breast cancer and pregnancy -...
TRANSCRIPT

BREAST CANCER AND PREGNANCY
F. Cardoso, MDDirector, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal
ESO Breast Cancer Program CoordinatorESMO Board of Directors & NR Committee Chair
EORTC Breast Group Past-Chair
www.abc-lisbon.org
DISCLOSURES
Consultant/Ad Board:
Amgen, Astellas/Medivation, AstraZeneca, Celgene, Daiichi-Sankyo,
Eisai, GE Oncology, Genentech, GlaxoSmithKline, Macrogenics,
Merck-Sharp, Merus BV, Mylan, Mundipharma, Novartis, Pfizer,
Pierre-Fabre, Roche, Sanofi, Seattle Genetics, Teva
PREGNANCY AFTER BREAST CANCER
SAFE?
• Same risk of recurrence and death• Even in Luminal Breast Cancers
YES
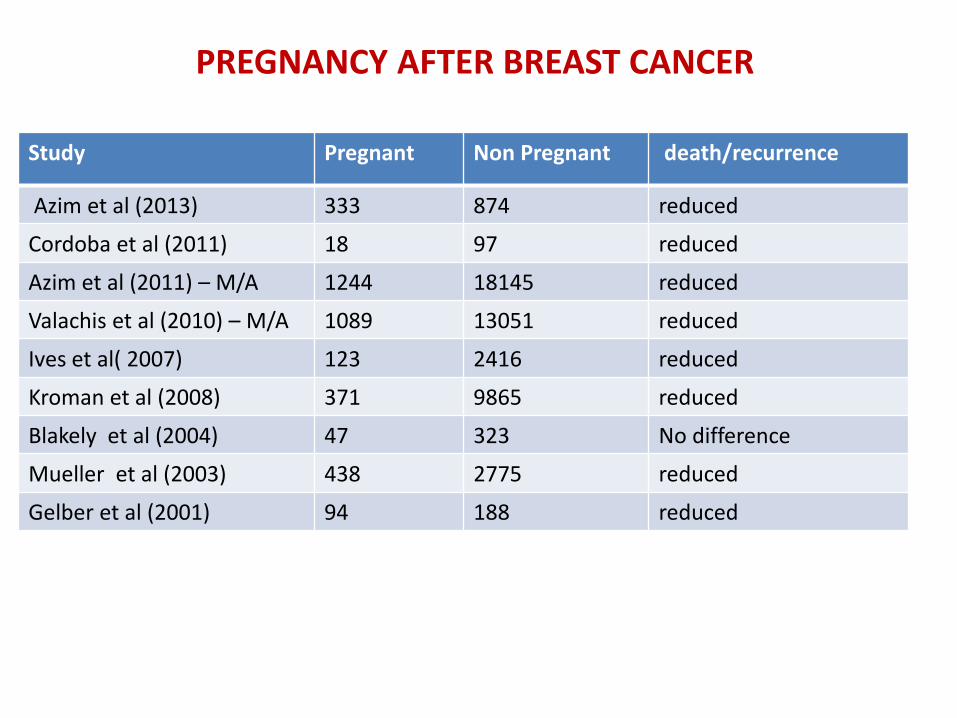
death/recurrenceNon PregnantPregnantStudy
reduced874333Azim et al (2013)
reduced9718Cordoba et al (2011)
reduced181451244Azim et al (2011) – M/A
reduced130511089Valachis et al (2010) – M/A
reduced2416123Ives et al( 2007)
reduced9865371Kroman et al (2008)
No difference32347Blakely et al (2004)
reduced2775438Mueller et al (2003)
reduced18894Gelber et al (2001)
PREGNANCY AFTER BREAST CANCER

Differences in DFS between the pregnant group and matched non-
pregnant group
Azim H A et al. JCO 2013;31:73-79

SUPPORTIVE CARE
Pregnancy after breast cancer should not be discouraged even inpatients with HR positive disease, although all available data havelimitations.
PREGNANCY AFTER BREAST CANCER
Prospective data from a global clinical trial are being collected (POSITIVE Trial).
• What is the ideal interval between ET interruption and pregnancy?
• When is it considered safe to interrupt ET?
• What is the impact of different ETs in fertility?
Tamoxifen
Ovarian Function Suppression
Open questions
PREGNANCY AFTER BREAST CANCER
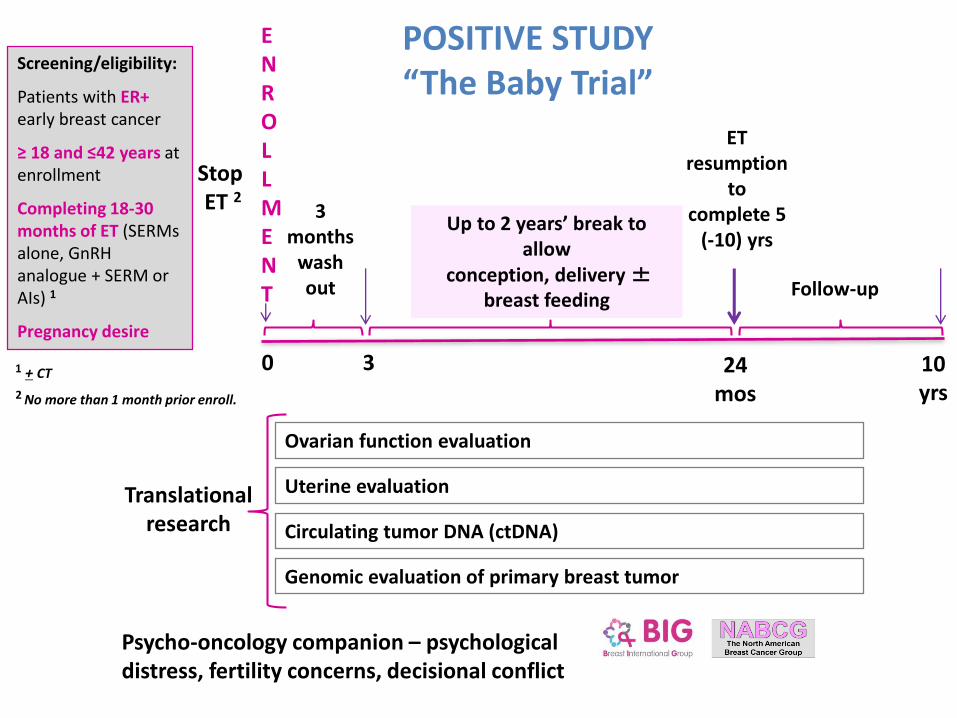
1 + CT
StopET 2
Up to 2 years’ break to allow
conception, delivery ±breast feeding
Follow-up
Screening/eligibility:
Patients with ER+early breast cancer
≥ 18 and ≤42 years at enrollment
Completing 18-30 months of ET (SERMs alone, GnRH analogue + SERM or AIs) 1
Pregnancy desire
0
ENROLLMENT
3
3 months
wash out
24 mos
ET resumption
to complete 5
(-10) yrs
10 yrs2 No more than 1 month prior enroll.
Translational research
Ovarian function evaluation
Uterine evaluation
Genomic evaluation of primary breast tumor
Circulating tumor DNA (ctDNA)
POSITIVE STUDY“The Baby Trial”
Psycho-oncology companion – psychological distress, fertility concerns, decisional conflict
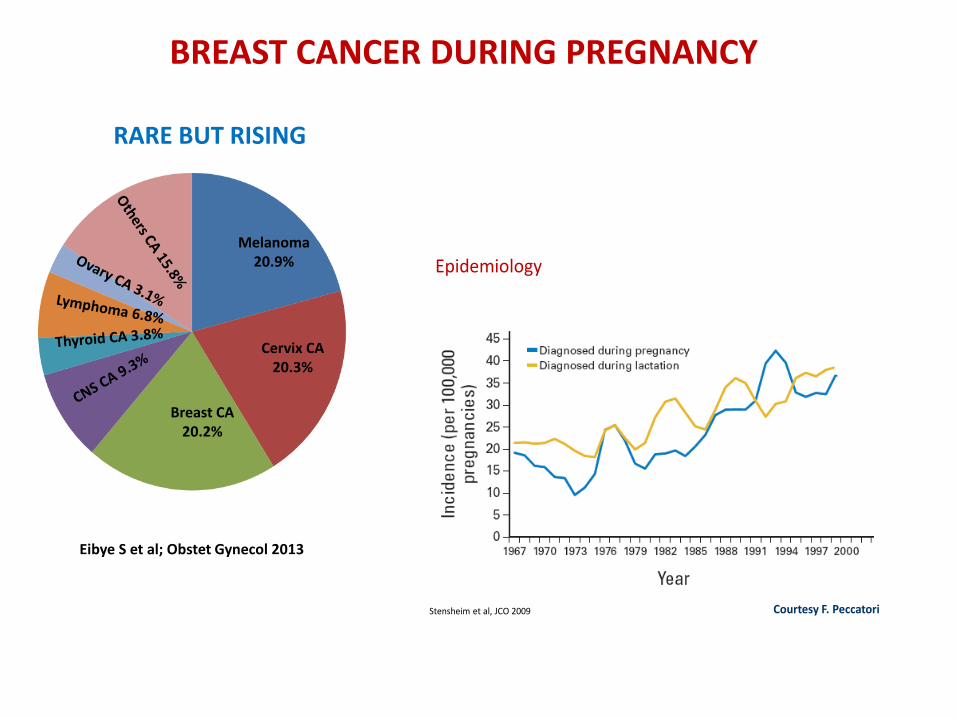
BREAST CANCER DURING PREGNANCY
RARE BUT RISING
Eibye S et al; Obstet Gynecol 2013
Melanoma20.9%
Cervix CA20.3%
Breast CA 20.2%
Stensheim et al, JCO 2009
Epidemiology
Courtesy F. Peccatori
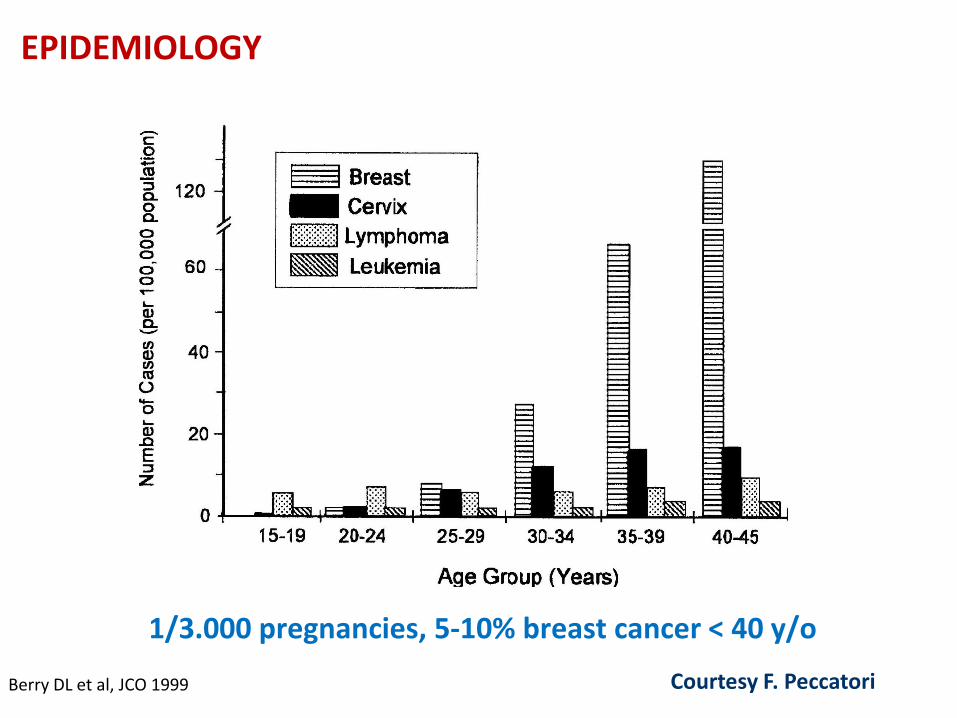
Berry DL et al, JCO 1999
EPIDEMIOLOGY
1/3.000 pregnancies, 5-10% breast cancer < 40 y/o
Courtesy F. Peccatori
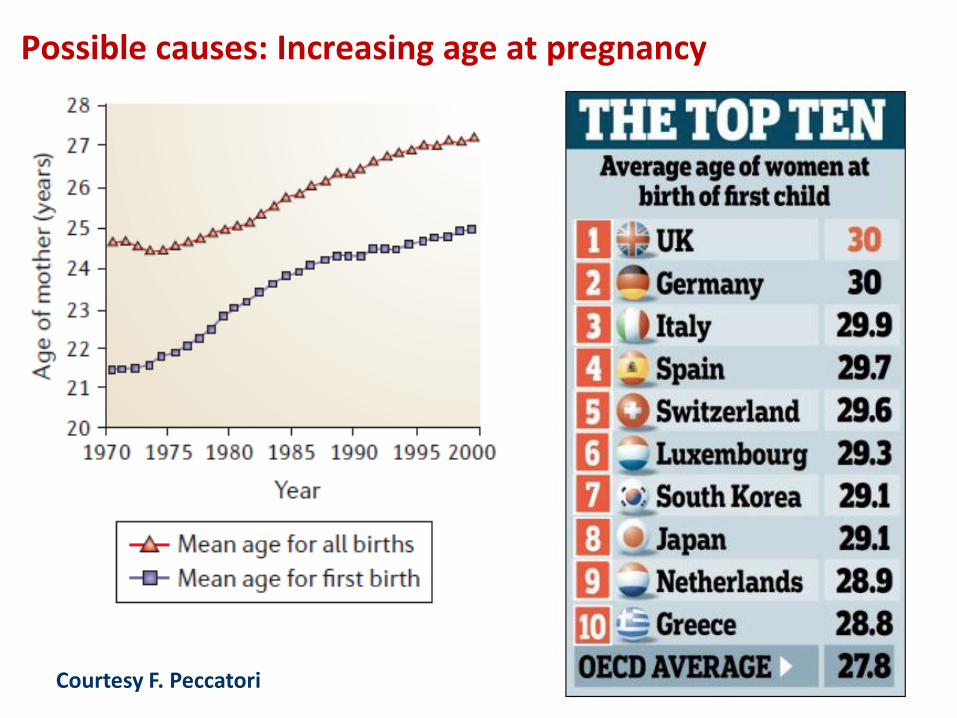
Possible causes: Increasing age at pregnancy
Courtesy F. Peccatori
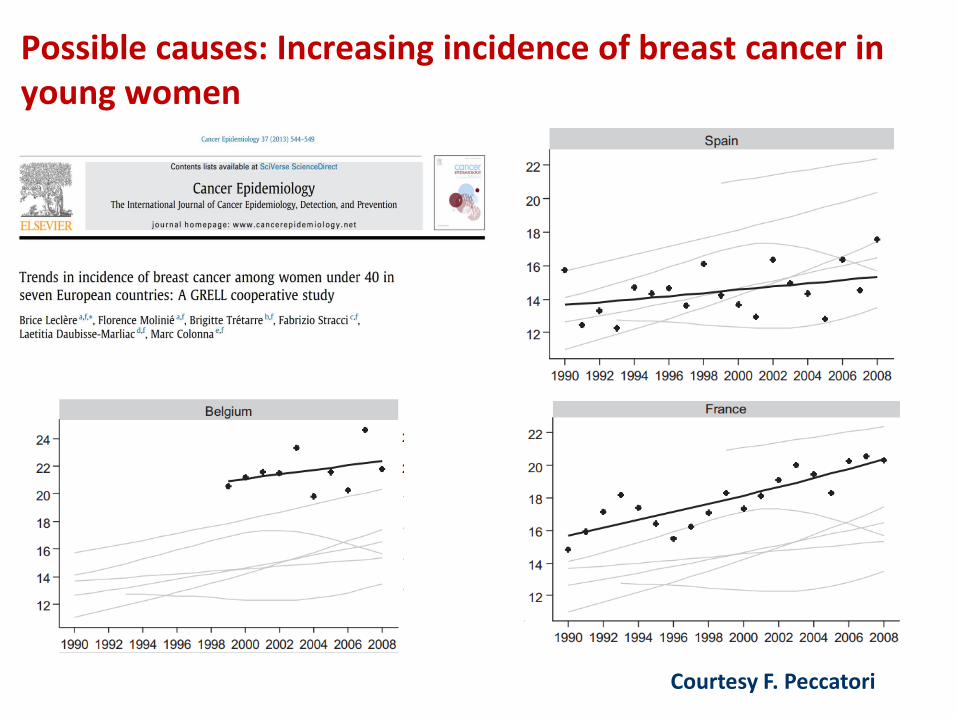
Possible causes: Increasing incidence of breast cancer in young women
Courtesy F. Peccatori

Incidence
✓ Possible absolute increase, at least in some countries
✓ Probable relative increase in countries with high percentage of young women
✓ Relative increase in countries where HRT dependent postmenopausal breast cancer is decreasing (e.g. US)
Courtesy F. Peccatori
Matching variables (1 case: 2 controls)
Age (±2 years)
Year of surgery (±2 years)
pT (1a vs. 1b vs. 1c vs. 2 vs. 3 vs. X)
# of positive nodes (0 vs. 1-3 vs. 4-9 vs. 10+)
Neoadjuvant chemotherapy (Yes vs. No)
Azim HA Jr et al; Acta Oncol 2012

Pregnant CasesN = 65
ControlsN = 130
Age (years)
< 3535-39≥ 40
20 (30.8)33 (50.8)12 (18.5)
41 (31.5)61 (46.9)28 (21.5)
Median 36 (28-47) 36 (28-47)
Year of Surgery
1996 - 20032004 - 20052006 - 20082009 - 2010
16 (24.6)20 (30.8)16 (24.6)13 (20.0)
37 (28.5)35 (26.9)36 (27.7)22 (16.9)
Median 2005 2005
pT
1a-b1c23X
5 (7.6)21 (32.3)31 (47.7)6 (9.2)2 (3.1)
10 (7.6)42 (32.3)62 (47.7)12 (9.2)4 (3.1)
pN
pN0pN1pN2pN3pNx
28 (43.1)19 (29.2)10 (15.4)6 (9.2)2 (3.1)
56 (43.1)38 (29.2)20 (15.4)12 (9.2)4 (3.1)
Azim HA Jr et al; Acta Oncol 2012
Clinical characteristics
Courtesy F. Peccatori

Estrogen Receptor
PresentAbsent
43 (66.1)22 (33.9)
98 (75.4)32 (24.6)
0.175
ProgesteronReceptor
PresentAbsent
42 (64.6)23 (35.4)
87 (66.9)43 (33.1)
0.748
Grade123
4 (7.5)18 (34.0)31 (58.5)
4 (3.6)43 (39.1)63 (57.3)
0.503
Ki-67 %< 20≥ 20
18 (28.6)45 (71.4)
30 (23.4)98 (76.6)
0.442
Her2/neuNegative Positive
54 (83.1)11 (16.9)
103 (81.1)24 (18.9)
0.737
Perivascular Invasion
Absent Present
31 (47.7)34 (52.3)
70 (55.1)57 (44.9)
0.330
Molecular subtypes
Luminal ALuminal BHer2/NeuTriple Negative
8 (12.3)37 (56.9)6 (9.2)
14 (21.5)
13 (10.3)82 (65.1)4 (3.2)
27 (21.4)
0.306
ControlsN = 130
p
Azim HA Jr et al; Acta Oncol 2012
Pregnant CasesN = 65
Biological characteristics: no major differences
ControlsN = 130
Courtesy F. Peccatori

Chi-square: p=0.68
Basal Luminal-A Luminal-B HER2
Azim HA Jr et al; Acta Oncol 2012
Molecular subtypes (IHC): similar distribution
Courtesy F. Peccatori

Azim HA Jr et al; Endocrine Rel Cancer 2014Courtesy F. Peccatori
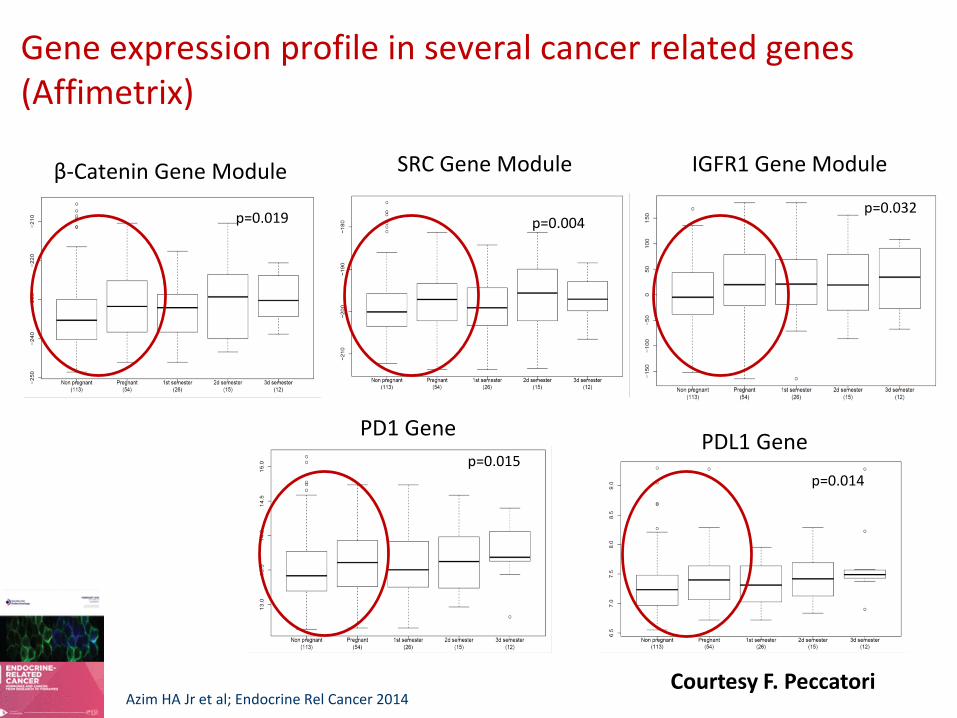
SRC Gene Module
p=0.004
β-Catenin Gene Module
p=0.019
Gene expression profile in several cancer related genes (Affimetrix)
IGFR1 Gene Module
p=0.032
PDL1 GenePD1 Gene
p=0.015p=0.014
Azim HA Jr et al; Endocrine Rel Cancer 2014Courtesy F. Peccatori

...but the same happens in normal (mouse) breast during pregnancy
SRC Gene Module
β-Catenin Gene Module
PD1 Gene
p=0.001p=0.035
p=0.008
IGF1 Gene Module
p=0.004
Azim HA Jr et al; Endocrine Rel Cancer 2014Courtesy F. Peccatori
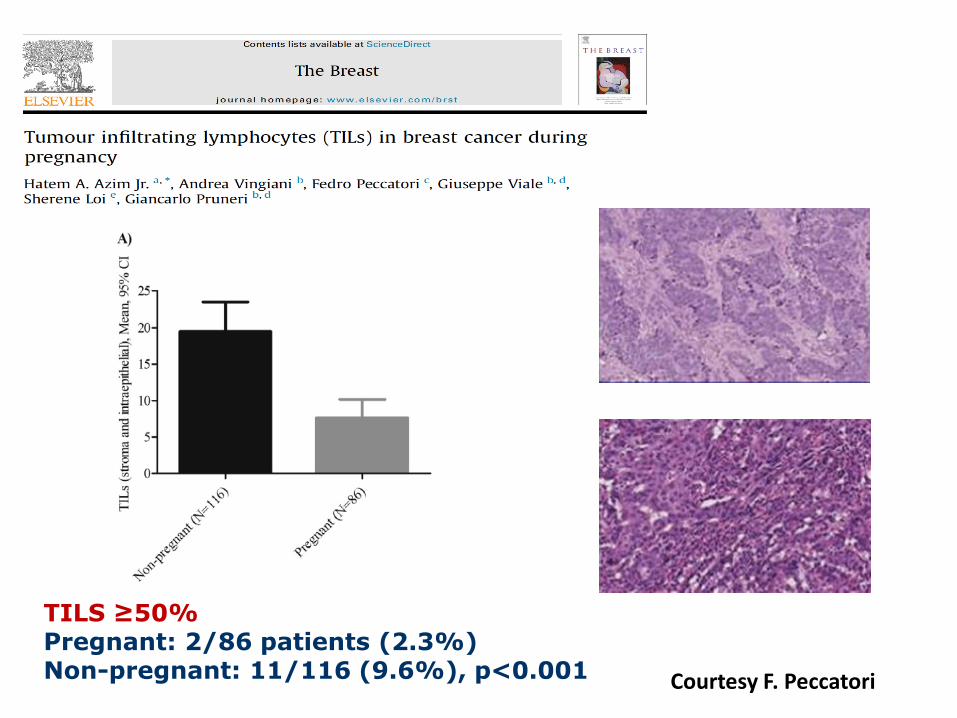
TILS ≥50%Pregnant: 2/86 patients (2.3%)Non-pregnant: 11/116 (9.6%), p<0.001 Courtesy F. Peccatori
MAIN MESSAGE
TREATMENT MUST BE PERFORMED IN A SPECIALISED CENTER BY AN EXPERIENT
MULTIDISCIPLINARY TEAM!
Managing Breast Cancer during Pregnancy

FIRST QUESTION:TO CONTINUE OR TO STOP THE PREGNANCY?
• Only when diagnosis happens very early (first trimester) this hypothesis needs consideration
• However, this is always a parents decision (independently of the time of pregnancy)
• NO IMPACT ON PROGNOSIS
BREAST CANCER DURING PREGNANCY

Azim HA Jr et al; Acta Oncol 2012
INTERRUPTING THE PREGANCY DOESN’T ADD ANYBENEFIT TOTHE MOTHER
BREAST CANCER DURING PREGNANCY
1st QUESTION:To Continue or To Stop the Pregnancy?
If the decision is to continue pregnancy:
1st MAIN MESSAGE:
AVOID PREMATURE DELIVERY!
2nd MAIN MESSAGE:
TREAT AS YOU WOULD IN A NON-PREGNANT CASE (only few exceptions: ET, anti-HER2)
BREAST CANCER DURING PREGNANCY
ULTRASSOUND: YESMRI WITHOUT CONTRAST
MAMMOGRAPHY: IF INDISPENSABLERX: YES BUT PREFERABLE AFTER DELIVERY
BONE SCAN, CTs, PETs: NO
2nd QUESTION:Which type of exams can you perform during pregnancy?
BREAST CANCER DURING PREGNANCY

SURGERY: YESCHEMOTHERAPY: YES
RADIOTHERAPY: Yes, with protection but preferable after deliveryHormonal and biological treatments: NO
3th QUESTION:Which type of treatments are possible during pregnancy?
BREAST CANCER DURING PREGNANCY

BREAST CANCER DURING PREGNANCY
• Breast Conservative Surgery is possible and preferable. Identical indications as in non-pregnant women.
• Sentinel node biopsy is feasible but without using blue dye. Radioisotope dosing should be the minimum possible.
SURGERY
No difference in the surgical approach of breast cancer during pregnancy, but:
- careful anesthesiological evaluation- fetal monitoring, when appropriate
SURGERY
Pic
ture
co
urt
esy
of
Pro
f F
Am
ant
Courtesy F. Peccatori

Lymphatic mapping
Dosimetry studies in non-pregnant women:10 MBq fetal exposure < 0.1 mGy
SNB with radioactivelymphatic mapping is safe !
Gentilini O et al, Ann Oncol 2004;15:1348ff
Sentinel node sampling during pregnancy is safe
Courtesy F. Peccatori

Breast reconstruction during pregnancy is safe
• Usually contra-indicated
• Associated to serious adverse impact on the fetus
• Wait until after delivery (no problem with the needed time)
RADIOTHERAPY
BREAST CANCER DURING PREGNANCY

SYSTEMIC TREATMENTS: crucial importance of GESTACIONAL AGE
BREAST CANCER DURING PREGNANCY
1st TRIMESTER – Risk of malformations is 20%
Cardonick E & Iacobucci; Lancet Oncol 2004

The placenta
CHEMOTHERAPY DURING PREGNANCY
Courtesy F. Peccatori

SYSTEMIC TREATMENT: CHEMOTHERAPY
Number of patients
drug in the fetus (n) % drug in the fetus
Doxorubicin 15 6 7.5 ± 3.2
Epirubicina 11 8 4.0 ± 1.6
Paclitaxel 11 7 1.4 ± 0.8
Docetaxel 9 0 0
Ciclofosfamide 4 3 25.1 ± 6.3
Carboplatin 7 7 57.5 ± 14.2
PLACENTAL ROLE!
van Calsteren et al; Acta Obstet Gynecol 2011van Calsteren et al; Gynecol Oncol 2011
PACLITAXELEPIRUBICIN
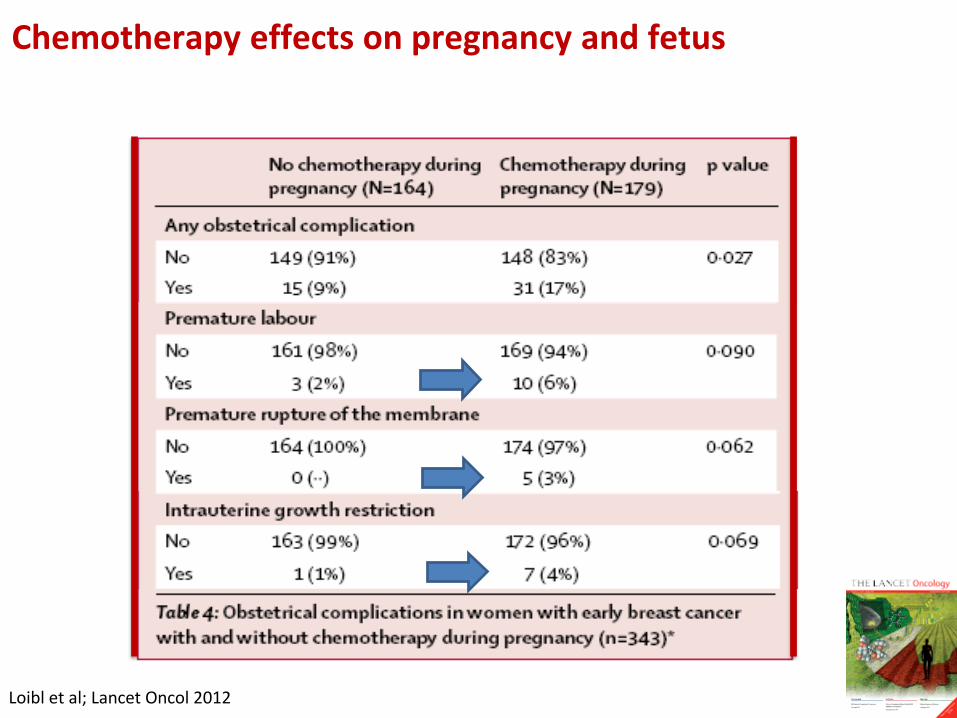
Loibl et al; Lancet Oncol 2012
Chemotherapy effects on pregnancy and fetus
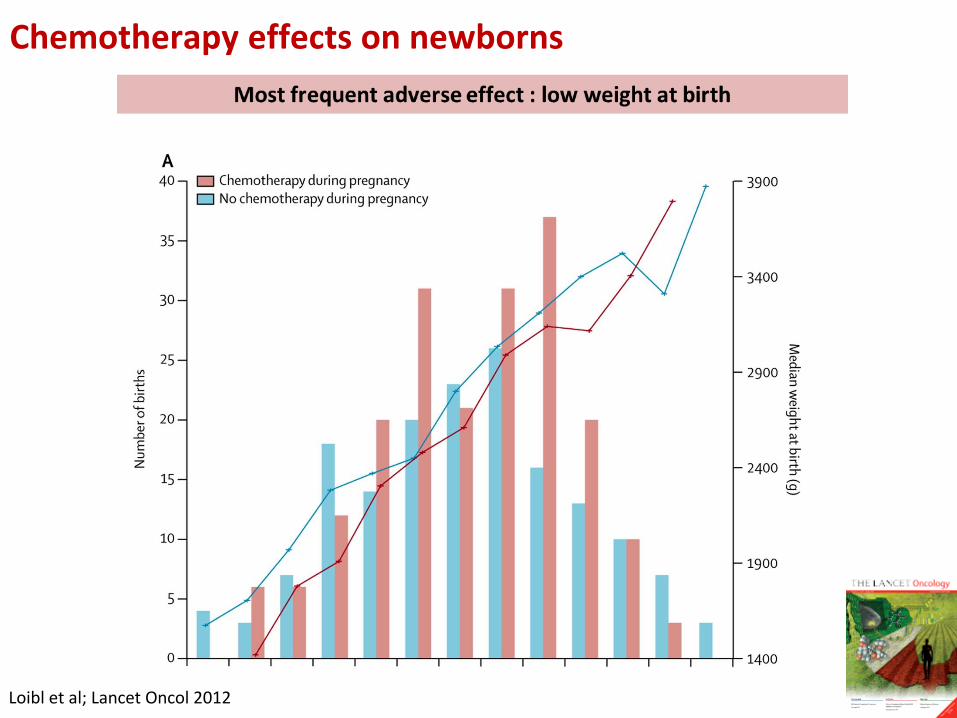
Loibl et al; Lancet Oncol 2012
Chemotherapy effects on newborns
CHEMOTHERAPY RECOMMENDATIONS
• MDT team (including also obstetrics and neonatalogy)
• Treat as similiar as possible to a non pregant patien
• Prefer sequential CT (less toxic, identical efficacy) e.g. EC-Paclitaxel weekly or Paclitaxel weekly – EC
• Dosing according to real weight (not excluding the baby)
• Support measures (ex: antiemetics yes; no growth factors)
• Pregnancy Surveillance: Ultrasound after each cycle of CT
BREAST CANCER DURING PREGNANCY

SYSTEMIC TREATMENT: HORMONAL THERAPY
NO!
HIGH RISK OF MALFORMATIONS!
SYSTEMIC TREATMENT: TRASTUZUMAB
NO!
HIGH RISK OF MALFORMATIONS! (anidramnios)Specially in the 2nd e 3rd trimester (different from other drugs)
BREAST CANCER DURING PREGNANCY
LHRHa + AROMATASE INHIBITORS
- No data
TAMOXIFEN
- 90 cases on file (Lancet 1993)
- Labia minor coalescence and clitoris hypertrophy in 2 cases(Lancet 1997)
- Goldenhar syndrome in 1 case (JAMA 1994)
Hormonal treatment during pregnancy
Courtesy F. Peccatori
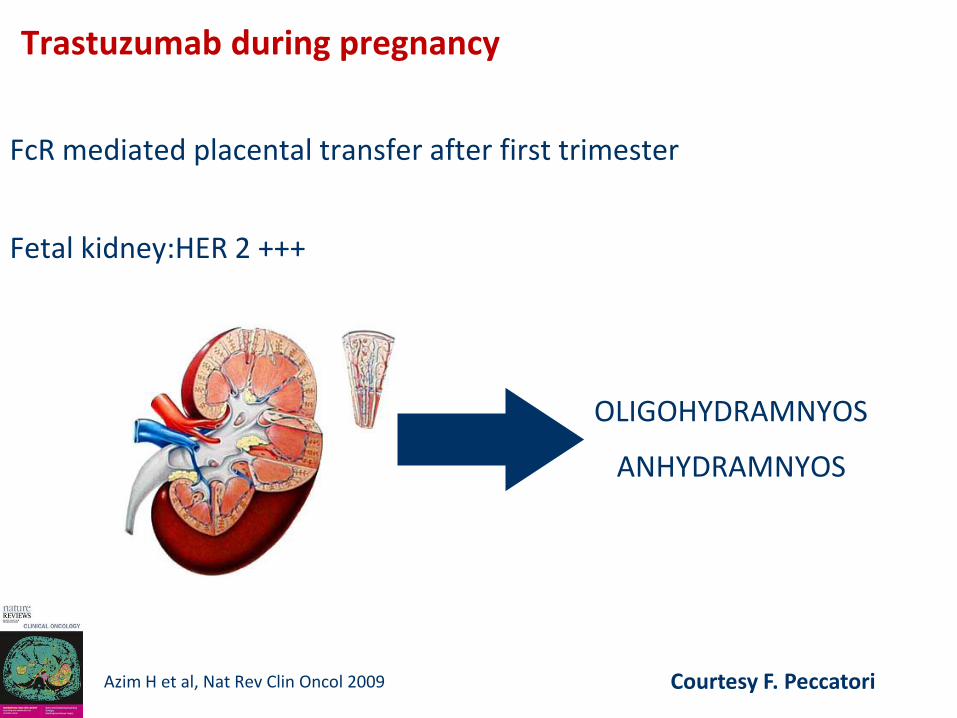
FcR mediated placental transfer after first trimester
Fetal kidney:HER 2 +++
OLIGOHYDRAMNYOS
ANHYDRAMNYOS
Azim H et al, Nat Rev Clin Oncol 2009
Trastuzumab during pregnancy
Courtesy F. Peccatori

- 18 cases
- Oligo-anhydramnios in 11/18 cases
- Neonatal death in 4/11 cases (respiratory and renal failure due to premature delivery)
- Increased risk with prolonged administration
TRASTUZUMAB CONTRAINDICATED !
Trastuzumab during pregnancy
Courtesy F. Peccatori

MOTHER PROGNOSIS (Young women!)


Median follow up: 51 months
p-value: 0.0339
DFS
p-value: 0.0499
OS
Pregnant cases (n=65)
Controls (n=120)
Prognosis (DFS & OS)
Azim HA Jr et al; Acta Oncol 2012Courtesy F. Peccatori

Lancet Oncol 2012; 13: 256–64
CHILD LONG TERM EFFECTS
Fetal exposure to chemotherapy was not associated with increased
CNS morbidity….compared with the general population.

CHILD LONG TERM EFFECTS
• Long term cognitive function is related with date of delivery but not with the number of CT cycles
• Each additional pregnancy month is associated to a rise of 11.6 points in the Intelligence Coefficient Scale
MAIN MESSAGE:
AVOID PREMATURE DELIVERY!
NEED FOR MORE INFORMATION: EUROPEAN REGISTRIES
Registry for breast cancer
during pregnancy
GBG-29
BIG 02-03
www. germanbreastgroup.de/pregnancy
With support of the BANSS-Foundation
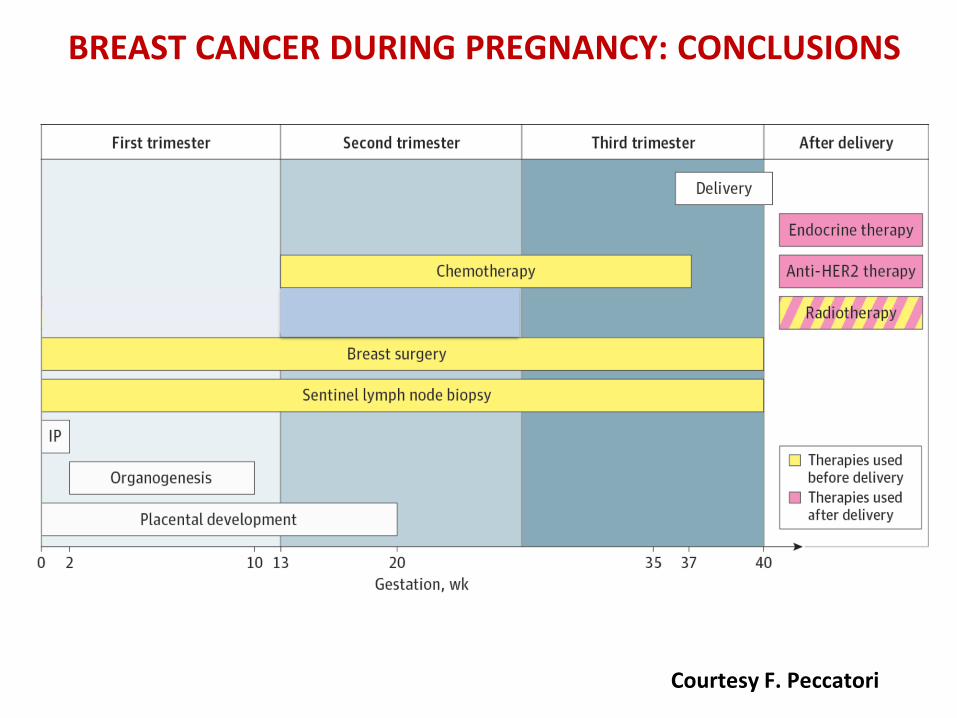
BREAST CANCER DURING PREGNANCY: CONCLUSIONS
Courtesy F. Peccatori

SUPPORTIVE CARE
BREAST CANCER DURING PREGNANCY
Treatment of patients with breast cancer during pregnancy shouldbe decided on an individual basis according to internationalguidelines within an expert multidisciplinary team, expanded toinclude obstetricians and perinatologists, and according topatients' preferences.
