cbcl pediatric bipolar disorder profile and adhd: comorbidity and quantitative trait loci analysis
TRANSCRIPT

CBCL Pediatric Bipolar Disorder Profile and ADHD:Comorbidity and Quantitative Trait Loci AnalysisJAMES J. MCGOUGH, M.D., SANDRA K. LOO, PH.D., JAMES T. MCCRACKEN, M.D.,
JEFFREY DANG, M.S., SHAUNNA CLARK, M.A., STANLEY F. NELSON, M.D.,AND SUSAN L. SMALLEY, PH.D.
ABSTRACT
Objective: The pediatric bipolar disorder profilme of the Child Behavior Checklist (CBCL-PBD), a parent-completedmeasure
that avoids clinician ideological bias, has proven useful in differentiating patients with attention-deficit/hyperactivity disorder
(ADHD). We used CBCL-PBD profiles to distinguish patterns of comorbidity and to search for quantitative trait loci in a
genomewide scan in a sample of multiple affected ADHD sibling pairs. Method: A total of 540 ADHD subjects ages 5 to
18 years were assessed with the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and
Lifetime version and CBCL. Parents were assessed with the Schedule for Affective Disorders and Schizophrenia-Lifetime
version supplemented by the Schedule for Affective Disorders and Schizophrenia for School-Age Children for disruptive
behavioral disorders. Patterns of psychiatric comorbidity were contrasted based on the CBCL-PBD profile. A quantitative trait
loci variance component analysis was used to identify potential genomic regions that may harbor susceptibility genes for the
CBCL-PBD quantitative phenotype. Results: Bipolar spectrum disorders represented less than 2% of the overall sample.
The CBCL-PBD classification was associated with increased generalized anxiety disorder (p = .001), oppositional defiant
disorder (p = .008), conduct disorder (p = .003), and parental substance abuse (p = .005). A moderately significant linkage
signal (multipoint maximum lod score = 2.5) was found on chromosome 2q. Conclusions: The CBCL-PBD profile
distinguishes a subset of ADHD patients with significant comorbidity. Linkage analysis of the CBCL-PBD phenotype suggests
certain genomic regions that merit further investigation for genes predisposing to severe psychopathology. J. Am. Acad. Child
Adolesc. Psychiatry, 2008;47(10):1151Y1157. Key Words: attention-deficit/hyperactivity disorder, bipolar disorder, Child
Behavior Checklist, quantitative trait loci, linkage analysis.
The Child Behavior Checklist (CBCL) has beenproposed as a nonideological measure to characterizecomorbidity in individuals with attention-deficit/hyper-
activity disorder (ADHD).1,2 The CBCL is an empiri-cally derived, highly valid and reliable parent checklist ofpediatric psychopathology that is composed of severaldimensions and scored according to established algo-rithms.3 As a parent-completed measure, the CBCL pro-vides a common metric across patients and studies that isfree from clinician interpretation.4 Subsequent reportshave proven the utility of this approach.5Y9 Numerousstudies have demonstrated that a CBCL pediatric bipolardisorder (PBD) profile, defined by clinical increases(T scores 9 70) on the CBCL Attention Problems(AP), Aggression (AGG), and Anxious/Depressed (A/D) subscales scores, may represent a susceptibilityprofile for PBD in children with ADHD.4Y7,9 TheCBCL-PBD profile is highly heritable,5,10,11 and itsgenetic architecture has been established.10 It is clearfrom this previous work that the CBCL-PBD profiledoes not substitute for a categorical DSM-IV diagnosis
Accepted May 21, 2008.Drs. McGough and McCracken are with the Division of Child and Adolescent
Psychiatry at the UCLA Semel Institute for Neuroscience and Human Behaviorand David Geffen School of Medicine; Drs. Loo and Smalley and Mr. Dang arewith the Center for Neurobehavioral Genetics at the UCLA Semel Institute; andDr. Nelson and Ms. Clark are with the Center for Neurobehavioral Genetics atthe UCLA Semel Institute and Department of Human Genetics in the DavidGeffen School of Medicine.This work was supported by National Institute of Mental Health grants
MH01969 (to J.J.M.), HD40275 (to S.K.L.), MH01805 (to J.T.M.),MH071852 (to S.F.N.), and MH58277 (to S.L.S.).The authors dedicate this article to the memory of Richard D. Todd, M.D.,
Ph.D. (1951Y2008).Correspondence to Dr. James J. McGough, 300 UCLA Medical Plaza, Suite
1414, Los Angeles, CA 90095; e-mail: [email protected]/08/4710-1151�2008 by the American Academy of Child and
Adolescent Psychiatry.DOI: 10.1097/CHI.0b013e3181825a68
WWW.JAACAP.COM 1151J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:10, OCTOBER 2008

of bipolar disorder, but serves as a risk profile for severepsychiatric illness.4,7,10
The sum of the scores on the subscales that make upthe PBD profile also provides a putative quantitativetrait suitable for genetic investigation. Unlike discretetraits, which are either present or absent in individuals,quantitative traits occur along continua within popula-tions and provide greater measured variability amongindividuals, which can improve power to detect under-lying genes. The paucity of clear genetic findings in psy-chiatry, in spite of the well-demonstrated heritability ofmany psychiatric disorders, has been attributed in partto their complex nature and the concomitant difficultyin measuring underlying liability with more quantitativeapproaches.12Y14
We previously conducted genomewide linkage stud-ies in our sample of multiple affected sibling pairs andidentified several genetic regions associated with in-creased risk for ADHD, although quantitative trait lo-cus (QTL) analysis of ADHD symptom scores yieldedno significant linkages.15Y18 In the present study, weused CBCL subscales to compare patterns of lifetimepsychiatric comorbidity in the same sample of ADHDyouths. Given that we knew rates of PBD in our samplewere low, we assessed whether subjects meeting CBCL-PBD criteria were characterized by other mood disordersor, alternatively, other patterns of comorbidity. Similarly,we assessed patterns of lifetime psychiatric diagnoses inparents based on their children_s CBCL-PBD status todetermine whether parents from CBCL-PBD familieshad increased rates of bipolar or other mood disordersor, alternatively, to assess other potential differences. Last,we used each ADHD proband_s quantitative CBCL-PBD phenotype to conduct a genomewide QTL anal-ysis in search for genomic regions that may harbor riskgenes influencing severe psychopathology in ADHDsubjects.
METHOD
Subjects
Study subjects were 540 children and adolescents ages 5 to 18 years(mean 10.6, SD 3.2) and 519 of their parents ascertained from 270families with ADHD-affected sibling pairs. Families were included ifat least one child met fullDSM-IV ADHD criteria and a second childhad a diagnosis of definite or probable ADHD, defined as being nomore than one symptom short of full criteria, but with evidence ofimpairment in two settings. All of the families were English speaking.Mean socioeconomic status as defined by Hollingshead19 was 2.4(SD 0.9) (Hollingshead range IYV).
After receiving a full oral explanation of study requirements,subjects provided written informed consent/assent under proce-dures approved by the UCLA Institutional Review Board. Detaileddescriptions of recruitment methods, screening, and subject assess-ment have been previously described.20,21 Briefly, lifetime psychi-atric diagnoses were based on semistructured diagnostic interviewsconducted by clinical psychologists or highly trained interviewerswith extensive experience and reliability training. Children andadolescents were assessed using the Schedule for Affective Disordersand Schizophrenia for School-Age Children-Present and Lifetimeversion (K-SADS-PL).22 Adult parents were assessed using theSchedule for Affective Disorders and Schizophrenia-Lifetime version(SADS-LA-IV),23 supplemented with the K-SADS BehavioralDisorders module for diagnosis of ADHD and disruptive behaviordisorders.22 Direct interviews were supplemented with parent andteacher versions of the Swanson, Nolan, and Pelham, version IV(SNAP-IV) rating scale,24 as well as a parent-completed CBCL andTeacher Report Form.3 Parents also completed current ratings of selfand spouse behavior with the ADHD Rating Scale IV.25
Best estimate diagnoses were assigned using all of the availableclinical information according to strict DSM-IV criteria26 and re-viewed by senior clinicians ( J.J.M., J.T.M.). Themeanweighted. forproband diagnoses was .84 (SD 0.14), including values for ADHD(1.0), oppositional defiant disorder (.93), and conduct disorder (1.0).Meanweighted. for parent diagnoseswas .88 (SD0.10), including val-ues for ADHD (.91), oppositional defiant disorder (.86), and conductdisorder (.83). The mean weighted . comparing agreement betweeninitial rater and best estimate diagnoses for 10 psychiatric conditionsoccurring in more than 5% of all subjects was .95 (SD 0.03).
Procedures
Children and adolescents were assigned to categorical groupswith or without the CBCL-PBD profile based on T scores using pre-viously established thresholds.4,10 The CBCL-PBD group (n = 45)consisted of subjects with T score increases >70 on the CBCL-AP,AGG, and A/D subscales. The CBCL-AP group (n = 103)consisted of subjects with T score increases >70 on the AP subscale,but T score values e70 on AGG and A/D subscales. CBCLcomparison subjects (n = 392) had values e70 on all threesubscales. All of the probands had definite or probable ADHD. Thetotal sample was 72% male and 77% white, with no differences be-tween the three groups for age (F = 0.89, p = .41), sex ratio (W2 =4.20, p = .12), or race (W2 = 1.55, p = .46). In addition, familieswith at least one child meeting CBCL-PBD criteria were classifiedas CBCL-PBD families (n = 42), and those with no child meetingCBCL-PBD criteria were classified as nonYCBCL-PBD families(n = 228). Finally, a quantitative CBCL-PBD phenotype was com-puted for all ADHD probands by summing raw scores on CBCLAP, AGG, and A/D subscales.Genotype data for all of the ADHD probands and parents were
obtained as previously described.15,17 Data were available for 423highly polymorphic markers spanning all 22 autosomes. Densersets of microsatellite and single nucleotide polymorphism markers(~2- or 3-cM density) were included for nine chromosomal regionschosen on the basis of increased linkage peaks in previous genomescan studies of ADHD.16
Data Analysis
Descriptive statistics were summarized and rates of DSM-IV dis-orders in ADHD probands and parents were computed. Sibling
MCGOUGH ET AL.
1152 WWW.JAACAP.COM J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:10, OCTOBER 2008
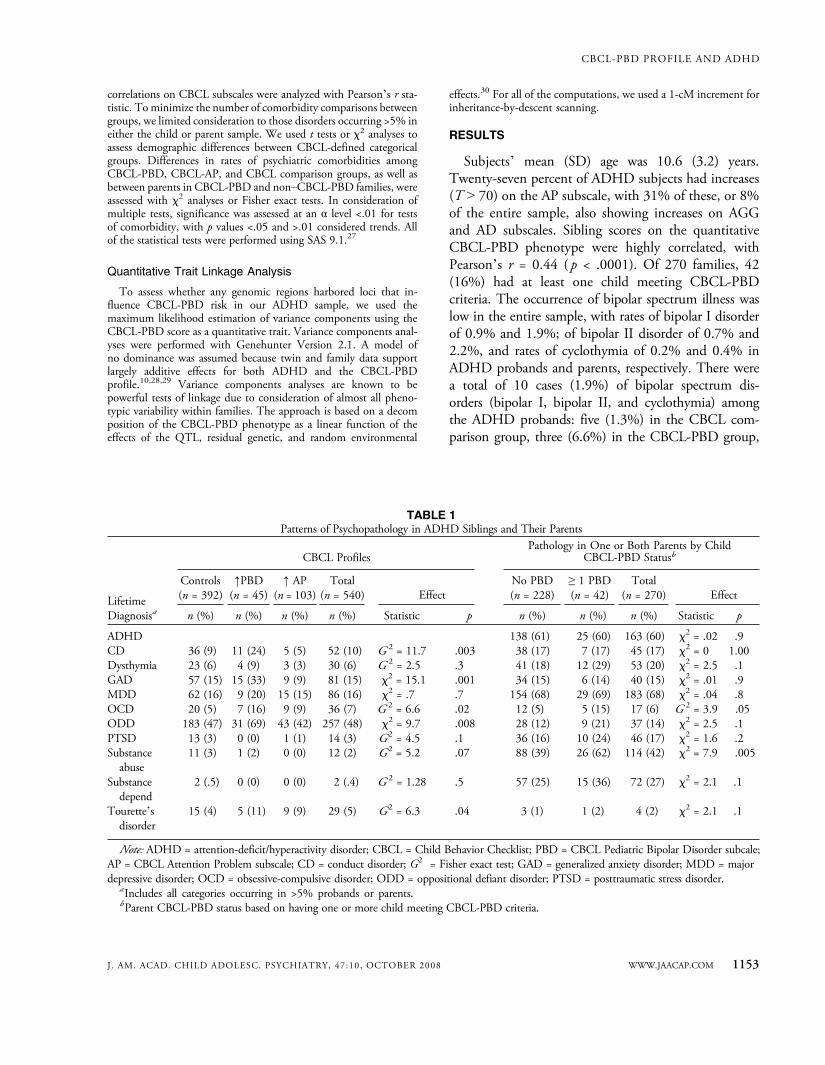
correlations on CBCL subscales were analyzed with Pearson_s r sta-tistic. To minimize the number of comorbidity comparisons betweengroups, we limited consideration to those disorders occurring >5% ineither the child or parent sample. We used t tests or W2 analyses toassess demographic differences between CBCL-defined categoricalgroups. Differences in rates of psychiatric comorbidities amongCBCL-PBD, CBCL-AP, and CBCL comparison groups, as well asbetween parents in CBCL-PBD and nonYCBCL-PBD families, wereassessed with W2 analyses or Fisher exact tests. In consideration ofmultiple tests, significance was assessed at an ! level <.01 for testsof comorbidity, with p values <.05 and >.01 considered trends. Allof the statistical tests were performed using SAS 9.1.27
Quantitative Trait Linkage Analysis
To assess whether any genomic regions harbored loci that in-fluence CBCL-PBD risk in our ADHD sample, we used themaximum likelihood estimation of variance components using theCBCL-PBD score as a quantitative trait. Variance components anal-yses were performed with Genehunter Version 2.1. A model ofno dominance was assumed because twin and family data supportlargely additive effects for both ADHD and the CBCL-PBDprofile.10,28,29 Variance components analyses are known to bepowerful tests of linkage due to consideration of almost all pheno-typic variability within families. The approach is based on a decomposition of the CBCL-PBD phenotype as a linear function of theeffects of the QTL, residual genetic, and random environmental
effects.30 For all of the computations, we used a 1-cM increment forinheritance-by-descent scanning.
RESULTS
Subjects_ mean (SD) age was 10.6 (3.2) years.Twenty-seven percent of ADHD subjects had increases(T 9 70) on the AP subscale, with 31% of these, or 8%of the entire sample, also showing increases on AGGand AD subscales. Sibling scores on the quantitativeCBCL-PBD phenotype were highly correlated, withPearson_s r = 0.44 ( p < .0001). Of 270 families, 42(16%) had at least one child meeting CBCL-PBDcriteria. The occurrence of bipolar spectrum illness waslow in the entire sample, with rates of bipolar I disorderof 0.9% and 1.9%; of bipolar II disorder of 0.7% and2.2%, and rates of cyclothymia of 0.2% and 0.4% inADHD probands and parents, respectively. There werea total of 10 cases (1.9%) of bipolar spectrum dis-orders (bipolar I, bipolar II, and cyclothymia) amongthe ADHD probands: five (1.3%) in the CBCL com-parison group, three (6.6%) in the CBCL-PBD group,
TABLE 1Patterns of Psychopathology in ADHD Siblings and Their Parents
CBCL ProfilesPathology in One or Both Parents by Child
CBCL-PBD Statusb
Controls(n = 392)
jPBD(n = 45)
j AP(n = 103)
Total(n = 540) Effect
No PBD(n = 228)
Q 1 PBD(n = 42)
Total(n = 270) EffectLifetime
Diagnosisa n (%) n (%) n (%) n (%) Statistic p n (%) n (%) n (%) Statistic p
ADHD 138 (61) 25 (60) 163 (60) W2 = .02 .9CD 36 (9) 11 (24) 5 (5) 52 (10) G 2 = 11.7 .003 38 (17) 7 (17) 45 (17) W2 = 0 1.00Dysthymia 23 (6) 4 (9) 3 (3) 30 (6) G 2 = 2.5 .3 41 (18) 12 (29) 53 (20) W2 = 2.5 .1GAD 57 (15) 15 (33) 9 (9) 81 (15) W2 = 15.1 .001 34 (15) 6 (14) 40 (15) W2 = .01 .9MDD 62 (16) 9 (20) 15 (15) 86 (16) W2 = .7 .7 154 (68) 29 (69) 183 (68) W2 = .04 .8OCD 20 (5) 7 (16) 9 (9) 36 (7) G 2 = 6.6 .02 12 (5) 5 (15) 17 (6) G 2 = 3.9 .05ODD 183 (47) 31 (69) 43 (42) 257 (48) W2 = 9.7 .008 28 (12) 9 (21) 37 (14) W2 = 2.5 .1PTSD 13 (3) 0 (0) 1 (1) 14 (3) G2 = 4.5 .1 36 (16) 10 (24) 46 (17) W2 = 1.6 .2Substanceabuse
11 (3) 1 (2) 0 (0) 12 (2) G2 = 5.2 .07 88 (39) 26 (62) 114 (42) W2 = 7.9 .005
Substancedepend
2 (.5) 0 (0) 0 (0) 2 (.4) G 2 = 1.28 .5 57 (25) 15 (36) 72 (27) W2 = 2.1 .1
Tourette_sdisorder
15 (4) 5 (11) 9 (9) 29 (5) G2 = 6.3 .04 3 (1) 1 (2) 4 (2) W2 = 2.1 .1
Note: ADHD = attention-deficit/hyperactivity disorder; CBCL = Child Behavior Checklist; PBD = CBCL Pediatric Bipolar Disorder subcale;AP = CBCL Attention Problem subscale; CD = conduct disorder; G2 = Fisher exact test; GAD = generalized anxiety disorder; MDD = majordepressive disorder; OCD = obsessive-compulsive disorder; ODD = oppositional defiant disorder; PTSD = posttraumatic stress disorder.
a Includes all categories occurring in >5% probands or parents.bParent CBCL-PBD status based on having one or more child meeting CBCL-PBD criteria.
CBCL-PBD PROFILE AND ADHD
WWW.JAACAP.COM 1153J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:10, OCTOBER 2008
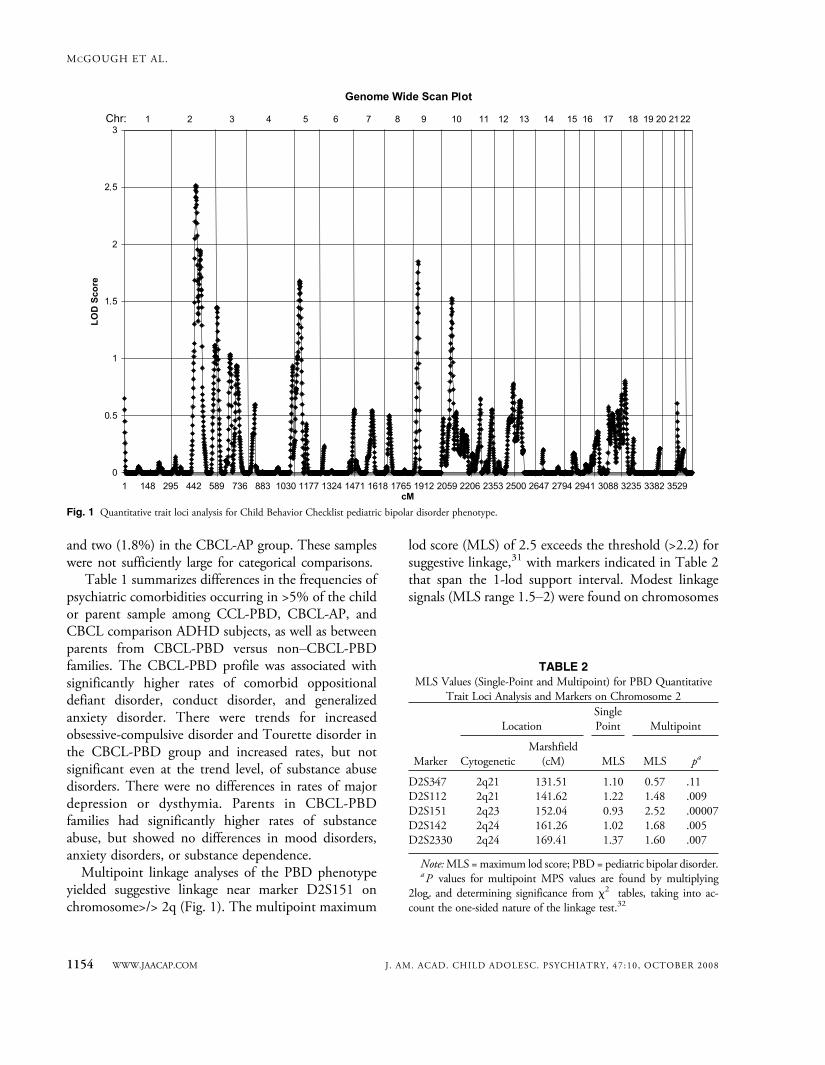
and two (1.8%) in the CBCL-AP group. These sampleswere not sufficiently large for categorical comparisons.
Table 1 summarizes differences in the frequencies ofpsychiatric comorbidities occurring in >5% of the childor parent sample among CCL-PBD, CBCL-AP, andCBCL comparison ADHD subjects, as well as betweenparents from CBCL-PBD versus nonYCBCL-PBDfamilies. The CBCL-PBD profile was associated withsignificantly higher rates of comorbid oppositionaldefiant disorder, conduct disorder, and generalizedanxiety disorder. There were trends for increasedobsessive-compulsive disorder and Tourette disorder inthe CBCL-PBD group and increased rates, but notsignificant even at the trend level, of substance abusedisorders. There were no differences in rates of majordepression or dysthymia. Parents in CBCL-PBDfamilies had significantly higher rates of substanceabuse, but showed no differences in mood disorders,anxiety disorders, or substance dependence.Multipoint linkage analyses of the PBD phenotype
yielded suggestive linkage near marker D2S151 onchromosome>/> 2q (Fig. 1). The multipoint maximum
lod score (MLS) of 2.5 exceeds the threshold (>2.2) forsuggestive linkage,31 with markers indicated in Table 2that span the 1-lod support interval. Modest linkagesignals (MLS range 1.5Y2) were found on chromosomes
TABLE 2MLS Values (Single-Point and Multipoint) for PBD Quantitative
Trait Loci Analysis and Markers on Chromosome 2
Marker
LocationSinglePoint Multipoint
CytogeneticMarshfield
(cM) MLS MLS pa
D2S347 2q21 131.51 1.10 0.57 .11D2S112 2q21 141.62 1.22 1.48 .009D2S151 2q23 152.04 0.93 2.52 .00007D2S142 2q24 161.26 1.02 1.68 .005D2S2330 2q24 169.41 1.37 1.60 .007
Note:MLS =maximum lod score; PBD = pediatric bipolar disorder.aP values for multipoint MPS values are found by multiplying
2loge and determining significance from W2 tables, taking into ac-count the one-sided nature of the linkage test.32
Fig. 1 Quantitative trait loci analysis for Child Behavior Checklist pediatric bipolar disorder phenotype.
MCGOUGH ET AL.
1154 WWW.JAACAP.COM J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:10, OCTOBER 2008

5, 9, and 10, also suggesting regions of nominal linkagethat may merit further study.
DISCUSSION
In a genetically enriched sample of ADHD affectedsibling pairs, the CBCL-PBD profile identified a small(8%) but distinct subset of individuals with severepsychopathology. These results are consistent with anearlier report describing similarly increased ratesof oppositional defiant, conduct, and anxiety disordersin clinical samples.2 Also in other reports, the CBCL-PBD profile identified increased ADHD, oppositionaldefiant disorder, conduct disorder, and suicidality in apopulation-based twin sample11 and increased delin-quency and suicidality in an epidemiological sample.33
The increased rate of substance abuse in the CBCL-PBD sample, although not significant, is notable giventhat many subjects in our sample had not yet enteredthe age of risk of substance use initiation, but is alsoconsistent with previous findings.34 Looking across oursample and others, it is clear that children andadolescents identified by the CBCL-PBD profilepossess significant psychopathology. There remains anongoing clinical imperative to recognize, characterize,and develop more specific treatment strategies for theseseverely ill youths.
Although the potential value of QTL analyses inADHD genetics studies has been discussed,35 we are notaware of any previous studies that have successfully usedthis approach with the quantitative CBCL-PBD pheno-type. Our previous investigations of ADHD symptomscounts within ADHD affected sibling pairs revealed nosignificant evidence of linkage,15 in contrast to when thediscrete ADHD phenotype was used.16 However, in thepresent study using the CBCL-PBD quantitative phe-notype, we found suggestive evidence of linkage on chro-mosome 2 in a region that showed nominal linkage(MLS 1.0) in our first scan of ADHD on the discreteADHD phenotype and later fell below that nominal levelin an extended sample.15,16 Of particular related interestis the recent finding of significant linkage on chromo-some 2q22-q24, the same region underlying our peaklinkage signal, with bipolar disorder in a study of 52families of European descent.36 This region has not, toour knowledge, been previously examined in relation toADHD. These emerging results may support furtherstudy of this region and use of the CBCL-PBD measure
as a susceptibility profile within ADHD to identify pu-tative genes involved in that condition and its clinicalheterogeneity.Although the overall rates of bipolar spectrum ill-
nesses in our sample were lower than in other reports,they still represent up to a twofold increase above adultrates usually described in community samples, but arenot near the increased rates described with ADHD.37 Itis notable that the CBCL-PBD group did have rates ofdiagnosed bipolar spectrum illness three to five timesgreater than those seen in the CBCL comparison andCBCL-AP groups, although these differences were nottestable given the low overall rates in the sample. To oursurprise, the CBCL-PBD profile did not identify sub-jects or families characterized by increased rates of anyDSM-IV mood disorder. This contrasts with numerousprevious investigations1,2,4,6Y9 but is consistent withsome reports.11,33 It is unclear why such large differen-ces in ADHD comorbidity occur across extant studies.Our sample, which required the participation of bothbiological parents, may be biased toward healthier,better functioning families, although in previous reportswe demonstrated expected rates of comorbid disordersand psychiatric impairment.20,21,38 There are subtle as-sessment differences between investigations. Somestudies relied on the epidemiological version of theKSADS, which contains fewer probes and allows lessclinician discretion than the K-SADS-PL used in ourinvestigation.1,37 Other reports used the CBCL itselfas the diagnostic phenotype,5,10,33 without considera-tion of DSM-defined syndromes.Another explanation for the relatively low overall rates
of bipolar spectrum illness seen in our sample is themethod used at our site in interpreting the DSM. PBDhas been defined by some investigators as phenomeno-logically dissimilar from the adult presentation, moretypically characterized by chronic irritability and arelative lack of positive affective features and distinctepisodes.32,34,39Y41 Others have argued that this approachin community settings has led to inconsistent applica-tion of DSM criteria and a general tendency to assign adiagnosis of bipolar disorder to any child with impulsecontrol deficits and affective instability.42Y44 Oneattempt to address the challenges of establishing validsymptomatic boundaries for PBD is a proposed differ-entiation of narrow versus broad bipolar phenotypes.44
The narrow phenotype, which informed our applicationof DSM criteria in this study, is defined by strict DSM
CBCL-PBD PROFILE AND ADHD
WWW.JAACAP.COM 1155J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:10, OCTOBER 2008

criteria for mania or hypomania, including discreteepisodes of elevated, expansive, or irritable mood. Incontrast, the broad phenotype is defined by chronic,nonepisodic illness that generally lacks the hallmarksymptoms of grandiosity and hyperarousal. The pre-dominance of anxiety, oppositional defiant disorder,and conduct disorder in our CBCL-PBD group is moresuggestive of the chronic irritability described with thebroad PBD phenotype. It is noteworthy that while theCBCL-PBD profile failed to differentiate ADHD pro-bands or parents with higher rates of mood disorders,almost 70% of all families had evidence of lifetimeparental depression. The overall high rates of depressionin these parents have previously been described and mayreflect the psychosocial stress of raising multiple siblingswith ADHD, in addition to any underlying biologicalpredisposition.20 Particularly in view of our linkage find-ings, the increased rates of psychoactive substance abusein parents of CBCL-PBD families favors a biological eti-ology for these disorders that merits further investigation.There should be no disagreement, however, on the
existence of a distinct pediatric syndrome characterizedby chronic irritability and affective instability. Our sug-gestive linkage findings provide supporting evidence of abiological basis for this subgroup of ADHD patients. Aswe develop future editions of the DSM, the nosologicalchoice to be made is whether we should continue todescribe these individuals as bipolar, while acknowledgingdevelopmental differences in younger patients, or insteadoperationalize a new diagnostic category that avoidsconfusion with the typical adult bipolar presentation. Aspreviously proposed, the CBCL-PBD profile appearsuseful as a standardized measure in understandingsubjects across studies and in potentially identifying bio-logical susceptibility to severe comorbidity.This study has several methodological limitations.
First, in constructing our CBCL categories, we relied onpreviously described group thresholds.4,10 Other groupshave demonstrated that slightly lower cutoffs points orquantitative interpretations of the CBCL-PBD scalelead to increased sensitivity for detecting comorbidpathology.5,7 However, because our interest was in char-acterizing subjects who met the originally defined cate-gorical CBCL-PBD cutoff, not in establishing thepredictive power of the rating, we chose to use the moreconservative threshold. This also reflected our wish toavoid repeated testing at various threshold levels in anattempt to force the data to fit some a priori expectation.
Second, we relied on a model of additive effects in ourQTL analysis, based on some previous studies.10,29
However, other work has suggested that ADHDmay beinherited under a dominant model.45 Although thisremains a possibility, in QTL analysis, the power todetect a dominant or recessive effect (if present) is gener-ally greater than additive alone across a range of allelefrequencies and residual polygenic effects.46 Thus, mis-specification of our inheritance model would, in fact,reduce the power available to detect genetic effects. Fi-nally, the study dataset has been used in previousgenomewide scans for ADHD and reading disor-der.15Y18,47 Although linkage peaks identified in thisstudy do not overlap with these previous scans, we chosenot to emphasize nominal linkage peaks due to the in-creased probability of type I error. Our findings need beconsidered with caution in light of the multiple pheno-type testing in the sample. They are offered as prelim-inary data for comparison with other groups using thisquantitative trait. Replication is needed before furtherinvestigation (i.e., fine mapping and single nucleotidepolymorphism association studies) is warranted.This study may be one of the first to identify a
suggestive genetic association with such severe behav-ioral problems in children. It remains unclear whetherthe CBCL-PBD profile serves to identify a more homo-geneous group of children with ADHD or whether itis also useful in identifying severe psychopathology inindividuals without ADHD. The question is relevantas one considers whether the identified individuals shouldbe viewed as suffering from a severe ADHD subtype ora separate, but commonly comorbid, condition. Consen-sus on the diagnostic classification of these patients willenhance ongoing research and support-directed treatmentstudies that will provide a basis for improved clinicalmanagement.
Disclosure: Dr. McGough has served as a consultant to Eli Lilly, JanssenPharmaceuticals, and Shire Pharmaceuticals and has received researchsupport from Eli Lilly, Janssen, and Shire. Dr. McCracken has served asa consultant to Abbott, Janssen, Pfizer, Sanofi-Aventis, and Wyeth andhas received research support from Aspect, Bristol-Myers Squibb, EliLilly, and Janssen and speaker honoraria from UCB. The other authorsreport no conflicts of interest.
REFERENCES
1. Biederman J, Monuteaux MC, Kendrick E, Klein KL, Faraone SV. TheCBCL as a screen for psychiatric comorbidity in paediatric patients withADHD. Arch Dis Child. 2005;90:1010Y1015.
MCGOUGH ET AL.
1156 WWW.JAACAP.COM J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:10, OCTOBER 2008
2. Biederman J, Wozniak J, Kiely K, et al. CBCL clinical scales discriminateprepubertal children with structured interview-derived diagnosis of maniafrom those with ADHD. J Am Acad Child Adolesc Psychiatry. 1995;34:464Y471.
3. Achenbach TM. Manual for the Child Behavior Checklist/4-18 and 1991profile. Burlington: University of Vermont, Department of Psychiatry;1991.
4. Mick E, Biederman J, Pandina G, Faraone SV. A preliminary meta-analysis of the child behavior checklist in pediatric bipolar disorder.Biol Psychiatry. 2003;53:1021Y1027.
5. Althoff RR, Rettew DC, Faraone SV, Boomsa DI, Hudziak JJ. Latentclass analysis shows strong heritability of the child behavior checklist-juvenile bipolar disorder phenotype. Biol Psychiatry. 2006;60:903Y911.
6. Dienes KA, Chang KD, Blasey CM, Adleman NE, Steiner H. Char-acterization of children of bipolar parents by parent report CBCL.J Psychiatr Res. 2002;36:337Y345.
7. Faraone SV, Althoff RR, Hudziak JJ, Monuteaux M, Biederman J.The CBCL predicts DSM bipolar disorder in children: a receiver oper-ating characteristic curve analysis. Bipolar Disord. 2005;7:518Y524.
8. Geller B, Warner K, Williams M, Zimerman B. Prepubertal andyoung adolescent bipolarity versus ADHD: assessment and validityusing the WASH-U-KSADS, CBCL, and TRF. J Affect Disord. 1998;51:93Y100.
9. Hazell PL, Lewin TJ, Carr VJ. Confirmation that Child BehaviorChecklist clinical scales discriminate juvenile mania from attentiondeficit/hyperactivity disorder. J Pediatr Child Health. 1999;35:199Y203.
10. Hudziak JJ, Althoff RR, Derks EM, Faraone SV, Boomsma DI.Prevalence and genetic architecture of child-behavior checklist-juvenilebipolar disorder. Biol Psychiatry. 2005;58:562Y568.
11. Volk H, Todd R. Does the child behavior checklist juvenile bipolardisorder phenotype identify bipolar disorder? Biol Psychiatry.2007;62:115Y120.
12. Dean M. Approaches to identify genes for complex human diseases:lessons from Mendelian disorder. Hum Mutat. 2003;22:261Y274.
13. Kendler KS. Psychiatric genetics; a methodologic critique. Am JPsychiatry. 2005;162:3Y11.
14. Risch N. Searching for genetic determinants in the new millennium.Nature. 2000;405:847Y856.
15. Fisher SE, Franks C, McCracken JT, et al. A genome-wide scan for lociinvolved in attention-deficit/hyperactivity disorder (ADHD). Am J HumGenet. 2002;70:1183Y1196.
16. Ogdie MN, Fisher SE, Yang M, et al. Attention deficit hyperactivitydisorder: fine mapping support linkage to 5p13, 6q12, 16p13, and17p11. Am J Hum Genet. 2004;75:661Y668.
17. Ogdie MN, Macphie IL, Minassian SL, et al. A genome-wide scan forattention-deficit/hyperactivity disorder in an extended sample: suggestivelinkage on 17p11. Am J Hum Genet. 2003;72:1268Y1279.
18. Smalley SL, Kustanovich V, Minassian SL, et al. Genetic linkage ofattention-deficit hyperactivity disorder (ADHD) on chromosome16p13 in a region implicated in autism. Am J Hum Genet. 2002;71:959Y963.
19. Hollingshead AB. Two-Factor Index of Social Position. New Haven, CT:Yale University Press; 1957.
20. McGough JJ, Smalley SL, McCracken JT, et al. Psychiatric comorbidityin adult attention deficit hyperactivity disorder: findings from multiplexfamilies. Am J Psychiatry. 2005;162:1621Y1627.
21. Smalley S, McGough J, Del_Homme M, et al. Familial clustering ofsymptoms and disruptive behaviors in multiplex families with attentiondeficit hyperactivity disorder. J Am Acad Child Adolesc Psychiatry.2000;39:1135Y1143.
22. Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disordersand Schizophrenia for School-Age ChildrenYPresent and LifetimeVersion (KSADS-PL): initial reliability and validity data. J Am AcadChild Adolesc Psychiatry. 1997;36:980Y988.
23. Fyer AJ, Mannuzza SM, Klein DF, Endicott J. Schedule for AffectiveDisorders and SchizophreniaYLifetime Version Modified for the Study ofAnxiety Disorders (SADS-LA), Updated for DSM IV (SADS-LA IV). NewYork: New York State Psychiatric Institute; 1995.
24. Swanson JM. SNAP-IV Scale. Irvine, CA: University of California IrvineChild Development Center; 1995.
25. DuPaul GJ, Power TJ, Anastopoulos AD, Reid R. ADHD Rating ScaleIV: Checklists, Norms, and Clinical Interpretation. New York: GuilfordPress; 1998.
26. Leckman JF, Sholomskas D, Thompson WD, Belanger A, WeissmanMM. Best estimate of lifetime psychiatric diagnosis: a methodologicalstudy. Arch Gen Psychiatry. 1982;39:879Y883.
27. SAS Version 9.1. Cary, NC: SAS Institute; 2006.28. Smalley SL. Genetic influences in childhood-onset psychiatric disorders:
autism and attention-deficit/hyperactivity disorder. Am J Hum Genet.1997;60:1276Y1282.
29. Derks EM, Dolan CV, Hudziak JJ, Neale MC, Boomsma DI.Assessment and etiology of attention deficit hyperactivity disorder andoppositional defiant disorder in boys and girls. Behav Genet. 2007;37:559Y566.
30. Blangero J, Williams JT, Almasy L. Quantitative trail locus mappingusing human pedigrees. Hum Biol. 2000;72:35Y62.
31. Lander E, Kruglyak L. Genetic dissection of complex traits: guidelinesfor interpreting and reporting linkage results. Nat Genet. 1995;11:241Y247.
32. Wozniak J, Biederman J, Kwon A, et al. How cardinal are cardinalsymptoms in pediatric bipolar disorder? An examination of clinicalcorrelates. Biol Psychiatry. 2005;58:583Y588.
33. Holtmann M, Bolte S, Goth K, et al. Prevalence of the Child BehaviorChecklist-pediatric bipolar disorder phenotype in a German generalpopulation sample. Bipolar Disord. 2007;9:895Y900.
34. Wozniak J, Spencer T, Biederman J, Kwon A, Monuteaux M, Rettew J.The clinical characteristics of unipolar vs. bipolar major depression inADHD youth. J Affect Disord. 2004;82(Suppl 1):S59YS69.
35. Todd RD. Genetics of attention deficit/hyperactivity disorder: are weready for molecular genetic studies? Am J Med Genet. 2000;96:241Y243.
36. Abou Jamra R, Fuerst R, Kaneva R, et al. The first genomewideinteraction and locus-heterogeneity linkage scan in bipolar affectivedisorder: strong evidence of epistatic effects between loci on chromo-somes 2q and 6q. Am J Hum Genet. 2007;81:974Y986.
37. Wozniak J, Biederman J, Kiely K, et al. Mania-like symptoms suggestiveof childhood-onset bipolar disorder in clinically referred children. J AmAcad Child Adolesc Psychiatry. 1995;34:867Y876.
38. Smalley SL, McGough JJ, Moilanen IK, et al. Prevalence and psychiatriccomorbidity of attention deficit hyperactivity disorder in an adolescentFinnish population. J Am Acad Child Adolesc Psychiatry. 2007;46:1575Y1583.
39. Carlson GA, Meyer SE. Phenomenology and diagnosis of bipolardisorder in children, adolescents, and adults: complexities and develop-mental issues. Dev Psychopathol. 2006;18:939Y969.
40. Geller B, Luby J. Child and adolescent bipolar disorder: a review of thepast 10 years. J Am Acad Child Adolesc Psychiatry. 1997;36:1168Y1176.
41. Mick E, Spencer T, Wozniak J, Biederman J. Heterogeneity of irritabilityin attention-deficit/hyperactivity disorder subjects with and withoutmood disorders. Biol Psychiatry. 2005;58:576Y582.
42. Blader JC, Carlson GA. Increased rates of bipolar disorder diagnosesamong U.S. child, adolescent, and adult inpatients, 1996-2004. BiolPsychiatry. 2007;62:107Y114.
43. Pogge DL, Wayland-Smith D, Zaccario M, Borgaro S, Stokes J, HarveyPD. Diagnosis of manic episodes in adolescent inpatients: structureddiagnostic procedures compared to clinical chart diagnoses. Psychiatry Res.2001;101:47Y54.
44. Leibenluft E, Charney DS, Towbin KE, Bhangoo RK. Defining clinicalphenotypes of juvenile mania. Am J Psychiatry. 2003;160:430Y437.
45. Hudziak JJ, Derks EM, Althoff RR, Rettew DC, Boomsma DI. Thegenetic and environmental contributions to attention deficit hyperactiv-ity disorder as measured by the Conners_ rating scalesYrevised. Am JPsychiatry. 2005;162:1614Y1620.
46. Alcaıs A, Abel L. Linkage analysis of quantitative trait loci: sibpairs orsibships? Hum Hered. 2000;50:251Y256.
47. Loo SK, Fisher SE, Francks C, et al. Genome-wide scan of readingability in affected sibling pairs with attention-deficit/hyperactivitydisorder: unique and shared genetic effects. Mol Psychiatry. 2004;9:485Y493.
CBCL-PBD PROFILE AND ADHD
WWW.JAACAP.COM 1157J . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 47:10, OCTOBER 2008