for providing recommendations to the client.
Article IV. Relation of Professionals to Each Other 1. A CPSS/CPSC shall not falsely or maliciously attempt to injure the
reputation of another. 2. A CPSS/CPSC shall freely give credit for work done by others, to
whom the credit is due, and shall refrain from plagiarism of oral and written communications and shall not knowingly accept credit rightfully due another person.
3. A CPSS/CPSC shall not use the advantage of public employment (i.e., university, government) to compete unfairly with other certi-fied professions.
4. A CPSS/CPSC shall endeavor to cooperate with others in the profession and encourage the ethical dissemination of technical knowledge.
Article V. Duty to the Profession 1. A CPSS/CPSC shall aid in exclusion from certification those who
have not followed this Code of Ethics or who do not have the re-quired education and experience.
2. A CPSS/CPSC shall uphold this Code of Ethics by precept and example and encourage, by counsel and advice, other Registrants to do the same.
3. A CPSS/CPSC having positive knowledge of deviation from this Code by another Registrant shall bring such deviation to the atten-tion of the Soils Certifying Board.
Soils Certifying Board 8/11
SSSA Soils Certifying Board Code of Ethics
Certified ProfessionalSoil Scientist
CPSS

5
Soil
Scie
nce
Cor
e R
equi
rem
ents
Thi
s fo
rm d
oes
not s
ubst
itut
e fo
r tr
ansc
ript
s, o
ffici
al tr
ansc
ript
s ar
e re
quir
ed.
Cer
tifie
d Pr
ofes
sion
al S
oil S
cien
tist,
5585
Gui
lfor
d R
oad,
Mad
ison
, WI
5371
1-58
01 •
(60
8) 2
68-4
955
FOR
OFF
ICE
USE
No.
Cer
tifi
ed P
rofe
ssio
nal
Soil
Sci
enti
st
CP
SS
Firs
t Nam
e/G
iven
Nam
e
Las
t Nam
e/Su
rnam
e
Deg
ree
Uni
vers
ity
Maj
or
Min
or
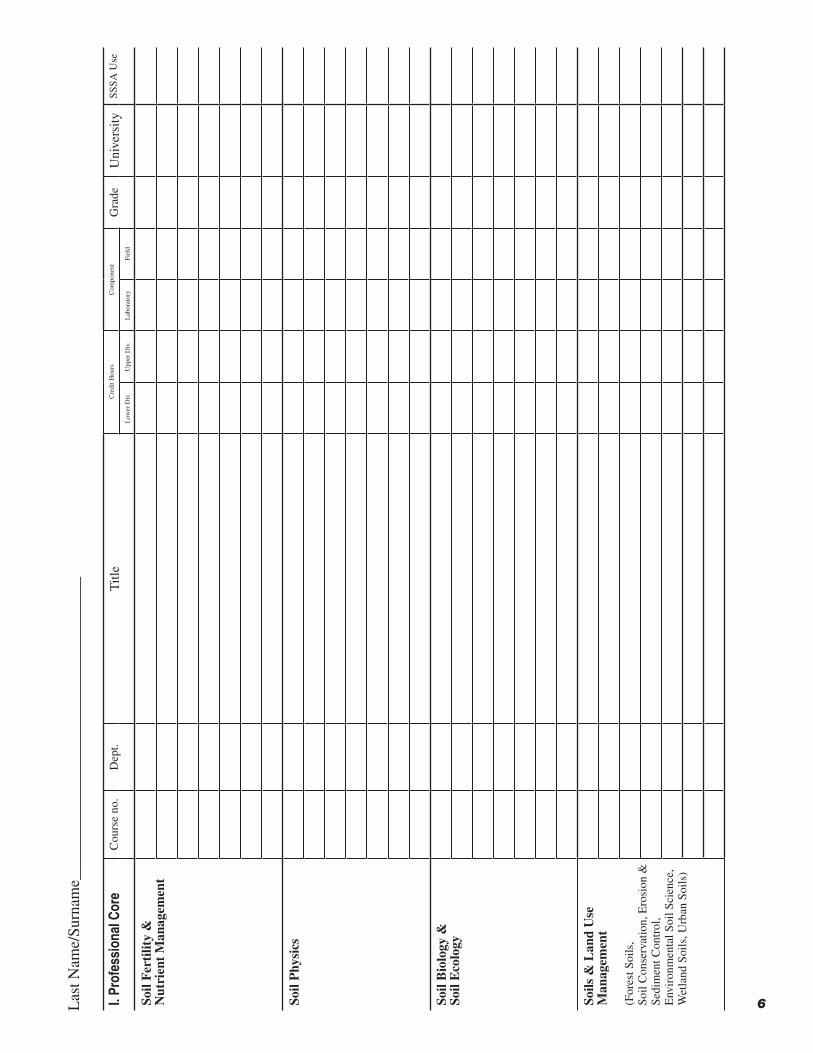
I. Pr
ofes
sion
al C
ore
Cou
rse
no.
Dep
t.T
itle
Cre
dit H
ours
Com
pone
ntG
rade
Uni
vers
itySS
SA U
seL
ower
Div
.U
pper
Div
.L
abor
ator
yFi
eld
Soil
Gen
esis
, M
orph
olog
y, &
C
lass
ifica
tion
Soil
Che
mis
try
&
Min
eral
ogy
Pro
fess
iona
l Cor
e R
equi
rem
ents
incl
ude:
• >
15
sem
este
r cr
edits
tota
l of
whi
ch >
9 s
emes
ter
cred
its m
ust b
e up
per
divi
sion
•
Low
er d
ivis
ion=
Fres
hman
and
sop
hom
ore
leve
l cou
rses
. •
Upp
er d
ivis
ion=
Juni
or, s
enio
r, an
d gr
adua
te le
vel c
ours
es.
• I
n th
e co
mpo
nent
col
umn,
put
an
X in
eith
er th
e la
bora
tory
or
field
col
umn
that
bes
t des
crib
es th
e co
urse
•
Lab
orat
ory
and/
or F
ield
cou
rsew
ork
is a
req
uire
d co
mpo
nent
in >
2 o
f th
e so
il Sc
ienc
e C
ore
clas
ses.
Exa
mpl
es in
clud
ing
soil
judg
ing,
und
ergr
adua
te r
esea
rch,
labo
rato
ry e
xer-
cise
s, fi
eld
cour
ses.
•
A m
inim
um g
rade
poi
nt a
vera
ge (
GPA
) of
2.5
is r
equi
red
in th
e to
tal p
rofe
ssio
nal c
ore
cour
se
requ
irem
ent.
Thi
s do
es n
ot in
clud
e th
e su
ppor
ting
core
cou
rses
. •
In
the
cred
it ho
urs
colu
mn,
indi
cate
if th
ey a
re s
emes
ter
or q
uart
er h
ours
(e
x 3
Sem
or
3 Q
tr).
6I. Pr
ofes
sion
al C
ore
Cou
rse
no.
Dep
t.T
itle
Cre
dit H
ours
Com
pone
ntG
rade
Uni
vers
itySS
SA U
seL
ower
Div
.U
pper
Div
.L
abor
ator
yFi
eld
Soil
Fer
tilit
y &
Nut
rien
t M
anag
emen
t
Soil
Phy
sics
Soil
Bio
logy
&So
il E
colo
gy
Soils
& L
and
Use
M
anag
emen
t
(For
est S
oils
, So
il C
onse
rvat
ion,
Ero
sion
&
Sedi
men
t Con
trol
,E
nvir
onm
enta
l Soi
l Sci
ence
, W
etla
nd S
oils
, Urb
an S
oils
)
Las
t Nam
e/Su
rnam
e___
____
____
____
____
____
____
____
____
___

7
II. S
uppo
rting
Cor
eC
ours
e no
.D
ept.
Titl
e C
redi
t Hou
rsG
rade
Uni
vers
itySS
SA U
seL
ower
Div
.U
pper
Div
.
Agr
icul
tura
l Sci
ence
(Agr
onom
y, C
rop
Scie
nce,
A
grof
ores
ty, H
ortic
ultu
re,
Prec
isio
n A
gric
ultu
re,
Sust
aina
ble
Agr
icul
ture
, R
ange
Sci
ence
, Tur
f Sc
ienc
e,
Wee
d Sc
ienc
e)
Bio
logi
cal &
Eco
logi
cal
Scie
nces
(Bio
logy
, Bot
any,
Eco
logy
, Fo
rest
ry, M
icro
biol
ogy,
R
ange
Sci
ence
, Wet
land
Sc
ienc
e)
Che
mis
try,
M
athe
mat
ics,
Phy
sics
, St
atis
tics
Com
mun
icat
ions
(Spe
ech,
Tec
hnic
al W
ritin
g)
Las
t Nam
e/Su
rnam
e___
____
____
____
____
____
____
____
____
____
_Su
ppor
ting
Cor
e R
equi
rem
ents
Inc
lude
:
• >
45
sem
este
r cr
edits
tota
l of
whi
ch >
15
sem
este
r cr
edits
mus
t be
uppe
r di
visi
on.
• L
ower
div
isio
n=Fr
eshm
an a
nd s
opho
mor
e le
vel c
ours
es. U
pper
div
isio
n=Ju
nior
, Sen
ior,
and
grad
uate
cou
rses
.
• 4
of
the
follo
win
g 8
area
s m
ust
have
> 5
cre
dits
.
• E
xam
ples
are
pro
vide
d fo
r ea
ch c
ateg
ory
• I
f yo
u ar
e sh
ort c
redi
ts, y
our
appl
icat
ion
will
be
reje
cted
unl
ess
you
prov
ide
a w
ritte
n ex
plan
a-tio
n of
oth
er c
ours
es/e
xper
ienc
e to
ful
fill t
he m
issi
ng c
redi
t req
uire
men
t(s)
.

8
II. S
uppo
rting
Cor
eC
ours
e no
.D
ept.
Titl
e C
redi
t Hou
rsG
rade
Uni
vers
itySS
SA U
seL
ower
Div
.U
pper
Div
.
Geo
scie
nce
Scie
nce
(Arc
heol
ogy,
Phy
sica
l Geo
g-ra
phy,
Geo
grap
hic
Info
rma-
tion
Syst
ems,
Met
eoro
logy
, R
emot
e Se
nsin
g, T
erra
in
Ana
lysi
s, &
Atm
osph
eric
Sc
ienc
e)
Hum
an H
ealt
h &
L
and
Use
(Env
iron
men
tal L
aw &
Po
licy,
Env
iron
men
tal E
thic
s &
Phi
loso
phy,
Env
iron
men
tal
Qua
lity,
Haz
ards
, Lan
d U
se
Plan
ning
, Site
Ass
essm
ent,
Sust
aina
bilit
y, T
oxic
olog
y,
Was
te M
anag
emen
t,
HA
ZW
OPE
R)
Tech
nolo
gy &
E
ngin
eeri
ng(A
gric
ultu
ral E
ngin
eeri
ng,
Bio
engi
neer
ing
Soil,
Civ
il,
Con
stru
ctio
n &
Geo
tech
nica
l E
ngin
eeri
ng,
Env
iron
men
tal E
ngin
eeri
ng,
Irri
gatio
n Te
chno
logy
, C
ompu
ter
Aid
ed D
raft
ing)
Wat
er S
cien
ces
(Hyd
rolo
gy, H
ydro
geol
ogy,
L
imno
logy
, Wat
er R
esou
rces
, V
ados
e Z
one,
Wet
land
Sc
ienc
e)
Las
t Nam
e/Su
rnam
e___
____
____
____
____
____
____
____
____
____
____
__

9
EX
AM
PL
E
Prof
essi
onal
Wor
k E
xper
ienc
e Fo
rmSO
IL S
CIE
NC
E C
ER
TIF
ICA
TIO
N
INST
RU
CT
ION
S1.
L
ist f
ull-
time
posi
tions
in s
eque
ntia
l ord
er, e
ndin
g w
ith c
urre
nt p
ositi
on.
2. L
ist
only
pro
fess
iona
l-le
vel
posi
tions
in
the
area
of
soil
scie
nce
beyo
nd t
he b
ac ca
laur
e ate
deg
ree.
W
ork
expe
rien
ce w
hile
obt
aini
ng a
n ad
vanc
ed d
egre
e sh
ould
not
be
incl
uded
.3.
Lis
t beg
inni
ng a
nd e
ndin
g m
onth
and
yea
r fo
r al
l pos
ition
s.4.
If y
ou h
ave
wor
ked
in tw
o po
sitio
ns c
oncu
rren
tly, i
ndic
ate
unde
r the
per
cent
tim
e ca
tego
ry th
e ye
arly
pe
rcen
tage
tim
e yo
u w
orke
d in
eac
h po
sitio
n.
5. S
how
the
perc
ent t
ime
on a
n an
nual
bas
is f
or e
ach
wor
k ac
tivity
(sh
ould
tota
l 100
%).
6. U
nder
ref
eren
ce, l
ist t
he r
efer
ence
(s)
mos
t fam
iliar
with
eac
h w
ork
expe
rien
ce.
7. D
utie
s an
d re
spon
sibi
litie
s sh
ould
be
spec
ific
and
det
aile
d.8.
Be
sure
to to
tal m
onth
s of
exp
erie
nce.
R
emem
ber
wor
k ex
peri
ence
gai
ned
whi
le s
eeki
ng a
deg
ree
does
not
cou
nt t
owar
d th
e C
PSS
/SC
w
ork
expe
rien
ce r
equi
rem
ent.
9. C
opy/
prin
t add
ition
al p
ages
if n
eede
d.
EX
AM
PL
E
Em
ploy
men
t Inf
orm
atio
n
L
engt
h D
egre
e E
mpl
oyer
P
rofe
ssio
nal
%
%
Tim
e/
Fro
m
To
L
evel
N
ame,
Loc
atio
n T
itle
T
ime
Dut
ies
and
Res
pons
ibili
ties
A
ctiv
ity
Ref
eren
ce
9/
88–9
/90
BS
Dav
is E
ngin
eeri
ng
Soil
Scie
ntis
t 10
0 D
elin
eate
hyd
ric
soils
on
pote
ntia
l hig
hway
Polly
Ped
on
Cul
pepe
r, V
A
rig
ht o
f w
ays
50
John
Mud
d
D
escr
ibe
soils
on
arch
aeol
ogy
site
s to
mee
t
Dav
id A
uger
env
iron
men
tal i
mpa
ct r
equi
rem
ents
5
W
illia
m P
rofi
le
M
anag
e eq
uipm
ent f
or s
ite in
vest
igat
ions
10
Coo
rdin
ate
GIS
land
use
inte
rpre
tatio
n 35
9/
90–p
rese
nt
BS
Soil
Pro’
s So
ils I
nves
tigat
or
100
Soil
char
acte
riza
tion
for
drai
n fi
elds
50
St
eve
Pitts
Y
ork,
PA
D
evel
opm
ent r
epor
ts f
or c
ount
y an
d st
ate
agen
cies
for
site
sui
tabi
lity,
per
mits
for
sep
tic fi
elds
, lan
dfill
s,
a
nd s
econ
dary
roa
d co
nstr
uctio
n 40
Wor
ksho
ps f
or c
lient
s on
reg
ulat
ory
requ
irem
ents
and
per
mits
for
con
stru
ctio
n 10
Mon
ths
of e
xper
ienc
e th
is p
age
100
Cer
tifi
ed P
rofe
ssio
nal
Soil
Sci
enti
st
CP
SS

010
Pro
fess
iona
l Wor
k E
xper
ienc
e F
orm
SOIL
SC
IEN
CE
CE
RT
IFIC
AT
ION
D
ate
of D
egre
e: B
ache
lors
____
____
____
____
__
MS
____
____
____
____
__
PhD
___
____
____
____
___
Las
t Nam
e/Su
rnam
e___
____
____
____
____
____
____
____
____
____
____
____
___
Fir
st N
ame/
Giv
en N
ame
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
Cer
tifi
ed P
rofe
ssio
nal
Soil
Sci
enti
st
CP
SS
Em
ploy
men
t Inf
orm
atio
n—P
leas
e se
e ex
ampl
e pa
ge fo
r in
stru
ctio
ns.
L
engt
h D
egre
e E
mpl
oyer
P
rofe
ssio
nal
%
%
Tim
e/
Fro
m
To
L
evel
N
ame,
Loc
atio
n T
itle
T
ime
Dut
ies
and
Res
pons
ibili
ties
A
ctiv
ity
Ref
eren
ce
Mon
ths
of e
xper
ienc
e th
is p
age

Em
ploy
men
t Inf
orm
atio
n—P
leas
e se
e ex
ampl
e pa
ge fo
r in
stru
ctio
ns.
L
engt
h D
egre
e E
mpl
oyer
P
rofe
ssio
nal
%
%
Tim
e/
Fro
m
To
L
evel
N
ame,
Loc
atio
n T
itle
T
ime
Dut
ies
and
Res
pons
ibili
ties
A
ctiv
ity
Ref
eren
ce
Mon
ths
of e
xper
ienc
e th
is p
age
____
____
____
__
To
tal m
onth
s of
exp
erie
nce
incl
udin
g al
l pag
es _
____
____
____
__
Las
t Nam
e/Su
rnam
e___
____
____
____
____
____
____
____
____
____
____
____
____
_
Fir
st N
ame/
Giv
en N
ame
____
____
____
____
____
____
____
____
____
____
____
____
____
11

12
5585 Guilford Road • Madison, WI 53711-5801 • 608-268-4955 • FAX 608-273-2081
Certification Programs
Certified Professional Soil Scientist sponsored by the Soil Science Society of America
www.soils.org/certifications
From: ___________________________________ To: ___________________________________ Applicant’s Name Reference’s Name
____________________________________ ___________________________________ Applicant’s Address Reference’s Address
____________________________________ ___________________________________
____________________________________ ___________________________________
____________________________________ ___________________________________ Applicant’s phone number Reference’s Phone Number
AREA OF CERTIFICATION APPLYING FOR:
❑ Certified Professional Soil Scientist (CPSS)
❑ Associate Professional Soil Scientist (APSS)
Note to Applicant: Please complete the above information and give this form to the reference. The reference needs to complete the questions on the reverse side and forward to the SSSA Offices (see below).
Note to Reference: The above-named individual is applying for certification and has requested that you act as a reference. An applicant must provide at least five references (including at least one that is a CPSS or CPAg, a licensed soil scientist, or a faculty member familiar with the applicants work experience in soil science, as refer-enced in I.B.3 of the CPSS Policy Document), and others who are familiar with her/his experience. By completing this form you will be acting as a reference for the applicant named above.
Please answer the questions on the back of this form, and include any additional comments that you feel may be helpful. This form will be reviewed by the Certifying Board to ensure that the applicant has the necessary educa-tion and experience to be certified.
Prospective applicants must meet rigorous educational, experience, and ethical standards. They must have a mini-mum of a Bachelor's level degree, meet certain course requirements, and adhere to the code of ethics. No experi-ence is required for Associate Professional (AP) status.
Because we want to certify only individuals who meet the professional standards, we solicit your confidential and frank opinion of this applicant.
Experience: Applicants for Certified Professional status (no experience is needed for Associate Professional status) must have at least five years of professional experience beyond the baccalaureate degree in each area of certification. An advanced degree will substitute for two years professional experience; for example three years of professional experience at both the MS and/or PhD level.
Reference Request
Certified ProfessionalSoil Scientist
CPSS
Check if reference is:
❑ CPSS ❑ CPAg
❑ Licensed Soil Scientist (State)________________________
❑ Soil Science Faculty
Please sign and return this form (2 pages) directly to: Marta Krist at [email protected] or mail toSSSA Certification Department, 5585 Guilford Road, Madison, WI 53711-5801 or fax to 608-273-2081
*Reference letters sent to the applicant will not be considered.

13
Please respond to the following items and include any pertinent information that you feel will aid in the evaluation of the applicant’s credentials.
1. In what capacity have you had association with the applicant(family members/relatives not valid references)?I am (was) the applicant’s:
_____ Supervisor _____ Subordinate _____ Academic Advisor _____ Colleague _____ Classmate _____ Client _____ Other as: ______________________
2. What length of time have you known the applicant in the above capacity? _________________ years
3. For what period of time are you familiar with the applicant’s professional work experience? From _________________ to ________________ month/year month/year
4. Knowing the minimum requirements for certification, do you feel qualified to recommend this applicant to become certified in the area of certification as stated on the reverse side? ________ Yes ________ No
If “yes”, please proceed and complete the reference. If “no”, please give a brief statement in # 7 below of your reason(s); sign and return this letter immediately.
5. What particular strengths do you feel the applicant has that may be important in the evaluation of a professional?
___________________________________________________________________________________________________
___________________________________________________________________________________________________
6. Do you feel that the applicant is fully qualified at this time for the certification listed? ________ Yes ________ No If no, how could the applicant overcome any weaknesses or deficiencies?
___________________________________________________________________________________________________
___________________________________________________________________________________________________
7. Please comment on the applicant’s professional growth and development, ability to analyze and solve problems, resourceful-ness, professionalism, and knowledge in the area of application. Also, please make any additional comments which will aid in making a fair evaluation of this applicant.
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
8. Do you recommend this applicant to be certified in the area of certification as stated on the reverse side? ____ Yes ____ No
Your response will remain confidential.Print Name _____________________________________________________________________________________________
Signature ________________________________________________ Professional Title ________________________________
Employer _________________________________________ Location ______________________________________________
Date _________________ Licensed or Certified as _________________________ Telephone ___________________________
Email _________________________________________________________________________________________________
Please sign and return this form (2 pages) directly to: Marta Krist at [email protected] or mail toSSSA Certification Department, 5585 Guilford Road, Madison, WI 53711-5801 or fax to 608-273-2081
*Reference letters sent to the applicant will not be considered.
14
5585 Guilford Road • Madison, WI 53711-5801 • 608-268-4955 • FAX 608-273-2081
Certification Programs
Certified Professional Soil Scientist sponsored by the Soil Science Society of America
www.soils.org/certifications
From: ___________________________________ To: ___________________________________ Applicant’s Name Reference’s Name
____________________________________ ___________________________________ Applicant’s Address Reference’s Address
____________________________________ ___________________________________
____________________________________ ___________________________________
____________________________________ ___________________________________ Applicant’s phone number Reference’s Phone Number
AREA OF CERTIFICATION APPLYING FOR:
❑ Certified Professional Soil Scientist (CPSS)
❑ Associate Professional Soil Scientist (APSS)
Note to Applicant: Please complete the above information and give this form to the reference. The reference needs to complete the questions on the reverse side and forward to the SSSA Offices (see below).
Note to Reference: The above-named individual is applying for certification and has requested that you act as a reference. An applicant must provide at least five references (including at least one that is a CPSS or CPAg, a licensed soil scientist, or a faculty member familiar with the applicants work experience in soil science, as refer-enced in I.B.3 of the CPSS Policy Document), and others who are familiar with her/his experience. By completing this form you will be acting as a reference for the applicant named above.
Please answer the questions on the back of this form, and include any additional comments that you feel may be helpful. This form will be reviewed by the Certifying Board to ensure that the applicant has the necessary educa-tion and experience to be certified.
Prospective applicants must meet rigorous educational, experience, and ethical standards. They must have a mini-mum of a Bachelor's level degree, meet certain course requirements, and adhere to the code of ethics. No experi-ence is required for Associate Professional (AP) status.
Because we want to certify only individuals who meet the professional standards, we solicit your confidential and frank opinion of this applicant.
Experience: Applicants for Certified Professional status (no experience is needed for Associate Professional status) must have at least five years of professional experience beyond the baccalaureate degree in each area of certification. An advanced degree will substitute for two years professional experience; for example three years of professional experience at both the MS and/or PhD level.
Reference Request
Certified ProfessionalSoil Scientist
CPSS
Check if reference is:
❑ CPSS ❑ CPAg
❑ Licensed Soil Scientist (State)________________________
❑ Soil Science Faculty
Please sign and return this form (2 pages) directly to: Marta Krist at [email protected] or mail toSSSA Certification Department, 5585 Guilford Road, Madison, WI 53711-5801 or fax to 608-273-2081
*Reference letters sent to the applicant will not be considered.

15
Please respond to the following items and include any pertinent information that you feel will aid in the evaluation of the applicant’s credentials.
1. In what capacity have you had association with the applicant(family members/relatives not valid references)?I am (was) the applicant’s:
_____ Supervisor _____ Subordinate _____ Academic Advisor _____ Colleague _____ Classmate _____ Client _____ Other as: ______________________
2. What length of time have you known the applicant in the above capacity? _________________ years
3. For what period of time are you familiar with the applicant’s professional work experience? From _________________ to ________________ month/year month/year
4. Knowing the minimum requirements for certification, do you feel qualified to recommend this applicant to become certified in the area of certification as stated on the reverse side? ________ Yes ________ No
If “yes”, please proceed and complete the reference. If “no”, please give a brief statement in # 7 below of your reason(s); sign and return this letter immediately.
5. What particular strengths do you feel the applicant has that may be important in the evaluation of a professional?
___________________________________________________________________________________________________
___________________________________________________________________________________________________
6. Do you feel that the applicant is fully qualified at this time for the certification listed? ________ Yes ________ No If no, how could the applicant overcome any weaknesses or deficiencies?
___________________________________________________________________________________________________
___________________________________________________________________________________________________
7. Please comment on the applicant’s professional growth and development, ability to analyze and solve problems, resourceful-ness, professionalism, and knowledge in the area of application. Also, please make any additional comments which will aid in making a fair evaluation of this applicant.
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
8. Do you recommend this applicant to be certified in the area of certification as stated on the reverse side? ____ Yes ____ No
Your response will remain confidential.Print Name _____________________________________________________________________________________________
Signature ________________________________________________ Professional Title ________________________________
Employer _________________________________________ Location ______________________________________________
Date _________________ Licensed or Certified as _________________________ Telephone ___________________________
Email _________________________________________________________________________________________________
Please sign and return this form (2 pages) directly to: Marta Krist at [email protected] or mail toSSSA Certification Department, 5585 Guilford Road, Madison, WI 53711-5801 or fax to 608-273-2081
*Reference letters sent to the applicant will not be considered.

16
5585 Guilford Road • Madison, WI 53711-5801 • 608-268-4955 • FAX 608-273-2081
Certification Programs
Certified Professional Soil Scientist sponsored by the Soil Science Society of America
www.soils.org/certifications
From: ___________________________________ To: ___________________________________ Applicant’s Name Reference’s Name
____________________________________ ___________________________________ Applicant’s Address Reference’s Address
____________________________________ ___________________________________
____________________________________ ___________________________________
____________________________________ ___________________________________ Applicant’s phone number Reference’s Phone Number
AREA OF CERTIFICATION APPLYING FOR:
❑ Certified Professional Soil Scientist (CPSS)
❑ Associate Professional Soil Scientist (APSS)
Note to Applicant: Please complete the above information and give this form to the reference. The reference needs to complete the questions on the reverse side and forward to the SSSA Offices (see below).
Note to Reference: The above-named individual is applying for certification and has requested that you act as a reference. An applicant must provide at least five references (including at least one that is a CPSS or CPAg, a licensed soil scientist, or a faculty member familiar with the applicants work experience in soil science, as refer-enced in I.B.3 of the CPSS Policy Document), and others who are familiar with her/his experience. By completing this form you will be acting as a reference for the applicant named above.
Please answer the questions on the back of this form, and include any additional comments that you feel may be helpful. This form will be reviewed by the Certifying Board to ensure that the applicant has the necessary educa-tion and experience to be certified.
Prospective applicants must meet rigorous educational, experience, and ethical standards. They must have a mini-mum of a Bachelor's level degree, meet certain course requirements, and adhere to the code of ethics. No experi-ence is required for Associate Professional (AP) status.
Because we want to certify only individuals who meet the professional standards, we solicit your confidential and frank opinion of this applicant.
Experience: Applicants for Certified Professional status (no experience is needed for Associate Professional status) must have at least five years of professional experience beyond the baccalaureate degree in each area of certification. An advanced degree will substitute for two years professional experience; for example three years of professional experience at both the MS and/or PhD level.
Reference Request
Certified ProfessionalSoil Scientist
CPSS
Check if reference is:
❑ CPSS ❑ CPAg
❑ Licensed Soil Scientist (State)________________________
❑ Soil Science Faculty
Please sign and return this form (2 pages) directly to: Marta Krist at [email protected] or mail toSSSA Certification Department, 5585 Guilford Road, Madison, WI 53711-5801 or fax to 608-273-2081
*Reference letters sent to the applicant will not be considered.

17
Please respond to the following items and include any pertinent information that you feel will aid in the evaluation of the applicant’s credentials.
1. In what capacity have you had association with the applicant(family members/relatives not valid references)?I am (was) the applicant’s:
_____ Supervisor _____ Subordinate _____ Academic Advisor _____ Colleague _____ Classmate _____ Client _____ Other as: ______________________
2. What length of time have you known the applicant in the above capacity? _________________ years
3. For what period of time are you familiar with the applicant’s professional work experience? From _________________ to ________________ month/year month/year
4. Knowing the minimum requirements for certification, do you feel qualified to recommend this applicant to become certified in the area of certification as stated on the reverse side? ________ Yes ________ No
If “yes”, please proceed and complete the reference. If “no”, please give a brief statement in # 7 below of your reason(s); sign and return this letter immediately.
5. What particular strengths do you feel the applicant has that may be important in the evaluation of a professional?
___________________________________________________________________________________________________
___________________________________________________________________________________________________
6. Do you feel that the applicant is fully qualified at this time for the certification listed? ________ Yes ________ No If no, how could the applicant overcome any weaknesses or deficiencies?
___________________________________________________________________________________________________
___________________________________________________________________________________________________
7. Please comment on the applicant’s professional growth and development, ability to analyze and solve problems, resourceful-ness, professionalism, and knowledge in the area of application. Also, please make any additional comments which will aid in making a fair evaluation of this applicant.
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
8. Do you recommend this applicant to be certified in the area of certification as stated on the reverse side? ____ Yes ____ No
Your response will remain confidential.Print Name _____________________________________________________________________________________________
Signature ________________________________________________ Professional Title ________________________________
Employer _________________________________________ Location ______________________________________________
Date _________________ Licensed or Certified as _________________________ Telephone ___________________________
Email _________________________________________________________________________________________________
Please sign and return this form (2 pages) directly to: Marta Krist at [email protected] or mail toSSSA Certification Department, 5585 Guilford Road, Madison, WI 53711-5801 or fax to 608-273-2081
*Reference letters sent to the applicant will not be considered.

18
5585 Guilford Road • Madison, WI 53711-5801 • 608-268-4955 • FAX 608-273-2081
Certification Programs
Certified Professional Soil Scientist sponsored by the Soil Science Society of America
www.soils.org/certifications
From: ___________________________________ To: ___________________________________ Applicant’s Name Reference’s Name
____________________________________ ___________________________________ Applicant’s Address Reference’s Address
____________________________________ ___________________________________
____________________________________ ___________________________________
____________________________________ ___________________________________ Applicant’s phone number Reference’s Phone Number
AREA OF CERTIFICATION APPLYING FOR:
❑ Certified Professional Soil Scientist (CPSS)
❑ Associate Professional Soil Scientist (APSS)
Note to Applicant: Please complete the above information and give this form to the reference. The reference needs to complete the questions on the reverse side and forward to the SSSA Offices (see below).
Note to Reference: The above-named individual is applying for certification and has requested that you act as a reference. An applicant must provide at least five references (including at least one that is a CPSS or CPAg, a licensed soil scientist, or a faculty member familiar with the applicants work experience in soil science, as refer-enced in I.B.3 of the CPSS Policy Document), and others who are familiar with her/his experience. By completing this form you will be acting as a reference for the applicant named above.
Please answer the questions on the back of this form, and include any additional comments that you feel may be helpful. This form will be reviewed by the Certifying Board to ensure that the applicant has the necessary educa-tion and experience to be certified.
Prospective applicants must meet rigorous educational, experience, and ethical standards. They must have a mini-mum of a Bachelor's level degree, meet certain course requirements, and adhere to the code of ethics. No experi-ence is required for Associate Professional (AP) status.
Because we want to certify only individuals who meet the professional standards, we solicit your confidential and frank opinion of this applicant.
Experience: Applicants for Certified Professional status (no experience is needed for Associate Professional status) must have at least five years of professional experience beyond the baccalaureate degree in each area of certification. An advanced degree will substitute for two years professional experience; for example three years of professional experience at both the MS and/or PhD level.
Reference Request
Certified ProfessionalSoil Scientist
CPSS
Check if reference is:
❑ CPSS ❑ CPAg
❑ Licensed Soil Scientist (State)________________________
❑ Soil Science Faculty
Please sign and return this form (2 pages) directly to: Marta Krist at [email protected] or mail toSSSA Certification Department, 5585 Guilford Road, Madison, WI 53711-5801 or fax to 608-273-2081
*Reference letters sent to the applicant will not be considered.

19
Please respond to the following items and include any pertinent information that you feel will aid in the evaluation of the applicant’s credentials.
1. In what capacity have you had association with the applicant(family members/relatives not valid references)?I am (was) the applicant’s:
_____ Supervisor _____ Subordinate _____ Academic Advisor _____ Colleague _____ Classmate _____ Client _____ Other as: ______________________
2. What length of time have you known the applicant in the above capacity? _________________ years
3. For what period of time are you familiar with the applicant’s professional work experience? From _________________ to ________________ month/year month/year
4. Knowing the minimum requirements for certification, do you feel qualified to recommend this applicant to become certified in the area of certification as stated on the reverse side? ________ Yes ________ No
If “yes”, please proceed and complete the reference. If “no”, please give a brief statement in # 7 below of your reason(s); sign and return this letter immediately.
5. What particular strengths do you feel the applicant has that may be important in the evaluation of a professional?
___________________________________________________________________________________________________
___________________________________________________________________________________________________
6. Do you feel that the applicant is fully qualified at this time for the certification listed? ________ Yes ________ No If no, how could the applicant overcome any weaknesses or deficiencies?
___________________________________________________________________________________________________
___________________________________________________________________________________________________
7. Please comment on the applicant’s professional growth and development, ability to analyze and solve problems, resourceful-ness, professionalism, and knowledge in the area of application. Also, please make any additional comments which will aid in making a fair evaluation of this applicant.
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
8. Do you recommend this applicant to be certified in the area of certification as stated on the reverse side? ____ Yes ____ No
Your response will remain confidential.Print Name _____________________________________________________________________________________________
Signature ________________________________________________ Professional Title ________________________________
Employer _________________________________________ Location ______________________________________________
Date _________________ Licensed or Certified as _________________________ Telephone ___________________________
Email _________________________________________________________________________________________________
Please sign and return this form (2 pages) directly to: Marta Krist at [email protected] or mail toSSSA Certification Department, 5585 Guilford Road, Madison, WI 53711-5801 or fax to 608-273-2081
*Reference letters sent to the applicant will not be considered.

20
5585 Guilford Road • Madison, WI 53711-5801 • 608-268-4955 • FAX 608-273-2081
Certification Programs
Certified Professional Soil Scientist sponsored by the Soil Science Society of America
www.soils.org/certifications
From: ___________________________________ To: ___________________________________ Applicant’s Name Reference’s Name
____________________________________ ___________________________________ Applicant’s Address Reference’s Address
____________________________________ ___________________________________
____________________________________ ___________________________________
____________________________________ ___________________________________ Applicant’s phone number Reference’s Phone Number
AREA OF CERTIFICATION APPLYING FOR:
❑ Certified Professional Soil Scientist (CPSS)
❑ Associate Professional Soil Scientist (APSS)
Note to Applicant: Please complete the above information and give this form to the reference. The reference needs to complete the questions on the reverse side and forward to the SSSA Offices (see below).
Note to Reference: The above-named individual is applying for certification and has requested that you act as a reference. An applicant must provide at least five references (including at least one that is a CPSS or CPAg, a licensed soil scientist, or a faculty member familiar with the applicants work experience in soil science, as refer-enced in I.B.3 of the CPSS Policy Document), and others who are familiar with her/his experience. By completing this form you will be acting as a reference for the applicant named above.
Please answer the questions on the back of this form, and include any additional comments that you feel may be helpful. This form will be reviewed by the Certifying Board to ensure that the applicant has the necessary educa-tion and experience to be certified.
Prospective applicants must meet rigorous educational, experience, and ethical standards. They must have a mini-mum of a Bachelor's level degree, meet certain course requirements, and adhere to the code of ethics. No experi-ence is required for Associate Professional (AP) status.
Because we want to certify only individuals who meet the professional standards, we solicit your confidential and frank opinion of this applicant.
Experience: Applicants for Certified Professional status (no experience is needed for Associate Professional status) must have at least five years of professional experience beyond the baccalaureate degree in each area of certification. An advanced degree will substitute for two years professional experience; for example three years of professional experience at both the MS and/or PhD level.
Reference Request
Certified ProfessionalSoil Scientist
CPSS
Check if reference is:
❑ CPSS ❑ CPAg
❑ Licensed Soil Scientist (State)________________________
❑ Soil Science Faculty
Please sign and return this form (2 pages) directly to: Marta Krist at [email protected] or mail toSSSA Certification Department, 5585 Guilford Road, Madison, WI 53711-5801 or fax to 608-273-2081
*Reference letters sent to the applicant will not be considered.
21
Please respond to the following items and include any pertinent information that you feel will aid in the evaluation of the applicant’s credentials.
1. In what capacity have you had association with the applicant(family members/relatives not valid references)?I am (was) the applicant’s:
_____ Supervisor _____ Subordinate _____ Academic Advisor _____ Colleague _____ Classmate _____ Client _____ Other as: ______________________
2. What length of time have you known the applicant in the above capacity? _________________ years
3. For what period of time are you familiar with the applicant’s professional work experience? From _________________ to ________________ month/year month/year
4. Knowing the minimum requirements for certification, do you feel qualified to recommend this applicant to become certified in the area of certification as stated on the reverse side? ________ Yes ________ No
If “yes”, please proceed and complete the reference. If “no”, please give a brief statement in # 7 below of your reason(s); sign and return this letter immediately.
5. What particular strengths do you feel the applicant has that may be important in the evaluation of a professional?
___________________________________________________________________________________________________
___________________________________________________________________________________________________
6. Do you feel that the applicant is fully qualified at this time for the certification listed? ________ Yes ________ No If no, how could the applicant overcome any weaknesses or deficiencies?
___________________________________________________________________________________________________
___________________________________________________________________________________________________
7. Please comment on the applicant’s professional growth and development, ability to analyze and solve problems, resourceful-ness, professionalism, and knowledge in the area of application. Also, please make any additional comments which will aid in making a fair evaluation of this applicant.
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
___________________________________________________________________________________________________
8. Do you recommend this applicant to be certified in the area of certification as stated on the reverse side? ____ Yes ____ No
Your response will remain confidential.Print Name _____________________________________________________________________________________________
Signature ________________________________________________ Professional Title ________________________________
Employer _________________________________________ Location ______________________________________________
Date _________________ Licensed or Certified as _________________________ Telephone ___________________________
Email _________________________________________________________________________________________________
Please sign and return this form (2 pages) directly to: Marta Krist at [email protected] or mail toSSSA Certification Department, 5585 Guilford Road, Madison, WI 53711-5801 or fax to 608-273-2081
*Reference letters sent to the applicant will not be considered.