cardiac catheterization lab rotation expectations and ... · cardiac catheterization lab rotation...
TRANSCRIPT
Cardiac Catheterization Lab Rotation Expectations and Objectives (Updated July2012)
The main goals for first year rotation are to understand the indications, risks, performance of right and left heart cath, basic hemodynamics and management of complications. We want to emphasize the need to read around your patients, review angiograms after each case, become proficient at groin management, log cases and ensure that you receive feedback at the end of the rotation. Please meet with interventional fellow to discuss role/orientation.
- Before the first rotation, read the chapter in Grossman’s about arterial access (know the anatomy and standard access techniques). Practice with the manifold at home prior to the rotation (obtain manifold in cath lab by asking the other fellows). Grossman pages 36-55 and 80-96.
- Know the risks of catheterization. Consent should be observed with an upper level fellow during the first day of the rotation.
- In the first couple days, learn how to set up the cath table, prep the patient and set up the manifold.
- Make sure to go over femoral access technique with multiple attendings and cath lab fellows to understand different approaches.
- Complete the consent and H&P on at least the first patient every day (get to the lab at 7 am to do before 7:30 am conference if patient has arrived). Subsequent consents and H&Ps may be completed by the PA, but the first year fellow should assist when available.
- The first year fellow should present patients to the attending prior to the start of the case. Fellows should know patients well prior to scrubbing into a case. A supervising attending must be present for all procedures in the lab.
- Review cath films and hemodynamic tracings with the attending or cath fellow after each case (or all at the end of the day if not time). Be proactive- the first year fellow should specifically ask the attending to go over the angiogram at the conclusion of the case. If there is not time, all angiograms should be reviewed at the end of the day (or during a break) with the attending.
- During the first rotation in the cath lab, the first year fellow must pull 10 sheaths and record them in medhub for review at the end of the rotation. Learning to manage groin hemostasis is a critical skill.
- By the end of the second month, first year fellows should consistently be able to identify fluoroscopy views and distinguish each coronary artery.
- Understand basic cath lab pharmacology, including use of anticoagulation and antiplatelet drugs for elective PCI, NSTEMI, and STEMI. Know the commonly used drugs and doses in each scenario.
- Know the ACC class I and class III guidelines for PCI, NSTEMI, and STEMI.
- Understand basic hemodynamics in the cath lab (the following chapters from Cardiovascular Hemodynamics for the Clinician by Stouffer are minimal reading: 2,3,7,8,9,12,15,16,17,20). Chapters 2, 3, 8 should be read prior to rotation.
- Read the following chapters in Grossman during first rotation: 3,4,11,12.
- ACCF board review lectures on NSTEMI (Delemos) and STEMI (O’Gara) can be accessed by cardiosource plus.
- Mayo DVD lectures on NSTEMI and STEMI are also excellent. Remember to log your procedures in medhub. During the last week of the rotation please meet with Dr. Menees for feedback Landmark Trials in Coronary Artery Disease
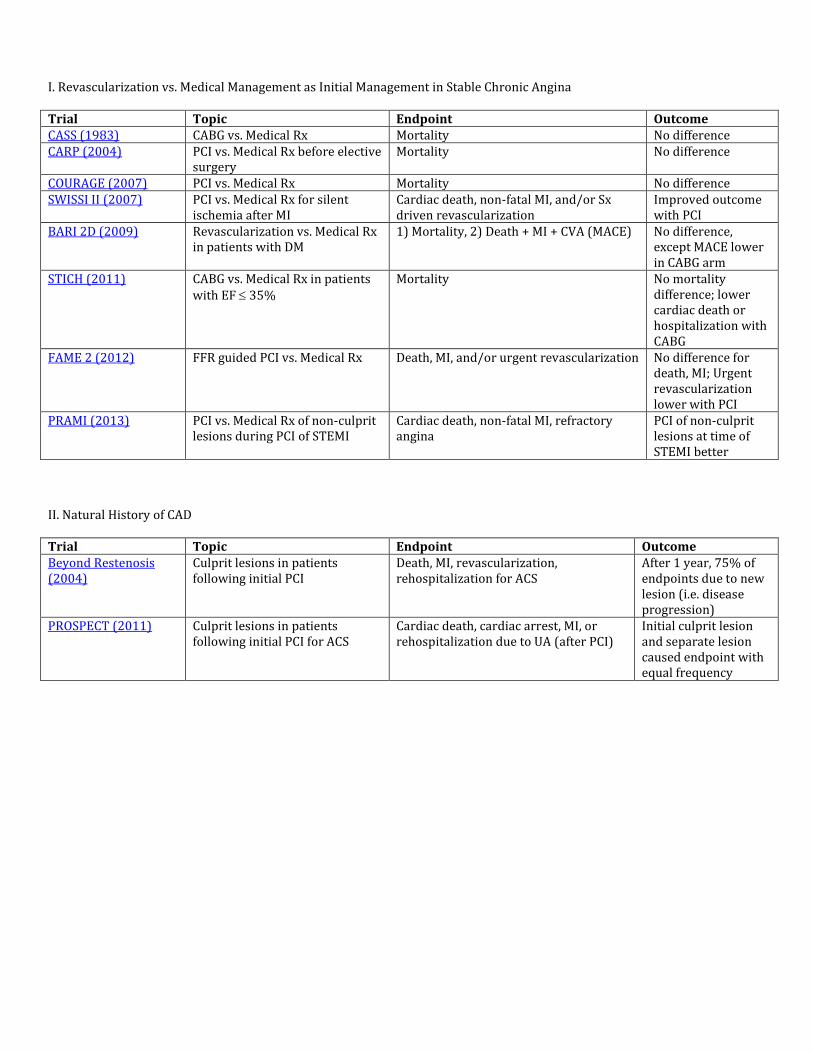
I. Revascularization vs. Medical Management as Initial Management in Stable Chronic Angina Trial Topic Endpoint Outcome CASS (1983) CABG vs. Medical Rx Mortality No difference CARP (2004) PCI vs. Medical Rx before elective
surgery Mortality No difference
COURAGE (2007) PCI vs. Medical Rx Mortality No difference SWISSI II (2007) PCI vs. Medical Rx for silent
ischemia after MI Cardiac death, non-fatal MI, and/or Sx driven revascularization
Improved outcome with PCI
BARI 2D (2009) Revascularization vs. Medical Rx in patients with DM
1) Mortality, 2) Death + MI + CVA (MACE) No difference, except MACE lower in CABG arm
STICH (2011) CABG vs. Medical Rx in patients with EF 35%
Mortality No mortality difference; lower cardiac death or hospitalization with CABG
FAME 2 (2012) FFR guided PCI vs. Medical Rx Death, MI, and/or urgent revascularization No difference for death, MI; Urgent revascularization lower with PCI
PRAMI (2013) PCI vs. Medical Rx of non-culprit lesions during PCI of STEMI
Cardiac death, non-fatal MI, refractory angina
PCI of non-culprit lesions at time of STEMI better
II. Natural History of CAD Trial Topic Endpoint Outcome Beyond Restenosis (2004)
Culprit lesions in patients following initial PCI
Death, MI, revascularization, rehospitalization for ACS
After 1 year, 75% of endpoints due to new lesion (i.e. disease progression)
PROSPECT (2011) Culprit lesions in patients following initial PCI for ACS
Cardiac death, cardiac arrest, MI, or rehospitalization due to UA (after PCI)
Initial culprit lesion and separate lesion caused endpoint with equal frequency
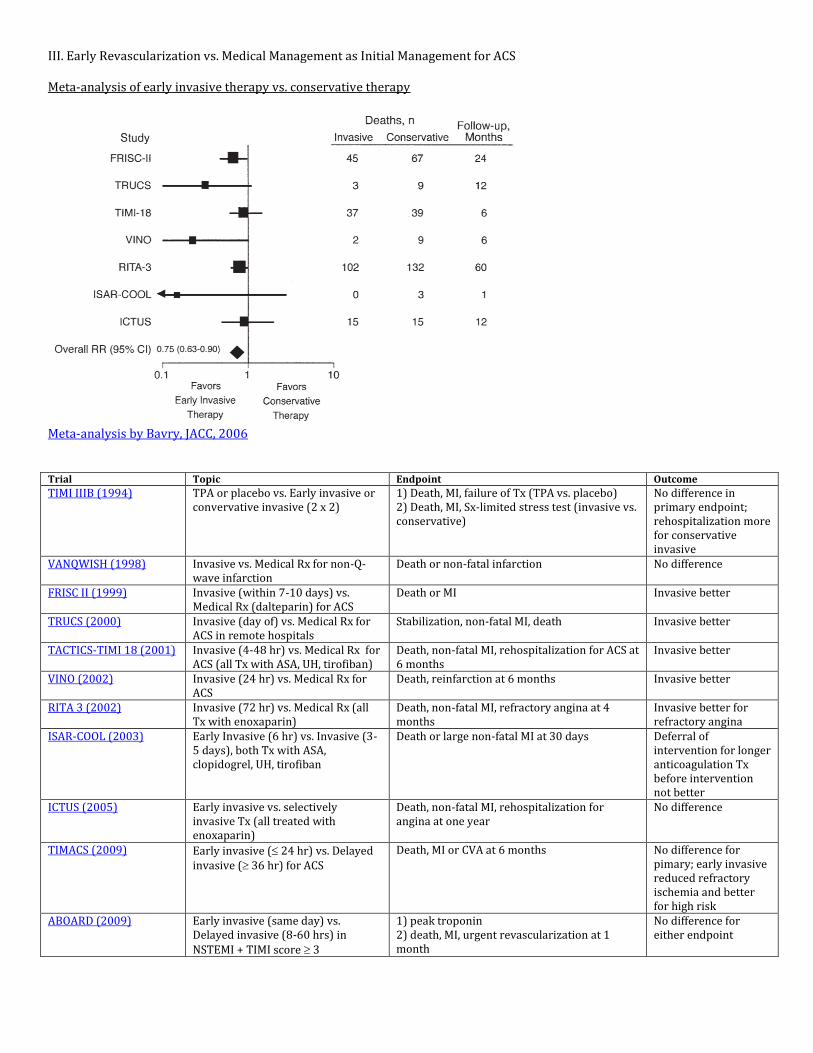
III. Early Revascularization vs. Medical Management as Initial Management for ACS Meta-analysis of early invasive therapy vs. conservative therapy
Meta-analysis by Bavry, JACC, 2006 Trial Topic Endpoint Outcome
TIMI IIIB (1994) TPA or placebo vs. Early invasive or convervative invasive (2 x 2)
1) Death, MI, failure of Tx (TPA vs. placebo) 2) Death, MI, Sx-limited stress test (invasive vs. conservative)
No difference in primary endpoint; rehospitalization more for conservative invasive
VANQWISH (1998) Invasive vs. Medical Rx for non-Q-wave infarction
Death or non-fatal infarction No difference
FRISC II (1999) Invasive (within 7-10 days) vs. Medical Rx (dalteparin) for ACS
Death or MI Invasive better
TRUCS (2000) Invasive (day of) vs. Medical Rx for ACS in remote hospitals
Stabilization, non-fatal MI, death Invasive better
TACTICS-TIMI 18 (2001) Invasive (4-48 hr) vs. Medical Rx for ACS (all Tx with ASA, UH, tirofiban)
Death, non-fatal MI, rehospitalization for ACS at 6 months
Invasive better
VINO (2002) Invasive (24 hr) vs. Medical Rx for ACS
Death, reinfarction at 6 months Invasive better
RITA 3 (2002) Invasive (72 hr) vs. Medical Rx (all Tx with enoxaparin)
Death, non-fatal MI, refractory angina at 4 months
Invasive better for refractory angina
ISAR-COOL (2003) Early Invasive (6 hr) vs. Invasive (3-5 days), both Tx with ASA, clopidogrel, UH, tirofiban
Death or large non-fatal MI at 30 days Deferral of intervention for longer anticoagulation Tx before intervention not better
ICTUS (2005) Early invasive vs. selectively invasive Tx (all treated with enoxaparin)
Death, non-fatal MI, rehospitalization for angina at one year
No difference
TIMACS (2009) Early invasive ( 24 hr) vs. Delayed invasive ( 36 hr) for ACS
Death, MI or CVA at 6 months No difference for pimary; early invasive reduced refractory ischemia and better for high risk
ABOARD (2009) Early invasive (same day) vs. Delayed invasive (8-60 hrs) in NSTEMI + TIMI score 3
1) peak troponin 2) death, MI, urgent revascularization at 1 month
No difference for either endpoint
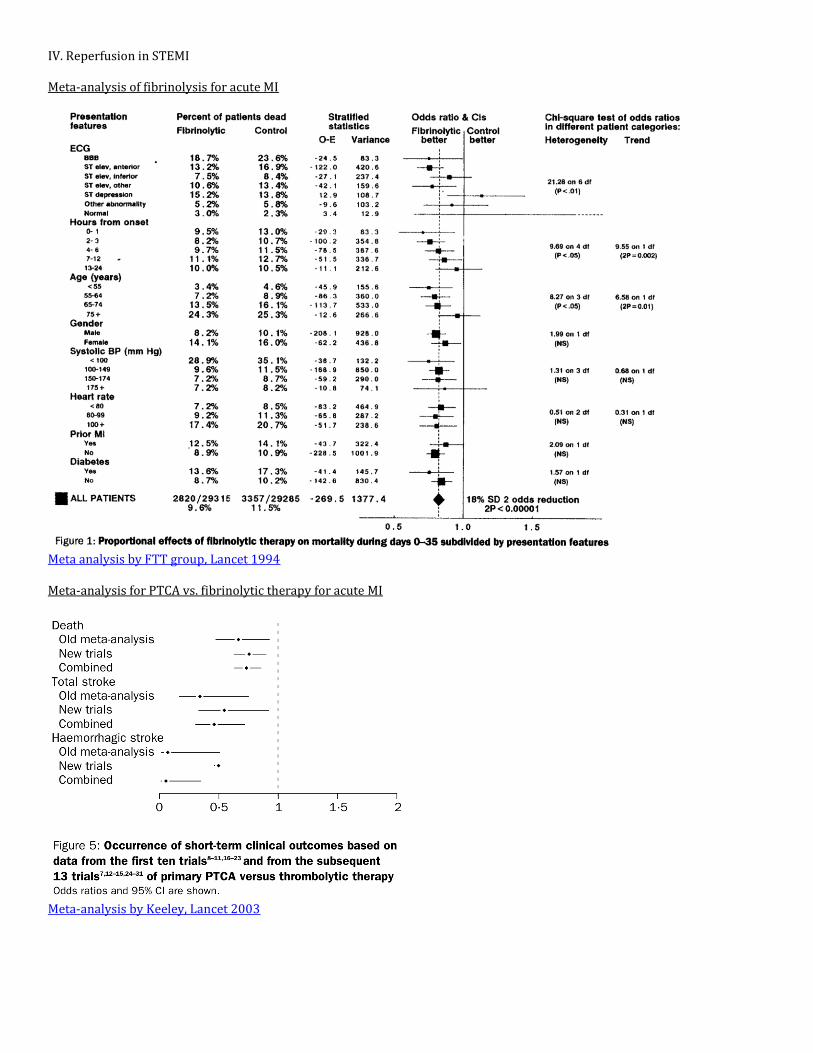
IV. Reperfusion in STEMI Meta-analysis of fibrinolysis for acute MI
Meta analysis by FTT group, Lancet 1994 Meta-analysis for PTCA vs. fibrinolytic therapy for acute MI
Meta-analysis by Keeley, Lancet 2003
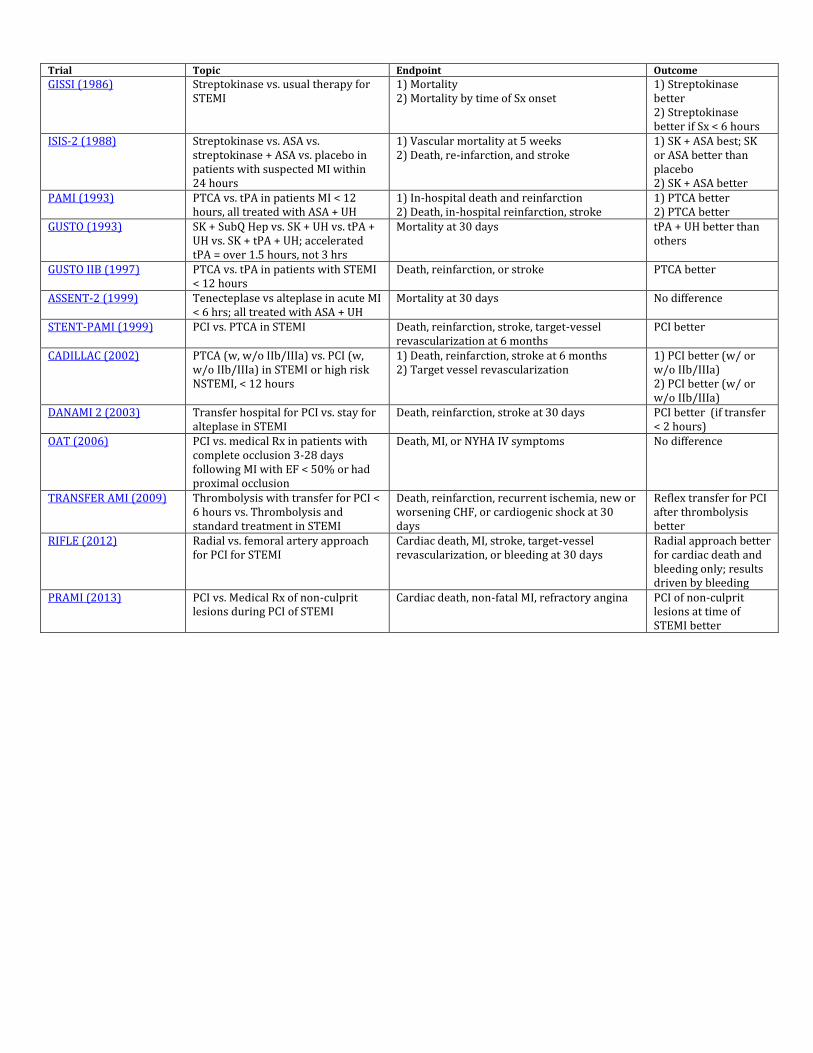
Trial Topic Endpoint Outcome
GISSI (1986) Streptokinase vs. usual therapy for STEMI
1) Mortality 2) Mortality by time of Sx onset
1) Streptokinase better 2) Streptokinase better if Sx < 6 hours
ISIS-2 (1988) Streptokinase vs. ASA vs. streptokinase + ASA vs. placebo in patients with suspected MI within 24 hours
1) Vascular mortality at 5 weeks 2) Death, re-infarction, and stroke
1) SK + ASA best; SK or ASA better than placebo 2) SK + ASA better
PAMI (1993) PTCA vs. tPA in patients MI < 12 hours, all treated with ASA + UH
1) In-hospital death and reinfarction 2) Death, in-hospital reinfarction, stroke
1) PTCA better 2) PTCA better
GUSTO (1993) SK + SubQ Hep vs. SK + UH vs. tPA + UH vs. SK + tPA + UH; accelerated tPA = over 1.5 hours, not 3 hrs
Mortality at 30 days tPA + UH better than others
GUSTO IIB (1997) PTCA vs. tPA in patients with STEMI < 12 hours
Death, reinfarction, or stroke PTCA better
ASSENT-2 (1999) Tenecteplase vs alteplase in acute MI < 6 hrs; all treated with ASA + UH
Mortality at 30 days No difference
STENT-PAMI (1999) PCI vs. PTCA in STEMI Death, reinfarction, stroke, target-vessel revascularization at 6 months
PCI better
CADILLAC (2002) PTCA (w, w/o IIb/IIIa) vs. PCI (w, w/o IIb/IIIa) in STEMI or high risk NSTEMI, < 12 hours
1) Death, reinfarction, stroke at 6 months 2) Target vessel revascularization
1) PCI better (w/ or w/o IIb/IIIa) 2) PCI better (w/ or w/o IIb/IIIa)
DANAMI 2 (2003) Transfer hospital for PCI vs. stay for alteplase in STEMI
Death, reinfarction, stroke at 30 days PCI better (if transfer < 2 hours)
OAT (2006) PCI vs. medical Rx in patients with complete occlusion 3-28 days following MI with EF < 50% or had proximal occlusion
Death, MI, or NYHA IV symptoms No difference
TRANSFER AMI (2009) Thrombolysis with transfer for PCI < 6 hours vs. Thrombolysis and standard treatment in STEMI
Death, reinfarction, recurrent ischemia, new or worsening CHF, or cardiogenic shock at 30 days
Reflex transfer for PCI after thrombolysis better
RIFLE (2012) Radial vs. femoral artery approach for PCI for STEMI
Cardiac death, MI, stroke, target-vessel revascularization, or bleeding at 30 days
Radial approach better for cardiac death and bleeding only; results driven by bleeding
PRAMI (2013) PCI vs. Medical Rx of non-culprit lesions during PCI of STEMI
Cardiac death, non-fatal MI, refractory angina PCI of non-culprit lesions at time of STEMI better
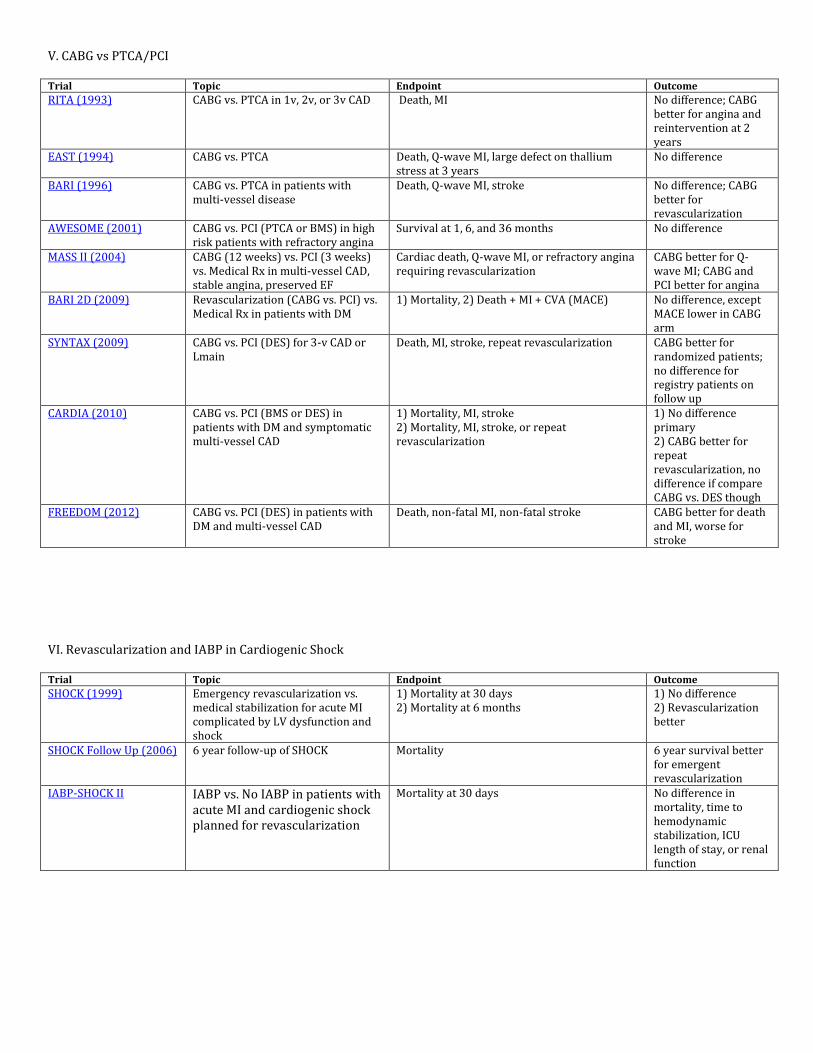
V. CABG vs PTCA/PCI Trial Topic Endpoint Outcome
RITA (1993) CABG vs. PTCA in 1v, 2v, or 3v CAD Death, MI No difference; CABG better for angina and reintervention at 2 years
EAST (1994) CABG vs. PTCA Death, Q-wave MI, large defect on thallium stress at 3 years
No difference
BARI (1996) CABG vs. PTCA in patients with multi-vessel disease
Death, Q-wave MI, stroke No difference; CABG better for revascularization
AWESOME (2001) CABG vs. PCI (PTCA or BMS) in high risk patients with refractory angina
Survival at 1, 6, and 36 months No difference
MASS II (2004) CABG (12 weeks) vs. PCI (3 weeks) vs. Medical Rx in multi-vessel CAD, stable angina, preserved EF
Cardiac death, Q-wave MI, or refractory angina requiring revascularization
CABG better for Q-wave MI; CABG and PCI better for angina
BARI 2D (2009) Revascularization (CABG vs. PCI) vs. Medical Rx in patients with DM
1) Mortality, 2) Death + MI + CVA (MACE) No difference, except MACE lower in CABG arm
SYNTAX (2009) CABG vs. PCI (DES) for 3-v CAD or Lmain
Death, MI, stroke, repeat revascularization CABG better for randomized patients; no difference for registry patients on follow up
CARDIA (2010) CABG vs. PCI (BMS or DES) in patients with DM and symptomatic multi-vessel CAD
1) Mortality, MI, stroke 2) Mortality, MI, stroke, or repeat revascularization
1) No difference primary 2) CABG better for repeat revascularization, no difference if compare CABG vs. DES though
FREEDOM (2012) CABG vs. PCI (DES) in patients with DM and multi-vessel CAD
Death, non-fatal MI, non-fatal stroke CABG better for death and MI, worse for stroke
VI. Revascularization and IABP in Cardiogenic Shock Trial Topic Endpoint Outcome
SHOCK (1999) Emergency revascularization vs. medical stabilization for acute MI complicated by LV dysfunction and shock
1) Mortality at 30 days 2) Mortality at 6 months
1) No difference 2) Revascularization better
SHOCK Follow Up (2006) 6 year follow-up of SHOCK Mortality 6 year survival better for emergent revascularization
IABP-SHOCK II IABP vs. No IABP in patients with acute MI and cardiogenic shock planned for revascularization
Mortality at 30 days No difference in mortality, time to hemodynamic stabilization, ICU length of stay, or renal function
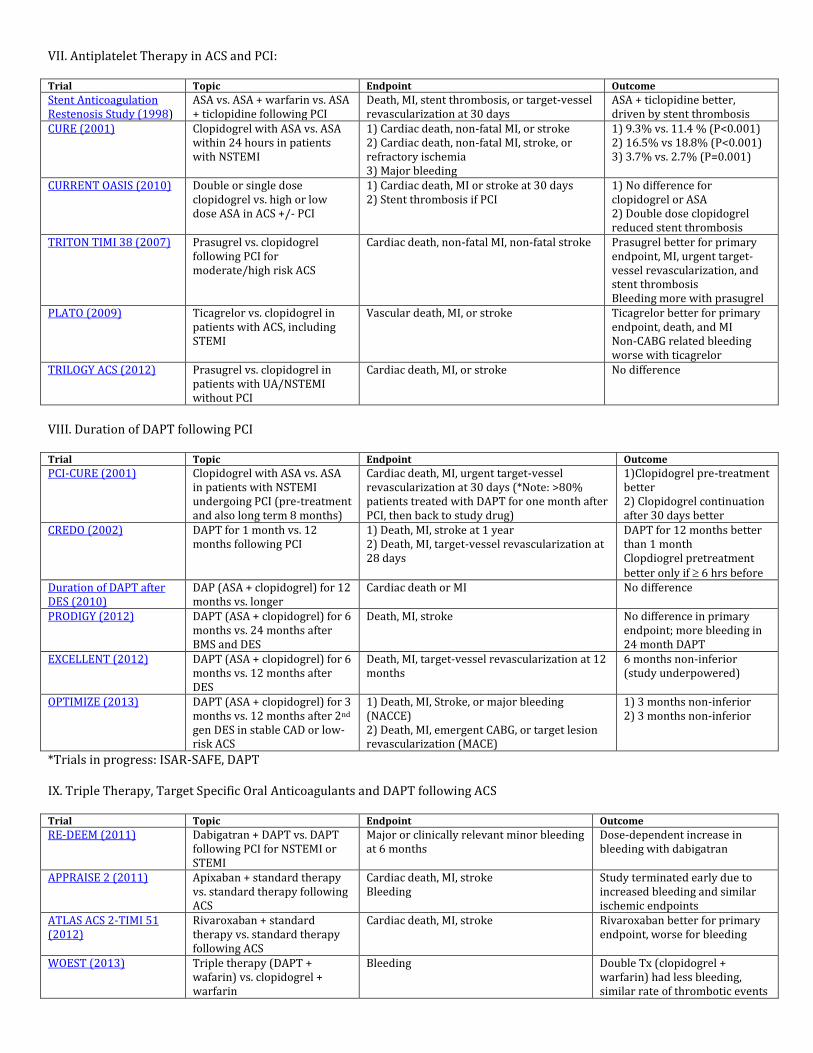
VII. Antiplatelet Therapy in ACS and PCI: Trial Topic Endpoint Outcome
Stent Anticoagulation Restenosis Study (1998)
ASA vs. ASA + warfarin vs. ASA + ticlopidine following PCI
Death, MI, stent thrombosis, or target-vessel revascularization at 30 days
ASA + ticlopidine better, driven by stent thrombosis
CURE (2001) Clopidogrel with ASA vs. ASA within 24 hours in patients with NSTEMI
1) Cardiac death, non-fatal MI, or stroke 2) Cardiac death, non-fatal MI, stroke, or refractory ischemia 3) Major bleeding
1) 9.3% vs. 11.4 % (P<0.001) 2) 16.5% vs 18.8% (P<0.001) 3) 3.7% vs. 2.7% (P=0.001)
CURRENT OASIS (2010) Double or single dose clopidogrel vs. high or low dose ASA in ACS +/- PCI
1) Cardiac death, MI or stroke at 30 days 2) Stent thrombosis if PCI
1) No difference for clopidogrel or ASA 2) Double dose clopidogrel reduced stent thrombosis
TRITON TIMI 38 (2007) Prasugrel vs. clopidogrel following PCI for moderate/high risk ACS
Cardiac death, non-fatal MI, non-fatal stroke Prasugrel better for primary endpoint, MI, urgent target-vessel revascularization, and stent thrombosis Bleeding more with prasugrel
PLATO (2009) Ticagrelor vs. clopidogrel in patients with ACS, including STEMI
Vascular death, MI, or stroke Ticagrelor better for primary endpoint, death, and MI Non-CABG related bleeding worse with ticagrelor
TRILOGY ACS (2012) Prasugrel vs. clopidogrel in patients with UA/NSTEMI without PCI
Cardiac death, MI, or stroke No difference
VIII. Duration of DAPT following PCI Trial Topic Endpoint Outcome
PCI-CURE (2001) Clopidogrel with ASA vs. ASA in patients with NSTEMI undergoing PCI (pre-treatment and also long term 8 months)
Cardiac death, MI, urgent target-vessel revascularization at 30 days (*Note: >80% patients treated with DAPT for one month after PCI, then back to study drug)
1)Clopidogrel pre-treatment better 2) Clopidogrel continuation after 30 days better
CREDO (2002) DAPT for 1 month vs. 12 months following PCI
1) Death, MI, stroke at 1 year 2) Death, MI, target-vessel revascularization at 28 days
DAPT for 12 months better than 1 month Clopdiogrel pretreatment better only if 6 hrs before
Duration of DAPT after DES (2010)
DAP (ASA + clopidogrel) for 12 months vs. longer
Cardiac death or MI No difference
PRODIGY (2012) DAPT (ASA + clopidogrel) for 6 months vs. 24 months after BMS and DES
Death, MI, stroke No difference in primary endpoint; more bleeding in 24 month DAPT
EXCELLENT (2012) DAPT (ASA + clopidogrel) for 6 months vs. 12 months after DES
Death, MI, target-vessel revascularization at 12 months
6 months non-inferior (study underpowered)
OPTIMIZE (2013) DAPT (ASA + clopidogrel) for 3 months vs. 12 months after 2nd gen DES in stable CAD or low-risk ACS
1) Death, MI, Stroke, or major bleeding (NACCE) 2) Death, MI, emergent CABG, or target lesion revascularization (MACE)
1) 3 months non-inferior 2) 3 months non-inferior
*Trials in progress: ISAR-SAFE, DAPT IX. Triple Therapy, Target Specific Oral Anticoagulants and DAPT following ACS Trial Topic Endpoint Outcome
RE-DEEM (2011) Dabigatran + DAPT vs. DAPT following PCI for NSTEMI or STEMI
Major or clinically relevant minor bleeding at 6 months
Dose-dependent increase in bleeding with dabigatran
APPRAISE 2 (2011) Apixaban + standard therapy vs. standard therapy following ACS
Cardiac death, MI, stroke Bleeding
Study terminated early due to increased bleeding and similar ischemic endpoints
ATLAS ACS 2-TIMI 51 (2012)
Rivaroxaban + standard therapy vs. standard therapy following ACS
Cardiac death, MI, stroke Rivaroxaban better for primary endpoint, worse for bleeding
WOEST (2013) Triple therapy (DAPT + wafarin) vs. clopidogrel + warfarin
Bleeding Double Tx (clopidogrel + warfarin) had less bleeding, similar rate of thrombotic events
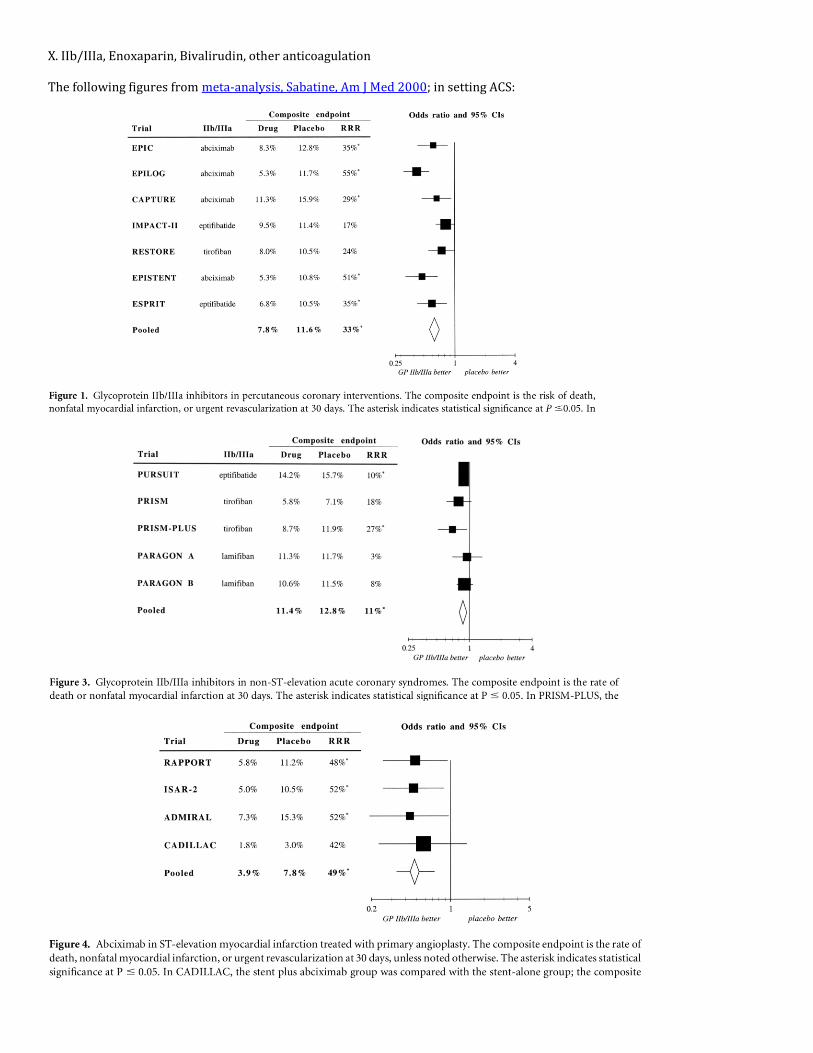
X. IIb/IIIa, Enoxaparin, Bivalirudin, other anticoagulation The following figures from meta-analysis, Sabatine, Am J Med 2000; in setting ACS:
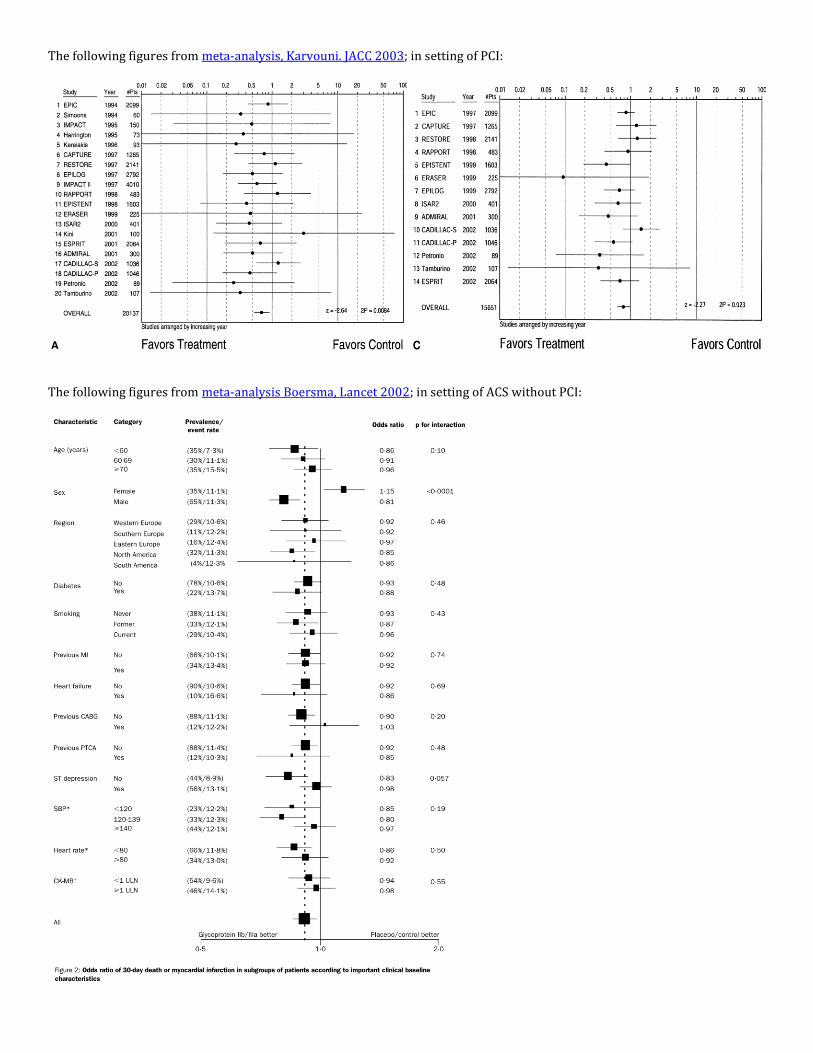
The following figures from meta-analysis, Karvouni. JACC 2003; in setting of PCI:
The following figures from meta-analysis Boersma, Lancet 2002; in setting of ACS without PCI:
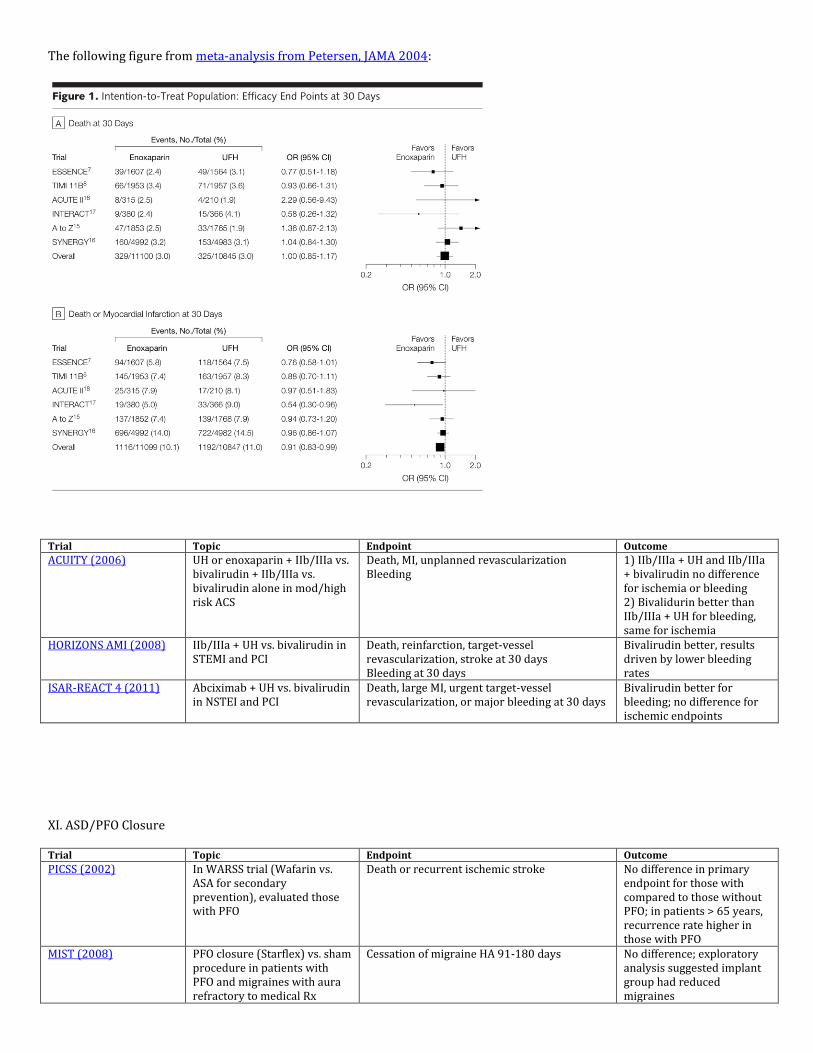
The following figure from meta-analysis from Petersen, JAMA 2004:
Trial Topic Endpoint Outcome
ACUITY (2006) UH or enoxaparin + IIb/IIIa vs. bivalirudin + IIb/IIIa vs. bivalirudin alone in mod/high risk ACS
Death, MI, unplanned revascularization Bleeding
1) IIb/IIIa + UH and IIb/IIIa + bivalirudin no difference for ischemia or bleeding 2) Bivalidurin better than IIb/IIIa + UH for bleeding, same for ischemia
HORIZONS AMI (2008) IIb/IIIa + UH vs. bivalirudin in STEMI and PCI
Death, reinfarction, target-vessel revascularization, stroke at 30 days Bleeding at 30 days
Bivalirudin better, results driven by lower bleeding rates
ISAR-REACT 4 (2011) Abciximab + UH vs. bivalirudin in NSTEI and PCI
Death, large MI, urgent target-vessel revascularization, or major bleeding at 30 days
Bivalirudin better for bleeding; no difference for ischemic endpoints
XI. ASD/PFO Closure Trial Topic Endpoint Outcome
PICSS (2002) In WARSS trial (Wafarin vs. ASA for secondary prevention), evaluated those with PFO
Death or recurrent ischemic stroke No difference in primary endpoint for those with compared to those without PFO; in patients > 65 years, recurrence rate higher in those with PFO
MIST (2008) PFO closure (Starflex) vs. sham procedure in patients with PFO and migraines with aura refractory to medical Rx
Cessation of migraine HA 91-180 days No difference; exploratory analysis suggested implant group had reduced migraines
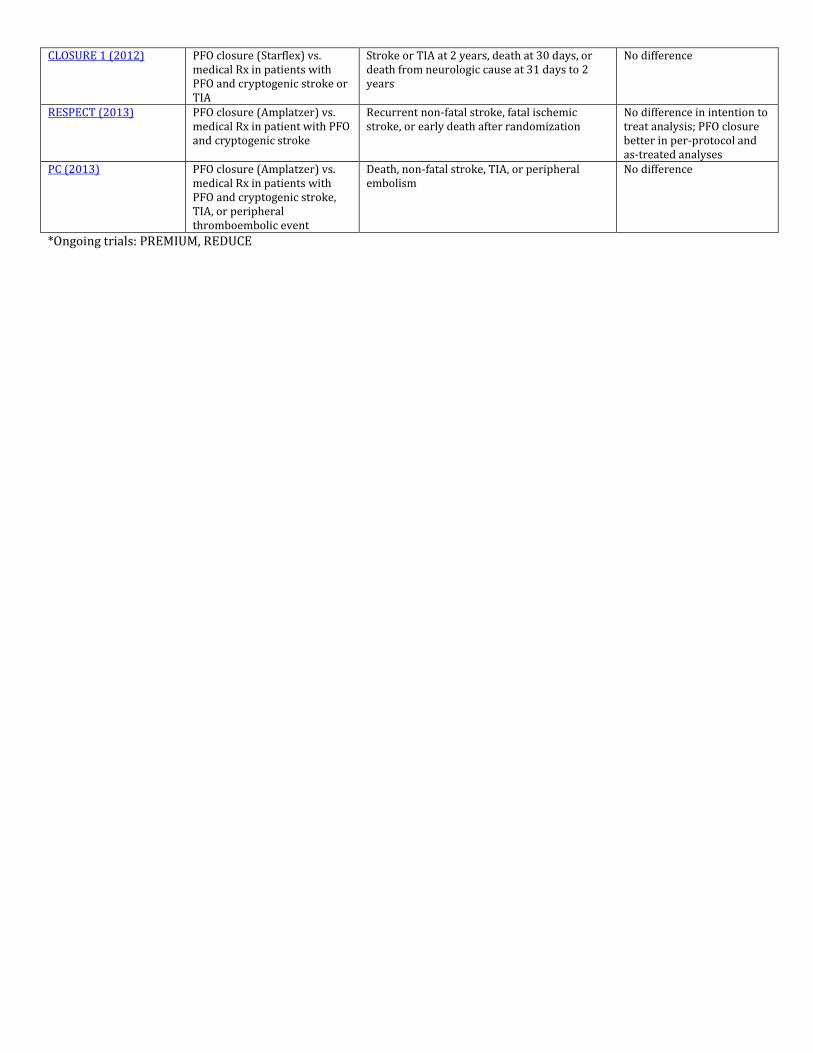
CLOSURE 1 (2012) PFO closure (Starflex) vs. medical Rx in patients with PFO and cryptogenic stroke or TIA
Stroke or TIA at 2 years, death at 30 days, or death from neurologic cause at 31 days to 2 years
No difference
RESPECT (2013) PFO closure (Amplatzer) vs. medical Rx in patient with PFO and cryptogenic stroke
Recurrent non-fatal stroke, fatal ischemic stroke, or early death after randomization
No difference in intention to treat analysis; PFO closure better in per-protocol and as-treated analyses
PC (2013) PFO closure (Amplatzer) vs. medical Rx in patients with PFO and cryptogenic stroke, TIA, or peripheral thromboembolic event
Death, non-fatal stroke, TIA, or peripheral embolism
No difference
*Ongoing trials: PREMIUM, REDUCE