cardiovascular function in extreme obesity
TRANSCRIPT

Acta med. scand. Vol. 193, pp. 437-446, 1973
CARDIOVASCULAR FUNCTION IN EXTREME OBESITY
L. Backman, U. Freyschuss, D. Hallberg and A. Melcher
From the Departments of Surgery and Cfinicaf Physiology, Karolinska sjukhuset, Stockholm, Sweden
Abstract. Cardiovascular function in 19 patients with obe- sity has been studied by electrocardiography (ECG), exercise test, determination of heart and blood volumes, and right heart catheterization. Pathological ECG find- ings appeared in one patient at rest and during exercise, and in another only during exercise. Blood volume was low in relation to body weight, but hemoglobin con- centration was normal. Heart volume and stroke volume were normally related to the total amount of hemoglobin (THb), while the working capacity (W,,,J in eight cases was low in relation to THb. The cardiac output was found to be normal when related to the oxygen intake both at rest and during exercise. There was a statisti- cally significant linear relationship between intravascular pressures and cardiac output. Brachial artery pressures and left ventricle filling pressure were significantly ele- vated at rest and during exercise, while pulmonary ar- tery pressures and end-diastolic pressure of the right ventricle showed a statistically significant steeper rise with increase in cardiac output than normally found. It is concluded that the circulatory dimensions and the cardiac output reflect an adequate adaptation to the metabolic demands laid upon the circulation in obesity. The ele- vated filling pressures of the ventricles and the high sys- temic and pulmonary vascular resistance, however, sug- gest that obesity is not without deleterious effect on cardiovascular function.
It is widely accepted that obesity induces cardio- vascular disturbances, such as prevalence of high blood pressure (for review see 12), and in far ad- vanced cases also congestive heart failure (2, 4, 5, 9). In contrast to the number of clinical re- ports there are surprisingly few hemodynamic studies of obese patients. Some data obtained at rest during heart catheterization have been pre- sented in case reports (16, 17, 29). Blood volume and cardiac output at rest of 40 obese subjects were determined by Alexander (2), who in the
same material measured regional blood flow to the cerebral, splanchnic and renal vascular beds in a few subjects. Pulmonary arterial and pul- monary capillary venous pressures of the same patients were later commented on (l), but not un- til recently has the central hemodynamic func- tion of a small obese material been described in greater detail (3). The data of the central vascular and intracardiac pressures are, however, rather incomplete and refer to eight and two patients, respectively. Furthermore, most of the data are obtained at rest, and when exercise is included in the investigation procedure, only a single load and a very low one is chosen, provoking an aver- age oxygen consumption of not more than three times the resting value.
The present paper is one in a series of investi- gations concerning the effect on cardiopulmonary function of weight reduction through jejunoileos- tomy. The preoperative study of circulatory di- mensions and central hemodynamics will be pre- sented below.
MATERIAL Five male and 14 female patients, 17-59 years of age and weighing 108-172 kg, were investigated prior to je- junoileostomy. They had been obese for several years and treatment with calory intake reduction supported by hospitalization had been of only temporary success.
Fifteen patients had no other diagnosis than obesity, while the remaining four had additional diseases. Three subjects were treated for an arterial hypertension and one of them (aged 59) was also taking digitalis and had a typical history of angina pectoris. The fourth patient had a mild, tablet-treated diabetes.
Vital characteristics are presented in Table 1.
Acta med. scand. 193

438 L. Backman e f al.
Table I. Vital statistics of 19 obese patients. Work test data from sitting position
Case Age Height Weight weight BV W1,O HRBP
- Over-
no. (Y.) (cm) (kg) (%) (1) (kpm/min) (kpm/min) (beats/min)
Males 1 34 2 33 3 44 4 34 5 47
Mean 38 S.D. 6.6 Range 33-47
Females 6 17 7 31 8a 35 9 34
l o b 52 11 26 12 45 13 42 14bc 59 15 32 16 46 17 27
19 47
Mean 38 S.D. 11.4 Range 17-59
18b 43
179 184 189 175 182
182 5.3
175-1 89
179 158 156 167 172 155 170 174 171 176 163 170 176 162
168 7.8
155-1 79
170 167 146 125 140
149.6 18.9
125.0-170.0
143 115 129 154 109 108 122 150 131 136 141 153 172 158
137.3 19.4
108.0-172.0
137 6.8 96 7.9 85 8.8 55 7.0 63 7.3
81.4 7.6 32.3 0.81
55.1-137.0 6.8-8.8
93 6.2 106 5.5 119 5.9 130 8.3 44 6.7 80 5.8 73 6.1
7.0 83 7.3 76 6.4
107 7.4 120 7.9 114 7.7 133 7.5
98.1 6.8 26.1 0.87
-
43.8-133.0 5.5-8.3
360 990
1 650 1230 1495
1145 506
360-1 650
300 600
1 000 935 690 810 920
1 090
655 1150
890 780
818 225.0
-
-
300 162 900 164 200 152 200 167 000 140
920 157 370 11.0 DO-1 200 140-167
265 172 600 170 465 144 800 160 635 166 665 161 600 145 600 138 150 132 600 165 465 124 600 145 600 152 - -
542 152 171.4 15.2
300-1 150 150-800 124172 ~
Clinical diagnosis: a mild diabetes, arterial hypertension, angina pectoris + digitalis treatment.
METHODS Before heart catheterization the patients were subjected to a thorough investigation at the laboratory, including ECG recordings, exercise tests and determination of total amount of hemoglobin, blood volume and heart volume.
Ideal weight was calculated from height and a measure of skeletal frame, the sum of the wrist widths (13, 14). Overweight is expressed as excess weight in % of the ideal weight.
ECGs were recorded with a direct-writing ink-jet re- corder (Mingograf 61 and 81, Elema), both at rest in the supine and standing position and during and after sitting and supine exercise.
The exercise test consisted of stepwise increased work loads (25, 27) on an electrodynamically braked bicycle ergometer (Elema). The loads were increased every 6th min until the subjects were exhausted. The work load at break point, (WBp), was taken to be the heaviest load at which the subjects worked for 6 min with an incre- ment proportional to the completed period at the next higher load. Physical working capacity (25, 27) is ex- pressed as the working intensity in kpm/min correspond- ing to a heart rate of 170 beats/min (W,J obtained by intra- or extrapolation.
The heart volume (HV) was measured in the prone position (21).
Acta med. scand. 193
The total amount of hemoglobin (THb) was deter- mined by the alveolar method of Sjostrand (26, 27).
The blood volume (BV) was calculated from THb and Hb concentration in finger blood with a standard correc- tion factor (0.91) for the difference between total body hematocrit and the hematocrit of peripheral blood (19).
Right heart catheterization was performed by percu- taneous insertion of a double lumen catheter into the left antecubital vein. In the brachial artery of the oppo- site arm a short teflon catheter was inserted percutane- ously.
Blood pressures were measured with strain-gauge trans- ducers (Medec) and recorded, together with an ECG lead, on a UV recorder (Oscilloscript, Siemens). The reference point was taken as the midthoracic point of the anteroposterior plane at the insertion of the fourth rib of the sternum.
Heart rate (HR) was determined from ECG. The cardiac output was measured according to the
direct Fick method. Oxygen uptake was determined by the Douglas bag technique, expired air being measured with a spirometer, and gas analyses were made by the Haldane technique. Blood samples were drawn during 1 min from the pulmonary and brachial arteries simul- taneously. The oxygen saturation was determined spectro- photometrically, and the oxygen content was calculated

Cardiovascular function in extreme obesity 439
from the oxygen saturation and Hb concentration, using the factor 1.34 for the oxygen-combining power of Hb. A correction for physically dissolved oxygen was made according to Peters and van Slyke.
The pulmonary resistance index was calculated as the difference between the mean pressure in the pulmonary artery and the mean pulmonary capillary venous (PVC) pressure divided by the cardiac output; and the systemic resistance index as the mean pressure in the brachial artery divided by the cardiac output.
Current statistical methods have been applied (28). Comparisons between two regression lines have been made according to Hald (18).
The catheterization commenced in the morning after a light meal. All measurements were made at rest and during supine exercise at two loads. The work loads were chosen, with the guidance of the previous exercise tests, to correspond to one submaximal and one close to maxi- mal (WBp) work intensity.
RESULTS
Individual data on blood volume are given in Table I. Expressed in ml/kg body weight the mean value for the males was 51.1 (S.D. 7.9) and for females 50.5 (S.D. 5.0), which are lower val- ues than observed in healthy subjects (74 and 73 ml, respectively) (27), and there was a negative correlation between percentage overweight and BV/kg b. wt. (p<O.O5). If the BV is expressed in ml/kg ideal b. wt., mean values were 94.3 (S.D. 10.5) and 99.2 (S.D. 12.3). A positive relationship between oxygen uptake at rest and BV was, how- ever, found in this material ( p < 0.001).
Hemoglobin concentration was normal and hence the THb (Fig. 1) varied in accordance with the BV.
The values of heart volume must probably be regarded as somewhat approximate due to diffi- culties in getting satisfactory X-ray projections of the cardiac borderlines, caused by the amount of adipose tissue. The absolute values of Hv aver- aged 1208 ml for the males (range 1065-1 330) and 976 ml for the females (range 675-1 325). When related to THb four cases were above, one below, and the remaining 12 patients within nor- mal limits (Fig. 1).
ECG recordings at rest were normal in 14 pa- tients. Three cases had ventricular ectopic beats, which, however, vanished during exercise. Patho- logical left ventricle ST-T depressions appeared in one case (no. 14, Table I) and slight such changes in another.
During exercise pathological ST depressions
1300
1100
900
700
500
Heart volume,ml /
/ /
1 /-
/ 0 1 4
0
Fig. 1. Heart volume in supine position in relation to total amount of hemoglobin. 0, Males (n= 3); 0, fe- males (a = 14). Regression line 5 2 S.D. for healthy controls are given (27).
corresponding to the left ventricle were demon- strated in case 14 (Table I) and in one patient (no. 12) when working in the supine but not in the sitting position. In another case (no. 10) ECG during supine exercise demonstrated slight ST de- pressions, while no such changes were recorded during sitting exercise. No patients had symptoms of coronary insufficiency during the work tests.
Individual and mean data on physical working capacity in the sitting position are given in Table I. The W,,, representing the work actually per- formed, is lower than WIT,, as most patients dis- continued the exercise test before reaching HR 170. The maximal HR, recorded at the end of work, is listed as HR,,. The usual complaint during the final part of the test was a sensation of fatigue in the legs and/or breathlessness.
The WBP was on an average 80 kpm/min higher in the sitting than in the supine position
Acta med. scand. I93
440 L. Backman et al.
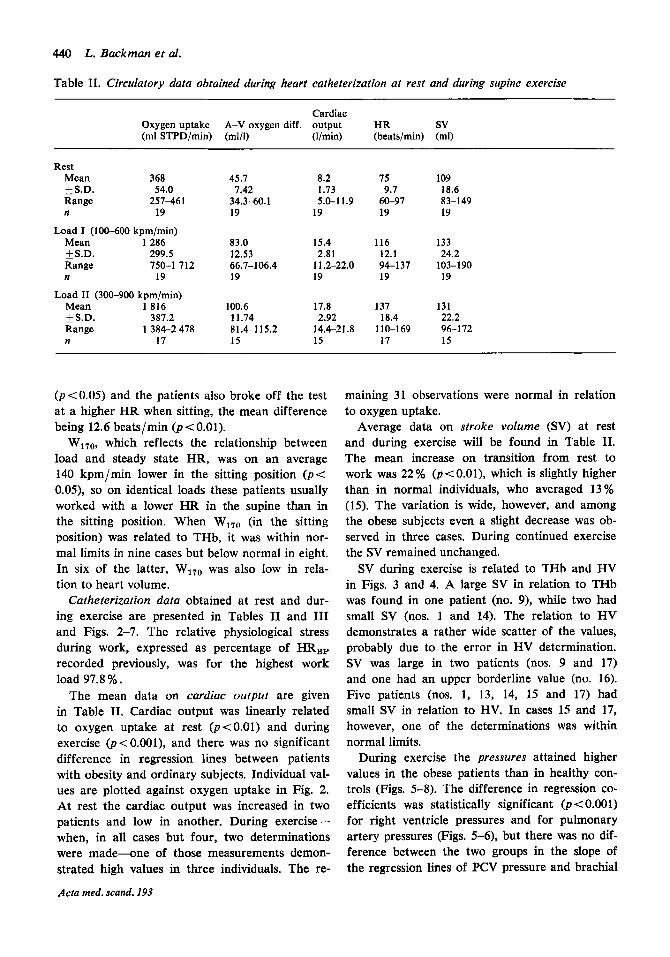
Table 11. Circulatory data obtained during heart catheterization at rest and during supine exercise
Cardiac Oxygen uptake A-V oxygen diff. output HR sv (ml STPD/min) (ml/l) (I/min) (beats/min) (ml)
Rest Mean 368
S.D. 54.0 Range 257-461 n 19
Load I (100-600 kpmlmin) Mean 1286
S.D. 299.5 Range 750-1 712 n 19
Load I1 (300-900 kpm/min) Mean 1816 kS.D. 387.2 Range 1 384-2 478 n 17
45.7
34.3-60.1 7.42
19
83.0 12.53
19 66.7-106.4
100.6 11.74 81.4-115.2 15
8.2 1.73 5.0-1 1.9
19
15.4
11.2-22.0 19
2.81
17.8
14.4-21.8 15
2.92
75 9.7
60-97 19
116 12.1 94-137 19
137
110-169 18.4
17
109 18.6 83-149 19
133
103-190 24.2
19
131 22.2 96-172 15
( p < 0.05) and the patients also broke off the test at a higher HR when sitting, the mean difference being 12.6 beats/min ( ~ ( 0 . 0 1 ) .
W170, which reflects the relationship between load and steady state HR, was on an average 140 kpm/min lower in the sitting position ( p < O.OS), so on identical loads these patients usually worked with a lower H R in the supine than in the sitting position. When W170 (in the sitting position) was related to THb, it was within nor- mal limits in nine cases but below normal in eight. In six of the latter, W1,o was also low in rela- tion to heart volume.
Catheterization data obtained at rest and dur- ing exercise are presented in Tables I1 and I11 and Figs. 2-7. The relative physiological stress during work, expressed as percentage of HR,, recorded previously, was for the highest work load 97.8 % .
The mean data on cardiac output are given in Table 11. Cardiac output was linearly related to oxygen uptake at rest (~(0.01) and during exercise (p < 0.001), and there was no significant difference in regression lines between patients with obesity and ordinary subjects. Individual val- ues are plotted against oxygen uptake in Fig. 2. At rest the cardiac output was increased in two patients and low in another. During exercise- when, in all cases but four, two determinations were made-one of those measurements demon- strated high values in three individuals. The re-
Acta med. scand. 193
maining 31 observations were normal in relation to oxygen uptake.
Average data on stroke volume (SV) at rest and during exercise will be found in Table 11. The mean increase on transition from rest to work was 22% ( p < O . O l ) , which is slightly higher than in normal individuals, who averaged 13 % (15). The variation is wide, however, and among the obese subjects even a slight decrease was ob- served in three cases. During continued exercise the SV remained unchanged.
SV during exercise is related to THb and HV in Figs. 3 and 4. A large SV in relation to THb was found in one patient (no. 9), while two had small SV (nos. 1 and 14). The relation to HV demonstrates a rather wide scatter of the values, probably due to the error in HV determination. SV was large in two patients (nos. 9 and 17) and one had an upper borderline value (no. 16). Five patients (nos. 1, 13, 14, 15 and 17) had small SV in relation to HV. In cases 15 and 17, however, one of the determinations was within normal limits.
During exercise the pressures attained higher values in the obese patients than in healthy con- trols (Figs. 5-8). The difference in regression CO-
efficients was statistically significant (p < 0.001) for right ventricle pressures and for pulmonary artery pressures (Figs. 5-6), but there was no dif- ference between the two groups in the slope of the regression lines of PCV pressure and brachial

Cardiovascular function in extreme obesity 441
Table 111. Pressures (mmHg) at rest and during supine exercise RV=right ventricle, PA = pulmonary artery, PCV = pulmonary capillary vein, BrA = brachial artery, S = systolic, D = diastolic, D, = end-diastolic, M = mean pressure
RV, Rv,, PA, PA, PA, PCV BrA, BrA, BrA,
Rest Mean +S.D. Range n
Load I Mean +S.D. Range n
Load I1 Mean S.D.
Range n
28 0.1
17-32 17
47 7.9
37-59 6a
55 10.5 39-67 14
9 2.8 2-14
17
12 4.1 4-16 6a
12 3.6 4-2 1
14
25 3.9
16-31 19
43 10.2 29-60 18
48 7.7
38-70 13
13 3.0 9-19
19
23 6.6
1&36 18
27 4.4
21-37 13
18 3.4
11-23 19
32 8.2
18-47 18
34
21-50 7.1
15
12 3.6 6-19
19
21 7.3 7-32
17
21 6.9 8-3 1
11
143
1 12-202 22.1
19
184
149-272 29.3
17
196 28.4
17 153-257
81 11.5 59-103 19
94 12.0 77-127 17
99 11.1 77-121 17
106 16.1 77-142 19
126
101-193 22.3
16
133 15.3
17 99-167
a Catheter not withdrawn from PCV position in the remaining cases.
artery pressure on cardiac output (Figs. 7-8). However, when testing the distance between the two lines, statistically significant differences (p<O.OOl) were also found for PCV pressure and brachial artery systolic, mean and diastolic pres- sures.
The difference between pulmonary artery mean pressure and PCV pressure increased linearly with cardiac output (pt0.001). This rise was more marked in the obese group than in healthy sub- jects (p<O.O5), and the mean fall in pulmonary vascular resistance index from 0.81 at rest to 0.75 during exercise was less than in healthy con- trols.
Cardiac output,I/min
DISCUSSION Obesity is defined as overweight due to an in- crease mainly in the amount of adipose tissue. Fat is an important and active tissue from a meta- bolic point of view. In obese subjects, for in- stance, the basic metabolic rate is positively cor- related to total body weight (30). The basal blood flow in subcutaneous adipose tissue is of the same order as in resting skeletal muscle and, at least under experimental conditions, the flow capacity may be increased considerably (22, 31). In obesity the total blood flow to fat depots is considered to form an important fraction of the cardiac out- put, contributing to the reported high resting out- put of obese subjects (2).
Fig. 2. Relation between cardiac output and oxygen uptake at rest (n= 19) and during supine exercise (n = 34). Symbols and re- gression line as in Fig. 1.
Oxygen uptake, ml STPD/min
-, 500 1000 1500 2000 2500
Acta med. scand. 193
442 L. Backman et al.
Stroke volume, ml
J
180-
-
160-
- 140-
-
120-
- 100-
-
80-
0
/ 0 0 /
/ /
/
/ /
/ Total amount of hemoglobin,g
I 1 1 I I > 500 709 900 1100
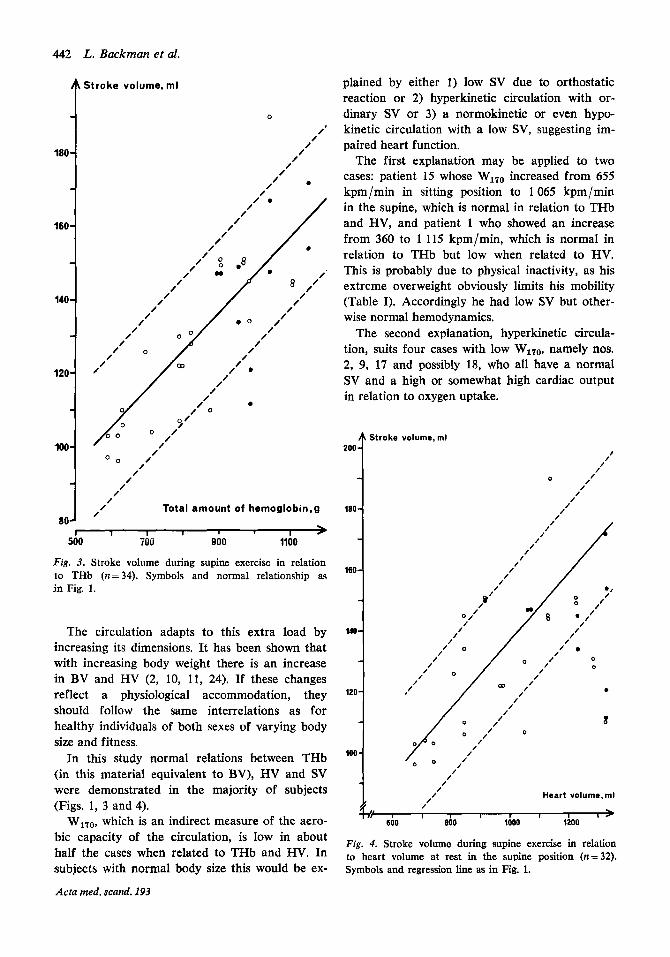
Fig. 3. Stroke volume during supine exercise in relation to THb (n=34). Symbols and normal relationship as in Fig. 1.
The circulation adapts to this extra load by increasing its dimensions. It has been shown that with increasing body weight there is an increase in BV and HV (2, 10, 11, 24). If these changes reflect a physiological accommodation, they should follow the same interrelations as for healthy individuals of both sexes of varying body size and fitness.
In this study normal relations between THb (in this material equivalent to BV), HV and SV were demonstrated in the majority of subjects {Figs. 1, 3 and 4).
WlT0, which is an indirect measure of the aero- bic capacity of the circulation, is low in about half the cases when related to THb and HV. In subjects with normal body size this would be ex-
Acta med. scand. 193
plained by either 1) low SV due to orthostatic reaction or 2) hyperkinetic circulation with or- dinary SV or 3) a normokinetic or even hypo- kinetic circulation with a low SV, suggesting im- paired heart function.
The first explanation may be applied to two cases: patient 15 whose W170 increased from 655 kpm/min in sitting position to 1065 kpm/min in the supine, which is normal in relation to THb and HV, and patient 1 who showed an increase from 360 to 1 115 kpm/min, which is normal in relation to THb but low when related to HV. This is probably due to physical inactivity, as his extreme overweight obviously limits his mobility (Table I). Accordingly he had low SV but other- wise normal hemodynamics.
The second explanation, hyperkinetic circula- tion, suits four cases with low W170, namely nos. 2, 9, 17 and possibly 18, who all have a normal SV and a high or somewhat high cardiac output in relation to oxygen uptake.
200
180
160
140
120
100
Stroke
f I I I 1 I I ,
1200 I - I
600 800 I000
Fig. 4. Stroke volume during supine exercise in relation to heart volume at rest in the supine position (n= 32). Symbols and regression line as in Fig. 1.

Cardiovascular function in extreme obesity 443
Fig. 5. Relation between right ventricle systolic, P E V ~ (a), and end-diastolic pres- sure, P w D e ( 0 ), and cardiac output at rest and during exercise in the supine posi- tion ( n = 36). Full heavy line and shaded area repre- sent the regression 2 S.D. found in ordinary subjects (7, 15, 20). Full thin line indicates regression for obese subjects.
Thirdly, in four patients, nos. 5, 10, 13 and 14, the reason may be an impaired heart function. Patients 5, 13 and 14 have a large HV, small SV, and filIing pressures of the left ventricle which were among the highest obtained in these patients. The fourth patient, no. 10, had a nor- mal SV, but myocardial insufficiency is likely, as she also had an elevated filling pressure. Besides, the most elevated arterial pressures were found in cases 5, 10 and 14, in the two latter thus con- firming the clinical diagnosis of hypertension. In patients 14 and 10 left ventricle dysfunction was also revealed by a pathological ECG reaction dur- ing work.
It cannot be ruled out that the heart volumes to some degree are overestimated due, as already mentioned, to an increased error of the method owing to inclusion of epicardial fat in the volume. On the other hand no bias is obvious when HV is related to THb, and the importance of this error, which is emphasized by some authors (24), is considered less important by others (5, 10, 11).
The normal relationship between oxygen up- take and cardiac output found in this study both at rest and during exercise means that there is an ordinary adjustment of the cardiac output to the oxygen demands.
Regression lines as in Fig. 5. between cardiac output and oxygen consumption
Acta med. scand. 193
444 L. Backman et al.
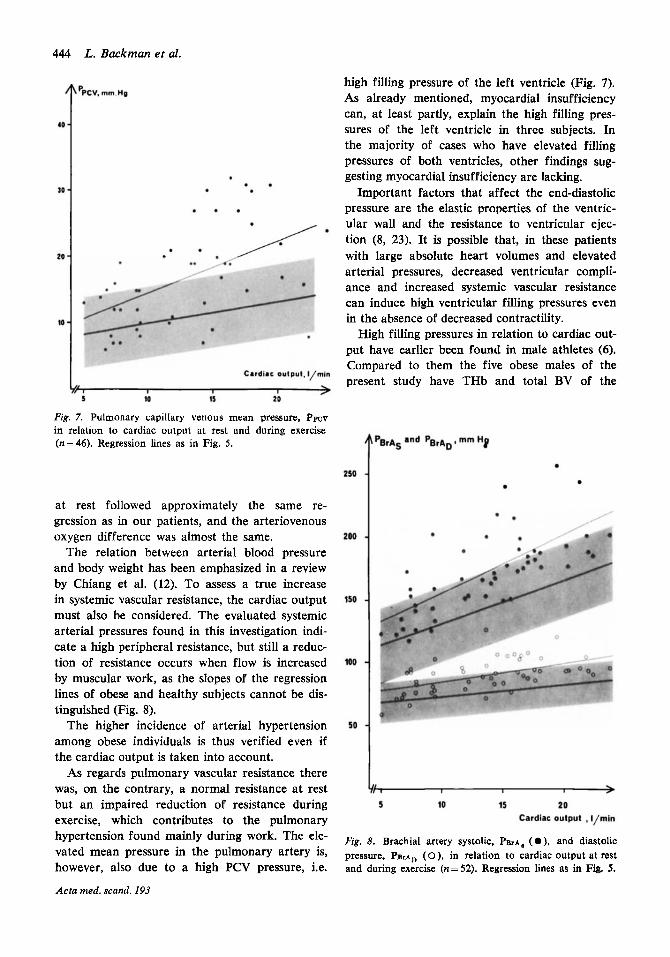
high filling pressure of the left ventricle (Fig. 7). As already mentioned, myocardial insufficiency can, at least partly, explain the high filling pres- sures of the left ventricle in three subjects. In the majority of cases who have elevated filling pressures of both ventricles, other findings sug- gesting myocardial insufficiency are lacking.
Important factors that affect the end-diastolic pressure are the elastic properties of the ventric- ular wall and the resistance to ventricular ejec- tion (8, 23). It is possible that, in these patients with large absolute heart volumes and elevated arterial pressures, decreased ventricular compli- ance and increased systemic vascular resistance can induce high ventricular filling pressures even in the absence of decreased contractility.
High filling pressures in relation to cardiac out- put have earlier been found in male athletes (6). Compared to them the five obese males of the present study have THb and total BV of the
Fig. 7. Pulmonary capillary venous mean pressure, Ppcv in relation to cardiac output at rest and during exercise (n= 46). Regression lines as in Fig. 5.
at rest followed approximately the same re- gression as in our patients, and the arteriovenous oxygen difference was almost the same.
The relation between arterial blood pressure and body weight has been emphasized in a review by Chiang et al. (12). To assess a true increase in systemic vascular resistance, the cardiac output must also be considered. The evaluated systemic arterial pressures found in this investigation indi- cate a high peripheral resistance, but still a reduc- tion of resistance occurs when flow is increased by muscular work, as the slopes of the regression lines of obese and healthy subjects cannot be dis- tinguished (Fig. 8).
The higher incidence of arterial hypertension among obese individuals is thus verified even if the cardiac output is taken into account.
As regards pulmonary vascular resistance there was, on the contrary, a normal resistance at rest but an impaired reduction of resistance during exercise, which contributes to the pulmonary Cardiac output , I/min
hypertension found Fig. 8. Brachial artery systolic, PB~A, ( O ) , and diastolic vated mean pressure in the pulmonary artery is, pressure, P B ~ A ~ (O), in relation to cardiac output at rest however, also due to a high PCV pressure, i.e. and during exercise (n=52). Regression lines as in Fig. 5.
Acta med. scand. I93
during work' The

Cardiovascular junction in extreme obesity 445
same order. The range of SV during exercise was for the athletes 149-180 ml and for the obese males 112-172 ml. There is no difference at rest in filling pressure of the left ventricle between the obese males and the athletes, but during exer- cise two obese males seem to follow the same relation to cardiac output as the athletes and three show a marked increase in filling pressure.
Increased circulatory dimensions can thus, per se, contribute to the raised filling pressures, but it is likely that decreased ventricular compliance and/or impending heart failure are the main rea- sons. It has also recently been found that, al- though weight reduction in patients with obesity is accompanied by decreased blood and heart vol- umes, the filling pressure of the left ventricle re- mains unchanged (3).
In conclusion, the present study demonstrates, in the majority of the patients, an adequate ac- commodation of circuIatory dimensions and car- diac output to the metabolic demands. The hemo- dynamic findings, however, reveal increased sys- temic and pulmonary vascular resistance, which brings about an increased load on the central circulation and may lead to impaired heart func- tion.
REFERENCES
1. Alexander, J. K.: Obesity and cardiac performance. Amer. J. Cardiol. 14: 860, 1964.
2. Alexander, J. K., Dennis, E. W., Smith, W. G., Amad, K. H., Duncan, W. C. & Austin, R. C.: Blood volume, cardiac output and distribution of systemic blood flow in extreme obesity. Cardiovasc. Res. Cent. Bull., Bay- lor Univ. Sch. Med. 1: 39, Winter 1962-63.
3. Alexander, J. K. & Peterson. K. L.: Cardiovascular effects of weight reduction. Circulation 45: 310, 1972.
4. Alexander, J. K. & Pettigrove, J. R.: Obesity and congestive heart failure. Geriatrics 22: 101, 1967.
5. Amad, K. H., Brennan, J. C. & Alexander, J. K.: The cardiac pathology of chronic exogenous obesity. Circulation 32: 740, 1965.
6. Bevegird, S., Holmgren, A. & Jonsson, B.: Circula- tory studies in well trained athletes at rest and during heavy exercise with special reference to stroke volume and the influence of body position. Acta physiol. scand. 57: 26, 1963.
7. - Effect of body position on the circulation at rest and during exercise, with special reference to the in- fluence on the stroke volume. Acta physiol. scand. 49: 279, 1960.
8. Braunwald, E. & Ross, J., Jr: The ventricular end- diastolic pressure. Appraisal of its value in the re-
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
cognition of ventricular failure in man. Editorial, Amer. J. Med. 34: 147, 1963. Burwell, S., Robin, E. D., Whaley, R. D. & Bickel- mann, A. G,: Extreme obesity associated with al- veolar hypoventilation. A Pickwickian syndrome. Amer. J. Med. 21: 811, 1956. Cermak, J.: Das Herzvolumen bei Fettleibigen. Arch. Kreislaufforsch. 47: 234, 1965. CermBk, J. & Bosik, V.: Das Herzvolumen bei Fett- leibigen. Arch. Kreislaufforsch. 62: 12, 1970. Chiang, B. N., Perlman, L. V. & Epstein, F. H.: Overweight and hypertension. A review. Circulation 39: 403, 1969. yon Dobeln, W.: Anthropometric determination of fat-free body weight. Acta med. scand. 165: 37, 1959. - Om begreppet overvikt. Lakartidningen 61: 3988, 1964.
Ekelund, L.-G. & Holmgren, A.: Central hemodyna- mics during exercise. Circulat. Res., Suppl. 1: 33, 1967. Estes, E. H., Jr, Sieker, H. O., McIntosh, H. D. & Kelser, G. A,: Reversible cardiopulmonary syndrome with extreme obesity. Circulation 16: 179, 1957. Ggitzsche, H. & Posborg Petersen, V.: Obesity asso- ciated with cardiopulmonary failure-the Pickwickian syndrome. Acta med. scand. 161: 383, 1958. Hald, A.: Statistical theory with engineering applica- tions, pp. 571-579. Wiley, New York 1960. Holmgren, A. & Ekelund, L.-G.: Determination of total blood volume. In: Clinical physiology (ed.: T. Sjostrand), pp. 241-245. Svenska Bokforlaget, Stock- holm 1967. Holmgren, A., Jonsson, B. & Sjostrand, T.: Circula- tory data in normal subjects at rest and during exer- cise in the recumbent position, with special reference to the stroke volume at different work intensities. Acta physiol. scand. 49: 343, 1960. Kjellberg, S. R., Rudhe, U. & Sjostrand, T.: The relation of the cardiac volume to the weight and surface area of the body, the blood volume and the physical capacity for work. Acta radiol. 31: 113, 1949. Larsson, 0. A., Lassen, N. A. & Quaade, F.: Blood flow through human adipose tissue determined with radioactive Xenon. Acta physiol. scand. 66: 337, 1966. Ross, J. & Braunwald, E.: The study of left ventric- ular function in man by increasing resistance to ven- tricular ejection with angiotensin. Circulation 29: 739, 1964.
24. Schwalb, H. & Schimert, G.: Das Herz bei Fett- sucht. Med. Ktin. 65: 1908, 1970.
25. Sjostrand, T.: Changes in respiratory organs of work- men at an ore smelting works. Acta med. scand., Suppl. 196: 687, 1947.
26. - A method for the determination of the total hemo- globin content of the body. Acta physiol. scand. 16: 211, 1948.
27. - Clinical physiology (ed. T. Sjostrand). Svenska Bokforlaget, Stockholm 1967.
Acta med. scand. 193

446 L. Backman et al.
28. Snedecor, G. W.: Statistical methods. Iowa State Col-
29. Wallgren, G., Bager, B. & Okmian, L.: Ventilatory
consumption and pulmonary ventilation in obese sub- lege Press, Iowa 1959. jects. J. appl. Physiol. 20: 197, 1965.
31. Oberg, B. & Rosell, S.: Circulatory responses in adi- insufficiency in an obese girl. Acta paediat. scand. pose tissue during sympathetic stimulation. Acta 54: 288, 1965. physiol. scand., Suppl. 277: 233, 1966.
30. White, R. I., Jr & Alexander, J. K.: Body oxygen
Acra med. scand. 193