case of 46 year old male with asthma...
TRANSCRIPT
Case of 46 year old male with asthma comorbidities
History (1)
• A 46 year old male, with past medical history significant for allergic rhino conjunctivitis, GERD (gastro esophageal reflux), hiatal hernia, OSA (obstructive sleep apnea) and a former smoker (20 pack year history) presents with an 8 month history of cough.
• He describes the cough as dry during daytime, but productive of clear sputum at night, often causing nocturnal awakenings.
• It is associated with chest tightness, wheezing, shortness of breath at rest and dyspnea on exertion (< 1 flight of stairs).
• At times he would feel chest pain prior to the onset of the cough, which he attributes to GERD.
Case available at: https://www.thoracic.org/professionals/clinical-resources/asthma-center/cases/asthma-comorbidities.php
History (2)
• The patient feels that triggers of the cough include exercise, pollens, reflux symptoms and weather changes. Medications used in the past to treat these symptoms include inhaled combination ICS/LABA, which have provided poor relief of symptoms, and has since been discontinued.
• The patient has no contributing family history of asthma.
Case available at: https://www.thoracic.org/professionals/clinical-resources/asthma-center/cases/asthma-comorbidities.php
Physical exam and lab test result
Physical Exam
• No wheezing or other significant findings on exam. BMI of 32.4
Lab
• Initial spirometry showed reversible obstructive physiology, FEV1/FVC 0.64, FEV1 1.9L (60% predicted), and post-bronchodilator, the FEV1 increases to 2.2L (390cc, 15%).
• His skin prick testing showed positive wheal/flare reactions to dust mite, cat dander, tree, grass and weed pollens.
Case available at: https://www.thoracic.org/professionals/clinical-resources/asthma-center/cases/asthma-comorbidities.php
What should be assessed next for this patient? a. Asthma control
b. Treatment issues
c. Comorbidities
d. All of the above
Polling Question #1
Assessment of asthma
1. Asthma control - two domains• Assess symptom control over the last 4 weeks
• Assess risk factors for poor outcomes, including low lung function
2. Treatment issues• Check inhaler technique and adherence
• Ask about side-effects
• Does the patient have a written asthma action plan?
• What are the patient’s attitudes and goals for their asthma?
3. Comorbidities• Think of rhinosinusitis, GERD, obesity, obstructive sleep apnea, depression, anxiety
• These may contribute to symptoms and poor quality of life
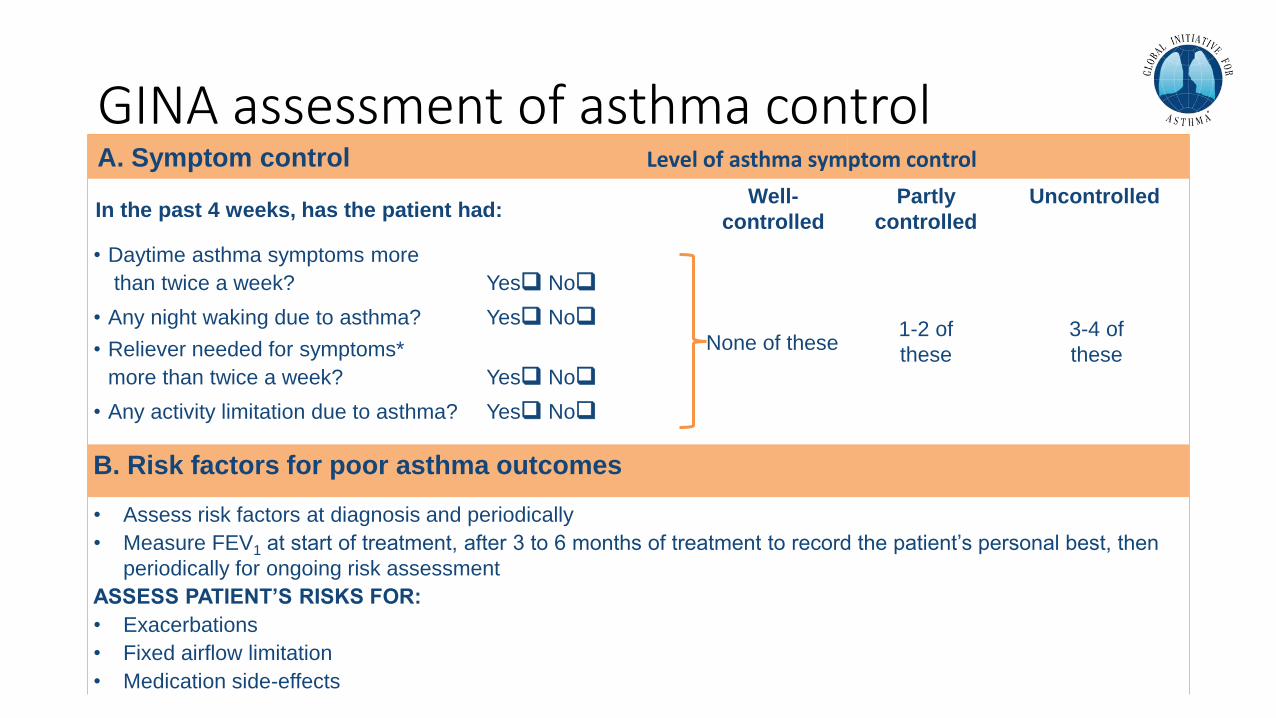
GINA assessment of asthma controlA. Symptom control
In the past 4 weeks, has the patient had:Well-
controlled
Partly
controlled
Uncontrolled
• Daytime asthma symptoms more
than twice a week? Yes No
None of these1-2 of
these
3-4 of
these
• Any night waking due to asthma? Yes No
• Reliever needed for symptoms*
more than twice a week? Yes No
• Any activity limitation due to asthma? Yes No
B. Risk factors for poor asthma outcomes
• Assess risk factors at diagnosis and periodically
• Measure FEV1 at start of treatment, after 3 to 6 months of treatment to record the patient’s personal best, then
periodically for ongoing risk assessment
ASSESS PATIENT’S RISKS FOR:
• Exacerbations
• Fixed airflow limitation
• Medication side-effects
Level of asthma symptom control
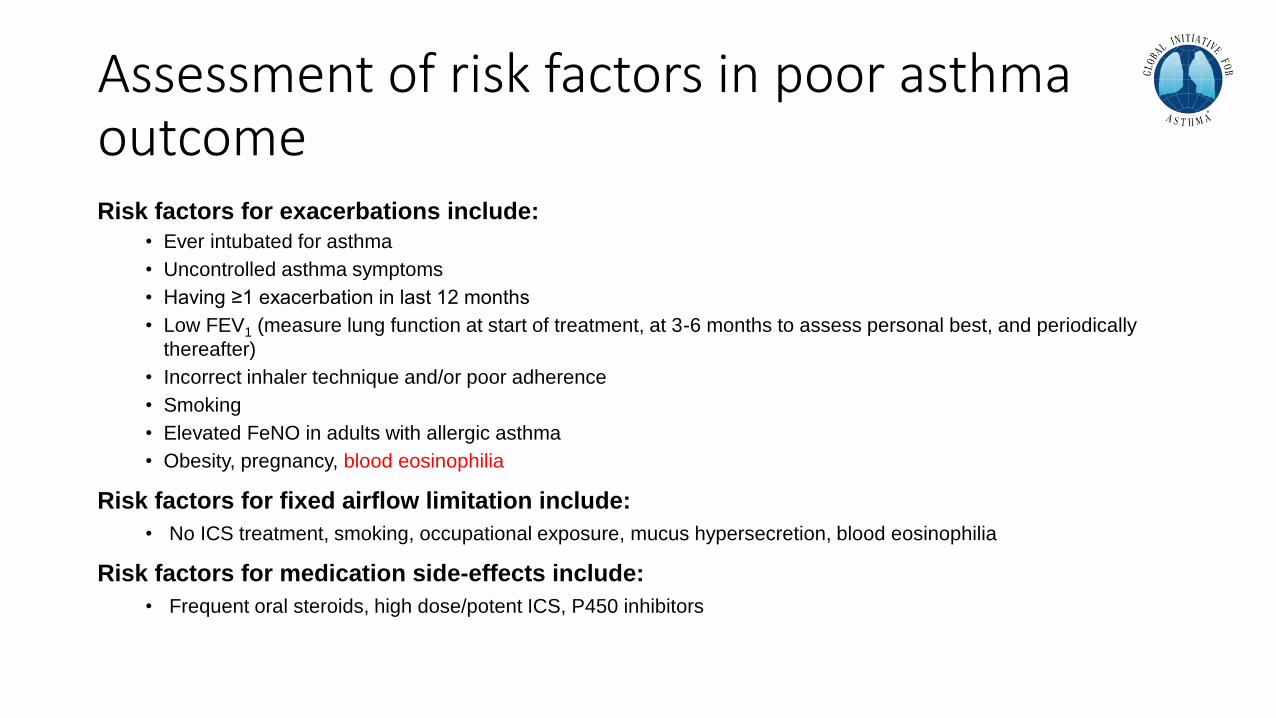
Assessment of risk factors in poor asthma outcomeRisk factors for exacerbations include:
• Ever intubated for asthma
• Uncontrolled asthma symptoms
• Having ≥1 exacerbation in last 12 months
• Low FEV1 (measure lung function at start of treatment, at 3-6 months to assess personal best, and periodically
thereafter)
• Incorrect inhaler technique and/or poor adherence
• Smoking
• Elevated FeNO in adults with allergic asthma
• Obesity, pregnancy, blood eosinophilia
Risk factors for fixed airflow limitation include:
• No ICS treatment, smoking, occupational exposure, mucus hypersecretion, blood eosinophilia
Risk factors for medication side-effects include:
• Frequent oral steroids, high dose/potent ICS, P450 inhibitors
What is the right treatment for this patient?a. As needed SABA
b. Low dose ICS + as needed SABA
c. Low dose ICS/LABA + as needed SABA
d. Med/High dose ICS/LABA + as needed SABA
Polling Question #2
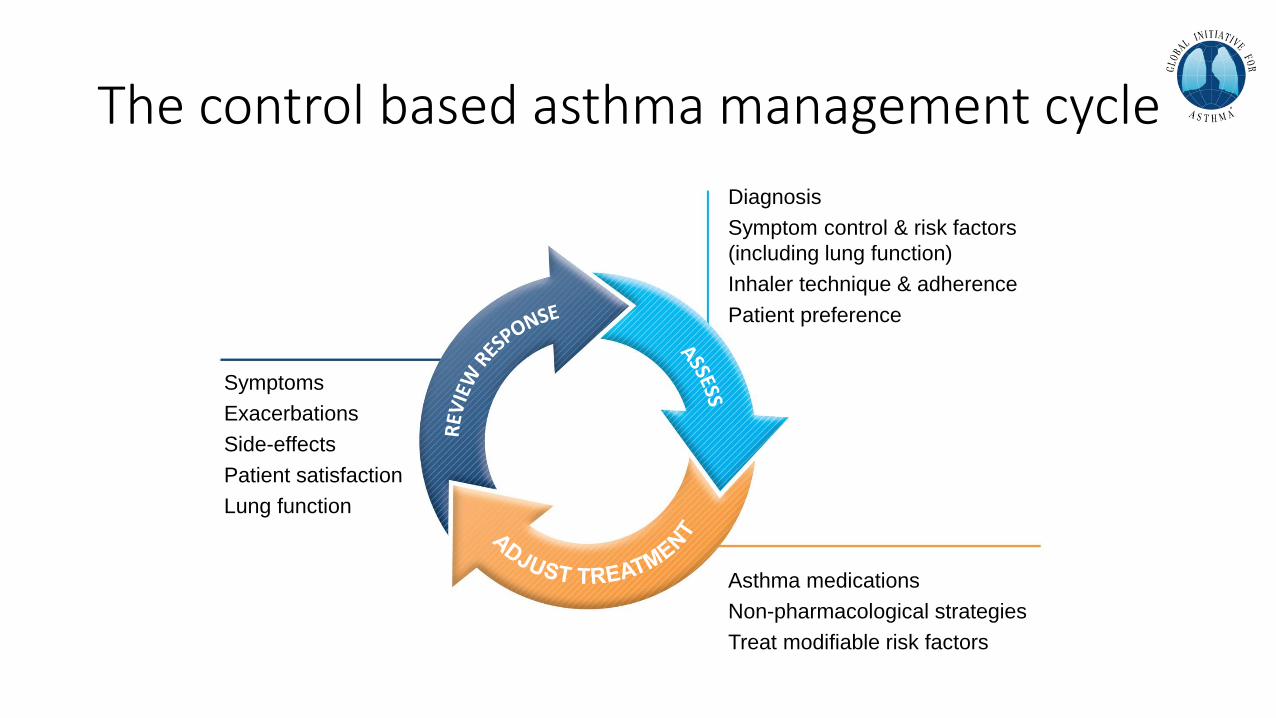
The control based asthma management cycle
Diagnosis
Symptom control & risk factors
(including lung function)
Inhaler technique & adherence
Patient preference
Asthma medications
Non-pharmacological strategies
Treat modifiable risk factors
Symptoms
Exacerbations
Side-effects
Patient satisfaction
Lung function
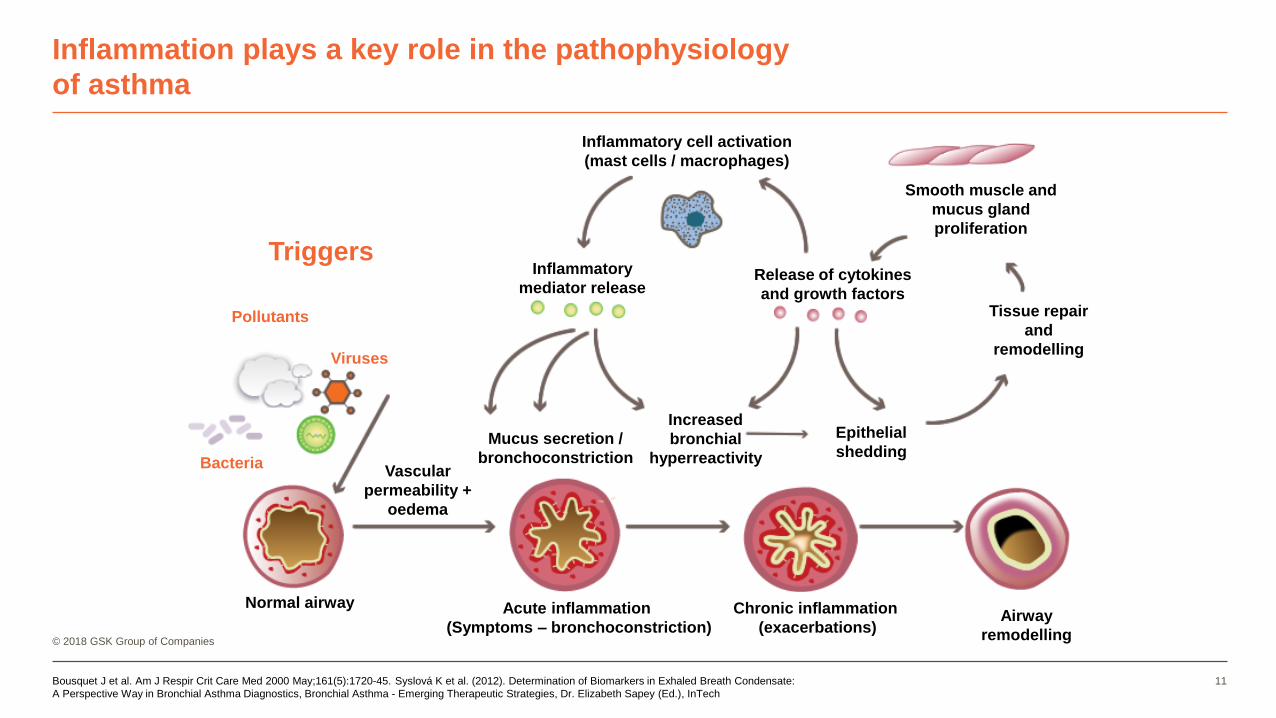
Inflammation plays a key role in the pathophysiology
of asthma
© 2018 GSK Group of Companies
Bousquet J et al. Am J Respir Crit Care Med 2000 May;161(5):1720-45. Syslová K et al. (2012). Determination of Biomarkers in Exhaled Breath Condensate:
A Perspective Way in Bronchial Asthma Diagnostics, Bronchial Asthma - Emerging Therapeutic Strategies, Dr. Elizabeth Sapey (Ed.), InTech
11
Inflammatory cell activation
(mast cells / macrophages)
Inflammatory
mediator releaseRelease of cytokines
and growth factorsTissue repair
and
remodelling
Smooth muscle and
mucus gland
proliferation
Airway
remodelling
Chronic inflammation
(exacerbations)
Acute inflammation
(Symptoms – bronchoconstriction)
Normal airway
Increased
bronchial
hyperreactivity
Epithelial
sheddingMucus secretion /
bronchoconstrictionVascular
permeability +
oedema
Pollutants
Bacteria
Viruses
Triggers
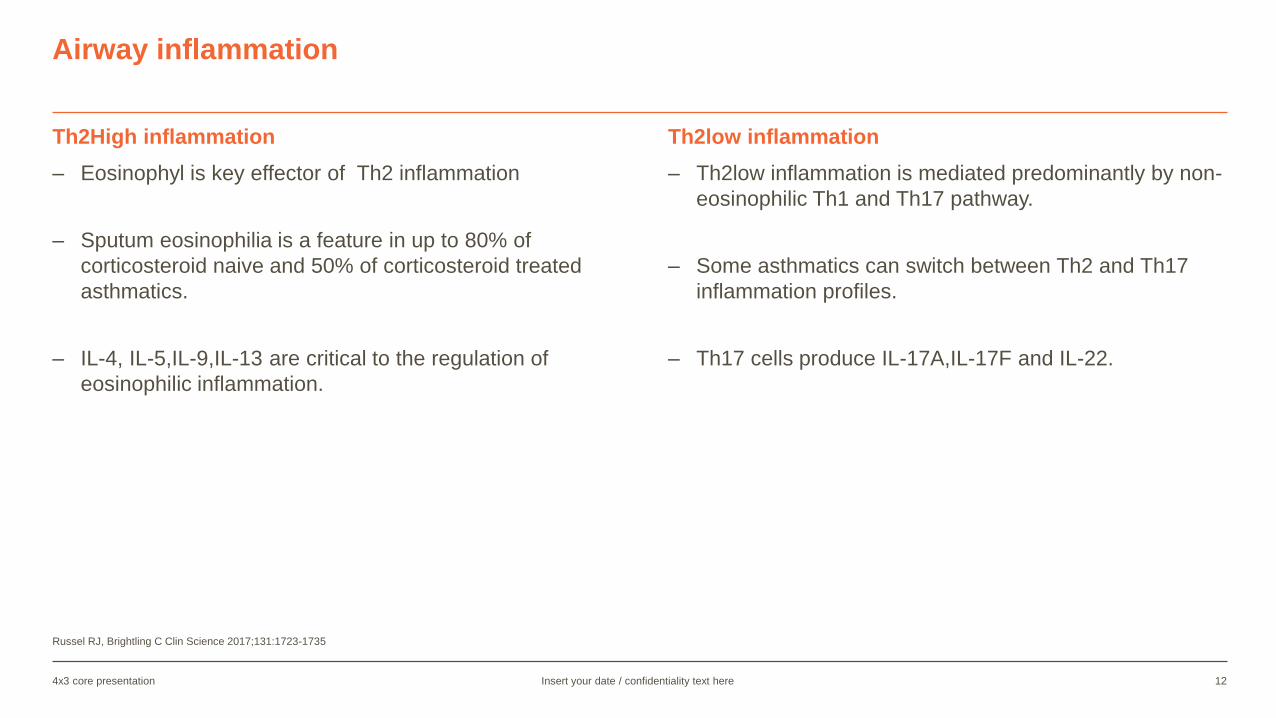
Th2High inflammation
– Eosinophyl is key effector of Th2 inflammation
– Sputum eosinophilia is a feature in up to 80% of
corticosteroid naive and 50% of corticosteroid treated
asthmatics.
– IL-4, IL-5,IL-9,IL-13 are critical to the regulation of
eosinophilic inflammation.
Th2low inflammation
– Th2low inflammation is mediated predominantly by non-
eosinophilic Th1 and Th17 pathway.
– Some asthmatics can switch between Th2 and Th17
inflammation profiles.
– Th17 cells produce IL-17A,IL-17F and IL-22.
Russel RJ, Brightling C Clin Science 2017;131:1723-1735
Insert your date / confidentiality text here4x3 core presentation 12
Airway inflammation
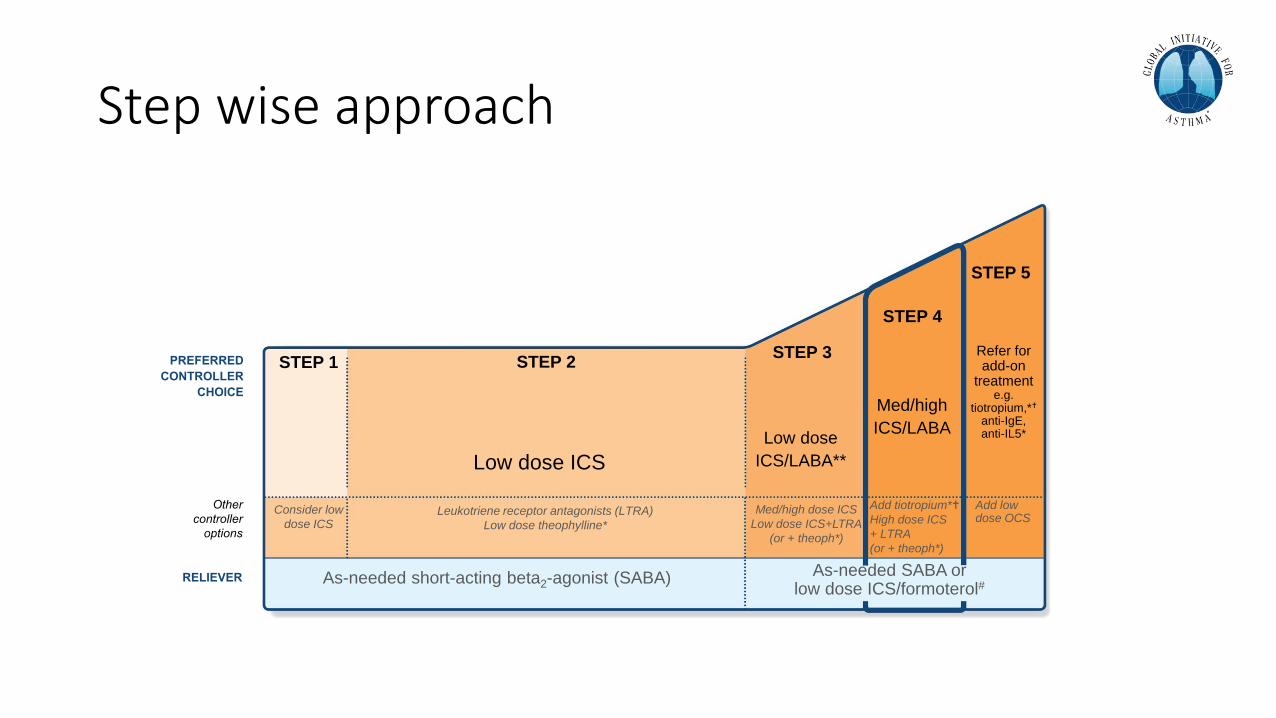
Step wise approach
Other
controller
options
RELIEVER
STEP 1 STEP 2STEP 3
STEP 4
STEP 5
Low dose ICS
Consider low
dose ICS Leukotriene receptor antagonists (LTRA)
Low dose theophylline*
Med/high dose ICS
Low dose ICS+LTRA
(or + theoph*)
As-needed short-acting beta2-agonist (SABA)
Low dose
ICS/LABA**
Med/high
ICS/LABA
PREFERRED
CONTROLLER
CHOICE
Refer for add-on
treatment e.g.
tiotropium,*
anti-IgE, anti-IL5*
As-needed SABA or low dose ICS/formoterol#
Add tiotropium*
High dose ICS
+ LTRA
(or + theoph*)
Add low dose OCS
Management
• The patient was resumed on high dose ICS/LABA (Fluticasone/Salmeterol)
• Intranasal steroid spray was prescribed for his rhinitis.
Case available at: https://www.thoracic.org/professionals/clinical-resources/asthma-center/cases/asthma-comorbidities.php
Salmeterol Fluticasone combination improve patient quality of life and reduce symptom and exacerbation
15
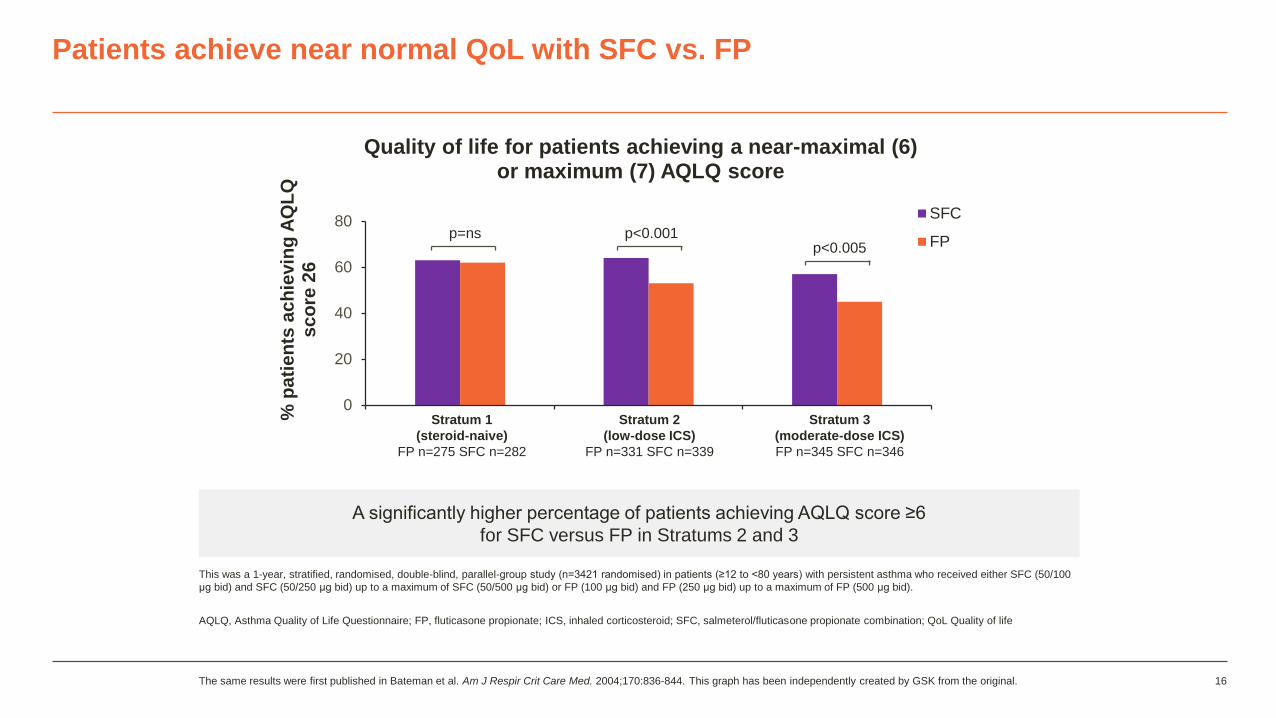
Patients achieve near normal QoL with SFC vs. FP
This was a 1-year, stratified, randomised, double-blind, parallel-group study (n=3421 randomised) in patients (≥12 to <80 years) with persistent asthma who received either SFC (50/100
μg bid) and SFC (50/250 μg bid) up to a maximum of SFC (50/500 μg bid) or FP (100 μg bid) and FP (250 μg bid) up to a maximum of FP (500 μg bid).
AQLQ, Asthma Quality of Life Questionnaire; FP, fluticasone propionate; ICS, inhaled corticosteroid; SFC, salmeterol/fluticasone propionate combination; QoL Quality of life
The same results were first published in Bateman et al. Am J Respir Crit Care Med. 2004;170:836-844. This graph has been independently created by GSK from the original. 16
0
20
40
60
80
% p
ati
en
ts a
ch
ievin
g A
QL
Q
sc
ore
26
Quality of life for patients achieving a near-maximal (6)or maximum (7) AQLQ score
SFC
FP
Stratum 3
(moderate-dose ICS)
FP n=345 SFC n=346
Stratum 2
(low-dose ICS)
FP n=331 SFC n=339
Stratum 1
(steroid-naive)
FP n=275 SFC n=282
p=ns p<0.001p<0.005
A significantly higher percentage of patients achieving AQLQ score ≥6
for SFC versus FP in Stratums 2 and 3
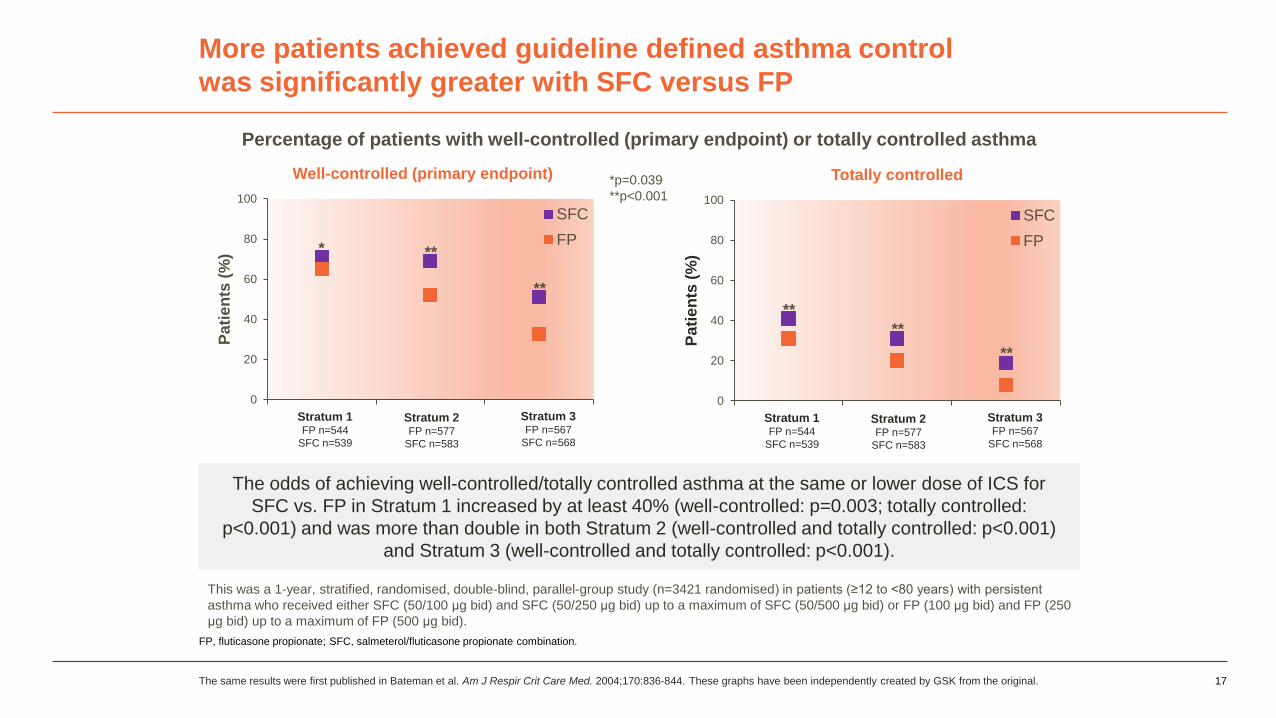
More patients achieved guideline defined asthma control
was significantly greater with SFC versus FP
FP, fluticasone propionate; SFC, salmeterol/fluticasone propionate combination.
17
The odds of achieving well-controlled/totally controlled asthma at the same or lower dose of ICS for
SFC vs. FP in Stratum 1 increased by at least 40% (well-controlled: p=0.003; totally controlled:
p<0.001) and was more than double in both Stratum 2 (well-controlled and totally controlled: p<0.001)
and Stratum 3 (well-controlled and totally controlled: p<0.001).
The same results were first published in Bateman et al. Am J Respir Crit Care Med. 2004;170:836-844. These graphs have been independently created by GSK from the original.
0
20
40
60
80
100
Pa
tie
nts
(%
)
Totally controlled
SFC
FP
Stratum 1FP n=544
SFC n=539
Stratum 2FP n=577
SFC n=583
Stratum 3FP n=567
SFC n=568
0
20
40
60
80
100
Pa
tie
nts
(%
)
Well-controlled (primary endpoint)
SFC
FP
Stratum 1FP n=544
SFC n=539
Stratum 2FP n=577
SFC n=583
Stratum 3FP n=567
SFC n=568
* **
**
**
**
**
Percentage of patients with well-controlled (primary endpoint) or totally controlled asthma
*p=0.039
**p<0.001
This was a 1-year, stratified, randomised, double-blind, parallel-group study (n=3421 randomised) in patients (≥12 to <80 years) with persistent
asthma who received either SFC (50/100 μg bid) and SFC (50/250 μg bid) up to a maximum of SFC (50/500 μg bid) or FP (100 μg bid) and FP (250
μg bid) up to a maximum of FP (500 μg bid).
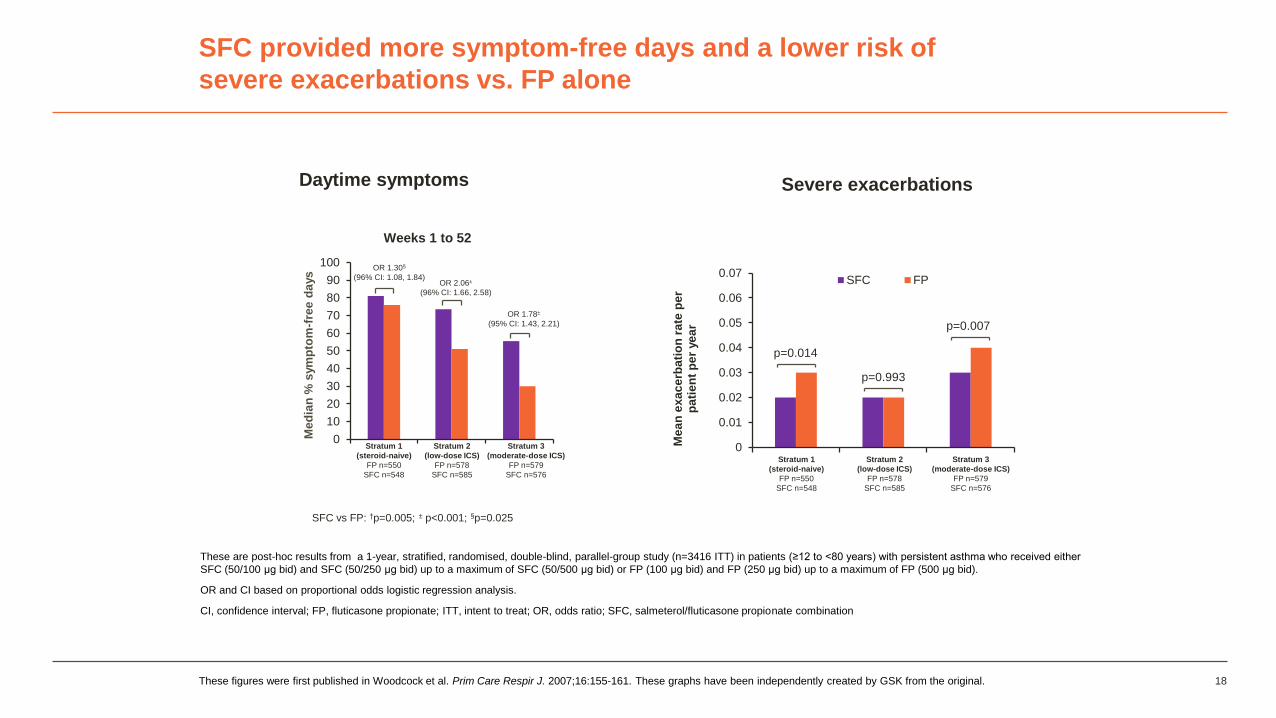
SFC provided more symptom-free days and a lower risk of
severe exacerbations vs. FP alone
These are post-hoc results from a 1-year, stratified, randomised, double-blind, parallel-group study (n=3416 ITT) in patients (≥12 to <80 years) with persistent asthma who received either
SFC (50/100 μg bid) and SFC (50/250 μg bid) up to a maximum of SFC (50/500 μg bid) or FP (100 μg bid) and FP (250 μg bid) up to a maximum of FP (500 μg bid).
OR and CI based on proportional odds logistic regression analysis.
CI, confidence interval; FP, fluticasone propionate; ITT, intent to treat; OR, odds ratio; SFC, salmeterol/fluticasone propionate combination
These figures were first published in Woodcock et al. Prim Care Respir J. 2007;16:155-161. These graphs have been independently created by GSK from the original. 18
SFC vs FP: †p=0.005; ± p<0.001; §p=0.025
0
10
20
30
40
50
60
70
80
90
100
Me
dia
n %
sym
pto
m-f
ree
da
ys
Weeks 1 to 52
Stratum 3
(moderate-dose ICS)
FP n=579
SFC n=576
Stratum 2
(low-dose ICS)
FP n=578
SFC n=585
Stratum 1
(steroid-naive)
FP n=550
SFC n=548
OR 1.30§
(96% CI: 1.08, 1.84)OR 2.06±
(96% CI: 1.66, 2.58)
OR 1.78±
(95% CI: 1.43, 2.21)
0
0.01
0.02
0.03
0.04
0.05
0.06
0.07
Me
an
ex
ac
erb
ati
on
rate
pe
r p
ati
en
t p
er
ye
ar
SFC FP
Stratum 3
(moderate-dose ICS)
FP n=579
SFC n=576
Stratum 2
(low-dose ICS)
FP n=578
SFC n=585
Stratum 1
(steroid-naive)
FP n=550
SFC n=548
Daytime symptoms Severe exacerbations
p=0.014
p=0.993
p=0.007

Regular maintenance dose v. Single maintenance and reliever therapy (SMART)
19
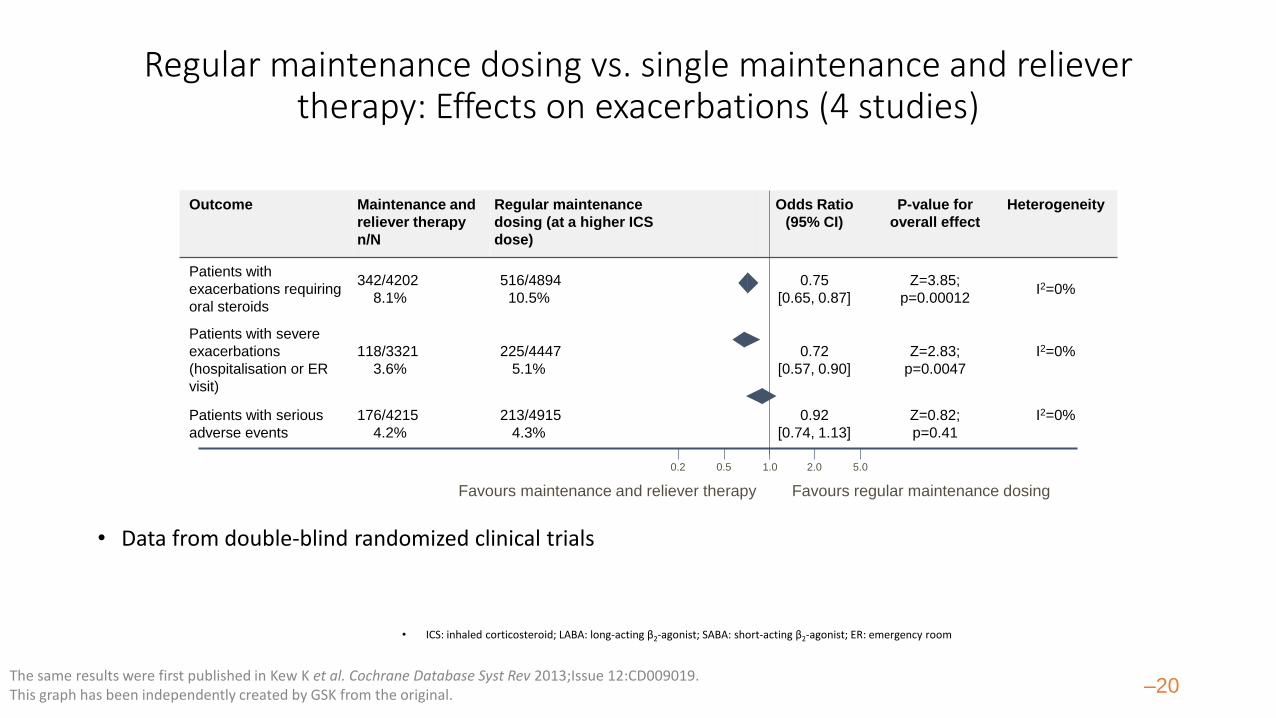
Outcome Maintenance and
reliever therapy
n/N
Regular maintenance
dosing (at a higher ICS
dose)
Odds Ratio
(95% CI)
P-value for
overall effect
Heterogeneity
Patients with
exacerbations requiring
oral steroids
342/4202
8.1%
516/4894
10.5%
0.75
[0.65, 0.87]
Z=3.85;
p=0.00012I2=0%
Patients with severe
exacerbations
(hospitalisation or ER
visit)
118/3321
3.6%
225/4447
5.1%
0.72
[0.57, 0.90]
Z=2.83;
p=0.0047
I2=0%
Patients with serious
adverse events
176/4215
4.2%
213/4915
4.3%
0.92
[0.74, 1.13]
Z=0.82;
p=0.41
I2=0%
Regular maintenance dosing vs. single maintenance and reliever therapy: Effects on exacerbations (4 studies)
• Data from double-blind randomized clinical trials
The same results were first published in Kew K et al. Cochrane Database Syst Rev 2013;Issue 12:CD009019. This graph has been independently created by GSK from the original. –20
• ICS: inhaled corticosteroid; LABA: long-acting β2-agonist; SABA: short-acting β2-agonist; ER: emergency room
Favours maintenance and reliever therapy Favours regular maintenance dosing
1.0 2.0 5.00.50.2
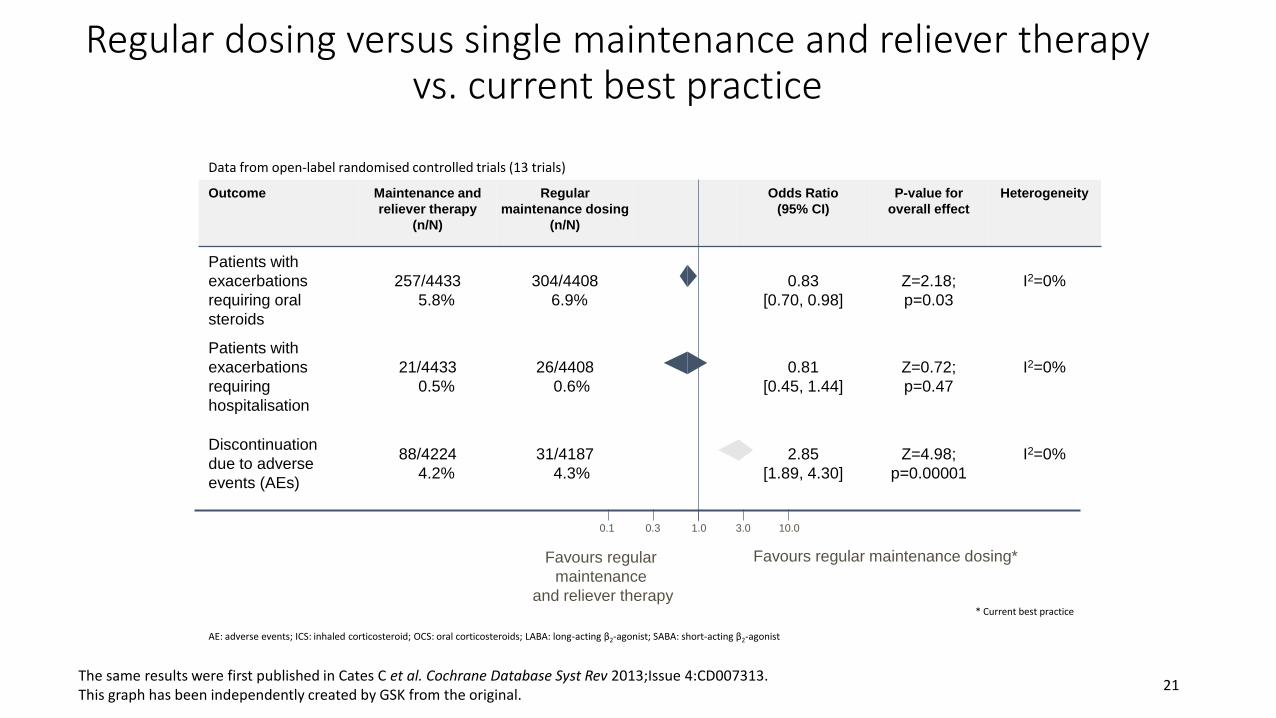
Outcome Maintenance and
reliever therapy
(n/N)
Regular
maintenance dosing
(n/N)
Odds Ratio
(95% CI)
P-value for
overall effect
Heterogeneity
Patients with
exacerbations
requiring oral
steroids
257/4433
5.8%
304/4408
6.9%
0.83
[0.70, 0.98]
Z=2.18;
p=0.03
I2=0%
Patients with
exacerbations
requiring
hospitalisation
21/4433
0.5%
26/4408
0.6%
0.81
[0.45, 1.44]
Z=0.72;
p=0.47
I2=0%
Discontinuation
due to adverse
events (AEs)
88/4224
4.2%
31/4187
4.3%
2.85
[1.89, 4.30]
Z=4.98;
p=0.00001
I2=0%
Regular dosing versus single maintenance and reliever therapy vs. current best practice
* Current best practice
AE: adverse events; ICS: inhaled corticosteroid; OCS: oral corticosteroids; LABA: long-acting β2-agonist; SABA: short-acting β2-agonist
The same results were first published in Cates C et al. Cochrane Database Syst Rev 2013;Issue 4:CD007313. This graph has been independently created by GSK from the original.
21
Favours regular
maintenance
and reliever therapy
1.0 3.0 10.00.30.1
Favours regular maintenance dosing*
Data from open-label randomised controlled trials (13 trials)
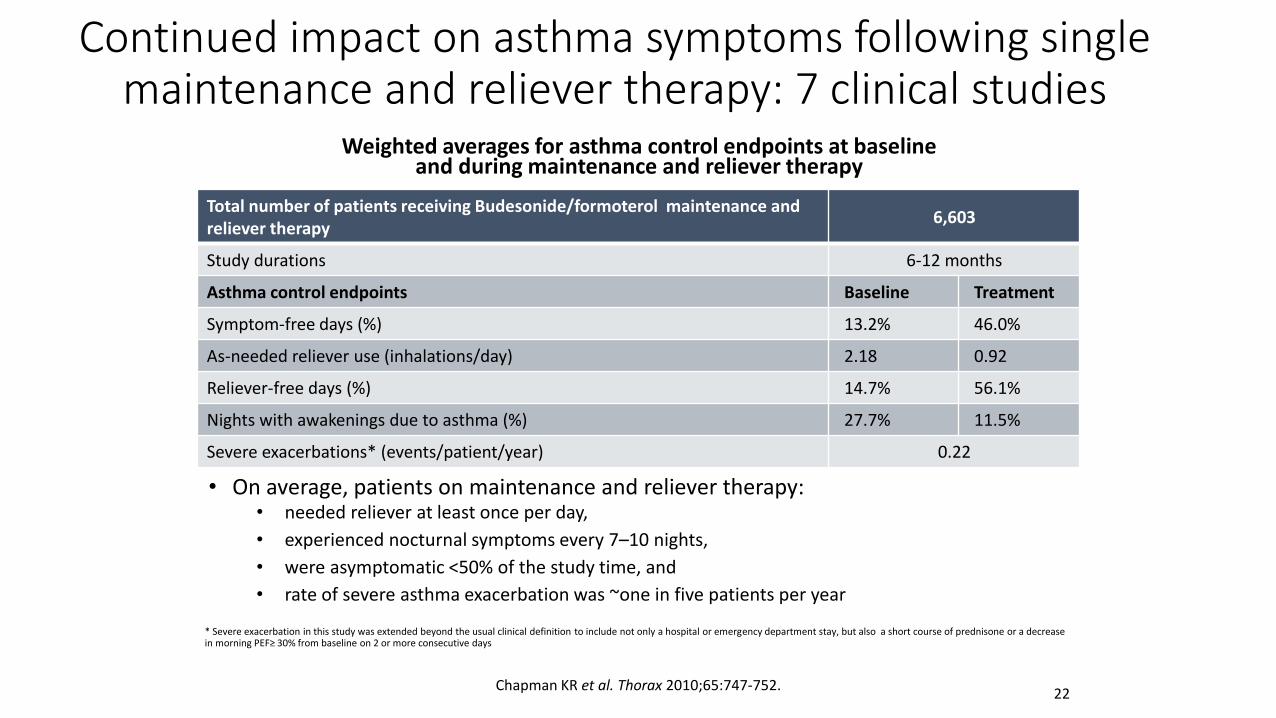
Continued impact on asthma symptoms following single maintenance and reliever therapy: 7 clinical studies
Weighted averages for asthma control endpoints at baselineand during maintenance and reliever therapy
• On average, patients on maintenance and reliever therapy:• needed reliever at least once per day,
• experienced nocturnal symptoms every 7–10 nights,
• were asymptomatic <50% of the study time, and
• rate of severe asthma exacerbation was ~one in five patients per year
* Severe exacerbation in this study was extended beyond the usual clinical definition to include not only a hospital or emergency department stay, but also a short course of prednisone or a decrease in morning PEF≥ 30% from baseline on 2 or more consecutive days
Chapman KR et al. Thorax 2010;65:747-752.
Total number of patients receiving Budesonide/formoterol maintenance and reliever therapy
6,603
Study durations 6-12 months
Asthma control endpoints Baseline Treatment
Symptom-free days (%) 13.2% 46.0%
As-needed reliever use (inhalations/day) 2.18 0.92
Reliever-free days (%) 14.7% 56.1%
Nights with awakenings due to asthma (%) 27.7% 11.5%
Severe exacerbations* (events/patient/year) 0.22
22
This is a weekly control measure. GINA: Global Initiative for Asthma; Patients all had ≥ 1 exacerbation in previous year.1. The same results were first published in Bateman E et al. J Allergy Clin Immunol. 2010;125:600–608. This graph has been
independently created by GSK from the original. 2. GSK DoF RF/SFC/0030/17. 3. Global Strategy for Asthma Management
and Prevention, Global Initiative for Asthma (GINA) 2018,
23
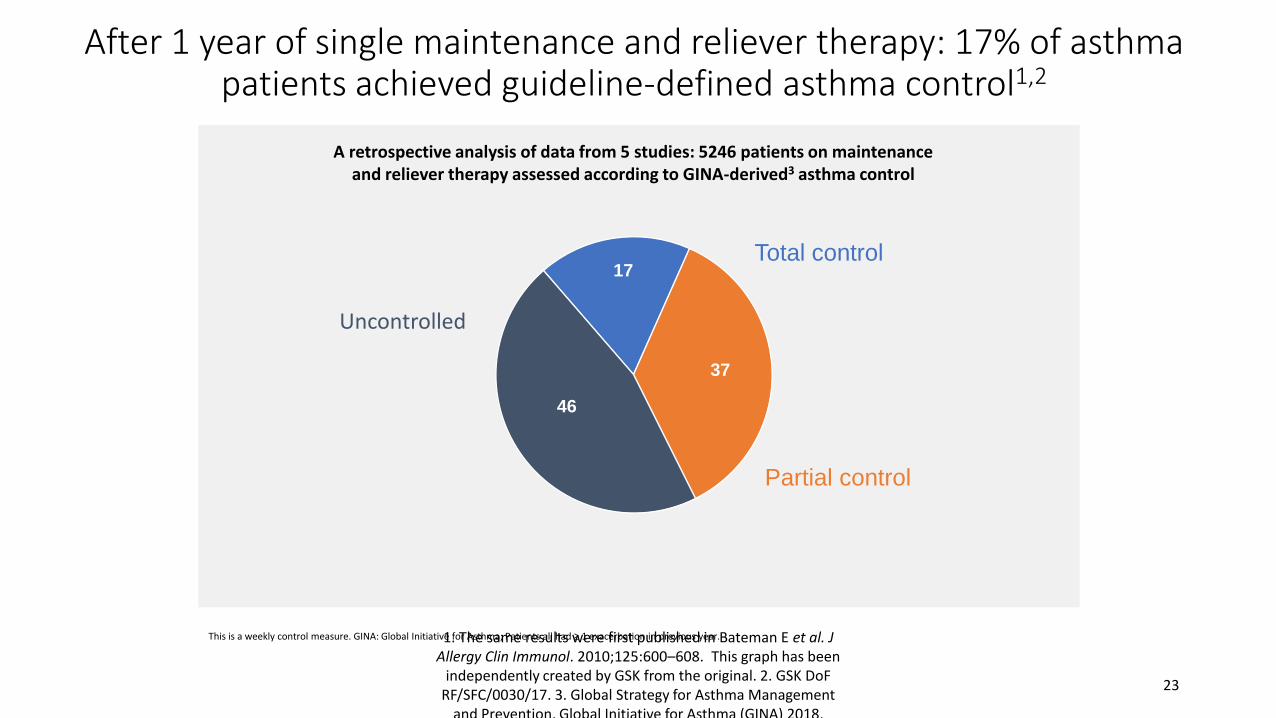
After 1 year of single maintenance and reliever therapy: 17% of asthma patients achieved guideline-defined asthma control1,2
17
37
46
A retrospective analysis of data from 5 studies: 5246 patients on maintenanceand reliever therapy assessed according to GINA-derived3 asthma control
Total control
Uncontrolled
Partial control
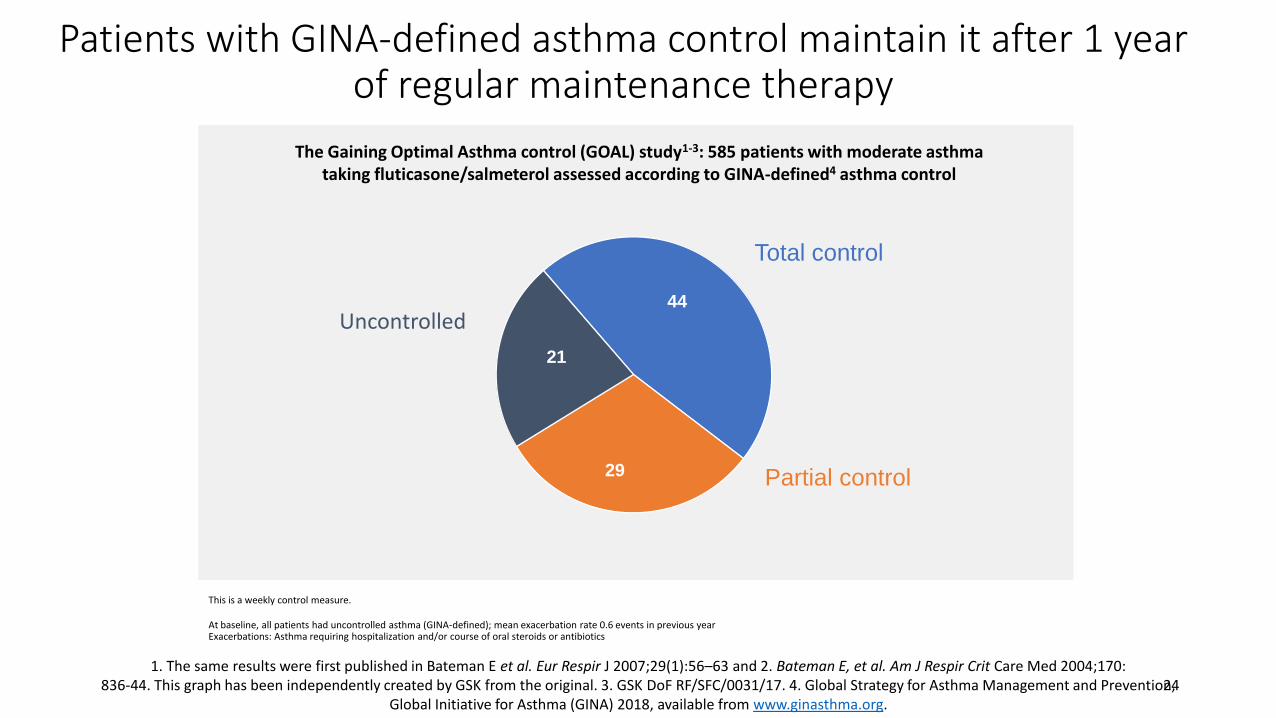
44
29
21
This is a weekly control measure.
At baseline, all patients had uncontrolled asthma (GINA-defined); mean exacerbation rate 0.6 events in previous yearExacerbations: Asthma requiring hospitalization and/or course of oral steroids or antibiotics
1. The same results were first published in Bateman E et al. Eur Respir J 2007;29(1):56–63 and 2. Bateman E, et al. Am J Respir Crit Care Med 2004;170:836-44. This graph has been independently created by GSK from the original. 3. GSK DoF RF/SFC/0031/17. 4. Global Strategy for Asthma Management and Prevention,
Global Initiative for Asthma (GINA) 2018, available from www.ginasthma.org.24
The Gaining Optimal Asthma control (GOAL) study1-3: 585 patients with moderate asthmataking fluticasone/salmeterol assessed according to GINA-defined4 asthma control
Total control
Uncontrolled
Partial control
Patients with GINA-defined asthma control maintain it after 1 year of regular maintenance therapy
-60
-40
-20
0
20
40
60
80
100C
han
ge f
rom
bas
elin
e (%
)
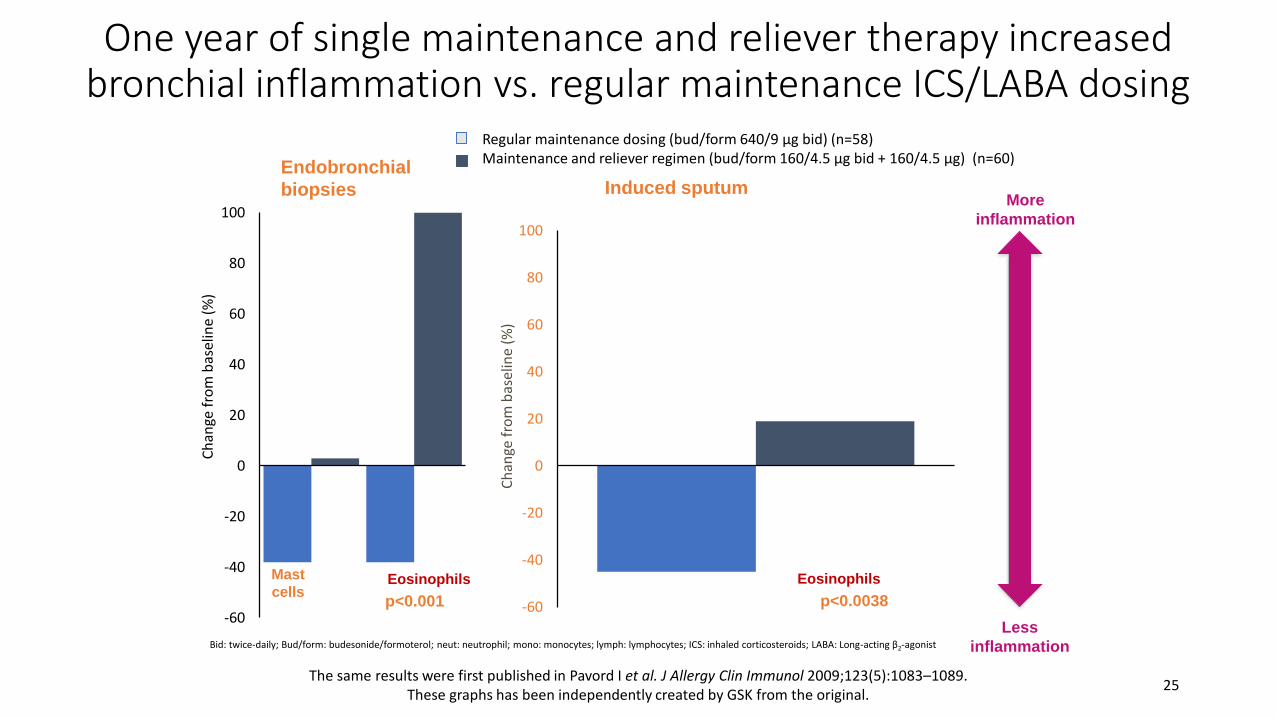
One year of single maintenance and reliever therapy increased bronchial inflammation vs. regular maintenance ICS/LABA dosing
Bid: twice-daily; Bud/form: budesonide/formoterol; neut: neutrophil; mono: monocytes; lymph: lymphocytes; ICS: inhaled corticosteroids; LABA: Long-acting β2-agonist
The same results were first published in Pavord I et al. J Allergy Clin Immunol 2009;123(5):1083–1089. These graphs has been independently created by GSK from the original.
25
Endobronchial
biopsiesMore
inflammation
Mast
cellsEosinophils
p<0.001
Regular maintenance dosing (bud/form 640/9 µg bid) (n=58)Maintenance and reliever regimen (bud/form 160/4.5 µg bid + 160/4.5 µg) (n=60)
-60
-40
-20
0
20
40
60
80
100
Induced sputum
Eosinophils
p<0.0038
Ch
ange
fro
m b
asel
ine
(%)
Less
inflammation
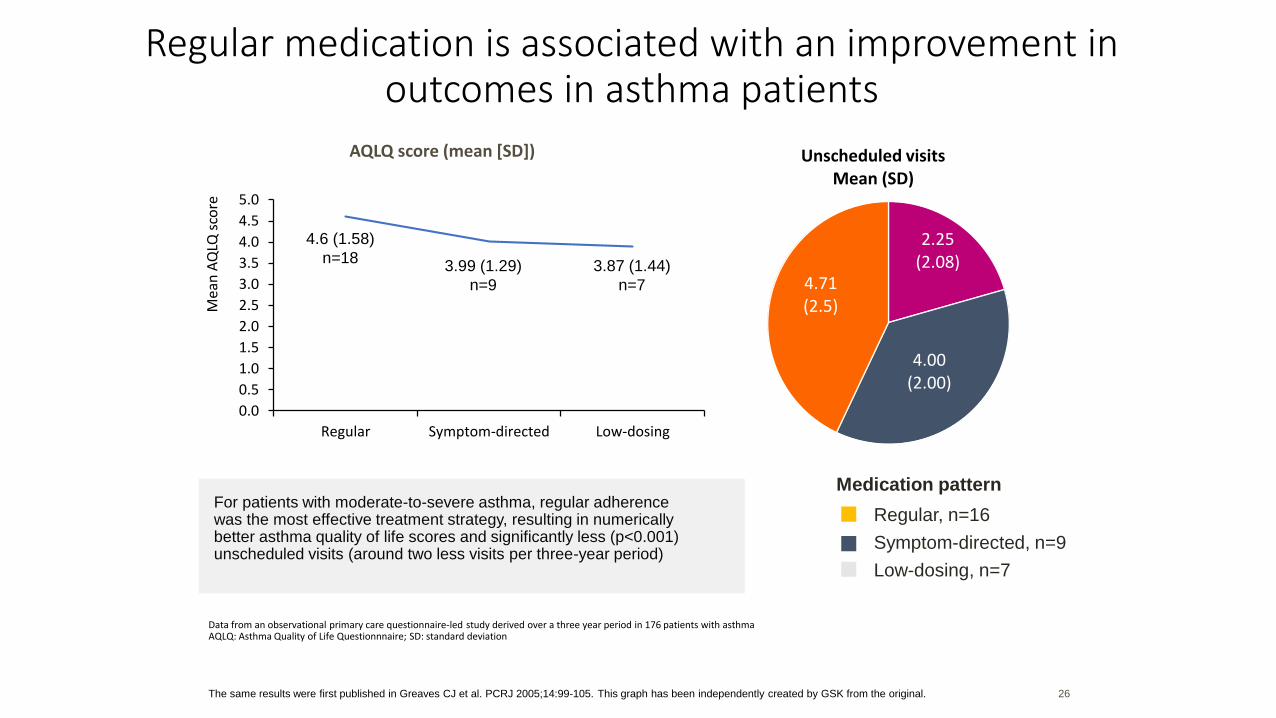
2.25 (2.08)
4.00 (2.00)
4.71 (2.5)
Unscheduled visits Mean (SD)
Regular medication is associated with an improvement in outcomes in asthma patients
Data from an observational primary care questionnaire-led study derived over a three year period in 176 patients with asthmaAQLQ: Asthma Quality of Life Questionnnaire; SD: standard deviation
Medication pattern
Regular, n=16
Symptom-directed, n=9
Low-dosing, n=7
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Regular Symptom-directed Low-dosing
Mea
n A
QLQ
sco
re
AQLQ score (mean [SD])
3.87 (1.44)
n=7
3.99 (1.29)
n=9
4.6 (1.58)
n=18
The same results were first published in Greaves CJ et al. PCRJ 2005;14:99-105. This graph has been independently created by GSK from the original. 26
For patients with moderate-to-severe asthma, regular adherence was the most effective treatment strategy, resulting in numerically better asthma quality of life scores and significantly less (p<0.001) unscheduled visits (around two less visits per three-year period)
How long should we follow up the patient asthma control?a. 1 week
b. 4-6 weeks
c. 1 month
d. 1-3 months
Polling Question #3
Reviewing response and adjusting treatment
• How often should asthma be reviewed?• 1-3 months after treatment started, then every 3-12 months
• During pregnancy, every 4-6 weeks
• After an exacerbation, within 1 week
When to consider step down treatment?a. After good control maintained for 1 months
b. After good control maintained for 2 months
c. After good control maintained for 3 months
d. After good control maintained for 6 months
Polling Question #4
Reviewing response and adjusting treatment
• Stepping down asthma treatment• Consider step-down after good control maintained for 3 months
• Find each patient’s minimum effective dose, that controls both symptoms and exacerbations
Case continued…
• Symptoms improved on six month follow-up and due to being well controlled he was stepped down to a medium dose ICS/LABA.
• With step down his symptoms worsened at next six month follow-up.
Case available at: https://www.thoracic.org/professionals/clinical-resources/asthma-center/cases/asthma-comorbidities.php
Should we resume the treatment to high dose ICS/LABA?a. Yes
b. No
Polling Question #5
Stepping up asthma treatment
• Sustained step-up, for at least 2-3 months if asthma poorly controlled• Important: first check for common causes (symptoms not due to asthma,
incorrect inhaler technique, poor adherence)
• Short-term step-up, for 1-2 weeks, e.g. with viral infection or allergen• May be initiated by patient with written asthma action plan
• Day-to-day adjustment• For patients prescribed low-dose ICS/formoterol maintenance and reliever
regimen*
Case continued …
• He was resumed at high dose ICS/LABA.
• At the next follow-up he voiced that the cough had improved, but he still had symptoms of chest tightness, dyspnea on exertion. He also described a sensation of lung burning. He added that he was experiencing frequent episodes of GERD, despite being on BID dosing of omeprazole.
Case available at: https://www.thoracic.org/professionals/clinical-resources/asthma-center/cases/asthma-comorbidities.php
What’s next for the patient?a. Check inhaler technique
b. Address treatment issues
c. Manage comorbidities
d. All of the above
Polling Question #6
Managing asthma with comorbidities
• Identify and manage comorbidities such as rhinosinusitis, obesity and gastro-esophageal reflux disease.
• Comorbidities may contribute to respiratory symptoms and impaired quality of life, and some contribute to poor asthma control
Case continued …
• The patient was referred to gastroenterology (GI) and cardiology. Cardiology ruled out CAD via stress testing and commented that chest tightness was likely related to his reflux.
• GI commented that the patient had gained an additional 20 lbs in the last year.
• They switched the patient to maximal dose of BID esomeprazole, encouraged him to lose weight and ordered eesophageal manometry, pH monitoring and an EGD.
• The patient improved marginally with weight loss
Case available at: https://www.thoracic.org/professionals/clinical-resources/asthma-center/cases/asthma-comorbidities.php
Case continued …
• He returned for follow-up 5 months after his procedure, his coughing was minimal, dyspnea was much improved and he reported no use of his as needed SABA. He was stepped down to medium dose ICS/LABA.
• The patient called 2 months later, reporting that he had no residual cough and enquired if he may stop his ICS/LABA.
Case available at: https://www.thoracic.org/professionals/clinical-resources/asthma-center/cases/asthma-comorbidities.php
Should we step down the ICS/LABA?a. Yes
b. No
Polling Question #7
Case continued …
• He was advised to continue current regimen until next follow-up, at which time we stepped down to low dose ICS/LABA.
• We ultimately discontinued his ICS/LABA due to resolution of cough, chest tightness and SOB. He continues on as needed SABA.
Case available at: https://www.thoracic.org/professionals/clinical-resources/asthma-center/cases/asthma-comorbidities.php
Thank you