burns medicine
TRANSCRIPT
Primary Complaints 207
Bu
rns
Anatomic essentials
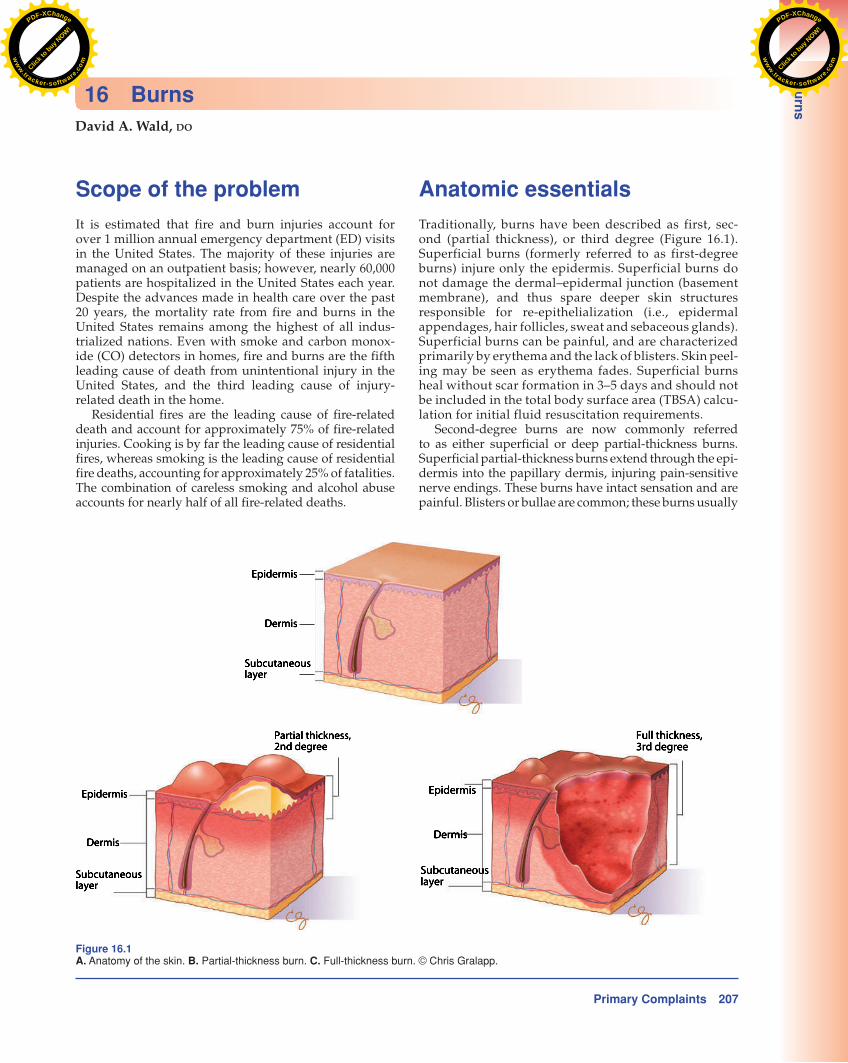
Traditionally, burns have been described as first, sec-ond (partial thickness), or third degree ( Figure 16.1 ). Superficial burns (formerly referred to as first-degree burns) injure only the epidermis. Superficial burns do not damage the dermal–epidermal junction (basement membrane), and thus spare deeper skin structures responsible for re-epithelialization (i.e., epidermal appendages, hair follicles, sweat and sebaceous glands). Superficial burns can be painful, and are characterized primarily by erythema and the lack of blisters. Skin peel-ing may be seen as erythema fades. Superficial burns heal without scar formation in 3–5 days and should not be included in the total body surface area (TBSA) calcu-lation for initial fluid resuscitation requirements.
Second-degree burns are now commonly referred to as either superficial or deep partial-thickness burns. Superficial partial-thickness burns extend through the epi-dermis into the papillary dermis, injuring pain-sensitive nerve endings. These burns have intact sensation and are painful. Blisters or bullae are common; these burns usually
Scope of the problem
It is estimated that fire and burn injuries account for over 1 million annual emergency department (ED) visits in the United States. The majority of these injuries are managed on an outpatient basis; however, nearly 60,000 patients are hospitalized in the United States each year. Despite the advances made in health care over the past 20 years, the mortality rate from fire and burns in the United States remains among the highest of all indus-trialized nations. Even with smoke and carbon monox-ide (CO) detectors in homes, fire and burns are the fifth leading cause of death from unintentional injury in the United States, and the third leading cause of injury-related death in the home.
Residential fires are the leading cause of fire-related death and account for approximately 75% of fire-related injuries. Cooking is by far the leading cause of residential fires, whereas smoking is the leading cause of residential fire deaths, accounting for approximately 25% of fatalities. The combination of careless smoking and alcohol abuse accounts for nearly half of all fire-related deaths.
David A. Wald , DO
16 Burns
Figure 16.1 A. Anatomy of the skin. B. Partial-thickness burn. C. Full-thickness burn. © Chris Gralapp.
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om
208 Primary Complaints
Bu
rns
nerve endings; however, surrounding areas may be pain-ful. All but the smallest full-thickness burns are treated with skin grafting to help limit the development of hypertrophic scarring. Some references in the literature may describe
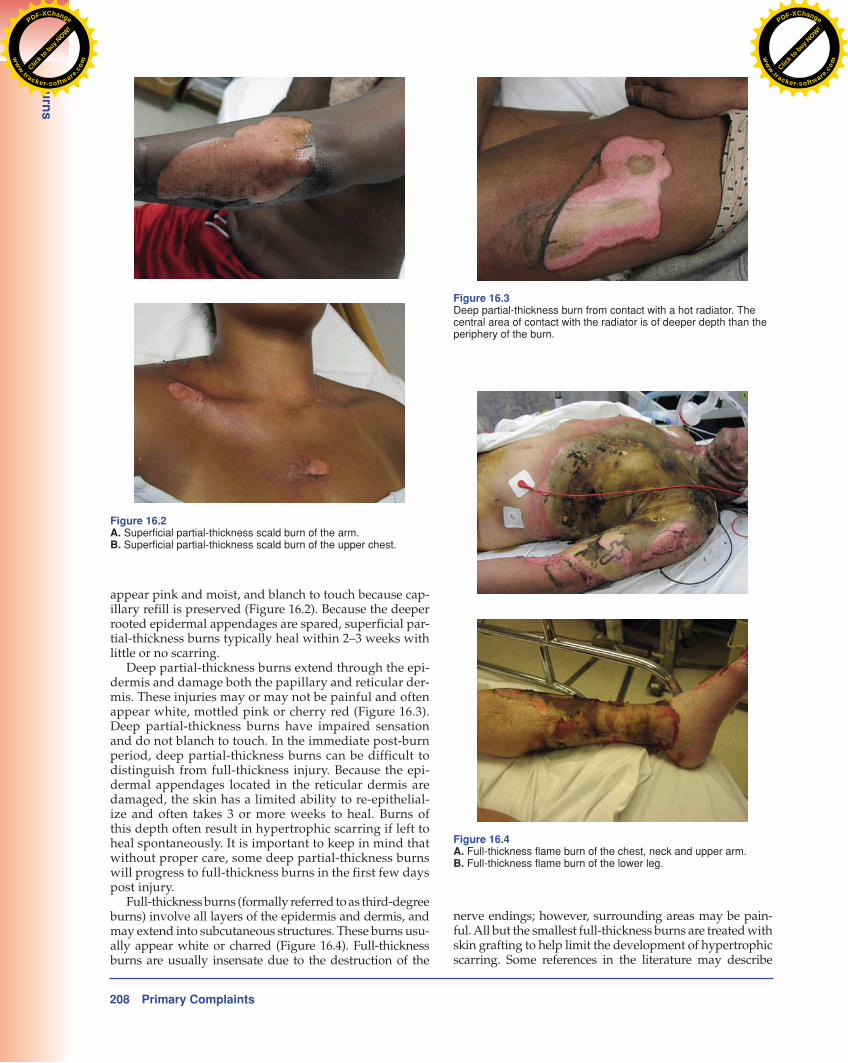
appear pink and moist, and blanch to touch because cap-illary refill is preserved ( Figure 16.2 ). Because the deeper rooted epidermal appendages are spared, superficial par-tial-thickness burns typically heal within 2–3 weeks with little or no scarring.
Deep partial-thickness burns extend through the epi-dermis and damage both the papillary and reticular der-mis. These injuries may or may not be painful and often appear white, mottled pink or cherry red ( Figure 16.3 ). Deep partial-thickness burns have impaired sensation and do not blanch to touch. In the immediate post-burn period, deep partial-thickness burns can be difficult to distinguish from full-thickness injury. Because the epi-dermal appendages located in the reticular dermis are damaged, the skin has a limited ability to re-epithelial-ize and often takes 3 or more weeks to heal. Burns of this depth often result in hypertrophic scarring if left to heal spontaneously. It is important to keep in mind that without proper care, some deep partial-thickness burns will progress to full-thickness burns in the first few days post injury .
Full- thickness burns (formally referred to as third-degree burns) involve all layers of the epidermis and dermis, and may extend into subcutaneous structures. These burns usu-ally appear white or charred ( Figure 16.4 ). Full-thickness burns are usually insensate due to the destruction of the
Figure 16.2 A. Superficial partial-thickness scald burn of the arm. B. Superficial partial-thickness scald burn of the upper chest.
Figure 16.3 Deep partial-thickness burn from contact with a hot radiator. The central area of contact with the radiator is of deeper depth than the periphery of the burn.
Figure 16.4 A. Full-thickness flame burn of the chest, neck and upper arm. B. Full-thickness flame burn of the lower leg.
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om
Primary Complaints 209
Bu
rns
What were the circumstances surrounding the injury?
Information regarding the circumstances surrounding the injury should be obtained from the patient, family, wit-nesses, or prehospital care providers. Was the injury caused by hot tap water, grease, or another hot liquid? Was the injury caused by flame or contact with a hot object? Were chemicals or industrial solvents involved? Details regard-ing the mechanism of injury may suggest the depth of burn injury and alert physicians to potential associated injuries. The patient’s condition at the scene and any treatment pro-vided by bystanders or an outside referring hospital should also be sought.
Was the patient confined in a burning environment, or was there a history of an explosion?
Patients involved in a closed space fire or an explosion are at risk for inhalation injury . In addition, a history of an explosion places patients at risk for barotrauma and blast-related injuries.
Did the patient sustain associated traumatic injuries?
Associated trauma may be masked in a patient with a sig-nificant burn injury. All “burn” patients should undergo a systematic trauma assessment. If the patient was in a house fire, it is important to find out how the patient got out of
fourth-degree burns which involve deeper structures (i.e., muscle and bone).
Red flags
Emergency clinicians must be adept at recognizing “red flags” (warning signs and symptoms) from the history and physical examination that raise concern for life-threatening or dangerous diagnoses ( Table 16.1 ).
History
A focused history should be performed on all burn patients. Key historical information may heighten the suspicion for associated injuries and can influence management.
When did the burn occur?
Determining the timing of a burn is important for patients requiring IV fluid resuscitation. Delays in initiating fluid resuscitation increase fluid requirements, and delays greater than 2 hours after burn injury are associated with increased mortality. Determining the time of injury is important when evaluating acute or subacute burn inju-ries, as the depth of certain deep burns will not be evident in the immediate post-burn period.
Table 16.1 Burns red flags
History Concerning diagnosis
Burns in a confined space Inhalation injury
Explosion Barotrauma or other associated trauma
Difficulty speaking, swallowing or drooling Upper airway burns or inhalation injury
Coughing, wheezing or difficulty breathing Inhalation injury
Headache, dizziness, or history of loss of consciousness at the scene Carbon monoxide toxicity
Burn wound inconsistent with history Non-accidental trauma
Preexisting medical conditions (HIV/AIDS, renal disease, liver disease, and metastatic cancer)
Increased morbidity, mortality and length of hospitalization
Examination finding Concerning diagnosis
Tachypnea Airway burn
Hypotension Volume depletion or other associated significant trauma
Burns to the face, neck or upper torso; singed eyebrows and nasal vibrissae; carbon deposits and acute inflammatory changes in the oropharynx; carbonaceous sputum
Airway burns or inhalation injury
Burns that are painful and characterized primarily by erythema and lack of blisters
Superficial burns
Burns that are painful and usually appear pink, moist, with blisters or bullae
Superficial partial-thickness burns
Burns that appear white, mottled pink or cherry red with impaired sensation
Deep partial-thickness burns
Burns that appear white or charred with impaired sensation Full-thickness burns
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om

210 Primary Complaints
Bu
rns
Neurologic
Ask about headache, dizziness, or a history of loss of con-sciousness at the scene? In the context of a burn injury or fire exposure, these symptoms suggest concomitant CO toxicity. Complaints of CO toxicity are often subtle, so a high index of suspicion must be maintained.
Past medical
After controlling for patient age, sex, TBSA burned and the presence of inhalation injury, several preexisting medi-cal conditions are associated with increased mortality risk and length of hospital stay in patients with an acute burn injury. Preexisting medical conditions with the highest mortality risk include HIV/AIDS, renal disease, liver dis-ease and metastatic cancer. Other conditions independ-ently associated with an increased mortality risk in the burn patient are pulmonary circulation disorders, con-gestive heart failure, obesity, non-metastatic malignan-cies, alcohol abuse, peripheral vascular disorders, cardiac dysrhythmias and patients with neurologic disorders. Several conditions are associated with prolonged hospital stays but no increase in mortality. These include paraly-sis, dementia, peptic ulcer disease, psychiatric illness, cerebrovascular disease, valvular disease, diabetes, drug abuse and hypertension. The presence of one or more preexisting comorbidities may warrant hospital admis-sion or transfer to a regional burn center for patients with otherwise minor or moderate size burns.
Physical examination
When evaluating a burn patient, the physical examina-tion should be performed in a systematic fashion (as for all trauma victims). After life-threatening conditions are identified and addressed, the emergency physician should determine the depth and TBSA of the burn.
Vital signs
Major burns lead to a hyperdynamic state commonly associated with tachycardia. For this reason, the heart rate should not be used in isolation as a reliable indicator of volume status. Tachypnea may also indicate a hyper-dynamic state or airway involvement. If hypotension is present, volume depletion resulting from third spac-ing of fluids or associated trauma should be given high priority.
Primary and secondary surveys
The physical examination begins with the primary sur-vey. Immediate life-threats should be addressed first, which may be difficult given the dramatic nature and overpowering odor of burns. Additional attention should be given to clinical findings associated with inhalation injury, such as burns to the face, neck or upper torso; singed eyebrows and nasal vibrissae; carbon deposits
the building (i.e., did they jump out of a window or were they found in bed). Burns associated with motor vehicle collisions are often associated with traumatic injuries.
Is the burn painful?
Typically, all superficial partial thickness burns are pain-ful. Deeper burns, such as deep partial-thickness and full-thickness burns, are often less painful or painless, respectively.
Were there suspicious circumstances surrounding the burn injury?
It is important to consider that burn injuries might be self-inflicted, perhaps in a suicide attempt or gesture. Additionally, toxic ingestions or potentially lethal over-doses can occur prior to setting oneself or a building on fire.
Is the burn pattern consistent with the explanation?
Burns with a clear line of demarcation, or located on the buttocks, between the child’s legs or other areas that would be difficult for the child to reach should be very concerning for burns inflicted by another individual (abuse). Concurrent injuries or bruises at different stages of healing are also suspicious for child abuse, which is far more common than most physicians believe. Additional information suggestive of non-accidental burn injury includes delays in seeking care, a pattern of burn injury inconsistent with the child’s motor abilities, or witness stories that do not correlate or seem possible. Abuse should be considered when caregivers appear angry, resentful toward the child, or even overly protective or afraid of letting their child speak to physicians alone. In other words, the possibility of abuse should be considered in all traumatic injuries in children, especially burns.
Associated symptoms
Head, eyes, ears, nose and throat (HEENT)
Ask about difficulty speaking or swallowing? Difficulty speaking or swallowing, or pain during these activi-ties suggests an upper airway burn or inhalation injury, which may portend future airway compromise. Any voice change (including hoarseness) may indicate injury to or edema of the larynx and vocal cords.
Ask about difficulty with vision, such as blurred vision, photophobia, or pain? Visual complaints suggest ocular involvement, including burns, abrasions, or edema of the cornea. Foreign bodies (including penetration of the globe or orbit from flying debris) may accompany some burn injuries or explosions.
Pulmonary
Ask about coughing, wheezing, or trouble breathing? These respiratory complaints suggest the possibility of lung inhalation injury .
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om
Primary Complaints 211
Bu
rns
However, distinguishing between superficial partial-thickness and all deeper burns may help reduce hospi-tal transfers of some patients with minor burns. Bedside testing may help emergency physicians differentiate between burns of different depth, specifically between superficial partial-thickness and all deeper burns . A clini-cal approach to evaluating burn depth at the bedside is provided ( Table 16.2 ).
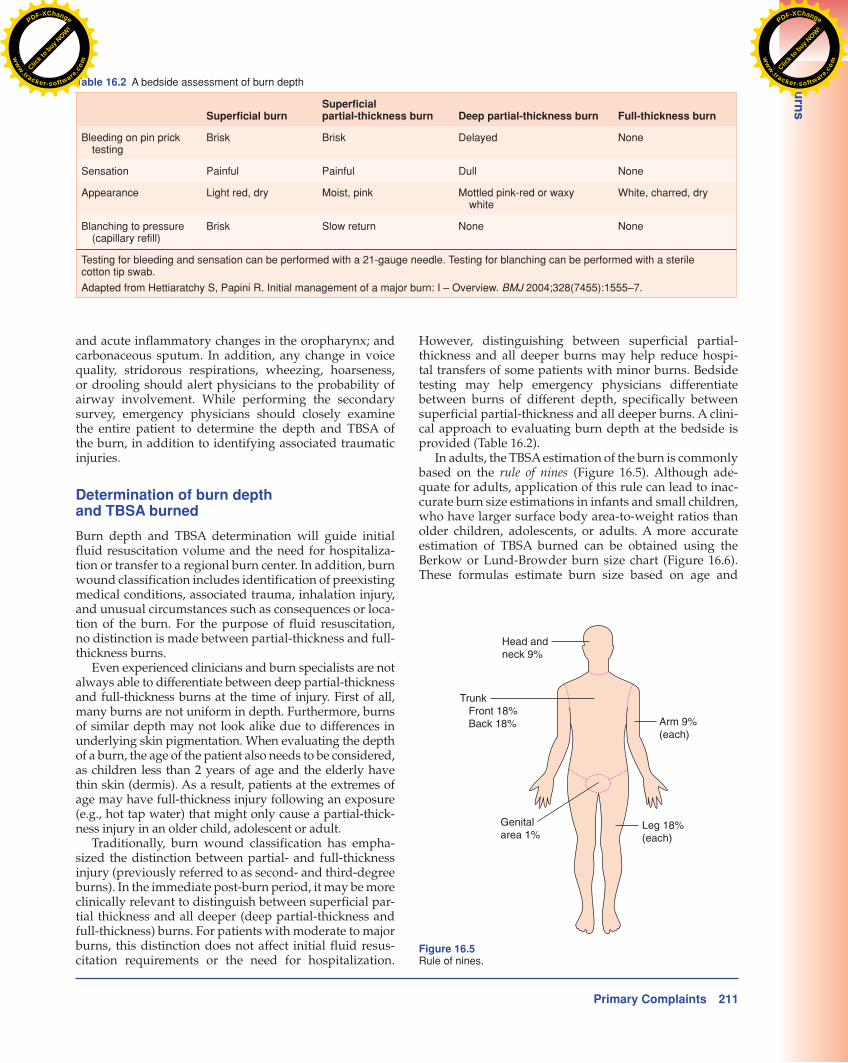
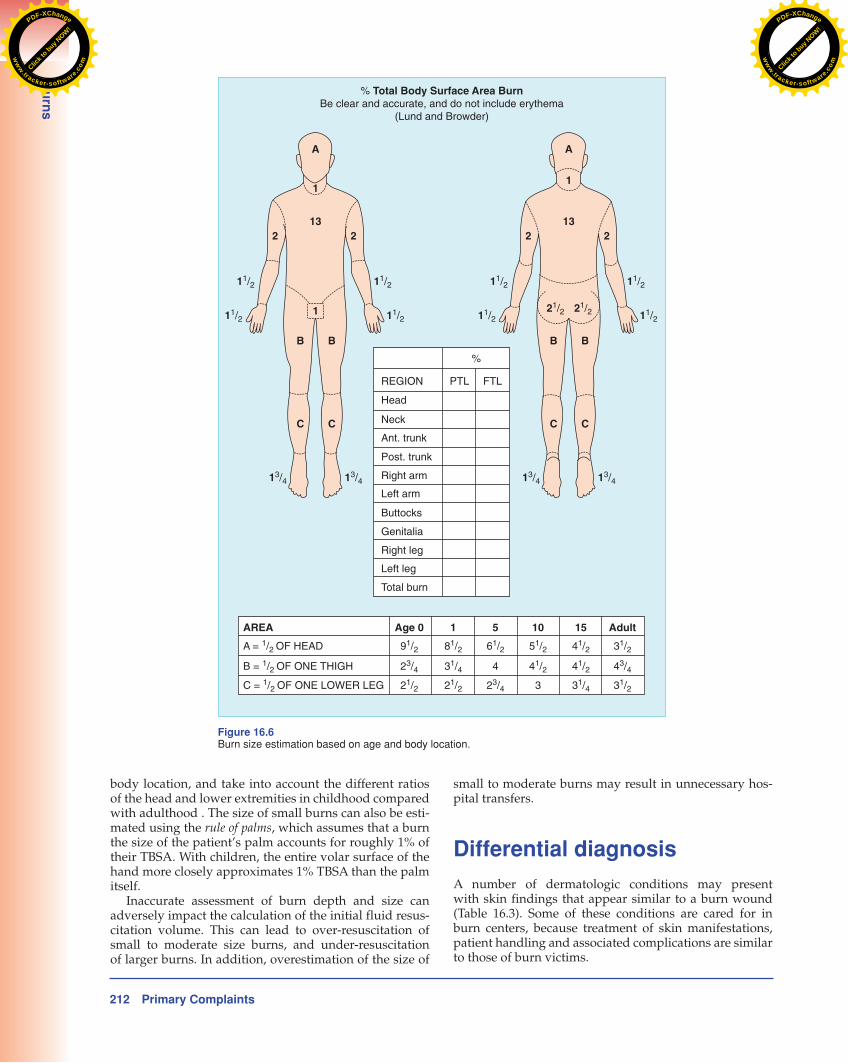
In adults, the TBSA estimation of the burn is commonly based on the rule of nines ( Figure 16.5 ). Although ade-quate for adults, application of this rule can lead to inac-curate burn size estimations in infants and small children, who have larger surface body area-to-weight ratios than older children, adolescents, or adults . A more accurate estimation of TBSA burned can be obtained using the Berkow or Lund-Browder burn size chart ( Figure 16.6 ) . These formulas estimate burn size based on age and
and acute inflammatory changes in the oropharynx; and carbonaceous sputum. In addition, any change in voice quality, stridorous respirations, wheezing, hoarseness, or drooling should alert physicians to the probability of airway involvement . While performing the secondary survey, emergency physicians should closely examine the entire patient to determine the depth and TBSA of the burn, in addition to identifying associated traumatic injuries.
Determination of burn depth and TBSA burned
Burn depth and TBSA determination will guide initial fluid resuscitation volume and the need for hospitaliza-tion or transfer to a regional burn center. In addition, burn wound classification includes identification of preexisting medical conditions, associated trauma, inhalation injury, and unusual circumstances such as consequences or loca-tion of the burn. For the purpose of fluid resuscitation, no distinction is made between partial-thickness and full-thickness burns.
Even experienced clinicians and burn specialists are not always able to differentiate between deep partial-thickness and full-thickness burns at the time of injury. First of all, many burns are not uniform in depth. Furthermore, burns of similar depth may not look alike due to differences in underlying skin pigmentation. When evaluating the depth of a burn, the age of the patient also needs to be considered, as children less than 2 years of age and the elderly have thin skin (dermis). As a result, patients at the extremes of age may have full-thickness injury following an exposure (e.g., hot tap water) that might only cause a partial-thick-ness injury in an older child, adolescent or adult.
Traditionally, burn wound classification has empha-sized the distinction between partial- and full-thickness injury (previously referred to as second- and third-degree burns). In the immediate post-burn period, it may be more clinically relevant to distinguish between superficial par-tial thickness and all deeper (deep partial-thickness and full-thickness) burns. For patients with moderate to major burns, this distinction does not affect initial fluid resus-citation requirements or the need for hospitalization.
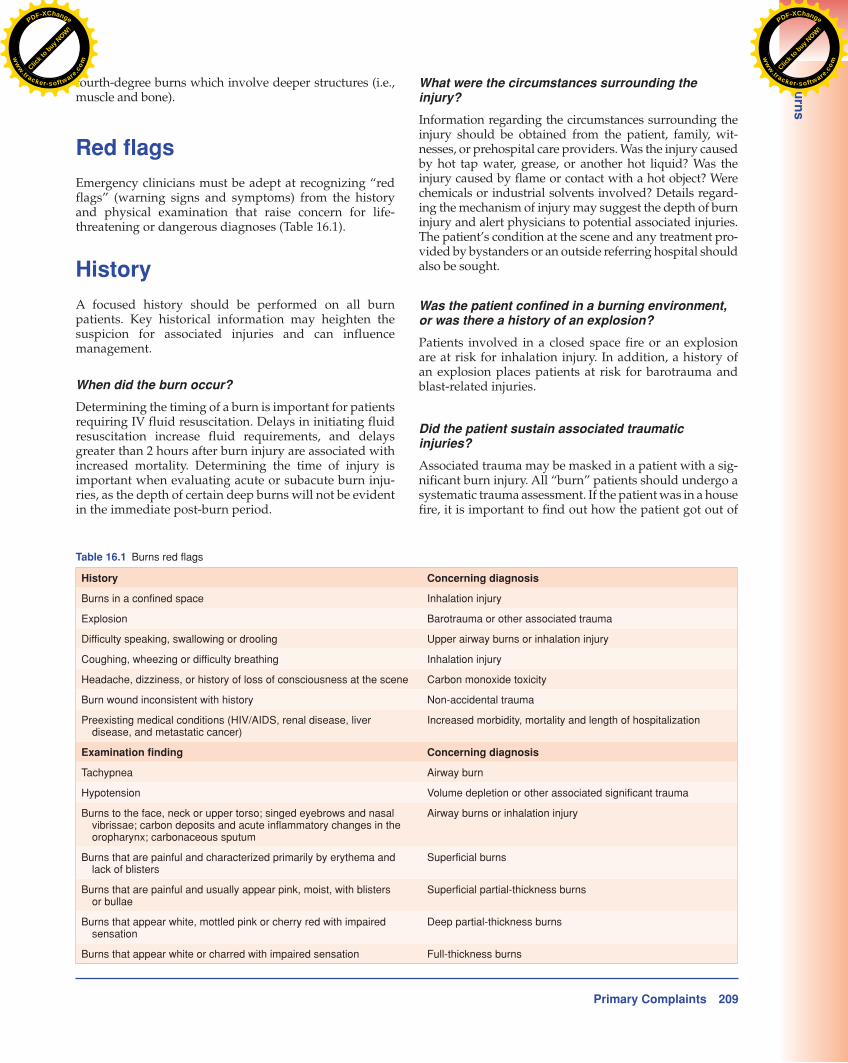
Table 16.2 A bedside assessment of burn depth
Superficial burn Superficial partial-thickness burn Deep partial-thickness burn Full-thickness burn
Bleeding on pin prick testing
Brisk Brisk Delayed None
Sensation Painful Painful Dull None
Appearance Light red, dry Moist, pink Mottled pink-red or waxy white
White, charred, dry
Blanching to pressure (capillary refill)
Brisk Slow return None None
Testing for bleeding and sensation can be performed with a 21-gauge needle. Testing for blanching can be performed with a sterile cotton tip swab.
Adapted from Hettiaratchy S, Papini R. Initial management of a major burn: I – Overview. BMJ 2004;328(7455):1555–7.
Head andneck 9%
Trunk Front 18% Back 18% Arm 9%
(each)
Genitalarea 1%
Leg 18%(each)
Figure 16.5 Rule of nines.
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om
212 Primary Complaints
Bu
rns
small to moderate burns may result in unnecessary hos-pital transfers.
Differential diagnosis
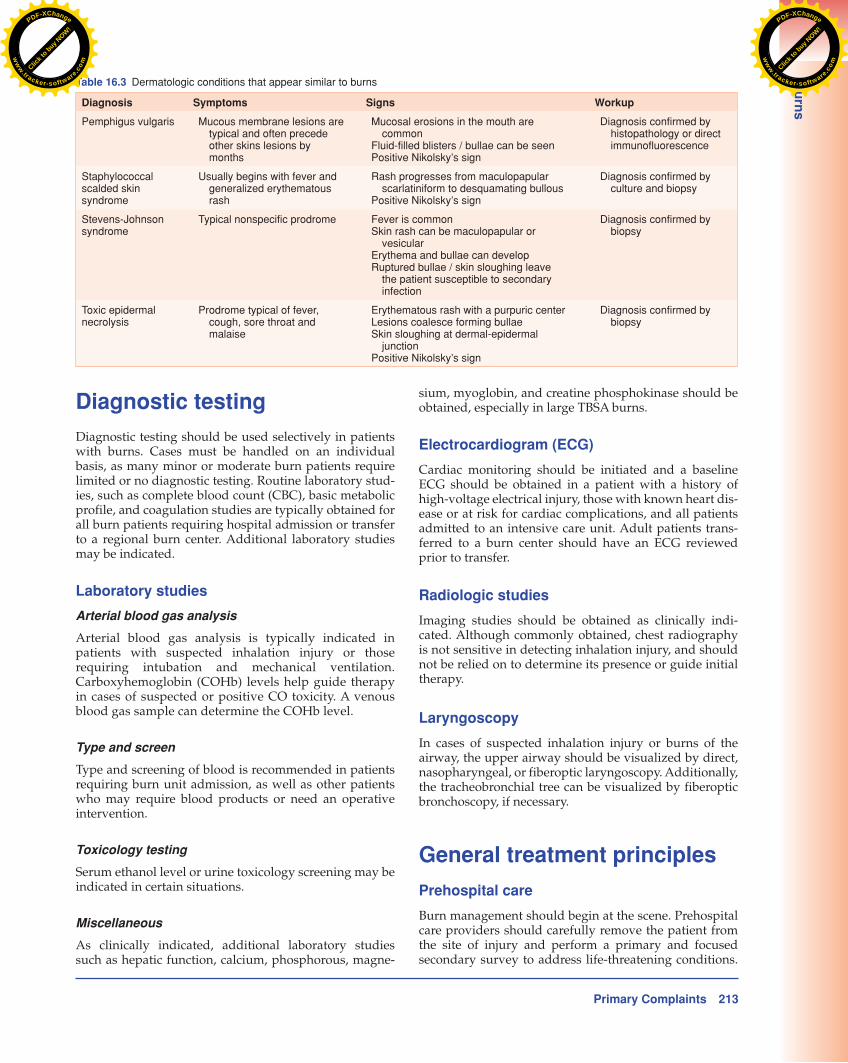
A number of dermatologic conditions may present with skin findings that appear similar to a burn wound ( Table 16.3 ). Some of these conditions are cared for in burn centers, because treatment of skin manifestations, patient handling and associated complications are similar to those of burn victims.
body location, and take into account the different ratios of the head and lower extremities in childhood compared with adulthood . The size of small burns can also be esti-mated using the rule of palms , which assumes that a burn the size of the patient’s palm accounts for roughly 1% of their TBSA. With children, the entire volar surface of the hand more closely approximates 1% TBSA than the palm itself.
Inaccurate assessment of burn depth and size can adversely impact the calculation of the initial fluid resus-citation volume. This can lead to over-resuscitation of small to moderate size burns, and under-resuscitation of larger burns. In addition, overestimation of the size of
A
% Total Body Surface Area BurnBe clear and accurate, and do not include erythema
(Lund and Browder)
1
132
11/2 11/2
11/2 11/2
13/4 13/4
2
1
B
C
B
C
A
1
132
11/2
21/2 21/2
11/2
11/2 11/2
13/4 13/4
2
B
C
B
C
REGION FTLPTL
%
Head
Neck
Ant. trunk
Post. trunk
Right arm
Left arm
Buttocks
Genitalia
Right leg
Left leg
Total burn
AREA Age 0 1 5 10 Adult15
A = 1/2 OF HEAD
B = 1/2 OF ONE THIGH
C = 1/2 OF ONE LOWER LEG
91/2
23/4
21/2
81/2
31/4
21/2
41/2
41/2
31/4
31/2
43/4
31/2
51/2
41/2
3
61/2
4
23/4
Figure 16. 6 Burn size estimation based on age and body location.
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om
Primary Complaints 213
Bu
rns
sium, myoglobin, and creatine phosphokinase should be obtained, especially in large TBSA burns.
Electrocardiogram (ECG)
Cardiac monitoring should be initiated and a baseline ECG should be obtained in a patient with a history of high-voltage electrical injury, those with known heart dis-ease or at risk for cardiac complications, and all patients admitted to an intensive care unit. Adult patients trans-ferred to a burn center should have an ECG reviewed prior to transfer.
Radiologic studies
Imaging studies should be obtained as clinically indi-cated. Although commonly obtained, chest radiography is not sensitive in detecting inhalation injury, and should not be relied on to determine its presence or guide initial therapy.
Laryngoscopy
In cases of suspected inhalation injury or burns of the airway, the upper airway should be visualized by direct, nasopharyngeal, or fiberoptic laryngoscopy. Additionally, the tracheobronchial tree can be visualized by fiberoptic bronchoscopy, if necessary.
General treatment principles
Prehospital care
Burn management should begin at the scene. Prehospital care providers should carefully remove the patient from the site of injury and perform a primary and focused secondary survey to address life-threatening conditions.
Diagnostic testing
Diagnostic testing should be used selectively in patients with burns. Cases must be handled on an individual basis, as many minor or moderate burn patients require limited or no diagnostic testing. Routine laboratory stud-ies, such as complete blood count (CBC), basic metabolic profile, and coagulation studies are typically obtained for all burn patients requiring hospital admission or transfer to a regional burn center. Additional laboratory studies may be indicated.
Laboratory studies
Arterial blood gas analysis
Arterial blood gas analysis is typically indicated in patients with suspected inhalation injury or those requiring intubation and mechanical ventilation. Carboxyhemoglobin (COHb) levels help guide therapy in cases of suspected or positive CO toxicity. A venous blood gas sample can determine the COHb level .
Type and screen
Type and screening of blood is recommended in patients requiring burn unit admission, as well as other patients who may require blood products or need an operative intervention.
Toxicology testing
Serum ethanol level or urine toxicology screening may be indicated in certain situations.
Miscellaneous
As clinically indicated, additional laboratory studies such as hepatic function, calcium, phosphorous, magne-
Table 16.3 Dermatologic conditions that appear similar to burns
Diagnosis Symptoms Signs Workup
Pemphigus vulgaris Mucous membrane lesions are typical and often precede other skins lesions by months
Mucosal erosions in the mouth are common
Fluid-filled blisters / bullae can be seenPositive Nikolsky’s sign
Diagnosis confirmed by histopathology or direct immunofluorescence
Staphylococcal scalded skin syndrome
Usually begins with fever and generalized erythematous rash
Rash progresses from maculopapular scarlatiniform to desquamating bullous
Positive Nikolsky’s sign
Diagnosis confirmed by culture and biopsy
Stevens-Johnson syndrome
Typical nonspecific prodrome Fever is common Skin rash can be maculopapular or
vesicularErythema and bullae can develop Ruptured bullae / skin sloughing leave
the patient susceptible to secondary infection
Diagnosis confirmed by biopsy
Toxic epidermal necrolysis
Prodrome typical of fever, cough, sore throat and malaise
Erythematous rash with a purpuric center Lesions coalesce forming bullae Skin sloughing at dermal-epidermal
junction Positive Nikolsky’s sign
Diagnosis confirmed by biopsy
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om

214 Primary Complaints
Bu
rns
Prehospital care providers should determine the need for any immediate interventions, such as airway control, breathing or circulatory support, and cervical spine immo-bilization. Large burns should be covered with dry sterile dressings; small or moderate size burns can be covered with cool wet dressings to help relieve pain. Supplemental oxygen should be administered if smoke inhalation is sus-pected. Intravenous fluid administration should be initi-ated, preferably at a site that does not involve the burn . Intravenous narcotics should be administered (according to protocol) . Whenever possible, individuals with exten-sive burns should be transported directly to a trauma or regional burn center.
Emergency department care
The resuscitation area should be prepared with dry sterile sheets, appropriate protective covering for medical per-sonnel, and airway equipment for the anticipated arrival of a major burn victim. The ED evaluation should be sys-tematic and be performed as any other trauma scenario, starting with the ABCs (airway, breathing, circulation). The airway is the most important initial consideration in the severely burned patient. Assessment for possible air-way involvement in a patient with suspected inhalation injury is vital. After the primary survey and treatment of any immediate life-threats, the emergency physician should perform a detailed trauma–burn secondary sur-vey. This specifically focuses on evaluating for possible smoke inhalation and identifying associated traumatic injuries, followed by an estimation of burn depth and size. This critical step will determine the initial fluid resuscitation volume and influence patient disposition. In the patient requiring transfer to a regional burn referral center, early communication with the burn specialist is recommended.
Inhalation injury
Inhalation injury has been reported in 7% of cases reported to the National Burn Registry, and in approximately one-quarter of patients with burns ≥20% TBSA. The incidence of inhalation injury increases with larger burns, presenting in approximately two-thirds of patients with TBSA burns that exceed 70%. Smoke inhalation accounts for >50% of fire-related deaths; when present, it increases the morbid-ity and mortality associated with all burn injuries. It also increases the initial fluid resuscitation requirements after thermal injury.
Smoke inhalation can cause both airway injury and systemic toxicity. Injury to the upper airway structures (lips to glottis) occurs from inhalation of superheated gases from flame, smoke, or steam. Thermal injury to the lower airway (subglottic structures) is rare because of reflex closure of the glottis and heat dissipation that occurs throughout the tracheobronchial tree. An excep-tion is inhalation injury resulting from steam, because of its ability to carry approximately 4,000 times as much heat as dry air.
Injury to the lower airway usually occurs as a result of inhalation of toxic gases and particulate matter. This
Figure 16.7 Flash burns to the face represent a high risk for an inhalation injury.
can lead to airflow obstruction from the production of mucosal edema, intraluminal debris, inspissated secre-tions and bronchospasm, subsequently resulting in a chemical tracheobronchitis. If severe, the clinical picture can resemble adult respiratory distress syndrome (ARDS) and further manifest with decreasing pulmonary compli-ance, increasing airway resistance, hypoxemia and hyper-carbia.
Patients suffering from smoke inhalation may also exhibit toxicity from systemic absorption of products of combustion, possibly leading to CO or cyanide tox-icity. On arrival, all spontaneously breathing patients with suspected smoke inhalation should immediately be placed on high-flow humidified oxygen. Early intu-bation should be considered if airway compromise is supported by history and bedside examination. It is crucial to identify which patients with smoke inhalation require early endotracheal intubation. The presence of classic indicators of smoke inhalation (i.e., facial burns, carbonaceous sputum, wheezing, voice change) does not necessarily mandate emergent endotracheal intubation ( Figure 16.7 ). Unfortunately, no group of signs or symp-toms can substitute for sound bedside clinical judgment. Furthermore, intubation may become more difficult as edema of the upper airway increases with time. When emergent intubation is not necessary, close observation with frequent serial examinations must be performed, and airway equipment (including equipment for man-aging the difficult airway) must be available at the bedside.
Carbon monoxide toxicity
CO has an affinity for hemoglobin (Hb) approximately 230 times that of oxygen. COHb decreases the amount of hemoglobin available for oxygen binding and reduces the oxygen-carrying capacity of the blood, leading to impaired tissue oxygenation.
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om

Primary Complaints 215
Bu
rns
resuscitation. However, in patients with severe burns (>40% TBSA), central venous access using the internal jugular or subclavian vein is the preferred route for fluid resuscitation.
Lactated Ringer’s solution is most frequently used for fluid resuscitation of burn patients. In comparison with normal saline solution, which contains sodium 154 mEq/L and chloride 154 mEq/L, Lactated Ringer’s solution con-tains sodium 130 mEq/L, chloride 109 mEq/L, calcium 3 mEq/L, potassium 4 mEq/L and lactate 28 mEq/L. In addition, Lactated Ringer’s solution has a higher pH compared with normal saline and more closely resembles physiologic pH (6.5 vs. 5.0, respectively).
The Parkland formula is most commonly used to guide initial fluid resuscitation during the first 24 hours after burn injury. This formula has gained almost uni-versal acceptance, not necessarily for its demonstrated superiority, but more likely because it is easy to remem-ber and use. The Parkland formula calls for the admin-istration of 4 mL/kg of body weight per %TBSA burn (partial- or full-thickness) of intravenous crystalloid fluid over the first 24 hours. Half of the calculated fluid requirement should be administered over the first 8 hours post burn, and the remaining volume over the next 16 hours. Front loading the burn resuscitation flu-ids over the first 8 hours is required because the early post-burn period is highlighted by increased capillary permeability, protein leak, edema formation and loss of plasma volume.
No resuscitation formulas can accurately predict vol-ume requirements for an individual patient. Therefore, continuous monitoring and reassessment of resuscitation targets such as blood pressure, mental status and urine output is necessary. In adults, a common goal is urine out-put of at least 0.5 to 1 mL/kg/hr, a reasonable indicator of renal perfusion. However, urine output can be affected by the use of diuretics or the presence of glycosuria (result-ing in an osmotic diuresis). Greater urine output may be needed in the presence of rhabdomyolysis to prevent pigment-induced nephropathy. A bladder catheter and urometer should be used to monitor urine output in all critically ill patients.
Escharotomy
An escharotomy may be indicated to relieve restricted ven-tilation (from circumferential thorax burns) or impaired extremity circulation (from eschar formation in circum-ferential deep partial-thickness or full-thickness extrem-ity burns). In either of these cases, the eschar should be incised through the dermis down to the level of the sub-cutaneous fat. If a chest wall escharotomy is required, a vertical incision should be made from the clavicles to the costal margin along the anterior axillary line. This inci-sion may be joined by a transverse incision along the superior, anterior abdominal wall. If a neck escharotomy is required, incisions should be made posterolaterally to avoid vascular structures. On the extremities, incisions are made on the medial and lateral surfaces, with special attention when crossing joints to avoid injuring neuro-vascular structures.
Pulse oximetry is a noninvasive tool that measures functional oxygen saturation. The pulse oximeter can-not distinguish between COHb and oxyhemoglobin, and the presence of COHb produces falsely elevated oxygen saturation readings. This overestimation of oxygen satu-ration (known as the “pulse oximetry gap”) approaches the measured COHb level.
Alternatively, a co-oximeter is a device that analyzes a small blood sample to measure concentrations of oxyhemoglobin, deoxyhemoglobin, COHb, and meth-emoglobin. Therefore, it can confirm CO toxicity by iden-tifying elevated COHb levels. Traditionally, an arterial blood sample has been used to determine the COHb level; however, a venous blood sample provides a reliable, often less painful alternative. The Masimo Rainbow SET Pulse CO-Oximeter is now available as a noninvasive alterna-tive to screen for CO toxicity.
All patients with known or suspected CO toxicity should receive high-flow oxygen. This can reduce the elimination half-life of COHb (COHb T ½ ) from 240–320 minutes at room air to 60–90 minutes. The COHb T ½ of patients treated with high-flow oxygen by face mask or 100% oxygen if intubated does not appear to be influenced by patient age, gender, history of loss of consciousness, concurrent tobacco use, or initial COHb level.
Hyperbaric oxygen (HBO) therapy has been shown to further reduce the COHb T ½ to approximately 23 minutes (at three atmospheres with 100% oxygen). Specific selec-tion criteria can identify candidates appropriate for HBO therapy. Patients with myocardial ischemia, cardiac dys-rhythmias, neuropsychiatric abnormalities, syncope or persistent neurologic findings in the face of CO toxicity should be considered for HBO therapy. All patients with COHb levels >25% , and pregnant women and young children with levels ≥15% are also candidates for HBO therapy.
It is also important to recognize that patients with similar COHb levels may exhibit varying systemic toxic-ity. Cyanide toxicity can also complicate severe cases of CO toxicity and should be considered in victims of smoke inhalation with persistent hypotension and acidemia despite adequate arterial oxygenation.
Fluid resuscitation
Fluid resuscitation in the early post-burn period is cru-cial and should be the top management priority once the airway and other life-threats have been addressed. Over the past 50 years, aggressive volume replacement in the hours immediately following a severe burn has decreased the morbidity and mortality associated with these injuries. The goal of initial fluid resuscitation is to restore and maintain vital organ perfusion and prevent burn shock.
Intravenous fluid resuscitation should be initiated in adults with partial- or full-thickness TBSA burns >20%, in older children with burns ≥15% TBSA, and in infants with burns ≥10% TBSA. Peripheral intravenous access is sufficient for the majority of patients requiring fluid
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om

216 Primary Complaints
Bu
rns
outpatient setting, topical antimicrobial agents are most effective for small- to moderate-sized superficial partial-thickness burns that are expected to heal within 2–3 weeks. When applied to deeper burns, topical antimicrobials can prevent wound infections in anticipation of a skin graft. Unfortunately, no consensus opinion or high-quality research presently exists to support one antimicrobial
Outpatient care of burns
Proper patient selection is necessary to ensure optimal burn care in an outpatient setting. The American Burn Association (ABA) has proposed a grading system for esti-mating burn severity and disposition ( Table 16.4 ). Under ideal conditions, adults with superficial partial-thickness burns <10% TBSA and children with TSBA burns <5% may be considered candidates for outpatient management, as these burns fall into the “minor category” according to the ABA grading system.
The wound care principles for minor burns are the same as for other minor wounds. Minor burns should be cleansed with gentle soap and water, and hair around the burn should not be shaved. Devitalized skin or ruptured blisters should be debrided using aseptic technique. In general, blisters should be left intact. Large or tense blis-ters can be decompressed by needle aspiration. Tetanus status should be updated according to current Centers for Disease Control and Prevention (CDC) guidelines.
Most burns managed in the outpatient setting are covered with closed dressings. The first layer should be non-adherent, porous, dry sterile gauze. This is covered with a layer of bulky gauze to absorb wound exudate, and subsequently covered with a semi-elastic wrap. Silver sul-fadiazine cream (Silvadene) is commonly used for super-ficial partial-thickness burns. A thin layer of Silvadene can be applied to non-adherent, porous sterile gauze using a tongue blade. The gauze is then applied directly to the burn ( Figure 16.8 ). In general, these dressings are changed once or twice daily, and can be removed in the shower or under running water. The burn is gently washed with mild soap and water and the old cream removed. The wound is then patted dry and re-dressed as above.
Topical antibiotic ointments (Bacitracin, Polymyxin B sulfate, Neomycin, Polysporin, Neosporin) may be applied to partial-thickness burns when Silvadene is con-traindicated, such as in patients allergic to sulfonamides, pregnant women approaching or at term, newborn infants during the first 2 months of life, or patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency. In the
Table 16.4 American Burn Association grading system for burn severity and disposition
Minor burn Moderate burn Major burn
Criteria <10% TBSA in adult 10–20% TBSA in adult >20% TBSA in adult
<5% TBSA in young (<10 years) or old (>50 years)
5–10% TBSA in young or old >10% TBSA in young or old
<2% full-thickness burn 2–5% full-thickness burn >5% full-thickness burn
High-voltage injury High-voltage burn
Suspected inhalation injury Known inhalation injury
Circumferential burn
Concomitant medical problem predisposing to infection (e.g., diabetes, sickle cell disease)
Any significant burn to face, eyes, ears, genitalia, hands, feet, or major joints
Significant associated injuries (e.g., major trauma)
Disposition Outpatient management Hospital admission Referral to burn center
From American Burn Association. Hospital and Prehospital Resources for Optimal Care of Patients with Burn Injury: Guidelines for Development and Operation of Burn Centers. J Burn Care Rehabil 1990;11:98–104.
Figure 16.8 A. Application of a thin layer of Silvadene to sterile gauze. B. Silvadene- covered sterile gauze is applied to a burn wound.
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om

Primary Complaints 217
Bu
rns
(mean 4%); however, they can be associated with signifi-cant morbidity, as they often occur in critical areas such as the face, hands and feet. Occupational injuries that occur during roofing and road paving account for the majority of tar burns.
Used commonly as a protective coating, roofing tar is generally heated to higher temperatures (232°C) than road paving tar (140°C) to achieve the desired viscosity. As a result, roofing tar burns tend to injure deeper ana-tomic structures. When tar splatters, it cools to a tempera-ture of 93°–104°C, forming a hard, water-resistant residue. Removing adherent tar without causing further damage to the underlying skin is challenging. A number of non-toxic preparations are efficacious for removing adherent tar, including Neosporin, Tween 80, moist exposed burn ointment (MEBO), De-Solv-it, NISA baby oil, butter, may-onnaise and sunflower oil.
Scald burns
Scald burns from hot liquid or steam account for more than half of all burn-related hospitalizations in the United States. Scald burns are the most common type of injury in children less than 3 years of age, accounting for approxi-mately 70% of all pediatric burns requiring hospitaliza-tion. In the elderly (age >65 years), non-fatal scald burns from hot food most commonly affect the arm and hand. Scald burns typically occur in the home, specifically the kitchen. In addition, scald burns are a common occupa-tional injury in restaurant workers. Preventive measures include avoiding mixing water with hot oil when frying, turning pot handles away from the stove’s edge, and using dry oven mitts or pot holders.
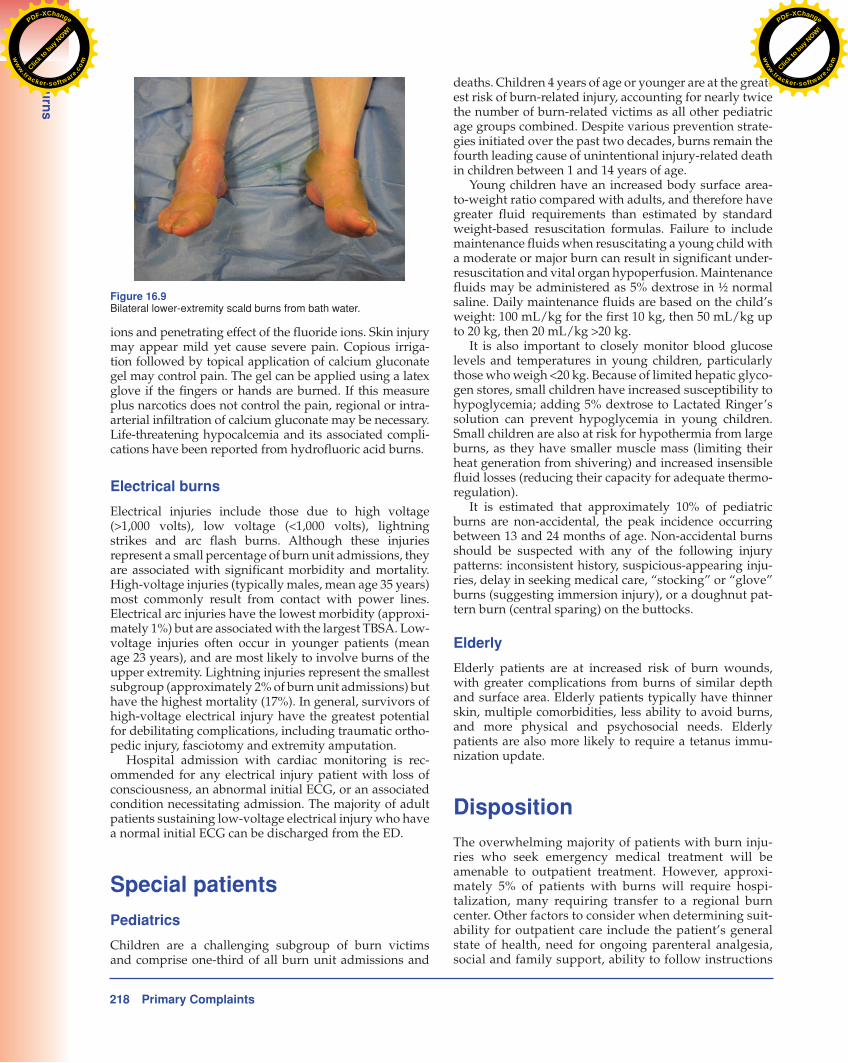
Despite being somewhat under-recognized, hot tap water is a preventable cause of scald burns ( Figure 16.9 ). Patients at greatest risk for tap water scald burns include the elderly, children <5 years of age, and those with disa-bilities. Scald burns from hot tap water are directly related to the duration of exposure. Many home water heaters are set at between 60°C and 70°C (140°F and 158°F). Exposure at these temperatures can cause full-thickness burns in less than 5 seconds. Lowering the temperature of a home water heater to 49°C (120°F) would drastically reduce the number and severity of burns from hot tap water. At this temperature, it would take between 5 and 9 minutes to cause a full-thickness injury.
Chemical burns
Chemical burns can be especially challenging to treat. Initial treatment at the scene consists of copious irrigation with water and removal of any particles. Burns due to ele-mental chemicals (e.g., lithium, sodium, magnesium and potassium) are important exceptions to irrigation with water because the resulting exothermic reaction increases the amount of burn.
Burns caused by hydrofluoric acid (a strong inorganic acid commonly found in rust removers, etching solu-tions, metal cleaners and electronics manufacturing) are extremely painful due to the corrosive effect of the hydrogen
agent over another. Topical neomycin or neomycin-containing agents (e.g., Neosporin) may cause an allergic dermatitis and should be avoided whenever possible . In recent years, newer long-acting silver impregnated and other synthetic dressings have become available.
Select outpatient burns can be managed in an “open” fashion without occlusive dressings. Wounds most com-monly treated in this fashion are superficial partial- thickness burns on the neck and face. These burns should be gently washed twice daily with soap and water, fol-lowed by application of a topical antibiotic ointment, and then left open to air. Silvadene can cause permanent silver staining of the skin and should not be used on the face.
Patients should be instructed to avoid sun exposure during wound maturation, as this may lead to permanent hyperpigmentation of newly re-epithelialized skin. After re-epithelialization occurs, an unscented moisturizing cream (such as Vaseline Intensive Care, Eucerin, or cocoa butter) should be applied to the wound until the natural lubricating mechanisms of the skin return.
Patients managed in the outpatient setting should first be reevaluated in 24–48 hours, and then every few days until the burn wounds have healed. Minor burns initially managed as an outpatient should be promptly referred to a burn specialist if re-epithelialization has not occurred within 2–3 weeks or if any complications occur.
Analgesia
The majority of burns are painful. Most outpatients can be managed with nonsteroidal antiinflammatory medica-tion with or without the addition of oral narcotic agents. Patients admitted to the hospital often require intravenous narcotic agents. Intramuscular (IM) analgesics should be administered with caution (if at all) in burn victims, as absorption is less reliable and titration is more difficult.
Antibiotics
Routine use of systemic antibiotics is not recommended for patients with acute burn injuries.
Nasogastric tube
Patients with burns ≥20% TBSA may develop a paralytic ileus; a nasogastric tube may prevent gastric distention and emesis.
Bladder catheterization
In critically ill patients, bladder catheterization and urom-eter placement is recommended to monitor urine output.
Special burns
Tar burns
Hot tar burns, while uncommon, remain a distinct and problematic injury. Tar burns typically affect a small TBSA
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om
218 Primary Complaints
Bu
rns
deaths. Children 4 years of age or younger are at the great-est risk of burn-related injury, accounting for nearly twice the number of burn-related victims as all other pediatric age groups combined. Despite various prevention strate-gies initiated over the past two decades, burns remain the fourth leading cause of unintentional injury-related death in children between 1 and 14 years of age.
Young children have an increased body surface area-to-weight ratio compared with adults, and therefore have greater fluid requirements than estimated by standard weight-based resuscitation formulas. Failure to include maintenance fluids when resuscitating a young child with a moderate or major burn can result in significant under-resuscitation and vital organ hypoperfusion. Maintenance fluids may be administered as 5% dextrose in ½ normal saline. Daily maintenance fluids are based on the child’s weight: 100 mL/kg for the first 10 kg, then 50 mL/kg up to 20 kg, then 20 mL/kg > 20 kg.
It is also important to closely monitor blood glucose levels and temperatures in young children, particularly those who weigh <20 kg. Because of limited hepatic glyco-gen stores, small children have increased susceptibility to hypoglycemia; adding 5% dextrose to Lactated Ringer’s solution can prevent hypoglycemia in young children. Small children are also at risk for hypothermia from large burns, as they have smaller muscle mass (limiting their heat generation from shivering) and increased insensible fluid losses (reducing their capacity for adequate thermo-regulation).
It is estimated that approximately 10% of pediatric burns are non-accidental, the peak incidence occurring between 13 and 24 months of age. Non-accidental burns should be suspected with any of the following injury patterns: inconsistent history, suspicious-appearing inju-ries, delay in seeking medical care, “stocking” or “glove” burns (suggesting immersion injury), or a doughnut pat-tern burn (central sparing) on the buttocks .
Elderly
Elderly patients are at increased risk of burn wounds, with greater complications from burns of similar depth and surface area. Elderly patients typically have thinner skin, multiple comorbidities, less ability to avoid burns, and more physical and psychosocial needs. Elderly patients are also more likely to require a tetanus immu-nization update.
Disposition
The overwhelming majority of patients with burn inju-ries who seek emergency medical treatment will be amenable to outpatient treatment. However, approxi-mately 5% of patients with burns will require hospi-talization, many requiring transfer to a regional burn center. Other factors to consider when determining suit-ability for outpatient care include the patient’s general state of health, need for ongoing parenteral analgesia, social and family support, ability to follow instructions
ions and penetrating effect of the fluoride ions. Skin injury may appear mild yet cause severe pain. Copious irriga-tion followed by topical application of calcium gluconate gel may control pain. The gel can be applied using a latex glove if the fingers or hands are burned. If this measure plus narcotics does not control the pain, regional or intra-arterial infiltration of calcium gluconate may be necessary. Life-threatening hypocalcemia and its associated compli-cations have been reported from hydrofluoric acid burns.
Electrical burns
Electrical injuries include those due to high voltage (>1,000 volts), low voltage (<1,000 volts), lightning strikes and arc flash burns. Although these injuries represent a small percentage of burn unit admissions, they are associated with significant morbidity and mortality. High-voltage injuries (typically males, mean age 35 years) most commonly result from contact with power lines. Electrical arc injuries have the lowest morbidity (approxi-mately 1%) but are associated with the largest TBSA. Low-voltage injuries often occur in younger patients (mean age 23 years), and are most likely to involve burns of the upper extremity. Lightning injuries represent the smallest subgroup (approximately 2% of burn unit admissions) but have the highest mortality (17%). In general, survivors of high-voltage electrical injury have the greatest potential for debilitating complications, including traumatic ortho-pedic injury, fasciotomy and extremity amputation.
Hospital admission with cardiac monitoring is rec-ommended for any electrical injury patient with loss of consciousness, an abnormal initial ECG, or an associated condition necessitating admission. The majority of adult patients sustaining low-voltage electrical injury who have a normal initial ECG can be discharged from the ED.
Special patients
Pediatrics
Children are a challenging subgroup of burn victims and comprise one-third of all burn unit admissions and
Figure 16.9 Bilateral lower-extremity scald burns from bath water.
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om
Primary Complaints 219
Bu
rns
References
1. Arnoldo B , Klein M , Gibran NS . Practice guidelines for the management of electrical injuries . J Burn Care Res 2006 ; 27 : 436 –47.
2. Ayers DE , Kay AR . Management of burns in the wilderness . Travel Med Infect Dis 2005 ; 3 (4): 239 –48.
3. Baruchin AM , Schraf S , Rosenberg L . Hot bitumen burns: 92 hospitalized patients . Burns 1997 ; 23 (5): 438 –41.
4. Burn injuries in child abuse . US Department of Justice, Office of Justice Programs, Washington, DC, 2001 .
5. Duffy BJ , McLaughlin PM , Eichelberger MR . Assessment, triage, and early management of burns in children . Clin Pediatr Emerg Med 2006 ; 7 (2): 82 –93.
6. Gomez R , Leopoldo CC . Management of burn wounds in the emergency department . Emerg Med Clin North Am 2007 ; 25 (1): 135 –46.
7. Hagstrom M , Wirth GA , Evans GRD , et al. A review of emergency department fluid resuscitation of burn patients transferred to a regional, verified burn center . Ann Plast Surg 2003 ; 51 (2): 173 –6.
8. Hampson NB . Pulse oximetry in severe carbon monoxide poisoning . Chest 1998 ; 114 (4): 1036 –41.
9. Hettiaratchy S , Papini R . Initial management of a major burn: I – Overview . BMJ 2004 ; 328 (7455): 1555 –7.
10. Huyer DW , Corkum SH . Reducing the incidence of tap-water scalds: Strategies for the physician . Can Med Assoc J 1997 ; 156 (6): 841 –4.
11. Moss LS . Outpatient management of the burn patient . Crit Care Nurs Clin North Am 2004 ; 16 (1): 109 –17.
12. National Burn Registry 2005 Report . American Burn Association, Chicago, IL, 2006 .
13. Nonfatal scald-related burns among adult aged ≥ 65 years – United States 2001–2006. MMWR Morb Mortal Wkly Rep 2009 ; 58 (36): 993 –6.
14. Purdue GF , Hunt JL , Burris AM . Pediatric burn care . Clin Pediatr Emerg Med 2002 ; 3 (1): 76 –84.
15. Runyan CW , Casteel C , Perkis D , et al. Unintentional injuries in the home in the United States . Am J Prev Med 2005 ; 28 (1): 80 –7.
16. Sheridan RL . Burns . Crit Care Med 2002 ; 30 (11): S500 –14.
17. Singer AJ , Dagum AB . Current management of acute cutaneous wounds . N Engl J Med 2008 ; 359 (10): 1037 –46.
18. Thombs BD , Singh VA , Halonen J , et al. The effects of preexisting medical comorbidities on mortality and length of hospital stay in acute burn injury . Ann Surg 2007 ; 245 (4): 629 –34.
19. Tomkins D , Rossi LA . Care of outpatient burns . Burns 2004 ; 30 (8): A7 –9.
20. US Fire Administration/National Fire Data Center . Fire in the United States 1995–2004, 14th ed. US Department of Homeland Security, Federal Emergency Management Agency, August 2007 . Available at: http://www.usfa.dhs.gov/downloads/pdf/publications/fa-311.pdf (accessed January 6, 2011).
and perform dressing changes, and access to follow-up health care.
Several questions should be asked when considering a patient for outpatient care:
1. Does the patient have an adequate home environment suitable for outpatient care?
2. Is the patient capable of caring for the burn at home? 3. Are friends or family members available to assist
with burn care or activities of daily living? 4. Does the patient have the financial means to be cared
for as an outpatient? 5. Is the patient able to follow up as instructed,
including transportation to and from follow-up appointments?
6. Do any psychosocial factors exist that may decrease suitability for outpatient burn care?
Pearls, pitfalls and myths
• Residential fires are the leading cause of fire-related deaths, accounting for approximately 75% of fire-related injuries.
• Patients involved in a closed-space fire or explosion are at risk of inhalation injury.
• Complaints of headache or dizziness in the context of a fire or burn injury suggest concomitant CO toxicity.
• Even experienced clinicians are not always able to accurately determine the depth of the burn, including differentiating between a deep partial-thickness and full-thickness burn at the time of injury.
• Intravenous fluid resuscitation should be initiated in adults with partial- or full-thickness TBSA burns >20%, in older children with burns ≥15% TBSA, and in infants with burns ≥10% TBSA.
• Lactated Ringer’s solution is the most commonly used fluid for burn resuscitation.
• The Parkland formula calls for the administration of 4 mL/kg of body weight per %TBSA burn (partial- or full-thickness burns) of intravenous fluid over the first 24 hours (half over the initial 8 hours and the remainder over the next 16 hours).
• Direct thermal injury predominantly affects upper airway structures. Injury to the lower airway typically occurs due to inhalation of toxic gases and particulate matter.
• Wound care principles for minor wounds can be applied to patients with minor burns.
• Silver sulfadiazine cream (Silvadene) is most commonly used with closed burn dressings for the management of superficial partial-thickness burns. It should be avoided on the face, in infants, in late-term pregnancy, or in those with sulfonamide allergy or G6PD deficiency.
• Young children have an increased body surface area to weight ratio compared with adults, therefore requiring greater fluid than determined with the use of standard weight-based resuscitation formulas.
Click t
o buy NOW!
PDF-XChange
ww
w.tracker-software
.comClic
k to buy N
OW!PDF-XChange
ww
w.tracker-software.c
om