brachial plexus anatomy, diagnosis and orthopaedic treatment
TRANSCRIPT
PRESENTED BY : Harjot singh gurudatta
MODERATOR : Dr. Rohit Sharma
12-2
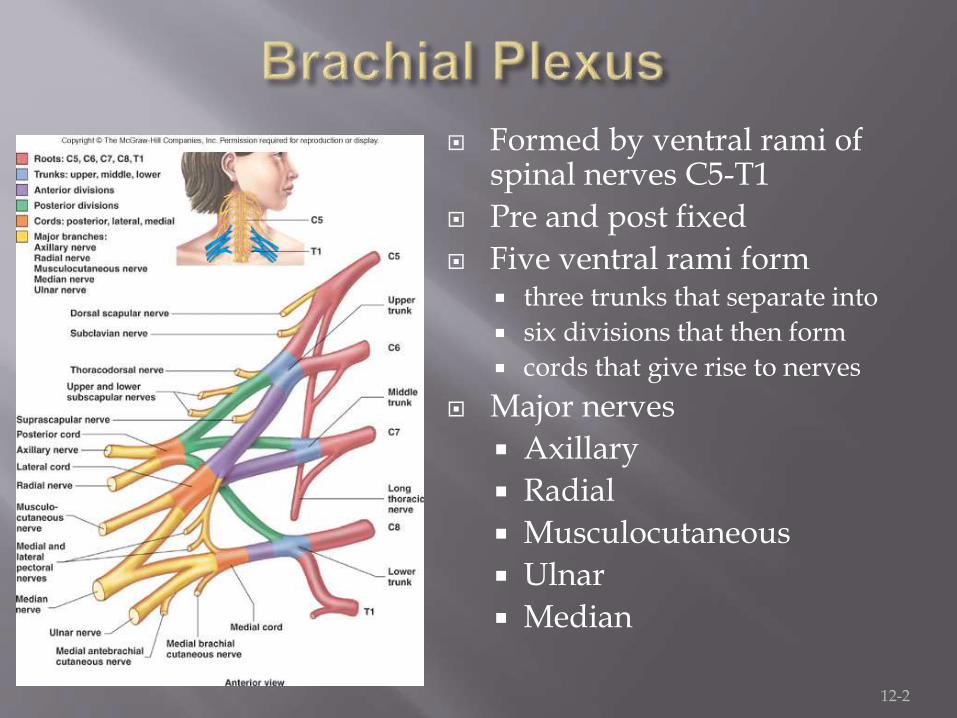
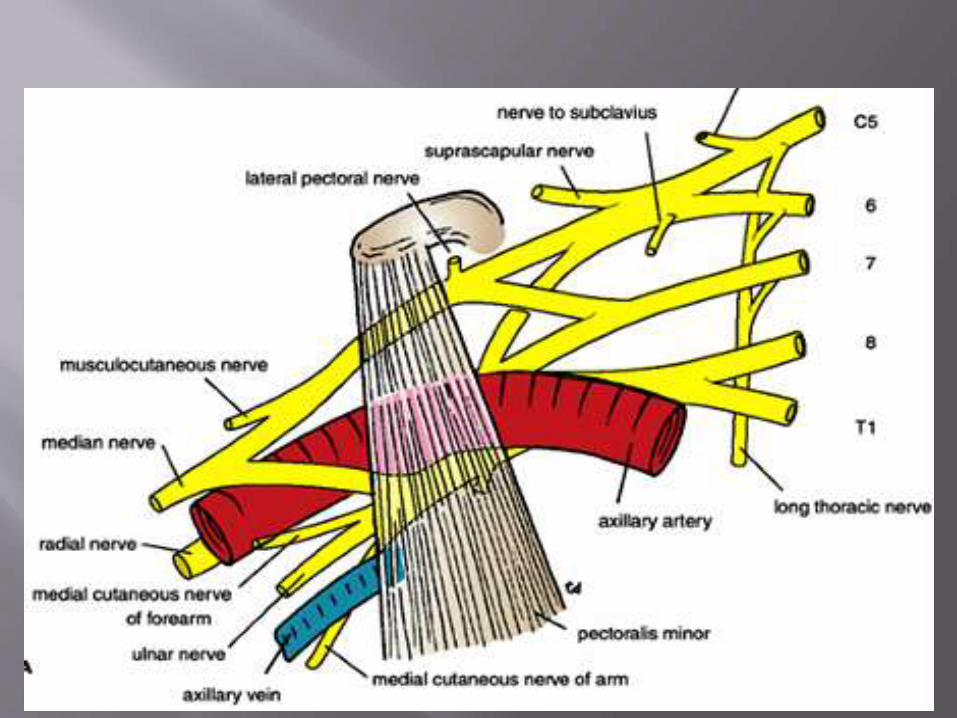
Formed by ventral rami of spinal nerves C5-T1
Pre and post fixed
Five ventral rami form three trunks that separate into
six divisions that then form
cords that give rise to nerves
Major nerves
Axillary
Radial
Musculocutaneous
Ulnar
Median
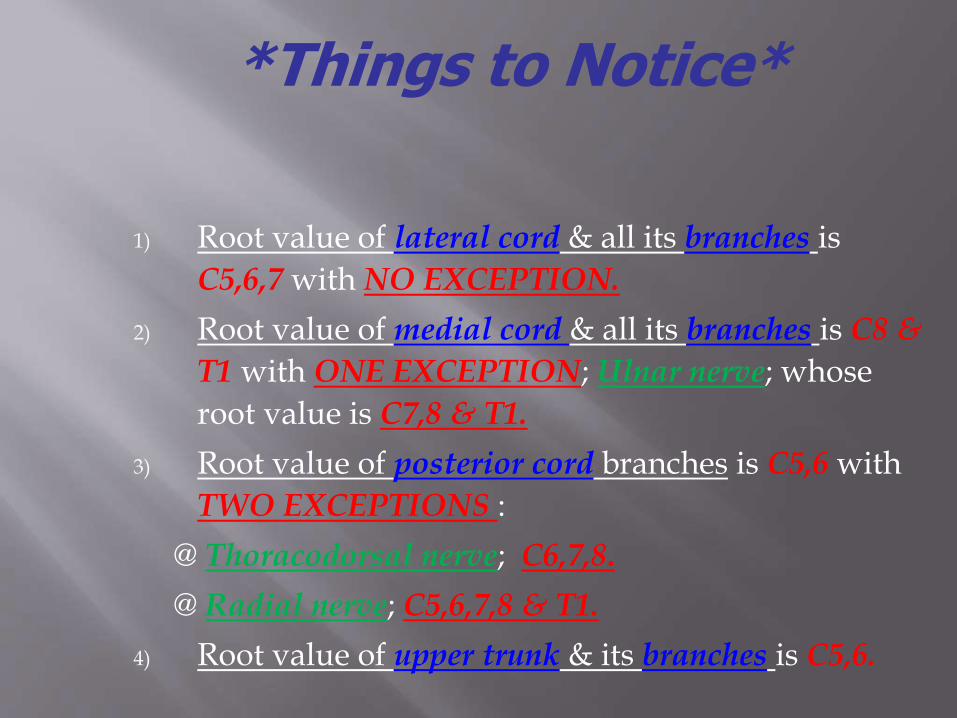
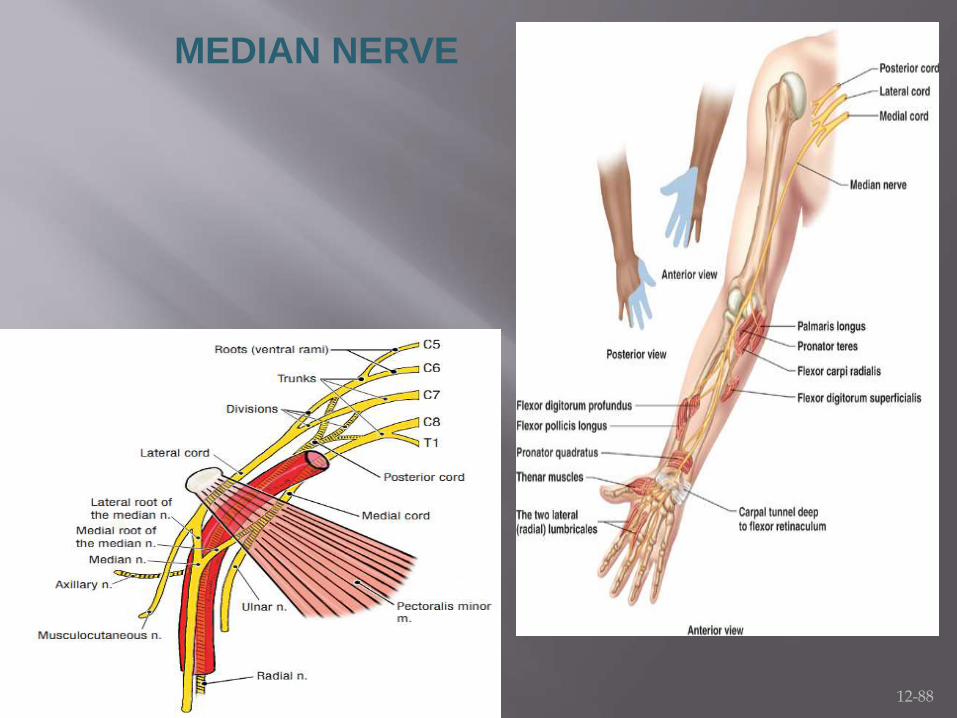
1) Root value of lateral cord & all its branches is
C5,6,7 with NO EXCEPTION.
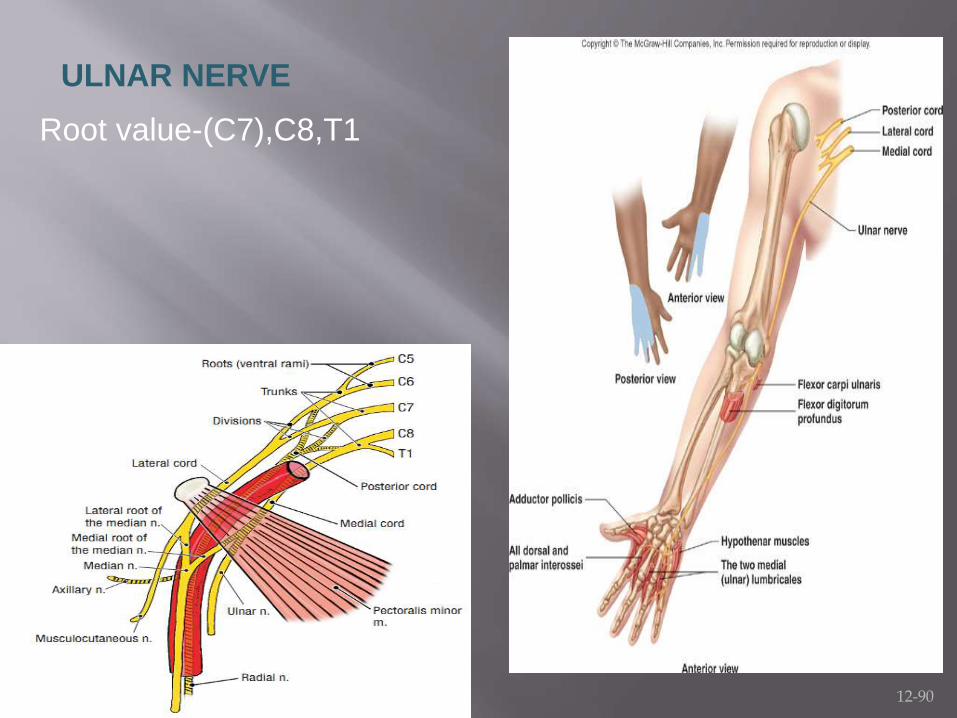
2) Root value of medial cord & all its branches is C8 &
T1 with ONE EXCEPTION; Ulnar nerve; whose
root value is C7,8 & T1.
3) Root value of posterior cord branches is C5,6 with
TWO EXCEPTIONS :
@ Thoracodorsal nerve; C6,7,8.
@ Radial nerve; C5,6,7,8 & T1.
4) Root value of upper trunk & its branches is C5,6.
*Things to Notice*

Some mnemonics for remembering the branches: Posterior Cord Branches
STAR - Subscapular (upper and lower), Thoracodorsal, Axillary, Radial
ULTRA or ULNAR- Upper subscapular, Lower subscapular, Thoracodorsal, Radial, Axillary
Lateral Cord Branches LML or LLM "Lucy Loves Me" - Lateral pectoral, Lateral
root of the median nerve, Musculocutaneous
Medial Cord Branches M4U or MMMUM "Most Medical Men Use Morphine" -
Medial pectoral, Medial cutaneous nerve of arm, Medial cutaneous nerve of forearm, Ulnar, Medial root of the median nerve
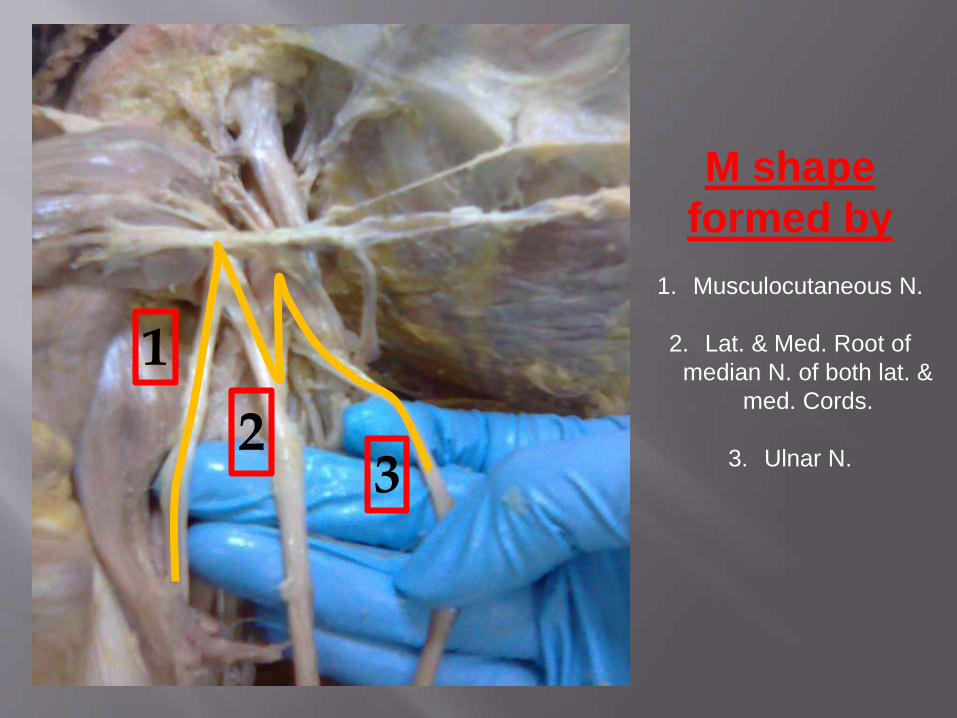
M shape
formed by
1. Musculocutaneous N.
2. Lat. & Med. Root of
median N. of both lat. &
med. Cords.
3. Ulnar N.
1
23
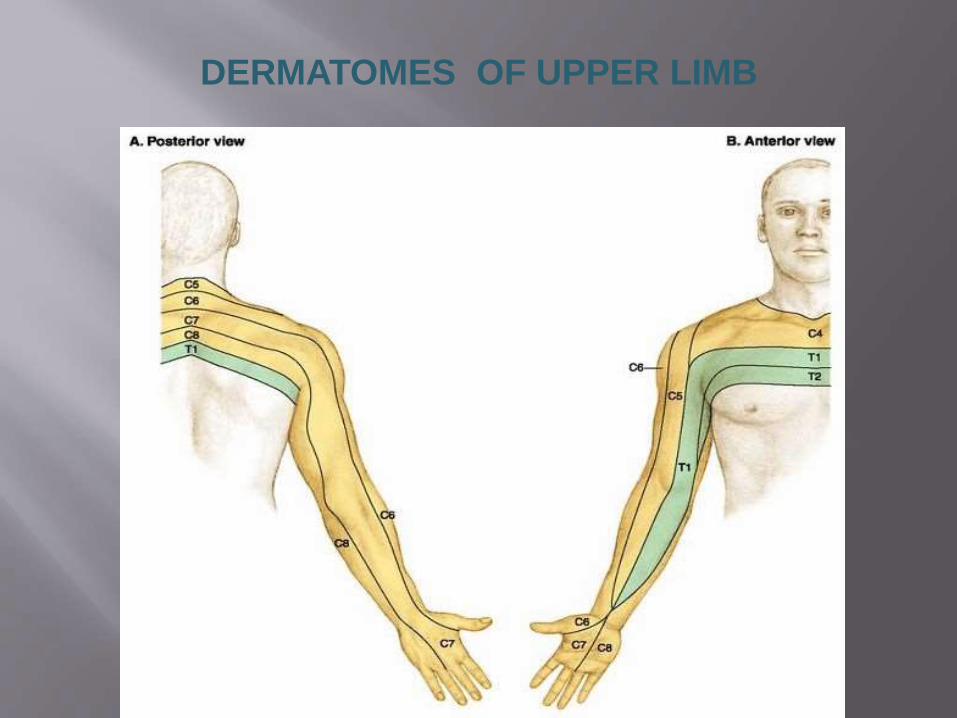
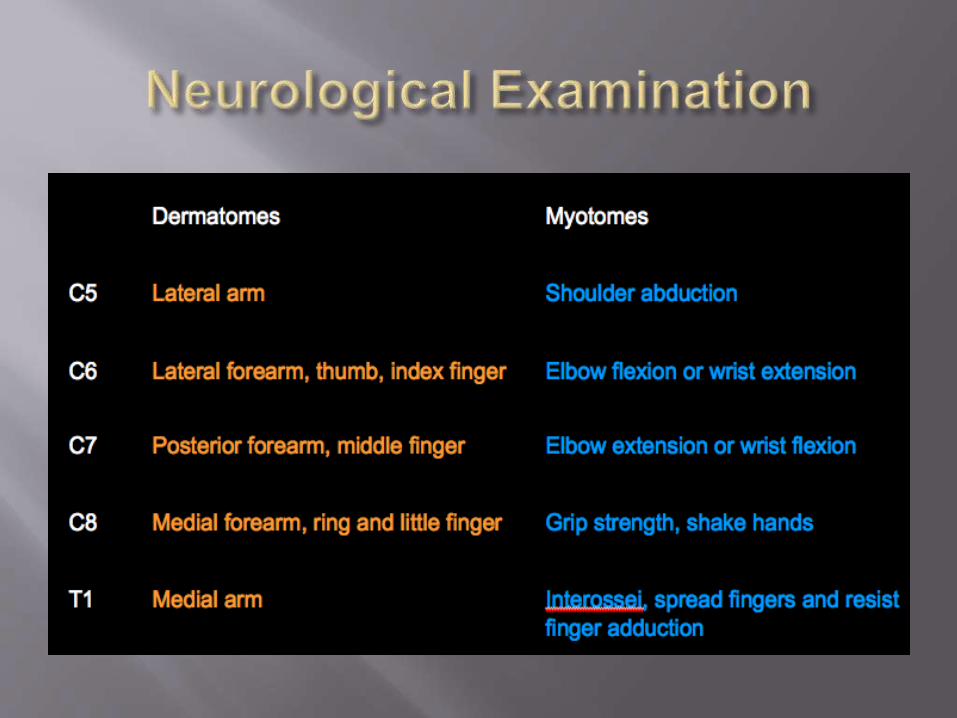
DERMATOMES OF UPPER LIMB
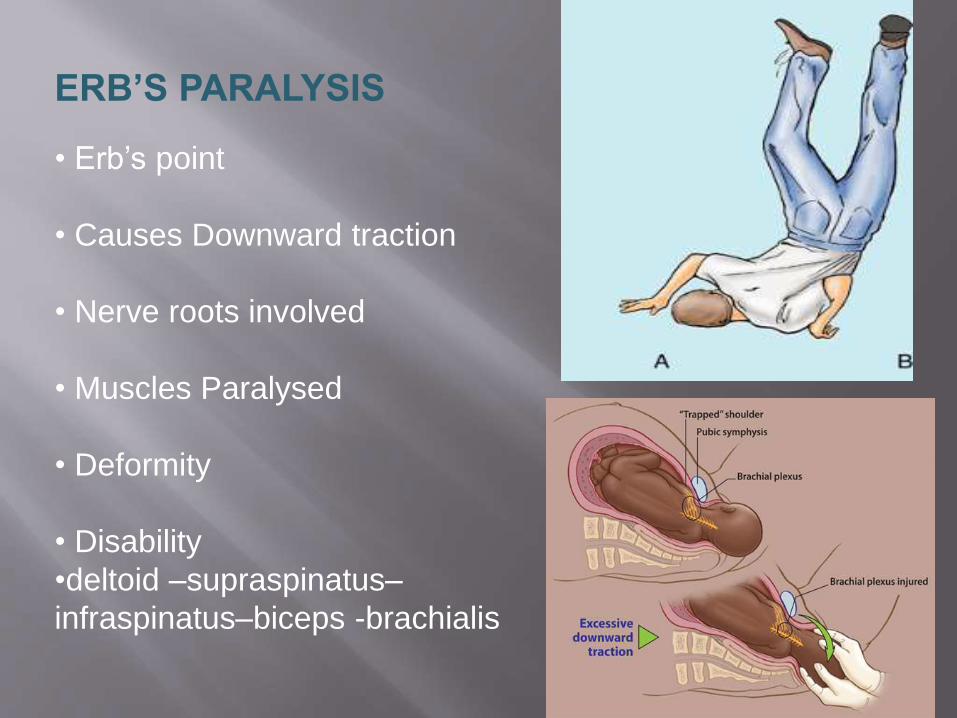
ERB’S PARALYSIS
• Erb’s point
• Causes Downward traction
• Nerve roots involved
• Muscles Paralysed
• Deformity
• Disability
•deltoid –supraspinatus–
infraspinatus–biceps -brachialis
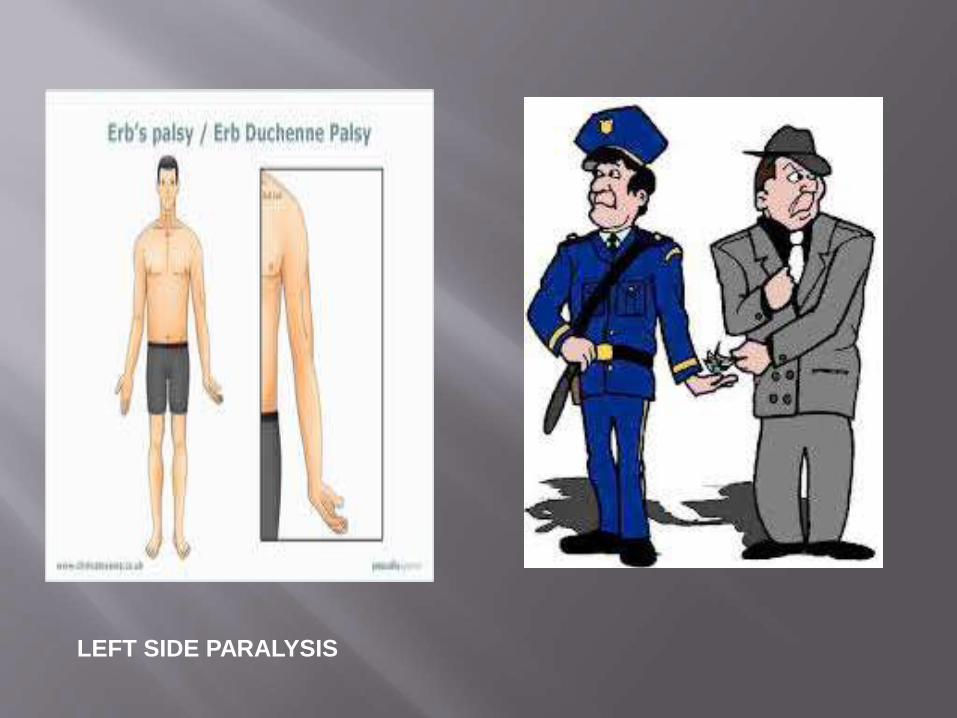
LEFT SIDE PARALYSIS
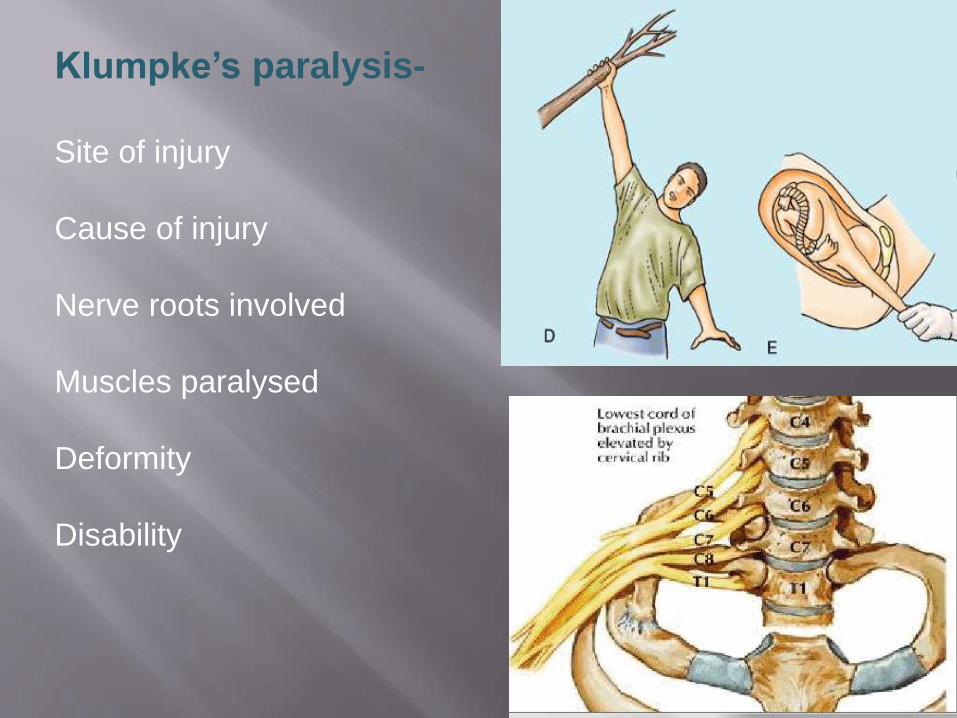
Klumpke’s paralysis-
Site of injury
Cause of injury
Nerve roots involved
Muscles paralysed
Deformity
Disability
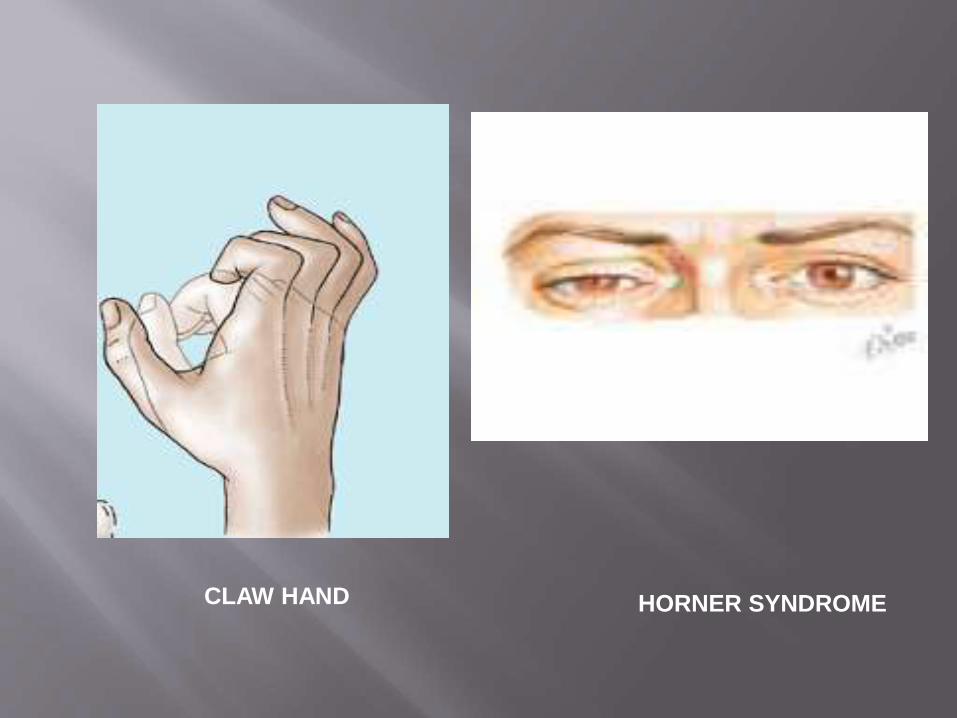
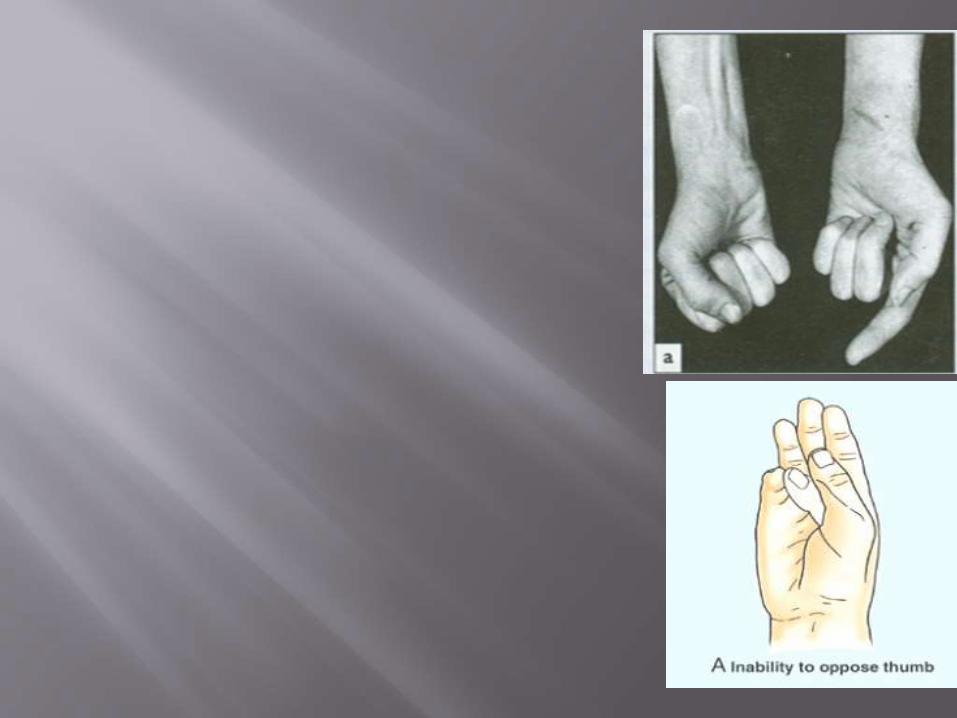
CLAW HAND HORNER SYNDROME
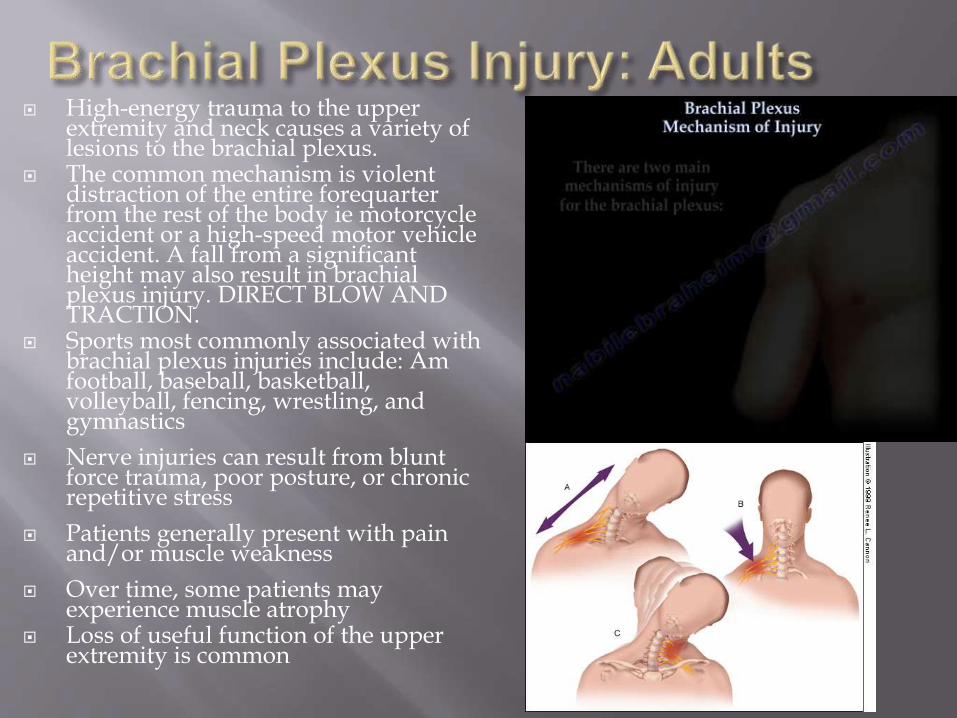
High-energy trauma to the upper extremity and neck causes a variety of lesions to the brachial plexus.
The common mechanism is violent distraction of the entire forequarter from the rest of the body ie motorcycle accident or a high-speed motor vehicle accident. A fall from a significant height may also result in brachial plexus injury. DIRECT BLOW AND TRACTION.
Sports most commonly associated with brachial plexus injuries include: Am football, baseball, basketball, volleyball, fencing, wrestling, and gymnastics
Nerve injuries can result from blunt force trauma, poor posture, or chronic repetitive stress
Patients generally present with pain and/or muscle weakness
Over time, some patients may experience muscle atrophy
Loss of useful function of the upper extremity is common

Millesi classification*
Supraganglionic
Infraganglionic
Trunk
Cord
Anatomical Classification
C5-6 waiters tip (Erbspalsy)
C5-7 as above, elbow slightly flexed
C5-T1 flail limb, claw hand, vasomotor changes, +/- Hornerssyndrome
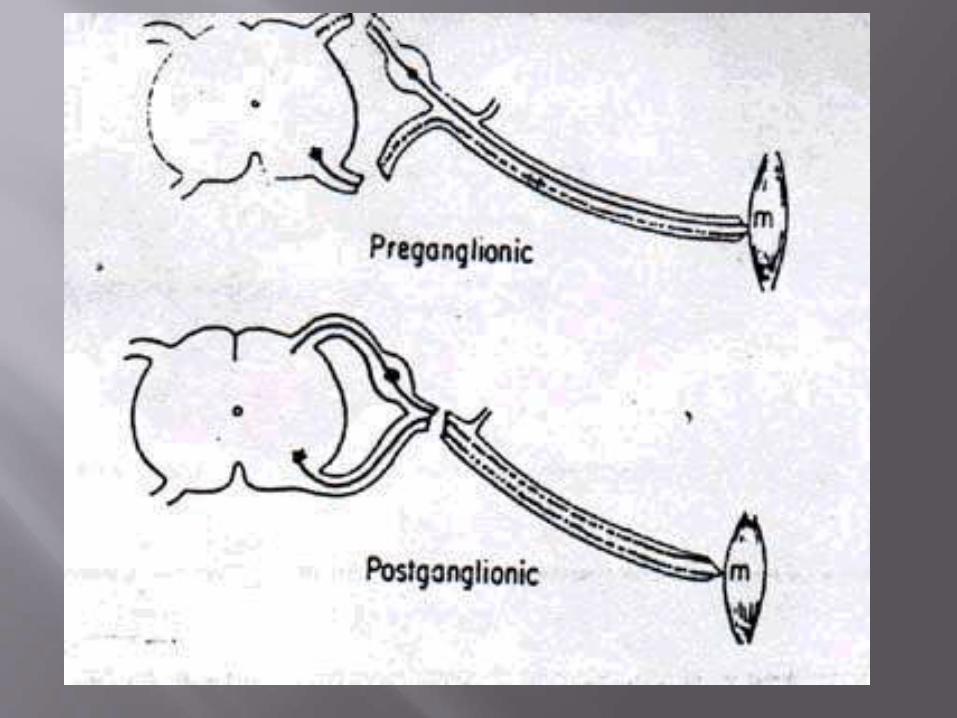
Nerve root avulsion
dorsal & ventral rootlets
invested by pia mater / dural funnel
etiology: traction (occasionally missile, knife)
Significant traction causes dural rupture / root vulnerability
ventral > dorsal root (esp C8-T1) at higher risk
POOR Prognosis!
Grade 1 – Neuropraxia Disruption in nerve function that produces numbness and tingling
Most common grade within athletics
Symptoms usually resolve within several minutes
Grade 2 – Axonotmesis Damage to the nerve’s axon
Symptoms = numbness, tingling, and affected function (may last several days)
Long nerves have a greater healing time than short nerves
Rare within athletics
Motor march, Tinel sign
Grade 3 – Neurotmesis Permanent nerve damage occurs
Very rare within athletics
“Occurs with high-energy trauma, fractures, and penetrating injuries”
How do you Rx the patient knocked off his motorcycle with clavicle # and flail arm?
Manage acute injury according to ATLS principles; look for concomitant injury ie c-spine.
History Age, handedness, occupation, special skills
Cause of injury: arm hyperabducted vs neck laterally flexed
Immediate or delayed arm weakness
Concomitant injury
General health: PMH, DH, Smoker
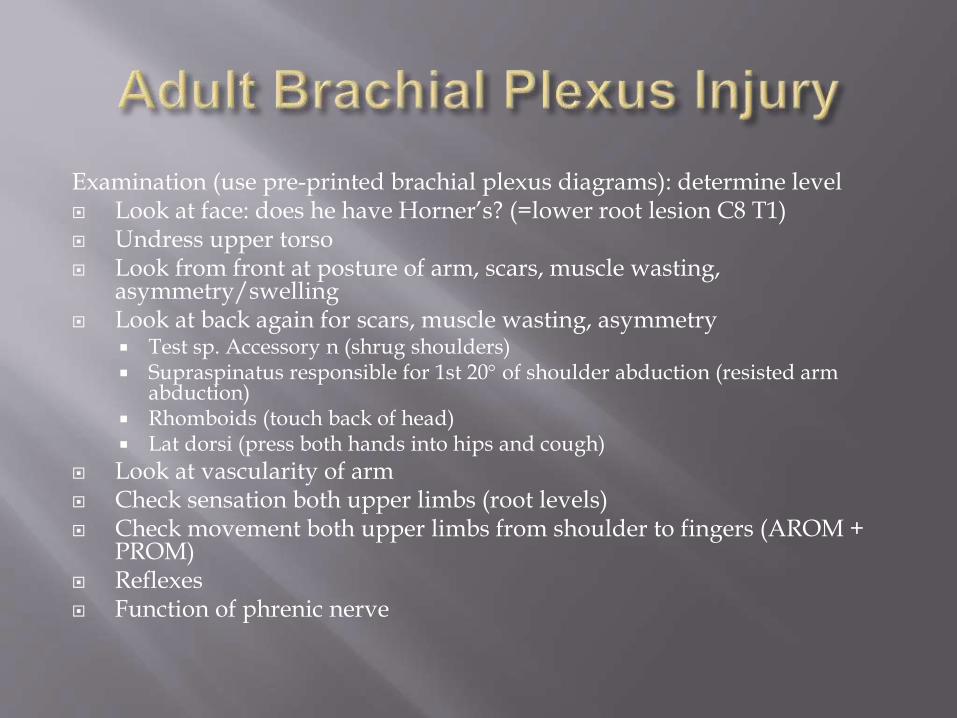
Examination (use pre-printed brachial plexus diagrams): determine level Look at face: does he have Horner’s? (=lower root lesion C8 T1) Undress upper torso Look from front at posture of arm, scars, muscle wasting,
asymmetry/swelling Look at back again for scars, muscle wasting, asymmetry
Test sp. Accessory n (shrug shoulders) Supraspinatus responsible for 1st 20 of shoulder abduction (resisted arm
abduction) Rhomboids (touch back of head) Lat dorsi (press both hands into hips and cough)
Look at vascularity of arm Check sensation both upper limbs (root levels) Check movement both upper limbs from shoulder to fingers (AROM +
PROM) Reflexes Function of phrenic nerve
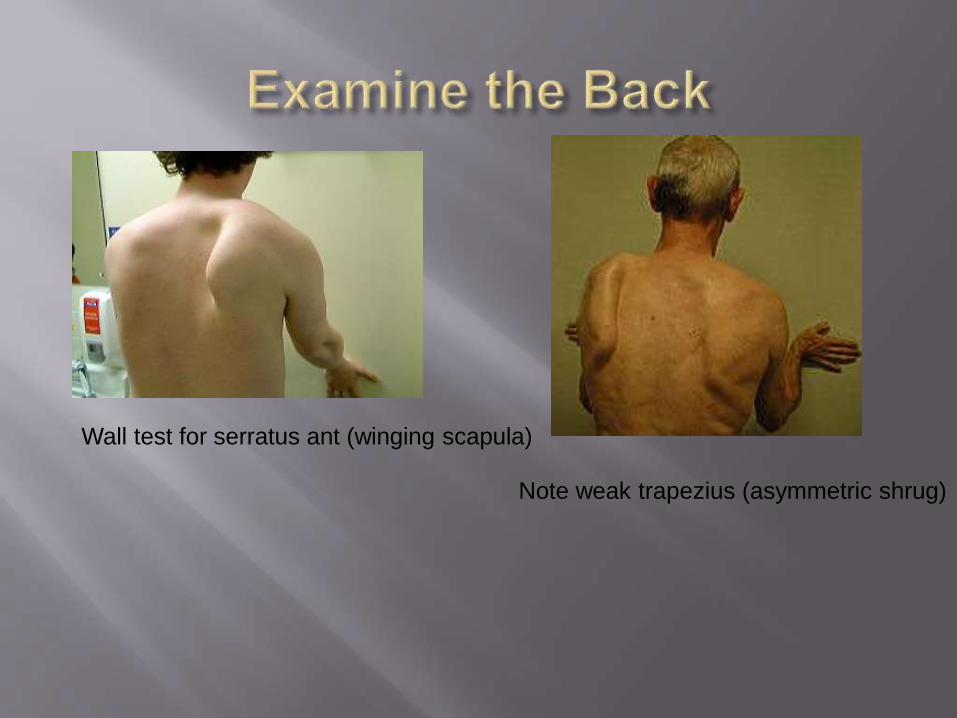
Wall test for serratus ant (winging scapula)
Note weak trapezius (asymmetric shrug)
Brachial Plexus Cervical Compression
Test
Cervical Distraction Test
Spurling’s Test
Brachial Plexus Traction Test
Thoracic Outlet Syndrome
Adson’s Test
Allen’s Test
Axillary N. Sensory – Lateral arm Motor – Shoulder
abductionMusculocutaneous N. Sensory – Anterior arm Motor – Elbow flexion
Radial N. Sensory – 1st Dorsal web
space Motor – Wrist extension
and thumb extensionMedian N. Sensory – Pad of Index
finger Motor – Thumb pinch
and abductionUlnar N. Sensory – Pad of little
finger Motor – Finger
abduction
C5 – Biceps brachii reflex (anterior arm near antecubital fossa)
C6 – Supinator reflex (lateral aspect of forearm)
C7 – Triceps brachii reflex (at insertion of tricepbrachii)
C8 and T1 do not have reflex tests
Imaging: Xray: AP chest (look for teeth and fractures ), AP + lat views shoulder, C-Spine (AP, lat, odontoid peg), Fine-cut CT,
MRI
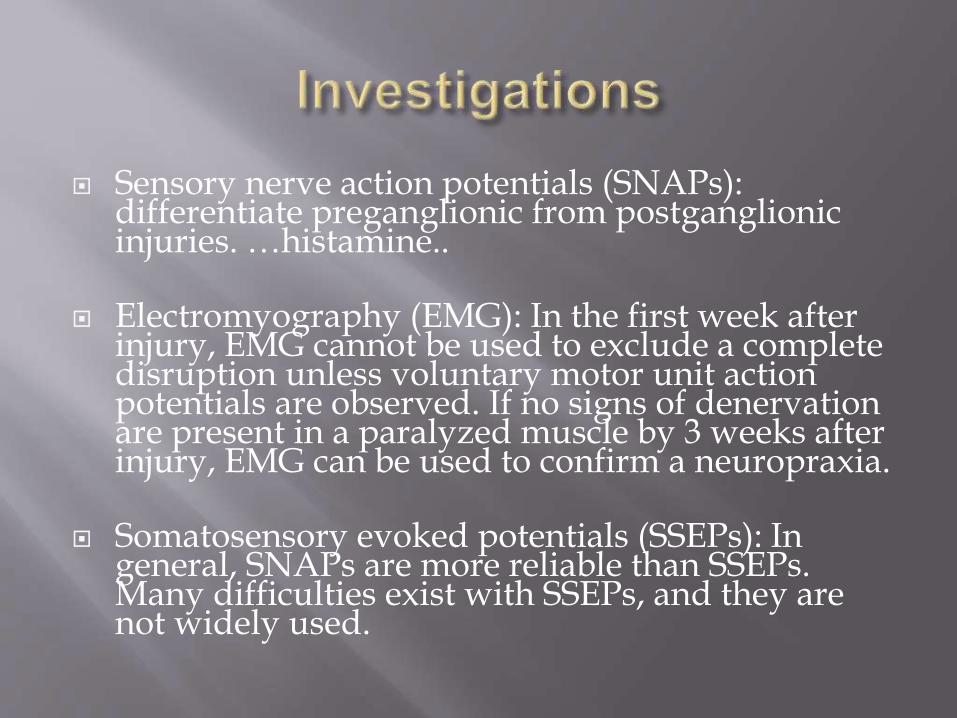
Sensory nerve action potentials (SNAPs): differentiate preganglionic from postganglionic injuries. …histamine..
Electromyography (EMG): In the first week after injury, EMG cannot be used to exclude a complete disruption unless voluntary motor unit action potentials are observed. If no signs of denervationare present in a paralyzed muscle by 3 weeks after injury, EMG can be used to confirm a neuropraxia.
Somatosensory evoked potentials (SSEPs): In general, SNAPs are more reliable than SSEPs. Many difficulties exist with SSEPs, and they are not widely used.

Medical: MDT physio: maintain supple joints with FROM
Orthoptists / splinting
Pain control
Surgical options: nerve transfers
nerve grafting
muscle transfers
free muscle transfers
neurolysis of scar in incomplete lesions
Arthrodesis to stabilise joints
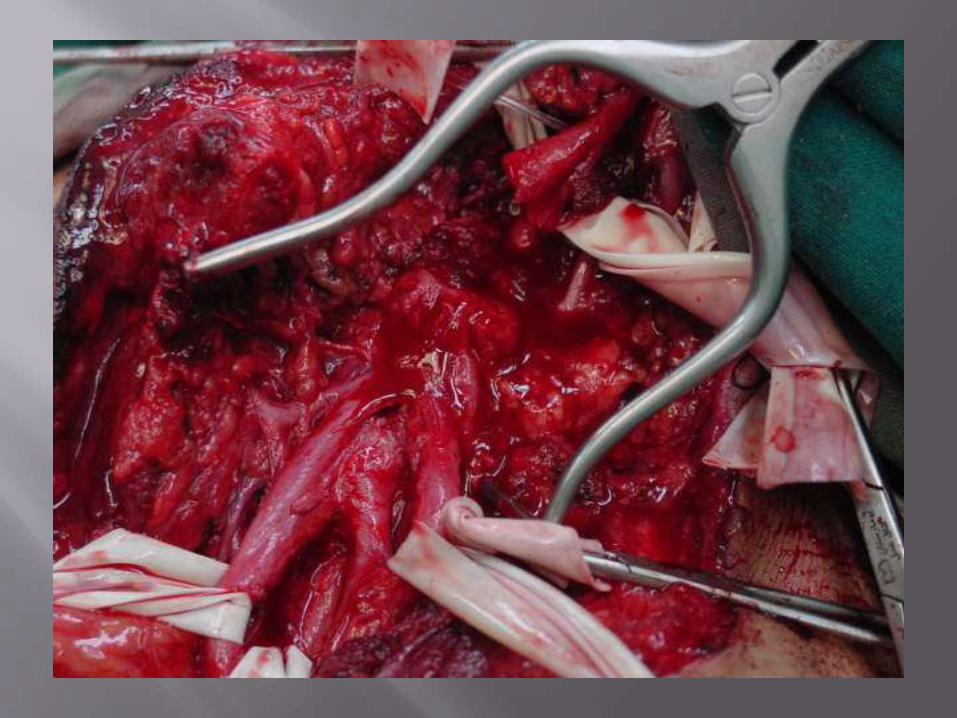
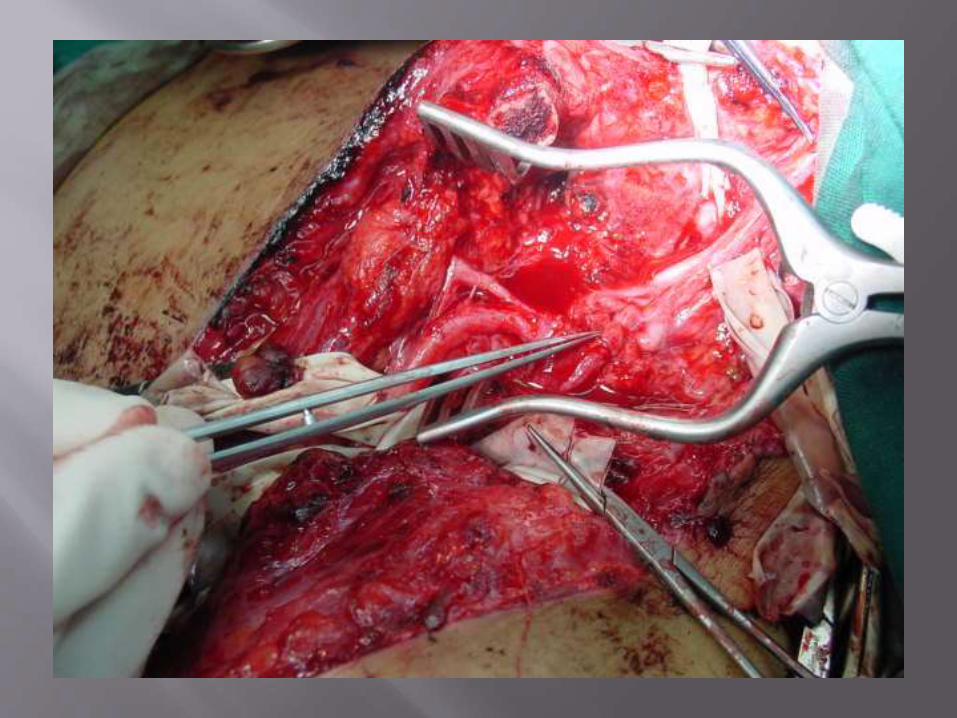
Open wounds
Sharp injury
Bullet injury
Closed injuries

Chest tube

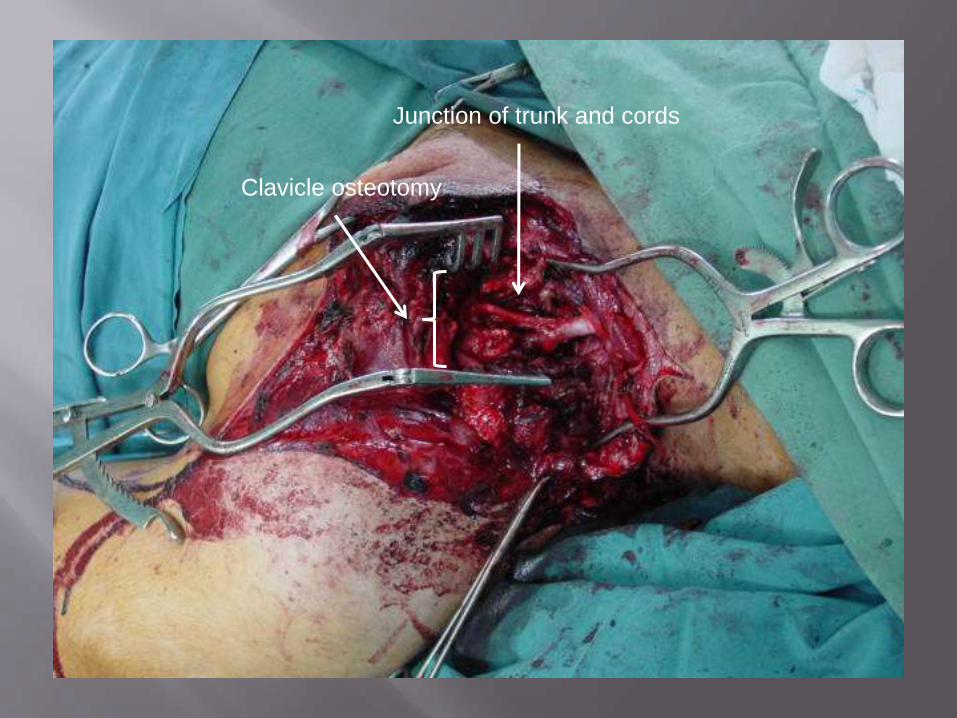
Bullet woundClavicle osteotomy
Junction of trunk and cords
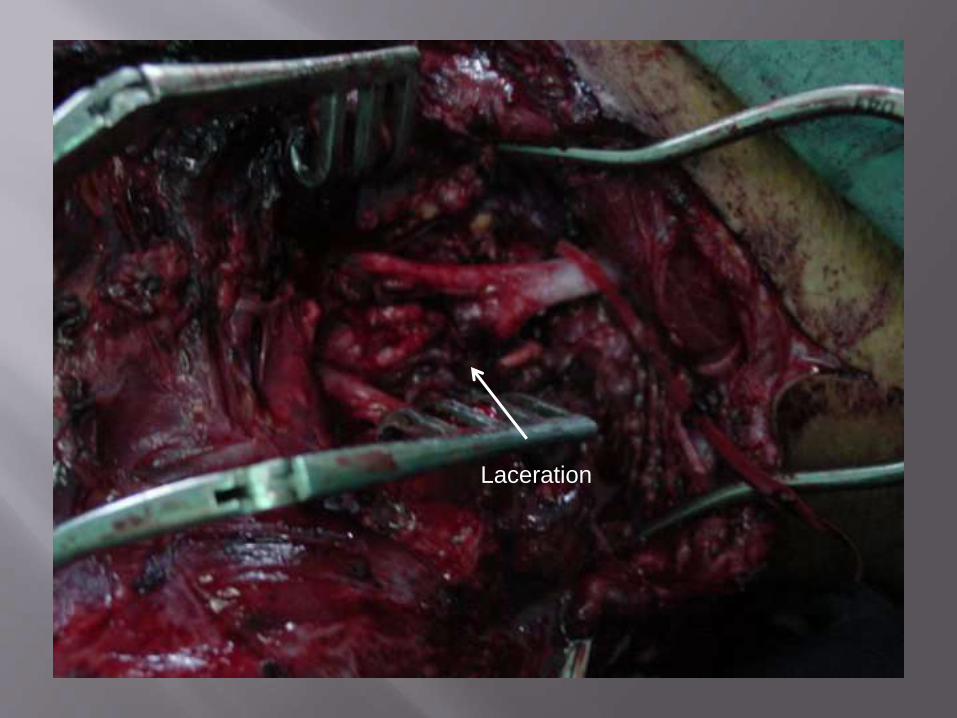
Laceration
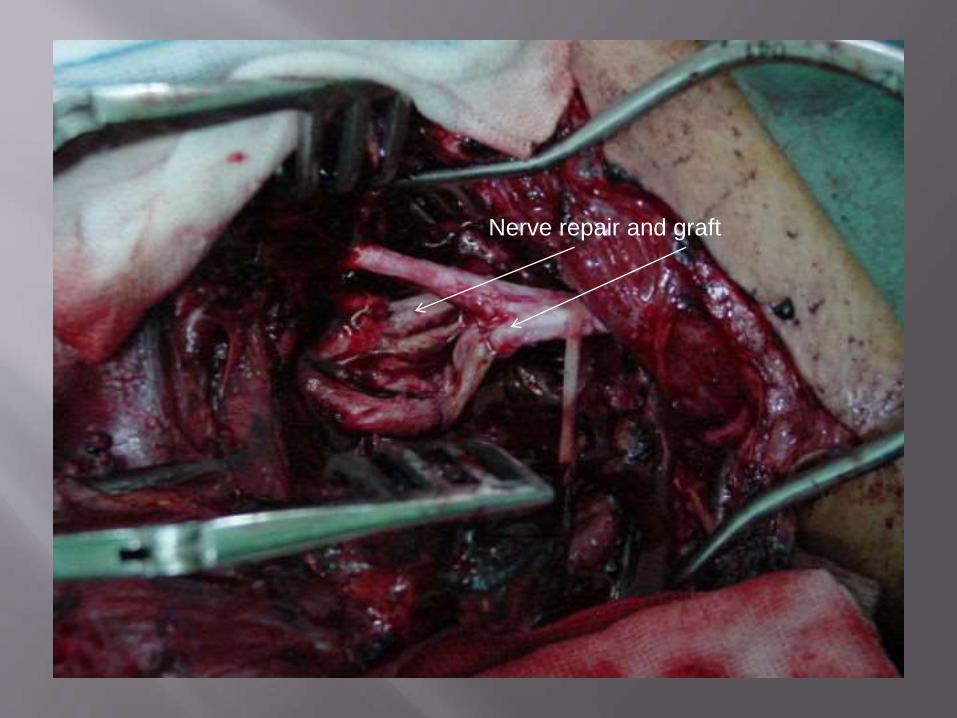
Nerve repair and graft
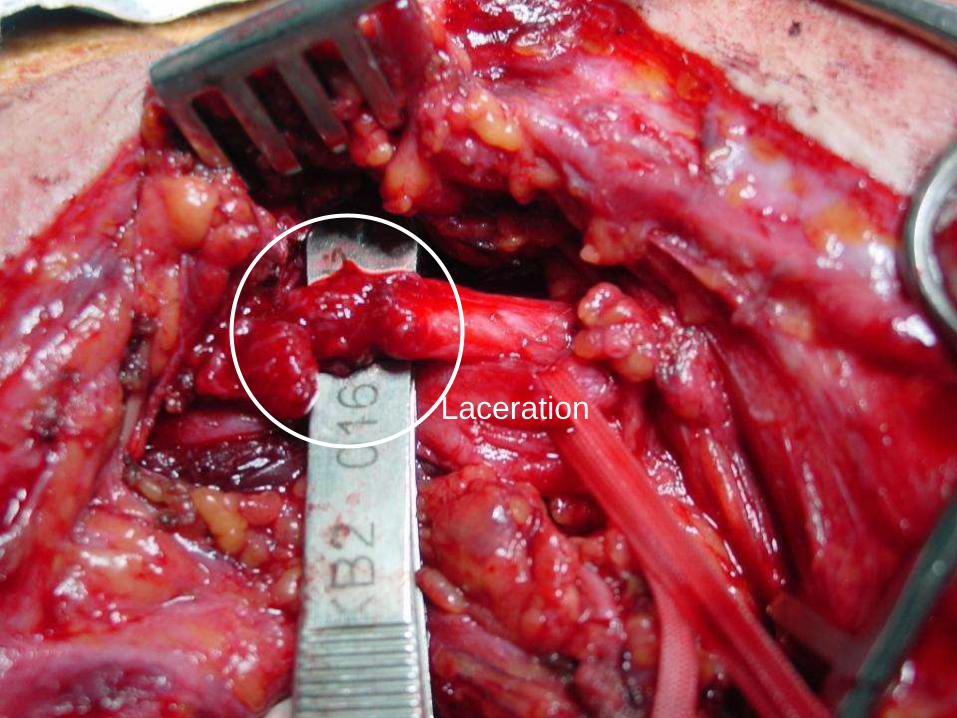
Laceration
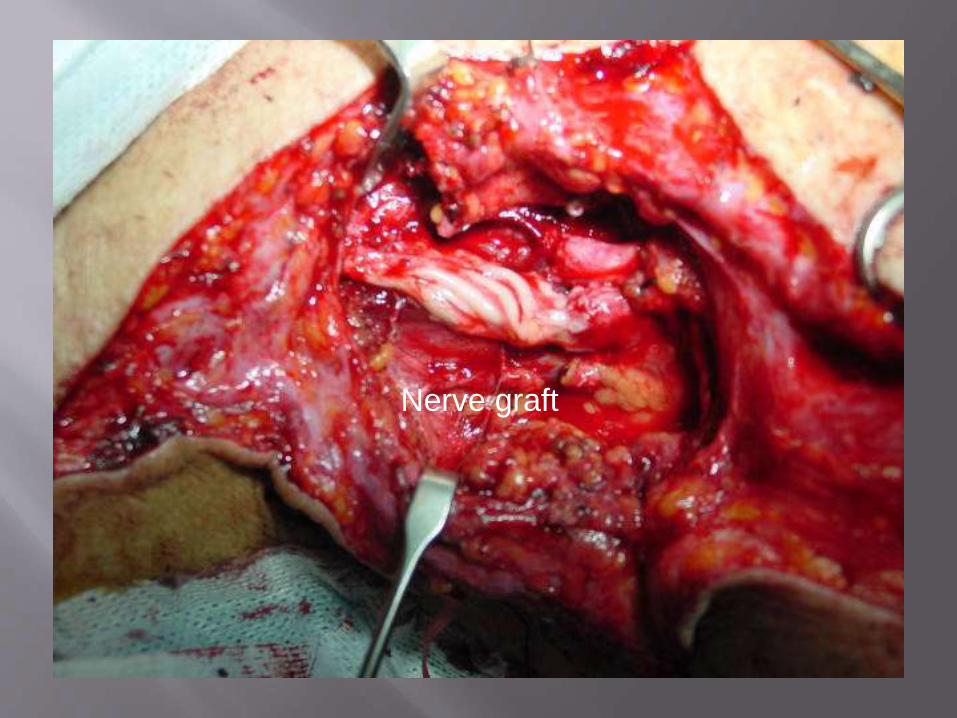
Nerve graft

Closed injury, (tractional injuries)
Closed injury, (tractional injuries)
Early exploration
Underobservation
Decision for the time of delay exploration
Decision for the type of the treatment
Late recostruction
Closed injury, (tractional injuries)
Early exploration
Underobservation
Decision for the time of delay exploration
Decision for the type of the treatment
Late recostructionPeripheral reconstruction
Closed injury, (tractional injuries)
Early exploration vascular reconstruction

Closed injury, (tractional injuries)
Early exploration
Underobservation
First 6-12 weeks
Stabilization of the patient
Stabilization of the injury
Evaluation of the improvement
After 2-3 monthsNo improvement; exploration
Progressive improve; wait & watch
Non-anatomic recovery; explor.
Based on severity
Closed injury, (tractional injuries)
Early exploration
Underobservation
Decision for the time of delay exploration
No recovery
After 6-12 weeks (based on the severity of the trauma)
Progressive improvement
Wait for further improvement
Non-anatomic recovery
Exploration before 9-12 months

Closed injury, (tractional injuries)
Early exploration
Underobservation
Decision for the time of delay exploration
Decision for the type of the treatment
Neurolysis
Nerve repair
Nerve graft
Nerve transfer
Tendon transfer
Arthrodesis
Functional muscle flaps
Straight on Brachial Plexus
Early exploration
Delay exploration
Peripheral reconstruction
Late reconstruction
Danger of more damage
Failure is obvious

Neurolysis….check…potential
Nerve repair
Nerve graft
Nerve transfer
Tendon transfer
Arthrodesis
Functional muscle flaps

Gun shot injury

After neurolysis from scar tissue

Neurolysis
Nerve repair…
Nerve graft
Nerve transfer
Tendon transfer
Arthrodesis
Functional muscle flaps

Neurolysis
Nerve repair
Nerve graft
Nerve transfer
Tendon transfer
Arthrodesis
Functional muscle flaps
Suralmedial cutaneous forearmulnar (vascularised)
Self transfer (i.e. Sural
Nerve)
Manufactured Nerve
Processed Nerve
Cadaver Transplant
Living Related Transplant
Neurolysis
Nerve repair
Nerve graft
Nerve transfer..neurotization
Tendon transfer
Arthrodesis
Functional muscle flaps
Accessory nerveCervical plexusPhrenic nerveIntercostal nervesUlnar ECU nerveCrossed C7Hypoglossal nerve
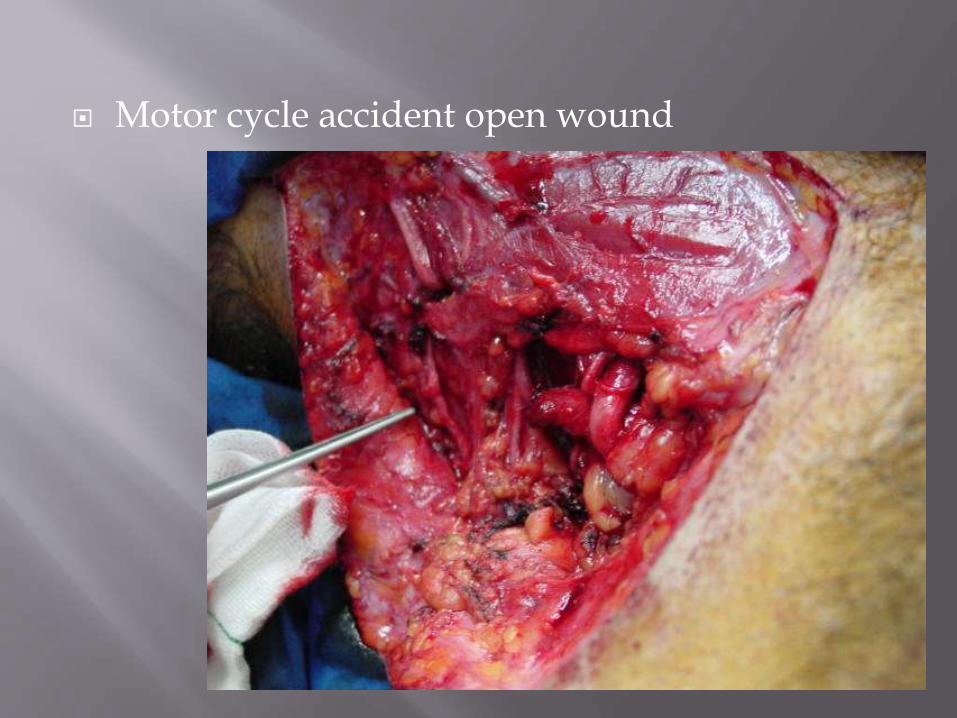
Motor cycle accident open wound
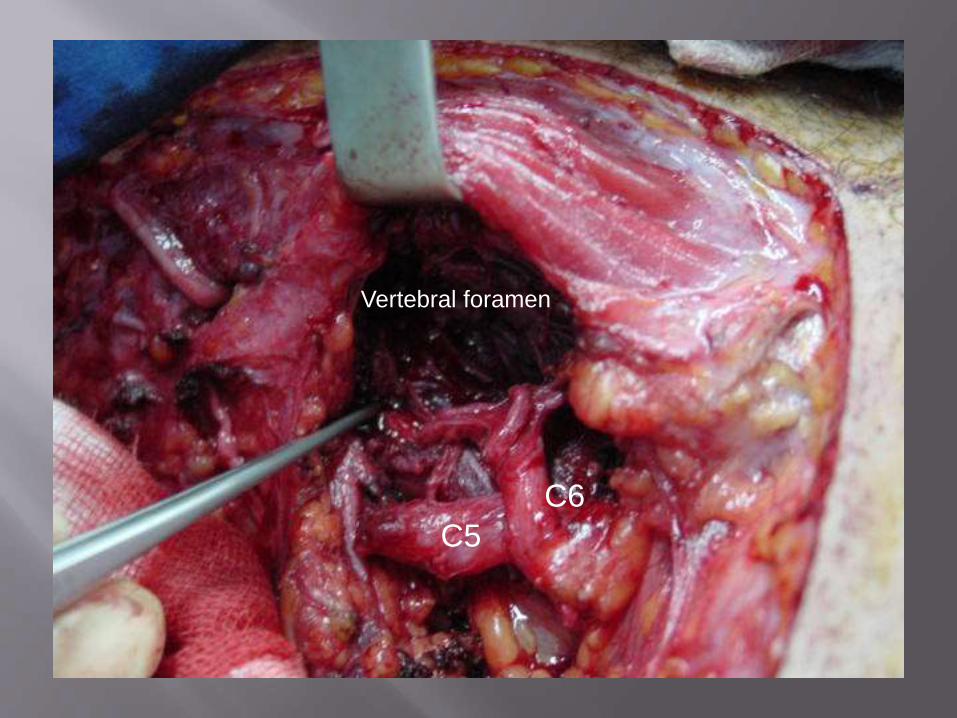
C5
C6
Vertebral foramen

Accessory to suprascapular
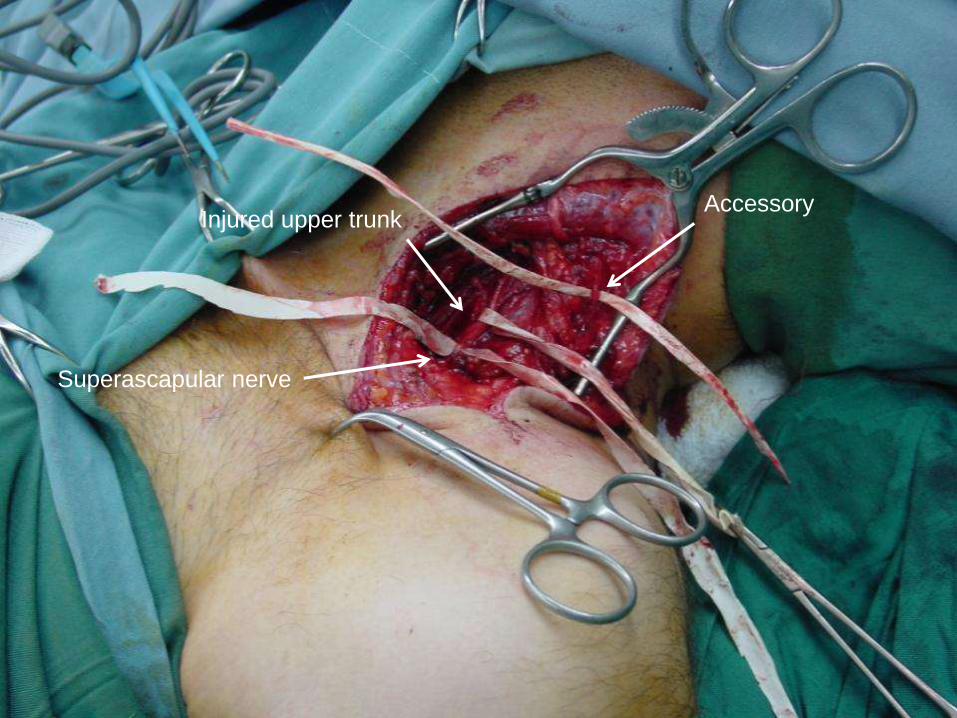
Accessory Injured upper trunk
Superascapular nerve

Oberlin nerve transfer
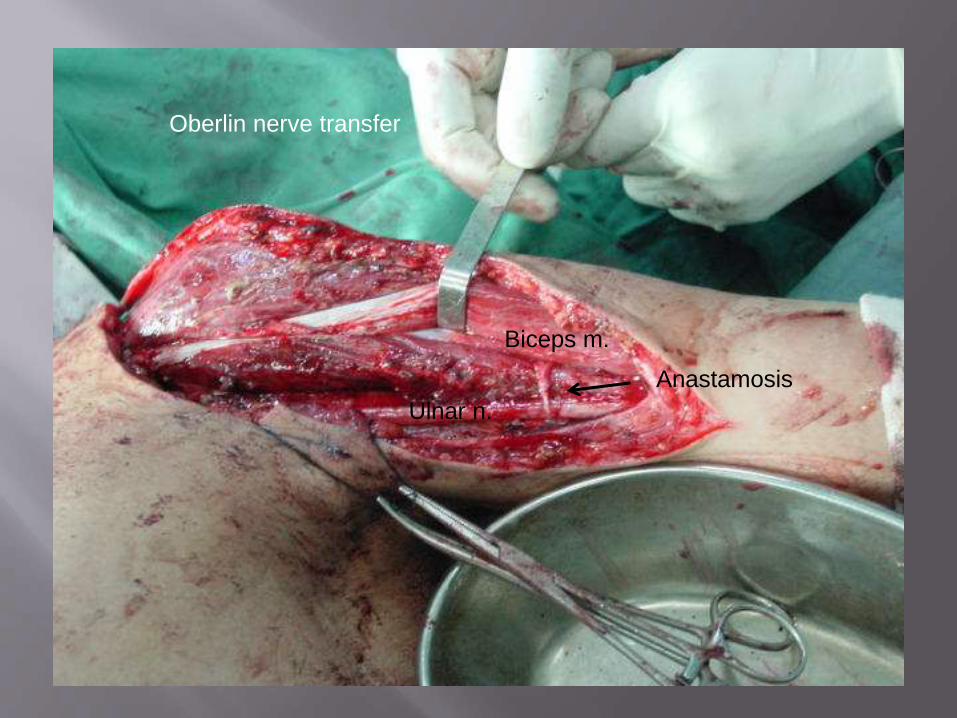
Oberlin nerve transfer
Biceps m.
Ulnar n.
Anastamosis

Radial to axillary transfer
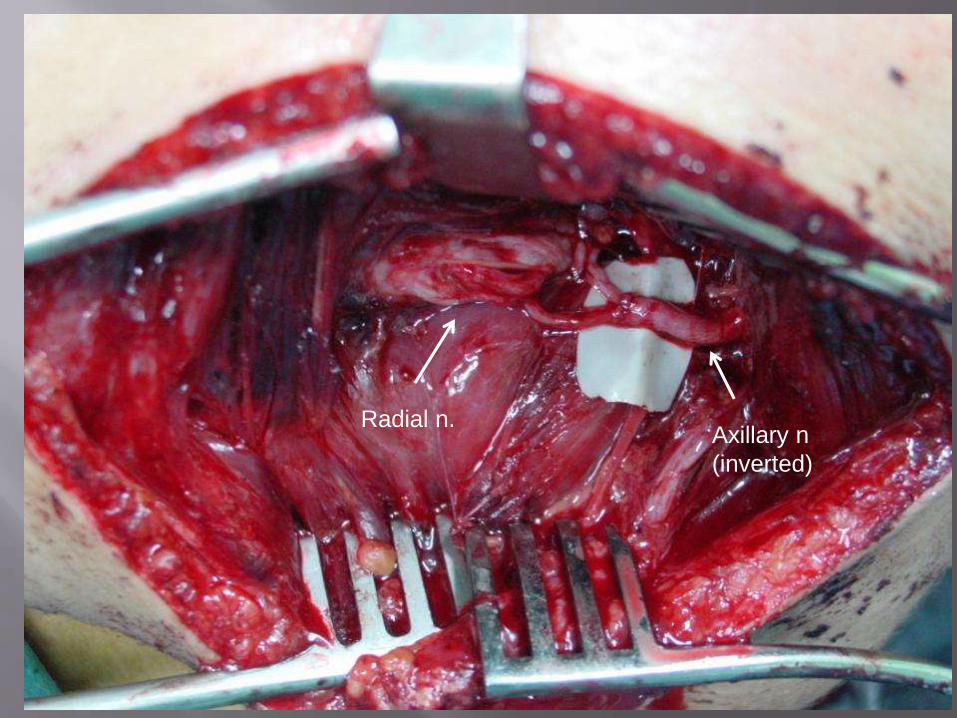
Axillary n
(inverted)
Radial n.
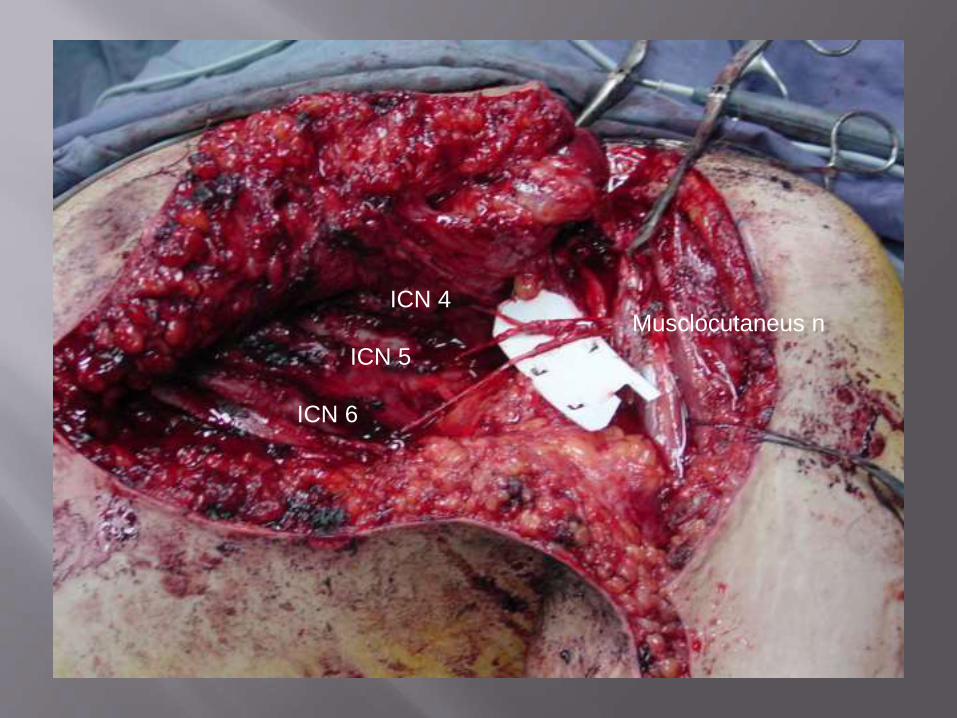
ICN 4
ICN 5
ICN 6
Musclocutaneus n

Neurolysis
Nerve repair
Nerve graft
Nerve transfer
Tendon transfer
Arthrodesis
Functional muscle flaps


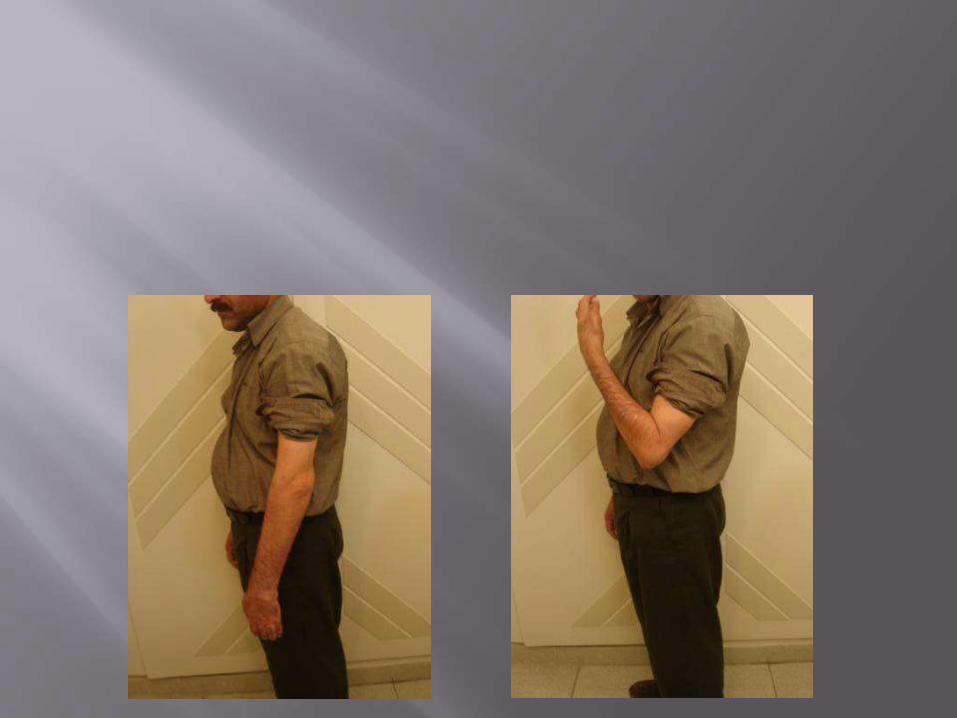
Triceps to Biceps


Latismus dorsi m.

Latismus dorsi transfer
to flexion elbow
and extension finger

Deltoid paralysis

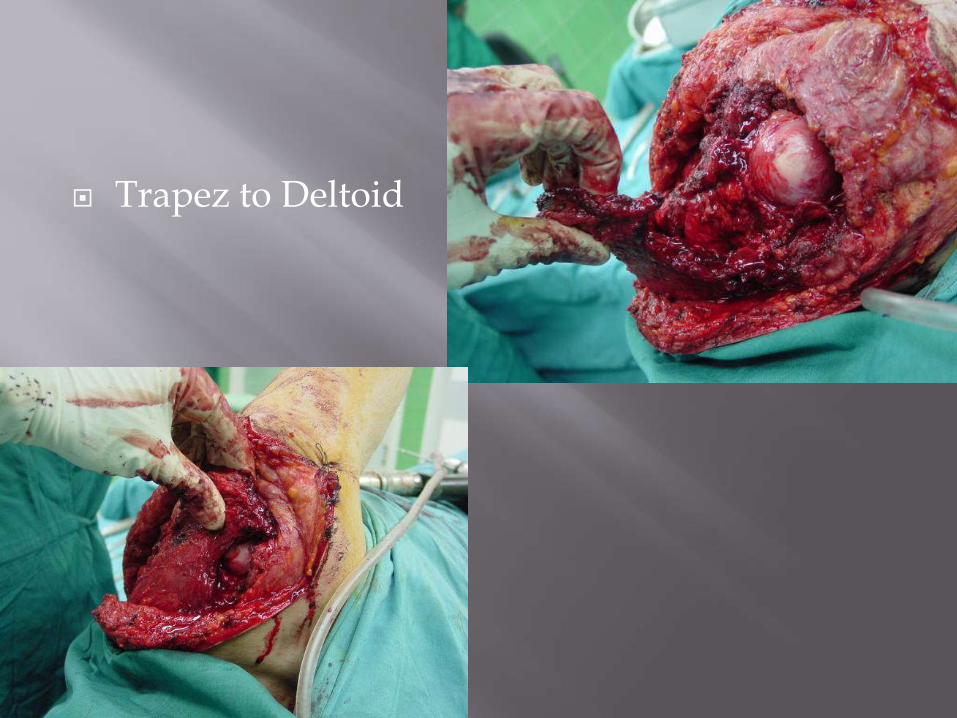
Trapez to Deltoid

Neurolysis
Nerve repair
Nerve graft
Nerve transfer
Tendon transfer
Arthrodesis
Functional muscle flaps
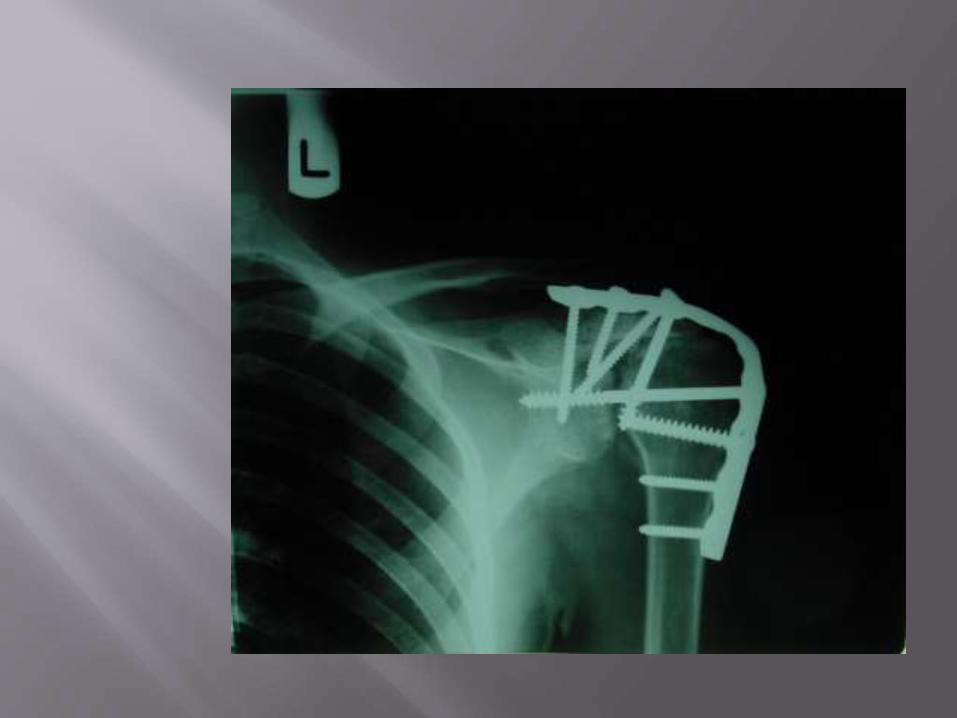
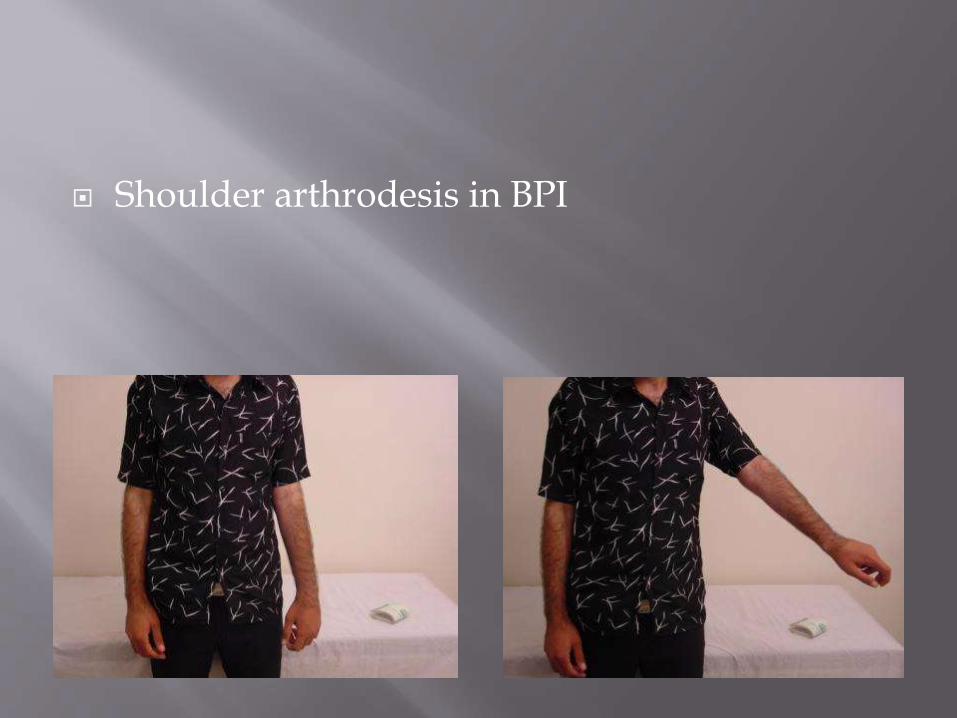
Shoulder arthrodesis in BPI

Neurolysis
Nerve repair
Nerve graft
Nerve transfer
Tendon transfer
Arthrodesis
Functional muscle flaps

Gracillis harvest Accessory n.

First stage of Doi procedure
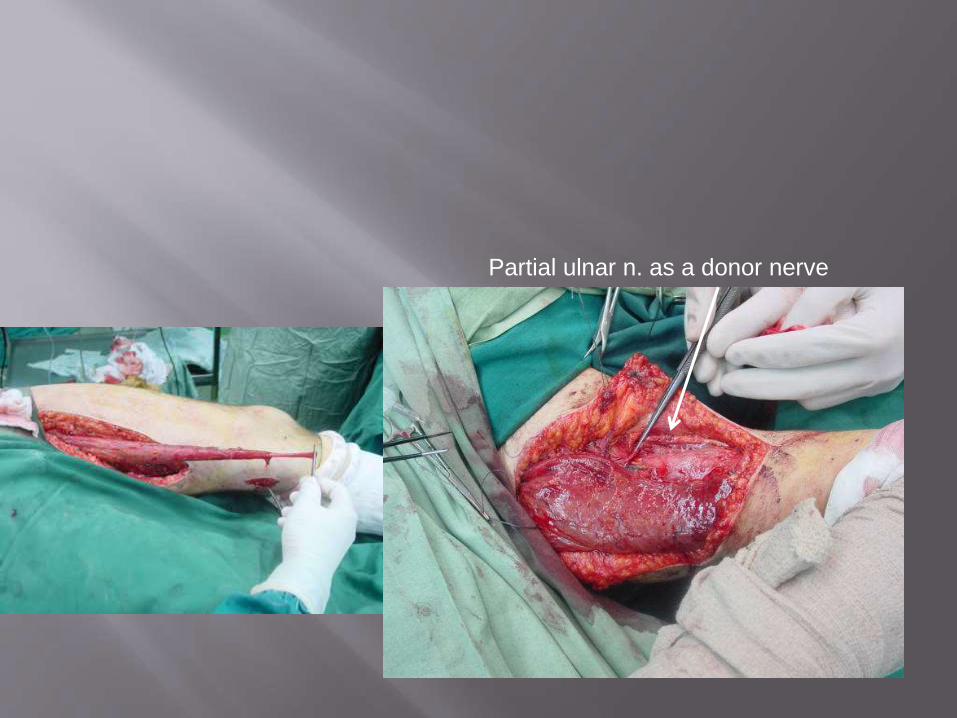
Partial ulnar n. as a donor nerve


Extra plexus donor
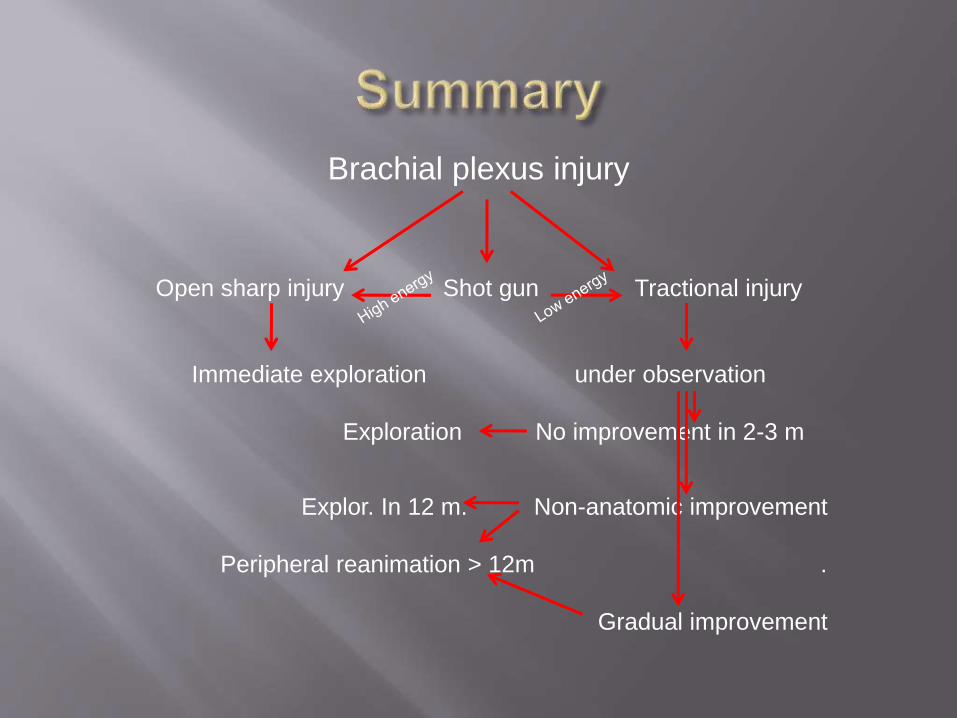
Brachial plexus injury
Open sharp injury Shot gun Tractional injury
Immediate exploration under observation
Exploration No improvement in 2-3 m
Explor. In 12 m. Non-anatomic improvement
Peripheral reanimation > 12m .
Gradual improvement

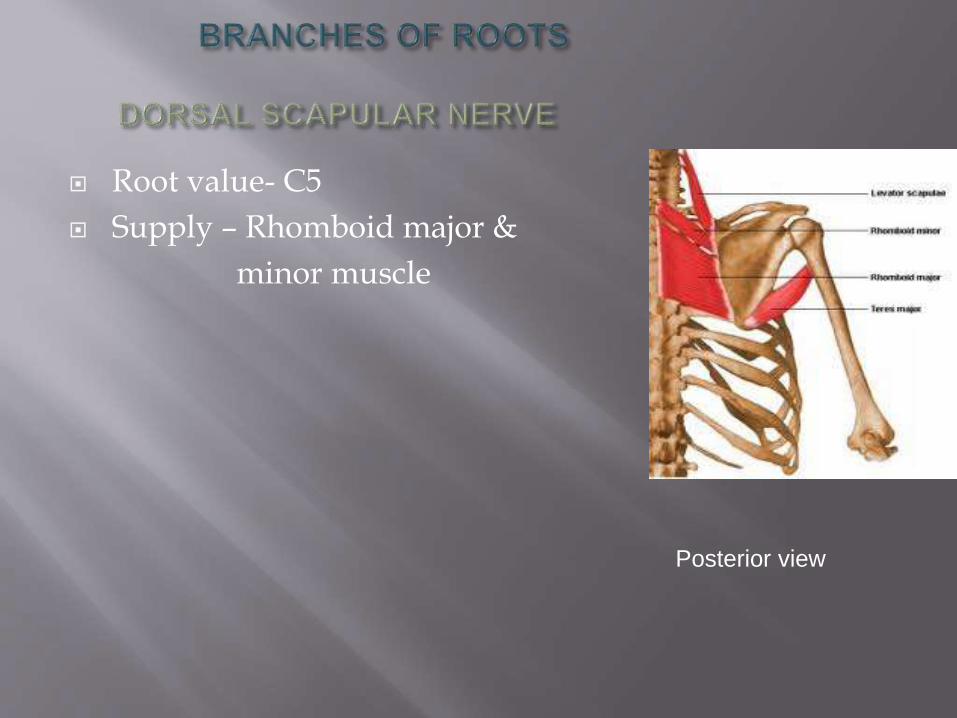
Root value- C5
Supply – Rhomboid major &
minor muscle
Posterior view
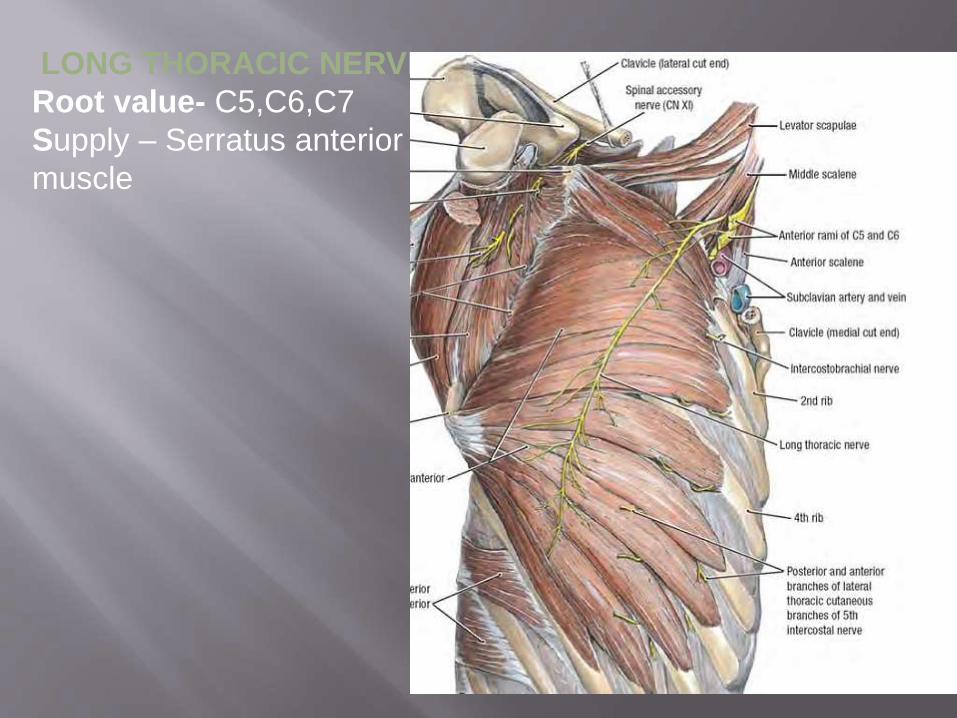
LONG THORACIC NERVE
Root value- C5,C6,C7
Supply – Serratus anterior
muscle
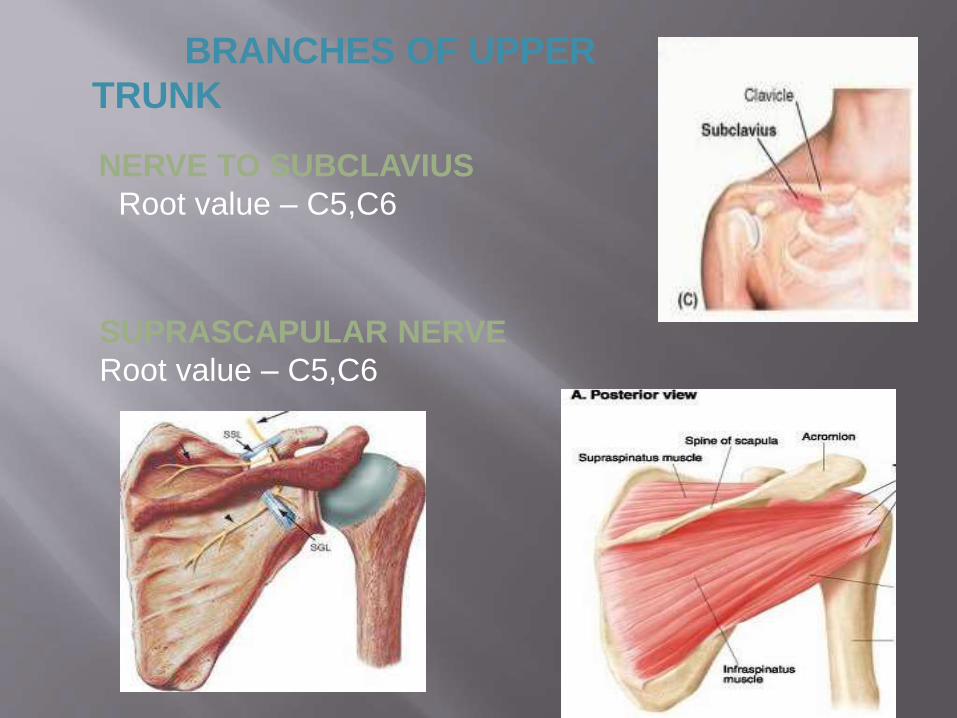
BRANCHES OF UPPER
TRUNK
NERVE TO SUBCLAVIUS
Root value – C5,C6
SUPRASCAPULAR NERVE
Root value – C5,C6
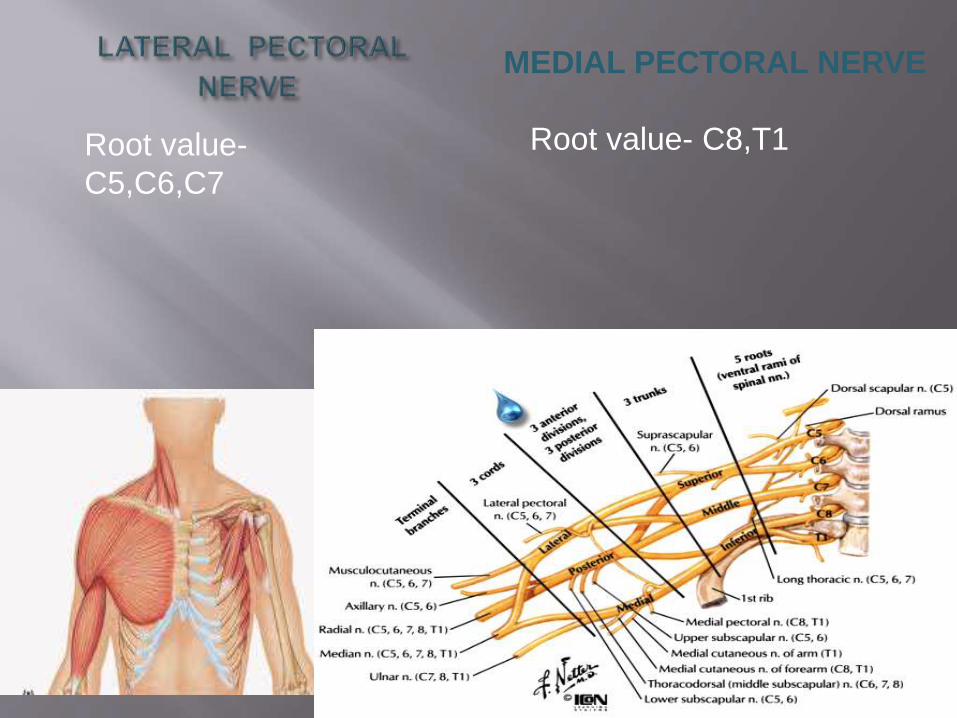
Root value-
C5,C6,C7
MEDIAL PECTORAL NERVE
Root value- C8,T1
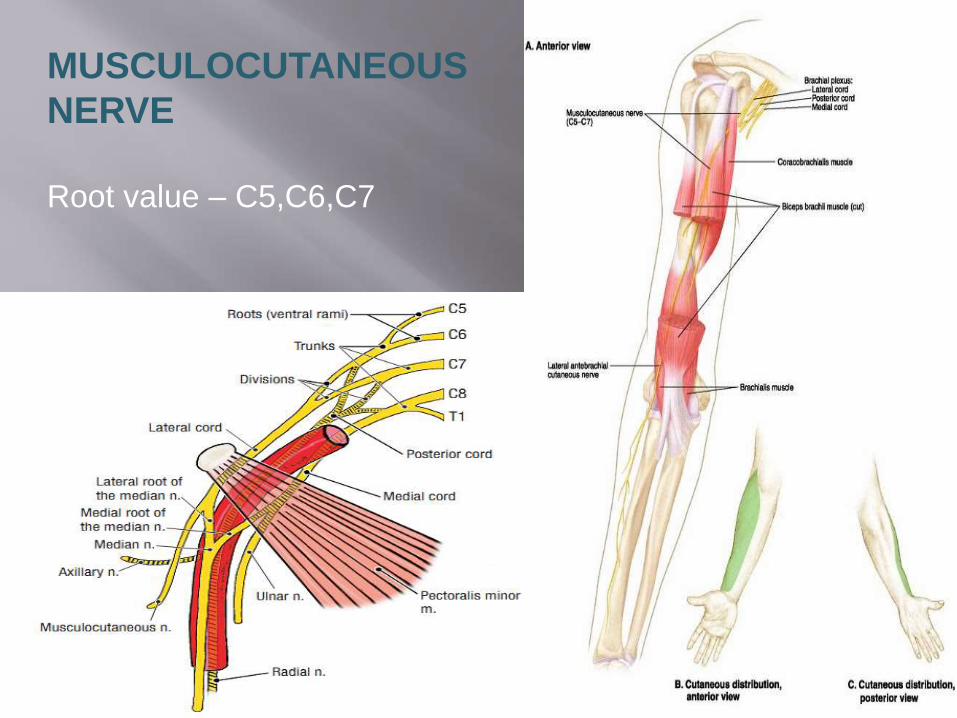
MUSCULOCUTANEOUS
NERVE
Root value – C5,C6,C7
12-88
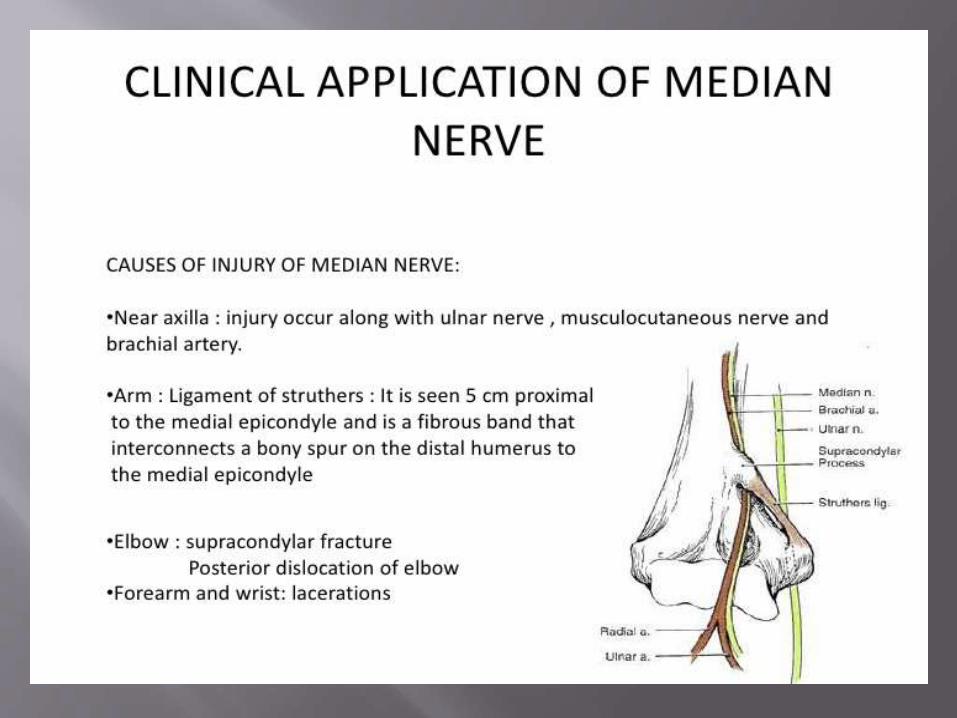
MEDIAN NERVE
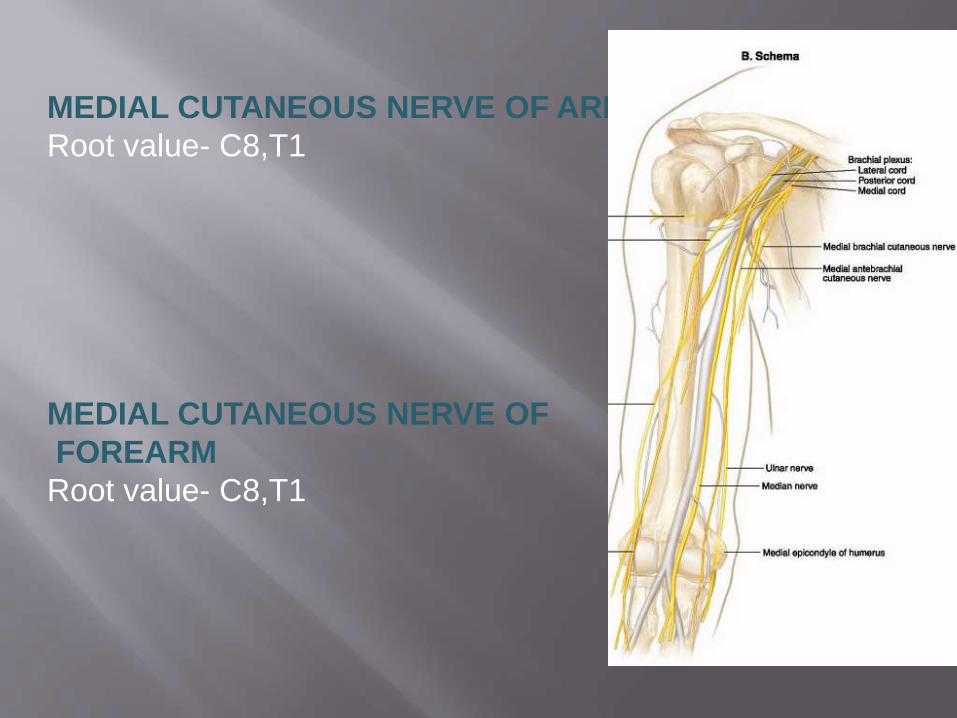
MEDIAL CUTANEOUS NERVE OF ARM
Root value- C8,T1
MEDIAL CUTANEOUS NERVE OF
FOREARM
Root value- C8,T1
12-90
ULNAR NERVE
Root value-(C7),C8,T1
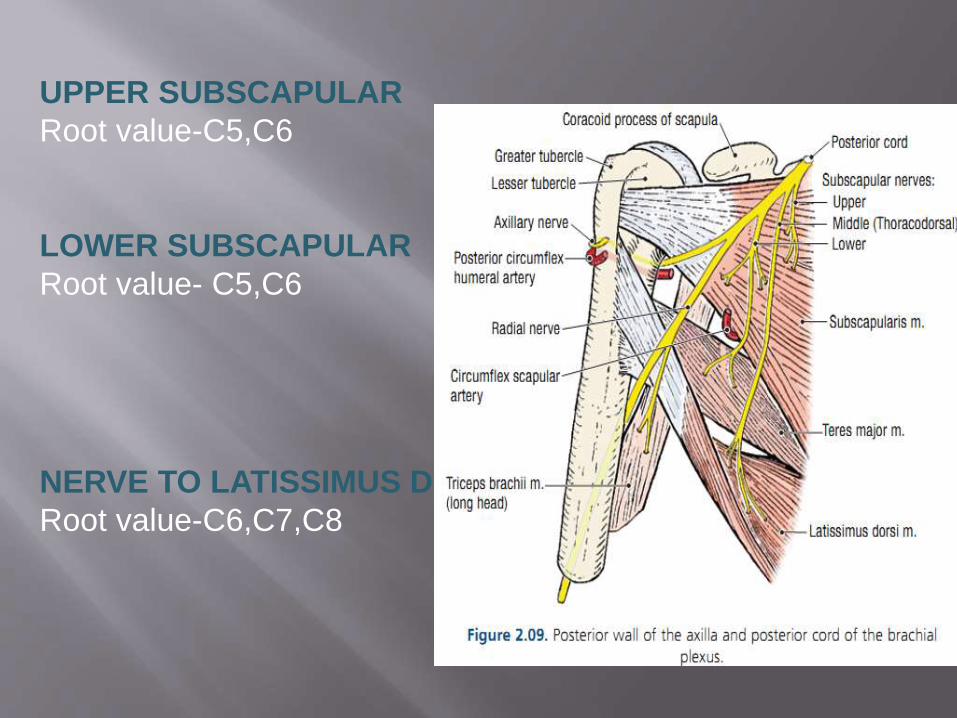
UPPER SUBSCAPULAR
Root value-C5,C6
LOWER SUBSCAPULAR
Root value- C5,C6
NERVE TO LATISSIMUS DORSI
Root value-C6,C7,C8
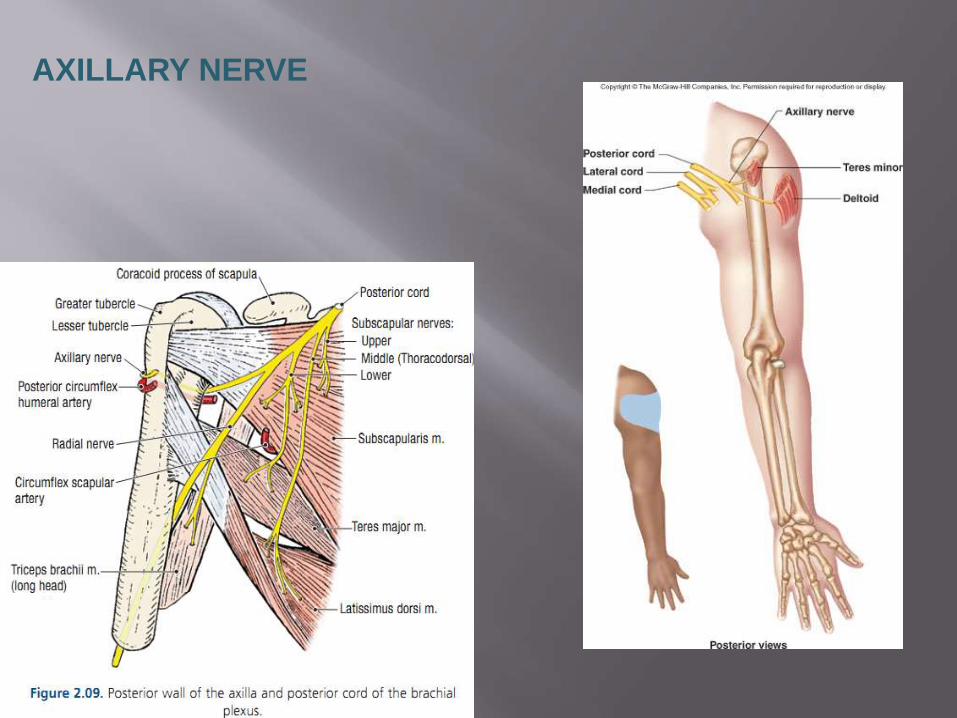
AXILLARY NERVE
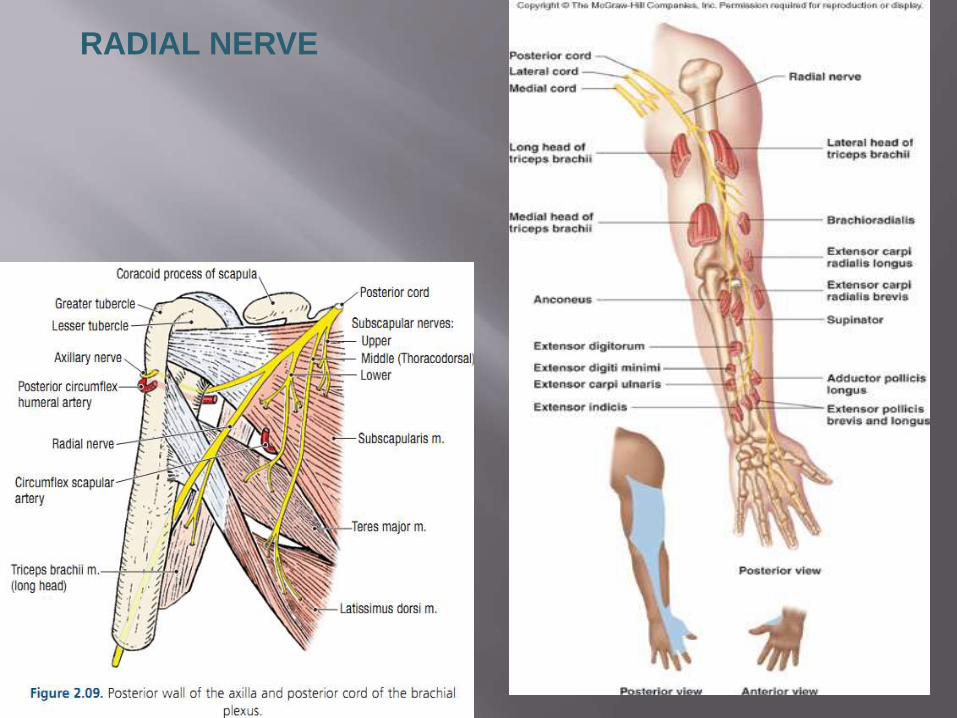
RADIAL NERVE

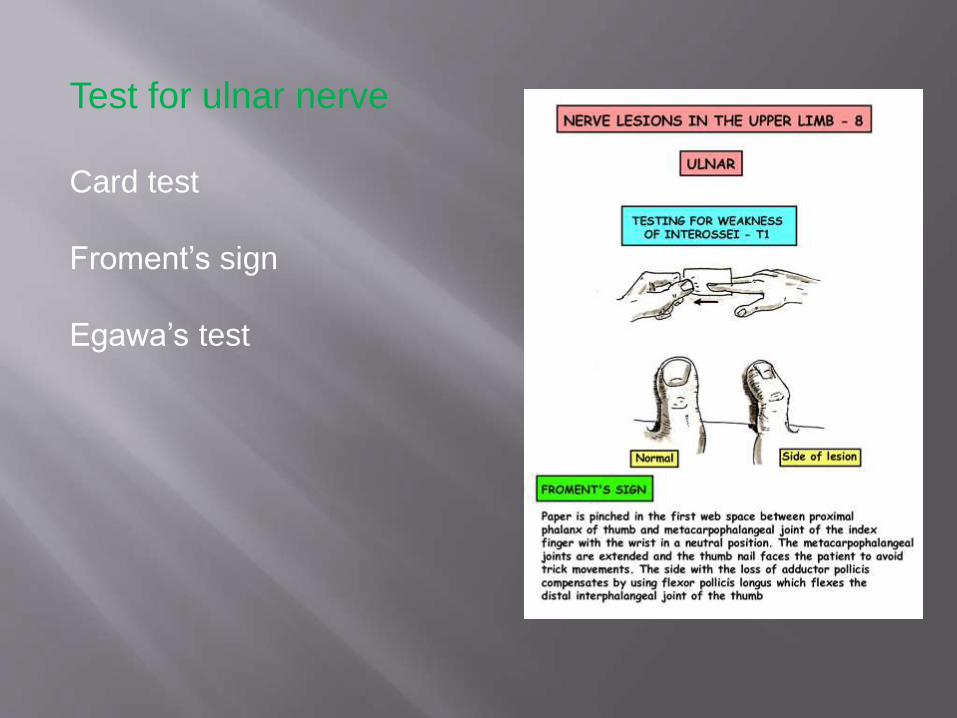
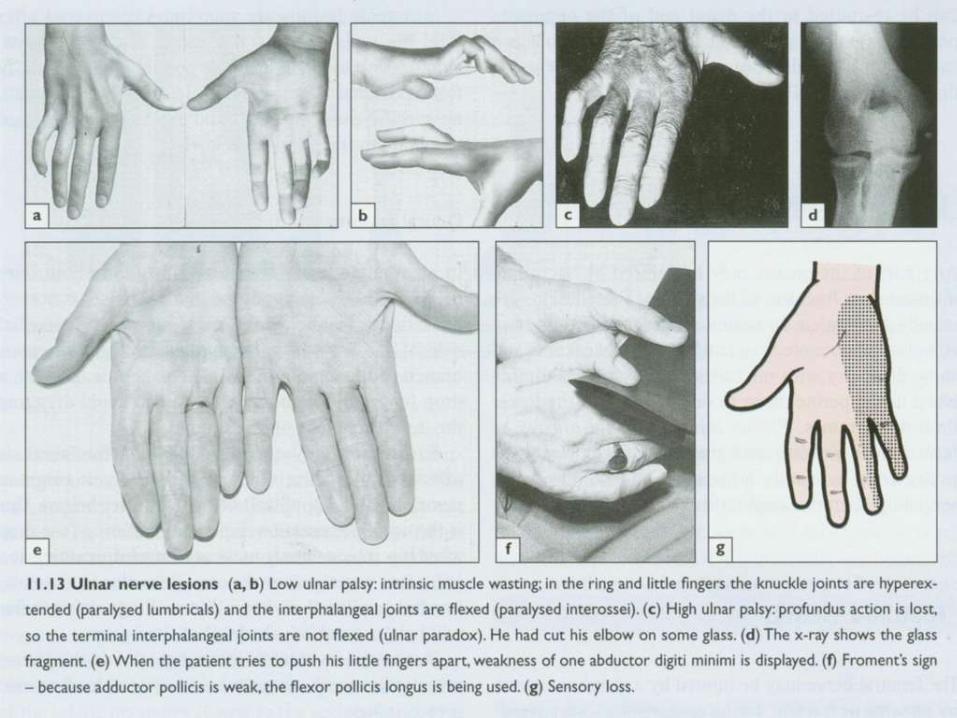
Test for ulnar nerve
Card test
Froment’s sign
Egawa’s test
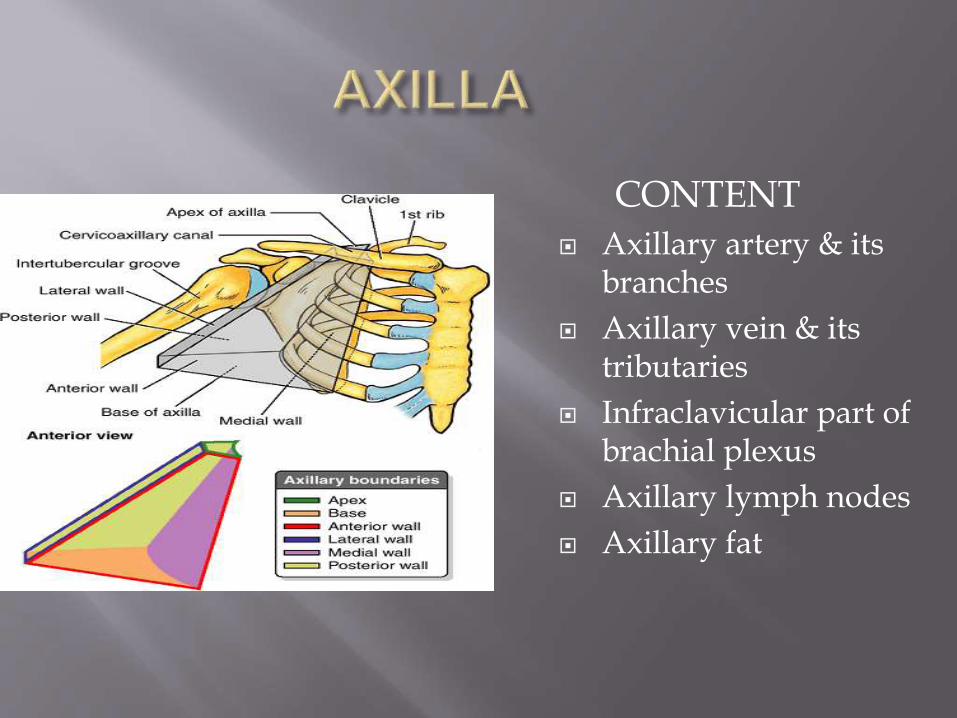
CONTENT
Axillary artery & its branches
Axillary vein & its tributaries
Infraclavicular part of brachial plexus
Axillary lymph nodes
Axillary fat
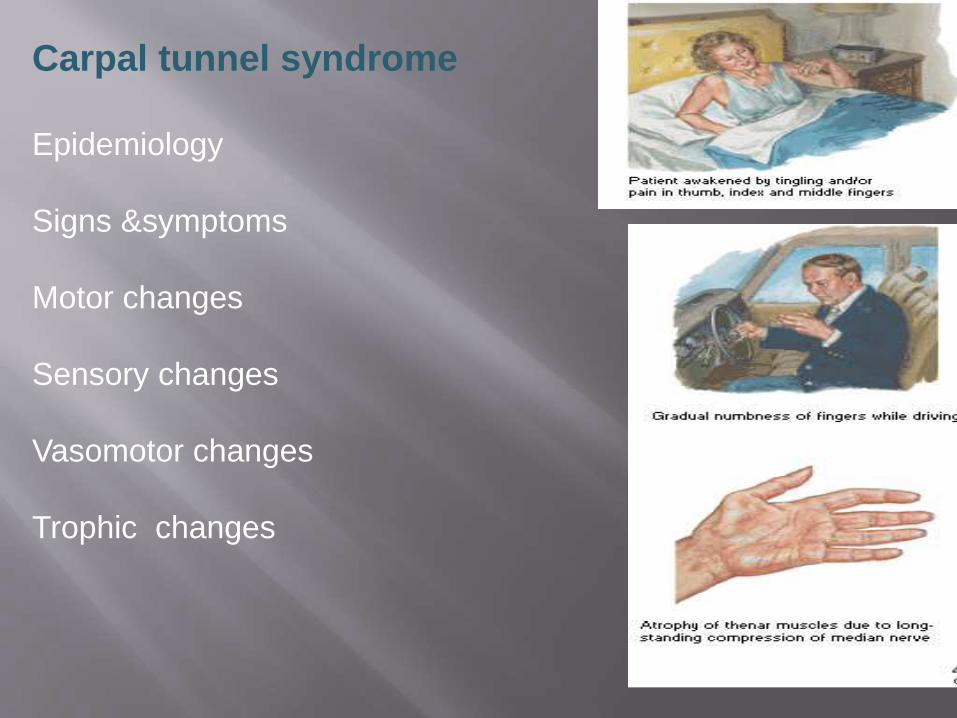
Carpal tunnel syndrome
Epidemiology
Signs &symptoms
Motor changes
Sensory changes
Vasomotor changes
Trophic changes

Tests done
Tinel sign Phalen’s
maneavure
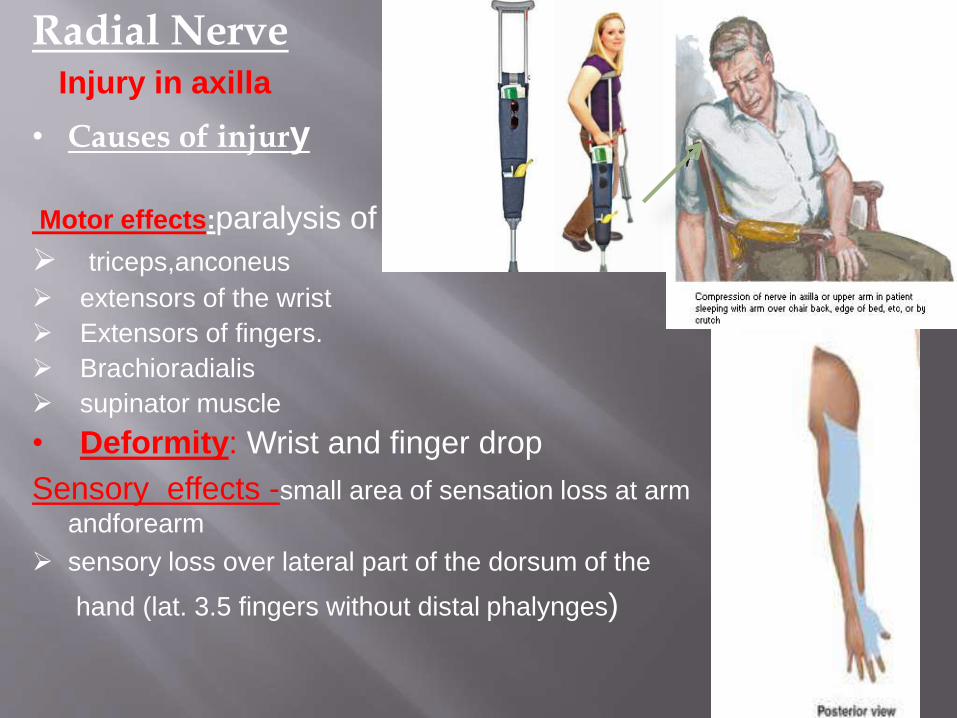
Radial NerveInjury in axilla
• Causes of injury
Motor effects:paralysis of
triceps,anconeus
extensors of the wrist
Extensors of fingers.
Brachioradialis
supinator muscle
• Deformity: Wrist and finger drop
Sensory effects -small area of sensation loss at arm
andforearm
sensory loss over lateral part of the dorsum of the
hand (lat. 3.5 fingers without distal phalynges)
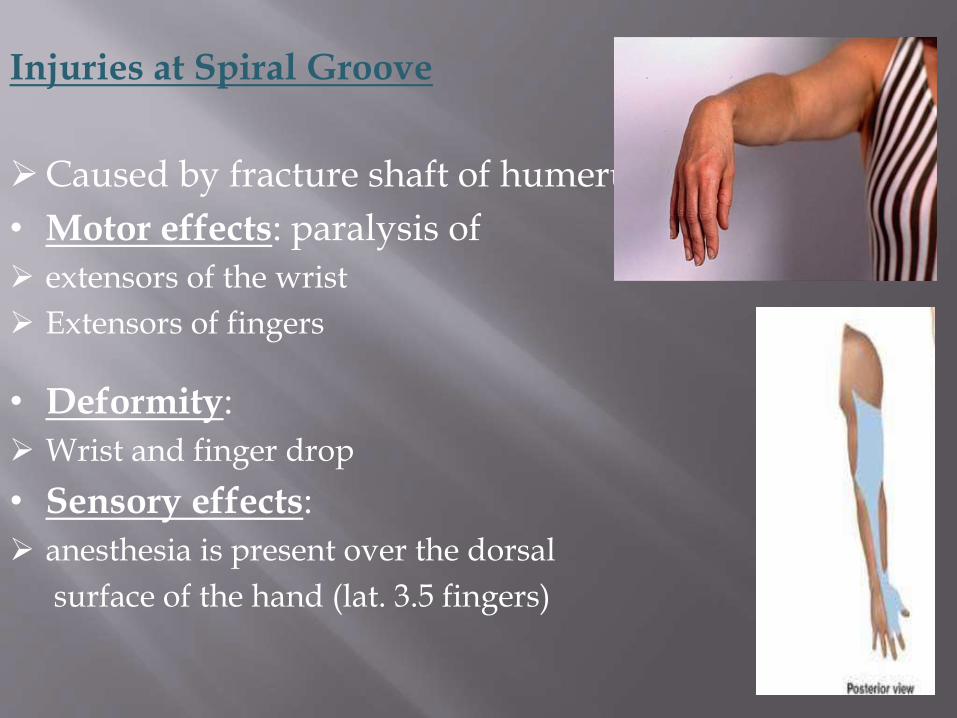
Injuries at Spiral Groove
Caused by fracture shaft of humerus.
• Motor effects: paralysis of
extensors of the wrist
Extensors of fingers
• Deformity:
Wrist and finger drop
• Sensory effects:
anesthesia is present over the dorsal
surface of the hand (lat. 3.5 fingers)
12-105
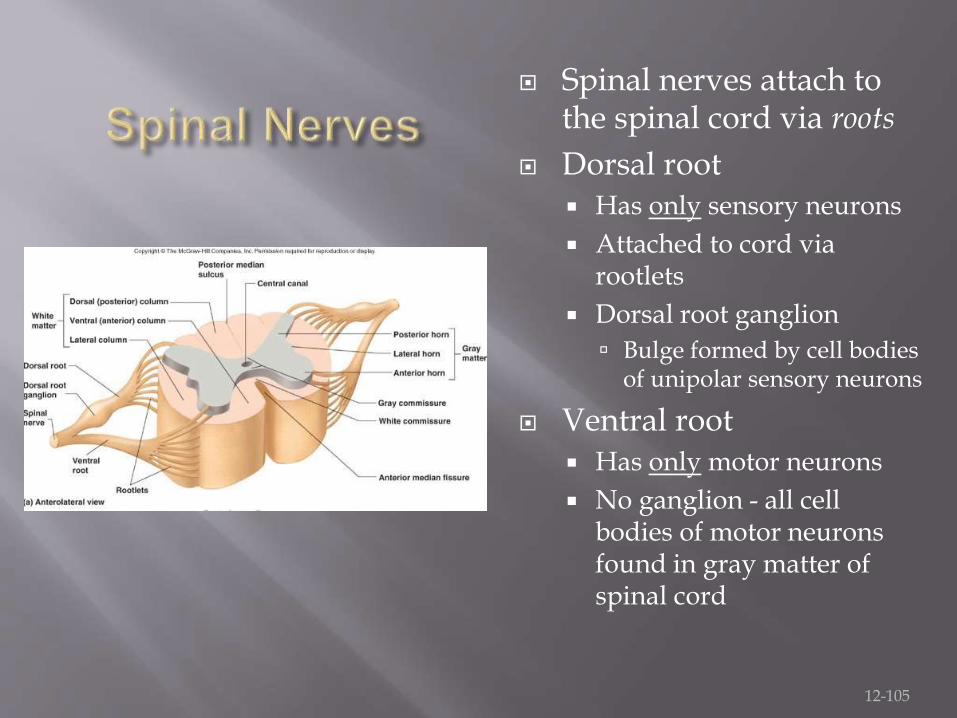
Spinal nerves attach to the spinal cord via roots
Dorsal root Has only sensory neurons
Attached to cord via rootlets
Dorsal root ganglion
Bulge formed by cell bodies of unipolar sensory neurons
Ventral root Has only motor neurons
No ganglion - all cell bodies of motor neurons found in gray matter of spinal cord
12-106
31 pair each contains thousands of nerve fibers
All are mixed nerves have both sensory and motor neurons)
Connect to the spinal cord
Named for point of issue from the spinal cord 8 pairs of cervical nerves (C1-C8)
12 pairs of thoracic nerves (T1-T12)
5 pairs of lumbar nerves (L1-L5)
5 pairs of sacral nerves (S1-S5)
1 pair of coccygeal nerves (Co1)
12-107
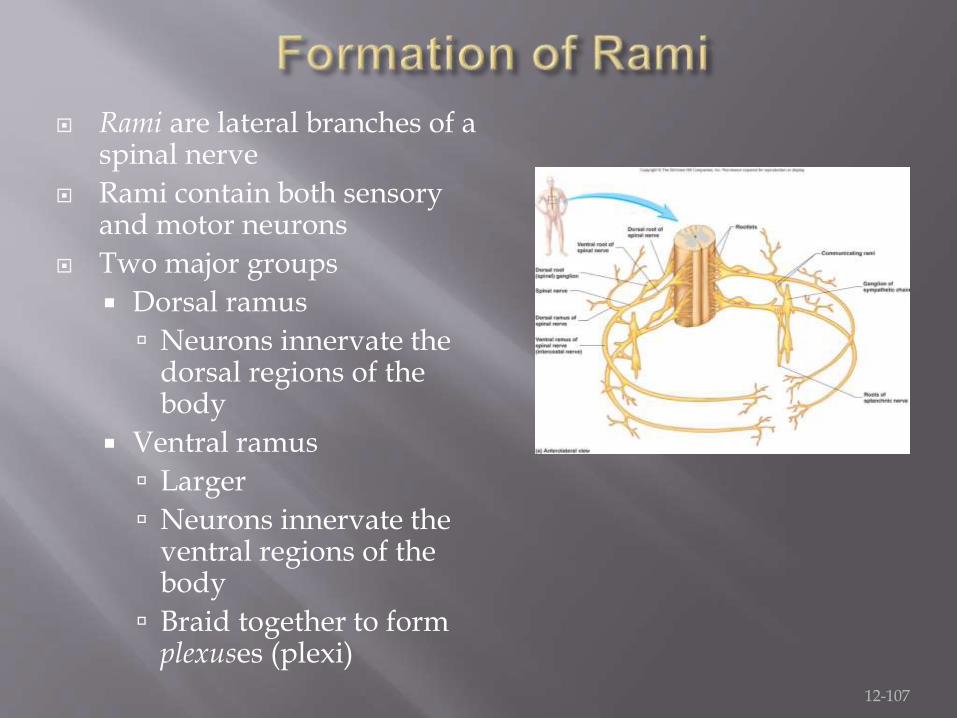
Rami are lateral branches of a spinal nerve
Rami contain both sensory and motor neurons
Two major groups
Dorsal ramus
Neurons innervate the dorsal regions of the body
Ventral ramus
Larger
Neurons innervate the ventral regions of the body
Braid together to form plexuses (plexi)
12-108
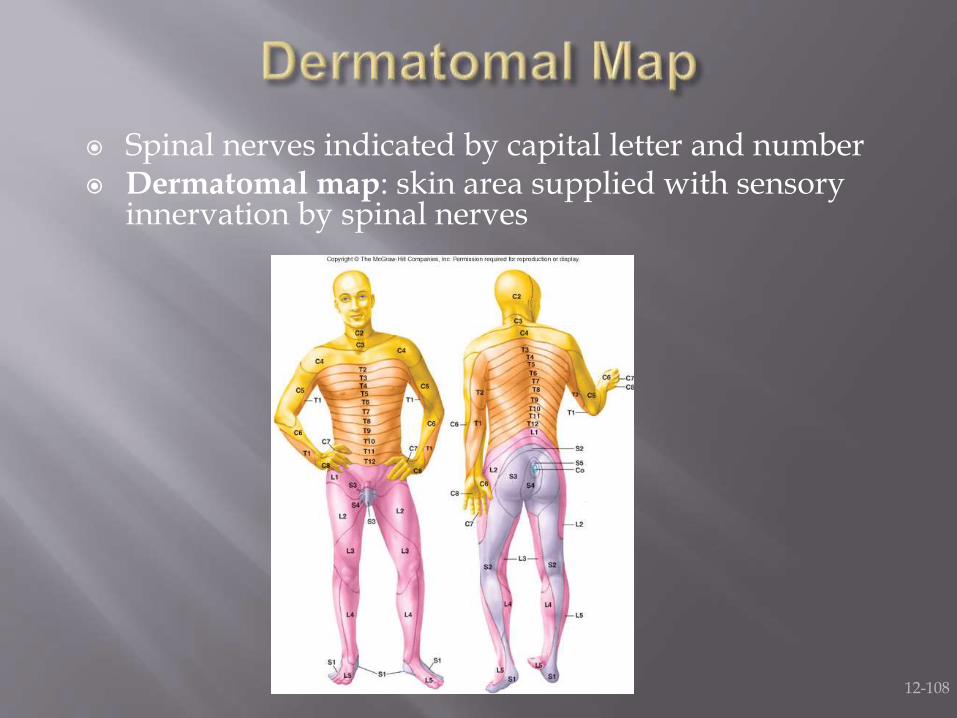
Spinal nerves indicated by capital letter and number Dermatomal map: skin area supplied with sensory
innervation by spinal nerves
12-109
Nerve plexus A network of ventral rami
Ventral rami (except T2-T12) Branch and join with one another
Form nerve plexuses In cervical, brachial, lumbar, and sacral regions
No plexus formed in thoracic region of s.c.
12-110
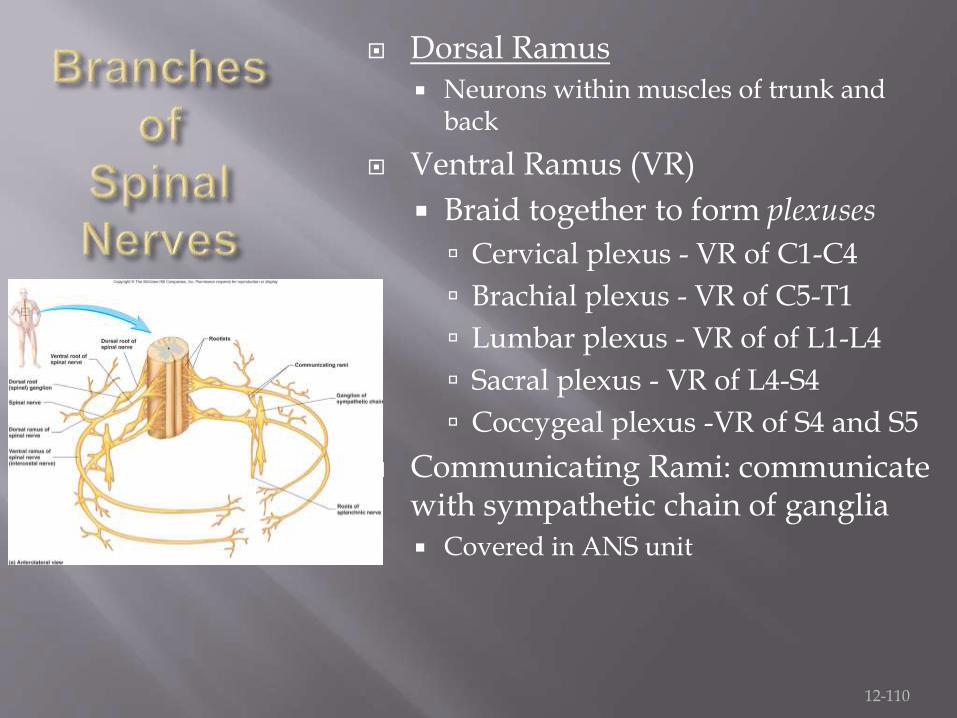
Dorsal Ramus Neurons within muscles of trunk and
back
Ventral Ramus (VR)
Braid together to form plexuses
Cervical plexus - VR of C1-C4
Brachial plexus - VR of C5-T1
Lumbar plexus - VR of of L1-L4
Sacral plexus - VR of L4-S4
Coccygeal plexus -VR of S4 and S5
Communicating Rami: communicate with sympathetic chain of ganglia Covered in ANS unit
12-111
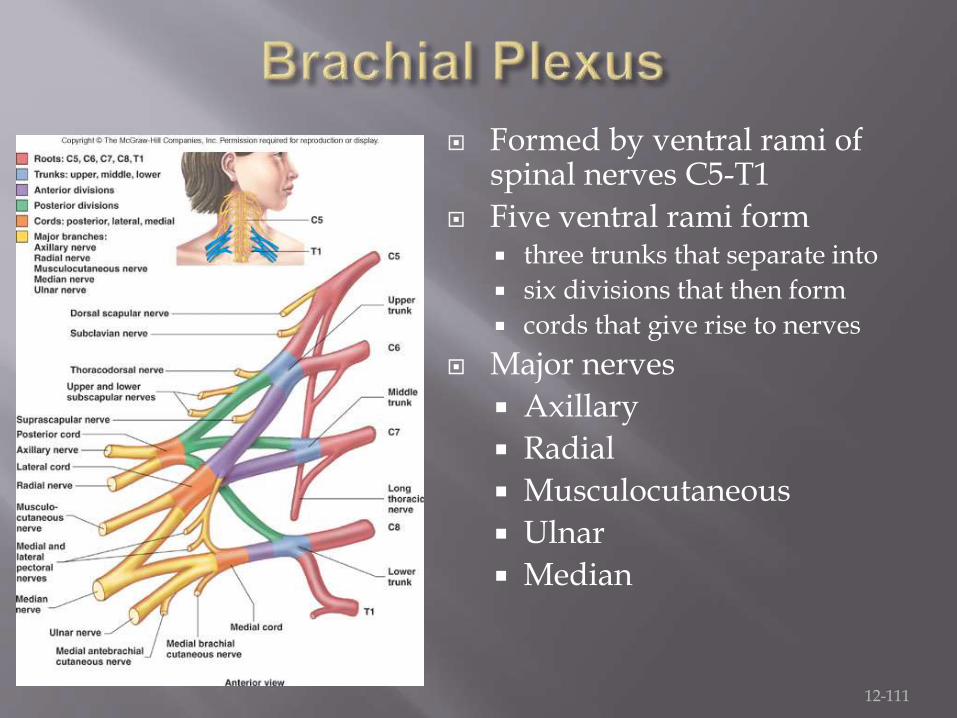
Formed by ventral rami of spinal nerves C5-T1
Five ventral rami form three trunks that separate into
six divisions that then form
cords that give rise to nerves
Major nerves
Axillary
Radial
Musculocutaneous
Ulnar
Median