breath testing in the presence of chronic respiratory disease · breath test, a number of drivers...
TRANSCRIPT

Breath testing in the presence of chronic respiratory
disease
Dr M orris Odell*, Dr Christine M cDonald**, John Farrar B.*** and Jeff Pretto**
* Victorian Institute o f Forensic Medicine
**Austin and Repatriation Medical Centre
***Traffic Alcohol SectionVictoria Police
ABSTRACT
The presence of chronic respiratory disease is sometimes claimed as a defence by drivers who
refuse or fail a breath test. Trials were conducted with two instruments used in Victoria in
order to determine the effort required for a satisfactory test. Patients with restrictive and
obstructive conditions participated in the trial which was conducted at the respiratory unit o f a
large hospital. The results are presented. They provide information useful in refuting defenses
o f inability to provide a breath sample due to respiratory incapacity.
INTRODUCTION
In Victoria, breath testing for alcohol is carried out under provisions of the Road Safety A ct
1986 (Ref 7) . This act provides for compulsory breath testing o f drivers under certain
circumstances. W hile inability to provide a suitable sample results in a blood sample being
required, refusal to provide a breath sample is an offence under the act and carries a heavy
penalty.
Notwithstanding the requirement for a blood sample to be provided in the event o f a failed
breath test, a num ber o f drivers have attempted to use the presence of chronic respiratory
disease as a defence against the charge of refusing a breath test. This trial was carried out in
an attempt to quantify the minimum respiratory effort required for a satisfactory breath test in
order that such defences could be evaluated in the light of formal respiratory function testing.
- 3 29-
Two instruments are used by Victoria Police for conducting breath tests. These are the Lion
Alcometer SD2, a portable hand-held device used for screening tests, and the Drager Alcotest
7110 which is a precision instrument used to provide evidentiary print-outs accepted by the
courts. The Drager Alcotest 7110 has been in use in Victoria since 1994 and is a substantially
different instrument to one with the same name used in other jurisdictions (Ref 2). Each of
the two instruments contains sensors and circuitry for the purpose of determining when an
adequate breath sample has been provided and will not produce a reading unless their criteria
have been satisfied.
The Lion Alcotest uses a simple timer to define the sampling interval. The timer is started
once the breath flow exceeds a trigger level and runs for 2.7 seconds. There is no check on
whether flow continues during the delay period. Flow characteristics are defined by the
disposable plastic tubular mouthpiece which are mass produced in large numbers with a high
degree of reproducibility. The Drager Alcometer is a complex microprocessor controlled
instrument which progressively displays a row of asterisks as the subject exhales, a
satisfactory effort being indicated by 16 asterisks appearing .
Studies with instruments formerly used for breath analysis have concluded that persons
unable to provide a breath sample for analysis because of respiratory impairment would be so
severely affected that they would be incapable of driving, thus rendering the need for breath
testing superfluous. These have always required a respiratory effort which has been great
enough to exclude a significant number of drivers from being able to provide a breath
specimen. In fact, formal guidelines for assessment o f suitability for driving are quite tolerant
o f remarkably high levels of impairment.(Ref 8,9) The Victorian guidelines allow m otor car
drivers to exhibit a high level of impairment even to the extent of requiring intranasal oxygen.
The commercial vehicle guidelines are even less specific, only citing “severe respiratory
failure” as an exclusion. Thus it is possible for persons with various types o f advanced
respiratory disease to be driving cars and heavy commercial vehicles.
PROCEDURE
The study was conducted in two stages. The first stage involved a comparison of six Drager
units to determine whether there were significant differences in the volume required to
- 330-
achieve a satisfactory sample as indicated by 16 asterisks on the unit’s display panel. This
was done in order to check that the machines were substantially identical and that the
remainder o f the trial could be conducted using only one machine.
The minimum volume required to provide an adequate sample for the Drager units was
measured using a 3-litre graduated calibration syringe (Hans Rudloph model XXXX) with a
resolution of 25 millilitres. The procedure involved manually injecting air at room
temperature (23 degC) at a rate of approximately 100 - 150 ml/sec until an adequate sample
was provided (ie when the 16th asterisk was illuminated), and noting the injected volume.
This procedure was measured in triplicate in each of 6 Drager units. The mean minimum
sample volume thus measured was 840 ml with a range of 775 - 925 mis.
Staff from the Austin & Repatriation Medical Centre (ARMC ) attended a Police Random
Breath Testing Station to observe police breath testing procedures. This was done to ensure
that trial conditions mimicked field conditions as much as possible. Ethics committee
approval was obtained prior to patients attending the Respiratory Laboratory at the ARM C for
routine respiratory function testing being recruited for the study. Criteria for eligibility were:
1. No alcohol to have been consumed on the day o f the test
2. Known respiratory disability, as reflected by an FEV1 of less than or equal to 1.5 litres
(Refs 1,2,4) and one or more of the following ventilatory abnormalities:
a) an obstructive ventilatory defect secondary to asthma or COPD
b) a restrictive ventilatory defect secondary to neuromuscular disease affecting the
respiratory musculature
c) a restrictive ventilatory defect secondary to some form of diffuse interstitial lung
disease.
Informed consent was sought and the patient then asked to blow into each device using the
standard instructions used by the police in the field. In accordance with police practice,
subjects who failed an initial test were asked to repeat it up to 3 times. Information gathered
was:
• Age and sex of patient
• Type of respiratory problem
• Result o f respiratory function tests
-331 -
• Result o f attempt to blow into a Lion Alcometer (Pass/Fail)
• Result o f attempt to blow into a Drager Alcotest (Pass/Fail/no o f asterisks achieved)
Statistical analysis was performed using SPSS for W indows Version 6 .1
RESULTS
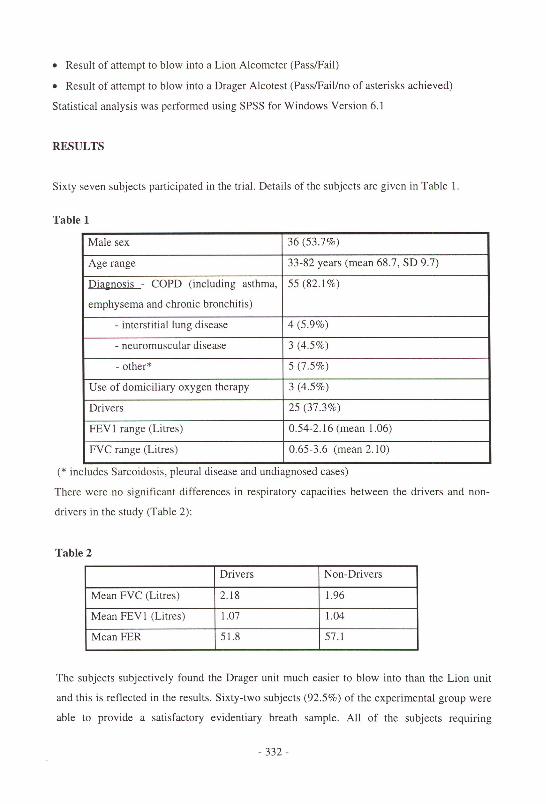
Sixty seven subjects participated in the trial. Details of the subjects are given in Table 1.
Table 1
Male sex 36 (53.7%)
Age range 33-82 years (mean 68.7, SD 9.7)
Diagnosis - COPD ("including asthma,
emphysema and chronic bronchitis)
55 (82.1%)
- interstitial lung disease 4 (5.9%)
- neuromuscular disease 3 (4.5%)
- other* 5 (7.5%)
Use of domiciliary oxygen therapy 3 (4.5%)
Drivers 25 (37.3%)
F E V 1 range (Litres) 0.54-2.16 (mean 1.06)
FVC range (Litres) 0.65-3.6 (mean 2.10)
(* includes Sarcoidosis, pleural disease and undiagnosed cases)
There were no significant differences in respiratory capacities between the drivers and non
drivers in the study (Table 2 ):
Table 2
Drivers Non-Drivers
M ean FVC (Litres) 2.18 1.96
M ean FEV 1 (Litres) 1.07 1.04
Mean FER 51.8 57.1
The subjects subjectively found the Drager unit much easier to blow into than the Lion unit
and this is reflected in the results. Sixty-two subjects (92.5%) of the experimental group were
able to provide a satisfactory evidentiary breath sample. All o f the subjects requiring
- 332 -
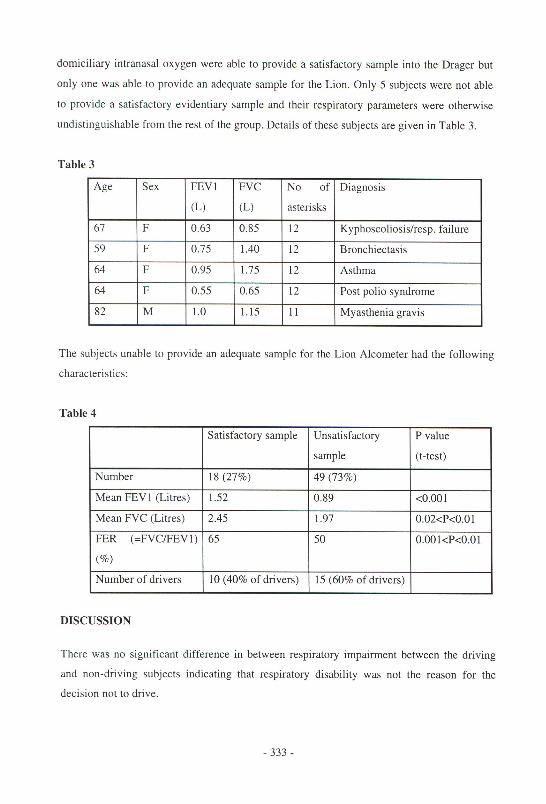
domiciliary intranasal oxygen were able to provide a satisfactory sample into the Drager but
only one was able to provide an adequate sample for the Lion. Only 5 subjects were not able
to provide a satisfactory evidentiary sample and their respiratory parameters were otherwise
undistinguishable from the rest of the group. Details of these subjects are given in Table 3.
Table 3
Age Sex FEV1
(L)
FVC
(L)
No of
asterisks
Diagnosis
67 F 0.63 0.85 1 2 Kyphoscoliosis/resp. failure
59 F 0.75 1.40 1 2 Bronchiectasis
64 F 0.95 1.75 1 2 Asthma
64 F 0.55 0.65 1 2 Post polio syndrome
82 M 1 . 0 1.15 1 1 Myasthenia gravis
The subjects unable to provide an adequate sample for the Lion Alcometer had the following
characteristics:
Table 4
Satisfactory sample Unsatisfactory
sample
P value
(t-test)
Number 18 (27%) 49 (73%)
Mean FE V 1 (Litres) 1.52 0.89 <0 . 0 0 1
Mean FVC (Litres) 2.45 1.97 0.02<P<0.01
FER (=FVC/FEV1)
(%)
65 50 0.001<P<0.01
Num ber o f drivers 10 (40% of drivers) 15 (60% o f drivers)
DISCUSSION
There was no significant difference in between respiratory impairment between the driving
and non-driving subjects indicating that respiratory disability was not the reason for the
decision not to drive.
- 333 -
These results are broadly similar to those obtained in other studies. The Lion Alcometer is
widely used and is accepted as evidentiary in some jurisdictions. It requires a greater
respiratory effort than more modern instruments and a significant number of drivers are not
able to provide a satisfactory breath sample for this device. Commonly measured respiratory
parameters may be helpful in assessing claimed inability to blow into this device.
The number o f subjects who could not provide a satisfactory sample for the Drager machine
was very low and not enough for formal statistical evaluation. It would appear however that
the Drager machine used in Victoria is able to be used at the limits o f respiratory function
likely to be encountered in drivers.
REFERENCES
1. Briggs J E, Patel H, Butterfield K, Honeybourne D "The effects of chronic obstructive airways disease on the ability to drive and use a roadside alcometer” Resp. Med. (1990) 84:43-46
2. Crockett AJ, Schembri D A, Smith D J, Laslett R, Alpers J H “M inimum respiratory function for breath testing in South Australia” J. Forens Sci Soc (1992) 32(4):349-56
3. Morris MJ “Alcohol breath testing in patients with respiratory disease” (editorial) Thorax (1990) 45:717-721
4. Gomm P J, Osselton M D, Broster C G, Johnson N M cl, Upton K “Study into the ability o f patients with impaired lung function to use breath alcohol testing devices” Med. Sci. Law (1991) 31:221-225
5. Gomm P J, Osselton M D, Broster C G, Johnson N M cl, Upton K “The Effect of Salbutamol on Breath Alcohol Testing in Asthmatics” Med. Sci. Law (1991) 31:226-228
6 . Marks P “Drink Driving Legislation: Medicine and the Law” Medico-Legal Journal 63/3:119-127
7. “Road Safety Act 1986” No 127/1986 Victorian Government Printer, Melbourne.
8 . “Interim General Driver Licensing Guidelines” Vicroads 1994
9. “Medical Examination o f Commercial vehicle Drivers” Federal Office of Road Safety 1994
- 334 -