case study liver cirrhosis
DESCRIPTION
Anatomy, decription, statistic, currrent trendsTRANSCRIPT
INTRODUCTION
The liver is the largest and one of the most internal organs, performing more than 400
functions and affecting every system in the body. When the liver is diseased or damage, it cannot
provide digestion, nutrition and metabolism can be severely affected. Liver disease ranged in
severity from mild to hepatic inflammation to chronic end stage cirrhosis.
Liver cirrhosis is extensive, irreversible scaring of the liver, usually caused by a chronic
reaction to hepatic inflammation and necrosis. The diseased typically develops slowly and has a
progressive, prolonged, destructive course resulting in end-stage liver disease. The most common
causes for cirrhosis in the United States are alcoholic liver disease and hepatitis C. Worldwide,
hepatitis b and hepatitis D are leading causes. Without liver transplantation, cirrhosis is usually
fatal.
Cirrhosis is characterized by widespread fibrotic (scarred) bands of connective tissue that
changed the liver’s normal makeup. Inflammation caused by either toxins or diseased results in
extensive degeneration and destruction of hepatocytes (liver cells). As cirrhosis develops, the
tissue becomes nodular. These nodules can block bile ducts and normal blood flow throughout
the liver. Impairments in blood and lymph flow result from compression caused by excessive
fibrous tissue. In early diseased, the liver enlarged, firm, and hard. As the pathologic process
continues, the liver shrinks in size, resulting in decreased in function, which can occurs in weeks
to years (40% of chronic patient are asymptomatic). This impaired liver function results in
elevated serum liver enzymes.
Cirrhosis of the liver can divided into several types, depending on the cause of the disease;
Laennec’s or alcohol cirrhosis (caused by chronic alcolism)
Postnecrotic cirrhosis (caused by viral hepatitis and certain drugs or chemicals)
Biliary cirrhosis (also called choloestatis; caused by chronic biliary obstruction,
usually from gallbladder disease)
Cardiac cirrhosis (caused by heart failure as rare complication)
1
Cirrhosis, along with the resulting ascites, can be treated with the fallowing interventions:
fluid restriction of 1,000 to 1,500 mL per day, sodium restriction (limited to 200 to 500 mg per
day) and diuretic therapy. Spironolactone (Aldactone) is the diuretic of choices because of its
potassium sparing properties. However, amiloride (Moduretic) or triamterene (Dyazide or
Maxzide) may also be used if the patient is compliant with sodium and fluid restrictions,
furosemide (lasix) may be added. Further management can be paracentesis, peritonevenous
shunt, and transjugular intrahepatic portosystemic shunt. Paracentesis is the limited removal of
fluid from the peritoneal cavity for diagnostic or therapeutic purposes. This can be performed at
the bedside. It is most often used palliatively to reduce abdominal pressure which can cause
respiratory distress and abdominal pain. Fluid is removed slowly to avoid hypovolemic shock.
The peritoneal fluid contains plasma proteins and electrolytes. Usually only 750 to 1,000 mL are
removed at a time; however, larger volumes of 3 to 5 liters or more have been reported in the
literature. Before the procedure, the nurse has the patient empty their bladder to decrease the
possibility of injury to the bladder. Baseline vital signs, regularity of heartbeat (or
elevctrocardiogram (ECG)), weight level of consciousness (LOC), and abdominal girt need to be
recorded. A consent from required, so the nurse should allow for the patient questions and
ascertain the understanding of the procedure. During and after the procedure, the nurse need to
monitor the patient for hemodynamic changes, acid base imbalances, and signs of electrolyte
depletion. Cardiac arrhythmias may result from depletion of potassium or hypovolemia.
Temperature is monitored to assess for infection, dressings are assessed for leakage, and urine is
measured to ensure adequate output. The head of the bed can be kept at 30 degrees to allow for
maximal respiratory to expansion and minimize shortness of breath.
When ascites continues to be problem, a surgical shunt to divert excessive peritoneal fluid
into the venous system may be attempted. A LeVeenperitoneovenous shunt (LPVS) diverts
ascetic fluid via pressure-sensitive one way valve from the peritoneum to the internal jugular
vein and ultimately into the superior vena cava. The movement of respiration helps to pump fluid
through the abdomen, allowing fluid to move toward the heart and reenter the vascular system.
With the plasma proteins and electrolytes circulating, perfusion of the kidneys is improved,
urinary output can increase, and there can be an increase in renal system excretion. Clinical
improvements could include decrease abdominal girth, and weight loss.
2
Cirrhosis can occur as a result of many factors and diseases. Alcohol has a direct toxisc effect
on hapatocytes and causes liver inflammation (alcoholic hepatitis). The liver becomes enlarged,
with cellular degeneration and infiltration by fat, leukocytes, and lympocytes. Over time, the
inflammatory process decreases and the destructive phase increases. Early scar formation is
caused fibroblast infiltration and collagen formation. Damage the liver tissue progresses as
malnutrition and repeated expoxure to the alcohol continue. If alcohol is withheld, the fatty
infiltration and inflammation is reversible. If alcohol abuse continues, widespread scar tissue
formation and fibrosis infiltrate the liver as a result of celluar necrosis. The amounh of alcohol
necessary cause cirrhosis varies widely from the person to person, and there are gender
differences. In women, it may take as few two to three drinks per day over a minnimum of 10
years. In men, perhaps six drinks per day over the same time period may be needed cause
disesase. Binge drinking can increase risk for hepattis and fatty liver.
Hepatitis C is now the leading cause of cirrhosis in the United States. It is an infectious
bllodborne illness that usually cause chronic disease. Inflammation caused by infection over time
leads to progressive scarring of the liver. It usually takes decades for cirrhosis to develop,
although alcohol use in combination with hepatitis C may speed the process.
Hepattis B and hepatitis D are the most common causes of cirrhosis worldwide. Hepatitis B
also causes inflammation and low-grade damage over decades that can ultimately lead to
cirrhois.(Ignatavicus& Workman,2008)
REASON FOR CHOOSING
We as a student nurse choose this case to come up with a more in depth understanding of
the disease liver cirrhosis, for us to be able to come up with the quality of care for our patient,
and also to gain knowledge and to make appropriate observations, understanding the rationale for
the activities performed, and appreciate how differences among individuals who are dealing to
this certain disease. We as an individual make us vigilant to be more aware on our health status.
NUMBER OF CASES/STATISTICS DATA OF THE DISEASE
Approximately 1 in 12 persons worldwide, or some 500 million people, are living with chronic
viral hepatitis ;1 million of those who are infected die each year, primarily from cirrhosis or liver
cancer resulting from their hepatitis B and hepatitis C infections .Many of those who are
3
chronically infected with viral hepatitis are unaware of their infection as the virus can go 20 to
30 years before they develop symptoms or feel sick. As a result, even though a person has no
symptoms and may appear healthy, the virus can still be detected in the blood and damage to the
liver can still be occurring.
Viral hepatitis is among the top 10 infectious disease killers and the leading cause of liver cancer
and cirrhosis. Both chronic hepatitis B and chronic hepatitis C cause approximately 80% of the
world's liver cancer and cirrhosis that have contributed to the increases in rates of liver cancer in
recent decades.(CDC, 2012)
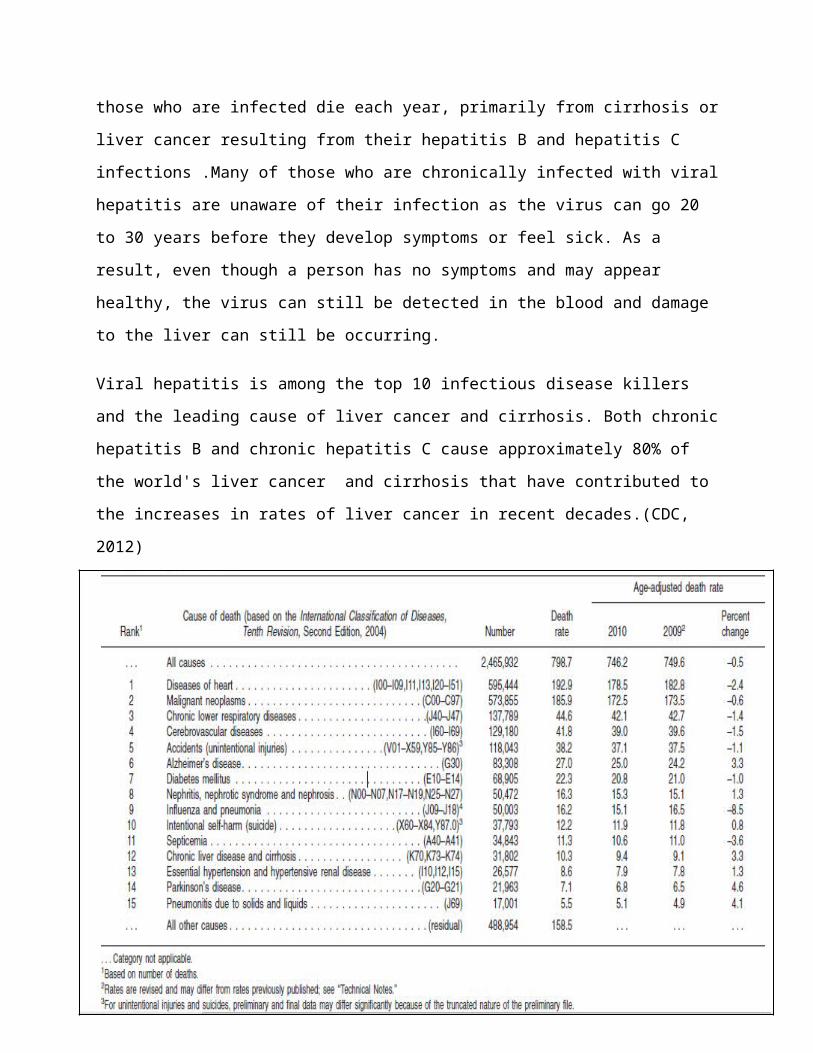
Top Leading Causes of Death from 2009 to 2010
(Figure 1: Top Leading Causes of Death from 2009 to 2010)
4
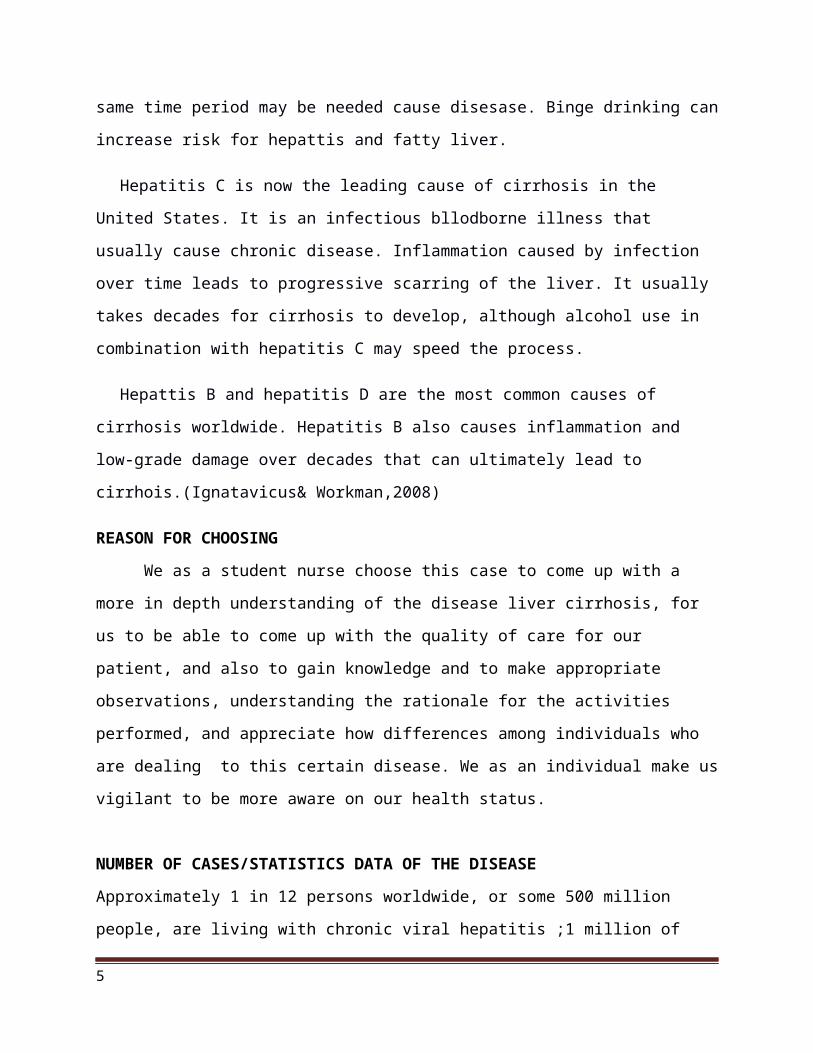
Chronic liver and cirrhosis is ranked 9th with 311,802 number of deaths out 2,465,932 on
top causes of death worldwide. It has a death rate of 10.3 out of 798.7 death rates.
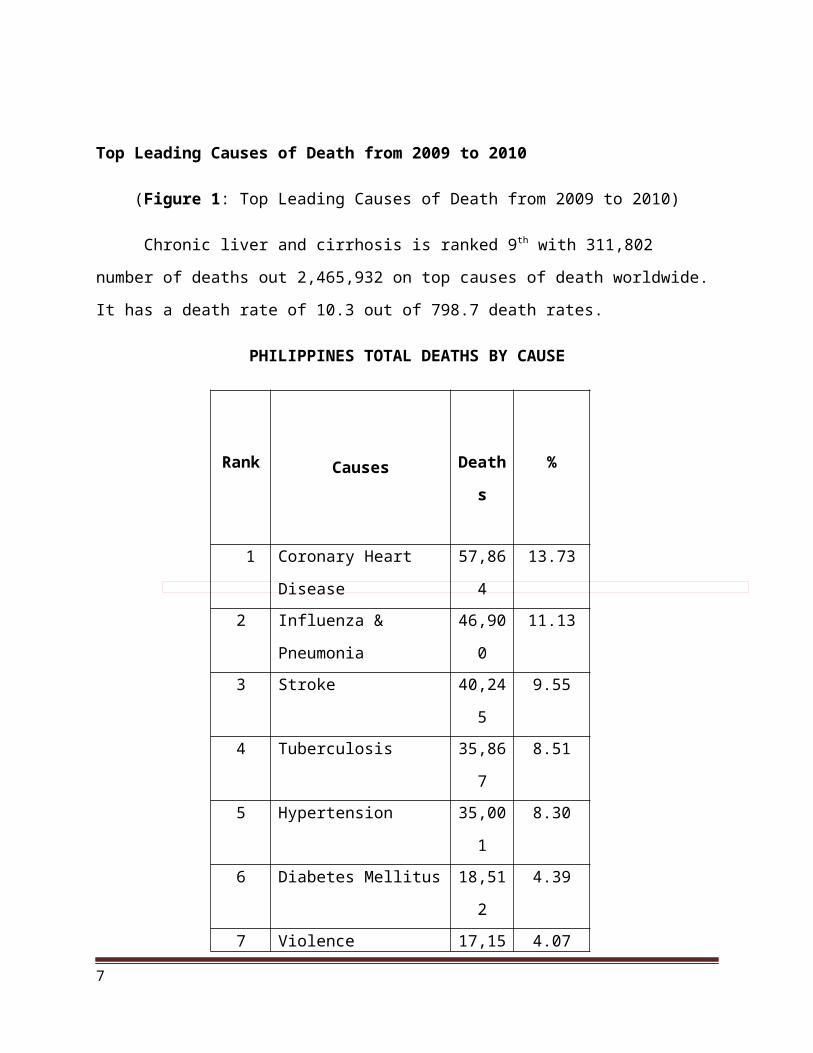
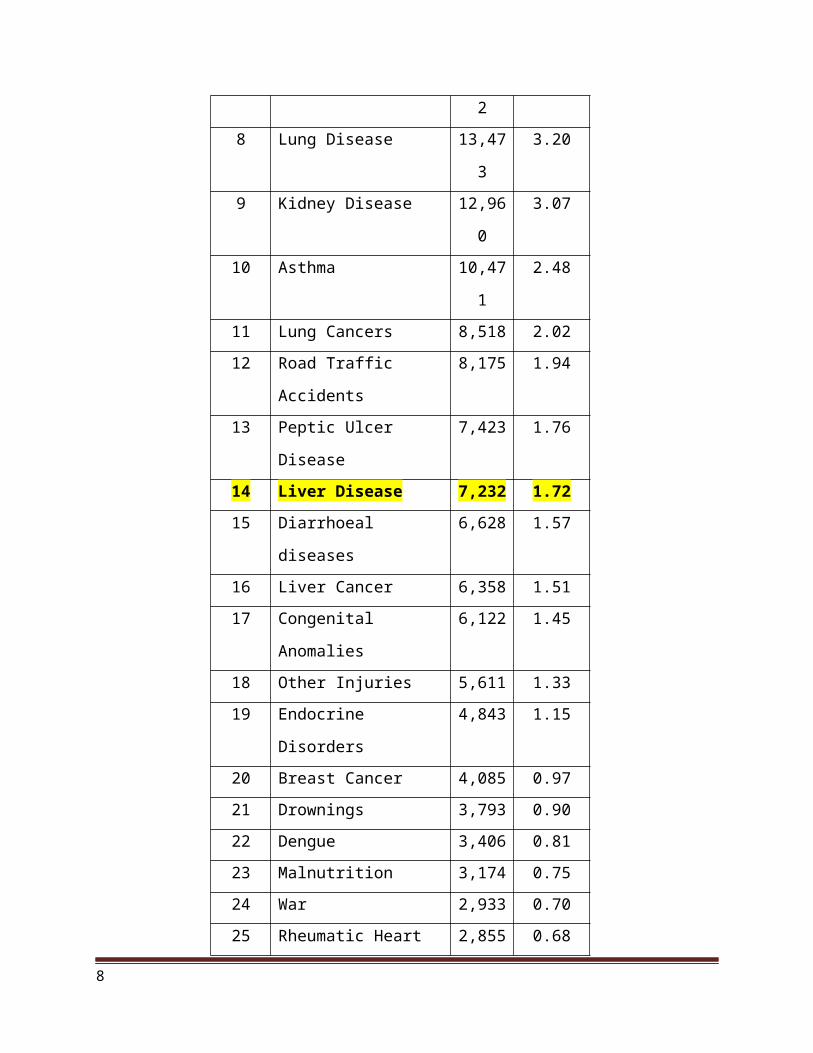
PHILIPPINES TOTAL DEATHS BY CAUSE
Rank Causes Deaths %
1 Coronary Heart Disease 57,864 13.73
2 Influenza & Pneumonia 46,900 11.13
3 Stroke 40,245 9.55
4 Tuberculosis 35,867 8.51
5 Hypertension 35,001 8.30
6 Diabetes Mellitus 18,512 4.39
7 Violence 17,152 4.07
8 Lung Disease 13,473 3.20
9 Kidney Disease 12,960 3.07
10 Asthma 10,471 2.48
11 Lung Cancers 8,518 2.02
12 Road Traffic Accidents 8,175 1.94
13 Peptic Ulcer Disease 7,423 1.76
14 Liver Disease 7,232 1.72
15 Diarrhoeal diseases 6,628 1.57
16 Liver Cancer 6,358 1.51
17 Congenital Anomalies 6,122 1.45
18 Other Injuries 5,611 1.33
19 Endocrine Disorders 4,843 1.15
20 Breast Cancer 4,085 0.97
21 Drownings 3,793 0.90
22 Dengue 3,406 0.81
23 Malnutrition 3,174 0.75
5
24 War 2,933 0.70
25 Rheumatic Heart Disease 2,855 0.68
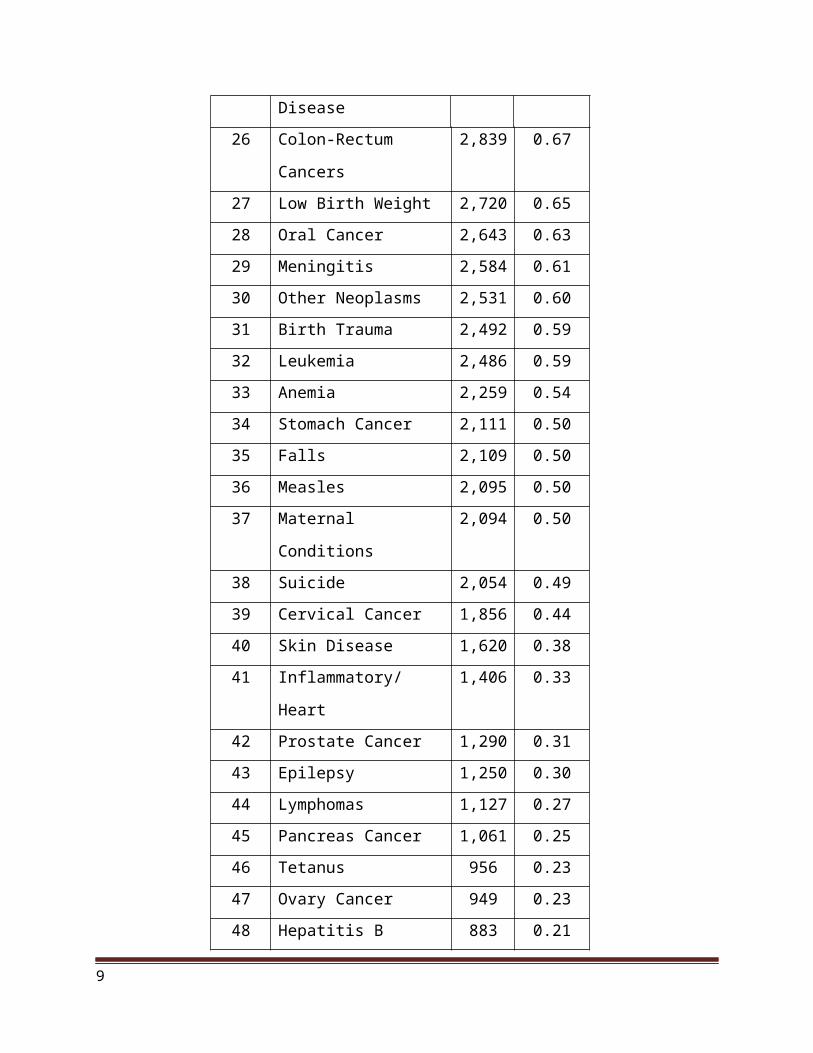
26 Colon-Rectum Cancers 2,839 0.67
27 Low Birth Weight 2,720 0.65
28 Oral Cancer 2,643 0.63
29 Meningitis 2,584 0.61
30 Other Neoplasms 2,531 0.60
31 Birth Trauma 2,492 0.59
32 Leukemia 2,486 0.59
33 Anemia 2,259 0.54
34 Stomach Cancer 2,111 0.50
35 Falls 2,109 0.50
36 Measles 2,095 0.50
37 Maternal Conditions 2,094 0.50
38 Suicide 2,054 0.49
39 Cervical Cancer 1,856 0.44
40 Skin Disease 1,620 0.38
41 Inflammatory/Heart 1,406 0.33
42 Prostate Cancer 1,290 0.31
43 Epilepsy 1,250 0.30
44 Lymphomas 1,127 0.27
45 Pancreas Cancer 1,061 0.25
46 Tetanus 956 0.23
47 Ovary Cancer 949 0.23
48 Hepatitis B 883 0.21
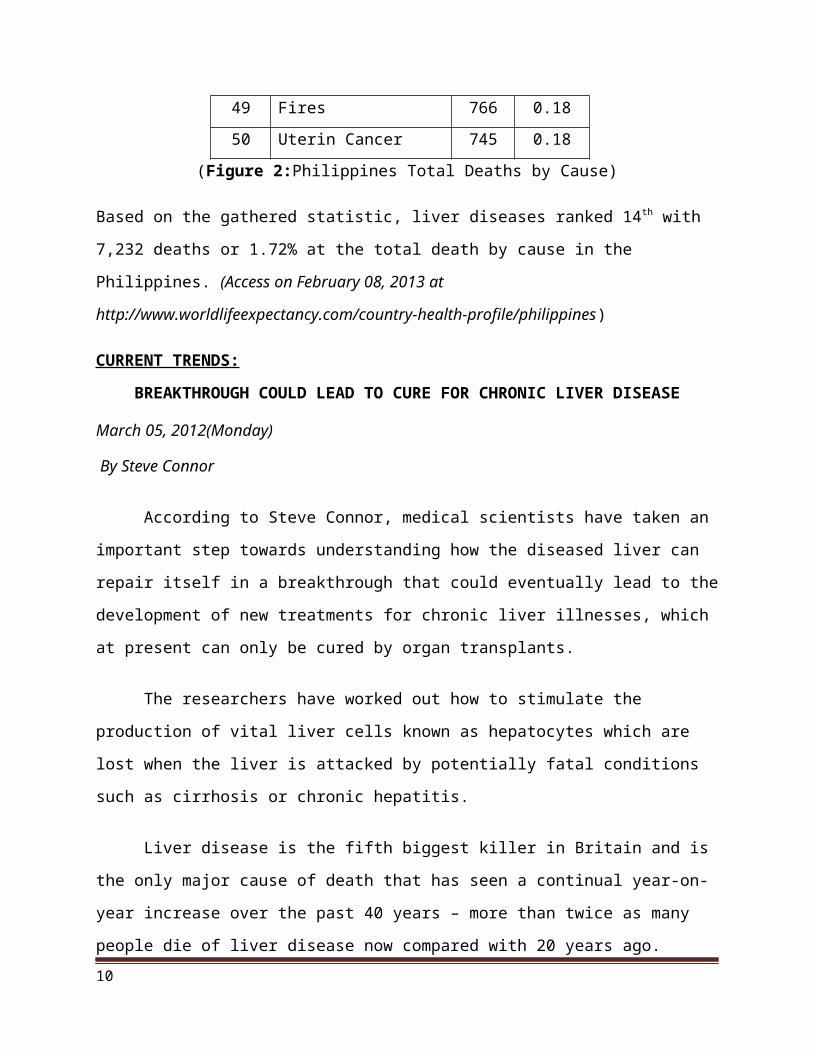
49 Fires 766 0.18
50 Uterin Cancer 745 0.18
(Figure 2:Philippines Total Deaths by Cause)
Based on the gathered statistic, liver diseases ranked 14th with 7,232 deaths or 1.72% at the total
death by cause in the Philippines. (Access on February 08, 2013 at
http://www.worldlifeexpectancy.com/country-health-profile/philippines)
6
CURRENT TRENDS:
BREAKTHROUGH COULD LEAD TO CURE FOR CHRONIC LIVER DISEASE
March 05, 2012(Monday)
By Steve Connor
According to Steve Connor, medical scientists have taken an important step towards
understanding how the diseased liver can repair itself in a breakthrough that could eventually
lead to the development of new treatments for chronic liver illnesses, which at present can only
be cured by organ transplants.
The researchers have worked out how to stimulate the production of vital liver cells
known as hepatocytes which are lost when the liver is attacked by potentially fatal conditions
such as cirrhosis or chronic hepatitis.
Liver disease is the fifth biggest killer in Britain and is the only major cause of death that
has seen a continual year-on-year increase over the past 40 years – more than twice as many
people die of liver disease now compared with 20 years ago.
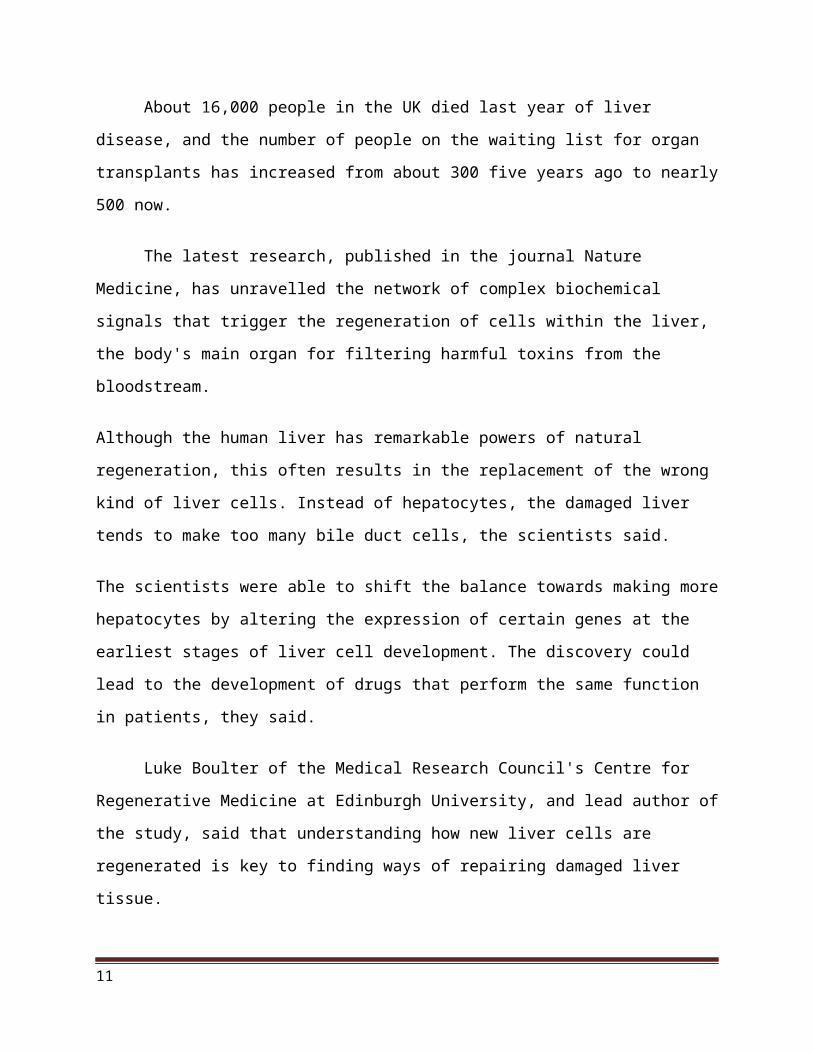
About 16,000 people in the UK died last year of liver disease, and the number of people
on the waiting list for organ transplants has increased from about 300 five years ago to nearly
500 now.
The latest research, published in the journal Nature Medicine, has unravelled the network
of complex biochemical signals that trigger the regeneration of cells within the liver, the body's
main organ for filtering harmful toxins from the bloodstream.
Although the human liver has remarkable powers of natural regeneration, this often results in the
replacement of the wrong kind of liver cells. Instead of hepatocytes, the damaged liver tends to
make too many bile duct cells, the scientists said.
The scientists were able to shift the balance towards making more hepatocytes by altering the
expression of certain genes at the earliest stages of liver cell development. The discovery could
lead to the development of drugs that perform the same function in patients, they said.
7
Luke Boulter of the Medical Research Council's Centre for Regenerative Medicine at
Edinburgh University, and lead author of the study, said that understanding how new liver cells
are regenerated is key to finding ways of repairing damaged liver tissue.
"This research helps us to know how to increase numbers of cells that are needed for
healthy liver function and could pave the way to finding drugs that help liver repair," DrBoulter
said.
Professor Stuart Forbes, associate director of the Centre for Regenerative Medicine, said
such studies are needed to tackle the increase in demand for liver transplants. "But the supply of
donated organs is not keeping pace with the demand. If we can find ways to encourage the liver
to heal itself then we could ease the pressure on waiting lists."
500: The number of people in the UK on the waiting list for organ transplants, up from
300: five years ago
8
OBJECTIVES:
After 8 hours of nurse-interaction, each of the student nurses will be able to:
Cognitive
1. To gain a deep knowledge about liver cirrhosis, its etiology, disease process, risk factors,
signs and symptoms and its treatment.
2. Broaden the understanding concerning the nature of the disease.
3. Impart the information to the concerned individuals most especially to those persons with
this kind of disease.
Psychomotor
1. Enhanced nursing skills in applying nursing management.
2. Improved critical thinking in making nursing care plan according to patient’s health
status.
3. To apply well learned skills in some advance procedure as part of interventions in
said disease.
Affective
1. Improved sense of responsibility and appropriate attitude in dealing with patient.
2. Enhanced self-confidence in handling and giving care for the patient.
3. Perceive positive behaviour in and maintaining wellness on patient’s condition
9
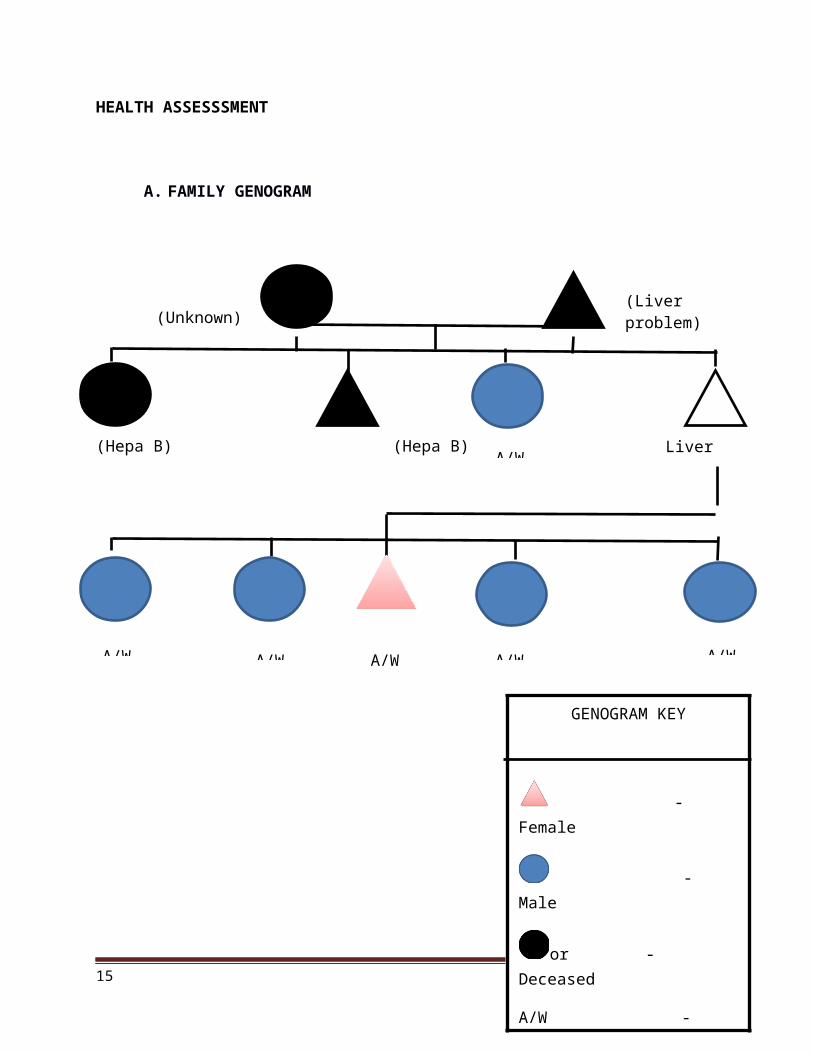
HEALTH ASSESSSMENT
A. FAMILY GENOGRAM
(Hepa B) (Hepa B)
10
(Liver problem)(Unknown)
Liver cirrhosis
Unknown
A/W A/W A/W A/W A/W
A/W
GENOGRAM KEY
- Female
- Male
or - Deceased
A/W - Alive and well
( ) - Cause of death
- Patient
(Figure 3: Family Genogram)
PHYSICAL ASSESSMENT
January 31, 2013(Thursday)
The following information was taken from the chart dated January 31, 2013, 6:45am.
Skin
- Swollen skin
Head and neck
-sclera, pale palpebral, conjunctiva
Thorax and lungs
-SCE, clear breath sounds
Heart
-Adynamic pericardium, normal rate regular rhythm, (-) murmur
Abdomen
Distended abdomen, GI fluid masses
Extremities
- (+) edema
Admitting diagnosis
- To consider massive Ascites secondary to liver cirrhosis
11
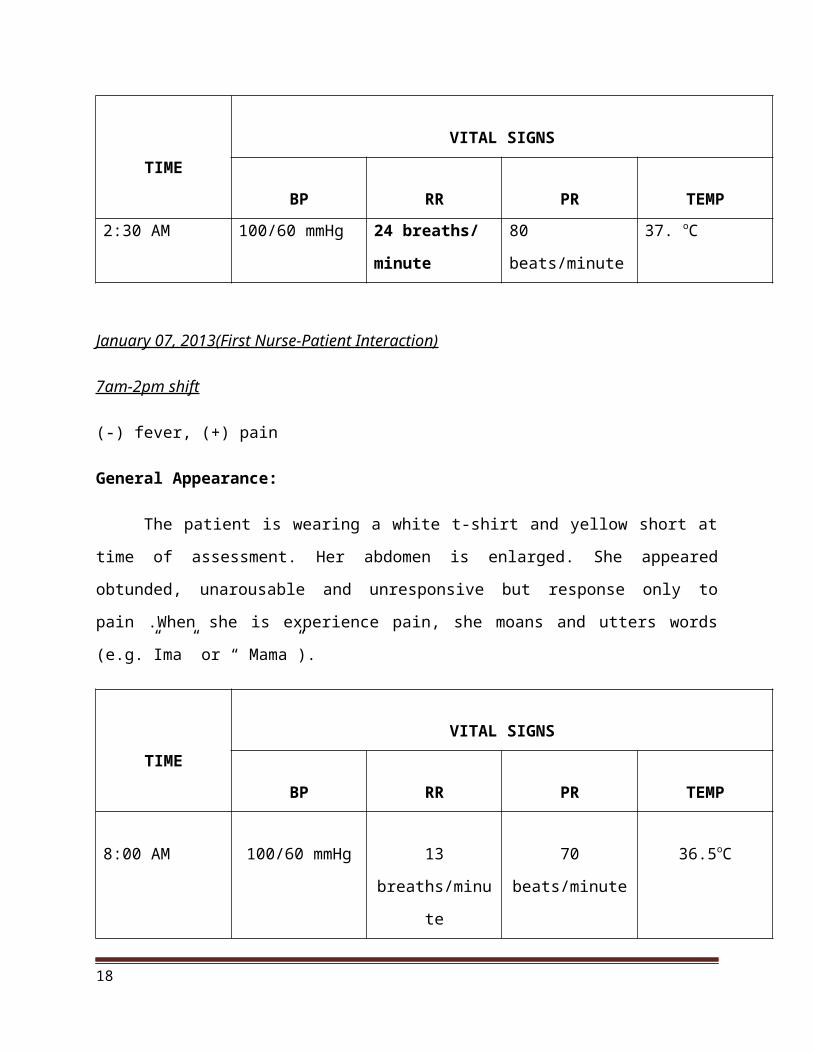
TIME
VITAL SIGNS
BP RR PR TEMP
2:30 AM 100/60 mmHg 24 breaths/
minute
80 beats/minute 37. oC
January 07, 2013(First Nurse-Patient Interaction)
7am-2pm shift
(-) fever, (+) pain
General Appearance:
The patient is wearing a white t-shirt and yellow short at time of assessment. Her
abdomen is enlarged. She appeared obtunded, unarousable and unresponsive but response only to
pain .When she is experience pain, she moans and utters words (e.g.”Ima” or “ Mama”).
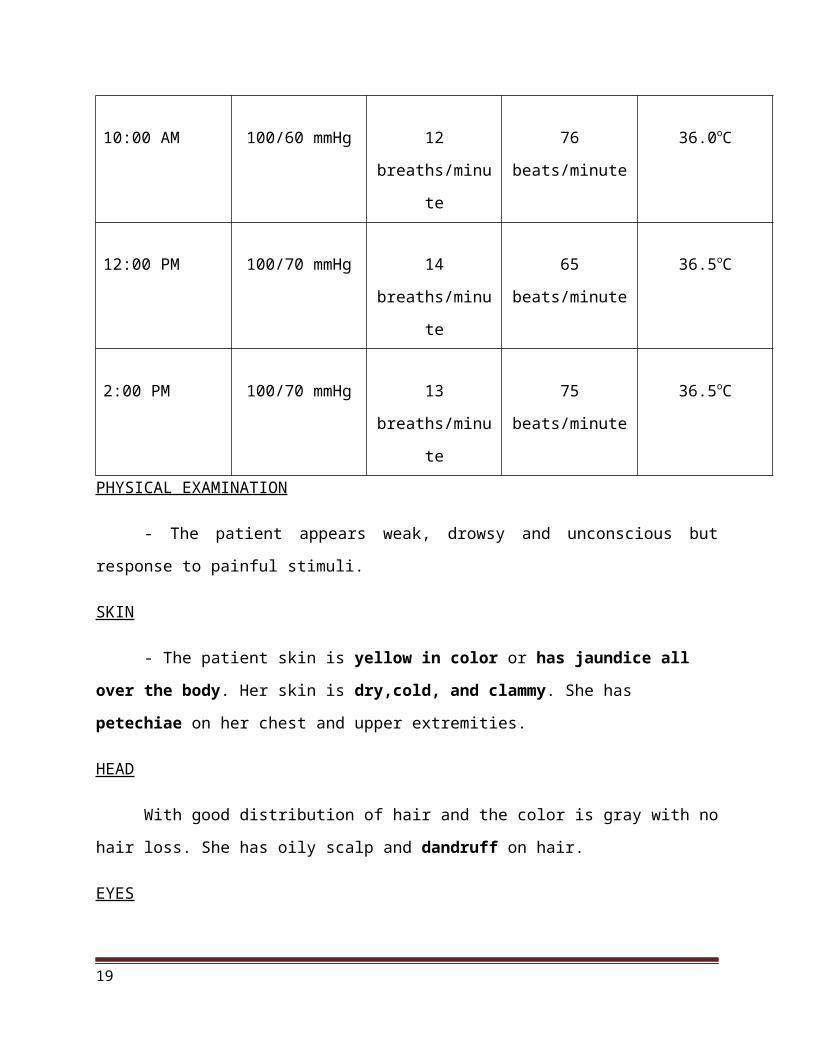
TIME
VITAL SIGNS
BP RR PR TEMP
8:00 AM 100/60 mmHg 13 breaths/minute 70 beats/minute 36.5oC
10:00 AM 100/60 mmHg 12 breaths/minute 76 beats/minute 36.0oC
12:00 PM 100/70 mmHg 14 breaths/minute 65 beats/minute 36.5oC
2:00 PM 100/70 mmHg 13 breaths/minute 75 beats/minute 36.5oC
PHYSICAL EXAMINATION
- The patient appears weak, drowsy and unconscious but response to painful stimuli.
12

SKIN
- The patient skin is yellow in color or has jaundice all over the body. Her skin is
dry,cold, and clammy. She has petechiae on her chest and upper extremities.
HEAD
With good distribution of hair and the color is gray with no hair loss. She has oily scalp
and dandruff on hair.
EYES
The patient has yellow palpebral conjunctiva and icterus (yellowish sclera). The patient
also has ptosis.
EARS
Her earlobes are turned inward. Presence of cerumen in minimal amount. No pain and
tenderness on her both ears.
NOSE
Her skin appearances are the same as face. Nares are dry with crusting. The nose is
symmetrical appearance.
MOUTH AND THROAT
Her lips are dry and dark. No presence of teeth.
ABDOMEN
Has striae and ascites with abdominal girth that measures at 39 inches since January 06,
2013 at 6 A.M and January 07, 2013 at 6 A. M and 9:30 A.M.
EXTREMITIES
The patient has positive pitting edema on upper and lower extremities.
NEUROLOGICAL
13

Patient is obtunded and has a Glascow Coma Scale with a score of 9 (Eye opening-2,
Verbal response-2, Motor response-5).
ANATOMY AND PHYSIOLOGY
(Figure 4: Parts of the Digestive System)
Liver
The liver is a reddish brown organ with four lobes of unequal size and shape. A human liver normally weighs 1.4 kg (about 3 lb) and after the skin, is the second largest organ of the body. It is also located below the diaphragm, mostly on the right side of the body. A connective tissue capsule covers the liver, which in turn is covered by peritoneum, the serous membrane that covers all the viscera.
14
(Figure 4.1: Liver)
Function of the Liver
The liver performs many other vital functions in addition to the secretion of bile and bile salts and the phagocytosis of bacteria and dead or foreign material by the kupffer cells.
1. Carbohydrate metabolism. The liver is especially important in maintaining a normal blood glucose level. When blood glucose is low, the liver can break down glycogen to glucose and release glucose into blood-stream. The liver can also convert certain amino acids and lactic acid to glucose and it can convert other sugars, such as fructose and galactose, into glucose. When blood glucose is high, as occurs just after eating a meal, the liver converts glucose to glycogen and triglycerides for storage.
2. Lipid metabolism. Hepatocytes store some triglycerides; break down fatty acids to generate ATP; synthesize lipoproteins, which transport fatty acids, triglycerides, and cholesterol to and from body cells; synthesize cholesterol; and use cholesterol to make bile salts.
3. Protein metabolism. Hepatocytes remove the amino group (-NH2) from amino acids so that the amino acids can be used for ATP production or converted to carbohydrates or fats. They also convert the resulting toxic ammonia (NH3) into the much less toxic urea, which is excreted in urine. Hepatocytes also synthesize most plasma proteins, such as globulins, albumin, prothrombin, and fibrinogen.
4. Processing of drugs and hormones. The liver can detoxify substances such as alcohol or secrete drugs such as penicillin, erythromycin, and sulfonamides into bile. It can also inactivate thyroid hormones and steroid hormones such as estrogens and aldosterone.
15
5. Excretion of bilirubin. Bilirubin, derived from the heme of aged red blood cells, is absorbed by the liver from the blood and secreted into bile. Most of the bilirubin in bile is metabolized in the small intestine by bacteria and eliminated in feces.
6. Storage of vitamins and minerals. In addition to storing glycogen, the liver stores certain vitamins (A, D, E, and K) and minerals (iron and copper), which are released from the liver when needed elsewhere in the body.
7. Activation of vitamin D. the skin, liver, and kidneys participate in synthesizing the activate form of vitamin D.
Gall bladder
The gall bladder is a pear-shaped organ joined to the ventral surface of the liver by the cystic duct. It’s covered with visceral peritoneum. The gall bladder stores and concentrates bile produced by the liver. It also releases bile into the common bile duct for delivery to the duodenum in response to the contraction and relaxation Oddi’s sphincter.
Functions of the gall bladder:
the gall bladder stores bile that enters it by way of the hepatic and cystic ducts. During this time, the gall bladder concentrates bile fivefold to tenfold. Then later, when digestion occurs in the stomach and intestines, the gall bladder contracts and ejects the concentrated bile in the duodenum. Jaundice, a yellow discoloration of the skin and mucosa, results when obstruction of bile flow into the duodenum occurs. Bile is thereby denied its normal exit from the body in feces. Instead, it is absorbed into the blood, and an excess of bile pigments with a yellow hue enters the blood and is deposited in tissues.
Large intestine
The large intestine averages about 6.5 cm (2.5 in.) in diameter and about 1.5 m (5 ft) in length. It extends form the ileum to the anus and is attached to the posterior abdominal wall by its mesentery. The large intestine (or bowel, colon) is the last part of the digestive system invertebrate animals. Its function is to absorb water from the remaining indigestible food matter, and then to pass useless waste material from the body.The large intestine has four principal regions: cecum, colon, rectum, and anal canal. It starts in the right iliac region of the pelvis, just at or below the right waist, where it is joined to the bottom end of the small intestine.From here it continues up the abdomen, then across the width of the abdominal cavity, and then it turns down, continuing to its endpoint at the anus.
The large intestine is the last part of the GI tract. Its overall functions are the completion of absorption, the production of certain vitamins, the formation of feces and the expulsion of feces from the body.
16
At the opening of the ileum into the large intestine is a valve called the ileocecalsphincter. It allows materials form the small intestine to pass into large intestine. Inferior to the ileocecal sphincter is the first segment of large intestine, called the cecum. Attached to the cecum is a twisted coiled tube called the appendix.
Small intestine
The small intestine (or small bowel) is the part of the gastrointestinal tract following the stomach and followed by the large intestine, and is where much of the digestion and absorption of food takes place. In invertebrates such as worms, the terms "gastrointestinal tract" and "large intestine" are often used to describe the entire intestine.The primary function of the small intestine is the absorption of nutrients and minerals found in food. The small intestine is where most chemical digestion takes place. Most of the digestive enzyme that act in the small intestine are secreted by the pancreas and enter the small intestine via the pancreatic duct. Enzymes enter the small intestine in response to the hormone cholecystokinin, which is produced in the small intestine in response to the presence of nutrients. The hormone secret in also causes bicarbonate to be released into the small intestine from the pancreas in order to neutralize the potentially harmful acid coming from the stomach.
Spleen
The spleen is the largest single mass of lymphatic tissue in the body. It lies between the stomach and diaphragm and is covered by a capsule of dense connective tissue. The spleen is the organ most often damaged in cases of abdominal trauma. A ruptured spleen causes severe internal hemorrhage and shock.
Function of the spleen:
the spleen has many and sundry functions, including defense, hematopoiesis, and red blood cell and platelet destruction; it also serves as a reservoir for blood.
1. Defense. As blood passes through the sinusoids of the spleen, reticuloendothelial cells (macrophages) lining these venous spaces remove microorganisms from the blood and destroy them by phagocytosis. Therefore the spleen plays a part in the body's defense against microorganisms.
2. Hematopoeisis.Nongranular leukocytes, that is, monocytes and lymphocytes, complete their development and become activated in the spleen, but after birth, red blood cells are also formed in the spleen forms red blood cells only in cases of extreme hemolytic anemia.
3. Red blood cell destruction and platelet destruction. Macrophages lining the spleen's sinusoids remove wornout red blood cells and imperfect platelets from the blood and destroy them by phagocytosis. They also break apart the hemoglobin molecules from the
17
destroyed red blood cells and salavage their iron and globin content by returning them to the bloostream for storage in bone marrow and liver.
4. Blood reservoir. At any given point in time the pulp of the spleen and its venous sinuses contain a considerable amount of blood. Although continually moving slowly through the spleen, blood can rapidly be added back into the circulatory system from this functional reservoir if needed. Its normal volume of about 350 ml is said to decrease by about 200 ml in less than 1 minute sympathetic stimulation that produces marked constriction of its smooth-muscle capsule.
Stomach
The stomach is a muscular, hollow, dilated part of the digestion system which functions as an important organ of the digestive tract in some animals, including vertebrates,echinoderms,insects (mid-gut), and mollusc's. It is involved in the second phase of digestion, following mastication(chewing).
The stomach is located between the esophagus and the small intestine. It secretes protein-digesting enzymes called protease and strong acids to aid in food digestion, (sent to it via esophageal peristalsis) through smooth muscular contortions (called segmentation) before sending partially digested food (chyme) to the small intestines.
Function of the stomach:
Serves as a food reservoir, its main function; food is stored in the stomach until it can be partially digested and moved further along the gastro intestinal tract.
Secretes gastric juice, which contains acid and enzymes that aid in the digestion of food.
Churns the food (by contractions of its muscular coat), breaking it into small particles and mixing them well with the gastric juice; in time, gastric contents are moved along into the duodenum.
Secretes intrinsic factor.
Performs a limited amount of absorption; absorbed substances include certain drugs, some water, alcohol, and some short-chain fatty acids found in butter or milk fat.
Produces the hormones gastrin, which helps regulate digestive functions, and ghrelin (GHRL), which increases appetite.
Helps protect the body by destroying pathogenic bacteria swallowed with food or with mucus from the respiratory tract.
Kidney
The kidneys are bean-shaped, highly vascular organs. The kidneys are protected in front by the contents of the abdomen and behind by the muscles attached to the vertebral column. A layer of fat surrounding each kidney offers further protection. Each kidney is supplied with blood by a renal artery, which subdivides into several branches when it enters the kidney. The kidneys are
18
highly vascular (relating to or containing blood vessels), receiving about 20% of the blood pumped by the heart each minute.
Surrounding each kidney is the smooth, transparent renal capsule, a connective tissue sheath that helps maintain the shape of the kidney and serves as a barrier against trauma. Adipose (fatty) tissue surrounds the renal capsule and cushions the kidney. Along with a thin layer of dense irregular connective tissue, the adipose tissue anchors the kidney to the posterior abdominal wall.
PATIENT AND HIS ILLNESS
DEFINITION OF THE DISEASE
Cirrhosis is extensive, Irreversible scarring of the liver, usually caused by a chronic reaction to hepatic inflammation and necrosis. The disease typically develops slowly and has progressive, prolonged, destructive course resulting in end stage liver disease. The most common causes of cirrhosis in the United States are alcoholic liver disease and Hepatitis C. Worldwide, Hepatitis B and Hepatitis D are the leading causes. Without liver transplantation, cirrhosis is usually fatal (Kelso, 2008).
Cirrhosis of the liver can be divided into several types, depending on the cause of the disease. Laennec’s or alcoholic cirrhosis, cause by chronic alcoholism, Post necrotic cirrhosis caused by viral hepatitis and certain drugs or chemicals, Biliary cirrhosis caused by chronic biliary obstruction, usually from gall bladder disease and Cardiac cirrhosis caused by heart failure as rare complication.
SYSNTHESIS OF THE DISEASE
RISK FACTORS(PATIENT BASED)
Incidence is higher in males. Excessive Alcohol consumption, has a direct toxic effect on the hepatocytes causes liver
inflammation. Viral Hepatitis, due to inflammation caused by infection over time leads to progressive
scarring of the liver.
SIGNS AND SYMPTOMS (PATIENT-BASED)
Abdominal pain, which may feel like squeezing pain, tightness or burning due to liver scars.
Jaundice, due to destructive bilirubin excretion
19
Ascites, edema, due to fluid retention. Petechiae, due to clotting defect. Fever, as compensatory mechanism to inflammation and decreased WBc Obtunded, due to decreased tissue perfusion in other organs and brain.
20