capsaicin an irritant anti-inflammatory compound 21 n1-2.pdf2 promotes premature aging and a wide...
TRANSCRIPT

Journal of Biological Regulators and Homeostatic Agents
0393-974XCopyright © by BIOLIFE, s.a.s
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyrighter holder.
Unauthorized reproduction may result in financial and other penalties1
Capsaicin an irritant anti-inflammatory compound A. ANOGIANAKI1, N.N. NEGREV2, Y.B. SHAIK3, M.L. CASTELLANI4, S. FRYDAS5, J. VECCHIET6,S. TETE7, V. SALINI8, D. DE AMICIS8, M.A. DE LUTIIS9, F. CONTI10, A. CARAFFA11, G. CERULLI11
1Department of Physiology, Faculty of Medicine, Aristotle University of Thessaloniki, Greece2 Department of Physiology and Pathophysiology, Varna University of Medicine, Varna, Bulgaria3 Department of Medicine, Section of Infectious Diseases, Boston University School of Medicine, Boston,
MA, USA4 Immunology Division, Medical School, University of Chieti-Pescara, Chieti, Italy5Parasitology and Parasitic Diseases Departmet, Aristotle University of Thessaloniki, Greece6Clinical of Infectious Diseases, Medical School, University of Chieti-Pescara, Chieti, Italy7Dental School, University of Chieti-Pescara, Chieti, Italy8Orthopedic Division, University of Chieti-Pescara, Chieti, Italy9Biology Unit, Medical School, University of Chieti-Pescara, Chieti, Italy10 Gynaecology Division, University of Chieti, Italy11Orthopedic Division, University of Perugia, Perugia, Italy
Received: February 26, 2006Accepted: March 29, 2006
Since ancient times all around the world humans have found remedies in herbs and plants. Patients often seek complementary therapies including herbal medicines due to reasons such as unsatisfactory effects, high cost, non-availability, or adverse effects of conventional medicines (1-2). Capsaicin is a chemical compound derived from peppers, specifically, capsicum, also known as cayenne (3). Capsaicin is the ingredient found in different types of hot peppers, such as cayenne peppers, that makes the peppers spicy hot (4).
Capsaicin has been used for centuries as a folk medicine for stimulating circulation, aiding digestion and relieving pain (topically). It may also have potential in treating neuropathic pain (5-8). Pharmacologic therapies for pain control include tricylic antidepressants, anticonvulsants, analgesics, and capsaicin (9-12). Capsaicin is used to relieve neuropathic pain, uremic pruritus, and bladder overactivity (5). Vanilloid (capsaicin) receptor subtype 1 (VR1) integrates multiple noxious stimuli on peripheral terminals of primary sensory neurons (13-16). In addition, VR1-expressing neurons are present in a number of brain nuclei and in non-neuronal tissues (17). The expression of VR1 is down-regulated during vanilloid therapy, which might have a pivotal role in desensitization. Evidence suggests an altered VR1 expression in various disease states (18-20). The existence of vanilloid receptors in several brain nuclei as well as in non-neuronal tissues predicts novel,
innovative therapeutic indications for vanilloids (21-22). This recognition may provide novel insights into pathogenesis and may be useful in diagnosis. However, these findings also suggest that vanilloids might cause side-effects.
Pharmacologic therapies for pain control may also include capsaicin. Capsaicin is a specific neurotoxin for type C non-myelinated vesical afferent fibres involved in the transmission of nociceptive stimuli and reorganization of voiding reflexes in disease (5, 23). Capsaicin is a potent anti-inflammatory compound, and has been proposed as a fighter of chronic, sub-clinical inflammation (8, 10). Capsaicin as a blocking agent of neuropeptides, blocks the axon reflex and may exert a curative effect on allergic rhinitis (24). A small pharmacological effect on clinical histamine dose response has also been noted. However, because capsaicin may induce bronchoconstriction, people suffering from chronic obstructive lung disease may be hypersensitive to it (25). Although the results of one study indicate that asthmatics do not develop additional bronchoconstriction following inhalation of capsaicin.
The human nuclear transcription factors (NTFs), two of which—activator protein 1 (AP-1) and NF-kappa B—are especially important targets when it comes to prevention of cancer and premature aging of organs. Each of these NTFs can be “activated” by ultraviolet light and free radicals: a result that produces a pro-inflammatory chain reaction that
EDITORIAL

2
promotes premature aging and a wide variety of degenerative diseases (26). As it turns out, nature offers several effective NTF-activation blockers, including the capsaicin in chilies.
Clinical studies have shown that capsaicin, a compound in hot peppers, is extremely effective for relieving and preventing cluster headaches, migraine headaches, and sinus headaches (27). People suffering from arthritis pain typically have elevated levels in their blood and in the synovial fluid of Substance P which is the key transmitter of pain to the brain. Research has shown that eating foods that contain capsaicin can suppress Substance P production (28).
As a digestive aid, cayenne is known to increase secretion of gastric acids in the stomach (4, 26). Capsaicin may improve digestion by increasing the digestive fluids in the stomach and by fighting bacteria that could cause an infection (20, 29). It may also help fight diarrhea caused by bacterial infection (24). Capsaicin may help prevent heart disease (30). It may stimulate the cardiovascular system and may lower blood cholesterol levels and blood pressure (18). It also helps prevent clotting and hardening of arteries (atherosclerosis) (18). Capsaicin acts as an antioxidant, protecting the cells of the body from damage by harmful molecules called free radicals (27). Capsaicin also may help prevent bacterial infections. Capsaicin may also make mucus thinner and help move it out of the lungs. It is also thought to strengthen lung tissues and help to prevent or treat emphysema.
Biological effect of capsaicinDigestive aid (stimulates gastric secretions) Arthritis pain reliever Raises metabolic rate Reduces allergic symptoms (hay fever-type
allergies) Prevents migraine headaches
Concentrated capsicum in the eyes or in contact with other mucous membranes, causes intense burning sensation. When rubbed on the skin, cayenne can be a very useful analgesic (pain-reliever) with benefits in reducing arthritic pain and stiffness. This effect, called a counterirritant effect, causes a mild irritation when applied to the surface of the skin and “distracts” us from sensing pain from other areas (such as the joint pain common to arthritis).
The development of osteoarthritis is dependent on age, sex, genetic predisposition, and previous trauma to the joint and abnormal mechanical forces caused primarily by obesity. Biochemically, there is an imbalance in the enzymes of cartilage
degradation and cartilage regeneration (21). Pain and inflammation in osteoarthritis may be treated with combinations of pharmacologic (NSAID) and non-pharmacologic (capsaicin) remedies. Contemporary uses have placed cayenne extracts as thermogenic aids to help increase metabolism, an effect that may be related to its ability to dilate blood vessels and cause a local sensation of “warming.” A thermogenic agent, capsaicin helps to increase overall metabolic activity, thus helping the body burn calories and fat.
As indicated above, cayenne contains capsaicin, which can relieve pain by interfering with sensory nerve signaling. In addition to the “confusion” that capsaicin induces in sensory nerves, it also results in a temporary depletion of neurotransmitters from sensory nerves – an effect that reduces the ability of the nerve to sense pain in other areas of the body (31).
Capsaicin can not only cause a mild burning sensation, but it can also cause severe discomfort if you get it in the wrong place (as in the eyes). Used the correct way, no serious side effects are expected from capsaicin ingested in the diet. Caution should be used during pregnancy (to avoid gastrointestinal irritation) and lactation (because capsaicin may pass into breast milk and cause the milk to be unpalatable to the infant).
As a mild digestive aid, cayenne extracts may be somewhat beneficial for individuals with inadequate gastric secretions. For many people, however, gastric secretions are not the primary concern in terms of digestive support (whereas intestinal concerns predominate). As a thermogenic aid to increase metabolism, cayenne may have some modest effects at very high doses (3 grams or more), but these effects are small and the risk of gastrointestinal side effects (heartburn) is high. A specific nerve cell receptor appears to be necessary to initiate the development of inflammatory bowel disease (IBD), a general term given to a variety of chronic disorders in which the intestine becomes inflamed—resulting in recurring abdominal cramps, pain and diarrhea. The cause of IBD is unknown. Capsaicin may lead to a cure for certain intestinal diseases. It is likely that Capsaicin can enhance the effects of conventional medical therapy while mitigating toxic side effects.
Applied to the skin, capsaicin may help relieve pain from:
Pain disorders, including pain after surgery. Nervous system problems such as
diabetic neuropathy, trigeminal neuralgia, and postherpetic neuralgia (shingles).
Cluster headaches.
Capsaicin an irritant anti-inflammatory compound
3
Joint problems such as osteoarthritis and rheumatoid arthritis.
Skin conditions such as psoriasis. Mouth sores due to chemotherapy or radiation.In general, capsaicin gives relief from pain.
When capsaicin is applied in the skin (up to 4 times a day) provokes burning or/and itching sensation
When you eat hot peppers, the capsaicin may improve your digestion by increasing the digestive fluids in the stomach and by fighting bacteria that could cause an infection. It may also help fight diarrhea caused by bacterial infection. Capsaicin is very effective in fighting and preventing chronic sinus infections (sinusitis) and chronic nasal congestion. This purely natural chemical will also clear out congested nasal passages like nothing else, and is helpful in treating sinus-related allergy symptoms. Capsaicin may help prevent heart disease. It may stimulate the cardiovascular system and may lower blood cholesterol levels and blood pressure. In fact, capsaicin is considered an actively “heart healthy” compound. Capsaicin acts as an antioxidant, protecting the cells of the body from damage by harmful molecules (free radicals). It also helps prevent clotting and hardening of arteries (atherosclerosis).
Several recent studies have shown that capsaicin may actually prevent the growth of certain types of cancer (28). Scientists concluded that daily consumption of hot peppers may actually prevent certain types of cancer. In fact, throughout South America, intestinal, stomach, and colon cancer rates are very low compared to other countries. It is widely regarded by medical experts that this low cancer rate may be tied to the large amounts of capsaicin in their diets. Of course, we must also take into consideration the fact that these cultures also consume fiber-rich beans on a daily basis.
REFERENCES
1. Lim K, Yoshioka M, Kikuzato S, Kiyonaga A, Tanaka H, Shindo M, Suzuki M. Dietary red pepper ingestion increases carbohydrate oxidation at rest and during exercise in runners. Med Sci Sports Exerc 1997; 29:355-61.
2. Miller CH, Zhang Z, Hamilton SM, Teel RW. Effects of capsaicin on liver microsomal metabolism of the tobacco-specific nitrosamine NNK. Cancer Lett 1993; 75:45-52.
3. Egger G, Cameron-Smith D, Stanton R. The effectiveness of popular, non-prescription weight loss supplements. Med J Aust 1999; 171:604-8.
4. Guengerich FP. Influence of nutrients and other dietary materials on cytochrome P-450
enzymes. Am J Clin Nutr 1995; 61:651S-658S. 5. Thomas C, Kim JH, Torimoto K, Kwon DD, Kim
YT, Tyagi P, Yoshimura N, Chancellor MB. Early capsaicin intervention for neurogenic bladder in a rat model of spinal cord injury. Biomed Res 2007; 28:255-9.
6. Mayerhofer M, KJ Aichberger, S Florian, P Valent. Recognition-sites for microbes and components of the immune system on human mast cells: relationship to CD antigens and implications for host defense. Int J Immunopathol Pharmacol 2007; 20:421-434.
7. Cinnella G, Vendemiale G Dambrosio M, Serviddio G, Pugliese PL, G Aspromonte, E Altomare. Effect of Propofol, Sevoflurane and desflurane on systemic redox balance. Int J Immunopathol Pharmacol 2007; 20:585-594
8. Sbarsi I, Falcone C, Boiocchi C, Campo I, Zorzetto M, De Silvestri A, Cuccia M. Inflammation and atherosclerosis: the role of TNF nd TNF receptors polymorphisms in coronary artery disease. Int J Immunopathol Pharmacol 2007; 20:145-154.
9. Ro JY, Lee J, Capra NF, Zhang Y. Role of soluble guanylate cyclase in the trigeminal subnucleus caudalis in capsaicin-induced muscle hypersensitivity. Brain Res 2007; 1184:141-8.
10. Castellani ML, Bhattacharya K, Tagen M, Kempuraj D, Perrella A, De Lutiis M, Boucher W, Conti P, Theoharides TC. Anti-chemokine therapy for inflammatory diseases. Int J Immunopathol Pharmacol 2007; 20:447-454.
11. D’Alimonte I, Ciccarelli R, Di Iorio P, Nargi E, Buccella S, Giuliani P, Rathbone MP, Jiang S, Caciagli F, Ballerini P. Activation of P2X7 receptors stimulates the expression of P2Y2 receptor mRNA in astrocytes cultured from rat brain. Int J Immunopathol Pharmacol 2007;20:301-315.
12. Deviri E, Glenville BE. Inflammatory response in infective endocarditis. Eur J Inflamm 2007; 5: 57-63.
13. Aprile I, Tonali P, Stalberg E, Di Stasio E, Caliandro P, Foschini M, Vergili G, Padua L. Double peak sensory responses: effects of capsaicin. Neurol Sci 2007; 28:264-9.
14. Rosati E, Mencarelli S, Magini A, Sabatini R, Tassi C, Orlacchio A, Coaccioli S, Frenguelli A, Marconi P, Emiliani C. Enhancement of lysosomal glycohydrolase activity in human primary B lymphocytes during spontaneous apoptosis. Int J Immunopathol Pharmacol 2007; 20:279-288.
15. Ingber A, Cohen Y, Krimsky M, Yedgar S. A novel treatment of contact dermatitis by topical
Anogianaki et al
4
application of phospholipase A2 inhibitor: a double-blind placebo controlled pilot study. Int J Immunopathol Pharmacol 2007; 20:191-195.
16. Caroselli C, Plocco M, Pratticò F, Bruno C, Antonaglia C, Rota F, Curreli I, Caroselli A, Bruno G. Ulcerative colitis masked by giant urticaria. Int J Immunopathol Pharmacol 2007; 20:181-184.
17. Garozzo A, Tempera G, Ungheri D, Timpanaro R, Castro A. N-acetylcysteine synergizes with oseltamivir in protecting mice from lethal influenza infection. Int J Immunopathol Pharmacol 2007; 20:349-354.
18. Pyun BJ, Choi S, Lee Y, Kim TW, Min JK, Kim Y, Kim BD, Kim JH, Kim TY, Kim YM, Kwon YG. Capsiate, a nonpungent capsaicin-like compound, inhibits angiogenesis and vascular permeability via a direct inhibition of Src kinase activity. Cancer Res 2008; 68:227-35.
19. di Lorenzo L, Vacca A, Corfiati M, Lovreglio P, Soleo L. Evaluation of tumor necrosis factor-alpha and granulocyte colony-stimulating factor serum levels in lead-exposed smoker workers. Int J Immunopathol Pharmacol 2007; 20:239-247.
20. Di Bonaventura G, Piccolomini R, Pompilio A, Zappacosta R, Piccolomini M, Neri M. Serum and mucosal cytokine profiles in patients with active Helicobacter pylorind ischemic heart disease: is there a relationship? Int J Immunopathol Pharmacol 2007; 20: 163-172.
21. Surh Y. Molecular mechanisms of chemopreventive effects of selected dietary and medicinal phenolic substances. Mutat Res 1999; 428:305-27.
22. Ciardelli L, Garofoli F, Avanzini MA, De Silvestri A, Gasparoni A, Sabatino G, Stronati M. Escherichia coli specific secretory IgA and cytokines in human milk from mothers of different ethnic groups resident in northern Italy. Int J Immunopathol Pharmacol 2007; 20:335-340.
23. Ahangari G, Chavoshzadeh Z, Lari Z, Ramyar A, Farhoudi A. Novel mutation detection of an inflammatory molecule Elastase II gene encoding neutrophil Elastase in Kostmann
syndrome. Eur J Inflamm 2007; 5:65-7124. Banche G, Allizond V, Mandras N, Garzaro
M, Cavallo GP, Baldi C, Scutera S, Musso T, Roana J, Tullio V, Carlone NA, Cuffini AM. Improvement of clinical response in allergic rhinitis patients treated with an oral immunostimulating bacterial lysate: in vivo immunological effects. Int J Immunopathol Pharmacol 2007; 20: 129-138.
25. Ciprandi G, Cirillo I, Troisi RM, Marseglia GL. Allergic subjects have more numerous respiratory infections and severe gastrointestinal infections than non-allergic subjects: preliminary results. Eur J Inflamm 2007; 5:27-29.
26. Komori Y, Aiba T, Nakai C, Sugiyama R, Kawasaki H, Kurosaki Y. Capsaicin-induced increase of intestinal cefazolin absorption in rats. Drug Metab Pharmacokinet. 2007; 22:445-9.
27. Yoshioka M, St-Pierre S, Drapeau V, Dionne I, Doucet E, Suzuki M, Tremblay A. Effects of red pepper on appetite and energy intake. Br J Nutr 1999; 82:115-23.
28. Lopez-Carrillo L, Hernandez Avila M, Dubrow R. Chili pepper consumption and gastric cancer in Mexico: a case-control study. Am J Epidemiol 1994; 139:263-71.
29. Montagna M, Avanzini MA, Visai L, Locatelli F, Montillo M, Morra E, Regazzi MB. A new sensitive enzyme-linked immunosorbent assay (ELISA) for Alemtuzumad determination: development, validation and application. Int J Immunopathol Pharmacol 2007; 20:363-372.
30. Yamasaki M, Ebihara S, Ebihara T, Freeman S, Yamanda S, Asada M, Yoshida M, Arai H. Cough reflex and oral chemesthesis induced by capsaicin and capsiate in healthy never-smokers. Cough. 2007;3:9-17.
31. Gazerani P, Andersen OK, Arendt-Nielsen L. Site-specific, dose-dependent, and sex-related responses to the experimental pain model induced by intradermal injection of capsaicin to the foreheads and forearms of healthy humans. J Orofac Pain 2007;21:289-302.
Capsaicin an irritant anti-inflammatory compound
Journal of Biological Regulators and Homeostatic Agents
0393-974XCopyright © by BIOLIFE, s.a.s
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyrighter holder.
Unauthorized reproduction may result in financial and other penalties5
CD157 is part of a supramolecular complex with CD11b/CD18 on the human neutrophil cell surfaceL. LAVAGNO, E. FERRERO, E. ORTOLAN, F. MALAVASI, A. FUNARO
Laboratory of Immunogenetics, Department of Genetics, Biology and Biochemistry, University of Torino, and CeRMS Research Center for Experimental Medicine, Torino, Italy
Received: January 15, 2006Accepted: March 23, 2006
ABSTRACT: CD157 is a GPI-anchored cell surface glycoprotein expressed by human peripheral blood neutrophils. Cross-linking of CD157 induces intracellular Ca2+ mobilization and re-shaping in neutrophils, thus regulating their adhesive and migratory properties. Results obtained by immunolocalization and confocal microscopy indicate that CD157 lies in close proximity to the CD11b/CD18 complex which is strongly expressed on the activated neutrophil cell membrane where it plays a predominant role in adhesion. This study analyses the physical association between CD157 and CD18 in human neutrophils by co-immunoprecipitation experiments. The anti-CD157 monoclonal antibody RF3 co-precipitates CD18, and the anti-CD18 antibody TS1/18 co-precipitates CD157 from human neutrophil lysates. These results confirm that CD157 physically interacts with CD11b/CD18 complex in human neutrophils.
KEY WORDS: CD157, ectoenzyme, integrin, neutrophil
INTRODUCTION
CD157 is a glycosyl-phosphatidylinositol (GPI)-anchored cell surface glycoprotein mainly expressed by cells of the myeloid lineage, bone marrow stroma and endothelium (1-4) where it acts simultaneously as both receptor (5) and enzyme (6). Molecular cloning revealed that CD157 belongs to the eukaryotic NAD glycohydrolase/ADP-ribosyl cyclase gene family (7). CD157 is a paralog of CD38, a lymphoid ectoenzyme receptor implicated in the regulation of both the innate and adaptive immune responses (8).
A functional role of CD157 in inflammation seemed plausible in view of its expression in neutrophils and endothelial cells. This hypothesis was first confirmed by demonstrating that CD157 cross-linking induces a phosphatidyl-inositol 3-kinase-dependent increase in intracellular Ca2+ in human neutrophils, and promotes cell polarization with profound modifications of the cytoskeleton and cell polarity (9), the hallmarks of neutrophil migration. F-actin re-locates to the cell front or leading edge of polarized cells, and CD157 is enriched at the back of the cell, within the retracting uropod. Similar effects can be observed when
neutrophils are activated by N-formyl-Met-Leu-Phe (fMLP). In addition, we recently demonstrated that CD157 orchestrates neutrophil migration across human endothelium (10).
The intrinsic structural inability of GPI-anchored CD157 to signal might be overcome by assuming strong lateral interactions or selective membrane localization close to professional receptors, a strategy adopted by many other GPI-linked proteins (11) and also by its paralog CD38 which is instead a type II transmembrane protein (12). Among the potential candidates, we considered the CD11b/CD18 heterodimer and member of the β
2 integrin
family which is a key effector of neutrophil migration (13). It has been established that integrins and their partner receptors recruit transmembrane signalling molecules from distinct membrane complexes to each receptor’s mutual benefit (13).
Immunolocalization and confocal microscopy showed that CD157, CD11b and CD18 are physically juxtaposed in neutrophils after β
2
integrin ligand binding (9). In addition, the downstream events elicited by CD157 signaling can be prevented by neutrophil pretreatment with an anti-CD18 monoclonal antibody (mAb) (9). The goal of this study is to demonstrate a

6
structural interaction between CD157 and CD18 by co-immunoprecipitation experiments. This would support the hypothesis that CD157 signals by exploiting the β
2 integrin pathway.
MATERIALS AND METHODS
Antibodies and reagentsThe mouse anti-human CD157 mAbs RF3
(IgG2a
) and Bec-7 (IgG1) were kindly provided by
K. Ishihara and T. Hirano, Osaka University, Japan (2). The mouse anti-human CD18 mAb MEM-148 (IgG
1) was purchased from Serotec (Milan, Italy)
while anti-CD18 TS1/18 (IgG2a
) and anti-CD11b mAb 107 (IgG
1) were provided by M.A. Arnaout,
Harvard Medical School, Boston, MA. TS1/18, 107 and P3.X63.Ag8 (IgG
1 secreted by a mouse
myeloma) isotype control mAb were purified by affinity chromatography as described (14). Tetramethylrhodamine isothiocyanate (TRITC)-conjugated avidin, fluorescein isothiocyanate (FITC)-labelled F(ab’)
2-RaMIg were purchased from
Jackson ImmunoResearch (ListarFish, Milan, Italy). Protease Inhibitor Cocktail and anti-mouse-IgG-conjugated agarose beads were purchased from Sigma-Aldrich (Milan, Italy).
Isolation of peripheral blood polymorphonuclear leukocytes
Blood was obtained by venipuncture from healthy donors and centrifuged through Ficoll-Paque (Amersham Biosciences, Milan, Italy). Polymorphonuclear leukocytes (PMNs) were isolated by sedimentation in 1% gelatin in Ca2+/Mg2+-free PBS, followed by hypotonic lysis (20 sec in H
2O) of erythrocytes. Isolated PMN were >95%
pure and expressed the CD11b/CD18 complex, according to flow cytometric analysis (9).
Immunofluorescence and flow cytometryPMNs (3x105/samples) were suspended in
PBS added with 0.5% bovine serum albumin (BSA) and incubated with 5 μg/mL of the selected mAb (30 min, 4°C). After washing, cells were additionally incubated with F(ab’)
2-RaMIg-FITC and
fluorescence was analyzed using a FACSCalibur flow cytometer and CellQuest software (Becton Dickinson, Milan, Italy). Background mAb binding was estimated by means of isotype-matched negative control mAb.
Laser confocal microscopyPMNs were initially incubated with saturating
amounts of RF3-biotin mAb (20 min, 4°C), successively with avidin-TRITC (60 min, 4oC),
washed, fixed with 4% paraformaldehyde (PFA) and finally incubated with anti-CD11b-FITC (15 min, 4°C). The slides were analyzed using an Olympus FV300 confocal microscope equipped with a Green Helium Neon (543 nm) laser, a Blue Argon (488 nm) laser, and Fluo View 300 software (Olympus Biosystem, Milan, Italy).
Co-immunoprecipitation and Western blottingPMNs (~1 x 108 cells) were solubilized in
lysis buffer (0.5% NP-40 detergent, 20 mM Tris-HCl pH 7.6, 100 mM NaCl, 5 mM EDTA) in the presence of protease inhibitors. Lysates were pre-cleared with P3.X63.Ag8 mAb (2 hrs with gentle rotation), followed by the addition of anti-mouse-IgG-conjugated agarose beads and overnight rotation at 4°C. After centrifugation, the supernatant was divided into 3 aliquots, incubated with RF3 (anti-CD157), TS1/18 (anti-CD18) and P3.X63.Ag8 control mAbs respectively used at a final concentration of 2 μg/ml. Following 2 hrs of gentle rotation at 4°C, anti-mouse-IgG-conjugated agarose beads were added and left overnight at 4°C. After extensive washing, immunoprecipitates were eluted from beads by boiling 5 min in SDS sample buffer in non-reducing conditions. Immunoprecipitates were analysed by 8% SDS-PAGE and western blot. Eluates were transferred onto PVDF membranes and probed with either MEM-148 (anti-CD18) or with Bec-7 (anti-CD157) mAbs. As controls, each gel included a sample of the P3.X63.Ag8 eluate, anti-mouse-IgG-conjugated agarose beads eluate, and an aliquot of the mAbs used for immunoprecipitation. Immunoreactive bands were detected by ECL (Western Lightning Chemi-luminescence Reagent Plus, Perkin Elmer Life Sciences, Milan, Italy).
RESULTS
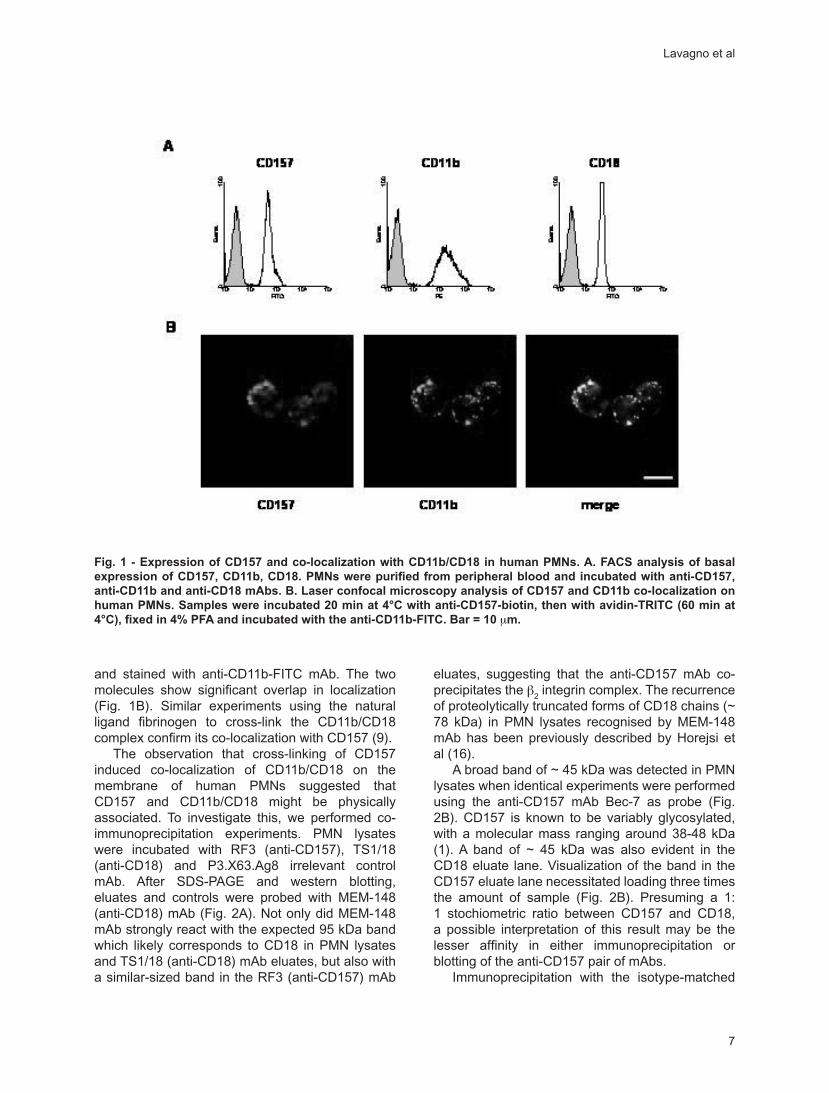
It is well known that PMNs isolated by density gradient centrifugation from peripheral blood uni-formly express CD11b (15). To evaluate expression of CD157 and CD18, human PMN were isolated from peripheral blood and analysed by immunofluo-rescence and flow cytometry. The results show that both CD157 and CD18 are expressed by all circulat-ing PMNs at high epitope density (Fig. 1A). On the other hand CD38, a sibling of CD157, is absent or expressed at very low levels by a small percentage of cells with significant interdonor variability (9).
By confocal analysis, next we evaluated the functional co-localization of CD157 and CD11b/CD18. PMNs were incubated with biotinylated anti-CD157 mAb, cross-linked with avidin-TRITC, fixed
CD157 is part of a supramolecular complex with CD11b/CD18
7
and stained with anti-CD11b-FITC mAb. The two molecules show significant overlap in localization (Fig. 1B). Similar experiments using the natural ligand fibrinogen to cross-link the CD11b/CD18 complex confirm its co-localization with CD157 (9).
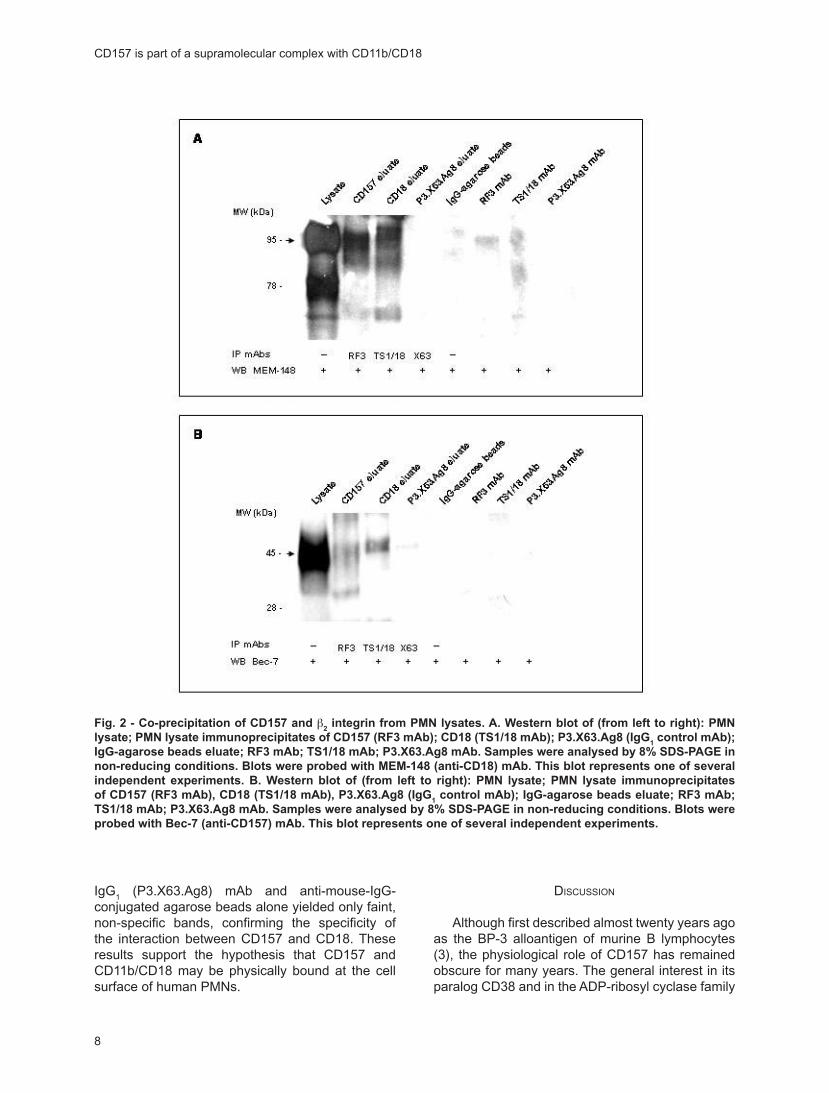
The observation that cross-linking of CD157 induced co-localization of CD11b/CD18 on the membrane of human PMNs suggested that CD157 and CD11b/CD18 might be physically associated. To investigate this, we performed co-immunoprecipitation experiments. PMN lysates were incubated with RF3 (anti-CD157), TS1/18 (anti-CD18) and P3.X63.Ag8 irrelevant control mAb. After SDS-PAGE and western blotting, eluates and controls were probed with MEM-148 (anti-CD18) mAb (Fig. 2A). Not only did MEM-148 mAb strongly react with the expected 95 kDa band which likely corresponds to CD18 in PMN lysates and TS1/18 (anti-CD18) mAb eluates, but also with a similar-sized band in the RF3 (anti-CD157) mAb
eluates, suggesting that the anti-CD157 mAb co-precipitates the β
2 integrin complex. The recurrence
of proteolytically truncated forms of CD18 chains (~ 78 kDa) in PMN lysates recognised by MEM-148 mAb has been previously described by Horejsi et al (16).
A broad band of ~ 45 kDa was detected in PMN lysates when identical experiments were performed using the anti-CD157 mAb Bec-7 as probe (Fig. 2B). CD157 is known to be variably glycosylated, with a molecular mass ranging around 38-48 kDa (1). A band of ~ 45 kDa was also evident in the CD18 eluate lane. Visualization of the band in the CD157 eluate lane necessitated loading three times the amount of sample (Fig. 2B). Presuming a 1:1 stochiometric ratio between CD157 and CD18, a possible interpretation of this result may be the lesser affinity in either immunoprecipitation or blotting of the anti-CD157 pair of mAbs.
Immunoprecipitation with the isotype-matched
Fig. 1 - Expression of CD157 and co-localization with CD11b/CD18 in human PMNs. A. FACS analysis of basal expression of CD157, CD11b, CD18. PMNs were purified from peripheral blood and incubated with anti-CD157, anti-CD11b and anti-CD18 mAbs. B. Laser confocal microscopy analysis of CD157 and CD11b co-localization on human PMNs. Samples were incubated 20 min at 4°C with anti-CD157-biotin, then with avidin-TRITC (60 min at 4°C), fixed in 4% PFA and incubated with the anti-CD11b-FITC. Bar = 10 μm.
Lavagno et al
8
IgG1 (P3.X63.Ag8) mAb and anti-mouse-IgG-
conjugated agarose beads alone yielded only faint, non-specific bands, confirming the specificity of the interaction between CD157 and CD18. These results support the hypothesis that CD157 and CD11b/CD18 may be physically bound at the cell surface of human PMNs.
DISCUSSION
Although first described almost twenty years ago as the BP-3 alloantigen of murine B lymphocytes (3), the physiological role of CD157 has remained obscure for many years. The general interest in its paralog CD38 and in the ADP-ribosyl cyclase family
Fig. 2 - Co-precipitation of CD157 and β2 integrin from PMN lysates. A. Western blot of (from left to right): PMN
lysate; PMN lysate immunoprecipitates of CD157 (RF3 mAb); CD18 (TS1/18 mAb); P3.X63.Ag8 (IgG1 control mAb);
IgG-agarose beads eluate; RF3 mAb; TS1/18 mAb; P3.X63.Ag8 mAb. Samples were analysed by 8% SDS-PAGE in non-reducing conditions. Blots were probed with MEM-148 (anti-CD18) mAb. This blot represents one of several independent experiments. B. Western blot of (from left to right): PMN lysate; PMN lysate immunoprecipitates of CD157 (RF3 mAb), CD18 (TS1/18 mAb), P3.X63.Ag8 (IgG
1 control mAb); IgG-agarose beads eluate; RF3 mAb;
TS1/18 mAb; P3.X63.Ag8 mAb. Samples were analysed by 8% SDS-PAGE in non-reducing conditions. Blots were probed with Bec-7 (anti-CD157) mAb. This blot represents one of several independent experiments.
CD157 is part of a supramolecular complex with CD11b/CD18

9
has brought increased attention to CD157, which differs from its more illustrious relative in terms of structure and tissue distribution. Both molecules are dual-function ectoenzymes and receptors, although CD157 is strictly a NAD+ glycohydrolase and appears not to have the same capacity of CD38 to convert NAD+ to the calcium-mobilizing second messengers cyclic ADPR (cADPR) and nicotinamide adenine ADP (NAADP) (6, 9, 17).
An important clue that members of the NADase/ADP-ribosyl cyclase gene family are involved in the regulation of the innate immune response came from the observation that CD38-/- mice show increased susceptibility over controls to S. pneumoniae infection, owing to a defect in neutrophil chemotaxis (18). Receptors critical for immune function may differ in man and mouse: indeed, the results obtained by experiments of chemotaxis show that human neutrophil migration is not influenced by CD38 but by CD157. These findings could also be read as the functional replacement of one gene family member by another in different species and explain the lack of a marked phenotype in CD38-
/- mice.Our previous observations led to the conclusion
that the receptorial activity of CD157 is directly or indirectly involved in the modulation of human neutrophil migration and adhesion (9). We also suggested that the spatial proximity of CD157 to CD11b/CD18 on the membrane of neutrophils might indicate the assembly of a dynamic signalling complex, similar to those formed when b
2 integrin pairs with other molecules such as the
GPI-anchored CD14 (19), CD87 (20), and GPI-80 (21). However, the capacity of integrins to serve as signalling partners may not be limited to members of the GPI family: indeed, integrins can co-cluster with other types of transmembrane receptors including CD9 (22), CD81 (23) and CD151 (13), all of which are members of the tetraspanin family. Subsequent steps of cell migration use a G-protein-coupled signaling cascade that is evolutionarily conserved from Dictyostelium to mammals (24).
The results reported here confirm that CD157 and CD11b/CD18 are spatially juxtaposed and are actually physically bound to one another, according to the co-immunoprecipitation experiments presented here. The experimental model adopted is centred on human neutrophils, where membrane perturbation induced by the isolation procedure leads CD11b/CD18 to translocate from intracellular pools to the plasma membrane (9, 15), where the dimer is joined by CD157 (9). The CD157 domain involved in the interaction described here with CD11b/CD18 is not yet known. A number of studies
demonstrated that other GPI-linked molecules such as CD14, CD16, CD87 and GPI-80 also signal through membrane-spanning integrins (25, 26). Several of these GPI-linked receptors appears to form cis interactions with a lectin site on the integrin (27) contributing to its acquiring an active conformation (13, 28). The association between CD157 and CD11b/CD18 complex is indirectly supported by the recent observation that CD38 (the other member of the family) also associates with the complex in human dendritic cells (29). Although CD157 and CD38 present inverse membrane topology, their highly conserved 3-D structure suggests that CD157 and CD38 may share features in their interaction with the CD11b/CD18 complex in myeloid cells: this issue may deserve further investigation in the light of the impact of CD38 and CD157 in regulating processes critical for the immune response (30, 31).
We conclude that CD157 physically associates with CD11b/CD18, a member of the integrin family. This supramolecular complex may provide a signalling mechanism through which the receptorial activity of CD157 is fulfilled.
ACKNOWLEDGEMENTS
This work was supported by AIRC (the Italian Cancer Research Association), by P.R.I.N. grants (to AF, to FM) from the Ministry for Education, Universities and Research, and by the Special Project “Oncologia” Compagnia San Paolo (Torino, Italy). The Compagnia San Paolo, the Regione Piemonte, and FIRMS (International Foundation for Research in Experimental Medicine) also provided financial support.
We are grateful to Drs. I. Durelli and R. Lusso of the MAb Production Unit at the CeRMS-Research Center of Experimental Medicine for antibody purification, to Drs. K. Ishihara and T. Hirano for kindly providing the anti-CD157 mAbs and to Dr. M.A. Arnaout for the anti-CD11b (107) and anti-CD18 (TS1/18) mAbs.
Reprint requests to:Professor Ada Funaro,Immunogenetics Laboratory,Dept. Biology, Biochemistry & Genetics,University of Turin Medical School,Via Santena 1910126 Torino, ItalyTel: ++39-011-670-5991Fax: ++39-011-696-6155e-mail: [email protected]
Lavagno et al
10
REFERENCES
1. Goldstein SC, Todd RF 3rd. Structural and biosynthetic features of the Mo5 human myeloid differentiation antigen. Tissue Antigens 1993; 41: 214-218.
2. Kaisho T, Ishikawa J, Oritani K et al. BST-1, a surface molecule of bone marrow stromal cell lines that facilitates pre-B-cell growth. Proc Natl Acad Sci U S A 1994; 91: 5325-5329.
3. McNagny KM, Cazenave PA, Cooper MD. BP-3 alloantigen. A cell surface glycoprotein that marks early B lineage cells and mature myeloid lineage cells in mice. J Immunol 1988; 141: 2551-2556.
4. Ortolan E, Vacca P, Capobianco A et al. CD157, the Janus of CD38 but with a unique personality. Cell Biochem Funct 2002; 20: 309-322.
5. Okuyama Y, Ishihara K, Kimura N et al. Human BST-1 expressed on myeloid cells functions as a receptor molecule. Biochem Biophys Res Commun 1996; 228: 838-845.
6. Hirata Y, Kimura N, Sato K et al. ADP ribosyl cyclase activity of a novel bone marrow stromal cell surface molecule, BST-1. FEBS Lett 1994; 356: 244-248.
7. Dong C, Wang J, Neame P, Cooper MD. The murine BP-3 gene encodes a relative of the CD38/NAD glycohydrolase family. Int Immunol 1994; 6: 1353-1360.
8. Ferrero E, Malavasi F. Human CD38, a leukocyte receptor and ectoenzyme, is a member of a novel eukaryotic gene family of nicotinamide adenine dinucleotide+-converting enzymes: extensive structural homology with the genes for murine bone marrow stromal cell antigen 1 and aplysian ADP-ribosyl cyclase. J Immunol 1997; 159: 3858-3865.
9. Funaro A, Ortolan E, Ferranti B et al. CD157 is an important mediator of neutrophil adhesion and migration. Blood 2004; 104: 4269-4278.
10. Ortolan E, Tibaldi EV, Ferranti B et al. CD157 plays a pivotal role in neutrophil transendothelial migration. Blood 2006; 108: 4214-4222.
11. Brown EJ. Integrin-associated proteins. Curr Opin Cell Biol 2002; 14: 603-607.
12. Deaglio S, Zubiaur M, Gregorini A et al. Human CD38 and CD16 are functionally dependent and physically associated in natural killer cells. Blood 2002; 99: 2490-2498.
13. Porter JC, Hogg N. Integrins take partners: cross-talk between integrins and other membrane receptors. Trends Cell Biol 1998; 8: 390-396.
14. Horenstein AL, Crivellin F, Funaro A, Said M, Malavasi F. Design and scaleup of downstream
processing of monoclonal antibodies for cancer therapy: from research to clinical proof of principle. J Immunol Methods 2003; 275: 99-112.
15. Saxton JM, Pockley AG. Effect of ex vivo storage on human peripheral blood neutrophil expression of CD11b and the stabilizing effects of Cyto-Chex. J Immunol Methods 1998; 214: 11-17.
16. Drbal K, Angelisova P, Cerny J et al. Human leukocytes contain a large pool of free forms of CD18. Biochem Biophys Res Commun 2000; 275: 295-299.
17. Hussain AM, Lee HC, Chang CF. Functional expression of secreted mouse BST-1 in yeast. Protein Expr Purif 1998; 12: 133-137.
18. Partida-Sanchez S, Cockayne DA, Monard S et al. Cyclic ADP-ribose production by CD38 regulates intracellular calcium release, extracellular calcium influx and chemotaxis in neutrophils and is required for bacterial clearance in vivo. Nat Med 2001; 7: 1209-1216.
19. Zarewych DM, Kindzelskii AL, Todd RF 3rd, Petty HR. LPS induces CD14 association with complement receptor type 3, which is reversed by neutrophil adhesion. J Immunol 1996; 156: 430-433.
20. Wei Y, Lukashev M, Simon DI et al. Regulation of integrin function by the urokinase receptor. Science 1996; 273: 1551-1555.
21. Watanabe T, Sendo F. Physical association of beta 2 integrin with GPI-80, a novel glycosylphosphatidylinositol-anchored protein with potential for regulating adhesion and migration. Biochem Biophys Res Commun 2002; 294: 692-694.
22. Berditchevski F, Zutter MM, Hemler ME. Characterization of novel complexes on the cell surface between integrins and proteins with 4 transmembrane domains (TM4 proteins). Mol Biol Cell 1996; 7: 193-207.
23. Maecker HT, Todd SC, Levy S. The tetraspanin superfamily: molecular facilitators. FASEB J 1997; 11: 428-442.
24. Van Haastert PJ, Devreotes PN. Chemotaxis: signalling the way forward. Nat Rev Mol Cell Biol 2004; 5: 626-634.
25. Sendo F, Suzuki K, Watanabe T, Takeda Y, Araki Y. Modulation of leukocyte transendothelial migration by integrin-associated glycosyl phosphatidyl inositol (GPI)-anchored proteins. Inflamm Res 1998; 47 Suppl 3:S133-136.
26. Ossowski L, Aguirre-Ghiso JA. Urokinase receptor and integrin partnership: coordination of signaling for cell adhesion, migration and
CD157 is part of a supramolecular complex with CD11b/CD18
11
growth. Curr Opin Cell Biol 2000; 12: 613-620.27. Thornton BP, Vetvicka V, Pitman M, Goldman
RC, Ross GD. Analysis of the sugar specificity and molecular location of the beta-glucan-binding lectin site of complement receptor type 3 (CD11b/CD18). J Immunol 1996; 156: 1235-1246.
28. Xia Y, Borland G, Huang J et al. Function of the lectin domain of Mac-1/complement receptor type 3 (CD11b/CD18) in regulating neutrophil adhesion. J Immunol 2002; 169: 6417-6426.
29. Frasca L, Fedele G, Deaglio S et al. CD38
orchestrates migration, survival, and Th1 immune response of human mature dendritic cells. Blood 2006; 107: 2392-2399.
30. Yamamoto-Katayama S, Ariyoshi M, Ishihara K, Hirano T, Jingami H, Morikawa K. Crystallographic studies on human BST-1/CD157 with ADP-ribosyl cyclase and NAD glycohydrolase activities. J Mol Biol 2002; 316: 711-723.
31. Liu Q, Kriksunov IA, Graeff R, Munshi C, Lee HC, Hao Q. Crystal structure of human CD38 extracellular domain. Structure 2005; 13: 1331-1339.
Lavagno et al

Journal of Biological Regulators and Homeostatic Agents
0393-974XCopyright © by BIOLIFE, s.a.s
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyrighter holder.
Unauthorized reproduction may result in financial and other penalties13
Prospective study on prognostic significance of DNA ploidy and Ki-67 expressionin colorectal cancerA. SANTAGOSTINO1, C. SAGGIA2, P. MIGLIORA3, M.C. PAVANELLI3, G. FORTI2,G. BIAGGI4, G. ANGELI3, M. DACORSI3, O. ALABISO5
1Citometria-Ematologia, Ospedale S. Andrea Vercelli, Italy 2Dipartimento di Medicina Specialistica ASL-11, Vercelli, Italy 3Anatomia Patologica, Ospedale S. Andrea, Vercelli, Italy 4Ematologia, Ospedale S. Andrea, Vercelli, Italy 5Cattedra di Oncologia Medica Università Piemonte Orientale, Novara, Italy
Received: February 14, 2006Accepted: April 2, 2006
ABSTRACT: The aim of the study is to correlate tumoral DNA ploidy and Ki-67 expression with therapy response, Overall Survival (OS), Disease Specific Survival (DSS) and Disease Free Survival (DFS). Three samples of colorectal cancer were collected from each patient. One sample of normal tissue was our internal control. DNA ploidy was evaluated by FACSCalibur cytometer and Ki-67 by immunohistochemistry. 67 patients were studied and aneuploidy was found in 65.7% of carcinoma with a Ki-67 median expression of 55%. After surgery and chemotherapy in 35% of the patients with aneuploid carcinoma and high proliferative activity (Ki-67>55%) there was no evidence of disease in 100% of patients with DNA diploidy and low proliferative activity (Ki-67<55%). Tumoral aneuploidy significantly correlated with lower OS, DSS and DFS (18% vs 86% at 30 months). Univariated analysis demonstrated a significant correlation between aneuploidy and develop disease progression (p=0,033, odd ratio=5.7), while the cut-off of 55% for Ki-67 expression did not correlate with OS, DSS and DFS. Preliminary results (the study is still in progress) seem to suggest that DNA ploidy has a prognostic and predictive significance in colorectal carcinoma.
KEY WORDS: Prognostic factors, DNA ploidy, Cytofluorimetric analysis, Ki-67 expression, Colorectal cancer
INTRODUCTION
Colorectal carcinoma has an incidence of 800.000 cases in the world with 450.000 tumor related deaths every year (1).
In the last decades the development of new prognostic parameters and therapeutic criteria has resulted in the improvement of colorectal cancer treatment. Among the new parameters we studied the analysis of tumor cell DNA and proliferative activity by Ki-67 expression.
In colorectal cancer the incidence of aneuploid DNA content was 60-70%. The presence of aneuploidy was correlated with more aggressive disease (2-4) and was significantly associated with a lower response to chemotherapy with irinotecan plus fluorofolates and with lower time to
progression and overall survival in every stage of colorectal cancer (5-8). Lanza et al demonstrated that the ploidy of the DNA tumor, measured with flow cytometry, was a significant and independent prognostic factor for DFS and OS in patients affected by colorectal cancer, particularly in stage II of the disease; therefore it may represent an important decision factor in adjuvant chemotherapy application (9). Nevertheless, the role of DNA ploidy in colorectal cancer remained uncertain because the published studies were retrospective and analysed a small number of patients without standardized methods of analysis (10).
Another important prognostic factor was represented by the neoplastic cell proliferative activity: The assessment of the proliferative index was performed with Ki-67 evaluation by

14
immunohistochemistry. This nuclear antigen is expressed in the cell during the proliferative phase of cellular cycle. An increased expression is correlated with poorer prognosis (11, 12).
Garrity et al (13) demonstrated that the higher expression of Ki-67 and the aneuploidy were significant independent prognostic factors in patients affected by colorectal cancer in Dukes stages B
2 and C after radical surgical resection with
or without chemotherapy and radiotherapy.On the base of this data we planned a prospective
study that consists in the determination of DNA content with flow cytometry and in the evaluation Ki-67 expression by immunohistochemistry on the tumors of patients with colorectal cancer resected from September 2002 to August 2007.
The aim of this study is to evaluate of the importance of DNA ploidy and Ki-67 expression on clinical presentation, DFS and OS. We analysed the preliminary results referred to the samples collected from September 2002 and June 2005; this corresponds to half of the duration of the study.
MATERIALS AND METHODS
PatientsFrom September 2002 for 5 years, all patients
resected for colorectal carcinoma were enrolled for the study. The date of entry into the study is the date of surgical removal. All patients, in accordance with International Guidelines, were submitted to clinical, biochemical (levels of CEA and GIKA) and instrumental (Chest x-ray, TC scan) stadiation; when recommended, the surgical resection was followed by chemotherapy and/or radiotherapy. Finally, the follow-up program was planned. Adjuvant therapy was based on the use of fluorofolates with or without oxaliplatin. Therapy for metastatic disease were based on all available drugs (fluorofolates, oxaliplatin, irinotecan, target therapy: bevacizumab and cetuximab), according to guidelines (14).
Histological analysisFor each patient, fresh, multiple samples were
collected immediately after surgical resection of primary tumor: 3 specimens of each neoplasm were sampled at different sites and 1 specimen was of normal mucosa (each of them measuring 8x8x2 mm, to assure a final concentration of 1000000 cells/ml (Phase I). Specimens were preserved at –80°C until analysis.
For each specimen we examined one histological section (stained with ematoxilin-eosin). Based on routine histological section, tumours were classified using the WHO histological criteria and staged by TNM system. Grade of differentiation, vascular
invasion and perineural tumour spread were evaluated on histological sections. The assessment of proliferative activity was performed by evaluation of proliferative index measuring Ki-67 expression by immunohistochemistry (Monoclonal Mouse Anti-Human Ki-67 Antigen, Clone MIB-1, Dako) on histological sections containing the worst pattern of differentiation seen anywhere in the tumor.
Evaluation of DNA ploidyDNA ploidy was evaluated by DNA flow
cytometry, according to recommendations of S. Francisco Consensus Conference and guidelines of “Gruppo italiano di lavoro in citometria” (9, 10).
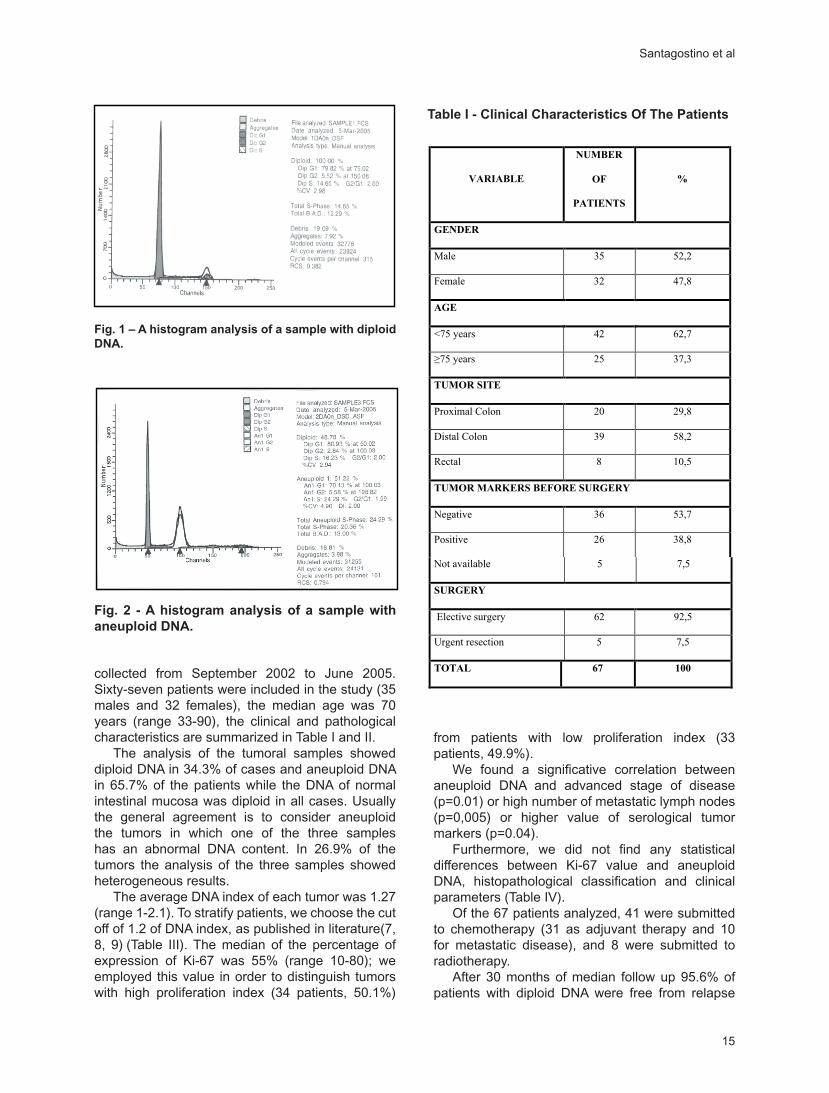
Frozen samples were processed (Phase II): thawed at room temperature, manual disintegration (by scalpel), mechanical disintegration (by Medimachine®), cellular concentration (by centrifugation), enzymatic disintegration of solid tissue by Tripsine (Cycle TEST PLUS DNA, Becton Dickinson), addition of RNAsi and tripsine inhibitory (Cycle TEST PLUS DNA, Becton Dickinson) and finally DNA labelling with propidium iodide. The analysis was performed with a cytometer FACSCalibur Becton Dickinson®. The instrumental setting (Phase III) was established with chicken erythrocytes (CEN), calf thymus nuclei (CTN) and micro spheres of 2 µm. Phase IV, consisting in the acquisition of the samples, was made with the program CELL Quest Software Version 3.0.®. At least 20.000 events were acquired; firstly, we analysed controls of normal mucosa. Cytometric analysis (PHASE V) was performed by the ModFitLT V3.0 software (PMac) ®; evaluated parameters were DNA ploidy, DNA index (DI) and coefficient of variation (CV) of the peak G0/G1. With data interpretation (Phase VI) we can define diploidy (unimodal pick 2n), aneuploidy (bimodal or multimodal distribution of DNA on the histogram) and DI for aneuploid population. Moreover, for each sample we calculated: percentage of diploid and aneuploid cells, percentage of cells in every phase of cellular cycle, percentage of debris, number of analyzed events and total number of events (Fig. 1, Fig. 2).
Statistical analysis Statistical analysis was performed by Software
Statistica.6 (Stat Soft) using χ 2 test ; survival analysis was calculated with Kaplan-Meier curves (Log-Rank Test); the correlation between stage of disease, clinico-pathological variables and survival was assessed by univariate analysis.
RESULTS
In order to have an appropriate follow-up, the results are referred to the analysis of the data
Prospective study on prognostic significance of DNA ploidy and Ki-67 expression in colorectal cancer
15
collected from September 2002 to June 2005. Sixty-seven patients were included in the study (35 males and 32 females), the median age was 70 years (range 33-90), the clinical and pathological characteristics are summarized in Table I and II.
The analysis of the tumoral samples showed diploid DNA in 34.3% of cases and aneuploid DNA in 65.7% of the patients while the DNA of normal intestinal mucosa was diploid in all cases. Usually the general agreement is to consider aneuploid the tumors in which one of the three samples has an abnormal DNA content. In 26.9% of the tumors the analysis of the three samples showed heterogeneous results.
The average DNA index of each tumor was 1.27 (range 1-2.1). To stratify patients, we choose the cut off of 1.2 of DNA index, as published in literature(7, 8, 9) (Table III). The median of the percentage of expression of Ki-67 was 55% (range 10-80); we employed this value in order to distinguish tumors with high proliferation index (34 patients, 50.1%)
from patients with low proliferation index (33 patients, 49.9%).
We found a significative correlation between aneuploid DNA and advanced stage of disease (p=0.01) or high number of metastatic lymph nodes (p=0,005) or higher value of serological tumor markers (p=0.04).
Furthermore, we did not find any statistical differences between Ki-67 value and aneuploid DNA, histopathological classification and clinical parameters (Table IV).
Of the 67 patients analyzed, 41 were submitted to chemotherapy (31 as adjuvant therapy and 10 for metastatic disease), and 8 were submitted to radiotherapy.
After 30 months of median follow up 95.6% of patients with diploid DNA were free from relapse
����� �� � ������� ���� ��������� ����������� �������� ��� ��� ������ ���
����������������
FIG 1 – HYSTOGRAM OF A SAMPLE WITH DIPLOID DNA
Fig. 1 – A histogram analysis of a sample with diploid DNA.FIG 2 - HYSTOGRAM OF A SAMPLE WITH ANEUPLOID DNA
Fig. 2 - A histogram analysis of a sample with aneuploid DNA.
Table I - Clinical Characteristics Of The Patients
TAB I – CLINICAL CHARACTERISTICS OF THE PATIENTS
TAB I CLINICAL CHARACTERISTICS OF THE PATIENTS
VARIABLE
NUMBER
OF
PATIENTS
%
GENDER
Male 35 52,2
Female 32 47,8
AGE
<75 years 42 62,7
�75 years 25 37,3
TUMOR SITE
Proximal Colon 20 29,8
Distal Colon 39 58,2
Rectal 8 10,5
TUMOR MARKERS BEFORE SURGERY
Negative 36 53,7
Positive 26 38,8
Not available 5 7,5
SURGERY
Elective surgery 62 92,5
Urgent resection 5 7,5
TOTAL 67 100
TAB II – PATHOLOGICAL CHARACTERISTICS OF THE PATIENTS
TAB II PATHOLOGICAL CHARACTERISTICS OF THE
PATIENTS
VARIABLE
NUMBER OF
PATIENTS
%
II 22 32,8
III 20 29,8
IV 12 17,9
NUMBER OF POSITIVE LYMPH NODES
N0 38 56,7
N1 16 23,9
N2 13 19,4
GRADING
G 1 6 8,9
G 2 49 73,1
G 3 12 17,9
TOTAL 67 100
Santagostino et al
16
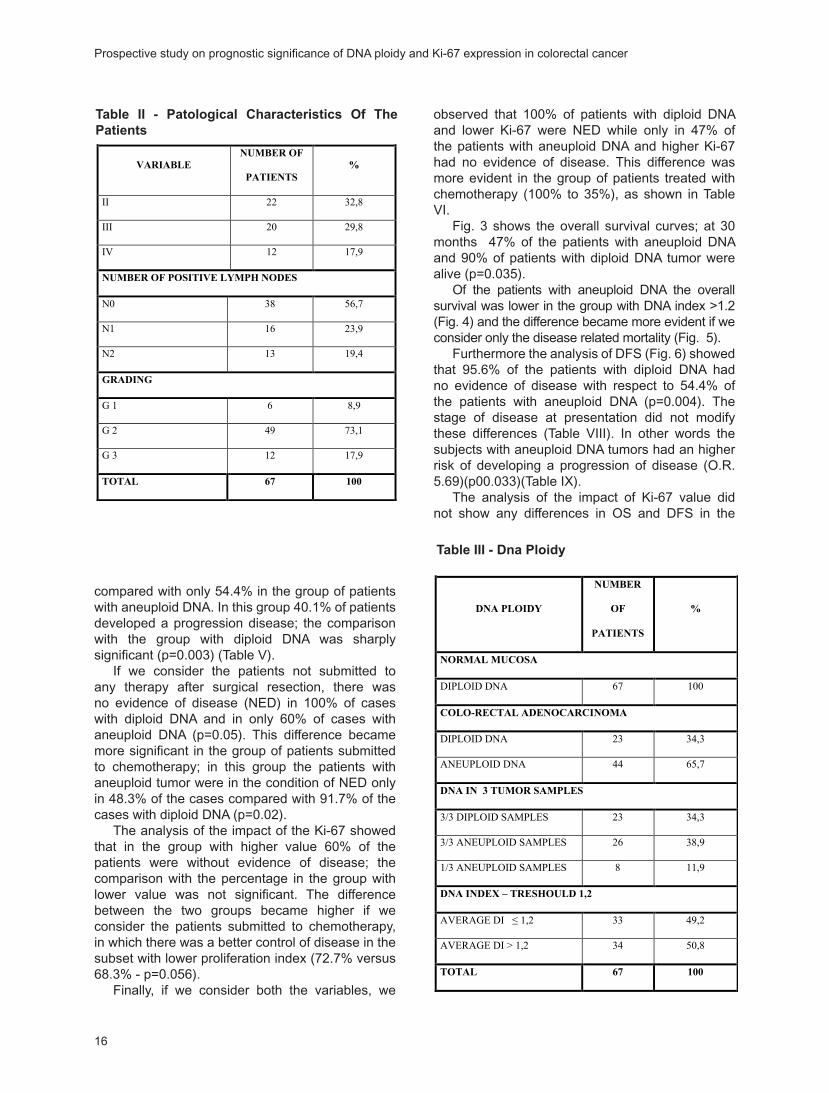
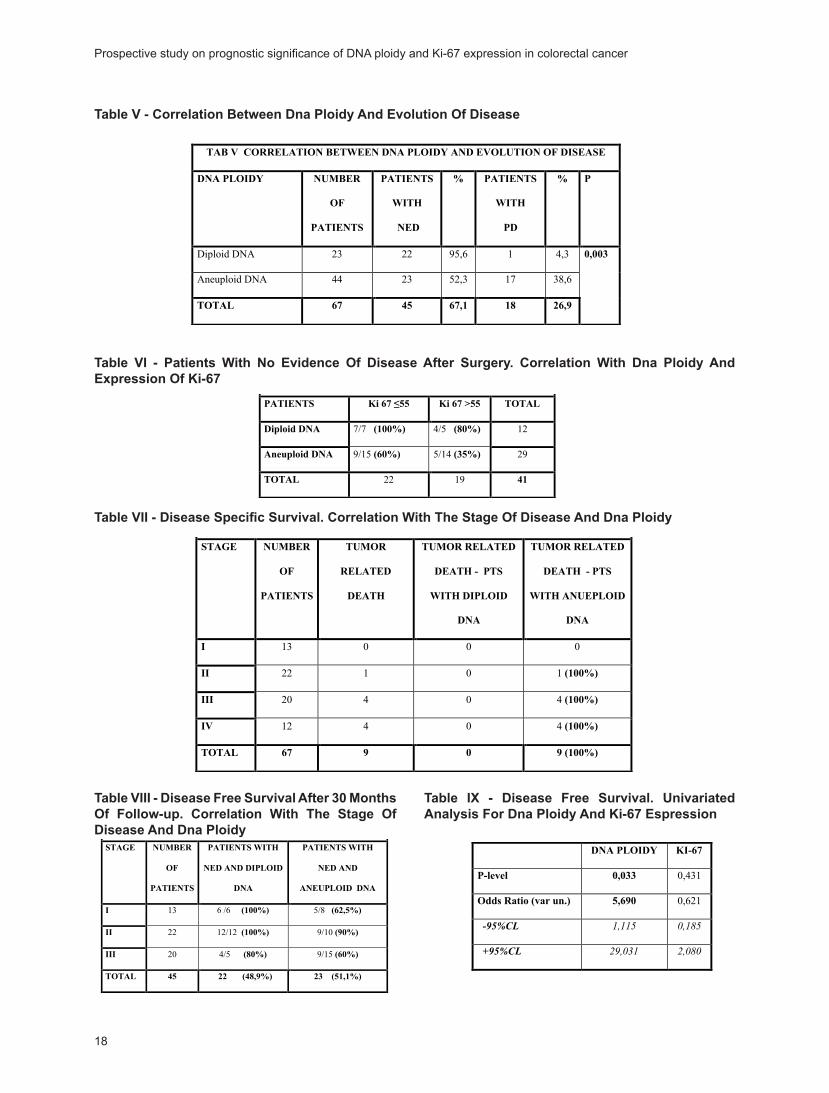
compared with only 54.4% in the group of patients with aneuploid DNA. In this group 40.1% of patients developed a progression disease; the comparison with the group with diploid DNA was sharply significant (p=0.003) (Table V).
If we consider the patients not submitted to any therapy after surgical resection, there was no evidence of disease (NED) in 100% of cases with diploid DNA and in only 60% of cases with aneuploid DNA (p=0.05). This difference became more significant in the group of patients submitted to chemotherapy; in this group the patients with aneuploid tumor were in the condition of NED only in 48.3% of the cases compared with 91.7% of the cases with diploid DNA (p=0.02).
The analysis of the impact of the Ki-67 showed that in the group with higher value 60% of the patients were without evidence of disease; the comparison with the percentage in the group with lower value was not significant. The difference between the two groups became higher if we consider the patients submitted to chemotherapy, in which there was a better control of disease in the subset with lower proliferation index (72.7% versus 68.3% - p=0.056).
Finally, if we consider both the variables, we
observed that 100% of patients with diploid DNA and lower Ki-67 were NED while only in 47% of the patients with aneuploid DNA and higher Ki-67 had no evidence of disease. This difference was more evident in the group of patients treated with chemotherapy (100% to 35%), as shown in Table VI.
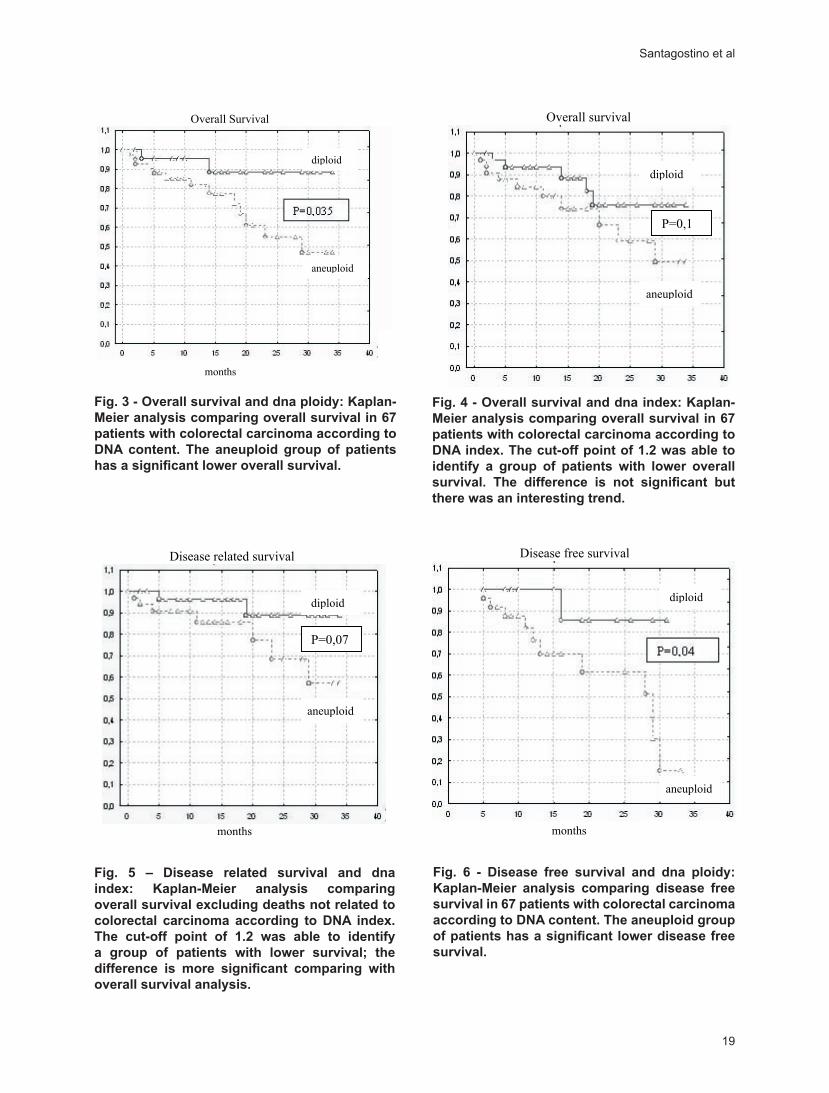
Fig. 3 shows the overall survival curves; at 30 months 47% of the patients with aneuploid DNA and 90% of patients with diploid DNA tumor were alive (p=0.035).
Of the patients with aneuploid DNA the overall survival was lower in the group with DNA index >1.2 (Fig. 4) and the difference became more evident if we consider only the disease related mortality (Fig. 5).
Furthermore the analysis of DFS (Fig. 6) showed that 95.6% of the patients with diploid DNA had no evidence of disease with respect to 54.4% of the patients with aneuploid DNA (p=0.004). The stage of disease at presentation did not modify these differences (Table VIII). In other words the subjects with aneuploid DNA tumors had an higher risk of developing a progression of disease (O.R. 5.69)(p00.033)(Table IX).
The analysis of the impact of Ki-67 value did not show any differences in OS and DFS in the
Not available 5 7,5
SURGERY
Elective surgery 62 92,5
Urgent resection 5 7,5
TOTAL 67 100
TAB II – PATHOLOGICAL CHARACTERISTICS OF THE PATIENTS
TAB II PATHOLOGICAL CHARACTERISTICS OF THE
PATIENTS
VARIABLE
NUMBER OF
PATIENTS
%
II 22 32,8
III 20 29,8
IV 12 17,9
NUMBER OF POSITIVE LYMPH NODES
N0 38 56,7
N1 16 23,9
N2 13 19,4
GRADING
G 1 6 8,9
G 2 49 73,1
G 3 12 17,9
TOTAL 67 100
Table II - Patological Characteristics Of The Patients
TAB III – DNA PLOIDY
TAB III DNA PLOIDY
DNA PLOIDY
NUMBER
OF
PATIENTS
%
NORMAL MUCOSA
DIPLOID DNA 67 100
COLO-RECTAL ADENOCARCINOMA
DIPLOID DNA 23 34,3
ANEUPLOID DNA 44 65,7
DNA IN 3 TUMOR SAMPLES
3/3 DIPLOID SAMPLES 23 34,3
3/3 ANEUPLOID SAMPLES 26 38,9
1/3 ANEUPLOID SAMPLES 8 11,9
DNA INDEX – TRESHOULD 1,2
AVERAGE DI � 1,2 33 49,2
AVERAGE DI > 1,2 34 50,8
TOTAL 67 100
Table III - Dna Ploidy
Prospective study on prognostic significance of DNA ploidy and Ki-67 expression in colorectal cancer

17
two groups subdivided on the basis of the cut-off of 55%.
DISCUSSION
In the last few years the therapeutic approach to colorectal cancer has led to a progressive improvement of OS, principally due to the timely diagnosis, novel drugs and therapeutic strategies based on the knowledge of prognostic factors. In particular, it is important to recognize the level of risk of the single patient in order to apply the best therapeutic approach. From this point of view it is important to identify new diagnostic markers and new prognostic factors that might be helpful to predict response to therapy, DFS and OS.
In this sense our study suggests a possible
role of the analysis of tumor DNA and proliferative activity to assess the prognosis and the therapeutic strategies for the treatment of colorectal cancer.
The analysis of the data collected at 30 months from the beginning of the study led to the following observations:• DNA content in neoplastic population is
heterogeneous• There are significative correlations between
aneuploid DNA and stage of disease (p=0.01), number of positive lymph nodes (p=0.005) and level of oncological markers (p=0.04)
• The aneuploidy of the tumor is correlated with the probability of progression (p=0.05)
• The DFS after adjuvant therapy is significantly improved in the cases with diploid DNA
TAB IV – CORRELATION BETWEEN DNA PLOIDY vs CLINICAL AND
PATHOLOGICAL VARIABLES
VARIABLE NUMBER
PTS
% DIPLOYD
DNA
% ANEUPLOYD
DNA
% P
GENDER
Male 35 52,2 12 34,3 23 65,7
Female 32 47,8 11 34,3 21 65,7
0,83
AGE
<75 years 42 62,7 13 30,9 29 69,1
�75 years 25 37,3 10 40 15 60
0,62
TUMOR SITE
Proximal Colon 20 29,8 10 50 10 50
Distal Colon 39 58,2 10 25,6 29 74,3
Rectal 8 10,5 3 28,6 5 71,4
0,17
STAGE OF DISEASE
I 13 19,4 6 46,1 7 53,9
II 22 32,8 12 54,5 10 45,5
III 20 29,8 5 25 15 75
IV 12 17,9 0 0 12 100
0,01
NUMBER OF POSITIVE LYMPH NODES
N0 38 56,7 19 50 19 50
N1 16 23,9 1 6,2 15 93,8
N2 13 19,4 3 23 10 77
0,005
GRADING
G 1 6 8,9 3 50 3 50
G 2 49 73,1 16 32,6 33 67,4
G 3 12 17,9 4 33,3 8 66,7
0,69
Ki 67
� 55 34 50,1 13 38,2 21 61,8
> 55 33 49,9 10 30,3 23 69,7
0,67
TUMOR MARKERS BEFORE SURGERY
Negative 36 53,7 17 47,2 19 52,8
Positive 26 38,8 5 19,2 21 80,8
Not available 5 7,5 1 20 4 80
0,04
TOTAL 67 100 23 34,3 44 65,7
Table IV - Correlation Between Dna Ploidy Vs Clinical And Pathological Variables
Santagostino et al
18
TAB V – CORRELATION BETWEEN DNA PLOIDY AND EVOLUTION OF DISEASE
TAB V CORRELATION BETWEEN DNA PLOIDY AND EVOLUTION OF DISEASE
DNA PLOIDY NUMBER
OF
PATIENTS
PATIENTS
WITH
NED
% PATIENTS
WITH
PD
% P
Diploid DNA 23 22 95,6 1 4,3
Aneuploid DNA 44 23 52,3 17 38,6
TOTAL 67 45 67,1 18 26,9
0,003
Table V - Correlation Between Dna Ploidy And Evolution Of Disease
TAB VI – PATIENTS WITH NO EVIDENCE OF DISEASE AFTER SURGERY.
CORRELATION WITH DNA PLOIDY AND EXPRESSION OF Ki-67
TAB VI - PATIENTS WITH NO EVIDENCE OF DISEASE
AFTER SURGERY. CORRELATION WITH DNA PLOIDY
AND EXPRESSION OF KI-67
PATIENTS Ki 67 �55 Ki 67 >55 TOTAL
Diploid DNA 7/7 (100%) 4/5 (80%) 12
Aneuploid DNA 9/15 (60%) 5/14 (35%) 29
TOTAL 22 19 41
Table VI - Patients With No Evidence Of Disease After Surgery. Correlation With Dna Ploidy And Expression Of Ki-67
TAB VII - DISEASE SPECIFIC SURVIVAL. CORRELATION WITH THE STAGE OF
DISEASE AND DNA PLOIDY
TAB VII DISEASE SPECIFIC SURVIVAL. CORRELATION WITH THE STAGE OF
DISEASE AND DNA PLOIDY
STAGE NUMBER
OF
PATIENTS
TUMOR
RELATED
DEATH
TUMOR RELATED
DEATH - PTS
WITH DIPLOID
DNA
TUMOR RELATED
DEATH - PTS
WITH ANUEPLOID
DNA
I 13 0 0 0
II 22 1 0 1 (100%)
III 20 4 0 4 (100%)
IV 12 4 0 4 (100%)
TOTAL 67 9 0 9 (100%)
Table VII - Disease Specific Survival. Correlation With The Stage Of Disease And Dna Ploidy
TAB VIII - DISEASE FREE SURVIVAL AFTER 30 MONTHS OF FOLLOW-UP.
CORRELATION WITH THE STAGE OF DISEASE AND DNA PLOIDY
TAB VIII. DISEASE FREE SURVIVAL AFTER 30 MONTHS OF
FOLLOW-UP. CORRELATION WITH THE STAGE OF DISEASE
AND DNA PLOIDY
STAGE NUMBER
OF
PATIENTS
PATIENTS WITH
NED AND DIPLOID
DNA
PATIENTS WITH
NED AND
ANEUPLOID DNA
I 13 6 /6 (100%) 5/8 (62,5%)
II 22 12/12 (100%) 9/10 (90%)
III 20 4/5 (80%) 9/15 (60%)
TOTAL 45 22 (48,9%) 23 (51,1%)
Table VIII - Disease Free Survival After 30 Months Of Follow-up. Correlation With The Stage Of Disease And Dna Ploidy
TAB IX – DISEASE FREE SURVIVAL. UNIVARIATED ANALYSIS FOR DNA PLOIDY
AND Ki-67 EXPRESSION
DNA PLOIDY KI-67
P-level 0,033 0,431
Odds Ratio (var un.) 5,690 0,621
�������� ����� �����
�������� ������ �����
Table IX - Disease Free Survival. Univariated Analysis For Dna Ploidy And Ki-67 Espression
Prospective study on prognostic significance of DNA ploidy and Ki-67 expression in colorectal cancer
19
FIG 3 - OVERALL SURVIVAL AND DNA PLOIDY
Overall Survival
months
diploid
aneuploid
Fig. 3 - Overall survival and dna ploidy: Kaplan-Meier analysis comparing overall survival in 67 patients with colorectal carcinoma according to DNA content. The aneuploid group of patients has a significant lower overall survival.
FIG 4 - OVERALL SURVIVAL AND DNA INDEX
Overall survival
months
aneuploid
diploid
P=0,1
Fig. 4 - Overall survival and dna index: Kaplan-Meier analysis comparing overall survival in 67 patients with colorectal carcinoma according to DNA index. The cut-off point of 1.2 was able to identify a group of patients with lower overall survival. The difference is not significant but there was an interesting trend.
FIG 5 – DISEASE RELATED SURVIVAL AND DNA INDEX
Disease related survival
months
P=0,07
diploid
aneuploid
Fig. 5 – Disease related survival and dna index: Kaplan-Meier analysis comparing overall survival excluding deaths not related to colorectal carcinoma according to DNA index. The cut-off point of 1.2 was able to identify a group of patients with lower survival; the difference is more significant comparing with overall survival analysis.
FIG 6 – DISEASE FREE SURVIVAL AND DNA PLOIDY
Disease free survival
months
diploid
aneuploid
Fig. 6 - Disease free survival and dna ploidy: Kaplan-Meier analysis comparing disease free survival in 67 patients with colorectal carcinoma according to DNA content. The aneuploid group of patients has a significant lower disease free survival.
Santagostino et al
20
(p=0.02)• The presence of lower proliferative activity (Ki-
67<55%) is correlated to a better response to the therapy
• Considering DNA ploidy and proliferation activity together, we can see that all the patients with diploid tumor DNA and Ki-67<55% are free from disease, while only 47% of the patients with aneuploid tumor DNA and Ki-67>55% are in continuous complete remission.
• The OS is significantly better in patients with diploid DNA tumor (p=0.035)
• Also the index of aneuploidy is important: in fact the OS and the DFS are decreased in patients with DNA index >1.2
• All tumor related deaths are in the group of patients with aneuploid DNA tumor
• In each stage of disease the DFS at 30 months is lower in the group of patients with aneuploid DNA tumor
• The risk of progression of disease is 5.7 times higher in the aneuploid group (p=0.033)
• The chosen cut-off of Ki-67 index seems to be useless in identifying groups with different OS and DFS.
The obtained preliminary results, even if the study is ongoing, seems to confirm the importance of the assessment of DNA ploidy with flow cytometry in order to establish the prognosis and the prediction of response to the therapies. Therefore, this biological marker seems to be helpful for the establishment of tailored therapeutic strategies. The importance of Ki-67 is also clear but probably is necessary to establish a more specific cut-off value.
This study is ongoing and a longer follow-up with a larger number of cases will be able to confirm or not these preliminary results.
Reprint requests to:Alberto SantagostinoU.O. Onco-ematologia, Ospedale S.Andrea, C.so M. Abbiate 21, Vercelli, ItalyTel: ++39340 8165298e-mail: [email protected]
REFERENCES
1. De Vita VT. Cancer Principles & practice of oncology: Cancer of gastrointestinal tract: Cancer of the colon. 6Th ed Lippincott Williams & Wilkins, 2005; 1061.
2. Kouri M. DNA ploidy of colorectal carcinoma by tumour site, gender and history of noncolorectal malignancies. Oncology 1993; 50: 41-5.
3. Yamamoto T, Matsumoto K, Yamamoto J et al. Clinical significance of DNA index in hematogenous dissemination of aneuploid colorectal cancer. Surg Today 1997; 27: 973-4.
4. Risques RA, Moreno V, Marcuelllo E et al. Redefining the significance of aneuploidy in the prognostic assessment of colorectal cancer. Lab Invest 2001; 3: 307-15.
5. Karelia NH, Patel DD, Desai NS et al. Prognostic significance of DNA aneuploidy expression in colorectal cancer and their role in the determination of treatment modalities. Int J Biol Markers 2001; 16: 97-104.
6. Bendardaf R, Lamulum H, Ristamaki R et al. Response to chemotherapy (irinotecan plus 5-fluorouracil) in colorectal carcinoma can be predicted by tumour DNA content. Oncology 2004; 66: 46-52.
7. Armitage NC, Robin RA, Evans DF et al. The influence of tumour cell DNA abnormalities on survival in colorectal cancer. Br J Surg 1985; 72: 828-830.
8. Tang R, Ho YS, Hsu KC et al. Prognostic evaluation of DNA flow cytometric and histopathologic parameters of colorectal cancer. Cancer 1995; 76: 1724-1730.
9. Lanza G, Gafà R, Santini A et al. Prognostic significance of DNA ploidy in patients with stage II and III colon carcinoma. Cancer 1998; 82: 9-53.
10. Bauer KD, Bagwell CB, Giaretti W et al. Consensus Review of the clinical utility of DNA flow cytometry in colorectal cancer. Cytometry 1993; 14: 486-391.
11. Sinicrope FA, Hart J, Hsu HA et al. Apoptotic and mitotic indices predict survival rates in lymph nodes-negative colon carcinomas. Clin Cancer Res 1999; 5: 1793-1804.
12. Kimura T, Tanaka S, Hamura K et al. Clinical significance of MUC1 and E-cadherin expression, cellular proliferation and angiogenesis at the deepest invasive portion of colorectal cancer. Int J Oncol 2000; 16: 55-64.
13. Garrity MM, Burgart LJ, Witzig TE et al. Prognostic value of proliferation, apoptosis, defective DNA Mismatch Repair, and p53 overexpression in patients with resected Duke’s B2 or C colon cancer: a North Central Cancer Treatment Group Study. J Clin Oncol 2004; 22: 1572-1582.
14. Cancer Guidance Sub-Group of the Clinical Outcomes Group. Improving outcomes in colorectal cancer: the research evidence. Leeds, NHS executive, 1997.
Prospective study on prognostic significance of DNA ploidy and Ki-67 expression in colorectal cancer
Journal of Biological Regulators and Homeostatic Agents
0393-974XCopyright © by BIOLIFE, s.a.s
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyrighter holder.
Unauthorized reproduction may result in financial and other penalties21
Plasmatic Markers of Muscular Stressin Isokinetic ExerciseL. SPERANZA1, A. GRILLI1
, A. PATRUNO2, S. FRANCESCHELLI1, G. FELZANI1, M. PESCE1,
I. VINCIGUERRA1, M.A. DE LUTIIS1, M. FELACO1
1Department of Human Dynamics, 2Departement of Drug Sciences,University “G. d’Annunzio, Chieti, Italy2On line University “Leonardo Da Vinci” Torrevecchia Teatina, Chieti, Italy
Received: January 31, 2006Accepted: April 28, 2006
KEY WORDS: Hypoxanthine, Xanthine, Myoglobin, Creatine-kinase, Troponin I
ABSTRACT: In this paper we examined the variations of plasmatic concentrations of hypoxanthine and xanthine, and their relation with other important indicators of muscular stress [creatine-kinase (CK), myoglobin, uric acid, leucocytes], in prolonged, isokynetic physical exercise, performed in a concentric mode at different joint excursion. 20 healthy male subjects performed isokinetic exercises in concentric-concentric mode, with joint excursion of 30, 60, 90 deg/sec. Blood samples were taken at rest, immediately after exercise and after 45 min of recovery. The plasmatic concentration of hypoxanthine increased at the end of physical exercise, compared to the rest value of about 1.5 µmol/L, up to a level of >19 µmol/L; the values were higher after a period of recovery of 45’ and the increase varies considerably according to the type of exercise performed. Myoglobin also has a slight but sensible increment, with the same trend as hypoxanthine, while CK increase without correlation to the type of exercises. The relation with other indicators of muscular activity demonstrates that in none of the different isokinetic exercises, performed at concentric mode, was there ultrastructural damage, while it is possible to come across a considerable metabolic stress, which is dissimilar in the different kinds of exercises. The results suggest that hypoxanthine can be useful in monitoring the effectiveness of a work load and the metabolic stress consequences on the muscle tissue in training or rehabilitation programs. The results also suggest that even myoglobin, at small concentrations, can have the same function.
INTRODUCTION
Muscular injury represents one of the most recurrent traumas in sport activity. Aside from muscular damage taking place during the competition itself, in which case the cause can also be accidental, it may be connected with the type of training and occur during the training itself or later. In fact, the injury can be associated with the type of muscular activation and can be caused either by a single contraction or by the cumulative effect of a series of contractions. Generally, the eccentric contraction, during which the muscle produces strength stretching out, instead of shrinking, as is the case of concentric work, results as being the major cause of ultra structural level injury (1). Also in this type of
contraction there are greater modifications of the plasmatic indicators compared to the concentric exercise (2). There is however, data indicating evidence of muscle injury due to concentric muscle contractions (3). The causes of the injuries for these two types of muscular activities are different: the damage due to the concentric exercise seems due to metabolic stress, while the eccentric exercise can initially cause a rupture in the fibers due to physical stress, which can eventually be followed by metabolic events similar to those found in the concentric exercise (4). Previous studies have already revealed the presence of morphostructural modifications, such as the slide of the Z bands, rupture of the sarcoplasmatic reticule, swelling of mitochondria, that were directly revealed via an electronic
22
microscope in tissue samples obtained through serial biopsies (5). It is however comprehensible that this method is not well tolerated by patients and involves technical difficulties whether taking the samples or processing them, not to mention the ethical problems and those related to legal medicine. In this paper we try to evaluate whether the dosage of certain plasmatic metabolites could give us valid indications on the consequences that an exercise has on a muscular level when this exercise was done at different intensities in
the concentric mode. To be able to thoroughly evaluate muscular performance, isokinetic test was used. This machine allowed the muscle to perform a type of contraction with a constant and continuous development of strength during the whole movement. In this way, the unfavourable angles of contraction were compensated and the maximum recruitment of the fibers in the muscles interested in the activity was permitted (6). Thanks to the isokinetic dinamometer, it was possible to examine the various functional
��
���������������������
���������� ���������� ����������
�
��
��
��
������������
����������������
�
��
������������
������
������
�����������������
���������� ���������� ����������
�
��
��������������
���������������
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
������
��
���������������������
���������� ���������� ����������
�
��
��
��
������������
����������������
�
��
������������
������
������
�����������������
���������� ���������� ����������
�
��
��������������
���������������
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
������
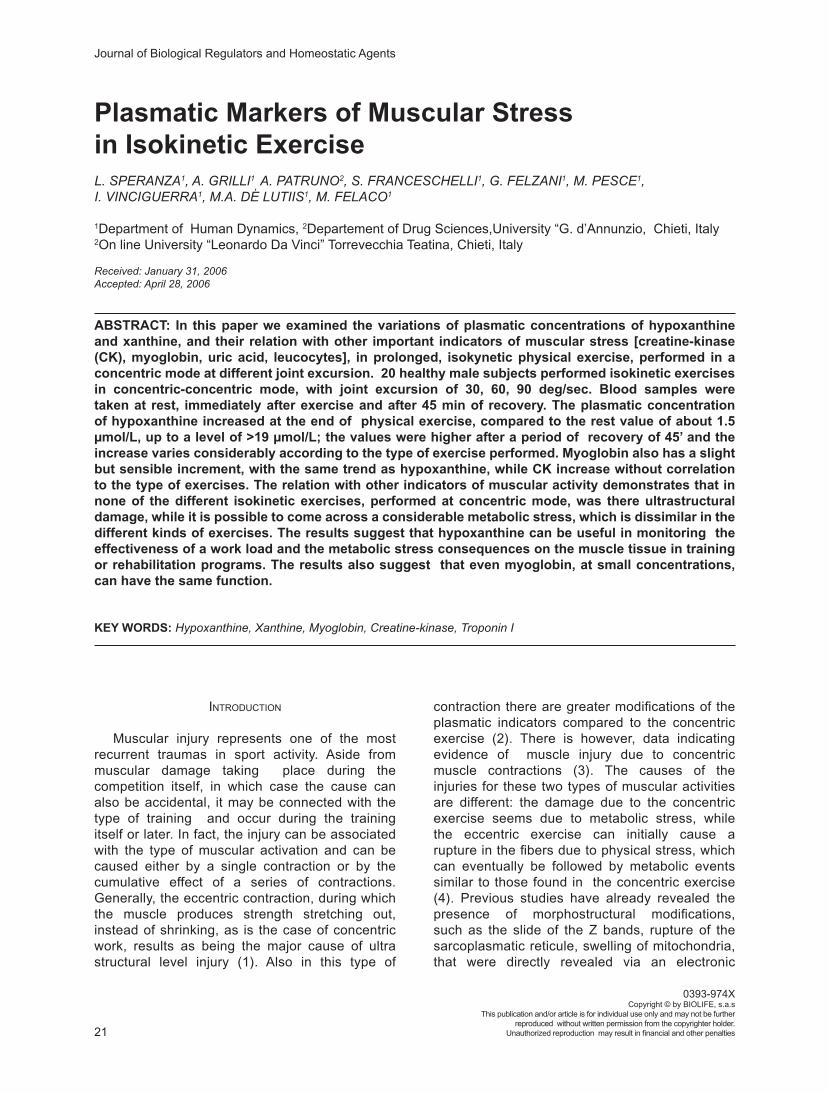
Fig. 1 - Increase of hypoxanthine compared with basal value. For hypoxanthine, increase is stronger in samples drawn 45 minutes after the end of exercises. For each kind of exercise, there is a substantial difference between samples drawn at the end of the exercise and samples drawn at recovery. The difference is greater in exercise performed at 30 deg/sec. * statistically significant (P>0.05).
Fig. 2 - Increase of xanthine compared with basal value. For xanthine the differences between samples drawn at the end of the exercise and samples drawn at recovery are non so perceptible as for hypoxanthine.In various exercises, difference between end-exercise and recovery are statistically non significant.
Plasmatic Markers of Muscular Stress in Isokinetic Exercise
23
muscular parameters during the whole concentric contraction.
MATERIALS AND METHODS
Subject recruitment20 healthy male subjects were recruited from
students of the local University Center of Sport Medicine (CUMS) of the “G. d’Annunzio” University of Chieti-Pescara, and amongst staff members of the University campus. All subjects were homogeneous
for age (25-28 years old), sex (males) and for training (not regularly trained). All subjects were instructed to abstain from heavy physical activity the day before the experiment. We excluded regular smokers and alcoholics, those who regularly assumed dietary supplements or those who, in the preceding 12 hours, ingested substances like coffee, tea, cola or similar. All subjects were scrupulously informed about the experiments and gave written informed consent before entering the trials. The study received the approval from the Ethics Commitee of the “G. d’Annunzio” University
��
������������������
���������� ���������� �����������
�
�������������
���������������
���������
�����������
�����
�
��
������
�����������������������������
���������� ���������� �����������
�
�������������
���������������
��
�����������
�����
������
��
������������������
���������� ���������� �����������
�
�������������
���������������
���������
�����������
�����
�
��
������
�����������������������������
���������� ���������� �����������
�
�������������
���������������
��
�����������
�����
������
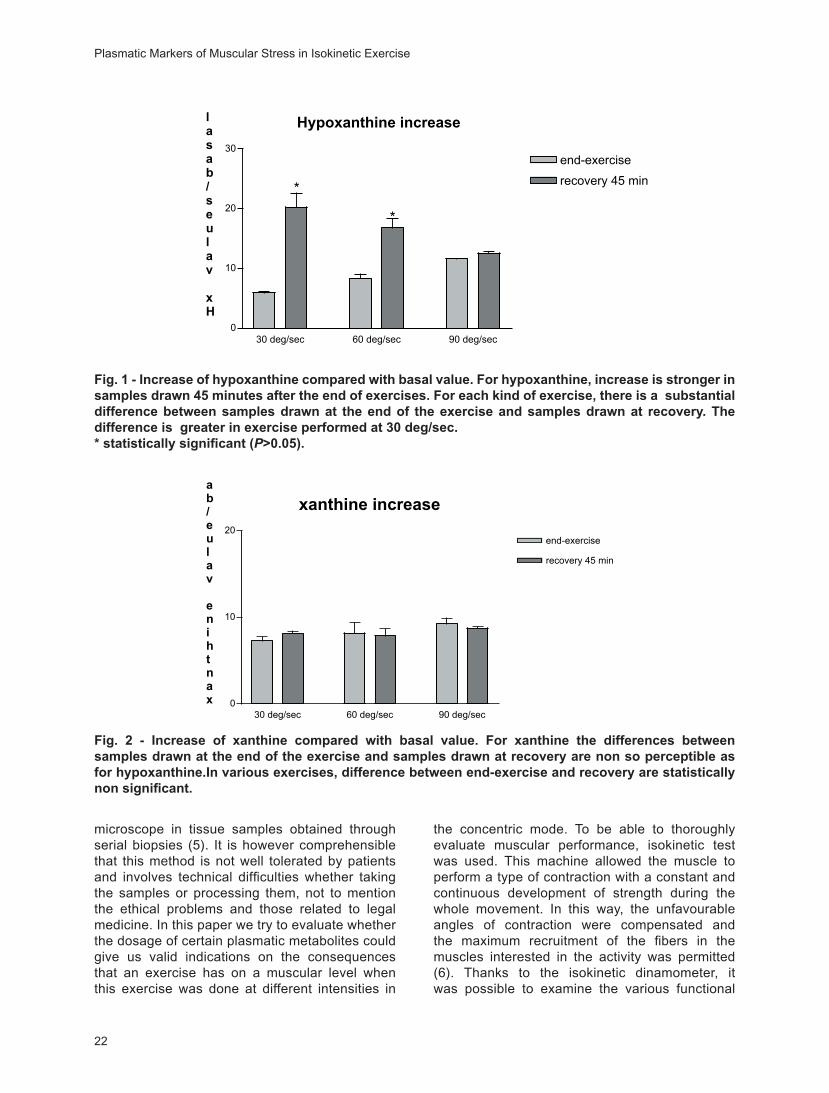
Fig. 3 - Increase of myoglobine, compared with basal value.For myoglobine there is an evident difference between increase at end of the exercise and increase at recovery. The trend of these increases are similar to those of hypoxanthine (r= 1,000). * statistically significant (P>0.05).
Fig. 4 - Increase of total creatine-kinase (CK), compared with basal value.For CK, the increase in not so high and there is almost no diversity between samples drawn at end of exercise and samples drawn at recovery.For various exercises, differences between end-exercise and recovery are not statistically significant.
Speranza et al
24
of Chieti-Pescara. The exercise protocol consisted of cycles of flexo-extension of the knee at maximal effort in concentric-concentric modality on an isokynetic dinamometer (Cybex 6000, CSMI, MA USA). Each subject executed three tests at different angular speed: 30 deg/sec, 60 deg/sec, 90 deg/sec. Between tests, each subject observed a period of recovery of 72 hours. After a 2-3 min warm-up, subjects executed exercises to exhaustion. Fatigue was defined as the point at which the subjects were unable to maintain the required frequency of movements, despite verbal encouragement. Heart rate and O
2 consumption were
monitored continuously during the entire exercise. Three different blood samples were taken from the antecubital vein. The first at rest, before the exercise. The second was taken at the end of the exercise, at the maximum peak of the effort. The third was taken after a recovery period of 45 minutes from the end of exercise. Blood samples were drawn into two different “vacutainer” tubes: with EDTA, for hemocytometric analysis; without additive, for serum assay of methabolites. On each blood sample we executed: a) hemocytometric analysis b) serum metabolites assay c) serum troponin-I (cTn-I) and myoglobin assay d) serum hypoxanthine and xanthine assay, using respectively a) an automatic counter type “CA 500 (Dade Behring, IL USA ), b) a “Vitros 550” system (Ortho Clinical Diagnostics, Eng UE) c) a “Stratus II” system (Dade Behring, IL USA) d) a “TSP UV 1000” HPLC system (TSP, CA, USA). Blood samples for purine assays were drawn and quickly centrifuged. The serum was immediately stored at -20° C. At the moment of the chromatographic analysis, samples were deproteinized with percloric acid (PCA, 1.5 mol/
L) and, after centrifuge, supernatant was neutralized with potassium hydroxide (KOH, 2.1 mol/L) (7). A 20 μL sample was injected in the HPLC system (TSP CA, USA), and purinic bases were separated by a C18 column “Nova pack” (Waters, MA USA), using an easily reproducible isocratic method (8). Tests at different angular speeds were executed to fatigue. The exercises lasted an average of 4.5 + 0.5 minutes. The number of sets was an average of 69 for the test at 30 deg/sec, an average of 67 at 68 deg/sec, and an average of 70 at 90 deg/sec. The results were corrected considering the variation of the haematocrit compared to the basal value, due to the redistribution of the plasmatic volume which occurs in intense exercise (9).
Statistical AnalysisAll statistical procedures employed the statistical
software GraphPad Prism 3.02 for Windows (GraphPad Software Inc, San Diego CA USA). Differences were analyzed by parametric (t test and ANOVA) and non-parametric (Mann-Whitney and Kruskall-Wallis ANOVA on ranks) methods according to the normal or skewed distribution of data, respectively. Pearson’s correlation coefficient (r) was used to test the associations between pairs of variables. All data are reported as means + SD unless otherwise stated. The level of significance was set at P <0,05.
RESULTS
In Table I, the concentrations of hypoxanthine, xanthine and uric acid in basal conditions, at the
��
���������������
���������� ��������� �������������
���
���
���
���
���
���
��� �����������
�����������
���
�����������
�����
������Fig. 5 - Increase of neutrophils and decrease of lymphocytes after 45 min of recovery. In the muscle tissue, an increase in the number of neutrophils indicates the presence of stress. The reduced numbers of lymphocytes suggest that there aren’t damaged cells.
Plasmatic Markers of Muscular Stress in Isokinetic Exercise
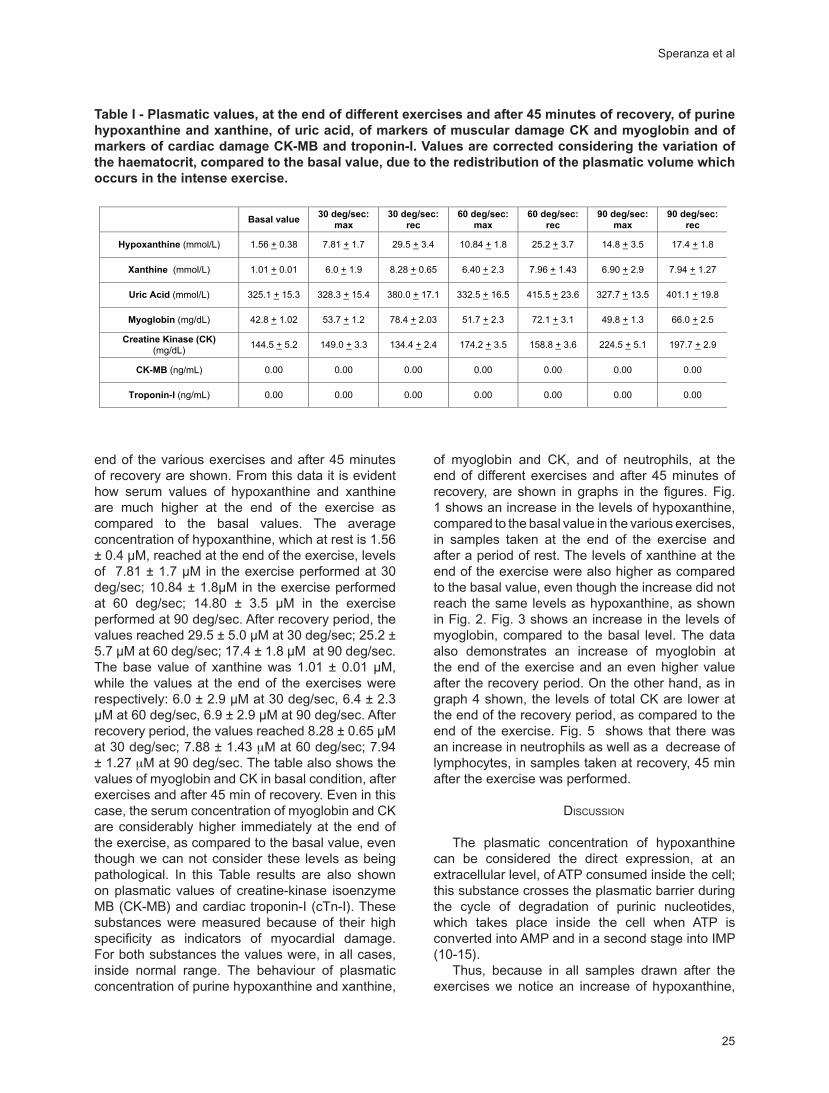
25
end of the various exercises and after 45 minutes of recovery are shown. From this data it is evident how serum values of hypoxanthine and xanthine are much higher at the end of the exercise as compared to the basal values. The average concentration of hypoxanthine, which at rest is 1.56 ± 0.4 µM, reached at the end of the exercise, levels of 7.81 ± 1.7 µM in the exercise performed at 30 deg/sec; 10.84 ± 1.8µM in the exercise performed at 60 deg/sec; 14.80 ± 3.5 µM in the exercise performed at 90 deg/sec. After recovery period, the values reached 29.5 ± 5.0 µM at 30 deg/sec; 25.2 ± 5.7 µM at 60 deg/sec; 17.4 ± 1.8 µM at 90 deg/sec. The base value of xanthine was 1.01 ± 0.01 µM, while the values at the end of the exercises were respectively: 6.0 ± 2.9 µM at 30 deg/sec, 6.4 ± 2.3 µM at 60 deg/sec, 6.9 ± 2.9 µM at 90 deg/sec. After recovery period, the values reached 8.28 ± 0.65 µM at 30 deg/sec; 7.88 ± 1.43 μM at 60 deg/sec; 7.94 ± 1.27 μM at 90 deg/sec. The table also shows the values of myoglobin and CK in basal condition, after exercises and after 45 min of recovery. Even in this case, the serum concentration of myoglobin and CK are considerably higher immediately at the end of the exercise, as compared to the basal value, even though we can not consider these levels as being pathological. In this Table results are also shown on plasmatic values of creatine-kinase isoenzyme MB (CK-MB) and cardiac troponin-I (cTn-I). These substances were measured because of their high specificity as indicators of myocardial damage. For both substances the values were, in all cases, inside normal range. The behaviour of plasmatic concentration of purine hypoxanthine and xanthine,
of myoglobin and CK, and of neutrophils, at the end of different exercises and after 45 minutes of recovery, are shown in graphs in the figures. Fig. 1 shows an increase in the levels of hypoxanthine, compared to the basal value in the various exercises, in samples taken at the end of the exercise and after a period of rest. The levels of xanthine at the end of the exercise were also higher as compared to the basal value, even though the increase did not reach the same levels as hypoxanthine, as shown in Fig. 2. Fig. 3 shows an increase in the levels of myoglobin, compared to the basal level. The data also demonstrates an increase of myoglobin at the end of the exercise and an even higher value after the recovery period. On the other hand, as in graph 4 shown, the levels of total CK are lower at the end of the recovery period, as compared to the end of the exercise. Fig. 5 shows that there was an increase in neutrophils as well as a decrease of lymphocytes, in samples taken at recovery, 45 min after the exercise was performed.
DISCUSSION
The plasmatic concentration of hypoxanthine can be considered the direct expression, at an extracellular level, of ATP consumed inside the cell; this substance crosses the plasmatic barrier during the cycle of degradation of purinic nucleotides, which takes place inside the cell when ATP is converted into AMP and in a second stage into IMP (10-15).
Thus, because in all samples drawn after the exercises we notice an increase of hypoxanthine,
����������������������
���
�����������
���
�����������
���
�����������
���
�����������
���
�����������
���
��������������������� ����������� ���������� ���������� ����������� ���������� ���������� ����������
������������������ ����������� ��������� ����������� ���������� ����������� ���������� �����������
������������������ ������������ ������������ ������������ ������������ ������������ ������������ ������������
����������������� ����������� ���������� ����������� ���������� ���������� ���������� ����������
��������������������
������������������ ����������� ����������� ����������� ����������� ����������� �����������
������������� ���� ���� ���� ���� ���� ���� ����
������������������ ���� ���� ���� ���� ���� ���� ����
�������
Table I - Plasmatic values, at the end of different exercises and after 45 minutes of recovery, of purine hypoxanthine and xanthine, of uric acid, of markers of muscular damage CK and myoglobin and of markers of cardiac damage CK-MB and troponin-I. Values are corrected considering the variation of the haematocrit, compared to the basal value, due to the redistribution of the plasmatic volume which occurs in the intense exercise.
Speranza et al

26
xanthine and uric acid, we can hypothesize, in accordance with previous studies, that in this type of muscular contraction there is an intense metabolic stress (16-20). Furthermore, our data shows that the metabolic stress is more intense when these exercises are performed with a joint excursion of 30 deg/sec. We assumed the increase of plasmatic myoglobin and CK as indicators of structural damage (21-30). In exercises performed with a 30 deg/sec joint excursion, there is only a slight increase of plasmatic levels of myoglobin as compared to basal level. We therefore deduce that in this type of exercises there is an injury in the muscular cell, but this damage is limited because plasmatic myoglobin and CK are not at pathological levels. In exercises performed with joint excursion of 90 deg/sec, we observe opposite results: the values of purinic bases hypoxanthine and xanthine are not as high as those in the 30 deg/sec joint excursion, while the values of myoglobin and CK are greater. So, we assume that in this condition, there is a less significant level of metabolical stress, but muscular cells are more injured. Even in this case, the injury is not at pathological level, in fact the levels of myoglobin and CK are not above normal range (21). We notice a different behavior between myoglobin and CK. In fact, CK values are higher in exercises performed at a wider angle of contraction compared to that performed at a smaller angle of contraction. They resulted already increased at the end of exercise and remain almost the same in samples drawn after 45 min. For CK, the difference among post-exercise and post-recovery values is not significant (p= 0.25). Even myoglobin increased immediately after the exercises, but this increase is higher after 45 min post exercises and levels are higher in exercises performed at 30 deg/sec. For this substance there is a significant difference between post-exercise values and post-recovery values (p = 0.005). Hence, its trend is well related to that of hypoxanthine (r = 1,000), and this can be considered a further data that confirms a metabolic stress in muscular cells. To exclude a miocardial involvement (31-35), we measured in all samples the levels of a highly sensitive plasmatic indicator of heart damage: troponin-I (1). The value of this indicator resulted not measurable in all samples (Table 1).
In all samples taken 45 min after exercises, hypoxanthine and xanthine values were higher than those measured immediately after the end of the exercises. This seems related to kinetic limitations in the formation and release of these bases (36). It has already been proposed that 5’ nucleotidase, which degrades IMP into inosine, from which hypoxanthine derives, has a lower activity in the
high intensity exercise in the contraction phase, while it increases after the end of the exercise, even though the exact mechanism that regulates this activity is unknown (37). In the recovery phase, the reoxigenation of the muscle tissues is very important since it gives way to the formation of free radicals (38). In this phase the formation of hypoxanthine is greater as a consequence of the increased catabolism of adenilic nucleotides at the tissue level with an increase of IMP (39). Xantine oxidase (XOD) acts when it has hypoxanthine and xanthine as a substrate. In basal conditions it acts as a dehydrogenase and it can be transformed into an oxidized form thanks to different kinds of stimuli, such as metabolic stress and the presence of neutrophils (40). In our experiment, we found an increased number of neutrophils 45 min after the end of exercises performed either at 30 deg/sec or at 60 deg/sec or at 90 deg/sec, in respect to the basal value, with a reduced number of lymphocytes in all cases (41). The recruitment of neutrophils from the marginated pool represents a non-specific immune response (42), which occurs in the presence of inflammation or ischemia of a stressed tissue, even though there is no a real injury (43). Lymphocytes, also recruited from the marginated pool, act by removing damaged cells (44). Therefore, this data confirms that in all the exercises performed in our study the muscular tissue was not damaged.
However, an important effect of the presence of these cells in the area of interest is that the enzymes contained in its cytoplasm, especially myeloperoxidase and NADPH oxidase, facilitate the formation of free radicals (45). In addition, neutrophils can convert XOD, from its reduced form to the oxidized one, increasing the formation of xanthine and thus uric acid (46). It is well known how the increase of uric acid is a consequence of muscular activity (47) and how this is a useful mechanism against free radical formation and in the defence against oxidative stress (48). As expected, in samples drawn after 45 min from the end of the exercises, in all cases an increase in uric acid concentration was noted. Even though in clinical practice plasmatic myoglobin is usually considered an indicator of muscular damage (49), recent studies have shown that, aside from its main function of reserve and rapid release of O
2, it can also acts like
an NO oxidase in muscle cells (50). Thus, it has a relevant role in moderating oxidative stress caused by intense physical exercise in the muscle tissue. In the light of this hypothesis, we can in fact observe that the variation of the plasmatic concentrations of myoglobin in the different exercises performed is strongly related (r = 1.000) to that of hypoxanthine. Thus, according with these recent data, we can
Plasmatic Markers of Muscular Stress in Isokinetic Exercise
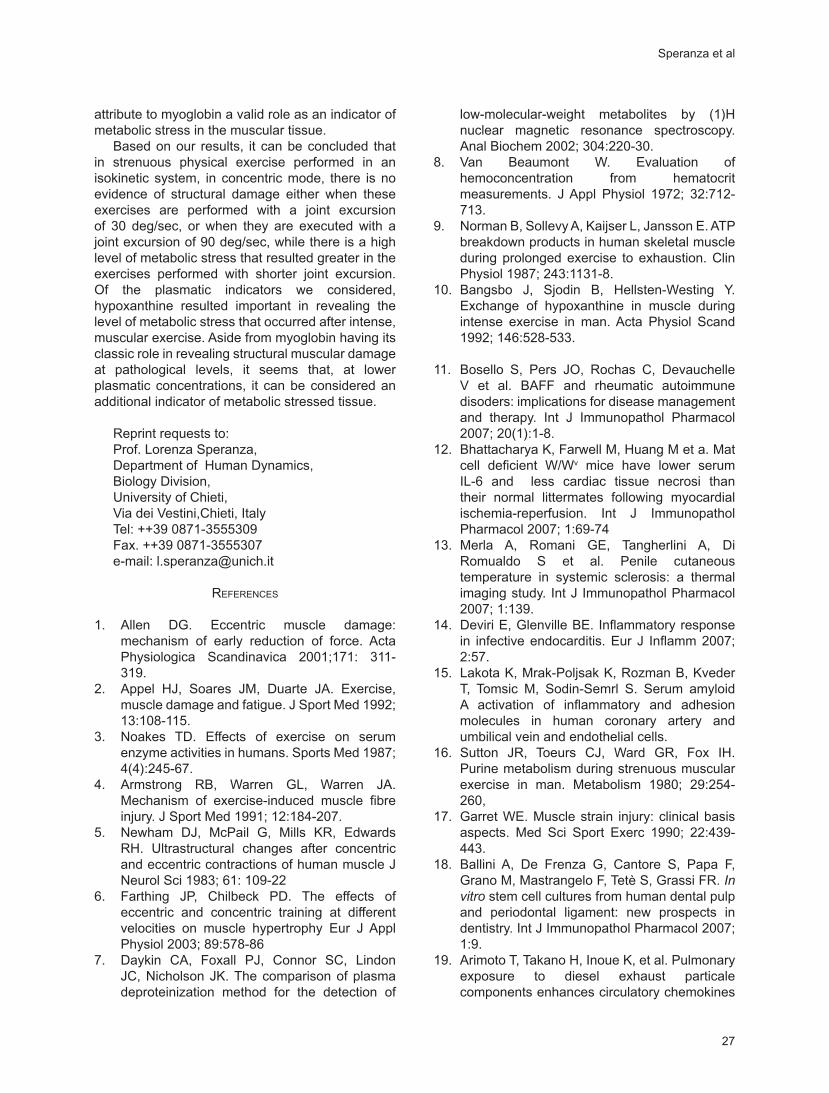
27
attribute to myoglobin a valid role as an indicator of metabolic stress in the muscular tissue.
Based on our results, it can be concluded that in strenuous physical exercise performed in an isokinetic system, in concentric mode, there is no evidence of structural damage either when these exercises are performed with a joint excursion of 30 deg/sec, or when they are executed with a joint excursion of 90 deg/sec, while there is a high level of metabolic stress that resulted greater in the exercises performed with shorter joint excursion. Of the plasmatic indicators we considered, hypoxanthine resulted important in revealing the level of metabolic stress that occurred after intense, muscular exercise. Aside from myoglobin having its classic role in revealing structural muscular damage at pathological levels, it seems that, at lower plasmatic concentrations, it can be considered an additional indicator of metabolic stressed tissue.
Reprint requests to:Prof. Lorenza Speranza,
Department of Human Dynamics,Biology Division,University of Chieti,Via dei Vestini,Chieti, ItalyTel: ++39 0871-3555309Fax. ++39 0871-3555307e-mail: [email protected]
REFERENCES
1. Allen DG. Eccentric muscle damage: mechanism of early reduction of force. Acta Physiologica Scandinavica 2001;171: 311-319.
2. Appel HJ, Soares JM, Duarte JA. Exercise, muscle damage and fatigue. J Sport Med 1992; 13:108-115.
3. Noakes TD. Effects of exercise on serum enzyme activities in humans. Sports Med 1987; 4(4):245-67.
4. Armstrong RB, Warren GL, Warren JA. Mechanism of exercise-induced muscle fibre injury. J Sport Med 1991; 12:184-207.
5. Newham DJ, McPail G, Mills KR, Edwards RH. Ultrastructural changes after concentric and eccentric contractions of human muscle J Neurol Sci 1983; 61: 109-22
6. Farthing JP, Chilbeck PD. The effects of eccentric and concentric training at different velocities on muscle hypertrophy Eur J Appl Physiol 2003; 89:578-86
7. Daykin CA, Foxall PJ, Connor SC, Lindon JC, Nicholson JK. The comparison of plasma deproteinization method for the detection of
low-molecular-weight metabolites by (1)H nuclear magnetic resonance spectroscopy. Anal Biochem 2002; 304:220-30.
8. Van Beaumont W. Evaluation of hemoconcentration from hematocrit measurements. J Appl Physiol 1972; 32:712-713.
9. Norman B, Sollevy A, Kaijser L, Jansson E. ATP breakdown products in human skeletal muscle during prolonged exercise to exhaustion. Clin Physiol 1987; 243:1131-8.
10. Bangsbo J, Sjodin B, Hellsten-Westing Y. Exchange of hypoxanthine in muscle during intense exercise in man. Acta Physiol Scand 1992; 146:528-533.
11. Bosello S, Pers JO, Rochas C, Devauchelle V et al. BAFF and rheumatic autoimmune disoders: implications for disease management and therapy. Int J Immunopathol Pharmacol 2007; 20(1):1-8.
12. Bhattacharya K, Farwell M, Huang M et a. Mat cell deficient W/Wv mice have lower serum IL-6 and less cardiac tissue necrosi than their normal littermates following myocardial ischemia-reperfusion. Int J Immunopathol Pharmacol 2007; 1:69-74
13. Merla A, Romani GE, Tangherlini A, Di Romualdo S et al. Penile cutaneous temperature in systemic sclerosis: a thermal imaging study. Int J Immunopathol Pharmacol 2007; 1:139.
14. Deviri E, Glenville BE. Inflammatory response in infective endocarditis. Eur J Inflamm 2007; 2:57.
15. Lakota K, Mrak-Poljsak K, Rozman B, Kveder T, Tomsic M, Sodin-Semrl S. Serum amyloid A activation of inflammatory and adhesion molecules in human coronary artery and umbilical vein and endothelial cells.
16. Sutton JR, Toeurs CJ, Ward GR, Fox IH. Purine metabolism during strenuous muscular exercise in man. Metabolism 1980; 29:254-260,
17. Garret WE. Muscle strain injury: clinical basis aspects. Med Sci Sport Exerc 1990; 22:439-443.
18. Ballini A, De Frenza G, Cantore S, Papa F, Grano M, Mastrangelo F, Tetè S, Grassi FR. In vitro stem cell cultures from human dental pulp and periodontal ligament: new prospects in dentistry. Int J Immunopathol Pharmacol 2007; 1:9.
19. Arimoto T, Takano H, Inoue K, et al. Pulmonary exposure to diesel exhaust particale components enhances circulatory chemokines
Speranza et al
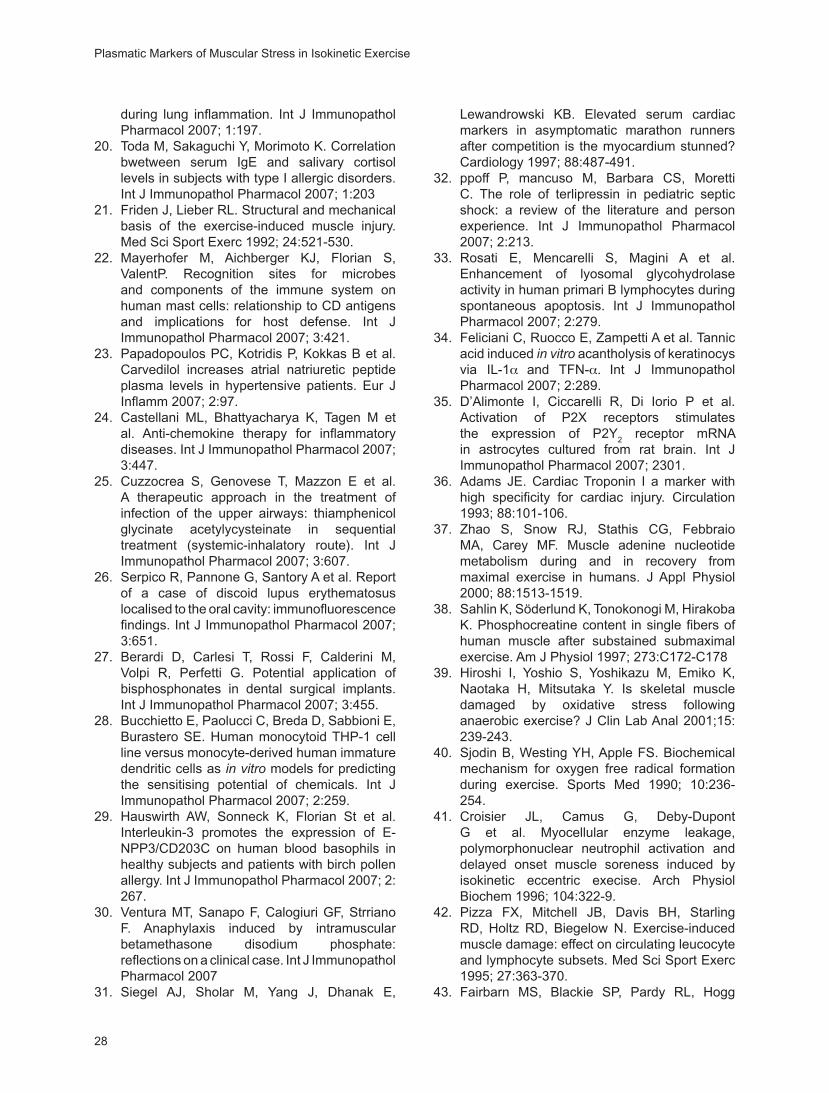
28
during lung inflammation. Int J Immunopathol Pharmacol 2007; 1:197.
20. Toda M, Sakaguchi Y, Morimoto K. Correlation bwetween serum IgE and salivary cortisol levels in subjects with type I allergic disorders. Int J Immunopathol Pharmacol 2007; 1:203
21. Friden J, Lieber RL. Structural and mechanical basis of the exercise-induced muscle injury. Med Sci Sport Exerc 1992; 24:521-530.
22. Mayerhofer M, Aichberger KJ, Florian S, ValentP. Recognition sites for microbes and components of the immune system on human mast cells: relationship to CD antigens and implications for host defense. Int J Immunopathol Pharmacol 2007; 3:421.
23. Papadopoulos PC, Kotridis P, Kokkas B et al. Carvedilol increases atrial natriuretic peptide plasma levels in hypertensive patients. Eur J Inflamm 2007; 2:97.
24. Castellani ML, Bhattyacharya K, Tagen M et al. Anti-chemokine therapy for inflammatory diseases. Int J Immunopathol Pharmacol 2007; 3:447.
25. Cuzzocrea S, Genovese T, Mazzon E et al. A therapeutic approach in the treatment of infection of the upper airways: thiamphenicol glycinate acetylycysteinate in sequential treatment (systemic-inhalatory route). Int J Immunopathol Pharmacol 2007; 3:607.
26. Serpico R, Pannone G, Santory A et al. Report of a case of discoid lupus erythematosus localised to the oral cavity: immunofluorescence findings. Int J Immunopathol Pharmacol 2007; 3:651.
27. Berardi D, Carlesi T, Rossi F, Calderini M, Volpi R, Perfetti G. Potential application of bisphosphonates in dental surgical implants. Int J Immunopathol Pharmacol 2007; 3:455.
28. Bucchietto E, Paolucci C, Breda D, Sabbioni E, Burastero SE. Human monocytoid THP-1 cell line versus monocyte-derived human immature dendritic cells as in vitro models for predicting the sensitising potential of chemicals. Int J Immunopathol Pharmacol 2007; 2:259.
29. Hauswirth AW, Sonneck K, Florian St et al. Interleukin-3 promotes the expression of E-NPP3/CD203C on human blood basophils in healthy subjects and patients with birch pollen allergy. Int J Immunopathol Pharmacol 2007; 2:267.
30. Ventura MT, Sanapo F, Calogiuri GF, Strriano F. Anaphylaxis induced by intramuscular betamethasone disodium phosphate: reflections on a clinical case. Int J Immunopathol Pharmacol 2007
31. Siegel AJ, Sholar M, Yang J, Dhanak E,
Lewandrowski KB. Elevated serum cardiac markers in asymptomatic marathon runners after competition is the myocardium stunned? Cardiology 1997; 88:487-491.
32. ppoff P, mancuso M, Barbara CS, Moretti C. The role of terlipressin in pediatric septic shock: a review of the literature and person experience. Int J Immunopathol Pharmacol 2007; 2:213.
33. Rosati E, Mencarelli S, Magini A et al. Enhancement of lyosomal glycohydrolase activity in human primari B lymphocytes during spontaneous apoptosis. Int J Immunopathol Pharmacol 2007; 2:279.
34. Feliciani C, Ruocco E, Zampetti A et al. Tannic acid induced in vitro acantholysis of keratinocys via IL-1α and TFN-α. Int J Immunopathol Pharmacol 2007; 2:289.
35. D’Alimonte I, Ciccarelli R, Di Iorio P et al. Activation of P2X receptors stimulates the expression of P2Y
2 receptor mRNA
in astrocytes cultured from rat brain. Int J Immunopathol Pharmacol 2007; 2301.
36. Adams JE. Cardiac Troponin I a marker with high specificity for cardiac injury. Circulation 1993; 88:101-106.
37. Zhao S, Snow RJ, Stathis CG, Febbraio MA, Carey MF. Muscle adenine nucleotide metabolism during and in recovery from maximal exercise in humans. J Appl Physiol 2000; 88:1513-1519.
38. Sahlin K, Söderlund K, Tonokonogi M, Hirakoba K. Phosphocreatine content in single fibers of human muscle after substained submaximal exercise. Am J Physiol 1997; 273:C172-C178
39. Hiroshi I, Yoshio S, Yoshikazu M, Emiko K, Naotaka H, Mitsutaka Y. Is skeletal muscle damaged by oxidative stress following anaerobic exercise? J Clin Lab Anal 2001;15:239-243.
40. Sjodin B, Westing YH, Apple FS. Biochemical mechanism for oxygen free radical formation during exercise. Sports Med 1990; 10:236-254.
41. Croisier JL, Camus G, Deby-Dupont G et al. Myocellular enzyme leakage, polymorphonuclear neutrophil activation and delayed onset muscle soreness induced by isokinetic eccentric execise. Arch Physiol Biochem 1996; 104:322-9.
42. Pizza FX, Mitchell JB, Davis BH, Starling RD, Holtz RD, Biegelow N. Exercise-induced muscle damage: effect on circulating leucocyte and lymphocyte subsets. Med Sci Sport Exerc 1995; 27:363-370.
43. Fairbarn MS, Blackie SP, Pardy RL, Hogg
Plasmatic Markers of Muscular Stress in Isokinetic Exercise
29
JC. Comparison of effects of exercise and hyperventilation on leukocyte kinetics in humans. J Appl Physiol 1993; 75:2425-2428.
44. Nieman DC, Henson DA, Johnson R, Lebeck L, Davis JM, Nehlsen-Cannarella SL. Effect of brief, heavy exertion on circulating lymphocyte subpopulations and proliferative response. Med Sci Sport Exerc 1992; 24:1339-1345.
45. Sjodin B, Westing YH, Apple FS. Biochemical mechanism for oxygen free radical formation during exercise. Sports Med 1990; 10:236-254.
46. Vina J, Gimeno A, Sastre J, Desco C, Asensi M, Pallardo FV, Cuesta A, Ferrero A, Ferrero JA, Terada LS, Repine JE. Mechanism of free radical production in exhaustive exercise in human and rats; role of xanthine oxidase and
protection by allopurinol. IUBMB Life 2000; 49:539-44.
47. Hellsten Y, Tullson PC, Richter EA, Bangsbo J. Oxidation of urate in human skeletal muscle during exercise. Free Radic Biol Med 1997; 22:169-174.
48. Cohen AM, Aberdroth RE, Hochstein P. Inhibition of free radical-induced DNA damage by uric acid. FEBS Lett 1984; 174:147-150.
49. Woo J, Lacbawan F, Sunheimer R, LeFevre D, McCabe JB. Is myoglobin useful in the diagnosis of acute myocardial infarction in the emergency department setting? Am J Clin Pathol 1995; 103:725-729.
50. Flogel U, Godegke A, Klotz LO, Schrader J. Role of myoglobin in the antioxidant defence of the heart. FASEB J 2004;18:1156-8.
Speranza et al

Journal of Biological Regulators and Homeostatic Agents
0393-974XCopyright © by BIOLIFE, s.a.s
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyrighter holder.
Unauthorized reproduction may result in financial and other penalties31
Dentin sialophosphoprotein expressionduring human matrix developmentF. MASTRANGELO1, A.P. SCIOLETTI2,3, M. TRANASI1, S. TECCO1, M.T. SBERNA4, R. VINCI4, A. GRILLI5, L. STUPPIA2,3, E. GHERLONE4, S. TETÈ1
1Deparment of Oral Science, University “G. d’Annunzio“, Chieti, Italy 2Center of Excellence of Aging (CESI), University “G. d’Annunzio“ Chieti, Italy 3Department of Clinical Sciences and Bio-imaging-University “G. d’Annunzio“ Chieti, Italy 4Department of Dentistry, University “Vita e Salute, San Raffaele”, Milano, Italy5Biomorphology Department, University “G. d’Annunzio“, Chieti, Italy
Received: March 23, 2006Accepted: June 16, 2006
ABSTRACT: Dentin sialophosphoprotein (DSPP) is a phosphorylated parent protein that is cleaved post-translationally into three dentin components: dentin sialoprotein, dentin glycoprotein, and dentin phosphoprotein. In this study we evaluated the dentin sialophosphoprotein expression in human tooth germs to determine its role in tooth development and matrix deposition. DSPP gene expression was investigated performing reverse-transcription polymerase chain-reaction (RT-PCR) and a microarray analysis carried out using high density array containing 21.329 transcripts in replicates. To test for the expression of the DSPP protein, western immunoblot and immunohistochemical analyses were performed during different phases of tissues and matrix formation. All the analyses performed showed high expression level of DSPP in human tooth germs, indicating that it may play an essential role in physiological and pathological events in tooth development.
KEY WORDS: Dentin sialophosphoprotein, Matrix deposition, tooth development
INTRODUCTION
DSPP is a member of Small Integrin-Binding Ligand N-linked Glycoproteins (SIBLINGs) (Fisher et al. 2001). The SIBLING family includes dentin sialophosphoprotein (DSPP) (1), osteopontin (OPN) (2), dentin matrix protein 1 (DMP1) (3), bone sialoprotein (BSP) (4), and matrix extracellular phosphoglycoprotein (MEPE) (5). These proteins are associated with mineralized tissue and calcium phosphate stabilization in the body fluids (6). Dentin Sialophosphoprotein (DSPP) is an extracellular matrix protein of primary importance for tooth formation (7) and is expressed by odontoblasts and preameloblasts
(8, 9). The DSPP gene is located on the long (q) arm of chromosome 4 at position 21.3, more precisely, from base pair 88,748,704 to base pair 88,757,048 on chromosome 4. DSPP protein is post-translationally cleaved into three dentin components: dentin sialoprotein (DSP), dentin glycoprotein (DGP) and dentin phosphoprotein (DPP).
Dentin phosphoprotein (DPP), a highly phosphorylated serine and aspartic acid–rich protein
that represent the major non-collagenous component of dentin (Lee et al. 1977; Dimuzio and Veis 1978), is strongly associated with the mineral phase of dentin, being expressed by the ectomesenchymal derived odontoblast cells (10) and represent more than 50% of the non-collagenous proteins in dentin extracellular matrix (Patel P. 2001). DSP is a 95-kDa glycoprotein that accounts for 5–8% of the DECM and has a high carbohydrate (30%) and sialic acid (10%) content. DGP is a stains-all positive protein with an apparent molecular weight of 19 kDa (11) and its most abundant amino acids are glycine (12) and serine (13). For some time DSPP has been considered to be tooth specific, but some studies show the expression of DSPP gene in other tissues such as the inner ear (14) and in bone (15). In this study we evaluated the dentin sialophosphoprotein expression in human tooth germs to determine its role in tooth development.
MATERIALS AND METHODS
Human tooth germs were obtained from 15 third molars extracted for orthodontic purposes from
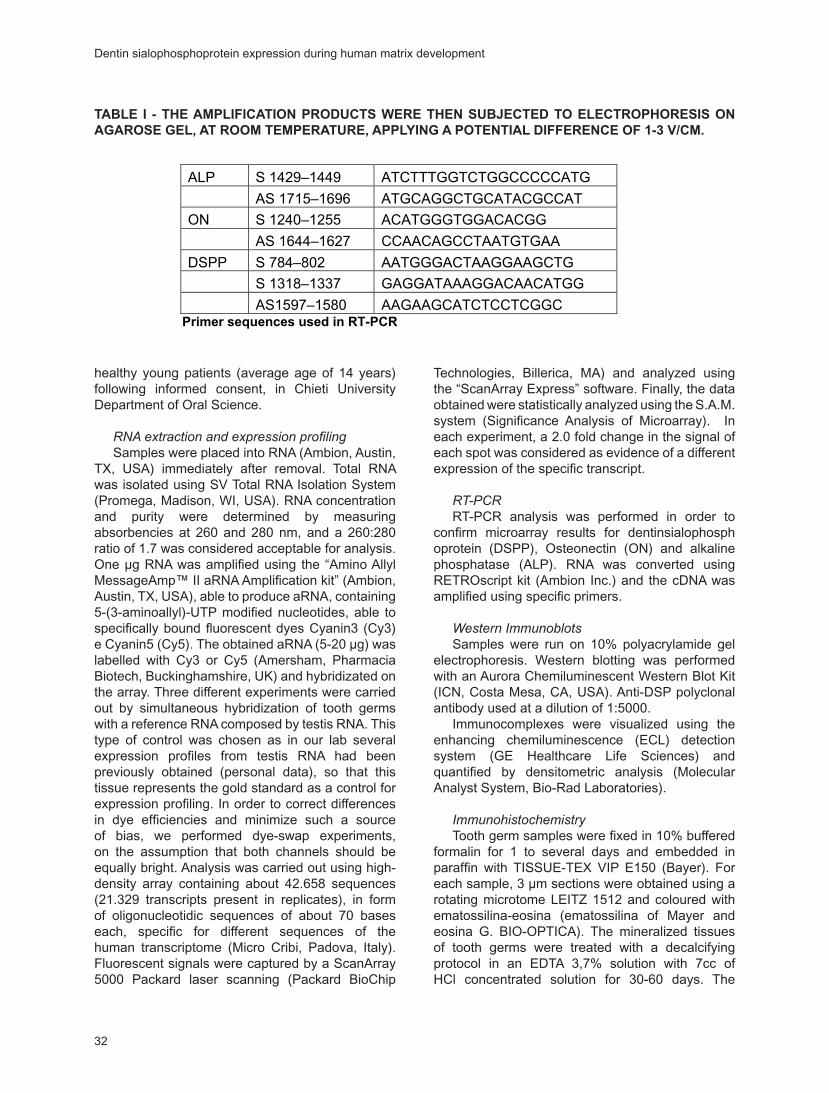
32
healthy young patients (average age of 14 years) following informed consent, in Chieti University Department of Oral Science.
RNA extraction and expression profilingSamples were placed into RNA (Ambion, Austin,
TX, USA) immediately after removal. Total RNA was isolated using SV Total RNA Isolation System (Promega, Madison, WI, USA). RNA concentration and purity were determined by measuring absorbencies at 260 and 280 nm, and a 260:280 ratio of 1.7 was considered acceptable for analysis. One µg RNA was amplified using the “Amino Allyl MessageAmp™ II aRNA Amplification kit” (Ambion, Austin, TX, USA), able to produce aRNA, containing 5-(3-aminoallyl)-UTP modified nucleotides, able to specifically bound fluorescent dyes Cyanin3 (Cy3) e Cyanin5 (Cy5). The obtained aRNA (5-20 µg) was labelled with Cy3 or Cy5 (Amersham, Pharmacia Biotech, Buckinghamshire, UK) and hybridizated on the array. Three different experiments were carried out by simultaneous hybridization of tooth germs with a reference RNA composed by testis RNA. This type of control was chosen as in our lab several expression profiles from testis RNA had been previously obtained (personal data), so that this tissue represents the gold standard as a control for expression profiling. In order to correct differences in dye efficiencies and minimize such a source of bias, we performed dye-swap experiments, on the assumption that both channels should be equally bright. Analysis was carried out using high-density array containing about 42.658 sequences (21.329 transcripts present in replicates), in form of oligonucleotidic sequences of about 70 bases each, specific for different sequences of the human transcriptome (Micro Cribi, Padova, Italy). Fluorescent signals were captured by a ScanArray 5000 Packard laser scanning (Packard BioChip
Technologies, Billerica, MA) and analyzed using the “ScanArray Express” software. Finally, the data obtained were statistically analyzed using the S.A.M. system (Significance Analysis of Microarray). In each experiment, a 2.0 fold change in the signal of each spot was considered as evidence of a different expression of the specific transcript.
RT-PCRRT-PCR analysis was performed in order to
confirm microarray results for dentinsialophosphoprotein (DSPP), Osteonectin (ON) and alkaline phosphatase (ALP). RNA was converted using RETROscript kit (Ambion Inc.) and the cDNA was amplified using specific primers.
Western ImmunoblotsSamples were run on 10% polyacrylamide gel
electrophoresis. Western blotting was performed with an Aurora Chemiluminescent Western Blot Kit (ICN, Costa Mesa, CA, USA). Anti-DSP polyclonal antibody used at a dilution of 1:5000.
Immunocomplexes were visualized using the enhancing chemiluminescence (ECL) detection system (GE Healthcare Life Sciences) and quantified by densitometric analysis (Molecular Analyst System, Bio-Rad Laboratories).
ImmunohistochemistryTooth germ samples were fixed in 10% buffered
formalin for 1 to several days and embedded in paraffin with TISSUE-TEX VIP E150 (Bayer). For each sample, 3 µm sections were obtained using a rotating microtome LEITZ 1512 and coloured with ematossilina-eosina (ematossilina of Mayer and eosina G. BIO-OPTICA). The mineralized tissues of tooth germs were treated with a decalcifying protocol in an EDTA 3,7% solution with 7cc of HCl concentrated solution for 30-60 days. The
����� � � ��� ������������� �������� ���� ���� ��������� �� ��������������� ��������������������������������������������������������������������������������
ALP S 1429–1449 ATCTTTGGTCTGGCCCCCATG
AS 1715–1696 ATGCAGGCTGCATACGCCAT
ON S 1240–1255 ACATGGGTGGACACGG
AS 1644–1627 CCAACAGCCTAATGTGAA
DSPP S 784–802 AATGGGACTAAGGAAGCTG
S 1318–1337 GAGGATAAAGGACAACATGG
AS1597–1580 AAGAAGCATCTCCTCGGC�������������������������������
�������������������
Samples were run on 10% polyacrylamide gel electrophoresis. Western blotting was performed
with an Aurora Chemiluminescent Western Blot Kit (ICN, Costa Mesa, CA, USA). Anti-DSP
polyclonal antibody used at a dilution of 1:5000.
Immunocomplexes were visualized using the enhancing chemiluminescence (ECL) detection
system (GE Healthcare Life Sciences) and quantified by densitometric analysis (Molecular Analyst
System, Bio-Rad Laboratories).
��������������������
Tooth germ samples were fixed in 10% buffered formalin for 1 to several days and embedded in
paraffin with TISSUE-TEX VIP E150 (Bayer). For each sample, 3 �m sections were obtained using
a rotating microtome LEITZ 1512 and coloured with ematossilina-eosina (ematossilina of Mayer
and eosina G. BIO-OPTICA). The mineralized tissues of tooth germs were treated with a
decalcifying protocol in an EDTA 3,7% solution with 7cc of HCl concentrated solution for 30-60
days. The samples thus obtained underwent dehydration using a growing solution of alcohols, and
therefore they underwent dyaphanization with of the BIO-CLEAR and finally embedded in liquid
paraffin. 3 �m sections of all samples were obtained using a rotating microtome LEITZ 1512 and
for each sample which underwent immunocoloration with the STREP.ABC method (streptavidina-
biotina-perossidasi). The sections were incubated with primary monoclonal antibody anti-DSPP
(1:100 Saint Cruz) for 30 minutes at room temperature. The immunoreaction was completed with
TABLE I - THE AMPLIFICATION PRODUCTS WERE THEN SUBJECTED TO ELECTROPHORESIS ON AGAROSE GEL, AT ROOM TEMPERATURE, APPLYING A POTENTIAL DIFFERENCE OF 1-3 V/CM.
Dentin sialophosphoprotein expression during human matrix development
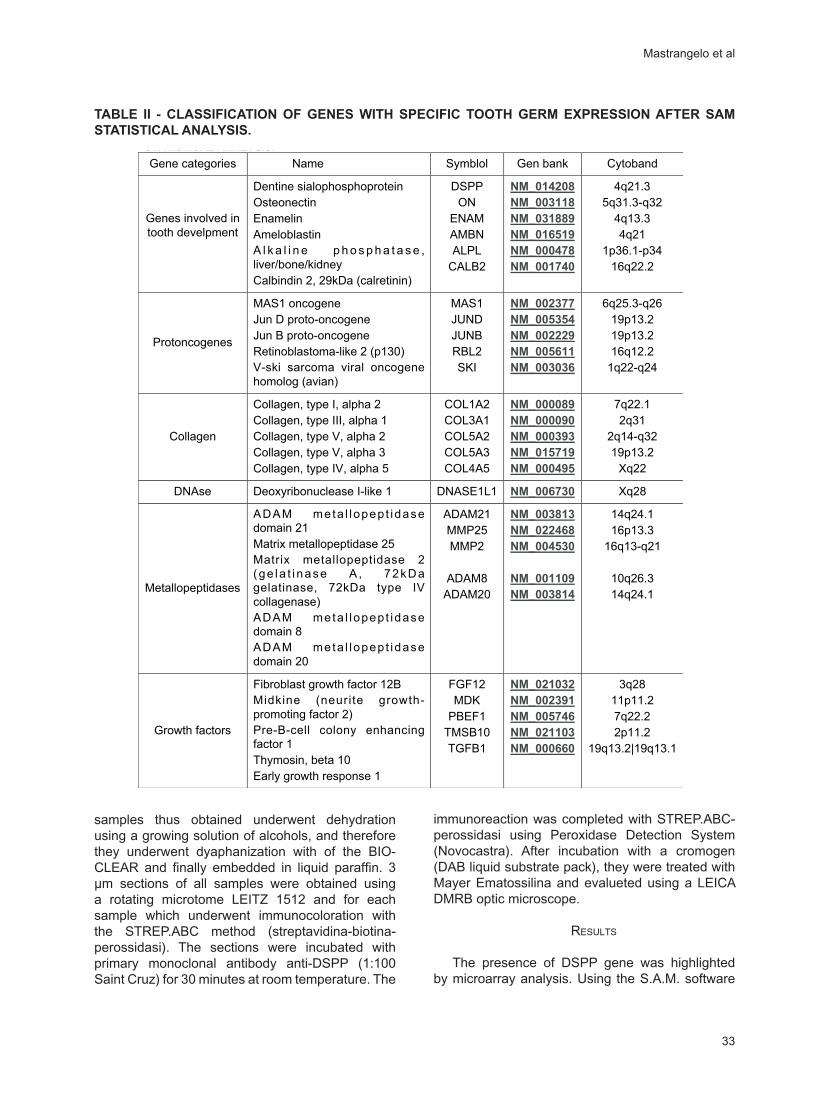
33
samples thus obtained underwent dehydration using a growing solution of alcohols, and therefore they underwent dyaphanization with of the BIO-CLEAR and finally embedded in liquid paraffin. 3 µm sections of all samples were obtained using a rotating microtome LEITZ 1512 and for each sample which underwent immunocoloration with the STREP.ABC method (streptavidina-biotina-perossidasi). The sections were incubated with primary monoclonal antibody anti-DSPP (1:100 Saint Cruz) for 30 minutes at room temperature. The
immunoreaction was completed with STREP.ABC-perossidasi using Peroxidase Detection System (Novocastra). After incubation with a cromogen (DAB liquid substrate pack), they were treated with Mayer Ematossilina and evalueted using a LEICA DMRB optic microscope.
RESULTS
The presence of DSPP gene was highlighted by microarray analysis. Using the S.A.M. software
�����������������������������������������������������������������������������������������������������
Gene categories Name Symblol Gen bank Cytoband
Genes involved in
tooth develpment
Dentine sialophosphoprotein
Osteonectin
Enamelin
Ameloblastin
A l k a l i n e p h o s p h a t a s e ,
liver/bone/kidney
Calbindin 2, 29kDa (calretinin)
DSPP
ON
ENAM
AMBN
ALPL
CALB2
���������
���������
���������
���������
���������
���������
4q21.3
5q31.3-q32
4q13.3
4q21
1p36.1-p34
16q22.2
Protoncogenes
MAS1 oncogene
Jun D proto-oncogene
Jun B proto-oncogene
Retinoblastoma-like 2 (p130)
V-ski sarcoma viral oncogene
homolog (avian)
MAS1
JUND
JUNB
RBL2
SKI
���������
���������
���������
���������
���������
6q25.3-q26
19p13.2
19p13.2
16q12.2
1q22-q24
Collagen
Collagen, type I, alpha 2
Collagen, type III, alpha 1
Collagen, type V, alpha 2
Collagen, type V, alpha 3
Collagen, type IV, alpha 5
COL1A2
COL3A1
COL5A2
COL5A3
COL4A5
���������
���������
���������
���������
���������
7q22.1
2q31
2q14-q32
19p13.2
Xq22
DNAse Deoxyribonuclease I-like 1 DNASE1L1 ��������� Xq28
Metallopeptidases
ADAM meta l lopep t idase
domain 21
Matrix metallopeptidase 25
Matrix metallopeptidase 2
(ge la t i nase A , 72kDa
gelatinase, 72kDa type IV
collagenase)
ADAM meta l lopep t idase
domain 8
ADAM meta l lopep t idase
domain 20
ADAM21
MMP25
MMP2
ADAM8
ADAM20
���������
���������
���������
���������
���������
14q24.1
16p13.3
16q13-q21
10q26.3
14q24.1
Growth factors
Fibroblast growth factor 12B
Midkine (neurite growth-
promoting factor 2)
Pre-B-cell colony enhancing
factor 1
Thymosin, beta 10
Early growth response 1
FGF12
MDK
PBEF1
TMSB10
TGFB1
���������
���������
���������
���������
���������
3q28
11p11.2
7q22.2
2p11.2
19q13.2|19q13.1
TABLE II - CLASSIFICATION OF GENES WITH SPECIFIC TOOTH GERM EXPRESSION AFTER SAM STATISTICAL ANALYSIS.
Mastrangelo et al
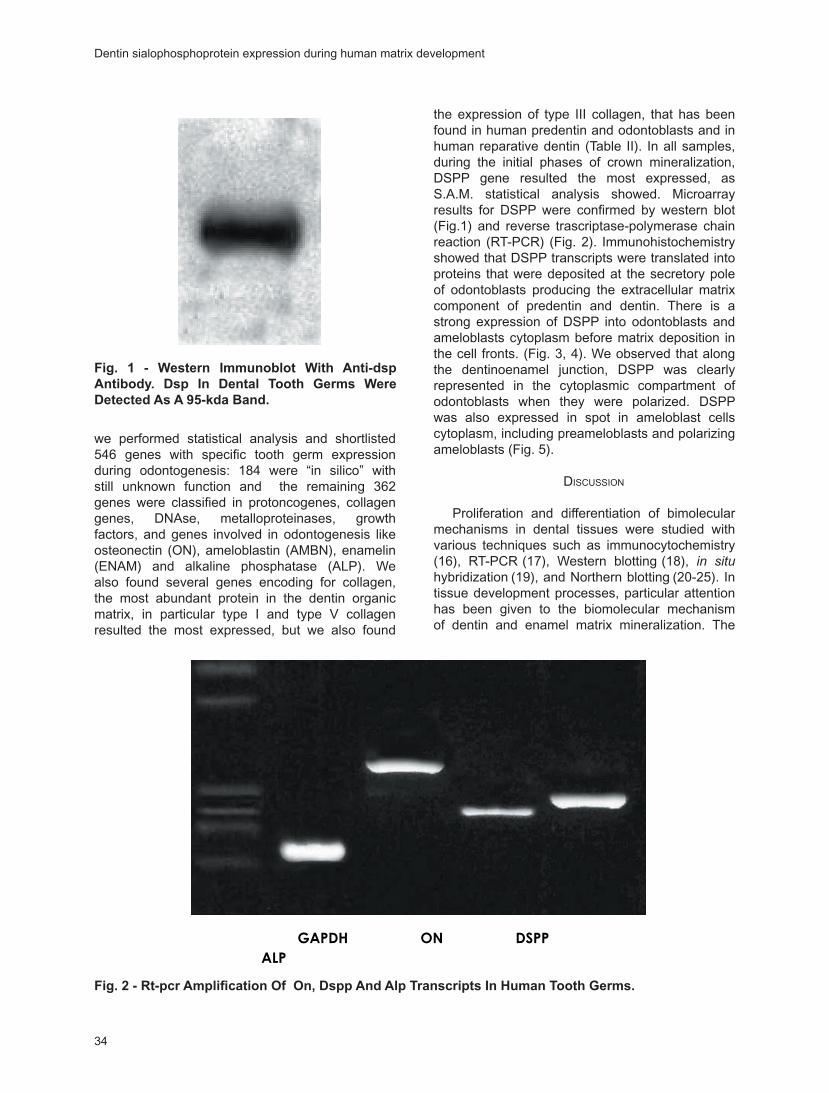
34
we performed statistical analysis and shortlisted 546 genes with specific tooth germ expression during odontogenesis: 184 were “in silico” with still unknown function and the remaining 362 genes were classified in protoncogenes, collagen genes, DNAse, metalloproteinases, growth factors, and genes involved in odontogenesis like osteonectin (ON), ameloblastin (AMBN), enamelin (ENAM) and alkaline phosphatase (ALP). We also found several genes encoding for collagen, the most abundant protein in the dentin organic matrix, in particular type I and type V collagen resulted the most expressed, but we also found
the expression of type III collagen, that has been found in human predentin and odontoblasts and in human reparative dentin (Table II). In all samples, during the initial phases of crown mineralization, DSPP gene resulted the most expressed, as S.A.M. statistical analysis showed. Microarray results for DSPP were confirmed by western blot (Fig.1) and reverse trascriptase-polymerase chain reaction (RT-PCR) (Fig. 2). Immunohistochemistry showed that DSPP transcripts were translated into proteins that were deposited at the secretory pole of odontoblasts producing the extracellular matrix component of predentin and dentin. There is a strong expression of DSPP into odontoblasts and ameloblasts cytoplasm before matrix deposition in the cell fronts. (Fig. 3, 4). We observed that along the dentinoenamel junction, DSPP was clearly represented in the cytoplasmic compartment of odontoblasts when they were polarized. DSPP was also expressed in spot in ameloblast cells cytoplasm, including preameloblasts and polarizing ameloblasts (Fig. 5).
DISCUSSION
Proliferation and differentiation of bimolecular mechanisms in dental tissues were studied with various techniques such as immunocytochemistry
(16), RT-PCR (17), Western blotting (18), in situ hybridization (19), and Northern blotting (20-25). In tissue development processes, particular attention has been given to the biomolecular mechanism of dentin and enamel matrix mineralization. The
������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������
��������������������������������������������������������
���
Fig. 1 - Western Immunoblot With Anti-dsp Antibody. Dsp In Dental Tooth Germs Were Detected As A 95-kda Band.
������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������
��������������������������������������������������������
���
Fig. 2 - Rt-pcr Amplification Of On, Dspp And Alp Transcripts In Human Tooth Germs.
Dentin sialophosphoprotein expression during human matrix development

35
chemical compositions, structural organization, and mechanical properties of the various dental tissues are a result of extracellular processes that regulate the nucleation, growth and organization of mineral crystals (26-31).
Numerous molecules have been connected to odontogenesis: dentin is formed when odontoblasts secrete the extracellular matrices (ECM), called predentin, which is afterwards mineralized when apatite crystals are deposited. The extracellular matrix (ECM) of dentin contains several non-collagenous proteins (SIBLING) that play essential biological roles in dentin mineralization.
The protein matrix of forming enamel during the early stages of amelogenesis is composed predominantly of amelogenin and its cleavage products, making up over 90% of the enamel matrix, (Termine et al,1980; Fincham et al, 1999) but other enamel matrix proteins, such as enamelin and ameloblastin, also regulate enamel formation (26).
Dentin sialophosphoprotein (DSPP), a member of the SIBLING protein family, is critical for proper tooth formation. In fact, there are conspicuous dental anomalies that occur when this gene is damaged by mutations. Eight different mutations causing DGI type II have been reported in the gene encoding dentin sialophosphoprotein (32-34), and one of these mutations manifests itself as DGI type III. A DSPP mutation has also been shown to cause type I dentin dysplasia (DD) (35-40). It has also been proposed that the dental manifestations in X-linked hypophosphatemia (XLH), a condition caused by mutations in a gene encoding a membrane bound matrix metalloproteinase (PHEX; Xp22), may be due to a failure to process DSPP into smaller functional domains (41). In our study DSPP was evaluated performing Microarray, RT-PCR, Western blotting and Immunohistochemistry. DSPP gene resulted highly expressed in tooth germs as microarray results showed, confirming the great importance of DSPP protein for matrix deposition. DSPP protein, performing the immunohistochemistry analysis, was observed at the secretory pole of odontoblasts and in presecretory ameloblasts. DSPP resulted particularly expressed in the early stages of matrix mineralization while successively its expression decreased showing the specific role of this protein during dentin and enamel mineralization and the significance of evaluation of DSPP expression in dental tissues to better understand its rule during biomineralization and odontogenesis. Reprint requests to:Prof. Stefano TetèDepartment of Oral SciencesUniversity of Chieti
�������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������
�������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������������
������������������������������������������������������������������������������������������
Fig. 3 - Intracytoplasmatic Strong Expression For Dspp Protein In Odontoblastic Cells Into Human Dental Germs At Low Grade Of Cell Differentiation Before Dentine Matrix Was Produced (10x).
Fig. 4 - At Higher Magnification Odontoblastic Cells Show A High Expression For Dspp (20x).
���� � � ���������� ��� ���� ������� �� ������������ ���� ��� ������������� ��������� ���� ����� ������ ����� �� ������� ����� �� ����� ��������������� �� � ����������������������������������������������������������������������������������
DISCUSSION
Proliferation and differentiation of bimolecular mechanisms in dental tissues were studied with
various techniques such as immunocytochemistry (16), RT-PCR (17), Western blotting (18), �� ����
hybridization (19), and Northern blotting (20-25). In tissue development processes, particular
attention has been given to the biomolecular mechanism of dentin and enamel matrix
mineralization. The chemical compositions, structural organization, and mechanical properties of
the various dental tissues are a result of extracellular processes that regulate the nucleation,
growth and organization of mineral crystals (26-31).
Numerous molecules have been connected to odontogenesis: dentin is formed when
odontoblasts secrete the extracellular matrices (ECM), called predentin, which is afterwards
mineralized when apatite crystals are deposited. The extracellular matrix (ECM) of dentin contains
several non-collagenous proteins (SIBLING) that play essential biological roles in dentin
mineralization.
The protein matrix of forming enamel during the early stages of amelogenesis is composed
predominantly of amelogenin and its cleavage products, making up over 90% of the enamel matrix,
Fig. 5 - Expression For Dspp Protein In Ameloblastic (Am) And Odontoblastic (Od) Cells Into Human Dental Germs At Initial Phase Of Crown Mineralization, At A Low Degree Of Cell Differentiation. (20x); Arrows: Dspp In Matrix Deposition Front.
Mastrangelo et al
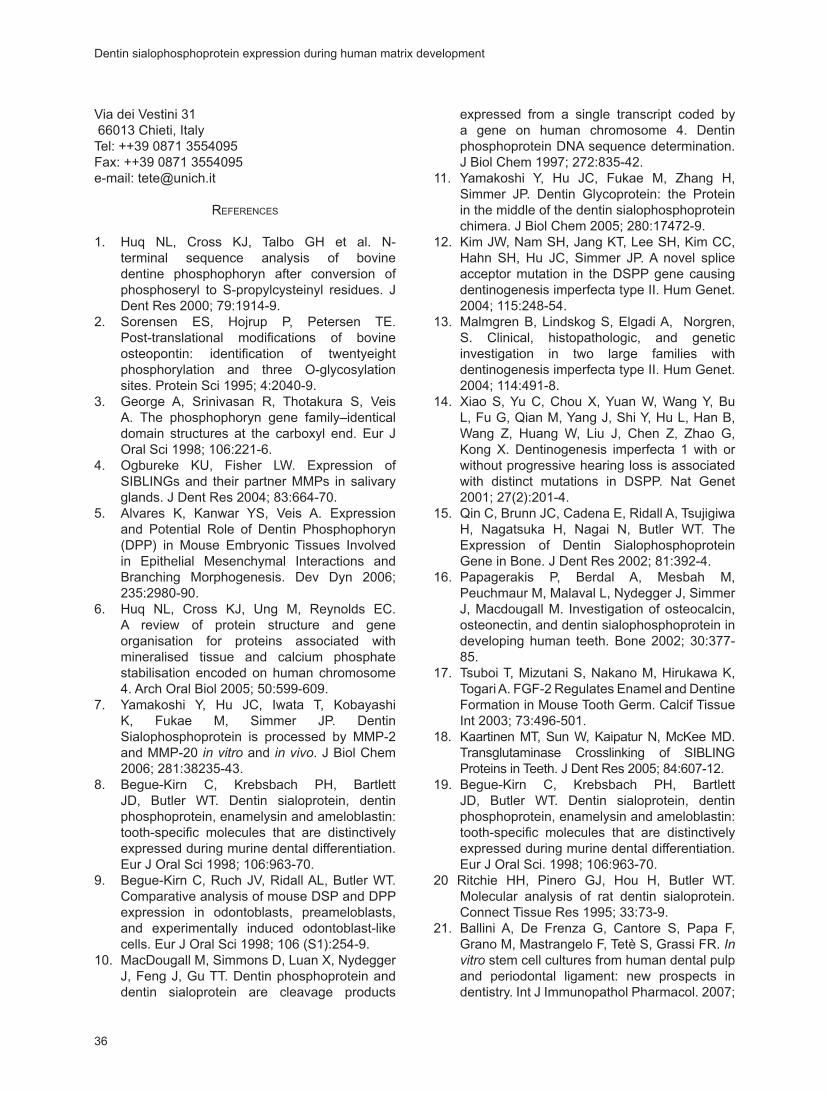
36
Via dei Vestini 31 66013 Chieti, ItalyTel: ++39 0871 3554095Fax: ++39 0871 3554095e-mail: [email protected]
REFERENCES
1. Huq NL, Cross KJ, Talbo GH et al. N-terminal sequence analysis of bovine dentine phosphophoryn after conversion of phosphoseryl to S-propylcysteinyl residues. J Dent Res 2000; 79:1914-9.
2. Sorensen ES, Hojrup P, Petersen TE. Post-translational modifications of bovine osteopontin: identification of twentyeight phosphorylation and three O-glycosylation sites. Protein Sci 1995; 4:2040-9.
3. George A, Srinivasan R, Thotakura S, Veis A. The phosphophoryn gene family–identical domain structures at the carboxyl end. Eur J Oral Sci 1998; 106:221-6.
4. Ogbureke KU, Fisher LW. Expression of SIBLINGs and their partner MMPs in salivary glands. J Dent Res 2004; 83:664-70.
5. Alvares K, Kanwar YS, Veis A. Expression and Potential Role of Dentin Phosphophoryn (DPP) in Mouse Embryonic Tissues Involved in Epithelial Mesenchymal Interactions and Branching Morphogenesis. Dev Dyn 2006; 235:2980-90.
6. Huq NL, Cross KJ, Ung M, Reynolds EC. A review of protein structure and gene organisation for proteins associated with mineralised tissue and calcium phosphate stabilisation encoded on human chromosome 4. Arch Oral Biol 2005; 50:599-609.
7. Yamakoshi Y, Hu JC, Iwata T, Kobayashi K, Fukae M, Simmer JP. Dentin Sialophosphoprotein is processed by MMP-2 and MMP-20 in vitro and in vivo. J Biol Chem 2006; 281:38235-43.
8. Begue-Kirn C, Krebsbach PH, Bartlett JD, Butler WT. Dentin sialoprotein, dentin phosphoprotein, enamelysin and ameloblastin: tooth-specific molecules that are distinctively expressed during murine dental differentiation. Eur J Oral Sci 1998; 106:963-70.
9. Begue-Kirn C, Ruch JV, Ridall AL, Butler WT. Comparative analysis of mouse DSP and DPP expression in odontoblasts, preameloblasts, and experimentally induced odontoblast-like cells. Eur J Oral Sci 1998; 106 (S1):254-9.
10. MacDougall M, Simmons D, Luan X, Nydegger J, Feng J, Gu TT. Dentin phosphoprotein and dentin sialoprotein are cleavage products
expressed from a single transcript coded by a gene on human chromosome 4. Dentin phosphoprotein DNA sequence determination. J Biol Chem 1997; 272:835-42.
11. Yamakoshi Y, Hu JC, Fukae M, Zhang H, Simmer JP. Dentin Glycoprotein: the Protein in the middle of the dentin sialophosphoprotein chimera. J Biol Chem 2005; 280:17472-9.
12. Kim JW, Nam SH, Jang KT, Lee SH, Kim CC, Hahn SH, Hu JC, Simmer JP. A novel splice acceptor mutation in the DSPP gene causing dentinogenesis imperfecta type II. Hum Genet. 2004; 115:248-54.
13. Malmgren B, Lindskog S, Elgadi A, Norgren, S. Clinical, histopathologic, and genetic investigation in two large families with dentinogenesis imperfecta type II. Hum Genet. 2004; 114:491-8.
14. Xiao S, Yu C, Chou X, Yuan W, Wang Y, Bu L, Fu G, Qian M, Yang J, Shi Y, Hu L, Han B, Wang Z, Huang W, Liu J, Chen Z, Zhao G, Kong X. Dentinogenesis imperfecta 1 with or without progressive hearing loss is associated with distinct mutations in DSPP. Nat Genet 2001; 27(2):201-4.
15. Qin C, Brunn JC, Cadena E, Ridall A, Tsujigiwa H, Nagatsuka H, Nagai N, Butler WT. The Expression of Dentin Sialophosphoprotein Gene in Bone. J Dent Res 2002; 81:392-4.
16. Papagerakis P, Berdal A, Mesbah M, Peuchmaur M, Malaval L, Nydegger J, Simmer J, Macdougall M. Investigation of osteocalcin, osteonectin, and dentin sialophosphoprotein in developing human teeth. Bone 2002; 30:377-85.
17. Tsuboi T, Mizutani S, Nakano M, Hirukawa K, Togari A. FGF-2 Regulates Enamel and Dentine Formation in Mouse Tooth Germ. Calcif Tissue Int 2003; 73:496-501.
18. Kaartinen MT, Sun W, Kaipatur N, McKee MD. Transglutaminase Crosslinking of SIBLING Proteins in Teeth. J Dent Res 2005; 84:607-12.
19. Begue-Kirn C, Krebsbach PH, Bartlett JD, Butler WT. Dentin sialoprotein, dentin phosphoprotein, enamelysin and ameloblastin: tooth-specific molecules that are distinctively expressed during murine dental differentiation. Eur J Oral Sci. 1998; 106:963-70.
20 Ritchie HH, Pinero GJ, Hou H, Butler WT. Molecular analysis of rat dentin sialoprotein. Connect Tissue Res 1995; 33:73-9.
21. Ballini A, De Frenza G, Cantore S, Papa F, Grano M, Mastrangelo F, Tetè S, Grassi FR. In vitro stem cell cultures from human dental pulp and periodontal ligament: new prospects in dentistry. Int J Immunopathol Pharmacol. 2007;
Dentin sialophosphoprotein expression during human matrix development
37
20:9-16. 22. Cunnea P, Fernandes AP, Capitanio A, Eken S,
Spyrou G, Björnstedt M. Increased expression of specific thioredoxin family proteins; a pilot immunohistochemical study on human hepatocellular carcinoma. Int J Immunopathol Pharmacol. 2007; 20:17-24.
23. Cardillo MR, Ippoliti F. Interleukin-6, interleukin-10 and heat shock protein-90 expression in renal epithelial neoplasias and surrounding normal-appearing renal parenchyma. Int J Immunopathol Pharmacol. 2007; 20:37-46.
24. Berardi D, Carlesi T, Rossi F, Calderini M, Volpi R, Perfetti G. Potential applications of biphosphonates in dental surgical implants. Int J Immunopathol Pharmacol. 2007; 20:455-65.
25. Di Bonaventura G, Prosseda G, Del Chierico F, et al. Molecular characterization of virulence determinants of Stenotrophomonas maltophilia strains isolated from patients affected by cystic fibrosis. Int J Immunopathol Pharmacol. 2007; 20:529-37.
26. Margolis HC, Beniash E, Fowler CE. Role of macromolecular assembly of enamel matrix proteins in enamel formation. J Dent Res 2006; 85:775-93.
27. Bocchietto E, Paolucci C, Breda D, Sabbioni E, Burastero SE. Human monocytoid THP-1 cell line versus monocyte-derived human immature dendritic cells as in vitro models for predicting the sensitising potential of chemicals. Int J Immunopathol Pharmacol. 2007; 20:259-65.
28. Feliciani C, Ruocco E, Zampetti A, Toto P, Amerio P, Tulli A, Amerio P, Ruocco V. Tannic acid induces in vitro acantholysis of keratinocytes via IL-1alpha and TNF-alpha. Int J Immunopathol Pharmacol. 2007; 20:289-99.
29. D’Alimonte I, Ciccarelli R, Di Iorio P, Nargi E, Buccella S, Giuliani P, Rathbone MP, Jiang S, Caciagli F, Ballerini P. Activation of P2X(7) receptors stimulates the expression of P2Y(2) receptor mRNA in astrocytes cultured from rat brain. Int J Immunopathol Pharmacol. 2007; 20:301-16.
30. Pannone G, Sanguedolce F, De Maria S, et al. Cyclooxygenase isozymes in oral squamous cell carcinoma:a real-time RT-PCR study with clinic pathological correlations. Int J Immunopathol Pharmacol. 2007; 20:317-24.
31. Simonetti O, Goteri G, Lucarini G, Rubini C, Stramazzotti D, Lo Muzio L, Biagini G, Offidani A. In melanoma changes of immature and mature dendritic cell expression correlate with tumor thickness:an immunohistochemical
study. Int J Immunopathol Pharmacol. 2007; 20:325-33.
32. Zhang X, Zhao J, Li C, Gao S, Qiu C, Liu P, Wu G, Qiang B, Lo WH, Shen Y. DSPP mutation in dentinogenesis imperfecta Shields type II. Nat Genet 2001; 27:129-30.
33. Malmgren B, Lindskog S, Elgadi A, Norgren S. Clinical, histopathologic, and genetic investigation in two large families with dentinogenesis imperfecta type II. Hum Genet. 2004; 114:491-8.
34. Kim JW, Nam SH, Jang KT, Lee SH, Kim CC, Hahn SH, Hu JC, Simmer JP. A novel splice acceptor mutation in the DSPP gene causing dentinogenesis imperfecta type II. Hum Genet 2004; 115:248-54.
35. Rajpar MH, Koch MJ, Davies RM, Mellody KT, Kielty CM, Dixon MJ. Mutation of the signal peptide region of the bicistronic gene DSPP affects translocation to the endoplasmic reticulum and results in defective dentine biomineralization. Hum Mol Genet 2002; 11:2559-65.
36. D’Arcangelo C, Di Nardo Di Maio F, Stracci N, Spoto G, Malagnino VA, Caputi S. Pulp-dissolving ability of several endodontic irrigants: a spectrophotometric evaluation. Int J Immunopathol Pharmacol. 2007; 20:381-6.
37. Ventura MT, Sanapo F, Calogiuri GF, Anaphylaxis induced by intramuscular betamethasone disodium phosphate: reflections on a clinical case. Int J Immunopathol Pharmacol. 2007; 20:387-91.
38. K. Lakota, K. Mrak-Poljšak, B. Rozman, T. Kveder, M. Tomši� and S. Sodin-Semrl. Serum amyloid A activation of inflammatory and adhesion molecules in human coronary artery and umbilical vein endothelial cells. Eur J Inflamm. 2007; 5:73-82.
39. G. Ahangari, Z. Chavoshzadeh, Z. Lari, A. Ramyar and A. Farhoudi. Novel mutation detection of an inflammatory molecule Elastase II gene encoding neutrophil Elastase in Kostmann syndrome. Eur J Inflamm. 2007; 5:65-72.
40. S. Capodiferro, C. Scully, G. Ficarra, G. de Frenza, R. Grassi, E. Maiorano, G. Favia, F. Mastrangelo and S. Tetè. Orofacial granulomatosis: report of two cases with gingival onset. Eur J Inflamm. 2007; 5:51-56.
41. Qin C, Baba O, Butler WT. Post-translational modifications of sibling proteins and their roles in osteogenesis and dentinogenesis. Crit Rev Oral Biol Med 2004; 15:126-36.
Mastrangelo et al
Journal of Biological Regulators and Homeostatic Agents
0393-974XCopyright © by BIOLIFE, s.a.s
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyrighter holder.
Unauthorized reproduction may result in financial and other penalties39
Statistical evaluation and parametersof phlogosis in patients sensitized to cypress M.T. VENTURA¹, M. GELARDI2, R. DI GIOIA¹, R. BUQUICCHIO¹, G. ACCETTURA¹, R.A. TUMMOLO¹, A. ARSIENI¹
¹Department of Internal Medicine, Immunology and Infectious Disease (MIDIM). 2University of Bari; ¹Department of Otolaryngology, University of Bari, Bari, Italy
Received: October 10, 2006Accepted January 17, 2007
ABSTRACT: To assess the increasing sensitivity to cypress, we evaluated a group of allergic subjects living in Apulia who had been referred for respiratory symptoms to the Section for Allergic and Immunological Diseases (SAID) of Bari University Hospital in the period between January and March 2006, and compared them with a group evaluated during the same months of 2003.We submitted all patients to Skin Prick Tests (SPT) and Radio-Allergo-Sorbent Tests (RAST). Our data show that the percentage of people sensitised to cypress has increased from 28.6% (2003) to 65.5% (2006). By contrast, we observed no variations in sensitisation to other substances. Since according to data furnished by the Italian Association of Areobiology (AIA), Monitoring Center of Brindisi 1, there was a variation in the quantity of pollen grains in 2006 as compared to 2003, it seems conceivable that an increase in the amount of pollen grains, together with other factors such as the volume and the brittleness of the grain may influence the increasing sensitization.In addition, other allergo-immunologic parameters were evaluated for a better evaluation of this allergic phlogosis.
KEY WORDS: Pollinosis, Cypress, Aerobiology, Eosinophil, ECP
INTRODUCTION
“Pollinosis” is a seasonal allergic pathology, also defined as “hay fever”, characterized by symptoms like nasal itch, rinorrhea, nasal obstruction, con-junctivitis and sometimes asthma after exposure to pollens in predisposed subjects (1). The pollens form a biological aerosol and, after spontaneous inhalation, penetrate the upper respiratory mucosa and release their allergenic content. Clinical symp-toms appear in subjects specifically sensitized to allergens, who synthesize IgE after pollen stimula-tion (2). The pollens of cypress appear punctually after blooming: they are present in the air from the beginning of January, and with the subsequent flow-ering of different species belonging to this family, remaining in high concentrations (some hundred granules per cubic meter of air) up to the end of April. In Southern Italy, according to some studies, the minimum has been reported to be equal to 2 % (4-5). Other Authors found that the prevalence
of allergy to cypress in the general population in Italy varies from 9.2% in the North, to 28.2% in Central Italy and 20.1% to the South (3). In Europe the prevalence ranges from 20% in South Italy to 35% in Cordoba, Spain (3-4). The present study was conducted retrospectively with the purpose of evaluating increased sensitization to Cypress sem-pervirens and Cypress arizonica in a large group of allergic subjects living in Puglia, Italy, by comparing evaluations made during the winter periods of 2003 and 2006. In addition, some parameters of inflam-mation were evaluated in order to determine varia-tions of allergic stimulation.
MATERIALS AND METHODS
For this study we evaluated allergic patients with respiratory symptoms referred to the SAID of the University of Bari in the period between January and March 2006 and compared them with patients examined at the same University hospital in the pe-
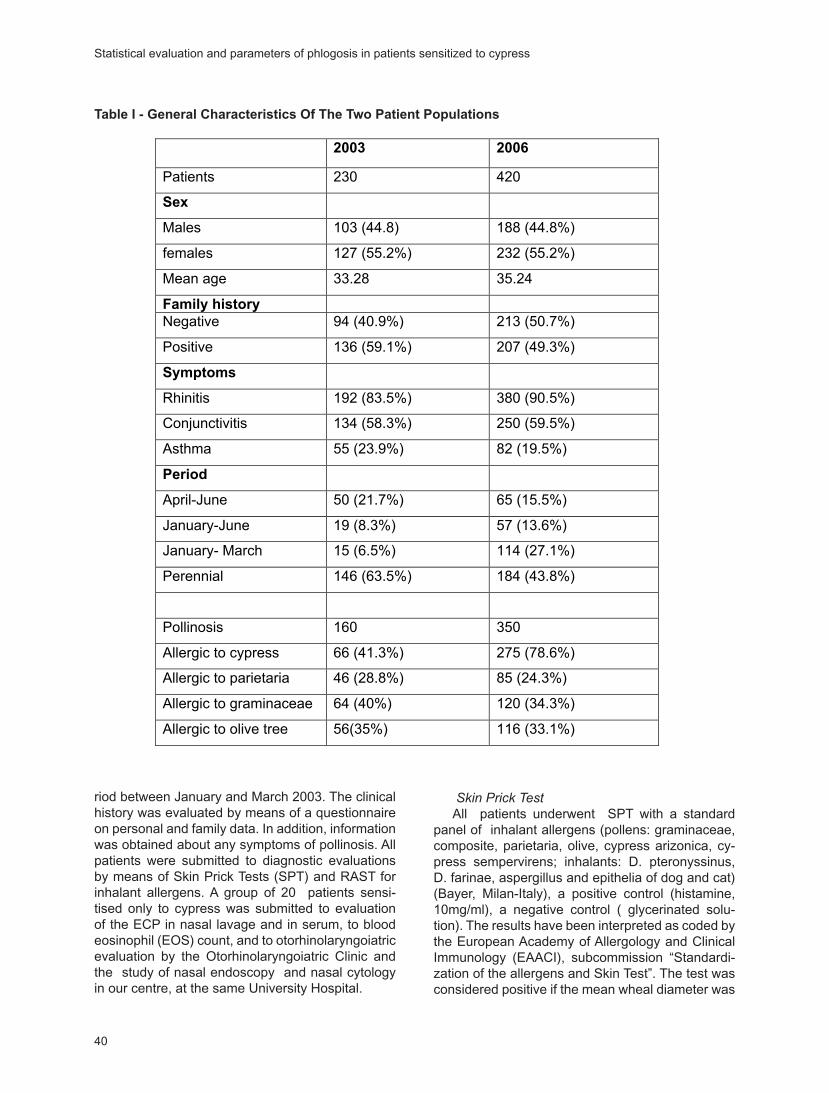
40
riod between January and March 2003. The clinical history was evaluated by means of a questionnaire on personal and family data. In addition, information was obtained about any symptoms of pollinosis. All patients were submitted to diagnostic evaluations by means of Skin Prick Tests (SPT) and RAST for inhalant allergens. A group of 20 patients sensi-tised only to cypress was submitted to evaluation of the ECP in nasal lavage and in serum, to blood eosinophil (EOS) count, and to otorhinolaryngoiatric evaluation by the Otorhinolaryngoiatric Clinic and the study of nasal endoscopy and nasal cytology in our centre, at the same University Hospital.
Skin Prick TestAll patients underwent SPT with a standard
panel of inhalant allergens (pollens: graminaceae, composite, parietaria, olive, cypress arizonica, cy-press sempervirens; inhalants: D. pteronyssinus, D. farinae, aspergillus and epithelia of dog and cat) (Bayer, Milan-Italy), a positive control (histamine, 10mg/ml), a negative control ( glycerinated solu-tion). The results have been interpreted as coded by the European Academy of Allergology and Clinical Immunology (EAACI), subcommission “Standardi-zation of the allergens and Skin Test”. The test was considered positive if the mean wheal diameter was
����������������������������������������������������������������
���� ����
Patients 230 420
���
Males 103 (44.8) 188 (44.8%)
females 127 (55.2%) 232 (55.2%)
Mean age 33.28 35.24
��������������
Negative 94 (40.9%) 213 (50.7%)
Positive 136 (59.1%) 207 (49.3%)
��������
Rhinitis 192 (83.5%) 380 (90.5%)
Conjunctivitis 134 (58.3%) 250 (59.5%)
Asthma 55 (23.9%) 82 (19.5%)
������
April-June 50 (21.7%) 65 (15.5%)
January-June 19 (8.3%) 57 (13.6%)
January- March 15 (6.5%) 114 (27.1%)
Perennial 146 (63.5%) 184 (43.8%)
Pollinosis 160 350
Allergic to cypress 66 (41.3%) 275 (78.6%)
Allergic to parietaria 46 (28.8%) 85 (24.3%)
Allergic to graminaceae 64 (40%) 120 (34.3%)
Allergic to olive tree 56(35%) 116 (33.1%)
Table I - General Characteristics Of The Two Patient Populations
Statistical evaluation and parameters of phlogosis in patients sensitized to cypress
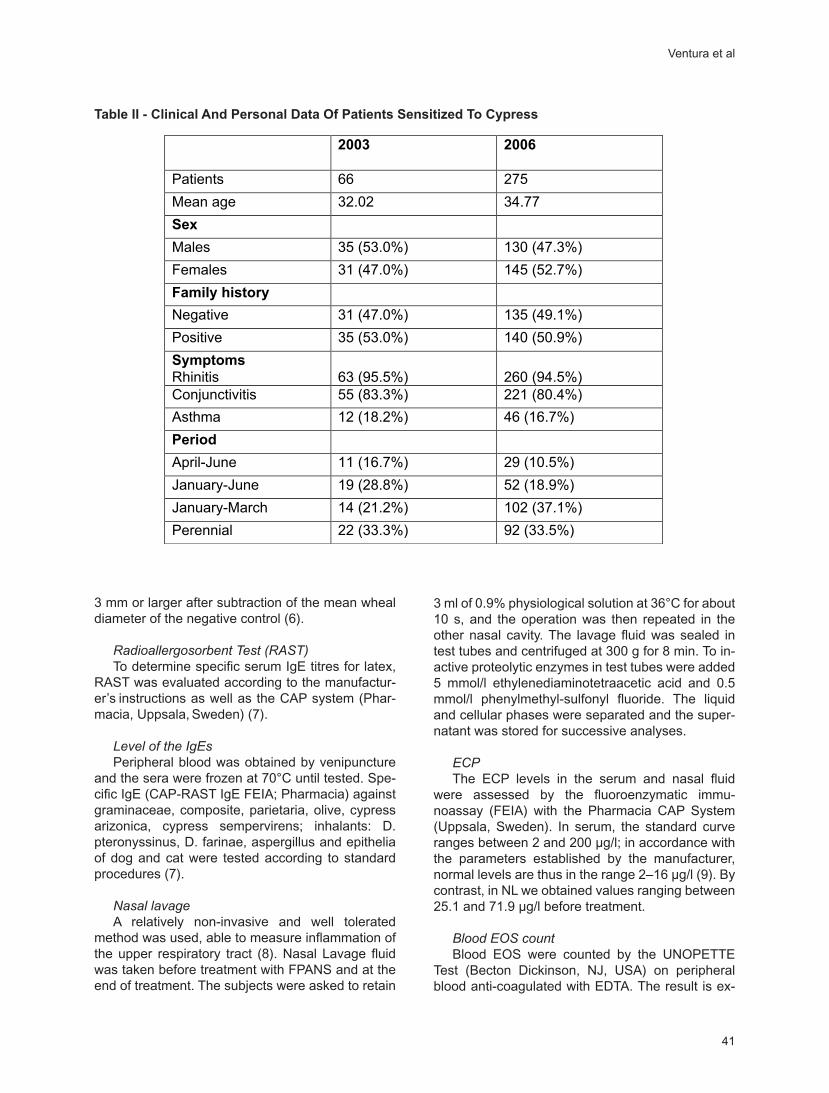
41
3 mm or larger after subtraction of the mean wheal diameter of the negative control (6).
Radioallergosorbent Test (RAST)To determine specific serum IgE titres for latex,
RAST was evaluated according to the manufactur-er’s instructions as well as the CAP system (Phar-macia, Uppsala, Sweden) (7).
Level of the IgEs Peripheral blood was obtained by venipuncture
and the sera were frozen at 70°C until tested. Spe-cific IgE (CAP-RAST IgE FEIA; Pharmacia) against graminaceae, composite, parietaria, olive, cypress arizonica, cypress sempervirens; inhalants: D. pteronyssinus, D. farinae, aspergillus and epithelia of dog and cat were tested according to standard procedures (7).
Nasal lavage A relatively non-invasive and well tolerated
method was used, able to measure inflammation of the upper respiratory tract (8). Nasal Lavage fluid was taken before treatment with FPANS and at the end of treatment. The subjects were asked to retain
3 ml of 0.9% physiological solution at 36°C for about 10 s, and the operation was then repeated in the other nasal cavity. The lavage fluid was sealed in test tubes and centrifuged at 300 g for 8 min. To in-active proteolytic enzymes in test tubes were added 5 mmol/l ethylenediaminotetraacetic acid and 0.5 mmol/l phenylmethyl-sulfonyl fluoride. The liquid and cellular phases were separated and the super-natant was stored for successive analyses.
ECPThe ECP levels in the serum and nasal fluid
were assessed by the fluoroenzymatic immu-noassay (FEIA) with the Pharmacia CAP System (Uppsala, Sweden). In serum, the standard curve ranges between 2 and 200 µg/l; in accordance with the parameters established by the manufacturer, normal levels are thus in the range 2–16 µg/l (9). By contrast, in NL we obtained values ranging between 25.1 and 71.9 µg/l before treatment.
Blood EOS countBlood EOS were counted by the UNOPETTE
Test (Becton Dickinson, NJ, USA) on peripheral blood anti-coagulated with EDTA. The result is ex-
�����������������������������������������������������������������������
���� ����
Patients 66 275
Mean age 32.02 34.77
���
Males 35 (53.0%) 130 (47.3%)
Females 31 (47.0%) 145 (52.7%)
��������������
Negative 31 (47.0%) 135 (49.1%)
Positive 35 (53.0%) 140 (50.9%)
��������
Rhinitis 63 (95.5%) 260 (94.5%)
Conjunctivitis 55 (83.3%) 221 (80.4%)
Asthma 12 (18.2%) 46 (16.7%)
������
April-June 11 (16.7%) 29 (10.5%)
January-June 19 (28.8%) 52 (18.9%)
January-March 14 (21.2%) 102 (37.1%)
Perennial 22 (33.3%) 92 (33.5%)
Table II - Clinical And Personal Data Of Patients Sensitized To Cypress
Ventura et al
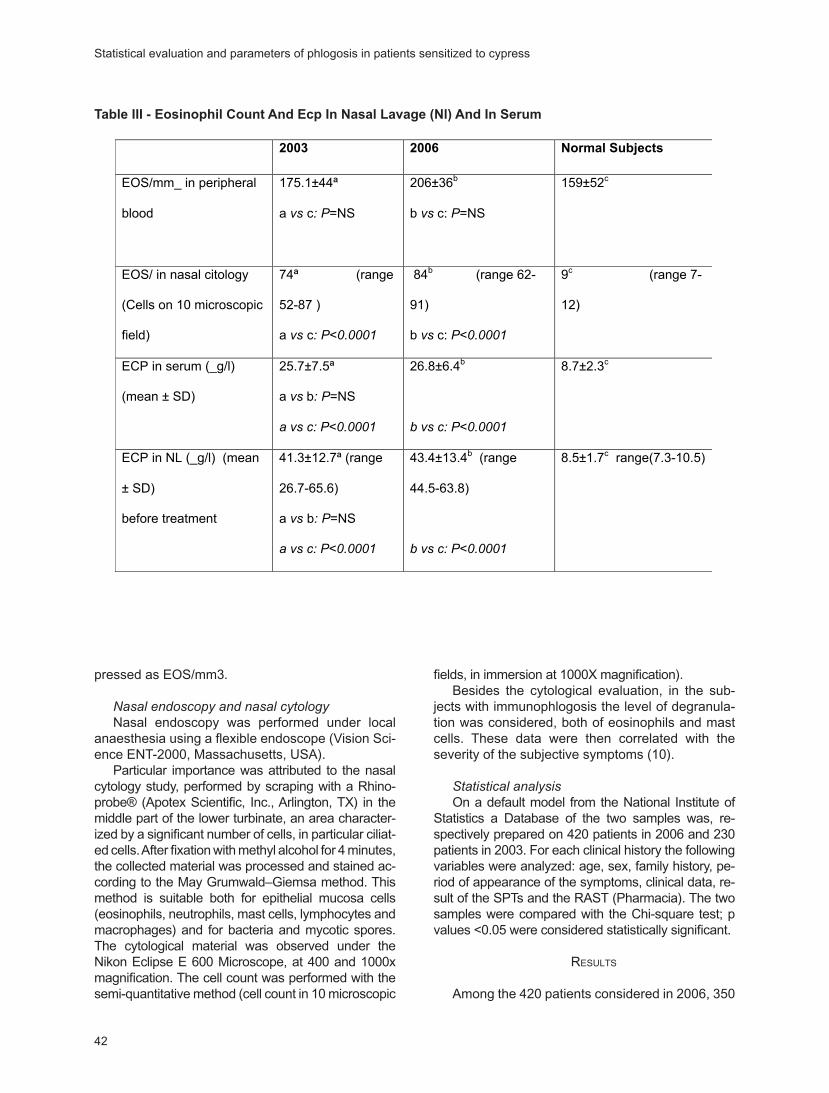
42
pressed as EOS/mm3.
Nasal endoscopy and nasal cytologyNasal endoscopy was performed under local
anaesthesia using a flexible endoscope (Vision Sci-ence ENT-2000, Massachusetts, USA).
Particular importance was attributed to the nasal cytology study, performed by scraping with a Rhino-probe® (Apotex Scientific, Inc., Arlington, TX) in the middle part of the lower turbinate, an area character-ized by a significant number of cells, in particular ciliat-ed cells. After fixation with methyl alcohol for 4 minutes, the collected material was processed and stained ac-cording to the May Grumwald–Giemsa method. This method is suitable both for epithelial mucosa cells (eosinophils, neutrophils, mast cells, lymphocytes and macrophages) and for bacteria and mycotic spores. The cytological material was observed under the Nikon Eclipse E 600 Microscope, at 400 and 1000x magnification. The cell count was performed with the semi-quantitative method (cell count in 10 microscopic
fields, in immersion at 1000X magnification). Besides the cytological evaluation, in the sub-
jects with immunophlogosis the level of degranula-tion was considered, both of eosinophils and mast cells. These data were then correlated with the severity of the subjective symptoms (10).
Statistical analysisOn a default model from the National Institute of
Statistics a Database of the two samples was, re-spectively prepared on 420 patients in 2006 and 230 patients in 2003. For each clinical history the following variables were analyzed: age, sex, family history, pe-riod of appearance of the symptoms, clinical data, re-sult of the SPTs and the RAST (Pharmacia). The two samples were compared with the Chi-square test; p values <0.05 were considered statistically significant.
RESULTS
Among the 420 patients considered in 2006, 350
����������������������������������������������������������������������
���� ���� ���������������
EOS/mm_ in peripheral
blood
175.1±44ª
a����c� �=NS
206±36b
b �� c: �=NS
159±52c
EOS/ in nasal citology
(Cells on 10 microscopic
field)
74ª (range
52-87 )
a����c� ��������
84b (range 62-
91)
b �� c: ��������
9c (range 7-
12)
ECP in serum (_g/l)
(mean ± SD)
25.7±7.5ª
a����b� �=NS
����������������
26.8±6.4b
����������������
8.7±2.3c
ECP in NL (_g/l) (mean
± SD)
before treatment
41.3±12.7ª (range
26.7-65.6)
a����b� �=NS
����������������
43.4±13.4b (range
44.5-63.8)
����������������
8.5±1.7c range(7.3-10.5)
Table III - Eosinophil Count And Ecp In Nasal Lavage (Nl) And In Serum
Statistical evaluation and parameters of phlogosis in patients sensitized to cypress
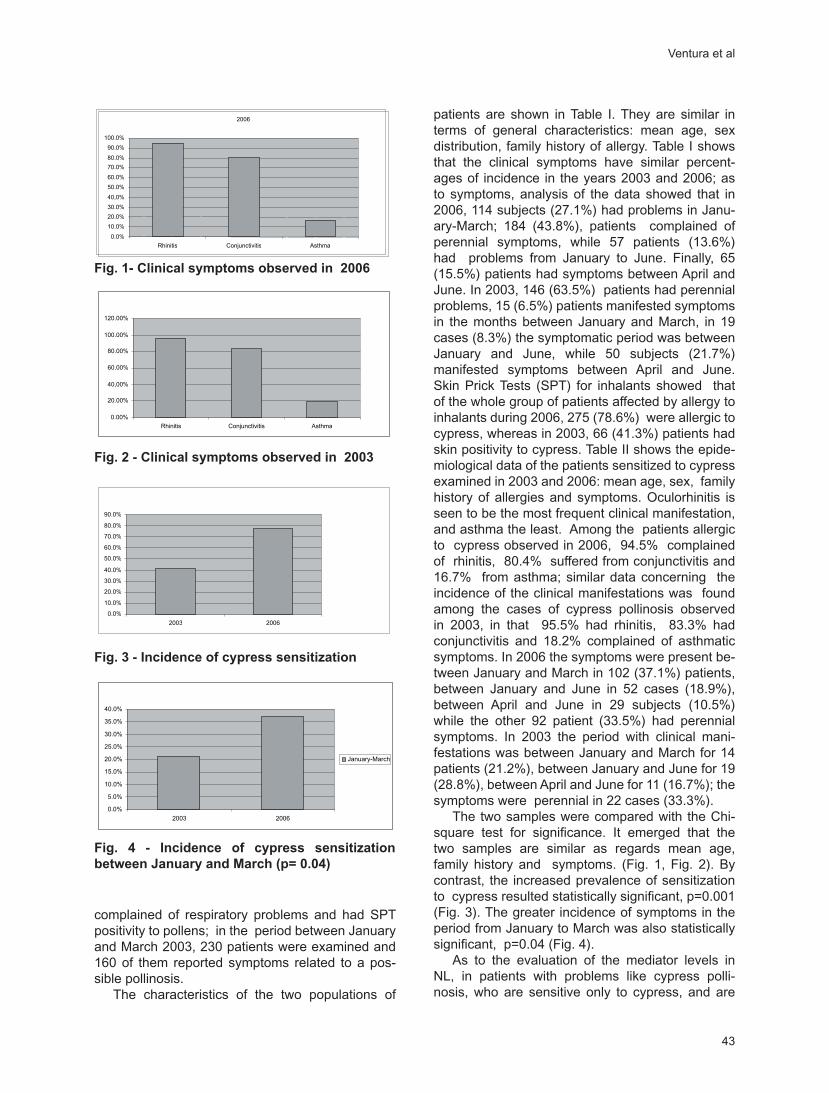
43
complained of respiratory problems and had SPT positivity to pollens; in the period between January and March 2003, 230 patients were examined and 160 of them reported symptoms related to a pos-sible pollinosis.
The characteristics of the two populations of
patients are shown in Table I. They are similar in terms of general characteristics: mean age, sex distribution, family history of allergy. Table I shows that the clinical symptoms have similar percent-ages of incidence in the years 2003 and 2006; as to symptoms, analysis of the data showed that in 2006, 114 subjects (27.1%) had problems in Janu-ary-March; 184 (43.8%), patients complained of perennial symptoms, while 57 patients (13.6%) had problems from January to June. Finally, 65 (15.5%) patients had symptoms between April and June. In 2003, 146 (63.5%) patients had perennial problems, 15 (6.5%) patients manifested symptoms in the months between January and March, in 19 cases (8.3%) the symptomatic period was between January and June, while 50 subjects (21.7%) manifested symptoms between April and June. Skin Prick Tests (SPT) for inhalants showed that of the whole group of patients affected by allergy to inhalants during 2006, 275 (78.6%) were allergic to cypress, whereas in 2003, 66 (41.3%) patients had skin positivity to cypress. Table II shows the epide-miological data of the patients sensitized to cypress examined in 2003 and 2006: mean age, sex, family history of allergies and symptoms. Oculorhinitis is seen to be the most frequent clinical manifestation, and asthma the least. Among the patients allergic to cypress observed in 2006, 94.5% complained of rhinitis, 80.4% suffered from conjunctivitis and 16.7% from asthma; similar data concerning the incidence of the clinical manifestations was found among the cases of cypress pollinosis observed in 2003, in that 95.5% had rhinitis, 83.3% had conjunctivitis and 18.2% complained of asthmatic symptoms. In 2006 the symptoms were present be-tween January and March in 102 (37.1%) patients, between January and June in 52 cases (18.9%), between April and June in 29 subjects (10.5%) while the other 92 patient (33.5%) had perennial symptoms. In 2003 the period with clinical mani-festations was between January and March for 14 patients (21.2%), between January and June for 19 (28.8%), between April and June for 11 (16.7%); the symptoms were perennial in 22 cases (33.3%).
The two samples were compared with the Chi-square test for significance. It emerged that the two samples are similar as regards mean age, family history and symptoms. (Fig. 1, Fig. 2). By contrast, the increased prevalence of sensitization to cypress resulted statistically significant, p=0.001 (Fig. 3). The greater incidence of symptoms in the period from January to March was also statistically significant, p=0.04 (Fig. 4).
As to the evaluation of the mediator levels in NL, in patients with problems like cypress polli-nosis, who are sensitive only to cypress, and are
�������������������������������������������
��������������������������������������������
�������������������������������������������
0.00%
20.00%
40,00%
60.00%
80.00%
100.00%
120.00%
Rhinitis Conjunctivitis Asthma
2006
0.0%
10.0%
20.0%
30.0%
40,0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Rhinitis Conjunctivitis Asthma
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
2003 2006
Fig. 1- Clinical symptoms observed in 2006
�������������������������������������������
��������������������������������������������
�������������������������������������������
0.00%
20.00%
40,00%
60.00%
80.00%
100.00%
120.00%
Rhinitis Conjunctivitis Asthma
2006
0.0%
10.0%
20.0%
30.0%
40,0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Rhinitis Conjunctivitis Asthma
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
2003 2006
Fig. 2 - Clinical symptoms observed in 2003
�������������������������������������������
��������������������������������������������
�������������������������������������������
0.00%
20.00%
40,00%
60.00%
80.00%
100.00%
120.00%
Rhinitis Conjunctivitis Asthma
2006
0.0%
10.0%
20.0%
30.0%
40,0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Rhinitis Conjunctivitis Asthma
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
2003 2006
Fig. 3 - Incidence of cypress sensitization
�������������������������������������������������������������������������������
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
2003 2006
January-March
Fig. 4 - Incidence of cypress sensitization between January and March (p= 0.04)
Ventura et al

44
not in treatment with specific immunotherapy, our data show higher values of ECP than the norm (P<0.0001), both in serum and NL. This was true in 2003 as well as in 2006. Evaluation of the na-sal cytology revealed increased eosinophils in the nasal secretion of patients sensitized to cypress (P<0.0001). The values in 2003 overlap those in 2006. By contrast, there were no statistical differ-ences in the values of EOS assessed in peripheral blood in patients evaluated in 2003 and 2006 when compared with normal subjects (Table III).
DISCUSSION
Pollinosis toward Cupressaceae in the last few years has acquired the importance of an “emergent” pollinosis (11). In countries with a Mediterranean climate the pollen of Cypress is the most common aeroallergen in the winter and at the beginning of spring. The Cupressus (C.) species is native to the oriental regions of the Mediterranean, but has now spread to Italy, where the most common species are C. sempervirens (common Cypress) and C. ari-zonica, used for reforestation, as a windbreak and often as ornamental plants (12). In the same family other species are also employed as urban green plants, such as C. Lawsonii, that is one of the most efficient for acoustic absorption and is therefore used to pose barriers against noise. The species Taxus and Juniperus are also the more allergenic of the Cupressaceae; this should be kept in mind when exotic species are imported for ornamental purposes such as Criptomeria japonica and some junipers from the American continent (Juniperus pinchottii and Juniperus ashei) with autumn and winter flowering (13). The greater spread of Cupres-saceae explains the reason for the increase of this allergy, unknown in Italy until about twenty years ago. Subsequently, it was known as “smaller polli-nosis” and today as “emergent pollinosis”. The season of cypress pollinosis is centred in winter but varies from species to species (14). In Italy it starts in January and ends in February for cy arizonica and in March or April for cy sempervirens (15). The flowering of C. arizonica, which goes from January to February, overlaps that of C. sempervirens, that goes from February to March, and represents the earlier marker of the beginning of the pollen season. In general the maximum pollination has shifted from mid-March to mid-February, and this seems to be correlated to progressive global warming. In the family of Cupressaceae the genus cupressus is of greater allergological interest, with 12 different spe-cies (16); the C. sempervirens and the C. arizonica are the most common species in Italy. In the sample of 2006, 275 patients of 420 patients with pollinosis
(65.5% of cases) had positive SPT to cypress; this prevalence is interesting because, according to the literature, the pollen of the Parietaria and the Olive Tree, in southern Italy, can be responsible for the high incidence of allergy in the population (17). Moreover, the increase of sensitization for Parietar-ia, graminacea and olive tree, as evaluated during these two years show a not significant variation. Comparing patients in 2003 and 2006, our study has underlined a statistically significant increase of sensitization to cypress (p=0.001). According to some Authors the increased prevalence of sensiti-zation to cypress could be attributed to two factors: 1) the increased use of Cupressaceae as ornamen-tal plants for reforestation, where the rapid growth of pre-existing trees would determine an increased release of pollen particles every year (18) 2) the in-teraction of cypress pollen with pollution particles (13, 17). However, an increase in the prevalence of SPT positivity to the pollens of Graminaceae, Pari-etaria and Olive Tree was not found, even though they are the most important pollens in our geo-graphical area (19). In our opinion, it is possible that these pollens, endowed with a greater allergenic power in comparison to those of cypress, have “ex-hausted” their abilities to increase the rate of sensi-tization on the basis of the degree of exposure, in the sense that when a plateau is reached, the limit-ing factor for the development of the allergic pheno-type might not be linked to exposure but exclusively to individual genetic factors or to other, different environmental factors (20) The interactions be-tween airborne particles and the different pollens or allergens with possibly greater local concentrations and presence could be important to justify the in-crease of sensitization to the pollen of cypress. Air-borne particles, pointed out as the most important pollutant for most cities in a 1996 United Nations document, consist of solid and liquid particles of dif-ferent size and origin, including soot, acids, sulfates and nitrates (21). More than 90% of the solid air-borne particles in the big cities derive from the com-bustion of gas-oil in diesel motors, now termed die-sel exhaust particles or DEPs (22). The reported morphological alterations of the pollen granules and the ability to bond with and transport allergens de-veloped by DEPs, could contribute to sensitisation to some allergens (23). Besides, being carried by liposoluble substances, allergens with an easier transepithelial penetration could also achieve a sort of accumulation at local level (24). The greater rate of sensitization to the pollen of cypress finds an echo in the historical study by Ishizaki of Critomeria japonica or Japanese cedar, shown to be more harmful in urban than rural areas, regardless of the degree of exposure (13). The pollens of cypress
Statistical evaluation and parameters of phlogosis in patients sensitized to cypress

45
and cedar could undergo analogous morphological alterations on interaction with airborne particles from car exhausts and their allergens. Also, the cross-reactivity among the greater allergens of the two conifers is well known due to their structural analogy and the presence of a glycosylated resi-due in Cry j1 (25). Another study demonstrated gly-cosylation of the allergenic elements of the extract of C. arizonica, thanks to their ability to bind differ-ent lectins(26). This further supports the hypothesis that Lol p1, a glycosylated protein, binds DEPs and not Lol p5 (not glycosylated), and that the allergens of cypress and Japanese cedar can have analo-gous relationships with the organic components of DEPs. In addition, respiratory disease, the winter peak of which coincides with that of cypress pollina-tion in particular, could contribute to bring on sensi-tization to cypress (27). The trend of the cypress pollen count for the period studied, kindly supplied by the Italian Association of Aerobiology (AIA), Monitoring Center of Brindisi 1, reveals increased amounts in the atmosphere of daily counts during the main pollen season in the first quarter of 2006 (about 264/m³ of air) in comparison with the first quarter of 2003 (about 201/m³ of air), that may ex-plain our observations. Another important factor is the volume and brittleness of the grain. In fact, the pollen of cypress is small and weak, and conse-quently could be subject to rupture and become the source of a particulate aerosol containing pollen al-lergens (28). This phenomenon was hypothesized by D’Amato et al to explain the increased asthma epidemics observed during thunderstorms (29). The Authors believe that osmotic shock and the conse-quent release of allergen-rich cytoplasmic frag-ments could explain this increase. In our case the small-sized, weak cypress grains could better pen-etrate the upper respiratory tract, causing more symptoms and hence increasing the number of al-lergic tests and diagnoses (30). No variation in the presentation of symptoms was observed in our study between 2003 and 2006. In fact, in both years rhinitis was the most frequent clinical mani-festation, followed by conjunctivitis and finally, asthma, all showing comparable percentages for the two years under study. An interesting point emerged from the comparison of the period of onset of the symptoms observed in the two samples. In fact, in 2006 37.1% of the subjects with sensitiza-tion to cypress had symptoms from January to March, whereas in 2003 only 21.2% of the sensi-tized patients suffered symptoms in this same peri-od. This significant difference points out an in-creased correlation between sensitization to cy-press and the referred clinical history. According to the pollen calendar, the cypress pollination season
starts in January and finishes in March. Neverthe-less, it should be borne in mind that each year the dates of maximum pollination can vary by one month, depending on climatic conditions. Different studies have underlined that the peak of maximum pollination has moved from mid-March to mid-Feb-ruary and this data can be correlated with progres-sive global warming. The pollen season of the Cu-pressaceae is inaugurated by C. arizonica, that is pollinated from January to February.
As to the evaluation of the ECP, in the group of 10 patients sensitized only to cypress this parameter is a good basis on which to control al-lergic inflammation, being more reliable than other parameters such as the number of eosinophils in peripheral blood (31). All 10 patients observed had higher levels of ECP, both in serum and NL. In ad-dition, in all cases there was an increased presence of eosinophils in the nasal secretion, but not in se-rum. The explanation for this phenomenon is that the level of the ECP indicates that of the allergic phlogosis, because it reflects a state of activation of the eosinophils that release ECP only when they are “activated” (32). In conclusion, in agreement with the data in literature, our study supports an increased sensitization to the pollen of cypress. Our data show that cypress pollen is responsible for res-piratory allergy in an increasing number of subjects and that periodic controls of the ECP can enable screening of the clinical conditions of the patient, as well as evaluation of the benefits of the planned therapies.
ACKNOWLEDGEMENTS
We thank Dott. Augusto Arsieni of the Italian As-sociation of Aerobiology (AIA) for the pollen count data furnished.
Reprint requests to:Mariateresa Ventura, M.D., Department of Internal Medicine, Immunology and Infectious Diseases (MIDIM),University of Bari, Policlinico, Piazza G. Cesare, 70124 Bari (Italy).Tel.++390805478793 Fax:++390805593007e-mail: [email protected]
REFERENCES
1. Tas J. Hay fever due to the pollen of cupressus sempervirens. Acta Allergol 1965; 53: 405-7.
2. Mari A, Di Felice G, Afferni C, Barletta B, Ting-hino R, Sallusto F, Pini C. Assessment of skin prick test and serum specific IgE detection in
Ventura et al
46
the diagnosis of Cupressaceae pollinosis. J Al-lergy Clin Immunol 196l; 98:21-31.
3. Italian Association of Aerobiology. An epide-miological survey of Cupressaceae pollenosis in Italy. J Investig Allergol Clin Immunol 2002; 12: 287-92.
4. D’Amato G, Lobefalo G. Allergenic pollens in the southern Mediterranean area. J. Allergy Clin Immunol 1989; 83:116-22.
5. Guerra F, Daza JC, Miguel R, Moreno C, Galan C, Dominguez E, Sanchez Guijo P. Sensitivity to Cupressus: allergenic significance in Cor-doba (Spain). J Investig Allergol Clin Immunol 1996; 6:117-20.
6. European Academy of Allergology and Clinical Immunology. Skin tests used in type I allergy test-ing Position paper. Allergy 1989; 44(S10):1-59.
7. Paganelli R, Ansotegui IJ, Sastre J, Lange CE, Roovers MH, de Groot H, Lindholm NB. Spe-cific IgE antibodies in the diagnosis of atopic disease. Clinical evaluation of a new in vitro test system, Uni-CAP, in six European allergy clinics. Allergy 1998; 53:763-8.
8. Naclerio RM, Proud D, Togias AG, Adkinson NF Jr, Meyers DA, Kagey-Sobotka A, Plaut M, Nor-man PS, Lichtenstein LM. Inflammatory media-tors in late antigen-induced rhinitis. N Engl J Med 1985; 313:65-70.
9. Venge P. Serum measurements of eosinophil cationic protein (ECP) in bronchial asthma. Clin Exp Allergy 1993; 23:3-7.
10. Meltzer EO, Orgel HA, Bronsky EA, et al. A dose-ranging study of fluticasone propionate aqueous nasal spray for seasonal allergic rhinitis assessed by symptoms, rhinomanom-etry and nasal cytology. J Allergy Clin Immunol 1990; 86:221-30.
11. Mari A, Di Felice G, Afferni C, Barletta B, Ting-hino R, Pini C. Cypress allergy: an underesti-mated pollinosis. Allergy 1997; 52:355-6.
12. Charpin D, Calleja M, Lahoz C, Pichot C, Wai-sel Y. Allergy to cypress pollen. Allergy 2005; 60:293-6.
13. Ishizaki T, Koizumi K, Ikemori R, Ishiyama Y, Kushibiki E. Studies of prevalence of Japa-nese cedar pollinosis among the residents in a densely cultivated area. Ann Allergy 1987; 58:265-71.
14. Raddi P, Morioka S, Underlie C. Cypress pol-len: botanic aspects in fourteen cypress spe-cies and prospects for research. All Immunol 2000; 32: 25.
15. Calleja M, Farrera I. Le cypress: un nouveau fléau pour la region Rhône-Alpes. All Immunol 2003; 35:92-6.
16. Gadek PA, Alpers DL, Heslewood MM, Quinn
CJ. Relationships within Cupressaceae sensu latu: a combined morphological and molecular approach. Am J Bot 2000; 87:1044-50.
17. Papa G, Romano A, Quaratino D, Di Fonso M, Viola M, Artesani MC, Sernia S, Di Gioacchino M, Venuti A. Prevalence of sensitization to Cu-pressus sempervirens: a 4-year retrospective study. Sci Total Environ 2001; 270:83.
18. Panzani R, Zerboni R, Ariano R. 1991. Al-lergenic significance of Cupressaceae pollen in some parts of the Mediterranean area. In: D’Amato G, Spieksma FThM, Bonini S, editors. Allergenic pollen and pollinosis in Europe. Ox-ford: Blackwell Scientific: p. 179-84.
19. Negrini AC. Allergenic pollens and pollinosis in Italy: recent advances. Allergy 1992; 47:371-9.
20. D’Amato G, Spieksma FT, Liccardi G, Jager S, Russo M, Kontou-Fili K, Nikkels H, Wuthrich B, Bonini S. Pollen-related allergy in Europe. Al-lergy 1998; 53:567-78.
21. Krämer U, Koch T, Ranft U, Ring J, Behrendt H. Traffic-related air pollution is associated with atopy in children living in urban areas. Epidemi-ology 2000; 11: 64-70.
22. Takenaka H, Zhang K, Diaz-Sanchez D, Tsien A, Saxon A. Enhanced human IgE production results from exposure to the aromatic hydro-carbons from diesel exhaust: direct effects on B-cell IgE Production. J Allergy Cin Immunol 1995; 95:103-15.
23. Diaz-Sanchez D, Tsien A, Fleming J, Saxon A. Combined diesel exhaust particulate and rag-weed allergen challenge markedly enhances human in vivo nasal ragweed-specific IgE and skews cytokine production to a T helper cell 2-type pattern. J Immunol 1997; 158:2406-13.
24. Riedl M, Diaz-Sanchez D. Biology of diesel ex-haust effects on respiratory function. J Allergy Cin Immunol 2005; 115:221-8.
25. Barletta B, Afferni C, Tinghino R, Mari A, Di Felice G, Pini C. Cross-reactivity between Cupressus arizonica and Cupressus semper-virens pollen extracts. J Allergy Cin Immunol 1996; 98:797-80.
26. Caiaffa MF, Macchia L, Strada S, Bariletto G, Scarpelli F, Tursi A. Airborne Cupressaceae pol-len in southern Italy. Ann Allergy 1993; 71:45-.
27. Zanolin ME, Pattaro C, Corsico A, Bugiani M, Carrozzi L, Casali L, Dallari R, Ferrari M, Mari-noni A, Migliore E, Olivieri M, Pirina P, Verlato G, Villani S, de Marco R for the ISAYA Study Group. The role of climate on the geographic variability of asthma, allergic rhinitis and respi-ratory symptoms: results from the Italian study of asthma in young adults. Allergy 2004; 59:306-9.
Statistical evaluation and parameters of phlogosis in patients sensitized to cypress
47
28. Taylor PE, Hagan R, Valenta R, Glovsky MM. Release of allergens in respirable aerosols: a link between grass pollen and asthma. J Allergy Clin Immunol 2002; 109:51-5.
29. D’Amato G, Liccardi G, Frenguelli G. Thunder-storm-asthma and pollen allergy. Allergy 2007; 62:11-15.
30. D’Amato G, Liccardi G, D’Amato M, Volgate S. Environmental risk factors and allergic bronchi-al asthma. Clin Exp Allergy 2005; 35:1113-7.
31. Ventura MT, Bruno LM, Iacobelli A, Tursi A. Eosinophils in allergic diseases: immunophar-macological regulation. Immunopharmacol Im-munotoxicol 1997; 19:405-9.
32. Ventura MT, Piccinni T, Matino MG, Giuliano G, Di Corato R, Di Napoli P, Tursi A. Retrospective study on fluticasone propinate aqueous nasal spray efficacy in patients with allergic rhinitis: evaluation of clinical and laboratory param-eters. Allergy 2001; 56:29-33.
Ventura et al