cadasil management or what to do when there is little one can do
TRANSCRIPT
197
Review
www.expert-reviews.com ISSN 1473-7175© 2009 Expert Reviews Ltd10.1586/14737175.9.2.197
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalop-athy (CADASIL) is a rare, autosomal dominant disease that plays a major role in here ditary strokes and vascular cognitive impairment [1,2]. Although little is known regarding its epidemiology, it has been reported that preva-lence of CADASIL in West Scotland is 1.98 per 100,000 adults, or 4.14 per 100,000 if also considering the predicted carriers of the mutation [3].
The CADASIL syndrome is an adult-onset systemic angiopathy, characterized by migraine with aura and recurrent lacunar strokes that leads to vascular cognitive impairment. CADASIL patients become unable to walk without assistance between 56 and 64 years of age, are bedridden between 59 and 69 years and die between 61 and 74 years of age [4]. The qual-ity of life of these patients is not only threatened by recurrent strokes, but also by other disabling symptoms, such as mood disorders, migraine and seizures [5,6].
The disease-causing mutations are located in the NOTCH3 gene, on the long arm of chro-mosome 19 [7]. This gene encodes a cytoplas-matic membrane receptor involved in cellular differentiation and cell cycle regulation [8]. This receptor is necessary for neuronal and vascular development during embryogenesis [9–11]. In adults, it only remains active on vascular smooth
muscle cells (VSMCs) and pericytes [12], which may be the primary cellular type involved in the syndrome.
Despite all the data collected during the past 10 years, the pathophysiology of CADASIL remains elusive. At present, there are three theo-ries attempting to explain the mechanism of the disease, yet none of them has shown conclusive evidence [13,14]. It is hard to develop an effective therapy against the disease when the underly-ing pathogenic mechanisms have not yet been identified. As a consequence, nowadays there is no useful treatment to cure CADASIL and we only have drugs to relieve the symptoms at our disposal [15].
The aims of this review are first to help physicians in the management of CADASIL patients, and second to introduce the clini-cians to the current biological knowledge on CADASIL syndrome.
PathophysiologyMutations associated with CADASIL cluster in the extracellular domain of Notch3 receptor, mostly in cysteine residues [16]. The mutated extracellular domain accumulates in the vicin-ity of VSMCs as granular osmiophilic mate-rial (GOM), which is the histologic pathog-nomonic hallmark of the disease [17,18]. In addition, VSMC and neuronal apoptosis have been seen by the terminal deoxynucleotidyl
Alberto del Río-Espínola*, Maite Mendióroz*, Sophie Domingues-Montanari, Patricia Pozo-Rosich, Esther Solé, Jessica Fernández-Morales, Israel Fernández-Cadenas and Joan Montaner†
†Author for correspondence Neurovascular Research Laboratory and Neurovascular Unit, Institut de Recerca, Hospital Vall d’Hebron, Pg Vall d’Hebron 119-129, 08035 Barcelona, Spain Tel.: +34 934 894 073 Fax: +34 934 894 102 [email protected] *Authors contributed equally to this work
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is a rare disease that leads to migraine, mood disorders, recurrent lacunar strokes and early vascular dementia. This autosomal-dominant condition is caused by mutations in the NOTCH3 gene and is characterized by degeneration of vascular smooth muscle cells. At present, no evidence-based treatment for CADASIL is available and only relief of symptoms can be offered to patients. This review focuses on an update of CADASIL management, based on the recent clinical and basic evidence, and discusses possible new treatment targets for CADASIL.
Keywords: CADASIL • notch3 • reactive oxygen species • sirtuin • stroke • vascular dementia • vascular smooth muscle cell
CADASIL management or what to do when there is little one can doExpert Rev. Neurother. 9(2), 197–210 (2009)

Expert Rev. Neurother. 9(2), (2009)198
Review del Río-Espínola, Mendióroz, Domingues-Montanari et al.
transferase-mediated dUTP–biotin nick end labeling method in brain tissue of autopsy cases [19–21]. Currently, there is no consensus about the relationship between both processes, GOM accumulation and apoptosis.
Classically, two theories have been proposed to explain how CADASIL mutations might influence receptor synthesis and function, leading to the development of the disease [13]:
The mutated receptor causes protein accumulation, and this •accumulation is cytotoxic, as with the β-amyloid protein accu-mulation in Alzheimer’s disease. Considering this theory, the main issue would be to prevent GOM formation that might take part in the disease course, and to clear those depositions;
The mutated receptor is not functional and, by an unknown •mechanism, the wild-type receptor also becomes useless. Fol-lowing this theory, the main point would be to recover pro-tein function. In this model, GOM accumulation is only a consequence of the disease.
Evidence has been raised against both theories, and they have been used as a proof of the alternative model. Moreover, in May 2007, a third theory was added based on a proteomic experi-ment with VSMC cultures [14]. Mutated cells were obtained from umbilical cord of a CADASIL mutation carrier and were compared with five controls.
The mutated receptor has an altered disulphide bond for-mation that disables its folding. This causes rough endoplas-mic reticulum stress, and this oxidative stress triggers VSMC apoptosis. A proportion of the mutated receptor can escape this cycle and is transferred to the cell membrane, but its clear-ance is diminished and leads to GOM accumulation. In this latter hypothesis, the main point would be to avoid oxidative stress of VSMC, and GOM would only be a consequence of the pathologic process.
Clinical manifestations & diagnosisSigns and symptoms of CADASIL are migraine (often with severe, long-lasting aura), lacunar strokes, mood disorders and vascular cognitive impairment [5,6]. Patients become seriously disabled and die in their 60s, mainly due to respiratory problems, similar to individuals suffering from dementia [4]. In a small but significant proportion of patients (9%), seizures are also present [22–25].
On MRI, there is prominent leukoaraiosis usually affecting the external capsule and the anterior temporal pole. Brain MRI appears clearly affected after the age of 35 years, which is a good marker for CADASIL suspicion [26]. Lacunar infarcts are located in the external capsule, basal ganglia and anterior temporal pole, whereas the corpus callosum and most infratentorial regions (except the pons) are spared [27]. Microhemorrhages are found in the thalamus, basal ganglia, cortical–subcortical junction and deep structures. Their prevalence and main location varies between the examined cohorts [28–30].
There are several infrequent clinical features: intracerebral hemor rhages [31–33], encephalopathy [34–38], mental retardation [39–41] and, finally, retinal and optic nerve abnormalities, which may be due to irrigation deficiency [38,42–44].
Other signs have also been reported, such as multiple simul-taneous strokes [45], cortical infarct [46], cerebellar stroke [47], spinal cord infarcts [48], Virchow–Robin spaces dilation [49], arteriovenous malformations and aneurysms [50]. Regarding dermatological signs, generalized erythematous macules and patches [51], and varicose veins [52] have been referred. There are also documented movement disorders: parkinsonism, including progressive supranuclear palsy [53], and facial dystonia [54]. This latter group of signs and symptoms has been documented only in a single family, and their implication in CADASIL phenotype needs to be proven.
Several reports have been published showing the presence of oligoclonal bands and complement factor B in the cerebrospinal fluid, both characteristics of multiple sclerosis [55,56]. However, no relationship between CADASIL and multiple sclerosis has been demonstrated [57]. Conversely, anticipation phenomenon, or earlier onset in succeeding generations, may also be present in CADASIL [25,58].
When physicians detect patients highly suggestive of CADASIL, three diagnostic tests can be considered:
Genetic testing, either by direct sequencing or denaturing •HPLC of the 2–24 exons of the NOTCH3 gene. It only requires a blood sample and, thus, is the most comfortable test for the patient [59];
Immunohistochemistry in small vessels of a skin biopsy sample, •with a monoclonal antibody against the extracellular domain of the Notch3 receptor [12,60];
Electron microscopy in the same skin biopsy sample to assess •GOM accumulation directly [61].
These three tests are the main tools to reach a diagnosis, and could be combined to optimize the process. Genetic testing is the gold standard when the complete gene is studied, because it has a sensitivity and specificity very close to 100%, but it is time- and money-consuming. The usual solution is to reduce the number of exons studied, but that decreases test sensitivity; although a sensitivity of 95% can be obtained by sequencing 23 of the 33 exons of the NOTCH gene [60]. The antibody has been proven to be highly effective, with sensitivity up to 90%, but not complete specificity, which is approximately 98% [12,60]. In a disease with such a low prevalence, it could be used only as a complementary or first-step test. Electron microscopy has high specificity (100%) but its sensitivity is low (57%) [62]. However, sensitivity varies depending on the number of vessels examined. Thus, it could be used as a confirmative test (Table 1).
In our center, we start with genetic testing of the exons where mutations are found more frequently. This is because of the minor invasiveness when compared with skin biopsy; because, if the pathogenic mutation is found, family members could be studied as well; and because it offers the best sensitivity, which is mandatory in any screening test.
If the result of testing these frequent mutated exons is nega-tive, then skin biopsy for electronic microscopy and immuno-histochemistry tests are considered. When both tests are negative,
www.expert-reviews.com 199
Review
Mild stage Moderate stage Severe stage
Vascular dementia
20 30 40 50 60 70Age(years)
Migraine with aura
Mood disorders
Lacunar strokes
Update of CADASIL management
we consider studying exon 25 of NOTCH3, involved in another small-vessel disease different from CADASIL, but affecting the same gene [63]. Owing to its low sensitivity, detection of GOM by electronic microscopy is only useful when positive and it is difficult to study patients’ relatives. If GOM are not found, CADASIL cannot be ruled out. On the contrary, when immunohisto chemistry is positive, it is highly probable that the patient is affected, but this should be proved by sequencing the rest of the gene to find the pathogenic mutation. If not found, an option might be to study NOTCH3 at the mRNA level to detect expression changes or possible midintronic mutations that modify the splicing process, although the mutant allele might not be detected.
When CADASIL diagnosis is reached, a neurological exami-nation, psychometric evaluation and brain MRI, including T2-weighted, fluid attenuated inversion recovery and gradi-ent echo sequences, are recommended. At this point, all cur-rent medication and adjuvant treatments should be reconsid-ered. Unfortunately, there is no evidence-based treatment for CADASIL, but symptoms can be relieved following general treat-ment recommendations. In addition, some drugs or proceedings should be avoided (Table 2).
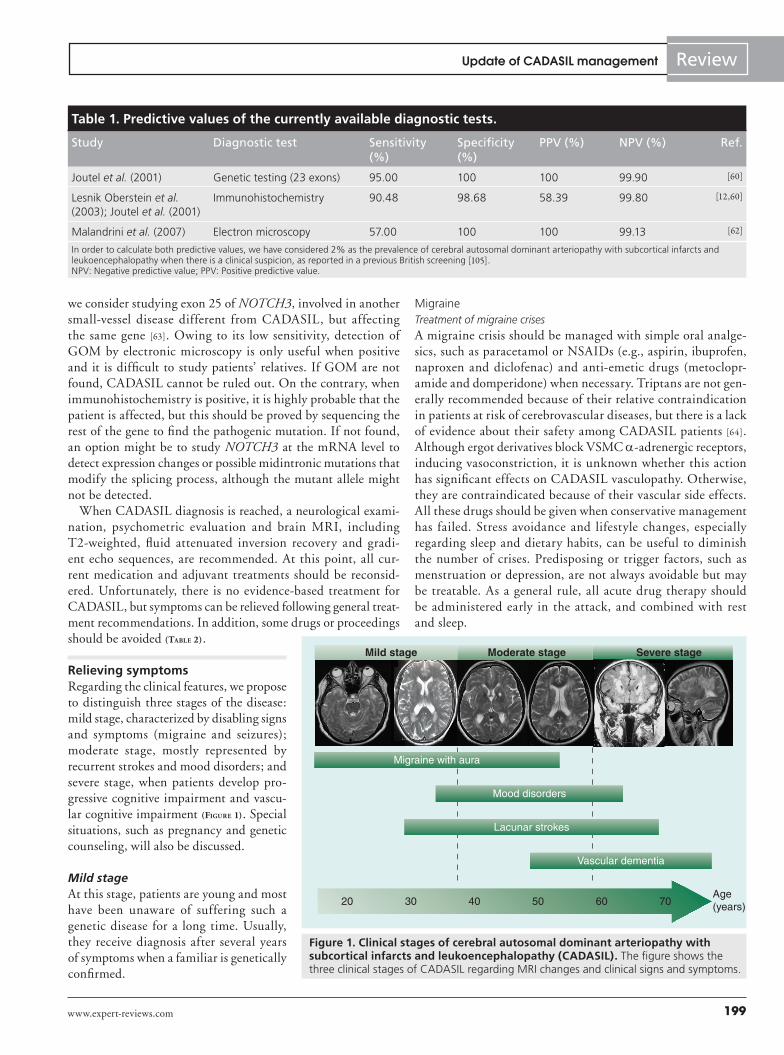
Relieving symptomsRegarding the clinical features, we propose to distinguish three stages of the disease: mild stage, characterized by disabling signs and symptoms (migraine and seizures); moderate stage, mostly represented by recurrent strokes and mood disorders; and severe stage, when patients develop pro-gressive cognitive impairment and vascu-lar cognitive impairment (Figure 1). Special situations, such as pregnancy and genetic counseling, will also be discussed.
Mild stageAt this stage, patients are young and most have been unaware of suffering such a genetic disease for a long time. Usually, they receive diagnosis after several years of symptoms when a familiar is genetically confirmed.
MigraineTreatment of migraine crisesA migraine crisis should be managed with simple oral analge-sics, such as paracetamol or NSAIDs (e.g., aspirin, ibuprofen, naproxen and diclofenac) and anti-emetic drugs (metoclopr-amide and domperidone) when necessary. Triptans are not gen-erally recommended because of their relative contraindication in patients at risk of cerebrovascular diseases, but there is a lack of evidence about their safety among CADASIL patients [64]. Although ergot derivatives block VSMC α-adrenergic receptors, inducing vasoconstriction, it is unknown whether this action has significant effects on CADASIL vasculopathy. Otherwise, they are contraindicated because of their vascular side effects. All these drugs should be given when conservative management has failed. Stress avoidance and lifestyle changes, especially regarding sleep and dietary habits, can be useful to diminish the number of crises. Predisposing or trigger factors, such as menstruation or depression, are not always avoidable but may be treatable. As a general rule, all acute drug therapy should be administered early in the attack, and combined with rest and sleep.
Table 1. Predictive values of the currently available diagnostic tests.
Study Diagnostic test Sensitivity (%)
Specificity (%)
PPV (%) NPV (%) Ref.
Joutel et al. (2001) Genetic testing (23 exons) 95.00 100 100 99.90 [60]
Lesnik Oberstein et al. (2003); Joutel et al. (2001)
Immunohistochemistry 90.48 98.68 58.39 99.80 [12,60]
Malandrini et al. (2007) Electron microscopy 57.00 100 100 99.13 [62]
In order to calculate both predictive values, we have considered 2% as the prevalence of cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy when there is a clinical suspicion, as reported in a previous British screening [105]. NPV: Negative predictive value; PPV: Positive predictive value.
Figure 1. Clinical stages of cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL). The figure shows the three clinical stages of CADASIL regarding MRI changes and clinical signs and symptoms.

Expert Rev. Neurother. 9(2), (2009)200
Review del Río-Espínola, Mendióroz, Domingues-Montanari et al.
Migraine prophylaxisProphylactic drugs can be considered to reduce the number of attacks or when there is inadequate symptom control or long-lasting aura, as in the general migraine population [201]. Well-known first-line prophylactic treatments, such as β-blockers [65], flunarizine [66], amitryptiline [67] and topiramate [68], should be used carefully because of their potential adverse effects on mood and cognition. Sodium valproate, a second-line option in general migraine patients [69], could be useful when epilepsy coexists, as well as the other antiepileptic drugs. Although evi-dence of efficacy is far from robust, gabapentin [70] is a good option owing to the safety profile of this drug. Moreover, selec-tive serotonin-reuptake inhibitors (SSRIs), although of uncertain value in preventing migraine crises [71], might be useful in those patients with concomitant mood disorders. It has been suggested that acetazolamide, a carbonic anhydrase inhibitor, might be a promising prophylatic treatment in CADASIL patients, probably by increasing cerebral perfusion to oligemic cortical areas [72]. Acetazolamide infusion induces a significant increase in cerebral perfusion, even within areas with impaired cerebral vasoreactiv-ity in CADASIL patients, especially in the cortex [73]. Specific studies are necessary to prove its efficacy in these patients. Before any treatment, patients should be advised to maintain a regular lifestyle, with regular sleep, meals, exercise and management of stress, perhaps through relaxation techniques. Even though the
Table 2. Allowed and contraindicated drugs for cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy.
Recommended Not recommended
Migraine attack
Simple oral analgesics• Aspirin 500 mg/8 h*
• Ibuprofen 400–600 mg/8 h*
• Naproxen 750 mg/12 h*
• Diclofenac 50 mg/12 h• Paracetamol 500–1000 mg/8 h*‡
± Antiemetic• Metoclopramide 10 mg• Domperidone 20 mg
Triptans: vascular riskErgot derivatives: vascular risk
Migraine prophylaxis
β-blockers§
• Atenolol 25–100 mg daily• Metoprolol 50–100 mg daily• Propanolol 80–160 mg daily‡
• Bisoprolol 5–10 mg dailyAmitryptiline 10–150 mg daily§¶
Flunarizine 2.5–5 mg daily§
Topiramate 25–50 mg daily§#
Sodium valproate 300–1000 mg dailyGabapentin 300–800 mg daily#
Selective serotonin-reuptake inhibitors• Fluoxetine 20 mg daily¶ Acetazolamide 125–250 mg daily**
Mood disorders (depression)
Selective serotonin-reuptake inhibitors• Fluoxetine 20–40 mg daily‡‡
• Citalopram 20 mg daily• Paroxetine 20 mg daily• Sertraline 50 mg daily
Ischemic stroke
Secondary prevention• Aspirin 50–325 mg daily• Clopidogrel 75 mg daily• Aspirin 50–325 mg (once daily) plus extended-release dipyridamole 200 mg (twice daily)Atorvastatin 80 mg daily
Angiography: risk for strokeAnticoagulants: risk for brain bleeding
Vascular dementia
Cholinesterase inhibitors • Donepezil 5–10 mg daily§§ [88]
• Rivastigmine 6–12 mg twice daily¶
• Galantamine 8 mg twice daily¶¶
Memantine 5–10 mg twice daily¶¶
Table 2. Allowed and contraindicated drugs for cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy.
Recommended Not recommended
Pregnancy
Preeclampsia• l-arginine (20g/500 ml intravenously daily for 5 days followed by 4 g/day orally for 2 weeks)¶¶
Migraine • Paracetamol 500–1000 mg /8 h (FDA, class B)• Metoprolol 50–100 mg daily (FDA, class B)• Fluoxetine 20 mg daily (FDA, class B) • Sertraline 50 mg daily (FDA, class B)• Magnesium (trimagnesium dicitrate) 600 mg dailyStroke• Clopidogrel 75 mg daily (FDA, class B)## • Enoxaparin/fraxiparine (FDA, class B)
Aspirin (FDA, class D)is not recommended, mainly during the third trimester
*Contraindicated under antiplatelet treatment. ‡Safe during pregnancy (FDA, class B). §Advisable to follow mood side effects. ¶Recommended when migraine coexists with depression. #Recommended when migraine coexists with epilepsy. **Possible future therapy. ‡‡May improve pseudobulbar syndrome symptoms. §§Improves some executive functions.¶¶Possibly useful but more evidence is necessary. ##More evidence is necessary regarding safety.

www.expert-reviews.com 201
ReviewUpdate of CADASIL management
efficacy of magnesium, riboflavin and coenzyme Q10 are low at best, their safety profile makes them alternative treatment options, as in general migraine patients [66].
Moderate stageMost CADASIL patients are diagnosed in this phase, when they present with lacunar strokes usually without vascular risk factors. At this moment, we should focus on preventing recurrent strokes to reduce the disease progression.
Stroke: acute managementAs mentioned earlier, transient ischemic attacks and strokes are found in approximately 85% of CADASIL patients [74], usually as typical classic lacunar syndromes with high recurrence rates, leading to severe disability. There is no drug tested in acute stroke in CADASIL patients and, as a rule, we treat them as we do the general stroke population. Since CADASIL is a small-vessel dis-ease, patients do not usually benefit from recanalization therapy, but tissue plasminogen activator should be administered when patients meet the criteria. Although rare, strokes involving a ter-ritory of a large vessel have also been described [46]. In these cases, a complete ultrasound examination of cervical and intracranial arteries is required, as well as a cardiac and aortic arch examina-tion looking for a source of emboli. An interesting point is that angiography is contraindicated in CADASIL patients, since it may provoke strokes [75].
Stroke preventive therapyAt primary prevention level, no evidence-based measures have been tested in order to prevent strokes in asymptomatic CADASIL patients. Since smoking increases the risk of stroke in patients with CADASIL, this habit should be avoided [76]. Different stud-ies suggest that progression of CADASIL is faster in patients who also have increased blood pressure [77–79]. Nevertheless, there is a lack of data regarding the effect of antihypertensive drug intake on disease progression.
These patients have an age-related increased risk of intra-cerebral microbleeds [30]. Even though aspirin-associated intra-cerebral hemorrhage has been reported [80], further research is needed to determine if the presence of microbleeds and use of anti-thrombotics may be associated with intracerebral hemor-rhage in patients with CADASIL. Conversely, whether antiplate-lets are effective for the secondary prevention of stroke is not well known, and specific trials are necessary. Meanwhile, following general recommendations of stroke management guidelines, low- or medium-dose aspirin (50–325 mg) can be useful in sec-ondary prevention of ischemic cerebrovascular events, as well as clopidogrel or the combination of aspirin and extended-release dypiridamole. Moreover, triflusal, which seems to cause fewer bleeding complications than aspirin, is also an acceptable option for preventing recurrent stroke [81,82]. In the end, the selection of an antiplatelet agent should be individualized on the basis of patient risk-factor profiles and tolerance. By contrast, other anticoagulants are contraindicated in CADASIL, as they may provoke hemorrhagic events [30].
Although statins might have beneficial actions on the vascular system, Peters et al. found no significant improvement on cerebral vasoreactivity in 24 CADASIL subjects who were treated with up to 80 mg of atorvastatin for 8 weeks [83]. All the conditions and lifestyle characteristics identified as risk factors for stroke, such as high blood pressure, diabetes mellitus, high cholesterol, hyperhomocysteinemia, obesity, physical inactivity and heavy alcohol intake, should be strictly controlled.
Stroke rehabilitationAfter an acute stroke, CADASIL patients should receive multi-disciplinary early active rehabilitation, providing the patient is clinically stable. Rehabilitation should be continued as long as perceptible recovery is taking place. Physiotherapy and occupa-tional therapy might be helpful but the optimal mode of delivery is yet unclear [81].
Mood disordersNo studies have been performed to test the effects of different drugs in CADASIL-related mood disorders. However, it is widely known that SSRIs can be useful in depression, and SSRIs might have an additional benefit in modulating pseudobulbar syndrome [84]. Nevertheless, the use of SSRI remains controversial regard-ing the risk of both ischemic and hemorrhagic strokes. A higher risk of ischemic stroke has been recently described in patients currently taking SSRIs [85]. However, Swenson et al. performed a systematic review, that failed to find an association between SSRI intake and higher risk of adverse cardiovascular events, including stroke [86]. Recently, a case–control study has found no association between SSRI intake and increased risk of intracerebral hemor-rhage [87]. Further studies are needed to assess the cardiovascular risk of these drugs; meanwhile, they may be effective in improving depressive symptoms in CADASIL patients.
Severe stageBy this time, the patient is severely disabled and the therapy is focused on maintaining the cognitive status and trying to help patients to live with their handicaps.
Vascular cognitive impairment treatmentA double-blind, placebo-controlled trial evaluating the effi-cacy and safety of donepezil, a cholinesterase inhibitor, in 168 CADASIL patients with subcortical vascular cognitive impairment has been performed recently [88]. Although donepe-zil was not found to improve general cognition, it seems that this drug could improve some executive functions, such as processing speed and attention [89].
In addition, other cholinesterase inhibitors, such as rivastigmine and galantamine, might be valuable, since a cholinergic deficit has been reported in the brain and cerebrovascular fluid of patients with vascular cognitive impairment [21,90]. Posada et al. conducted an open pilot trial of galantamine in four CADASIL patients. Clinical improvement was achieved in one subject, stabilization was noticed in two and one patient was forced to retire because of the side effects [91]. The small sample size and the absence of a
Expert Rev. Neurother. 9(2), (2009)202
Review del Río-Espínola, Mendióroz, Domingues-Montanari et al.
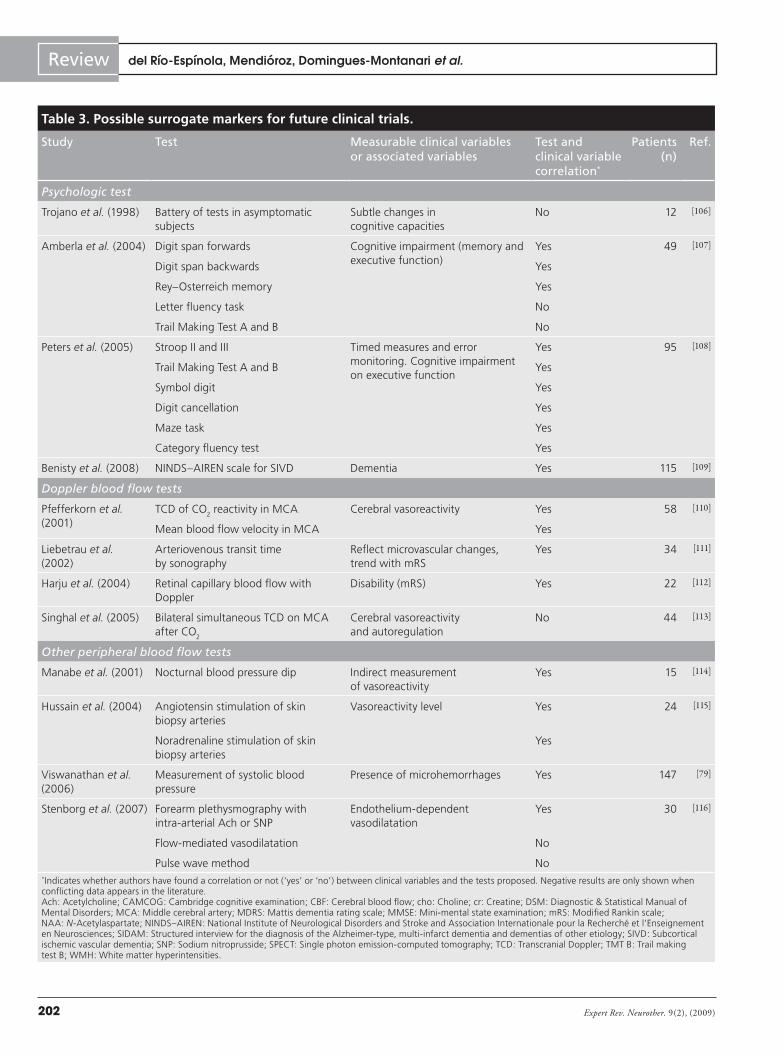
Table 3. Possible surrogate markers for future clinical trials.
Study Test Measurable clinical variables or associated variables
Test and clinical variable correlation*
Patients (n)
Ref.
Psychologic test
Trojano et al. (1998) Battery of tests in asymptomatic subjects
Subtle changes in cognitive capacities
No 12 [106]
Amberla et al. (2004) Digit span forwards Cognitive impairment (memory and executive function)
Yes 49 [107]
Digit span backwards Yes
Rey–Osterreich memory Yes
Letter fluency task No
Trail Making Test A and B No
Peters et al. (2005) Stroop II and III Timed measures and error monitoring. Cognitive impairment on executive function
Yes 95 [108]
Trail Making Test A and B Yes
Symbol digit Yes
Digit cancellation Yes
Maze task Yes
Category fluency test Yes
Benisty et al. (2008) NINDS–AIREN scale for SIVD Dementia Yes 115 [109]
Doppler blood flow tests
Pfefferkorn et al. (2001)
TCD of CO2 reactivity in MCA Cerebral vasoreactivity Yes 58 [110]
Mean blood flow velocity in MCA Yes
Liebetrau et al. (2002)
Arteriovenous transit time by sonography
Reflect microvascular changes, trend with mRS
Yes 34 [111]
Harju et al. (2004) Retinal capillary blood flow with Doppler
Disability (mRS) Yes 22 [112]
Singhal et al. (2005) Bilateral simultaneous TCD on MCA after CO
2
Cerebral vasoreactivity and autoregulation
No 44 [113]
Other peripheral blood flow tests
Manabe et al. (2001) Nocturnal blood pressure dip Indirect measurement of vasoreactivity
Yes 15 [114]
Hussain et al. (2004) Angiotensin stimulation of skin biopsy arteries
Vasoreactivity level Yes 24 [115]
Noradrenaline stimulation of skin biopsy arteries
Yes
Viswanathan et al. (2006)
Measurement of systolic blood pressure
Presence of microhemorrhages Yes 147 [79]
Stenborg et al. (2007) Forearm plethysmography with intra-arterial Ach or SNP
Endothelium-dependent vasodilatation
Yes 30 [116]
Flow-mediated vasodilatation No
Pulse wave method No*Indicates whether authors have found a correlation or not (‘yes’ or ‘no’) between clinical variables and the tests proposed. Negative results are only shown when conflicting data appears in the literature. Ach: Acetylcholine; CAMCOG: Cambridge cognitive examination; CBF: Cerebral blood flow; cho: Choline; cr: Creatine; DSM: Diagnostic & Statistical Manual of Mental Disorders; MCA: Middle cerebral artery; MDRS: Mattis dementia rating scale; MMSE: Mini-mental state examination; mRS: Modified Rankin scale; NAA: N-Acetylaspartate; NINDS–AIREN: National Institute of Neurological Disorders and Stroke and Association Internationale pour la Recherché et l’Enseignement en Neurosciences; SIDAM: Structured interview for the diagnosis of the Alzheimer-type, multi-infarct dementia and dementias of other etiology; SIVD: Subcortical ischemic vascular dementia; SNP: Sodium nitroprusside; SPECT: Single photon emission-computed tomography; TCD: Transcranial Doppler; TMT B: Trail making test B; WMH: White matter hyperintensities.
www.expert-reviews.com 203
ReviewUpdate of CADASIL management
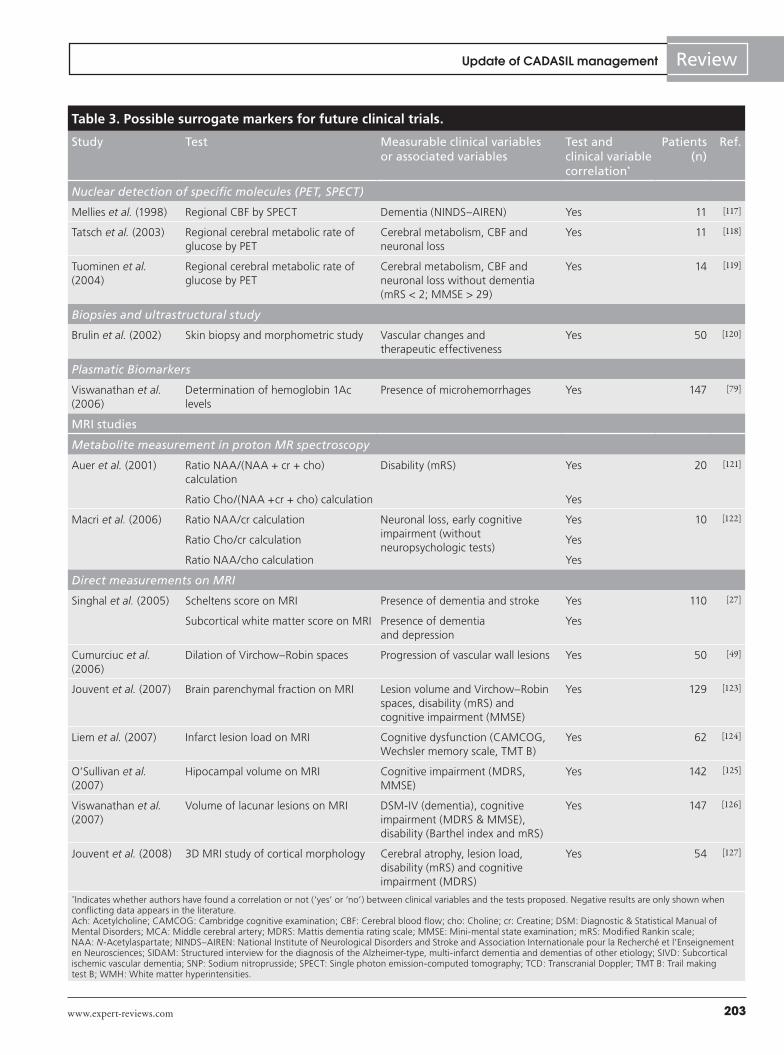
Table 3. Possible surrogate markers for future clinical trials.
Study Test Measurable clinical variables or associated variables
Test and clinical variable correlation*
Patients (n)
Ref.
Nuclear detection of specific molecules (PET, SPECT)
Mellies et al. (1998) Regional CBF by SPECT Dementia (NINDS–AIREN) Yes 11 [117]
Tatsch et al. (2003) Regional cerebral metabolic rate of glucose by PET
Cerebral metabolism, CBF and neuronal loss
Yes 11 [118]
Tuominen et al. (2004)
Regional cerebral metabolic rate of glucose by PET
Cerebral metabolism, CBF and neuronal loss without dementia (mRS < 2; MMSE > 29)
Yes 14 [119]
Biopsies and ultrastructural study
Brulin et al. (2002) Skin biopsy and morphometric study Vascular changes and therapeutic effectiveness
Yes 50 [120]
Plasmatic Biomarkers
Viswanathan et al. (2006)
Determination of hemoglobin 1Ac levels
Presence of microhemorrhages Yes 147 [79]
MRI studies
Metabolite measurement in proton MR spectroscopy
Auer et al. (2001) Ratio NAA/(NAA + cr + cho) calculation
Disability (mRS) Yes 20 [121]
Ratio Cho/(NAA +cr + cho) calculation Yes
Macri et al. (2006) Ratio NAA/cr calculation Neuronal loss, early cognitive impairment (without neuropsychologic tests)
Yes 10 [122]
Ratio Cho/cr calculation Yes
Ratio NAA/cho calculation Yes
Direct measurements on MRI
Singhal et al. (2005) Scheltens score on MRI Presence of dementia and stroke Yes 110 [27]
Subcortical white matter score on MRI Presence of dementia and depression
Yes
Cumurciuc et al. (2006)
Dilation of Virchow–Robin spaces Progression of vascular wall lesions Yes 50 [49]
Jouvent et al. (2007) Brain parenchymal fraction on MRI Lesion volume and Virchow–Robin spaces, disability (mRS) and cognitive impairment (MMSE)
Yes 129 [123]
Liem et al. (2007) Infarct lesion load on MRI Cognitive dysfunction (CAMCOG, Wechsler memory scale, TMT B)
Yes 62 [124]
O’Sullivan et al. (2007)
Hipocampal volume on MRI Cognitive impairment (MDRS, MMSE)
Yes 142 [125]
Viswanathan et al. (2007)
Volume of lacunar lesions on MRI DSM-IV (dementia), cognitive impairment (MDRS & MMSE), disability (Barthel index and mRS)
Yes 147 [126]
Jouvent et al. (2008) 3D MRI study of cortical morphology Cerebral atrophy, lesion load, disability (mRS) and cognitive impairment (MDRS)
Yes 54 [127]
*Indicates whether authors have found a correlation or not (‘yes’ or ‘no’) between clinical variables and the tests proposed. Negative results are only shown when conflicting data appears in the literature. Ach: Acetylcholine; CAMCOG: Cambridge cognitive examination; CBF: Cerebral blood flow; cho: Choline; cr: Creatine; DSM: Diagnostic & Statistical Manual of Mental Disorders; MCA: Middle cerebral artery; MDRS: Mattis dementia rating scale; MMSE: Mini-mental state examination; mRS: Modified Rankin scale; NAA: N-Acetylaspartate; NINDS–AIREN: National Institute of Neurological Disorders and Stroke and Association Internationale pour la Recherché et l’Enseignement en Neurosciences; SIDAM: Structured interview for the diagnosis of the Alzheimer-type, multi-infarct dementia and dementias of other etiology; SIVD: Subcortical ischemic vascular dementia; SNP: Sodium nitroprusside; SPECT: Single photon emission-computed tomography; TCD: Transcranial Doppler; TMT B: Trail making test B; WMH: White matter hyperintensities.
Expert Rev. Neurother. 9(2), (2009)204
Review del Río-Espínola, Mendióroz, Domingues-Montanari et al.
placebo group are serious limitations of this study, but this kind of assay may, at least, help us to increase the clinical experience with these patients.
Memantine, a low-affinity glutamate NMDA receptor antago-nist, might be a second-line option, since this drug has shown a small beneficial effect in moderate-to-severe Alzheimer’s disease. However, this effect on cognition was not clinically detectable in those with vascular cognitive impairment [92]; thus, we do not have enough evidence about this treatment. Finally, the choice of the pharmacologic agent should be based on tolerability, adverse-effect profile, ease of use and cost of medication [93]. Nevertheless, specific clinical trials should be carried out if we want to deter-mine the real efficacy of these drugs for improving cognition among CADASIL patients.
Supportive care (i.e., practical help, emotional support and counseling) is necessary for affected individuals and their fami-lies [202]. Although no specific group gives support to CADASIL patients, some foundations or associations may be quite helpful for
them, such as the Huntington’s Disease Society of America [203], the United Leukodystrophy Foundation [204] or the Alzheimer’s Association [205].
Other general measures in supporting individuals with demen-tia, such as avoiding pressure ulcer, gastrostomy or respiratory physiotherapy, ought to be considered when necessary.
PregnancyIn the general population, ischemic cerebrovascular complica-tions during gestation and puerperium are rare (8.1 per 100,000 pregnancies) [94]. Nevertheless, transient neurologic symptoms and preeclampsia appear to be common in CADASIL patients, particularly in women older than 30 years of age. Roine et al. reported data from a Finnish group of 39 CADASIL women who had been pregnant and found that preeclampsia was more frequent (10.3%) in CADASIL patients than in the general popu-lation (3–5%) [95,96]. In addition, in 15 of the 19 complicated pregnancies, neurological events appeared during puerperium
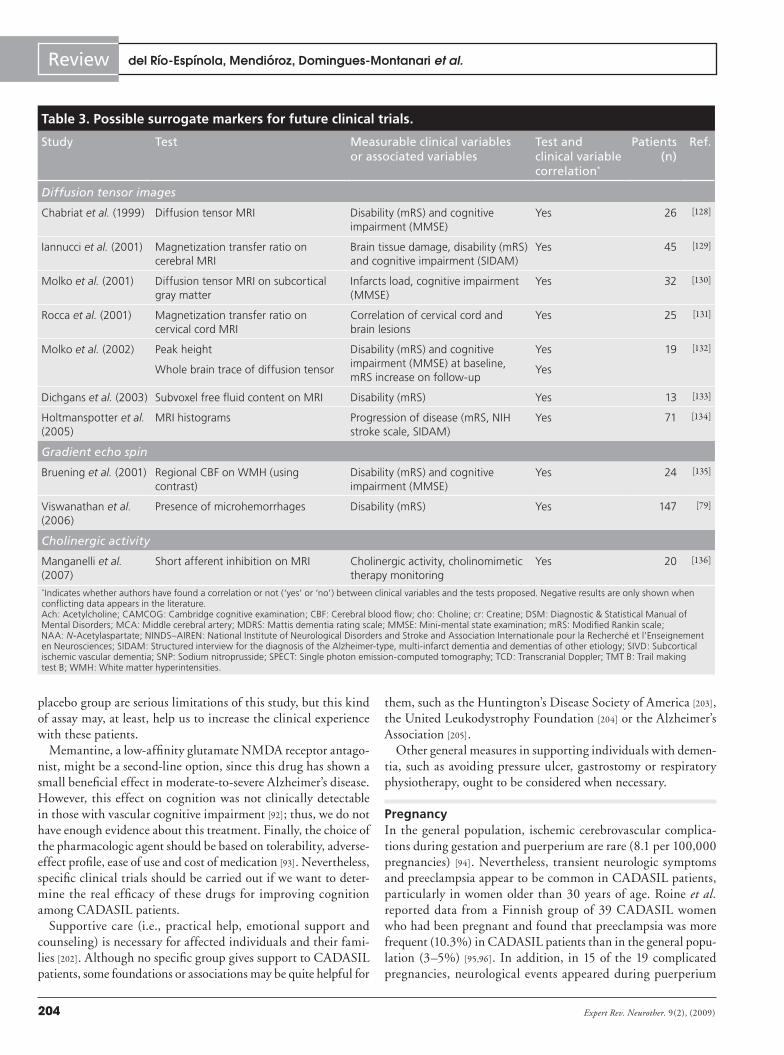
Table 3. Possible surrogate markers for future clinical trials.
Study Test Measurable clinical variables or associated variables
Test and clinical variable correlation*
Patients (n)
Ref.
Diffusion tensor images
Chabriat et al. (1999) Diffusion tensor MRI Disability (mRS) and cognitive impairment (MMSE)
Yes 26 [128]
Iannucci et al. (2001) Magnetization transfer ratio on cerebral MRI
Brain tissue damage, disability (mRS) and cognitive impairment (SIDAM)
Yes 45 [129]
Molko et al. (2001) Diffusion tensor MRI on subcortical gray matter
Infarcts load, cognitive impairment (MMSE)
Yes 32 [130]
Rocca et al. (2001) Magnetization transfer ratio on cervical cord MRI
Correlation of cervical cord and brain lesions
Yes 25 [131]
Molko et al. (2002) Peak height Disability (mRS) and cognitive impairment (MMSE) at baseline, mRS increase on follow-up
Yes 19 [132]
Whole brain trace of diffusion tensor Yes
Dichgans et al. (2003) Subvoxel free fluid content on MRI Disability (mRS) Yes 13 [133]
Holtmanspotter et al. (2005)
MRI histograms Progression of disease (mRS, NIH stroke scale, SIDAM)
Yes 71 [134]
Gradient echo spin
Bruening et al. (2001) Regional CBF on WMH (using contrast)
Disability (mRS) and cognitive impairment (MMSE)
Yes 24 [135]
Viswanathan et al. (2006)
Presence of microhemorrhages Disability (mRS) Yes 147 [79]
Cholinergic activity
Manganelli et al. (2007)
Short afferent inhibition on MRI Cholinergic activity, cholinomimetic therapy monitoring
Yes 20 [136]
*Indicates whether authors have found a correlation or not (‘yes’ or ‘no’) between clinical variables and the tests proposed. Negative results are only shown when conflicting data appears in the literature. Ach: Acetylcholine; CAMCOG: Cambridge cognitive examination; CBF: Cerebral blood flow; cho: Choline; cr: Creatine; DSM: Diagnostic & Statistical Manual of Mental Disorders; MCA: Middle cerebral artery; MDRS: Mattis dementia rating scale; MMSE: Mini-mental state examination; mRS: Modified Rankin scale; NAA: N-Acetylaspartate; NINDS–AIREN: National Institute of Neurological Disorders and Stroke and Association Internationale pour la Recherché et l’Enseignement en Neurosciences; SIDAM: Structured interview for the diagnosis of the Alzheimer-type, multi-infarct dementia and dementias of other etiology; SIVD: Subcortical ischemic vascular dementia; SNP: Sodium nitroprusside; SPECT: Single photon emission-computed tomography; TCD: Transcranial Doppler; TMT B: Trail making test B; WMH: White matter hyperintensities.

www.expert-reviews.com 205
ReviewUpdate of CADASIL management
and, in 82% of the symptomatic group, these symptoms were the first clinical manifestations of CADASIL. This higher incidence of preeclampsia is not surprising if we consider the pathogenic role of impaired cerebral hemodynamics and endothelial dys-function in CADASIL [97]. Peters et al. have recently described an enhanced l-arginine-induced vasoreactivity in CADASIL patients compared with controls, suggesting endothelial dys-function in CADASIL [97]. Interestingly, the authors suggest that, by enhancing vasodilatation, l-arginine may be a possible therapeutic approach for CADASIL. Nevertheless, a limiting factor could be headache, a frequent adverse effect associated with l-arginine treatment. In this sense, l-arginine supplementa-tion seems promising in reducing blood pressure in patients with gestational hypertension [98].
Even if migraine usually improves during pregnancy, some patients may need prophylactic treatment. In these cases, a β-blocker, metoprolol, is an acceptable first-line option as well as sertraline or fluoxetine (US FDA, class B). A good alterna-tive option in these patients is magnesium. Paracetamol is safe throughout pregnancy and may be useful to ameliorate acute migraine crisis. (FDA, class B). Regarding secondary preven-tion of stroke, it should be remembered that aspirin should be avoided in pregnant women during the first trimester (FDA, class D) because of its potentially teratogenic effect. Clopidogrel may be an alternative (FDA, class B) although more studies should be performed in order to determine the real teratogenic effect of this drug. Regardless, these pregnancies should be monitored carefully.
Genetic counselingPatients with CADASIL should receive proper disease and genetic information to help them make informed medical and personal decisions. Regarding asymptomatic individuals, it is advisable to follow the guidelines for presymptomatic testing for Huntington’s disease. An interview should be carried out in order to assess the possible impact of positive and negative test results; informed consent is necessary and records should be kept confidential. The recommended evaluation is molecular genetic testing.
During childhood, consensus holds that underaged individu-als should not be tested in the absence of symptoms, mainly to allow them to decide if they want this information, since predictive testing only provides the presence of mutation and is not useful in predicting either clinical onset or progression of the disease. The identification of effective primary prevention therapies might modify this statement. Nevertheless, symptom-atic individuals below 18 years of age usually benefit from having a specific diagnosis established.
While prenatal testing of adult-onset disorders is unusual, it is possible to perform a prenatal diagnosis of CADASIL [99]. When the disease-causing mutation has been previously identified in a family, DNA may be extracted from fetal cells obtained by amniocentesis or chorionic villus sampling to perform a molecular analysis. Furthermore, preimplantation genetic diagnosis may be considered as a reproductive option, since CADASIL a dominant, highly penetrant and potentially serious disease [100].
Expert commentary & five-year viewSince CADASIL is an orphan disease (very-low-prevalence illness) and since, according to market conditions, the pharma ceutical industry is reluctant to support research into drugs for rare dis-eases, an effective treatment for CADASIL is, thus, difficult to develop. Nevertheless, recent changes in national public-health programs, such as the Orphan Drugs strategy in the EU, raise hope for finding a helpful drug for these conditions.
Fortunately, research on CADASIL’s pathogenesis and bio-markers may contribute to new drug findings. Interestingly, Ihalainen et al. have identified 11 differentially expressed proteins, which are involved in protein degradation and fold-ing, contraction of VSMCs and cellular stress, in genetically genuine cultured human CADASIL VSMCs by proteomic analysis [14]. Some of these proteins might be a possible target for researchers developing new drugs. In addition, since endo-plasmic reticulum stress and increased reactive oxygen species (ROS) concentration seem to play a role in pathogenesis, drugs modulating or reversing these reactions underlying cell damage from oxidative stress, such as B(6)-vitamin-derived molecules
Key issues
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is an inherited small-vessel • disease manifesting as migraine with aura, mood disorders, recurrent lacunar strokes and vascular cognitive impairment.
CADASIL is diagnosed on the basis of skin biopsy and molecular genetic testing, but it may be overlooked or misdiagnosed.•
Migraine attacks can be aborted with simple analgesics, and triptans are generally not recommended because of their potential • vascular side effects.
Angiography is not recommended due to its high risk of cerebrovascular events in CADASIL patients.•
Regarding stroke prevention, anticoagulants are contraindicated owing to the risk of hemorrhagic stroke.•
l• -arginine, if tolerated, might be a promising treatment for enhancing cerebral vasodilatation.
Donepezil did not improve general cognition, but it could improve some executive functions, such as processing speed and attention.•
Pregnancies should be carefully followed in CADASIL women. Prenatal testing and preimplantational diagnosis are possible for families • in which the disease-causing mutations have been identified.
Resveratrol, a SIRT1 enhancer, appears to be a good candidate for testing in future clinical trials.•
Further clinical trials and basic research are necessary to improve evidence-based management in CADASIL patients.•

Expert Rev. Neurother. 9(2), (2009)206
Review del Río-Espínola, Mendióroz, Domingues-Montanari et al.
[101], appear to be promising future therapeutics in CADASIL disease. In the same way, increasing silent information regula-tor (SIRT)1 has been found to protect cells against amyloid-β-induced ROS production and DNA damage in Alzheimer’s disease, thereby reducing apoptotic death in vitro [102]. SIRT1 belongs to the sirtuins family, a new family of enzymes that regulate gene silencing, DNA repair, rDNA recombination and apoptosis, thus extending lifespan. Resveratrol, a polyphenolic SIRT1 activator, is considered to be a potential drug for the treatment of neurodegenerative [103] and metabolic diseases [104]; in fact, clinical trials in Type 2 diabetic patients are currently in progress. Hence, according to the third model attempting to explain CADASIL, in which ROS production plays a central role, resveratrol seems promising as a future CADASIL thera-peutic and further research will help to elucidate its efficacy in these patients.
Regarding diagnosis of CADASIL, it would be interesting to develop new tests in order to facilitate screening of the dis-ease. Finally, although it is highly difficult to recruit patients considering the low prevalence of rare diseases, clinical trials are mandatory to test effective drugs for CADASIL. Several
secondary end points have been assessed during the last few years (Table 3), which may be useful to increase sensitivity of the trials and reduce sample size and cost.
AcknowledgementThe authors would like to thank Anna Vilalta for help with manuscript preparation.
Financial & competing interests disclosureThis study was funded by the stroke research network (RENEVAS). A del Río-Espínola has a grant from the Vall d’Hebrón Research Institute; M Mendióroz is the recipient of a grant from the Instituto de Salud Carlos III for medical research training (FI05/00081); S Domingues-Montanari is the recipient of a grant from the Ramón Areces Fundation; P Pozo-Rosich has a grant for Post-Medical Sanitary Specialization (postMIR); and I Fernández-Cadenas has a post-doctoral research contract from RENEVAS. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
ReferencesPapers of special note have been highlighted as:•ofinterest••ofconsiderableinterest
Kalimo H, Ruchoux MM, Viitanen M, 1
Kalaria RN. CADASIL: a common form of hereditary arteriopathy causing brain infarcts and dementia. Brain Pathol. 12(3), 371–384 (2002).
Dotti MT, Federico A, Mazzei R2 et al. The spectrum of Notch3 mutations in 28 Italian CADASIL families. J. Neurol. Neurosurg. Psychiatry 76(5), 736–738 (2005).
Razvi SS, Davidson R, Bone I, Muir KW. 3
The prevalence of cerebral autosomal dominant arteriopathy with subcortical infarcts and leucoencephalopathy (CADASIL) in the west of Scotland. J. Neurol. Neurosurg. Psychiatry 76(5), 739–741 (2005).
Opherk C, Peters N, Herzog J, Luedtke R, 4
Dichgans M. Long-term prognosis and causes of death in CADASIL: a retrospective study in 411 patients. Brain 127(Pt 11), 2533–2539 (2004).
Davous P. The natural history of 5
CADASIL. Stroke 30(10), 2247 (1999).
Desmond DW, Moroney JT, Lynch T, 6
Chan S, Chin SS, Mohr JP. The natural history of CADASIL: a pooled analysis of previously published cases. Stroke 30(6), 1230–1233 (1999).
Joutel A, Corpechot C, Ducros A7 et al. Notch3 mutations in CADASIL, a hereditary adult-onset condition causing stroke and dementia. Nature 383(6602), 707–710 (1996).
Since •• Notch3 was identified as the responsible gene for cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) in 1996, little has been discovered regarding possible treatments for this disease.
Artavanis-Tsakonas S, Matsuno K, Fortini 8
ME. Notch signaling. Science 268(5208), 225–232 (1995).
Lindsell CE, Boulter J, DiSibio G, Gossler 9
A, Weinmaster G. Expression patterns of Jagged, Delta1, Notch1, Notch2, and Notch3 genes identify ligand-receptor pairs that may function in neural development. Mol. Cell. Neurosci. 8(1), 14–27 (1996).
Villa N, Walker L, Lindsell CE, Gasson J, 10
Iruela-Arispe ML, Weinmaster G. Vascular expression of Notch pathway receptors and ligands is restricted to arterial vessels. Mech. Dev. 108(1–2), 161–164 (2001).
Domenga V, Fardoux P, Lacombe P11 et al. Notch3 is required for arterial identity and maturation of vascular smooth muscle cells. Genes Dev. 18(22), 2730–2735 (2004).
Lesnik Oberstein SA, van Duinen SG, van 12
den Boom R et al. Evaluation of diagnostic NOTCH3 immunostaining in CADASIL. Acta Neuropathol. 106(2), 107–111 (2003).
Ihalainen S, Soliymani R, Iivanainen E13 et al. Proteome analysis of cultivated vascular smooth muscle cells from a CADASIL patient. Mol. Med. 13(5–6), 305–314 (2007).
Proteomic experiments have led to a new ••third theory to explain CADASIL pathogenesis: oxidative stress in vascular smooth muscle cells might be involved.
Spinner NB. CADASIL: Notch signaling 14
defect or protein accumulation problem? J. Clin. Invest. 105(5), 561–562 (2000).
Vikelis M, Xifaras M, Mitsikostas DD. 15
CADASIL: a short review of the literature and a description of the first family from Greece. Funct. Neurol. 21(2), 77–82 (2006).
Joutel A, Vahedi K, Corpechot C16 et al. Strong clustering and stereotyped nature of Notch3 mutations in CADASIL patients. Lancet 350(9090), 1511–1515 (1997).
Joutel A, Andreux F, Gaulis S17 et al. The ectodomain of the Notch3 receptor accumulates within the cerebrovasculature of CADASIL patients. J. Clin. Invest. 105(5), 597–605 (2000).
Ishiko A, Shimizu A, Nagata E, Takahashi 18
K, Tabira T, Suzuki N. Notch3 ectodomain is a major component of granular osmiophilic material (GOM) in CADASIL. Acta Neuropathol. 112(3), 333–339 (2006).
Mesulam M, Siddique T, Cohen B. 19
Cholinergic denervation in a pure multi-infarct state: observations on CADASIL. Neurology 60(7), 1183–1185 (2003).
www.expert-reviews.com 207
ReviewUpdate of CADASIL management
Gray F, Polivka M, Viswanathan A, 20
Baudrimont M, Bousser MG, Chabriat H. Apoptosis in cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy. J. Neuropathol. Exp. Neurol. 66(7), 597–607 (2007).
Keverne JS, Low WC, Ziabreva I, Court 21
JA, Oakley AE, Kalaria RN. Cholinergic neuronal deficits in CADASIL. Stroke 38(1), 188–191 (2007).
Sharma P, Wang T, Brown MJ, Schapira 22
AH. Fits and strokes. Lancet 358(9276), 120 (2001).
Haan J, Lesnik Oberstein SA, Ferrari MD. 23
Epilepsy in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. Cerebrovasc. Dis. 24(2–3), 316–317 (2007).
Valko PO, Siccoli MM, Schiller A, Wieser 24
HG, Jung HH. Non-convulsive status epilepticus causing focal neurological deficits in CADASIL. J. Neurol. Neurosurg. Psychiatr. 78(11), 1287–1289 (2007).
Nakamura T, Watanabe H, Hirayama M25 et al. CADASIL with NOTCH3 S180C presenting anticipation of onset age and hallucinations. J. Neurol. Sci. 238(1–2), 87–91 (2005).
O’Sullivan M, Jarosz JM, Martin RJ, 26
Deasy N, Powell JF, Markus HS. MRI hyperintensities of the temporal lobe and external capsule in patients with CADASIL. Neurology 56(5), 628–634 (2001).
Singhal S, Rich P, Markus HS. The spatial 27
distribution of MR imaging abnormalities in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy and their relationship to age and clinical features. AJNR Am. J. Neuroradiol. 26(10), 2481–2487 (2005).
Dichgans M, Holtmannspotter M, Herzog 28
J, Peters N, Bergmann M, Yousry TA. Cerebral microbleeds in CADASIL: a gradient-echo magnetic resonance imaging and autopsy study. Stroke 33(1), 67–71 (2002).
Viswanathan A , Chabriat H. Cerebral 29
microhemorrhage. Stroke 37(2), 550–555 (2006).
Lesnik Oberstein SA, van den Boom R, 30
van Buchem MA et al. Cerebral microbleeds in CADASIL. Neurology 57(6), 1066–1070 (2001).
Ragoschke-Schumm A, Axer H, Fitzek C31 et al. Intracerebral haemorrhage in CADASIL. J. Neurol. Neurosurg. Psychiatr. 76(11), 1606–1607 (2005).
Choi JC, Kang SY, Kang JH, Park JK. 32
Intracerebral hemorrhages in CADASIL. Neurology 67(11), 2042–2044 (2006).
Werbrouck BF , De Bleecker JL. 33
Intracerebral haemorrhage in CADASIL. A case report. Acta Neurol. Belg. 106(4), 219–221 (2006).
Requena I, Indakoetxea B, Lema C, Santos 34
B, Garcia-Castineira A, Arias M. [Coma associated with migraine]. Rev. Neurol. 29(11), 1048–1051 (1999).
Le Ber I, Carluer L, Derache N, Lalevee C, 35
Ledoze F, Defer GL. Unusual presentation of CADASIL with reversible coma and confusion. Neurology 59(7), 1115–1116 (2002).
Feuerhake F, Volk B, Ostertag CB36 et al. Reversible coma with raised intracranial pressure: an unusual clinical manifestation of CADASIL. Acta Neuropathol. (Berl.) 103(2), 188–192 (2002).
Kleinig TJ, Kimber T, Thompson PD. 37
Acute encephalopathy as the initial symptom of CADASIL. Intern. Med. J. 37(11), 786–787 (2007).
Schon F, Martin RJ, Prevett M, Clough C, 38
Enevoldson TP, Markus HS. “CADASIL coma”: an underdiagnosed acute encephalopathy. J. Neurol. Neurosurg. Psychiatr. 74(2), 249–252 (2003).
Desmond DW, Moroney JT, Lynch T39 et al. CADASIL in a North American family: clinical, pathologic, and radiologic findings. Neurology 51(3), 844–849 (1998).
Kotorii S, Sakae N, Yamada N, Yamanaka 40
H, Fujii N, Nakashima Y. [A case of CADASIL in early stage]. Rinsho Shinkeigaku 41(6), 306–309 (2001).
Avila A, Bello J, Maho P, Gomez MI. 41
[A new Spanish family with CADASIL associated with 346C>T mutation of NOTCH3 gene]. Neurologia 22(7), 484–487 (2007).
Cumurciuc R, Massin P, Paques M42 et al. Retinal abnormalities in CADASIL: a retrospective study of 18 patients. J. Neurol. Neurosurg. Psychiatry 75(7), 1058–1060 (2004).
Haritoglou C, Rudolph G, Hoops JP, 43
Opherk C, Kampik A, Dichgans M. Retinal vascular abnormalities in CADASIL. Neurology 62(7), 1202–1205 (2004).
Rufa A, Malandrini A, Dotti MT, Berti G, 44
Salvadori C, Federico A. Typical pathological changes of CADASIL in the optic nerve. Neurol. Sci. 26(4), 271–274 (2005).
Gobron C, Viswanathan A, Bousser MG, 45
Chabriat H. Multiple simultaneous cerebral infarctions in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. Cerebrovasc. Dis. 22(5–6), 445–446 (2006).
Rubio A, Rifkin D, Powers JM46 et al. Phenotypic variability of CADASIL and novel morphologic findings. Acta Neuropathol. 94(3), 247–254 (1997).
Cocho D, Martí-Fábregas J, Rio E, 47
Gallardo E, Baiget M, Martí-Vilalta JL. [A new mutation of CADASIL disease in a patient with cerebellar stroke]. Neurologia 21(9), 589 (2006).
Hutchinson M, O’Riordan J, Javed M 48 et al. Familial hemiplegic migraine and autosomal dominant arteriopathy with leukoencephalopathy (CADASIL). Ann. Neurol. 38(5), 817–824 (1995).
Cumurciuc R, Guichard JP, Reizine D, 49
Gray F, Bousser MG, Chabriat H. Dilation of Virchow–Robin spaces in CADASIL. Eur. J. Neurol. 13(2), 187–190 (2006).
Pescini F, Sarti C, Pantoni L50 et al. Cerebellar arteriovenous malformation and vertebral artery aneurysm in a CADASIL patient. Acta Neurol. Scand. 113(1), 62–63 (2006).
Ratzinger G, Ransmayr G, Romani N, 51
Zelger B. CADASIL – an unusual manifestation with prominent cutaneous involvement. Br. J. Dermatol. 152(2), 346–349 (2005).
Saiki S, Sakai K, Saiki M52 et al. Varicose veins associated with CADASIL result from a novel mutation in the Notch3 gene. Neurology 67(2), 337–339 (2006).
Van Gerpen JA, Ahlskog JE, Petty GW. 53
Progressive supranuclear palsy phenotype secondary to CADASIL. Parkinsonism Relat. Disord. 9(6), 367–369 (2003).
Miranda M, Dichgans M, Slachevsky A54 et al. CADASIL presenting with a movement disorder: a clinical study of a Chilean kindred. Mov. Disord. 21(7), 1008–1012 (2006).
Dichgans M, Wick M, Gasser T. 55
Cerebrospinal fluid findings in CADASIL. Neurology 53(1), 233 (1999).
Unlu M, De Lange RP, de Silva R, Kalaria 56
R, St Clair D. Detection of complement factor B in the cerebrospinal fluid of patients with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy disease using two-dimensional gel electrophoresis and mass spectrometry. Neurosci. Lett. 282(3), 149–152 (2000).
Expert Rev. Neurother. 9(2), (2009)208
Review del Río-Espínola, Mendióroz, Domingues-Montanari et al.
Broadley SA, Sawcer SJ, Chataway SJ57 et al. No association between multiple sclerosis and the Notch3 gene responsible for cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL). J. Neurol. Neurosurg. Psychiatry 71(1), 97–99 (2001).
Ruibal M, de Arce A, Martínez Pérez-Balsa 58
A et al. [X Annual Meeting of the Neurology Society of Basque Country]. Revista Neurología 23(122), 922 (1995).
Escary JL, Cecillon M, Maciazek J, 59
Lathrop M, Tournier-Lasserve E, Joutel A. Evaluation of DHPLC analysis in mutational scanning of Notch3, a gene with a high G-C content. Hum. Mutat. 16(6), 518–526 (2000).
Joutel A, Favrole P, Labauge P60 et al. Skin biopsy immunostaining with a Notch3 monoclonal antibody for CADASIL diagnosis. Lancet 358(9298), 2049–2051 (2001).
Baudrimont M, Dubas F, Joutel A, 61
Tournier-Lasserve E, Bousser MG. Autosomal dominant leukoencephalopathy and subcortical ischemic stroke. A clinicopathological study. Stroke 24(1), 122–125 (1993).
Malandrini A, Gaudiano C, Gambelli S 62
et al. Diagnostic value of ultrastructural skin biopsy studies in CADASIL. Neurology 68(17), 1430–1432 (2007).
Fouillade C, Chabriat H, Riant F63 et al. Activating NOTCH3 mutation in a patient with small-vessel-disease of the brain. Hum. Mutat. 29(3), 452 (2008).
Ferrari MD, Roon KI, Lipton RB, Goadsby 64
PJ. Oral triptans (serotonin 5-HT [1B/1D] agonists) in acute migraine treatment: a meta-analysis of 53 trials. Lancet 358(9294), 1668–1675 (2001).
Holroyd KA, Penzien DB, Cordingley GE. 65
Propranolol in the management of recurrent migraine: a meta-analytic review. Headache 31(5), 333–340 (1991).
Schurks M, Diener HC, Goadsby P. 66
Update on the prophylaxis of migraine. Curr. Treat. Options Neurol. 10(1), 20–29 (2008).
Couch JR, Ziegler DK, Hassanein R. 67
Amitriptyline in the prophylaxis of migraine. Effectiveness and relationship of antimigraine and antidepressant effects. Neurology 26(2), 121–127 (1976).
Silberstein SD, Neto W, Schmitt J, Jacobs 68
D. Topiramate in migraine prevention: results of a large controlled trial. Arch. Neurol. 61(4), 490–495 (2004).
Shaygannejad V, Janghorbani M, 69
Ghorbani A, Ashtary F, Zakizade N, Nasr V. Comparison of the effect of topiramate and sodium valporate in migraine prevention: a randomized blinded crossover study. Headache 46(4), 642–648 (2006).
Mathew NT, Rapoport A, Saper J70 et al. Efficacy of gabapentin in migraine prophylaxis. Headache 41(2), 119–128 (2001).
Steiner TJ, Ahmed F, Findley LJ, 71
MacGregor EA, Wilkinson M. S-fluoxetine in the prophylaxis of migraine: a Phase II double-blind randomized placebo-controlled study. Cephalalgia 18(5), 283–286 (1998).
Forteza AM, Brozman B, Rabinstein AA, 72
Romano JG, Bradley WG. Acetazolamide for the treatment of migraine with aura in CADASIL. Neurology 57(11), 2144–2145 (2001).
Chabriat H, Pappata S, Ostergaard L73 et al. Cerebral hemodynamics in CADASIL before and after acetazolamide challenge assessed with MRI bolus tracking. Stroke 31(8), 1904–1912 (2000).
Chabriat H, Vahedi K, Iba-Zizen MT74 et al. Clinical spectrum of CADASIL: a study of 7 families. Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. Lancet 346(8980), 934–939 (1995).
Dichgans M, Petersen D. Angiographic 75
complications in CADASIL. Lancet 349(9054), 776–777 (1997).
Singhal S, Bevan S, Barrick T, Rich P, 76
Markus HS. The influence of genetic and cardiovascular risk factors on the CADASIL phenotype. Brain 127(Pt 9), 2031–2038 (2004).
Holtmannspotter M, Peters N, Opherk C77 et al. Diffusion magnetic resonance histograms as a surrogate marker and predictor of disease progression in CADASIL: a two-year follow-up study. Stroke 36(12), 2559–2565 (2005).
Viswanathan A, Guichard JP, 78
Gschwendtner A et al. Blood pressure and haemoglobin A1c are associated with microhaemorrhage in CADASIL: a two-centre cohort study. Brain 129(Pt 9), 2375–2383 (2006).
Peters N, Holtmannspotter M, Opherk C79 et al. Brain volume changes in CADASIL: a serial MRI study in pure subcortical ischemic vascular disease. Neurology 66(10), 1517–1522 (2006).
Oh JH, Lee JS, Kang SY, Kang JH, Choi 80
JC. Aspirin-associated intracerebral hemorrhage in a patient with CADASIL. Clin. Neurol. Neurosurg. 110(4), 384–386 (2008).
European Stroke Organisation Executive 81
Committee. Guidelines for management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovasc. Dis. 25(5), 457–507 (2008).
Costa J, Ferro JM, Matias-Guiu J, 82
varez-Sabin J, Torres F. Triflusal for preventing serious vascular events in people at high risk. Cochrane Database Syst. Rev. 3, CD004296 (2005).
Peters N, Freilinger T, Opherk C, 83
Pfefferkorn T, Dichgans M. Effects of short term atorvastatin treatment on cerebral hemodynamics in CADASIL. J. Neurol. Sci. 260(1–2), 100–105 (2007).
Lauterbach EC , Schweri MM. 84
Amelioration of pseudobulbar affect by fluoxetine: possible alteration of dopamine-related pathophysiology by a selective serotonin reuptake inhibitor. J. Clin. Psychopharmacol. 11(6), 392–393 (1991).
Chen Y, Guo JJ, Li H, Wulsin L, Patel NC. 85
Risk of cerebrovascular events associated with antidepressant use in patients with depression: a population-based, nested case–control study. Ann. Pharmacother. 42(2), 177–184 (2008).
Swenson JR, Doucette S, Fergusson D. 86
Adverse cardiovascular events in antidepressant trials involving high-risk patients: a systematic review of randomized trials. Can. J. Psychiatry 51(14), 923–929 (2006).
Kharofa J, Sekar P, Haverbusch M87 et al. Selective serotonin reuptake inhibitors and risk of hemorrhagic stroke. Stroke 38(11), 3049–3051 (2007).
Dichgans M, Markus HS, Salloway S88 et al. Donepezil in patients with subcortical vascular cognitive impairment: a randomised double-blind trial in CADASIL. Lancet Neurol. 7(4), 310–318 (2008).
First randomized placebo-controlled study ••performed in CADASIL patients with cognitive impairment demonstrates that donepezil has no effect on global cognition but improves some executive functions.
Schneider LS. Does donepezil improve 89
executive function in patients with CADASIL? Lancet Neurol. 7(4), 287–289 (2008).
www.expert-reviews.com 209
ReviewUpdate of CADASIL management
Roman GC. Cholinergic dysfunction in 90
vascular dementia. Curr. Psychiatry Rep. 7(1), 18–26 (2005).
Posada IJ, Ferrero Ros M, López Valdés E, 91
Goñi Imizcoz M. [Galantamina in CADASIL dementia]. Neurologia 22(9), 722 (2007).
Areosa SA, Sherriff F, McShane R. 92
Memantine for dementia. Cochrane Database Syst. Rev. 3, CD003154 (2005).
Qaseem A, Snow V, Cross JT Jr93 et al. Current pharmacologic treatment of dementia: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann. Intern. Med. 148(5), 370–378 (2008).
Grosset DG, Ebrahim S, Bone I, Warlow 94
C. Stroke in pregnancy and the puerperium: what magnitude of risk? J. Neurol. Neurosurg. Psychiatr. 58(2), 129–131 (1995).
Roine S, Poyhonen M, Timonen S95 et al. Neurologic symptoms are common during gestation and puerperium in CADASIL. Neurology 64(8), 1441–1443 (2005).
Roberts JM, Taylor RN, Musci TJ, Rodgers 96
GM, Hubel CA, McLaughlin MK. Preeclampsia: an endothelial cell disorder. Am. J. Obstet. Gynecol. 161(5), 1200–1204 (1989).
Peters N, Freilinger T, Opherk C, 97
Pfefferkorn T, Dichgans M. Enhanced l-arginine-induced vasoreactivity suggests endothelial dysfunction in CADASIL. J. Neurol. 255(8), 1203–1208 (2008).
We can translate knowledge from basic •research to clinical practice in order to find a treatment for rare disease, such as CADASIL syndrome.
Facchinetti F, Saade GR, Neri I, Pizzi C, 98
Longo M, Volpe A. l-arginine supplementation in patients with gestational hypertension: a pilot study. Hypertens. Pregnancy 26(1), 121–130 (2007).
Milunsky A, Konialis C, Shim SH99 et al. The prenatal diagnosis of cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) by mutation analysis. Prenat. Diagn. 25(11), 1057–1058 (2005).
Konialis C, Hagnefelt B, Kokkali G, 100
Pantos C, Pangalos C. Pregnancy following preimplantation genetic diagnosis of cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL). Prenat. Diagn. 27(11), 1079–1083 (2007).
Wondrak GT. Reactivity-based drug 101
discovery using vitamin B6-derived pharmacophores. Mini Rev. Med. Chem. 8(5), 519–528 (2008).
Qin W, Yang T, Ho L102 et al. Neuronal SIRT1 activation as a novel mechanism underlying the prevention of Alzheimer disease amyloid neuropathology by calorie restriction. J. Biol. Chem. 281(31), 21745–21754 (2006).
Pallas M, Verdaguer E, Tajes M, Gutierrez-103
Cuesta J, Camins A. Modulation of sirtuins: new targets for antiageing. Recent Patents CNS Drug Discov. 3(1), 61–69 (2008).
Modulation of sirtuins, a new family of •enzymes that regulate gene silencing, DNA repair, DNA recombination and apoptosis, seems promising for CADASIL treatment.
Elliott PJ, Jirousek M. Sirtuins: novel 104
targets for metabolic disease. Curr. Opin. Investig. Drugs 9(4), 371–378 (2008).
Dong Y, Hassan A, Zhang Z 105 et al. Yield of screening for CADASIL mutations in lacunar stroke and leukoaraiosis. Stroke 34(1), 203–205 (2003).
Trojano L, Ragno M, Manca A, Caruso G. 106
A kindred affected by cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL). A 2-year neuropsychological follow-up. J. Neurol. 245(4), 217–222 (1998).
Amberla K, Waljas M, Tuominen S 107 et al. Insidious cognitive decline in CADASIL. Stroke 35(7), 1598–1602 (2004).
Peters N, Opherk C, Danek A 108 et al. The pattern of cognitive performance in CADASIL: a monogenic condition leading to subcortical ischemic vascular dementia. Am. J. Psychiatry 162(11), 2078–2085 (2005).
Benisty S, Hernandez K, Viswanathan A 109
et al. Diagnostic criteria of vascular dementia in CADASIL. Stroke 39(3), 838–844 (2008).
Pfefferkorn T, Von Stuckrad-Barre S, 110
Herzog J et al. Reduced cerebrovascular CO
2 reactivity in CADASIL: a
transcranial Doppler sonography study. Stroke 32(1), 17–21 (2001).
Liebetrau M, Herzog J, Kloss CU, 111
Hamann GF, Dichgans M. Prolonged cerebral transit time in CADASIL: a transcranial ultrasound study. Stroke 33(2), 509–512 (2002).
Harju M, Tuominen S, Summanen P 112 et al. Scanning laser Doppler flowmetry shows reduced retinal capillary blood flow in CADASIL. Stroke 35(11), 2449–2452 (2004).
Singhal S, Markus HS. Cerebrovascular 113
reactivity and dynamic autoregulation in nondemented patients with CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy). J. Neurol. 252(2), 163–167 (2005).
Manabe Y, Murakami T, Iwatsuki K 114 et al. Nocturnal blood pressure dip in CADASIL. J. Neurol. Sci. 193(1), 13–16 (2001).
Hussain MB, Singhal S, Markus HS, 115
Singer DR. Abnormal vasoconstrictor responses to angiotensin II and noradrenaline in isolated small arteries from patients with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL). Stroke 35(4), 853–858 (2004).
Stenborg A, Kalimo H, Viitanen M, Terent 116
A, Lind L. Impaired endothelial function of forearm resistance arteries in CADASIL patients. Stroke 38(10), 2692–2697 (2007).
Mellies JK, Baumer T, Muller JA 117 et al. SPECT study of a German CADASIL family: a phenotype with migraine and progressive dementia only. Neurology 50(6), 1715–1721 (1998).
Tatsch K, Koch W, Linke R 118 et al. Cortical hypometabolism and crossed cerebellar diaschisis suggest subcortically induced disconnection in CADASIL: an 18F-FDG PET study. J. Nucl. Med. 44(6), 862–869 (2003).
Tuominen S, Miao Q, Kurki T 119 et al. Positron emission tomography examination of cerebral blood flow and glucose metabolism in young CADASIL patients. Stroke 35(5), 1063–1067 (2004).
Brulin P, Godfraind C, Leteurtre E, 120
Ruchoux MM. Morphometric analysis of ultrastructural vascular changes in CADASIL: analysis of 50 skin biopsy specimens and pathogenic implications. Acta Neuropathol. 104(3), 241–248 (2002).
Auer DP, Schirmer T, Heidenreich JO 121 et al. Altered white and gray matter metabolism in CADASIL: a proton MR spectroscopy and 1H-MRSI study. Neurology 56(5), 635–642 (2001).
Macri MA, Colonnese C, Garreffa G 122 et al. A chemical shift imaging study on regional metabolite distribution in a CADASIL family. Magn. Reson. Imaging 24(4), 443–447 (2006).
Expert Rev. Neurother. 9(2), (2009)210
Review del Río-Espínola, Mendióroz, Domingues-Montanari et al.
Jouvent E, Viswanathan A, Mangin JF 123 et al. Brain atrophy is related to lacunar lesions and tissue microstructural changes in CADASIL. Stroke 38(6), 1786–1790 (2007).
Liem MK, van der Grond J, Haan J 124 et al. Lacunar infarcts are the main correlate with cognitive dysfunction in CADASIL. Stroke 38(3), 923–928 (2007).
O’Sullivan M, Ngo E, Viswanathan A 125 et al. Hippocampal volume is an independent predictor of cognitive performance in CADASIL. Neurobiol. Aging DOI:10.1016/j.neurobiolaging.2007.09.002 (2007) (Epub ahead of print).
Viswanathan A, Gschwendtner A, 126
Guichard JP et al. Lacunar lesions are independently associated with disability and cognitive impairment in CADASIL. Neurology 69(2), 172–179 (2007).
Jouvent E, Mangin JF, Porcher R 127 et al. Cortical changes in cerebral small vessel diseases: a 3D MRI study of cortical morphology in CADASIL. Brain 131(Pt 8), 2201–2208 (2008).
Chabriat H, Pappata S, Poupon C 128 et al. Clinical severity in CADASIL related to ultrastructural damage in white matter: in vivo study with diffusion tensor MRI. Stroke 30(12), 2637–2643 (1999).
Iannucci G, Dichgans M, Rovaris M 129 et al. Correlations between clinical findings and magnetization transfer imaging metrics of tissue damage in individuals with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. Stroke 32(3), 643–648 (2001).
Molko N, Pappata S, Mangin JF 130 et al. Diffusion tensor imaging study of subcortical gray matter in cadasil. Stroke 32(9), 2049–2054 (2001).
Rocca MA, Filippi M, Herzog J 131 et al. A magnetic resonance imaging study of the cervical cord of patients with CADASIL. Neurology 56(10), 1392–1394 (2001).
Molko N, Pappata S, Mangin JF 132 et al. Monitoring disease progression in CADASIL with diffusion magnetic resonance imaging: a study with whole brain histogram analysis. Stroke 33(12), 2902–2908 (2002).
Dichgans M, Putz B, Boos D, Auer DP. 133
Role of subvoxel free fluid on diffusion parameters in brain tissue with cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy and its correlation with physical disability: histogram analysis of standard and fluid-attenuated MR diffusion. AJNR Am. J. Neuroradiol. 24(6), 1083–1089 (2003).
Holtmannspotter M, Peters N, Opherk C 134
et al. Diffusion magnetic resonance histograms as a surrogate marker and predictor of disease progression in CADASIL: a two-year follow-up study. Stroke 36(12), 2559–2565 (2005).
Bruening R, Dichgans M, Berchtenbreiter 135
C et al. Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy: decrease in regional cerebral blood volume in hyperintense subcortical lesions inversely correlates with disability and cognitive performance. AJNR Am. J. Neuroradiol. 22(7), 1268–1274 (2001).
Manganelli F, Ragno M, Cacchio G 136 et al. Motor cortex cholinergic dysfunction in CADASIL: a transcranial magnetic demonstration. Clin. Neurophysiol. 119(2), 351–355 (2008).
Websites
BASH – British Association for the Study 201
of Headache www.bash.org.uk
Genereviews: Lesnik Oberstein SA, Boon 202
E, Dichgans M. CADASIL (Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy) www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=gene&part=cadasil
Huntington’s Disease Society of America 203
www.hdsa.org
United Leukodystrophy Foundation 204
www.ulf.org
Alzheimer’s association 205
www.alz.org
AffiliationsAlberto del Río-Espínola •Neurovascular Research Laboratory and Neurovascular Unit, Vall d’Hebrón Hospital, Neurology and Medicine Departments-Universitat Autònoma de Barcelona, Spain
Maite Mendióroz •Neurovascular Research Laboratory and Neurovascular Unit, Vall d’Hebrón Hospital, Neurology and Medicine Departments-Universitat Autònoma de Barcelona, Spain
Sophie Domingues-Montanari •Neurovascular Research Laboratory and Neurovascular Unit, Vall d’Hebrón Hospital, Neurology and Medicine Departments-Universitat Autònoma de Barcelona, Spain
Patricia Pozo-Rosich •Neurovascular Research Laboratory and Neurovascular Unit, Vall d’Hebrón Hospital, Neurology and Medicine Departments-Universitat Autònoma de Barcelona, Spain
Esther Solé •Molecular Biology Unit, Biochemistry Department, Vall d’Hebrón Hospital, Barcelona, Spain
Jessica Fernández-Morales •Neurovascular Research Laboratory and Neurovascular Unit. Vall d’Hebrón Hospital, Neurology and Medicine Departments-Universitat Autònoma de Barcelona, Spain
Israel Fernández-Cadenas •Neurovascular Research Laboratory and Neurovascular Unit, Vall d’Hebrón Hospital, Neurology and Medicine Departments-Universitat Autònoma de Barcelona, Spain
Joan Montaner •Neurovascular Research Laboratory and Neurovascular Unit, Institut de Recerca, Hospital Vall d’Hebron, Pg Vall d’Hebron 119-129, 08035 Barcelona, Spain Tel.: +34 934 894 073 Fax: +34 934 894 102 [email protected]