cardiac failure by m.a.lateef siddiqui
TRANSCRIPT

CARDIAC FAILURE
1

What is Cardiac Failure / Heart Failure?
• Heart failure is defined as a clinico patholigical condition in which the cardiac muscles are unable to pump out sufficient amount of blood into circulation at a rate that meets the requirements of metabolizing tissues inspite of normal or above normal filling pressures.
• Almost all forms of heart disease may lead to heart failure.
2

Aetiology
• Depending on the origin it is divided into two types
CARDIAC CAUSES (where the lesion is in the heart)
NON CARDIAC CAUSES (due to increased work load)
3

Cardiac Causes
• Depending on the part involved it is further divided into three types
Pericardial Causes
Myocardial Causes
Endocardial Causes
4

Pericardial Causes
• Pericarditis• Haemopericardium• Pyopericardium• Pericardial Effusion
5

Myocardial Causes
• Myocardial Infarction• Myocarditis• Ischemic Heart Disease• Conduction Defects

Endocardial Causes
• Tricuspid Stenosis & Regurgitation• Mitral Stenosis & Regurgitation• Aortic Stenosis & Regurgitation• Pulmonary Stenosis & Regurgitation• Rupture of Cordiae Tendinae• Atrial Septal Defect (ASD)• Ventricular Septal Defect (VSD)
6

Non-Cardiac Causes
• Anaemia• Hypo proteinaemia• Hypertension• Beriberi• Cor pulmonale• Thyrotoxicosis
8

• Cardiac Output = Heart Rate x Stroke Volume
• Changes in Cardiac Output =
Changes in Heart Rate & Changes in Stroke Volume
• Heart Rate is Controlled by
Autonomic Nervous System & Hormonal System
• Stroke Volume is Controlled by
Preload, Afterload and Myocardial Contractility
Patho-Physiology
11

Patho-Physiology
• Cardiac output is the function of Pre load (the stretching of the ventricular myocardium after filling just before contraction), After load (the resistance against which myocardium has to contract and eject the blood out) and Myocardial Contractility, and is controlled by Neuro-Hormonal System
• This forms the basis of Starling’s Law.
12

Patho-Physiology
• Starling’s Law:
The force of
contraction
of heart is directly
proportional to the
initial length of the
muscle fibers before
the onset of
contraction
13

• In Heart failure due to inability of ventricles to fulfill metabolic demand Renin angiotensin aldosterone system gets activated.
• This system causes vasoconstriction, salt and water retention and sympathetic nervous system activation.
• Activation of the sympathetic nervous system may initially maintain cardiac output through an increase in myocardial contractility, heart rate and peripheral vasoconstriction.
Patho-Physiology
14

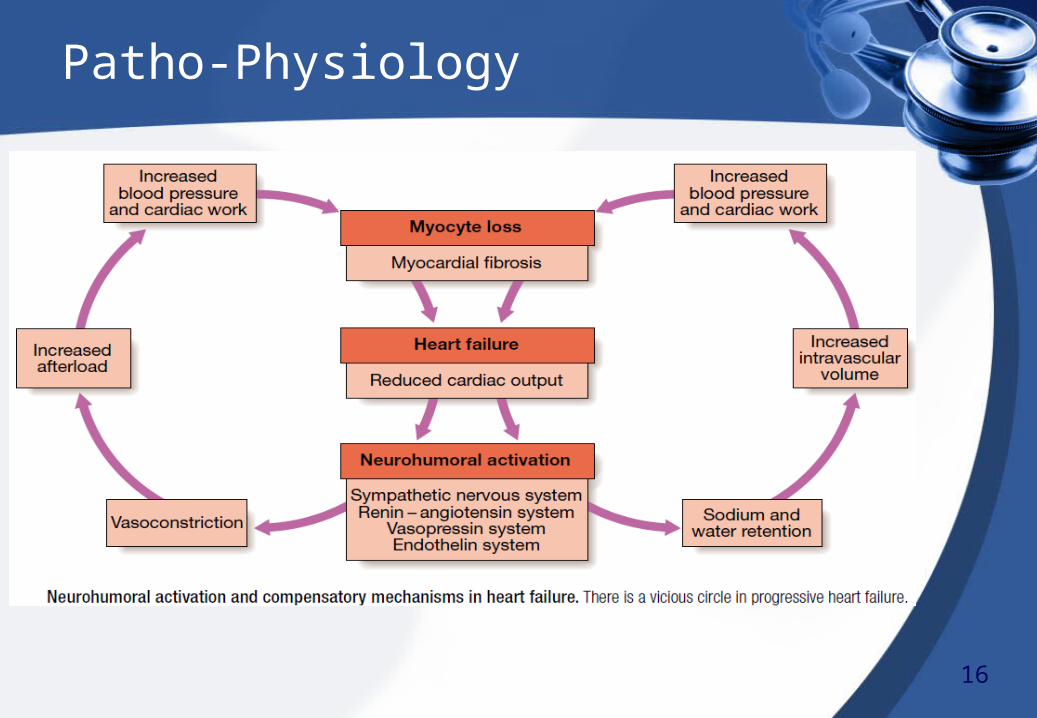
• However, prolonged stimulation often reduce cardiac output by causing an inappropriate and excessive increase in peripheral vascular resistance, cardiac myocyte apoptosis, hypertrophy and focal myocardial necrosis.
• Ultimately a vicious cycle is established which cause further Neuro hormonal activation and increase peripheral vascular resistance.
• The onset of Pulmonary and Peripheral oedema is due to high atrial pressures compounded by salt and water retention.
Patho-Physiology
15
Patho-Physiology
16

Mechanisms of Cardiac Failure
• Reduced Ventricular Contractility• Ventricular outflow obstruction• Ventricular inflow obstruction• Ventricular volume overload• Arrhythmia• Diastolic dysfunction
10

1. Acute and Chronic Heart Failure:• Heart Failure may develop suddenly, as in Myocardial
Infarction known as Acute Heart Failure.
• It may develop in a gradual manner, as in Progressive Valvular Heart Disease known as Chronic Heart Failure.
• In the gradual impairment, a variety of compensatory changes may took place which although initially improve cardiac function, but as the disease progresses they often become counterproductive.
Types of Heart Failure
17

2. Left, Right and Biventricular Heart Failure:• If there is reduction in the Left Ventricular output and/or
increase in Left atrial or pulmonary venous pressure then it is Left sided Heart Failure.
• If there is reduction in the Right Ventricular output for any given Right atrial pressure then it is Right sided Heart Failure.
• Failure of Both Left and Right sided Heart is Biventricular Heart Failure.
Types of Heart Failure
18

Types of Heart Failure
19

3. Forward and Backward Heart Failure:• If in the forward blood circulation there is inadequate
cardiac output then it is Forward Heart Failure.
• In some cases there is normal or near normal cardiac output but with marked salt and water retention causing pulmonary and systemic venous congestion then it is Backward Heart Failure.
Types of Heart Failure
20

4. Systolic and Diastolic Heart Failure:• Systolic Cardiac failure is due to impaired systolic
function or poor ventricular contractility.
• Diastolic Cardiac failure is due to impaired diastole or poor ventricular filling because of abnormal relaxation.
Types of Heart Failure
21

SYMPTOMS:
Left Ventricular Failure• Dyspnoea (Exertional Dyspoea, Orthopnoea, Paroxysmal
nocturnal dyspnoea)• Cough (with pink frothy sputum)• General Weakness• Fatigue
Clinical Features
22

SYMPTOMS:
Right Ventricular Failure• Oedema feet• General Weakness• Fatigue• Anorexia• Nausea• Insomnia
Clinical Features
22

SIGNS:
Left Ventricular Failure• Pulmonary oedema• Pleural effusion• Bilateral basal Creptations• Cardiomegaly• Audible S3, S4 heart sounds• Murmurs• Cheyne’s Strokes Respiration• Pulsus alterans
Clinical Features
23
SIGNS:
Right Ventricular Failure• Peripheral pitting oedema• Raised JVP• Hepatomegaly• Ascites• Murmurs
Clinical Features
23

Classification
• Class I : No limitation of Physical Activity.• Class II : Slight limitation of physical activity, comfortable at
rest. • Class III: Marked limitation of physical activity, comfortable at
rest. Less than ordinary activity causes fatigue,
palpitation, dyspnoea, or anginal pain. • Class IV: Inability to carry on any physical activity without
marked discomfort. Symptoms of heart failure may
be present even at rest. If any physical activity is
undertaken, discomfort is increased.
9
• Renal Failure• Hypokalaemia• Hyperkalaemia• Hyponatraemia• Impaired Liver Function• Atrial and Vetricular Arrhythmias• Shock• Death
Complications
24

• Chest X-Ray• ECG• 2D Echo• TMT• Serum Electrolytes• Serum Urea• Serum Creatinine
Investigations
25

1. Bronchial Asthma:• Dyspnoea is present• It has seasonal attacks• In Bronchial Asthma Cough is followed by Dyspnoea• Basal Creptations are absent but there is wheezing all
over the chest• In X-Ray no Abnormality is detected
Differential Diagnosis
26
2. Pneumonia:• Dyspnoea is present,• In Pneumonia Expectorant Cough is present with high
fever and flushing of face.• Creptations are present in middle and lower zone of Lung• X-Ray shows consolidation in middle and lower zone
29
Differential Diagnosis
27

3. Plueral Effusion:• Dyspnoea is present,• Cough is not prominent.• Movements of chest wall is restricted, chest pain occurs
while inspiration• X-Ray shows opacity in the lower and lateral side of the
chest
Differential Diagnosis
28

4. Renal Disease:• Dyspnoea and Cough are present,• Oedema of upper body especially face is present.• Oliguria is present• Increased Serum Urea and Creatinine• Ultrasound shows degeneration of Renal Parenchyma
Differential Diagnosis
29

Management
General Measures: • Treat the underlying cause• Education of the Patient and attendants• Bed rest• Restricted Salt Diet• Cessation of Alcohol, Smoking• Oxygen Therapy (Acute Condition)
30

Management
Drug Therapy:• Diuretic therapy• Vasodilators• ACE inhibitors• Digoxin• Nitrates• Amiodarone
30
