case study dm hpn furuncle
TRANSCRIPT
A. Introduction
Diabetes is a metabolic disorder characterized by a relative or absolute
lack of the hormone insulin or insulin resistance, or both, which is impaired
use of carbohydrates and altered metabolism of fats and protein. The word
diabetes, from the Greek meaning “a siphon”, suggests urine formation, the
word mellitus, from the Greek meaning “honey”, suggests sweetness. Type 2
diabetes was formerly known by a variety of partially misleading names,
including “adult-onset diabetes,” obesity-related diabetes”, or non-insulin-
dependent diabetes” (NIDDM). It is characterized by “insulin resistance” as
body cells do not respond appropriately when insulin is present. This is more
complex problem than type 1, but it is sometimes easier to treat, since
insulin is still in many, especially in the initial years. Type 2 may go unnoticed
for years in a patient before diagnosis, since the symptoms are typically
milder and can be sporadic. The 3 cardinal signs of Type 2 DM are polyphagia
(excessive hunger), polydipsia (excessive thirst), and polyuria (excessive
urination). Other signs and symptoms of this disease are weight loss or gain,
blurred vision, headaches lethargy, impotence, vaginal discharge, increased
vaginal infection, increased wound healing time, orthostatic hypertension,
decreased pedal pulses, paresthesics, and decreased sensations
(extremities). If these signs and symptoms were not given proper or enough
attention, it may lead to the following complications” diabetic neurophatics
(low of sensation in extremities), Charcot’s syndrome, Retinopathy, kidney
failure, Atherosclerosis of the heart and large vessels and amputation.
In 2004, according to the World Health Organization, more than 150
million people worldwide suffer from diabetes. Its incidence is increasing
rapidly, and it is estimated that by the year 2025 this number will double.
Diabetes mellitus occurs throughout the world, but it is common (especially
Type 2) in the more developed countries. In 2002 there were about 18.2
million diabetics in the United States alone. Diabetes is in the top 10, and
perhaps the top 5, of the most significant disease in the developed world, and
is gaining insignificance. For at least 20 years, diabetes rates in North
America have been increasing substantially. The Centers for Disease Control
has termed the change an epidemic. The National Diabetes Information
Clearing house estimates that diabetes costs $132 billion in the United States
alone every year.
Diabetes has become a multibillion dollar industry in Europe
specifically; Type 2 Diabetes contributes to an annual economic cost of 129
billion among developed countries. Due to this, the traditional urine testing
as the only method for gauging blood glucose levels of patients, a variety of
devices designed to monitor glucose while easing the burden of frequent
blood tests. There is a growing demand for portable glucose meters that are
compact user friendly in monitoring blood glucose levels efficiently accurate.
Through technological improvements, Point of Case Testing (POC) is the
largest profit making segment in the market. POC testing provides simple and
quick results. With this, POC testing is expected to play a key role in the fight
against Diabetes and will dominate the market over clinical diagnostics
Glycosylated hemoglobin (HbAlc) is another test that is expected to rise
slightly and is being processed and prices for cheaper than hospital-based
laboratories since it is already adopted by health Care Teams even outpatient
clinics and small hospital based laboratories. Manufacturers will identify
customers unmet needs and develop competent technologies that focus on
dedicated systems to improve efficiency and profitability. New technologies
and challenges may occur; it will remain for more patient friendly screening
and treatments. The future care for Diabetes will non-invasive and make
glucose regulation for more accurate and easier to manage.
Current Trends CDC Criteria for Anemia in Children and Childbearing-Aged
Women
Hemoglobin (Hb) and hematocrit (Hct) measurements are the
laboratory tests used most commonly in clinical and public health settings for
screening for anemia. Because most anemia in children and women of
childbearing age is related to iron deficiency (1), the main purpose of anemia
screening is to detect those persons at increased risk for iron deficiency.
Proper anemia screening requires not only sound laboratory methods and
procedures but also appropriate Hb and Hct cutoff values to define anemia.
The "normal" ranges of Hb and Hct change throughout childhood and during
pregnancy, and are higher for men than women (1,2). Thus, criteria for
anemia should be specific for age, sex, and stage of pregnancy. Current
major reference criteria for anemia, however, are not based on
representative samples and fail to take into account the normal hematologic
changes occurring during pregnancy. To address these limitations, CDC has
formulated new reference criteria for use in clinical practice for public health
and nutrition programs and the CDC Pediatric and Pregnancy Nutrition
Surveillance Systems. The new criteria may also be useful for defining
anemia in clinical research and nutrition surveys.
The anemia reference values for children, nonpregnant women, and
men are derived from the most current nationally representative sample--the
Second National Health and Nutrition Examination Survey, 1976-1980
(NHANES II). Because representative data are not yet available for pregnant
women, anemia reference values are based on the most current clinical
studies available. Adjustment values of Hb and Hct cutoffs are provided for
persons who reside at higher altitudes and for those who smoke cigarettes.
Anemia Cutoffs for Children, Nonpregnant Women, and Men
Because hematologic values normally change as children grow older, it is
necessary to use age-specific criteria for diagnosing anemia in children (1).
The best hematologic reference data for the United States are available from
the NHANES II. The Hb and Hct cutoffs recommended represent the age-
specific fifth percentile values for "healthy" persons from NHANES II (Table 1)
(3, 4). The healthy sample was defined by excluding persons who were likely
to have iron deficiency based on multiple iron biochemical measures. The
anemia cutoff values based on these NHANES II studies for younger children
are in close agreement with the cutoff values recommended by the American
Academy of Pediatrics, which were based on a sample of healthy white
middle-class children (5). Even though no data are available from NHANES II
to determine anemia cutoffs for infants less than 1 year of age, cutoff values
for children 1-2 years can be extrapolated back to 6 months of age. In
general, anemia screening to detect iron deficiency is not indicated for
infants less than 6 months of age because younger infants usually have
adequate iron nutritional status (6). Anemia Cutoffs during Pregnancy
During a normal pregnancy, a woman's hematologic values change
substantially (2). For women with adequate iron nutrition, Hb and Hct values
start to decline during the early part of first trimester, reach their nadir near
the end of second trimester, then gradually rise during the third trimester
(2,7-10). Because of the change of Hb and Hct during pregnancy, anemia
must be characterized according to the specific stage of pregnancy. The
normal range of Hb and Hct during pregnancy is based on data aggregated
from four European studies of healthy iron-supplemented pregnant women
(7-10). These studies provide similar findings at each specific month of
pregnancy. The month-specific fifth percentile values for Hb of the pooled
data have been adopted for use in the CDC Pregnancy Nutrition Surveillance
System (Table 2). In addition, trimester-specific cutoffs also have been
developed for use in the clinical setting (Table 2). These trimester-specific
cutoffs are based on the mid-trimester values; cutoffs for the first trimester,
the time at which most women are initially seen for prenatal care, are based
on a late-trimester value. Adjustment of Hb and Hct Cutoffs for Altitude and
Smoking
Persons residing at higher altitudes ( greater than 1000 meters (3300
feet)) have higher Hb and Hct levels than those residing at sea level. This
variation is due to the lower oxygen partial pressure at higher altitudes, a
reduction in oxygen saturation of blood (11), and a compensatory increase in
red cell production to ensure adequate oxygen supply to the tissues. Thus,
higher altitude causes a generalized upward shift of the Hb and Hct
distributions. This shift may be associated with the underdiagnosis of anemia
for residents of higher altitudes when sea-level cutoffs are applied (CDC,
unpublished data). Therefore, the proper diagnosis of anemia for those
residing at higher altitudes requires an upward adjustment of Hb and Hct
cutoffs. The values for altitude-specific adjustment of Hb and Hct are derived
from data collected by the CDC Pediatric Nutrition Surveillance System on
children residing at various altitudes in the mountain states (Table 3).
Altitude affects Hb and Hct levels throughout pregnancy in a similar way (J.N.
Chatfield, unpublished data).
The influence of cigarette smoking is similar to that of altitude, in that
smoking increases Hb and Hct levels substantially. The higher Hb and Hct of
smokers is a consequence of an increased carboxyhemoglobin from inhaling
carbon monoxide during smoking. Because carboxyhemoglobin has no
oxygen carrying capacity, its presence causes a generalized upward shift of
the Hb and Hct distribution curves (CDC, unpublished data). Therefore, a
smoking-specific adjustment to the anemia cutoff is necessary for the proper
diagnosis of anemia in smokers. The smoking-specific Hb and Hct
adjustments are derived from the NHANES II data (Table 4). The altitude and
smoking adjustments are additive. For example, a woman living at 6000 feet
and smoking two or more packs of cigarettes per day would have her cutoff
for anemia adjusted upward by a total of 1.4 grams of Hb or 4% Hct.
Reported by: Div of Nutrition, Center for Chronic Disease Prevention and
Health Promotion; Div of Environmental Health Laboratory Sciences, Center
for Environmental Health and Injury Control; Div of Health Examination
Statistics, National Center for Health Statistics; Div of Host Factors, Center for
Infectious Diseases, CDC.
Hypertension is a common clinical problem faced by both primary care
clinicians and specialists. While the exact prevalence of resistant
hypertension is unknown, clinical trials suggest that it is not rare, involving
perhaps 20% to 30% of study participants. As older age and obesity are 2 of
the strongest risk factors for uncontrolled hypertension, the incidence of
resistant hypertension will likely increase as the population becomes more
elderly and heavier. The prognosis of resistant hypertension is unknown, but
cardiovascular risk is undoubtedly increased as patients often have a history
of long-standing, severe hypertension complicated by multiple other
cardiovascular risk factors such as obesity, sleep apnea, diabetes, and
chronic kidney disease. The diagnosis of resistant hypertension requires use
of good blood pressure technique to confirm persistently elevated blood
pressure levels. Pseudoresistance, including lack of blood pressure control
secondary to poor medication adherence or white coat hypertension, must be
excluded. Resistant hypertension is almost always multifactorial in etiology.
Successful treatment requires identification and reversal of lifestyle factors
contributing to treatment resistance; diagnosis and appropriate treatment of
secondary causes of hypertension; and use of effective multidrug regimens.
As a subgroup, patients with resistant hypertension have not been widely
studied. Observational assessments have allowed for identification of
demographic and lifestyle characteristics associated with resistant
hypertension, and the role of secondary causes of hypertension in promoting
treatment resistance is well documented; however, identification of broader
mechanisms of treatment resistance is lacking. In particular, attempts to
elucidate potential genetic causes of resistant hypertension have been
limited. Recommendations for the pharmacological treatment of resistant
hypertension remain largely empiric due to the lack of systematic
assessments of 3 or 4 drug combinations. Studies of resistant hypertension
are limited by the high cardiovascular risk of patients within this subgroup,
which generally precludes safe withdrawal of medications; the presence of
multiple disease processes (eg, sleep apnea, diabetes, chronic kidney
disease, atherosclerotic disease) and their associated medical therapies,
which confound interpretation of study results; and the difficulty in enrolling
large numbers of study participants. Expanding our understanding of the
causes of resistant hypertension and thereby potentially allowing for more
effective prevention and/or treatment will be essential to improve the long-
term clinical management of this disorder.
Furuncles are very common. They are caused by staphylococcus
bacteria, which are normally found on the skin surface. Damage to the hair
follicle allows these bacteria to enter deeper into the tissues of the follicle
and the subcutaneous tissue. Furuncles may occur in the hair follicles
anywhere on the body, but they are most common on the face, neck, armpit,
buttocks, and thighs.
Furuncles are generally caused by Staphylococcus aureus, but they may be
caused by other bacteria or fungi. They may begin as a tender, red,
subcutaneous nodule but ultimately become fluctuant (feel like a water-filled
balloon). A furuncle may drain spontaneously, producing pus. More often the
patient or someone else opens the furuncle.
Furuncles can be single or multiple. Some people have recurrent bouts with
abscesses and little success at preventing them. Furuncles can be very
painful if they occur in areas like the ear canal or nose. A health care provider
should treat furuncles of the nose. Furuncles that develop close together may
expand and join, causing a condition called carbunculosis.
Electrolytes are salts that conduct electricity and are found in the body
fluid, tissue, and blood. Examples are chloride, calcium, magnesium, sodium,
and potassium. Sodium (Na+) is concentrated in the extracellular fluid (ECF)
and potassium (K+) is concentrated in the intracellular fluid (ICF). Proper
balance is essential for muscle coordination, heart function, fluid absorption
and excretion, nerve function, and concentration.
The kidneys regulate fluid absorption and excretion and maintain a
narrow range of electrolyte fluctuation. Normally, sodium and potassium are
filtered and excreted in the urine and feces according to the body's needs.
Too much or too little sodium or potassium, caused by poor diet, dehydration,
medication, and disease, results in an imbalance. Too much sodium is called
hypernatremia; too little is called hyponatremia. Too much potassium is
called hyperkalemia; too little is called hypokalemia.
B. Reasons for choosing such case for Presentation
One of the formidable parts in doing a case study is choosing what
case is to present. We had this unanimous decision of choosing our patients
case, first and foremost because with our initial contact we already
established harmonious relationship with the patient and his significant
others. We had established the “trust” we yearn from them and that makes it
easy for us to ask certain questions we need for our case and interact with
them properly. Another thing is because we find them kind and humorous
that is why our previous interaction with them is smooth and conventional.
Most importantly, our patient’s case is very critical because he has five
diagnoses. With that thought alone, we want to further enhance our
knowledge about the disease such as to ensure appropriate evaluation of the
etiology, reassess and address the course of the illness takes in its
progression. Also, to have an experience in handling and providing
humanitarian health services to a patient who has it and provide any
intervention or treatment indicated based on the specific etiology and the
course it follows in that specific patient. With that scenario, it is not only the
knowledge that was enhanced but also our skills as health care practitioners.
II. NURSING ASSESSMENT
A. Personal History
1. Demographic Data
Mr. Mickey (not his real name) is a 52 years old married male, Filipino
who was born on February 16, 1954 in Angeles City. He is the eldest among
the eight siblings of Disney family (not their real family name) and has 5
unmarried sisters. He, together with Mrs. Minnie (not her wife’s real name)
and their eight children, currently resides near main road in Robinson’s mall,
Angeles City, Pampanga. He is religiously affiliated as a Roman Catholic. He is
presently working as a Barangay Tanod. He was admitted at Ospital Ning
Angeles (ONA) on April 27, 2008 because of hypertension and Diabetes
Mellitus type 2.
2. Socio-economic and cultural factors
Mr. Mickey was able to finish a full course of elementary until second
year college but had not gone to school to continue his studies due to
financial constraints.
Mr. Mickey was a construction worker before and now he is presently
working as a barangay tanod. He doesn’t earn much, he just earn 2000 per
month that’s why he cannot able to support his family. They spend about 300
pesos a day through the financial support of his children.
Mr. Mickey, does not like having exercises, he has a sedentary lifestyle.
He gets easily stressed because of their financial status plus his job as a
barangay tanod. He usually comes home at 2 am in the morning. He does not
engage in any vices such as drinking alcoholic beverages nor smoking
cigarettes. As for the foods he eats before he acquired hypertension and
diabetes mellitus type 2, Mr. Mickey preferred fatty and salty foods and also
those glucose rich or sweets.
Mr. Mickey and his family also believe in consulting the “herbolaryos
or manghihilot” for any problems or illness that would occur. They also use
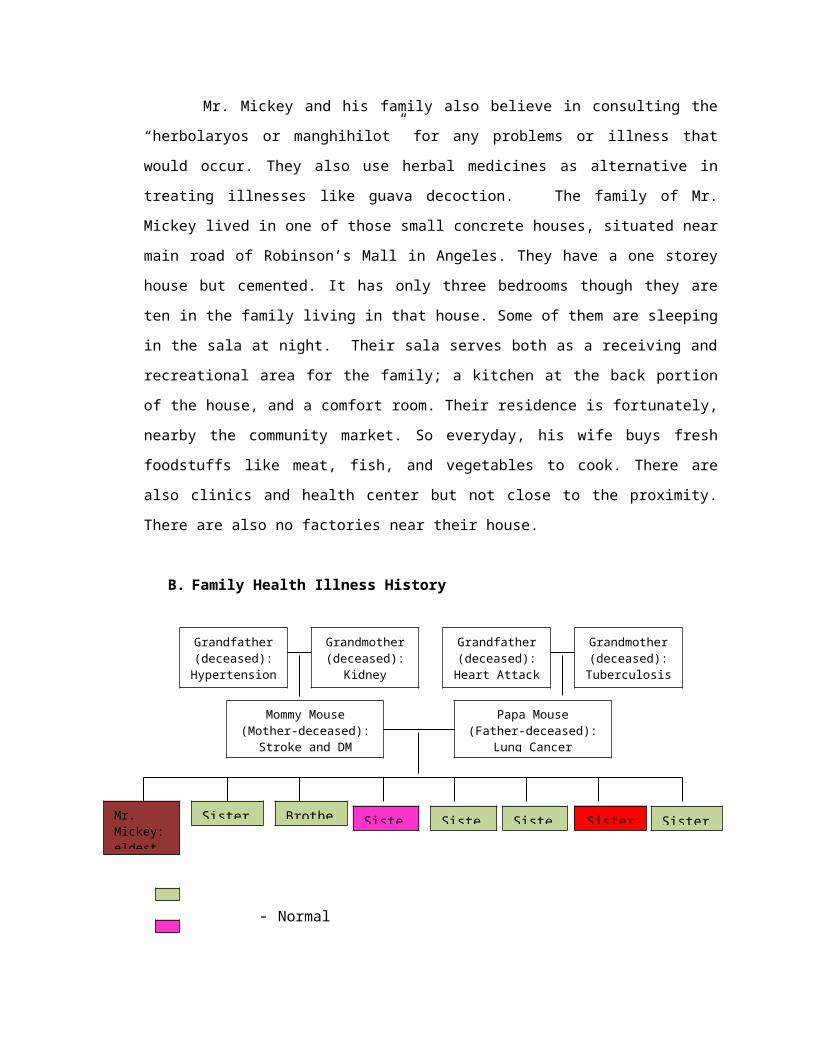
Mommy Mouse(Mother-deceased):
Stroke and DM
Mr. Mickey: eldest
herbal medicines as alternative in treating illnesses like guava decoction.
The family of Mr. Mickey lived in one of those small concrete houses, situated
near main road of Robinson’s Mall in Angeles. They have a one storey house
but cemented. It has only three bedrooms though they are ten in the family
living in that house. Some of them are sleeping in the sala at night. Their
sala serves both as a receiving and recreational area for the family; a kitchen
at the back portion of the house, and a comfort room. Their residence is
fortunately, nearby the community market. So everyday, his wife buys fresh
foodstuffs like meat, fish, and vegetables to cook. There are also clinics and
health center but not close to the proximity. There are also no factories near
their house.
B. Family Health Illness History
- Normal
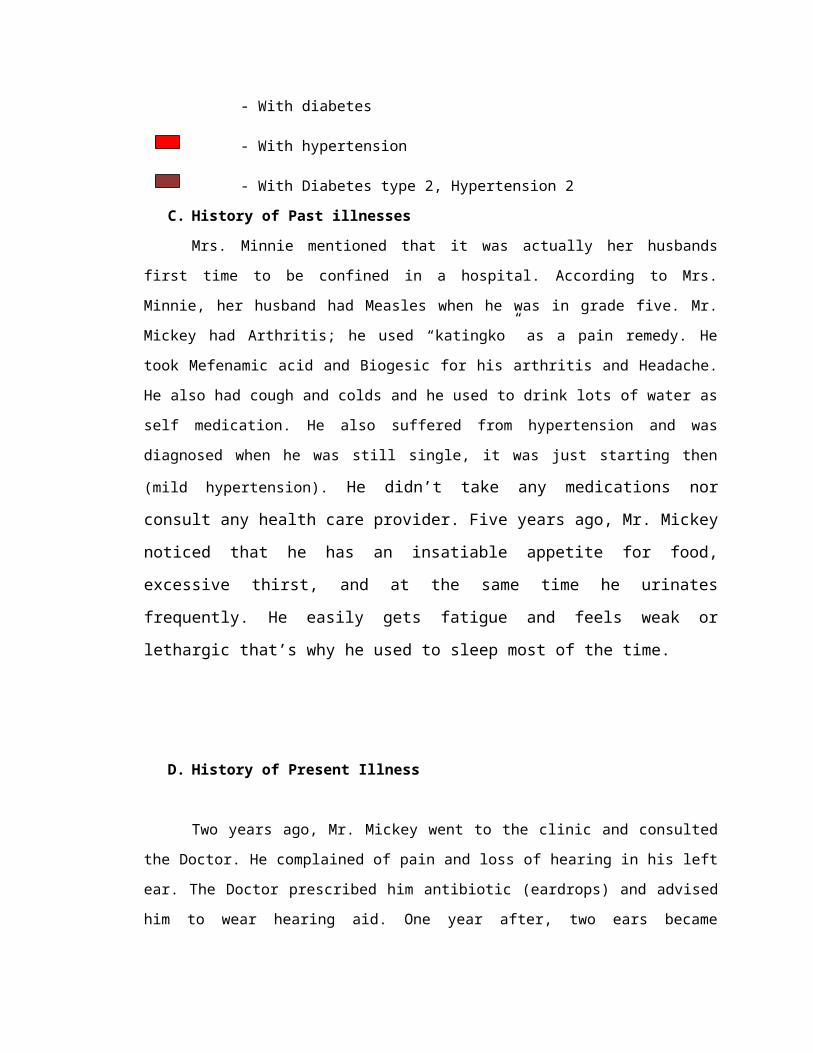
- With diabetes - With hypertension - With Diabetes type 2, Hypertension 2
C. History of Past illnesses
Mrs. Minnie mentioned that it was actually her husbands first time to
be confined in a hospital. According to Mrs. Minnie, her husband had Measles
when he was in grade five. Mr. Mickey had Arthritis; he used “katingko” as a
pain remedy. He took Mefenamic acid and Biogesic for his arthritis and
Headache. He also had cough and colds and he used to drink lots of water as
Grandfather(deceased):
Hypertension
Grandmother(deceased):
Kidney Failure
Grandfather(deceased): Heart Attack
Grandmother(deceased): Tuberculosis
Papa Mouse(Father-deceased):
Lung Cancer
Sister 1 Brother Sister Sister Sister Sister 5 Sister

self medication. He also suffered from hypertension and was diagnosed when
he was still single, it was just starting then (mild hypertension). He didn’t take
any medications nor consult any health care provider. Five years ago, Mr. Mickey noticed
that he has an insatiable appetite for food, excessive thirst, and at the same time he
urinates frequently. He easily gets fatigue and feels weak or lethargic that’s why he used
to sleep most of the time.
D. History of Present Illness
Two years ago, Mr. Mickey went to the clinic and consulted the Doctor.
He complained of pain and loss of hearing in his left ear. The Doctor
prescribed him antibiotic (eardrops) and advised him to wear hearing aid.
One year after, two ears became affected. In January 2008 when he went to
health center, his blood pressure was increased, it was 140/90. Last April 23,
morning, when he sought medical help in the OPD of ONA. During that time,
he has no appetite in eating and his furuncle was still small. The Doctor
prescribed him to take Amoxicillin, Appebon with Iron and Cetrizine
Dihydrochloride. On the night of April 27, 2008, he was admitted to the
hospital for the first time with admitting diagnosis of intractable vomiting,
Electrolyte imbalance, Anemia, furuncle, Diabetes Mellitus type 2,
Hypertension 2.
The following doctor’s orders were given: (lifted from the Mr. Mickey’s
chart):
Initial V/S were, T-36.0 PR-84 RR-21 BP-170/100
Pls admit to medical ward
Secure consent from admin and management
NPO temporarily except meds
IVF PNSS 1L x 30 gtts/min
Dxtic: CBC-done RBC-done
U/A-done
Na, K-done
Creatinine-Requested
BUN
FBS
Lipid profile
CXR-PA
12 lead ECG
Tx: Ceftriaxone 1g/IV q 12
Metformin 500mg 1 tab BID
Plasil tab TID PRN for Vomiting
FeSO4 tab BID
Monitor VS q4
Refer accordingly
Amlodipine (Lopicard) 5g I tab OD
E. Physical Examination
Physical Assessment/Doctor’s Notes: April 27, 2008 (admission-lifted
from the chart)
Diagnosis: Intractable Vomiting, Electrolyte Imbalance,
Anemia, Furuncle, DM type 2, Hypertension 2
Vomiting, three times
Body weakness
BP= 170/100 mmHg
Pulse Rate= 84 beats per minute
Respiratory Rate= 21 cycles per minute
Temperature= 36.6 ˚C
*** for Lipid profile, triglycerides, BUA, CXR posterior-anterior view, ECG
Physical Assessment: April 28, 2008
Vital Signs:
T- 37°C RR- 17 cpm
PR- 74 bpm BP- 150/90 mmHg
1. General Appearance
a. Body built is ectomorphic
b. Presence of halitosis for the breath odor
c. Attitude is cooperative
d. Affect or mood is appropriate for the situation
2. Skin
a. There is good skin turgor
b. Skin is dry, pale on the palms and soles of the feet, with scars on lower
extremities
c. Absence of facial and periorbital edema
d. (+) 3-cm-diameter furuncle on left upper arm, draining purulent
secretion
3. Head
a. Skull is round in shape and has normal contour, with no palpated
depressions
b. Hair is thick, with fine strands; scalp is excessively oily with no masses
palpated
c. Facial features are symmetrical with no noted abnormalities
4. Eyes
a. Pupils are equally round and reactive to light and accommodation
b. Palpebral conjunctiva are pale
c. Eyebrows are symmetrically aligned, hair is thick, evenly distributed;
skin is intact
d. Eyelashes are equally distributed and curled slightly outward
e. No discharges present
f. Absence of periorbital edema
g. Cornea is transparent, smooth and shiny
h. Details of the iris are visible, color brown
i. Sclera appears white
5. Ears
a. Ears are symmetrical and aligned with the outer canthus of the eye,
with no lesions noted.
b. Color is same as facial skin
c. Ears have no foul smelling discharges, with impacted cerumen on the
middle ear
d. Pinna recoils after being folded
6. Nose
a. Nose has no discharge, no lesions, not occluded & with patent airway
b. Color is same as facial skin
7. Throat and Mouth
a. Throat & mouth have no sores and swellings/inflammation
b. Lips are dry and pinkish
c. There is slight difficulty in swallowing
d. Grade of (+) 1 for tonsils-normal; pale, smooth, with no inflammation
e. Tongue is positioned at the center, furry, white, moist, rough, with
fissures
f. Gums are pale and with firm texture
8. Neck
a. Color is slightly darker than facial skin
b. Absence of enlarged thyroid area
c. Absence of jugular vein distention
d. Movement is coordinated and smooth
9. Chest
a. Breasts are not enlarged, with no lesions
b. No masses assessed upon palpation
10. Cardiovascular
a. Absence of chest pain and murmurs
b. Normal heart rhythm, PR = 74 bpm
11. Respiratory
a. Chest is symmetric; anteroposterior to transverse diameter ratio is 1:2
b. Chest expansions are symmetrical
c. Absence of rales on both lung fields
12. Gastrointestinal
a. Presence of bowel sounds 5/min, presence of flatus
b. Absence of bowel movement
c. Absence of organomegaly
13. Extremities
a. Upper- symmetrical, absence of edema; capillary refill >2 seconds; (+)
3-cm-diameter furuncle on left upper arm, draining purulent secretion
b. Lower- symmetrical, absence of edema
14. Urogenital
a. Urine output: approximately 30cc per hour, amber yellow in color,
cloudy
b. Genitals- no foul smelling discharges
Neurological Assessment
Cranial Nerve Normal Findings Actual Findings
1. Olfactory
Type: Sensory
Client must be able to
identify the scent of
Client was able to
identify the scent of
Fxn: Sense of smell perfume when allowed to
smell it.
perfume when allowed
to smell it.
2. Optic
Type: Sensory
Fxn: Sense of vision and
visual fields
Client must see the pen or
penlight clearly from a
certain distance; must be
able to read newspaper
print.
Client was able to see
the pen or penlight
from a certain distance,
but was not able to
read newspaper print.
Client needs to wear
eyeglasses for better
vision.
3. Oculomotor
Type: Motor
Fxn: Pupil constriction and
raising of eyelid
Eyes must follow the
direction of the movement
of the penlight;
In lightly dimmed
environment, the pupils of
the eyes will dilate but
upon the introduction of
light, pupils will constrict.
The client was able to
follow the movement of
the penlight through
her eyes.
4. Trochlear
Type: Motor
Fxn: Downward inward
eye movement
The eye must follow the
movement of a pen in
different directions with
coordination.
The client was able to
follow the pen with her
eyes without moving
her head.
5. Trigeminal
Type: Sensory and Motor
Fxn: Jaw movements,
chewing and mastication
The client must elicit
blinking reflex upon
touching the cornea with
the use of cotton.
(Corneal Sensitivity Test)
The client elicited
blinking reflex upon
touching the cornea.
6. Abducens
Type: Motor
Fxn: Lateral movements
of the eyes
Client must follow the
index finger of the
examiner and its
movements.
The client was able to
follow the index finger
of the examiner and its
movements.
7. Facial
Type: Motor and Sensory
Client must be able to
raise eyebrows, show
The client was able to
raise eyebrows, show
Fxn: Movement of
muscles of the face and
sense of taste on the
anterior two-thirds of the
tongue
teeth, frown, smile, pout
and puff out cheeks. Also,
the client must also be
able to distinguish sweet,
sour, and salty foods.
teeth frown, smile, pout
and puff out cheeks.
Also, the client was not
able to distinguish
sweet, sour, and salty
foods. Test not
performed due to
anorexia and vomiting.
8. Acoustic
(Vestibulocochlear)
Type: Sensory
Fxn: Sense of hearing
Client must be able to
hear a snap of the finger.
The client was not able
to hear the snap of the
finger.
9. Glossopharyngeal
Type: Motor and Sensory
Fxn: Pharyngeal
movements and
swallowing
Sense of taste on the
posterior one-third of the
tongue
The patient must be able
to swallow foods that were
chewed and taste bitter
foods. Also, the gag reflex
should be stimulated.
The client was not able
to taste the food. Test
not performed due to
anorexia and vomiting.
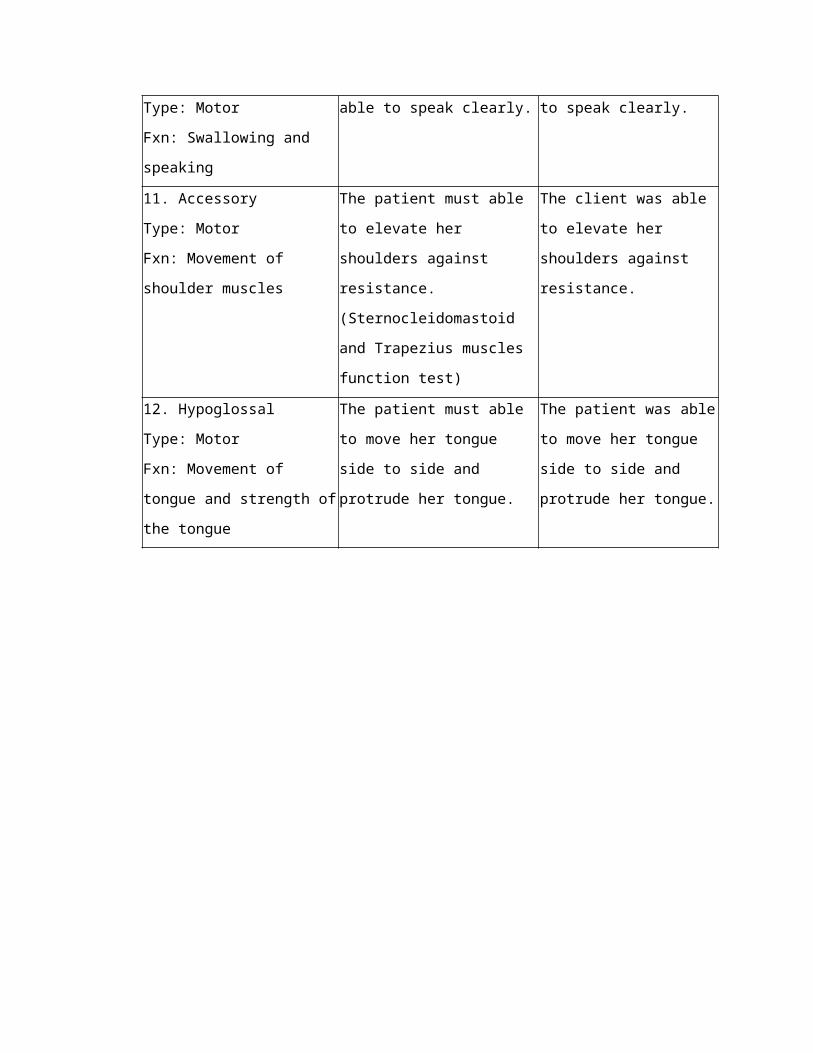
10. Vagus
Type: Motor
Fxn: Swallowing and
speaking
The patient must be able
to speak clearly.
The client was able to
speak clearly.
11. Accessory
Type: Motor
Fxn: Movement of
shoulder muscles
The patient must able to
elevate her shoulders
against resistance.
(Sternocleidomastoid and
Trapezius muscles
function test)
The client was able to
elevate her shoulders
against resistance.
12. Hypoglossal
Type: Motor
Fxn: Movement of tongue
The patient must able to
move her tongue side to
side and protrude her
The patient was able to
move her tongue side
to side and protrude
and strength of the
tongue
tongue. her tongue.
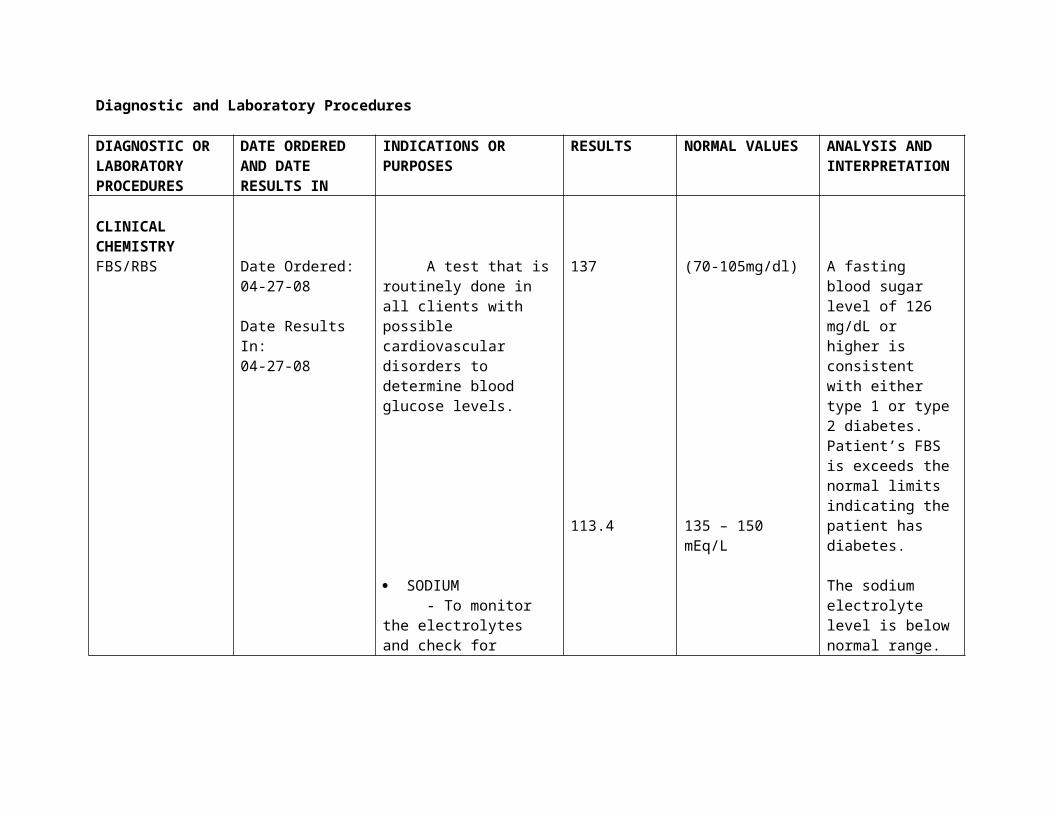
Diagnostic and Laboratory Procedures
DIAGNOSTIC OR LABORATORY PROCEDURES
DATE ORDERED AND DATE RESULTS IN
INDICATIONS OR PURPOSES
RESULTS NORMAL VALUES
ANALYSIS AND INTERPRETATION
CLINICAL CHEMISTRYFBS/RBS Date Ordered:
04-27-08
Date Results In:04-27-08
A test that is routinely done in all clients with possible cardiovascular disorders to determine blood glucose levels.
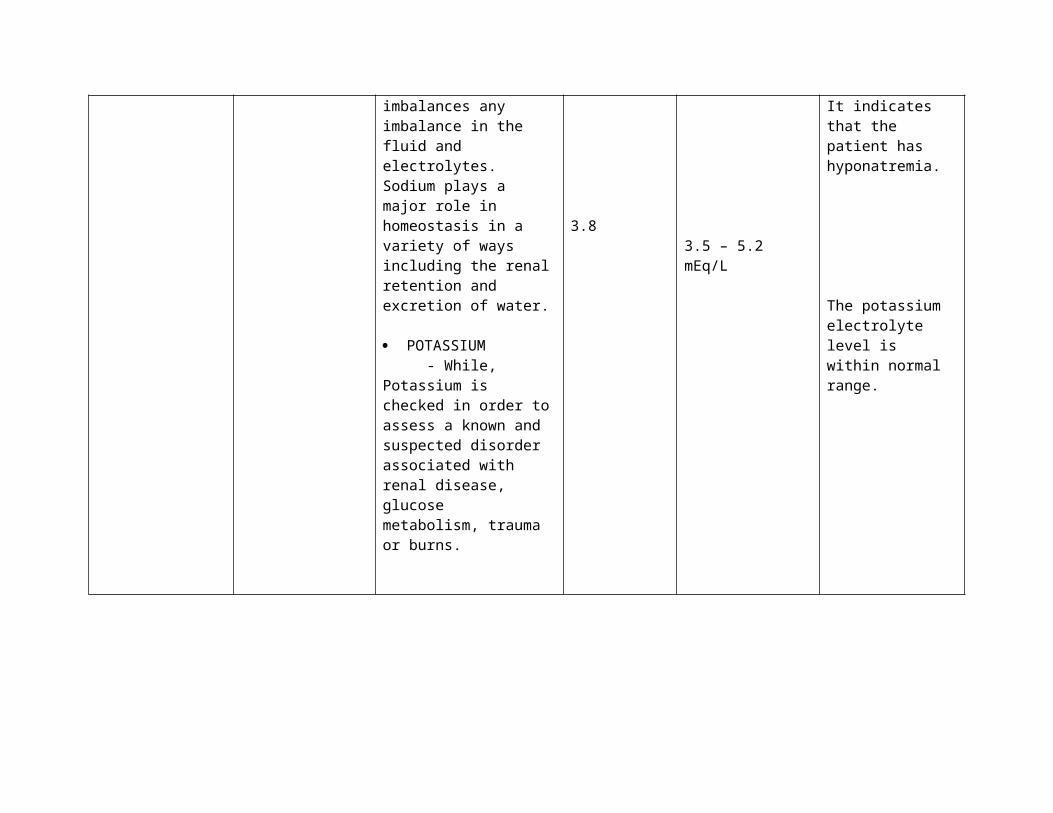
SODIUM - To monitor the electrolytes and check for imbalances any imbalance in the fluid and electrolytes. Sodium plays a major role in homeostasis in a variety of ways including the renal
137
113.4
(70-105mg/dl)
135 – 150 mEq/L
A fasting blood sugar level of 126 mg/dL or higher is consistent with either type 1 or type 2 diabetes. Patient’s FBS is exceeds the normal limits indicating the patient has diabetes.
The sodium electrolyte level is below normal range. It indicates that the patient has hyponatremia.
retention and excretion of water.
POTASSIUM - While, Potassium is checked in order to assess a known and suspected disorder associated with renal disease, glucose metabolism, trauma or burns.
3.8 3.5 – 5.2 mEq/LThe potassium electrolyte level is within normal range.
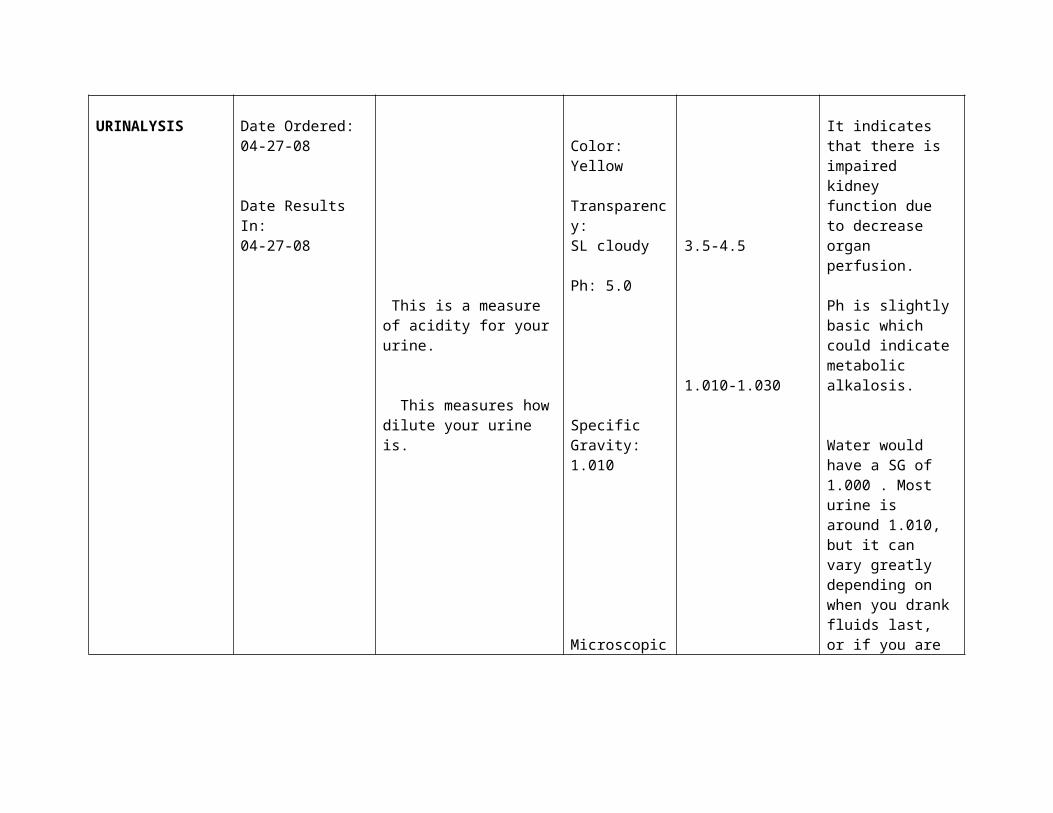
URINALYSIS Date Ordered:04-27-08
Date Results In:04-27-08
This is a measure of acidity for your urine.
This measures how dilute your urine is.
Color: Yellow
Transparency:SL cloudy
Ph: 5.0
Specific Gravity: 1.010
3.5-4.5
1.010-1.030
It indicates that there is impaired kidney function due to decrease organ perfusion.
Ph is slightly basic which could indicate metabolic alkalosis.
Water would have a SG of 1.000 . Most urine is around 1.010, but it can
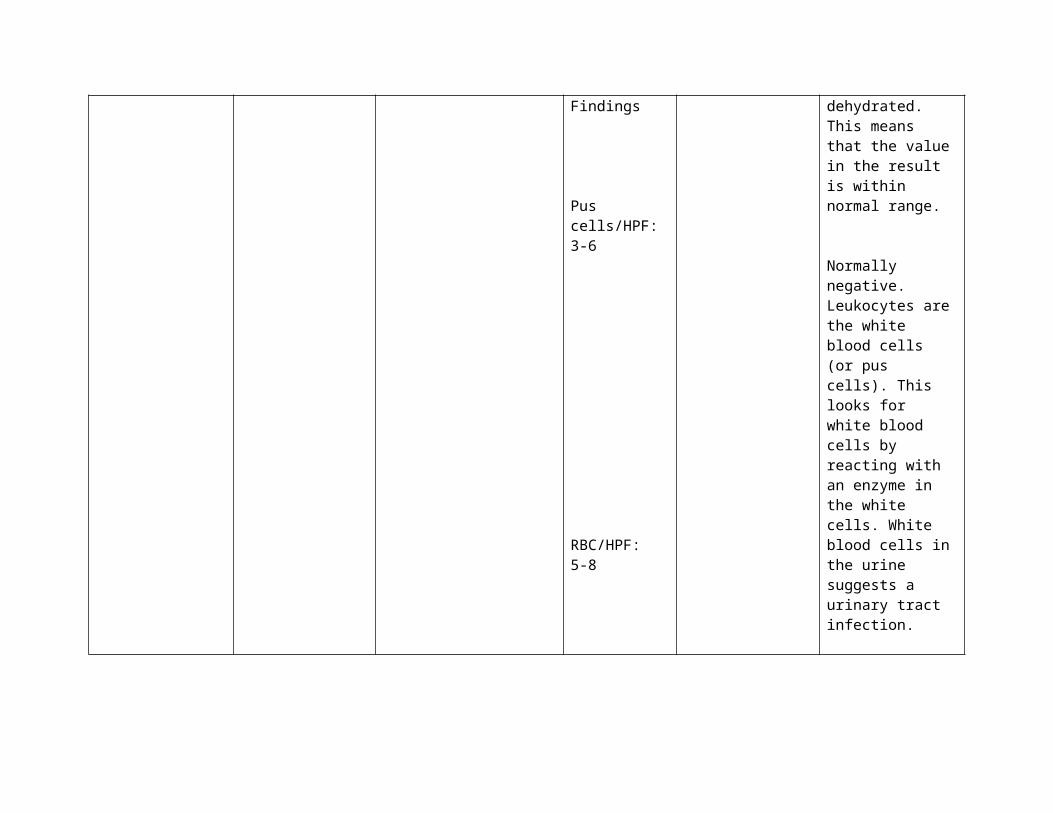
Microscopic Findings
Pus cells/HPF:3-6
RBC/HPF:5-8
vary greatly depending on when you drank fluids last, or if you are dehydrated. This means that the value in the result is within normal range.
Normally negative. Leukocytes are the white blood cells (or pus cells). This looks for white blood cells by reacting with an enzyme in the white cells. White blood cells in the urine suggests a urinary tract infection.
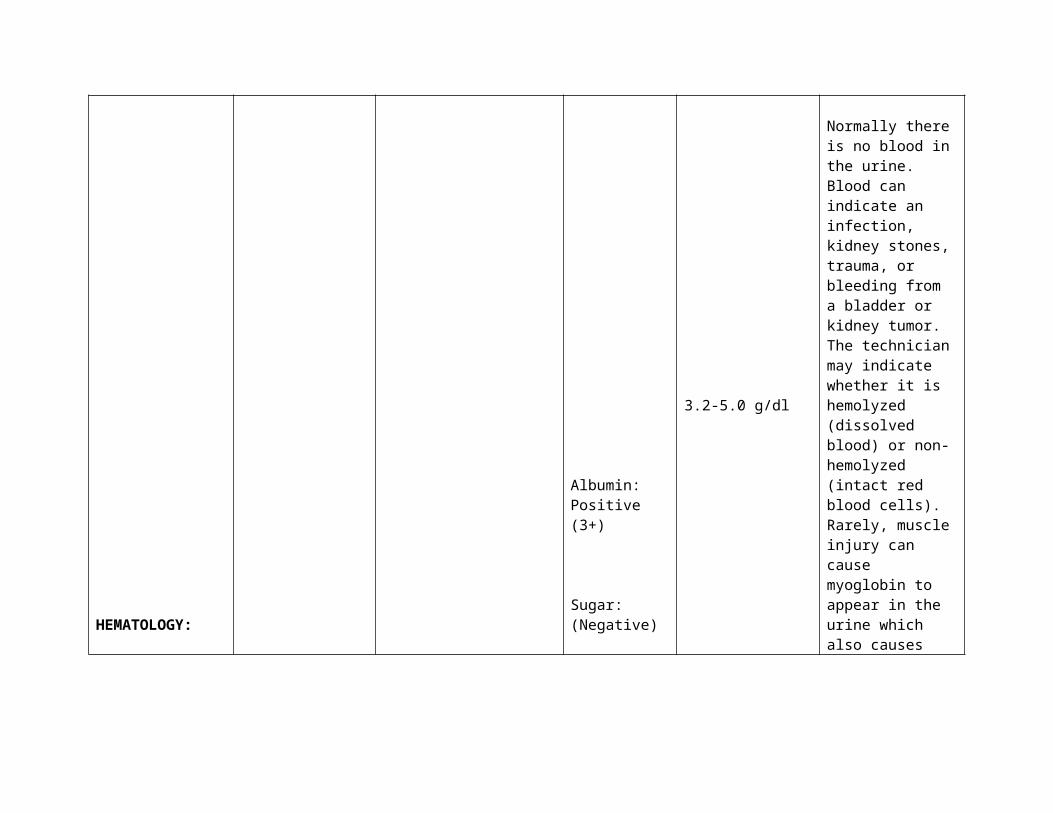
Normally there is no blood in the urine. Blood can indicate an
HEMATOLOGY:
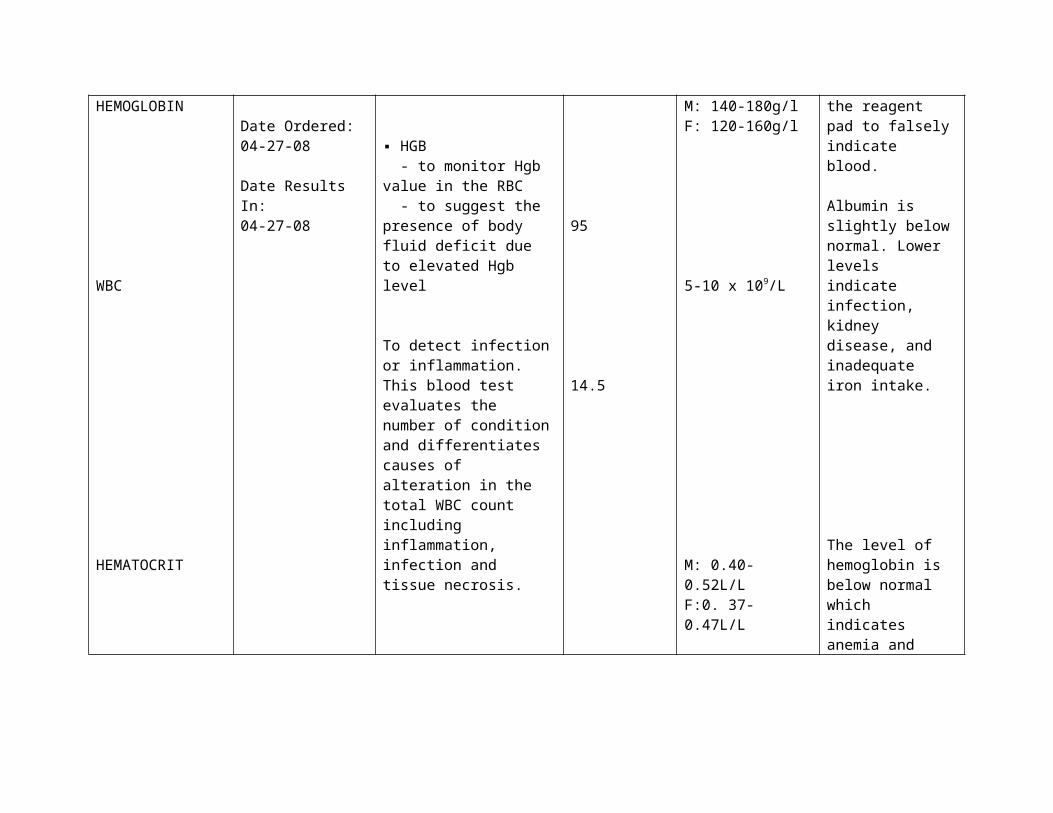
HEMOGLOBIN Date Ordered: ▪ HGB
Albumin:Positive (3+)
Sugar:(Negative)
3.2-5.0 g/dl
M: 140-180g/l
infection, kidney stones, trauma, or bleeding from a bladder or kidney tumor. The technician may indicate whether it is hemolyzed (dissolved blood) or non-hemolyzed (intact red blood cells). Rarely, muscle injury can cause myoglobin to appear in the urine which also causes the reagent pad to falsely indicate blood.
Albumin is slightly below normal. Lower levels indicate infection, kidney disease, and inadequate iron intake.
WBC
HEMATOCRIT
04-27-08
Date Results In:04-27-08
- to monitor Hgb value in the RBC - to suggest the presence of body fluid deficit due to elevated Hgb level
To detect infection or inflammation. This blood test evaluates the number of condition and differentiates causes of alteration in the total WBC count including inflammation, infection and tissue necrosis.
to aid diagnosis of abnormal states of hydration, polycythemia and anemia. - It measures the concentration of RBC within the blood volume and is expressed as a percentage.
95
14.5
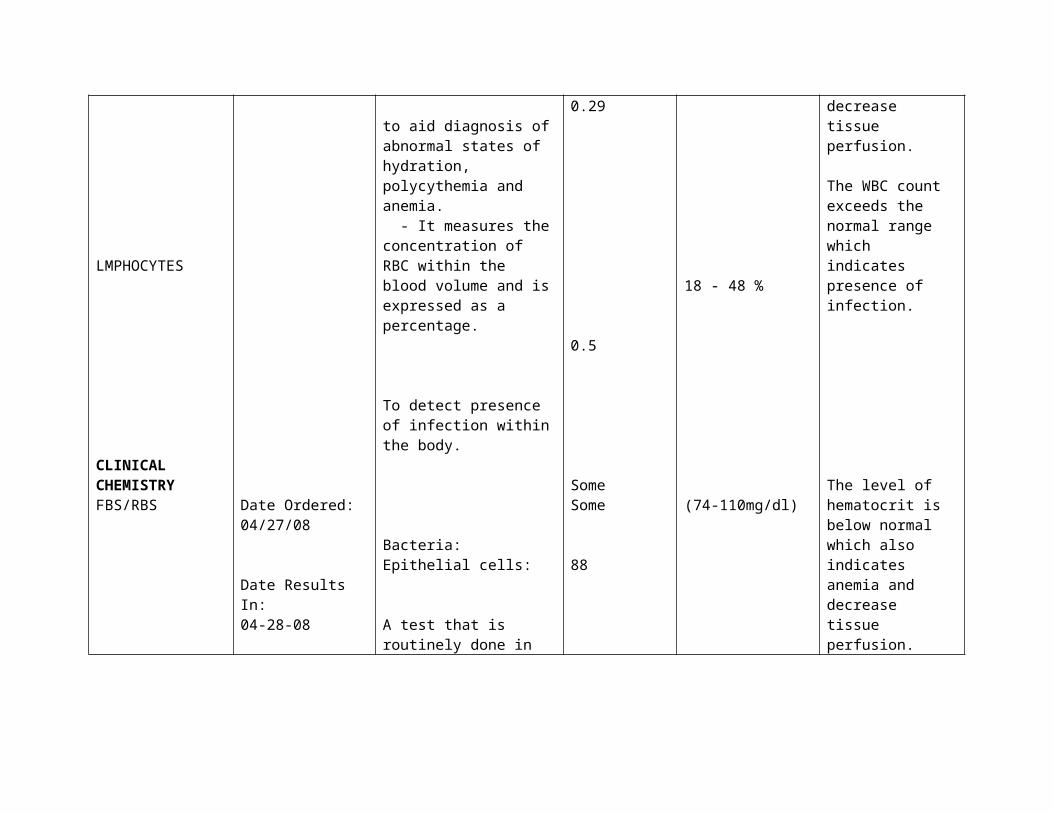
0.29
F: 120-160g/l
5-10 x 109/L
M: 0.40-0.52L/LF:0. 37-0.47L/L
The level of hemoglobin is below normal which indicates anemia and decrease tissue perfusion.
The WBC count exceeds the normal range which indicates presence of infection.
The level of hematocrit is below normal which also indicates anemia and decrease
LMPHOCYTES
CLINICAL CHEMISTRYFBS/RBS
CHOLESTEROL
Date Ordered:04/27/08
Date Results In:04-28-08
To detect presence of infection within the body.
Bacteria:Epithelial cells:
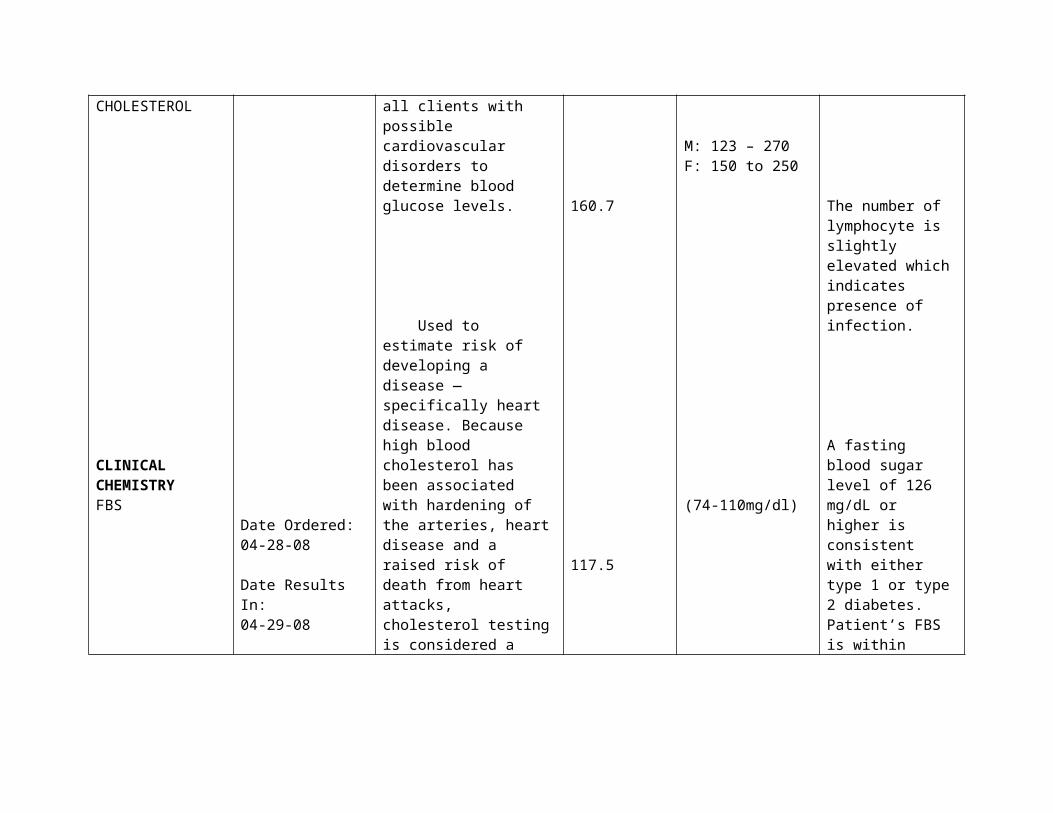
A test that is routinely done in all clients with possible cardiovascular disorders to determine blood glucose levels.
Used to estimate risk of developing a disease — specifically heart disease. Because high blood cholesterol has been associated with hardening of the arteries, heart disease and a raised risk of
0.5
SomeSome
88
160.7
18 - 48 %
(74-110mg/dl)
M: 123 – 270F: 150 to 250
tissue perfusion.
The number of lymphocyte is slightly elevated which indicates presence of infection.
A fasting blood sugar level of 126 mg/dL or higher is consistent with either type 1 or type 2 diabetes. Patient’s FBS is within normal range
The cholesterol level is within the normal range.
CLINICAL CHEMISTRYFBS
BUN
CHOLESTEROL
Date Ordered:04-28-08
Date Results In:04-29-08
death from heart attacks, cholesterol testing is considered a routine part of preventive health care.
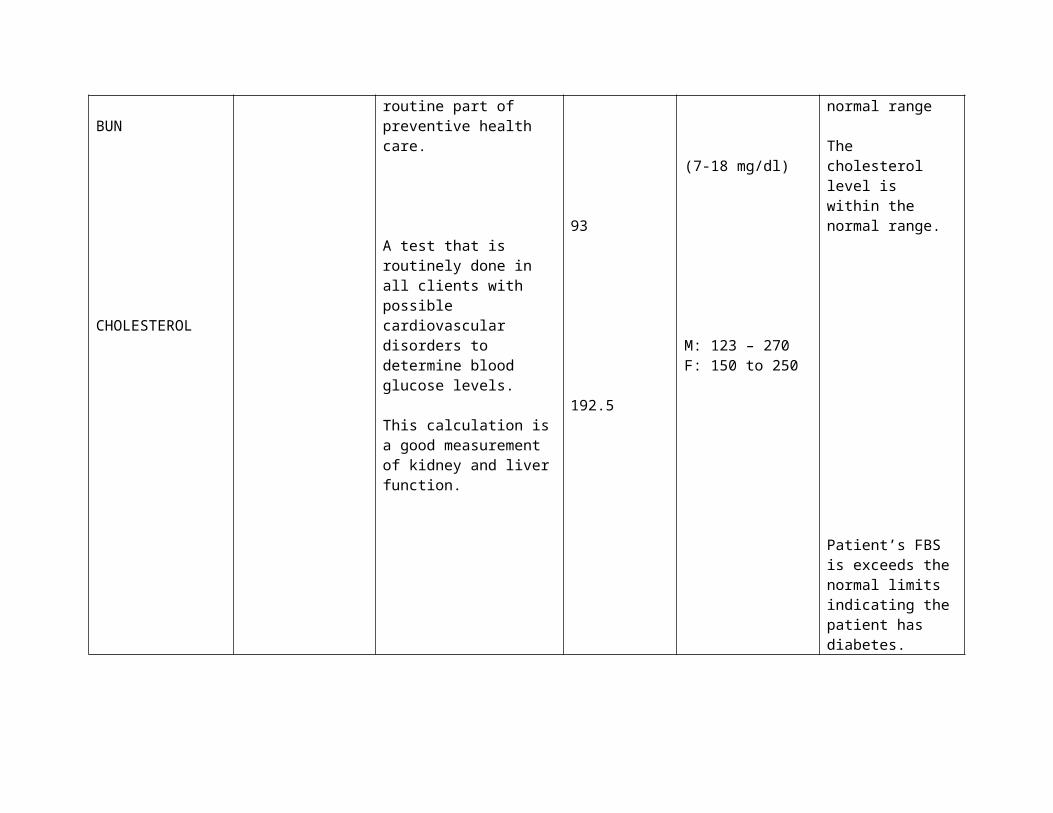
A test that is routinely done in all clients with possible cardiovascular disorders to determine blood glucose levels.
This calculation is a good measurement of kidney and liver function.
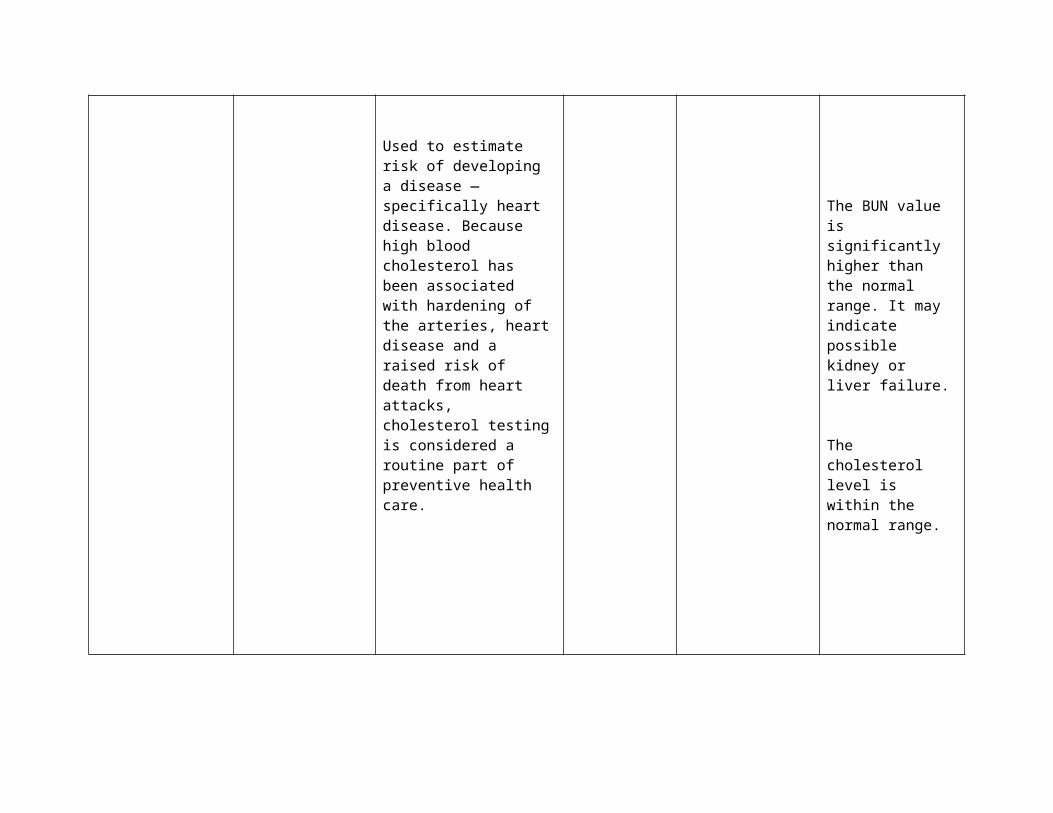
Used to estimate risk of developing a disease — specifically heart disease. Because
117.5
93
192.5
(74-110mg/dl)
(7-18 mg/dl)
M: 123 – 270F: 150 to 250
Patient’s FBS is exceeds the normal limits indicating the patient has diabetes.
The BUN value is significantly higher than the normal range. It may indicate possible kidney or liver failure.
high blood cholesterol has been associated with hardening of the arteries, heart disease and a raised risk of death from heart attacks, cholesterol testing is considered a routine part of preventive health care.
The cholesterol level is within the normal range.
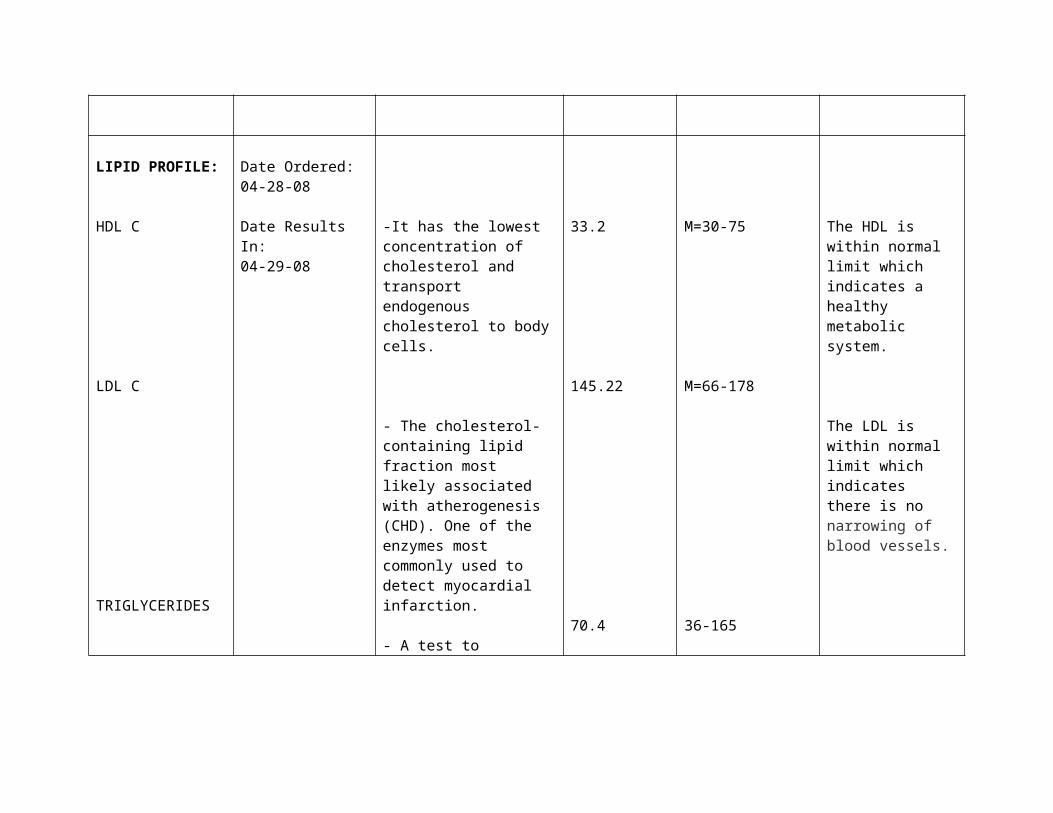
LIPID PROFILE:
HDL C
LDL C
Date Ordered:04-28-08
Date Results In:04-29-08
-It has the lowest concentration of cholesterol and transport endogenous cholesterol to body cells.
- The cholesterol-containing lipid fraction most likely associated with atherogenesis (CHD). One of the enzymes most commonly used to detect myocardial infarction.
33.2
145.22
M=30-75
M=66-178
The HDL is within normal limit which indicates a healthy metabolic system.
The LDL is within normal limit which indicates there is no narrowing of blood vessels.
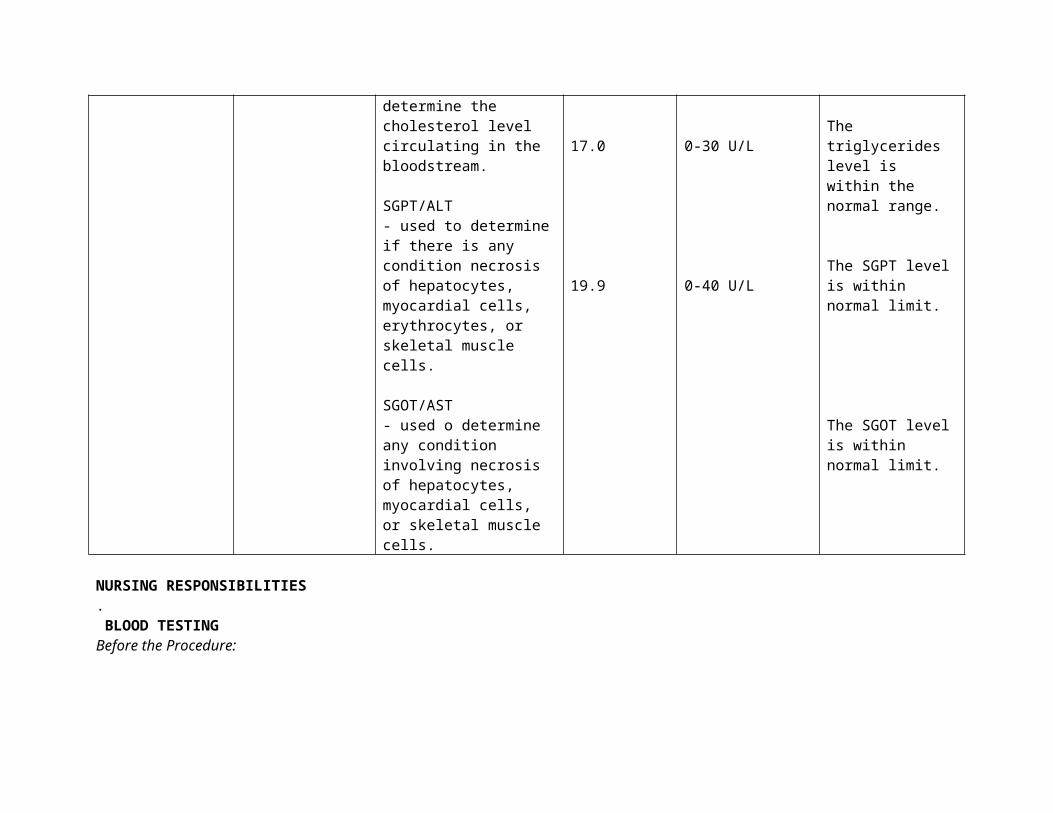
TRIGLYCERIDES - A test to determine the cholesterol level circulating in the bloodstream.
SGPT/ALT- used to determine if there is any condition necrosis of hepatocytes, myocardial cells, erythrocytes, or skeletal muscle cells.
SGOT/AST- used o determine any condition involving necrosis of hepatocytes, myocardial cells, or skeletal muscle cells.
70.4
17.0
19.9
36-165
0-30 U/L
0-40 U/L
The triglycerides level is within the normal range.
The SGPT level is within normal limit.
The SGOT level is within normal limit.
NURSING RESPONSIBILITIES. BLOOD TESTINGBefore the Procedure:
a. Explain the procedure to the client in order to gain cooperation.b. Inform the client that she may feel pain during needle insertion.c. Prepare the materials necessary for the test.d. Practice aseptic technique by cleaning the area of blood extraction with alcohol in an outward circular
motion.
During the Procedure:a. Provide comfort to the client.b. Encourage the patient to relax and refrain from unnecessary movements.
After the Procedure:a. Apply pressure on the site of puncture to prevent bleeding.b. Handle the blood sample carefully to prevent hemolysis.
URINALYSISBefore the Procedure:
a. Explain the procedure to the client in order to gain her b. Inform the client that there is no need for NPO.c. Educate the patient on the proper way of collecting urine (clean catch midstream specimen).d. Prepare the container for the urine.
During the Procedure:a. Provide privacy.b. Assist the patient if unable to get her urine sample on her own.c. Instruct the patient to prevent contamination of the urine and not to add water to the urine specimen , to
prevent alteration of reslts.
After the Procedure:a. Refrigerate the specimen.b. Continue taking the medications that were stopped prior to the procedure.
III . ANATOMY AND PHYSIOLOGY
The Cardiovascular System
The heart and circulatory system make up the cardiovascular system.
The heart works as a pump that pushes blood to the organs, tissues, and cells
of the body. Blood delivers oxygen and nutrients to every cell and removes
the carbon dioxide and waste products made by those cells. Blood is carried
from the heart to the rest of the body through a complex network of arteries,
arterioles, and capillaries. Blood is returned to the heart through venules and
veins.
The one-way circulatory system carries blood to all parts of the body.
This process of blood flow within the body is called circulation. Arteries carry
oxygen-rich blood away from the heart, and veins carry oxygen-poor blood
back to the heart. In pulmonary circulation, though, the roles are switched. It
is the pulmonary artery that brings oxygen-poor blood into the lungs and the
pulmonary vein that brings oxygen-rich blood back to the heart.
Twenty major arteries make a path through the tissues, where they
branch into smaller vessels called arterioles. Arterioles further branch into
capillaries, the true deliverers of oxygen and nutrients to the cells. Most
capillaries are thinner than a hair. In fact, many are so tiny, only one blood
cell can move through them at a time. Once the capillaries deliver oxygen
and nutrients and pick up carbon dioxide and other waste, they move the
blood back through wider vessels called venules. Venules eventually join to
form veins, which deliver the blood back to the heart to pick up oxygen.
Vasoconstriction or the spasm of smooth muscles around the blood
vessels causes and decrease in blood flow but an increase in pressure. In
vasodilation, the lumen of the blood vessel increase in diameter thereby
allowing increase in blood flow. There is no tension on the walls of the vessels
therefore, there is lower pressure.
Various external factors also cause changes in blood pressure and
pulse rate. An elevation or decline may be detrimental to health. Changes
may also be caused or aggravated by other disease conditions existing in
other parts of the body.
The blood is part of the circulatory system. Whole blood contains three
types of blood cells, including: red blood cells, white blood cells and platelets.
These three types of blood cells are mostly manufactured in the bone
marrow of the vertebrae, ribs, pelvis, skull, and sternum. These cells travel
through the circulatory system suspended in a yellowish fluid called plasma.
Plasma is 90% water and contains nutrients, proteins, hormones, and waste
products. Whole blood is a mixture of blood cells and plasma.
Red blood cells (also called erythrocytes) are shaped like slightly
indented, flattened disks. Red blood cells contain an iron-rich protein called
hemoglobin. Blood gets its bright red color when hemoglobin in red blood
cells picks up oxygen in the lungs. As the blood travels through the body, the
hemoglobin releases oxygen to the tissues. The body contains more red
blood cells than any other type of cell, and each red blood cell has a life span
of about 4 months. Each day, the body produces new red blood cells to
replace those that die or are lost from the body.
White blood cells (also called leukocytes) are a key part of the body's
system for defending itself against infection. They can move in and out of the
bloodstream to reach affected tissues. The blood contains far fewer white
blood cells than red cells, although the body can increase production of white
blood cells to fight infection. There are several types of white blood cells, and
their life spans vary from a few days to months. New cells are constantly
being formed in the bone marrow.
Several different parts of blood are involved in fighting infection. White
blood cells called granulocytes and lymphocytes travel along the walls of
blood vessels. They fight bacteria and viruses and may also attempt to
destroy cells that have become infected or have changed into cancer cells.
Certain types of white blood cells produce antibodies, special proteins
that recognize foreign materials and help the body destroy or neutralize
them. When a person has an infection, his or her white cell count often is
higher than when he or she is well because more white blood cells are being
produced or are entering the bloodstream to battle the infection. After the
body has been challenged by some infections, lymphocytes remember how to
make the specific antibodies that will quickly attack the same germ if it
enters the body again.
Platelets (also called thrombocytes) are tiny oval-shaped cells made in
the bone marrow. They help in the clotting process. When a blood vessel
breaks, platelets gather in the area and help seal off the leak. Platelets
survive only about 9 days in the bloodstream and are constantly being
replaced by new cells.
Blood also contains important proteins called clotting factors, which
are critical to the clotting process. Although platelets alone can plug small
blood vessel leaks and temporarily stop or slow bleeding, the action of
clotting factors is needed to produce a strong, stable clot.
Platelets and clotting factors work together to form solid lumps to seal
leaks, wounds, cuts, and scratches and to prevent bleeding inside and on the
surfaces of our bodies. The process of clotting is like a puzzle with
interlocking parts. When the last part is in place, the clot is formed.
When large blood vessels are cut the body may not be able to repair
itself through clotting alone. In these cases, dressings or stitches are used to
help control bleeding.
In addition to the cells and clotting factors, blood contains other
important substances, such as nutrients from the food that has been
processed by the digestive system. Blood also carries hormones released by
the endocrine glands and carries them to the body parts that need them.
Blood is essential for good health because the body depends on a
steady supply of fuel and oxygen to reach its billions of cells. Even the heart
couldn't survive without blood flowing through the vessels that bring
nourishment to its muscular walls. Blood also carries carbon dioxide and
other waste materials to the lungs, kidneys, and digestive system, from
where they are removed from the body.
The Urinary System
The components of the urinary system are: two kidneys, two ureters, urinary
bladder and urethra. The kidneys process blood and form urine by filtering
blood plasma (glomerular filtration) and returning most of the water and
solutes to the bloodstream (tubular reabsorption). The remaining water and
solutes constitute the urine (secretion) which passes through ureters, are
stored in the urinary bladder, then excreted from the body through the
urethra.
The main functions of the kidneys are to regulate blood volume and
composition, help regulate blood pressure, synthesize glucose, release
erythropoietin, participate in vitamin D synthesis and excrete wastes in the
urine.
The nephron is functional unit of the kidney. The parts of the nephron are:
renal corpuscle- where blood plasma is filtered and renal tubule- into which
filtered fluid passes. The renal corpusclelies within the renal cortex and
consists of two components: glomerulus and the glomerular (Bowman's)
capsule- a double-walled epithelial cup that surrounds the glomerulus. The
parts of a renal tubule are: proximal convoluted tubule- lies within the renal
cortex, loop of Henle (nephron loop)- extends into the renal medulla, distal
convoluted tubule- lies within the renal cortex, distal convoluted tubules of
several nephrons empty into a single collecting duct.
Malfunctioning of one of the small portions that make up the nephron will
cause impairment in the functioning of the kidneys. Glomerular filtration rate
may decrease, and as a result, large molecules are drained out and secreted
in the urine. Examples of which are RBC and protein molecules. Likewise,
accumulation of sodium causes formation of crystals, which, when dislodged,
may either block passageways of urine, or be excreted and seen as crystals
in the urine.
The Endocrine System
The endocrine system is made up of glands that produce and secrete
hormones. These hormones regulate the body’s growth, metabolism (the
physical and chemical processes of the body), and sexual development and
function. The hormones are released into the bloodstream and may affect
one or several organs throughout the body.
The role of the endocrine system is to maintain the body in balance
through the release of hormones which transfer information and instructions
from one set of cells to another. Many different hormones move through the
bloodstream, but each type of hormone is designed to affect only certain
cells.
Hormones are chemical messengers created by the body. They
transfer information from one set of cells to another to coordinate the
functions of different parts of the body. Hormones can act on some specific
cells because they themselves do not actually cause an effect. It is only
through binding with a receptor (part of the cell specifically designed to
recognize the hormone) like a key into a lock - that causes a chain reaction to
occur, changing the activity of the cells. If a cell does not have a receptor for
a hormone then there will be no effect. Also, there can be different receptors
for the same hormone, and so the same hormone can have different effects
on different cells.
The major glands of the endocrine system are the pituitary, thyroid,
parathyroids, adrenals, pineal body, thymus, and the reproductive organs
(ovaries and testes). The pancreas is also a part of this system; it has a role
in hormone production as well as in digestion. A gland is a group of cells that
produces and secretes chemicals. A gland selects and removes materials
from the blood, processes them, and secretes the finished chemical product
for use somewhere in the body. The endocrine gland cells release a hormone
into the blood stream for distribution throughout the entire body. These
hormones act as chemical messengers and can alter the activity of many
organs at once.
The hypothalamus controls all the processes undergone by the anterior
and posterior pituitary glands. It initiates the production of hormones by the
APG. The APG is controlled by releasing hormones which are chemical signals
produced by the nerve cells of the hypothalamus, causing either stimulation
or inhibition of hormone production. Secretion of hormones by the PPG is
controlled by nervous system stimulation of nerve cells in the hypothalamus.
Parathyroid glands secrete parathyroid hormone which is essential for the
regulation of blood calcium levels. Adrenal glands produce epinephrine and
norepinephrine which are fight-or-flight hormones that prepare the body for
vigorous physical activity. Testes and ovaries produce hormones that are
responsible for secondary sex characteristics, spermatogenesis, and
oogenesis. The thymus gland secretes thymosin which aids in the synthesis
of WBC for fighting infection. This gland decreases in size in some older
adults. The pineal body releases melatonin that is thought to decrease the
secretion of LSH & FSH by decreasing the release of hypothalamic-releasing
hormones. The thyroid gland, located on either side of the trachea, is
controlled by the thyroid stimulating hormone releases by the anterior
pituitary gland, which was initially stimulated by the TSH releasing hormone
from the hypothalamus.
The pancreas is also part of the body's hormone-secreting system,
even though it is also associated with the digestive system because it
produces and secretes digestive enzymes. The pancreas produces two
important hormones, insulin and glucagon. They work together to maintain a
steady level of glucose, or sugar, in the blood and to keep the body supplied
with fuel to produce and maintain stores of energy. The pancreas completes
the job of breaking down protein, carbohydrates, and fats using digestive
juices of pancreas combined with juices from the intestines, secretes
hormones that affect the level of sugar in the blood, and produces chemicals
that neutralize stomach acids that pass from the stomach into the small
intestine by using substances in pancreatic juice. It contains Islets of
Langerhans, which are tiny groups of specialized cells that are scattered
throughout the organ.
In humans, the pancreas is a 15-25 cm (6-10 inch) elongated organ in
the abdomen adjacent to the small intestine and lies toward the back. It has
three regions: a head (abuts a part of the duodenum), body (at the level of L2
of the spine) and tail (extends toward the spleen).
The pancreatic duct (also called the duct of Wirsung) runs the length of
the pancreas and empties into the second part of the duodenum at the
ampulla of Vater. The common bile duct usually joins the pancreatic duct at
or near this point. Many people also have a small accessory duct, the duct of
Santorini, which extends from the main duct more upstream (towards the
tail) to the duodenum, joining it more proximal than the ampulla of Vater.
The pancreas is supplied arterially by the Pancreaticoduodenal arteries
and the splenic artery: the splenic artery supplies the neck, body, and tail of
the pancreas; the superior mesenteric artery provides the inferior
pancreaticoduodenal artery; and the gastroduodenal artery provides the
superior pancreaticoduodenal artery.
Venous drainage is via the pancreaticoduodenal veins which end up in
the portal vein. The splenic vein passes posterior to the pancreas but is said
to not drain the pancreas itself. The portal vein is formed by the union of the
superior mesenteric vein and splenic vein posterior to the neck of the
pancreas. In some people (some books say 40% of people), the inferior
mesenteric vein also joins with the splenic vein behind the pancreas (in
others it simply joins with the superior mesenteric vein instead).
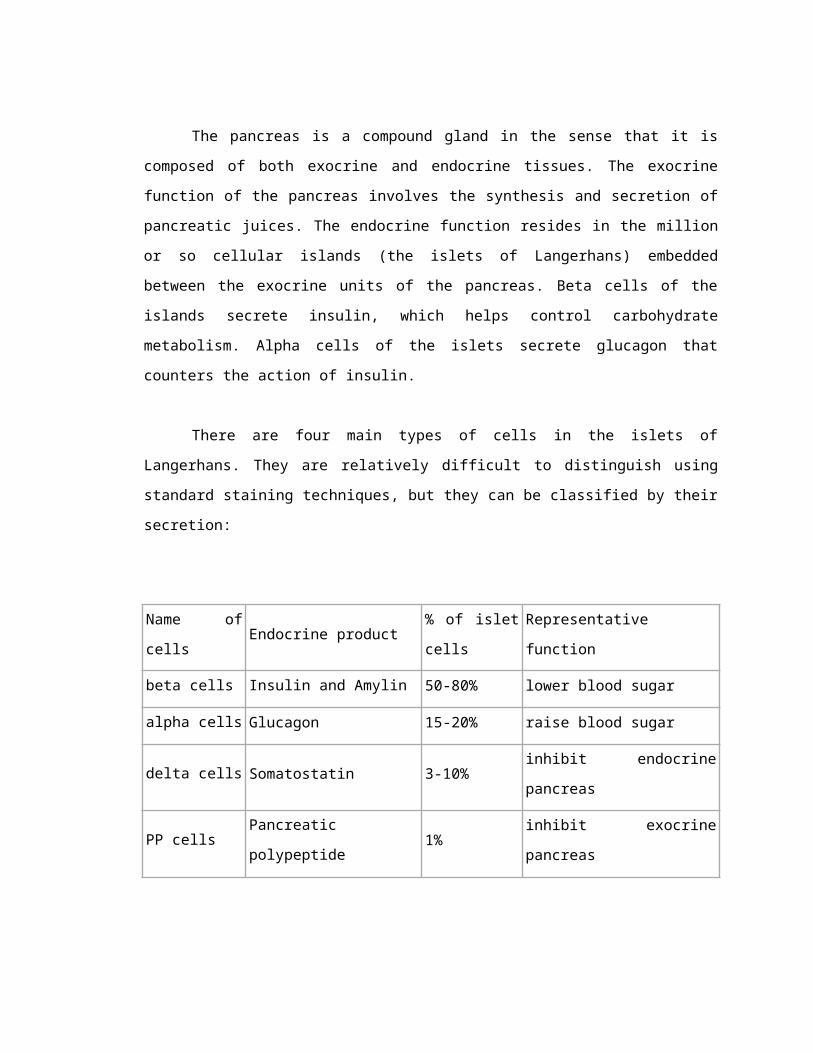
The pancreas is a compound gland in the sense that it is composed of
both exocrine and endocrine tissues. The exocrine function of the pancreas
involves the synthesis and secretion of pancreatic juices. The endocrine
function resides in the million or so cellular islands (the islets of Langerhans)
embedded between the exocrine units of the pancreas. Beta cells of the
islands secrete insulin, which helps control carbohydrate metabolism. Alpha
cells of the islets secrete glucagon that counters the action of insulin.
There are four main types of cells in the islets of Langerhans. They are
relatively difficult to distinguish using standard staining techniques, but they
can be classified by their secretion:
Name of
cellsEndocrine product
% of islet
cellsRepresentative function
beta cells Insulin and Amylin 50-80% lower blood sugar
alpha cells Glucagon 15-20% raise blood sugar
delta cells Somatostatin 3-10%inhibit endocrine
pancreas
PP cells Pancreatic polypeptide 1% inhibit exocrine pancreas
The islets are a compact collection of endocrine cells arranged in
clusters and cords and are crisscrossed by a dense network of capillaries. The
capillaries of the islets are lined by layers of endocrine cells in direct contact
with vessels, and most endocrine cells are in direct contact with blood
vessels, by either cytoplasmic processes or by direct apposition.
There are two main types of exocrine pancreatic cells, responsible for
two main classes of secretions:
Name of cells Exocrine secretion Primary signal
Centroacinar cells bicarbonate ions Secretin
Basophilic cells
digestive enzymes
(pancreatic amylase, Pancreatic
lipase,
trypsinogen, chymotrypsinogen, etc.)
CCK
THE INTEGUMENTARY SYSTEM
Integumentary System
The skin is the largest organ in the body: 12-15% of body weight, with a
surface area of 1-2 meters. Skin is continuous with, but structurally distinct
from mucous membranes that line the mouth, anus, urethra, and vagina. Two
distinct layers occur in the skin: the dermis and epidermis. The basic cell type
of the epidermis is the keratinocyte, which contain keratin, a fibrous protein.
Basal cells are the innermost layer of the epidermis. Melanocytes produce the
pigment melanin, and are also in the inner layer of the epidermis. The dermis
is a connective tissue layer under the epidermis, and contains nerve endings,
sensory receptors, capillaries, and elastic fibers.
The integumentary system has multiple roles in homeostasis, including
protection, temperature regulation, sensory reception, biochemical synthesis,
and absorption. All body systems work in an interconnected manner to
maintain the internal conditions essential to the function of the body.
Follicles and Glands
Hair follicles are lined with cells that synthesize the proteins that form hair. A
sebaceous gland (that secretes the oily coating of the hair shaft), capillary
bed, nerve ending, and small muscle are associated with each hair follicle. If
the sebaceous glands becomes plugged and infected, it becomes a skin
blemish (or pimple). The sweat glands open to the surface through the skin
pores. Eccrine glands are a type of sweat gland linked to the sympathetic
nervous system; they occur all over the body. Apocrine glands are the other
type of sweat gland, and are larger and occur in the armpits and groin areas;
these produce a solution that bacteria act upon to produce "body odor".
The Digestive System
The human digestive system, as shown in Figure 2, is a coiled, muscular tube
(6-9 meters long when fully extended) stretching from the mouth to the anus.
Several specialized compartments occur along this length: mouth, pharynx,
esophagus, stomach, small intestine, large intestine, and anus. Accessory
digestive organs are connected to the main system by a series of ducts:
salivary glands, parts of the pancreas, and the liver and gall bladder (bilary
system).
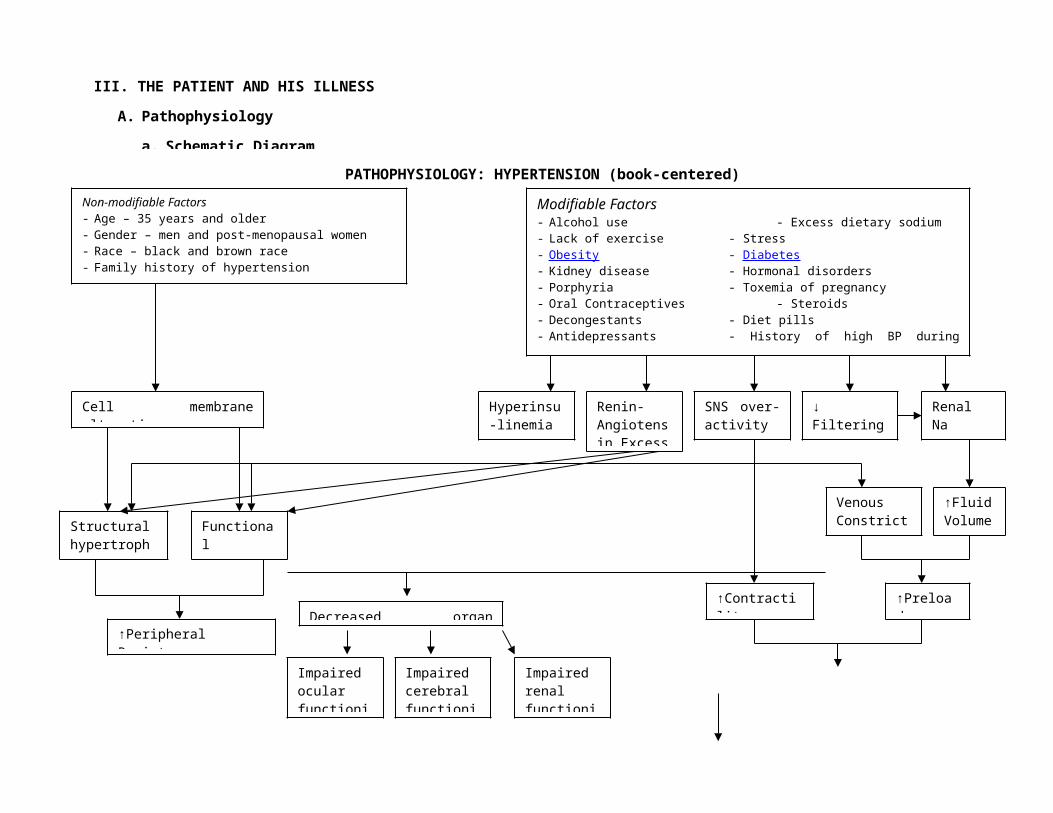
III. THE PATIENT AND HIS ILLNESS
A. Pathophysiology
a. Schematic Diagram
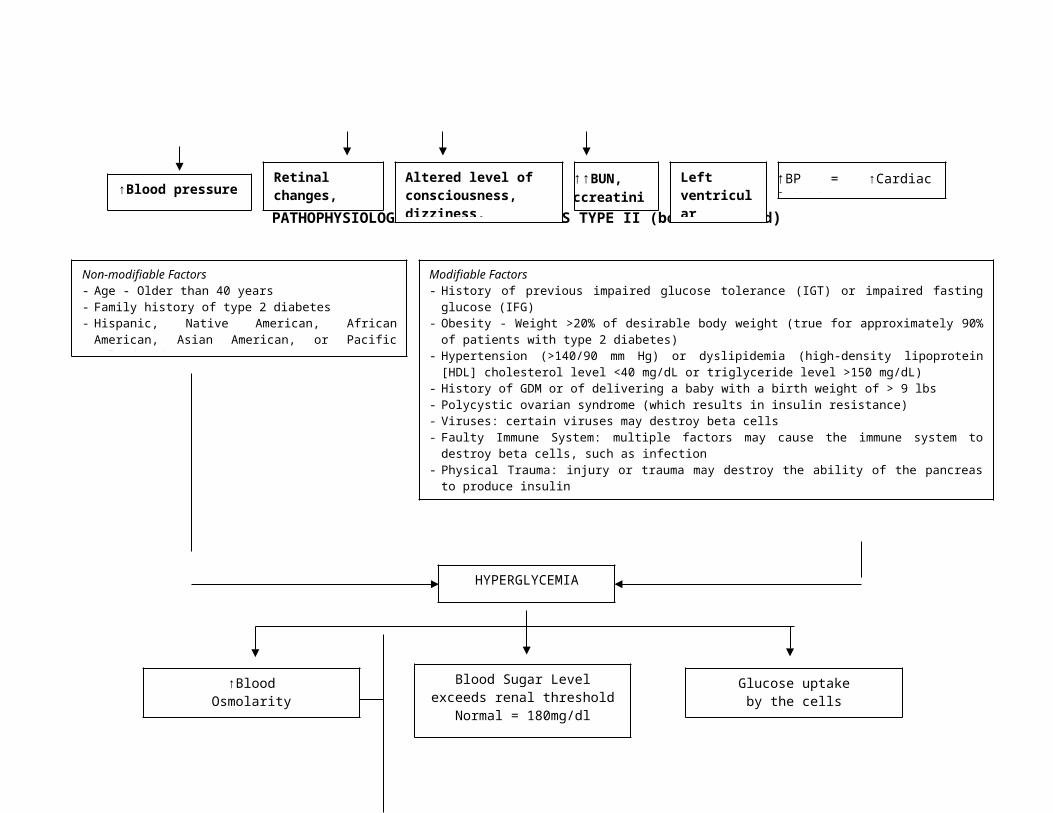
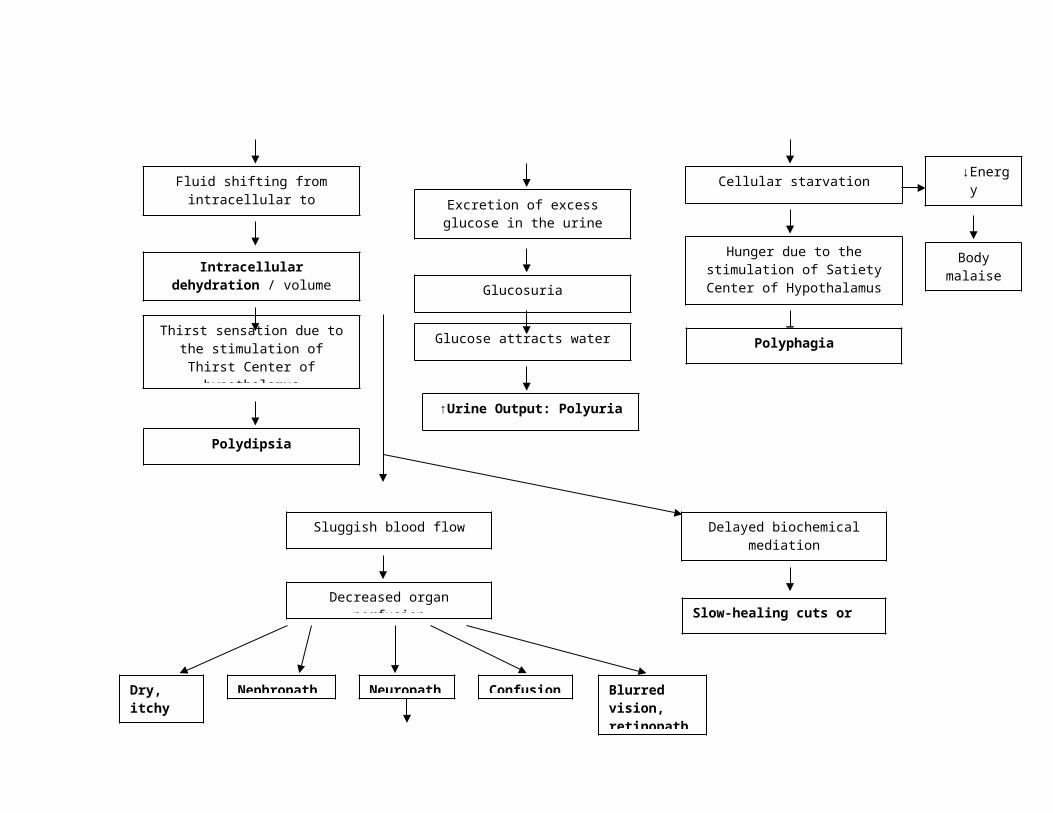
PATHOPHYSIOLOGY: DIABETES MELLITUS TYPE II (book-centered)
Non-modifiable Factors - Age – 35 years and older- Gender – men and post-menopausal women- Race – black and brown race - Family history of hypertension
Modifiable Factors - Alcohol use - Excess dietary sodium - Lack of exercise - Stress - Obesity - Diabetes - Kidney disease - Hormonal disorders - Porphyria - Toxemia of pregnancy- Oral Contraceptives - Steroids - Decongestants - Diet pills - Antidepressants - History of high BP during pregnancy - Nonsteroidal anti-inflammatory drugs
Cell membrane alteration
Structural hypertrophy
Functional Constriction
SNS over-activity
↓ Filtering surface
Renin-Angiotensin Excess
Hyperinsu-linemia
↑Contractility
Venous Constriction
Renal Na retention
↑Fluid Volume
↑Preload
↑BP = ↑Cardiac Output
↑Peripheral Resistance
↑Blood pressure
Decreased organ perfusion
Impaired ocular functioning
Impaired cerebral functioning
Impaired renal functioning
Retinal changes, papilledema
↑↑BUN, ccreatinine
Altered level of consciousness, dizziness, headache
Left ventricular hypertrop
PATHOPHYSIOLOGY: HYPERTENSION (book-centered)
HYPERGLYCEMIA
↑BloodOsmolarity
Fluid shifting fromintracellular to extracellular
Intracellular dehydration / volume
depletion
Thirst sensation due to the stimulation of Thirst Center
of hypothalamus
Blood Sugar Level exceeds renal threshold
Normal = 180mg/dl
Excretion of excess glucose in the urine
Glucosuria
Glucose attracts water
Glucose uptakeby the cells
Cellular starvation
Hunger due to the stimulation of Satiety Center
of Hypothalamus
↓Energy Level
Polyphagia
Body malaise
Non-modifiable Factors - Age - Older than 40 years - Family history of type 2 diabetes - Hispanic, Native American, African American,
Asian American, or Pacific Islander descent, Asian
Modifiable Factors - History of previous impaired glucose tolerance (IGT) or impaired fasting glucose (IFG) - Obesity - Weight >20% of desirable body weight (true for approximately 90% of patients
with type 2 diabetes) - Hypertension (>140/90 mm Hg) or dyslipidemia (high-density lipoprotein [HDL]
cholesterol level <40 mg/dL or triglyceride level >150 mg/dL) - History of GDM or of delivering a baby with a birth weight of > 9 lbs - Polycystic ovarian syndrome (which results in insulin resistance) - Viruses: certain viruses may destroy beta cells- Faulty Immune System: multiple factors may cause the immune system to destroy beta
cells, such as infection- Physical Trauma: injury or trauma may destroy the ability of the pancreas to produce
insulin- Drugs: drugs used for other conditions could cause the development of diabetes- Stress: hormones at times of stress may block the effectiveness of insulin- Pregnancy: hormones produced during pregnancy can block the effectiveness of insulin
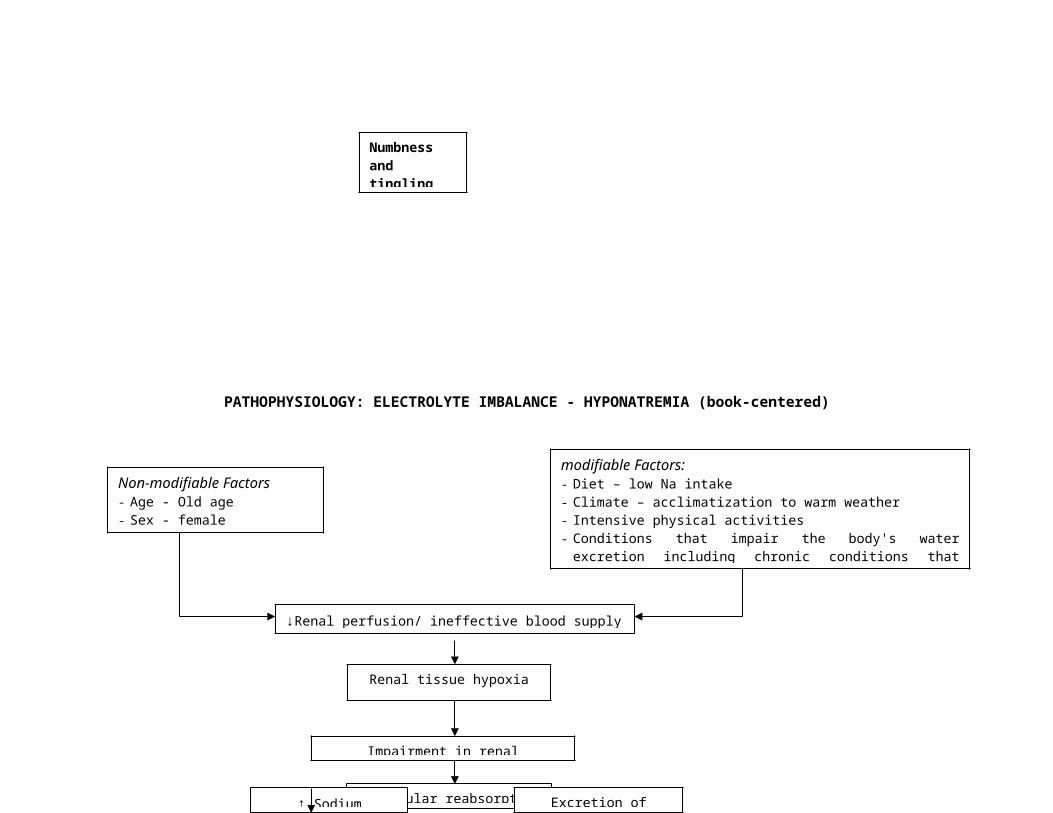
PATHOPHYSIOLOGY: ELECTROLYTE IMBALANCE - HYPONATREMIA (book-centered)
↑Urine Output: Polyuria
Polydipsia
Sluggish blood flow
Decreased organ perfusion
Blurred vision, retinopathy
Dry, itchy skin
ConfusioNephropat
Numbness and tingling sensation
Slow-healing cuts or sores
Neuropat
Delayed biochemical mediation
↓Renal perfusion/ ineffective blood supply to the kidneys
Non-modifiable Factors- Age - Old age- Sex - female
modifiable Factors:- Diet – low Na intake- Climate – acclimatization to warm weather- Intensive physical activities- Conditions that impair the body's water excretion
including chronic conditions that cause organ failure
Renal tissue hypoxia
Impairment in renal functioning
↓ tubular reabsorption
↑ Sodium excretion
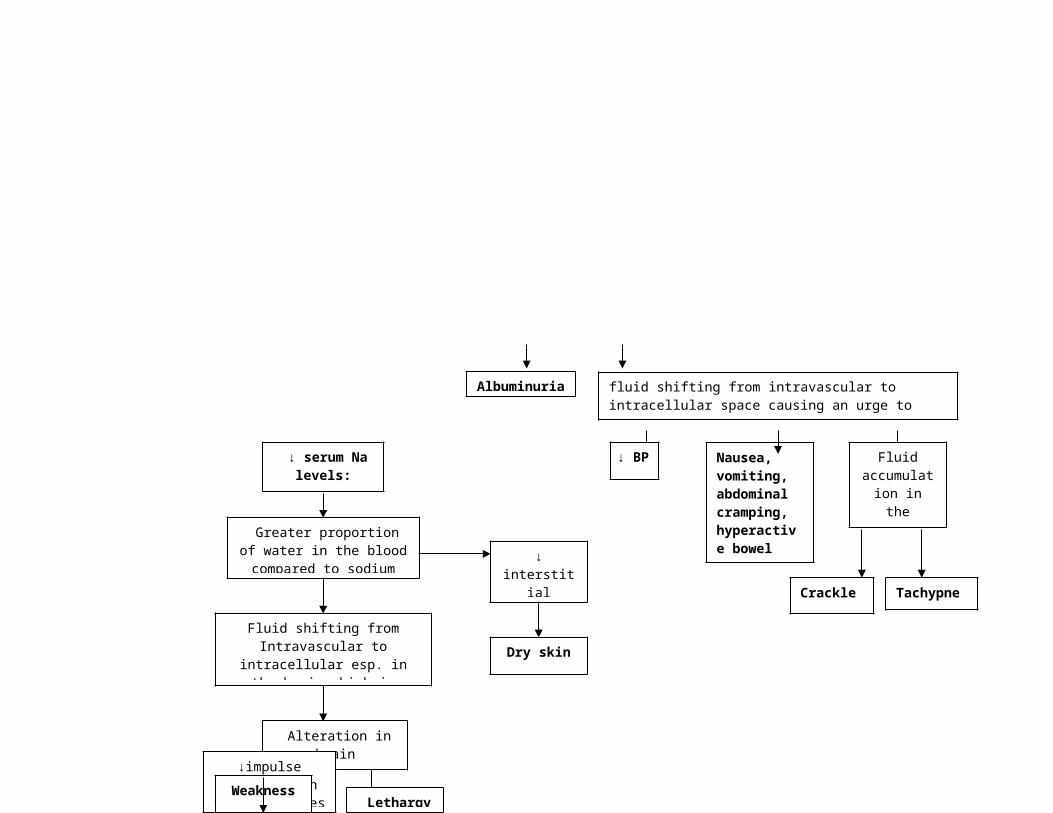
Albuminuri
Excretion of albumin
↓ serum Na levels:
Greater proportion of water in the blood
compared to sodiumFluid shifting from
Intravascular to intracellular esp. in the brain which is
sensitive to serum Na changes
↓ interstitial
fluid volumeDry skin
Alteration in brain functioning
Lethargy
↓impulse transmission to
the musclesWeakness
Nausea, vomiting, abdominal cramping, hyperactive bowel sounds
fluid shifting from intravascular to intracellular space causing an urge to expel excess water
Crackles
Fluid accumulation in the alveoli
Tachypnea
↓ BP
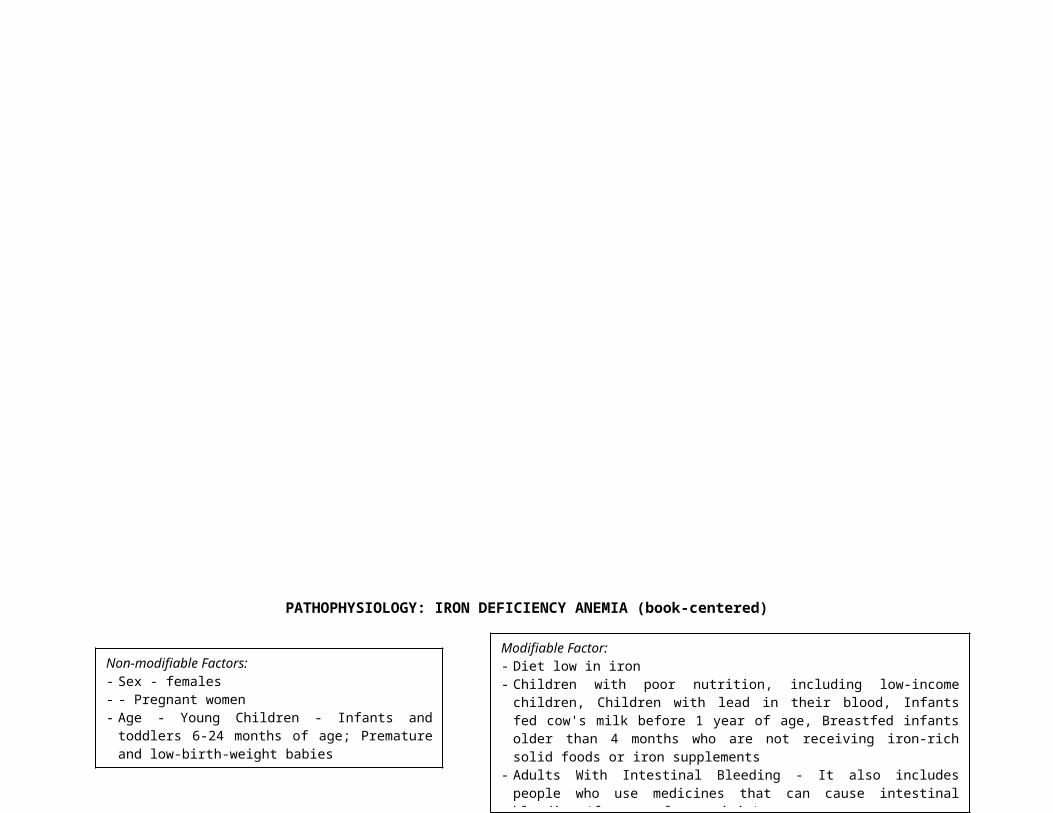
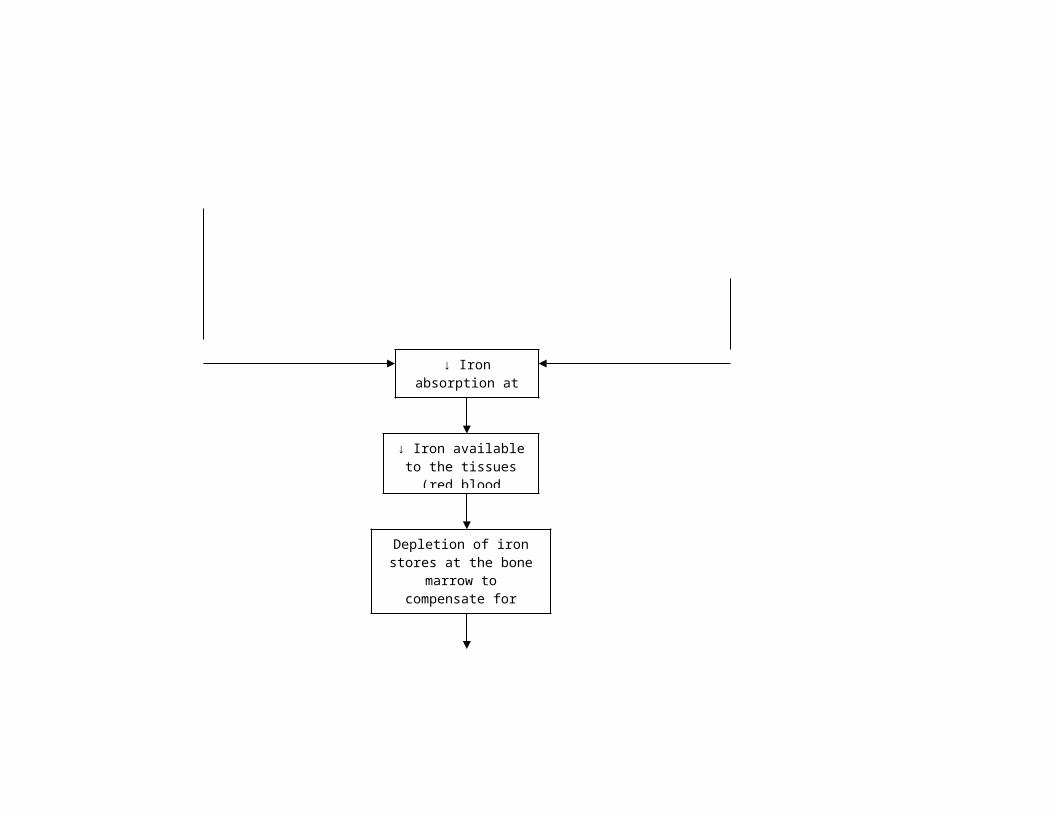
PATHOPHYSIOLOGY: IRON DEFICIENCY ANEMIA (book-centered)
Modifiable Factor: - Diet low in iron - Children with poor nutrition, including low-income children,
Children with lead in their blood, Infants fed cow's milk before 1 year of age, Breastfed infants older than 4 months who are not receiving iron-rich solid foods or iron supplements
- Adults With Intestinal Bleeding - It also includes people who use medicines that can cause intestinal bleeding (for example, aspirin).
- People who are on kidney dialysis, vegetarians, with low socioeconomic status and older adults who have poor diets.
↓ Iron absorption at the intestines
↓ Iron available to the tissues (red
blood cells)
Depletion of iron stores at the bone marrow to
compensate for decreased availability
Non-modifiable Factors:- Sex - females- - Pregnant women - Age - Young Children - Infants and toddlers 6-
24 months of age; Premature and low-birth-weight babies
PATHOPHYSIOLOGY: FURUNCLE (patient-centered)
Impaired hemoglobin and red blood cell synthesis
Decrease circulating red
blood cell along with its hemoglobin
Pallor
Fatigue
Shortness of breath,
tachypnea
Decreased oxyen supply to the body
Increased need for the heart to pump more blood to meet oxygen demand
Decrease in hemoglobin
Decrease oxygenation and circulating blood that provides heat
Cold hands and feet, brittle nails
Decrease oxygen supply to the integument
Swelling or soreness of the tongue and cracks
Enlarged Spleen
decreased perfusion to any affected part causing delay in biochemical mediation
Frequent Infectio
PATHOPHYSIOLOGY (patient-centered)
Modifiable Factors Poor hygiene Insect bite Excessive perspiration Increased pressure Increased friction
Development of wound
Enlargement of wound, turning red, firm and swollen
Development of a single, small, firm, swollen,
red/pink, tender nodule (furuncle) draining purulent secretions
↑Biochemical mediation through ↑
blood flow

Non-modifiable Factors - Age – 54 y/o- Gender – male- Race – brown race - Family history of hypertension
Modifiable Factors - Excess dietary sodium - Lack of exercise - Stress - Diabetes
Cell membrane alteration
Functional Constriction
SNS over-activity
Renin-Angiotensin Excess
Ineffective utilization of insulin
↑Contractility
Venous Constriction
Renal Na retention
↑Fluid Volume
↑Preload
↑↑Cardiac Output
↑Peripheral Resistance
↓Perfusion to the pancreas
Impairment in thefunctioning of the pancreas
Impaired insulin secretion
Hyperglycemia
↓Renal perfusion/ ineffective blood supply to the kidneys
Non-modifiable Factors- Age – 54 years old
Modifiable Factors- Diabetes mellitus;- active electrolyte loss from
vomiting; current low Na intake
↑BP: 170/100 mmHg: April 27, 2008; 150/90mmHg: April 28, 2008,
140/100 mmHg: April 29, 2008
↓Renal perfusion/ ineffective blood supply to the kidneys
Non-modifiable Factors- Age – 54 years old
Modifiable Factors- Diabetes mellitus;- active electrolyte loss from
vomiting; current low Na intake
Non-modifiable Factors- Age - Older than 40
years- Family history of DM
Modifiable Factors - History of previous impaired fasting
glucose - Hypertension (>140/90 mm Hg);
dyslipidemia (HDL level <40 mg/dl) - Stress: hormones at times of stress
may block the effectiveness of
↑BloodOsmolarity
Fluid shifting from
intracellular to extracellular
Intracellular dehydration
/ volume depletion
Thirst sensation due to the stimulation of Thirst Center of hypotha-
lamus
Blood Sugar Level exceeds renal
threshold : 137 mg/dl: April 27,
2008, 117.5mg/dl: April 28, 2008
Excretion of excess glucose in the urine
Glucose attracts water
↑Urine Output: polyuria
Glucose uptakeby the cells
Cellular starvation
Hunger due to the stimulation of Satiety
Center of Hypothalamus
Polyphagia
↓Energy
Level
Body malaise, Fatigue: April 27-
30, 2008
Renal tissue
hypoxia
Impairment in
renal functioning
↓ tubularreabsorption
↑ Sodiumexcretion
↓ serum Na levels: 113.4 mEq/l: April
27, 2008
Anorexia: April 23-30,
2008 Modifiable Factor: ↓ Iron intake & low socio-economic status
Sluggish blood
Albuminuria : +3 :
U/A- April 27, 2008
Excretion of albumin
Modifiable Factor: ↓ Iron intake & low socio-economic status
↓ Iron absorption at the intestines
↓ Iron available to the tissues (red
blood cells)
Depletion of iron stores at the bone marrow to
compensate for decreased availability
BUN: 93
mg/dl – April
29,

Polydipsia
Greater proportion of water in the blood
compared to sodium: Hemodilution: Hct – 0.29: April 27, 2008
Fluid shifting fromIntravascular to
intracellular esp. in the brain which is sensitive to serum
Na changes
Alteration in brain functioning
Lethargy: April 29,
2008
↓cerebralperfusion/ineffective
blood supplyto the brain
↓impulse transmission to
the muscles
Weakness: April 27-30, 2008
↓ interstitialfluid
volume
↓ interstitial
fluid volume
Dry skin: April 28-30,
2008
↓ sodium intake
↓ Iron absorption at the intestines
↓ Iron available to the tissues (red
blood cells)
Depletion of iron stores at the bone marrow to
compensate for decreased availability
Impaired hemoglobin and red blood cell synthesis
Decrease circulating red
blood cell along with its hemoglobin
Delayed biochemical mediation
Development of wound
Enlargement of wound, turning red, firm and swollen
Development of a single, red, swollen firm furuncle (approx. 3cm diameter, located at the left upper arm) draining purulent
secretions: April 27-30, 2008
Pallor: April 28-30, 2008
Fatigue - April 27-30, 2008
Shortness of breath, tachypnea (April 27, 2008)
Decreased oxyen supply to the body
Increased need for the heart to pump more blood to meet oxygen demand
Decrease in hemoglobin: 95
g/l: April 27, 2008
↓organ perfusi
on
Dry skin:
April
28-30,
Modifiable Factor:-Insect bite
↑Biochemical mediation through ↑ blood flow

b. Synthesis of the Disease
b.1 Hypertension
b.1.1 Definition
Hypertension is defined as systolic pressure greater than 140 mmHg
and a diastolic pressure greater thank 90 mmHg based on the average of two
or more accurate blood pressure measurements taken during two or more
contacts with a health care provider. Blood pressure of less than 120/80
mmHg diastolic as normal, 120 to 129/80 to 89 mmHg as pre-hypertension,
and 140/90 mmHg or higher as hypertension. (Bare, B. et. al. , 2008)
High blood pressure or hypertension means high pressure (tension) in
the arteries. Arteries are vessels that carry blood from the pumping heart to
all the tissues and organs of the body. High blood pressure does not mean
excessive emotional tension, although emotional tension and stress can
temporarily increase blood pressure. Normal blood pressure is below 120/80;
blood pressure between 120/80 and 139/89 is called "pre–hypertension", and
a blood pressure of 140/90 or above is considered high. An elevation of the
systolic and/or diastolic blood pressure increases the risk of developing heart
(cardiac) disease, kidney (renal) disease, hardening of the arteries
(atherosclerosis or arteriosclerosis), eye damage, and stroke (brain damage).
These complications of hypertension are often referred to as end–organ
damage because damage to these organs is the end result of chronic (long
duration) high blood pressure. For that reason, the diagnosis of high blood
pressure is important so efforts can be made to normalize blood pressure and
prevent complications.
b.1.2 Non-modifiable and Modifiable Risk Factors
***factors specific to the patient are highlighted
Non-modifiable Risk Factors:
Age – 35 years and older
Gender – men and post-menopausal women
Race – black and brown race
Family history of hypertension
Modifiable Risk Factors:
Alcohol use
Excess dietary sodium
Lack of exercise
Stress
Obesity
Diabetes
Kidney disease
Hormonal disorders
Porphyria
History of high blood pressure
during pregnancy
Toxemia of pregnancy
Oral Contraceptives (Birth Control
Pills)
Steroids
Nonsteroidal anti-inflammatory
drugs
Decongestants
Diet pills
Antidepressants
b.1.3 Signs and Symptoms, Complications with Rationale
***factors specific to the patient are highlighted
high blood pressure – due to vasoconstriction and increase in circulating
fluid (↑BP: 170/100 mmHg: April 27, 2008; 150/90mmHg: April 28,
2008, 140/100 mmHg: April 29, 2008)
retinal changes and papilledemea (swelling of the optic disk) –due to
increased pressure exerted by the walls of the vessels supplying the
eye and increased intraocular pressure related to cranial nerve II
affectation
increased blood urea nitrogen (93mg/dl: April 29, 2008) and serum
creatinine levels – due to poor oragn (kidney) perfusion which alters
renal processes and causes destruction and release of substances (i.e.
creatinine)
left ventricular hypertrophy – may occur in response to increased
workload placed on the ventricle as it tries to contract against higher
systemic pressure
cerebrovascular involvement which may be manifested by dizziness,
headache and impaired level of consciousness – related to ineffective
blood supply to the brain which causes impairment in the functioning
of brain structures
impairment in organ function – occurs to the organs being supplied by the
narrowed vessels; takes place due to decreased perfusion brought
about by narrowed arteries
b.2 Diabetes Mellitus
b.2.1 Definition
Diabetes mellitus type 2 (diabetes mellitus type II, non insulin-
dependent diabetes (NIDDM), obesity related diabetes, or adult-onset
diabetes) is a metabolic disorder that is primarily characterized by insulin
resistance, relative insulin deficiency, and hyperglycemia. It is often managed
by engaging in exercise and modifying one's diet. It is rapidly increasing in
the developed world, and there is some evidence that this pattern will be
followed in much of the rest of the world in coming years. It is a non-ketosis
prone hyperglycemia and glucose intolerance due to defects in insulin
secretion and peripheral insulin action. DM type 2 comprises 80% of diabetic
cases.
Type 2 diabetes often goes undetected for long periods of time, since
symptoms are usually not pronounced. Insulin is produced, but it is not
enough, or it does not work properly to transport glucose through the
receptor cells. Type 2 diabetics can often be controlled with a carefully
planned diet, an exercise program, oral medication, or insulin, used as
necessary.Uncontrolled Type 2 diabetes results in hyperglycemia. Since
symptoms have an insidious onset, the patient may not recognize that there
is any difficulty. Left uncontrolled for a long period of time, Type 2 diabetics
develop more serious symptoms such as severe hyperglycemia, dehydration,
confusion, and shock. This is called “hyperglycemic hyperosmolar non-ketotic
coma.” These symptoms are most common in the elderly population and
people suffering from illness or infection.
The following are the criteria for the diagnosis of DM Type 2:
o Symptoms of diabetes (polyuria, polydipsia, weight loss) plus casual
(random) plasma glucose ≥ 200 mg/dL (11.1 mmol/L)
o Fasting plasma glucose ≥ 126 mg/dL (7.0 mmol/L) on 2 occasions
o 2 hour plasma glucose ≥ 200 mg/dL (11.1 mmol/L) during OGTT with
75 g glucose load
o LFTs, amylase, lipase - abd pain
b.2.2 Non-modifiable and Modifiable Risk Factors
***factors specific to the patient are highlighted
Non-modifiable Factors:
Age - Older than 40 years
Family history of type 2 diabetes
Hispanic, Native American, African American, Asian American, or Pacific
Islander descent, Asian
Modifiable Factors:
History of previous impaired glucose tolerance (IGT) or impaired fasting
glucose (IFG) – FBS:137 mg/dl: April 27, 2008; 117.5mg/dl: April 28,
2008
Obesity - Weight >20% of desirable body weight (true for approximately
90% of patients with type 2 diabetes)
Hypertension (>140/90 mm Hg)(↑BP: 170/100 mmHg: April 27, 2008;
150/90mmHg: April 28, 2008, 140/100 mmHg: April 29, 2008), or
dyslipidemia (high-density lipoprotein [HDL] cholesterol level <40
mg/dL or triglyceride level >150 mg/dL)
History of GDM or of delivering a baby with a birth weight of > 9 lbs
Polycystic ovarian syndrome (which results in insulin resistance)
Viruses: certain viruses may destroy beta cells
Faulty Immune System: multiple factors may cause the immune system to
destroy beta cells, such as infection
Physical Trauma: injury or trauma may destroy the ability of the pancreas
to produce insulin
Drugs: drugs used for other conditions could cause the development of
diabetes
Stress: hormones at times of stress may block the effectiveness of insulin
Pregnancy: hormones produced during pregnancy can block the
effectiveness of insulin
b.2.3 Signs and Symptoms, Complications with Rationale
Polyuria – due to excretion of excess glucose that causes more water
attraction in the urine
Polydipsia – due to the stimulation of the thirst center of the
hypothalamus brought about by intracellular dehydration
Polyphagia – due to the stimulation of the satiety center of the
hypothalamus which brought about by cellular starvation from inadequate
glucose uptake
Weight loss – due to cellular starvation from inadequate glucose uptake
Weakness – due to cellular starvation which causes decreased energy
levels (April 27-30, 2008)
Fatigue – due to cellular starvation which causes decreased energy levels
(April 27-30,2008)
Blurred vision, retinopathy – related to poor organ perfusion brough about
by sluggish blood flow
Slow-healing cuts or sores – related to poor peripheral perfusion due to
sluggish blood flow
Dry, itchy skin – related to poor organ perfusion due to sluggish blood
flow(April 28-30, 2008-manifested by dry skin)
Frequent infections – related to poor perfusion due to sluggish blood flow
thereby decreasing number and speed of readily available WBC; delay in
biochemical mediation
Hyperglycemia – related to inadequate insulin production FBS:137 mg/dl:
April 27, 2008; 117.5mg/dl: April 28, 2008
Dehydration – due to increased blood osmolarity leading to fluid shifting
from intracellular to extracellular compartment(April 28-30, 2008-
manifested by dry skin)
Confusion – related to inadequate cerebral perfusion due to sluggish blood
flow
Numbness and tingling sensation – related to poor peripheral perfusion
due to sluggish blood flow
Nephropathy, neuropathy – common to older patients – related to poor
organ perfusion due to sluggish blood flow, causing impairment in organ
function
b.3 Electrolyte Imbalance: Hyponatremia
b.3.1 Definition
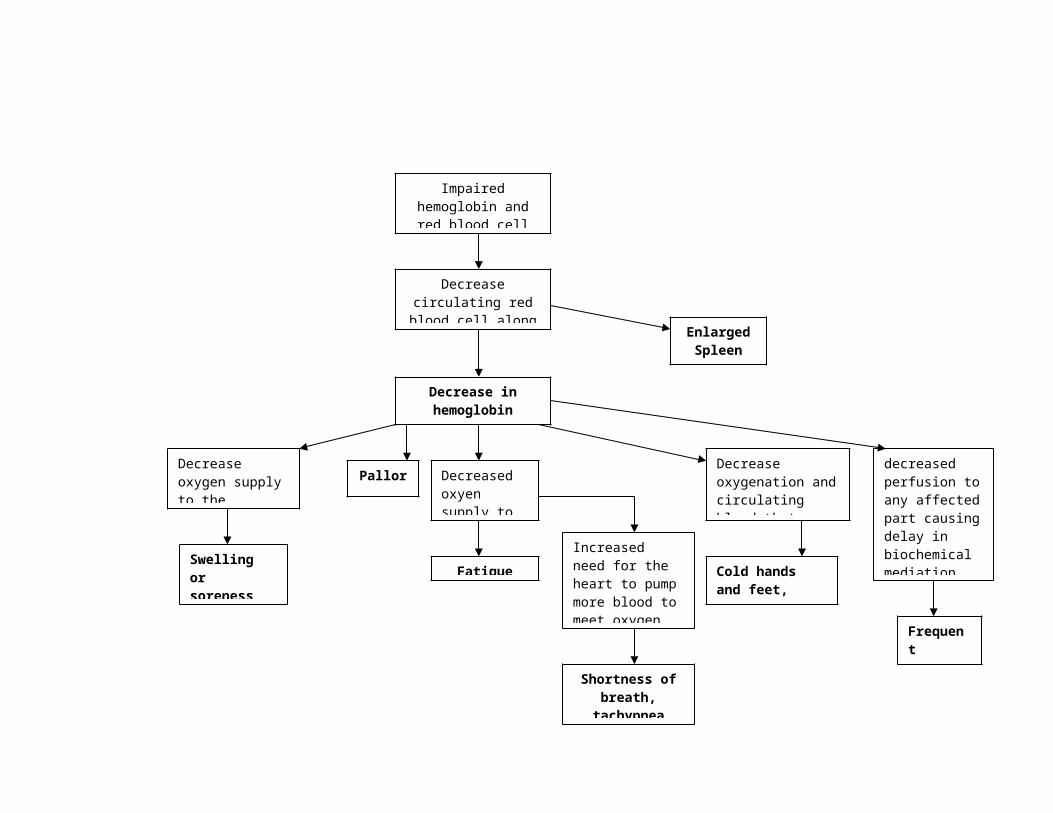
Hyponatremia refers to a serum level that is below normal (<135
mEq/l). (Bare, B. et. al. , 2008) When the blood sodium is too low, the cells
malfunction — causing swelling. In chronic hyponatremia, sodium levels drop
gradually over several days or weeks — and symptoms are typically
moderate. In acute hyponatremia, sodium levels drop rapidly — resulting in
potentially dangerous effects, such as rapid brain swelling, which can result
in coma and death.
Hyponatremia (hypervolemic) occurs when the sodium in the blood is
diluted by excess water. Hyponatremia (euvolemic, hypervolemic) may result
from medical conditions that impair excretion of water from your body, or by
a significant increase in water consumption(hypovolemic), such as by
athletes competing in marathons and other high-endurance events.
b.3.2 Non-modifiable and Modifiable Risk Factors
***factors specific to the patient are highlighted
Non-modifiable Factors:
Age. Low blood sodium is more common in older adults. This is due to
age-related change s and increased prevalence of chronic disease that
may impair the body's normal sodium balance.
Sex. Hyponatremia is more common in women than in men.
Non-modifiable Factors:
Diet. Patient may be at an increased risk of hyponatremia if following a
low-sodium diet, especially if combined with diuretic intake.
Intensive physical activities. People who take part in marathons,
ultramarathons, triathlons and other long-distance, high-intensity
activities are at an increased risk of hyponatremia.
Climate. Not being acclimated to hot weather can increase the amount of
sodium you lose through sweating during exercise.
Conditions that impair the body's water excretion. Medical conditions that
may increase your risk of hyponatremia include kidney disease, syndrome
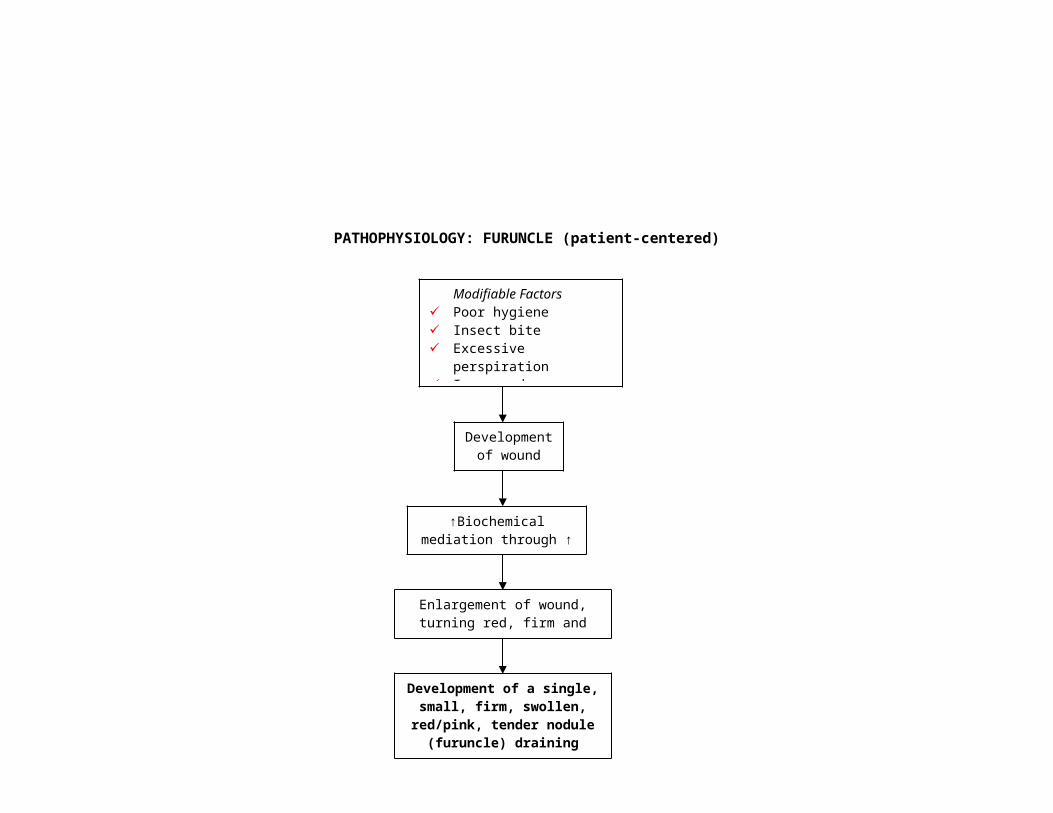
of inappropriate anti-diuretic hormone (SIADH) and heart failure, and
other chronic diseases that cause organ failure.
b.3.3 Signs and Symptoms, Complications with Rationale
Serum sodium level that is below normal (<135 mEq/l): 113.4 meQ/l:April
27
Neurologic manifestations such as headache, lethargy (April 29, 2008),
confusion, apprehension – due to fluid shifting from intravascular to
intracellular space in an attempt to raise the proportion of Na with water
Decreased BP, orthostatic hypotension – due to decreased vascular
volume secondary to water and sodium loss
Tachycardia – compensatory response which is a direct result of triggering
sympathetic catecholamine
Sympathetic responses of the heart – due to stimulation of
chemoreceptors on the aortic and carotid bodies
Crackles in the lungs – due to fluid shifting to the pulmonary alveoli
secondary to increased pressure of circulating fluids in the pulmonary
capillaries
Greater blood volume (water component>serum Na) – Hct of 0.29: April
27
Tachypnea (April 27, 2008), dyspnea, othopnea, shortness of breath – fluid
accumulation in the alveoli alters oxygen-carbon dioxide exchange
transport
Nausea, vomiting, abdominal cramping, hyperactive bowel sounds – due
to fluid shifting from intravascular to intracellular space causing an urge to
expel excess water
Dry skin (April 28-30, 2008), tongue and mucous membranes – due to
decrease in interstitial fluid caused by sodium deficit in the blood
b.4 Anemia (Iron Deficiency)
b.4.1 Definition
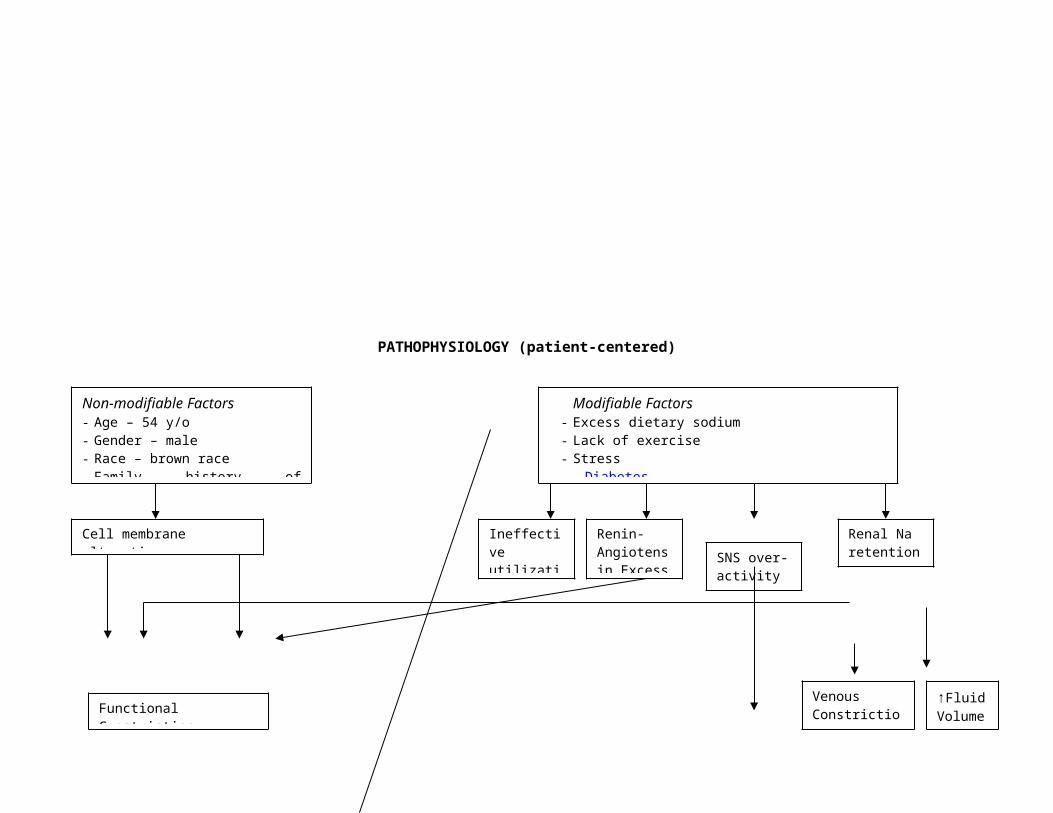
Iron-deficiency anemia typically results when the intake of dietary iron
is inadequate for hemoglobin synthesis. (Bare, B. et. al. , 2008) It is the most
common type of anemia. A lack of iron in the body can come from bleeding,
not eating enough foods that contain iron, or not absorbing enough iron from
food that is eaten. (Retieved at
http://www.nhlbi.nih.gov/health/dci/Diseases/anemia/anemia_whatis.html
accessed on May 1, 2008, 8:22 pm)
The term anemiais used for a group of conditions in which the number
of red blood cells in the blood is lower than normal, or the red blood cells do
not have enough hemoglobin. Hemoglobin—an iron-rich protein that gives
the red color to blood—carries the oxygen from the lungs to the rest of the
body. In people with anemia, the blood does not carry enough oxygen to the
rest of the body. Red blood cells also remove carbon dioxide, a waste
product, from cells and carry it to the lungs to be exhaled.
There are many types of anemia. The three major causes of anemia
are blood loss, decreased production of red blood cells, or increased
destruction of red blood cells. White blood cells and platelets are the two
other kinds of blood cells. White blood cells help fight infection. Platelets help
blood to clot. In some kinds of anemia, there are low amounts of all three
types of blood cells. The most common symptom of all types of anemia is
feeling tired because the body is not receiving enough oxygen.
In iron-deficiency anemia, the body does not have enough iron to form
hemoglobin, which means there is not enough hemoglobin to carry oxygen to
the whole body. The body gets its iron from food. The main foods that contain
iron are meat and shellfish as well as iron-fortified foods. A steady supply of
iron is needed to form hemoglobin and healthy red blood cells.
The four main causes of IDA include: Blood loss, either from disease or
injury, Not getting enough iron in the diet, Not being able to absorb the iron
in the diet. Iron-deficiency anemia also can develop when the body needs
higher levels of iron, such as during pregnancy
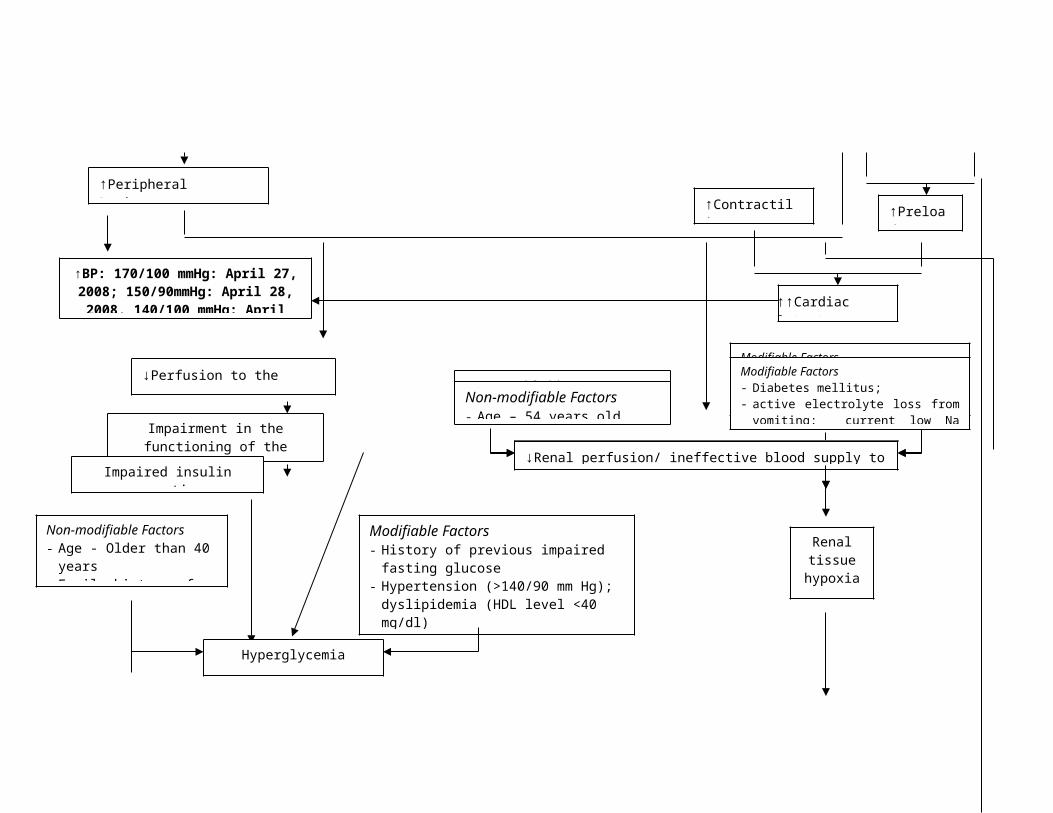
b.4.2 Non-modifiable and Modifiable Risk Factors
***factors specific to the patient are highlighted
Non-modifiable Factors:
Sex - Women - Women who lose a lot of blood during their monthly
periods are at higher risk of developing iron-deficiency anemia. About 1 in
5 women of childbearing age has iron-deficiency anemia. - Pregnant
women need twice as much iron in their diet than women who are not
pregnant. If a pregnant woman doesn't get enough iron for herself and the
growing baby, she can develop iron-deficiency anemia. About half of all
pregnant women have this type of anemia.
Age - Young Children - Infants and toddlers 6-24 months of age need a lot
of iron to grow and develop. Premature and low-birth-weight babies are at
even greater risk for iron-deficiency anemia because they don't have as
much iron stored in their bodies.
Modifiable Factors:
Diet low in iron – decreased intake of Iron-rich foods
Blood loss – causes decrease in blood volume
Other children at risk for anemia are: Children with poor nutrition,
including low-income children, Children with lead in their blood, Infants
fed cow's milk before 1 year of age, Breastfed infants older than 4 months
who are not receiving iron-rich solid foods or iron supplements
Adults With Intestinal Bleeding - Adults who bleed in their intestinal tract
are at risk for iron-deficiency anemia. This includes people who have
bleeding ulcers or colon cancer. It also includes people who use medicines
that can cause intestinal bleeding (for example, aspirin).
Other Adults - Other adults who are at risk for iron-deficiency anemia
include those who are on kidney dialysis, vegetarians, with low
socioeconomic status and older adults who have poor diets.
b.4.3 Signs and Symptoms, Complications with Rationale
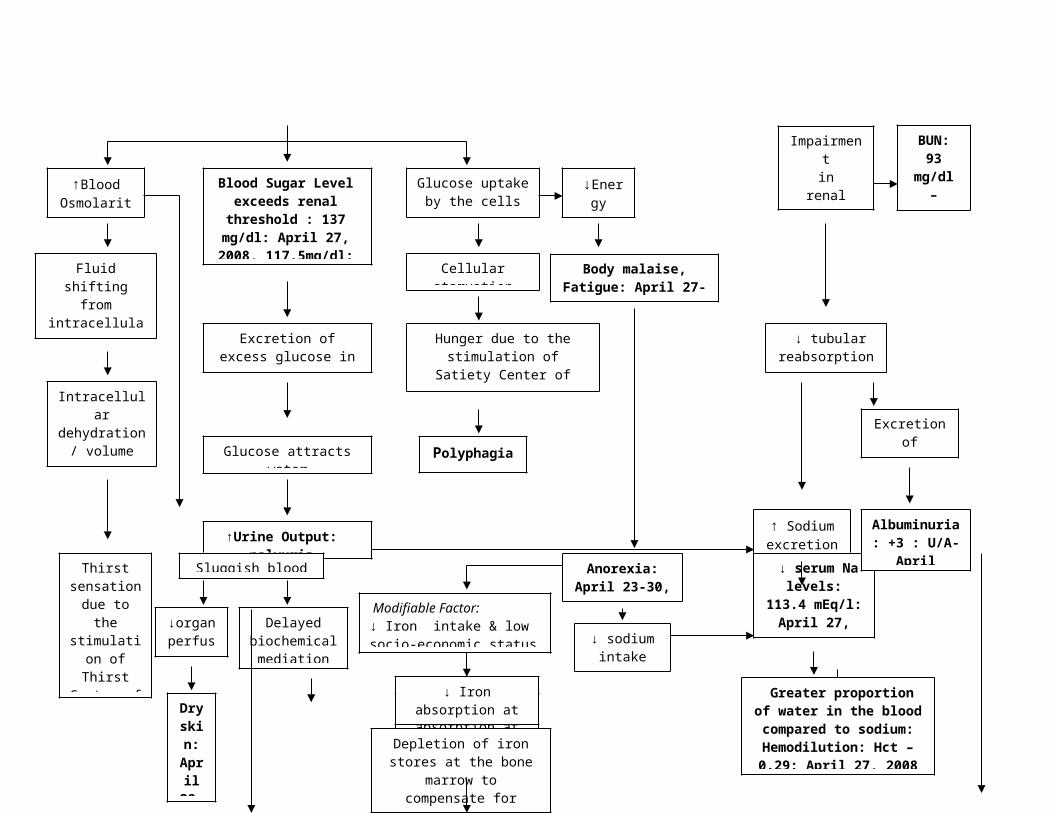
Fatigue (April 27-30, 2008) is caused by having too few red blood cells to
carry oxygen to the body. This lack of oxygen in the body can cause
people to feel weak or dizzy, have a headache, or even pass out when
changing position (for example, standing up).
Shortness of breath, tachypnea (April 27, 2008) and chest pain - Since the
heart must work harder to move the reduced amount of oxygen, signs and
symptoms may include shortness of breath and chest pain. This can lead
to a fast or irregular heartbeat or a heart murmur.
Pallor (April 28-30, 2008) - In anemia, the red blood cells don't have
enough hemoglobin. Common signs of lack of hemoglobin include pale
skin, tongue, gums, and nail beds.
Cold hands and feet as well as brittle nails – due to decrease oxygenation
and circulating blood that provides heat to the body
Swelling or soreness of the tongue and cracks in the sides of the mouth –
due to decrease oxygen supply to the integument causing easy bruising
An enlarged spleen – due to increased number of dead RBC
Frequent infections – due to compromised immune system and decreased
perfusion to any affected part causing delay in biochemical mediation
Some of the signs and symptoms of iron-deficiency anemia are related to
its causes, such as blood loss. Blood loss is most often seen with very
heavy or long lasting menstrual bleeding or vaginal bleeding in women
after menopause. Other signs of internal bleeding are bright red blood in
the stool or black, tarry-looking stools.
Decreased hemoglobin on lab exams – 95g/l: April 27, 2008
b.5 Furuncle
b.5.1 Definition
A furuncle or boil is an acute inflammation arising deep in one or more
hair follicles and spreading in the surrounding dermis. It is a deep form of
follliculitis. Furunculosis refers to multiple or recurrent lesions. Furuncles may
occur anywhere in the body but are more prevalent in areas subjected to
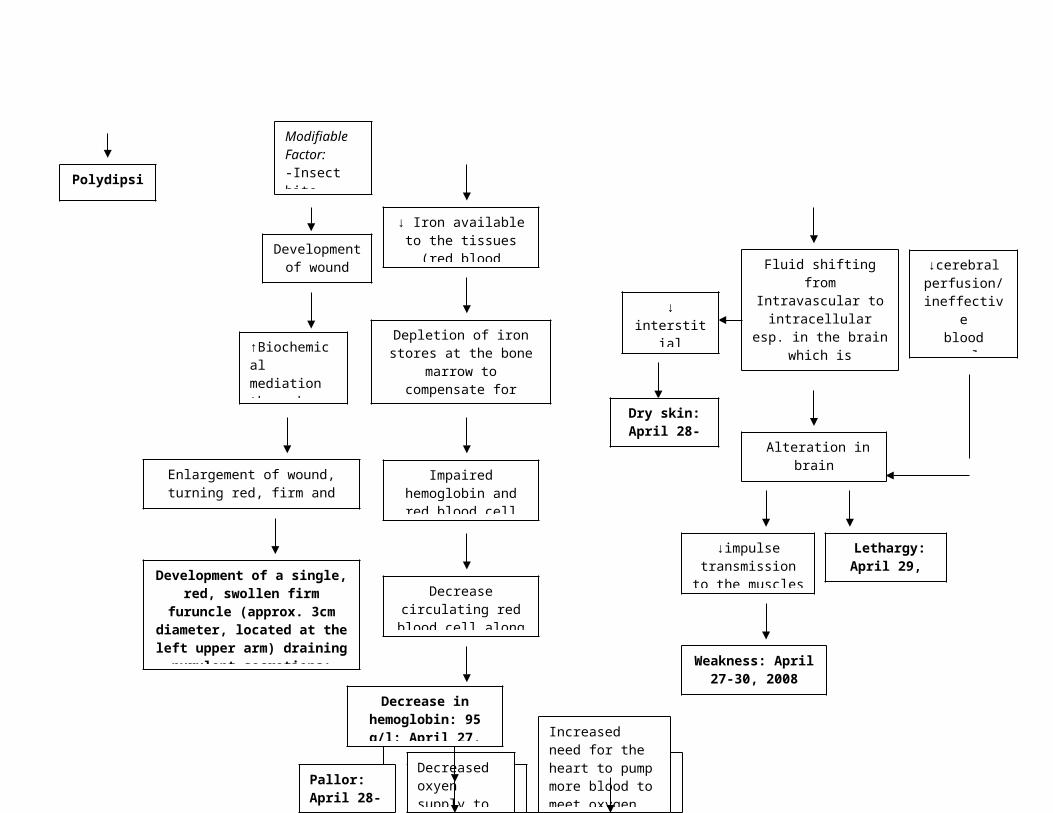
irritation, pressure, friction and excessive perspiration, such as the buttocks,
back of the neck and the axilla. (Bare, B. et. al., 2008)
A furuncle may start as a small, red, raised, painful pimple. Frequently
the infection progresses and involves the skin and subcutaneous fatty tissue,
causing tenderness, pain and surrounding cellulites. The area of redness and
induration represents and effort of the body to keep the infection localized.
The bacteria, usually staphylococci, produce necrosis of invaded tissue. The
characteristic pointing of a boil follows in a few days. When this occurs, the
character becomes yellow or black, and the boil is said to have “come to a
head.”
b.5.2 Non-modifiable and Modifiable Risk Factors
***factors specific to the patient are highlighted
Non-modifiable Factors – no particular non-modifiable factors
Modifiable Factors
Poor hygiene
Insect bite
Excessive perspiration
Increased pressure
Increased friction
b.4.3 Signs and Symptoms, Complications with Rationale
The lesions themselves are the primary symptoms:
- Small firm tender red nodule in skin (early)
- Fluctuant nodule (later)
- Located with hair follicles
- Tender, mildly to moderately painful
- May be single or multiple
- Usually pea-sized, but may be as large as a golf ball
- Swollen
- Pink or red

- May grow rapidly
- May develop white or yellow centers (pustules)
- May weep, ooze, crust
- May join together or spread to other skin areas and progress into a
carbuncle
- Decreasing pain as the area drains
The above-mentioned are characteristics of a furuncle. The furuncle is the
symptom itself. Its characteristics are changes in the site of indurations due
to biochemical mediation. Whenever there is an injury or any break in the
skin integrity, the body attempts to localize the infection by increasing blood
flow to the affected part in order to supply necessary chemicals that will aid
in controlling infection. Localized infection is generally characterized by the
following:
- Increasing pain as pus and dead tissue fills the area – due to release of
prostaglandins
- Skin redness or inflammation around the lesion
- Swollen, tender – due to increased blood flow and accumulation of
dead bacteria and WBC that engulf them
- Pink or red – due to increased blood flow

V. The Patient and His Care
A. Medical Management
a. IVFs, NGT feeding, BT, Nebulization, TPN, Oxygen therapy, etc...
Medical management or treatment
Date ordered/ Date performed:
General Description Indication(s) or purposes Client’s Reponse to the treatment
D5LRS D.O.: 04-27-0804-28-0804-29-08
D.P.:04-27-0804-28-0804-29-08
Lactated Ringer’s Injection, USP is a sterile, nonpyrogenic solution containing isotonic concentrations of electrolytes in water for injection. It is administered by intravenous infusion for parenteral replacement of extracellular losses of fluid and electrolytes
This medication is an intravenous (IV) solution used to supply water and electrolytes (e.g., calcium, potassium, sodium, chloride), either with or without calories (dextrose), to the body. It is also used as a mixing solution (diluent) for other IV medications.
The patient was supplied with adequate fluid. No adverse responses were noted.
D5NM D.O.04-30-08
D.P.04-30-08
Hypertonic solutions draw fluid
out of the intracellular and
interstitial compartments into the
vascular compartment, expanding
vascular volume.
It is a sterile, nonpyrogenic solution for fluid and electrolyte replenishment and caloric supply.
The patient was supplied with adequate fluid. No adverse responses were noted.
Nursing Responsibilities:Prior to:
1. Prepare the equipment2. Verify doctor’s order3. Use strict aseptic technique4. Explain the procedure to the S0 and give formation about the purpose of IVF to be inserted 5. Identify the client
6. Assess vital signs for baseline data7. Assess skin turgor, allergy to tape8. Check the status or veins to determine appropriate venipuncture site
During:9. Use the smallest gauge needle possible. 10.Check for patency of the tubing11.Spike the solution container12.Cleanse the fluid to be given, make sure it is the same with the prescribed fluid. 13.Partially fill the drip chamber gently with solution. 14.Select a suitable vein for venipuncture15.Dilate the vein16.Put on clean gloves and clean the venipuncture site.
After:17.Label the IVF (name, date started, number)18.Ensure appropriate infusion flow.19.Adjust the rate of fluids appropriate to the needs f the patient as ordered. If there is any question with the
flow rate ordered, check with the physician who gave the order.20.Monitor IV flow and patient’s response21.Monitor patient for evidence of IV infiltrations 22.Check for presence of air in the tubing, if air is present, remove immediately23.Check for the patency of the line always.24.Regulate and monitor the IV rate of fluid.25.Document relevant data.
b. DrugsName of Drugs: Date
ordered, performed,
Route Dosage and Frequency
Indication(s) or Purpose(s)
Client’s Response to the Treatment
Nursing Responsibilities
Generic Name:ceftriaxone
D.O.04-27-08
1g/IV q 12 Treatment of: Skin and skin structure
No adverse reaction with
1.Assess for infection (vital signs; appearance of wound, sputum, urine, and stool; WBC) at

Brand Name:Rocephin
D.P.04-27-0804-28-0804-29-0804-30-08
infections, bone and joint infections, urinary and gynecologic infections including gonorrhea, resp. tract infections, intra-abdominal inmfections, septicemia, meningitis.
Ceftriaxone was noted.
beginning of and throughout therapy.
2.IV: Monitor injection site frequently for phlebitis (pain, redness, swelling)
3.Advise patient to report signs of superinfection (furry overgrowth on the tongue, loose or foul smelling stools) and allergy.
Generic Name:Metformin
Brand Name: Fortamet
D.O.04-27-08
D.P.04-28-0804-29-0804-30-08
500mg 1 tab BID
Management of type 2 diabetes mellitus; may be used with diet, insulin, or sulfonylurea oral hypoglycemics.
The patient’s blood glucose decreased from 137 to 88 on April 28, 2008 AEB lab results (FBS/RBS).
1. Observe for signs and symptoms of hypoglycemic reactions (abdominal pain, sweating, hunger, weakness,dizziness, h/a,tremor,tachycardia,anxiety) when combined with oral sulfonylureas.
2. PO: Administer metformin with meals to minimize GI effects.
3. Explain to explain that metformin helps control hyperglycemia but does not cure diabetes. Treatment is usually long term.
Generic Name:Metoclopramide
D.O.04-27-08
1 tab TID for
Disturbances of GI motility.
No adverse reaction
1. Assess pt. for nausea, vomiting, abdominal
Brand Name:Plasil
D.P.04-28-0804-29-0804-30-08
Vomiting Nausea & vomiting of central & peripheral origin associated w/ surgery, metabolic diseases, infectious & drug-induced diseases. Facilitate small bowel intubation & radiological procedures of GIT
with Plasil was noted.
distention, and bowel sounds before and after administration.
2. PO: Administer doses 30min. before meals and at bedtime.
3. Advise pt. to avoid concurrent use of alcohol and other CNS depressants while taking this medication.
Generic Name:FeSO4
Brand Name:Feosol
D.O.04-27-08
D.P.04-28-0804-29-0804-30-08
1 tab BID Simple Fe deficiency & Fe-deficiency anemia. Patient intolerant to conventional Fe & those prone to GI upsets
The patient responded well with the medication and no adverse reaction was noted.
1. Assess nutritional status and dietary history to determine possible cause of anemia and need for patient teaching.
2. Discontinue oral iron preparations prior to parenteral administration.
3. Advise patient that stools may become dark green or black and that this change is harmless.
Generic Name:Amlodipine
Brand Name:Norvasc
D.O.04-27-08
D.P.04-28-0804-29-0804-30-08
5g 1 tab OD
Hypertension, angina, myocardial ischemia. Reduce the risk of coronary revascularizatio
The patient’s blood pressure decreased from 170/100 to
1. Monitor BP and pulse before therapy, during dose titration, and periodically during therapy.
2. PO: May be administered without regard to meals.
3. Advise pt. to take
n. 150/100 on April 28, 2008.
medication as directed, even if feeling well.
Generic Name:Clindamycin
Brand Name:Clindal
D.O.04-28-08
D.P.04-28-0804-29-0804-30-08
300 mg/tab q 12
Treatment of serious anaerobic infections esp those caused by Bacteroides fragilis. Alternative to penicillin in some severe Staph & Strep infections, including Staph osteomyelitis.
No adverse reaction with Clindamycin was noted.
1. Assess for infection (vital signs; appearance of wound, sputum, urine, and stool; WBC) at beginning of and during therapy.
2. PO: administer with a full glass of water. May be given with meals. Do not refrigerate.
3. Instruct pt. to notify HCP immediately if diarrhea, abdominal cramping, fever, or bloody stools occur and not to treat with antidiarrheals without consulting HCP.
Generic Name:Pizotifen
Brand Name:Mosegor Vita cap
D.O. 04-29-08
D.P.04-30-08
1 cap OD Underwt due to lack of appetite associated w/ vit B deficiency secondary to impaired dietary intake or absorption; nervous disorders in puberty (anorexia nervosa) old age when prevention of deficiency of B-
The patient’s appetite was enhanced as verbalized by himself.
1. May be taken with or without food (May be taken w/ meals to reduce GI discomfort.).
2. Timed-release tablets and capsules should be swallowed whole, without crushing, breaking or chewing.
3. Emphasize the importance of follow-up examinations to evaluate progress.
group vit is indicated.
Nursing Responsibilities:Prior:
1. Check the written medication order for completeness. It should include the drug name, dosage, frequency, and duration of the therapy.
2. Check if IV in.3. Check to see if there are any special circumstances surrounding administration of the dose to the patient.4. Be certain that you know the expected action, safe dosage range, special instructions for administration and
adverse effects associated with drug orders. 5. Prepare the necessary equipment.6. Wash your hands.7. Check the label on the medications three times before administering any drug.8. Prepare the dosage as ordered. 9. Explain the procedure to the patient. The action of the drug and its side effects.
During:10.Identify the patient.11.Identify if the patient expresses any doubt about the medication; always recheck the order, drug label and
dosage on the medication card.12.For oral meds do special regulation and precaution to avoid or prevent aspiration.
After:13.Following administration, be certain that the patient is comfortable, then immediately record the procedure. 14.Maintain patient’s safety15.Monitor patient for side effects16.Instruct the patient to report signs of superinfection and allergy. 17.Inspect IV insertion sites for sign of phlebitis.18.Document and assess the patient's reaction to the given drug
c. Diet
Type of Diet
Date
ordered,
date
General
Description
Indications
or Purposes
Specific
foods taken
Client’s
response
and
performed reaction to
the diet
Low Fat,
Low Salt
Diet
D.O.
04-27-08
D.P.
04-27-08
04-28-08
04-29-08
04-30-08
The low fat
and salt diet
is designed
to limit the
total
amount of
fat, salt and
cholesterol
in the diet
to reduce
serum lipid
levels and
avoid
excessive
sodium
retention
Indicated for
bed patients
whose
condition
requires
modified
diet in order
to prevent
further
aggravation
of condition.
Low salt and
low fat
foods.
The client complied with the
prescribed diet.
Nursing Responsibilities:
Prior to:
1. Check the doctor’s order for the type of diet prescribed
2. Explain the importance of the diet given.
3. Explain the importance of compliance to the diet given.
4. Inform dietary department on the patient’s diet
During:
5. Give appropriate foods to the patient.
6. Enumerate the foods that the patient may or may not take.
7. Emphasize strict compliance to diet
8. Reiterate diet frequently
After:
9. Document the patient’s tolerance to the diet given.
April 28, 2008
7am – 7pm shift
S>Ø
O>received supine on bed; asleep; with an ongoing IVF #1 0.9 NaCl 1L @ 550
ml level, regulated @ 30gtts/min, infusing well on right hand; appears weak;
with 3cm-diameter open wound on left upper arm, with erythematous,
inflamed surroundings, draining purulent secretions; with dry, scaly skin on
left upper arm; with difficulty hearing; (+) pallor; with cold, clammy skin;
capillary refill in 3 seconds; with VS taken and recorded as follows: T=37°C,
PR=74bpm, RR=17cpm, BP=150/90mmHg.
A>Decreased cardiac output related to decreased afterload as evidenced by
blood pressure elevation, cold, clammy skin, prolonged capillary refill >2
seconds, and pallor.
P>After 4 hours of nursing interventions, patient will display hemodynamic
stability as evidenced by decrease in blood pressure from 150/90 to
130/80mmHg.
I>Established rapport
>Assessed patient’s condition
>VS taken and recorded
>Assessed character of wound and wound drainage
>Reviewed laboratory data for any deviations from the normal range
>Assessed for capillary refill through blanch test
>Assisted in position changes
>Maintained aseptic technique during wound care
>Advised to inform health care provider should vomiting occur
>Instructed to dangle feet first before standing and walking
>Emphasized the importance of hand washing technique before and after
would cleaning
>Instructed SO on the proper and aseptic method of doing wound cleaning
>Encouraged rest periods
>Encouraged to avoid sweet, fatty and salty foods
>Seen on rounds by Dr. Delmas @ 7am with orders made and carried out
- FBS, lipid profile SGPT, SGOT, BUN, Creatinine – requested
- daily wound cleaning – done
- IVF to FF D5LRS 1 liter x 30gtts
- start Clindamycin 300mg/tab q 12 hrs – prescribed
- refer
>Monitored and regulated IVF as ordered
>Due meds given as prescribed
>Needs attended
>Refer accordingly
>Endorsed
E>Goal met; patient will displayed hemodynamic stability as evidenced by
decrease in blood pressure from 150/90 to 130/80mmHg.
_______________________________________________Kathleen Kaye D. Tobias, AUF-
SN
April 29, 2008
S>Ø
O>received lying on bed; awake, unconscious and incoherent; with an
ongoing IVF #53 D5LRS 1L @ 350 ml level, regulated @ 30gtts/min, infusing
well on right hand; appears weak, pale and lethargic; with dry skin; inflamed
3-cm-diameter furuncle with purulent secretion @ left upper arm noted; with
pale conjunctiva; vomitus noted, thick in consistency, approximately 50 cc
within the shift; with VS taken and recorded as follows: T=37.1°C,
PR=80bpm, RR=19cpm, BP=140/100mmHg.
A> Impaired Skin Integrity related to presence of inflamed 3-cm-diameter
eruption (wound) on left upper arm.
P> After 4 hours of nursing interventions, the patient will understand and
cooperate to the health teachings and interventions given.
I> Established Rapport
> Assessed condition
> Monitored and Recorded Vital Signs
> Assessed presence of cyanosis
> Assessed Skin Turgor
> Instructed on proper and aseptic wound care
> Instructed to increase fluid intake
> Instructed to eat foods rich in protein and vitamin C once DAT
>Emphasized the importance of hand washing especially before and after
wound care
>Reinforced low salt, low fat diet
>Practiced aseptic technique in wound cleaning
>Due meds given
>Regulated IVF as ordered
>Needs attended
>Refer accordingly
>Endorsed
E> Goal met. Patient cooperated in nursing interventions given and
verbalized understanding of the health teachings.
___________________________________________Kathleen Kaye D. Tobias, AUF-SN
April 30, 2008
7am – 7pm shift
S>Ø
O>received sitting on bed; awake, conscious and coherent; with an ongoing
IVF #5 D5LRS 1L @ 900 ml level, regulated @ 30gtts/min, infusing well on
right hand; appears weak; (+) pallor; with purulent secretion draining from
inflamed 3-cm-diameter furuncle @ left upper arm; with dry, scaly skin; with
vomiting 2x, vomitus is thick in consistency, yellowish color, approximately
100cc within the shift; with difficulty hearing; with pale conjunctiva; capillary
refill within 2 seconds; with VS taken and recorded as follows: T=36.2°C,
PR=73bpm, RR=20cpm, BP=110/70mmHg.
A>Risk for deficient fluid volume related to loss of fluid through normal route
(vomiting).
P>After 4 hours of nursing interventions, patient will not manifest evidences
of fluid volume deficit such as poor skin turgor, dry mucous membranes,
increased PR and temperature, and decreased BP.
I>Established rapport
>Assessed patient’s condition
>Monitored and recorded vital signs
>Determined ability to chew, swallow, taste
>Assessed skin turgor and capillary refill
>assessed body built, activity, rest level
>Reviewed laboratory results
>Auscultated bowel sounds
>Practiced aseptic technique in wound cleaning
>Promoted relaxing environment to enhance intake
>Encouraged small frequent feedings
>Reinforced low salt, low fat diet
>Instructed SO on the proper way of doing wound care
>Emphasized the importance of hand washing before and after wound care
>Seen on rounds by Dr. Bondoc @ 9:00 am with orders made and carried out
- continue meds
- D5NM 1L x 8hrs
- change dressing OD – done
- refer
>Due meds given as prescribed
>Regulated IVF as ordered
>Needs attended
>Refer according ly
>Endorsed
E>Goal met; patient did not manifest evidences of fluid volume deficit such
as poor skin turgor, dry mucous membranes, increased PR and temperature,
and decreased BP.
_______________Charmaigne Hazelyn Cruz, AUF-SN/Kathleen Kaye Tobias, AUF-
SN
VI. CLIENT’S DAILY PROGRESS CHART
1. Client’s Daily Progress Chart
April 27(Admission) April 28 April 29 April 30
Nursing Diagnosis
>
Decreased
cardiac output
related to
decreased
afterload as
evidenced by
blood pressure
elevation,
cold, clammy
skin,
prolonged
capillary refill
>2 seconds,
and pallor.
> Impaired
Skin Integrity.
> Risk for
deficient fluid
volume
related to loss
of fluid
through
normal route
(vomiting).
*
*
*
April 27 April 28 April 29 April 30
Vital Signs7am to 7pm
7pm to 7 am
7am to 7pm
7pm to 7 am
7am to 7pm
7pm to 7 am
7am to 7pm
7pm to 7 am
Temperature (degrees Celsius)
36.6 37 36.6 37.1 37.2 36.2
Pulse Rate (beats per minute)
84 74 82 80 78 73
Respiratory Rate (cycles per minute)
21 17 21 19 22 20
Blood Pressure (mmHg)170-100
150-90
140-90
140-100
110-60
110-70
Diagnostic/ Laboratory procedures
27 28 29 30FBS/RBS(70-100mg/dl) 137 88 117.5
Na (135-150 mg/dl) 113.4
K(3.5-5.2 mg/dl) 3.8
Urinalysis *
Hgb(140-180 gm/L) 95
WBC(5-10 x 10 ^9/L) 14.5
Hct.(0.40-0.54 L/L) .29
Seg. 0.90 .90
Lymph.= 0.10.10
BUN= 93(7-18 mg/dl) 93
Cholesterol= 192.5 (150-250 mg/dl) 160.7 192.5
Creatinine= 18(0.4-1.4) 18.0
HDL C=33.2(30-75) 33.2
LDL C= 145.22(66-178) 145.22
Triglycerides= 70.4 (36-165) 70.4
SGPT/ALT= 17(up to lu/ml) 17.0
SGOT/AST= 19.9(up to 40 lu/ml) 19.9
Medical Management
IVF’S 27 28 29 30
D5LRS * * *
D5NM *
April 27 April 28 April 29 April 30MEDICATIO
NS7am-7pm
7pm-7am
7am-7pm
7pm-7am
7am-7pm
7pm-7am
7am-7pm
7pm-7am
Ceftriaxone 1g/IV q 12
* * * * * *
Metformin 500mg 1 tab BID
* * * * *
Plasil tab TID for Vomiting
* * * *
FeSO4 tab BID
* * * * *
Amlodipine 5g 1 tab OD
* * *
Clindamycin 300 mg/tab q 12
* * * * *
Mosegor Vita cap
*
Diet am pm am pm am pm am pm
Low fat, low salt
* * * * * *
Conclusion:
The Groups’ Goal in this study is to at least help the patient deal with
the situation in order to prevent further complications and gain cooperation
with the nurses and to somewhat help in stabilizing and improve the patient’s
health and well-being because the patient is still responsible in achieving his
health goal. Many Interventions were done according to the level of
knowledge and understanding of the student nurses about the diseases he is
afflicting right now in order to meet the said Goal. Through constant
monitoring of his Vital Signs, laboratory results and checking the patient’s
Daily Progress chart, the Group was able to identify if their Goals were
achieved. During the first day of handling the patient, his vital signs were
monitored and blood pressure appeared to be elevated and at the same time
he feels weak. Vital signs were normal during the second day except for the
blood pressure same with the third day. On the last day that the group
handled the patient, Vital Signs were normal and the patient was still
appeared weak, pale and lethargic. Medications were given on time at the
desired dose. Other records such as laboratory results show that there are
still complications particularly the Random Blood Sugar, however, some
laboratory findings show within normal range. The Goal was not totally met
because there are still abnormalities presented during the first until the last
day that the group handled him though he is cooperative when it comes to
medical regimen.
VIII. BIBLIOGRAPHY
Bare, B. et. al. (2008). Brunner and Suddarth’s Textbook of Medical-Surgical Nursing. Philadelphia:Lippincott-Williams & Wilkins
Deglin, J. and Velerand, A. (2007). Davis’s Drug Guide for Nurses. Pensylvania: E.A. Davis Company.
Doenges, Marilynn E. Nursing Care Plans: Guidelines for Planning Patient Care
Seely, R., Stephens, T., Tate, P. (2005). Essentials of Human Anatomy & Physiology. New York: McGrw-Hill.
Wolff L: Fundamentals of Nursing, 7 th edition , JB Lippincott Co.
Retrieved at http://www.medicinenet.com/high_blood_pressure/article.htm accessed on April 29, 2008 at 5:30 pm
Retrieved at http://www.emedicinehealth.com/anatomy_of_the_endocrine_system/article_em.htm accessed on April 29, 2008 9:37 pm
Retrieved at http://en.wikipedia.org/wiki/Diabetes_mellitus_type_2 accessed on April 29, 2008 9:37 pm
Retrieved at http://www.nurseslearning.com/courses/nrp/NRP1605/course/diabetes.pdf accessed on April 30, 2008 at 7:05 pm
Retrieved at http://webpages.charter.net/saabrio/ENDO_Diabetes_mellitus.htm, accessed on April 30, 2008 at 7:05 pm
Retieved at http://www.nhlbi.nih.gov/health/dci/Diseases/anemia/anemia_whatis.html accessed on May 1, 2008, 8:22 pm
Retrieved at http://en.wikipedia.org/wiki/Pancreas accessed on May 2, 2008 11:03 pm
Retrieved at http://www.mayoclinic.com/health/hyponatremia/DS00974/DSECTION=1 accessed on May 2, 2008, 11:50am
Retrieved at http://health.allrefer.com/health/furuncle-symptoms.html accessed on May 2, 2008, 3:46pm
Retrieved at http://en.wikipedia.org/wiki/Diabetes_mellitus_type_2 accessed
on April 30, 2008 at 7:05 pm)
Retrieved at
http://health.discovery.com/diseasesandcond/encyclopedia/2935.html.
Retrieved
at http://webpages.charter.net/saabrio/ENDO_Diabetes_mellitus.htm ,
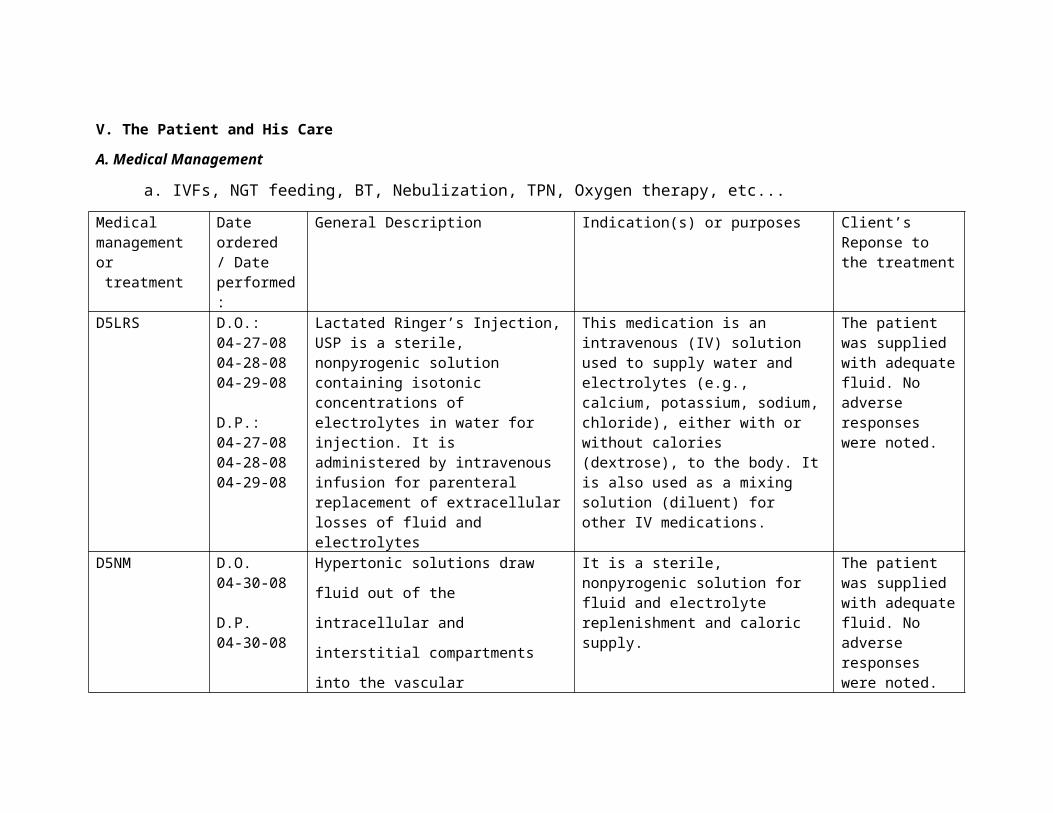
Retrieved at
http://www.mayoclinic.com/health/hyponatremia/DS00974/DSECTION=1
accessed on May 2, 2008, 11:50am)
Retrieved at http://www.medicinenet.com/high_blood_pressure/article.htm
Retrieved at
http://www.nurseslearning.com/courses/nrp/NRP1605/course/diabetes.pdf ,
ANGELES UNIVERSITY FOUNDATIONAngeles City
College of Nursing
CASE STUDY:
HYPERTENSION II
DIABETES MELLITUS TYPE II
ELECTROLYTE IMBALANCE
(HYPONATREMIA)
IRON DEFICIENCY ANEMIA
FURUNCLE