cardiac devices in the golden years - med.upenn.edu · cardiac devices in the goldencardiac devices...
TRANSCRIPT
Cardiac devices in the GoldenCardiac devices in the Golden Years
All that glittersAll that glitters…
James N. Kirkpatrick, MDCardiovascular Division
Center for BioethicsUniversity of Pennsylvania
Di lDisclosures• No related disclosures
• No industry affiliations
• Grant from Greenwall Foundation: Caregiver Stress in DestinationCaregiver Stress in Destination Ventricular Assist Devices
• 2 NIH Data Safety Monitoring Boards

Outline• Device Therapy for Advanced Heart
Failure• Ethical conflicts/considerations• Complexities of Advance Care Planning• Complexities of Advance Care Planning
in Heart Failure“Shi ” P j t• “Shiny” Projects

MAGAZINE | June 20, 2010| ,
What Broke My Father's Heart By KATY BUTLERBy KATY BUTLER
How putting in a pacemaker wrecked a family's lifefamily s life.
“Th k b ht t t• “The pacemaker bought my parents two years of limbo, two of purgatory and two f h ll ”of hell…”
• “…If we did nothing, his pacemaker would not stop for years. Like the tireless charmed brooms in Disney’s “Fantasia,” it would prompt my father’s heart to beat after he became too demented to speak, sit up or eat.”
Heart FailureHeart Failure23,000,000 worldwide (5.7 million US)( )
Incidence: 500-700,000/year in US
20% of population will get it
Including 11% of patients with no CAD
5-10% NYHA class IV: 13-40% 2 year survival
Swedberg, et al. Eur Heart J. 2005;26(11):1115-40.Lloyd-Jones,DM, et al. Circulation. 2002;106(24):3068–72. Dembitsky WP. Semin Cardiothorac Vasc Anesth 2006; 10:253–255.Rosamond W, et al. Cir 2007 115:e69-171Stevenson, LW. ISHLT Monograph Series, 2006. 1 Chapter 11: p. 181-204.
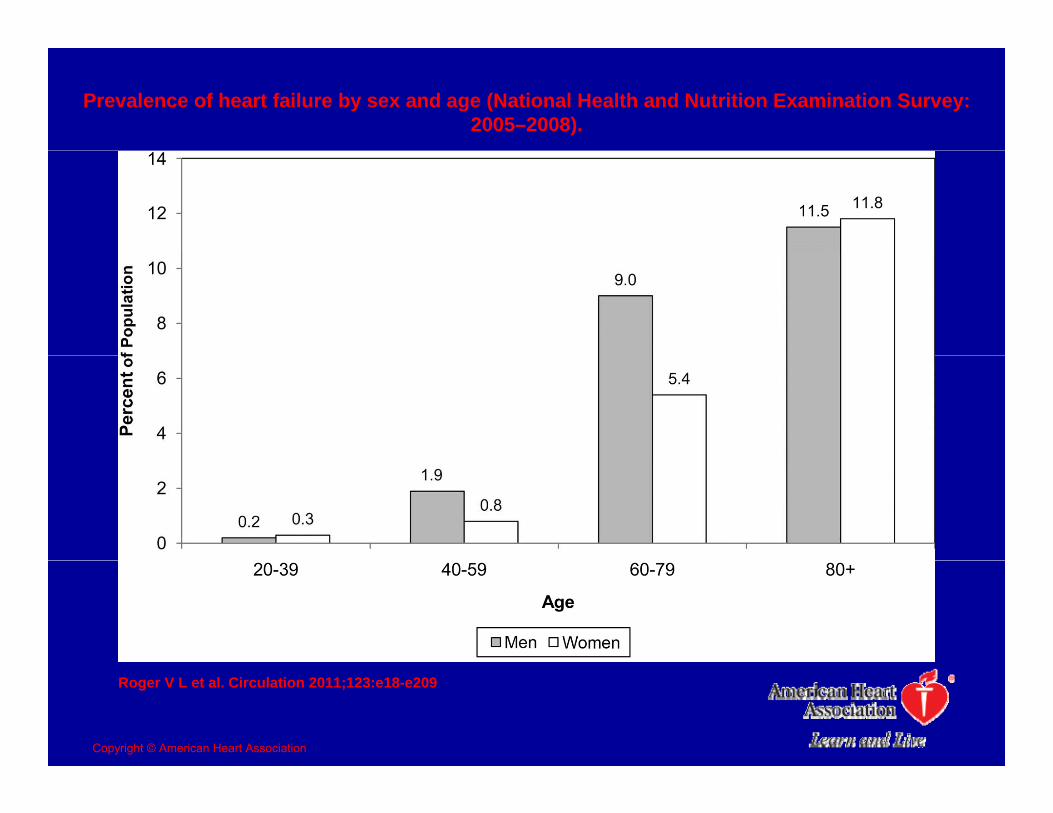
Prevalence of heart failure by sex and age (National Health and Nutrition Examination Survey: 2005–2008).
Roger V L et al. Circulation 2011;123:e18-e209
Copyright © American Heart Association
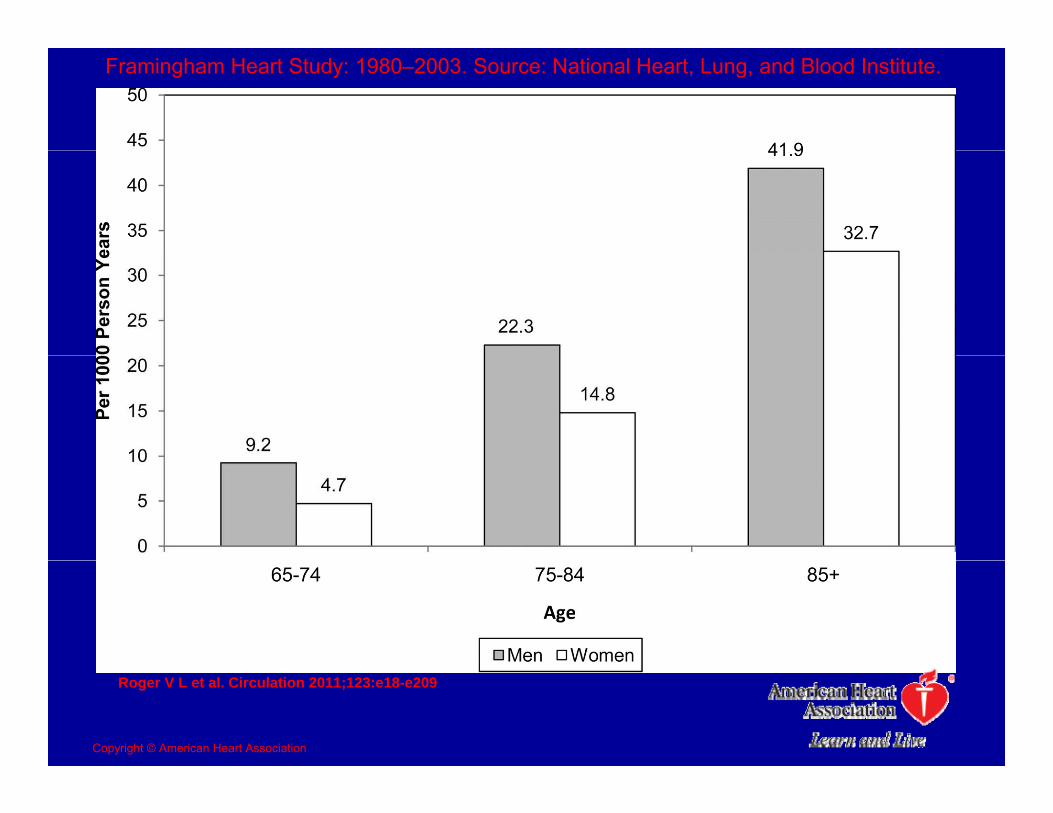
Framingham Heart Study: 1980–2003. Source: National Heart, Lung, and Blood Institute.
Roger V L et al. Circulation 2011;123:e18-e209
Copyright © American Heart Association
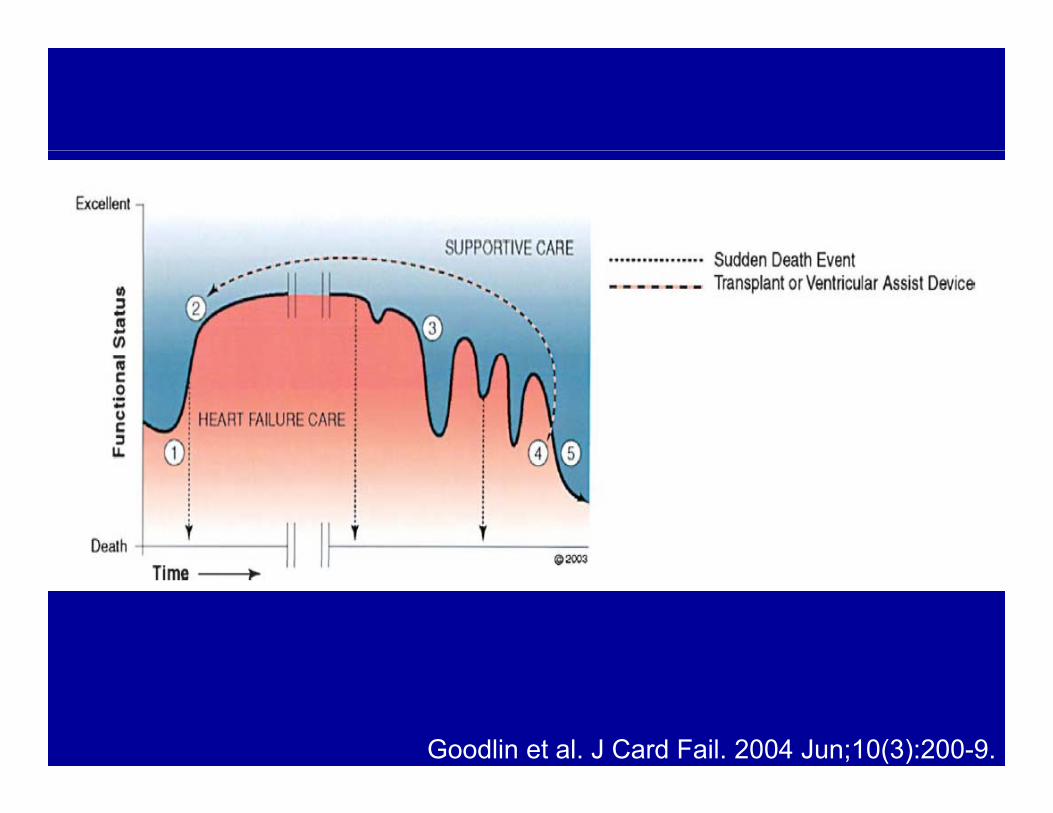
Goodlin et al. J Card Fail. 2004 Jun;10(3):200-9.
“Can vs Do”Can vs. Do
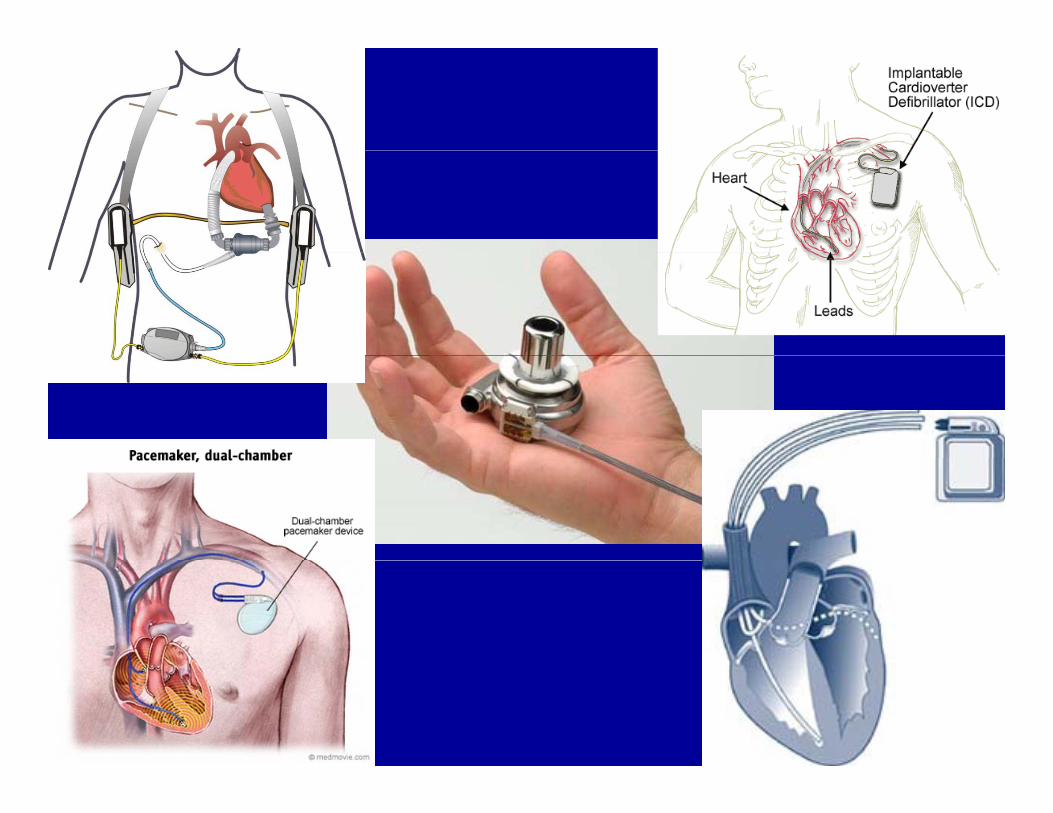
Heart Failure Devices
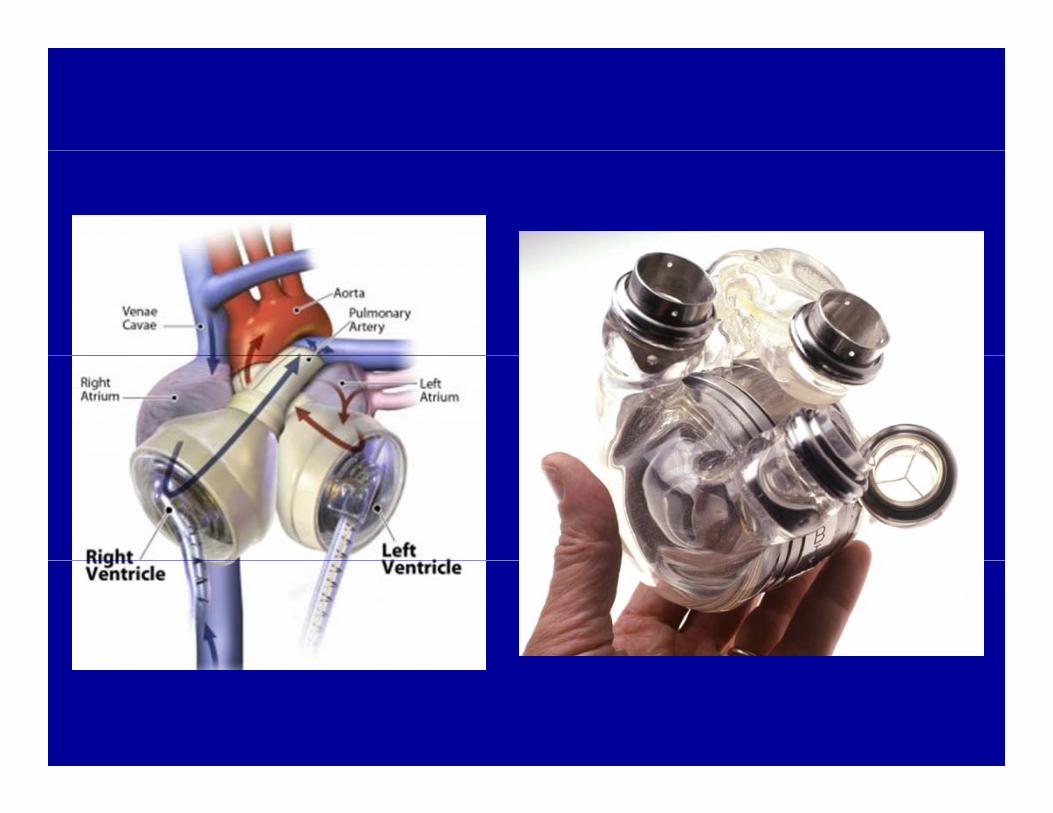
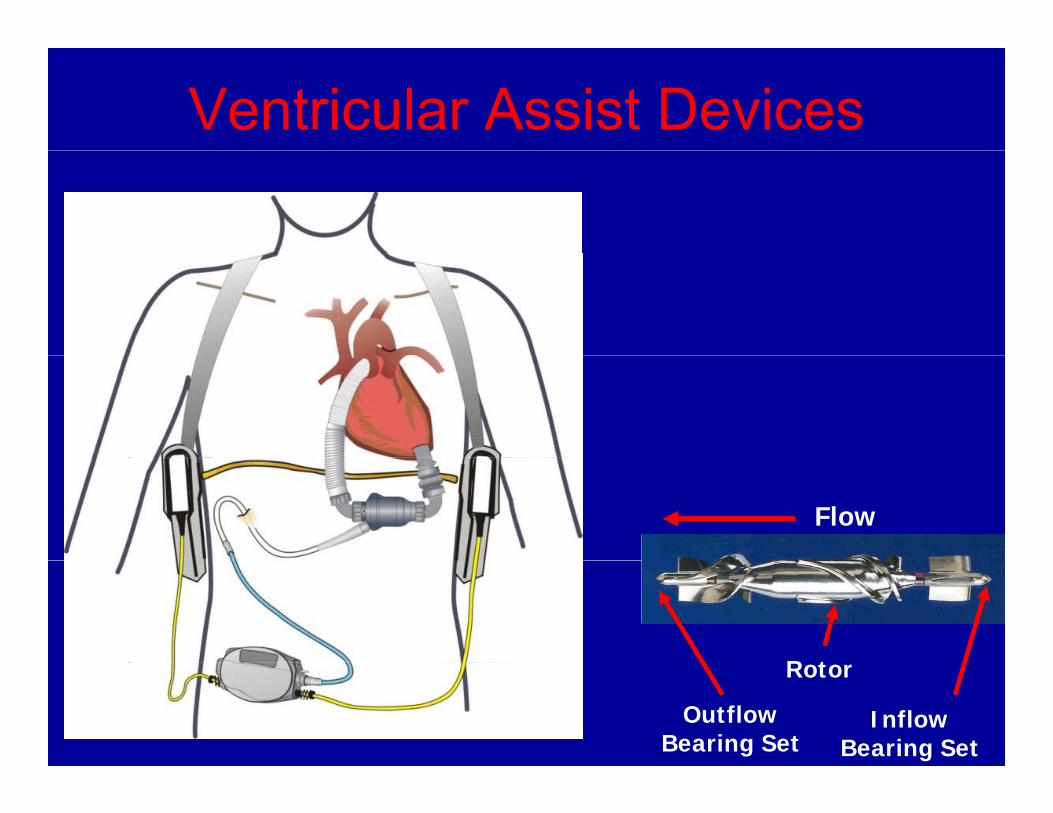
Ventricular Assist Devices
Flow
R t
Inflow Bearing Set
Outflow Bearing Set
Rotor
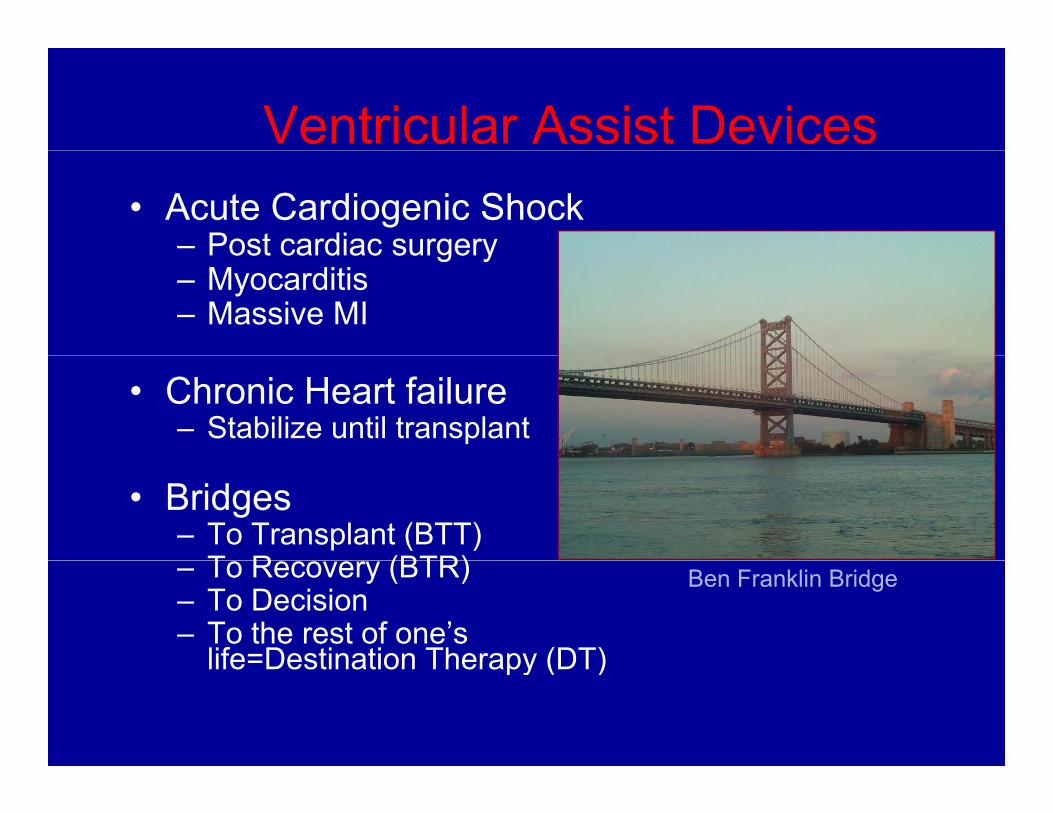
Ventricular Assist Devices• Acute Cardiogenic Shock
– Post cardiac surgeryPost cardiac surgery– Myocarditis– Massive MI
• Chronic Heart failure– Stabilize until transplant
• Bridges– To Transplant (BTT)
T R (BTR)– To Recovery (BTR)– To Decision– To the rest of one’s
life=Destination Therapy (DT)
Ben Franklin Bridge
life Destination Therapy (DT)
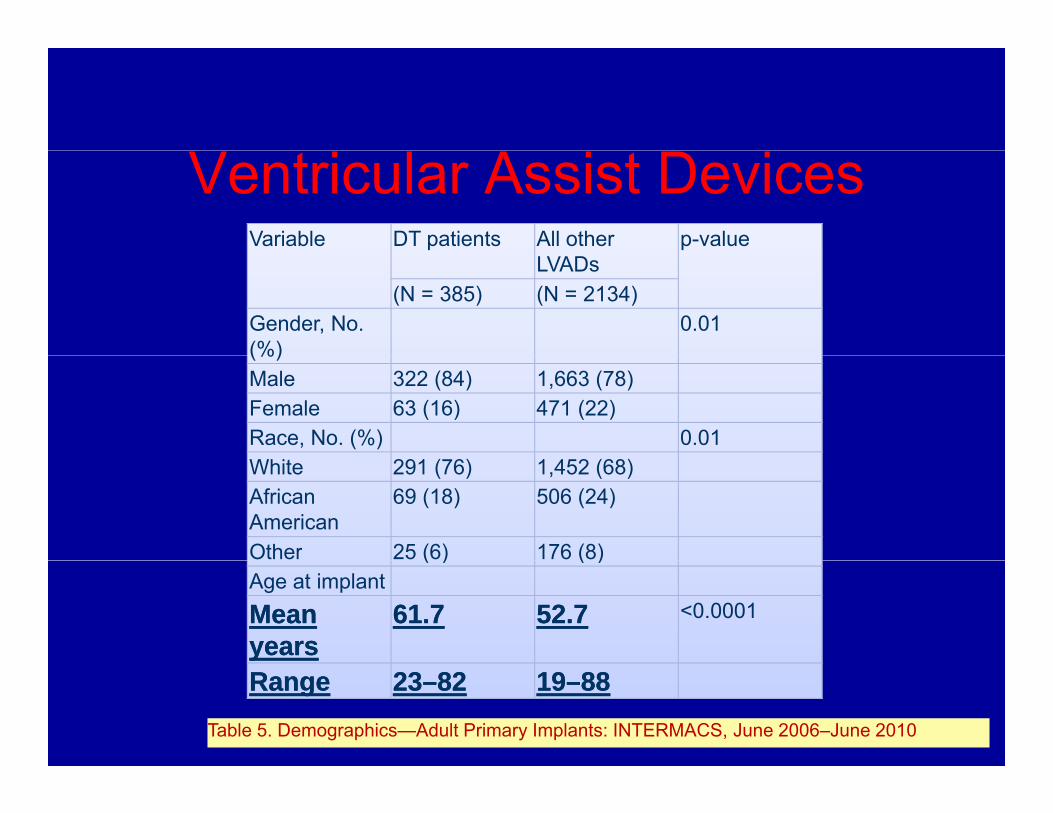
Ventricular Assist DevicesVariable DT patients All other p-value
LVADs(N = 385) (N = 2134)
Gender, No. (%)
0.01(%)Male 322 (84) 1,663 (78)Female 63 (16) 471 (22)Race, No. (%) 0.01White 291 (76) 1,452 (68)African American
69 (18) 506 (24)
Other 25 (6) 176 (8)( ) ( )Age at implantMean Mean yearsyears
61.761.7 52.752.7 <0.0001
RangeRange 2323––8282 1919––8888Table 5. Demographics—Adult Primary Implants: INTERMACS, June 2006–June 2010
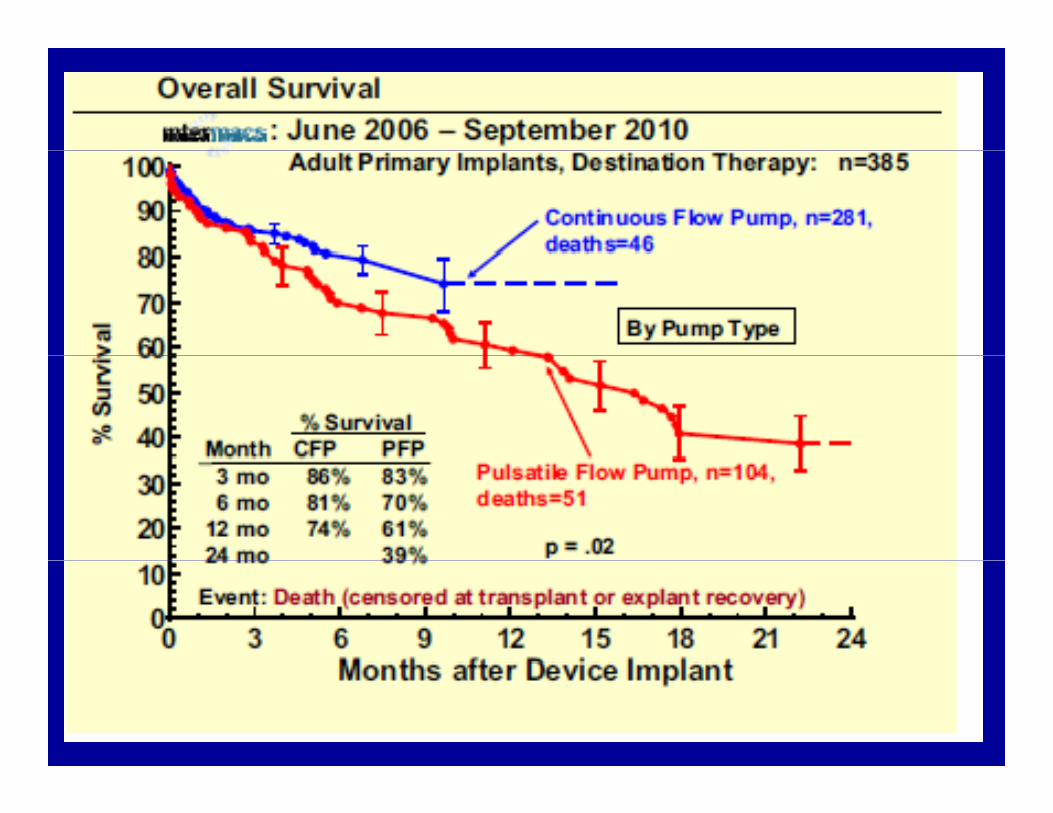
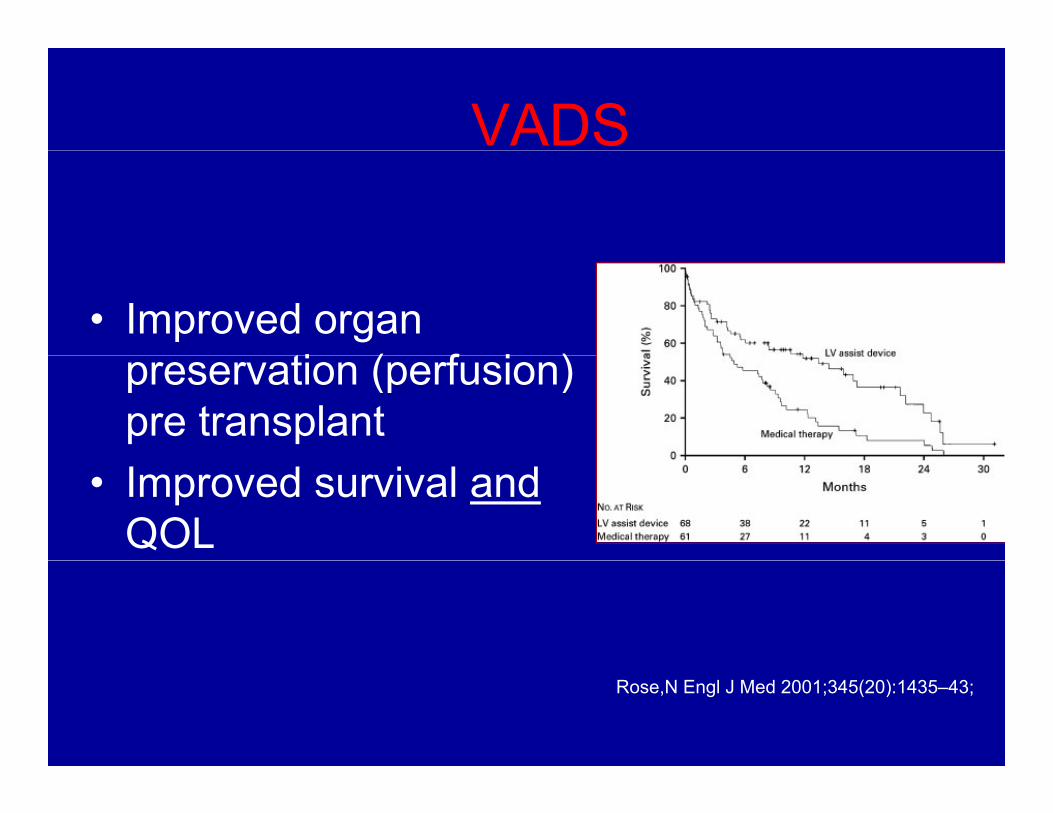
VADS
• Improved organ ti ( f i )preservation (perfusion)
pre transplant• Improved survival and
QOL
Rose,N Engl J Med 2001;345(20):1435–43;
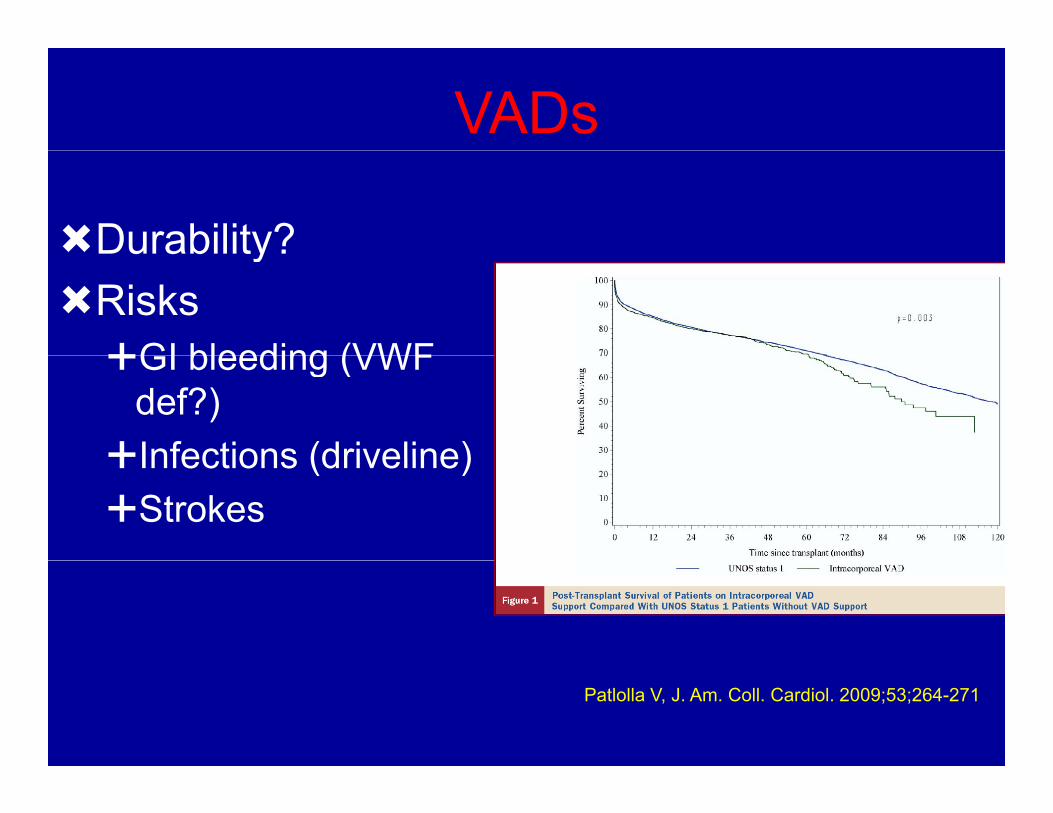
VADs
Durability?Durability?RisksGI bleeding (VWFGI bleeding (VWF
def?)Infections (driveline)Infections (driveline)Strokes
Patlolla V, J. Am. Coll. Cardiol. 2009;53;264-271
Examples of Criteria for Implantable LVAD
for Lifetime SupportC i l B A bl
More objectiveCrucial But Arguable
• “Frailty”• Other Co-morbidities
More objective• Clinical profiles
– Not crash and burn– Not post-surgical– Ambulatory for DT? Other Co morbidities
• Psychosocial limitations• Cognitive limitations• Social support
A ?
Ambulatory for DT?• Renal function-not on dialysis.
eGFR>50* , BUN < 50*• Hepatic function > 2X normal*• Lung function not intubated or on • Age?• Lung function-not intubated or on
home O2 or steroids• Infection - Not on systemic
antibiotics • Nutrition pre albumin >15* albumin• Nutrition- pre-albumin >15*, albumin
> 3*• RV function-not yet defined well• 2 year prognosis
* S*Proposed in:JHLT Supplement2010; 29:4SSlaughter,et al. HMII Investigators Adapted from Lynne Warner Stevenso
PacemakersPacemakers
• Symptomatic• Symptomatic BradycardiaUS I l t• US Implants per year– 250,000
• Increased 50% during the 1990s
Mond, Pacing and Clinical Electrophysiology 2008; 31(9): 1202-1212.
Implantable Cardioverter Defibrillator (ICD)
• 100 000 ICDs implanted/year
Implantable Cardioverter Defibrillator (ICD)
100,000 ICDs implanted/year in USA
Ab i dd di• Aborting sudden cardiac arrest
• Termination of many lethal arrhythmias with antitachycardia pacing (ATP)antitachycardia pacing (ATP)
• Primary prevention andPrimary prevention and secondary prevention
--adapted from Ralph Verdino
Darn
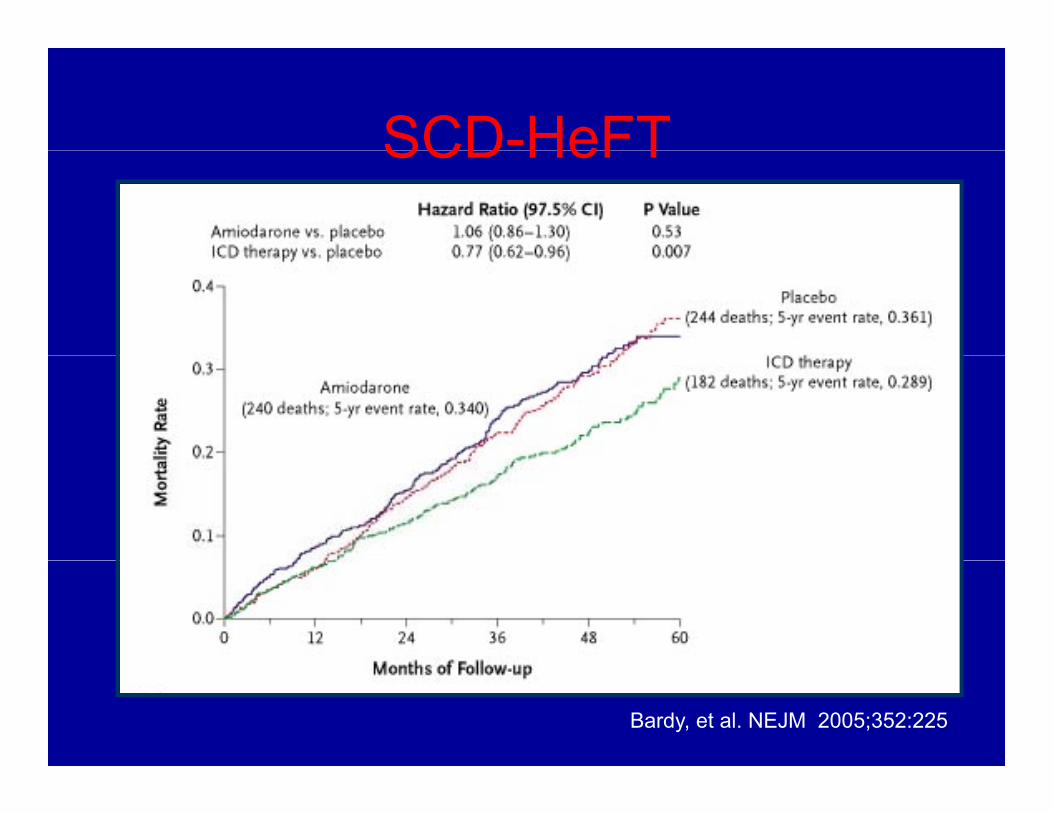
SCD-HeFTSCD HeFT
36%
29%29%
Bardy, et al. NEJM 2005;352:225
ICD
• Inappropriate ShocksInappropriate Shocks– Anxiety
Depression– Depression– ED resource utilization
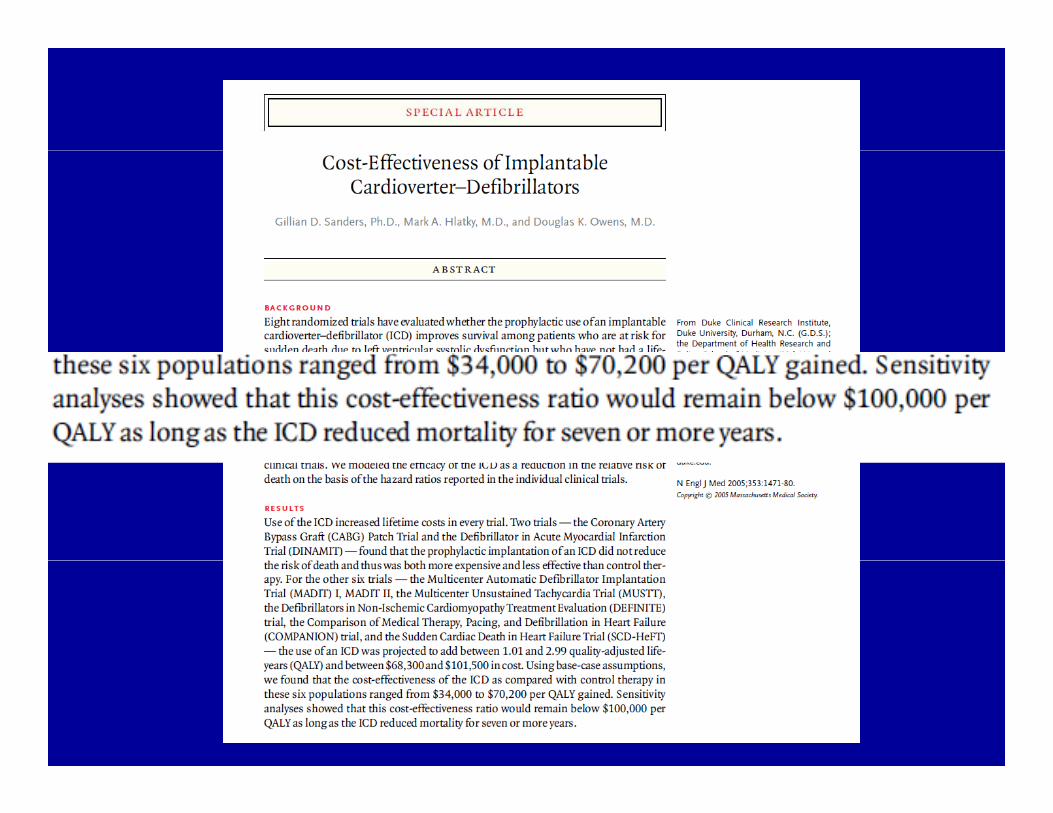
Hunt, Circulation. 2005; 112(12):e154-235 Sanders, et al NEJM, 2005. 353(14): p. 1471-8080 Moss, A.J., et al. NEJM, 1996. 335(26): p. 1933-40.Stevenson, LW. Circ 2006. 114;101-103
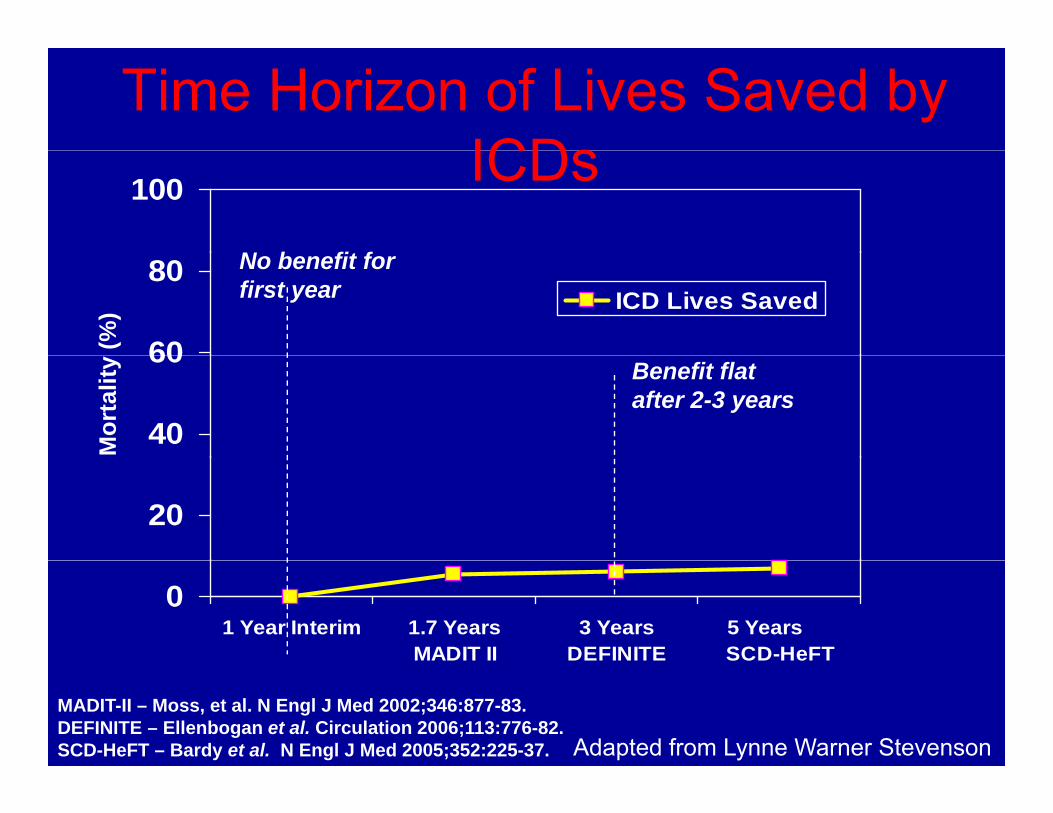
Time Horizon of Lives Saved by ICDsICDs100
N b fit f
60
80ICD Lives Saved
(%)
No benefit forfirst year
40
60
Mor
talit
y Benefit flatafter 2-3 years
20
01 Year Interim 1.7 Years
MADIT II3 Years
DEFINITE5 Years SCD-HeFT
MADIT-II – Moss, et al. N Engl J Med 2002;346:877-83.DEFINITE – Ellenbogan et al. Circulation 2006;113:776-82. SCD-HeFT – Bardy et al. N Engl J Med 2005;352:225-37. Adapted from Lynne Warner Stevenson
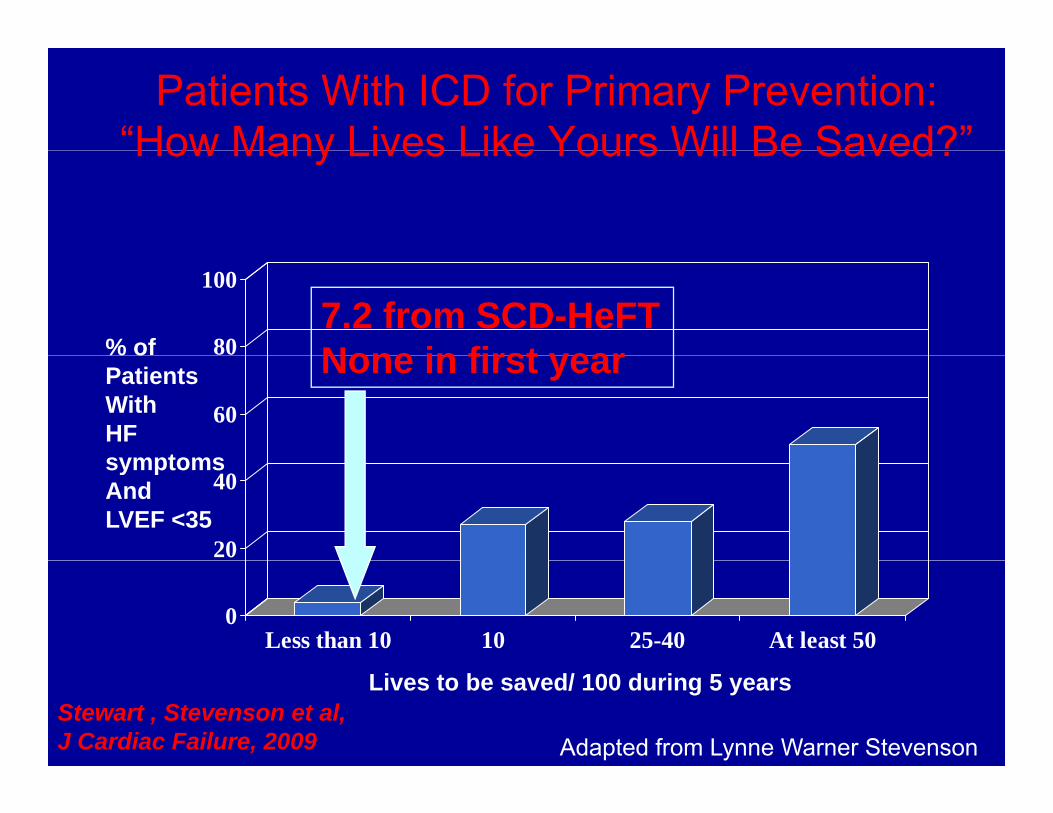
Patients With ICD for Primary Prevention:“How Many Lives Like Yours Will Be Saved?”How Many Lives Like Yours Will Be Saved?
80
100
% of 7.2 from SCD-HeFTNone in first year
60
% oPatientsWith HF symptoms
None in first year
20
40symptomsAnd LVEF <35
0Less than 10 10 25-40 At least 50
Stewart , Stevenson et al, J Cardiac Failure, 2009
Lives to be saved/ 100 during 5 years
Adapted from Lynne Warner Stevenson
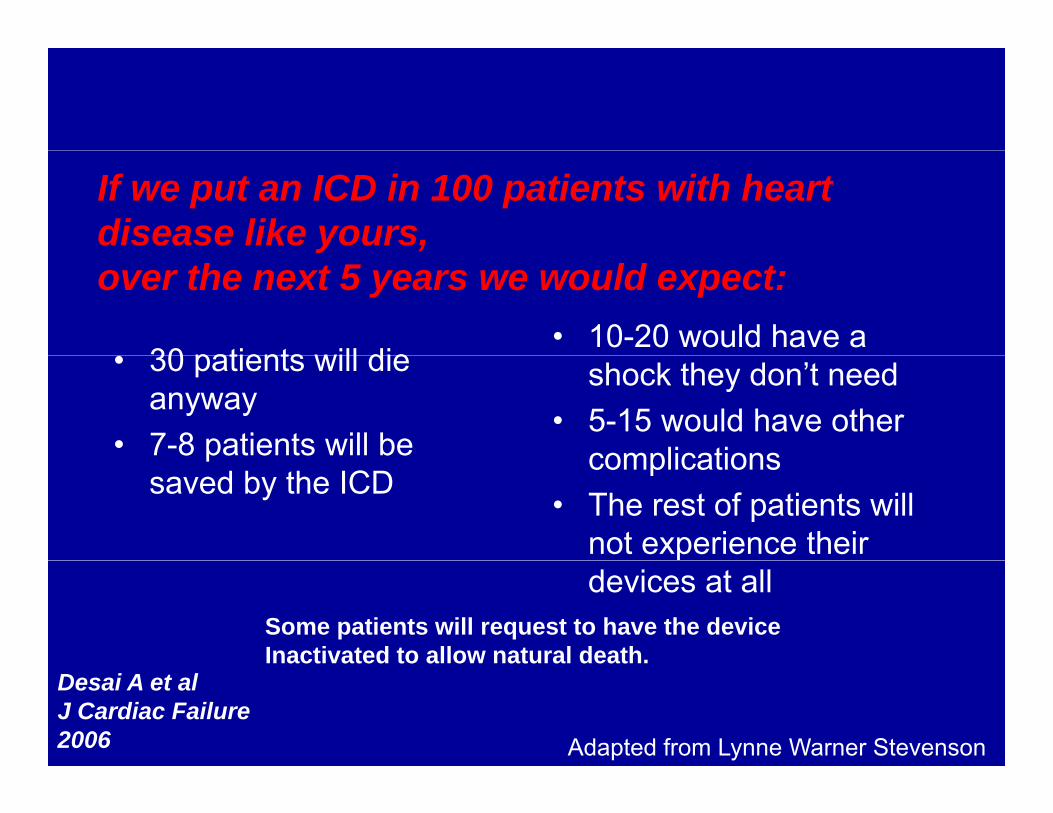
If we put an ICD in 100 patients with heart disease like yours,
30 patients will die• 10-20 would have a
yover the next 5 years we would expect:
• 30 patients will die anyway
• 7-8 patients will be
shock they don’t need• 5-15 would have other
complicationspsaved by the ICD
complications• The rest of patients will
not experience their devices at all
Some patients will request to have the deviceInactivated to allow natural death.Inactivated to allow natural death.
Desai A et alJ Cardiac Failure2006 Adapted from Lynne Warner Stevenson
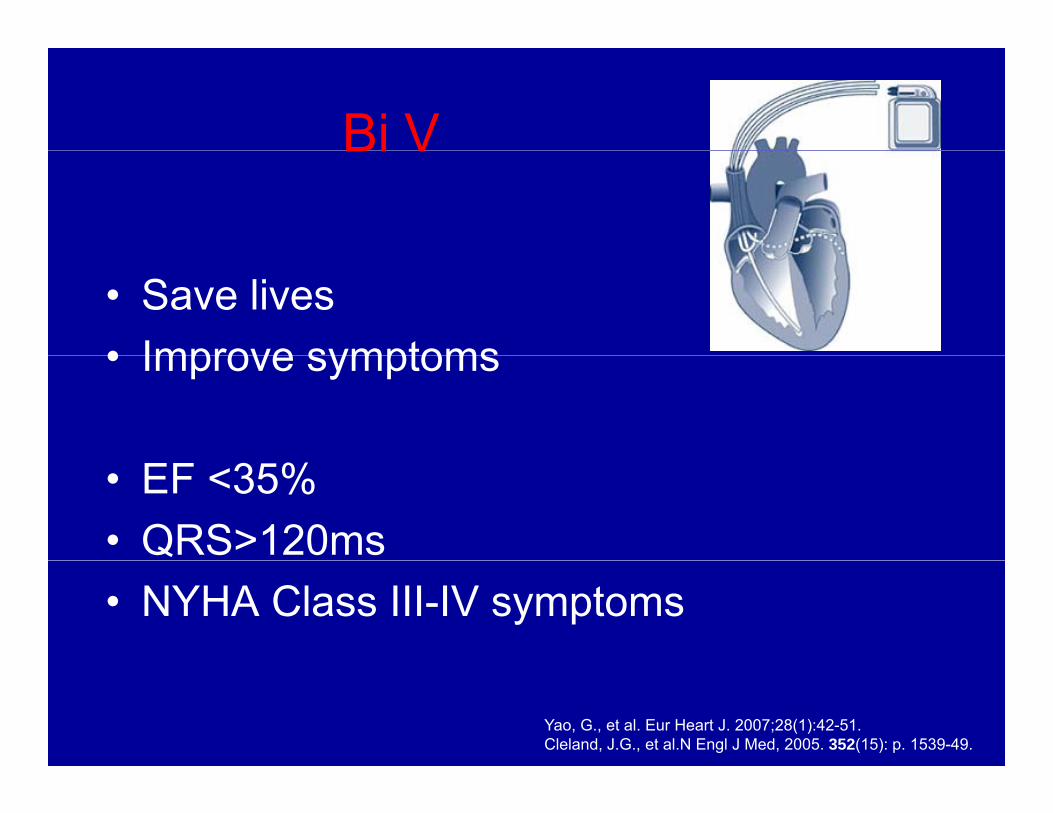
Bi VBi V
• Save lives• Improve symptoms• Improve symptoms
• EF <35%• QRS>120ms• NYHA Class III-IV symptoms
Yao, G., et al. Eur Heart J. 2007;28(1):42-51. Cleland, J.G., et al.N Engl J Med, 2005. 352(15): p. 1539-49.
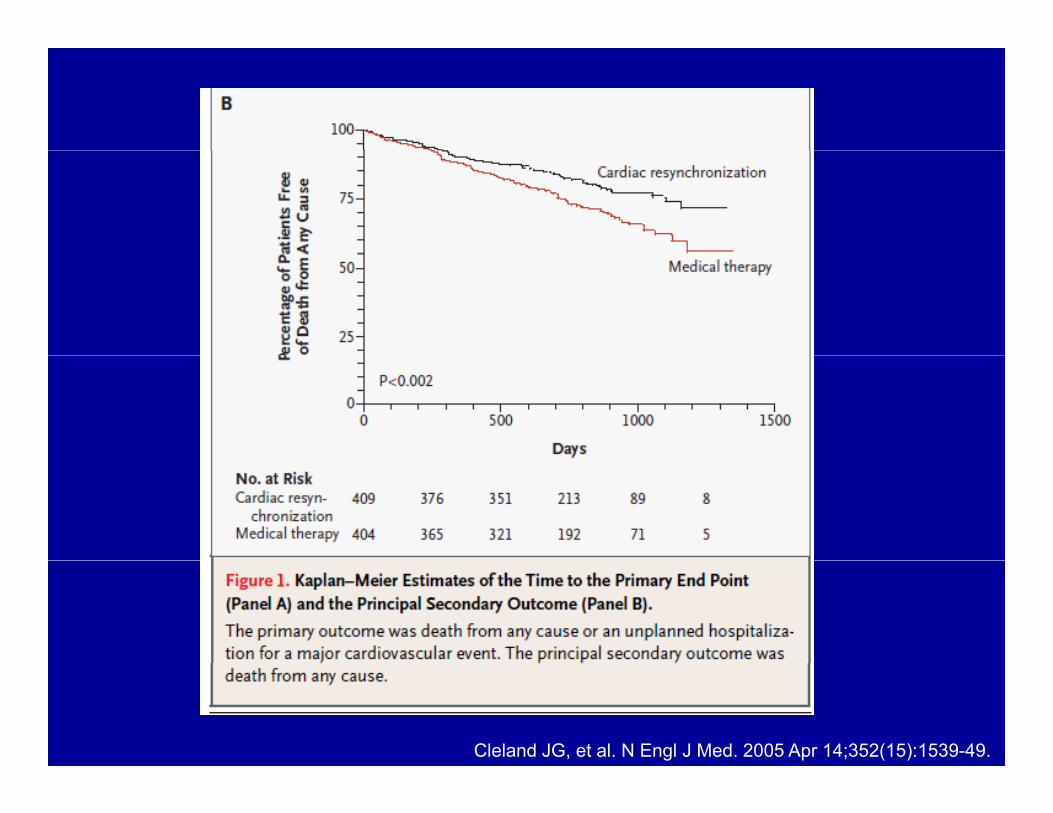
Cleland JG, et al. N Engl J Med. 2005 Apr 14;352(15):1539-49.
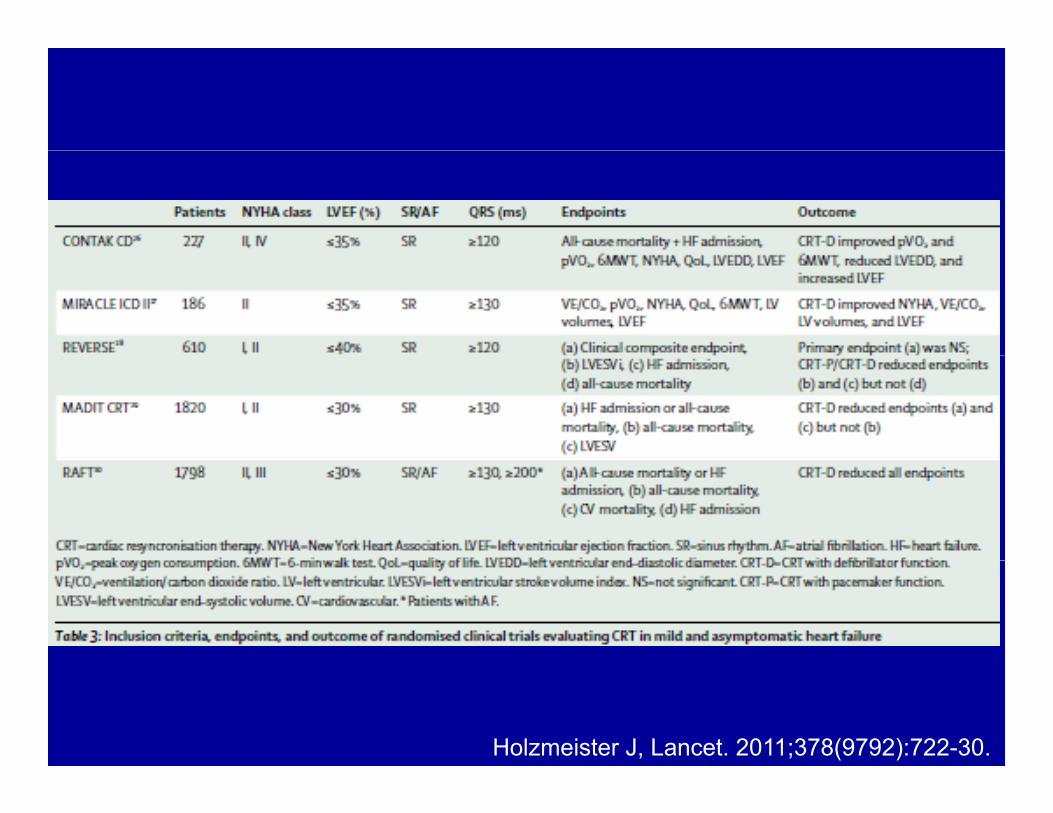
Holzmeister J, Lancet. 2011;378(9792):722-30.
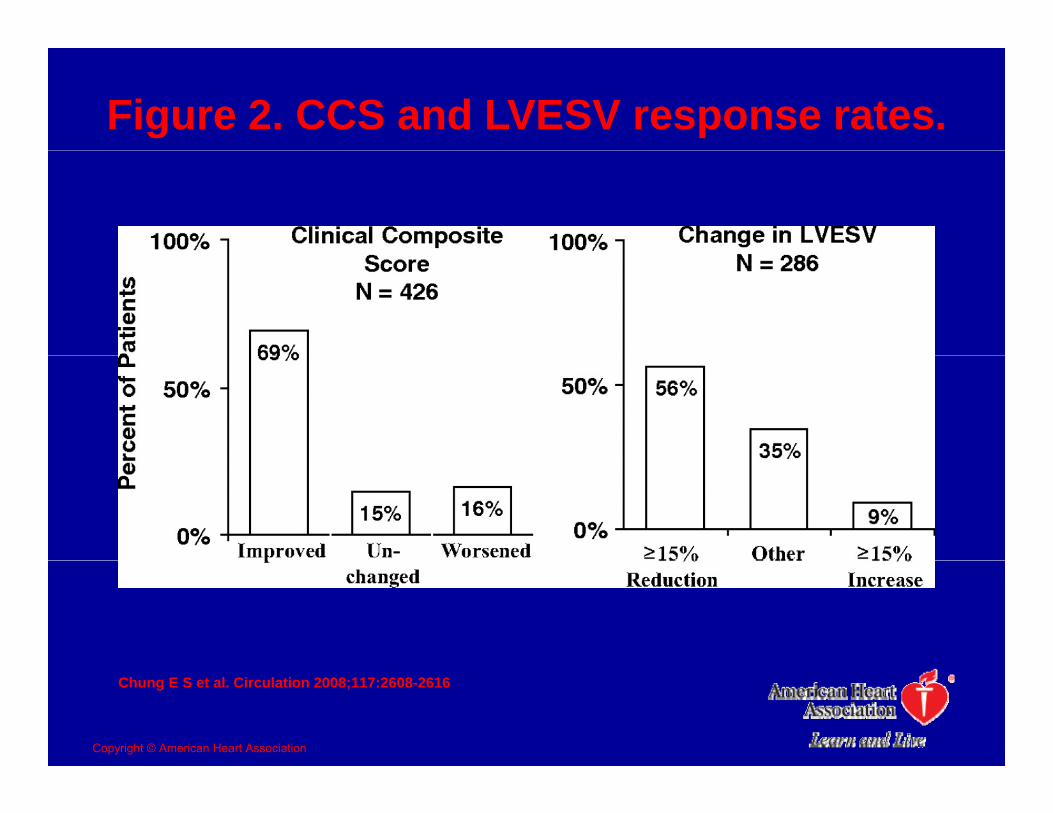
Figure 2. CCS and LVESV response rates.
Chung E S et al. Circulation 2008;117:2608-2616
Copyright © American Heart Association
Implant complications
• 3.2% (CI, 2.8% to 3.6%) – sinus dissection or perforationsinus dissection or perforation– pericardial effusion or tamponade– PneumothoraxPneumothorax– hemothorax
Al‐Majed, Annals of Internal Medicine. 154(6):401‐412, 2011.
“There are no ethical dilemmas; the technology is proved and the patients have shortthe patients have short wretched lives.”
Westaby and Poole-Wilson, BMJ. 2007 334(7586): 167–168
Who gets a VAD?• Transition from “rescue” to “chronic• Transition from rescue to chronic
disease management tool”• How like transplant should it be?• How like transplant should it be?
– Age requirements?– Psychosocial Requirements?Psychosocial Requirements?– Ideal candidacy?– Palliative VAD?Palliative VAD?– VAD “waiting list”?
Discrimination
• Physiological vs. Numerical Age• FinancialFinancial• Social support
Mild d ti• Mild dementia• Addictions
End of Life: When the heart isEnd of Life: When the heart is taken out of the equation…
• Life prolongation• Relief of symptomsRelief of symptomsThere may be more time to consider goals
of careof careThere may be more time for patients and
surrogates to change their minds aboutsurrogates to change their minds about goals of care
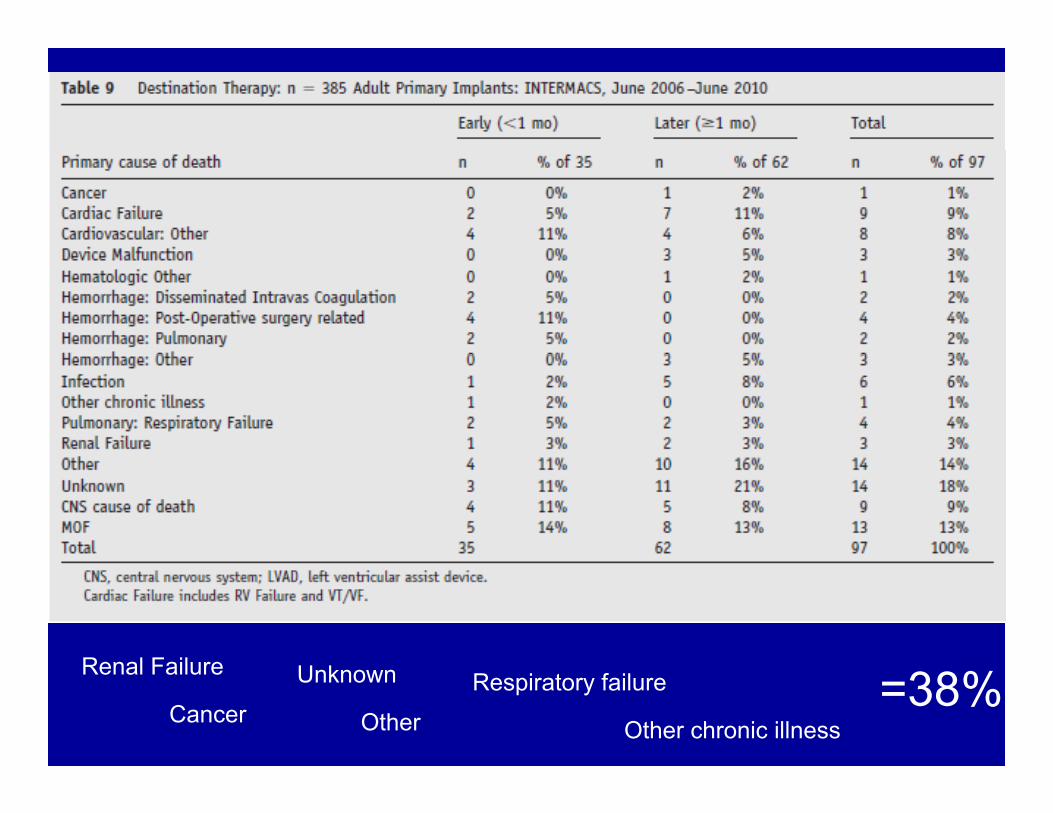
Renal Failure
Cancer
Renal Failure
Other
Unknown
Other chronic illness
Respiratory failure =38%
Palliative and End of Life VAD carecare
• Surgical removal incompatible with palliative care?
• “Letting nature take its course”?• Deactivation as a terminal (planned)Deactivation as a terminal (planned)
event• Physician Assisted Suicide?• Physician Assisted Suicide?
(constitutive or replacement therapy)
VAD discontinuation
• Back pressure on failing heart• Disruption of apical contractilityDisruption of apical contractility • Thrombus formationH t d thHastens deathLeaving endotrachal tube in after extubation
Bramstedt KA, J Heart Lung Transplant. 2001;20:544–8.
VAD discontinuationVAD discontinuation• Physician Assisted Suicide/Euthanasia
– Constitutive therapy—integrated part of the body
– Replacement therapy– Surrounding responsibility– OK if Non-cardiac cause of death
Asscher J. Bioethics. 2008;22(5):278-85 Rizzieri, A.G.,Philosophy, Ethics, and Humanities in Medicine, 2008; 3, 20-3520 35.Sulmasy DP. J Gen Intern Med. 2008;23 Suppl 1:69–72.Simon, J. Hastings Center Report, 2008; 38(1), 14-15.
VAD withdrawal/witholdingVAD withdrawal/witholding• Planned withdrawalPlanned withdrawal
– Anxiolytics– AnalgesicsAnalgesics– Palliative sedation
• Withholding device changeout
Von Gunten C, et al. 2nd edition. Fast Facts andConcepts. July 2005; 34.
VADs in Hospice
• How should they be managed?• When and how should devices be
deactivated?• Can hospice meet the growing need?• What to do if there is no hospice?What to do if there is no hospice?
Self discontinuation
© 2003 Mayo Foundation for Medical Education and Research
Volume 78(8) August 2003 pp 959-963
Ethical Analysis of Withdrawal of Pacemaker or Implantable Cardioverter-Defibrillator Support at the End of Life[Original Article]Mueller, Paul S. MD; Hook, C. Christopher MD; Hayes, David L. MD, ; , p ; y ,From the Division of General Internal Medicine (P.S.M.), Division of Hematology and Internal Medicine (C.C.H.), and Division of Cardiovascular Diseases and Internal Medicine (D.L.H.), Mayo Clinic, Rochester, Minn.Address reprint requests and correspondence to Paul S. Mueller, MD, Division of General Internal Medicine, Mayo Clinic, 200 First St SW, Rochester, MN 55905.
“Every 20 minutes, he would [get a y [gshock and get] jolted awake. Meanwhile he was on morphine. . . . I saw this ppattern . . . he was waking up from like a really bad dream type of thing . . . and y yp ghe would say a word or something, and after 20 seconds he would be unconscious again.”
Deactivation: ICD vs. PPM
• ICD– Shocking function +
• PPM– Symptom relief vs.
ATP?– Backup pacing?
Predictability of lethal
life prolongation• Indication?• Underlying rhythm?– Predictability of lethal
arrhythmia?– DNR=deactivation?
Underlying rhythm?
• CRT– d/c defibrillation
only?
EP consult EP consult
What do patients think aboutWhat do patients think about ICDs?
• Would you want your device turned off if you hady– Cancer: 30%– Certain death within 1 month: 40%Certain death within 1 month: 40%– Daily shocks: 50%– I would never want the device turned off:I would never want the device turned off:
10-40%
Weintraub, et al. Heart Rhythm 2006;3(5) S139.
278 ICD patients
• 5.15 years since implant• 1/3 received shocks (avg 4 7 shocks)1/3 received shocks (avg. 4.7 shocks)• 50% had advance directives
O l 3 h d i l d d l f ICD– Only 3 had included plan for ICD
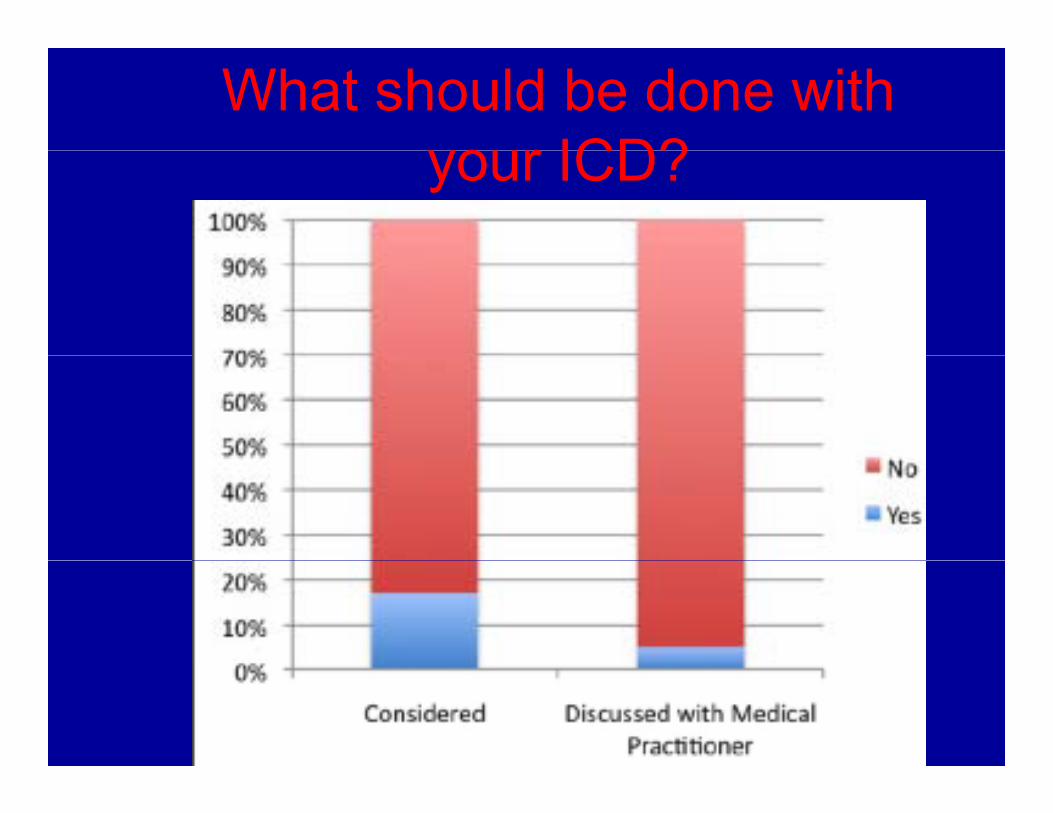
What should be done with your ICD?your ICD?
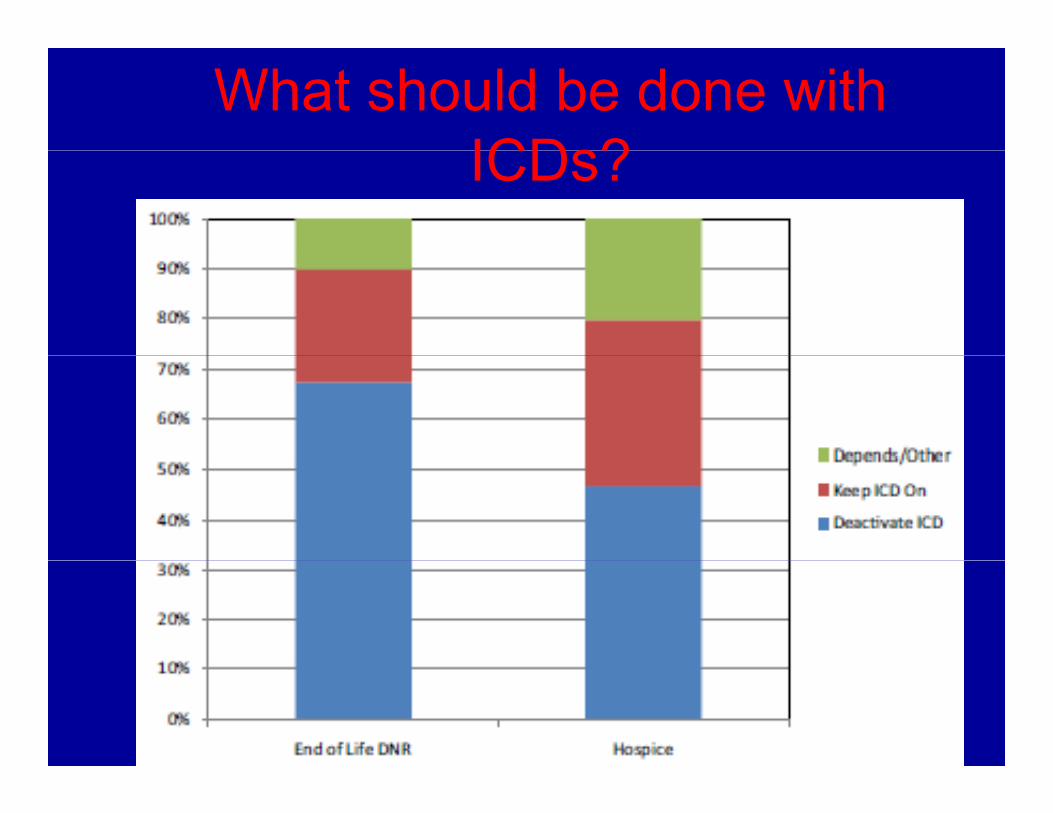
What should be done with ICDs?ICDs?
ICDQ lit f D thQuality of Death
“…we rescue people from a relatively sudden death from myocardial i f ti l t i fli t th infarction only to inflict on them a more prolonged death from progressive heart failure.”failure.
Taking away your chance to die quicklyTaking away your chance to die quickly and painlessly.
Goodman NW. BMJ. 314(7092):1484, 1997
Costs
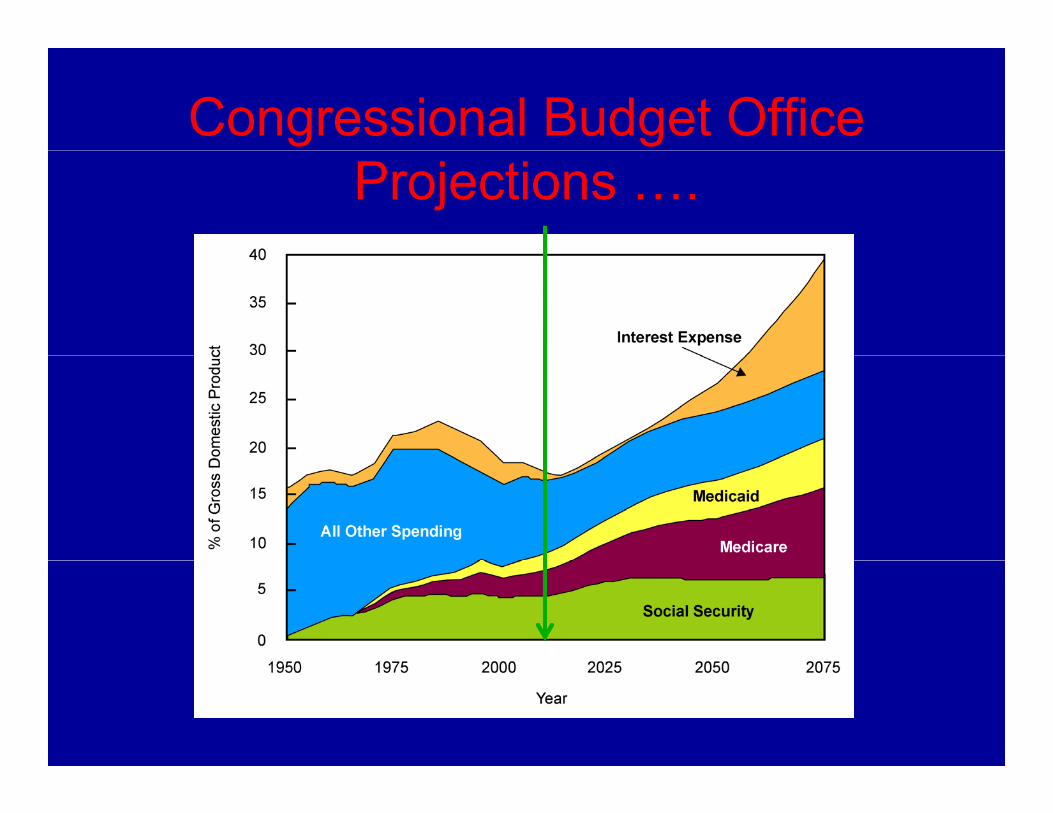
Congressional Budget Office Projections ….
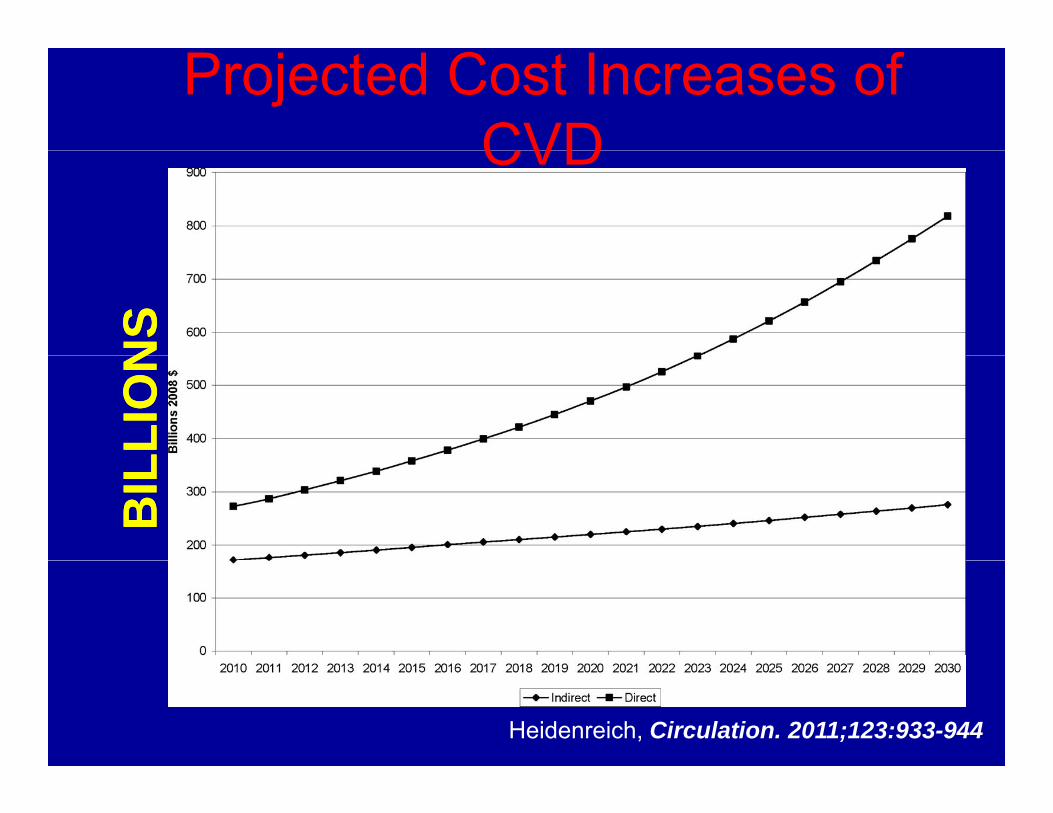
Projected Cost Increases of CVDCVD
NS
NS
LLIO
NLL
ION
BIL
BIL
Heidenreich, Circulation. 2011;123:933-944
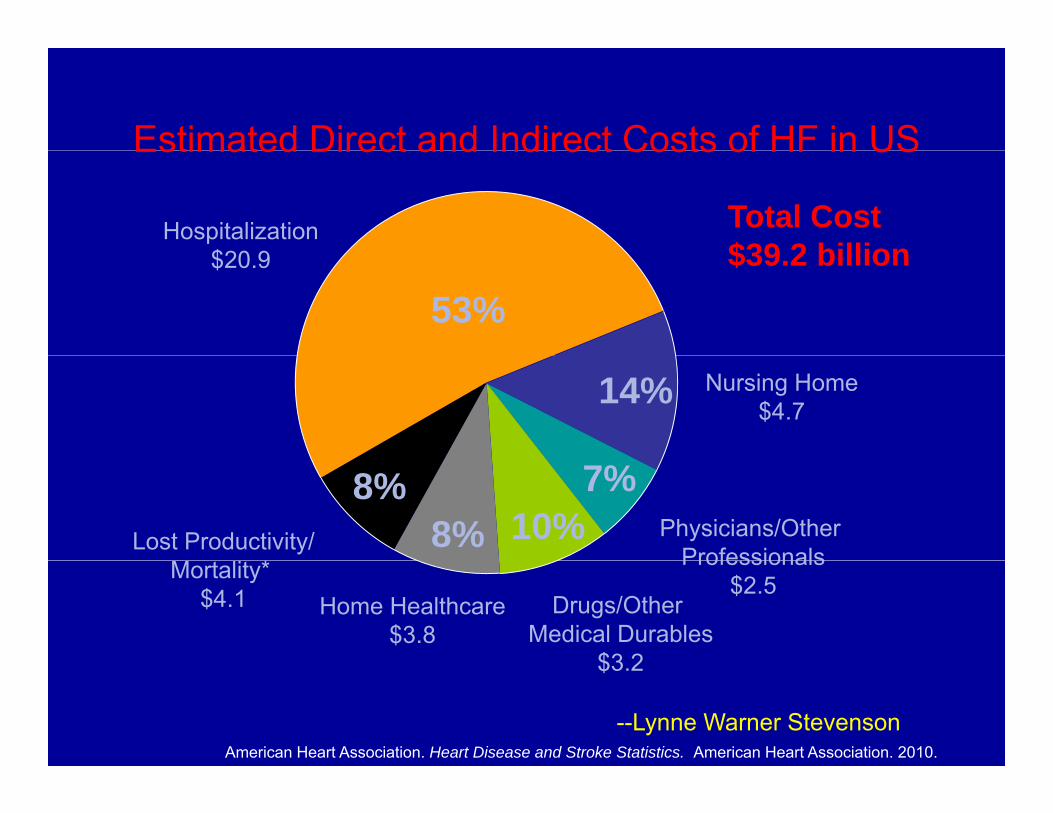
Estimated Direct and Indirect Costs of HF in USEstimated Direct and Indirect Costs of HF in US
Hospitalization$20 9
Total Cost$39 2 billion
53%$20.9 $39.2 billion
14% Nursing Home$4.7
8%8% 10%
7%Lost Productivity/ Physicians/Other
ProfessionalsMortality* $4.1 Home Healthcare
$3.8Drugs/Other
Medical Durables$3 2
Professionals$2.5
$3.2
American Heart Association. Heart Disease and Stroke Statistics. American Heart Association. 2010.
--Lynne Warner Stevenson
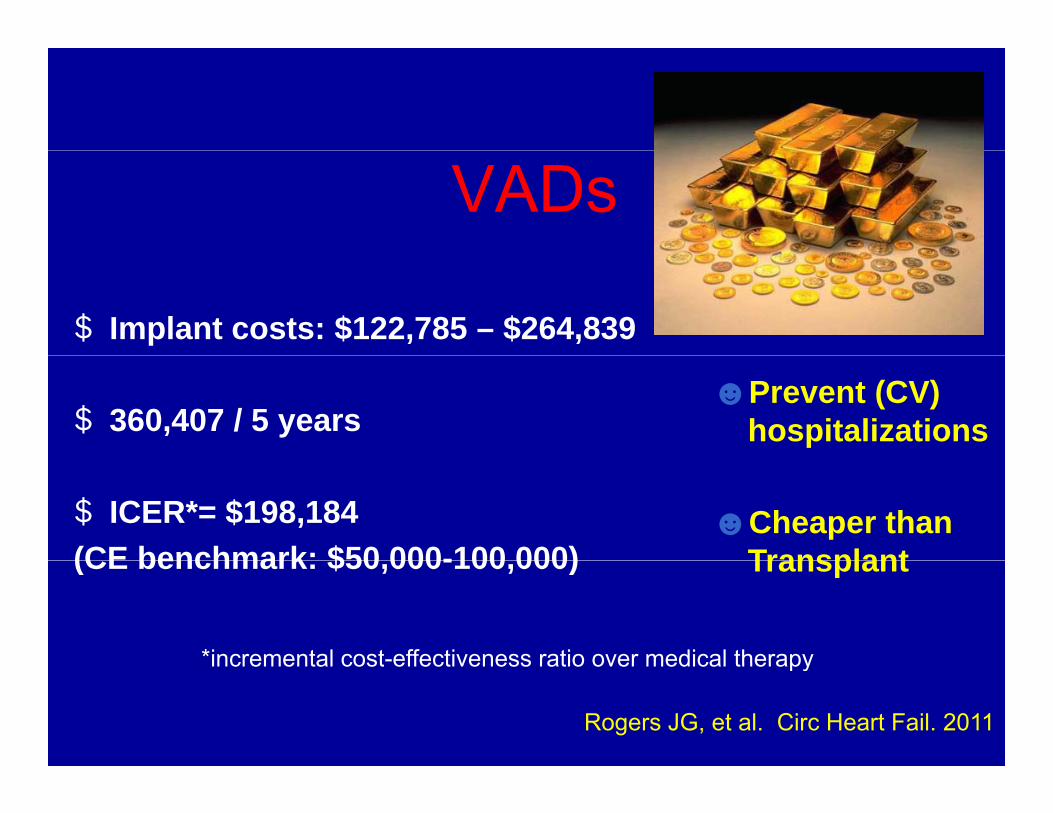
VADs
$ Implant costs: $122,785 – $264,839
$ 360,407 / 5 years☻Prevent (CV)
hospitalizations
$ ICER*= $198,184(CE benchmark: $50 000-100 000)
☻Cheaper than Transplant(CE benchmark: $50,000-100,000) Transplant
*incremental cost-effectiveness ratio over medical therapy
Rogers JG, et al. Circ Heart Fail. 2011
incremental cost effectiveness ratio over medical therapy
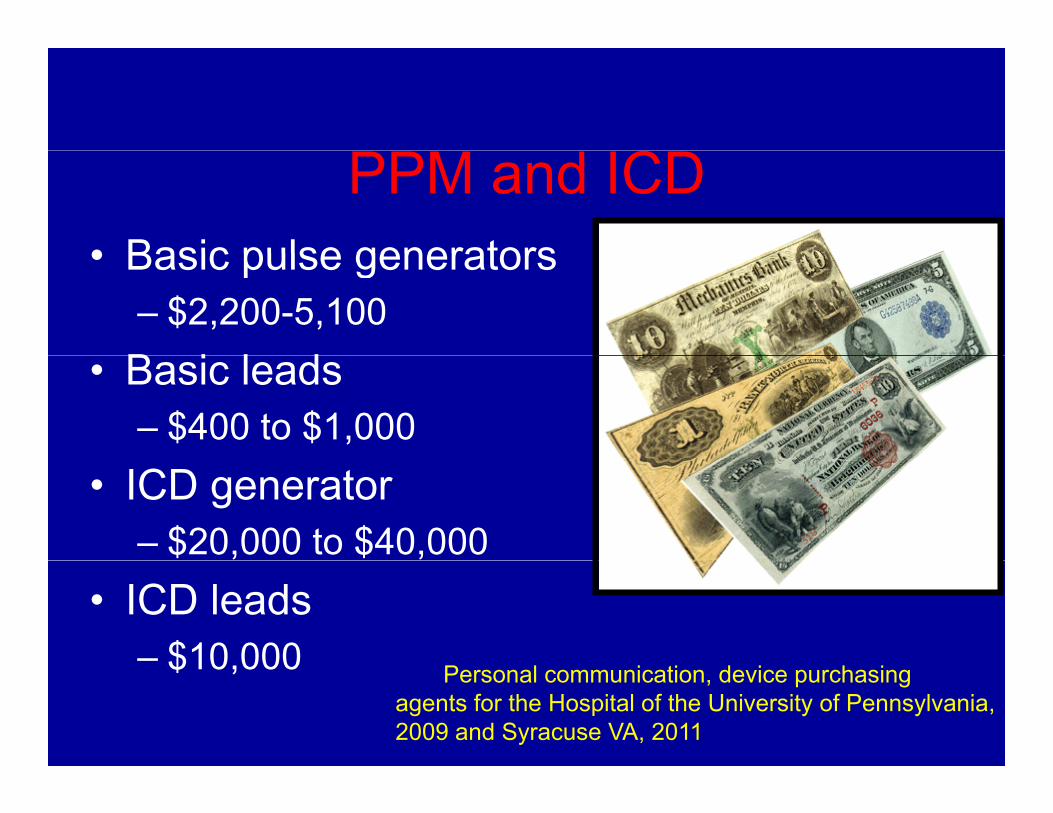
PPM and ICD• Basic pulse generators• Basic pulse generators
– $2,200-5,100B i l d• Basic leads– $400 to $1,000
• ICD generator– $20,000 to $40,000
• ICD leads – $10 000$10,000 Personal communication, device purchasing
agents for the Hospital of the University of Pennsylvania, 2009 and Syracuse VA, 2011
Costs
• CRT-D (additionalCRT D (additional $4,000 to $16,000 above ICD)above ICD)
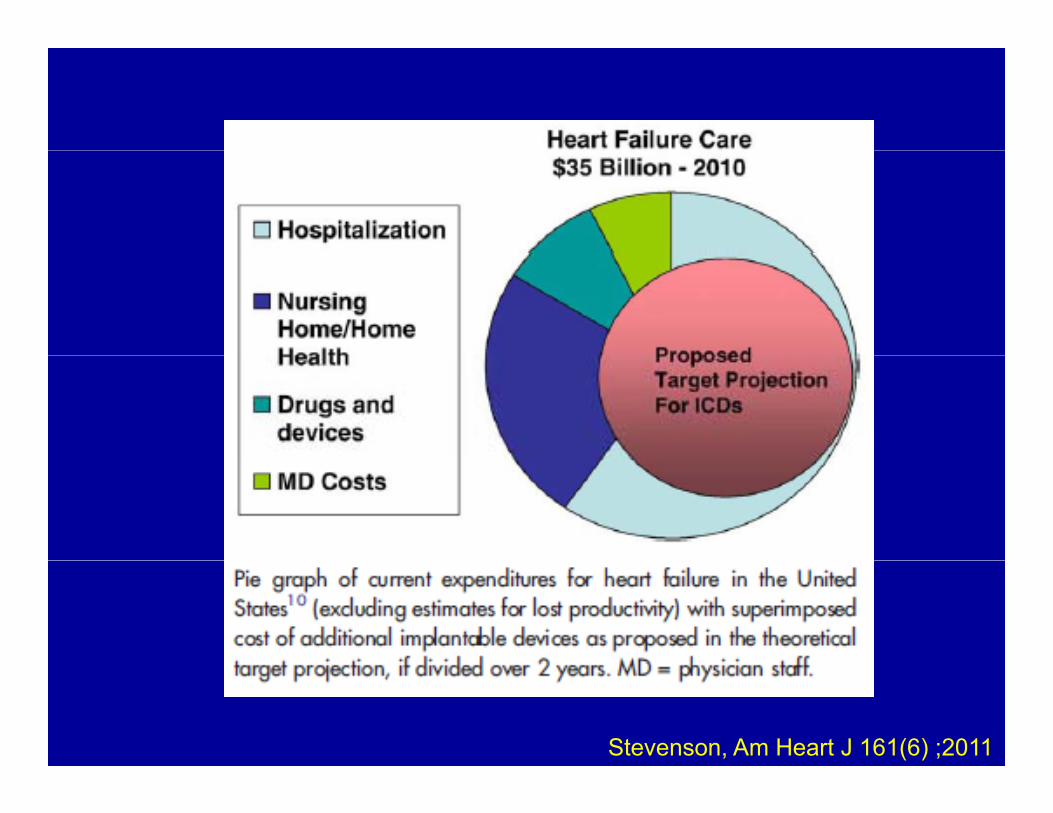
Stevenson, Am Heart J 161(6) ;2011
CostsCostsHow do we fairly (justly) allocate y (j y)
resources?What is “cost effective” and how is itWhat is cost effective and how is it
determined?Should we ration devices?Who Rations?Who Rations? Inclusion vs. exclusion
How do we identify a high enough riskHow do we identify a high enough risk group?
Sulmasy DP. Ann Int Med. 116(11):920-6, 1992
Implant RestrictionsImplant Restrictions• Medicare funding restrictions—what g
does this mean for cardiac devices?• DiscriminationDiscrimination
– Elderly vs. young—physiological age– Mild dementia—Am With Disabilities Act– Mild dementia—Am. With Disabilities Act– Severe Depression-- “
Waiting list?Waiting list?”Device committee”?
Complexities in Advance Care pPlanning
Complexities• Changing preferences• Changing preferences• Timing of AD discussions• Who is responsible for the
discussions?• What should be discussed?• How do you bring up the topic?How do you bring up the topic?
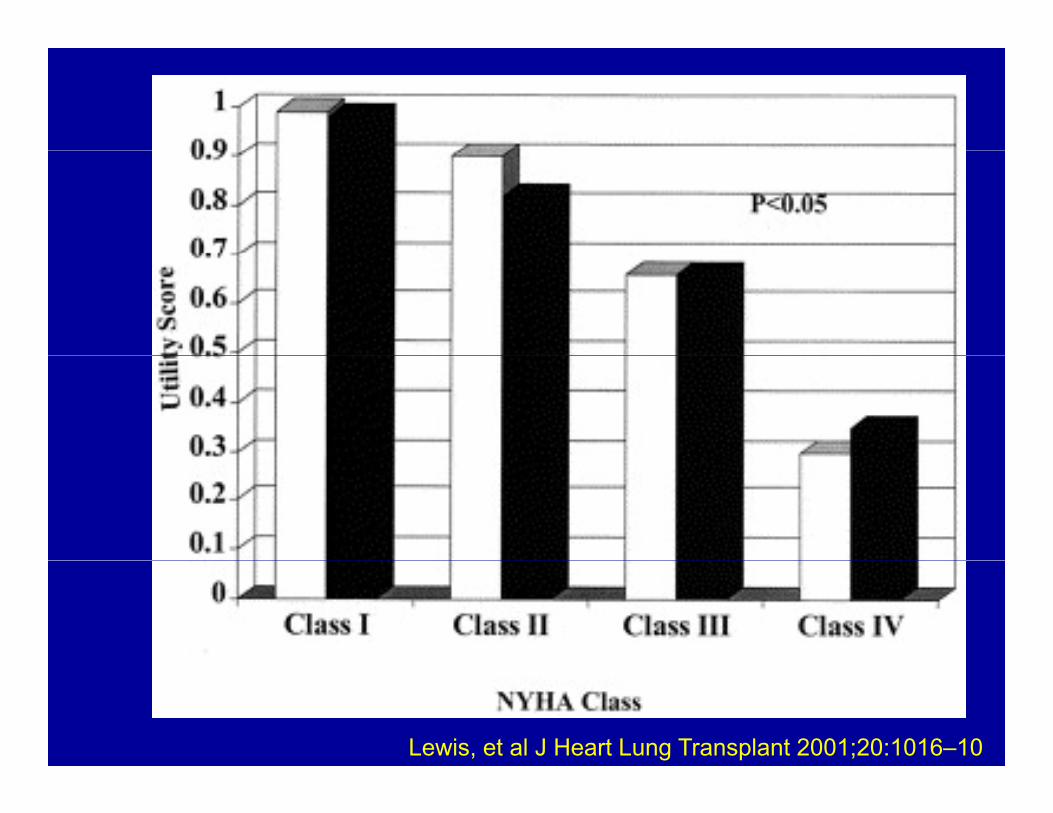
Lewis, et al J Heart Lung Transplant 2001;20:1016–10
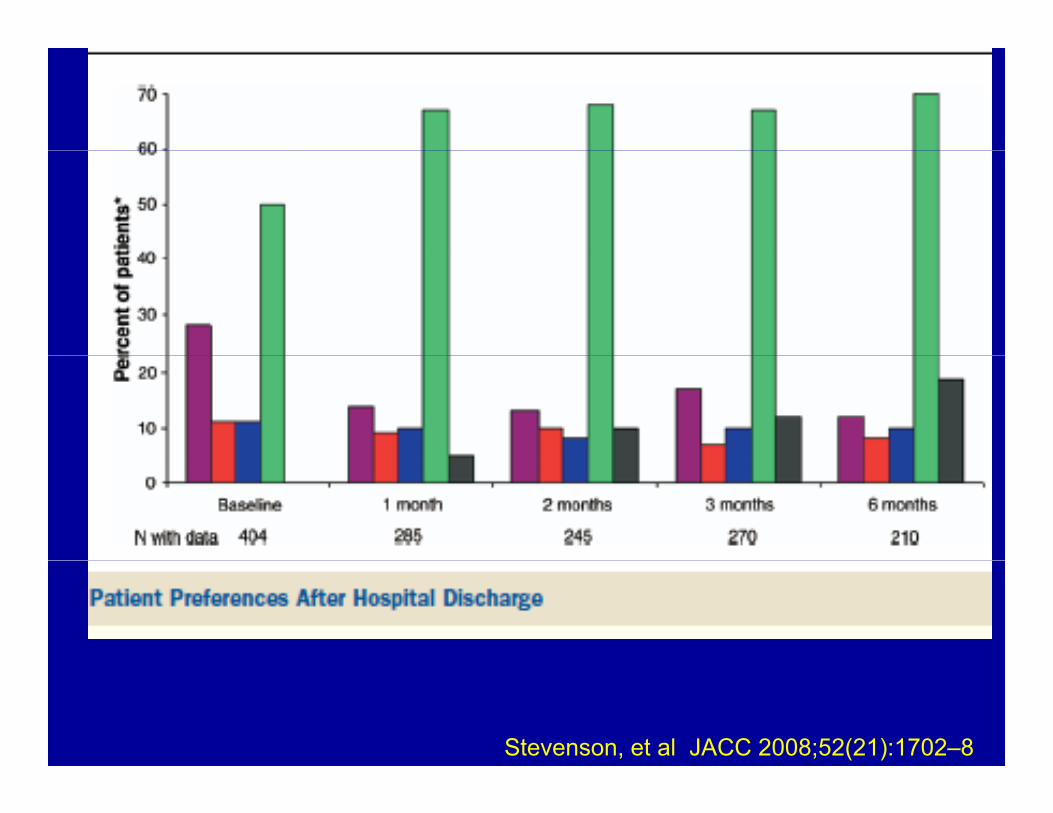
Change their minds
Stevenson, et al JACC 2008;52(21):1702–8
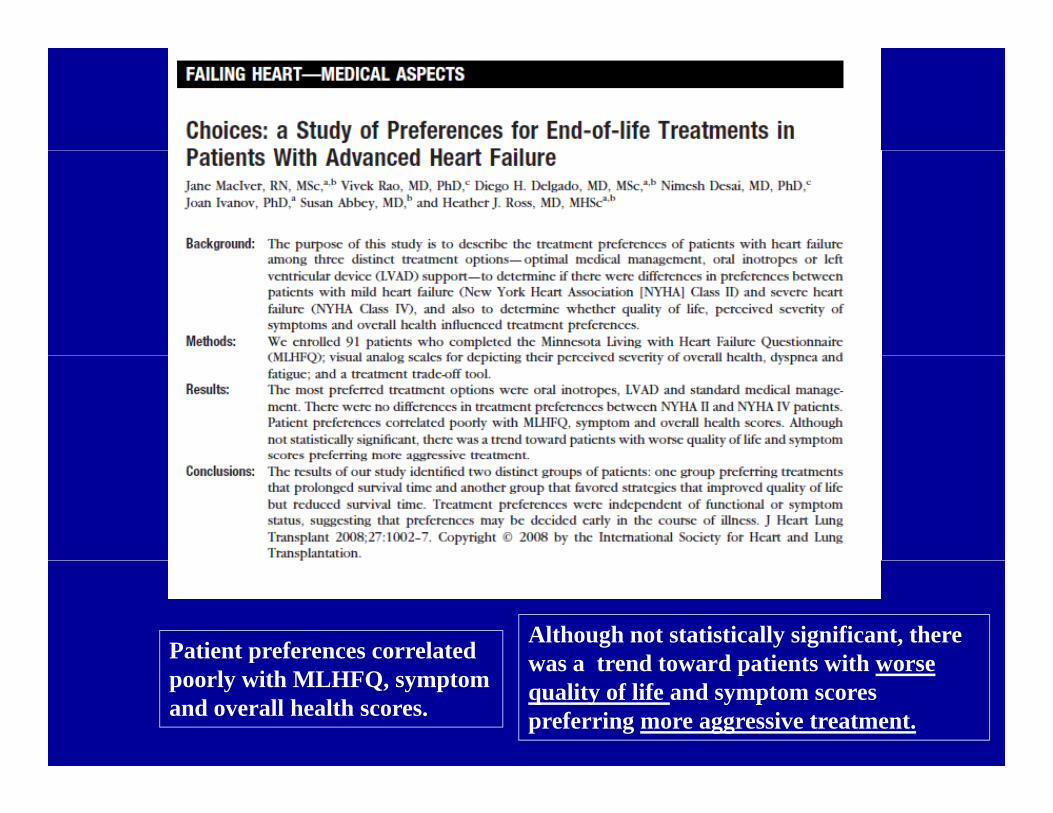
Although not statistically significant, there was a trend toward patients with worsePatient preferences correlated was a trend toward patients with worse quality of life and symptom scores preferring more aggressive treatment.
ppoorly with MLHFQ, symptom and overall health scores.
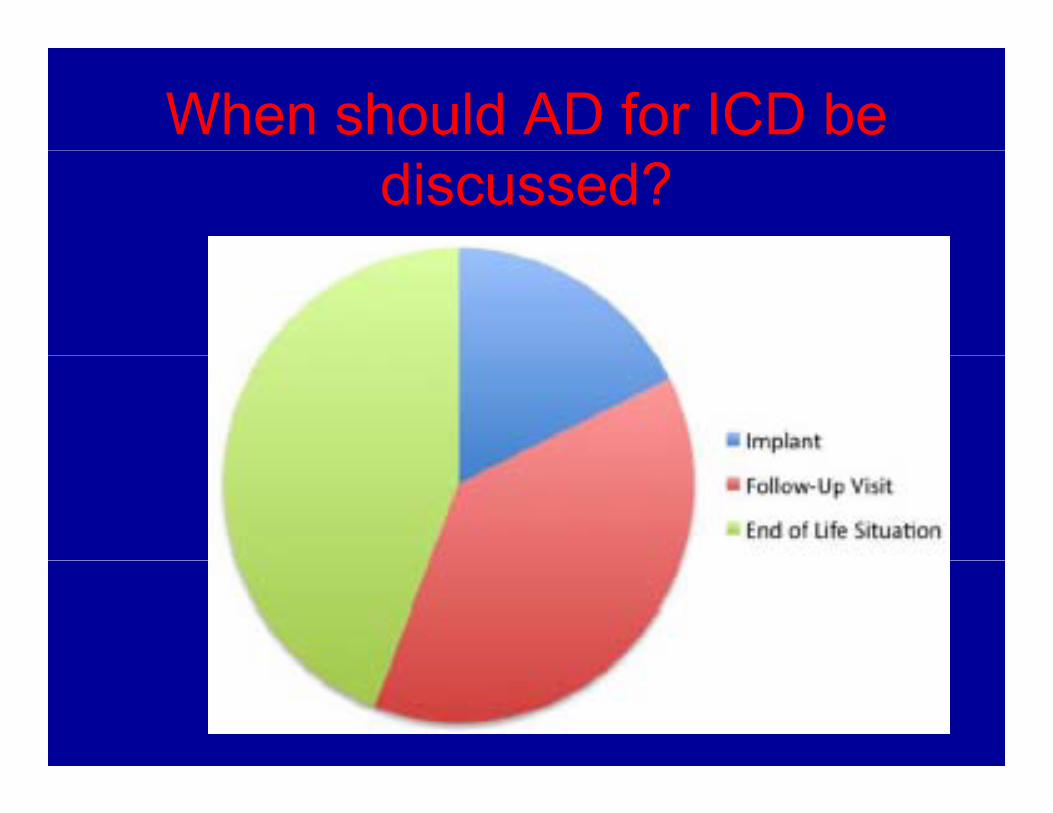
When should AD for ICD be discussed?
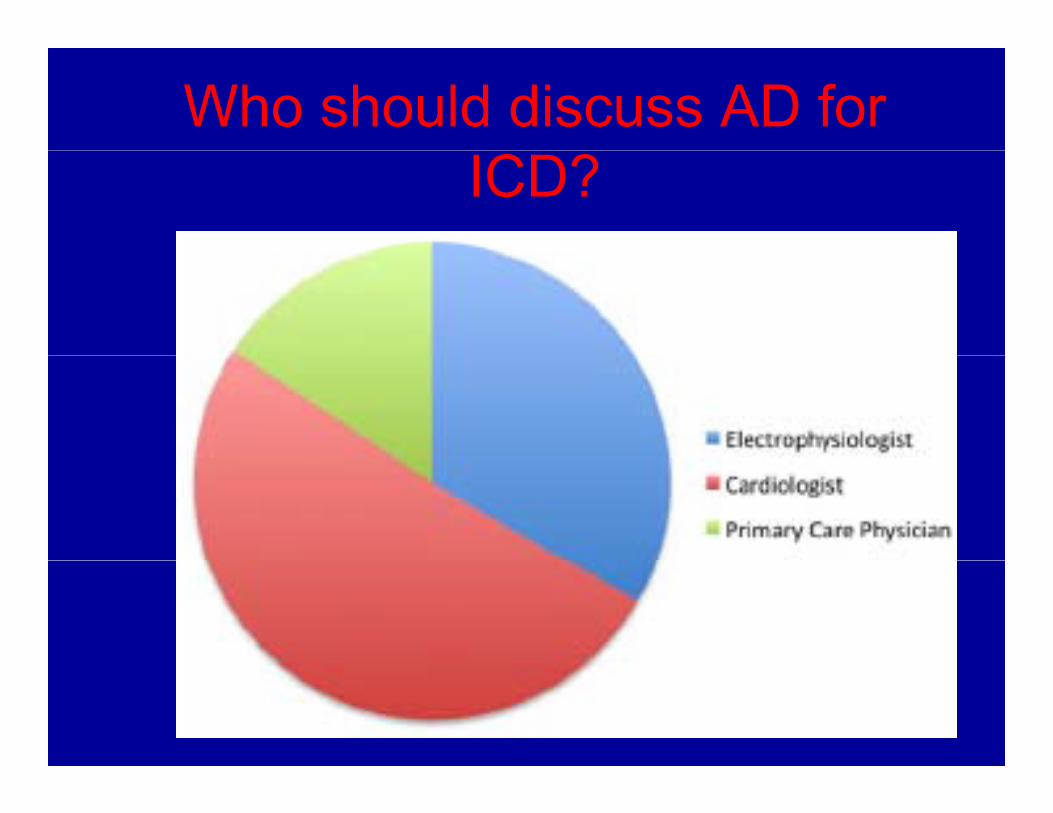
Who should discuss AD for ICD?
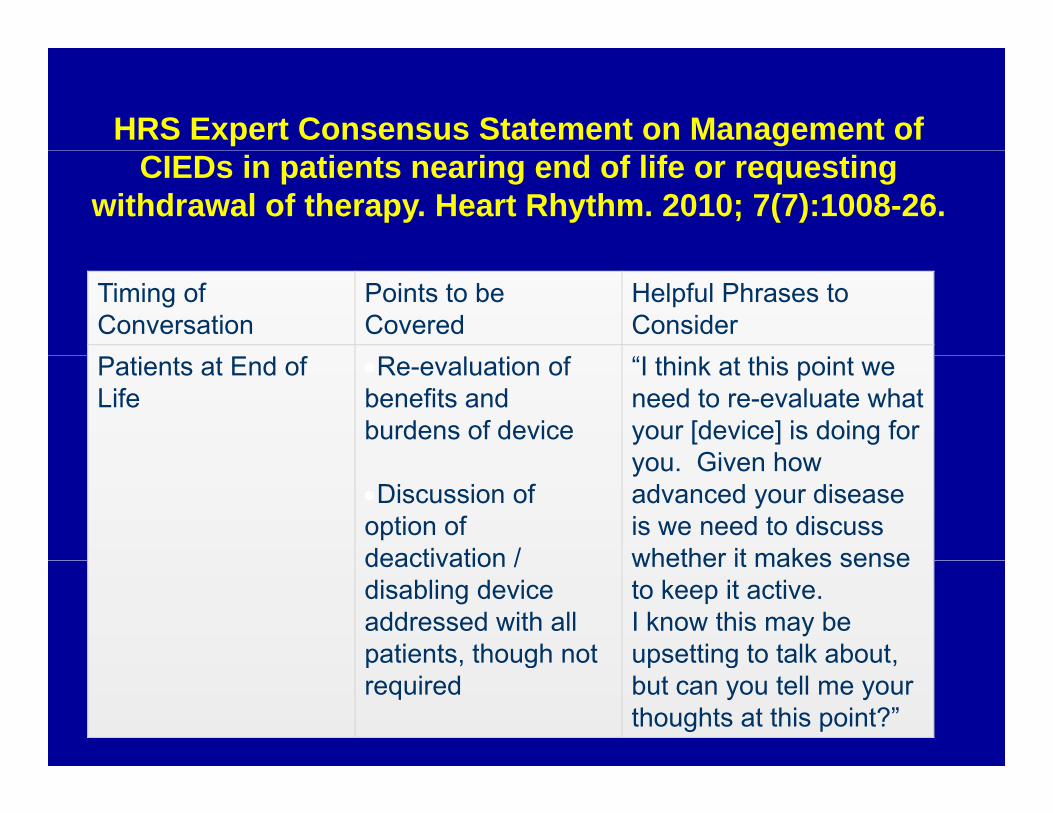
HRS Expert Consensus Statement on Management of CIEDs in patients nearing end of life or requesting
withdrawal of therapy. Heart Rhythm. 2010; 7(7):1008-26.
Timing of Conversation
Points to be Covered
Helpful Phrases to Consider
Patients at End of Life
Re-evaluation of benefits and burdens of device
“I think at this point we need to re-evaluate what your [device] is doing for you Given how
Discussion of option of deactivation /
you. Given how advanced your disease is we need to discuss whether it makes sensedeactivation /
disabling device addressed with all patients, though not
whether it makes sense to keep it active. I know this may be upsetting to talk about, p , g
requiredp g ,
but can you tell me your thoughts at this point?”
Introducing the “…Heart failure is a very serious disease, from which
many patients ultimately die Thankfully we have
notion that heart many patients ultimately die. Thankfully we have
some extremely good treatments...”
failure is
potentially fatal“People may die from heart failure, but it is not like
potentially fatal cancer in that it is very hard to predict how long
people with heart failure will live.”
Assessing “…is there anyone you trust to make medical
readinessdecisions for you, and have you talked with this
person about what is important to you? ”person about what is important to you?...
McKelvie, et al. Canadian Journal of Cardiology 27 (2011) 319–338
Complicated IssuespMultidisciplinary approachGeriatricsGeriatricsCardiologyPrimary careP lli tiPalliative careSubspecialty cardiologyNursingSocial workEthics
Dialogue
Joint Consensus Statements/Guidelines
Pacemaker/ICD ReusePacemaker/ICD ReuseVAD Advance Directive
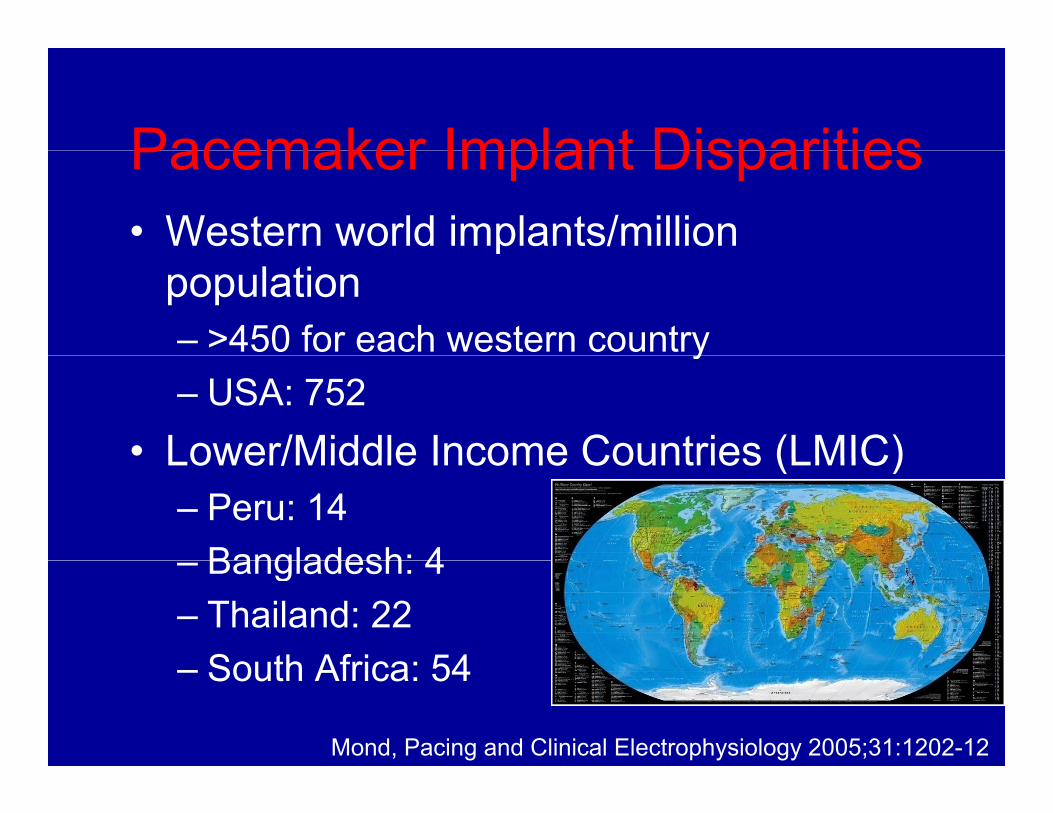
Pacemaker Implant DisparitiesPacemaker Implant Disparities• Western world implants/million p
population– >450 for each western countryy– USA: 752
• Lower/Middle Income Countries (LMIC)Lower/Middle Income Countries (LMIC)– Peru: 14
Bangladesh: 4– Bangladesh: 4– Thailand: 22
South Africa: 54– South Africa: 54
Mond, Pacing and Clinical Electrophysiology 2005;31:1202-12

Overseas NeedOverseas Need
• Cardiovascular diseaseCardiovascular disease burden in LMIC– Increased 137% 1990 to
2020– 14 million cardiovascular
d thdeaths– Younger age
• Loss of economic• Loss of economic productivity
Joshi, J Am Coll Cardiol. 2008; 52:1817-25WHO. Cardiovascular Disease. Factsheet
Cost• “The average wage in
Bolivia is between $50 $and $100 a month…”
• LMIC Healthcare budgets focus onbudgets focus on prevention
Device Donations
• New, expired Devices
• Used DevicesU d– Upgrades
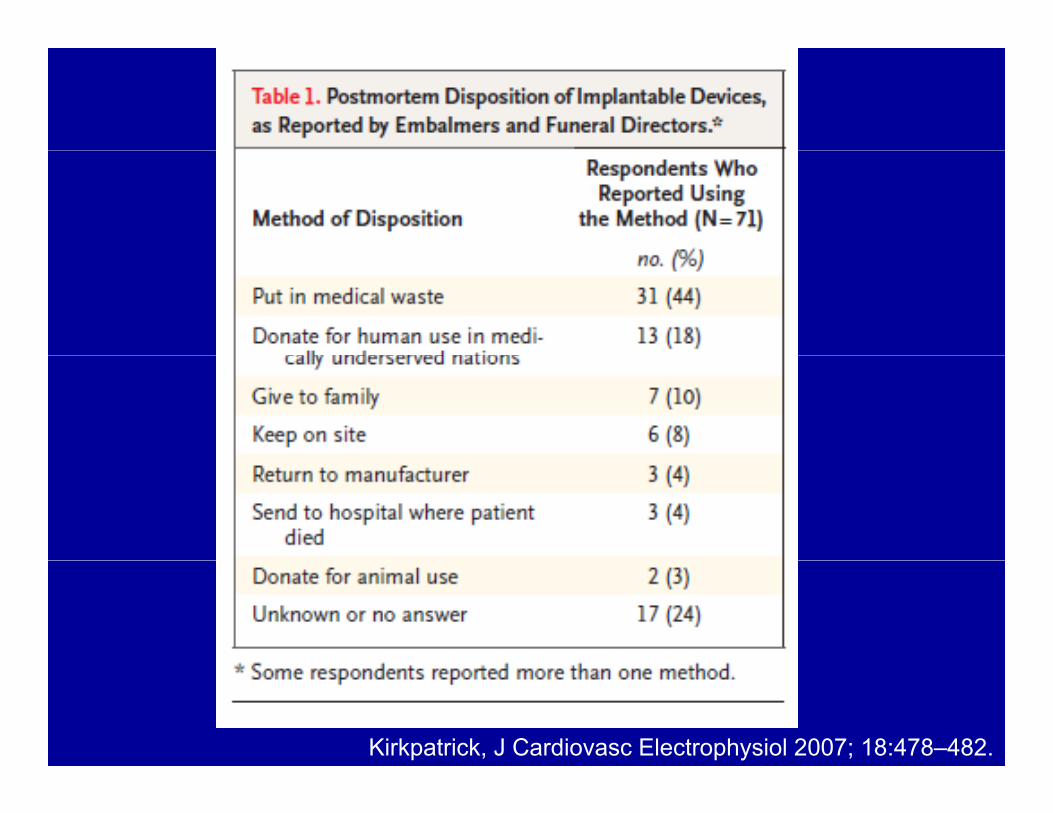
– Post mortem
Post MortemPost Mortem• Pacemaker deaths
– 20% within 33 months– 40% within 4 years
• Patients > 80 y/o– 32% of pacemaker
i l timplants• Pacemaker longevity:
10 years10 years
CPringle, Pacing Clin Electrophysiol. 1986;9:1295-8. Schmidt, Am Heart J 2003;146:908–913.
Schmidt,Eur Heart J 2004;25:88 –95.Pyatt, Europace 2002;4:113–119.
Post Mortem Removal
• Pacemakers and ICDs explode and damage the crematorium chamberg
• Cremation projected to reach 59% of all• Cremation projected to reach 59% of all deaths in the United States by 2025
National Funeral Directors Association. 2010 Selected Funeral Service Information and Statistics.
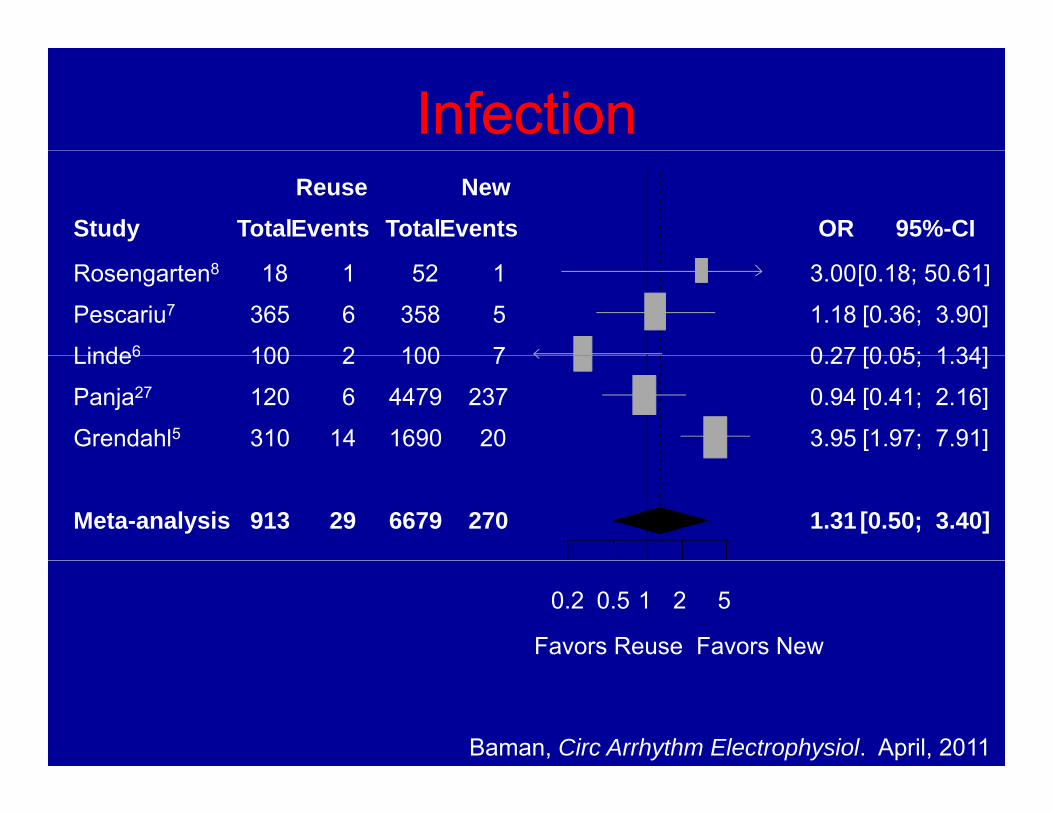
InfectionInfection
Study TotalEventsReuse
TotalEventsNew
OR 95%-CI
Rosengarten8
Pescariu7
Linde6
18
365
100
1
6
2
52
358
100
1
5
7
3.00
1.18
0 27
[0.18; 50.61]
[0.36; 3.90]
[0 05; 1 34]Linde6
Panja27
Grendahl5
100
120
310
2
6
14
100
4479
1690
7
237
20
0.27
0.94
3.95
[0.05; 1.34]
[0.41; 2.16]
[1.97; 7.91]
Meta-analysis 913 29 6679 270 1.31 [0.50; 3.40]
0.2 0.5 1 2 5
Favors Reuse Favors New
Baman, Circ Arrhythm Electrophysiol. April, 2011
Device Malfunction
• Low rate:– 0.68% (0.27 to 1.28)0.68% (0.27 to 1.28)
• Increased compared with new OR 5 80 [1 93 to 17 47] p= 0 002– OR 5.80 [1.93 to 17.47], p= 0.002
– Set screws“technical errors”– technical errors
Baman, Circ Arrhythm Electrophysiol. April, 2011
Precedent for Reuse
• 1991: 14% of primary implants p y pwere reused device
• 1996: 5% (incorporation in(incorporation in European Common Market)Market)
Kirkpatrick, J Cardiovasc Electrophysiol 2007; 18:478–482.
“Living Wills for Pacemakers”Living Wills for Pacemakers
Device specific advance directive– Options for post-mortem handling of deviceOptions for post mortem handling of device– Information
• DonationDonation• Return to manufacturers
– Appointment of surrogatepp g– (Deactivation at end of life)
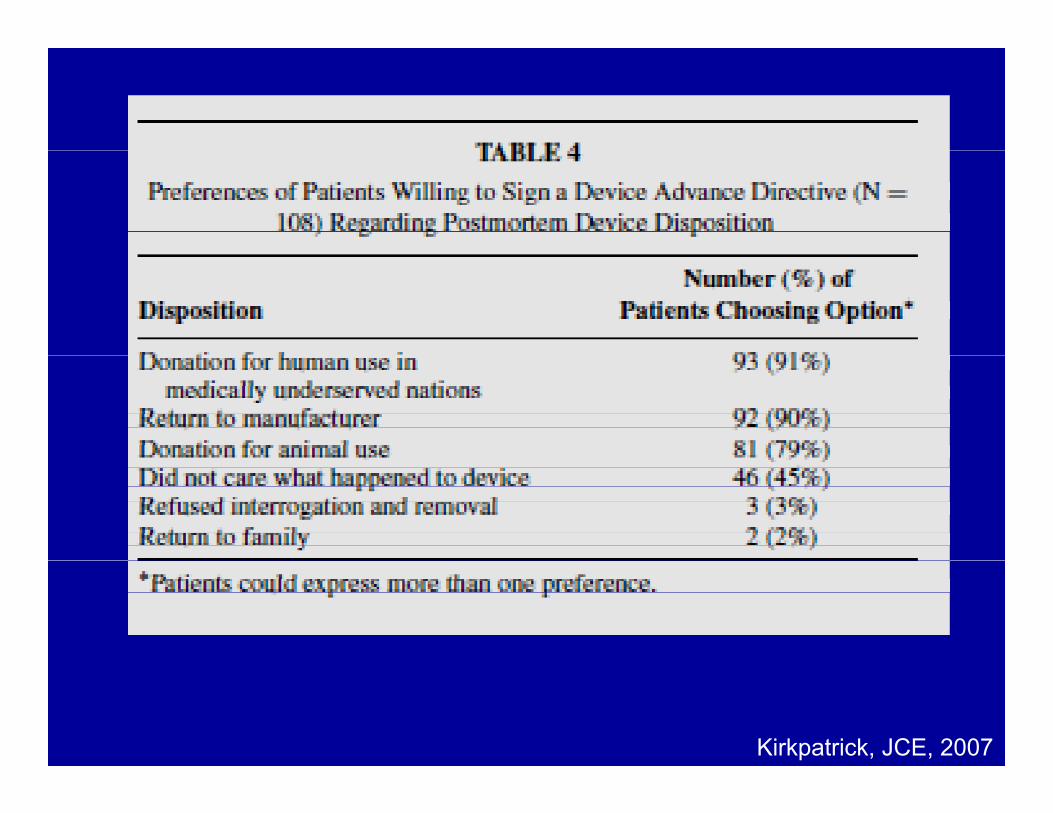
Kirkpatrick, JCE, 2007
Reuse of Pacemakers
• Survey patients in hospice re: willingness to donate their devicesg
• Pilot test “pacemaker living will” in hospice patientshospice patients
• Establish Penn as a collection and distribution center for cardiac devicesdistribution center for cardiac devices overseas
Cardiac DeviceCardiac Device Advance Directives
• Specific/individualized decisions re: devicesdec s o s e de ces– ICDs (discontinuation at
DNR, hospice, ATP)DNR, hospice, ATP)– Pacemakers and QOL
vs life prolongationvs. life prolongation (pacemaker dependent)
– CRT (QOL)– CRT (QOL)– VAD withdrawal
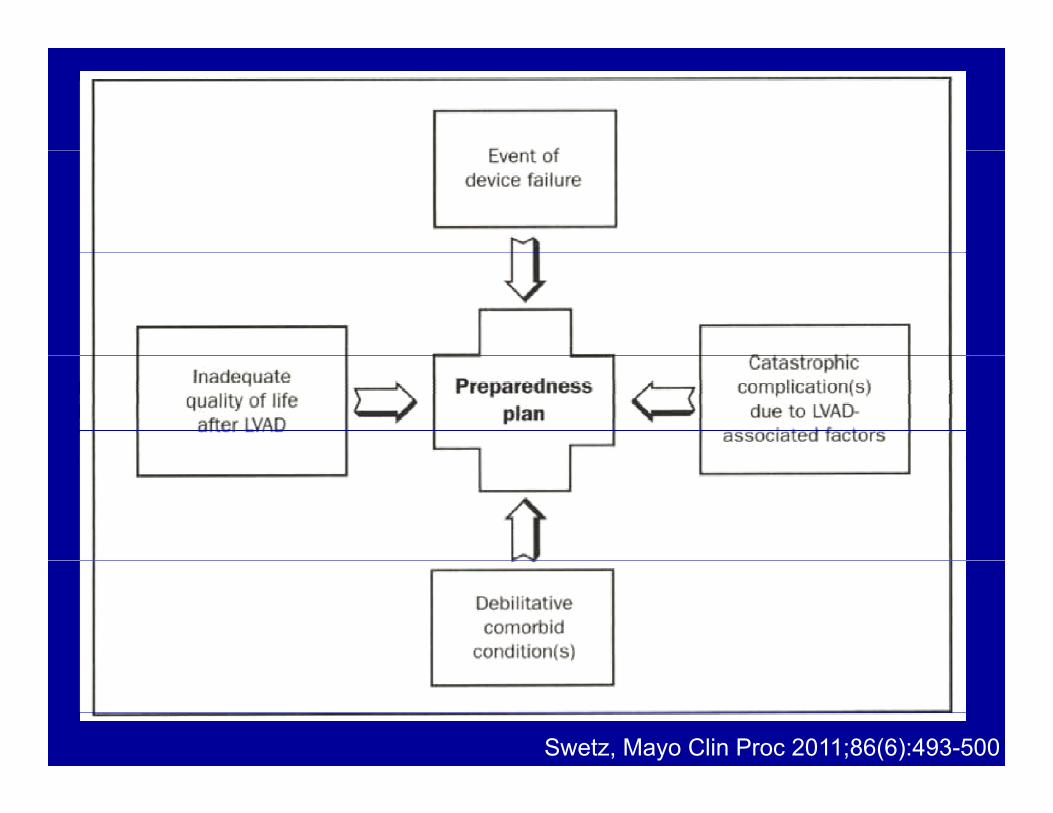
Swetz, Mayo Clin Proc 2011;86(6):493-500
VAD Advance Directives
• Supplement to 5 wishes• Offer pre-implantOffer pre implant• Re-address at 3 months
post implantpost implant• VAD specific issues
Recap• Cardiac devices definitely glitter, but
there ARE ethical dilemmas, especially in the golden years
• Cardiac advance directives “are golden” but complicated and require multidisciplinary input
• Reused pacemakers are worth their weight in gold for poor patients inweight in gold for poor patients in developing world countries
Thanks for your attention
HF Scores and Palliative Care
“Although these scores may be useful for defining a population for a clinical t i l th i li bilit i f ilit ti thtrial…their applicability in facilitating the decision between aggressive care and palliative care remains somewhatpalliative care remains somewhat limited by the inability to precisely determine prognosis for the individual p gpatient within the framework of rapidly changing parameters.”
Lewis, Current Treatment Options in Cardiovascular Medicine (2011) 13:7
Definitions of Death
• Irreversible cessation of cardiopulmonary functionp y
• Irreversible cessation of (whole or• Irreversible cessation of (whole or brainstem) neurological function
President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and Behavioral Research. Guidelines for the determination of death. JAMA 1981;246(19):2184–6.
Futile Therapy
• What is “futility?”– Physiological futilityPhysiological futility
• Won’t work (defibrillation in PEA arrest)– Quantitative futilityy
• Very little chance of working (LVAD in myocardial depression from bacterial sepsis)
– Qualitative futility• Won’t produce adequate QOL (DT LVAD in end
stage Alzheimer)stage Alzheimer)Pope, T.M. Journal of Clinical Ethics, 2009;20, 274-286.
Ethics and Cardiology
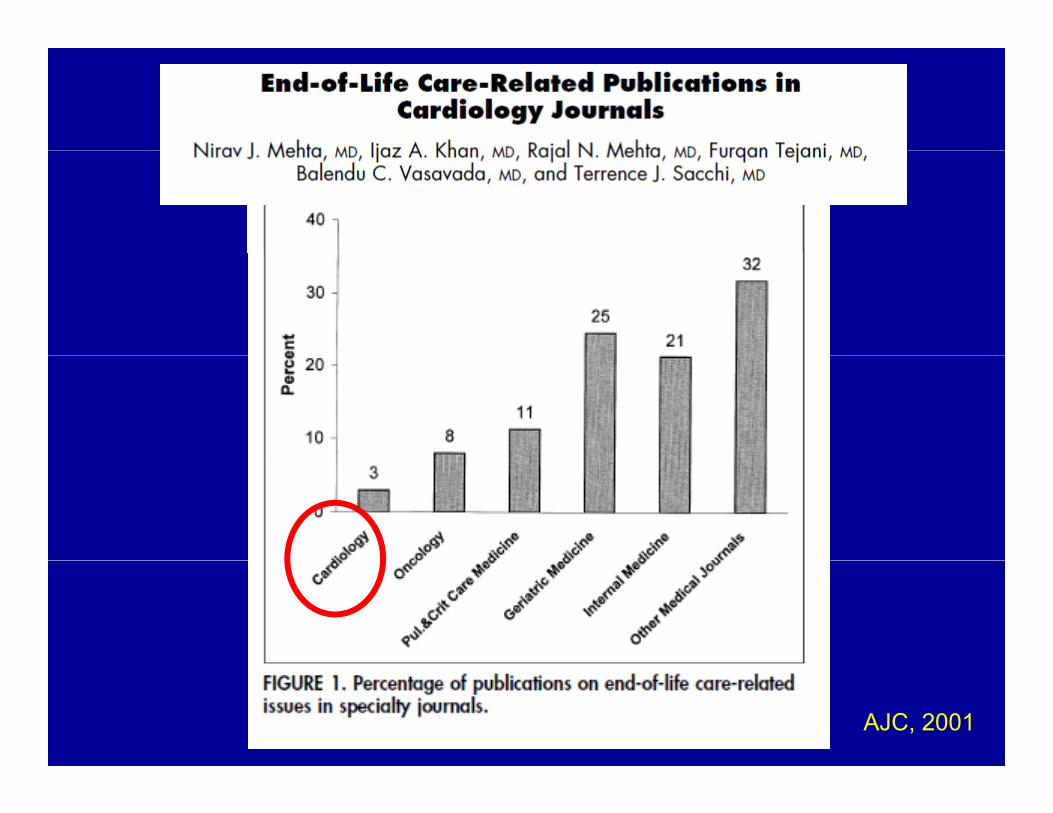
AJC, 2001
Pilot Data: LVAD DT icaregivers
10 caregivers• 10 caregivers • 90% female, mean age 59 years• 60% reported feeling emotionally and physically p g y p y y
overwhelmed • 70% reported feeling uninformed or ill prepared• 60% reported feeling have no choice in accepting• 60% reported feeling have no choice in accepting
caregiver role• 90% had not considered plans for deactivating
LVADLVAD• Employed caregivers: 100% reported adverse
impact on work
Sarah Hull, MD, MBE
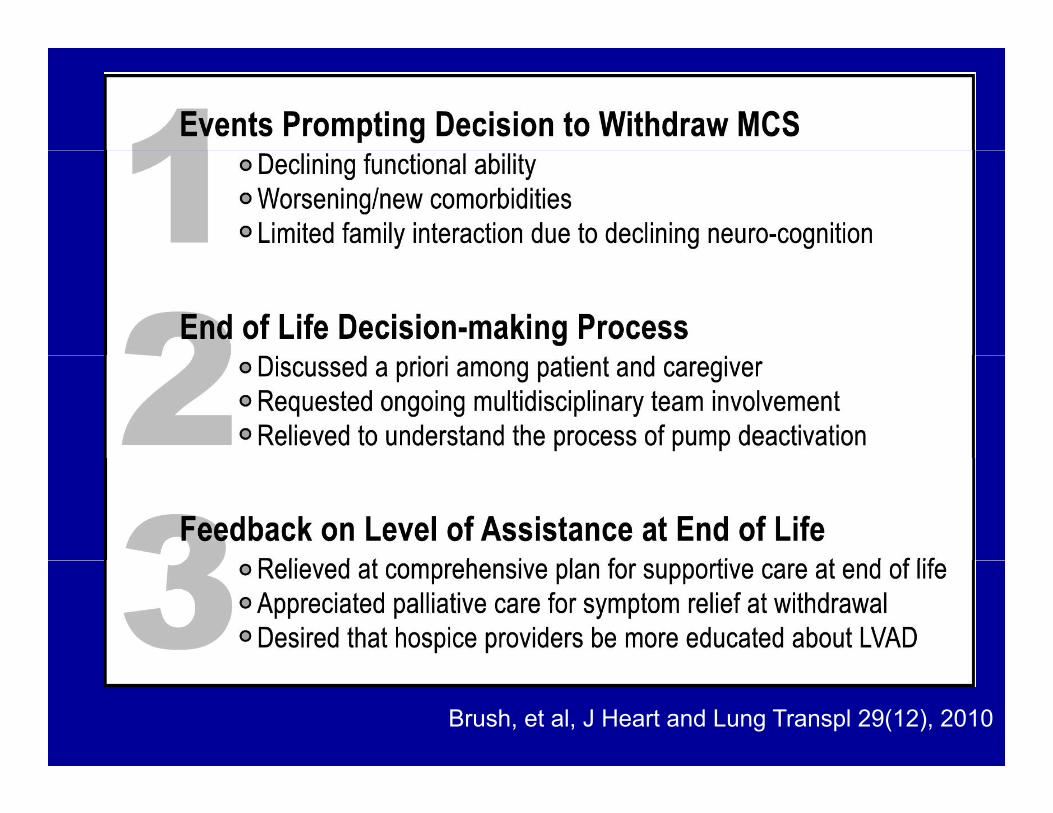
Brush, et al, J Heart and Lung Transpl 29(12), 2010
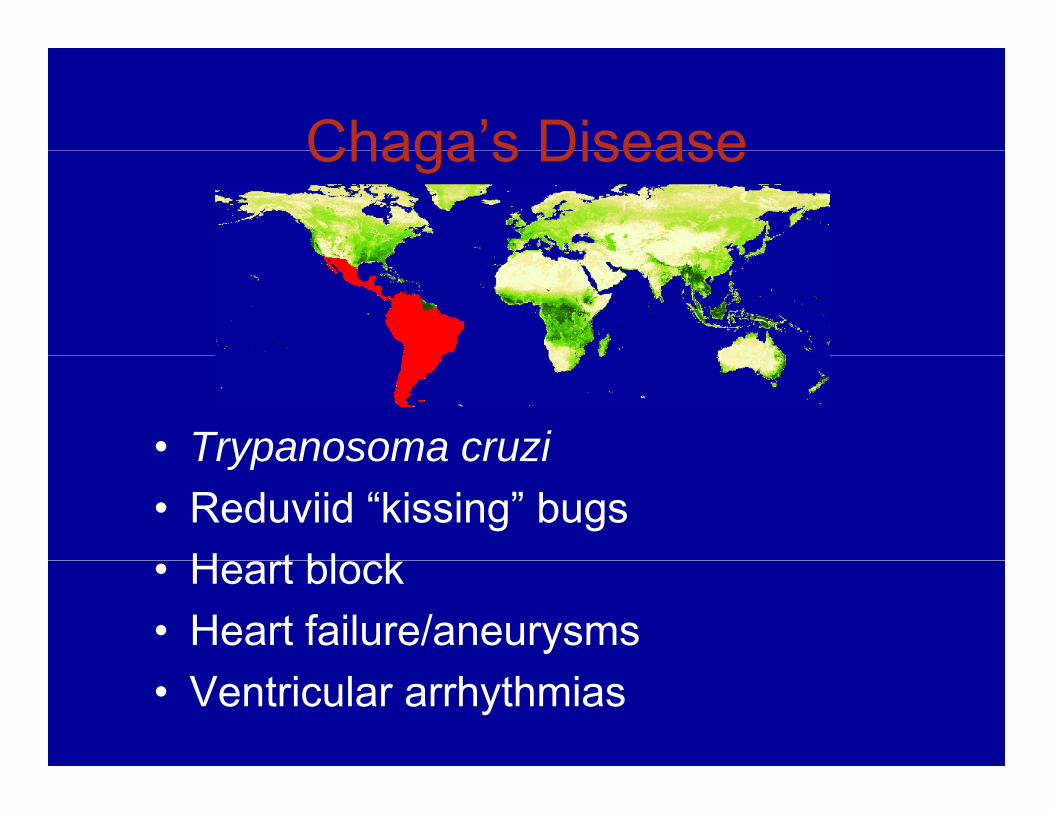
Chaga’s DiseaseChaga s Disease
• Trypanosoma cruziTrypanosoma cruzi• Reduviid “kissing” bugs
H t bl k• Heart block• Heart failure/aneurysms• Ventricular arrhythmias
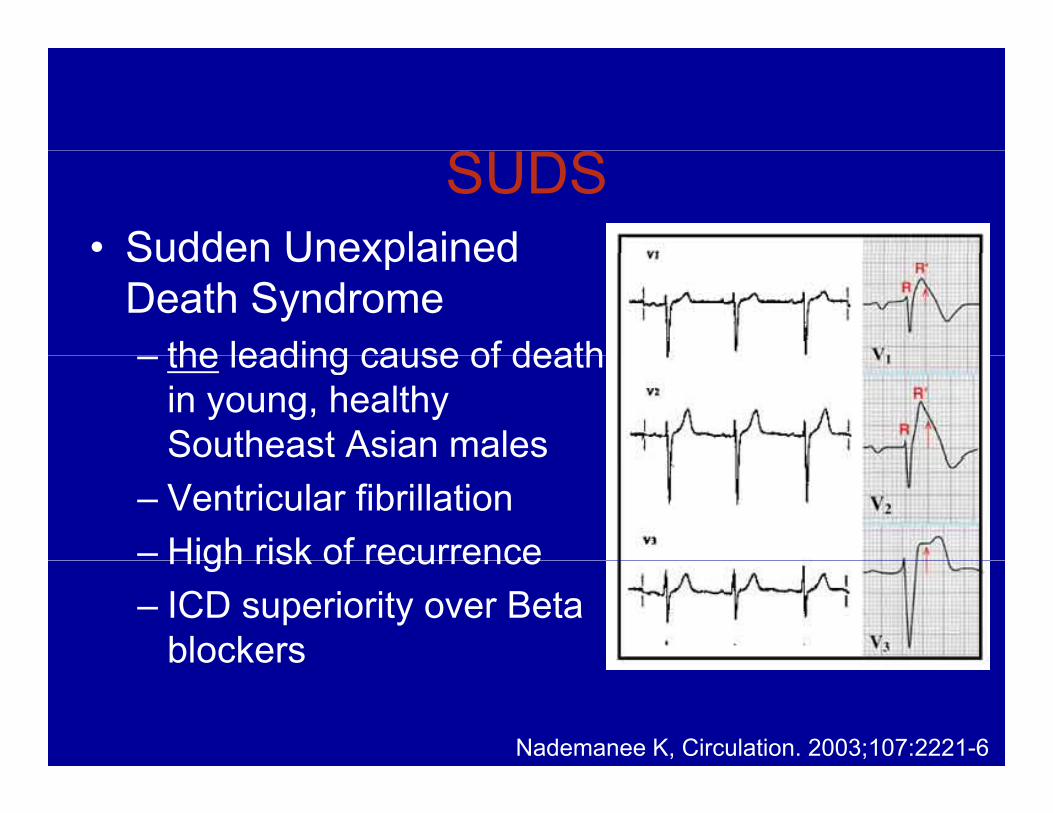
SUDS• Sudden UnexplainedSudden Unexplained
Death Syndromethe leading cause of death– the leading cause of death in young, healthy Southeast Asian males
– Ventricular fibrillation– High risk of recurrenceHigh risk of recurrence– ICD superiority over Beta
blockers
Nademanee K, Circulation. 2003;107:2221-6
Used Devices• UpgradesUpgrades
– RV pacing– ICDICD– CRT
• Infections• Infections– 0.13% to 12.6%
M ti 52 d ( til 1 t 3 24 t– Mean time 52 days (quartile 1 to 3, 24 to 162 days)
Wilkhoff, JAMA. 2002; 288:3115-3123Klug, Circulation. 2007;116:1349-55
Preliminary Experience Regarding Re-Use of Explanted ResterilizedUse of Explanted, Resterilized
Defibrillators• 31 patients Mean age 52±15 (range 16• 31 patients Mean age 52±15 (range 16 –
77)F ll 795 579 ( 13 2237)• Follow up: 795±579 (range 13 – 2237)days
• No infectious complications• LV lead dislodgement in 1 pt. g p• 42% pts experienced appropriate shocks • 5 pts received a second explanted ICD• 5 pts received a second explanted ICD
after 1057±807, range 362 – 2162 daysPavri, Circulation. 2010;122:A18350
Feasibility of Device Acquisition with Adequate Battery Life for
Potential Reuse in UnderservedPotential Reuse in Underserved Nations
Timir S. Baman, Lindsey Gakenheimer, Nathan E Sovitch, Patricia Sovitch, Joshua Romero, James N. Kirkpatrick, Brad Wasserman, George Samson, Howard Jones, Thomas Crawford, Hakan Oral, Kim A Eagle
• 2172 devices donated• 10% with ≥75% battery life or 4 years10% with ≥75% battery life or 4 years• Average time since implantation was
2 1±1 0 years2.1±1.0 years
CaregiversCaregivers
• Majority of VAD patients traditionally men, but with smaller devices entering the market more women expected to benefit from this technology
• Traumatic spinal cord injury patients’ relationships do not fare as well when patient is woman and caregiver is man
• Will this translate to VAD patients as well?Will this translate to VAD patients as well?
Bridge vs. Destination CaregiversCaregivers
• The few small studies that do exist suggest that partners/caregivers of VAD gg p gpatients experience significant psychological distressp y g
• This is often counterbalanced by feelings• This is often counterbalanced by feelings of pride and hope in caregivers of bridge patients (has not yet been studiedpatients (has not yet been studied specifically in Destination Therapy)
Competing Interests
• Post-market illsurveillance
• “Bench” analysis of generators
• Post-mortem≠ changeouts
Ellenbogen KA et al JACC 2003;41:73-80Return all devices
Ellenbogen KA, et al. JACC 2003;41:73-80Kron J, et al. Am Heart J 2001;141:92-98.Gradaus T, et al. Pacing Clin Electrophysiol 2003;26:649-657Heart Rhythm Society. Task Force on Device Performance Policies and Guidelines. 2006
to manufacturers!
Competing Interests
• All devices with inadequate battery life sent to manufacturers
• Increased return from donationsincrease rate of return todonationsincrease rate of return to manufacturers