case report intracranial aspergillus fumigatus infection ... · intracranial aspergillus fumigatus...
TRANSCRIPT
Int J Clin Exp Med 2015;8(11):20524-20531www.ijcem.com /ISSN:1940-5901/IJCEM0015918
Case ReportIntracranial aspergillus fumigatus infection complicated with cavernous hemangioma: case report and literature review
Yuxue Sun*, Jinlu Yu*, Guihong Li, Haiyan Huang
Department of Neurosurgery, The First Hospital of Jilin University, Changchun 130021, P. R. China. *Equal con-tributors.
Received September 9, 2015; Accepted November 6, 2015; Epub November 15, 2015; Published November 30, 2015
Abstract: The aim of this study was to report a rare case of Aspergillus fumigatus infection complicated with cav-ernous hemangioma in the central nervous system of a patient with normal immune function and to investigate its causes. A 60-year-old male patient was admitted three years ago due to meningioma-induced convulsions. In addition to meningioma, magnetic resonance imaging (MRI) results also suggested the presence of cystic and solid lesions in the left temporal lobe, which was considered to be a brain abscess due to the infection. After antibiotic treatment, the patient underwent meningioma resection, after which no more convulsions occurred. It was recom-mended that the patient receive treatment on the abscess in the left temporal lobe, but the patient did not consent. He was discharged with follow-up. Recently, the patient returned for treatment due to intermittent headaches with weakness in the right lower extremity for 10 days. MRI results revealed that the lesion in the left temporal lobe had expanded and was associated with abnormality in the midline. Surgical lumpectomy was performed, and the postop-erative pathological examination confirmed the brain abscess to be an Aspergillus fumigatus infection complicated with cavernous hemangioma, which indirectly confirmed that the lesion in the temporal lobe three years ago was from the Aspergillus fumigatus infection. On the 7th postoperative day, the patient died due to severe pneumonia. Because the intracranial Aspergillus fumigatus infection in the patient had lasted for three years, with no cavernous hemangioma present at the first assessment but with a lesion evident three years later, the hemangioma is consid-ered to be related to the Aspergillus fumigatus infection.
Keywords: Aspergillus fumigatus, infection, cavernous hemangioma
Introduction
Aspergillus fumigatus exists in soil, plants and corrupted materials and mainly infects people with immune dysfunction, particularly organ transplant recipients and patients who have been receiving immunosuppressive agents for long periods of time and those with hematologi-cal malignancies and human immunodeficiency virus (HIV) [1]. In immunocompetent patients, Aspergillus fumigatus infection in the central nervous system is uncommon, and the report-ed cases are all isolated [2-5]. The mortality of Aspergillus fumigatus infection is extremely high [1, 6]. The infections in the central nervous system are mostly acute, and focal chronic growth in the brain is unusual, while no induced cavernous hemangioma has been reported. This paper reported a case of cavernous hem-angioma that occurred in the foci of an immu-
nocompetent patient after Aspergillus fumiga-tus infection in the left temporal lobe three years prior.
Case report
A 60-year-old male patient was admitted in our hospital due to “intermittent headache with weakness in the right lower limb”. Physical examination: muscle strength was level IV in the right lower limb, without pathological reflec-tion. And no abnormalities were seen in the rest of the nervous system. The patient had no his-tory of rheumatism connective tissue disease, or the application history of glucocorticoids. The patient had a history of tuberculosis which had been cured 10 years ago. But 3 years ago, he appeared apathetic emotion, sudden loss of consciousness and convulsion of the limbs, and went to see a doctor. Head MRI showed that:
Intracranial aspergillus fumigatus infection complicated with cavernous hemangioma
20525 Int J Clin Exp Med 2015;8(11):20524-20531
Intracranial aspergillus fumigatus infection complicated with cavernous hemangioma
20526 Int J Clin Exp Med 2015;8(11):20524-20531
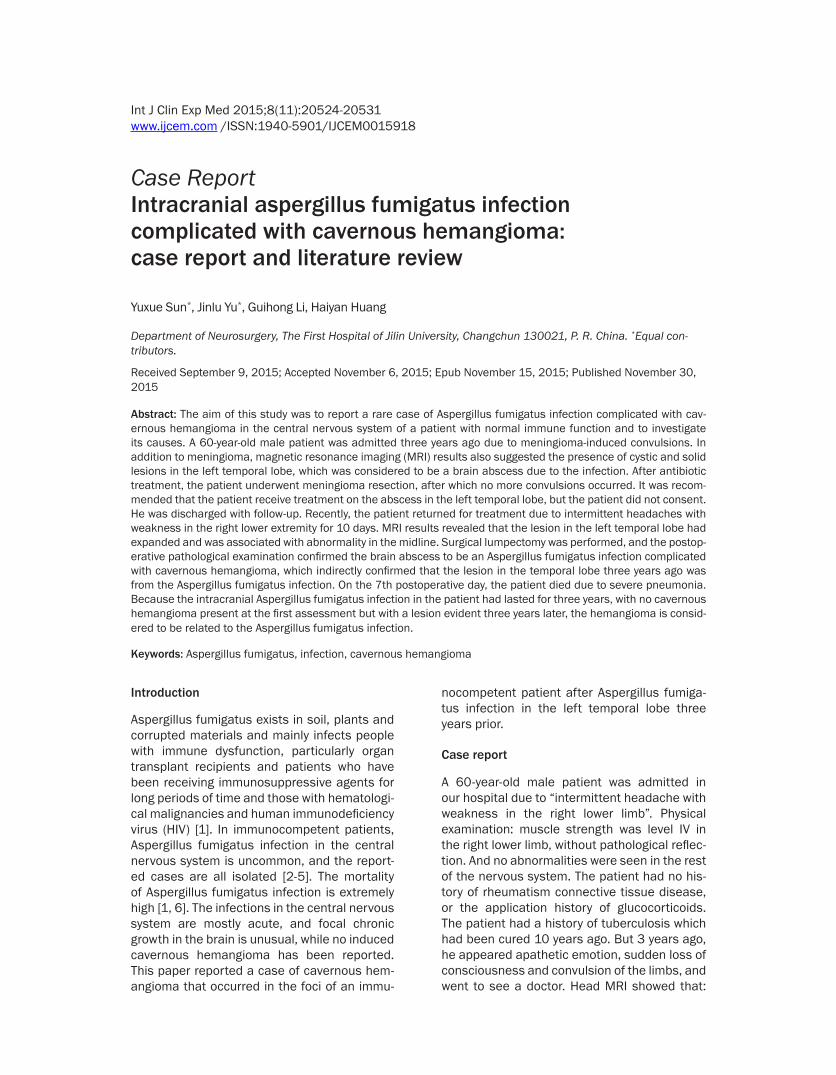
Left temporal lobe showed irregular long T1 and long T2 signal, while fat-suppression and water-suppression phases of low signal. It is about 4.0 cm×4.0 cm. The septum was seen inside. Patchy long T1 and long T2 signals were seen around, with mass reinforcement lesion inside (Figure 1A-D). Abnormal signals of oval equal T1 and equal T2 were seen in longitudinal division next to frontal cerebral falx. It was about 2.8 cm×2.8 cm. The reinforcement was uniformed (Figure 1A and 1D). There were no abnormal signals in nose sinus (Figure 1E). Chest anteroposterior X film: No irregular funic-ular and calcification density was seen in upper lobe of double lungs, and the diagnosis was obsolete pulmonary tuberculosis (Figure 1F). Laboratory examination: routine blood: the wh- ite blood cells for 6.96×109/L (normal: 4-10× 109/L), neutrophil percentage for 0.59 (normal: 0.4-0.6), lymphocyte percentage for 0.3 (nor-mal: 0.2-0.4), monocyte percentage for 0.05 (normal: 0.03-0.08×109/L), eosinophil percent-
age for 0.06 (normal: 0.005-0.05), basophil percentage for 0.00 (normal: 0.00-0.01), neu-trophils for 4.08×109/L (2-7×109/L), lympho-cyte for 2.1×109/L (0.8-4.0×109/L), monocytes for 0.34×109/L (0.12-0.8×109/L), eosinophils for 0.42×109/L (0.02-0.50×109/L), basophils for 0.02×109/L (0.00-0.10x109/L), HIV (-) and HBSag (-). The admission diagnosis was frontal meningioma and left temporal brain abscess-es. EEG was used for epilepsy positioning: dis-playing the epilepsy lesion was located in the forehead. The patient was given antibiotics tr- eatment, and then given resection of meningio-ma. No seizure was seen in postoperative peri-od. MRI was reviewed. The lesion did not disap-pear in left temporal lobe. Selective surgical treatment was informed to the patient. But the patient was not agreed; he was discharged fr- om the hospital and followed up.
Ten days before admission, the patient expe- rienced intermittent headaches and right leg
Figure 1. Imaging findings three years ago. A-C. Head MRI image: irregular mixed signal in the left temporal lobe showing an annular enhanced signal of a lesion in the temporal lobe (red arrow); D. T2-weighted signal of the lesion in a frontal image, with homogeneous enhancement after enhancement (white arrows); E. No abnormal signal in sinuses in T1-weighted imaging; F. Anteroposterior chest X-ray: old tuberculosis lesions in both upper lobes of the lung (black arrow).
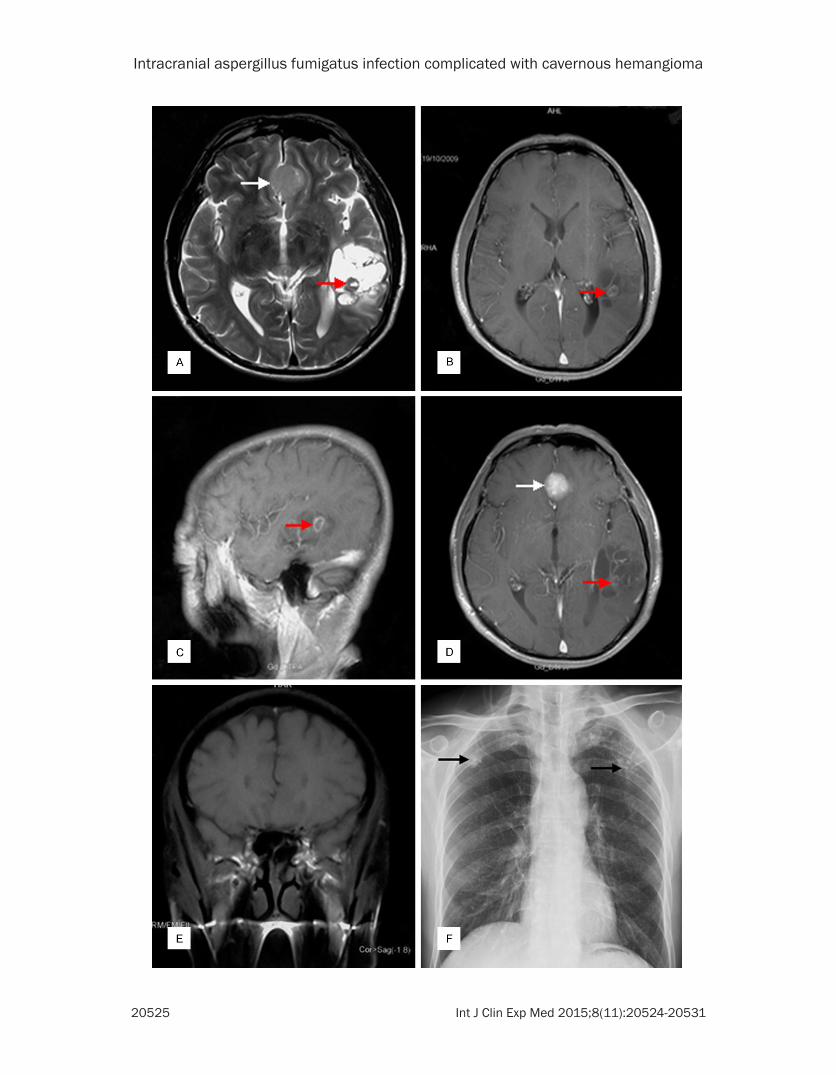
Figure 2. The head MRI image from the more recent admission. A. Sagittal T2 phase: the front lesion exhibited high signal mixed with low signal, with a surrounding annular low signal (white arrow); the rear lesion exhibited a mixture of high signal and other signals (red arrows). B. Enhanced axial T1 phase: the front lesion showed heterogeneous enhancement (white arrow), while the rear lesion showed annular cyst wall enhancement (red arrow). (Note: The pathological results confirmed that the front lesion was a cavernous hemangioma and that the rear lesion was an abscess of Aspergillus fumigatus infection).
Intracranial aspergillus fumigatus infection complicated with cavernous hemangioma
20527 Int J Clin Exp Med 2015;8(11):20524-20531
weakness. A magnetic resonance imaging (MRI) study of the head showed that the ab- scess in the left temporal lobe had expanded and that the left ventricle was compressed and narrowed, with the midline slightly shifted to the right. The lesion consisted of both front and rear portions. The size of the front lesion was approximately 3.5 cm×2.5 cm×4.0 cm, and the size of the rear lesion was approximately 1.7 cm×1.5 cm×0.8 cm. An enhanced scan showed heterogeneous enhancement in the front lesion (Figure 2A) and peripheral enhancement in the
rear lesion (Figure 2B). A brain abscess of the left temporal lobe was diagnosed, and surgical treatment was provided.
The surgery was conducted using a left tempo-ral approach. The front lesion was observed at approximately 3 cm subcortical and was red-dish-brown, with a slightly soft texture and a rich blood supply. The lesion was partially ad- hered to the brain tissue. The lesion was com-pletely removed, the rear lesion was soft and did not have a rich blood supply. Postoperative
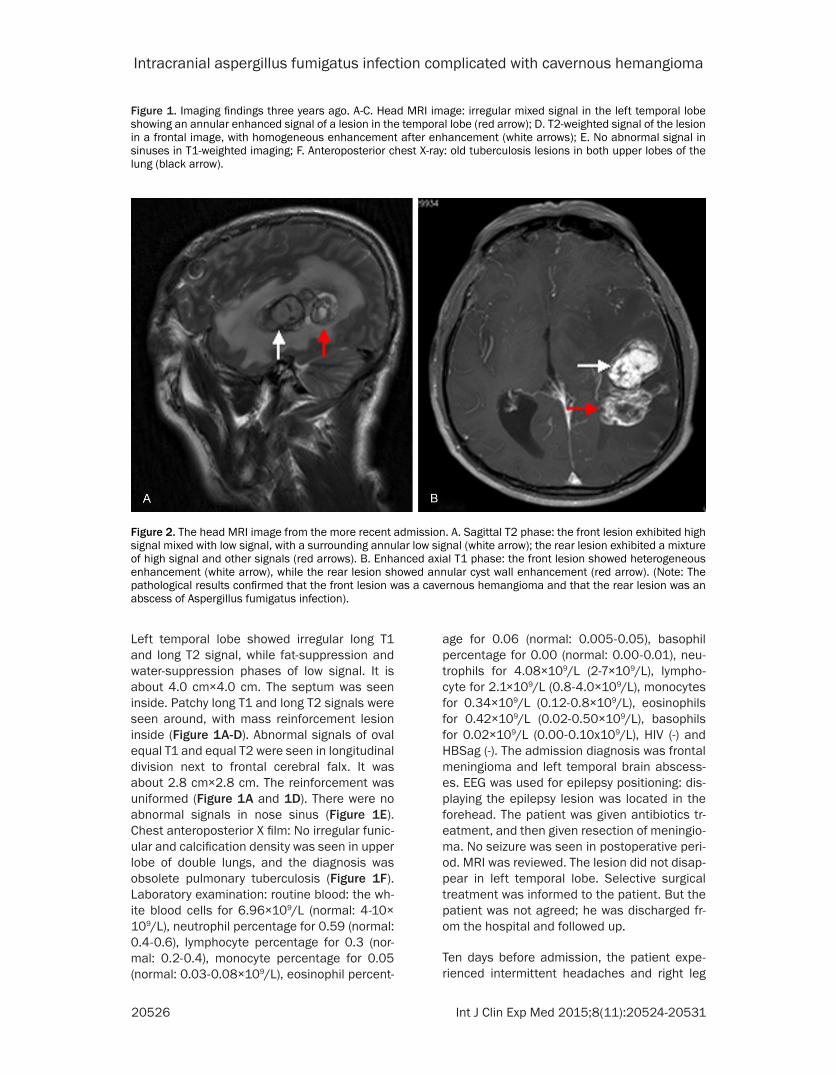
Figure 3. Pathology of the cavernous hemangioma and Aspergillus fumigatus infection. A. The cavernous hemangioma by hematoxylin and eosin (HE) stain-ing, ×200: cavernous sinuses of different sizes were present, and the structure lacked the muscular layer and elastic fibers (white arrows), with a little connec-tive tissue between the vessels. B. The Aspergillus fu-migatus infection by CD34 staining, ×400, and C. The Aspergillus fumigatus infection by HE staining ×200: fungal spores were observed, with the hyphal heads of Aspergillus fumigatus bifurcated at acute angles (black arrow). D. PAS staining (+), ×200, of the hy-phal heads of Aspergillus fumigatus (black arrows); E. VEGF staining (-), ×400, of the Aspergillus fumiga-tus and the surrounding brain tissue.

Intracranial aspergillus fumigatus infection complicated with cavernous hemangioma
20528 Int J Clin Exp Med 2015;8(11):20524-20531
computed tomography (CT) showed mixed sig-nals with high density in the surgical area, which was considered to be hemorrhage. Not much evidence of hemorrhage was found in the surgical area, and conservative treatment was provided. The pathological diagnosis was as follows: the front lesion was a cavernous hem-angioma with hemorrhage, infarction and orga-nization, while the dissection surface was mo- stly red-brown, solid and soft, reminiscent of blood clotting. The rear lesion was an abscess of an Aspergillus fumigatus infection; the dis-section surface was light brown, solid and soft. The cavernous hemangioma consisted of dif-ferent sizes of cavernous sinus and lacked the muscular layer and elastic fibers, with a little connective tissue between the vessels (Figure 3A) and the focal hematoma; fungal spores were observed in the abscess of Aspergillus fumigatus infection, with the hyphal heads bi- furcated at acute angles (Figure 3B, 3C). Pe- riodic acid-Schiff staining (PAS) for the indica-tive hyphae of Aspergillus fumigatus infection was positive (Figure 3D). The postoperative sit-uation of the patient was poor, and treatment consisting of voriconazole 200 mg, twice a day, was provided to the patient. Additionally, broad-spectrum antibiotics with Ceftezole Sodium was administered to the patient as a symptom-atic and supportive treatment to prevent infec-tion, but the patient died due to severe pneu-monia on the 7th day after surgery.
Discussion
Aspergillus fumigatus is widely present in air, soil and organic matter [7]. Many spores might be inhaled into our lungs every day, but these spores will be cleared by the immune system [8]. Aspergillus fumigatus infection is rare in the immunocompetent population [4, 9-14]. The literature has reported three cases of infec-tion that have occurred in patients with pulmo-nary tuberculosis [9-11] and one case of ulcer-ated lesions in the gastric wall [12]. Cases occurring in the nervous system are uncom-mon, with one reported case of hematogenous infection from the lung to the brain [15]. Other cases of central nervous system infections were mostly caused by the direct invasion of iatrogenic infections and adjacent infected tis-sue. The infections of Aspergillus fumigatus are usually asymptomatic and can be hidden in the lungs [6, 16]. The intracranial lesion of Asper- gillus fumigatus infection present in the patient
in this study had been identified by MRI in the surgery performed three years ago, and the patient had a history of pulmonary tuberculo-sis. These findings suggested that the tubercu-losis caused damage to the lung defensive bar-rier; thus, Aspergillus fumigatus had a high chance to cause a pulmonary hematogenous infection in the central nervous system.
The early manifestation of disease after As- pergillus fumigatus infection is inflammatory changes in the brain. An edema with ill-defined boundaries is generated in the brain tissue. Whether this edema is converted to a brain abscess depends on the immune status of the host [17]. For people with normal immune func-tions, a small amount of Aspergillus fumigatus can be killed in the brain. If the afflicted indi-vidual’s immune system functions poorly, the central nervous system can be infected with an acute onset infection. While growth in the brain for three years is rare, the findings of this study suggest that the body’s immunity and the Aspergillus fumigatus infection reached a state of equilibrium. Aspergillus fumigatus can rele- ase substances that are highly toxic to astro-cytes, microglia and neurons that can cause irreversible damage to these cell types at low concentrations and over a short period of time, thereby reducing the killing and defense effects of the brain tissue against Aspergillus fumiga-tus [18]. Aspergillus fumigatus has exhibited an obvious tendency to invade the arteries and veins, causing necrotizing vasculitis, secondary thrombosis and hemorrhage [2]. Masses of Aspergillus fumigatus are surrounded by many blood vessels, and the resulting erosion of the blood vessels might cause injury to the periph-eral brain tissue and thus reduce its killing effect on Aspergillus fumigatus. Therefore, the long-term survival of Aspergillus fumigatus in the brain of the patient of this study was the co-result of the weakened killing effect of the damaged brain tissue and the toxicity of As- pergillus fumigatus. However, with the growth of the fungus, its toxic secretions increased, causing huge amounts of damage in the sur-rounding astrocytes in the brain. Ultimately, the patient’s immune system could not contain the Aspergillus fumigatus, leading to the significant symptoms and disease indicative of brain da- mage.
The patient in this report was not only infected with Aspergillus fumigatus but also had a com-

Intracranial aspergillus fumigatus infection complicated with cavernous hemangioma
20529 Int J Clin Exp Med 2015;8(11):20524-20531
plicated cavernous hemangioma in the infec-tion region whose causes are unknown and that not been previously reported. Cavernous hemangiomas are divided into two categories: familial and sporadic. The familial hemangio-mas follow the rules of autosomal dominant inheritance and exhibit the common mutations CCM1, CCM2, and CCM3; however, sporadic hemangiomas do not possess these mutations [19]. Thus, the occurrence of a cavernous hem-angioma might be related to the undetected mutations or might be caused by external fac-tors that are not yet well understood. Recent studies have found that radiotherapy can cause the occurrence of cavernous hemangiomas [20-24]. Radiotherapy can up-regulate vascular endothelial growth factor (VEGF) expression in astrocytes [25], and increased VEGF expres-sion can cause endothelial cell proliferation, which results in the formation of the lumen of a cavernous hemangioma [21, 26]. The patient described in this report presented with intra-cranial Aspergillus fumigatus infection. Asper- gillus fumigatus hyphae and culture medium extract have significant serine protease activity [27]. Serine proteases can release a variety of growth factors and can increase the expression of adhesion molecules; thus, these proteases can play a significant role in angiogenesis [28]. The MRI of the patient three years ago revealed that the masses of Aspergillus fumigatus were surrounded by many blood vessels. Aspergillus fumigatus shows an obvious tendency to invade the arteries and veins, causing necrotizing vas-culitis, secondary thrombosis and hemorrhage [2] and providing the conditions for Aspergillus fumigatus-mediated vascular invasion and da- maged vascular proliferation. Studies have also shown that VEGF expression in cavernous hem-angiomas is significantly increased [26, 29]. The VEGF staining for Aspergillus fumigatus and its surrounding brain tissue showed no VEGF expression, indicating the death of a large number of glial cells (Figure 3E). These findings might be related to the toxic effects of As- pergillus fumigatus causing the destruction of the surrounding tissue: necrotic brain tissue surrounding the lesion might be the reason for the failure to detect VEGF expression in this case. However, we still could not rule out the possibility that the occurrence of Aspergillus fumigatus infection complicated with cavern-ous hemangioma in this patient was due to the release of substances with serine protease
activity by Aspergillus fumigatus, which would result in increased VEGF expression and endo-thelial cell proliferation. The long presence and repeated stimulation of Aspergillus fumigatus led to the formation of a cavernous hema- ngioma.
The MRI findings of the cavernous hemangioma in this patient were not typical, with rich blood vessels and MRI contrast enhancement, which were different from the signs of a common cav-ernous hemangioma. Common intracranial cav-ernous hemangiomas are usually not enhanced, instead possessing a typical peripheral hemo-siderin belt. The atypical findings of the cavern-ous hemangioma in this case might be related to its accompanying hemorrhage, infarction and organization. It has been reported that the MRI findings of a cavernous hemangioma out-side of the brain can be enhanced [30, 31], though cavernous hemangiomas in the central nervous system after radiotherapy have exhib-ited different manifestations. MRI enhance-ment can appear, and both uneven enhance-ment and no enhancement have been observed [20, 21, 32]. Considering the possible atypical MRI manifestations of a cavernous hemangio-ma, the result of enhancement could be related to the completeness of the blood-brain barrier. The patient in this report was associated with Aspergillus fumigatus infection, and increased VEGF expression could stimulate angiogenesis, leading to a rich blood supply for the cavernous hemangioma. At the same time, the Aspergillus fumigatus was vascular invasive, causing dam-age to the blood-brain barrier and resulting in atypical manifestations of cavernous hemangi-oma with contrast enhancement. For the treat-ment of Aspergillus fumigatus, voriconazole is effective in treating aspergillosis, and its effi-cacy is superior to that of amphotericin [33]. For patients with severe immune dysfunction, voriconazole could improve the cure rate of Aspergillus fumigatus infections [34]. The mor-tality of intracranial Aspergillus infection under-going surgical treatment is much lower than that of drug treatment only, confirming the important role of surgery in the treatment of Aspergillus fumigatus infection [1]. The patient in this report underwent surgery followed by voriconazole therapy and died on the seventh postoperative day due to severe pneumonia, which might be related to the impairment of the mechanical defensive barrier in the lung and surgical stress in the patient.

Intracranial aspergillus fumigatus infection complicated with cavernous hemangioma
20530 Int J Clin Exp Med 2015;8(11):20524-20531
Conclusions
Aspergillus fumigatus is an opportunistic patho-gen. The impairment of the mechanical defen-sive barrier could increase the chance of As- pergillus fumigatus infection. When an individu-al’s immune function is depressed, Aspergillus fumigatus can spread to the central nervous system through the blood and grow. The long-term colonization of Aspergillus fumigatus in the brain can then stimulate angiogenesis to form a cavernous hemangioma. For immuno-competent patients with Aspergillus fumigatus infection in the central nervous system, surgery combined with drug therapy has good efficacy and should be provided at an early disease stage. Postoperative complications should be prevented for patients with impaired mechani-cal defense barriers.
Disclosure of conflict of interest
None.
Address correspondence to: Haiyan Huang, Depart- ment of Neurosurgery, First Hospital of Jilin Uni- versity, 71 Xinmin Avenue, Changchun 130021, Jilin, P. R. China. E-mail: [email protected]
References
[1] Kourkoumpetis TK, Desalermos A, Muhammed M and Mylonakis E. Central nervous system aspergillosis: a series of 14 cases from a gen-eral hospital and review of 123 cases from the literature. Medicine (Baltimore) 2012; 91: 328-336.
[2] Gervas J and Kovacs FM. Index case for the fungal meningitis outbreak, United States. N Engl J Med 2013; 368: 970.
[3] Kose S, Cavdar G, Senger SS and Akkoclu G. Central nervous system aspergillosis in an im-munocompetent patient. J Infect Dev Ctries 2011; 5: 313-315.
[4] Saini J, Gupta AK, Jolapara MB, Chatterjee S, Pendharkar HS, Kesavadas C and Radhakrish-nan VV. Imaging findings in intracranial asper-gillus infection in immunocompetent patients. World Neurosurg 2010; 74: 661-670.
[5] Narayan SK, Kumar K, Swaminathan RP, Roo- peshkumar VR and Bhavna B. Isolated cere-bral aspergilloma in a young immunocompe-tent patient. Pract Neurol 2009; 9: 166-168.
[6] Patterson TF, Kirkpatrick WR, White M, Hie- menz JW, Wingard JR, Dupont B, Rinaldi MG, Stevens DA and Graybill JR. Invasive aspergil-losis. Disease spectrum, treatment practices, and outcomes. I3 Aspergillus Study Group. Medicine (Baltimore) 2000; 79: 250-260.
[7] Denning DW. Invasive aspergillosis. Clin Infect Dis 1998; 26: 781-803; quiz 804-785.
[8] Latgé JP. Aspergillus fumigatus and Aspergillo-sis. Clin Microbiol Rev 1999; 12: 310-350.
[9] Pornsuriyasak P, Murgu S and Colt H. Pseu- domembranous aspergillus tracheobronchitis superimposed on post-tuberculosis tracheal stenosis. Respirology 2009; 14: 144-147.
[10] Pathak V, Hurtado Rendon IS and Ciubotaru RL. Invasive pulmonary aspergillosis in an im-munocompetent patient. Respiratory Medicine CME 2011; 4: 105-106.
[11] Chien WL and Tseng JS. Pulmonary aspergillo-sis in an immunocompetent patient. Braz J In-fect Dis 2013; 17: 375-376.
[12] Karaman I, Karaman A, Boduroglu EC, Erdo-gan D and Tanir G. Invasive Aspergillus infec-tion localized to the gastric wall: report of a case. Surg Today 2013; 43: 682-684.
[13] Genzen JR and Kenney B. Central nervous sys-tem Aspergillus infection after epidural anal- gesia: diagnosis, therapeutic challenges, and literature review. Diagn Microbiol Infect Dis 2009; 65: 312-318.
[14] Marinovic T, Skrlin J, Vilendecic M, Rotim K and Grahovac G. Multiple Aspergillus brain absc- esses in immuno-competent patient with se-vere cranio-facial trauma. Acta Neurochir (Wi- en) 2007; 149: 629-632; discussion 632.
[15] Elgamal EA and Murshid WR. Intracavitary ad-ministration of amphotericin B in the treat-ment of cerebral aspergillosis in a non im-mune-compromised patient: case report and review of the literature. Br J Neurosurg 2000; 14: 137-141.
[16] Westney GE, Kesten S, De Hoyos A, Chapparro C, Winton T and Maurer JR. Aspergillus infec-tion in single and double lung transplant re-cipients. Transplantation 1996; 61: 915-919.
[17] Mukoyama M, Gimple K and Poser CM. Asper-gillosis of the central nervous system. Report of a brain abscess due to A. fumigatus and re-view of the literature. Neurology 1969; 19: 967-974.
[18] Speth C, Rambach G, Lass-Florl C, Wurzner R, Gasque P, Mohsenipour I and Dierich MP. Cul-ture supernatants of patient-derived Aspergil-lus isolates have toxic and lytic activity towards neurons and glial cells. FEMS Immunol Med Microbiol 2000; 29: 303-313.
[19] D’Angelo R, Marini V, Rinaldi C, Origone P, Dor-caratto A, Avolio M, Goitre L, Forni M, Capra V, Alafaci C, Mareni C, Garre C, Bramanti P, Sidoti A, Retta SF and Amato A. Mutation analysis of CCM1, CCM2 and CCM3 genes in a cohort of Italian patients with cerebral cavernous mal-formation. Brain Pathol 2011; 21: 215-224.
[20] Yoshino M, Morita A, Shibahara J and Kirino T. Radiation-induced spinal cord cavernous mal-
Intracranial aspergillus fumigatus infection complicated with cavernous hemangioma
20531 Int J Clin Exp Med 2015;8(11):20524-20531
formation. Case report. J Neurosurg 2005; 102: 101-104.
[21] Farid N, Zyroff J, Uchiyama CM, Thorson PK and Imbesi SG. Radiation-induced cavernous malformations of the cauda equina mimicking carcinomatous or infectious meningitis. A case report. J Neuroimaging 2014; 24: 92-94.
[22] Park YS, Kim SH, Chang JH, Chang JW and Park YG. Radiosurgery for radiosurgery-indu- ced cavernous malformation. World Neurosurg 2011; 75: 94-98.
[23] Battaglia F, Uro-Coste E, Delisle MB and Tanni-er C. [Radiation-induced cavernoma: two cas-es]. Rev Neurol (Paris) 2008; 164: 468-471.
[24] Strenger V, Sovinz P, Lackner H, Dornbusch HJ, Lingitz H, Eder HG, Moser A and Urban C. Intra-cerebral cavernous hemangioma after cranial irradiation in childhood. Incidence and risk fac-tors. Strahlenther Onkol 2008; 184: 276-280.
[25] Tsao MN, Li YQ, Lu G, Xu Y and Wong CS. Up-regulation of vascular endothelial growth fac-tor is associated with radiation-induced blood-spinal cord barrier breakdown. J Neuropathol Exp Neurol 1999; 58: 1051-1060.
[26] Jung KH, Chu K, Jeong SW, Park HK, Bae HJ and Yoon BW. Cerebral cavernous malforma-tions with dynamic and progressive course: correlation study with vascular endothelial gr- owth factor. Arch Neurol 2003; 60: 1613-1618.
[27] Reichard U, Buttner S, Eiffert H, Staib F and Ruchel R. Purification and characterisation of an extracellular serine proteinase from Asper-gillus fumigatus and its detection in tissue. J Med Microbiol 1990; 33: 243-251.
[28] Lakka SS, Gondi CS, Rao JS. Proteases and Glioma Angiogenesis. Brain Pathol 2005; 15: 327-341.
[29] Uranishi R, Baev NI, Ng PY, Kim JH and Awad IA. Expression of endothelial cell angiogenesis receptors in human cerebrovascular malfor-mations. Neurosurgery 2001; 48: 359-367; discussion 367-358.
[30] Vogler R and Castillo M. Dural cavernous angi-oma: MR features. AJNR Am J Neuroradiol 1995; 16: 773-775.
[31] Yum JH, Kim YD, Lee JH and Woo KI. Huge cav-ernous hemangiomas enveloping the optic nerve successfully removed by a vertical lid split orbitotomy. Case Rep Ophthalmol Med 2014; 2014: 135252.
[32] Kamide T, Nakada M, Hayashi Y, Suzuki T, Hayashi Y, Uchiyama N, Kijima T and Hamada J. Radiation-induced cerebellar high-grade gli-oma accompanied by meningioma and caver-noma 29 years after the treatment of medul-loblastoma: a case report. J Neurooncol 2010; 100: 299-303.
[33] Herbrecht R, Denning DW, Patterson TF, Ben-nett JE, Greene RE, Oestmann JW, Kern WV, Marr KA, Ribaud P, Lortholary O, Sylvester R, Rubin RH, Wingard JR, Stark P, Durand C, Cail-lot D, Thiel E, Chandrasekar PH, Hodges MR, Schlamm HT, Troke PF, de Pauw B; Invasive Fungal Infections Group of the European Or-ganisation for Research and Treatment of Can-cer and the Global Aspergillus Study Group. Voriconazole versus amphotericin B for prima-ry therapy of invasive aspergillosis. N Engl J Med 2002; 347: 408-15.
[34] Walsh TJ, Anaissie EJ, Denning DW, Herbrecht R, Kontoyiannis DP, Marr KA, Morrison VA, Se-gal BH, Steinbach WJ, Stevens DA, van Burik JA, Wingard JR, Patterson TF; Infectious Dis-eases Society of America. Treatment of asper-gillosis: clinical practice guidelines of the Infec-tious Diseases Society of America. Clin Infect Dis 2008; 46: 327-360.